MARKET Medical Cannabis & Epilepsy - American Botanical ...
84
US/CAN $6.95 The Journal of the American Botanical Council Number 115 | Aug — Oct 2017 Lemon Balm Profile • Field Dispatch: Kesum • Beetroot Juice Research Nigella & Asthma • Saffron & Postpartum Depression HERB M ARKET REPORT Medical Cannabis & Epilepsy Merian THE BOTANICAL ILLUSTRATIONS
-
Upload
khangminh22 -
Category
Documents
-
view
0 -
download
0
Transcript of MARKET Medical Cannabis & Epilepsy - American Botanical ...
US/CAN $6.95
The Journal of the American Botanical Council Number 115 | Aug — Oct 2017
Lemon Balm Profile • Field Dispatch: Kesum • Beetroot Juice ResearchNigella & Asthma • Saffron & Postpartum Depression
HERBMARKET
REPORT
Medical Cannabis& Epilepsy MerianTHE
BOTANICALILLUSTRATIONS

The forces that shaped the southern Oregon landscape endowed it with lofty mountains, sheltered valleys and crystal clear rivers. Blessed with early springs and long summers, a part of this unique region came to be known as Josephine County.
Herb Pharm planted its roots in this rich volcanic soil nearly four decades ago. We’ve been growing organic herbs and making effective liquid extracts with precision and environmental stewardship ever since. As one of the nation’s � rst GMO-free counties, we are happy to make Josephine our home.
Certi� ed organic Echinacea purpurea growing on the Herb Pharm farm.
See how the natural therapeutic properties of plants can bene� t you at www.herb-pharm.com.
Underwriters, Endorsers, and Supporters of the ABC-AHP-NCNPR Botanical Adulterants Program* As of August 11, 2017
*By acknowledging the generous support of these companies and organizations, ABC, AHP, and NCNPR are not endorsing any ingredients or products that may be produced or marketed by them.
Join more than 190 responsible companies, laboratories, nonprofits, trade associations, media outlets, and others in the international herb and natural products/natural medicine community. Become a valued underwriter of the ABC-AHP-NCNPR Botanical Adulterants Program, a multi-year, supply chain integrity program providing education about accidental and intentional adulteration of botanical materials and extracts on an international scale. For more details on joining the program, and access to the free publications produced to date, please see www.botanical adulterants.org or contact Denise Meikel at [email protected].
Financial Underwriters21st Century HealthcareAdvoCare International L.P. Agilent Technologies, Inc.Aloecorp, Inc.Amen ClinicsAmway/Nutrilite Health Institute Artemis International, Inc.Atrium InnovationsAveda CorporationBeachbody, LLCBI NutraceuticalsBioceuticalsBionorica SEBlackmoresBotanical LiaisonsBruker BioSpinCapsugelCepham, Inc.Chemi NutraCNCA HealthComplete Phytochemical
Solutions Crila Healthdicentra, Inc.Doctor’s BestDr. Bronner's Magic SoapsDolCas Biotech, LLCdōTERRA International, LLCDouglas LaboratoriesDraco Natural ProductsECONET, Inc.Emerson EcologicsEnzymatic Therapy, Inc.Ethical Naturals, Inc.Eu Yan Sang InternationalEuroMedEuroMedicaEuroPharmaFlavex Naturextrakte GmbHFlordisFoodState/MegaFoodFruit d’OrGaia HerbsGE Nutrients, Inc.Ginsana SAGlobal Health IndustriesGNC, Inc.Healthy Lifestyle Brands, LLCHelios Corp.Herb PharmHerbalife International, Inc.Horphag ResearchiHerbIndena USA, Inc.Indfrag LimitedIngredient IdentityIxoreal Biomed Inc.Jarrow FormulasKlaire LabsLayn USA, Inc.Linnea Markan Global Enterprises, Inc.Martin Bauer, Inc.MediHerb / Integria HealthcareMetagenics, Inc.Natreon, Inc.Natural Alternatives International,
Inc.
Natural Factors Nutritional Products, Inc.
/Bioclinic NaturalsNatural Grocers by Vitamin
CottageNatural Remedies Pvt. Ltd.Nature's Sunshine ProductsNature's WayNaturetechNaturex, Inc.NBTY, Inc.Nektium Pharma SLNetwork Nutrition – IMCDNew Chapter, Inc.The New Frontier Foundation
Fund of the Greater Cedar Rapids
Community FoundationNingbo Greenhealth
Pharmaceutical Co., Ltd.Novel IngredientsNOW Health GroupNu Skin Enterprises/PharmanexNutraceutical CorpOmniActive Health Technologies,
Inc.Organic IndiaOrtho Molecular ProductsPacific Nutritional Inc.Paragon Laboratories Pathway International Pty LimitedPerrigo CompanyPharmatoka SASPharmavite, LLCPhoenix FormulationsPLT Health Solutions, Inc.Polyphenolics, Division of
Constellation Brands, Inc.Potter’sProTheraPure EncapsulationsRainbow Light Nutritional
SystemsRFI Ingredients, LLCRosenbush and Zimmerman
Family FundSabinsa CorporationSchwabe North AmericaSeroyalSFI ResearchShaklee Corp.Soho Flordis InternationalSOHO Global HealthStandard Process, Inc.Strategic Sourcing, Inc.Thorne Research, Inc.Tishcon Corp.Traditional Medicinals, Inc.TSI GroupUnigenUnivera, Inc.Valensa InternationalV.D.F. FutureCeuticalsVerdure SciencesVitamin ShoppeVitaQuest InternationalWhole Foods MarketZMC-USA
Trade AssociationsAmerican Herbal Products
Association (US)Australian Self Medication
Industry (Australia)Australian Tea Tree Industry
Association (Australia)British Herbal Medicine
Association (UK)Canadian Health Food
Association (Canada)Complementary Medicines
Australia (Australia)Consumer Healthcare Products
Association (US)Council for Responsible Nutrition
(US)International Alliance of Dietary/
Food Supplement Associations (IADSA)
National Animal Supplement Council (US)
Natural Products Association (US)Natural Products New Zealand
(NZ)United Natural Products Alliance
(US)
Nonprofit/Professional Associations
Academy of Integrative Health & Medicine
American Association of Naturopathic Physicians
American Herbalists GuildAmerican Society of
PharmacognosyAOAC International Council of Colleges of
Acupuncture and Oriental Medicine
Homeopathic Pharmacopoeia Convention of the United States
Integrative Healthcare Policy Consortium
Irish Register of Herbalists (IRE)National Institute of Medical
Herbalists (UK)Natural Health Products Research
Society of Canada (NHPRS Canada)
Personalized Lifestyle Medicine Institute
Society for Medicinal Plant and Natural Product Research (GA)
US Pharmacopeia (USP)
Colleges/UniversitiesBastyr UniversityBoucher Institute for
Naturopathic MedicineCenter for Natural Products
Technologies, College of Pharmacy, University of Illinois-Chicago
Hong Kong Baptist University’s School of Chinese Medicine
Maryland University of Integrative Health
National University of Natural Medicine
Southwest College of Naturopathic Medicine
University of Bridgeport College of Naturopathic Medicine
Third-Party Analytical Laboratories
Alkemist LabsAuthenTechnologies LLCBent Creek Institute BotaniCert (France)British Columbia Institute of
TechnologyChromaDex Covance LaboratoriesCreative Accord, LLCEurofins Scientific Inc.Flora Research LabsNSF International PhytoLab (Germany)Spectrix LabsTampa Bay Analytical
MediaAlive Publishing GroupDelicious LivingEngredeaHolistic Primary CareInforma Exhibitions USIntegrator BlogMedia Relations, Inc.Modern Healthcare PractitionerNatural Foods MerchandiserNatural Medicine JournalNatural Products INSIDERNewHope360.comNutraceuticals WorldNutraingredientsUSA.comNutrition Business JournalNutrition Industry ExecutiveNutritional OutlookVitamin RetailerWholeFoods Magazine
Law Firms & Regulatory Consultants
Amin Talati & Upadhye, LLCGreenberg Traurig, LLP (James
Prochnow)Law Office of Holly Bayne, P.C.Robert Forbes & AssociatesSusan Brienza, LLCUllman, Shapiro & Ullman, LLP
Contract Research Organizations
KGK Synergize
Research InstitutesKorean Ginseng Research
InstituteShanghai Research Center for
TCM Modernization/Shanghai Institute of Materia Medica of the Chinese Academy of Sciences
Martin Bauer Inc. | www.martin-bauer-group.us | 300 Harmon Meadow Boulevard, Suite 510 Secaucus, NJ 07094
[email protected] +1 (201) 659 -3100
CUSTOM-MADETEA AND
BOTANICALINGREDIENTS
NORTH AMERICA
TOP SUPPLIER IN
EXPERT ISE
T: 7.375”
T: 10”

This issue contains our annual herb market report, which details 2016 retail sales of herbal dietary supplements in the United States. For the 13th consecutive year, herbal supplement sales continued to climb, reaching an estimated record of almost $7.5 billion. As usual, we have teamed up with colleagues at Nutrition Business Journal and the market research firms SPINS and IRI to provide reliable statistics on the growth of herbal supplement sales in the US and the 40 top-selling herbal supplements in both main-stream and natural retail channels. A tip of the hat to HerbalGram Managing Editor Tyler Smith and colleagues.
The energetic increase in the medical research, application, and acceptance of medical cannabis is based on a variety of increasingly documented safe and effective uses for this plant. Of particular significance is the use of cannabis preparations to treat patients with epilepsy, especially intractable forms of the disease (i.e., forms for which conventional pharmacotherapy has provided little if any relief). HerbalGram Assistant Editor Connor Yearsley has reviewed this compelling subject, including a summary of an important, recently published clinical trial on a clinically tested cannabidiol pharmaceutical preparation.
In this issue, we also introduce a new feature in the Research Reviews section: “Study Details: At a Glance.” This informative element will include key study details (e.g., number of subjects, study length and design, descriptions of herbal and placebo interventions, etc.) for each summarized journal article.
The prolific team of ABC’s Gayle Engels and Traditional Medicinals’ Josef Brinckmann has contributed a profile on the popular, utilitarian, and tasty herb lemon balm, a member of the mint family that has traditional and modern uses for improving digestion, as a mild sedative, and more. This is the 49th profile we’ve published in HerbalGram.
We appreciate Betsy Kruthoffer, cataloger and rare book librarian at the Lloyd Library in Cincinnati, Ohio — the largest medicinal plant reference book library in the Western hemi-sphere — for providing a narrative on the classic plant and insect paintings of German-born artist Maria Sibylla Merian (1647-1717). We are also grateful to the Lloyd Library for permis-sion to reprint these beautiful, naturalistic, and historic paintings.
Also in this issue is a field report from our good friend Medicine Hunter Chris Kilham on the Southeast Asian herb kesum. During a recent excursion to Malaysia, Kilham spoke with farmers, chefs, traditional healers, and others about the many ways in which this popu-lar botanical is used. Kilham generously provided multiple videos that accompany the online version of this article, which is available on ABC’s website.
While there are many responsible, ethical companies in the industry that supply high-qual-ity ingredients and make reliable products, there are also those — hopefully, a small minority — who, unfortunately, do not. Guest contributor Karen Raterman has profiled the Emerson Quality Program (EQP), which was developed by Emerson Ecologics, a wholesale distributor of dietary supplements and other health products exclusively for licensed health professionals. This self-regulatory program was designed to ensure that Emerson can rely on the authenticity of the ingredients in the products it distributes.
Finally, we fondly remember Bill Brevoort, an extraordinary man and pioneering champion of Chinese medicinal herbs in North America. An herbalist, scholar, mentor, friend, and much more, Bill inspired me when I started on the herbal path in the early 1970s. He had a positive influence on the lives of thousands, possibly millions, of people who rely on herbal formulas today.
www.herbalgram.org • 2017 • I S S U E 115 • 3
American Botanical Council
Mark Blumenthal Founder, Executive Director HerbalGram Editor-in-Chief
Hannah Bauman HerbalGram Associate Editor
Toby Bernal Head Gardener
Janie Carter Membership Coordinator
Caroline Caswell Assistant Gardener
Gayle Engels Special Projects Director
Stefan Gafner, PhD Chief Science Officer
Tanya Garduño Communications &
Marketing Coordinator
Lori Glenn HerbClip Managing Editor
Matthew Magruder Art Director
Denise Meikel Development Director
Anna Moreno Executive Assistant
Jenny Perez Education Coordinator
Tamarind Reaves HerbClip Assistant Editor HerbalGram Copy Editor
Perry Sauls Customer Service
Coordinator
Tyler Smith HerbalGram Managing Editor
Cecelia Thompson Finance Coordinator
Margaret Wright Accounting Coordinator
Connor Yearsley HerbalGram Assistant Editor
Mission: Provide education using science-based and
traditional information to promote responsible
use of herbal medicine—serving the public, researchers, educators, healthcare
professionals, industry, and media.
dear reader
Martin Bauer Inc. | www.martin-bauer-group.us | 300 Harmon Meadow Boulevard, Suite 510 Secaucus, NJ 07094
[email protected] +1 (201) 659 -3100
CUSTOM-MADETEA AND
BOTANICALINGREDIENTS
NORTH AMERICA
TOP SUPPLIER IN
EXPERT ISE
T: 7.375”
T: 10”

4 • I S S U E 115 • 2017 • www.herbalgram.org
ABC Advisory Board Each issue of HerbalGram is peer reviewed by members of the ABC Advisory Board and other qualified experts before publication.
4 • I S S U E 115 • 2017 • www.herbalgram.org
Donald I. Abrams, MD Professor of Clinical Medicine University of California San Francisco San Francisco, CA
Hamid-Reza Adhami, PhD, PharmD Assistant Professor, Dept. of Pharmacognosy Tehran University of Medical Sciences Tehran, Iran
Bharat (Bart) B. Aggarwal, PhD Founding Director Inflammation Research Institute San Diego, CA
Lise Alschuler, ND Naturopathic Specialists, Chicago, IL
Cindy K. Angerhofer, PhD Executive Director of Botanical Research, Aveda Minneapolis, MN
Giovanni Appendino, PhD Professor of Pharmaceutical Sciences University of Eastern Piedmont, Novara, Italy
Wendy L. Applequist, PhD Associate Curator, William L. Brown Center Missouri Botanical Garden, St. Louis, MO
John Thor Arnason, PhD Professor, Dept. of Biology, University of Ottawa Ottawa, ON, Canada
Gary N. Asher, MD, MPH Assistant Professor of Family Medicine University of North Carolina, Chapel Hill, NC
Valerie A. Assinewe, PhD NVision Insight Group, Inc. Ottawa, ON, Canada
Dennis V. C. Awang, PhD, FCIC MediPlant Natural Products Consulting Services Ottawa, ON, Canada
Joanne Barnes, PhD Associate Professor in Herbal Medicines School of Pharmacy, University of Auckland Auckland, New Zealand
Bruce Barrett, MD, PhD Associate Professor of Family Medicine University of Wisconsin-Madison Medical School Madison, WI
Marilyn Barrett, PhD Pharmacognosy Consulting Service Mill Valley, CA
K. Hüsnü Can Başer, PhD Professor of Pharmacognosy Faculty of Pharmacy, Near East University Nicosia, Northern Cyprus
Rudolf Bauer, PhD Department of Pharmacognosy Institute of Pharmaceutical Sciences University of Graz, Austria
Ezra Bejar, PhD Computational Science Research Center San Diego State University, San Diego, CA
Stacey J. Bell, DSc Nutritional Consultant Belmont, MA
Bradley C. Bennett, PhD Professor of Biology, Florida International University, Miami, FL
Alan Bensoussan, PhD Director, National Institute of Complementary Medicine, University of Western Sydney Sydney, Australia
Chantal Bergeron, PhD Manager of Research and Development Personal and Home Care Products, Seventh Generation Burlington, VT
Lori L. Bestervelt, PhD Executive VP and Chief Technical Officer NSF International Ann Arbor, MI
Joseph M. Betz, PhD Director, Analytical Methods and Reference Materials, Office of Dietary Supplements US National Institutes of Health Bethesda, MD
John A. Beutler, PhD Associate Scientist, Molecular Targets Lab National Cancer Institute, Frederick, MD
Keith I. Block, MD Medical and Scientific Director, Block Center for Integrative Cancer Treatment, Skokie, IL
Jeffrey B. Blumberg, PhD, FASN, FACN, CNS-S Professor, Friedman School of Nutrition Science and Policy; Senior Scientist, Antioxidants Research Laboratory, Tufts University Boston, MA
Robert Alan Bonakdar, MD Director of Pain Management Scripps Center for Integrative Medicine La Jolla, CA
Kerry Bone Director, Research and Development Integria Healthcare Warwick, Australia
Heather Boon, BScPhm, PhD Dean, Leslie Dan Faculty of Pharmacy University of Toronto Toronto, Ontario, Canada
Nancy L. Booth, PhD Bethesda, MD
Deni Bown Manager, International Institute of Tropical Agriculture Forest Project Ibadan, Nigeria
Thomas Brendler Founder/CEO, PlantaPhile Collingswood, NJ
Josef Brinckmann Research Fellow, Medicinal Plants & Botanical Supply Chain, Traditional Medicinals, Inc. Sebastopol, CA
Francis Brinker, ND Clinical Assistant Professor, Dept. of Medicine Arizona Center for Integrative Medicine University of Arizona, Tucson, AZ
Donald J. Brown, ND Natural Product Research Consultants Seattle, WA
Paula N. Brown, PhD Director of Applied Research in Biosciences British Columbia Institute of Technology Burnaby, BC, Canada
Veronika Butterweck, PhD Associate Professor, School of Life Sciences Institute for Pharma Technology, University of Applied Sciences Northwestern Switzerland Muttenz, Switzerland
John H. Cardellina II, PhD Reeves Group Virginia Beach, VA
Thomas J.S. Carlson, MS, MD Associate Adjunct Professor, Dept. of Integrative Biology; Director, Center for Health, Ecology, Biodiversity, & Ethnobiology; Curator of Ethnobotany, University and Jepson Herbaria; University of California, Berkeley, CA
Nadja Cech, PhD Associate Professor, Department of Chemistry and Biochemistry, The University of North Carolina Greensboro, Greensboro, NC
Il-Moo Chang, PhD Director, Korea-China Collaboration Center for Traditional Oriental Medicine Research; Professor Emeritus, Seoul National University, Seoul, Korea
Robert G. Chapman, PhD Principal Research Officer, Aquatic & Crop Resource Development, National Research Council Canada Charlottetown, PEI, Canada
Chun-Tao Che, PhD Norman R. Farnsworth Professor of Pharmacognosy, University of Illinois at Chicago College of Pharmacy, Chicago, IL
Bevin Clare, MS, RH, CNS Interim Program Director of the Masters of Science in Herbal Medicine Program Maryland University of Integrative Health Laurel, MD
Ray Cooper, PhDThe Hong Kong Polytechnic University, Hong Kong; PhytoScience, St Louis, MO
Jerry Cott, PhD Pharmacologist, Silver Spring, MD
Paul Alan Cox, PhD Executive Director, Institute for Ethnomedicine Jackson, WY
Lyle E. Craker, PhD Professor, Medicinal Plant Program University of Massachusetts Amherst, MA
Amanda McQuade Crawford Clinical Psychotherapist & Medical Herbalist PhytoHumana (Integrative Health Practice) Ojai, CA
Edward M. Croom, Jr., PhD Adjunct Associate Professor of Pharmacognosy University of Mississippi Oxford, MS
Muriel Cuendet, PhD Associate Professor, School of Pharmaceutical Sciences, University of Geneva and the University of Lausanne, Geneva, Switzerland
Alan M. Dattner, MD Founder, HolisticDermatology.com Manhattan and New Rochelle, NY
Wade Davis, PhD BC Leadership Chair in Cultures & Ecosystems at Risk, Professor of Anthropology, & Faculty Associate, Liu Institute for Global Issues University of British Columbia, Vancouver, BC, Canada
Steven Dentali, PhD Botanical Industry Consultant Redondo Beach, CA
Subhuti Dharmananda, PhD Director, Institute for Traditional Medicine Portland, OR
Hardy Eshbaugh, PhD Professor Emeritus, Miami University Oxford, OH
Trish Flaster, MS Executive Director, Botanical Liaisons, LLC Boulder, CO
Paula M. Gardiner, MD, MPH Assistant Professor, Dept. of Family Medicine Boston University Medical School, Boston, MA
Zoë Gardner, PhD Research & Development Manager Traditional Medicinals, Sebastopol, CA
Patricia Gerbarg, MD Kingston, NY
Gabriel I. Giancaspro, PhD VP, Foods, Dietary Supplements and Herbal Medicines, United States Pharmacopeia Rockville, MD
Joe Graedon, MS Author, Syndicated Columnist, Radio Host Durham, NC
Mindy Green, MS Green Scentsations Boulder, CO
Frank L. Greenway, MD Medical Director and Professor Pennington Biomedical Research Center of the Louisiana State University System Baton Rouge, LA
Joerg Gruenwald, PhD Founder and Chief Scientific Advisor analyze & realize GmbH, Berlin, Germany
Mimi Guarneri, MD, FACC Founder & Director, Guarneri Integrative Health La Jolla, CA
De-An Guo, PhD Professor, Shanghai Research Center for TCM Modernization, Shanghai Institute of Materia Medica, Shanghai, China
Ameenah Firdaus Gurib-Fakim, PhD President of Mauritius; Director, Centre for Phytotherapy & Research (CEPHYR) Ltd. Cyber City, Ebene, Mauritius
Bill J. Gurley, PhD Professor, College of Pharmacy, University of Arkansas for Medical Sciences, Little Rock, AR
Charlotte Gyllenhaal, PhD Adjunct Assistant Professor of Pharmacognosy College of Pharmacy, University of Illinois at Chicago; Research Program Manager, Block Center for Integrative Cancer Care, Skokie, IL
Pierre S. Haddad, PhD Professor of Pharmacology Université de Montréal Montreal, Quebec, Canada
Mary Hardy, MD George Washington Master’s in Integrative Medicine; Wellness Works Valley Village, CA
James Harnly, PhD Research Leader, Food Composition and Methods Laboratory, Agricultural Research Service, US Department of Agriculture, Beltsville, MD
Michael Heinrich, Dr. rer. nat. habil. Professor and Cluster Lead, Research Cluster Biodiversity & Medicines, UCL School of Pharmacy London, UK
Christopher Hobbs, PhD, LAc, AHG Research Scientist, Herbalist, Author Davis, CA

www.herbalgram.org • 2017 • I S S U E 115 • 5www.herbalgram.org • 2017 • I S S U E 115 • 5
Freddie Ann Hoffman, MDCEO and Managing Member, HeteroGeneity, LLC Washington, DC
David Hoffmann, BSc, FNIMH Medical Herbalist, Author, and Research Associate Traditional Medicinals Sebastopol, CA
Tori Hudson, ND Clinical Professor, National University of Natural Medicine, Portland, OR
Maurice M. Iwu, PhD President, Bioresources Development and Conservation Programme Wuse District, Abuja, Nigeria
Holly E. Johnson, PhD Laboratory Director, Alkemist Labs Costa Mesa, CA
Edward Kennelly, PhD Associate Professor and Chair, Dept. of Biological Sciences, Lehman College, City University of New York, Bronx, NY
Ikhlas Khan, PhD Research Professor of Pharmacognosy, Director, National Center for Natural Products Research University of Mississippi, Oxford, MS
Steven King, PhD EVP, Sustainable Supply, Ethnobotanical Research, and IP, Jaguar Animal Health San Francisco, CA
Richard Kingston, PharmD, CSPI President, Regulatory and Scientific Affairs, Safety Call International Poison Center; Professor, Dept. of Experimental & Clinical Pharmacology, University of Minnesota, Minneapolis, MN
Uwe Koetter, PhD Principal and Founder, Dr. Koetter Consulting Services, Uttwil, Switzerland
David Kroll, PhD President, Calluna Communications LLC Raleigh, NC
Thomas L. Kurt, MD, MPH Adjunct Professor of Emergency Medicine University of Texas Southwestern Medical Center Dallas, TX (Based in Aspen, CO)
Danna J. Leaman, PhD Conservation Biologist and Ethnobotanist Canadian Museum of Nature Ottawa, Ontario, Canada
Roberta A. Lee, MD Pantano Physician Offices University of Arizona, Tucson, AZ
Susan Leopold, PhD Executive Director, United Plant Savers East Barre, VT
Martha M. Libster, PhD, MSN, APRN-CNS, APHN-BC Associate Dean of Nursing, University of Wisconsin - Oshkosh, Oshkosh, Wisconsin
Tieraona Low Dog, MDInterprofessional Fellowship Director Academy of Integrative Health & Medicine La Jolla, CA
Douglas “Duffy” MacKay, ND Vice President, Scientific & Regulatory Affairs Council for Responsible Nutrition Washington, DC
Robin J. Marles, PhD Senior Scientific Advisor, Nutrition Premarket Assessment Division, Bureau of Nutritional Sciences, Health Canada, Ottawa, ON, Canada
Rachel Mata, PhD Professor of Pharmacognosy Universidad Nacional Autónoma de Mexico Mexico City, Mexico
Will C. McClatchey, PhD Thousand Arbor Refuge Eugene, OR
Joe-Ann McCoy, PhD Director, Medicinal Germplasm Repository Bent Creek Institute / NCSU Asheville, NC
Dennis J. McKenna, PhD Assistant Professor, Center for Spirituality & Healing, University of Minnesota Minneapolis, MN
John McPartland, DO Private Practice Vermont Alternative Medicine, Inc. Middlebury, VT
Mark Messina, PhD, MS President, Nutrition Matters, Inc. Eau Claire, WI
Marc S. Micozzi, MD, PhD Private Practice in Forensic Medicine; Policy Institute for Integrative Medicine Bethesda, MD
Simon Y. Mills Senior Teaching Fellow Peninsula Medical School, Exeter, UK
Daniel E. Moerman, PhD William E. Stirton Emeritus Professor of Anthropology, University of Michigan-Dearborn Dearborn, MI
William Morris, PhD, DAOM, LAc President Emeritus, AOMA Graduate School of Integrative Medicine, Austin, TX
Susan Murch, PhD Associate Professor and Canada Research Chair in Natural Products Chemistry, University of British Columbia-Kelowna, Kelowna, BC, Canada
James Neal-Kababick Founder and Director Flora Research Laboratories, Grants Pass, OR
Nicholas H. Oberlies, PhD Associate Professor, Dept. of Chemistry and Biochemistry, University of North Carolina at Greensboro, Greensboro, NC
Andrea Ottesen, PhD Research Area Coordinator for Metagenomics Division of Microbiology/Center for Food Safety and Applied Nutrition/FDA; Adjunct Assistant Professor/Plant Sciences and Landscape Architecture/UMD, College Park, MD
Alexander Panossian, PhD Science and Research Director, Europharma USA Green Bay, WI
Guido F. Pauli, PhD, FAPA Professor and Associate Director, Department of Medicinal Chemistry and Institute for Tuberculosis Research, University of Illinois at Chicago Chicago, IL
Joseph E. Pizzorno, Jr., ND President Emeritus, Bastyr University; Editor, Integrative Medicine: A Clinician's Journal Seattle, WA
Mark J. Plotkin, PhD Executive Director, Amazon Conservation Team Arlington, VA
G.N. Qazi, PhD Vice Chancellor, Hamdard University New Delhi, India
John Rashford, PhD Professor of Anthropology College of Charleston, Charleston, SC
Danica Harbaugh Reynaud, PhD Global Director of Scientific Innovation, NSF International; Founder, AuthenTechnologies Richmond, CA
John M. Riddle, PhD Professor, Department of History North Carolina State University, Raleigh, NC
Eloy Rodriguez, PhD James A. Perkins Endowed Professor, Research Scientist, Ethnobotanical Medicine and Zoopharmacognosy, Cornell University Ithaca, NY
Aviva Romm, MD Boston, MA
Robert Rountree, MD Practitioner, Boulder Wellcare Inc. Boulder, CO
Ethan B. Russo, MD Medical Director, Phytecs Los Angeles, CA
Jerome Sarris, PhD Professor of Integrative Mental Health Deputy Director, National Institute of Complementary Medicine, Western Sydney University, Penrith, NSW, Australia
Ric Scalzo Founder & CEO Gaia Herbs, Inc., Brevard, NC
Alexander G. Schauss, PhD, FACN, CFS Senior Research Director and CEO, Natural and Medicinal Products Research, AIBMR Life Sciences, Puyallup, WA
Paul Schulick Founder and Formulator, New Chapter, Inc.Brattleboro, VT
Navindra Seeram, PhD Associate Professor of Pharmacognosy University of Rhode Island College of Pharmacy Kingston, RI
Holly Shimizu Consultant, Writer, and Lecturer Former Executive Director, US Botanic Garden First Curator, The National Herb Garden Glen Echo, MD
Victor Sierpina, MD Associate Professor of Family Practice Medicine University of Texas Medical Branch, Galveston, TX
James E. Simon, PhD Professor, Director of the Center for New Use Agriculture and Natural Plant Products Rutgers University, New Brunswick, NJ
Ed Smith Co-founder, Herb Pharm Williams, OR
Michael Smith, ND, BPharm Natural Products Consultant Stratford, ON, Canada
S. H. Sohmer, PhD Alexandria, VA
Paul Stamets, DSc Director of Research, Fungi Laboratories Fungi Perfecti, LLC, Olympia, WA
Natascha Techen, PhD Senior Research Scientist National Center for Natural Products Research University of Mississippi, Oxford, MS
Michael S. Tempesta, PhD Managing Partner and Founder, Phenolics, LLC El Granada, CA
Barbara N. Timmermann, PhD Chairperson-Professor of Medicinal Chemistry University of Kansas Lawrence, KS
Michael Tims, PhD Academic Director of Herbal Programs Maryland University of Integrative Health Laurel, MD
Alain Touwaide, PhD Scientific Director, Institute for the Preservation of Medical Traditions, Washington, DC
Arthur O. Tucker, PhD Research Professor of Agriculture and Natural Resources, Delaware State University Dover, DE
Nancy Turner, PhD Distinguished Professor and Ethnobotanist Environmental Studies Program University of Victoria Victoria, BC, Canada
Roy Upton Executive Director, American Herbal Pharmacopoeia Scotts Valley, CA
Alvaro Viljoen, PhD National Research Chair in Phytomedicine Department of Pharmaceutical Sciences Tshwane University of Technology, Pretoria, South Africa
Daniel T. Wagner, RPh, MBA, PharmD President, Student Rainforest Fund Owner, Wildwood Wellness, LLC Wildwood, PA
John Weeks Publisher-Editor, The Integrator Blog Seattle, WA
Andrew T. Weil, MD Author, Director of the Arizona Center for Integrative Medicine, and Associate Director of the Division of Social Perspectives in Medicine, College of Medicine, University of Arizona Tucson, AZ
Elizabeth Williamson, PhD Professor of Pharmacy and Director of Pharmacy Practice, University of Reading, Reading, UK
David Winston, RH (AHG) Director, Herbal Therapeutics Research Library Herbalist & Alchemist, Inc. Washington, NJ
Hans Wohlmuth, PhD Research and Development Manager Integria Healthcare, Ballina, NSW, Australia
Jacqueline C. Wootton, MEd Founder and First Director, HerbMed/Pro; Former Director, Alternative Medicine Foundation North Yorkshire, UK
Peiying Yang, PhD Assistant Professor, Dept. of General Oncology, Section of Integrative Medicine University of Texas, MD Anderson Cancer Center Houston, TX
Eric L. Yarnell, ND Assistant Professor, Bastyr University Kenmore, WA
Zhongzhen Zhao, PhD, MH Associate Dean and Chair Professor Teaching and Research Division Hong Kong Baptist University Hong Kong, China

The Journal of the American Botanical Council
48 The Illustrious Life of Maria Sibylla Merian
By Betsy Kruthoffer
The Lloyd Library and Museum in Cincinnati, Ohio, presents a selection of the beautiful, detailed work of botanical illus-trator Maria Sibylla Merian. At a time when women were almost completely excluded from the arts and sciences, Merian produced her first book of illus-trations in 1679 and, in 1699, she embarked on an expedi-tion to Suriname to document the local flora and insects. Her illustrations illuminate the rela-tionships between insects and plants, and capture the intimate details of both with a deft eye and remarkable talent.
56 Herbal Supplement Sales in US Increase 7.7% in 2016 By Tyler Smith, Kimberly Kawa, Veronica Eckl, Claire Morton, and Ryan Stredney
In 2016, total retail sales of herbal dietary supplements in the United States increased by an estimated 7.7% — the second highest rate of growth for these products in more than a decade. And, for the first time, total sales of herbal supplements in all US market channels surpassed $7 billion. The 2016 Herb Market Report, which was produced in collaboration with the market research firms SPINS and IRI, and New Hope Network’s Nutrition Business Journal, details the top-selling herbs in 2016 in mainstream and natural retail outlets, and explores consumer trends driving some of the fastest-growing herbal ingredients.
Plate 1: Ananas / PineappleAnanas comosus (Bromeliaceae)Artwork courtesy of Lloyd Library and Museum
6 • I S S U E 115 • 2017 • www.herbalgram.org
Published by the American Botanical Council, P.O. Box 144345, Austin, TX 78714-4345.
Subscriptions to HerbalGram are a benefit of ABC membership at every level. One year memberships: Individual $50; Academic $100; Professional $150; Organization $250; Retailer $250; HerbClip Service $600; Small Business; Sponsor. Add $20 for memberships outside of the U.S. Student and Senior discounts are available. For information about Small Business or Sponsor Memberships, contact Denise Meikel at [email protected] or 512-926-4900. © 2017 American Botanical Council. ISSN #08102-5648. Printed in the U.S.A.The information in HerbalGram® is intended for educational purposes only and is not a substitution for the advice of a qualified healthcare professional. Although we attempt to ensure that advertising in HerbalGram is truthful and not misleading, the publication of an ad for a product or company in HerbalGram does not constitute an endorsement by ABC of the product or the company being advertised. Publication of an ad that makes a health claim or structure-function claim does not necessarily constitute an approval of that claim by ABC. Further, ABC has not reviewed any manufacturer’s Good Manufacturing Practices.
HerbalGram® is printed on recycled paper at
Craftsman Printers, Inc. Lubbock, Texas
departments
HerbalGram Staff
Mark Blumenthal Editor-in-Chief/Publisher
Tyler Smith Managing Editor
Matthew Magruder Art Director
Hannah Bauman Associate Editor
Connor Yearsley Assistant Editor
Stefan Gafner, PhD Science Editor
Tamarind Reaves Copy Editor
Steven Foster Contributing Editor
Gayle Engels Contributing Editor
Josef Brinckmann Contributing Editor
Lance Lawhon Advertising Sales
512-832-1889 [email protected]
www.herbalgram.org • 2017 • I S S U E 115 • 7
3 Dear Reader
8 Herb Profile
Lemon Balm Melissa officinalis, Lamiaceae
20 ABC News
ABC Recognizes Adoptions of Birch, Rhodiola, and Helichrysum through the Adopt-an-Herb Program
23 Botanical Adulterants Program News
New Laboratory Guidance Document Details Appropriate Methods of Analysis to Detect Synthetic Antimicrobial Compounds Sold as Grapefruit Seed Extract
24 World News
In the Land of Kesum
28 Research Reviews
Clinical Efficacy of Australian Eucalyptus and Lemon-scent Tea Tree Essential Oils for Head Lice Treatment
Saffron Comparable to Fluoxetine in the Treatment of Postpartum Depression
Nigella Supplementation Improves Overall Control and Decreases Exacerbations in Patients with Partly Controlled Asthma
Standardized Cranberry Extract Reduces Urinary Tract Infections, Urinary Symptoms, and Antibiotic Use during Radiotherapy for Prostate Cancer
New Research Bolsters Evidence of Hot Chili Peppers’ Health Benefits
New Buzz about Beets: Enhancing Sports Performance and Cognitive Function
39 Cannabis Update
The Use of Medical Cannabis Preparations to Treat Epilepsy
48 Features
The Illustrious Life of Maria Sibylla Merian
56 Market Report
Herbal Supplement Sales in US Increase 7.7% in 2016
66 Quality Control
Emerson Ecologics’ Quality Standards Program Evolves with Dietary Supplements Segment
70 Book Reviews
A Cree Healer and His Medicine Bundle: Revelations of Indigenous Wisdom
Botanical Medicine Manual
Roots of Our Renewal: Ethnobotany and Cherokee Environmental Governance
Cannabis: A Complete Guide
74 In Memoriam
William ‘Bill’ Brevoort
Johann Jurenitsch
Joel Taller
80 Photo Finish
Common Milkweed (Asclepias syriaca, Apocynaceae)
ContributorsValerie Assinewe, PhD
Michael BackesChanchal Cabrera, MSc,
FNIMH, RH (AHG)Edward M. Croom, Jr., PhD
Veronica EcklShari Henson
Kimberly KawaChris Kilham
Betsy Kruthoffer Helen Long
Claire MortonHeather S. Oliff, PhD
Karen RatermanRyan StredneyJames Sullivan
Roy Upton
MerianBOTANICALILLUSTRATIONS
THE
US/CAN $6.95
The Journal of the American Botanical Council Number 115 | Aug — Oct 2017
Lemon Balm Profile • Field Dispatch: Kesum • Beetroot Juice ResearchNigella & Asthma • Saffron & Postpartum Depression • Self-Regulatory Program
HERBMARKET
REPORT
Medical Cannabis& Epilepsy
On the CoverCannabis Cannabis spp.
Photo ©2017 Labuda (iStockPhoto.com)Echinacea Echinacea purpurea
Photo ©2017 Steven FosterCayenne (Capsicum annuum) illustration
by Maria Sibylla Merian
H E R B P R O F I L E
Lemon BalmMelissa officinalis
Family: Lamiaceae
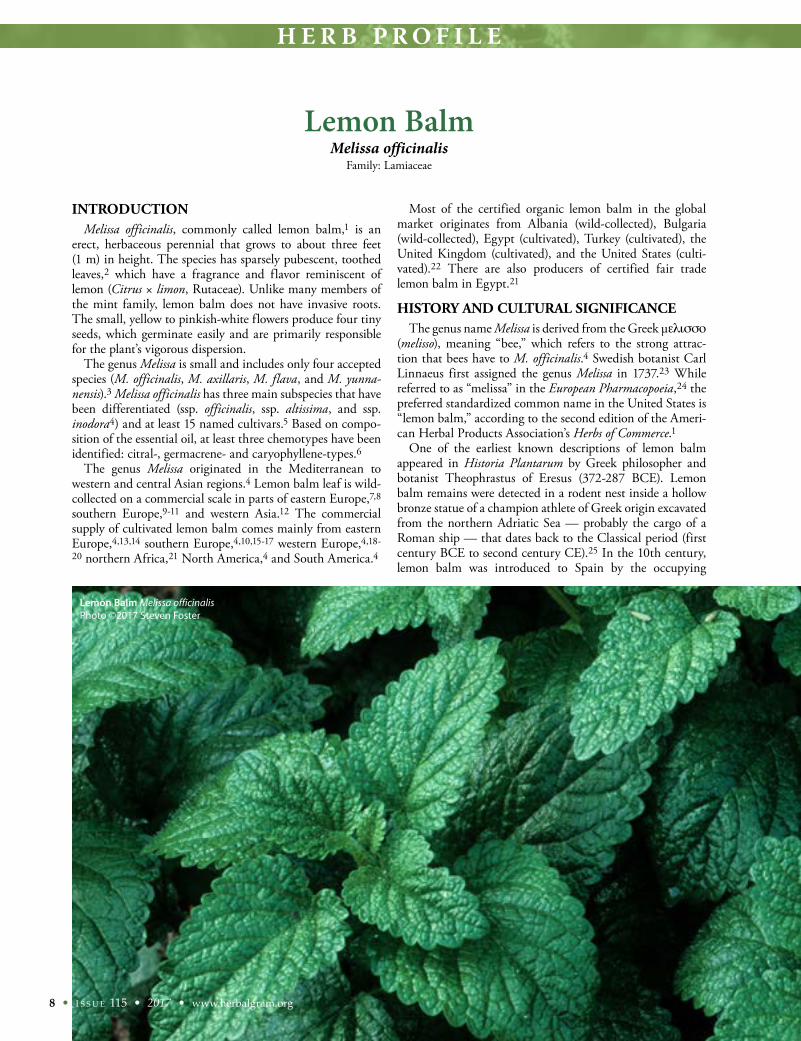
INTRODUCTION Melissa officinalis, commonly called lemon balm,1 is an
erect, herbaceous perennial that grows to about three feet (1 m) in height. The species has sparsely pubescent, toothed leaves,2 which have a fragrance and flavor reminiscent of lemon (Citrus × limon, Rutaceae). Unlike many members of the mint family, lemon balm does not have invasive roots. The small, yellow to pinkish-white flowers produce four tiny seeds, which germinate easily and are primarily responsible for the plant’s vigorous dispersion.
The genus Melissa is small and includes only four accepted species (M. officinalis, M. axillaris, M. flava, and M. yunna-nensis).3 Melissa officinalis has three main subspecies that have been differentiated (ssp. officinalis, ssp. altissima, and ssp. inodora4) and at least 15 named cultivars.5 Based on compo-sition of the essential oil, at least three chemotypes have been identified: citral-, germacrene- and caryophyllene-types.6
The genus Melissa originated in the Mediterranean to western and central Asian regions.4 Lemon balm leaf is wild-collected on a commercial scale in parts of eastern Europe,7,8 southern Europe,9-11 and western Asia.12 The commercial supply of cultivated lemon balm comes mainly from eastern Europe,4,13,14 southern Europe,4,10,15-17 western Europe,4,18-20 northern Africa,21 North America,4 and South America.4
Most of the certified organic lemon balm in the global market originates from Albania (wild-collected), Bulgaria (wild-collected), Egypt (cultivated), Turkey (cultivated), the United Kingdom (cultivated), and the United States (culti-vated).22 There are also producers of certified fair trade lemon balm in Egypt.21
HISTORY AND CULTURAL SIGNIFICANCEThe genus name Melissa is derived from the Greek μελισσο
(melisso), meaning “bee,” which refers to the strong attrac-tion that bees have to M. officinalis.4 Swedish botanist Carl Linnaeus first assigned the genus Melissa in 1737.23 While referred to as “melissa” in the European Pharmacopoeia,24 the preferred standardized common name in the United States is “lemon balm,” according to the second edition of the Ameri-can Herbal Products Association’s Herbs of Commerce.1
One of the earliest known descriptions of lemon balm appeared in Historia Plantarum by Greek philosopher and botanist Theophrastus of Eresus (372-287 BCE). Lemon balm remains were detected in a rodent nest inside a hollow bronze statue of a champion athlete of Greek origin excavated from the northern Adriatic Sea — probably the cargo of a Roman ship — that dates back to the Classical period (first century BCE to second century CE).25 In the 10th century, lemon balm was introduced to Spain by the occupying
8 • I S S U E 115 • 2017 • www.herbalgram.org
Lemon Balm Melissa officinalisPhoto ©2017 Steven Foster

H E R B P R O F I L E
Moors and was later brought to central Europe by Benedic-tine monks. In her book Physica, written between 1151 and 1158, Benedictine abbess Hildegard von Bingen (1098-1179) described medicinal uses of lemon balm.26 It is believed that the original idea of “Carmelite Water” (Eau de Carmélite, also known as “Spirit of Melissa”) may be traced back to around the year 1200, when Christian hermits, who began living in caves on Mount Carmel after the Crusaders retook Haifa, first realized the therapeutic properties of lemon balm.27 Lemon balm is among the 165 medicinal plant species used in Carinthian monastic medicine of the High Middle Ages (1001-1300), and it is still cultivated today at Carinthian monasteries in Austria.28
By the 16th century, lemon balm was being grown in several European countries.26 In his 1543 herbal New Kreüt-erbuch, botanist and physician Leonhart Fuchs (1501-1566) wrote that “Melissen” and “Honigblum” were the traditional names used because of the honey bee’s special love and desire for the flowers of lemon balm to make honey.29
In France, lemon balm cultivation began around 1611 in monastery gardens, where a process for distilling lemon balm water was developed by the Discalced Carmelites* in Paris, and Eau de Carmélite became a popular remedy for treat-ing toothache, syncope (fainting), and anxiety. A century later, in 1710, the Discalced Carmelites in Venice began to produce their version of Acqua di Melissa, but decided to use Dracocephalum moldavica (syn. M. moldavica) instead of M. officinalis.30 At the end of the 18th century, during a
church-hostile phase of the French Revolution, two Carmel-ite nuns fled Paris to take refuge at a German monastery in Baden-Baden and brought with them their secret recipe for Eau de Carmélite. In this way, the French tradition carried on in Germany where the name of the elixir changed to Melissengeist. The method of preparing Melissengeist was known by only the two nuns, who took an oath to pass it on to an initiated successor only when one of them died. In 2003, the sisters of the Holy Sepulcher of Baden-Baden came to an agreement with the sisters of Monastère du Carmel Notre Dame de l’Unité in Develier, Switzerland, to trans-fer the rights to manufacture the formula. The transfer took two years and required formal consent of the Archbishop of Freiburg (the legal owner of the formula) and authorization from the Swiss Alcohol Board for the manufacture of alco-holic beverages.31
In 1984, the German Commission E approved the use of lemon balm leaf, prepared as an herbal infusion, dry extract or fluidextract, as a nonprescription medicine for treating nervous sleeping disorders and functional gastrointestinal complaints.32 In 1997, the European Scientific Cooperative on Phytotherapy (ESCOP) indicated lemon balm internally for tenseness, restlessness, irritability, and for treatment of minor digestive issues, as well as externally for cold sores (herpes labialis).33 Since then, national labeling standards monographs of European Union (EU) member states, such as those of the German Commission E, have been superseded by monographs of the European Medicines Agency (EMA).
www.herbalgram.org • 2017 • I S S U E 115 • 9
* The Order of the Discalced Carmelites, founded in 1562, is a mendicant monastic order (i.e., dependent on charity) of the Roman Catholic Church. “Discalced” comes from the Latin word for “barefoot.”

H E R B P R O F I L E
10 • I S S U E 115 • 2017 • www.herbalgram.org
A quality standards monograph for “Melissa Leaf” first entered the European Pharmacopoeia (PhEur) in the 2000 supplement to the 1997 third edition,34 and subsequently a monograph for “Melissa Leaf Dry Extract” was added to the sixth supplement to the sixth edition (PhEur 6.6) in 2010. Both monographs have remained official through the current ninth edition published in July 2016.24 In 2004, a compre-hensive monograph (quality and therapeutics) for “Folium Melissae” was added to volume two of the WHO Monographs on Selected Medicinal Plants,35 and, in 2010, a monograph was included in the WHO Monographs on Medicinal Plants Commonly Used in the Newly Independent States (NIS).36 In 2007, the EMA published a labeling standards monograph, which was later superseded by a 2013 revised monograph.37
After the passage of the EU Directive on Traditional Herbal Medicinal Products (THMPD) of 2004, the first product in Europe to be issued a product registration under the new framework was Klosterfrau† Melissengeist (M.C.M. Klosterfrau Vertriebs GmbH; Cologne, Germany), issued by the German Federal Institute for Drugs and Medical Devices (BfArM) in December 2005.38
CURRENT AUTHORIZED USES IN COSMETICS, FOODS, AND MEDICINES
In the United States, the Food and Drug Administration (FDA) classifies “balm (lemon balm)” as Generally Recog-nized as Safe (GRAS) for use as a spice, natural seasoning, or flavoring.39 FDA also classifies essential oils and natural extractives (including distillates) of lemon balm as GRAS for use in food products.40 Lemon balm is also permit-ted as a component of dietary supplement products, which require FDA notification within 30 days of marketing if a structure-function claim is made and product manufacturing that conforms with current Good Manufacturing Practices (cGMPs) for dietary supplements.41
For herbal medicinal product companies in the EU or in non-EU countries where the PhEur is an official compen-dium (e.g., Australia and Canada), the aforementioned PhEur quality monographs can be used as the basis for active ingre-dient specifications. Registered Traditional Herbal Medicinal Products (THMPs) composed of PhEur-quality lemon balm and prepared as herbal teas, liquid extracts, or as solid dosage forms containing dry extract, may be labeled and marketed “for relief of mild symptoms of mental stress and to aid sleep” or “for symptomatic treatment of mild gastrointestinal complaints including bloating and flatulence.”37
For use in cosmetic products, the European Commission Health and Consumers Directorate lists “Melissa Officinalis Leaf Extract” and “Melissa Officinalis Leaf Water” (aqueous solution of the steam distillates obtained from the leaves) for skin-conditioning function, and “Melissa Officinalis Leaf Oil” (volatile oil obtained from the leaves and tops) for mask-ing, perfuming, and tonic functions.42
MODERN RESEARCHChemical constituents found in M. officinalis include
antioxidant phenolic acids, with rosmarinic acid (a caffeic acid derivative) as the major compound; flavonoids (e.g., luteolin-3’-O-glucuronide)43; and essential oil (with citro-nellal, neral, and geranial as the most abundant constitu-ents)33,44; among others.
In vitro and in vivo studies have shown lemon balm and its essential oil to have anti-anxiety,45 anti-inflammatory, analgesic,46 antibacterial, antiviral,47-53 antiproliferative, radical scavenging,54,55 sedative,45,56 thyroid-inhibiting,57 hypoglycemic, anti-diabetic (glucokinase-stimulating),58 antigenotoxic, antimutagenic,59 immunostimulating,60 and anticonvulsive properties.61,62
A number of clinical studies have shown various posi-tive outcomes when M. officinalis is used in combination with other herbs. These include the following: promot-ing sleep (with valerian [Valeriana officinalis, Caprifolia-ceae])63,64; treating restlessness in children (with valerian)64; stimulating alpha1 electrical brain activity (with laven-der [Lavandula spp., Lamiaceae], hops [Humulus lupulus, Cannabaceae], and oat [Avena sativa, Poaceae])65; treat-ing infantile colic (with German chamomile [Matricaria chamomilla, Asteraceae] and fennel [Foeniculum vulgare, Apiaceae])66; reducing oxidative stress (with cinnamon [Cinnamomum zeylanicum, Lauraceae])67 and laboratory-induced stress (with valerian)68; treating dyspepsia (in STW 5‡ [Steigerwald Arzneimittelwerk GmbH; Darm-stadt, Germany])69; treating abdominal pain and bloating in patients with irritable bowel syndrome (with spearmint [Mentha spicata, Lamiaceae] and coriander [Coriandrum sativum, Apiaceae]).70
Unfortunately, despite the approved uses of lemon balm based on its long history in traditional medicine, there are few high-quality clinical studies on M. officinalis alone.
A randomized, double-blind, placebo-controlled (RDBPC) study (N = 58) published in 2016 evaluated the effect of lemon balm on patients with borderline hyperlip-idemia. Outpatients with total serum cholesterol ranging from 200-260 mg/dL, low-density lipoprotein (LDL) levels ranging from 100-160 mg/dL, and/or serum triglycerides ranging from 150-300 mg/dL were randomly assigned to take 1,000 mg encapsulated lemon balm leaf powder (500 mg per capsule; no further information provided) or placebo three times per day after meals over two months. Participants were advised not to change their diet, and their daily intake of carbohydrates, protein, fiber, and fat were recorded via two 24-hour dietary recall questionnaires at the beginning and end of the study. No statistical differences were found within or between groups regarding dietary intake. The lemon balm group experienced a significant decrease in mg/dL of LDL cholesterol (139.64 ± 19.06 to
† Klosterfrau, literally translated as “cloister woman,” is a German term for “nun.”
‡ STW 5 is a combination herbal product that also contains bitter candytuft (Iberis amara, Brassicaceae), angelica (Angelica arch-angelica, Apiaceae), milk thistle (Silybum marianum, Asteraceae), caraway (Carum carvi, Apiaceae), celandine (Chelidonium majus, Papaveraceae), licorice (Glycyrrhiza glabra, Fabaceae), German chamomile, and peppermint (Mentha × piperita, Lamiaceae).

H E R B P R O F I L E
www.herbalgram.org • 2017 • I S S U E 115 • 11
125.68 ± 22.62) compared to the placebo group (129.90 ± 17.94 to 131.07 ± 21.21). While there were no significant differences between groups in levels of total cholesterol, fasting blood glucose, high-density lipoprotein (HDL), triglycerides, creatinine, or alanine transaminase (ALT) at the end of the study, the lemon balm group did not expe-rience the higher LDL:HDL ratio (a risk factor for athero-sclerosis and coronary heart disease) that was seen in the placebo group. According to the authors, this suggests that lemon balm may provide protection against atherosclerosis and coronary heart disease. Additionally, the lemon balm group experienced a significant change in levels of aspartate trans-aminase (AST; 23.64 ± 7.36 U/L to 22.30 ± 6.56 U/L) compared to the placebo group (20.27 ± 5.76 U/L to 22.50 ± 6.00 U/L). Since increased levels of AST are corre-lated with liver damage, this study suggests that lemon balm may have the ability to improve liver health, although the observed decrease is not likely to have a clinically relevant impact.44
Another RDBPC study explored the effect of lemon balm on heart palpitations, an indi-cation for lemon balm in tradi-tional Iranian medicine. Partici-pants (N = 55) with “an unpleas-ant sensation in the heart or awareness of heartbeat as their main complaint” were randomly assigned to take 500 mg encap-sulated lemon balm dry water extract powder (powdered dry leaves infused in 1,000 mL boil-ing water, filtered, then freeze dried; no additional information provided) or placebo twice daily for 14 days. At the end of the two-week period, palpitation episodes, based on patients’ diaries, had decreased by 36.8% in the lemon balm group, compared to a decrease of 4.19% in the placebo group. Moreover, the lemon balm group had fewer participants with anxiety and insomnia at the end of the study than the placebo group (decreases of 42.8% vs. 18.2%, respectively). Change in pain intensity between the two groups was not significant.71
A 2015 RDBPC study (N = 100) investigated the effect of lemon balm on the intensity of
premenstrual syndrome (PMS) symptoms in high school girls in Shiraz, Iran, over the course of three menstrual cycles. Participants with PMS Screening Tool scores greater than 20 (considered “average symptoms”) were randomly assigned to receive 1,200 mg per day of lemon balm essence (600 mg capsules made in the pharmacology department of the Shiraz University of Medical Sciences in Shiraz, Iran) or placebo. The test group experienced significant reduc-tions in PMS symptom intensity scores from the onset of the study (42.56 + 15.73) at one month (32.72 ± 13.24), two months (30.02 ± 12.08), and three months (13.90 ± 10.22).
Lemon Balm Melissa officinalisPhoto ©2017 Steven Foster

H E R B P R O F I L E
12 • I S S U E 115 • 2017 • www.herbalgram.org
The placebo group experienced non-significant reduc-tions in intensity of PMS symptoms, which the authors suggest may be attributable to the placebo effect.72
A randomized, single-blind study (N = 43) in 2016 compared lemon balm to the nonsteroidal anti-inf lam-matory drug (NSAID) mefenamic acid for their ability to relieve dysmenorrhea (i.e., pain associated with menstru-ation). From the onset of the menstrual period until the third day of menstruation, women with moderate-to-severe primary dysmenorrhea were randomly assigned to drink one cup of lemon balm tea made from tea bags (Golchai Co.; Alborz, Iran; no additional information provided) or take 250 mg of mefenamic acid (Razak Laboratories Co.; Tehran, Iran) every eight hours until pain was relieved. Both groups experienced decreases in pain intensity and duration over three menstrual cycles, but the lemon balm group experienced a greater decrease in pain intensity (5.61 ± 1.125 to 3.166 ± 0.632) than the mefenamic acid group (6.13 ± 1.38 to 4.095 ± 1.70). The authors recognize that the study’s findings are limited by the small sample size and short follow-up period.73
Published in 2003, one RDBPC study investigated the efficacy of lemon balm for treating mild-to-moderate Alzheimer’s disease (AD) over four months. Patients (N = 42; 65-80 years old) with scores of 12 or greater on the AD Assessment Scale (ADAS-cog) and 2 or less on the Clinical Dementia Rating-Sum of Boxes (CDR-SB) scale were randomly assigned to receive 60 drops per day of lemon balm extract (1:1 in 45% alcohol, standardized to contain at least 500 μg citral/mL; no additional informa-tion provided) or placebo. After four months, the lemon balm group experienced a significant improvement in cognition compared to placebo in both the ADAS-cog (-6.4 vs. 5.60, respectively) and the CDR-SB scores (-1.92 vs. 1.03, respectively). The authors state that while lemon balm may be effective in treating mild-to-moderate AD, further studies with larger sample sizes are needed to confirm lemon balm’s efficacy. The authors also list the short follow-up period as a limitation, but it is unclear from the paper if there was a follow-up period at all.74
One RDBPC study published in 2002 evaluated the effectiveness of lemon balm essential oil (LBEO) for managing agitation in patients with severe dementia. Patients with clinically significant agitation related to severe dementia (N = 72, mean age = 78.5 ± 8.1 years), who continued to use prescribed psychotropic medica-tions during the study, were randomly assigned to receive treatment with LBEO lotion or placebo (sunf lower [Helianthus spp., Asteraceae] oil lotion). The LBEO was obtained from G. Baldwin & Co. (London, England) and contained 22% citronellal, 18% caryophyllene, 7% neral, 7% geraniol, 3% geranyl acetate, and 4% citronallal. The test preparation was made by adding 10% by weight LBEO to a base lotion containing almond (Prunus dulcis, Rosaceae) oil, glycerine, stearic acid, cetearyl alcohol, and tocopheryl acetate. Over a four-week period, a measured dose of 0.16-0.17 g was applied for one to two minutes to
the patient’s face and arms twice a day for a total of six doses per day. To achieve blinding, two residential facili-ties were used and participants in each facility were given either the active treatment or placebo.
By the end of the study, the lemon balm group had experienced a 35% decrease from baseline in agitation on the Cohen-Mansfield Agitation Inventory (CMAI), compared to an 11% decrease in the placebo group, a significant between-group difference. Additionally, 21 of 36 subjects (58%) in the active treatment group expe-rienced a clinically significant improvement in agitation (defined as a 30% improvement) compared to only five of 36 (14%) in the placebo group. Moreover, the lemon balm group experienced a significant reduction in the amount of time spent socially withdrawn and a significant increase in the amount of time participating in construc-tive activities. The authors propose several hypotheses for the success of the treatment: physiological effect(s) of the LBEO terpenes; concentration of the monoter-pene citronellal in the hippocampus after administration; increased social contact between staff and subjects; the fragrance having a placebo effect on subjects (considered unlikely as patients with severe dementia commonly have an impaired sense of smell); and the fragrance having an impact on the caregivers’ reporting. However, the authors believe that none of these hypotheses taken individually can explain the magnitude of improvement in the active treatment group, and they recommend further multi-center studies to confirm and elucidate their findings.75
FUTURE OUTLOOKAlthough classified as a protected species in Croatia,76
the International Union for Conservation of Nature (IUCN) European Red List of Medicinal Plants assigns M. officinalis to the conservation category of least concern, meaning that the species is not threatened in Europe.77 However, the situation is different in parts of Asia. In Iran, wild M. officinalis is reportedly threat-ened due to habitat destruction, land use changes, and overharvesting.78 In Armenia, field studies on changes in distribution and structure of wild M. officinalis popu-lations were carried out from 2006 to 2009.79 A related eco-geographic survey of population dynamics of wild M. officinalis was conducted from 2007 to 2011.80 While historical data had shown that wild M. officinalis popu-lations were widely distributed in northern and central regions of Armenia, nearly half of the populations no longer existed in the previously cited locations. There is also evidence that the distribution of M. officinalis is expanding in southern Armenia. Current models predict that vulnerability of wild populations in central and northern Armenia will increase due to anthropogenic threats (e.g., poor land management, deforestation, live-stock overpopulation, and unsustainable wild-collection methods) and climate change (e.g., more frequent early spring frosts and abrupt weather changes).81
One of the biggest markets for lemon balm is Germany,

H E R B P R O F I L E
where the average annual demand is about 1.5 million kg (3.307 million lbs). While Germany imports most of its lemon balm supply, about 20% is grown in Germany on about 120 hectares (296.5 acres).82 There are approxi-mately 38 hectares (94 acres) of lemon balm cultivation in neighboring France.19 Bulgaria remains one of the main producers and exporters of both wild-collected and cultivated lemon balm with an annual average export volume of 330,629 kg (728,912 lbs) Folium Melissae (leaf ), plus another 118,840 kg (261,997 lbs) of Herba Melissae (aerial parts), and 11,400 kg (25,132 lbs) of Herba Melissae Stipites (stem).83 In 2015, Bulgaria had about 410 hectares (1,013 acres) of lemon balm cultiva-tion with an overall yield of 550,000 kg (1.212 million lbs).84 Albania exports about 350,000 kg (771,618 lbs) of wild-collected lemon balm annually.10 Hungary has an estimated 200-250 hectares (494-618 acres) of lemon balm cultivation with an annual production of up to 300,000 kg (661,387 lbs).85 In the United States, there are many small- to medium-sized organic lemon balm growers in several states, including California, Oregon, Washington, Vermont, Maine, and New York.22
There are no indications that the demand for lemon balm for use in herbal medicinal products, herbal dietary supplements, foods, and beverages will decrease. Although lemon balm is now cultivated in many coun-tries worldwide, the main production areas and highest demand remain in Europe, especially Germany. There is evidence that both cultivated and wild-collected lemon
balm are increasingly being produced according to inter-national sustainability standards, such as organic and fair trade. The production and market scenario appear stable.
—Gayle Engels and Josef Brinckmann
References1. McGuffin M, Kartesz JT, Leung AY, Tucker AO. American
Herbal Products Association’s Herbs of Commerce. 2nd ed. Silver Springs, MD: American Herbal Products Association; 2000.
2. Applequist W. The Identification of Medicinal Plants: A Hand-book of the Morphology of Botanicals in Commerce. St. Louis, MO: Missouri Botanical Garden; 2006.
3. The Plant List (2013). Version 1.1. 2013. Available at: www.theplantlist.org/tpl1.1/search?q=Melissa. Accessed April 15, 2017.
4. Bomme U, Honermeier B, Hoppe B, Kittler J, Lohwasser U, Marthe F. Melisse (Melissa officinalis L.). In: Hoppe B, ed. Handbuch des Arznei- und Gewürzpflanzenbaus, Band 5. Bernburg: Verein für Arznei- und Gewürzpflanzen SALU-PLANTA e.V. Bernburg; 2013:151-173.
5. Heine H, Eger H, Franz C, Blüthner W-D, Hoppe K. Sortenwesen und Sortenübersicht Arznei- und Gewürzpflan-zen. In: Verein für Arznei- und Gewürzpflanzen SALU-PLANTA e.V. Bernburg, ed. Handbuch des Arznei- und Gewürzpflanzenbaus, Band I. Bernburg: Verein für Arznei- und Gewürzpflanzen SALUPLANTA e.V. Bernburg; 2009.
Lemon Balm Melissa officinalisPhoto ©2017 Steven Foster
www.herbalgram.org • 2017 • I S S U E 115 • 13
H E R B P R O F I L E
14 • I S S U E 115 • 2017 • www.herbalgram.org
6. Kittler J, Krüger H, Schütze W, et al. Charakterisierung unter-schiedlicher Genpools der Melisse (Melissa officinalis) als Basis für die Entwicklung von züchterisch wertvollem Ausgangsmaterial. In: Humboldt-Universität zu Berlin, ed. 6. Fachtagung Arznei- und Gewürzpflanzen. Berlin: Deutscher Fachausschuß für Arznei-, Gewürz- und Aromapflanzen; 2011.
7. Bakalski Co. Ltd. List of Wild Collected Organic Herbs, season 2010. Available at: www.bakalskico.com/products/organic-wild-collected-herbs.html Accessed April 15, 2017.
8. Viola Ltd. List of Wild Collected Organic Herbs. Available at: www.viola.bg/LISTOFWILDCOLLECTED2009.pdf. Accessed April 16, 2017.
9. AgroHerbAl sh.p.k. Products. Available at: www.agroherbal.net/products-natural-biologic-organic-agroherbal.html. Accessed April 16, 2017.
10. Kathe W, Honnef S, Heym A. Medicinal and Aromatic Plants in Albania, Bosnia-Herzegovina, Bulgaria, Croatia and Romania. Bonn, Germany: Bundesamt für Naturschutz (BfN);2003.
11. Brinckmann JA, Huggins K, Gardner ZE. Managing Natural Resources for Sustainable Livelihoods: Threats to the Future of Sustainable Wild Collection and Field Experience with Implemen-tation of the FairWild Standard for Medicinal Plants. International Journal on Biodiversity Watch. 2014;3:13-29.
12. ANTARAM PC. Medicinal herbs and herbal teas. Yerevan, Arme-nia: ANTARAM PC; 2017.
13. Bernáth J, Németh E. Main fields of research activity on medicinal and aromatic plant species in Hungary in relation to the ECPGR “priority list”. In: Lipman E, ed. Report of a Working Group on Medicinal and Aromatic Plants. Second Meeting, 16-18 December 2004, Strumica, Macedonia FYR / Third Meeting, 26–28 June 2007, Olomouc, Czech Republic. Rome, Italy: Bioversity Interna-tional; 2009:115-128.
14. Węglarz Z, Geszprych A. The status of medicinal and aromatic plants in Poland. In: Baričevič D, Bernáth J, Maggioni L, Lipman E, eds. Report of a Working Group on Medicinal and Aromatic Plants. First meeting, 12-14 September 2002, Gozd Martuljek, Slovenia. Rome, Italy: International Plant Genetic Resources Insti-tute; 2004:96-105.
15. Foreign Trade Chamber of Bosnia and Herzegovina. Catalogue: Medicinal & Aromatic Plants | Mushrooms | Forest Fruits | Honey. Sarajevo: USAID/Sida FARMA; 2014.
16. Albinspekt. Organic Certificate: Annex C - Processed products - Agroproduct shpk - List of certified products. 2017. Available at: http://albinspekt.com/site.OLD/wp-content/uploads/2017/01/Annex-C_List-of-products-AP-170124.pdf. Accessed April 18, 2017.
17. Zivanovic ST, Stevanetic S, Ceranic S, Zivanovic T. Trends in production of raw medicinal and aromatic plants in Serbia. Paper presented at: Fifth International Scientific Agricultural Symposium “Agrosym 2014” - Jahorina, Bosnia and Herzegovina, October 23-26, 2014.
18. Kainz W. Medicinal and aromatic plants in Austria – status 2007. In: Lipman E, ed. Report of a Working Group on Medicinal and Aromatic Plants. Second Meeting, 16-18 December 2004, Strumica, Macedonia FYR / Third Meeting, 26–28 June 2007, Olomouc, Czech Republic. Rome, Italy: Bioversity International; 2009:45-58.
19. Délégation nationale de FranceAgriMer Volx. Données et bilans: Filières plantes à parfum, aromatiques et médicinales Panorama 2015 / direction Marchés, études et prospective. Montreuil cedex: FranceAgriMer; 2016.
20. Organic Herb Trading Company. Online Price List. Available at: www.organicherbtrading.com/. Accessed April 18, 2017.
21. FLO-CERT GmbH Fairtrade customer search. Available at: www.flocert.net/fairtrade-services/fairtrade-certification/fairtrade-customer-search/. Accessed April 16, 2017.
22. Organic INTEGRITY Database. USDA, Agricultural Market-ing Service; 2017. Available at: https://organic.ams.usda.gov/Integrity/. Accessed April 16, 2017.
23. Linnæi C. Genera plantarum :eorumque characteres naturales secundum numerum, figuram, situm, & proportionem omnium fructificationis partium. Batavorum Lugdunum [Leiden]: Conradum Wishoff; 1737.
24. European Pharmacopoeia Commission. European Pharmaco-poeia Ninth Edition (PhEur 9.0). Strasbourg, France: European Directorate for the Quality of Medicines; 2016.
25. Šoštarić R, Kovačić D, Ćaleta M, Alegro A, Mitić B. The Croa-tian Apoxyomenos as a luxurious rodent nest: archaeobotanical and zoological analyses of organic material found inside the classical bronze statue. Vegetation History and Archaeobotany. 2007;17(3):289-295.
26. Teuscher E. Medicinal Spices: A Handbook of Culinary Herbs, Spices, Spice MIxtures and their Essential Oils. Stuttgart: Medpharm Scientific Publishers; 2006.
27. Heckelmann H. Maria Clementine Martin (1775-1843) Ordens-frau, “Quacksalberin,” Unternehmerin. Eine rechtshistorische Untersuchung aus neuen Quellen, Universität Regensburg; 2014.
28. Kartnig T, Piendl S. Arzneipflanzen und Arzneidrogen in der Klostermedizin in Kärnten einst und jetzt. Carinthia II, Klagen-furt. 2004;194(114):83–95.
29. Fuchs L. New Kreüterbuch / in welchem nit allein die gantz histori / das ist / namen / gestalt/ statt und Zeit der wachsung / natur / krafft un würkung / des meysten theyls der Kreuter so in Teutschen unnd andern Landen wachsen / mit dem besten vleiß beschrieben. Basel, Switzerland: Michael Isingrin; 1543.
30. Favero C, Favero G. The Discalced Carmelites in Venice - The Church of Santa Maria di Nazareth and the Monastery Garden. BIBLOS EDIZIONI, Cittadella (Pd), Italy; 2015.
31. Gönnheimer S. Schätze aus der Schulstiftung der Erzdiözese – Das Elexier der Karmeliterinnen. FORUM Schulstiftung. 2006;45:106-109.
32. Blumenthal M, Busse WR, Goldberg A, Gruenwald J, Hall T, Riggins CW, Rister RS, eds. Klein S, Rister RS, trans. The Complete German Commission E Monographs — Therapeutic Guide to Herbal Medicines. Austin, TX: American Botanical Council; Boston: Integrative Medicine Communication; 1998.
33. ESCOP. Melissae folium. Monographs on the Medicinal Uses of Plant Drugs. Exeter, UK: European Scientific Cooperative on Phytotherapy; 1997.
34. European Pharmacopoeia Commission. Europäisches Arznei-buch Nachtrag 2000. Stuttgart/Eschborn: Deutscher Apotheker Verlag/Govi-Verlag - Pharmazeutischer Verlag GmbH; 2000.
35. World Health Organization. WHO Monographs on Selected Medicinal Plants, Volume 2. Geneva: World Health Organiza-tion; 2002.
36. World Health Organization. WHO Monographs on Medicinal Plants Commonly Used in the Newly Independent States (NIS). Geneva, Switzerland: World Health Organization; 2010.
37. Committee on Herbal Medicinal Products (HMPC). Commu-nity herbal monograph on Melissa officinalis L., folium. London, UK: European Medicines Agency; 2013.
38. Deutsches Institut für Medizinische Dokumentation und Information (DIMDI). Gebrauchsinformation: Klosterfrau Melissengeist. In: PharmNet.Bund. Arzneimittel-Informations-system. 2005; Available at: www.pharmnet-bund.de/dynamic/de/arzneimittel-informationssystem/index.html. Accessed April 16, 2017.
39. US Food and Drug Administration (FDA). § 182.10 Spices and other natural seasonings and flavorings. Code of Federal Regulations, Title 21 (21 CFR). Washington, DC: US Govern-ment Printing Office; 2016:474-475.
H E R B P R O F I L E
www.herbalgram.org • 2017 • I S S U E 115 • 15
40. US Food and Drug Administration. § 182.20 Essential oils, oleo-resins (solvent-free), and natural extractives (including distillates). In: Code of Federal Regulations (21 CFR). Washington, DC: US Government Printing Office; 2016.
41. US Food and Drug Administration. 21 CFR Part 111 Current Good Manufacturing Practice in Manufacturing, Packaging, Label-ing, or Holding Operations for Dietary Supplements; Final Rule. Federal Register. 2007;72(121):34752-34958.
42. Cosmetic Ingredients and Substances (CosIng®) Database. Euro-pean Commission; 2017. Available at: http://ec.europa.eu/growth/tools-databases/cosing/. Accessed April 16, 2017.
43. Herodež ŠS Hadolin M, Škerget M, Knez Ž. Solvent extraction study of antioxidants from balm (Melissa officinalis L.) leaves. Food Chem. 2003;80:275-282.
44. Jandaghi P, Noroozi M, Ardalani H, Alipour M. Lemon balm: A promising herbal therapy for patients with borderline hyperlipid-emia–A randomized double-blind placebo-controlled clinical trial. Complement Ther Med. 2016;26:136-140.
45. Heinrich M, Barnes J, Gibbons S, Williamson EM. Fundamentals of Pharmacognosy and Phytotherapy. London, UK: Elsevier; 2012.
46. Birdane YO Büyükokuroglu M, Birdane FM, Cemek M, Yavuz H. Anti-inflammatory and antinociceptive effects of Melissa officinalis L. in rodents. Revue Med Vet. 2007;158(2):75-81.
47. Pourghanbari G, Nili H, Moattari A, Mohammadi A, Iraji A. Antiviral activity of the oseltamivir and Melissa officinalis L. essential oil against avian influenza A virus (H9N2). Virusdisease. 2016;27(2):170-178.
48. Astani A, Navid MH, Schnitzler P. Attachment and penetration of acyclovir-resistant herpes simplex virus are inhibited by Melissa officinalis extract. Phytother Res. 2014;28(10):1547-1552.
49. Astani A, Reichling J, Schnitzler P. Melissa officinalis extract inhib-its attachment of herpes simplex virus in vitro. Chemotherapy. 2012;58(1):70-77.
50. Schnitzler P, Schuhmacher A, Astani A, Reichling J. Melissa officinalis oil affects infectivity of enveloped herpesviruses. Phytomedicine. 2008;15(9):734-740.
51. Mazzanti G, Battinelli L, Pompeo C, et al. Inhibi-tory activity of Melissa officinalis L. extract on Herpes simplex virus type 2 replication. Nat Prod Res. 2008;22(16):1433-1440.
52. Nolkemper S, Reichling J, Stintzing FC, Carle R, Schnitzler P. Antiviral effect of aqueous extracts from species of the Lamiaceae family against Herpes simplex virus type 1 and type 2 in vitro. Planta Med. 2006;72(15):1378-1382.
53. Allahverdiyev A, Duran N, Ozguven M, Koltas S. Antiviral activity of the volatile oils of Melissa officinalis L. against Herpes simplex virus type-2. Phytomedicine. 2004;11(7-8):657-661.
54. Čanadanović-Brunet J, Ćetković G, Djilas S, et al. Radical scavenging, antibacterial, and antiprolifera-tive activities of Melissa officinalis L. extracts. Journal of Medicinal Food. 2008;11(1):133-143.
55. Jeziorek M, Wasek M. Free radical scavenging activ-ity for infusions of 30 medicinal plants detected with electron paramagnetic resonance. Herba Polonica. 2008;54(1):7-14.
56. Soulimani R, Fleurentin J, Mortier F, Misslin R, Derrieu G, Pelt JM. Neurotropic action of the hydroalcoholic extract of Melissa officinalis in the mouse. Planta Med. 1991;57(2):105-109.
57. Santini F, Vitti P, Ceccarini G, et al. In vitro assay of thyroid disruptors affecting TSH-stimulated adenylate cyclase activity. J Endocrinol Invest. 2003;26(10):950-955.
58. Chung MJ, Cho SY, Bhuiyan MJ, Kim KH, Lee SJ. Anti-diabetic effects of lemon balm (Melissa officinalis) essential oil on glucose- and lipid-regulating enzymes in type 2 diabetic mice. Br J Nutr. 2010;104(2):180-188.
59. Cassettari de Carvalho N, Corrêa-Angeloni MJF, Leffa DD, Moreira J, et al. Evaluation of the genotoxic and antigenotoxic potential of Melissa officinalis in mice. Genetics and Molecular Biol-ogy. 2011;34(2):290-297.
60. Drozd J, Anuszewska E. The effect of the Melissa officinalis extract on immune response in mice. Acta Pol Pharm. 2003;60(6):467-470.
61. Hariry RE. Anticonvulsant effects of hydroalcoholic extract of Melissa officinalis on pentylenetetrazole (PTZ) model of convulsion in mice. J Med Plant Research. 2011;5(16):3803-3809.
62. Gorgich E, Komeili G, Zakeri Z, Ebrahimi S. Comparing anti-convulsive effect of Melissa officinalis hydro-alcohlic extract and phenytoin in rat. Journal of Health Scope. 2012;1(1):44-48.
63. Dressing H, Köhler S, Müller WE. Improvement of sleep quality with a high-dose valerian/lemon balm preparation: a placebo-controlled double-blind study. Psychopharmakotherapie. 1996;3:123-130.
64. Müller SF, Klement S. A combination of valerian and lemon balm is effective in the treatment of restlessness and dyssomnia in chil-dren. Phytomedicine. 2006;13(6):383-387.
65. Dimpfel W, Pischel I, Lehnfeld R. Effects of lozenge containing lavender oil, extracts from hops, lemon balm and oat on electrical brain activity of volunteers. Eur J Med Res. 2004;9(9):423-431.
66. Savino F, Cresi F, Castagno E, Silvestro L, Oggero R. A random-ized double-blind placebo-controlled trial of a standardized extract of Matricariae recutita, Foeniculum vulgare and Melissa officinalis (ColiMil) in the treatment of breastfed colicky infants. Phytother Res. 2005;19(4):335-340.
Michael J. Balick, PhD VP and Director,Institute of Economic Botany, New York Botanical Garden, Bronx, NY
Neil Blomquist President, Sustainable Solutions Consulting Services, Sebastopol, CA
Peggy Brevoort President, Brevoort, LLC, Kapa'au, HI
Steven Foster President, Steven Foster Group, Inc., Eureka Springs, AR
Bernadette P. Marriott, PhD Professor, Department of Medicine MUSC College of Medicine Div. of Gastroenterology & Hepatology & Department of Psychiatry and Behavioral Sciences Military Division Charleston, SC
Thomas M. Newmark Owner, Finca Luna Nueva Lodge, San Isidro de Peñas Blancas, Costa Rica
Morris Shriftman CEO, Mozart, Inc., Petaluma, CA
Margaret Wittenberg Former Global VP of Quality Standards & Public Affairs, Whole Foods Market, Inc., Austin, TX
James A. Duke, PhD (emeritus) Botanical Consultant, Economic Botanist (USDA, ret.), Herbal Vineyard Inc. / Green Farmacy Garden, Fulton, MD
Mark Blumenthal (ex officio) Founder & Executive Director American Botanical Council Austin, TX
ABC Board of Trustees

H E R B P R O F I L E
16 • I S S U E 115 • 2017 • www.herbalgram.org
67. Rashidi M, Malekirad AA, Abdollahi M, Habibollahi S, Dolatyari N, Narimani M. The effect of tea-cinnamon and Melissa officinalis L. aqueous extraction, on neuropsychology distress, biochemi-cal and oxidative stress biomarkers in glass production workers. Health. 2014;6:2592-2601.
68. Kennedy DO, Little W, Haskell CF, Scholey AB. Anxiolytic effects of a combination of Melissa officinalis and Valeriana officinalis during laboratory induced stress. Phytother Res. 2006;20(2):96-102.
69. Rösch W, Liebregts T, Gundermann KJ, Vinson B, Holtmann G. Phytotherapy for functional dyspepsia: a review of the clini-cal evidence for the herbal preparation STW 5. Phytomedicine. 2006;13 Suppl 5:114-121.
70. Vejdani R, Shalmani HR, Mir-Fattahi M, et al. The efficacy of an herbal medicine, Carmint, on the relief of abdominal pain and bloating in patients with irritable bowel syndrome: a pilot study. Dig Dis Sci. 2006;51(8):1501-1507.
71. Alijaniha F, Naseri M, Afsharypuor S, et al. Heart palpitation relief with Melissa officinalis leaf extract: double blind, random-ized, placebo controlled trial of efficacy and safety. Journal of Ethnopharmacology. 2015;164:378-384.
72. Akbarzadeh M, Dehghani M, Moshfeghy Z, Emamghoreishi M, Tavakoli P, Zare N. Effect of Melissa officinalis capsule on the intensity of premenstrual syndrome symptoms in high school girl students. Nurs Midwifery Stud. 2015;4(2):e27001.
73. Faranak SD, Parvin N. The effect of mefenamic acid and Melissa officinalis on primary dysmenorrhea: a randomized clinical trial study. International Journal of Pharmacognosy and Phytochemical Research. 2016;8(8):1286-1292.
74. Akhondzadeh S, Noroozian M, Mohammadi M, Ohadinia S, Jamshidi AH, Khani M. Melissa officinalis extract in the treatment of patients with mild to moderate Alzheimer’s disease: a double blind, randomised, placebo controlled trial. J Neurol Neurosurg Psychiatry. 2003;74(7):863-866.
75. Ballard CG, O’Brien JT, Reichelt K, Perry EK. Aromatherapy as a safe and effective treatment for the management of agitation in severe dementia: the results of a double-blind, placebo-controlled trial with Melissa. J Clin Psychiatry. 2002;63(7):553-558.
76. Sandev D, Mihelj D, Kovačić S. Meeting Target Eight – Ex situ conservation of Croatian threatened and statutorily protected plant species in the Botanical Garden of the Faculty of Science, University of Zagreb (Croatia). Natura Croatica. 2013;22(2):343–362.
77. Allen D, Bilz M, Leaman DJ, Miller RM, Timoshyna A, Window J. European Red List of Medicinal Plants. Luxembourg: Publications Office of the European Union; 2014.
78. Ghaffariyan S, Mohammadi SA, Aharizad S. DNA isolation protocol for the medicinal plant lemon balm (Melissa officinalis, Lamiaceae). Genet Mol Res. 2012;11(2):1049-1057.
79. Abrahamyan A. Changes in distribution and structure of wild Melissa officinalis L. populations during the last decade in Arme-nia and implications for conservation. Environment. Technology. Resources. Proceedings of the 8th International Scientific and Practi-cal Conference. 2011;2:321-324.
80. Abrahamyan A, Barsevskis A, Melikyan A. Populations dynam-ics in sizes of wild Melissa officinalis L. (Lamiaceae) during the last decade in Armenia. Journal of Medicinal Plants Studies.
2015;3(1):21-26.81. Abrahamyan A, Teilans A, Zorins A.
Climate change impact on conserva-tion status of wild Melissa officinalis L. (Lamiaceae) populations in Armenia. Paper presented at: First International Symposium on Medicinal, Aromatic and Nutraceutical Plants from Moun-tainous Areas (MAP-Mountain 2011), 6th – 9th July 2011, Saas-Fee, Swit-zerland.
82. Kästner U, Krüger H, Krähmer A, et al. Züchterische Bearbeitung von Melisse (Melissa officinalis). Paper presented at: 26. Bernburger Winterseminar Arznei- und Gewürz-pflanzen - February 23-24, 2016; Bernburg.
83. Evstatieva L, Hardalova R, Stoyanova R. Medicinal plants in Bulgaria: diversity, legislation, conservation and trade. Phytologia Balcanica. 2007;13(3):415-427.
84. Boshnakova M. GAIN Report Number: BU1653. Bulgaria Organic Sector and Trade Update. Sofia: USDA Foreign Agricultural Service; 2016.
85. Non-food Group Department of Agri-cultural Chemical Technology Buda-pest University of Technology and Economics. Report from the Republic of Hungary. Budapest, Hungary: Interac-tive European Network for Industrial Crops and their Applications; 2002 (with updates in January 2004).
Herbal Adopters
The American Botanical Council’s Adopt-an-Herb Program provides a mutually beneficial opportunity to support ABC’s nonprofit educational efforts and promote a company’s most important herbs.
One of the benefits of supporting the Adopt-an-Herb Program is that it ensures that the most current infor-mation on the adopted herb is available through ABC’s powerful HerbMedProTM database.
HerbMedPro provides online access to abstracts of scientific and clinical publications on more than 250 commonly used medicinal herbs. A free version, HerbMed®, is available to the general public. HerbMed features 20 to 30 herbs from HerbMedPro that are rotated on a regular basis with an emphasis on adopted herbs. HerbMedPro is available as a member benefit to all ABC members at the Academic Membership level and up.
In addition to ensuring that recently published infor-mation on an adopted herb is up to date on HerbMedPro, another benefit adopters enjoy is being included among their peers in each issue of ABC’s acclaimed quarterly, peer-reviewed scientific journal, HerbalGram, on the ABC website, and at scientific, medical, and other educational conferences. Press releases also are issued on new adop-tions, bringing attention to the program, the adopted herb, and the adopting company. Each adopted herb is featured on its own page on the ABC website.
Parties interested in taking part in the Adopt-an-Herb Program are invited to contact ABC Development Director Denise Meikel at 512-926-4900, extension 120, or by email at [email protected].
Theobroma cacaoCocoa Flavanols
Bacopa monnieriBacopa
Melaleuca alternifolia
Brassica oleracea Broccoli Group
Tea Tree
Broccoli
Boswellia serrata
Aspalathus linearis
Adansonia digitata
Urtica dioica
Sambucus nigra
Aronia melanocarpa
Bulbine natalensis
Cynara scolymus
Allium sativum
Helichrysum italicum
Indian Frankincense
Rooibos
Baobab
Stinging Nettle
Elderberry
Black Chokeberry
Bulbine
Artichoke
Garlic
Helichrysum
Zea maysPurple Corn
Curcuma longaTurmeric
Olive
Grape
Olea europaea
Vitis vinifera
Sceletium tortuosumSceletium
Vaccinium macrocarpon
Nigella sativa
Piper methysticum
Lepidium meyeniiRhodiola rosea
Cranberry
Black Cumin
Kava
MacaRhodiola
Harpagophytum spp.Devil's Claw
Coffea spp.Coffee Fruit
Garcinia cambogiaGarcinia
Humulus lupulusHops
Withania somniferaAshwagandha
Betula spp.Birch
Aloe veraAloe Vera
Malpighia spp.Acerola
Eurycoma longifoliaTongkat Ali
Visit us at www.herbalgram.org/adoptTo adopt, please contact us at [email protected]
Siraitia grosvenoriiMonk Fruit
Arnica montanaArnica
Hibiscus sabdariffaHibiscus
Continued on page 4Mitragyna speciosa
Kratom
Continued on page 4Ilex guayusa
Guayusa
PeppermintMentha x piperita
Melissa officinalisLemon Balm
CinnamonCinnamomum verumGinkgo biloba
Ginkgo
Herbal Adopters
Arnica Arnica montanaPhoto ©2017 Steven Foster
Adopt-an-Herb is an exciting and mutually beneficial way to support ABC!
Contact Denise Meikel at 512-926-4900 x120 or by email at [email protected]
Become an adopter today!Visit us at www.herbalgram.org/adopt
Theobroma cacaoCocoa Flavanols
Bacopa monnieriBacopa
Melaleuca alternifolia
Brassica oleracea Broccoli Group
Tea Tree
Broccoli
Boswellia serrata
Aspalathus linearis
Adansonia digitata
Urtica dioica
Sambucus nigra
Aronia melanocarpa
Bulbine natalensis
Cynara scolymus
Allium sativum
Helichrysum italicum
Indian Frankincense
Rooibos
Baobab
Stinging Nettle
Elderberry
Black Chokeberry
Bulbine
Artichoke
Garlic
Helichrysum
Zea maysPurple Corn
Curcuma longaTurmeric
Olive
Grape
Olea europaea
Vitis vinifera
Sceletium tortuosumSceletium
Vaccinium macrocarpon
Nigella sativa
Piper methysticum
Lepidium meyeniiRhodiola rosea
Cranberry
Black Cumin
Kava
MacaRhodiola
Harpagophytum spp.Devil's Claw
Coffea spp.Coffee Fruit
Garcinia cambogiaGarcinia
Humulus lupulusHops
Withania somniferaAshwagandha
Betula spp.Birch
Aloe veraAloe Vera
Malpighia spp.Acerola
Eurycoma longifoliaTongkat Ali
Visit us at www.herbalgram.org/adoptTo adopt, please contact us at [email protected]
Siraitia grosvenoriiMonk Fruit
Arnica montanaArnica
Hibiscus sabdariffaHibiscus
Continued on page 4Mitragyna speciosa
Kratom
Continued on page 4Ilex guayusa
Guayusa
PeppermintMentha x piperita
Melissa officinalisLemon Balm
CinnamonCinnamomum verumGinkgo biloba
Ginkgo
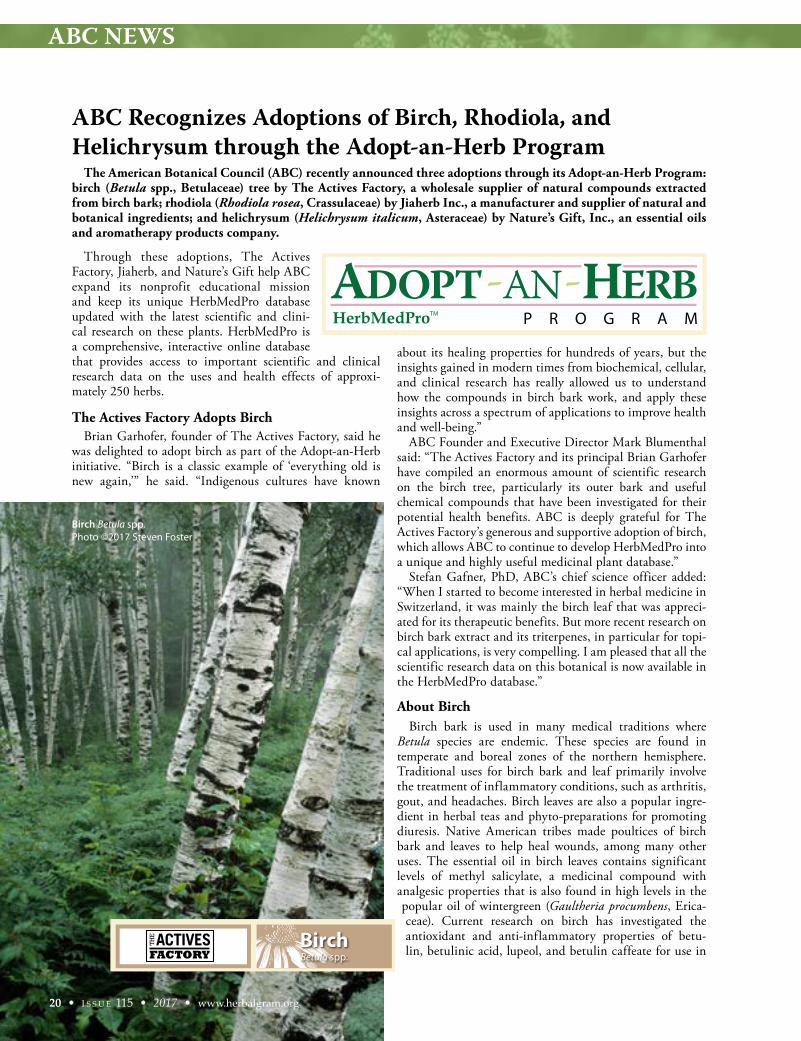
ABC NEWS
ABC Recognizes Adoptions of Birch, Rhodiola, and Helichrysum through the Adopt-an-Herb Program
Through these adoptions, The Actives Factory, Jiaherb, and Nature’s Gift help ABC expand its nonprofit educational mission and keep its unique HerbMedPro database updated with the latest scientific and clini-cal research on these plants. HerbMedPro is a comprehensive, interactive online database that provides access to important scientific and clinical research data on the uses and health effects of approxi-mately 250 herbs.
The Actives Factory Adopts BirchBrian Garhofer, founder of The Actives Factory, said he
was delighted to adopt birch as part of the Adopt-an-Herb initiative. “Birch is a classic example of ‘everything old is new again,’” he said. “Indigenous cultures have known
about its healing properties for hundreds of years, but the insights gained in modern times from biochemical, cellular, and clinical research has really allowed us to understand how the compounds in birch bark work, and apply these insights across a spectrum of applications to improve health and well-being.”
ABC Founder and Executive Director Mark Blumenthal said: “The Actives Factory and its principal Brian Garhofer have compiled an enormous amount of scientific research on the birch tree, particularly its outer bark and useful chemical compounds that have been investigated for their potential health benefits. ABC is deeply grateful for The Actives Factory’s generous and supportive adoption of birch, which allows ABC to continue to develop HerbMedPro into a unique and highly useful medicinal plant database.”
Stefan Gafner, PhD, ABC’s chief science officer added: “When I started to become interested in herbal medicine in Switzerland, it was mainly the birch leaf that was appreci-ated for its therapeutic benefits. But more recent research on birch bark extract and its triterpenes, in particular for topi-cal applications, is very compelling. I am pleased that all the scientific research data on this botanical is now available in the HerbMedPro database.”
About Birch Birch bark is used in many medical traditions where
Betula species are endemic. These species are found in temperate and boreal zones of the northern hemisphere. Traditional uses for birch bark and leaf primarily involve the treatment of inflammatory conditions, such as arthritis, gout, and headaches. Birch leaves are also a popular ingre-dient in herbal teas and phyto-preparations for promoting diuresis. Native American tribes made poultices of birch bark and leaves to help heal wounds, among many other uses. The essential oil in birch leaves contains significant levels of methyl salicylate, a medicinal compound with analgesic properties that is also found in high levels in the popular oil of wintergreen (Gaultheria procumbens, Erica-ceae). Current research on birch has investigated the antioxidant and anti-inflammatory properties of betu-lin, betulinic acid, lupeol, and betulin caffeate for use in
The American Botanical Council (ABC) recently announced three adoptions through its Adopt-an-Herb Program: birch (Betula spp., Betulaceae) tree by The Actives Factory, a wholesale supplier of natural compounds extracted from birch bark; rhodiola (Rhodiola rosea, Crassulaceae) by Jiaherb Inc., a manufacturer and supplier of natural and botanical ingredients; and helichrysum (Helichrysum italicum, Asteraceae) by Nature’s Gift, Inc., an essential oils and aromatherapy products company.
Theobroma cacaoCocoa Flavanols
Bacopa monnieriBacopa
Melaleuca alternifolia
Brassica oleracea Broccoli Group
Tea Tree
Broccoli
Boswellia serrata
Aspalathus linearis
Adansonia digitata
Urtica dioica
Sambucus nigra
Aronia melanocarpa
Bulbine natalensis
Cynara scolymus
Allium sativum
Helichrysum italicum
Indian Frankincense
Rooibos
Baobab
Stinging Nettle
Elderberry
Black Chokeberry
Bulbine
Artichoke
Garlic
Helichrysum
Zea maysPurple Corn
Curcuma longaTurmeric
Olive
Grape
Olea europaea
Vitis vinifera
Sceletium tortuosumSceletium
Vaccinium macrocarpon
Nigella sativa
Piper methysticum
Lepidium meyeniiRhodiola rosea
Cranberry
Black Cumin
Kava
MacaRhodiola
Harpagophytum spp.Devil's Claw
Coffea spp.Coffee Fruit
Garcinia cambogiaGarcinia
Humulus lupulusHops
Withania somniferaAshwagandha
Betula spp.Birch
Aloe veraAloe Vera
Malpighia spp.Acerola
Eurycoma longifoliaTongkat Ali
Visit us at www.herbalgram.org/adoptTo adopt, please contact us at [email protected]
Siraitia grosvenoriiMonk Fruit
Arnica montanaArnica
Hibiscus sabdariffaHibiscus
Continued on page 4Mitragyna speciosa
Kratom
Continued on page 4Ilex guayusa
Guayusa
PeppermintMentha x piperita
Melissa officinalisLemon Balm
CinnamonCinnamomum verumGinkgo biloba
Ginkgo
Theobroma cacaoCocoa Flavanols
Bacopa monnieriBacopa
Melaleuca alternifolia
Brassica oleracea Broccoli Group
Tea Tree
Broccoli
Boswellia serrata
Aspalathus linearis
Adansonia digitata
Urtica dioica
Sambucus nigra
Aronia melanocarpa
Bulbine natalensis
Cynara scolymus
Allium sativum
Helichrysum italicum
Indian Frankincense
Rooibos
Baobab
Stinging Nettle
Elderberry
Black Chokeberry
Bulbine
Artichoke
Garlic
Helichrysum
Zea maysPurple Corn
Curcuma longaTurmeric
Olive
Grape
Olea europaea
Vitis vinifera
Sceletium tortuosumSceletium
Vaccinium macrocarpon
Nigella sativa
Piper methysticum
Lepidium meyeniiRhodiola rosea
Cranberry
Black Cumin
Kava
MacaRhodiola
Harpagophytum spp.Devil's Claw
Coffea spp.Coffee Fruit
Garcinia cambogiaGarcinia
Humulus lupulusHops
Withania somniferaAshwagandha
Betula spp.Birch
Aloe veraAloe Vera
Malpighia spp.Acerola
Eurycoma longifoliaTongkat Ali
Visit us at www.herbalgram.org/adoptTo adopt, please contact us at [email protected]
Siraitia grosvenoriiMonk Fruit
Arnica montanaArnica
Hibiscus sabdariffaHibiscus
Continued on page 4Mitragyna speciosa
Kratom
Continued on page 4Ilex guayusa
Guayusa
PeppermintMentha x piperita
Melissa officinalisLemon Balm
CinnamonCinnamomum verumGinkgo biloba
Ginkgo
20 • I S S U E 115 • 2017 • www.herbalgram.org
Birch Betula spp.Photo ©2017 Steven Foster

ABC NEWS
www.herbalgram.org • 2017 • I S S U E 115 • 21
cosmetics, potential anticancer activity, and treatment of symptoms associated with human immunodeficiency virus (HIV) and hepatitis B and C viral infections.
About The Actives Factory Based in Two Harbors, Minnesota, The Actives Factory
supplies natural compounds extracted from the outer bark of the North American white birch (B. papyrifera). For nearly two decades, the company has led the manufac-ture of ethically sourced birch bark extract, highly puri-fied triterpenes, and specialized derivatives. The Actives Factory works with companies and manufacturers inter-ested in developing innovative birch-based formulations for dietary, skin care, and pharmaceutical products.
Jiaherb Adopts RhodiolaScott Chen, president of Jiaherb, said: “By supporting
the Adopt-an-Herb Program, we will be working together with ABC to ... help to educate the global herb commu-nity, including the botanical industry, about rhodi-ola, rhodiola’s traditional use, current applications, and sustainable development.”
Blumenthal said that “ABC is deeply grateful to Jiaherb for its generous support of ABC’s nonprofit educational mission via its adoption of Rhodiola rosea. There is increas-ing research and market interest in this adaptogenic root and its extracts, and ABC will be able to stay current with the scientific and clinical research on this important herb due to Jiaherb’s adoption.”
Chen noted that sustainability concerns for Rhodiola rosea have made research and conservation efforts particu-larly important. “In recent years, the sources of rhodiola have started to slowly diminish,” he said. “It is time for us to shift our attention to the sustainability of this naturally grown herb and its scientific use and benefits. We need to develop a sustainable future for rhodiola that will protect it from overharvest-ing, and to implement a solution that will protect the species from extinction.”
About RhodiolaRhodiola, also known as golden root, arctic root, and
roseroot, grows naturally at high altitudes and in arctic regions of Europe, North America, and Asia. Although it has long been used in traditional medicine for several disorders, it is mostly known as an adaptogenic herb used to help prevent and treat stress, mental and physical fatigue, depression, and to boost energy.
In Russia and Scandinavia, rhodiola has been used for centuries to cope with the cold climate and stress. It is also used to increase physical endurance and resistance to altitude sickness. The plant has been used in traditional Chinese medicine, where it is called hong jing tian. Scien-tists have identified about 140 compounds in the roots of rhodiola, including phenols, rosavin, rosin, rosarin, organic acids, terpenoids, phenolcarbonic acids and deriv-atives thereof, and flavonoids.
About JiaherbBased in Pine Brook, New Jersey, Jiaherb is an NSF
International-certified manufacturer of natural ingre-dients, including herbal extracts, powders, spices, and natural sweeteners. The company states that it has been committed to providing its customers with reliable and sustainable high-quality ingredients for more than 17 years. Jiaherb also says that its comprehensive and diverse sourcing program consists of a team of botanists and product specialists who travel the world looking for the best raw materials. The company has established programs that are designed to improve consumer confi-dence, including an identification verification program and a program with tracking procedures that control and verify product characteristics at every stage of the manu-facturing process, from arrival of raw materials through to storage, production, warehousing, and sales.
Theobroma cacaoCocoa Flavanols
Bacopa monnieriBacopa
Melaleuca alternifolia
Brassica oleracea Broccoli Group
Tea Tree
Broccoli
Boswellia serrata
Aspalathus linearis
Adansonia digitata
Urtica dioica
Sambucus nigra
Aronia melanocarpa
Bulbine natalensis
Cynara scolymus
Allium sativum
Helichrysum italicum
Indian Frankincense
Rooibos
Baobab
Stinging Nettle
Elderberry
Black Chokeberry
Bulbine
Artichoke
Garlic
Helichrysum
Zea maysPurple Corn
Curcuma longaTurmeric
Olive
Grape
Olea europaea
Vitis vinifera
Sceletium tortuosumSceletium
Vaccinium macrocarpon
Nigella sativa
Piper methysticum
Lepidium meyeniiRhodiola rosea
Cranberry
Black Cumin
Kava
MacaRhodiola
Harpagophytum spp.Devil's Claw
Coffea spp.Coffee Fruit
Garcinia cambogiaGarcinia
Humulus lupulusHops
Withania somniferaAshwagandha
Betula spp.Birch
Aloe veraAloe Vera
Malpighia spp.Acerola
Eurycoma longifoliaTongkat Ali
Visit us at www.herbalgram.org/adoptTo adopt, please contact us at [email protected]
Siraitia grosvenoriiMonk Fruit
Arnica montanaArnica
Hibiscus sabdariffaHibiscus
Continued on page 4Mitragyna speciosa
Kratom
Continued on page 4Ilex guayusa
Guayusa
PeppermintMentha x piperita
Melissa officinalisLemon Balm
CinnamonCinnamomum verumGinkgo biloba
Ginkgo
Rhodiola Rhodiola roseaPhoto ©2017 Steven Foster

ABC NEWS
Nature’s Gift Adopts Helichrysum According to Marge Clark, founder of Nature’s Gift,
“The Adopt-an-Herb Program is an invaluable educational opportunity from a highly trusted source. We appreciate the opportunity to help make more information available about Helichrysum italicum. There is not nearly enough research done about this remarkable plant and [its] amazing healing essential oil. Perhaps by our adopting it, more researchers will be inspired to study what we already know to be true: that the essential oil of H. italicum is an invaluable addition to a practitioner’s repertoire.”
Blumenthal said: “ABC deeply appreciates this adop-tion of helichrysum by Nature’s Gift. Helichrysum is an important medicinal and aromatic plant of the Mediter-ranean region, and it is becoming more popular in the marketplace, particularly in the area of essential oils and aromatherapy. Nature’s Gift’s adoption of helichrysum will greatly assist ABC in maintaining up-to-date records on the growing scientific research on this traditional medicinal and aromatic plant.”
About Helichrysum Helichrysum italicum, also known as immortelle, is a
member of the daisy family. The small shrub, which is sometimes called curry plant due to its aroma, has yellow flowers and grows to 30-70 centimeters (11.8-27.6 inches) in height. Helichrysum italicum contains essential oil and a variety of phytochemicals, including flavonoids, triter-penes, acetophenone derivatives, and phloroglucinols. Both the flowers and leaves of H. italicum have been used tradi-tionally in the Mediterranean and surrounding regions for respiratory, digestive, and skin conditions. Various prepara-tions of the plant have also been used historically for their anti-inflammatory and antimicrobial properties, which are supported by data from in vitro studies.
About Nature’s GiftProviding pure authentic essential oils for therapeutic
purposes and offering information on their safe and effec-tive use is at the heart of the Nature’s Gift mission. Based in Madison, Tennessee, Nature’s Gift has had an online presence for well over two decades, and the company works
with hospitals, hospices, pharmacies, clinical nursing programs, and educational institutions as a supplier of essential oils and aromatherapy products and accessories. The company offers retail, bulk, and wholesale options to meet nearly any aromatherapy need. Professional discounts are also available for health care practitioners.
About Adopt-an-Herb and HerbMedPro The Actives Factory, Jiaherb, and Nature’s Gift are
among the 45 companies that have supported ABC’s educational efforts to collect, organize, and disseminate reliable, traditional, science-based, and clinical infor-mation on herbs, medicinal plants, and other botani-cal- and fungal-based ingredients through the Adopt-an-Herb Program. This program encourages companies, organizations, and individuals to “adopt” one or more specific herbs for inclusion and ongoing maintenance in the HerbMedPro database. To date, 50 herbs have been adopted.
Each adopted herb is continuously researched for new articles and studies, ensuring that its HerbMedPro record stays current and robust. The result is an unparal-leled resource not only for researchers, health profession-als, industry, and consumers, but for all members of the herbal and dietary supplements community.
HerbMedPro is available to ABC members at the Academic level and higher. Its “sister” site, HerbMed, is free and available to the public. In keeping with the ABC’s position as an independent research and education organization, herb adopters do not influence the scientific information that is compiled for their respective adopted herbs.
—ABC Staff
22 • I S S U E 115 • 2017 • www.herbalgram.org
Theobroma cacaoCocoa Flavanols
Bacopa monnieriBacopa
Melaleuca alternifolia
Brassica oleracea Broccoli Group
Tea Tree
Broccoli
Boswellia serrata
Aspalathus linearis
Adansonia digitata
Urtica dioica
Sambucus nigra
Aronia melanocarpa
Bulbine natalensis
Cynara scolymus
Allium sativum
Helichrysum italicum
Indian Frankincense
Rooibos
Baobab
Stinging Nettle
Elderberry
Black Chokeberry
Bulbine
Artichoke
Garlic
Helichrysum
Zea maysPurple Corn
Curcuma longaTurmeric
Olive
Grape
Olea europaea
Vitis vinifera
Sceletium tortuosumSceletium
Vaccinium macrocarpon
Nigella sativa
Piper methysticum
Lepidium meyeniiRhodiola rosea
Cranberry
Black Cumin
Kava
MacaRhodiola
Harpagophytum spp.Devil's Claw
Coffea spp.Coffee Fruit
Garcinia cambogiaGarcinia
Humulus lupulusHops
Withania somniferaAshwagandha
Betula spp.Birch
Aloe veraAloe Vera
Malpighia spp.Acerola
Eurycoma longifoliaTongkat Ali
Visit us at www.herbalgram.org/adoptTo adopt, please contact us at [email protected]
Siraitia grosvenoriiMonk Fruit
Arnica montanaArnica
Hibiscus sabdariffaHibiscus
Continued on page 4Mitragyna speciosa
Kratom
Continued on page 4Ilex guayusa
Guayusa
PeppermintMentha x piperita
Melissa officinalisLemon Balm
CinnamonCinnamomum verumGinkgo biloba
Ginkgo
Helichrysum italicumPhoto ©2017 Steven Foster

www.herbalgram.org • 2017 • I S S U E 115 • 23
BOTANICAL ADULTERANTS PROGRAM NEWS
The LGD is the third publication from the program deal-ing with the adulteration of GFSE. In 2012, the program published a review of scientific papers on the adulteration of GFSE in HerbalGram issue 94. In March 2017, the program published a Botanical Adulterants Bulletin that reviews all of the available evidence that documents concerns about adulteration of GFSE with synthetic antimicrobial compounds.
The new LGD is the first detailed review of currently available laboratory analytical methods to identify synthetic antimicrobial compounds in products labeled to contain GFSE. GFSEs, which have no known history of use in traditional herbal medicine, are marketed as dietary supple-ments with antimicrobial activity and as natural preserva-tives for personal care and cosmetic products.
These analyses include techniques such as high-perfor-mance liquid chromatography (HPLC) with ultraviolet (HPLC-UV) or mass spectrometric (HPLC-MS) detection, thin-layer chromatography (TLC), gas chromatography-mass spectrometry (GC-MS), and nuclear magnetic reso-nance (NMR) spectrometry.
As with the program’s two previous publications on GFSE, the LGD was written by John Cardellina, PhD, chief technical consultant and associate editor of the Botan-ical Adulterants Program. It was peer-reviewed by program partners and five experts from independent contract analyt-ical laboratories and the herb and dietary supplement indus-try.
The program’s LGDs are intended for quality control personnel and lab technicians in the herbal medicine, botanical ingredient, dietary supplement, and food sectors of industry, to help them choose the most appropriate tech-
niques and methods for their specific analytical needs. The LGDs provide reliable, expert guidance on suitable meth-ods to comply with the mandate to establish identity as an integral part of the testing requirements (identity, purity, strength, and composition) outlined in the US Food and Drug Administration’s (FDA’s) current Good Manufac-turing Practices (cGMPs) for dietary supplements and/or conventional foods, as well as government-mandated cGMPs in other countries.
ABC Chief Science Officer Stefan Gafner, PhD, commented: “The changing nature of the antimicrobial compounds used to adulterate various batches of GFSE complicates the selection of an appropriate analytical method. A non-targeted approach, which means the use of a method in which the compounds to be analyzed are not known, is required for the detection of these adulterants. Due to their ability to identify the presence of synthetic microbicides at low concentrations, GC-MS and HPLC-MS are particularly well-suited to meet the challenge.”
ABC Founder and Executive Director Mark Blumenthal, who is also the director of the Botanical Adulterants Program, said: “As we have noted previously, adulteration of GFSE with synthetic industrial disinfectant chemicals is a particularly egregious practice. We believe that this should be the subject of appropriate regulatory action by the FDA.”
The GFSE LGD is the 31st peer-reviewed publication of the Botanical Adulterants Program and the fourth publica-tion in the series of LGDs. All publications of the program are freely accessible to ABC members, registered users of the ABC website, and all members of the public after registra-tion on the ABC website.
—ABC Staff
New Laboratory Guidance Document Details Appropriate Methods of Analysis to Detect Synthetic Antimicrobial Compounds Sold as Grapefruit Seed Extract
The ABC-AHP-NCNPR Botanical Adulterants Program has published a new Laboratory Guidance Document (LGD) on grapefruit (Citrus paradisi, Rutaceae) seed extract (GFSE).
1 G r a p e f r u i t S e e d E x t r a c t - L a b o r a t o r y G u i d a n c e D o c u m e n t • 2017 • www.botanicaladulterants.org
Keywords: Citrus paradisi, Rutaceae, grapefruit seed extract, GFSE, adulterant, adulteration, benzalkonium chloride, benzethonium chloride, triclosan
1. PurposeThe case of synthetic microbicides marketed as grapefruit seed extract (GFSE) differs from the other botanicals addressed
thus far by the Botanical Adulterants Program (BAP), in that the adulteration does not consist of substitution by or inclu-sion of other botanicals, but rather the inclusion of one or more synthetic microbicidal compounds (disinfectants) in the products. Therefore, this Guidance Document presents a review of the analytical technologies used to differentiate and identify the various microbicides that have been reported from commercial GFSE products, as well as methods to separate and identify natural grapefruit seed constituents.
2. ScopeWe are unaware of any pharmacopoeial standards or monographs for grapefruit seed extract. In addition, some of the
commercial GFSE products are reportedly prepared from dried, ground seeds that are boiled in water and distilled; that distillate is then treated with ascorbic acid, hydrochloric acid, and ammonium chloride under heat and pressure; this treat-ment purportedly produces microbicidal compounds resembling benzethonium chloride from the flavonoids in the grape-fruit seeds.1 However, there are no known natural or synthetic chemical pathways whereby the natural constituents of grapefruit seed could be transformed into such compounds, using the reagents listed above under the conditions described. It simply defies the logic and state of our knowledge of synthetic organic chemistry and biosynthesis. More interestingly, the majority of published analyses of GFSE products report only man-made microbicidal compounds and no compounds typical of grapefruit or any citrus fruit (e.g., flavonoids, limonoids, or essential oils).
Complicating the selection of an analytical method is the observation that the microbicidal compounds detected in GFSE products have changed over time. Therefore, the ideal analytical method should be flexible enough to detect and quantify not only any and all microbicides previously found in GFSE, but perhaps also any other similar, commercially available microbicidal compounds.
The recommendation of a specific method or methods in this Laboratory Guidance Document for testing GFSE materi-als does not take away the responsibility of laboratory personnel to demonstrate adequate method performance in their own laboratory using accepted protocols outlined in the 21 CFR Part 111 and by AOAC International, ISO, WHO, and ICH.
3. Common and Scientific Names3.1 Common name: grapefruit seed extract (GFSE)
3.2 Other common names:
French: Extrait de pépins de pamplemousseGerman: Grapefruitkern ExtraktItalian: Estratto di semi di pompelmoSpanish: Extracto de semilla de pomelo
3.3 Accepted Latin binomial: Citrus paradisi Macfad.2
3.4 Synonyms: Citrus x paradisi3
3.5 Botanical family: Rutaceae
Grapefruit Seed ExtractLaboratory Guidance DocumentBy John H. Cardellina II, PhD*
*ReevesGroup, Virginia Beach, VA 23451, [email protected] Seed Citrus paradisi. Photo ©2017 Steven Foster

WORLD NEWS
24 • I S S U E 115 • 2017 • www.herbalgram.org
This kesum farm is purportedly one of the largest of its kind, just a half-hour drive from Malaysia’s largest city Kuala Lumpur, near the famous Batu caves in Gombak. Kesum requires 90 days to grow to maturity from seed, according to Ismail. The aromatic herb, also known as laksa leaf, is popular in Southeast Asian cookery, loves water, and is best cultivated like rice (Oryza sativa, Poaceae) in paddies. In the case of Ismail’s farm, the paddy is fed by a stream that flows out of a dense rainforest.
It is January 2017, and I am traveling in the company of Nik Fahmi and Tengku Sharir of Biotropics Malaysia, a Malaysian government-owned botanical extraction and marketing company that specializes in plants native to the country. Due to an increased interest in the health benefits of kesum leaves, the government operation has taken an interest in this plant. As we continue our exploration of kesum, various other members of the Biotropics team will join us. Our plan is to investigate this popular savory herb, and to meet with people who understand its broad culinary and medicinal uses. Our visit to the kesum farm kicks off a week of traveling the countryside.
I stoop to pick a couple of leaves of fresh kesum that is one week from harvest. Rolling the leaves between my
thumb and forefinger releases aromatic compounds that smell like a blend of oregano (Origanum vulgare, Lamiaceae) and basil (Ocimum basilicum, Lamiaceae), with some other notes mixed in. It is an aroma I recognize from Malaysian, Thai, and Vietnamese dishes. The plant is a slender creep-ing shrub with climbing branches that stretch 1-1.5 meters (3.3-4.9 feet), and the green leaves are long and lanceo-late. In Malaysia and in the US Department of Agricul-ture’s PLANTS database, kesum is also called pygmy smart weed.1
After walking through several acres of cultivated kesum, we are led to a large shed where men are bundling kesum into bunches and listening to loud music. The men work quickly, converting large piles of the freshly harvested herb into bunches that will be sold in local markets later that day. The turnaround is fast. Kesum is picked, bundled, trucked to market, and sold fresh.
The leaf of kesum is used in numerous popular dishes in the traditional cuisines of Malaysia, Thailand, Vietnam, and Indonesia. The name “laksa leaf” refers to its use in the tradi-tional spicy noodle soup dish laksa. It is also known in Malay-sian cuisine as an ingredient in ulam, or salad, and is eaten finely sliced with other raw vegetables. It is a main ingre-
dient in the mango (Mangifera indica, Anacardiaceae)-based salad kerabu, and is a principal flavor in the rice dish nasi ulam.2
The leaf of kesum is known to contain an array of antioxidant compounds, including flavonoids, aliphatic aldehydes, and phenols, such as rutin, coumaric acid, quer-cetin, and gallic acid.3-5 Studies by Baharum et al. detected 48 compounds in the essential oil of kesum using mass spectrom-etry.6 These studies and the work by Vikram et al. provide greater insight into the complexity of the leaves.3
In the Land of KesumBy Chris Kilham
Editor’s note: This article was first published in the July 2017 issue of HerbalEGram, the American Botanical Council’s (ABC’s) monthly e-newsletter. Readers can find the original article, which features eight video clips produced by Chris Kilham, on ABC’s website.
At 85 years of age, Ismail looks fit and strong. The former Malaysian military commando now runs a small farm, overseeing a kesum (Persicaria minor syn. Polygonum minus, Polygonaceae) cultivation program that provides a metric ton (roughly 2,200 pounds) of the fresh herb to local markets every day. Ismail’s wife, Su, is more hands-on, personally working the harvest and keeping watch over other harvesters and the small group of workers who bundle bunches of fresh kesum plants with rubber bands.
Persicaria minor or Polygonum minus, a Southeast Asian herb used in cookery and as a tradi-tional medicine.
Photo ©2017 Chris Kilham

WORLD NEWS
www.herbalgram.org • 2017 • I S S U E 115 • 25
Published chemical analyses and in vitro pharmacologi-cal studies suggest that kesum leaves have antibacterial, antifungal, antioxidant, antiviral, cytotoxic, and cytopro-tective properties.2,3
The Forest Research Institute Malaysia (FRIM) in Kepong, Selangor, sits amid 544 hectares (roughly 1,344 acres) of landscaped grounds and verdant forest, and is a brief drive from the center of Kuala Lumpur. Surrounded by Bukit Lagong Forest Reserve, FRIM is Malaysia’s hub for forestry research and conservation. The FRIM herbarium contains more than 350,000 voucher samples that feature the flora of peninsular Malaysia and Sabah. Researchers at FRIM inves-tigate a wide array of plants, from Malaysian trees to food crops endemic to the region, and the center in Selangor over-sees research stations in various parts of Malaysia.
At the ethnobotany department of FRIM, researcher Tan Ai Lee shares the latest developments on kesum. The plant is undergoing a name change, we are informed, from Polygonum minus to Persicaria minor. We subsequently confirm this through correspondence with the Interna-tional Plant Names Index (IPNI). According to IPNI Editor Kanchi Gandhi of Harvard University: “Polygonum minus and Persicaria minor: both are correct names, and it is up to an individual to accept” (email, January 23, 2017).
According to Lee, FRIM has taken the unusual position of developing two kesum-based health product concepts, neither of which was being sold in the marketplace at the time of our visit. We are shown packaging, literature, and product samples. The first, called Kezo Kesum Leaves Seasoning, offers a convenient way to season local dishes with a mixture of dried kesum leaves and sea salt. The second product, called Digesto Digestive Drink, is an “antioxidant digestive beverage.” According to the FRIM literature accompanying this product: “Traditional medicine claims that a decoction of the fresh leaves of kesum is taken as a remedy for indi-gestion, constipation, flatulence and as a remedy for stomach pains.”
Launching products is a new idea for FRIM, the staff of which has not previously engaged in commercial enterprises of this type. A couple of the staff members there expressed to us that marketing health products was an endeavor far removed from their usual course of work.
Lee said that the FRIM product development program with kesum reflects the high regard with which FRIM researchers assess this traditional herb.
Traditional Malaysian Medicine Wisdom: A Conversation with Datin Sharifah Anisah
Datin Sharifah Anisah is popularly regarded as an expert on traditional Malaysian medicine, with a focus on women’s health. The subject of numerous articles, Datin Sharifah first provided herb-based therapies and spa treatments in the 1960s. She lectures widely on herbal approaches to health care, has appeared in popular Malaysian publications, and received the Jati Wanita (Teak Women) Award in 2003 from the United Malays National Organization (UMNO).
On a shaded cottage porch at Taman Botani Negara Shah Alam (TBNSA), a botanical garden where visitors can also stay in reconstructed traditional wooden Malaysian houses, Datin Sharifah and I sit to discuss traditional uses of kesum. The location seems perfect for our conversation. TBNSA sports forest acreage, plantations, and gardens.
“In our country, kesum is widely used by Malaysians,” she tells me. “The Malays and the Chinese use it in their food. They believe that kesum is part of health and beauty.”
Datin Sharifah explains that kesum is often added to fish, and that in this manner the herb is a valuable diges-tive cleansing agent. “We believe that kesum is very good for internal cleansing. It helps for flatulence, you know, ‘wind.’”
Top image: Women purchase kesum in the Pasar Siti Khadijah, a market run by women in Kota
Bharu, Kelantan, Malaysia.
Bottom image: Fresh ingredients, including kesum, for making nasi ulam, a traditional
Malaysian rice salad.
Photos ©2017 Chris Kilham

WORLD NEWS
26 • I S S U E 115 • 2017 • www.herbalgram.org
According to Datin Sharifah, kesum is often taken as an infusion for medicinal purposes, and is typically mixed with other herbs. “The Malays use it for the internal cleans-ing, especially for mothers after birth,” she said. “It helps to prevent and overcome postpartum problems.”
From a cosmetic standpoint, she noted that “kesum is often used for the skin, especially for stretch marks.”
For external use, she explained, the kesum leaves are ground into a paste and applied directly to skin. “You make the paste and you add in rice, and sometimes you add in turmeric [Curcuma longa, Zingiberaceae], and sometimes tamarind [Tamarindus indica, Fabaceae] juice. It is very effective to heal the stretch marks.”
Over the course of an hour, Datin Sharifah shared with me various traditional Malaysian approaches to the use of kesum and other herbs, for a broad range of health needs, from relieving indigestion and ulcers to enhancing vaginal health. I noted that her easy manner and broad knowledge of traditional herbal preparations and their uses made Datin Sharifah Anisah a treasure, much in the way that Amazo-nian shamans are considered “living libraries.”
Cooking with Kesum: A Discussion with Chef Ismail Ahmad
Malaysia, with its diverse regional cuisines, is not only a foodie paradise, but also a land where excellent chefs can make a reputation for themselves. Among the celebrated chefs in the country, Ismail Ahmad stands out as one of the most beloved and well-known. Flamboyant, funny, creative, and smart, Chef Ismail runs Restaurant Rebung in Kuala Lumpur, a mecca for those who seek authentic Malaysian country food. At noon sharp, when the doors of the restau-rant open, a crowd streams in, mostly women in hijab, their destination being the seemingly endless buffet.
Chef Ismail attempts modesty, but all the locals seem to know his celebrity, and patrons of the Restaurant Rebung look for him just to shake his hand and express thanks. Chef Ismail has appeared on the Asian Food Channel, Anthony Bourdain’s “No Reservations,” “Yan Can Cook,” “Aroma,” “Sri Murni,” “Poh’s Kitchen,” “Hey Good Cooking,” “Wok and Roll,” and a number of other food-related television programs.
The food at his restaurant is something to see: the vege-table dishes, soups, salads, various rice preparations, curries of all types, broiled and otherwise prepared fish and meats — every dish offers a different color, texture, and fragrance than the ones around it. There is magic in this cookery, which is aided by the herbs that Ismail grows on the restau-rant terrace, and by his upbringing in the Malaysian coun-tryside where he learned about herbs and cookery from his grandmother.
“My grandparents brought me up with organics, things that grow around the garden like pumpkins [Cucurbita pepo, Cucurbitaceae], bananas [Musa spp., Musaceae], cassava [Manihot esculenta, Euphorbiaceae], turmeric, fresh coconut [Cocos nucifera, Arecaceae], and river fishes,” Ismail explains. “It was very rare that we had meat.”
“What were some of the foods that were your favorites when you were a kid?” I ask.
“Oh, I love pumpkin; I love young bananas; oh, I love young jackfruit [Artocarpus heterophyllus, Moraceae]. My grandmother would make curries, you know.”
“Was your grandmother a great cook?” “She was limited because she did not travel around, but
she cooked the best village food.”Ismail beams when he talks about his grandmother.On a table before us, Ismail has laid out in bowls all of the
ingredients needed to make the mango salad kerabu, which uses a large portion of kesum. “Normally a salad like this we eat when the weather outside is too hot, and we want some-thing fresh and crunchy…. Kesum is my main ingredient. The leaf, you shred it very fine.”
As I watch Ismail perform his culinary magic, he describes every ingredient, and how all the ingredients are put together, as he concocts the salad. When he is done, three women who call themselves “The Fit Ladies of Kuala Lumpur” and I sample the salad. It is savory, citrusy, and fresh. We all pronounce it delicious. One of the Fit Ladies gets a bit teary-eyed, and comments that she hasn’t tasted a dish like this since she was a young girl.
We fly to Kota Bharu, south of Kuala Lumpur in Kelan-tan state, to visit the legendary Pasar Siti Khadijah, a very large and colorful market run almost entirely by women. The dry market features household goods, knives, brooms, and all manner of general supplies, while the wet market features fish, meat, fruits, vegetables, herbs, and spices. A mezzanine level affords a colorful view of all the food stalls, where a seemingly endless array of fruits, vegetables, and spices are displayed in large piles.
We make our way into the wet market, and immediately spot large piles of kesum stacked at almost every stall. As we stand near one stall, a woman approaches the vendor, and purchases a generous armload of kesum. We follow her upstairs to the restaurant area, and watch her finely chop the pile of kesum for the salads that will be served over the next few hours. She laughs at me as I take her photo. I kid her a bit, and that makes her chop faster. She seems to enjoy the moment.
After observing the food preparation, we purchase a few of the local dishes prepared by women running small stands and restaurants at the Pasar Siti Khadijah. I make sure to order something with kesum: an ulam, an aromatic and tangy salad with other finely-sliced vegetables, hot chiles (Capsicum spp., Solanaceae), salt, and a hint of lime (Citrus hystrix, Rutaceae) — very nice.
Investigating Kesum: An Interview with Annie George, MD
Back in Kuala Lumpur, I sit with Annie George, MD, senior manager of science and clinical trials at Biotropics, where investigation into the properties of kesum has been ongoing for a few years. I asked Annie: “I’m curious to know, of all the herbs you could investigate in Malaysia, what made you choose kesum?”

WORLD NEWS
www.herbalgram.org • 2017 • I S S U E 115 • 27
“Back in the year 2011, we were actually investigating several of the well-known herbs in Malaysia, also looking at the salads consumed by the people, and we tested them for antioxidant activity initially. We found that kesum itself has very high antioxidant values,” she said.
The high antioxidant value of kesum, as determined by standard ORAC* testing, was the first piece of information that set kesum apart from the other herbs being studied.
She continued: “What was very interesting was that it has this quer-cetin-3-O-glucuronide, and this particular compound has been shown to reduce beta amyloids, and beta amyloids, you find that a lot in patients with Alzheimer’s.”
Annie teamed up with Suzana Shahar, PhD, head of research at the Faculty of Health at the National Univer-sity of Malaysia (Universiti Kebangsaan Malaysia). Suzana's work focuses on dietary practices that help maintain good health and protect against degenerative diseases. Annie and Suzana thought that kesum seemed like the right candidate for a study on cognition. If it showed activity, it might help the elderly.
The possible cognitive effects of kesum were put to the test in a study of 35 healthy women, half of whom were given a concentrated water extract of kesum (20:1 ratio) daily (BioKesum Biotropics), while the other half received a placebo (maltodextrin). At the beginning of the study, after three weeks, and after six weeks, the subjects participated in a series of psychological and intelligence tests. The kesum extract group scored higher in overall good mood, short-term memory, and IQ. Several parameters of cognitive function also improved. This 2015 study, published in the medical journal Clinical Interventions in Aging, has piqued interest in the popular herb.7 Living up to its folk name “smart weed,” kesum appears to act as a nootropic, enhancing cognitive function. Both Annie and Suzana acknowledge that addi-tional studies may bolster this use, but they are happy with the results of this preliminary study.
My week of chasing kesum in Kuala Lumpur and other parts of Malaysia revealed several things. First, I was already familiar with the flavor and aroma of kesum, but didn’t know it yet: The herb was immediately recognizable once I smelled it and put it into my mouth. Second, the fresh herb bright-ens up dishes and makes a terrific salad ingredient. Finally, the herb is long-established as a traditional remedy, especially for digestive issues, but for others, too. The potential cogni-tive benefits of kesum, as investigated in the 2015 study, may prove to be consistent with the herb’s “smart weed” moniker.
Considering kesum’s traditional use as a food, its
presumed and observed safety, and its various known biological activities, it isn’t a stretch to suggest that it may be smart to consume this herb.
References1. Polygonum minus Huds. United States Department of Agricul-
ture Natural Resources Conservation Service website. Avail-able at: https://plants.usda.gov/core/profile?symbol=POMI22. Accessed July 10, 2017.
2. Christapher PV, Parasuraman S, Christina JMA, Asmawi MZ, Vikneswaran M. Review on Polygonum minus. Huds, a commonly used food additive in Southeast Asia. Pharmacognosy Research. 2015;7(1):1-6. doi:10.4103/0974-8490.147125.
3. Vikram P, Chiruvella KK, Ripain IHA, Arifullah M. A recent review on phytochemical constituents and medicinal proper-ties of kesum (Polygonum minus Huds.). Asian Pacific Journal of Tropical Biomedicine. 2014;4(6):430-435. doi:10.12980/APJTB.4.2014C1255.
4. Urones JG, Marcos IS, Pérez BG, Barcala PB. Flavonoids from Polygonum minus. Phytochemistry. 1990;29:3687-3689.
5. Yaacob KB. Kesom oil — a natural source of aliphatic alde-hydes. Perfum Flavor. 1987;12:27–30.
6. Baharum SN, Bunawan H, Ghani MA, Mustapha WAW, Noor NM. Analysis of the chemical composition of the essen-tial oil of Polygonum minus Huds. using two-dimensional gas chromatography-time-of-flight mass spectrometry (GC-TOF MS). Molecules. 2010 Oct 12;15(10):7006-7015.
7. Shahar S, Aziz AF, Ismail SNA, et al. The effect of Polygonum minus extract on cognitive and psychosocial parameters according to mood status among middle-aged women: a randomized, double-blind, placebo-controlled study. Clin Interv Aging. 2015 Sep 22;10:1505-20. doi: 10.2147/CIA.S86411.
Medicine Hunter Chris Kilham with celebrity chef
Ismail Ahmad, of Restaurant Rebung in Kuala Lumpur.
Photo ©2017 Chris Kilham
* ORAC (Oxygen Radical Absorbance Capacity) is an in vitro laboratory assay of the antioxidant value of a substance, and does not necessarily directly relate to the actual antioxidant activity of a substance when ingested by humans.
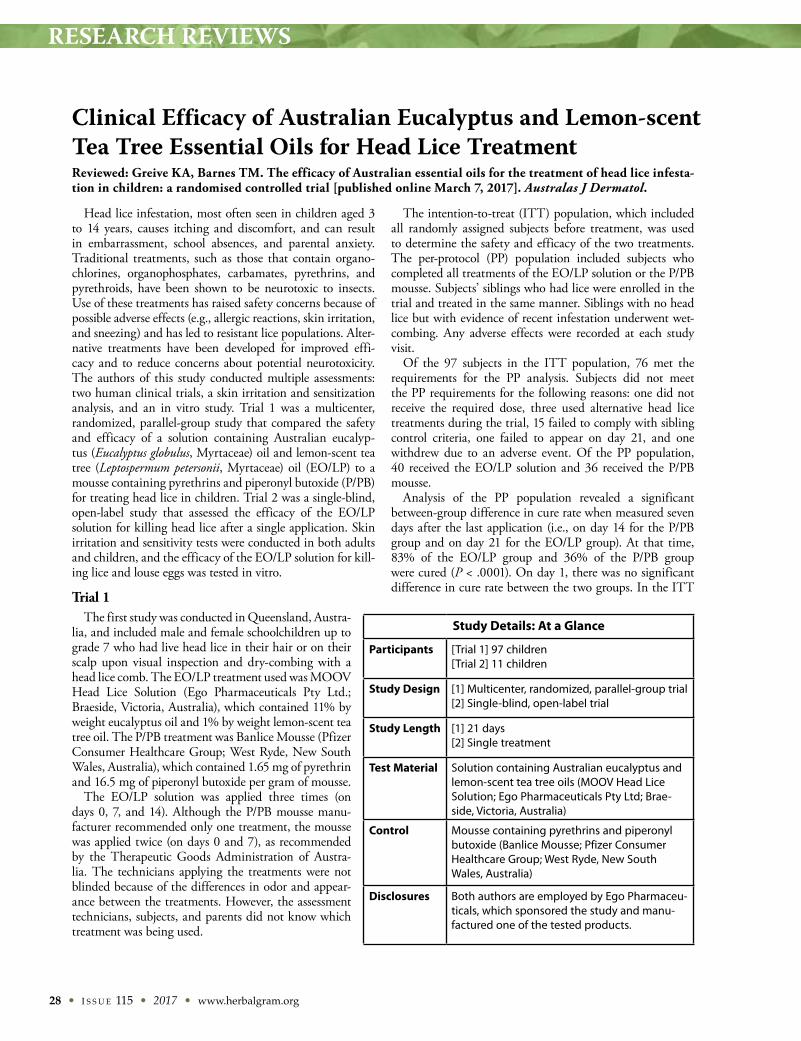
RESEARCH REVIEWS
28 • I S S U E 115 • 2017 • www.herbalgram.org
Head lice infestation, most often seen in children aged 3 to 14 years, causes itching and discomfort, and can result in embarrassment, school absences, and parental anxiety. Traditional treatments, such as those that contain organo-chlorines, organophosphates, carbamates, pyrethrins, and pyrethroids, have been shown to be neurotoxic to insects. Use of these treatments has raised safety concerns because of possible adverse effects (e.g., allergic reactions, skin irritation, and sneezing) and has led to resistant lice populations. Alter-native treatments have been developed for improved effi-cacy and to reduce concerns about potential neurotoxicity. The authors of this study conducted multiple assessments: two human clinical trials, a skin irritation and sensitization analysis, and an in vitro study. Trial 1 was a multicenter, randomized, parallel-group study that compared the safety and efficacy of a solution containing Australian eucalyp-tus (Eucalyptus globulus, Myrtaceae) oil and lemon-scent tea tree (Leptospermum petersonii, Myrtaceae) oil (EO/LP) to a mousse containing pyrethrins and piperonyl butoxide (P/PB) for treating head lice in children. Trial 2 was a single-blind, open-label study that assessed the efficacy of the EO/LP solution for killing head lice after a single application. Skin irritation and sensitivity tests were conducted in both adults and children, and the efficacy of the EO/LP solution for kill-ing lice and louse eggs was tested in vitro.
Trial 1The first study was conducted in Queensland, Austra-
lia, and included male and female schoolchildren up to grade 7 who had live head lice in their hair or on their scalp upon visual inspection and dry-combing with a head lice comb. The EO/LP treatment used was MOOV Head Lice Solution (Ego Pharmaceuticals Pty Ltd.; Braeside, Victoria, Australia), which contained 11% by weight eucalyptus oil and 1% by weight lemon-scent tea tree oil. The P/PB treatment was Banlice Mousse (Pfizer Consumer Healthcare Group; West Ryde, New South Wales, Australia), which contained 1.65 mg of pyrethrin and 16.5 mg of piperonyl butoxide per gram of mousse.
The EO/LP solution was applied three times (on days 0, 7, and 14). Although the P/PB mousse manu-facturer recommended only one treatment, the mousse was applied twice (on days 0 and 7), as recommended by the Therapeutic Goods Administration of Austra-lia. The technicians applying the treatments were not blinded because of the differences in odor and appear-ance between the treatments. However, the assessment technicians, subjects, and parents did not know which treatment was being used.
The intention-to-treat (ITT) population, which included all randomly assigned subjects before treatment, was used to determine the safety and efficacy of the two treatments. The per-protocol (PP) population included subjects who completed all treatments of the EO/LP solution or the P/PB mousse. Subjects’ siblings who had lice were enrolled in the trial and treated in the same manner. Siblings with no head lice but with evidence of recent infestation underwent wet-combing. Any adverse effects were recorded at each study visit.
Of the 97 subjects in the ITT population, 76 met the requirements for the PP analysis. Subjects did not meet the PP requirements for the following reasons: one did not receive the required dose, three used alternative head lice treatments during the trial, 15 failed to comply with sibling control criteria, one failed to appear on day 21, and one withdrew due to an adverse event. Of the PP population, 40 received the EO/LP solution and 36 received the P/PB mousse.
Analysis of the PP population revealed a significant between-group difference in cure rate when measured seven days after the last application (i.e., on day 14 for the P/PB group and on day 21 for the EO/LP group). At that time, 83% of the EO/LP group and 36% of the P/PB group were cured (P < .0001). On day 1, there was no significant difference in cure rate between the two groups. In the ITT
Study Details: At a Glance
Participants [Trial 1] 97 children [Trial 2] 11 children
Study Design [1] Multicenter, randomized, parallel-group trial [2] Single-blind, open-label trial
Study Length [1] 21 days [2] Single treatment
Test Material Solution containing Australian eucalyptus and lemon-scent tea tree oils (MOOV Head Lice Solution; Ego Pharmaceuticals Pty Ltd; Brae-side, Victoria, Australia)
Control Mousse containing pyrethrins and piperonyl butoxide (Banlice Mousse; Pfizer Consumer Healthcare Group; West Ryde, New South Wales, Australia)
Disclosures Both authors are employed by Ego Pharmaceu-ticals, which sponsored the study and manu-factured one of the tested products.
Clinical Efficacy of Australian Eucalyptus and Lemon-scent Tea Tree Essential Oils for Head Lice Treatment Reviewed: Greive KA, Barnes TM. The efficacy of Australian essential oils for the treatment of head lice infesta-tion in children: a randomised controlled trial [published online March 7, 2017]. Australas J Dermatol.
RESEARCH REVIEWS
www.herbalgram.org • 2017 • I S S U E 115 • 29
subjects, seven days after the last application, 71% of the EO/LP group and 33% of the P/PB group were cured (P = .0002). No significant between-group difference in cure rate was observed on day 1.
Of the 97 subjects who received at least one treatment, 21 adverse effects were reported in 13 subjects. The 18 adverse effects reported in the EO/LP group included transient mild-to-moderate sensations, such as itchiness, stinging, or burning that lasted no more than five minutes and required no treat-ment. The three adverse effects in the P/PB group included one crawling sensation and two stinging sensations.
Trial 2In the second trial, 11 subjects with live lice received treat-
ment with the EO/LP solution on day 0. The authors report that after the single EO/LP application, all of the 1,418 head lice collected from the children were considered dead as they were wet-combed out of the hair. Upon repeat examination 30 minutes after combing, all lice were confirmed dead.
Skin Irritation and Sensitivity StudyThe skin irritation and sensitivity study included separate
groups of both adults and children. Fifty-three of the 56 adult subjects (aged 28 to 74 years) enrolled in this study completed it. The three who withdrew from the study did so for reasons unrelated to the study protocol. A patch containing the EO/LP solution was applied to the skin of the back for 24 hours every Monday, Wednesday, and Friday for three consecutive weeks. Then, 10 to 14 days after the last application, a “challenge or retest dose” was applied to a previously unexposed test site on the skin of each subject and assessed 24 and 48 hours later. The authors observed no erythema (reddening of the skin), edema (inflammation of the skin), or adverse effects.
For the pediatric testing of skin irritation and sensitivity, the EO/LP solution was applied to the scalp, face, and neck of 20 children (aged six months to four years) on days 0, 7, and 14. The subjects were evaluated after each application and again 24 hours after the last application. The authors observed no test-related irritation, and the subjects (and their parents or guardians) made no “safety-related comments.”
In Vitro AssessmentsAs part of the in vitro component of the study, the authors
immersed louse eggs in the EO/LP solution and a control solution (purified water). The authors observed that no louse eggs hatched for 10 days after a 10-second immersion in the EO/LP solution. Following immersion in the control solu-tion, 92% of the louse eggs had hatched after 10 days.
In another in vitro analysis, the authors submerged live body lice in the EO/LP solution and control solution for 10 minutes. Sixty minutes after immersion, the authors observed that 100% of the body lice in the EO/LP solution were mori-bund or dead. All of the body lice immersed in water were alive after 60 minutes.
ConclusionIn trial 1, the authors attribute the treatment failures seen
in seven of the 40 subjects (17.5%) in the EO/LP group to the fact that lice or eggs had survived any one of the three treat-ments or that re-infestation had occurred. (For comparison, treatment failures were seen in 23 of the 36 subjects [63.9%] in the P/PB group.)
The authors conclude that “the EO/LP solution contains a proprietary combination of essential oils that has been shown to be safe and effective in eliminating head lice in Australia.” In addition, they suggest that head lice may be less likely to develop resistance to the EO/LP solution compared to the P/PB solution. “The resistance of head lice to neurotoxic treat-ments is thought to develop when there is an incomplete kill, or when low levels of therapeutic agents remain on the scalp,” the authors explain. Because the solution is both volatile and quickly effective, “it is unlikely to cause the development of head lice resistance in the community.”
— Shari Henson
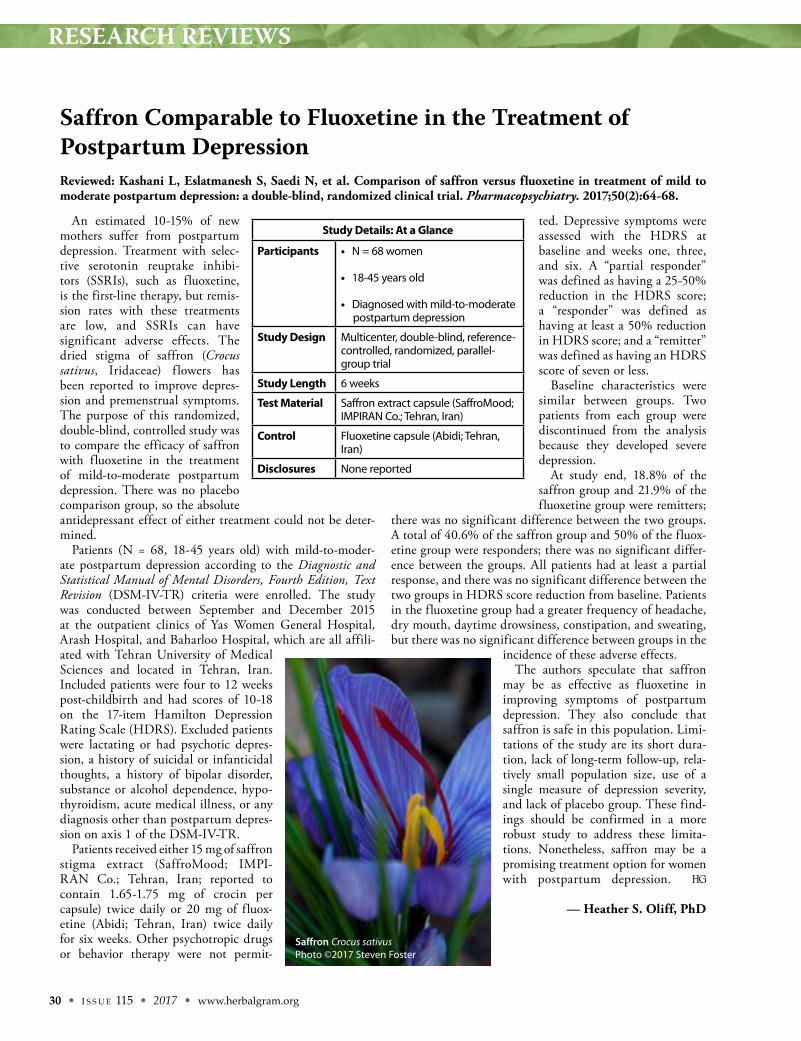
RESEARCH REVIEWS
30 • I S S U E 115 • 2017 • www.herbalgram.org
An estimated 10-15% of new mothers suffer from postpartum depression. Treatment with selec-tive serotonin reuptake inhibi-tors (SSRIs), such as fluoxetine, is the first-line therapy, but remis-sion rates with these treatments are low, and SSRIs can have significant adverse effects. The dried stigma of saffron (Crocus sativus, Iridaceae) f lowers has been reported to improve depres-sion and premenstrual symptoms. The purpose of this randomized, double-blind, controlled study was to compare the efficacy of saffron with fluoxetine in the treatment of mild-to-moderate postpartum depression. There was no placebo comparison group, so the absolute antidepressant effect of either treatment could not be deter-mined.
Patients (N = 68, 18-45 years old) with mild-to-moder-ate postpartum depression according to the Diagnostic and Statistical Manual of Mental Disorders, Fourth Edition, Text Revision (DSM-IV-TR) criteria were enrolled. The study was conducted between September and December 2015 at the outpatient clinics of Yas Women General Hospital, Arash Hospital, and Baharloo Hospital, which are all affili-ated with Tehran University of Medical Sciences and located in Tehran, Iran. Included patients were four to 12 weeks post-childbirth and had scores of 10-18 on the 17-item Hamilton Depression Rating Scale (HDRS). Excluded patients were lactating or had psychotic depres-sion, a history of suicidal or infanticidal thoughts, a history of bipolar disorder, substance or alcohol dependence, hypo-thyroidism, acute medical illness, or any diagnosis other than postpartum depres-sion on axis 1 of the DSM-IV-TR.
Patients received either 15 mg of saffron stigma extract (SaffroMood; IMPI-RAN Co.; Tehran, Iran; reported to contain 1.65-1.75 mg of crocin per capsule) twice daily or 20 mg of fluox-etine (Abidi; Tehran, Iran) twice daily for six weeks. Other psychotropic drugs or behavior therapy were not permit-
ted. Depressive symptoms were assessed with the HDRS at baseline and weeks one, three, and six. A “partial responder” was defined as having a 25-50% reduction in the HDRS score; a “responder” was defined as having at least a 50% reduction in HDRS score; and a “remitter” was defined as having an HDRS score of seven or less.
Baseline characteristics were similar between groups. Two patients from each group were discontinued from the analysis because they developed severe depression.
At study end, 18.8% of the saffron group and 21.9% of the fluoxetine group were remitters;
there was no significant difference between the two groups. A total of 40.6% of the saffron group and 50% of the fluox-etine group were responders; there was no significant differ-ence between the groups. All patients had at least a partial response, and there was no significant difference between the two groups in HDRS score reduction from baseline. Patients in the fluoxetine group had a greater frequency of headache, dry mouth, daytime drowsiness, constipation, and sweating, but there was no significant difference between groups in the
incidence of these adverse effects.The authors speculate that saffron
may be as effective as fluoxetine in improving symptoms of postpartum depression. They also conclude that saffron is safe in this population. Limi-tations of the study are its short dura-tion, lack of long-term follow-up, rela-tively small population size, use of a single measure of depression severity, and lack of placebo group. These find-ings should be confirmed in a more robust study to address these limita-tions. Nonetheless, saffron may be a promising treatment option for women with postpartum depression.
— Heather S. Oliff, PhD
Saffron Comparable to Fluoxetine in the Treatment of Postpartum Depression Reviewed: Kashani L, Eslatmanesh S, Saedi N, et al. Comparison of saffron versus fluoxetine in treatment of mild to moderate postpartum depression: a double-blind, randomized clinical trial. Pharmacopsychiatry. 2017;50(2):64-68.
Study Details: At a Glance
Participants • N = 68 women
• 18-45 years old
• Diagnosed with mild-to-moderate postpartum depression
Study Design Multicenter, double-blind, reference- controlled, randomized, parallel-group trial
Study Length 6 weeks
Test Material Saffron extract capsule (SaffroMood; IMPIRAN Co.; Tehran, Iran)
Control Fluoxetine capsule (Abidi; Tehran, Iran)
Disclosures None reported
Saffron Crocus sativusPhoto ©2017 Steven Foster
RESEARCH REVIEWS
www.herbalgram.org • 2017 • I S S U E 115 • 31
Asthma is an incurable condition caused by chronic inflammation in the lungs. The goal of treatment is to control or reduce the severity of exacerbations. Nigella (Nige-lla sativa, Ranunculaceae) seeds have anti-inflammatory, immunomodulatory, and anti-oxidant properties. Preliminary studies suggest that nigella may be beneficial for patients with asthma, but many of these stud-ies have had weak designs. The purpose of this single-blind, randomized, placebo-controlled study was to evaluate the effects of nigella on various clini-cal measures and indicators of airway inflammation and airway constriction in patients with partly controlled asthma.
Patients (N = 76, aged 18-65 years) with asthma according to the criteria of the US National Institutes of Health were recruited from the pulmonary outpatient clinic at the Univer-sity of Dammam in Saudi Arabia. Included patients had partly controlled asthma according to Global Initiative for Asthma guidelines, were nonsmokers, had been on daily maintenance therapy with inhaled corticosteroids for at least three months, and were not taking any other asthma medica-tions except for short-acting β-agonists. The study excluded patients who used additional asthma medications (e.g., leukotriene modifiers or oral steroids), had a severe exacerba-tion or hospitalization for asthma within one month prior to or during the study period, had a chronic disease, took less than 90% of the assigned study medication, or were pregnant
or lactating.Patients were randomly assigned
to receive 1 g or 2 g of ground nige-lla seeds taken as either one 500-mg capsule twice daily or two 500-mg capsules twice daily (Bio Extracts Pvt Ltd.; Colombo, Sri Lanka) or placebo (520 mg of charcoal powder; Arkopharma Laboratories; Carros, France) for 12 weeks. Patients were also required to continue with their regular maintenance inhaler therapy. Most patients were taking 400 mcg of budesonide (a conventional corti-costeroid asthma medication) once daily, and the remainder were taking 250 mcg of fluticasone propionate (a conventional drug used to treat non-allergic nasal symptoms) twice daily.
Control of asthma symptoms was assessed at six weeks and 12 weeks with the following measures: (1) the Asthma Control Test (ACT), which is used to assess daytime and nocturnal symptoms, activity limita-tions, rescue inhaler use/need, exacerbation frequency, and baseline lung function; (2) recording of moderate or severe exacerbations as defined by the American Thoracic Society and European Respiratory Society criteria; (3) spirometry to measure forced vital capacity, forced expiratory flow (FEF25-75%), and predicted values of forced expiratory volume at one second (FEV1% predicted); (4) peak expiratory flow (PEF) measured twice per day at home before medicine was taken; (5) measurement of fractional exhaled nitric oxide (FeNO); and (6) bloodwork to measure total levels of immunoglobulin E (IgE) and cytokines (interleukin [IL]-4, IL-10, IL-17, inter-feron-gamma [IFN-γ], and eotaxin).
Nigella Supplementation Improves Overall Control and Decreases Exacerbations in Patients with Partly Controlled Asthma Reviewed: Salem AM, Bamosa AO, Qutub HO, et al. Effect of Nigella sativa supplementation on lung function and inflammatory mediators in partly controlled asthma: a randomized controlled trial. Ann Saudi Med. 2017;37(1):64-67.
Study Details: At a Glance
Participants • 76 men and women
• 18-65 years old
• Diagnosed with asthma
Study Design Single-blind, randomized, placebo-controlled trial
Study Length 12 weeks
Test Material Ground nigella seed capsule (Bio Extracts Pvt Ltd; Colombo, Sri Lanka)
Control Charcoal powder capsule (Arkopharma Laboratories; Carros, France)
Disclosures None reported
QUALITY IS OUR PASSION.
Anklam Extrakt produces high quality extracts for the pharmaceutical and food industry.
As a young and ambitious company, we feel equally committed to technological progress and sustainability. Therefore we apply the latest processes and use state-of-the-art production facilities on the one hand, timeless values such as honesty, fairness, reliability and the know-how of our experienced sta� on the other.
For more information please send us an email to [email protected] visit our website:www.anklam-extrakt.com
Premium Extracts – for your project Branded Ingredients – our special extracts Custom-made Extracts – unlimited extract solutions
MADE IN GERMANY
GMP- certifi ed

RESEARCH REVIEWS
32 • I S S U E 115 • 2017 • www.herbalgram.org
At baseline, all three groups were similar in pulmonary function tests and all parameters. Treatment with placebo had no significant effect on any measured parameter. At 12 weeks, both nigella groups experienced significant increases in cytokine IFN-γ (P = .05 for both groups). There were no significant changes in any other cytokine measured. Compared with baseline, 1 g of nigella (but not the 2-g dose) significantly reduced FeNO at 12 weeks (P < .05). Compared with baseline, 2 g of nigella significantly reduced IgE at 12 weeks (P < .01). Both nigella groups had significantly higher ACT scores compared with baseline (P < .001 for both groups) and compared with placebo (P < .01 for both groups) at six weeks and 12 weeks.
For pulmonary function tests, FEV1% predicted was signif-icantly improved compared with baseline in patients treated with 2 g of nigella at six and 12 weeks (P < .05 for both time points). FEF25-75% predicted was significantly improved compared with baseline in patients treated with 2 g of nigella for six weeks (P < .01). Compared with placebo, the 1-g nigella groups had significant improvement in PEF variability at six and 12 weeks (P < .01 for both). The 2-g group experienced significant improvement in PEF variability only at 12 weeks (P < .05), compared to placebo.
Since nigella is a popular and traditionally used spice in India, the Mediterranean region, and other areas, it is not surprising that it was well-tolerated and that no adverse effects were reported.
The authors conclude that adding nigella to regular mainte-nance inhaler therapy can improve overall control and decrease exacerbations in patients with partly controlled asthma. The
authors state that this is the first study to demonstrate that nigella can significantly decrease FeNO (a marker of inflam-mation underlying the pathogenesis of asthma) in patients with asthma. However, this effect was observed only with the 1-g dose. The authors do not hypothesize why the 2-g dose did not have the same effect. The improvements in func-tion, as measured by the ACT, correspond with the decreases in FeNO seen in the 1-g group. IFN-γ is known to suppress inflammation in patients with asthma, and in this study there was a significant increase in IFN-γ with both doses of nigella. Prolonged inflammation can result in remodeling (structural changes) of lung tissue, and the authors point out that nige-lla may help reduce the severity of remodeling. The authors hypothesize that nigella may work by reducing pulmonary inflammation, which may ultimately prevent progression of bronchial remodeling. The authors were unable to receive consent for obtaining bronchoalveolar lavage or induced sputum samples to measure inflammatory cells directly.
One of the advantages of the study was the robust random-ization scheme. One limitation of this study was that it was single-blind (i.e., the patients were blinded but not the researchers) rather than double-blind, which could have intro-duced bias into the data.
—Heather S. Oliff, PhD
Editor’s note: For more information on nigella, the reader is directed to the herb profile on Nigella sativa in HerbalGram issue 114.
www.flavex.comGermany
Supercritical Extracts by
Experience the Essence of Nature
A-neu-28.11.13-3_Layout 1 05.12.13 16:01 Seite 1
RESEARCH REVIEWS
www.herbalgram.org • 2017 • I S S U E 115 • 33
Bacterial resistance to antibiotics is a growing concern, and new approaches are needed to prevent and treat bacte-rial infections. Consumption of cranberry (Vaccinium macrocarpon, Ericaceae) products that contain A-type double interflavan-bond proanthocyanidins (PAC-A) from cranberry fruit may reduce urinary tract infections by limiting the ability of bacteria to adhere to the lining of the bladder. Patients with prostate cancer who are treated with pelvic external beam radiotherapy (EBRT) have an increased risk of urinary tract infections. Previous research by the authors showed that an enteric-coated, standardized cranberry extract was effective in reducing EBRT-induced lower urinary tract infections (LUTIs) and symptoms.1 The purpose of this randomized, open-label, controlled study was to confirm those findings in a larger population and show that prophylactic use of the cranberry extract can decrease antibiotic use.
Patients (N = 924; mean age of approximately 70 years) diagnosed with prostatic adenocarcinoma and treated with radiotherapy were recruited between 2006 and 2016 at the Radiation Oncology Unit of Cremona Hospital in Cremona, Italy. Patients received radiotherapy to the prostate region and also to the pelvic area if the risk of
lymph node spread was estimated to be more than 15%. Included patients were treated with radical (2.3 grays [Gy; a measure of radiation dose] per fraction per day), postsur-gical (2.23/2.3 Gy per fraction per day), or personalized (3 Gy per fraction per day) radiotherapy five times per week. Patients were excluded if they refused daily treatment with cranberry extract, or if they had a history of pelvic EBRT, previous pelvic malignancies, a Karnofsky score (an assess-ment of the patients’ general wellbeing) of less than 80, or renal failure.
Patients received 200 mg per day of cranberry extract (MonoSelect Macrocarpon; PharmExtracta Srl; Pontenure, Piacenza, Italy [also called Ressuro; Helsinn Healthcare SA; Lugano, Switzerland]; standardized to 30% PACs according to the “European Pharmacopoeia method (version 6.0)”*)
Standardized Cranberry Extract Reduces Urinary Tract Infections, Urinary Symptoms, and Antibiotic Use during Radiotherapy for Prostate Cancer Reviewed: Bonetta A, Roviello G, Generali D, et al. Enteric-coated and highly standardized cranberry extract reduces antibiotic and nonsteroidal anti-inflammatory drug use for urinary tract infections during radiotherapy for prostate carcinoma. Res Rep Urol. 2017;9:65-69.
Study Details: At a Glance
Participants • 924 men and women
• Mean age = 70 years
• Diagnosed with prostatic adenocarcinoma and treated with radiotherapy
Study Design Randomized, open-label, controlled trial
Study Length 6-7 weeks
Test Material Standardized, enteric-coated cranberry extract tablets (MonoSelect Macrocarpon; PharmExtracta Srl; Pontenure, Piacenza, Italy)
Control No treatment
Disclosures One of the authors (Di Pierro) is on the scientific committee of a company that sells the test product. He is also the co-founder and scientific and research director of a company involved in the research and development of dietary supplements, including the test product.
”Expo East is the place to beon the forefront of emerging trends
and new items. To remain successful and competitive in the marketplace, we
must stay ahead of consumer trends and keep our customers delighted with
new items. With the ever-changing array of products showcased,
Expo East is an integral part of our merchandising plan every year.”
Thalia LawrenceEver’man Cooperative
Grocery & Cafe
Co-located with:
Education & Events September 13-16, 2017Trade Show September 14-16, 2017Baltimore Convention Center | Baltimore, MD USA
Questions? Contact us at1.866.458.4935 or 1.303.390.1776 | [email protected]
Register online at expoeast.com
Produced by:
I found my spark...
EE17_Herbalgram_QTR.indd 1 6/28/17 8:47 AM
* The European Pharmacopoeia (PhEur) method refers to a PAC assay originally developed for hawthorn (Crataegus spp., Rosaceae) berries (PhEur 6.0; 01/2008:1220). According to one expert peer reviewer of this article, this method has been known to overestimate the quantity of PACs in cranberry products.
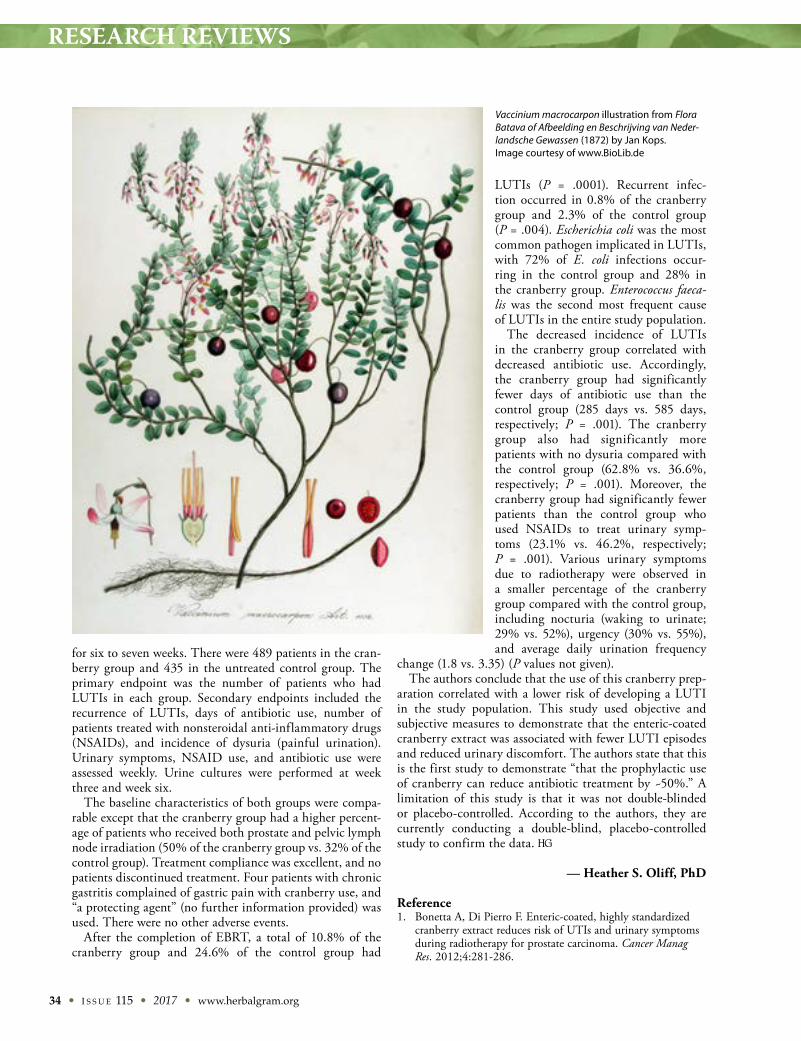
RESEARCH REVIEWS
34 • I S S U E 115 • 2017 • www.herbalgram.org
for six to seven weeks. There were 489 patients in the cran-berry group and 435 in the untreated control group. The primary endpoint was the number of patients who had LUTIs in each group. Secondary endpoints included the recurrence of LUTIs, days of antibiotic use, number of patients treated with nonsteroidal anti-inflammatory drugs (NSAIDs), and incidence of dysuria (painful urination). Urinary symptoms, NSAID use, and antibiotic use were assessed weekly. Urine cultures were performed at week three and week six.
The baseline characteristics of both groups were compa-rable except that the cranberry group had a higher percent-age of patients who received both prostate and pelvic lymph node irradiation (50% of the cranberry group vs. 32% of the control group). Treatment compliance was excellent, and no patients discontinued treatment. Four patients with chronic gastritis complained of gastric pain with cranberry use, and “a protecting agent” (no further information provided) was used. There were no other adverse events.
After the completion of EBRT, a total of 10.8% of the cranberry group and 24.6% of the control group had
LUTIs (P = .0001). Recurrent infec-tion occurred in 0.8% of the cranberry group and 2.3% of the control group (P = .004). Escherichia coli was the most common pathogen implicated in LUTIs, with 72% of E. coli infections occur-ring in the control group and 28% in the cranberry group. Enterococcus faeca-lis was the second most frequent cause of LUTIs in the entire study population.
The decreased incidence of LUTIs in the cranberry group correlated with decreased antibiotic use. Accordingly, the cranberry group had significantly fewer days of antibiotic use than the control group (285 days vs. 585 days, respectively; P = .001). The cranberry group also had significantly more patients with no dysuria compared with the control group (62.8% vs. 36.6%, respectively; P = .001). Moreover, the cranberry group had significantly fewer patients than the control group who used NSAIDs to treat urinary symp-toms (23.1% vs. 46.2%, respectively; P = .001). Various urinary symptoms due to radiotherapy were observed in a smaller percentage of the cranberry group compared with the control group, including nocturia (waking to urinate; 29% vs. 52%), urgency (30% vs. 55%), and average daily urination frequency
change (1.8 vs. 3.35) (P values not given).The authors conclude that the use of this cranberry prep-
aration correlated with a lower risk of developing a LUTI in the study population. This study used objective and subjective measures to demonstrate that the enteric-coated cranberry extract was associated with fewer LUTI episodes and reduced urinary discomfort. The authors state that this is the first study to demonstrate “that the prophylactic use of cranberry can reduce antibiotic treatment by ~50%.” A limitation of this study is that it was not double-blinded or placebo-controlled. According to the authors, they are currently conducting a double-blind, placebo-controlled study to confirm the data.
— Heather S. Oliff, PhD
Reference1. Bonetta A, Di Pierro F. Enteric-coated, highly standardized
cranberry extract reduces risk of UTIs and urinary symptoms during radiotherapy for prostate carcinoma. Cancer Manag Res. 2012;4:281-286.
Vaccinium macrocarpon illustration from Flora Batava of Afbeelding en Beschrijving van Neder-landsche Gewassen (1872) by Jan Kops. Image courtesy of www.BioLib.de
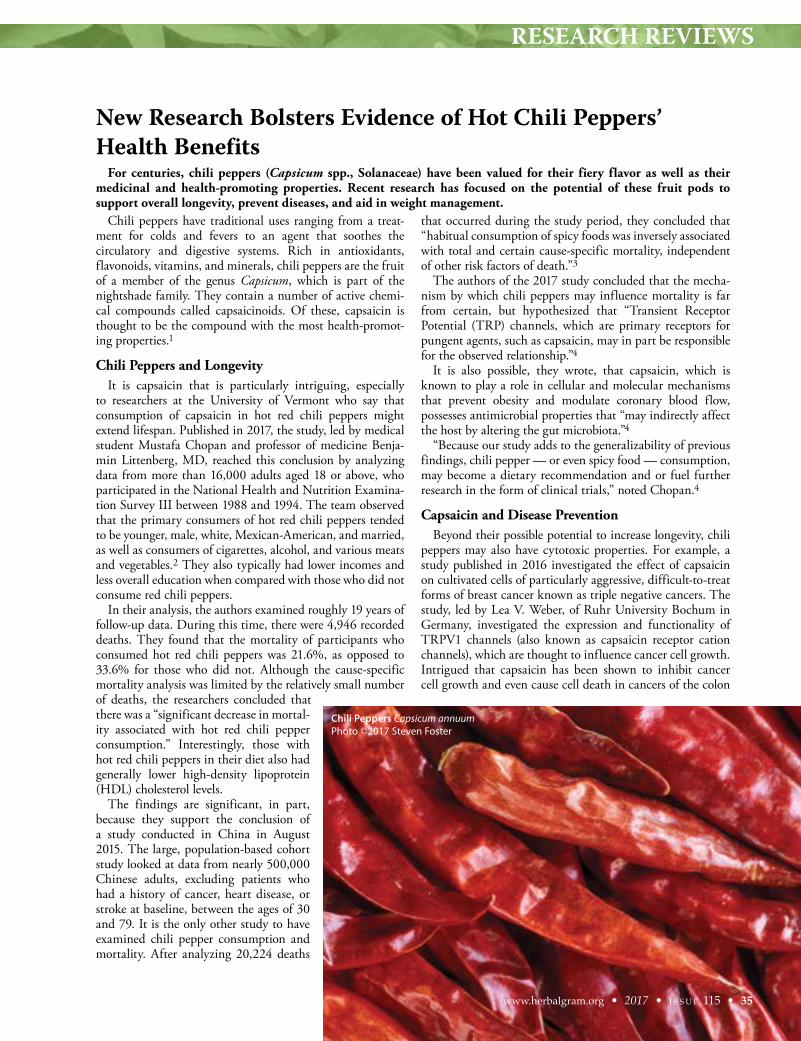
RESEARCH REVIEWS
New Research Bolsters Evidence of Hot Chili Peppers’ Health Benefits
Chili peppers have traditional uses ranging from a treat-ment for colds and fevers to an agent that soothes the circulatory and digestive systems. Rich in antioxidants, flavonoids, vitamins, and minerals, chili peppers are the fruit of a member of the genus Capsicum, which is part of the nightshade family. They contain a number of active chemi-cal compounds called capsaicinoids. Of these, capsaicin is thought to be the compound with the most health-promot-ing properties.1
Chili Peppers and LongevityIt is capsaicin that is particularly intriguing, especially
to researchers at the University of Vermont who say that consumption of capsaicin in hot red chili peppers might extend lifespan. Published in 2017, the study, led by medical student Mustafa Chopan and professor of medicine Benja-min Littenberg, MD, reached this conclusion by analyzing data from more than 16,000 adults aged 18 or above, who participated in the National Health and Nutrition Examina-tion Survey III between 1988 and 1994. The team observed that the primary consumers of hot red chili peppers tended to be younger, male, white, Mexican-American, and married, as well as consumers of cigarettes, alcohol, and various meats and vegetables.2 They also typically had lower incomes and less overall education when compared with those who did not consume red chili peppers.
In their analysis, the authors examined roughly 19 years of follow-up data. During this time, there were 4,946 recorded deaths. They found that the mortality of participants who consumed hot red chili peppers was 21.6%, as opposed to 33.6% for those who did not. Although the cause-specific mortality analysis was limited by the relatively small number of deaths, the researchers concluded that there was a “significant decrease in mortal-ity associated with hot red chili pepper consumption.” Interestingly, those with hot red chili peppers in their diet also had generally lower high-density lipoprotein (HDL) cholesterol levels.
The findings are significant, in part, because they support the conclusion of a study conducted in China in August 2015. The large, population-based cohort study looked at data from nearly 500,000 Chinese adults, excluding patients who had a history of cancer, heart disease, or stroke at baseline, between the ages of 30 and 79. It is the only other study to have examined chili pepper consumption and mortality. After analyzing 20,224 deaths
that occurred during the study period, they concluded that “habitual consumption of spicy foods was inversely associated with total and certain cause-specific mortality, independent of other risk factors of death.”3
The authors of the 2017 study concluded that the mecha-nism by which chili peppers may influence mortality is far from certain, but hypothesized that “Transient Receptor Potential (TRP) channels, which are primary receptors for pungent agents, such as capsaicin, may in part be responsible for the observed relationship.”4
It is also possible, they wrote, that capsaicin, which is known to play a role in cellular and molecular mechanisms that prevent obesity and modulate coronary blood flow, possesses antimicrobial properties that “may indirectly affect the host by altering the gut microbiota.”4
“Because our study adds to the generalizability of previous findings, chili pepper — or even spicy food — consumption, may become a dietary recommendation and or fuel further research in the form of clinical trials,” noted Chopan.4
Capsaicin and Disease PreventionBeyond their possible potential to increase longevity, chili
peppers may also have cytotoxic properties. For example, a study published in 2016 investigated the effect of capsaicin on cultivated cells of particularly aggressive, difficult-to-treat forms of breast cancer known as triple negative cancers. The study, led by Lea V. Weber, of Ruhr University Bochum in Germany, investigated the expression and functionality of TRPV1 channels (also known as capsaicin receptor cation channels), which are thought to influence cancer cell growth. Intrigued that capsaicin has been shown to inhibit cancer cell growth and even cause cell death in cancers of the colon
For centuries, chili peppers (Capsicum spp., Solanaceae) have been valued for their fiery flavor as well as their medicinal and health-promoting properties. Recent research has focused on the potential of these fruit pods to support overall longevity, prevent diseases, and aid in weight management.
www.herbalgram.org • 2017 • I S S U E 115 • 35
Chili Peppers Capsicum annuumPhoto ©2017 Steven Foster

RESEARCH REVIEWS
36 • I S S U E 115 • 2017 • www.herbalgram.org
and pancreas, the researchers set out to understand how the compound might be used in breast cancer treatments.5
They found that activation of TRPV1 by capsaicin caused significant inhibition of cancer cell growth and induced apoptosis (normal, programmed cell death) and necrosis. The authors concluded that “the current study revealed the expression of profiles of human TRP channels in 60 different breast cancer tissues and cell lines and furthermore validated the TRPV1 against SUM149PT breast cancers cells [a model system for the most aggressive breast cancer subtype], indicat-ing that activation of TRPV1 could be used as a therapeutic target, even in the most aggressive breast cancer types.”5
Weight ManagementThere is an increasing body of evidence that supports the
use of capsaicinoids as an important weight management tool, and researchers are making progress in identifying specific ingredients and innovating methods to make them more effec-tive.
For example, one study, authored by Stacie L. Urbina of the Department of Exercise and Sports Science at the University of Mary Hardin-Baylor, looked at the effects of daily supple-mentation with 2 mg of capsaicinoids on appetite reduction and body composition.6 Intrigued by the potential of capsa-icin to positively affect cardiovascular health, the researchers set out to examine the effects of different doses on healthy men and women using a commercially available capsicum extract (Capsimax; OmniActive Health Technologies; Morristown, New Jersey). The findings suggest that 12 weeks of supple-mentation may be effective at suppressing appetite and reduc-ing key body composition metrics. Results showed that waist and hip circumference decreased by 2.4% after six weeks, and there was a significant reduction in caloric intake over 12 weeks.
Another aspect of the study is that the ingredient deliv-ers effective levels of capsaicinoids without the side effects of oral and gastric burning common with raw hot red peppers. Capsimax is made using a proprietary OmniBead Beadlet Technology that encapsulates the highly active, natural capsi-cum extract in a controlled-release coating.7 In a 2017 study at Arizona State University led by Yue Deng of OmniActive Health Technologies, the product was also found to support healthy weight management by increasing healthy resting energy expenditure (the number of calories burned while at rest) by an average of 6% after a single dose.8
Synergistic PartnerThe news about chili peppers and capsaicin is not all posi-
tive. Some studies have suggested that capsaicin may have a carcinogenic effect. However, a new study led by Shengnan Geng of the Pharmacy College of Henan University in China suggests that ginger (Zingiber officinale, Zingiberaceae) and capsaicin may work synergistically, with ginger compound 6-gingerol counteracting capsaicin’s potentially harmful effects. Ginger has been shown to have health-promoting potential in its own right, but these researchers noted that capsaicin and 6-gingerol both bind to the same cellular recep-
tor — one that is related to tumor growth — and decided to investigate further.
Over a period of several weeks, the researchers fed mice either capsaicin in olive oil, 6-gingerol in olive oil, a combi-nation of the two in olive oil, or olive oil alone. Each subject received 50 mg/kg of body weight.9 They found that 100% of the mice that received capsaicin developed lung carcinomas, while only half of those that received the 6-gingerol developed the carcinomas. The development of carcinomas was even lower for mice that received both compounds at 20%.10 The study is notable for providing a new avenue to counteract the possibility of specific capsaicin-related adverse events.9
While many questions remain about the health effects of consuming hot chili peppers, emerging evidence is providing new insights on the role of capsaicin in metabolism and over-all health, and may lead to new dietary recommendations, as well as the potential development of new treatment options.
—Karen Raterman
References1. Chili Peppers Nutrition Facts. Nutrition and You website. Avail-
able at: www.nutrition-and-you.com/chili-peppers.html. Accessed April 22, 2017.
2. Chopan M, Littenberg B. The association of hot red chili pepper consumption and mortality: A large population-based cohort study. PLoS One. 2017;12(1):e0169876. Available at: www.ncbi.nlm.nih.gov/pmc/articles/PMC5222470/. Accessed April 22, 2017.
3. Lu J, Qi L, Yu C, et al. Consumption of spicy foods and total and cause specific mortality: population based cohort study. BMJ. 2015;351:h3942. Available at: www.bmj.com/content/351/bmj.h3942. Accessed April 25, 2017.
4. Study finds association between eating hot peppers and decreased mortality [press release]. Burlington, VT: University of Vermont. January 13, 2017. Available at: www.eurekalert.org/pub_releases/2017-01/uov-sfa011317.php. Accessed April 22, 2017.
5. Weber LV, Al-Refae K, Wölk G, et al. Expression and functional-ity of TRPV1 in breast cancer cells. Breast Cancer. 2016;8:243-252. Available at: www.ncbi.nlm.nih.gov/pmc/articles/PMC5167528/. Accessed August 15, 2017.
6. Urbina SL, Villa KB, Santos E, et al. Capsaicinoids supplementa-tion reduces appetite and body circumferences in healthy men and women, a placebo controlled randomized double blind study. The FASEB Journal. 2016;30(1):Supplement ib356. Avail-able at: www.fasebj.org/content/30/1_Supplement/lb356.short. Accessed August 15, 2017.
7. Award winning Capsimax Capsicum Extract provides the bene-fits of red hot peppers without the burn. OmniActive Health Technologies. Available at: http://omniactives.com/capsimax. Accessed August 15, 2017.
8. Deng Y, et al. Capsaicinoids advance metabolic rate using a novel metabolic tracker breezing device: an open-label study. Advances in Nutrition. January 2017;8(1):5. Available at: http://advances.nutrition.org/content/8/1/5.short. Accessed August 15, 2017.
9. Beer E. Mice study shows chilli and ginger cancer battling prop-erties. Nutraingredients.com. September 15, 2016. Available at: www.nutraingredients.com/Research/Mice-study-shows-chilli-ginger-cancer-battling-properties. Accessed August 15, 2017.
10. Geng S, Zheng Y, Meng M, et al. Gingerol reverses the cancer-promoting effect of capsacin by increased TRPV1 level in a urethane-induced lung carginogenic model. J Agric Food Chem. 2016;64(31):6203-6211. Available at: http://pubs.acs.org/doi/abs/10.1021/acs.jafc.6b02480.
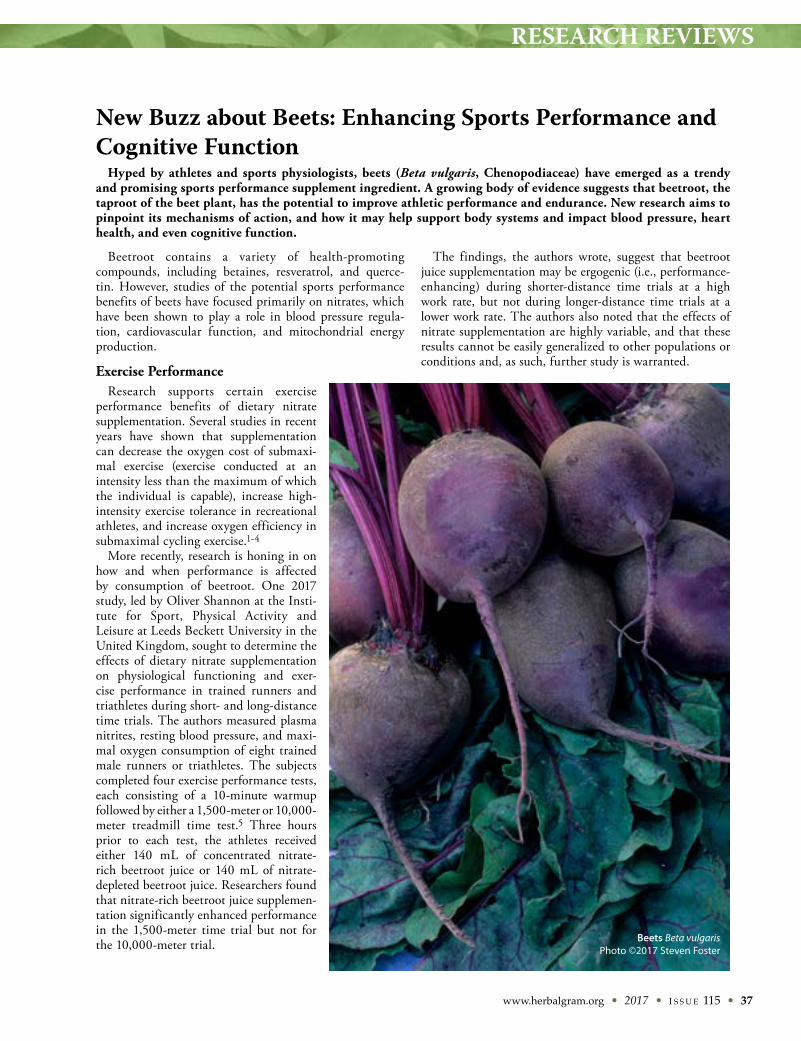
RESEARCH REVIEWS
www.herbalgram.org • 2017 • I S S U E 115 • 37
Beetroot contains a variety of health-promoting compounds, including betaines, resveratrol, and querce-tin. However, studies of the potential sports performance benefits of beets have focused primarily on nitrates, which have been shown to play a role in blood pressure regula-tion, cardiovascular function, and mitochondrial energy production.
Exercise PerformanceResearch supports certain exercise
performance benefits of dietary nitrate supplementation. Several studies in recent years have shown that supplementation can decrease the oxygen cost of submaxi-mal exercise (exercise conducted at an intensity less than the maximum of which the individual is capable), increase high-intensity exercise tolerance in recreational athletes, and increase oxygen efficiency in submaximal cycling exercise.1-4
More recently, research is honing in on how and when performance is affected by consumption of beetroot. One 2017 study, led by Oliver Shannon at the Insti-tute for Sport, Physical Activity and Leisure at Leeds Beckett University in the United Kingdom, sought to determine the effects of dietary nitrate supplementation on physiological functioning and exer-cise performance in trained runners and triathletes during short- and long-distance time trials. The authors measured plasma nitrites, resting blood pressure, and maxi-mal oxygen consumption of eight trained male runners or triathletes. The subjects completed four exercise performance tests, each consisting of a 10-minute warmup followed by either a 1,500-meter or 10,000-meter treadmill time test.5 Three hours prior to each test, the athletes received either 140 mL of concentrated nitrate-rich beetroot juice or 140 mL of nitrate-depleted beetroot juice. Researchers found that nitrate-rich beetroot juice supplemen-tation significantly enhanced performance in the 1,500-meter time trial but not for the 10,000-meter trial.
The findings, the authors wrote, suggest that beetroot juice supplementation may be ergogenic (i.e., performance-enhancing) during shorter-distance time trials at a high work rate, but not during longer-distance time trials at a lower work rate. The authors also noted that the effects of nitrate supplementation are highly variable, and that these results cannot be easily generalized to other populations or conditions and, as such, further study is warranted.
New Buzz about Beets: Enhancing Sports Performance and Cognitive Function
Hyped by athletes and sports physiologists, beets (Beta vulgaris, Chenopodiaceae) have emerged as a trendy and promising sports performance supplement ingredient. A growing body of evidence suggests that beetroot, the taproot of the beet plant, has the potential to improve athletic performance and endurance. New research aims to pinpoint its mechanisms of action, and how it may help support body systems and impact blood pressure, heart health, and even cognitive function.
Beets Beta vulgarisPhoto ©2017 Steven Foster

RESEARCH REVIEWS
38 • I S S U E 115 • 2017 • www.herbalgram.org
Previous research on beetroot has focused on endurance, but one new study from 2017 examined the impact of beet-root on high-intensity or intermittent-type exercise.6 The double-blind, placebo-controlled crossover study, led by Jean Nyakayiru of the Department of Human Movement Sciences at NUTRIM School of Nutrition and Transla-tional Research in Metabolism at Maastricht University Medical Centre in the Netherlands, investigated whether six days of nitrate-rich beetroot juice supplementation would improve exercise performance in trained soccer play-ers. Soccer players were chosen because the sport requires multiple bouts of high-intensity running and a heavy reli-ance on type II muscle fibers, which are thought to be the muscle group most impacted by nitrates.
The subjects (N = 32), of similar age, height, weight, and playing experience, ingested two 70-mL doses of beetroot juice (140 mL per day) containing 800 mg of nitrates or two 70-mL doses of a placebo beverage (with similar taste and appearance but depleted of nitrate) for six days.6 The final dose was ingested three hours prior to the exercise test. Subjects then completed two days of high-intensity inter-mittent running performance using the Yo-Yo intermittent recovery level 1 (YoYo IR1) test, which simulates soccer-specific activities in a controlled setting.
Distance covered during the test was the primary measure of performance, although heart rate was measured continu-ously, and blood and saliva samples were taken prior to the test. The authors found that nitrate-rich beetroot juice ingestion improved subject performance by 3.4 ± 1.3% compared to the placebo group. Subjects who consumed the nitrate-rich beetroot juice had higher plasma and salivary nitrate concentrations as well.
Interestingly, mean heart rates in the beetroot juice group were lower than in the placebo group during the test. This may have implications for further study on heart function. The results demonstrate that nitrate supplementation could represent an effective nutritional strategy to improve exer-cise performance in soccer players. Further study, however, is needed to see if these improvements translate to athletes at different performance levels.
Cognitive FunctionBeetroot juice also may have important benefits beyond
athletic performance that extend to healthy aging of the brain and cognitive function. A brain-imaging study published in 2016 examined whether beetroot juice might have a synergistic effect with exercise on neuroplasticity (i.e., the ability of the brain to reorganize by forming new nerve cell connections). Led by Meredith Petrie of Wake Forest University in Winston-Salem, North Carolina, the study looked at the effects of beetroot juice on the func-tional brain network of 26 older men (with a mean age of 65.4 years) who were randomly assigned to ingest beetroot juice or placebo for six weeks of exercise.7
Using measurements of peak metabolic equivalent capac-ity and resting state magnetic resonance imaging, the authors found that the community structure consistency of
the somatomotor cortex (an area of the brain that controls motor signals to the muscles) was significantly enhanced in the beetroot juice group compared to placebo.7 They also found significantly increased secondary connections between the somatomotor cortex and insular cortex in the beetroot juice group.
Based on these findings, the researchers wrote that subjects in “the exercise plus beetroot juice group had brain networks that more closely resembled those of younger adults, showing the potential enhanced neuroplas-ticity conferred by combining exercise and beetroot juice consumption.”
ConclusionThough these studies shed more light on the benefits of
beetroot juice and how dietary nitrates can improve exer-cise performance and tolerance, many questions remain. In addition to understanding more about when and how much nitrate-rich beetroot juice will have an impact, larger studies with more diverse populations are needed to better under-stand the potential exercise advantages and the broader health benefits of dietary nitrates. More safety data would also be useful to understand the effects of prolonged intake and the advantages or disadvantages of consuming dietary nitrates from beets alone, as opposed to obtaining the nitrates from other vegetable sources.
—Karen Raterman
References1. Bailey SJ, Winyard P, Vanhatalo A, et al. Dietary nitrate
supplementation reduces the O2 cost of low-intensity exercise and enhances tolerance to high-intensity exercise in humans. J Applied Physiol. 2009;107(4):1144-1155.
2. Larsen FJ, Weitzberg E, Lundberg JO, Ekblom B. Effects of dietary nitrate on oxygen cost during exercise. Acta Physiol. 2007;191(1):59-66.
3. Bailey SJ, Varnham RL, DiMenna FJ, Breese BC, Wylie LJ, Jones AM. Inorganic nitrate supplementation improves muscle oxygenation, O2 uptake kinetics, and exercise tolerance at high but not low pedal rates. J Appl Physiol 2015;118:1396-1405.
4. Cermak NM, Gibala MJ, van Loon LJC. Nitrate supplemen-tation’s improvement of 10-km time-trial performance in trained cyclists. Int J Sport Nutr Exerc Metab. 2012;22:64-71.
5. Shannon OM, Barlow MJ, Duckworth L, et al. Dietary nitrate supplementation enhances short but not longer dura-tion running time-trial performance. Eur J Appl Physiol. April 2017;117(4):775-785.
6. Nyakayiru J, Jonvik KL, Trommelen J, et al. Beetroot juice supplementation improves high-intensity intermittent type exercise performance in trained soccer players. Nutrients. March 2017;9(3):314.
7. Petrie M, Rejeski WJ, Basu S, et al. Beet root juice: An ergogenic aid for exercise and the aging brain. J Gerontol A Biol Sci Med Sci. 2016. doi: 10.1093/gerona/glw219.
CANNABIS UPDATE
www.herbalgram.org • 2017 • I S S U E 115 • 39
The Use of Medical Cannabis Preparations to Treat Epilepsy
* TRE (also sometimes called refractory or intractable epilepsy) occurs when sustained seizure remission is not achieved even after trials of at least two appropriately selected antiseizure medications that are tolerated by the patient at therapeutic dosages.2
Although more than 20 conventional antiseizure medications are available, treatment-resistant epilepsy (TRE*) reportedly affects about 30% of patients with epilepsy.1 Patients with TRE suffer from severe morbidity and have a significantly increased risk of sudden unexpected death in epilepsy (SUDEP) and other types of epilepsy-related mortality.2,3 (For those with TRE, the risk of SUDEP may exceed 10% per decade.4) Even patients with “treatment-responsive” epilepsy, when using conventional antiseizure medications, often suffer from serious, potentially life-threatening side effects and breakthrough seizures (i.e., seizures that occur despite the use of medica-tions that have otherwise prevented them) under various conditions. The potential dangers associated with these medications are even more relevant when they are used in multidrug regimens and at high doses. Controlling seizures sooner, more completely, and more safely can lead to improved outcomes.2
These factors and others have prompted some patients with epilepsy and their family members to turn to medi-cal cannabis (marijuana; Cannabis spp., Cannabaceae), in some cases as a last hope. Some of these patients have experienced dramatic relief that was not achieved with the antiseizure medica-tions they were prescribed. In addition, cannabis preparations have allowed some of these patients to reduce or even eliminate the use of other, more danger-ous interventions.2,5 (According to Ethan Russo, MD, a neurologist and highly respected medical cannabis expert, most of the conventional antiseizure medica-tions are quite sedating and contribute to psychomotor impairment.)
In the United States, the Drug Enforcement Adminis-tration (DEA) continues to classify cannabis and its constituents as Schedule I substances under the Controlled Substances Act (CSA) of 1970. The CSA defines Schedule I controlled substances, which also include heroin and lysergic acid diethylamide (LSD), as “those that have a high potential for abuse, no currently accepted medical use in treatment in the United States, and a lack of accepted safety for use under medical supervision.”
This classification means that physicians cannot legally prescribe or administer any preparations of cannabis. Even in states that have authorized the use of cannabis for medical purposes, physicians can only “certify” or “recom-mend” that a patient has a qualifying medical condition and may use cannabis for that purpose.6 Twenty-nine
www.herbalgram.org • 2017 • I S S U E 115 • 39
Cannabis spp. illustrationImage ©2017 Atypeek (iStockPhoto.com)
By Connor Yearsley

CANNABIS UPDATE
40 • I S S U E 115 • 2017 • www.herbalgram.org
states and Washington, DC, have authorized the medi-cal use of cannabis,7 and, in most of these places, seizure disorders are included among the qualifying conditions.8 Medical cannabis is often distributed to patients through dispensaries,6 but, in some places, there are few or no dispensaries, and medical cannabis is difficult or impossi-ble to obtain, even for persons with qualifying conditions. Perhaps because of this and because of success stories like that of Charlotte Figi, many families with members who have epilepsy have relocated to Colorado, where they hope to have similar success with medical cannabis.9
In 2013, CNN’s highly publicized WEED documentary told the story of Figi, a young girl with Dravet syndrome, a rare type of epilepsy that is usually caused by loss-of-function mutations in the SCN1A gene. Dravet syndrome presents in the first year of life and often begins with febrile seizures (fever-related seizures). Figi was suffering from more than 300 generalized tonic-clonic seizures† per week despite the use of antiseizure medications. Her parents, residents of Colorado, eventually began giving Figi an extract of a cannabis chemovar (chemical vari-ety) that is low in tetrahydrocannabinol (THC, the main psychoactive and intoxicating compound in cannabis) and high in cannabidiol (CBD, the most-studied biologically active, psychoactive but non-intoxicating compound in cannabis). They slowly increased the dose, and, eventually, Figi began having only two to three nocturnal general-ized tonic-clonic seizures per month. In addition, she was able to wean off other, more dangerous antiseizure medi-cations, and she showed behavioral, cognitive, and social improvements. The cannabis chemovar was renamed Charlotte’s Web after her.5,10
Figi’s case and other similar cases have received signifi-cant public attention, but many in the scientific commu-nity have remained skeptical about the safety and effi-cacy of cannabis and its constituents for the treatment of epilepsy. Widespread use of, and experimentation with, artisanal (or homemade) cannabis preparations, which are not highly standardized to specific cannabis constituents, have largely preceded rigorous scientific investigations and clinical trials that are required for US Food and Drug Administration (FDA) drug approval.8 However, encour-aging results from recent randomized, double-blind, placebo-controlled (RDBPC) clinical trials that investi-gated the effects of Epidiolex (GW Pharmaceuticals; Salis-bury, United Kingdom), a standardized oil-based CBD oral solution, may help validate the safety and efficacy of at least this specific preparation. The most recent of these trials was published in The New England Journal of Medi-cine in May 2017.12
Study in The New England Journal of MedicineDravet syndrome reportedly affects more than 5,400
people under the age of 20 in the United States. Patients with this severe, lifelong type of epilepsy often suffer from frequent seizures of multiple types.13 Although seizures associated with all types of epilepsy can be resistant to treat-ment, seizures associated with Dravet syndrome are among the most resistant.2 About 15% of patients with Dravet syndrome die within 10 years of diagnosis due to various factors, including SUDEP, status epilepticus,‡ and seizure-related accidents. There is currently no therapy approved by the FDA for the treatment of Dravet syndrome.13
This RDBPC study investigated the ability of CBD (20 mg/kg per day) to reduce seizure frequency and improve other measures in patients with Dravet syndrome who suffered from seizures that were not controlled by their standard treatment regimen. Patients were randomly assigned to take either the CBD oral solution (Epidiolex) or placebo, in conjunction with their standard antiseizure medication(s). (If approved by the FDA, Epidiolex will be the first therapy approved for the treatment of Dravet syndrome.) The CBD solution contained 100 mg of CBD per milliliter of solution. The placebo solution was identical to the CBD solution except that it did not contain CBD.12
The study consisted of a four-week baseline period, a 14-week treatment period, a 10-day taper period, and a four-week safety follow-up period. During the first two weeks of the 14-week treatment period, the dose was esca-lated up to 20 mg/kg per day or the equivalent volume (0.2 mL/kg per day) of placebo solution. During the latter 12 weeks of the 14-week treatment period, this dose was maintained.12
All interventions for epilepsy, including a ketogenic diet (a special high-fat, low-carbohydrate diet that may help control seizures in some patients with epilepsy) and vagus nerve stimulation,** were stable for four weeks before screening and were to remain unchanged through-out the study. Patients were eligible if they had been diagnosed with Dravet syndrome, were taking at least one conventional antiseizure medication, and had at least four convulsive seizures during the four-week baseline period.12
At 23 centers in the United States and Europe, 177 patients were screened and 120 were randomly assigned to receive either Epidiolex or placebo. Of the 61 patients assigned to the Epidiolex group, 52 (85%) completed the treatment period. Of the 59 patients assigned to the placebo group, 56 (95%) completed the treatment period. Of the 108 patients who completed the treatment period, 105 (97%) entered an open-label extension study.12
† Formerly called “grand mal” seizures, tonic-clonic seizures combine the characteristics of tonic (stiffening) and clonic (rhythmical jerking) seizures. A seizure is “generalized” if it starts in both sides of the brain.11
‡ Status epilepticus occurs when a seizure of any type lasts more than five minutes, or when seizures occur in succession without the patient returning to normal over the course of more than five minutes. It has been shown that the longer a seizure lasts, the less likely it is to stop without medical intervention.14
** Vagus nerve stimulation is a therapy that may help prevent seizures by using a device similar to a cardiac pacemaker to stimulate the vagus nerve, which is the longest and most complex cranial nerve and is associated with many different brain regions and functions.
OREGON GARDEN RESORT | SILVERTON, OROCTOBER 5-9, 2017
28TH ANNUAL SYMPOSIUM
HERBALISMIN ACTIONKeynote Speaker: Patrisia Gonzales
HERBALISTS GUILDAMERICAN
www.AmericanHerbalistsGuild.com

CANNABIS UPDATE
42 • I S S U E 115 • 2017 • www.herbalgram.org
The average age of participants was 9.8 years, with a range of 2.3 years to 18.4 years. Most participants (62, or 52%) were male. Patients had previously tried a median of four antisei-zure medications, with a range of zero to 26. During the study, patients were taking a median of three medications, with a range of one to five. The most common medications taken during the study were clobazam (78 participants, or 65%), valproate (all forms; 71 participants, or 59%), stiripentol (51 participants, or 42%), levetiracetam (33 participants, or 28%), and topiramate (31 participants, or 26%). Ten participants (8%) were on a ketogenic diet, and 15 (12%) were undergoing vagus nerve stimulation therapy. The two groups were similar in terms of these characteristics.12
In the Epidiolex group, convulsive-seizure frequency decreased from a median of 12.4 seizures per month (with a range of 3.9 to 1,717) at baseline to 5.9 seizures per month (with a range of zero to 2,159) during the treatment period. This represents a median change of –38.9% (with a range of –100% to 337%) from baseline. In the placebo group, the convulsive-seizure frequency decreased from a median of 14.9 seizures per month (with a range of 3.7 to 718) at baseline to 14.1 seizures per month (with a range of 0.9 to 709) during the treatment period. This represents a median change of –13.3% (with a range of –91.5% to 230%) from baseline. The adjusted median difference in convulsive-seizure frequency between the Epidiolex group and the placebo group was –22.8 percentage points (P = .01).12
During the treatment period, convulsive-seizure frequency decreased by 50% or more from baseline in 43% of patients in the Epidiolex group compared to 27% in the placebo group (P = 0.08). In addition, during the treatment period, three patients in the Epidiolex group were completely free of seizures, compared to no patients in the placebo group (P = 0.08).12
In the Epidiolex group, 37 of 60 caregivers (62%) judged their child’s overall condition to be improved, compared to 20 of 58 caregivers (34%) in the placebo group. This was measured using the Caregiver Global Impression of Change (CGIC) scale, a 7-point caregiver-rated scale that uses three categories of improvement, three categories of worsening, and an option of “no change.”12
During the treatment period, 93% of patients in the Epid-iolex group and 75% in the placebo group experienced adverse events (AEs). Among patients who experienced AEs, 84% in the Epidiolex group and 95% in the placebo group experienced AEs that were considered mild or moderate. Serious AEs were observed in 10 patients in the Epidiolex group (16%) and three in the placebo group (5%). Among those who experienced AEs, 75% in the Epidiolex group and 36% in the placebo group experienced AEs that were considered to be related to the treatment. In the Epidiolex group, the most common AEs (each observed in more than 10% of participants) were diarrhea, vomiting, fatigue, pyrexia (elevated body tempera-ture), respiratory tract infection, decreased appetite, convul-sion, lethargy, and somnolence. In the Epidiolex group, eight patients withdrew from the study because of AEs, compared to one in the placebo group.12
EpilepsyEpilepsy is a chronic neurological disorder character-
ized by recurrent seizures, which occur when neurons fire uncontrollably and cause a surge of electrical activity in the brain. There are a number of epilepsy syndromes, which can be diagnosed based on several factors, including the type(s) of seizures, the age of onset, the cause(s) of the seizures (if known), the part(s) of the brain involved, patterns on the electroencepha-logram (EEG), and others. The epilepsy syndrome will inform appropriate treatment options, so an accurate diagnosis is important. Epilepsy can be caused by genetic factors, head trauma, stroke, infections of the brain (e.g., cerebral malaria), and many other factors, but, often, the cause is not known.23 In fact, about 60% of cases are idiopathic (i.e., they arise from unknown origins).24
In addition, epilepsy is often progressive and is asso-ciated with continued loss of brain tissue and func-tion.3 For almost all patients with epilepsy, quality of life is negatively impacted by both the disorder and the treatments, and there are often devastating personal and economic consequences.2 Furthermore, many patients have cognitive, psychosocial, psychological, behavioral, and sensorimotor impairments, as well as others.3 Additionally, there is an association between epilepsy and autism spectrum disorders (ASD). ASD and epilepsy co-occur in about 30% of individuals with either ASD or epilepsy.25
When seizures occur, there can be many negative effects, including cuts, bruises, burns, head trauma (including concussion) if the patient hits his or her head, broken bones, a bitten tongue, choking, or drowning if the patient is in water.26
It is estimated that epilepsy affects about 50 million people worldwide and accounts for about 1% of the global disease burden. It is also estimated that about 10% of all people will have a seizure in their lifetime, and, of those, about 30% will develop epilepsy.24 In the United States, about 150,000 people will develop epilepsy each year. Epilepsy develops more often in children and in older adults. It is estimated that, in the United States, about 2.2 million people currently have epilepsy.27
Seizures can remit over time. In the past, it was observed that a large majority of patients who had been seizure-free for two or more years while using antiseizure medications remained seizure-free indefi-nitely after gradually tapering off the medications.28 Benign Rolandic epilepsy is an example of a syndrome that is almost always outgrown over time.
Surgery may be an option for some patients with epilepsy whose seizures cannot be controlled with medications. In some cases, surgery is now being performed on patients whose seizures have been uncontrolled for only one or two years. The types of seizures and the part(s) of the brain involved will determine whether surgery is likely to help. The most common type of surgery is called resection, in which the part of the brain that is responsible for the seizures is removed. A patient’s overall quality of life should be taken into account when considering surgery. However, surgery does not guarantee that seizures will be controlled.29,30
CANNABIS UPDATE
www.herbalgram.org • 2017 • I S S U E 115 • 43
The study authors suggest that some AEs in the Epid-iolex group may have been due to interactions with the antiseizure medications that were used. For example, the majority of patients who experienced somnolence, the most common AE during the trial, were taking clobazam.12
In addition, the study authors wrote that “the lack of a significant reduction in nonconvulsive-seizure frequency suggests that the antiseizure effect of cannabidiol may be specific to convulsive seizures in the Dravet syndrome or that the frequency of nonconvulsive seizures (e.g., brief star-ing spells) cannot be reliably counted by parents in develop-mentally delayed children. Nonconvulsive seizure frequency was a secondary end point but not part of the primary effi-cacy assessment in this trial.”12
Orrin Devinsky, MD, an epilepsy specialist at New York University’s Langone Medical Center and lead author of the study, stated that one of the advantages of choosing a disor-der like Dravet syndrome is that, unfortunately, patients have very frequent and severe seizures. “So, for a scientific study, the more frequent the seizures are, the better the
chance you can see how the intervention is working,” he said in a video about the study. “If [patients] had a seizure once a year, you might have to follow them for three or four years. In this study, seizures were frequent enough within this 14-week window that we were able to collect a lot of data.”15
One potential limitation of the study, according to the authors, was that the side effects of the Epidiolex and palat-ability differences between the Epidiolex and placebo may have caused some degree of unblinding.12
Antiseizure Effects of Cannabis and Its Constituents
The use of cannabis-derived therapies to treat epilepsy became less common after the introduction of phenobar-bital in 1912 and phenytoin in 1937, and the passage of the Marijuana Tax Act in 1937 (see “History ...” section). However, the discovery of the endocannabinoid system (ECS) in the 1990s helped renew interest in using canna-bis-derived therapies for various nervous system disorders,
www.herbalgram.org • 2017 • I S S U E 115 • 43
Cannabis spp.Image ©2017 Labuda (iStockPhoto.com)

CANNABIS UPDATE
44 • I S S U E 115 • 2017 • www.herbalgram.org
including epilepsy.1 The ECS is a biochemical signaling system that helps maintain normal cerebral and physiologi-cal functions. The effects of cannabis and its constituents are mediated primarily by the ECS.16
The ECS is composed of several receptor types, primar-ily the cannabinoid type I (CB1) receptor and the cannabi-noid type II (CB2) receptor. Because THC, CBD, and other plant cannabinoids (phytocannabinoids) are not naturally present in the body, these receptors exist for the endogenous cannabinoids (endocannabinoids), mainly anandamide and 2-arachidonoylglycerol (2-AG), which are produced natu-rally in the body. The cannabinoids are a class of compounds that have a 21-carbon terpenophenolic skeleton.1,16 THC and CBD, which are not known to be found in any other plant genus, are the most-studied cannabinoids present in cannabis.
Russo, a member of the American Botanical Coun-cil’s (ABC’s) Advisory Board, proposed that a “clinical endocannabinoid deficiency” could underlie certain condi-tions, including migraine, fibromyalgia, and irritable bowel syndrome, which exhibit common patterns, and that these conditions could effectively be alleviated with medical cannabis. He said he thinks this concept could also play a role in some cases of epilepsy, although he is not aware of a specific epilepsy syndrome in which it is a factor (oral communication, June 21, 2017). In fact, some studies have identified defects in the ECS in patients with epilepsy. For example, in one study, patients who had been newly diag-nosed with temporal lobe epilepsy had significantly lower levels of anandamide in cerebrospinal fluid than did healthy controls.1
Studies have shown that the ECS plays an important role in modulating seizure activity. In one study, THC completely eliminated spontaneous pilocarpine-induced seizures in rats. In addition, application of SR141716 (Rimonabant), a CB1 receptor inverse agonist (i.e., an agent that binds to the same site as an agonist but exerts an effect that is opposite of that agonist), significantly increased seizure duration and frequency. It was also determined that during a short-term pilocarpine-induced seizure, levels of 2-AG in the hippo-campal brain region increased significantly. Furthermore, expression of the CB1 receptor was significantly increased in the hippocampi of these rats, which had had epilepsy for almost one year. This indicates that the increase in recep-tor expression was prolonged and probably permanent. It is possible that the increases of 2-AG and CB1 expression were meant to counteract glutamate excitotoxicity. (Gluta-mate is the main excitatory neurotransmitter in the central nervous system, and it plays a role in the initiation and spread of seizure activity.) The implication of these effects is an improvement in neuroprotection.17
CBD may act as a neutral antagonist at CB1, which means it does nothing at this receptor in the absence of an agonist like THC or an inverse agonist like Rimonabant. In addi-tion, CBD is a negative allosteric modulator, meaning that it binds to a separate site on the receptor called the alloste-ric site and interferes with the activity of THC when THC
is present at the primary site (called the orthosteric site). Therefore, CBD can limit some of the undesirable effects of THC, including the psychoactive high, anxiety, and rapid heart rate.18,19
CBD exerts antiseizure effects by means other than the CB1 receptor, but these actions are not fully understood.1 According to Russo, CBD has more than 30 different phar-macological actions. “Fortunately, none of those are bad in terms of producing side effects,” he said. “What we seem to think is that CBD does not work though the sodium chan-nels. Drugs that do [work through the sodium channels] often exacerbate Dravet syndrome, for example, and that’s not the case with CBD.”
CBD’s antiseizure effects may be explained partially by the fact that it antagonizes the G-protein-coupled receptor 55 (GPR55), which reduces the excitability of nerve cells that are hyper-excitable in patients with epilepsy. Another possi-ble explanation is that CBD is an agonist at the serotonin receptor subtype 5-HT1A. This receptor also has antiseizure effects. CBD’s anti-inflammatory and antioxidant proper-ties also likely play a role.1 “I think the answer is going to be that it is not one mechanism of action,” Russo said. “It is multiple mechanisms of action…. In a multifactorial disease, it is better to have multifactorial pharmacological benefits.”
Although THC also has demonstrated antiseizure effects, some have labeled it an impractical antiseizure medication.20 Beyond the obvious concerns surrounding the psychoac-tive high produced by THC, there are also concerns that it may have irreversible effects on brain development, mainly by interfering with new synaptic connections. According to Russo, these claims stem from either animal studies that used extremely high doses, or from survey work in teenagers who were using cannabis in very high doses, chronically, on a recreational basis.
“There’s a world of difference between that kind of chronic, recreational use at a young age and much lower doses of cannabis, or THC, used therapeutically for whatever indi-cation,” Russo said. “These are not comparable at all. Addi-tionally, the danger of THC, whatever it is, and I think it’s minimal when it’s necessary medically, pales in comparison to the damage that is obviously done by these severe seizures. These severe seizure disorders can be considered a degenera-tive disease because of what they do to impair development, or even arrest it.”
Epidiolex was formulated without meaningful amounts of THC at least partially because the FDA was averse to the idea of giving the compound to children, according to Russo. (He suspects that many people at GW Pharmaceuti-cals were also hesitant about the idea, even though children under 10 years of age are quite resistant to the psychoactive effects of THC, he wrote.) Despite this reluctance, some anecdotal evidence indicates that including THC with CBD may allow for seizure control with much lower doses of CBD (e.g., 16.5 mg of CBD/kg per day maximum, compared to 25 mg of CBD/kg per day in some Epidiolex clinical trials). The potential benefit of combining CBD and THC remains to be confirmed in clinical trials.20
CANNABIS UPDATE
www.herbalgram.org • 2017 • I S S U E 115 • 45
In addition, for some patients who were using CBD as an adjunct to conventional antiseizure medications, the addition of other cannabis constituents, such as tetra-hydrocannabinolic acid (THCA) and/or alpha-linalool, resulted in improved antiseizure response.8 “What I believe is going on there is a synergy of ingredients,” Russo said. “These epilepsies are very complex disorders, and having multiple mechanisms of action seems to be an advantage.”
According to Russo, CBD seems to be more effective for addressing generalized seizures. “In contrast, canna-bidivarin (CBDV) seems to work better for seizures of partial onset, or what used to be called focal seizures [i.e., seizures that begin in one side of the brain],” he said. “So, that might indicate that you would do better with a combination of different cannabinoids, and there are some chemovars available out there that combine CBDV and CBD with a little THC, and they may turn out to be the best of all. That remains to be worked out.”
Comparing whole-plant cannabis preparations to canna-bis-derived pharmaceutical preparations, for both safety and efficacy, is important, according to Russo, but it presents chal-lenges. For example, it is diffi-cult to get approval from institu-tional review boards to conduct formal studies using what many would consider artisanal, or homemade, preparations that lack the standardization and consistency to qualify as phar-maceuticals. Furthermore, phar-maceutical companies usually do not fund these types of stud-ies. “To date, for example, there has never been a comparison of Sativex [a cannabis-derived oromucosal spray used to treat multiple sclerosis-related spasticity that is also produced by GW Pharmaceuticals] to other preparations,” Russo said. “It really becomes a problem of comparing apples to oranges, if the orange isn’t something you can vouch for, in terms of its specific, reproducible contents.”
In addition to these issues, some animal studies have raised the concern that THC, at high doses, may have proconvulsant effects. This situation may be similar to that of other antiseizure medications. For example, carba-mazepine has been known to produce tonic seizures when it is excessively present in the blood. Also, using valpro-ate and clonazepam together, although sometimes neces-sary, may precipitate clinical absence status epilepticus (an absence seizure causes a period of blanking out or star-ing).20
“When I was in [neurological medical] practice prior to 2003, I had a number of patients who used cannabis, either as their sole drug or as an adjunct to their anticon-vulsant treatment,” Russo said. “I never once, in my entire career, saw a situation in which I thought THC precipi-tated or exacerbated seizures…. I’ve never seen that in humans and it probably should not occur at conventional doses at all.”
It is noteworthy that these patients all most likely would have used cannabis that was THC-predominant, since evidence indicates that almost all cannabis chemovars in North America were devoid of meaningful amounts of CBD until relatively recently.20 According to Russo, CBD is not proconvulsant at any dose.
History of Cannabis as a Treatment for EpilepsyThere is evidence that
cannabis may have been used to treat epilepsy dating back about 4,000 years in Mesopota-mia. The British archaeologist, Assyriologist, and cuneiformist Reginald Campbell Thompson (1876-1941) dedicated much of his career to studying Assyrian medical texts from the Royal Library of Ashurbanipal, an Assyrian king who ruled from 668 to 626 BCE. This library is part of the mound of Kouyun-jik in Nineveh on the Tigris River near modern Mosul, Iraq. More than 600 broken clay cuneiform tablets excavated from the site were medical in nature. These tablets, which are now housed in the British Museum in London, compiled the knowledge of the much earlier Akkadian and Sume-rian cultures from the second millennium BCE.20
The tablets contain about 30 references to azallû in Akkadian (ancient Assyrian) and A.ZAL.LA in Sume-rian. Thompson believed these references clearly pointed to cannabis. (According to an expert peer reviewer of this article, Thompson’s hypothesis has been contested by many experts.) The plant in question was described as being psychoactive, a source of fiber, insecticidal, and deliverable orally, cutaneously, per rectum, or by fumiga-tion. In addition, it was pounded and filtered, as is done with hashish, and its seed, stem, leaf, and flower were all used. It was also described as a treatment for many indica-tions. Numerous passages in the tablets mention the plant as being a part of different complex, multi-plant mixtures that were used to treat a condition referred to as “hand of ghost.” Although Thompson never identified the condi-
Cannabis spp.Photo ©2017 Steven Foster

CANNABIS UPDATE
46 • I S S U E 115 • 2017 • www.herbalgram.org
tion referred to as “hand of ghost,” later translations of Neo-Assyrian tablets from 718 to 612 BCE indicated this may have referred to nocturnal epilepsy.20
A passage from the Arabic work Solace of the spirit in hash-ish and wine by 15th-century Damascene authority Taqi al-Din al-Badri retells an earlier account that he attributed to the eminent Persian physician Rhazes (865-925) in which cannabis was used to treat epilepsy. Rhazes supposedly described how the son of the registry chamberlain of Bagh-dad under the Abbasid powers, who suffered a seizure attack every week, was apparently cured with hashish (used regu-larly) and music. This story is open to question, however, because of the loss of key manuscripts and because of a liter-ary tradition in which embellishment was sometimes the sincerest form of flattery.20
In another account from the Arabic literature, Ali ibn al-Abbas al-Mayusi, who died circa 982-994, prescribed cannabis to treat epilepsy. The text reads: “the juice of the leaves of cannabis instilled in the nostril serves to treat epilepsy.” This administration route may have been an advantage with acute attacks in which oral administration may have been impractical or dangerous. In this case, it is also likely that THCA would have been the active constitu-ent.20 (An expert peer reviewer of this article noted that the Latin version of the text refers to “semen canapis” [hemp seed], rather than hemp leaves.)
In 1557, Italian physician and naturalist Pietro Mattioli mentioned the use of a cannabis seed decoction to treat epilepsy. He wrote: “For whose doctrine I never consider those silly women, who give a decoction of cannabis seed to children, who are epileptic, because of the harm added.” It is possible that hemp chemovars with cannabidiolic acid (CBDA), if unheated, or with CBD, but not THC, had little benefit.20
Irish physician William O’Shaughnessy, who was in service to the British Crown in India, studied the indig-enous uses of cannabis by Ayurveda medicine practitioners. He then experimented on animals and then his patients and, in 1840, reported that he successfully used a cannabis tincture to treat a 40-day-old girl with convulsions. After 20 days, he noted: “The child is now … in the enjoyment of robust health, and has regained her natural plump and happy appearance.” In 1842, O’Shaughnessy lectured in Britain on his successes with Indian hemp, and others later had similar success.20
In 1856, in North America, R.R. McMeens reported that he successfully used a tincture of Cannabis indica to treat four children, including a 7-week-old infant who was expe-riencing multiple seizures per day for more than two weeks. McMeens wrote: “from the time of its adoption, the patient never experienced another symptom of convulsion.”20
In 1868, Sir John Russell Reynolds, personal physician to Queen Victoria and one of the greatest 19th-century author-ities on medical cannabis, reported on the use of cannabis to treat three patients (two adults and one child) with epilepsy, with varying benefits.20 Later, in an 1890 publication, he wrote, “In true, chronic epilepsy I have found [hemp] abso-
lutely useless.” However, in the same publication, he also wrote, “Indian hemp is the most useful agent with which I am acquainted” for treating convulsions that he apparently thought were not associated with epilepsy,21 which indicates nosological confusion (i.e., confusion about how to classify a disease).20
Well into the 20th century, cannabis remained included in Western pharmacopeias, including the US Pharmacopeia (from which it was removed in 1942), but various factors, including a lack of standardization, bioavailability issues, and, ultimately, criminalization, prevented this ancient, multipurpose plant from becoming (or remaining) a main-stream antiseizure treatment.2
Conclusion The antiseizure effects of cannabis and some of its
constituents are by no means new discoveries, but the legal and political landscape has stifled research on the safety and efficacy of cannabis-derived therapies for all indications, including epilepsy. In 1979, Karler et al. wrote: “Because of the therapeutic failures and because of the toxicity asso-ciated with the currently used antiepileptics, the search for relatively non-toxic drugs with different mechanisms of action is an obvious goal in epilepsy research. Both the lack of toxicity and the anticonvulsant properties of CBD combine to enhance its therapeutic potential as an antiepi-leptic.”20
After this observation, however, little progress was made for decades. “There were sporadic studies but [CBD] wasn’t examined systematically until more than 30 years later,” Russo said. “So, that’s a shame.”
The use of cannabis-derived therapies, even non-intoxicat-ing preparations, will likely remain controversial. However, the recent Epidiolex clinical trials, which observed success both in patients with Dravet syndrome12 and Lennox-Gastaut syndrome (a type of epilepsy with difficult-to-control seizures of multiple types),22 may help convince some that these therapies deserve more consideration. “It is important to remember that these kids have been on multi-ple drugs without control,” Russo said. “So, everything that we have seen in terms of improvement is over and above the best that conventional medicine could provide to them.”
“It is clear that [cannabis] can be made into a medicine that meets all standards, including FDA standards as a pharmaceutical, and we need to get on with it and offer people better alternatives,” Russo added.
References1. Friedman D, Devinsky O. Cannabinoids in the treatment of Epilepsy.
N Engl J Med. 2015;373:1048-58. doi: 10.1056/NEJMra1407304.2. O’Connell BK, Gloss D, Devinsky O. Cannabinoids in treatment-
resistant epilepsy: A review. Epilepsy and Behavior. 2017;70:341-348. doi: 10.1016/j.yebeh.2016.11.012.
3. Rosenberg EC, Tsien RW, Whalley BJ, Devinsky O. Cannabinoids and epilepsy. Neurotherapeutics. 2015;12(4):747-768. doi: 10.1007/s13311-015-0375-5.
4. Kroner BL, Wright C, Friedman D, et al. Characteristics of epilepsy patients and caregivers who either have or have not heard of SUDEP. Epilepsia. 2014;55(10):1486-1494.
CANNABIS UPDATE
www.herbalgram.org • 2017 • I S S U E 115 • 47
5. Dr Sanjay Gupta: Weed -— CNN Special Documentary. YouTube website. Available at: www.youtube.com/watch?v=-SZzgfyXhJI. Accessed June 29, 2017.
6. Mead A. The legal status of cannabis (marijuana) and cannabidiol (CBD) under U.S. law. Epilepsy and Behavior. 2017;70:288-291. doi: 10.1016/j.yebeh.2016.11.021.
7. 29 Legal Medical Marijuana States and DC. ProCon website. Available at: http://medicalmarijuana.procon.org/view.resource.php?resourceID=000881. Accessed June 29, 2017.
8. Sulak D, Saneto R, Goldstein B. The current status of artisanal cannabis for the treatment of epilepsy in the United States. Epilepsy and Behavior. 2017;70:328-333. doi: 10.1016/j.yebeh.2016.12.032.
9. Detyniecki K, Hirsch L. Marijuana use in epilepsy: The myth and the reality. Curr Neurol Neurosci Rep. 2015;15(10):65. doi: 10.1007/s11910-015-0586-5.
10. Maa E, Figi P. The case for medical marijuana in epilepsy. Epilepsia. 2014;55(6):783-786. doi: 10.1111/epi.12610.
11. Tonic-clonic seizures. Epilepsy Foundation website. Available at: www.epilepsy.com/learn/types-seizures/tonic-clonic-seizures. Accessed July 12, 2017.
12. Devinsky O, Cross H, Laux L, et al. Trial of cannabidiol for drug-resistant seizures in the Dravet syndrome. N Engl J Med. 2017;376:2011-20. doi: 10.1056/NEJMoa1611618.
13. Dravet Syndrome. Greenwich Biosciences website. Available at: greenwich-biosciences.com. Accessed August 14, 2017.
14. Status Epilepticus. Epilepsy Foundation website. Available at: www.epilepsy.com/learn/impact/seizure-emergencies/status-epilepticus. Accessed July 12, 2017.
15. Medical marijuana aids some children with epilepsy, says study. YouTube website. Available at: www.youtube.com/watch?v=x97FZD_ObOo. Accessed July 10, 2017.
16. Marcu J. The biochemical system controlling the effects of cannabis — an introduction. HerbalGram. 2015;107:36-39.
17. Wallace MJ, Blair RE, Falenski KW, Martin BR, DeLorenzo RJ. The endog-enous cannabinoid system regulates seizure frequency and duration in a model of temporal lobe epilepsy. Journal of Pharmacology and Experimental Therapeutics. 2003;307(1):129-137. doi: 10.1124/jpet.103.051920.
18. Russo EB. Cannabidiol claims and misconceptions. Trends in Pharmacologi-cal Science. 2017;38(3):198-201. doi: 10.1016/j.tips.2016.12.004.
19. Dr. Ethan Russo: CBD and Clinical Endocannabinoid Deficiency. Project CBD website. Available at: www.projectcbd.org/science/cannabis-pharmacol-ogy/dr-ethan-russo-cbd-clinical-endocannabinoid-deficiency. Accessed July 18, 2017.
20. Russo EB. Cannabis and epilepsy: An ancient treatment returns to the fore. Epilepsy and Behavior. 2017;70:292-297. doi: 10.1016/j.yebeh.2016.09.040.
21. Reynolds JR. Therapeutical uses and toxic effects of Cannabis indica. The Lancet. 1890;1:637-638.
22. Thiele E, Mazurkiewicz-Beldzinska M, Benbadis S, et al. Cannabidiol (CBD) Significantly Reduces Drop Seizure Frequency in Lennox-Gastaut Syndrome: Results of a Multi-Center, Randomized, Double-blind, Placebo-controlled Trial. Available at: www.aesnet.org/meetings_events/annual_meet-ing_abstracts/view/2422092. Accessed July 20, 2017.
23. Types of Epilepsy Syndromes. Epilepsy Foundation website. Available at: www.epilepsy.com/learn/types-epilepsy-syndromes. Accessed July 12, 2017.
24. Whalley B. Cannabis and epilepsy: from recreational abuse to therapeutic use. Medicinal Genomics website. Available at: www.medicinalgenomics.com/wp-content/uploads/2013/11/Cannabis_Epilepsy_ben-whalley.pdf. Accessed July 12, 2017.
25. Tuchman R, Cuccaro M, Alessandri M. Autism and epilepsy: historical perspective. Brain and Development. 2010;32(9):709-18. doi: 10.1016/j.braindev.2010.04.008.
26. Injuries and Illnesses. Epilepsy Foundation website. Available at: www.epilepsy.com/learn/impact/injuries-and-illnesses. Accessed July 12, 2017.
27. Epilepsy Statistics. Epilepsy Foundation website. Available at: www.epilepsy.com/learn/epilepsy-statistics. Accessed July 12, 2017.
28. Brody JE. Personal Health; Childhood epilepsy is no longer a life sentence. The New York Times. October 19, 1994. Available at: www.nytimes.com/1994/10/19/us/personal-health-childhood-epilepsy-is-no-longer-a-life-sentence.html. Accessed July 19, 2017.
29. Surgery. Epilepsy Foundation website. Available at: www.epilepsy.com/learn/treating-seizures-and-epilepsy/surgery. Accessed July 19, 2017.
30. Types of Surgeries. Epilepsy Foundation website. Available at: www.epilepsy.com/learn/treating-seizures-and-epilepsy/surgery/types-surgeries. Accessed July 19, 2017.
www.herbalgram.org • 2017 • I S S U E 115 • 47
Cannabis spp.Photo ©2017 Steven Foster

Following the failure of her marriage in the summer of 1685, Merian joined her half-brother, Caspar, at a Labadist (named for Jean de Labadie, a Jesuit priest who had converted to Protestantism) community in West Friesland in the Netherlands. Converts to the Protestant sect were expected to abandon their normal lives to seek self-sufficiency and reach Christian regeneration. Meri-an’s mother and two daughters accompanied her and they lived there for six years. When missionaries returned from a Labadist plantation in the Dutch colony of Suriname on the northeast coast of South America with exotic flora and fauna specimens, Merian was especially captivated by the insects.
In 1691, Merian and her daughters moved to Amster-dam and made a living by giving painting lessons and selling watercolors. She also began to make connections with influential members of the Dutch natural history community as they commissioned her to paint the speci-mens in their collections. Her continued exposure to the insects of far-away places caused her interest to increase even more. In June of 1699, Merian and her youngest daughter, Dorothea, embarked on a two-year expedition to Suriname to observe and document the life cycles of these creatures in their natural habitat. However, they were forced to return to the Netherlands in the summer of 1701 when Merian contracted malaria.
Back in Amsterdam, Merian’s life’s work began in earnest when she had her Suriname paintings engraved and printed to form a book that was sold by subscrip-tion because of the immense cost to produce it. The first edition of Metamorphosis Insectorum Surinamensium (Transformation of the Surinamese Insects) was completed in 1705 and contained 60 plates, which were hand-colored by Merian and her daughters. Merian’s descrip-tions of the insects and plants in each image were written in both Dutch and Latin. According to the Maria Sibylla Merian Society, approximately 70 have survived. Four editions of Metamorphosis were produced posthumously (in 1719, 1726, 1730, and 1771) and included 12 addi-tional illustrations by Merian that feature reptiles and marsupials.
Maria Sibylla Merian produced important, ground-breaking work at a time when women were almost completely left out of both art and science. Over the centu-ries her contributions have largely been forgotten. This year, the 300th anniversary of her death, is a good time to reintroduce the world to the woman who produced a masterful collection that depicted the insect-plant relation-ship in such a beautiful way.
Notes about IllustrationsThe captions include the following information: (1) the
Dutch or Latin name used by Merian, (2) the current Latin binomial and standardized common name1 of the depicted plant, and (3) English translations of descriptions from the 2016 facsimile of the 1705 edition of Metamorphosis Insec-torum Surinamensium, with corresponding plate numbers.2 Merian, whose interest in plants was primarily related to their connection to insects, did not focus on the medici-nal properties of the plant species in her illustrations. In addition, her descriptions and depictions of the plants and insects (and the relationships between them) were based on her knowledge at the time, and therefore may not be fully accurate. The illustrations are in watercolor. (As a woman, Merian could not join a painters’ guild in Europe and therefore did not have access to oil paints.)
References1. McGuffin M, Kartesz JT, Leung AY, Tucker AO. American Herbal
Products Association’s Herbs of Commerce. 2nd ed. Silver Springs, MD: American Herbal Products Association; 2000.
2. van Delft M, Mulder H, eds. Metamorphosis Insectorum Surinamen-sium (1705). Tielt, Belgium: Lannoo Publishers and The Hague, Netherlands: Koninklijke Bibliotheek (National Library of the Neth-erlands); 2016.
By Betsy KruthofferCataloger and Rare Book Librarian, Lloyd Library and Museum
All artwork courtesy of Lloyd Library and Museum
The Illustrious Life ofMaria Sibylla MerianMaria Sibylla Merian (1647-1717) was born in Frankfurt, Germany, to a family of painters, engravers,
and printers. In the late 17th century, the art world belonged to men, but she learned to paint flow-ers with the encouragement of her stepfather, flower and still-life painter Jacob Marrel, alongside
his male pupils and apprentices. As a child, Merian developed a fascination with the life cycles of insects, and by 1679 she had combined her talents and interests in her first insect book, Der Raupen Wunderbare Verwandelung und Sonderbare Blumen-Nahrung (The Caterpillar’s Wondrous Metamorphosis and Extraordinary Nourishment from Flowers). This revolutionary volume of 50 illustrations was the first to show the stages of metamorphosis as it occurred on an insect’s food plant — an ecological depiction centuries before the science of ecology was defined.
Plate 8
Indiaansche Jasmynboom / Indian jasmine Plumeria rubra (Apocynaceae) / Frangipani
“They easily let themselves be multiplied. If one merely breaks off a twig and puts it in the ground before the milk [sap] runs off it, it will grow into a tall tree within a few months.”
48 • I S S U E 115 • 2017 • www.herbalgram.org
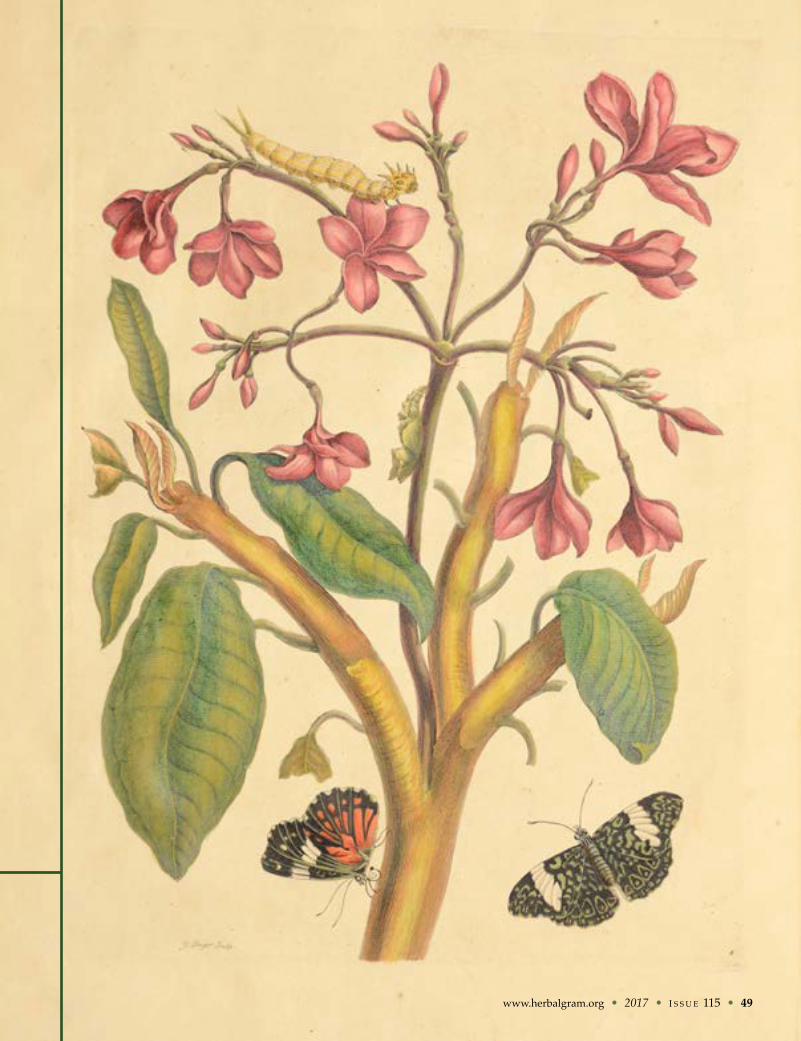
www.herbalgram.org • 2017 • I S S U E 115 • 49
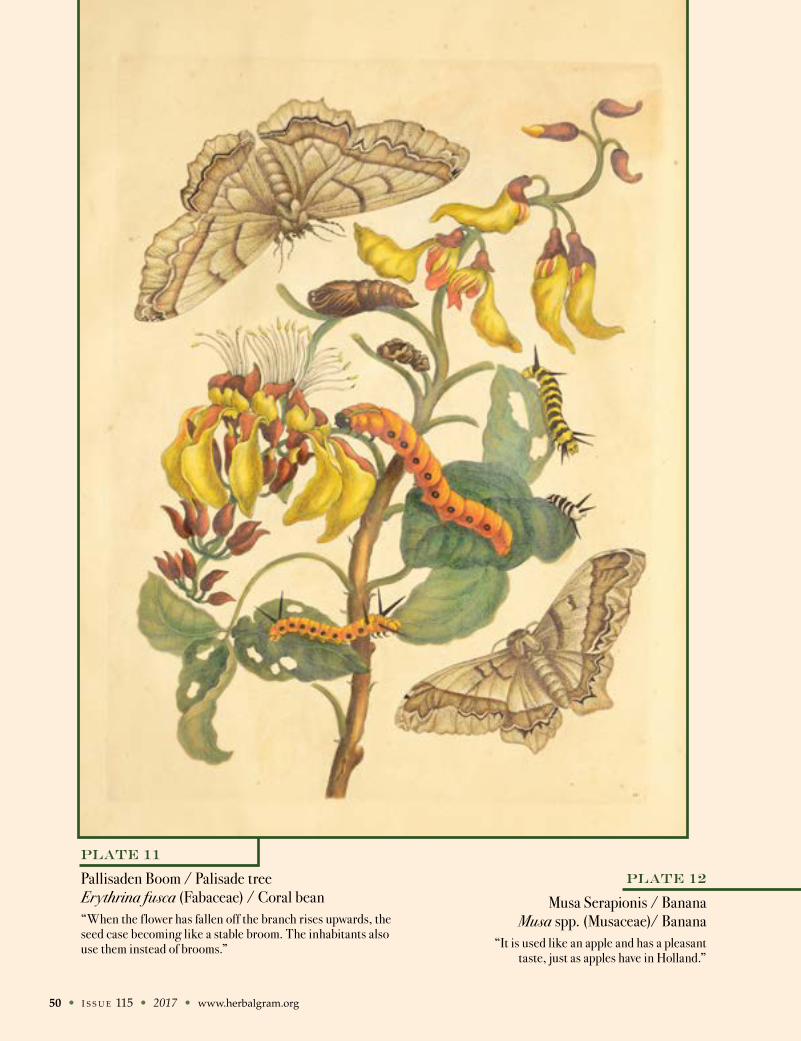
50 • I S S U E 115 • 2017 • www.herbalgram.org
Plate 11
Pallisaden Boom / Palisade tree Erythrina fusca (Fabaceae) / Coral bean“When the f lower has fallen off the branch rises upwards, the seed case becoming like a stable broom. The inhabitants also use them instead of brooms.”
Plate 12
Musa Serapionis / BananaMusa spp. (Musaceae)/ Banana
“It is used like an apple and has a pleasant taste, just as apples have in Holland.”
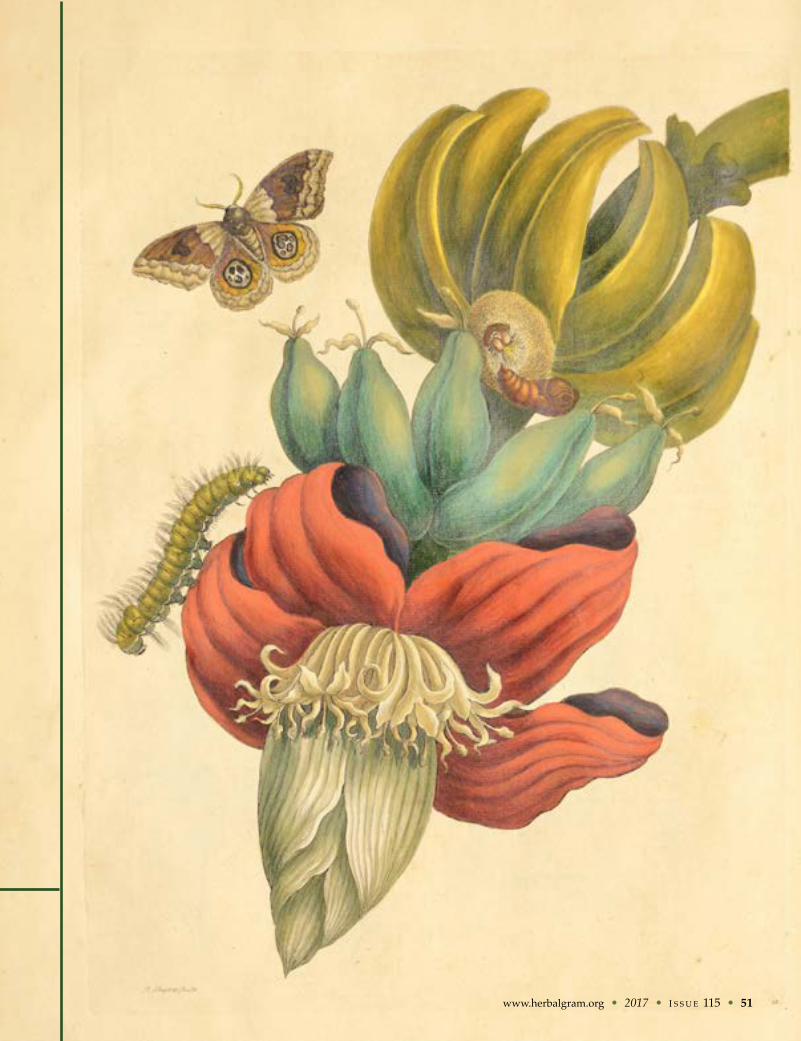
www.herbalgram.org • 2017 • I S S U E 115 • 51
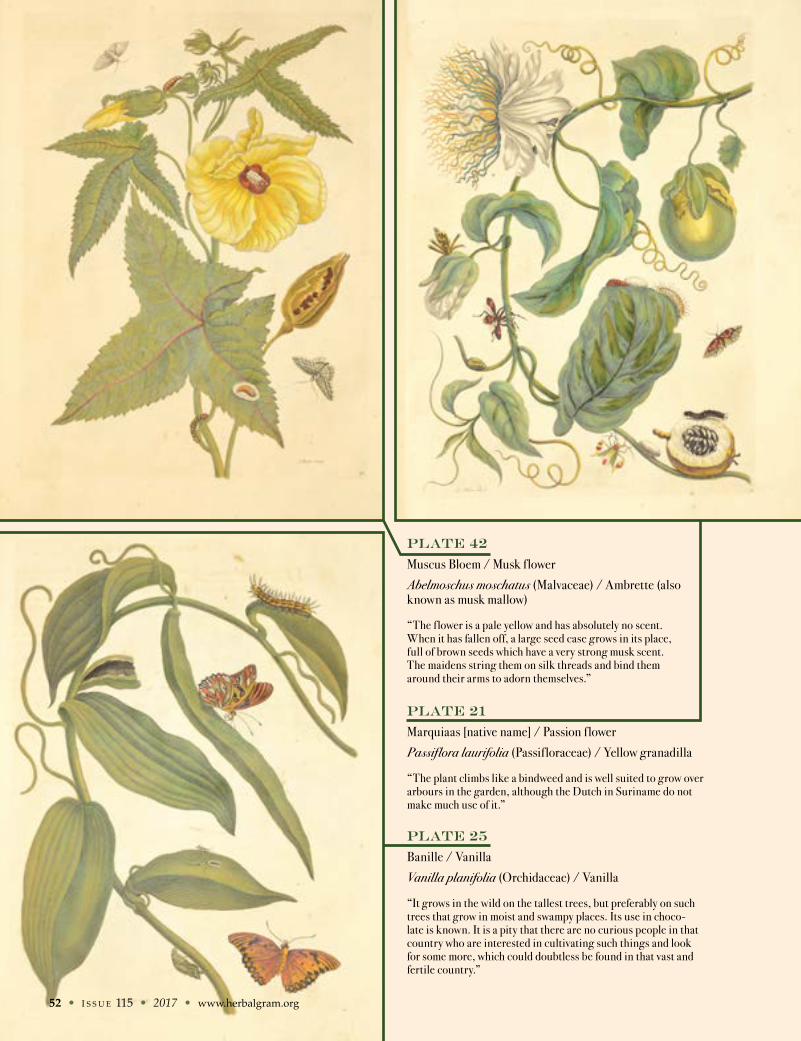
Plate 21
Marquiaas [native name] / Passion f lower
Passiflora laurifolia (Passif loraceae) / Yellow granadilla
“The plant climbs like a bindweed and is well suited to grow over arbours in the garden, although the Dutch in Suriname do not make much use of it.”
Plate 25
Banille / Vanilla
Vanilla planifolia (Orchidaceae) / Vanilla
“It grows in the wild on the tallest trees, but preferably on such trees that grow in moist and swampy places. Its use in choco-late is known. It is a pity that there are no curious people in that country who are interested in cultivating such things and look for some more, which could doubtless be found in that vast and fertile country.”
Plate 42
Muscus Bloem / Musk f lower
Abelmoschus moschatus (Malvaceae) / Ambrette (also known as musk mallow)
“The f lower is a pale yellow and has absolutely no scent. When it has fallen off, a large seed case grows in its place, full of brown seeds which have a very strong musk scent. The maidens string them on silk threads and bind them around their arms to adorn themselves.”
52 • I S S U E 115 • 2017 • www.herbalgram.org

Plate 55
Indiaanse Peper / Indian pepper or Piement / PimientoCapsicum annuum (Solanaceae) / Cayenne (also known as red pepper)
“The fruit is hot and pungent. The Indians spread it on their bread when they eat. The Dutch cut it up small and eat it with meat and fish. They also use it in sauces and vinegar, etc.”
www.herbalgram.org • 2017 • I S S U E 115 • 53
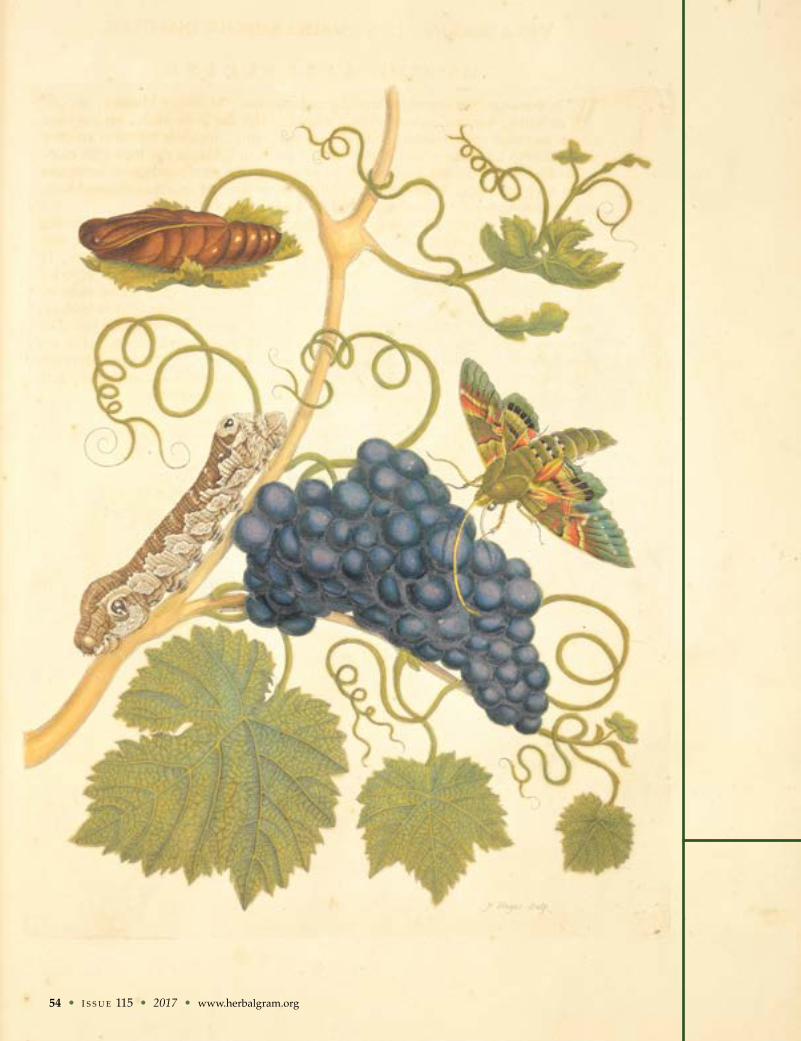
54 • I S S U E 115 • 2017 • www.herbalgram.org
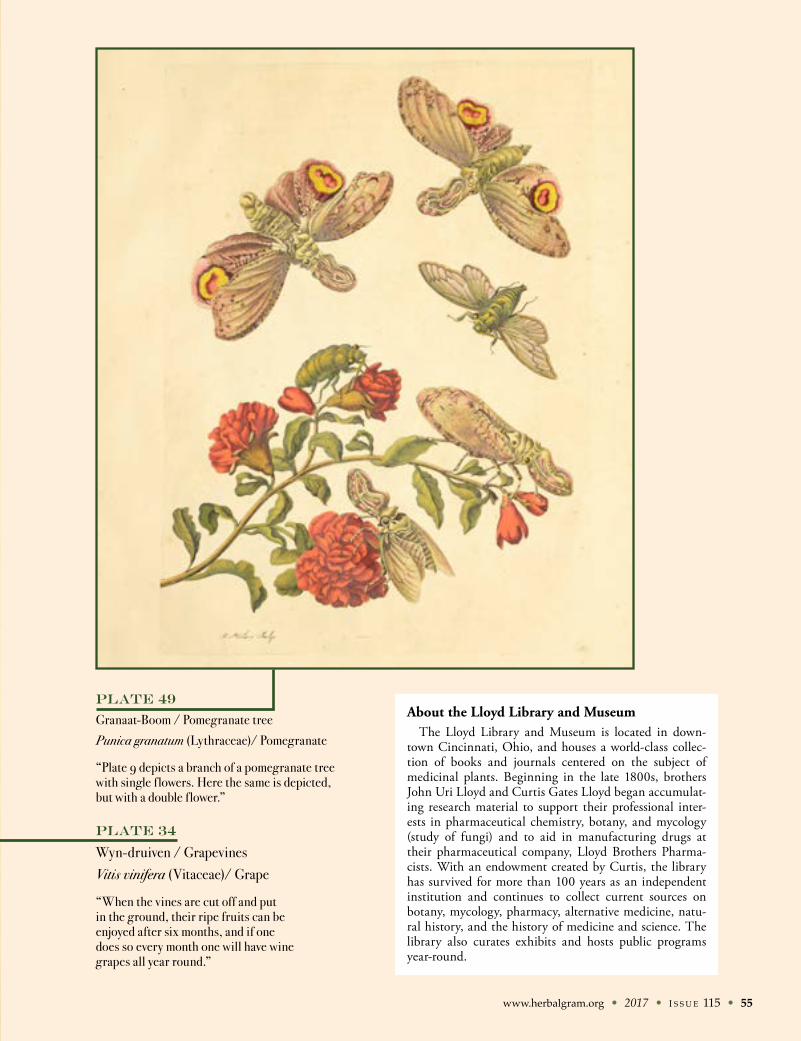
www.herbalgram.org • 2017 • I S S U E 115 • 55
Plate 49
Granaat-Boom / Pomegranate tree
Punica granatum (Lythraceae)/ Pomegranate
“Plate 9 depicts a branch of a pomegranate tree with single f lowers. Here the same is depicted, but with a double f lower.”
Plate 34
Wyn-druiven / GrapevinesVitis vinifera (Vitaceae)/ Grape
“When the vines are cut off and put in the ground, their ripe fruits can be enjoyed after six months, and if one does so every month one will have wine grapes all year round.”
About the Lloyd Library and MuseumThe Lloyd Library and Museum is located in down-
town Cincinnati, Ohio, and houses a world-class collec-tion of books and journals centered on the subject of medicinal plants. Beginning in the late 1800s, brothers John Uri Lloyd and Curtis Gates Lloyd began accumulat-ing research material to support their professional inter-ests in pharmaceutical chemistry, botany, and mycology (study of fungi) and to aid in manufacturing drugs at their pharmaceutical company, Lloyd Brothers Pharma-cists. With an endowment created by Curtis, the library has survived for more than 100 years as an independent institution and continues to collect current sources on botany, mycology, pharmacy, alternative medicine, natu-ral history, and the history of medicine and science. The library also curates exhibits and hosts public programs year-round.
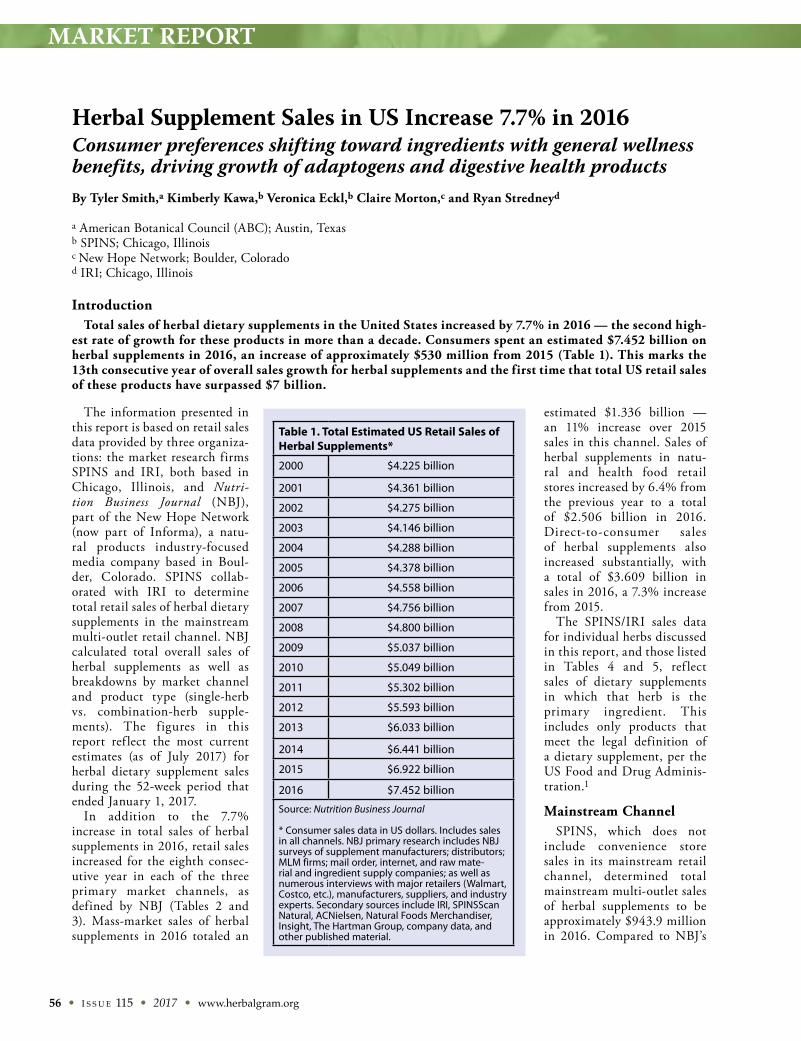
MARKET REPORT
56 • I S S U E 115 • 2017 • www.herbalgram.org
The information presented in this report is based on retail sales data provided by three organiza-tions: the market research firms SPINS and IRI, both based in Chicago, Illinois, and Nutri-tion Business Journal (NBJ), part of the New Hope Network (now part of Informa), a natu-ral products industry-focused media company based in Boul-der, Colorado. SPINS collab-orated with IRI to determine total retail sales of herbal dietary supplements in the mainstream multi-outlet retail channel. NBJ calculated total overall sales of herbal supplements as well as breakdowns by market channel and product type (single-herb vs. combination-herb supple-ments). The figures in this report ref lect the most current estimates (as of July 2017) for herbal dietary supplement sales during the 52-week period that ended January 1, 2017.
In addition to the 7.7% increase in total sales of herbal supplements in 2016, retail sales increased for the eighth consec-utive year in each of the three primary market channels, as defined by NBJ (Tables 2 and 3). Mass-market sales of herbal supplements in 2016 totaled an
estimated $1.336 billion — an 11% increase over 2015 sales in this channel. Sales of herbal supplements in natu-ral and health food retail stores increased by 6.4% from the previous year to a total of $2.506 billion in 2016. Direct-to-consumer sales of herbal supplements also increased substantially, with a total of $3.609 billion in sales in 2016, a 7.3% increase from 2015.
The SPINS/IRI sales data for individual herbs discussed in this report, and those listed in Tables 4 and 5, ref lect sales of dietary supplements in which that herb is the primary ingredient. This includes only products that meet the legal definition of a dietary supplement, per the US Food and Drug Adminis-tration.1
Mainstream ChannelSPINS, which does not
include convenience store sales in its mainstream retail channel, determined total mainstream multi-outlet sales of herbal supplements to be approximately $943.9 million in 2016. Compared to NBJ’s
IntroductionTotal sales of herbal dietary supplements in the United States increased by 7.7% in 2016 — the second high-
est rate of growth for these products in more than a decade. Consumers spent an estimated $7.452 billion on herbal supplements in 2016, an increase of approximately $530 million from 2015 (Table 1). This marks the 13th consecutive year of overall sales growth for herbal supplements and the first time that total US retail sales of these products have surpassed $7 billion.
By Tyler Smith,a Kimberly Kawa,b Veronica Eckl,b Claire Morton,c and Ryan Stredneyd
a American Botanical Council (ABC); Austin, Texasb SPINS; Chicago, Illinoisc New Hope Network; Boulder, Coloradod IRI; Chicago, Illinois
Herbal Supplement Sales in US Increase 7.7% in 2016Consumer preferences shifting toward ingredients with general wellness benefits, driving growth of adaptogens and digestive health products
Table 1. Total Estimated US Retail Sales of Herbal Supplements*
2000 $4.225 billion
2001 $4.361 billion
2002 $4.275 billion
2003 $4.146 billion
2004 $4.288 billion
2005 $4.378 billion
2006 $4.558 billion
2007 $4.756 billion
2008 $4.800 billion
2009 $5.037 billion
2010 $5.049 billion
2011 $5.302 billion
2012 $5.593 billion
2013 $6.033 billion
2014 $6.441 billion
2015 $6.922 billion
2016 $7.452 billion
Source: Nutrition Business Journal * Consumer sales data in US dollars. Includes sales in all channels. NBJ primary research includes NBJ surveys of supplement manufacturers; distributors; MLM firms; mail order, internet, and raw mate-rial and ingredient supply companies; as well as numerous interviews with major retailers (Walmart, Costco, etc.), manufacturers, suppliers, and industry experts. Secondary sources include IRI, SPINSScan Natural, ACNielsen, Natural Foods Merchandiser, Insight, The Hartman Group, company data, and other published material.
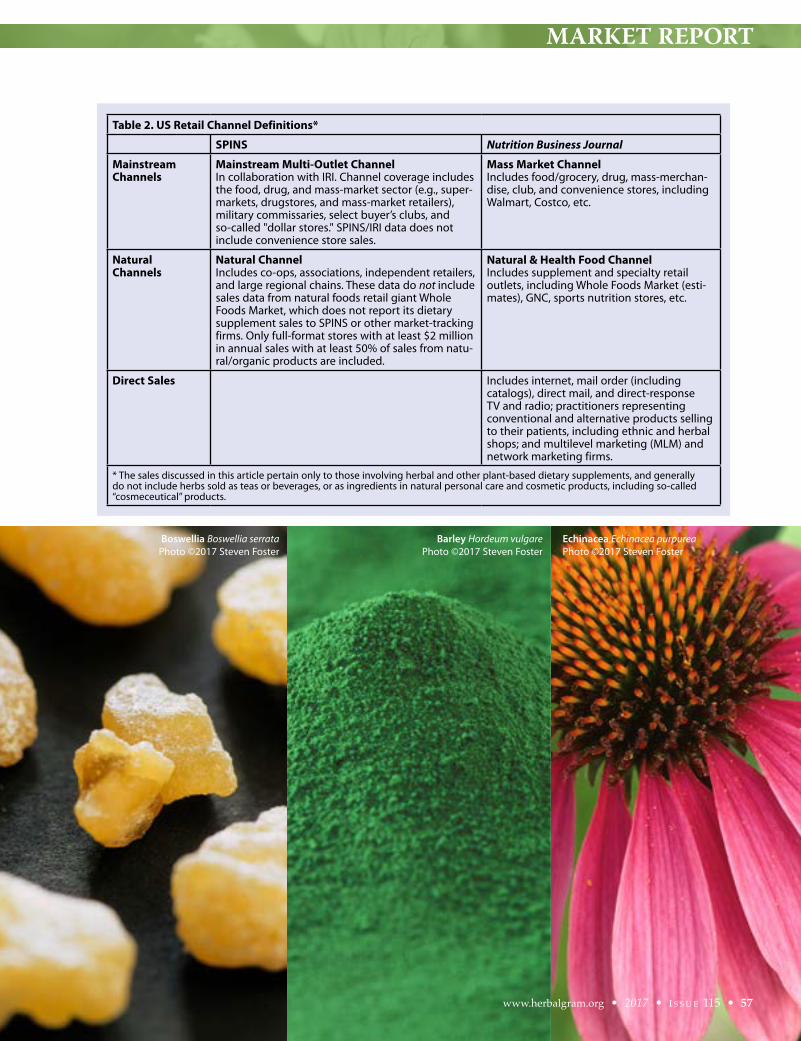
MARKET REPORT
Table 2. US Retail Channel Definitions*
SPINS Nutrition Business Journal
Mainstream Channels
Mainstream Multi-Outlet ChannelIn collaboration with IRI. Channel coverage includes the food, drug, and mass-market sector (e.g., super-markets, drugstores, and mass-market retailers), military commissaries, select buyer’s clubs, and so-called "dollar stores." SPINS/IRI data does not include convenience store sales.
Mass Market ChannelIncludes food/grocery, drug, mass-merchan-dise, club, and convenience stores, including Walmart, Costco, etc.
Natural Channels
Natural Channel Includes co-ops, associations, independent retailers, and large regional chains. These data do not include sales data from natural foods retail giant Whole Foods Market, which does not report its dietary supplement sales to SPINS or other market-tracking firms. Only full-format stores with at least $2 million in annual sales with at least 50% of sales from natu-ral/organic products are included.
Natural & Health Food ChannelIncludes supplement and specialty retail outlets, including Whole Foods Market (esti-mates), GNC, sports nutrition stores, etc.
Direct Sales
Includes internet, mail order (including catalogs), direct mail, and direct-response TV and radio; practitioners representing conventional and alternative products selling to their patients, including ethnic and herbal shops; and multilevel marketing (MLM) and network marketing firms.
* The sales discussed in this article pertain only to those involving herbal and other plant-based dietary supplements, and generally do not include herbs sold as teas or beverages, or as ingredients in natural personal care and cosmetic products, including so-called “cosmeceutical” products.
www.herbalgram.org • 2017 • I S S U E 115 • 57
Boswellia Boswellia serrataPhoto ©2017 Steven Foster
Echinacea Echinacea purpureaPhoto ©2017 Steven Foster
Barley Hordeum vulgarePhoto ©2017 Steven Foster
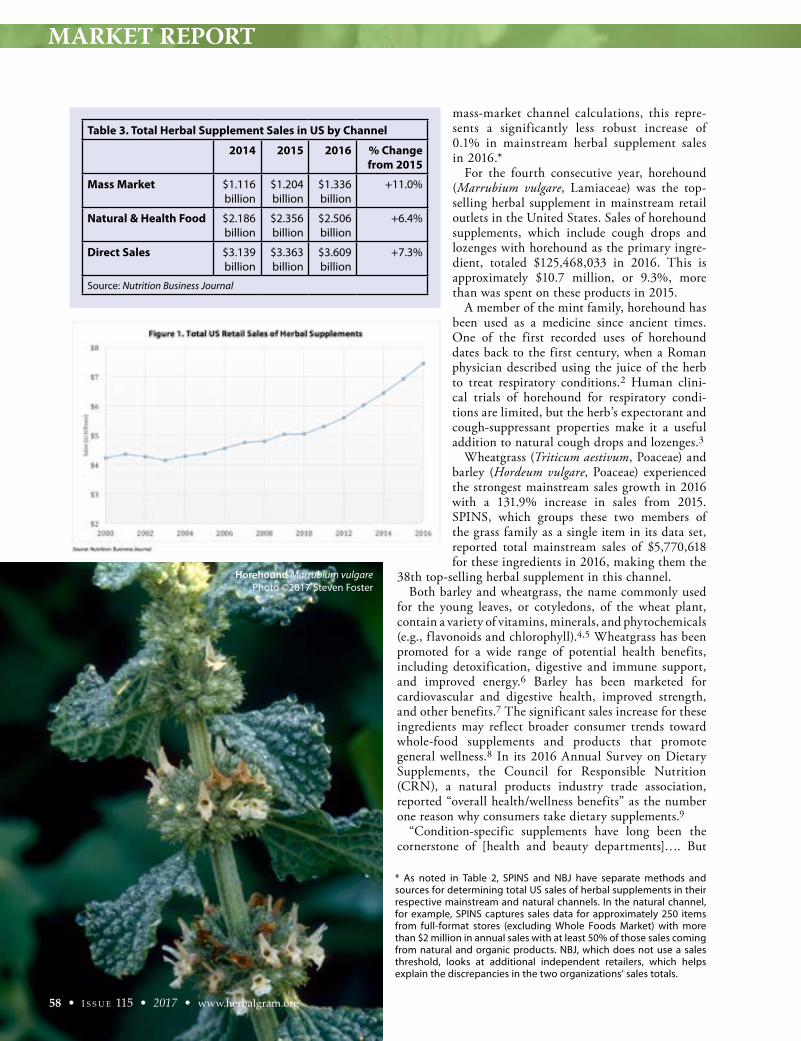
MARKET REPORT
mass-market channel calculations, this repre-sents a significantly less robust increase of 0.1% in mainstream herbal supplement sales in 2016.*
For the fourth consecutive year, horehound (Marrubium vulgare, Lamiaceae) was the top-selling herbal supplement in mainstream retail outlets in the United States. Sales of horehound supplements, which include cough drops and lozenges with horehound as the primary ingre-dient, totaled $125,468,033 in 2016. This is approximately $10.7 million, or 9.3%, more than was spent on these products in 2015.
A member of the mint family, horehound has been used as a medicine since ancient times. One of the first recorded uses of horehound dates back to the first century, when a Roman physician described using the juice of the herb to treat respiratory conditions.2 Human clini-cal trials of horehound for respiratory condi-tions are limited, but the herb’s expectorant and cough-suppressant properties make it a useful addition to natural cough drops and lozenges.3
Wheatgrass (Triticum aestivum, Poaceae) and barley (Hordeum vulgare, Poaceae) experienced the strongest mainstream sales growth in 2016 with a 131.9% increase in sales from 2015. SPINS, which groups these two members of the grass family as a single item in its data set, reported total mainstream sales of $5,770,618 for these ingredients in 2016, making them the
38th top-selling herbal supplement in this channel. Both barley and wheatgrass, the name commonly used
for the young leaves, or cotyledons, of the wheat plant, contain a variety of vitamins, minerals, and phytochemicals (e.g., f lavonoids and chlorophyll).4,5 Wheatgrass has been promoted for a wide range of potential health benefits, including detoxification, digestive and immune support, and improved energy.6 Barley has been marketed for cardiovascular and digestive health, improved strength, and other benefits.7 The significant sales increase for these ingredients may reflect broader consumer trends toward whole-food supplements and products that promote general wellness.8 In its 2016 Annual Survey on Dietary Supplements, the Council for Responsible Nutrition (CRN), a natural products industry trade association, reported “overall health/wellness benefits” as the number one reason why consumers take dietary supplements.9
“Condition-specific supplements have long been the cornerstone of [health and beauty departments]…. But
Table 3. Total Herbal Supplement Sales in US by Channel
2014 2015 2016 % Change from 2015
Mass Market $1.116 billion
$1.204 billion
$1.336 billion
+11.0%
Natural & Health Food $2.186 billion
$2.356 billion
$2.506 billion
+6.4%
Direct Sales $3.139 billion
$3.363 billion
$3.609 billion
+7.3%
Source: Nutrition Business Journal
58 • I S S U E 115 • 2017 • www.herbalgram.org
* As noted in Table 2, SPINS and NBJ have separate methods and sources for determining total US sales of herbal supplements in their respective mainstream and natural channels. In the natural channel, for example, SPINS captures sales data for approximately 250 items from full-format stores (excluding Whole Foods Market) with more than $2 million in annual sales with at least 50% of those sales coming from natural and organic products. NBJ, which does not use a sales threshold, looks at additional independent retailers, which helps explain the discrepancies in the two organizations’ sales totals.
Horehound Marrubium vulgarePhoto ©2017 Steven Foster
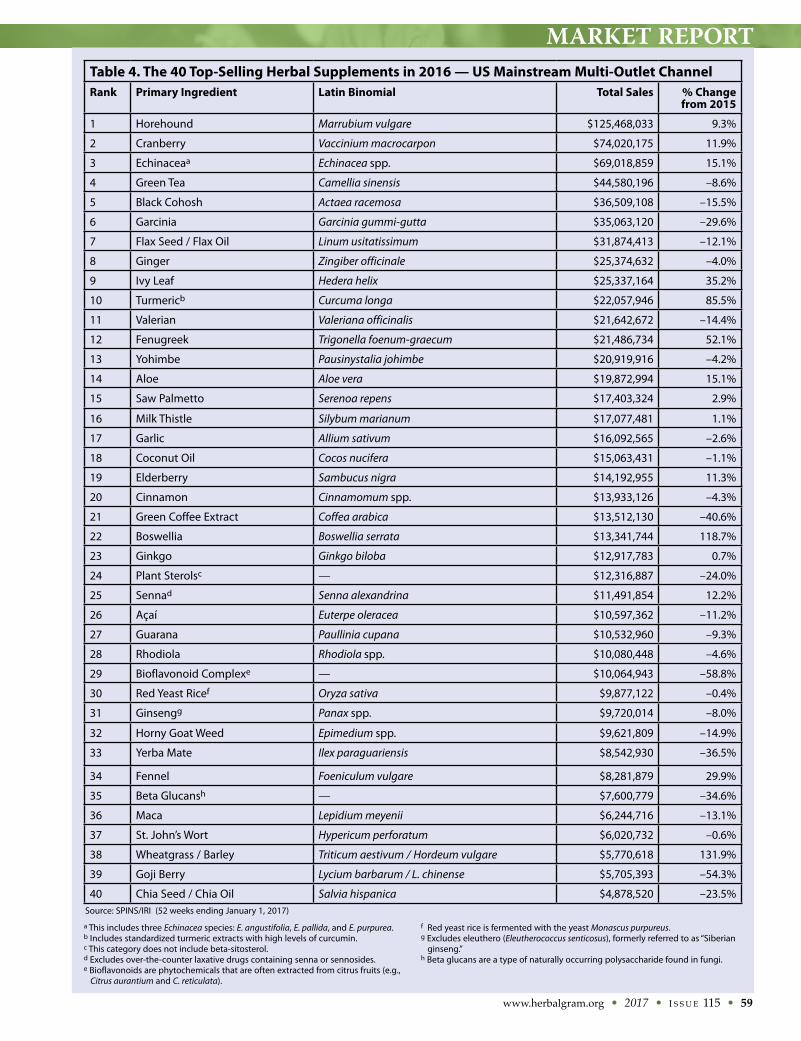
MARKET REPORT
www.herbalgram.org • 2017 • I S S U E 115 • 59
Table 4. The 40 Top-Selling Herbal Supplements in 2016 — US Mainstream Multi-Outlet Channel Rank Primary Ingredient Latin Binomial Total Sales % Change
from 2015
1 Horehound Marrubium vulgare $125,468,033 9.3%
2 Cranberry Vaccinium macrocarpon $74,020,175 11.9%
3 Echinaceaa Echinacea spp. $69,018,859 15.1%
4 Green Tea Camellia sinensis $44,580,196 –8.6%
5 Black Cohosh Actaea racemosa $36,509,108 –15.5%
6 Garcinia Garcinia gummi-gutta $35,063,120 –29.6%
7 Flax Seed / Flax Oil Linum usitatissimum $31,874,413 –12.1%
8 Ginger Zingiber officinale $25,374,632 –4.0%
9 Ivy Leaf Hedera helix $25,337,164 35.2%
10 Turmericb Curcuma longa $22,057,946 85.5%
11 Valerian Valeriana officinalis $21,642,672 –14.4%
12 Fenugreek Trigonella foenum-graecum $21,486,734 52.1%
13 Yohimbe Pausinystalia johimbe $20,919,916 –4.2%
14 Aloe Aloe vera $19,872,994 15.1%
15 Saw Palmetto Serenoa repens $17,403,324 2.9%
16 Milk Thistle Silybum marianum $17,077,481 1.1%
17 Garlic Allium sativum $16,092,565 –2.6%
18 Coconut Oil Cocos nucifera $15,063,431 –1.1%
19 Elderberry Sambucus nigra $14,192,955 11.3%
20 Cinnamon Cinnamomum spp. $13,933,126 –4.3%
21 Green Coffee Extract Coffea arabica $13,512,130 –40.6%
22 Boswellia Boswellia serrata $13,341,744 118.7%
23 Ginkgo Ginkgo biloba $12,917,783 0.7%
24 Plant Sterolsc — $12,316,887 –24.0%
25 Sennad Senna alexandrina $11,491,854 12.2%
26 Açaí Euterpe oleracea $10,597,362 –11.2%
27 Guarana Paullinia cupana $10,532,960 –9.3%
28 Rhodiola Rhodiola spp. $10,080,448 –4.6%
29 Bioflavonoid Complexe — $10,064,943 –58.8%
30 Red Yeast Ricef Oryza sativa $9,877,122 –0.4%
31 Ginsengg Panax spp. $9,720,014 –8.0%
32 Horny Goat Weed Epimedium spp. $9,621,809 –14.9%
33 Yerba Mate Ilex paraguariensis $8,542,930 –36.5%
34 Fennel Foeniculum vulgare $8,281,879 29.9%
35 Beta Glucansh — $7,600,779 –34.6%
36 Maca Lepidium meyenii $6,244,716 –13.1%
37 St. John’s Wort Hypericum perforatum $6,020,732 –0.6%
38 Wheatgrass / Barley Triticum aestivum / Hordeum vulgare $5,770,618 131.9%
39 Goji Berry Lycium barbarum / L. chinense $5,705,393 –54.3%
40 Chia Seed / Chia Oil Salvia hispanica $4,878,520 –23.5%
a This includes three Echinacea species: E. angustifolia, E. pallida, and E. purpurea.b Includes standardized turmeric extracts with high levels of curcumin.c This category does not include beta-sitosterol.d Excludes over-the-counter laxative drugs containing senna or sennosides.e Bioflavonoids are phytochemicals that are often extracted from citrus fruits (e.g., Citrus aurantium and C. reticulata).
f Red yeast rice is fermented with the yeast Monascus purpureus.g Excludes eleuthero (Eleutherococcus senticosus), formerly referred to as “Siberian ginseng.”h Beta glucans are a type of naturally occurring polysaccharide found in fungi.
Source: SPINS/IRI (52 weeks ending January 1, 2017)

MARKET REPORT
the new way forward isn’t predicated on any single health condition,” noted an October 2016 article from Natural Foods Merchandiser, a New Hope Network publication.8 “Rather, it focuses on supplements that support whole-body health.”
The nutrient density of wheatgrass and barley has earned them a reputation as so-called “superfoods.” These grasses are available in various forms, including as juices, capsules, and powders, as well as in combination products marketed as “supergreens” (a term that refers to various nutrient-rich leafy greens) that are used to boost the nutritional content of smoothies and other beverages. According to CRN’s 2016 survey, “filling in nutrient gaps in the diet” was the third most common reason for consumers to take supple-
ments.9 Suffering from “pill fatigue,” health-conscious consumers have turned to these easy-to-consume sources of nutrition that can be incorporated into beverages. As such, wheatgrass and barley sales likely were impacted by the “green beverage” trend that took hold in 2016.10
Three other ingredients experienced mainstream sales increases of more than 50% in 2016: boswellia (Boswellia serrata, Burseraceae; +118.7%), turmeric (Curcuma longa, Zingiberaceae; +85.5%), and fenugreek (Trigonella foenum-graecum, Fabaceae; +52.1%). This growth is less pronounced than the sales increases seen in 2015, in which mainstream sales for each of these herbs more than doubled from 2014. (Sales of boswellia, for example, increased by a remarkable 673.6% from 2014 to 2015.)
Boswellia, turmeric, and fenugreek have been used traditionally in Ayurveda, an ancient system of medicine in India that has become increasingly well-known to consumers in the West.11,12 The contin-ued popularity of these ingredients in 2016 may be due in part to the growing consumer awareness of Ayurvedic herbs.13
Bioflavonoid complex, the 29th top-selling herbal supplement in the main-stream channel in 2016, experienced a 58.8% decrease in sales from 2015 — the largest sales decline of any of the top 40 herbs in the mainstream channel. Biofla-vonoids are a group of phytochemicals that have been studied for a range of poten-tial health benefits. These compounds have been shown to increase vitamin C absorption, and researchers have exam-ined their ability to lower cholesterol, promote circulation, and reduce inflam-mation.14 In 2015, bioflavonoid complex was the 10th top-selling herbal supple-ment in this channel, and it experienced a 24.5% increase in mainstream sales from 2014 to 2015. The reasons for the sharp decline in sales in 2016 are unclear, but they may be related to consumer prefer-ences for easily recognizable ingredients that promote general wellness.10 Accord-ing to SPINS, some of the top-selling bioflavonoid products included in the 2016 data set were marketed for specific health conditions, which likely limited their general appeal.
With a 54.3% decline in sales from 2015 to 2016, goji berry (Lycium barbarum and L. chinense, Solanaceae) was the only other herbal ingredient with a decrease of more than 50% in mainstream sales during this period. Goji berry dropped from the 26th top-selling supplement in 2015 to the 39th in 2016. Goji berry,
60 • I S S U E 115 • 2017 • www.herbalgram.org
Dandelion Taraxacum officinalePhoto ©2017 Steven Foster
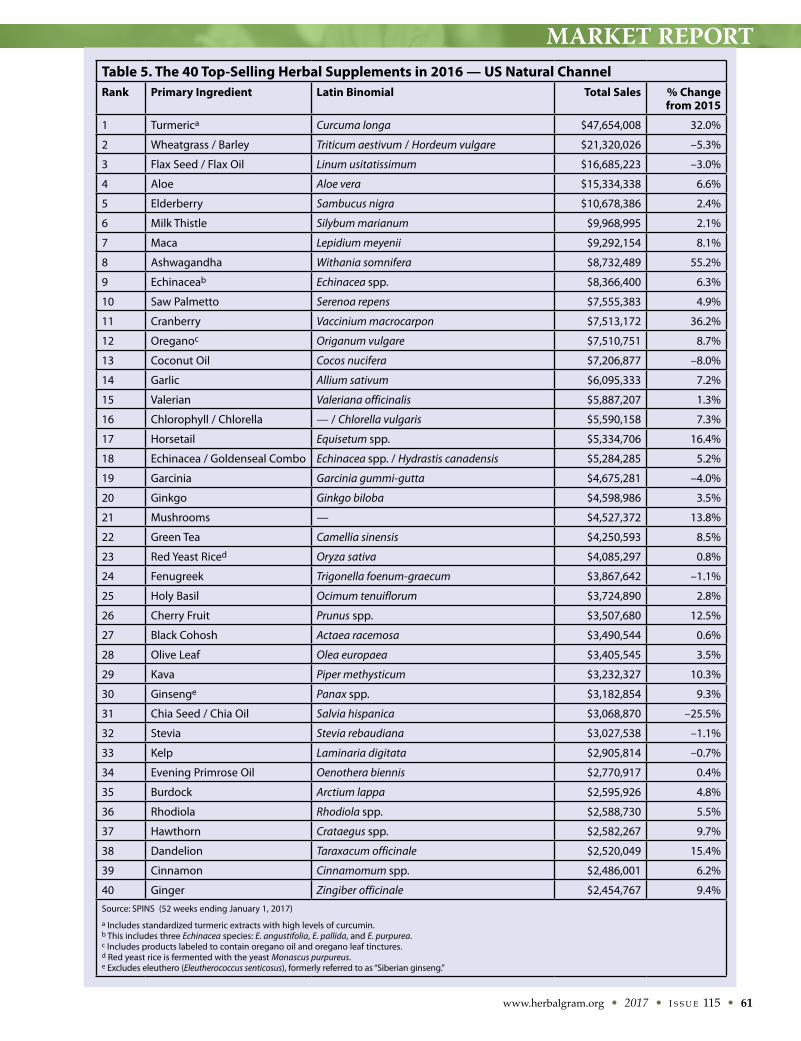
MARKET REPORT
www.herbalgram.org • 2017 • I S S U E 115 • 61
Table 5. The 40 Top-Selling Herbal Supplements in 2016 — US Natural Channel Rank Primary Ingredient Latin Binomial Total Sales % Change
from 2015
1 Turmerica Curcuma longa $47,654,008 32.0%
2 Wheatgrass / Barley Triticum aestivum / Hordeum vulgare $21,320,026 –5.3%
3 Flax Seed / Flax Oil Linum usitatissimum $16,685,223 –3.0%
4 Aloe Aloe vera $15,334,338 6.6%
5 Elderberry Sambucus nigra $10,678,386 2.4%
6 Milk Thistle Silybum marianum $9,968,995 2.1%
7 Maca Lepidium meyenii $9,292,154 8.1%
8 Ashwagandha Withania somnifera $8,732,489 55.2%
9 Echinaceab Echinacea spp. $8,366,400 6.3%
10 Saw Palmetto Serenoa repens $7,555,383 4.9%
11 Cranberry Vaccinium macrocarpon $7,513,172 36.2%
12 Oreganoc Origanum vulgare $7,510,751 8.7%
13 Coconut Oil Cocos nucifera $7,206,877 –8.0%
14 Garlic Allium sativum $6,095,333 7.2%
15 Valerian Valeriana officinalis $5,887,207 1.3%
16 Chlorophyll / Chlorella — / Chlorella vulgaris $5,590,158 7.3%
17 Horsetail Equisetum spp. $5,334,706 16.4%
18 Echinacea / Goldenseal Combo Echinacea spp. / Hydrastis canadensis $5,284,285 5.2%
19 Garcinia Garcinia gummi-gutta $4,675,281 –4.0%
20 Ginkgo Ginkgo biloba $4,598,986 3.5%
21 Mushrooms — $4,527,372 13.8%
22 Green Tea Camellia sinensis $4,250,593 8.5%
23 Red Yeast Riced Oryza sativa $4,085,297 0.8%
24 Fenugreek Trigonella foenum-graecum $3,867,642 –1.1%
25 Holy Basil Ocimum tenuiflorum $3,724,890 2.8%
26 Cherry Fruit Prunus spp. $3,507,680 12.5%
27 Black Cohosh Actaea racemosa $3,490,544 0.6%
28 Olive Leaf Olea europaea $3,405,545 3.5%
29 Kava Piper methysticum $3,232,327 10.3%
30 Ginsenge Panax spp. $3,182,854 9.3%
31 Chia Seed / Chia Oil Salvia hispanica $3,068,870 –25.5%
32 Stevia Stevia rebaudiana $3,027,538 –1.1%
33 Kelp Laminaria digitata $2,905,814 –0.7%
34 Evening Primrose Oil Oenothera biennis $2,770,917 0.4%
35 Burdock Arctium lappa $2,595,926 4.8%
36 Rhodiola Rhodiola spp. $2,588,730 5.5%
37 Hawthorn Crataegus spp. $2,582,267 9.7%
38 Dandelion Taraxacum officinale $2,520,049 15.4%
39 Cinnamon Cinnamomum spp. $2,486,001 6.2%
40 Ginger Zingiber officinale $2,454,767 9.4%
Source: SPINS (52 weeks ending January 1, 2017)
a Includes standardized turmeric extracts with high levels of curcumin.b This includes three Echinacea species: E. angustifolia, E. pallida, and E. purpurea.c Includes products labeled to contain oregano oil and oregano leaf tinctures. d Red yeast rice is fermented with the yeast Monascus purpureus.e Excludes eleuthero (Eleutherococcus senticosus), formerly referred to as “Siberian ginseng.”
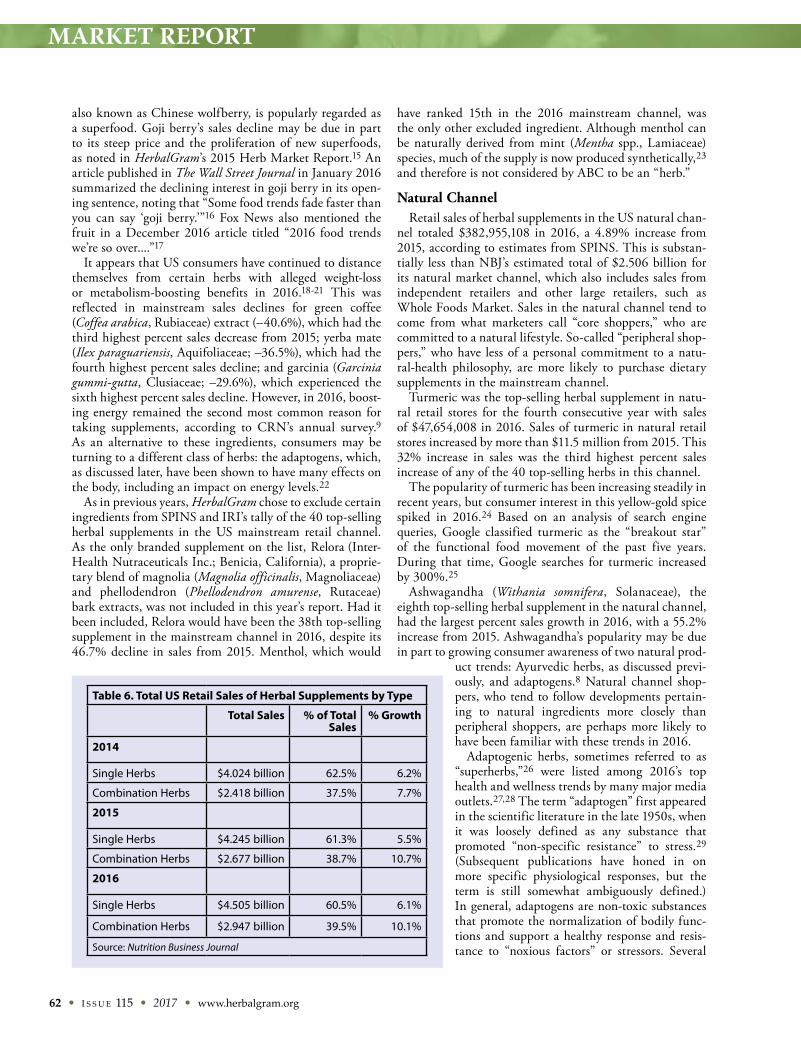
MARKET REPORT
62 • I S S U E 115 • 2017 • www.herbalgram.org
also known as Chinese wolfberry, is popularly regarded as a superfood. Goji berry’s sales decline may be due in part to its steep price and the proliferation of new superfoods, as noted in HerbalGram’s 2015 Herb Market Report.15 An article published in The Wall Street Journal in January 2016 summarized the declining interest in goji berry in its open-ing sentence, noting that “Some food trends fade faster than you can say ‘goji berry.’”16 Fox News also mentioned the fruit in a December 2016 article titled “2016 food trends we’re so over....”17
It appears that US consumers have continued to distance themselves from certain herbs with alleged weight-loss or metabolism-boosting benefits in 2016.18-21 This was reflected in mainstream sales declines for green coffee (Coffea arabica, Rubiaceae) extract (–40.6%), which had the third highest percent sales decrease from 2015; yerba mate (Ilex paraguariensis, Aquifoliaceae; –36.5%), which had the fourth highest percent sales decline; and garcinia (Garcinia gummi-gutta, Clusiaceae; –29.6%), which experienced the sixth highest percent sales decline. However, in 2016, boost-ing energy remained the second most common reason for taking supplements, according to CRN’s annual survey.9 As an alternative to these ingredients, consumers may be turning to a different class of herbs: the adaptogens, which, as discussed later, have been shown to have many effects on the body, including an impact on energy levels.22
As in previous years, HerbalGram chose to exclude certain ingredients from SPINS and IRI’s tally of the 40 top-selling herbal supplements in the US mainstream retail channel. As the only branded supplement on the list, Relora (Inter-Health Nutraceuticals Inc.; Benicia, California), a proprie-tary blend of magnolia (Magnolia officinalis, Magnoliaceae) and phellodendron (Phellodendron amurense, Rutaceae) bark extracts, was not included in this year’s report. Had it been included, Relora would have been the 38th top-selling supplement in the mainstream channel in 2016, despite its 46.7% decline in sales from 2015. Menthol, which would
have ranked 15th in the 2016 mainstream channel, was the only other excluded ingredient. Although menthol can be naturally derived from mint (Mentha spp., Lamiaceae) species, much of the supply is now produced synthetically,23 and therefore is not considered by ABC to be an “herb.”
Natural ChannelRetail sales of herbal supplements in the US natural chan-
nel totaled $382,955,108 in 2016, a 4.89% increase from 2015, according to estimates from SPINS. This is substan-tially less than NBJ’s estimated total of $2.506 billion for its natural market channel, which also includes sales from independent retailers and other large retailers, such as Whole Foods Market. Sales in the natural channel tend to come from what marketers call “core shoppers,” who are committed to a natural lifestyle. So-called “peripheral shop-pers,” who have less of a personal commitment to a natu-ral-health philosophy, are more likely to purchase dietary supplements in the mainstream channel.
Turmeric was the top-selling herbal supplement in natu-ral retail stores for the fourth consecutive year with sales of $47,654,008 in 2016. Sales of turmeric in natural retail stores increased by more than $11.5 million from 2015. This 32% increase in sales was the third highest percent sales increase of any of the 40 top-selling herbs in this channel.
The popularity of turmeric has been increasing steadily in recent years, but consumer interest in this yellow-gold spice spiked in 2016.24 Based on an analysis of search engine queries, Google classified turmeric as the “breakout star” of the functional food movement of the past five years. During that time, Google searches for turmeric increased by 300%.25
Ashwagandha (Withania somnifera, Solanaceae), the eighth top-selling herbal supplement in the natural channel, had the largest percent sales growth in 2016, with a 55.2% increase from 2015. Ashwagandha’s popularity may be due in part to growing consumer awareness of two natural prod-
uct trends: Ayurvedic herbs, as discussed previ-ously, and adaptogens.8 Natural channel shop-pers, who tend to follow developments pertain-ing to natural ingredients more closely than peripheral shoppers, are perhaps more likely to have been familiar with these trends in 2016.
Adaptogenic herbs, sometimes referred to as “superherbs,”26 were listed among 2016’s top health and wellness trends by many major media outlets.27,28 The term “adaptogen” first appeared in the scientific literature in the late 1950s, when it was loosely defined as any substance that promoted “non-specific resistance” to stress.29 (Subsequent publications have honed in on more specific physiological responses, but the term is still somewhat ambiguously defined.) In general, adaptogens are non-toxic substances that promote the normalization of bodily func-tions and support a healthy response and resis-tance to “noxious factors” or stressors. Several
Table 6. Total US Retail Sales of Herbal Supplements by Type
Total Sales % of Total Sales
% Growth
2014
Single Herbs $4.024 billion 62.5% 6.2%
Combination Herbs $2.418 billion 37.5% 7.7%
2015
Single Herbs $4.245 billion 61.3% 5.5%
Combination Herbs $2.677 billion 38.7% 10.7%
2016
Single Herbs $4.505 billion 60.5% 6.1%
Combination Herbs $2.947 billion 39.5% 10.1%
Source: Nutrition Business Journal

MARKET REPORT
www.herbalgram.org • 2017 • I S S U E 115 • 63
other ingredients with adaptogenic properties experienced natural channel sales growth in 2016, including mush-rooms (+13.8%), “ginseng” (Panax spp., Araliaceae; +9.3%), rhodiola (Rhodiola spp., Crassulaceae; +5.5%), and holy basil (Ocimum tenuiflorum, Lamiaceae; +2.8%).
The top-selling herbal ingredients in the 2016 natu-ral channel were the same as those that made the top-40 list in 2015, with one exception: dandelion (Taraxacum officinale, Asteraceae). Natural channel sales of dandelion in 2016 totaled $2,520,049, a 15.4% increase from 2015. (Dandelion, which came in as the 38th top-selling herb in 2016, displaced St. John’s wort [Hypericum perforatum, Hypericaceae] from the list.) Although dandelion may be better known as a weed, preparations of the root30,31 have been used for millennia as a medicine for liver and kidney diseases, upset stomach, and heartburn, among other condi-tions.32 As an ingredient in herbal dietary supplements, dandelion is commonly found in teas marketed for detoxification, weight loss, digestive health, and stimulation of urine flow and appetite.33
Dandelion30 is one of several herbal ingre-dients with bitter properties to make the list of top-selling herbal ingredients in 2016. Other herbs include green tea (Camellia sinensis, Theaceae; +8.5%), aloe (Aloe vera, Xanthor-rhoeaceae) +6.6%), echinacea (Echinacea spp., Asteraceae; +6.3%), burdock (Arctium lappa, Asteraceae; +4.8%), and milk thistle (Silybum marianum, Asteraceae; +2.1%).34 Bitterness as a flavor also ranked among the food and beverage trends of 2016. Herbs, includ-ing some of the previously discussed leafy greens, produce a wide variety of compounds that humans perceive as bitter-tasting. The consumption of certain bitter phytochemicals has been linked to a wide range of health benefits, but the compounds are perhaps most closely associated with digestion. The scientific explanation behind this relation-ship is well established. “As most naturally occurring bitter tasting stimuli are toxins at some concentration, the body responds to strong bitter tastes as if toxins are about to be ingested,” explained the authors of a 2013 review article.35 As part of the body’s first line of defense, the gastrointestinal system responds by attempting to limit the impact of the potential toxin.
Emerging research on the “gut-brain connection” and the importance of intesti-nal microbiota to overall health has likely fueled consumer interest in bitter and diges-tive health products.36 However, according to some sources, consumers are still buying
digestive health products primarily to address specific issues, such as constipation and diarrhea. “While these reactive digestive issues are the main reason for using these types of products, there are many opportunities for category expansion based on a prevention platform,” a 2016 “Mind of the Consumer” report by Natural Products INSIDER noted.37 “Within this white space are conditions such as immunity, mental focus, weight loss, energy and joint issues — all of which can be linked back to digestive health.”
Fenugreek Trigonella foenum-graecumPhoto ©2017 Steven Foster

MARKET REPORT
64 • I S S U E 115 • 2017 • www.herbalgram.org
Direct SalesDirect sales of herbal supplements totaled $3.609 billion
in 2016, a 7.3% increase from 2015 sales in this channel, according to NBJ. This is the highest percentage increase in direct sales of herbal supplements in more than a decade, according to previous HerbalGram herb market reports. Direct channel sales of herbal dietary supplements include multilevel marketing companies (also known as network marketing companies). This channel also encompasses mail- and internet-order sales companies, direct-response TV and radio sales, and sales by health practitioners.
According to a NutraIngredients-USA article from Octo-ber 2016: “Network marketing continues to be a huge outlet for nutritional products, and direct selling companies with supplements in their portfolios are among the best perform-ing of these companies.”38
Single-Herb vs. Combination-Herb SupplementsSince 2011, sales growth of combination-herb supplements
has outpaced that of single-herb supplements, and this trend continued in 2016. Combination-herb supplement sales in all channels grew 10.1% from 2015, and single-herb supple-ment sales increased by 6.1%. However, as noted in Table 6, total sales of single-herb supplements were higher overall than sales of combination-herb supplements in 2016, accord-ing to NBJ.
Conclusion2016 marked the 13th consecutive year of overall sales
growth for herbal supplements and the eighth year of increased sales in each of the three market channels. This suggests that consumers — from casual shoppers in main-stream retail outlets to core consumers of natural products — are continuing to turn to plant- and fungi-based options for their health care and self-care.
The shifts in sales of certain ingredients in 2016 point to the evolving preferences and priorities of consumers. Although shoppers are still buying supplements to address specific health concerns, increased sales for herbal ingredi-ents marketed for overall wellness and vitality suggest that some are taking a more proactive, holistic approach to well-ness. In particular, sales of adaptogenic herbs, a category of plants with broad and appealing effects, seem to have benefited from this trend. As scientific research continues to explore the connection between the digestive system and overall health, the rise of bitter herbs and other products marketed for gastrointestinal health may also be a compo-nent of this “systemic wellness” trend.
References1. FDA basics: What is a dietary supplement? US Food &
Drug Administration website. Available at: www.fda.gov/aboutfda/transparency/basics/ucm195635.htm. Accessed July 19, 2017.
2. Horehound herb. Natural Remedies website. Available at: www.naturalremedies.org/horehound/. Accessed July 19, 2017.
3. Horehound. University of Michigan Medicine website. Avail-able at: www.uofmhealth.org/health-library/hn-2109003. Accessed July 19, 2017.
4. What are the benefits of wheatgrass? Mercola website. Avail-able at: http://articles.mercola.com/herbs-spices/wheatgrass.aspx. Accessed July 19, 2017.
5. Barley grass. Drugs.com website. Available at: www.drugs.com/npc/barley-grass.html. Accessed July 19, 2017.
6. Wheatgrass benefits: 11 reasons to enjoy. Healthline website. Available at: www.healthline.com/health/food-nutrition/wheatgrass-benefits#superfood2. Accessed July 19, 2017.
7. Barley. WebMD website. Available at: www.webmd.com/vitamins-supplements/ingredientmono-799-barley.aspx?activeingredientid=799&activeingredientname=barley. Accessed July 19, 2017.
8. Runestad T. Supplement Trendspotting. October 24, 2016. Natural Foods Merchandiser. Available at: www.newhope.com/vitamins-and-supplements/supplement-trendspotting. Accessed July 19, 2017.
9. Consumer data: CRN 2016 Annual Survey on Dietary Supplements. Council for Responsible Nutrition website. Available at: www.crnusa.org/resources/crn-2016-annual-survey-dietary-supplements. Accessed July 19, 2017.
10. Now trending: 10 ways the smoothie is evolving in 2016. Fast Casual website. Available at: www.fastcasual.com/articles/now-trending-10-ways-the-smoothie-is-evolving-in-2016/. Accessed July 19, 2017.
11. Uses of Fenugreek in Ayurvedic Medicine. Livestrong website. Available at: www.livestrong.com/article/157975-uses-of-fenugreek-in-ayurvedic-medicine/. Accessed July 19, 2017.
12. Ayurveda: A New Way to Reduce Inflammation. Peoples Rx website. Available at: http://peoplesrx.com/ayurveda-a-new-way-to-reduce-inflammation/. Accessed July 19, 2017.
13. Wolff K. How Do FDA and FTC Regulate Ayurveda Prod-ucts? October 3, 2017. Nutritional Outlook. Available at: www.nutritionaloutlook.com/regulatory/how-do-fda-and-ftc-regulate-ayurveda-products. Accessed July 19, 2017.
14. What Are the Benefits of Citrus Bioflavonoids? Livestrong website. Available at: www.livestrong.com/article/425030-what-are-the-benefits-of-citrus-bioflavonoids/. Accessed July 19, 2017.
15. Smith T, Kawa K, Eckl V, Johnson J. Sales of Herbal Dietary Supplements in US Increased 7.5% in 2015. HerbalGram. 2016;111:67-73. Available at: http://cms.herbalgram.org/herbalgram/issue111/hg111-mktrpt.html. Accessed July 19, 2017.
16. Krieger E. Got matcha? Five healthy foods that will make their mark on 2016. January 12, 2016. The Wall Street Journal. Available at: www.washingtonpost.com/lifestyle/wellness/got-matcha-five-healthy-foods-that-will-make-their-mark-on-2016/2016/01/11/7a92bfca-b3dc-11e5-a76a-0b5145e8679a_story.html. Accessed July 19, 2017.
17. Sager R. 2016 food trends we’re so over and 5 big ideas we can’t for in 2017. Fox News website. Available at: www.foxnews.com/food-drink/2016/12/30/2016-food-trends-were-so-over-and-5-big-ideas-cant-for-in-2017.html. Accessed July 19, 2017.
18. Moloughney S. Energy Trends: The Market Charges On. January 3, 2017. Nutraceuticals World. Available at: www.nutraceuticalsworld.com/issues/2017-01/view_features/energy-trends-the-market-charges-on/. Accessed July 19, 2017.
http://www.nutraceuticalsworld.com/issues/2017-01/view_features/energy-trends-the-market-charges-on/
MARKET REPORT
www.herbalgram.org • 2017 • I S S U E 115 • 65
19. Can Garcinia Cambogia Help with Weight Loss? Healthline website. Available at: www.healthline.com/health/garcinia-cambogia-weight-loss#what-is-it1. Accessed July 25, 2017.
20. Yerba mate. WebMD website. Available at: www.webmd.com/vitamins-supplements/ingredientmono-828-yerba%20mate.aspx. Accessed July 25, 2017.
21. What is green coffee bean extract? Healthline website. Available at: http://www.healthline.com/health/green-coffee-bean-weight-loss. Accessed July 25, 2017.
22. Romm A. Adaptogens: Herbs for Beating Stress, Fighting Fatigue & Banishing Cravings. Aviva Romm, MD website. Available at: https://avivaromm.com/adaptogens-beating-stress/. Accessed July 19, 2017.
23. Cotton S. Menthol. March 6, 2013. Chemistry World. Available at: https://www.chemistryworld.com/podcasts/menthol/6109.article. Accessed July 19, 2017.
24. Pina P. The Rise of Functional Foods. April 2016. Think with Google website. Available at: www.thinkwithgoogle.com/consumer-insights/2016-food-trends-google/. Accessed July 19, 2017.
25. Food Trends 2016. Google. Available at: https://think.storage.googleapis.com/docs/FoodTrends-2016.pdf. Accessed July 19, 2017.
26. Wang J. The A to Z of health and fitness trends for 2016. January 2, 2017. South China Morning Post. Available at: http://www.scmp.com/lifestyle/health-beauty/article/1896785/z-hot-button-health-issues-2016. Accessed July 19, 2017.
27. Wellness trends to enhance your life in 2016. December 22, 2015. CBS News website. Available at: http://www.cbsnews.com/news/wellness-trends-to-enhance-your-life-in-2016/. Accessed July 19, 2017.
28. Norton S. 16 health trends to look out for in 2016. January 19, 2016. The Independent. Available at: www.indepen-dent.co.uk/life-style/16-health-trends-to-look-out-for-in-2016-a6815211.html. Accessed July 19, 2017.
29. Panossian A, Wagner H. Adaptogens: A review of their history, biological activity, and clinical benefits. HerbalGram. 2011;90:52-63. Available at: http://cms.herbalgram.org/herbal-gram/issue90/Feat_Adaptogens.html. Accessed July 19, 2017.
30. Chapter 1: A Field Trip. In: Green J. The Herbal Medicine-Maker’s Handbook: A Home Manual. New York, NY; Crossing Press: 2000:15-16.
31. Dandelion root with herb. Blumenthal M, Goldberg A, Brinckmann J. Herbal Medicine: Expanded Commission E Monographs. Austin, TX: American Botanical Council; Boston: Integrative Medicine Communications, 2000. Avail-able at: http://cms.herbalgram.org/expandedE/Dandelion-rootwithherb.html. Accessed July 25, 2017.
32. Dandelion. The University of Maryland Medical Center website. Available at: www.umm.edu/health/medical/altmed/herb/dandelion. Accessed July 19, 2017.
33. 7 Ways Dandelion Tea Could Be Good for You. Healthline website. Available at: www.healthline.com/health/ways-dandelion-tea-could-be-good-for-your#3. Accessed July 19, 2017.
34. Bitter Herbs for Better Digestion. Riordan Clinic website. Available at: https://riordanclinic.org/2014/03/bitter-herbs-for-better-digestion/. Accessed July 19, 2017.
35. Breslin PAS. An evolutionary perspective on food and human taste. Current Biology. 2013;23(9):409-418. Available at: www.sciencedirect.com/science/article/pii/S0960982213004181. Accessed July 19, 2017.
36. Moloughney S. Digestive Health: A Critical Pathway to Wellness. October 3, 2016. Nutraceuticals World. Available at: www.nutraceuticalsworld.com/issues/2016-10/view_features/digestive-health-a-critical-pathway-to-wellness/. Accessed July 19, 2017.
37. French S. The Mind of the Consumer: Digestive Health. November 2016. Natural Products INSIDER. Available at: www.naturalproductsinsider.com/~/media/Files/Nutrition/Ebooks/2016/11/11-16INS-MotC-DigestiveHealth-s.pdf. Accessed July 19, 2017.
38. Schultz H. Network marketing continues to be growing outlet for supplements. NutraIngredients-USA website. Available at: www.nutraingredients-usa.com/Markets/Network-marketing-continues-to-be-growing-outlet-for-supplements. Accessed July 19, 2017.
HerbalEGramABC’s Monthly eMagazineFeaturing timely, original articlesand a review of the month’s most important herbal happenings.
• An ABC membership benefit published the second week of each month.
• Exclusive excerpts from the latest herbal medicine-related books.
• All previous issues going back 10+ years available on ABC’s website at: http://cms.herbalgram.org/heg/index.html
66 • I S S U E 115 • 2017 • www.herbalgram.org
QUALITY CONTROL
Emerson Ecologics, a Manchester, New Hamp-shire-based wholesale distrib-utor of professional-oriented nutritional supplements for the integrative health care community has been a leader in bolstering the standards for these products with its Emer-son Quality Program (EQP). The program, launched in 2010, was the first program of its kind to assess and verify manufacturing practices of brands in the sector, according to Jaclyn Chasse, ND, vice president of science and regula-tory affairs for Emerson (email, July 17, 2017). Born from conversations with integrative health practitioners, the program was designed to ensure that the brands Emerson distributes comply with the US Food and Drug Admin-istration’s (FDA’s) current Good Manufacturing Practices (cGMPs) for dietary supplements, and to identify those brands that go above and beyond the baseline standards for compliance.
The launch of the EQP predated the full implementa-tion of cGMPs in June 2010 under the Dietary Supplement Health and Education Act of 1994 (DSHEA). Emerson was aware at the time of the challenges that practitioners faced with respect to the quality of supplements, said Chasse. “These practitioners were applying and using supplements as other practitioners apply medications. So they wanted to be sure they were not causing harm, that potencies were what they said on the label, and that they contained the correct plant to have the right effect,” she said (oral commu-nication, July 3, 2017).
Currently, the EQP requires all companies (also referred to as “brands” by Emerson) whose products are distributed by Emerson to complete a three-phase process.2 The first phase is cGMP compliance verification, which is reviewed and summarized by the Emerson Quality Department. The second phase of the program is a verification process in which Emerson conducts a document audit, requiring the brand to provide all requested manufacturing standard operating procedures (SOPs), as well as master manufactur-
ing records, batch/lot-specific manufacturing records, and analytical testing documenta-tion for selected products. The document audit is followed by verification product testing, in which certain potency or
contamination tests for selected products are conducted by an Emerson-qualified independent analytical labora-tory. The results must be consistent with the brand’s prod-uct specifications and standards, which must also meet EQP standards. The final phase is a full-day, onsite audit conducted by Emerson quality personnel with a review and audit report. Program participants must correct any find-ings from the audit.
The current Emerson Partner standard is required for all distributed brands and ensures practices that are consistent with high-quality, safe, and reliable dietary supplements.3
Getting Companies on BoardThere have been changes to the program over the years.
When it first rolled out, the basic certification was called a Green Partnership, which verified that brands met cGMP standards. Silver and Gold Partnerships, which required additional verifications and onsite audits, identified compa-nies that went beyond the baseline level.
Early on, it was difficult to get every company to embrace the program, Chasse recalled. Many company executives were excited about the program, but others were more cautious, so Emerson worked to anticipate any objections. “We took ownership of the cost, because in the beginning we wanted to be sure that EQP was not a ‘pay-to-play’ program,” she said. “We wanted to eliminate hurdles for small brands and any perception that you could throw money at the program and get the seal.”
Emerson found that the program struck a chord for prac-titioners in particular. “What we saw over time was that the majority of Emerson’s sales are in the brands that are current Gold and Silver Partners,” Chasse wrote (email, August 3, 2017).
Emerson Ecologics’ Quality Standards Program Evolves with Dietary Supplements SegmentEditor’s note: This article is part of a series from the American Botanical Council (ABC) that deals with various issues and self-regulatory initiatives in the global botanical supply chain that are related to the authentication and identity, adulteration, and/or contamination of botanical raw materials, extracts, and essential oils. Previously, we published an article on the National Animal Supplement Council (a trade association of manufacturers and suppliers of supplements for pets) and its self-regulatory program to monitor authenticity and quality of ingredients used in its members’ products.1
Procedures that help ensure quality in the supply chain have become increasingly important and relevant for the supplements industry in recent years. Standards for products in the practitioner channel have received particular scrutiny. As more and more integrative medicine practitioners turn to supplements to address common nutritional challenges and health issues, ensuring the safety, efficacy, and integrity of these products is critical.

www.herbalgram.org • 2017 • I S S U E 115 • 67
QUALITY CONTROL
The EQP faced other challenges in the beginning. For example, as it laid out testing parameters, Emer-son quickly realized that companies have many different ways of test-ing and verifying products at vari-ous stages of manufacturing. “We wanted to make sure we were using valid methods and set parameters around how often companies were verifying potency and testing for relevant contaminants,” Chasse said.
There were also hurdles getting companies to share their processes. “Many companies are very proud of their manufac-turing practices and were open to bringing us in to audit and take a look at their practices,” Chasse explained. However, she added, some brands were more hesitant to disclose what they were doing or share trade secrets, especially if they used a contract manufacturer. (A contract manufacturer [CM] produces finished consumer products for many brand hold-ers; the contract manufacturer usually procures the raw mate-rials [although often the brand holder actually sets the speci-fications and purchases raw materials to be processed by the CM], checks the quality of these materials, mixes them, and processes them into capsules, tablets, liquids, etc., and into the packaging of the brand holder.)
“The communication hurdles have gotten better over time,” she noted, but added that disclosing information about contract manufacturers can still be difficult for some compa-nies. “If we don’t know who the contract manufacturer is, we cannot ensure it is cGMP compliant.”
In 2014, with cGMP compliance having been a legal requirement for all dietary supplement companies since 2010, Emerson believed that being cGMP verified should no longer be a special distinction, but should be the standard. They therefore eliminated the Green Partnership. “When we elimi-nated the Green Partner level and made those standards the base requirement for distribution, the existing Green Part-ners either moved up (by enhancing their quality practices because they wanted to retain a special seal) or they simply lost the seal. We now have 41 EQP brands. The majority of the sales still go through these brands,” she said. But Emer-son also distributes several hundred other smaller brands that must at least meet the baseline requirements.
The Silver and Gold Partner standards remain for brands that want to certify above and beyond the basic Emerson Partner level. (Companies that meet the Gold and Silver Partner standards still are considered EQP Partners.) In addi-tion to adhering to the basic Emerson Partner certification program, Silver Partners must meet the following require-ments:
• Acceptable supplier and contract brand qualifica-tions, such as cGMP compliance, and regular onsite audits. (In addition, certificates of analysis for raw materials and finished products are initially vali-
dated by conducting full confirmation testing);• SOP demonstration of controlled manufacturing
processes for all finished products and cGMP opera-tions;
• Specifications for all raw materials and finished products with documented use of standards;
• Use of appropriate testing methodologies when testing for identity, microbiological contamination, heavy metals, pesticides/herbicides (for botanicals), aflatoxins (when applicable), melamine (when appli-cable), and residual solvents;
• Raw material testing on each batch/lot or raw mate-rial testing at a frequency justified by a written ratio-nale, which will include a certificate of analysis for each ingredient, batch/lot testing for identity, as well as analytical testing on at least every fifth batch/lot to determine microbiological load, heavy metals, pesticides/herbicides (for ingredients that are not certified organic; US Department of Agriculture organic certification would be an acceptable alterna-tive test for pesticides and herbicides), solvents (used in extracts), and adulterants. Each ingredient or product must be tested according to an established risk-based testing program;
• Potency testing procedures to ensure that finished products meet label claims in place and in use;
• Demonstrated industry knowledge of common adul-terants and contaminants and sufficient testing to guarantee the absence of these adulterants and contaminants in finished products, (with suppliers of adulterated ingredients being disqualified); and
• Re-qualification for the program through a ques-tionnaire or onsite audit at least every three years.2
In addition to adhering to all Silver Partner qualifica-tions, Gold Partners must also demonstrate the following additional requirements:
• Analytical testing on each batch/lot of raw mate-rial or finished product for identity, potency (label claims), microbiological contaminants, as well as other analytical tests on ingredients at risk for certain impurities, such as residual solvents (for extracts and concentrates), pesticides (for non-organ-ically grown botanicals), melamine (for animal proteins), aflatoxin (for high-risk herbs and foods), and adulterants;
In 2014, with cGMP compliance having been a legal requirement for all dietary supplement companies since 2010, Emerson believed that being cGMP verified should no longer be a special distinction, but should be the standard.

68 • I S S U E 115 • 2017 • www.herbalgram.org
QUALITY CONTROL
• A real-time stability program to ensure that all finished products meet label claims for their entire shelf life;
• Products contain adequate active ingredients for clinical efficacy (as evaluated by the Emerson clini-cal team), and clinical trials are conducted when-ever possible; and
• Evidence of total quality, including research and product development, sustainable environmental practices, support of efficacy and safety with data from clinical trials when possible, and good busi-ness practices.2
The primary difference between the Gold and Silver Partner programs, according to Chasse, is that Gold Part-ners are required to have real-time stability programs, while Silver Partners may employ accelerated stability test-ing. “Real-time [means] measurement of product stability/potency/contaminants (like microbes), through the shelf life of the product,” Chasse wrote (email, July 17, 2017). She noted that because the FDA allows skip-lot testing as an acceptable practice (e.g., for heavy metals in herbs purchased from the same supplier), Silver Partners can test for contaminants in up to every third batch/lot. “But they have to have a rationale as to why this is low risk,” Chasse said. Gold Partners test each batch/lot by EQP standards.
An Ongoing Investment Providing testing for EQP brands requires Emerson
to make a significant investment to keep the EQP going and evolving, as the industry changes and advances — so much so, Chasse said, that Emerson is considering an application fee for the brands, which will cover some of the initial certification costs.
Emerson would also like to get more leverage from some of the testing data it collects and best practices it moni-tors, which could be of value in the broader industry, she noted. But because Emerson has a non-disclosure agree-ment (NDA) with every client, there are limits on infor-mation sharing.
Emerson would also like to share more information about the lab testing of products. Four times a year, Emer-son sends products from its warehouse shelves to inde-pendent labs to be tested for heavy metals or some other issue of current industry concern. For example, Emerson recently tested grapefruit (Citrus paradisi, Rutaceae) seed extract for benzalkonium chloride and related compounds, which are used in hand sanitizers and other household products and that have been reported as known adulter-ants of grapefruit seed extract.4 The ABC-AHP-NCNPR Botanical Adulterants Program (BAP) is a prime resource for Emerson Ecologics as it determines what adulterants to test for.
“Because we have NDAs with all our partners, the only action we can take if we see a failed result is to discon-tinue the product or brand,” Chasse explained. She added that Emerson is talking with potential partners, such as
the nonprofit American Botanical Council (ABC) and the ABC-AHP-NCNPR Botanical Adulterants Program, about how to get permission from EQP brands to anonymously publish or make use of such test results.
Looking ahead, Emerson hopes to continue to use the EQP to help drive improvements in supplement quality through testing methods, transparency, and sharing best practices. “The herbal identification world is rapidly chang-ing with many partners trying DNA testing,” Chasse said. “We have had a lot of brand audits in the last year [and] we are seeing brands explore new analytical methods, includ-ing DNA testing. DNA testing is not ready to be an EQP standard yet, but this is an area we are paying attention to.”
Emerson also wants to keep things relevant for its clini-cian customers. “Practitioners don’t necessarily want to do the research themselves or review the [certificates of analy-sis], but they do appreciate full transparency, which guides their trust,” Chasse said.
The EQP strives to stay on top of changes and advances in the industry, and Emerson thinks there is an opportunity to bring partners together in a communication forum to share best practices and innovative ideas. “Some companies are reluctant to share these things because it gives them an industry advantage,” Chasse said, “but for us, we also care about the practitioners and their patients, and this is where information sharing is so valuable.”
—Karen Raterman
References1. Yearsley C. NASC Preferred supplier program focuses
on quality standards in animal supplement industry. HerbalGram. 2017;113:62-69. Available at: http://cms.herbalgram.org/herbalgram/issue113/HG113-qc-nasc.html. Accessed July 12, 2017.
2. About the EQP. Emerson Ecologics website. Available at: www.emersonecologics.com/Quality/AboutTheEmerson-QualityProgram/. Accessed June 15, 2017.
3. EQP Partner Standards. Emerson Ecologics website. Avail-able at: www.emersonecologics.com/Quality/EmersonQuali-tyProgramPartnerStandards/. Accessed June 30, 2017.
4. Cardellina JH. The adulteration of commercial ‘grapefruit seed extract’ with synthetic antimicrobial and disinfectant compounds. HerbalGram. 2012;94:62-66. Available at: http://cms.herbalgram.org/herbalgram/issue94/QUALCON-TROL_gfse.html. Accessed July 10, 2017.
Organic & Sustainable
MountainRoseHerbs.com | 800.879.3337
herbs, essential oils, teas, spices & bulk ingredients

BOOK REVIEWS
70 • I S S U E 115 • 2017 • www.herbalgram.org
A Cree Healer and His Medicine Bundle: Revelations of Indigenous Wisdom by David Young, Robert Rogers, and Russell Willier. Berke-ley, CA: North Atlantic Books; 2015. Paperback, 223 pages. ISBN: 978-1-58394-903-0. $24.95.
This book describes Russell Willier’s journey to regain the traditional heal-ing knowledge of his Cree elders and to claim his rightful place as a contem-porary Cree medicine man. Willier’s herbal compendium most commonly uses 28 plants and, to a lesser degree, 33 others. Included are the Cree name, English common name, and scientific name for each plant. Most impor-tantly, whether Willier uses the plant alone or as part of a combination remedy also is included.
Co-author David Young, an anthro-pologist, and Willier first met in 1984 on a project that documented tradi-tional tanning methods. Willier and Young developed a friendship based on a deep respect for each other and, the next year, began a collaboration to document Willier’s Cree healing practices.
As a young boy, Willier collected plants on the Sucker Creek Reserve in northern Alberta, Canada, for older women to clean and for medicine men to use in their heal-ing practices. Medicinal plant collection taught Willier that the species of plants he needed to harvest grew in specific habitats. To help readers gather the correct plants, Willier’s medicine bundle information includes color photographs of the plants, the habitats where they grow, and maps of the collection locations.
Collecting diverse plant species from various locations over many years, Willier observed how overharvesting and the destruction of native habitats resulted in the loss of local healing plants. Willier’s deep conservation ethic is based on this very real loss and the higher spiritual practice of acknowledging plants as having a living spirit that must be honored. To supplement the knowledge of the plants used personally by Willier, each botanical is identified and further discussed by a third author, Robert Rogers, a clini-cal herbalist and widely published expert in the medicinal uses of plants.
As a young adult, Willier first resisted his calling to be a medicine man, but later began to study the medicine bundle he received from his great-grandfather, Moostoos, a well-known Cree medicine man. Willier consulted Cree elders to learn the identity and uses of the herbs in this bundle and explore those used by other healers.
Willier was always concerned with verifying that the treatments used were effective. If a patient had been treated by Cree healers, Willier would assess the patient’s need to be further treated by a physician and/or pharmaceuticals.
If the patient did later seek Western medicine, Willier would continue his search for a more effective medicine bundle. In his own healing work, Willier collaborated with Young and other researchers to evaluate Cree healing practices that were used to treat several patients with psoria-sis. The book includes before-and-after treatment photographs showing dramatic healing of skin lesions using Willier’s Cree practices.
Willier’s healing protocols include counseling, performing traditional ceremonies, such as purification by the use of a sweat lodge, and the use of herbs, animal parts, and minerals from his materia medica. Conditions treated include purely physical ones, such as wounds, plus mental condi-tions, and those from the spirit world that could include the removal of a curse placed on a person.
Willier’s stated primary purpose in writing this book is to preserve the traditional Cree healing knowledge that could easily be lost. The composition and use of medicine bundles and healing protocols is known by only a few elderly Cree medicine men. Some Cree tribal leaders believe the tradi-tional healing knowledge should only be passed on to other Cree to be successful. This protection of sacred knowledge for exclusive use by the tribe may prevent it from being misused or exploited, but risks its loss by limiting those who can be taught. Willier has found Cree youth are not interested in becoming medicine men (the book does not mention whether women can attain this title), and this increases the likelihood that the knowledge will be lost. Because of the tribe’s opposition to revealing what is consid-ered sacred knowledge, Willier has chosen to discuss the specific uses of only some plants and, for others, to simply disclose that the plant is used in a combination, with no information on the specific illness or use of the bundle.
This is the story of one man’s modern journey to be a traditional First Nations medicine man and to preserve that knowledge for future generations. What should be open knowledge and what is considered sacred, and therefore cannot be freely shared, is a core debate that emerges from the book.
—Edward M. Croom, Jr., PhDPresident, Croomia Botanical Scientific and
Regulatory ConsultingOxford, Mississippi

BOOK REVIEWS
www.herbalgram.org • 2017 • I S S U E 115 • 71
Botanical Medicine Manual by Marisa Marciano. Burnaby, British Columbia, Canada: ProHealth Systems; 2016. ISBN: 978-0-9936191-1-3. Spiralbound, 432 pages. $39.95.
This practical reference book, spiral-bound for easy use, is part of the consis-tently professional ProHealth Systems series of clinical reference books and a “ready reckoner” for the serious student.
Marisa Marciano, ND, bills herself as “the naturopathic herbalist” and has made botanical medicine a specialty of her clini-cal practice for the past five years. She was recently appointed chair of the Depart-ment of Botanical Medicine at the Boucher Institute of Naturopathic Medicine in New Westminster, British Columbia, Canada. She brings this practical experience of teach-ing and using herbs in clinical practice into every page of this handy reference book.
Written with the naturopathic student in mind, this helpful primer includes introductory chapters on how to study and learn about the many herbs required for profes-sional exams; how to harvest, dry, and store herbs (I love that a reference to harvesting by moon phases is included); how to assess and critique herbal research; the practice of evidence-based medicine; what questions to ask when taking a patient’s case history; how to keep clinical case notes; meta-bolic and nutritional needs of the body; herbal actions; key plant constituents and their clinical applications; basics of herbal medicine making — whew, and that is only the first 83 pages!
This is a whirlwind account of the highlights of herbal medicine, but the writing is elegant and precise, the colum-nar layout allows for more text per page, and the first part of the book covers a surprising amount of ground quite compre-hensively in relatively few pages.
The next 280 or so pages are dedicated to an alphabeti-cal series of mini-monographs on the key 150 herbs required for the Naturopathic Physicians Licensing Examinations (NPLEX). This includes such standard-practice herbs as yarrow (Achillea millefolium, Asteraceae), calendula (Calen-dula officinalis, Asteraceae), lemon balm (Melissa officinale, Lamiaceae), comfrey (Symphytum officinale, Boraginaceae), and dandelion (Taraxacum officinale, Asteraceae). However, the adherence to NPLEX requirements means the book also provides monographs on melilot (Melilotus officinalis, Fabaceae), rauwolfia (Rauvolfia serpentina, Apocynaceae), cannabis (Cannabis spp., Cannabaceae), belladonna (Atropa belladonna, Solanaceae), and aconite (Aconitum napellus, Ranunculaceae) — herbs that are hardly standard for most herbalists and suitable for use by only qualified herbal or naturopathic professionals. Maybe at least separating these herbs into a separate section would have highlighted their potential dangers more effectively. Given that people who are not well-trained in botanical medicine may use this book, it
is prudent to proactively point out the poten-tial harm that can result if these herbs are misused.
Each monograph lists the Latin binomial, common name, botanical family, plant parts used, key active constituents, actions, key clinical applications, pharmacology, pharmacy, interactions, dosing, and safety. References are provided in each mono-graph. The material is concise and factual, and the essential parts are pared down for easier memorization, with occasional boxes that provide a little more insight (e.g., how the herb is classified in traditional Chinese medicine, or how it got its name). If I were still a student, this is exactly what I would want: just the facts, no frills; all the essen-tial information presented in a simple and consistent manner, referenced and reliable,
nothing extraneous. Each monograph also includes a line drawing and, in a
very nice touch, the reader is encouraged to color them as a way to learn the herbs. As an educator myself, I can say that this is an excellent and simple way to engage the learner and give visual cues for better recall.
At the back is a useful Latin/common name cross refer-ence, an excellent summary of toxicity signs and symptoms, and potential adverse effects. There is also a good discussion of risks from using herbs, cautions and contraindications, a list of herbs to avoid in pregnancy, guidelines for pediatric dosing, a classification of the monographed herbs by botani-cal family, a summary table of drug-nutrient interactions, and a detailed listing of known herb-drug interactions. This is all useful, well-considered, and practical information, and one of the things that makes this book different from other books that provide monographs on herbs. Marciano’s clini-cal experience with herbs is evident from how she discusses dosing and safety. She is pragmatic and precautionary with-out being alarmist.
The last part of the book lists commonly used conven-tional pharmaceutical drugs. This section serves as a quick reference guide, but is so abbreviated as to be fairly point-less. Most students or practitioners will have much better reference materials for drug uses or can look them up online. This section of the book seems unnecessary.
Overall, this is a practical reference book, reliable and accurate, for use in clinical practice. For those looking for gorgeous pictures of flowers or quirky recipes for cough syrups, this is not the book to choose. However, for those looking for specific herbal doses or constituents, or to confirm the safety of an herb with a conventional drug, this book will serve as a useful desk reference.
—Chanchal Cabrera, MSc, FNIMH, RH (AHG)Medical Herbalist, Horticulture Therapist
Courtenay, British Columbia, Canada

BOOK REVIEWS
72 • I S S U E 115 • 2017 • www.herbalgram.org
Roots of Our Renewal: Ethnobotany and Cherokee Environmental Governance by Clint Carroll. Minneapolis, MN: Univer-sity of Minnesota Press; 2015. Paperback, 251 pages. ISBN: 978-0-8166-9090-9. $25.00.
Clint Carroll’s goals for Roots of Our Renewal are threefold. The book tells the story of how the Cherokee in Okla-homa have developed material, spiritual, and political relationships with their new lands; it examines resource-based versus relationship-based approaches to indige-nous governance; and it discusses the inter-action between Native American studies and political ecology. Challenging goals at that level of complexity do not make for light reading. However, as Circe Sturm, the book’s reviewer writes: “This book is perfect for the class-room and for anyone interested in political ecology as it relates to indigenous struggles for self-determination.”
The book contains five chapters. The “Notes” section, which is at the end of the book before the comprehen-sive bibliography and index, includes explanations and comments for each chapter. The book begins with a “Note to the Reader” and a preface that gives readers a context to Roots of Our Renewal. This book is an expansion of Carroll’s doctoral studies, and it reflects both his commitment to the development of a strong Cherokee Nation and the policies, practices, and structures that ensure accountability for that community.
In the introduction, Carroll introduces the Cherokee elders who play a major role throughout his book. He worked with this group while conducting ethnobotanical research for the Cherokee Nation Natural Resources Department from 2004 to 2013. The goals of his research and the premise of this book are discussed in this section, which also provides helpful definitions and an introduction to the Cherokee, indigenous concerns, and ecological and governance theo-ries and practices. The rest of the book weaves these themes together and combines history, theory, and research.
A member of the Cherokee Nation himself, Carroll provides a broad overview of Cherokee pre-colonial history in Chapter 1. This chapter also sets out a number of impor-tant myths, discusses the pressures created by settler-colonial forces, and describes the impact of removal on his nation. Particularly insightful and moving is his account of the Cherokee Trail of Tears, a dark chapter in American history but, sadly, not a unique colonial treatment of indigenous peoples.
An important theme of the book, introduced in Chapter 2, is the dissolution over time of the original structure of the Cherokee Nation. Once a community of independent towns linked by trade and culture, surrounded by tilled fields and healthy fishing, hunting, and gathering territories, the Cher-okee Nation was broken and reassembled by outside forces into smaller landscapes in a few generations.
In Chapter 3, Carroll documents the devastating impact on the Cherokee community of loss of their current home-land through land grabs and environmen-tal degradation, and of restrictions on fish-ing, hunting, and gathering due to federal and state policies on allotments, fenc-ing, fire suppression, tourism, and water management. Under the pressure of these challenges, the Cherokee Nation developed a governance structure that is uniquely their own, a rejection of federal and state jurisdictions, and a powerful reassertion of political autonomy.
The collection, recording, and applica-tion of traditional knowledge, and its shar-ing within the community and with the
outside world, raises a wide range of ethical and cultural dilemmas. In Chapter 4, Carroll describes his experience conducting research in his own commu-nity, and how he developed relationships so that he could gather and document the knowledge he sought. From the outset, the elders and the Cherokee community were aware of the need for cultural revitalization, but they were also mindful of cultural appropriation, ownership of knowledge or intellectual property, and the safety of knowledge transmission. These issues are of critical inter-est to researchers in any field seeking to consult with indigenous communities, and Carroll’s observations are both insightful and useful.
Carroll’s final chapter, aptly titled “The Spirit of the Land: Terrains of Cherokee Governance,” examines the link between the Cherokee view of and relation-ship to the land, the concept and structures of environ-mental governance, and the relationships between the tribal bureaucracy and the people, specifically the rural community members. The elders believe that maintain-ing and sustaining their knowledge and practices honors the spirit of the land; that vision can find itself at odds with “modern” governance structures, Western science, and contemporary legislation and regulation. Carroll deftly uses the elders group and the dilemma of “gath-ering” rights and regulations to explain and argue for open communication and building trust as key elements of effective, appropriate, and sustainable environmental governance.
In his conclusion, Carroll summarizes and reaffirms his argument for self-determination based on a relationship approach to governance, citing the writings and insights of many noteworthy American and Canadian indigenous authors on community development and self-government. At the time of this book’s publication, Cherokee resource management was still driven by an economic, resource-based approach. Nevertheless, Carroll is optimistic about the elders group’s continued inf luence on tribal decision-making, and the eventual adoption of a more community-focused model.

BOOK REVIEWS
www.herbalgram.org • 2017 • I S S U E 115 • 73
Roots of Our Renewal: Ethnobotany and Cherokee Envi-ronmental Governance may not be an easy read for those unfamiliar with the fundamentals of ecology or indigenous studies. However, Carroll’s personal experiences during his nine-year research effort and the stories of the develop-ment of the elders group make this book more appealing than other reference books. Carroll argues persuasively for a relationship-based approach to indigenous environmen-tal governance, and this thorough review of the 300-year
Cherokee governance process is a compelling and worth-while addition to an important and timely discussion. I recommend this book to anyone interested in sustaining traditional knowledge and practices.
—Valerie Assinewe, PhDConsultant, NVision Insight Group Inc.
Ottawa, Ontario, Canada
Cannabis: A Complete Guide by Ernest Small. Boca Raton, FL: CRC Press; 2017. Hardcover, 567 pages. ISBN: 9781498761635. $119.95.
Cannabis (Cannabis spp., Cannabaceae) possesses considerable utility that extends far beyond its notoriety as an intoxicant. As a source of food, fiber, oil, and medicine, cannabis is a truly multipurpose plant. With scientific and clinical research considerably expanding our knowledge of this plant over the last few decades, an accessible survey of cannabis seems a necessity.
This book provides a comprehensive over-view of cannabis and covers, in great detail, nearly every aspect of cannabis, including its applications and role in society. The author, Ernest Small, PhD, is a highly respected and widely published plant scientist with decades of experience studying and publishing about cannabis in his role as a senior scientist in the Research Branch of Agriculture and Agri-Food Canada. His writing in this work is clear, evocative, and witty, and is accompanied by a profusion of photographs and illustrations, with even the occasional cartoon.
The introductory section of this book begins with a discus-sion of the controversy that has swirled around cannabis for centuries and transitions to the recent “resurrection” of canna-bis as a medicine and an increasingly accepted social intoxi-cant. Subsequent chapters explore cannabis history, ecology, and botany, with excellent visual references to assist the reader. The book then turns towards the wide ranges of uses for the plant’s fiber (e.g., for cloth and paper production) and its oil’s nutritional value. Particular attention is given to the condi-tions required to produce cannabis crops that yield high-value fiber and oil.
This volume may be among the first books to delve into the uses for cannabis essential oils and terpenes, a topic of recent interest because of their potential to reduce adverse effects asso-ciated with the medicinal use and recreational use of cannabis cultivars that contain significant amounts of tetrahydrocan-nabinol (THC). This section provides a launch pad for the book’s current overview of cannabis chemistry.
HerbalGram readers will likely find the central 200 pages of this book, which includes an in-depth survey of cannabis as a medicine and intoxicant, to be of considerable interest. With vigor and humor, the author busts many countercul-
ture myths about cannabis, and his insights into cannabis cultivation for medicinal content are valuable and well-informed. The section that covers the theory and practice of using medical cannabis for conditions ranging from cancer to brain injury reflects an up-to-date scientific understanding, and it is delivered with appropriate rigor and proper skepticism, since some popular claims of efficacy are based solely on preclinical or observational data. This portion of the book ends with a discussion of the challenges inherent in the production of drug cannabis varieties and is filled with sage and practical guidance that is supported by evidence collected in the field. The author even
weighs in on the likely trajectory of legalization/decriminaliza-tion efforts and potential future outlets for recreational canna-bis products, going as far as to anticipate “pot restaurants.” While some may dismiss such speculation as frivolous, the arguments that support it appear solid.
The final chapters cover topics from the environmental sustainability of cannabis production to the current state of cannabis germplasm resources, before wading into the highly contentious realm of Cannabis botanical classification and nomenclature — the sativa vs. indica debate. For more than half a century, scientists have argued about the taxonomy and nomenclature of Cannabis. Small has been a key figure in this debate, and his arguments are forceful, well-reasoned, and surprisingly entertaining. His conclusions about classification may not convert all his rivals, but will continue to garner their respect.
The greatest challenge in writing a survey of the science and culture of cannabis is the sheer volume of material that must be distilled. The author’s deep appreciation for the topic is evident, and his distillation is expert and passionate. This book will appeal to a professional audience seeking authorita-tive guidance about Cannabis, and is written from a perspective that can be gained only from an author of Small’s eminence and experience. He also manages to make this tour of his subject fun, which is quite laudable, indeed.
—Michael BackesAuthor, Cannabis Pharmacy
Principal, Blackbridge Consulting Group LLCLos Angeles, California

IN MEMORIAM
74 • I S S U E 115 • 2017 • www.herbalgram.org
Iconic and widely respected Chinese medicinal herb pioneer Bill Brevoort died at his home in Kona, Hawaii, on July 28, 2017, at the age of 75. He had been recently diagnosed with metastatic mela-noma.
Bill was a truly remarkable man — intelligent, intrepid, focused, and highly spiritual. An inveterate concocter of Chinese tonic formulations, he was still making customized botanical extracts until a month before his death.
William Harry Brevoort was born in Van Nuys, California, on March 24, 1942. He attended the University of Connecti-cut and then Columbia University, where he earned a master’s of fine arts degree in painting and sculpture in 1967. He and his wife, Peggy, then moved to Oregon, where he was a lecturer in the fine arts department at the University of Oregon from 1967 to 1969.
During this time, Brevoort became intensely interested in Chinese culture, and studied Chinese Buddhism and traditional Chinese medicine (TCM). He was a long-time disciple of Vener-able Master Hsuan Hua of the City of Ten Thousand Buddhas in Ukiah, California.
In 1971, Bill and Peggy founded East Earth Herb, which is considered to be the first company in the United States to educate the natural food community about the healing and vitality-empowering properties of traditional Chinese herbs.
The East Earth Herb booth was a popular location at many natural food trade shows and alternative medicine conferences in the 1970s, 80s, and 90s, where Brevoort would often listen to a person’s pulse, look at their tongue, and perk them up with one of his special blends of Chinese herbal tonic elixirs, teas, and other creatively blended formulations. East Earth Herb’s “Dragon Eggs” line of Chinese herbs was most likely the first American-made line of Chinese herbal formulas.
The Brevoorts are also largely credited with creating the initial interest in the Pacific herb kava (Piper methysticum, Piperaceae) with their popular after-conference kava parties in the 1990s.
A practicing Buddhist most of his adult life, Brevoort was an intensely spiritual person, with a wide range of interests to try to satisfy his strong intellect. Among his many hobbies, he was a dedicated organic gardener and an avid amateur astronomer. He took over the small observatory on the Kona coast that had belonged to the late author Terence McKenna, and spent countless
hours peering into the magnified depths of space. He was equally comfortable in frequent deep meditation as he was contemplating the exploration of outer space.
I knew Bill for 43 years. He was a truly amazing, bril-liant, spiritual, one-of-a kind person. He and Peggy are pioneers of the US herb movement, particularly with respect to Chinese herbs. They imported and distributed Chinese herbal patent medicines in the early 1970s and later distributed their own Chinese herbal dietary supple-ments. They were one of my first suppliers when I owned Sweethardt Herbs (1974-1986), my former herb wholesal-ing company in Austin, Texas.
When I first started ordering from them, they lived in Reedsport, Oregon, and I had to call them on a ship-to-shore radiophone line to order Chinese Ginseng Bee Secre-tion (which Bill probably received by “submarine” from Vancouver; the US Food and Drug Administration was not letting such products into the United States in those days, except for sale in ethnic Chinese stores in San Fran-cisco and a few other cities.) In addition to introducing me to many Chinese herbs and kava, Bill was also the first to introduce me to the fabled Chinese pu-erh tea (Camellia sinensis, Theaceae).
Numerous long-time friends and colleagues provided the following thoughts and reminiscences about Bill:
Lynda LeMole, an herb industry activist previously with Traditional Medicinals tea company (email, July 31, 2017):
BuddhaBrother, TonicMaster, StarGazer, VeggieGar-dener, WisdomGiver. How many of us sought his heal-
William ‘Bill’ Brevoort1942-2017
Bill Brevoort with one of the first plantings of fo-ti (Reynoutria multiflora syn. Polygonum multiflorum) in the United States. Photo ©2017 Steven Foster
IN MEMORIAM
www.herbalgram.org • 2017 • I S S U E 115 • 75
ing help at trade shows: “I’m taking your pulse. Stick out your tongue. Drink this tonic.”
Josef Brinckmann, noted medicinal plant sustainability authority, who was, at one time, an employee of East Earth Herb and now, for many years, at Traditional Medicinals (email, July 29, 2017):
One of my teachers, I learned so much from Bill in the three years that I worked and traveled with him (1995-1997) — not only about the traditional uses of almost everything in nature codified in the Chinese systems of medicine (of animal, botanical, fungal, metal, and mineral origin), but also about the past, present, and future of Buddhist practice. I was very fortunate to walk, for a time, with this truly remarkable man.
Drake Sadler, co-founder of Traditional Medicinals (email, July 29, 2017):
Like Josef, I, too, was fortunate to walk for a time with Wild Bill. On an AHPA [American Herbal Products Association] visit to the capitol many years ago, midway through a boring meeting with the usual government reps, Bill and I concluded [that] our lovely (and much more diplomatic) wives were better suited to the task, and [that] our time could be better spent exploring the US National Arboretum. The gardens were impressive, and Bill was most interested in the collection of Asian shrubs and trees. His breadth of knowledge was as expansive as the miles of park pathways and hundreds of landscaped acres.
Morris Shriftman, natural products industry marketing consultant (email, July 29, 2017):
I worked my way to his booth several times at each show. His knowledge of Chinese herbs and oriental tonics was a revelation to me. And I remember my delight in using his products. There was one in particular: I think it was called Dragon’s Brew; it was deep and dark and mysterious. It tasted of ginseng and ginger, and who knows what else? And I had a ride.
Rick Levine, syndicated astrologer and poet (email, July 31, 2017):
Bill Brevoort was a rare human being: pioneering in his work, conscious in his behavior, honest in his interactions, dedi-cated in his spiritual practice, unyielding in his search for truth, and loyal to his family and friends.
Kathi Keville, author and herbalist (email, July 31, 2017):
Bill was an expert connoisseur and collec-tor of fine Chinese tea. A visit always meant having afternoon tea — an experi-ence in itself. He also loved good music, photography, astronomy, and spent much
of his time at his own small telescope observatory in Hawaii that offered an amazing view of the sky.
Terry Wittenberg, avid bicyclist and former Whole Foods Market veteran (email, July 29, 2017):
My favorite memory of Bill and Black Belt [a type of Chinese tonic herbal “fruit leather”]: In the summer of 1989, [some friends and I] took a three-week vacation for some bike racing. From home (Texas), we first drove to upstate New York for a 24-hour race and afterwards stayed in the area for almost a week. Next race was in St. Louis for the 540-mile Race Across Missouri. On our way to St. Louis, we stopped overnight in Indianap-olis. When we were unpacking at the motel, I left our small trailer open and our box of supplements and herbs (including my supply of Black Belt) was stolen. I called Bill and he mailed more Black Belt to the hotel in St. Louis in time for the race. Bill saved the day.
Frank Lampe, vice president of community & industry relations at the United Natural Products Alliance (UNPA) (email, August 3, 2017):
“Hold out your tongue.” I’ll never forget those words as I was directed by colleagues to visit the East Earth Herb booth at Natural Products Expo West in 1989. The man with the constantly active, piercing blues eyes and flow-ing, graying beard behind the counter could easily have played a starring role in The Lord of the Rings or Harry Potter adventures. It was Bill Brevoort, getting ready to dispense a thick herbal concoction from a number of large plastic bottles that he said would balance my ener-gies. That encounter started a new chapter in my own life: the beginning of a long, intellectual and engaging relationship with an herbal and TCM legend, and yet another irrefutable case for the healing power of plants. In addition to being the best formulator I’ve ever met,
Bill BrevoortPhoto ©2017 Steven Foster

IN MEMORIAM
76 • I S S U E 115 • 2017 • www.herbalgram.org
which resulted in products that got your attention while they worked their magic, Bill’s areas of interest were wide; he could be confrontational as he challenged your thinking on any number of issues, those probing eyes peering out from underneath a deeply furrowed brow, but it was always in the spirit of pursuing intellectual growth, a deeper understanding of the chosen topic and the bigger picture—and usually with an accompanying impish grin and clear merriment in those eyes. Always inquisitive, always questioning, always seeking, always engaged.
And, finally, natural products industry leader Loren Israelsen, president of the UNPA, wrote that he, like many others, accepted the sad news of Bill’s passing “with a deep sense of loss but knowing Bill had prepared for the day of passing like few can” (email, July 31, 2017). Israelsen also wrote in an August 3, 2017 communication to UNPA members:
Bill Brevoort was unlike anyone I have known. He was a scholar of TCM, a master formulator — a wizard, actually — whose drops and tinctures carry true heal-ing power. He lived as a monk, sitting in meditation for many hours a day, with his mind in states of conscious-ness that few have experienced. He tended his garden, listened to classical music, talked politics, cooking ideas
and recipes and refused to wear shoes — shirt optional. He lived just north of Kona, Hawaii, with a panoramic view of the Pacific Ocean with whale spouts often in sight. The last time Bill and I were together, he gave me a bottle of his special cordyceps extract — a treasure then and more so now. His death came unexpectedly, and I have still not come to terms with this news. But I am sure he is filled with wonder and gratitude to be reunited with his masters and teachers. The long medi-tation sessions are, no doubt, already in progress. Peggy, his dear wife and materfamilias to many, will keep his memory alive as will all those who continue to hold the teachings and generosity of Bill as a living record of his remarkable life.
Bill Brevoort is survived by his wife Peggy, his daugh-ter Gretchen, son Joshua, and grandson Jacob Dickey. His extensive herbal library of Chinese medicinal classic texts and related literature, along with his unique collection of Chinese teas, herbs, and extracts are being donated to the City of Ten Thousand Buddhas in Ukiah. A service for placing his ashes will be held at the City of Ten Thousand Buddhas later this year.
—Mark Blumenthal
Specializing in medicinal and aromatic plants, along with the places they grow,
our stock photo fi les include more than 120,000 images shot around the world for over 30 years.
Visit our website: www.stevenfoster.com
Stock Photography that doesn’t look like Stock
Contact us at our NEW location in the heart of the Ozarks in Eureka Springs, ArkansasPhotography, Consulting, Publications
Steven Foster Group, Inc. • Steven Foster, President • P.O. Box 191 • Eureka Springs, AR 72632 Phone: 479-253-2629 • Fax: 479-253-2693 • email: [email protected] Foster Group, Inc. • Steven Foster, President • P.O. Box 191 • Eureka Springs, AR 72632 Phone: 479-253-2629 • Fax: 479-253-2693 • email: [email protected]
IN MEMORIAM
www.herbalgram.org • 2017 • I S S U E 115 • 77
Noted pharmacognosist Johann Jurenitsch, PhD, of the University of Vienna, Austria, passed away on April 16, 2017, at the age of 70. While he was well-known within the world of pharmacognosy, not many in the natural foods or herbal medi-cine communities in North America knew Jurenitsch. He was a professor of pharmacognosy and the vice-chancellor of the Univer-sity of Vienna from 2000 to 2011. Jurenitsch was also a holder of the Silver Decoration of Honor for Services to the Republic of Austria (Ehrenzeichen für Verdienste um die Republik Österreich). This is the most important award granted by the government of Austria in recogni-tion of people whose works in the fields of policy, economy, culture, intellect, or honorary service have contributed to the betterment of the nation.
After studying pharmacy at the University of Vienna, Jurenitsch received a doctorate of philosophy in 1976, and habilitated in 1983 in the subject “Pharmakognosie.” He continuously worked in the Department of Pharmacognosy at the University of Vienna and was appointed univer-sity professor there in 1991. Together with his colleagues, Jurenitsch mentored 120 graduate students and 25 doctoral students, and was involved in numerous international research projects that encompassed a wide range of research and teaching activities. Among Jurenitsch’s early works are a review of the safety of calamus (Acorus calamus, Acora-ceae), a number of scientific publications on cayenne pepper (Capsicum spp., Solanaceae) including its adulteration, numerous papers on the taxonomy and chemistry of Achil-lea (Asteraceae) species, and post-mortem screening for the detection of poisons in tissue and blood.
Johann Jurenitsch1947-2017
I came to know Jurenitsch serendipitously. In the early years of the formation of the American Herbal Pharmacopoeia (AHP), I belonged to a medicinal plant discussion group. As part of AHP’s mission to rekindle interest in classical botanical pharma-cognosy, I was referred to Jurenitsch by one of his students who was practicing pharmacognosy in Costa Rica. I reached out, explaining that the United States did not have the pharmacognosy expertise in the same way that Europe did and pleaded for help. The response from Jurenitsch was immediate, positive, and definitive: “Let me know what I can do to help and if I can, I will.” He remained true to his word for
more than 20 years.Jurenitsch and another colleague and friend from Vienna,
Wolfgang Kubelka, PhD, graciously invited me to present the work of AHP to the pharmacognosy department at the University of Vienna. Many of the researchers there have worked on AHP monographs over the decades, including expert microscopist Reinhard Laenger, who worked tire-lessly for years generating microscopic descriptions, illustra-tions, and images for AHP’s Microscopic Characterizations of Botanical Medicines, and most of the microscopic character-izations in AHP monographs.
The Department of Pharmacognosy at the University of Vienna has for decades focused attention on research-ing the botanical yarrow (Achillea millefolium) from all perspectives: botany, pharmacognosy, chemistry, and phar-macology. As a fitting tribute to the department and to Jurenitsch, and in return for the generosity and kindness he showed AHP, the soon-to-be released yarrow monograph will be respectfully dedicated in his name.
—Roy Upton President, American Herbal Pharmacopoeia
Scotts Valley, California
Herbal News & Events! Weekly eNewsletter from ABC
Keeping you up to date on upcoming conferences, symposia, webinars, and other herbal community events.Also includes a weekly roundup of media articles of interest. And more!
ABC members automatically receive the premium version of Herbal News & Events each week, so join today at www.herbalgram.org/join.
A free version is also available when you register at www.herbalgram.org.

IN MEMORIAM
78 • I S S U E 115 • 2017 • www.herbalgram.org
After a brief but valiant battle with cancer, Joel Taller, a pioneer of the Canadian natural product and food industry and perhaps the preeminent regulatory lawyer in Canada, passed away on May 13, 2017. A member of the Gowling WLG law firm team for 34 years, Taller worked exclu-sively in the area of product regulation. He received his law degree and MBA from the University of Ottawa, and a BSc (Honours) in physiology and pharmacology from the University of Western Ontario. In 1983, Taller’s career started as an articling student. He was called to the bar in 1985 and became a partner in 1991.
Along the way, Taller not only managed a strong regu-latory practice that specialized in natural health products, foods, drugs, cosmetics and medical devices, but he also nurtured the careers of many younger lawyers and profes-sionals. He started what became, and continues to be, the most significant food, beverage, and supplement legal practice in Canada. Advising on regulatory matters rang-ing from pre-market reviews and labeling issues to recall and good manufacturing practices, the practice grew from a single partner to a full multi-disciplinary team with an international reach.
During his career, Taller worked with numerous compa-nies and associations within the food, beverage, and supple-ments industries in Canada. He served as counsel to the Canadian Health Food Association (CHFA) for many years and was an integral part of the strategy and progress
that CHFA achieved over the years. Taller’s expertise and guidance as well as his breadth of knowledge, were invalu-able to the staff, board of directors, and members of CHFA for many years. His wisdom and logical approach will be missed.
For more than 20 years, Taller also acted as a registered lobbyist and worked to protect the industry on diverse files including bills C-51, C-52, and C-6, all of which proposed changes to the Canadian regulatory framework that suggested excessive regulation and threatened the avail-ability of natural health products (NHPs) in Canada. He also worked on the initial cost recovery file, finished prod-uct testing, the NHP regulations, and Unprocessed Product License Applications Regulations (UPLAR). He was known and respected by many within Health Canada and by those throughout the directorates who had the opportunity to work with him over the years. He also worked with the non-profit American Botanical Council, writing articles and sharing his knowledge of the Canadian regulatory system across the border.
As well as being a highly accomplished lawyer, Taller was a wonderful person. He was kind and generous to a fault; someone who gave not only his money, but more impor-tantly his time, to support others and to help those in need. And he did it quietly, with no desire for recognition or public praise. Stories abound of Taller’s support of groups in need. He donated rooms and funds for students who wanted to learn, and he was willing to help those who were going through a hard time.
Taller was also a man of faith and acted as an advisor at his synagogue. He continued to learn throughout his life and enjoyed a deep discussion or a debate. He lived by what he believed and demonstrated his beliefs so that others could benefit from his example. Finally, and most impor-tantly, Taller was a husband, father, and grandfather. He loved his family and enjoyed every moment he spent with them.
Those who knew Taller have described him as a mensch, a Yiddish word that means “a person of integrity and honor; a person who takes responsibility.” As a man who truly lived by his values and was kind to a fault, we should all aspire to be a bit more like Joel Taller. In recognition of his efforts and work on behalf of the natural health industry in Canada, CHFA will induct Taller into the CHFA Hall of Fame in September 2017.
—Helen LongPresident, Canadian Health Food Association
Toronto, Ontario, Canada
Joel Taller1956 – 2017

American Herb Association Quarterly Newsletter: $20/yr. AHA, P.O. Box 1673, Nevada City, CA 96969.Australian Journal of Herbal Medicine: Quarterly publication of the National Herbalists Association of Australia (founded in 1920). Deals with all aspects of Medical Herbalism, including latest medicinal plant research findings. Regular features include Australian medicinal plants, conferences, conference reports, book reviews, rare books, case studies, and medicinal plant reviews. AUD/$96 plus AUD/$15 if required by airmail. National Herbalists Association of Australia, P.O. Box 696, Ashfield, NSW 1800, Australia.Medical Herbalism: Subtitled “A Clinical Newsletter for the Herbal Practitioner.” Edited by Paul Bergner. $36/yr, $60/2 yrs. Canada $39/yr. Overseas $45/yr. Sample/$6. Medical Herbalism, P.O. Box 20512, Boul-der, CO 81308. American College of Healthcare Sciences: ACHS.edu is a DEAC accredited, fully online college offer-ing Graduate and Undergraduate degrees, diplomas, and career-training certificates in holistic health and herbal medicine. ACHS is committed to exceptional online education and is recognized as an indus-try leader in holistic health education worldwide. Federal financial aid available to those who qualify. Educational resources available to the public include: ACHS Health and Wellness Blog, Master Lecture Webinar Series, and eBooks. For more information: visit www.achs.edu, call (800) 487-8839, or stop by the College campus located at 5005 SW Macadam Avenue, Portland OR 97239.
Interns, get hands-on experience before you graduate! If you’re a future pharmacist or dietitian, you can choose a rotation through ABC’s internship program. You’ll get a comprehensive introduction to phytomedicines, researching the medicinal, culinary, and cosmetic uses of herbs, answering ABC members’ questions, working with medicinal plants in ABC’s 2.5 acres of herbal gardens, and preparing herbal salves, tinctures, or meals. For more information, call 512-926-4900 x114 or email [email protected]/Berry/Vegie farm seeking assistance with cultivation, processing, landscaping, web work, and GMP certifi-cation. Agri-Tourism startup. Work not hard but steady. Profit Sharing. Starting immediately in the Virginia Blue Ridge, Zone 7. [email protected] Photography that doesn’t look like Stock: Steven Foster Group, Inc. Photography, Consulting, Publica-tions. Specializing in medicinal and aromatic plants, along with the places they grow, our stock photo files include more than 120,000 images shot around the world for over 30 years. Contact us at our location in the heart of the Ozarks in Eureka Springs, Arkansas. Visit our website: www.Stevenfoster.com or email: [email protected] supplying herbal products in Europe? Ann Godsell Regulatory can offer consulting advice on regulatory strategy, and data requirements. Services for dossier preparation & submission also available. For more information email [email protected] Business Development: 60 years combined experience supporting new and existing tea ventures from start-ups to Fortune 500 companies. Original recipes, flavor and functionality enhancements, raw materials sourcing, production trouble-shooting, regulatory, scientific substantiation, and more. Former Whole Foods and Celes-tial Seasonings blend-masters, R&D / Q.C. Tea Bags, loose teas, RTD. Advisory services for wholesale, branded consumer products, and retail operations. Email us with your information and needs: [email protected] YewTip™ products, the natural Taxane source, Pacific Yew (Taxus brevifolia). Sustainably wildcrafted and manufactured exclusively by Bighorn Botanicals, Inc., Noxon, Montana. Capsules, tea, powder, tincture, oil, salve, lotion, soap, and lip balm. To review our products, go to www.bighornbotanicals.com. For more infor-mation, including ethnobotany, sustainable harvest protocols, safety, and biological activities, click on the “Plant Profile.” Order online or call toll-free 1-888-847-1223.
Publications
www.herbalgram.org • 2017 • I S S U E 115 • 79
Other
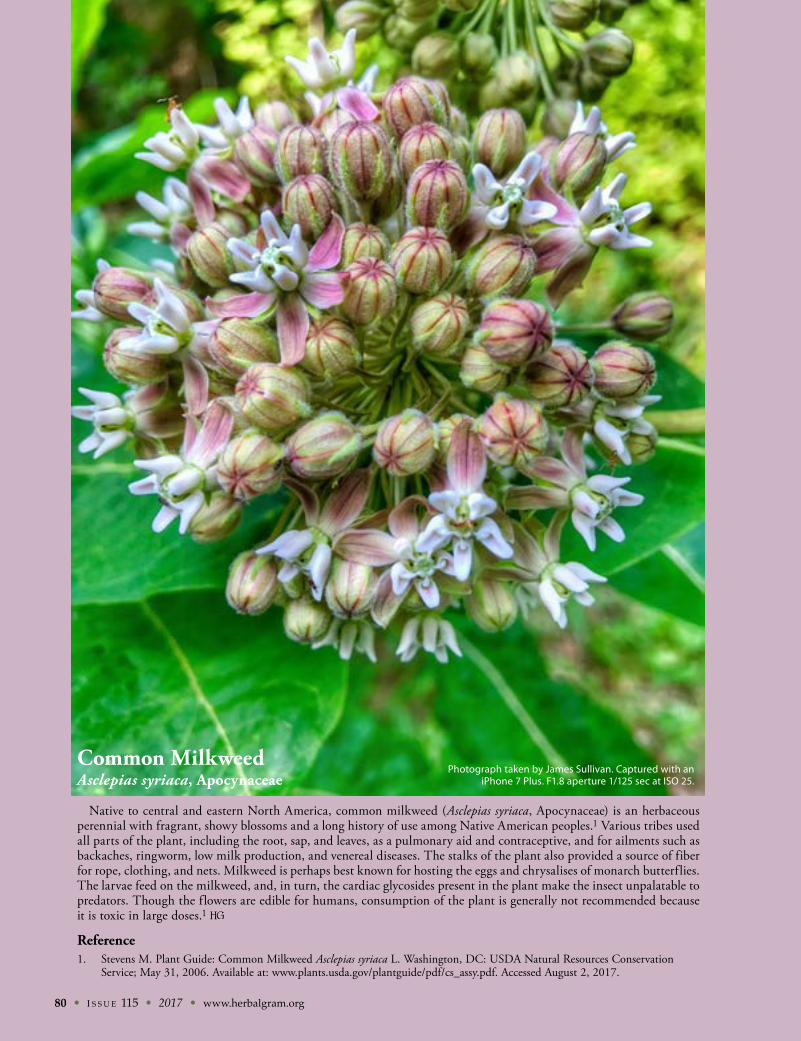
80 • I S S U E 115 • 2017 • www.herbalgram.org
Common MilkweedAsclepias syriaca, Apocynaceae
Native to central and eastern North America, common milkweed (Asclepias syriaca, Apocynaceae) is an herbaceous perennial with fragrant, showy blossoms and a long history of use among Native American peoples.1 Various tribes used all parts of the plant, including the root, sap, and leaves, as a pulmonary aid and contraceptive, and for ailments such as backaches, ringworm, low milk production, and venereal diseases. The stalks of the plant also provided a source of fiber for rope, clothing, and nets. Milkweed is perhaps best known for hosting the eggs and chrysalises of monarch butterflies. The larvae feed on the milkweed, and, in turn, the cardiac glycosides present in the plant make the insect unpalatable to predators. Though the flowers are edible for humans, consumption of the plant is generally not recommended because it is toxic in large doses.1
Reference1. Stevens M. Plant Guide: Common Milkweed Asclepias syriaca L. Washington, DC: USDA Natural Resources Conservation
Service; May 31, 2006. Available at: www.plants.usda.gov/plantguide/pdf/cs_assy.pdf. Accessed August 2, 2017.
Photograph taken by James Sullivan. Captured with an iPhone 7 Plus. F1.8 aperture 1/125 sec at ISO 25.
Founded in 1988, the member-supported American Botanical Council:SERVES members in more than 81 countries worldwideEDUCATES consumers, healthcare professionals, researchers, educators, industry and the media on the safe and effective use of medicinal plantsADVOCATES responsible herbal production and useADVISES the media on emerging herbal sciencePROMOTES a healthier world through responsible herbal use.
Join Us! In return, you’ll receive access to a wealth of herbal data via:
ABC’s acclaimed quarterly journal, HerbalGram8 online databases of herbal information (depending on membership level)Regular electronic updates on herbal news that matters to you
• 12 Monthly HerbalEGrams, 51 Weekly Herbal News & Events updates, and 360 HerbClips per year, plus other Member Advisories
And much more.
Join UsThe
Invites You To
Individuals, organizations, and companies support ABC through membership
or contact Denise Meikel at [email protected] or (512) 926-4900 ext. 120.
Learn more atwww.herbalgram.org
The American Botanical Council is the leading nonprofit education and research organization using science-based and traditional information to promote the responsible use of herbal medicine.
Curcumin, endowed with powerfulantioxidant activity, has been shown to
support joint mobility and eye health.Unfortunately, the bioavailability
of the natural form is low.Which is why Indena developed
Meriva®, a curcuminoidformulation that uses the exclusive,
patented Phytosome systemto increase bioavailability
of the natural active principles.Meriva® improved the treadmill
walking performance of subjects bymore than 200% in just two months.
Furthermore, Meriva® showeda significant improvement in
individuals with eye challenges.To discover more about how
Meriva® unlocks the benefits ofcurcuminoids, visit indena.com today.
11.125x8.625_MerivaKey_Herbalgram.indd 1 5/13/15 11:39 AM