Eating epilepsy. A narrative review
12
196 Eating epilepsy. A narrative review Mariana Ruiz-León 1 , Marco A. Sánchez-Torres 2 , Sonia Luquin-de Anda 2 , Mónica E. Salmerón-Mercado 3 , and José L. Ruiz-Sandoval 2,4 * 1 Department of Neurology, Hospital Civil de Guadalajara Fray Antonio Alcalde; 2 Department of Neurosciences, Centro Universitario de Ciencias de la Salud (CUCS), Universidad de Guadalajara; 3 Department of Neurophysiology, Hospital Civil de Guadalajara Fray Antonio Alcalde; 4 Instituto de Neurociencias Traslacionales. Guadalajara, Jalisco, Mexico Revista Mexicana de Neurociencia REVIEW ARTICLE Abstract Eating epilepsy (EE) is rare reflex epilepsy in which seizures are triggered by mechanisms related to the eating process. In this narrative review, we analyzed case series and case reports found in the literature and describe sociodemographic, se- miological, and radiological characteristics of patients with EE in the general population. Our analysis revealed that this epilepsy is more common in male patients and usually presents with focal onset seizures. There is wide variability in clinical presentation and there is not enough evidence to affirm that there is a specific food or diet that triggers the seizures. Tem- porolimbic and suprasylvian areas of the frontal and temporal lobes, particularly the insular and opercular cortex, play an important role in the pathophysiology of EE as found in neuroradiological and neurosurgical studies. As for the treatment, there is a high prevalence of pharmacoresistance and clobazam was the most used antiepileptic drug, usually as an add-on therapy. Key words: Eating epilepsy. Eating seizures. Reflex epilepsy. Reflex seizures. Epilepsia refleja por alimentación. Una revisión narrativa Resumen La epilepsia por alimentación es un tipo de epilepsia refleja poco frecuente, en donde las crisis epilépticas son detonadas por mecanismos relacionados con el proceso de alimentación. En esta revisión narrativa analizamos reportes y series de casos de este tipo de epilepsia en la población general y detallamos características sociodemográficas, semiológicas y radiológicas. Nuestro análisis reveló que la epilepsia por alimentación es más prevalente en el sexo masculino y general- mente se presenta como crisis convulsivas focales. Existe una alta variabilidad en la presentación clínica y no hay evidencia suficiente para afirmar su asociación con algún tipo de alimento o dieta específica. En los estudios complementarios se encontró relación clínico-radiológica y quirúrgica en áreas temporolímbicas y suprasilvianas de los lóbulos frontal y tempo- ral, particularmente la corteza insular y opercular, recalcando su importante papel en la fisiopatología de esta epilepsia. En cuanto al tratamiento, hay una alta prevalencia de farmacorresistencia y el clobazam fue el antiepiléptico más utilizado, generalmente en conjunto con otros fármacos. Palabras clave: Epilepsia por alimentación. Crisis epilépticas por alimentación. Epilepsia refleja. Crisis epilépticas reflejas. Correspondence: *José L. Ruiz-Sandoval E-mail: [email protected] Available online: 01-10-2021 Rev Mex Neuroci. 2021;22(5):196-207 www.revmexneurociencia.com Date of reception: 25-01-2021 Date of acceptance: 16-03-2021 DOI: 10.24875/RMN.21000005 2604-6180/ © 2021 Academia Mexicana de Neurología A.C. Published by Permanyer. This is an open access article under the CC BY-NC-ND license (http://creativecommons.org/licenses/by-nc-nd/4.0/).
-
Upload
khangminh22 -
Category
Documents
-
view
0 -
download
0
Transcript of Eating epilepsy. A narrative review

196
Eating epilepsy. A narrative reviewMariana Ruiz-León1, Marco A. Sánchez-Torres2, Sonia Luquin-de Anda2, Mónica E. Salmerón-Mercado3, and José L. Ruiz-Sandoval2,4*1Department of Neurology, Hospital Civil de Guadalajara Fray Antonio Alcalde; 2Department of Neurosciences, Centro Universitario de Ciencias de la Salud (CUCS), Universidad de Guadalajara; 3Department of Neurophysiology, Hospital Civil de Guadalajara Fray Antonio Alcalde; 4Instituto de Neurociencias Traslacionales. Guadalajara, Jalisco, Mexico
Revista Mexicana de Neurociencia
REVIEW ARTICLE
Abstract
Eating epilepsy (EE) is rare reflex epilepsy in which seizures are triggered by mechanisms related to the eating process. In this narrative review, we analyzed case series and case reports found in the literature and describe sociodemographic, se-miological, and radiological characteristics of patients with EE in the general population. Our analysis revealed that this epilepsy is more common in male patients and usually presents with focal onset seizures. There is wide variability in clinical presentation and there is not enough evidence to affirm that there is a specific food or diet that triggers the seizures. Tem-porolimbic and suprasylvian areas of the frontal and temporal lobes, particularly the insular and opercular cortex, play an important role in the pathophysiology of EE as found in neuroradiological and neurosurgical studies. As for the treatment, there is a high prevalence of pharmacoresistance and clobazam was the most used antiepileptic drug, usually as an add-on therapy.
Key words: Eating epilepsy. Eating seizures. Reflex epilepsy. Reflex seizures.
Epilepsia refleja por alimentación. Una revisión narrativa
Resumen
La epilepsia por alimentación es un tipo de epilepsia refleja poco frecuente, en donde las crisis epilépticas son detonadas por mecanismos relacionados con el proceso de alimentación. En esta revisión narrativa analizamos reportes y series de casos de este tipo de epilepsia en la población general y detallamos características sociodemográficas, semiológicas y radiológicas. Nuestro análisis reveló que la epilepsia por alimentación es más prevalente en el sexo masculino y general-mente se presenta como crisis convulsivas focales. Existe una alta variabilidad en la presentación clínica y no hay evidencia suficiente para afirmar su asociación con algún tipo de alimento o dieta específica. En los estudios complementarios se encontró relación clínico-radiológica y quirúrgica en áreas temporolímbicas y suprasilvianas de los lóbulos frontal y tempo-ral, particularmente la corteza insular y opercular, recalcando su importante papel en la fisiopatología de esta epilepsia. En cuanto al tratamiento, hay una alta prevalencia de farmacorresistencia y el clobazam fue el antiepiléptico más utilizado, generalmente en conjunto con otros fármacos.
Palabras clave: Epilepsia por alimentación. Crisis epilépticas por alimentación. Epilepsia refleja. Crisis epilépticas reflejas.
Correspondence: *José L. Ruiz-Sandoval
E-mail: [email protected]
Available online: 01-10-2021
Rev Mex Neuroci. 2021;22(5):196-207
www.revmexneurociencia.com
Date of reception: 25-01-2021
Date of acceptance: 16-03-2021
DOI: 10.24875/RMN.21000005
2604-6180/ © 2021 Academia Mexicana de Neurología A.C. Published by Permanyer. This is an open access article under the CC BY-NC-ND license (http://creativecommons.org/licenses/by-nc-nd/4.0/).

197
M. Ruiz-León, et al.: Eating epilepsy
Introduction
Reflex epilepsy (RE) or reflex seizures refers to epi-leptic syndromes characterized by focal or generalized seizures elicited by a specific stimulus or activity. These stimuli can be simple (visual, auditive, proprioceptive, or tactile) or complex (while eating, talking, tooth-brush-ing, bathing, etc.)1,2. RE estimated prevalence rep-resents 4-7% of all epilepsies and 21% of idiopathic generalized type, being photosensitive epilepsy the most common3.
Eating epilepsy (EE) is a rare form of RE with a prev-alence of 1:1000-2000 of all patients with epilepsy, al-though it ranges higher in Asia3-6. EE is more common in males and usually presents as focal seizures with impaired awareness which can occur before, during, and/or after eating3,4,7.
In this critical review, we aimed to answer the follow-ing questions: which are the sociodemographic, semi-ological, and radiological characteristics of EE in the general population?
Background
Eating is a complex mechanism that includes olfac-tory, taste, somatosensory, and other interoceptive in-puts, which activate brain structures such as the insular cortex, frontal operculum, orbitofrontal cortex, and the amygdala8. The hypothalamus and other com-ponents of the autonomic nervous system regulate central and peripheral homeostasis of digestion and metabolism9. These structures are of particular interest in the study of hunger, satiety, obesity, as well as eat-ing and body image disorders such as anorexia and bulimia. Moreover, all of the aforementioned structures are well recognized as trigger zones of EE in various studies8,10.
Although the pathophysiology of EE is not clear, ac-cording to case reports and small case series in the literature, plausible mechanisms for its appearance have been proposed. A genetic involvement is shown in sub-jects with mutations in genes SYNGAP12, MECP211; as well as familial EE5, associated with Rett12, Cri du Chat,13,14 and congenital or acquired bilateral opercular syndromes15,16. Ethnic origin and environmental factors such as chemical composition of food, culinary habits, feeding behavior, and emotional and psychological in-volvement may be important in EE etiology7,17. EE can present with other epileptic syndromes, structural pathol-ogies (malformations, tumors), and/or brain injury (hy-poxic brain damage, gliosis, encephalomalacia, and
meningoencephalitis)4,7,17. Therefore, it has been pro-posed that EE may be a long-term manifestation of an initial precipitating event in the past7,17.
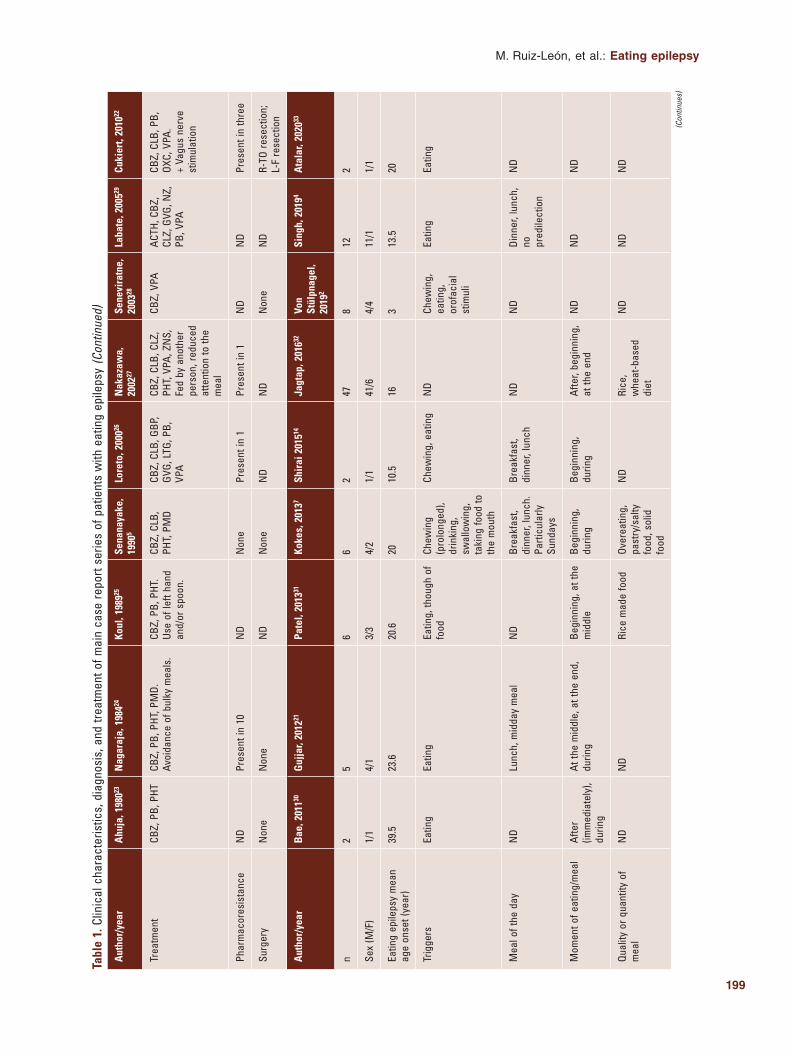
Clinical presentation of EE is diverse. Seizures usu-ally present as focal onset with impaired awareness and less commonly with generalized onset, including atonic, myoclonic, or even autonomic types3,4,7,17. EE occurs more frequently in the context of temporal or frontal lobe epilepsies4 and it usually is symptomatic or associated with imaging abnormalities in these loca-tions (Tables 1 and 2).
In patients with EE, seizures can be caused by di-verse and heterogeneous stimuli; nevertheless, all of them are related to the feeding process, either just before, during, or after it. These triggers may involve visual and olfactory stimuli (sight and smell), digestive and autonomic functions (salivating, chewing, swallow-ing, gastric distention, and gastric acid secretion), pro-prioceptive stimuli, thinking about food, bulky meals rich in carbohydrates, and gastroesophageal re-flux2,12,17-20. Moreover, association of EE to vasovagal syncope attacks has been reported, suggesting a vagal mechanism7.
Electroencephalographic (EEG) findings can be nor-mal or present focal or diffuse epileptiform abnormali-ties3. Magnetic resonance imaging (MRI) can also be normal or present structural abnormalities specifically in temporolimbic or suprasylvian areas, particularly in the insular and opercular cortex3,4,7,12. A clinical neuro-topographic correlation can be made with EEG finding and/or imaging findings.
Although identification and avoidance of stimulus in some patients could aid in seizure control, in EE, this is not always possible, except in very specific associat-ed situations3. Some patients respond and benefit from antiepileptic drugs. Although management of choice has not yet been established, intake of clobazam before meals may be effective as add-on therapy in the man-agement of EE3,4. Kokes et al. suggest that seizures that originate from the left temporal region may be more resistant to antiepileptic management7. Some patients with therapy resistance may benefit with surgical treat-ment21 or vagus nerve stimulation22, especially those with imaging abnormalities21.
Methods
This article is based on unsystematic research in Google Scholar and PubMed for original manuscripts about “Eating epilepsy,” “Eating reflex seizures,” “Eating seizures,” “Reflex eating epilepsy,” and “Reflex eating

198
Rev Mex Neuroci. 2021;22(5)
Aut
hor/
year
Ahu
ja, 1
98023
Nag
araj
a, 1
98424
Koul
, 198
925Se
nana
yake
, 19
905
Lore
to, 2
00026
Nak
azaw
a,
2002
27Se
nevi
ratn
e,
2003
28La
bate
, 200
529Cu
kier
t, 20
1022
n3
1350
203
228
23
Sex
(M/F
)3/
08/
5N
D13
/72/
12/
013
/15
2/0
2/1
Eatin
g ep
ileps
y m
ean
age
onse
t (ye
ar)
2214
15.2
1722
.69.
518
.68.
611
Trig
gers
Eatin
gCh
ewin
g, d
rinki
ng (w
ater
), ea
ting,
sna
cks
Chew
ing,
sw
allo
win
gN
DEa
ting
Chew
ing,
eat
ing,
sw
allo
win
gEa
ting
Eatin
gEa
ting
Mea
l of t
he d
ayN
DN
DN
DLu
nch
Mea
ls, l
unch
ND
ND
ND
ND
Mom
ent o
f eat
ing/
mea
lAf
ter,
durin
gAt
the
mid
dle,
at t
he e
ndDu
ring
Afte
r (30
min
po
st m
ain
mea
l), d
urin
g
At s
ight
, be
ginn
ing,
dur
ing
Afte
r, be
fore
, du
ring
Afte
r, du
ring
Begi
nnin
g,
durin
gDu
ring
Qual
ity o
r qua
ntity
of
mea
lN
DBu
lky
mea
ls, c
onve
ntio
nal
Indi
an m
eals
ND
ND
ND
ND
ND
ND
ND
Aura
(foc
al a
war
e)N
umbn
ess
ND
Forc
ed th
inki
ng
and
mem
orizi
ng,
visu
al
hallu
cina
tion
ND
ND
ND
ND
ND
ND
Eatin
g re
flex
seizu
re
type
At, F
BTC,
FO
IAFB
TC, F
O GT
CFB
TC, F
OA, F
OIA
FBTC
, FOA
, FO
IAFB
TC, F
OIA
FOA,
FOI
A,
FTBC
, GT
FBTC
, FOI
A GT
CFO
IA, G
TFO
IA
Radi
olog
ical
abn
orm
al
findi
ngs
(CT/
MRI
/PET
/SP
ECT)
ND
ND
NR
ND
MRI
: L
vent
ricul
omeg
aly,
R
retro
trigo
nal
hype
rinte
nsity
SPEC
T: M
e‑RT
lo
be fo
cal
hype
rper
f.
MRI
: non
eSP
ECT:
R‑F
hy
perp
erfu
sion
an
d R‑
stria
te
body
hyp
oper
f.
ND
MRI
: poo
r op
ercu
lum
fo
rmat
ion
with
th
icke
ned
Co
MRI
: B
peris
ylvi
an
poly
mic
rogy
ria
Elec
troen
ceph
alog
raph
ic
abno
rmal
find
ings
Inte
ricta
l EE
G:R‑
H: d
iffus
e,
unila
tera
l Spk
an
d Sh
w.
Gene
raliz
ed
disc
harg
es.
EEG:
L‑FT
Slw
Shw
.R‑
T Sw
v bu
rsts
.Ge
nera
lized
Spk
.
Inte
ricta
l EEG
: “p
ositi
ve”,
ED.
Inte
ricta
l EE
G:B‑
MT,
B‑P
oT
Shw
and
Slw
.
vEEG
: low
vo
ltage
slo
wed
ba
ckgr
ound
Icta
l vEE
G: h
igh
volta
ge S
lw +
di
ffuse
Slw
; R‑P
o Sh
‑Slw
Inte
ricta
l vEE
G:
R‑TF
, L‑T
pa
roxy
sm; R
‑T
ED
Icta
l vEE
G: h
igh
ampl
itude
del
ta
or th
eta
Inte
ricta
l EEG
: R‑
F Sp
and
Sh
w; R
‑O S
p
ND
Icta
l EEG
: di
ffuse
Spw
, ED
+ d
iffus
e at
tenu
atio
nIn
teric
tal E
EG:
gene
raliz
ed
Spk
or
poly
‑Spw
; R‑T
sl
owin
g an
d hi
gh a
mpl
itude
Sh
w S
lw
Icta
l EEG
: B‑T
lo
be o
nset
In
teric
tal E
EG:
B‑T
spik
ing;
L‑F
C Sp
k
Tabl
e 1.
Clin
ical
cha
ract
eris
tics,
dia
gnos
is, a
nd tr
eatm
ent o
f mai
n ca
se re
port
serie
s of
pat
ient
s w
ith e
atin
g ep
ileps
y (C
ontin
ued)
(Con
tinue
s)
199
M. Ruiz-León, et al.: Eating epilepsy
Aut
hor/
year
Ahu
ja, 1
98023
Nag
araj
a, 1
98424
Koul
, 198
925Se
nana
yake
, 19
905
Lore
to, 2
00026
Nak
azaw
a,
2002
27Se
nevi
ratn
e,
2003
28La
bate
, 200
529Cu
kier
t, 20
1022
Trea
tmen
tCB
Z, P
B, P
HTCB
Z, P
B, P
HT, P
MD.
Av
oida
nce
of b
ulky
mea
ls.
CBZ,
PB,
PHT
. Us
e of
left
hand
an
d/or
spo
on.
CBZ,
CLB
, PH
T, P
MD
CBZ,
CLB
, GBP
, GV
G, L
TG, P
B,
VPA
CBZ,
CLB
, CLZ
, PH
T, V
PA, Z
NS,
Fe
d by
ano
ther
pe
rson
, red
uced
at
tent
ion
to th
e m
eal
CBZ,
VPA
ACTH
, CBZ
, CL
Z, G
VG, N
Z,
PB, V
PA
CBZ,
CLB
, PB,
OX
C, V
PA.
+ Va
gus
nerv
e st
imul
atio
n
Phar
mac
ores
ista
nce
ND
Pres
ent i
n 10
ND
Non
ePr
esen
t in
1Pr
esen
t in
1N
DN
DPr
esen
t in
thre
e
Surg
ery
Non
eN
one
ND
Non
eN
DN
DN
one
ND
R‑TO
rese
ctio
n;
L‑F
rese
ctio
n
Aut
hor/
year
Bae
, 201
130G
ujja
r, 20
1221
Pate
l, 20
1331
Koke
s, 2
0137
Shir
ai 2
01514
Jagt
ap, 2
01632
Von
Stül
pnag
el,
2019
2
Sing
h, 2
0194
Ata
lar,
2020
33
n2
56
62
478
122
Sex
(M/F
)1/
14/
13/
34/
21/
141
/64/
411
/11/
1
Eatin
g ep
ileps
y m
ean
age
onse
t (ye
ar)
39.5
23.6
20.6
2010
.516
313
.520
Trig
gers
Eatin
gEa
ting
Eatin
g, th
ough
of
food
Chew
ing
(pro
long
ed),
drin
king
, sw
allo
win
g,
taki
ng fo
od to
th
e m
outh
Chew
ing,
eat
ing
ND
Chew
ing,
ea
ting,
or
ofac
ial
stim
uli
Eatin
gEa
ting
Mea
l of t
he d
ayN
DLu
nch,
mid
day
mea
lN
DBr
eakf
ast,
dinn
er, l
unch
. Pa
rticu
larly
Su
nday
s
Brea
kfas
t, di
nner
, lun
chN
DN
DDi
nner
, lun
ch,
no
pred
ilect
ion
ND
Mom
ent o
f eat
ing/
mea
lAf
ter
(imm
edia
tely
), du
ring
At th
e m
iddl
e, a
t the
end
, du
ring
Begi
nnin
g, a
t the
m
iddl
eBe
ginn
ing,
du
ring
Begi
nnin
g,
durin
gAf
ter,
begi
nnin
g,
at th
e en
dN
DN
DN
D
Qual
ity o
r qua
ntity
of
mea
lN
DN
DRi
ce m
ade
food
Over
eatin
g,
past
ry/s
alty
fo
od, s
olid
fo
od
ND
Rice
, w
heat
‑bas
ed
diet
ND
ND
ND
Tabl
e 1.
Clin
ical
cha
ract
eris
tics,
dia
gnos
is, a
nd tr
eatm
ent o
f mai
n ca
se re
port
serie
s of
pat
ient
s w
ith e
atin
g ep
ileps
y (C
ontin
ued)
(Con
tinue
s)

200
Rev Mex Neuroci. 2021;22(5)
Aut
hor/
year
Ahu
ja, 1
98023
Nag
araj
a, 1
98424
Koul
, 198
925Se
nana
yake
, 19
905
Lore
to, 2
00026
Nak
azaw
a,
2002
27Se
nevi
ratn
e,
2003
28La
bate
, 200
529Cu
kier
t, 20
1022
Aura
(foc
al a
war
e)Bl
urre
d vi
sion
, ja
mai
s‑vu
, pa
lpita
tions
, un
plea
sant
fe
ar.
ND
ND
Dysc
ogni
tive,
“e
xper
ient
ial”
ND
Ceph
alic
se
nsat
ion,
déj
à vu
, epi
gast
ric
risin
g se
nsat
ion,
fe
ar,
som
atos
enso
ry,
verti
go, v
isua
l,
ND
Ceph
alic
se
nsat
ion,
ep
igas
tric
sens
atio
n,
gidd
ines
s,
unea
sine
ss,
Epig
astri
c,
visu
al, v
ertig
o,
Eatin
g re
flex
seizu
re
type
A, F
BTC
FBTC
, FOI
A GT
CFO
FBTC
, FOA
, FO
IAFO
AFB
TC, F
OIA,
“H
D”Ab
, At,
EM,
GTC,
M, O
c,
To
FBTC
, FOI
A,
GTFB
TC, F
OIA
Radi
olog
ical
abn
orm
al
findi
ngs
(CT/
MRI
/PET
/SP
ECT)
MRI
: non
eCT
: non
eM
RI:
L‑M
eT s
cler
osis
, L‑T
: at
roph
y, c
ortic
al le
sion
,R‑
T ho
rn d
ilata
tion.
MRI
: L‑F
P pe
risyl
vian
co
rtica
l dy
spla
sia,
R a
nd
L Sy
lvia
n an
d pe
risyl
vian
gl
iosi
s, L
F ca
lcifi
ed
gran
ulom
a.SP
ECT:
F
hypo
perf.
; F, T
+
P‑in
sula
r hy
perp
erf.
MRI
:L‑
F‑EA
m
enin
giom
a,
L‑H
sequ
el
lesi
ons.
PE
T:L‑
MeT
, L‑L
aT,
O, a
nd
mul
tifoc
al
hypo
‑m
etab
olis
m.
MRI
: pon
tine
and
cere
bella
r hy
popl
asia
MRI
: PoT
PO
poly
mic
rogy
ria.
Perit
rigon
al
hype
rinte
nsiti
es,
pach
ygyr
ia,
glio
sis.
M
e‑T
scle
rosi
s.
T ca
vern
oma.
F
dysp
lasi
a.B
peris
ylvi
an,
MRI
:F
dila
tatio
n of
ext
erna
l sp
aces
of
CSF.
MRI
:B:
per
isyl
vian
gl
iosi
s.L‑
I‑F g
liosi
s.R‑
F pe
risyl
vian
sc
lero
sis,
R‑T
sc
lero
sis.
MIR
: “n
on‑s
peci
fic”
SPEC
T: L
‑T, L
‑I‑F,
and
R‑S‑
F hy
pope
rf.PE
T: R
‑T
hypo
met
abol
ism
.
Elec
troen
ceph
alog
raph
ic
abno
rmal
find
ings
Icta
l EEG
:L‑
T on
set o
f ge
nera
lized
rh
ythm
ic
thet
a an
d de
lta a
ctiv
ity.
Inte
ricta
l vE
EG:
B‑T:
Spk
.
Inte
ricta
l vEE
G:L‑
MT
onse
t of i
sola
ted
disc
harg
es.
Inte
ricta
l EEG
:R‑
FT, R
‑TP
gene
raliz
ed S
pk,
Shw
.
Icta
l EEG
: L‑P
T,
L‑FC
, R‑F
TC
slow
ing.
R‑F
CT
beta
, the
ta
activ
ity. L
‑FCT
Sh
wIn
teric
tal E
EG:
L‑C
thet
a w
v,
L‑FC
Shw
.
Icta
l EEG
on
set:
L‑FT
, L‑T
P.In
teric
tal
EEG:
L‑FT
, L‑P
T,
and
L‑T
Spk
and
slow
ing,
L‑
H sl
owin
g.R‑
TO S
pk a
nd
slow
ing.
Icta
l EEG
: Slw
(>
T);
nega
tive‑
posi
tive
pote
ntia
ls (>
F, m
idlin
e)In
teric
tal E
EG:
ED (>
MT,
PoT
), Sp
w
Icta
l vEE
GDi
ffuse
, F‑C
, Po
TPO
and
T ED
.In
teric
tal v
EEG:
Late
raliz
ed,
unce
rtain
, and
di
ffuse
ED.
vEEG
:B
(>O)
, B‑P
O Sp
w, B
‑O
slow
ed
back
grou
nd
activ
ity
(thet
a).
Diffu
se S
pk
and
Spw
.PO
slo
win
g.
Inte
ricta
l EEG
:B‑
Po E
D, B
pe
rirol
andi
c Sp
k.L‑
FT E
D, L
‑PoT
ED
with
se
cond
ary
gene
raliz
atio
n,
L‑T
Spk.
R‑CT
ED,
R‑P
o Sp
k.
Icta
l/Int
eric
tal:
R‑FT
slo
w a
nd
Spw
Trea
tmen
tCB
Z, L
EVCB
Z, C
LZ, L
EV, L
MT,
PB,
TP
M, V
PAN
DN
DCB
Z, C
LB, L
TG,
LEV,
TPM
, VPA
, ZN
S
ND
CLB,
ESM
, LE
V, L
TG,
TPM
, VPA
, ZN
S
CBZ,
CLB
, LEV
, LC
M, O
XC,
PHB,
PHT
, TP
M, V
PA
CBZ,
LCM
, LEV
Tabl
e 1.
Clin
ical
cha
ract
eris
tics,
dia
gnos
is, a
nd tr
eatm
ent o
f mai
n ca
se re
port
serie
s of
pat
ient
s w
ith e
atin
g ep
ileps
y (C
ontin
ued)
(Con
tinue
s)

201
M. Ruiz-León, et al.: Eating epilepsy
Aut
hor/
year
Ahu
ja, 1
98023
Nag
araj
a, 1
98424
Koul
, 198
925Se
nana
yake
, 19
905
Lore
to, 2
00026
Nak
azaw
a,
2002
27Se
nevi
ratn
e,
2003
28La
bate
, 200
529Cu
kier
t, 20
1022
Phar
mac
ores
ista
nce
ND
Pres
ent i
n 1
ND
Pres
ent i
n 5
Pres
ent i
n 2
Pres
ent i
n 16
Pres
ent i
n 6
ND
ND
Surg
ery
Non
eL‑
T lo
bect
omy
+ am
ygda
lohi
ppoc
ampe
ctom
yLe
sion
ecto
my
Non
eN
DYe
s (in
2)
Non
eN
DN
one
ACTH
: adr
enoc
ortic
otro
pic
horm
one;
At:
aton
ic; A
b: a
bsce
nse;
B: b
ilate
ral;
C: c
entro
; CBZ
: car
bam
azep
ine;
CES
: clu
ster
of e
pile
ptic
spa
sms;
CLB
: clo
baza
m; C
LZ: c
lona
zepa
m; C
o: c
orte
x; C
SF: c
ereb
rosp
inal
flui
d; C
T: c
ompu
teriz
ed to
mog
raph
y; D
A:
drop
atta
cks;
EA:
ext
ra‑a
xial
; ED:
epi
lept
iform
dis
char
ges;
EEG
: ele
ctro
ence
phal
ogra
m; E
M: e
yelid
myo
clon
ia; E
SM: e
thos
uxim
ide;
F: f
ront
al; F
OA: f
ocal
ons
et a
war
e; F
OAI:
foca
l ons
et im
paire
d aw
aren
ess;
FBT
C: fo
cal t
o bi
late
ral t
onic
‑clo
nic;
FC:
fro
nto‑
cent
ral;
fRM
I: fu
nctio
nal m
agne
tic re
sona
nce
imag
ing;
GBP
: gab
apen
tin; G
T: g
ener
alize
d to
nic;
GTC
: gen
eral
ized
toni
c‑cl
onic
; GVG
: vig
abat
rin; H
: hem
isph
ere;
HD:
hea
d dr
ops;
I: in
ferio
r; L:
left;
La:
late
ral;
LCM
: lac
osam
ide;
LEV
: le
vetir
acet
am; L
TG: l
amot
rigin
e; M
e: m
esia
l; M
: myo
clon
ic; M
RI: m
agne
tic re
sona
nce
imag
ing;
MT:
mid
‑tem
pora
l; N
D: n
o da
ta; N
R: n
o re
alize
d; N
Z: n
itraz
epam
; O: o
ccip
ital;
Oc: o
culo
ceph
alic
s; O
XC: o
xcar
baze
pine
; P: p
arie
tal;
PB: p
heno
barb
ital;
PET:
pos
ition
em
issi
on to
mog
raph
y; P
HT: p
heny
toin
; PN
ET: p
rimiti
ve n
euro
ecto
derm
al tu
mor
; Po:
pos
terio
r; PR
M: p
rimid
one;
R: r
ight
; sEE
G: s
tere
oele
ctro
ence
phal
ogra
phy;
Shw
: sha
rp w
ave;
Slw
: slo
w w
ave;
SPE
CT: s
ingl
e ph
oton
em
issi
on
tom
ogra
phy;
Sp:
spi
kes;
Spw
: spi
ke w
ave;
S: s
uper
ior;
T: te
mpo
ral;
To: t
onic
; TPM
: top
iram
ate;
vEE
G: v
ideo
elec
troen
ceph
alog
ram
; VPA
: val
proa
te; w
v: w
ave;
ZN
S: z
onis
amid
e.
Tabl
e 1.
Clin
ical
cha
ract
eris
tics,
dia
gnos
is, a
nd tr
eatm
ent o
f mai
n ca
se re
port
serie
s of
pat
ient
s w
ith e
atin
g ep
ileps
y (C
ontin
ued)
seizures;” followed by a discretionary selection of pub-lications. We included observational studies (such as case reports and case series) published between 1967 and 2020. Editorial notes, literature systematic reviews and clinical images were excluded from the study.
Results
In this review, we analyzed 18 case series and 23 case reports (Tables 1 and 2) and we included the case of a 40-year-old male patient with EE evaluated in our epilepsy clinic (T able 2).
Discussion
Due to the inherent limitations of the case report and case series, result heterogeneity is obvious, with the consequent weakness of the conclusions. Despite these limitations from the data not reported or speci-fied, the following information is relevant. We found that out of 237 patients, 126 were male and 61 were female (the sex of 50 patients was not specified by the author) with a resulting 2:1 ratio, highlighting the predominance among men. The reason why there is a clear predominance in males is unknown; we won-der if it has to do with the diagnosis approach, or if women are underdiagnosed or if there is a more com-plex pathophysiological explanation.
As for the type of seizures, the most frequently re-ported were the focal type with or without impaired awareness (Tables 1 and 2).
In both the case series and the case reports, the most common and constant trigger was by definition the act of eating itself2,4,11,13-19,21-24,26-31,33-38,42-46 but in some cases other stimuli were detailed such as chew-ing2,7,14,18,24,25,27,34,36, swallowing7,25,27,36, drinking7,24, seeing18,37,39,45, smelling11,37,39, and even thinking31,37 or talking37 about food. Orofacial stimuli2, taking food to the mouth7, hunger alone37, eating snacks24, and tasting food11 were also described.
In the case report series, other specific triggers to EE related to the type of food have also been described, including bulky meals, conventional Indian meals24, wheat-based diet, and on a rice-based diet31,32. Only 4 patients had a preference for a specific type of food (spicy food11, bread17, strawberry syrup42, and minced meat45). Furthermore, just a few authors specified the patient’s diet, so it remains unclear if EE has a relation to specific diet type.
MRI and CT findings were variable. Some abnor-malities were encephalomalacia, sclerosis,

202
Rev Mex Neuroci. 2021;22(5)
(Con
tinue
s)
Tabl
e 2.
Clin
ical
cha
ract
eris
tics,
dia
gnos
is, a
nd tr
eatm
ent o
f mai
n ca
se re
ports
of p
atie
nts
with
eat
ing
epile
psy
Aut
hor/
year
Lavi
zzar
i, 19
6718
Ciri
gnot
ta, 1
97719
Robe
rtso
n, 1
97834
Fiol
, 198
635M
ateo
s, 1
99515
Kish
i, 19
9916
Sex
MF
MF
MM
Eatin
g ep
ileps
y ag
e on
set (
yr)
1216
1412
118
Trig
gers
At s
ight
, che
win
g,
eatin
gEa
ting
Chew
ing,
eat
ing
Eatin
gEa
ting
Eatin
g
Mea
l of t
he d
ayN
DM
eals
*m
ore
frequ
ent a
t br
eakf
ast
ND
Mor
e at
bre
akfa
stM
eals
ND
Mom
ent o
f eat
ing/
mea
lN
DBe
ginn
ing,
dur
ing
ND
Begi
nnin
gN
DN
D
Qual
ity o
r qua
ntity
of m
eal
ND
ND
ND
Non
eN
DN
D
Aura
(Foc
al A
war
e)N
DN
DLe
ft up
per l
imb
num
bnes
s an
d le
ft fa
cial
par
esth
esia
.
ND
ND
ND
Eatin
g re
flex
seizu
re ty
peFO
AFO
IA, H
DFO
AFO
IA, G
TCFO
, FTB
CFO
IA
Radi
olog
ical
abn
orm
al fi
ndin
gs
(CT/
MRI
/PET
/SPE
CT)
NR
NR
CT: R
ast
rocy
tom
a of
ba
sal g
angl
ia.
CT: n
one.
CT/M
RI: B
rola
ndic
op
ercu
la a
troph
y.M
RI: B
per
isyl
vian
m
alfo
rmat
ions
, po
lym
icro
gyria
.
Elec
troen
ceph
alog
raph
ic
abno
rmal
find
ings
EEG:
B‑F
sha
rp
trans
ient
s, p
ositi
ve
spik
es.
Inte
ricta
l EEG
: ge
nera
lized
slo
w
wav
es.
EEG:
infre
quen
t diff
use
spik
e‑w
ave
disc
harg
es. B
rief
low
‑vol
tage
fast
act
ivity
and
di
ffuse
pol
yspi
ke‑w
ave
disc
harg
es d
urin
g sl
eep.
Icta
l EEG
: diff
use
shar
p w
ave.
B:
low
vol
tage
fast
act
ivity
. R‑T
: ra
pid
activ
ity m
ediu
m v
olta
ge.
EEG:
R‑
FT fo
cal s
low
ing.
R‑
F de
lta fo
cus,
sp
ikes
, sha
rp w
aves
.
Icta
l vEE
G: g
ener
alize
d lo
w‑v
olta
ge fa
st fr
eque
ncie
s.
L ‑T
or R
‑T o
nset
spi
kes.
Inte
ricta
l EEG
:Ge
nera
lized
pol
yspi
ke w
ave.
R‑Po
, R‑M
T, L
‑Po,
L‑M
T sp
ikes
, and
sha
rp w
aves
.
Inte
ricta
l EEG
: R‑C
T sl
ow
Spk,
Slw
.Ic
tal v
EEG:
gen
eral
ized
low
‑vol
tage
atte
nuat
ion.
Inte
ricta
l EEG
: B‑C
P sy
nchr
onou
s Sh
w.
Trea
tmen
tPH
T, P
RMN
DPB
, PHT
CBZ,
CZP
, ESM
, PB,
PHT
, VPA
CBZ,
CLB
, VPA
ND
Phar
mac
ores
ista
nce
No
Yes
ND
Yes
No
Yes
Surg
ery
No
No
Fron
tal c
rani
otom
y +
subt
otal
rese
ctio
n of
lo
w‑g
rade
as
trocy
tom
a.
No
ND
ND

203
M. Ruiz-León, et al.: Eating epilepsy
Tabl
e 2.
con
tinua
tion:
Clin
ical
cha
ract
eris
tics,
dia
gnos
is, a
nd tr
eatm
ent o
f mai
n ca
se re
ports
of p
atie
nts
with
eat
ing
epile
psy
(Con
tinue
d)
Aut
hor/
year
Dom
izio
, 200
620D
’Ors
i, 20
0736
El B
ouzi
di, 2
01037
Man
yam
, 201
038M
artín
ez, 2
01112
De
Palm
a, 2
01211
Sex
MM
FF
FM
Eatin
g ep
ileps
y ag
e on
set (
yr)
< 1
2544
2316
6
Trig
gers
Brea
stfe
edin
gCh
ewin
g, e
atin
g, s
wal
low
ing
At s
ight
, dis
cuss
ing
cook
ing,
eat
ing,
hu
nger
thou
ght o
r sm
ell o
f foo
d.
Eatin
gN
DEa
ting,
sm
ell,
tast
e, *
es
peci
ally
spi
cy fo
od.
Mea
l of t
he d
ayN
DLu
nch,
bre
akfa
st, d
inne
rDi
nner
, lun
ch, m
eals
, sn
acks
Mea
lsN
DN
D
Mom
ent o
f eat
ing/
mea
lAf
ter d
rinki
ng m
ilkN
DBe
ginn
ing,
dur
ing
ND
Begi
nnin
gN
D
Qual
ity o
r qua
ntity
of m
eal
Milk
ND
ND
ND
ND
ND
Aura
(Foc
al A
war
e)N
DN
DN
DN
DN
DN
D
Eatin
g re
flex
seizu
re ty
peDe
satu
ratio
n, c
yano
sis,
in
crea
se in
mus
cula
r to
ne.
At (g
ener
alize
d)FB
TC, F
OAFO
IAFO
ACE
S
Radi
olog
ical
abn
orm
al fi
ndin
gs
(CT/
MRI
/PET
/SPE
CT)
MRI
/CT:
non
eM
RI: B
ope
rcul
ar d
yspl
asia
+
corp
us c
allo
sum
hyp
opla
sia.
MRI
: L‑F
(pre
cent
ral)
hype
rinte
nsity
.M
RI: p
ost‑s
urgi
cal.
RMI:
none
RMI:
none
Elec
troen
ceph
alog
raph
ic
abno
rmal
find
ings
EEG:
R‑M
eT a
bnor
mal
w
aves
Icta
l EEG
: B‑A
n di
ffuse
Slw
Inte
ricta
l EEG
: diff
use
alph
a‑lik
e ba
ckgr
ound
+ L
‑TPO
th
eta
activ
ity a
nd S
pw.
Inte
ricta
l EEG
: non
e
*Ele
ctro
corti
cogr
aphy
: L‑
F op
ercu
lum
ep
ilept
iform
act
ivity
(a
nter
ior‑
infe
rior.
to
the
MRI
lesi
on)
Icta
l EEG
: del
ta a
ctiv
ity (>
F)In
teric
tal E
EG: L
‑H s
low
ing,
th
eta
and
delta
act
ivity
. L‑T
Sh
w.
Inte
ricta
l EEG
: F, C
ED.
Icta
l EEG
: diff
use
slow
‑wav
e co
mpl
ex, >
B‑
FC, f
ollo
wed
by
volta
ge a
ttenu
atio
n.
Trea
tmen
tPB
, ant
iaci
d th
erap
y (G
ER)
CBZ,
CLB
, CLZ
, LEV
, LTG
, OXC
, VP
ACB
Z, V
PALT
G, V
PAES
M, L
EV, V
PACL
B, V
PA, a
void
ance
of
spic
y fo
od.
Phar
mac
ores
ista
nce
No
Yes
Yes
No
No
Yes
Surg
ery
No
ND
‑Sub
tota
l res
ectio
n of
L‑
F op
ercu
lum
: Gra
de
IV g
liobl
asto
ma.
Post
‑res
ectio
n le
ft op
ercu
lar
PNET
.N
oN
o
(Con
tinue
s)

204
Rev Mex Neuroci. 2021;22(5)
Tabl
e 2.
con
tinua
tion:
Clin
ical
cha
ract
eris
tics,
dia
gnos
is, a
nd tr
eatm
ent o
f mai
n ca
se re
ports
of p
atie
nts
with
eat
ing
epile
psy
(Con
tinue
d)
Aut
hor/
year
Sand
hya,
201
339Ko
ul, 2
01340
Silla
npää
, 201
441Lo
di, 2
01513
Bla
uwbl
omm
e, 2
01542
Koba
yash
i, 20
1643
Sex
MF
FM
FF
Eatin
g ep
ileps
y ag
e on
set (
yr)
8<1
<127
288
Trig
gers
Sigh
t or s
mel
l of f
ood
Brea
st fe
edin
gBr
east
feed
ing
Eatin
gEa
ting
Eatin
g
Mea
l of t
he d
ayN
DN
DN
DN
DN
DN
D
Mom
ent o
f eat
ing/
mea
lAt
sig
ht, b
efor
eBe
ginn
ing,
afte
rBe
ginn
ing
ND
ND
Begi
nnin
g, d
urin
g
Qual
ity o
r qua
ntity
of m
eal
ND
ND
ND
ND
Espe
cial
ly s
traw
berr
y sy
rup
ND
Aura
(Foc
al A
war
e)N
DN
DCr
ying
and
cou
ghin
gN
DN
DN
D
Eatin
g re
flex
seizu
re ty
peN
DFO
, GT
FBTC
CES
FOIA
CES
Radi
olog
ical
abn
orm
al
findi
ngs
(CT/
MRI
/PET
/SPE
CT)
MRI
: non
eIn
teric
tal S
PECT
: L‑
FPO
perfu
sion
ch
ange
s.Ic
tal S
PECT
: B‑F
TPO
perfu
sion
cha
nges
.
MRI
: non
eM
RI: n
one
MRI
: non
eM
RI: p
ost‑s
urge
ry
cavi
tyfM
RI: a
ctiv
atio
n of
B
insu
la, R
‑dor
sola
tera
l‑F‑
Co a
nd d
orso
late
ral‑
P‑Co
.
MRI
: cor
pus
callo
sum
dy
sgen
esis
, cer
ebel
lar
hypo
gene
sis,
cer
ebra
l as
ymm
etry
, po
lym
icro
gyria
, pe
riven
tricu
lar
hete
roto
pia,
clo
sed
lip
schi
zenc
epha
ly.
Elec
troen
ceph
alog
raph
ic
abno
rmal
find
ings
Inte
ricta
l vEE
G: L
‑FT
ED EEG‑
fMRI
: ED,
ac
tivat
ion
of L
‑FT
lobe
s, B
‑P re
gion
, M
e‑st
ruct
ures
(p
arac
entra
l lob
ule,
ca
udat
e, c
ingu
late
an
d m
edia
l fro
ntal
, lin
gual
and
med
ial
occi
pita
l gyr
us.
Inte
ricta
l EEG
: non
eEE
G: R
‑PoT
slo
win
gIn
teric
tal E
EG:
R as
ymm
etric
ba
ckgr
ound
act
ivity
of
low
er a
mpl
itude
an
d re
peat
ed
slow
‑wav
e di
scha
rges
Inte
ricta
l EEG
: slo
w
back
grou
nd a
ctiv
ity, p
oor
orga
niza
tion
Icta
l EEG
:F‑
C (>
LH) d
iffus
e irr
egul
ar
spik
e an
d sl
ow‑w
ave
com
plex
, som
e fo
llow
ed b
y de
lta rh
ythm
ic a
ctiv
ity fr
om
L‑FC
and
An
verte
x.
vEEG
: An
hipp
ocam
pus
spik
es. A
n in
sula
r in
frequ
ent
asyn
chro
nous
spi
kes.
sEEG
: AnI
insu
la
high
‑am
plitu
de s
pike
fo
llow
ed b
y lo
w‑
volta
ge h
igh‑
frequ
ency
di
scha
rge
with
se
cond
ary
spre
adin
g to
hi
ppoc
ampu
s an
d TC
o.
Inte
ricta
l EEG
: slo
w
back
grou
nd a
ctiv
ity
with
mul
tifoc
al s
pike
s L‑
H, R
‑CT
regi
on.
Icta
l EEG
: diff
use
larg
e tri
phas
ic p
oten
tials
>R
‑CTP
regi
on.
Trea
tmen
tN
DVP
APB
CLB
ND
LTG,
TPM
, VPA
Phar
mac
ores
ista
nce
ND
No
No
Yes
Yes
ND
Surg
ery
No
No
No
No
‑9 y
ears
bef
ore
EE: O
perc
ular
‑insu
lar
R‑ c
aver
nom
a re
sect
ion
‑Epi
leps
y su
rger
y: A
n in
sula
rese
ctio
n.
ND
(Con
tinue
s)

205
M. Ruiz-León, et al.: Eating epilepsy
Tabl
e 2.
con
tinua
tion:
Clin
ical
cha
ract
eris
tics,
dia
gnos
is, a
nd tr
eatm
ent o
f mai
n ca
se re
ports
of p
atie
nts
with
eat
ing
epile
psy
(Con
tinue
d)
Aut
hor/
year
Lee,
201
644M
imur
a, 2
01745
Kisl
i, 20
1817
Ald
osar
i, 20
2046
Ruiz
-Leó
n, 2
020
(pre
sent
cas
e)
Sex
FF
FM
M
Eatin
g ep
ileps
y ag
e on
set (
yr)
6020
1930
20
Trig
gers
Eatin
gAt
sig
ht, e
atin
gEa
ting
Eatin
gEa
ting
Mea
l of t
he d
ayN
DN
DN
DN
DN
o pr
efer
ence
Mom
ent o
f eat
ing/
mea
lN
DBe
fore
, dur
ing
Mos
tly a
t the
be
ginn
ing
Mos
tly a
t the
beg
inni
ngM
iddl
e
Qual
ity o
r qua
ntity
of m
eal
ND
Spec
ially
min
ced
mea
tOn
ly w
hile
eat
ing
brea
dN
DOn
ly w
ith s
olid
food
Aura
(Foc
al A
war
e)Di
zzin
ess,
impa
ired
spee
chN
DN
DN
DDi
zzin
ess
Eatin
g re
flex
seizu
re ty
peFO
AFB
TC, F
OAFO
AFB
TC, F
OIA
FOIA
Radi
olog
ical
abn
orm
al
findi
ngs
(CT/
MRI
/PET
/SPE
CT)
MRI
: non
ePE
T: b
item
pora
l hy
pom
etab
olis
m (>
L)
ND
MRI
: B‑P
Co
ence
phal
omal
acia
ar
ea
MRI
/PET
: non
eM
RI: n
one
Elec
troen
ceph
alog
raph
ic
abno
rmal
find
ings
ND
Icta
l vEE
G:L‑
F to
MT:
rhyt
hmic
thet
a ac
tivity
follo
wed
by
gene
raliz
ed s
eizu
re p
atte
rn.
Icta
l EEG
: R‑F
T sh
arp
wav
e ac
tivity
Inte
ricta
l EEG
: non
e.
vEEG
: B‑T
ED.
Icta
l vEE
G: R
‑T rh
ythm
ic
activ
ity w
ithpe
risyl
vian
spr
eadi
ngsE
EG:
R‑An
MeT
, ins
ula,
am
ygda
la,
hipp
ocam
pus.
vEEG
: Int
erm
itten
t R‑H
slo
win
g w
aves
, pr
edom
inan
tly F
‑C a
nd w
ith n
o ep
ilept
iform
ab
norm
ality
.
Trea
tmen
tN
DN
DLE
VN
DOX
C
Phar
mac
ores
ista
nce
ND
ND
ND
Yes
No
Surg
ery
ND
ND
ND
R‑An
‑T lo
bect
omy
incl
udin
g M
e st
ruct
ures
(am
ygda
la,
uncu
s, h
ippo
cam
pus)
+
parti
al in
ferio
r ins
ulec
tom
y.
No
ACTH
: adr
enoc
ortic
otro
pic
horm
one;
At:
aton
ic; A
b: a
bsce
nse;
B: b
ilate
ral;
C: c
entro
; CBZ
: car
bam
azep
ine;
CES
: clu
ster
of e
pile
ptic
spa
sms;
CLB
: clo
baza
m; C
LZ: c
lona
zepa
m; C
o: c
orte
x; C
SF: c
ereb
rosp
inal
flui
d; C
T: c
ompu
tariz
ed to
mog
raph
y;
DA: d
rop
atta
cks;
EA:
ext
ra‑a
xtia
l; ED
: epi
lept
iform
dis
char
ges;
EEG
: ele
ctro
ence
phal
ogra
m; E
M: e
yelid
myo
clon
ia; E
SM: e
thos
uxim
ide;
F: f
ront
al; F
OA: f
ocal
ons
et a
war
e; F
OAI:
foca
l ons
et im
paire
d aw
aren
ess;
FBT
C: fo
cal t
o bi
late
ral t
onic
‑clo
nic;
FC
: fro
nto‑
cent
ral;
fRM
I: fu
nctio
nal m
agne
tic re
sona
nce
imag
ing;
GBP
: gab
apen
tin; G
T: g
ener
alize
d to
nic;
GTC
: gen
eral
ized
toni
c‑cl
onic
; GVG
: vig
abat
rin; H
: hem
isph
ere;
HD:
hea
d dr
ops;
I: in
ferio
r; L:
left;
La:
late
ral;
LCM
: lac
osam
ide;
LE
V: le
vetir
acet
am; L
TG: l
amot
rigin
e; M
e: m
esia
l; M
: myo
clon
ic; M
RI: m
agne
tic re
sona
nce
imag
ing;
MT:
mid
‑tem
pora
l; N
D: n
o da
ta; N
R: n
o re
alize
d; N
Z: n
itraz
epam
; O: o
ccip
ital;
Oc: o
culo
ceph
alog
yres
; OXC
: oxc
arba
zepi
ne; P
: par
ieta
l; PB
: ph
enob
arbi
tal;
PET:
pos
ition
em
issi
on to
mog
raph
y; P
HT: p
heny
toin
; PN
ET: p
rimiti
ve n
euro
ecto
derm
al tu
mor
; Po:
pos
terio
r; PR
M: p
rimid
one;
R: r
ight
; sEE
G: s
tere
oele
ctro
ence
phal
ogra
phy;
Shw
: sha
rp w
ave;
Slw
: slo
w w
ave;
SPE
CT: s
ingl
e ph
oton
em
issi
on to
mog
raph
y; S
p: s
pike
s; S
pw: s
pike
wav
e; S
: sup
erio
r; T:
tem
pora
l; To
: ton
ic; T
PM: t
opira
mat
e; v
EEG:
vid
eoel
ectro
ence
phal
ogra
m; V
PA: v
alpr
oate
; wv:
wav
e; Z
NS:
zon
isam
ide.

206
Rev Mex Neuroci. 2021;22(5)
pachygyria, polymicrogyria, dysplasia, glioma, ven-triculomegaly, meningioma, cavernoma, astrocytoma, and other lesions2,4,7,14-16,21,22,26,29,31,32,34,36,37,43. Four authors reported positron emission tomography; three presented hypometabolism7,33,44, and one was nor-mal46. Five authors reported single-photon emission computed tomography that showed perfusion chang-es26,27,31,33,39. Two authors reported functional MRI showing activation of both insula and dorsolateral frontal and parietal cortex42 and the other showing left temporal, bilateral parietal, paracentral lobule, cingu-late, medial frontal gyrus, and lingual and medial occipital gyrus abnormalities39. EEG findings were highly variable and different in each patient (Tables 1 and 2). Two authors detailed stereoelectro-encephalography, finding affectation of the insula, hippocampus, and temporal cortex and/or amigda-la42,48]. One patient underwent electrocorticography with operculum activity37. Surgery was performed on 10 patients, consisting of left-temporal lobectomy and amygdalohippocampectomy21, right-temporo-occipital resection, left-frontal resection22, lesionectomy31, subtotal resection of low grade astrocytoma34, subto-tal resection of left-frontal operculum (grade IV glio-blastoma)37, anterior insula resection42, right-anterior-temporal lobectomy including mesial structures and partial inferior insulectomy46, and non-specified in two patients. Only three patients un-derwent vagus nerve stimulation22.
Furthermore, the presence or absence of pharma-coresistance was specified in 131 patients (55% of the reviewed patients), of which 45 (41%) presented phar-macoresistance although sex, age, or type of seizure predominance was not clear.
Conclusion
EE is not the most frequent type of RE and be-cause it can coexist with other epileptic syndromes, we speculate that EE may be under-diagnosed, so RE should be investigated in all patients with known epilepsy. It is our belief that semiology and specific activities during the eating process should be spec-ified in order to identify the possible physiological-eti-ological mechanism, which until the present day is unknown. Finally, EE can be a therapeutic challenge since each patient presents variability in age of on-set, type of stimuli and seizure, clinical course, find-ings in complementary studies, and response to management.
Funding
None.
Conflicts of interest
None.
Ethical disclosures
Protection of human and animal subjects. The authors declare that no experiments were performed on humans or animals for this study.
Confidentiality of data. The authors declare that they have followed the protocols of their work center on the publication of patient data.
Right to privacy and informed consent. The au-thors have obtained the written informed consent of the patients or subjects mentioned in the article. The cor-responding author is in possession of this document.
Supplementary data
Supplementary data are available at Revista Mexi-cana de Neurociencia online (www.revmexneurocien-cia.com). These data are provided by the corresponding author and published online for the benefit of the read-er. The contents of supplementary data are the sole responsibility of the authors.
References 1. International League against Epilepsy. Diagnostic Manual: reflex Epilep-
sies; 2020. Available from: https://www.epilepsydiagnosis.org/syndrome/reflex-epilepsies-overview.html?locale=es.
2. von Stülpnagel C, Hartlieb T, Borggräfe I, Coppola A, Gennaro E, Escher-mann K, et al. Chewing induced reflex seizures (“eating epilepsy”) and eye closure sensitivity as a common feature in pediatric patients with SYNGAP1 mutations: review of literature and report of 8 cases. Seizure. 2019;65:131-7.
3. Okudan ZV, Özkara C. Reflex epilepsy: triggers and management stra-tegies. Neuropsychiatr Dis Treat. 2018;14:327-37.
4. Singh P, Bansal RA, More A, Bhuyan S, Garg A. (2019). Eating Epilepsy in North India: case series and its management. J Epilepsy Res. 2019;9:152-6.
5. Senanayake N. Familial eating epilepsy. J Neurol. 1990;237:388-91. 6. Seneviratne U. Reflex epilepsies; clinical and demographic characteris-
tics in a tropical country. J Clin Neurosci. 2005;12:767-69. 7. Kokes U, Baykan B, Bebek N, Gurses C, Gokigit A. Eating epilepsy is
associated with initial precipitating events and therapy resistance. Clin EEG Neurosci. 2013;44:161-6.
8. Wistehube T, Rullman M, Wiacek C, Braun P, Burkhard P. Fat perception in the human frontal operculum, insular and somatosensory cortex. Sci Rep. 2018;8:11825.
9. Wright H, Fallon NB, Crookall R, Giesbrecht T, Thomas A, Halford JC, et al. Differential effects of hunger and satiety on insular cortex and hypo-thalamic functional connectivity. Eur J Neurosci. 2016;43:1181-9.
10. Frank S, Kullman S, Veit R. Food related processes in the insular cortex. Front Hum Neurosci. 2013;7:499.
11. de Palma L, Boniver C, Cassina M, Toldo I, Nosadini M, Clementi M, et al. Eating-induced epileptic spasms in a boy with MECP2 duplication syndrome: insights into pathogenesis of genetic epilepsies. Epileptic Disord. 2012;14:414-7.

207
M. Ruiz-León, et al.: Eating epilepsy
12. Martínez AR, Colmenero MI, Pereira AG, Vilaplana FX, Morón JA, Marfa MR. Reflex seizures in Rett syndrome. Epileptic Disord. 2011;13:389-93.
13. Lodi M, Rebessi E, Parente E, Micalizzi E, Viri M, Milani D, et al. Eating epilepsy characterised by late-onset epileptic spasms in a case of Cri du chat syndrome. Seizure. 2015;32:49-51.
14. Shirai K, Saito Y, Yokoyama A, Nishimura Y, Tamasaki A, Maegaki Y. Stimulus-induced reflex epileptic spasms in 5p-syndrome. Brain Dev. 2016;38:261-5.
15. Mateos V, Salas-Puig J, Campos DM, Carrero V, Andermann F. Acquired bilateral opercular lesions or foix-chavany-marie syndrome and eating epilepsy. J Neurol Neurosurg Psychiatry. 1995;59:559-60.
16. Kishi T, Moriya M, Kimoto Y, Nishio Y, Tanaka T. Congenital bilate-ral perisylvian syndrome and eating epilepsy. Eur Neurol. 1999;42:241-3.
17. Kisli M, Yardim A. An interesting eating epilepsy case induced by bread eating. J Neurol Neurosci. 2018;9:276-8.
18. Lavizzari GS, Hess R. Sensory precipitation of epileptic seizures. Report on two unusual cases. Epilepsia. 1967;8:157-61.
19. Cirignotta F, Marcacci G, Lugaresi E. Epileptic seizures precipitated by eating. Epilepsia. 1977;18:445-9.
20. Dominizio R, Conte E, Puglielli C, Dominizio S, Margagni S, Pollice R, et al. Neonatal eating epilepsy: pathophysiological and pharmacologic aspects. Int J Immunopathol Pharmacol. 2016;19:697-702.
21. Gujjar AR, Jacob PC, Nandhagopal R, Al-Asmi A. Eating epilepsy in Oman: a case series and report on the efficacy of temporal lobectomy. Sultan Qaboos Univ Med J. 2013;13:156-61.
22. Cukiert A, Mariani PP, Burattini JA, Cukiert CM, Forster C, Baise C, et al. Vagus nerve stimulation might have a unique effect in reflex eating sei-zures. Epilepsia. 2010;51:301-3.
23. Ahuja GK, Mohandas S, Narayanaswamy AS. Eating epilepsy. Epilepsia. 1980;21:85-9.
24. Nagaraja D, Chand RP. Eating epilepsy. Clin Neurol Neurosurg. 1984;86:95-9.
25. Koul R, Koul S, Razdan S. Eating epilepsy. Acta Neurol Scand. 1989;80:78-80.
26. Loreto V, Nocerino C, Striano P, D’Aulos F, Boccella P, Striano S. Eating epilepsy. Heterogeneity of ictal semiology: the role of video-EEG moni-toring. Epileptic Disord. 2000;2:93-8.
27. Nakazawa C, Fujimoto S, Watanabe M, Tanaka M, Kageyama M, Ishi-kawa T, et al. Eating epilepsy characterized by periodic spasms. Neuro-pediatrics. 2002;33:294-7.
28. Seneviratne U, Seetha T, Pahirana R, Rajapakse P. High prevalence of eating epilepsy in Sri Lanka. Seizure. 2003;12:604-5.
29. Labate A, Colosimo E, Gambardella A, Leggio U, Ambrosio R, Loi M, et al. Reflex periodic spams induced by eating. Brain Dev. 2005;28:170-4.
30. Bae EK, Park H, Kim H, Jung KH, Lee ST, Chu K, et al. Ictal asystole and eating reflex seizures with temporal lobe epilepsy. Epilepsy Behav. 2011;20:404-6.
31. Patel M, Satishchandra P, Saini J, Bharath RD, Sinha S. Eating epilepsy: phenotype, MRI, SPECT and video-EEG observations. Epilepsy Res. 2013;107:115-20.
32. Jagtap S, Menon R, Cherian A, Baheti N, Ashalatha R, Thomas SV. “Eating” epilepsy revisited-an electro-clinico-radiological study. J Clin Neurosci. 2016;30:44-8.
33. Atalar AÇ, Vanlı-Yavuz EN, Yılmaz E, Bebek N, Baykan B. Reflex epi-leptic features in patients with focal epilepsy of unknown cause. Clin Neurol Neurosurg. 2020;190:105633.
34. Robertson WC Jr., Fariello RG. Eating epilepsy associated with a deep forebrain glioma. Ann Neurol. 1979;6:271-3.
35. Fiol ME, Leppik IE, Pretzel K. Eating epilepsy: EEG and clinical study. Epilepsia. 1986;27:441-5.
36. d’Orsi G, Demaio V, Minervini MG. Adult epileptic spasms: a clinical and video-polygraphic study. Epileptic Disord. 2007;9:276-83.
37. El Bouzidi K, Duncan S, Whittle IR, Butler CR. Lesional reflex epilepsy associated with the thought of food. Neurology. 2010;74:610-2.
38. Manyam SC, Kung DH, Rhodes LB, Newmark ME, Friedman DE. Unila-teral opercular lesion and eating-induced seizures. Epileptic Disord. 2010;12:309-13.
39. Sandhya M, Bharath RD, Panda R, Chandra SR, Kumar N, George L, et al. Understanding the pathophysiology of reflex epilepsy using simul-taneous EEG-fMRI. Epileptic Disord. 2014;16:19-29.
40. Koul R, Alshihi A, Mani R, Javad H, AlFutaisi A. Eating epilepsy or feeding epilepsy in an infant. Eur J Paediatr Neurol. 2014;18:409-12.
41. Sillanpää M, Schmidt D. Neonatal eating epilepsy: 50-year follow-up. Seizure. 2014;23:487-9.
42. Blauwblomme T, Kahane P, Minotti L, Grouiller F, Krainik A, Vercueil L, et al. Multimodal imaging reveals the role of γ activity in eating-reflex seizures. J Neurol Neurosurg Psychiatry. 2011;82:1171-3.
43. Kobayashi Y, Ishikawa N, Tani H, Fujii Y, Kobayashi M. Recurrence of epileptic spams as reflex seizures induced by eating: a case report and literature review. Neuropediatrics. 2016;48:119-22.
44. Chen YT, Sahaya K, Lee R, Hinkle J, Greenfield L. Eating epilepsy, a rare and under-recognized reflex epilepsy. Neurology. 2016;86:367-74.
45. Mimura N, Inoue T, Shimotake A, Matsumoto R, Ikeda A, Takahashi R. A case of epilepsy induced by eating or by visual stimuli of food made of minced meat. Rinsho Shinkeigaku. 2017;57:430-5.
46. Aldosari MM, Joswig H, Marti AS, Parrent A, Mirsattari SM. Non-lesional eating epilepsy with temporo-insular onset: a stereo-EEG study. Epilepsy Behav Rep. 2020;14:100368.