
Arsenic trioxide is highly cytotoxic to small cell lung carcinoma cells
Upload
independentCategory
view
2download
0
376
Sarcomatoid Carcinoma of the Lung Immunohistochemical and Ultrastructural Studies of 14 Cases
Jae Y. Ro, MD,* Jane L. Chen, MD,*,t ]in S. Lee, MD,S Aysegul A. Sahin, MD,* Nelson G. Ordhfiez, MD,* and Aiberfo G. Ayala, MD*
The authors retrospectively reviewed data regarding 14 patients with sarcomatoid carcinomas of the lung seen and treated at M. D. Anderson Cancer Center from 1955 to 1986. The following were the histologic criteria for in- clusion in the study: (1) the concurrent presence of malig- nant epithelial and sarcomatoid spindle cell components, and (2) positive immunoreactivity for antikeratin anti- body or ultrastructural demonstration of epithelial dif- ferentiation in sarcomatoid tumors in which the epithe- lial component was inconspicuous. For the sarcomatoid components, the most frequent pattern was malignant fi- brous histiocytoma, which was present in ten tumors. An unclassified sarcomatoid pattern was found in two cases and a fibrosarcomatous pattern in two remaining cases. Clinically, the median patient age was 59 years; 12 pa- tients were male and 2 were female; 13 were smokers and 1 used snuff. Three patients had Stage I, ten had Stage 111, and one had Stage IV disease. One patient with Stage I, seven with Stage 111, and one with Stage IV disease died of their carcinomas 2 to 26 months after diagnosis (median survival time 12 months). All patients who had lymph node metastases at presentation died of disease. The au- thors concluded the following: (1) patients with sarcoma- toid carcinoma of the lung usually presented at an ad- vanced stage; (2) lymph node metastasis, as with a usual carcinoma of the lung, is an important prognostic factor; and (3) for all lung tumors with a sarcomatoid pattern, especially a malignant fibrous histiocytoma pattern, ex- tensive samples should be obtained and immunoperoxi-
From the Departments of *Pathology and $Medical Oncology, The University of Texas M. D. Anderson Cancer Center, Houston, Texas
Supported in part by the Caduceus Foundation. tCurrent address: Department of Pathology, Halifax Medical
Center, 303 North Clyde Morris Boulevard, P. 0. Box Drawer 1990, Daytona Beach, FL 32015.
The authors thank Thomas Brooks, MT, for technical assistance and Bobbie A. Coleman for secretarial assistance.
Address for reprints: Jae Y. Ro, MD, Box 85, The University of Tcxas M. D. Anderson Cancer Center, 1515 Holcombe Boulevard, I louston, TX 77030.
Accepted for publication March 18, 1991.
dase or ultrastructural studies done to identify epithelial differentiation. Cancer 1992: 69:376-386.
Lung tumors in which a malignant mesenchymal com- ponent exists concurrently with a malignant epithelial component are uncommon neoplasms; these include pulmonary blastomas, polypoid endobronchial carci- nosarcomas, and sarcomatoid carcinomas. 1-3
Pulmonary blastoma is a distinctive clinicopatholo- gic entity in which the tumor resembles fetal lung tissue and consists of primitive epithelial and stromal ele- ments that may have derived from endodermal tra- cheobronchial b ~ d s . ~ , ~ Clinically, this tumor is located peripherally in the lung and occurs in patients in all age groups.6-8 Prognosis appears unpredictable but proba- bly is somewhat better than that for the usual broncho- genic carcinoma^.^-^
Polypoid endobronchial carcinosarcoma, as origi- nally defined, is also a distinctive clinicopathologic en- tity characterized by a central endobronchial location and associated with a good prognosis.' Histologically, the epithelial component of this tumor is usually a squamous cell carcinoma, and the mesenchymal compo- nent is described as resembling fibrosar~oma.'-'~
Pulmonary sarcomatoid carcinoma or spindle cell carcinoma is a biphasic malignant neoplasm showing a carcinomatous and spindle sarcomatoid component; the latter may show epithelial features on immunohisto- chemical or ultrastructural study, or b ~ t h . ' - ~ , ' ~
We retrospectively studied primary pulmonary sar- comatoid carcinomas diagnosed and treated at M. D. Anderson Cancer Center from 1955 to 1986. Our goals were as follows: (1) to define the clinicopathologic characteristics of these tumors; (2) to document the various histologic features that may be exhibited by these tumors; (3) to investigate whether the sarcoma- toid component of these neoplasms expresses epithelial or mesenchymal differentiation; and (4) to assess their biologic behavior.
Sarcomatoid Carcinoma of the Lung/Ro e t al. 377
Patients and Methods sections were stained with uranyl acetate and lead ci- trate.
The study group included 14 patients examined and treated at M. D. Anderson Cancer Center from 1955 to 1986. This group represented approximately 30% of the cases originally identified from M. D. Anderson Cancer Center Surpcal Pathology files as carrying diagnoses of primary pulmonary sarcoma, sarcomatoid carcinoma, pulmonary blastoma, carcinosarcoma, or sarcomatoid and biphasic mesothelioma. Original histologic sections and surgical pathology reports were reviewed in all cases. Follow-up information was obtained from the medical records.
Criteria for inclusion in the study were as follows: (1) cases in which the tumors expressed biphasic pat- terns of growth with carcinomatous and sarcomatoid elements, and (2) cases in which the sarcomatous pat- tern predominated without a recognizable epithelial component, in which case epithelial differentiation was established by positive immunoreactivity for keratin or evidence of epithelial differentiation at the ultrastruc- tural level. Patients whose medical records were incom- plete or who had pulmonary blastomas, endobronchial carcinosarcomas, or primary sarcomas were excluded from the study, as were patients in whom biphasic or sarcomatoid mesotheliomas were identified, based on a careful clinicopathologic evaluation.
Immunohistochemical studies were performed on formalin-fixed, paraffin-embedded sections from 12 of the 14 cases with the use of the avidin-biotin-peroxi- dase complex method of Hsu et ~ 1 . ’ ~ All primary anti- bodies were obtained commercially. The following were used: rabbit antihuman S-100 protein (1:BOO; Chemicon, El Segundo, CA), mouse monoclonal anti- body to keratin (AEl/AE3, 1:200; Hybritech, San Diego, CA), carcinoembryonic antigen (1:lOOO; Hybri- tech), epithelial membrane antigen (1:20; DAKO, Santa Barbara, CA), desmin (1:lO; DAKO), and vimentin (1:30; Labsystems, Chicago, IL). After incubation with the primary antibody, the sections were incubated with the appropriate biotin-labeled secondary antibody and avidin-biotin-peroxidase complex with the use of stan- dard avidin-biotin-peroxidase complex kits (Vector Laboratories, Burlingame, CA). The immunoperoxidase reaction was visualized by development in 3-amino-9- ethyl carbazole, and the sections were counterstained with Mayer’s hematoxylin. To verify the specificity of the immunoreaction, control tissue sections were stained in which the positive and negative reactions were known.
In five cases, ultrastructural studies were per- formed on tumor tissue fixed in 4% glutaraldehyde, postfixed in 1% osmium tetroxide, and routinely pro- cessed for electron microscopic examination. Ultrathin
Results
Sex and Age
Of the 14 cases that fulfilled the histologic criteria for inclusion in this study, 12 patients were men and 2 were women; 11 of these patients were white and 3 were black. The ages of the patients ranged from 43 to 78 years, with a median of 59 years at the time of diagnosis (Table 1).
Smoking History and Preexisting Pulmonary Disease
Smoking history was obtained for 13 patients. Among the 13 smokers, 3 were heavy users of cigarettes (greater than 100 pack-years) and 6 were moderate users (between 35 and 100 pack-years). In four pa- tients, the amount of cigarette usage was not recorded.
Five of the 14 patients had symptomatic emphy- sema or chronic bronchitis. One of these patients previ- ously had a ”coin” lesion in the contralateral lung as a result of ”valley fever,” but subsequent radiographic follow-up showed resolution of the lesion. The remain- ing patients had no known preexisting pulmonary dis- ease.
Clinical Presentation
The presenting symptoms included cough (either as a new symptom or a change in an existing cough pattern), blood-streaked sputum or frank hemoptysis, chest pain, shortness of breath, or weight loss, or a combina- tion of these complaints. Three patients had no pulmo- nary symptoms: one was evaluated for a supraclavicu- lar mass, and, in two patients, lung nodules were ob- served on routine chest roentgenograms performed for other reasons (cholecystitis and myocardial infarct).
Patients had symptoms from 0 to 1 2 months (me- dian duration, 2 months) before seeking medical atten- tion. In general, patients who had hemoptysis sought medical attention earlier than did those whose com- plaints were less specific ( eg . , cough, pain, and weight loss).
Clinical Staging
The diseases of the patients were staged according to the TNM system of the American Joint Committee on Cancer.15
Three patients had Stage I disease, ten had Stage I11 disease (six, Stage IIIA; four, Stage IIIB), and one had Stage IV disease (Table 1).
w U 0
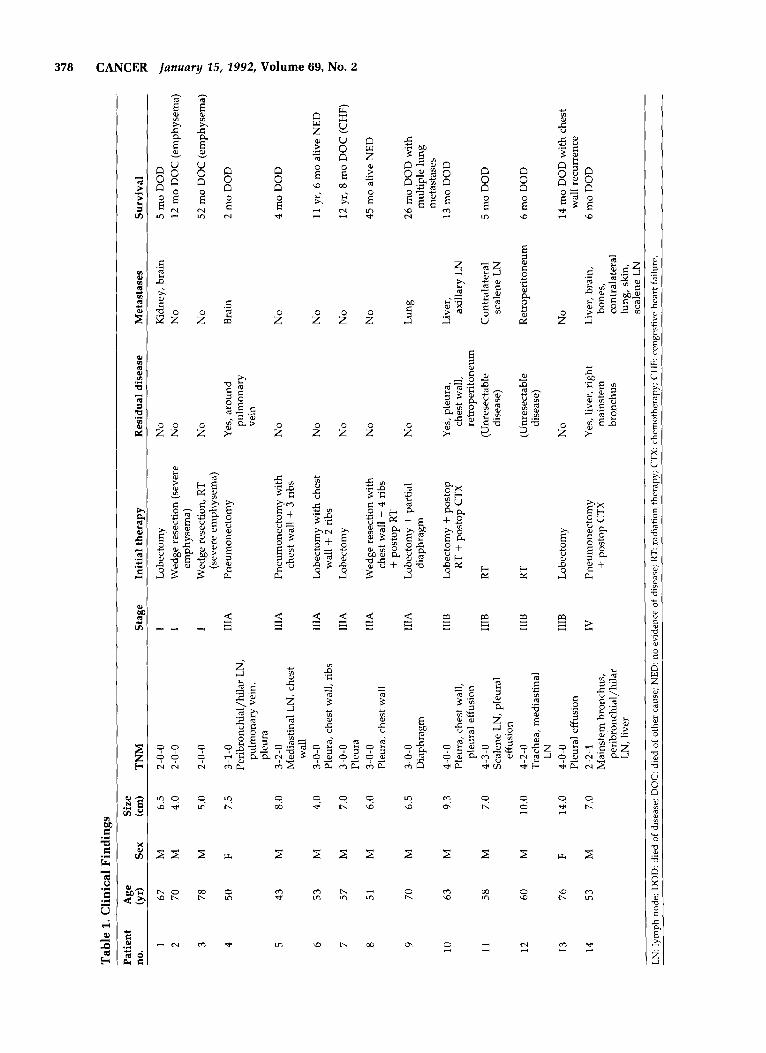
Table 1. Clinical Findings
no. (yr) Sex (cm) TNM Stage Initial therapy Residual disease Metastases Survival
.-
Patient Age Size 3 B
1 2
3
4
5
6
7
8
9
10
11
12
13
14
67 70
78
50
43
53
57
51
70
63
58
60
76
53
M M
M
F
M
M
M
M
M
M
M
M
F
M
6.5 4.0
5.0
7.5
8.0
4.0
7.0
6.0
6.5
9.3
7.0
10.0
14.0
7.0
2-0-0 2-0-0
1 1
1
IIIA
lllA
IllA
IIIA
IIIA
IIIA
IIIB
IIIB
IIIB
IIIB
IV
Lobectomy Wedge resection (severe
Wedge resection, RT
Pneumonectomy
emphysema)
(severe emphysema)
No No
Kidney, brain No 2
4
5 mo DOD 12 mo DOC (emphysema)
52 mo DOC (emphysema)
2 mo DOD v, CTI t4
v, h2
No No 2-0-0
3-1-0 Peribronchial/hilar LN,
pulmonary vein, pleura
3-2-0 Mediastinal LN, chest
wall 3-0-0 Pleura, chest wall, ribs
Pleura
Pleura, chest wall
3-0-0
3-0-0
Yes, around pulmonary vein
Brain
Pneumonectomy with chest wall + 3 ribs
No No 4 mo DOD
Q, (CI 11 yr, 6 mo alive NED z 0 12 yr, 8 mo DOC (CHF)
45 mo alive NED N
Lobectomy with chest
Lobectomy
Wedge resection with chest wall + 4 ribs + postop RT
Lobectomy + partial diaphragm
wall + 2 ribs No No
No
No
No
No
No 26 mo DOD with multiple lung metastases
13 mo DOD
3-0-0 Diaphragm
Lung
4-0-0 Pleura, chest wall,
pleural effusion
Scalene LN, pleural 4-3-0
effusion 4-2-0 Trachea, mediastinal
LN 4-0-0 Pleural effusion 2-2-1 Mainstem bronchus,
peribronchial/hilar LN, liver
Lobectomy + postop RT + postop CTX
Yes, pleura, chest wall, retroperitoneum
(Unresectable disease)
Liver, axillary LN
Contralateral scalene LN
RT 5 mo DOD
RT (Unresectable disease)
Retroperitoneum 6 mo DOD
Lobectomy No No 14 mo DOD with chest
6 mo DOD wall recurrence
Pneumonectomy + postop CTX
Yes, liver, right mains tem bronchus
Liver, brain, bones, contralateral luna, skin, scalvene LN
LN: lymph node; DOD: died of disease; DOC: died of other cause; NED: no evidence of disease; RT: radiation therapy; CTX: chemotherapy; CHF: congestive heart failure.

Sarcomatoid Carcinoma of the Lung/Ro et al. 379
Among patients with Stage I disease, one had me- tastases to the kidney and brain 3 months after lobec- tomy and died 2 months later. Two other patients died of other causes 12 and 52 months after diagnosis of the sarcomatoid carcinoma.
Of ten patients with Stage I11 disease, four had lymph node metastasis at presentation and five had distant metastases at the time of death. Seven patients, including four patients with lymph node metastases, died between 2 and 26 months after diagnosis. Of those seven, two had unresectable disease and received pal- liative radiation therapy and five had pneumonectomy or lobectomy, but two of these patients were known to have had residual disease after surgery. The remaining three patients with Stage I11 disease were alive without disease or died of other causes; all three had partially circumscribed subpleural tumors that had invaded the chest wall or diaphragm locally, but none had lymph node metastases. Follow-up evaluations were per- formed for these three patients at 45 months; 11 years, 6 months; and 12 years, 8 months, respectively.
One patient with Stage IV disease died of wide- spread metastatic disease 6 months after pneumonec- tomy.
Gross Pathology
All tumors were primarily intraparenchymal lesions. In six cases, the tumors were described as partially or wholly circumscribed. The cut surfaces were white, tan, gray, or yellow. Necrosis and hemorrhage were grossly observed in approximately half the specimens, includ- ing two that showed massive necrosis, resulting in cavi- tated lesions. Tumor consistency varied from soft and fleshy to firm and hard.
Histology
Among the 14 tumors, 12 had an identifiable epithelial component on the routine microscopic examination of hematoxylin and eosin-stained sections. Two tumors had only a malignant fibrous histiocytoma (MFH)-like sarcomatoid component in which epithelial differentia- tion was demonstrable by ultrastructural and immuno- histochemical methods.
In the 12 instances of epithelial patterns, adenocar- cinoma occurred in 4 cases, squamous cell carcinoma in 3 cases, combined adenocarcinoma and squamous carci- noma in 2 cases, and large cell undifferentiated carci- noma in 3 cases.
The sarcomatoid portions of the 14 tumors were composed predominantly of spindle cells and, occa- sionally, round or epithelioid cells. They had three ma- jor patterns of sarcomatoid growth: an MFH-like pat-
tern, a fibrosarcomatous pattern, and an unclassified sarcomatous pattern. In general, there tended to be a mixture of patterns of spindle cell proliferation, so that categorization was based on the predominant pattern. The most common histologic pattern exhibited by the tumor was MFH-like; this was present in ten tumors (Fig. 1). This pattern was similar to that of the soft tissue counterpart, characterized by a storiform pattern of pro- liferation of short fascicles of plump spindled cells showing cellular pleomorphism with occasional giant tumor cells. The cytoplasm of the spindle cells tended to be eosinophilic and abundant. In two cases, there was a fibrosarcomatous pattern, which, like its soft tissue counterpart, was characterized by a proliferation of rather uniform, spindled cells with a herringbone or fascicular pattern of growth (Fig. 2). When no special characterization could be determined in the pattern of spindle cell proliferation, it was categorized as unclassi- fied. The remaining two cases were in this category; in one of these cases, the tumor had a prominent myxoid appearance. There were no heterologous components in any of these tumors. In each case, the carcinomatous and sarcomatoid components directly abutted on each other (Fig. 3), and often there were areas of blending between them (Fig. 4).
Immunohistochemical Studies
Immunohistochemical studies were performed in 12 cases (10 had identifiable carcinoma components and 2 had only a sarcomatoid component). Results of staining by the sarcomatoid component are shown in Table 2. There was no staining for antibodies to desmin, 5-100 protein, or carcinoembryonic antigen in any of the 12 cases examined. In 10 of the 12 cases, the sarcomatous portion showed immunoreactivity for vimentin. Seven tumors showed diffuse reactivity, but three tumors showed only focal staining. Nine of the 12 cases (7 bi- phasic and 2 spindle tumors) showed immunoreactivity for keratin (Fig. 5). Of those, seven tumors (five with a biphasic and two with a spindle component only) had dual expression of keratin and vimentin. Four of the cases that showed keratin staining also had positive re- actions for epithelial membrane antigen.
Ultrastructural Findings
In four of the five cases in which ultrastructural studies were performed, there was evidence of epithelial dif- ferentiation in the sarcomatoid areas. In these cases, the tumor cells were closely apposed, joined by well- formed desmosomal-type cell junctions (Fig. 6). Some of the spindle cells showed scattered cytoplasmic bun-

380 CANCER January 25, 2992, Volume 69, No. 2
Figure 1. (Top) The most common sarcomatoid component is the malignant fibrous histiocytomatous pattern. Histologically, it is indistinguishable from its soft tissue counterpart. At the right side of the figure, alveolar spaces are discemable (H & E, X100). (Bottom) A higher magnification of the sarcomatoid component (H & E, X250).
dles of tonofilaments (Fig. 7). In the remaining case, the tumor cells in the sarcomatoid areas appeared to be joined by primitive junctions. The cytoplasm contained aggregates of intermediate filaments, dilated rough en-
doplasmic reticulum, and a moderate number of mito- chondria. Immunohistochemical studies demonstrated reactivity for keratin in the sarcomatoid components of the tumor.

Sarcomatoid Carcinoma of the Lung/Ro et al. 381
Figure 2. A fibrosarcomatous pattern is characterized by a herringbone or fascicular pattern of growth. At the left side of the figure, a focus of squamous carcinoma is seen (H & E, original magnification X100).
Discussion
Primary sarcomatoid carcinomas of the lungs are un- usual malignant neoplasm^.'-^,'^ Similar biphasic tu- mors have been found in the genitourinary tract,16-19 esophagus,20,21 upper respiratory t r a ~ t , ~ ~ , ~ ~ * ~ ~ skin,24 and b r e a ~ t . ~ ~ , ~ ~ The complex issue of histogenesis of these tumors is a point of ongoing debate with no clear-cut answers derivable from ultrastructural or immunohisto- chemical studies. Thus, although some have argued that these biphasic tumors result from independent cel- lular origins of malignant epithelial and malignant mes- enchymal ~ e l l s , ~ ~ , ~ ~ others have proposed that such tu- mors are derived from a common clone of anaplastic cell^.^^^^^ These anaplastic cells can and do express epi- thelial and mesenchymal differentiation simulta- neously, as surmised from concurrent antikeratin and antivimentin immunoreactivity and also from dual pro- liferation of histologically recognizable epithelial and spindle cell^.',^,'^,^^ An example of this would be the cutaneous spindle cell squamous c a r c i n ~ m a . ~ , ~ ~
In this report, we have not addressed the issue of histogenesis. Although we believe that pulmonary blastoma is a separate clinical pathologic entity to be distinguished from sarcomatoid carcinoma, we could not differentiate the endobronchial carcinosarcomas from intraparenchymal sarcomatoid carcinomas his- tologically. At present, we favor the idea (as have others9-12) that these two are similar tumors and that
the differences in biologic outcome probably are related to the location of the tumor, ease of early detection, and resectability .
Our 14 cases of pulmonary sarcomatoid carcinoma all had patient profiles similar to those for bronchogenic carcinoma with respect to age, sex, smoking history, and clinical p r e s e n t a t i ~ n . ~ ~ , ~ ~
Preoperative radiographic findings most often showed nonspecific mass lesions. Not unexpectedly, the concurrent findings of unresolved pneumonia, pleural effusion, or hilar enlargement herald poor prog- nosis. The only radiographic sign associated with good prognosis was the finding of a peripheral coin lesion in three patients. Although two of these three had Stage 111 disease by virtue of chest wall invasion, both are alive with no evidence of disease 45 months, and 11 years 6 months after en bloc chest wall resection.
A preoperative histologic diagnosis of sarcomatoid carcinoma was not made by cytologic examination or percutaneous needle biopsy in any of these cases. Four of 11 sputum cytologic samples had malignant cells. Five of 11 bronchial washing, brushing, and transbron- chial biopsy specimens showed malignancy. For four of nine cases in which percutaneous fine-needle aspira- tion biopsies were performed, results yielded diagnoses of squamous cell carcinoma, non-small cell carcinoma, malignant neoplasm (possible giant cell carcinoma ver- sus unclassified sarcoma), and large cell undiff eren- tiated carcinoma with squamous differentiation. In the remaining five cases, the biopsy results were nondiag- nostic for malignancy.
Figure 3. An adenocarcinoma is present on the top, abutting directly with a spindle sarcomatoid component (H & E, original magnification X 100).

382 CANCER January 25, 2992, Volume 69, No. 2
Figure 4. Large cell undifferentiated carcinoma intermingled with a sarcomatoid component. There are areas of blending between them (H & E, Xl00).
The patients tended to have locally aggressive dis- months of surgery (median survival length, 4.5 months). Of the six patients who had pleural, chest wall, or diaphragmatic involvement but did not have hilar, peribronchial, or mediastinal lymph node involve- ment, two are alive with no evidence of disease and one died of other causes. These results suggest that patients
ease at the time of diagnosis, accounting for the high proportion of patients in whom Stage I11 disease was diagnosed.
Of the four patients with hilar or mediastinal lymph node metastases, all died of disease within 2 to 6
Table 2. Pathologic Features With Their Immunohistochemical and Ultrastructural Findings on Spindle Components
Patient no. Carcinoma Sarcoma K V EMA EM
Spindle cell components
1 Adeno MFH + + - No epithelial features ND 2 LCU MFH
3 Adeno + Sq MFH ND ND Epithelial differentiation
5 - MFH + + + Epithelial differentiation 6 Squamous MFH ND ND
ND 7 Squamous Fibro + ND 8 LCU MFH + + Epithelial differentiation 9 LCU Unclass ND 10 Adeno MFH + +
11 Adeno + Sq MFH + + + ND 12 - MFH + + + Epithelial differentiation
ND 13 Adeno MFH 14 Squamous Unclass + + + ND
- + -
- - 4 Adeno Fibro +
- -
-
- + -
-
- + -
K: keratin; V. vimentin; EMA epithelial membrane antigen; EM: electron microscopy; Adeno: adenocarcinoma; LCU: large cell undifferentiated; Sq: squamous; ND: not done; MFH: malignant fibrous histiocytoma; Fibro: fibrosarcoma; Unclass: unclassified sarcoma.

Sarcomatoid Carcinoma of the Lung/Ro et al. 383
Figure 5. (Top) Keratin immunostaining shows a diffuse, strong reaction in both epithelial tumor cell nests (right upper corner) and the spindle sarcomatoid component. (Bottom) A higher magnification of the keratin immunostaining in the sarcomatoid area (ABC immunostaining: top, X100; bottom, X250).
with Stage I11 disease with hilar, peribronchial, or me- diastinal lymph node metastases fare considerably worse than do patients whose disease is classified as Stage I11 by virtue of pleural, chest wall, or diaphrag- matic involvement alone.
This series of patients was too small to allow effec- tive evaluation of the efficacy of alternate or adjuvant modes of therapy. The initial mode of treatment was radiation therapy in three patients, One patient with Stage I disease had a wedge resection only because of

384 CANCER January 15,1992, Volume 69, No. 2
Figure 6. Spindle sarcomatoid tumor cells are closely apposed and have a well-formed, desmosomal-type cell junction (orignal magnification X16,500).
poor pulmonary function, This patient died of respira- tory failure 52 months after radiation therapy, appar- ently without disease recurrence. Two patients with unresectable Stage I11 disease had palliative radiation therapy. Both died of their disease 5 months and 6 months later, respectively. Postoperative radiation ther- apy (5000-cGy total dose in 25 fractions) was adminis-
tered to one patient who had a wedge resection of the lung with en bloc chest wall resection. This patient is alive without evidence of disease 45 months after sur- gery. Another patient had postoperative radiation ther- apy followed by chemotherapy but died 13 months later of recurrent and metastatic disease. Postoperative chemotherapy was administered to another patient
Figure 7. Some of the spindle tumor cells show cytoplasmic bundles of tonofilaments (original magnification x20,000).

Sarcomatoid Carcinoma of the Lung/Ro et al. 385
who had known liver metastasis at the time of pneu- monectomy. That patient died 6 months later with wide- spread metastatic disease.
Histologically, most of these tumors were biphasic. The epithelial elements were adenocarcinoma, squa- mous cell carcinoma, or large cell undifferentiated carci- noma. The sarcomatoid component predominated in these tumors, with the MFH-like pattern being the most frequent type. Immunohistochemical studies showed epithelial differentiation by the sarcomatous compo- nent in 75% of the cases, as evidenced by immunoreac- tivity against keratin. Electron microscopically, epithe- lial differentiation was demonstrated in four of five cases.
There are several possible explanations for the ab- sence of epithelial differentiation in the spindle cell components observed on immunohistochemical studies or electron microscopic examination. First, the epithe- lial characteristics can be presented focally, and the neg- ative result may reflect a sampling error. Second, all spindle sarcomatoid components may not be of epithe- lial The last possibility suggests that some of these tumors may be true carcinosarcomas. A recent article by Humphrey et al.’ proposed that pulmonary carcinomas exhibiting evidence of epithelial differen- tiation in a sarcomatoid component should be termed spindle cell carcinomas and that biphasic tumors ex- hibiting mesenchymal differentiation ( i e . , neoplastic bone, cartilage, or striated muscle) or lacking epithelial differentiation by light microscopic examination, immu- nocytochemical studies, and electron microscopic exam- ination be classified as carcinosarcomas. Despite this distinction, those investigators indicated that this dif- ferentiation ultimately may be unnecessary because these two tumors may represent different points along a morphologic and biologic continuum. Nonetheless, Farrow ef al.” used the term sarcomatoid carcinoma to describe biphasic renal tumors exhibiting carcinoma- tous and sarcomatoid components on conventional light microscopic examination and suggested that, given the incomplete state of knowledge about this un- usual malignancy, ”sarcomatoid” is currently an ap- propriate term. We subscribe to their opinion and use the term sarcomatoid carcinoma for biphasic tumors with carcinoma and sarcomatoid components in every
It is difficult to determine whether spindle cells are truly of mesenchymal origin or are merely a sarcoma- toid transformation of an epithelial component. In ad- dition, it is our opinion, as well as that of others, that these tumors, whether truly carcinosarcoma or spindle cell sarcomatoid carcinoma, behave in the same
As discussed earlier, we have not at- tempted to address the question of these tumors’ histo- genesis using immunohistochemical data; rather, we
organ, 1 6 , 1 7 3
way.1,16,17.20,33-36
have used immunohistochemical methods solely as helpful aids in diagnosis. Some of the sarcomatoid carci- nomas showed coexpression of keratin and vimentin. This coexpression has been demonstrated in carcino- sarcomas of the uterus,34 upper aerodigestive thyroid,37 and urinary bladder.16 It is well known that the expression of vimentin is not specific for neoplasms with mesenchymal differentiation but in fact can be found in benign and malignant epithelial neoplasms and in normal epithelial cells on occasion.
In conclusion, pulmonary sarcomatoid carcinoma is a variant of lung carcinoma showing frequent local in- vasion and widespread metastasis. Histologically, the tumor is recognized by a biphasic population of carci- nomatous and sarcomatous cells. The most common sarcomatoid pattern resembles soft tissue MFH. In a primary malignant pulmonary neoplasm showing only spindle cell proliferation, we suggest extensive sam- pling of the tumor with ancillary studies to evaluate epithelial differentiation. Awareness of pulmonary sar- comatoid carcinoma can lead to coordinated future stud- ies to better define the biologic characteristics of this entity so that the most beneficial course of therapy can be determined and used.
References
1.
2.
3.
4. 5.
6.
7.
8.
9.
10.
11.
12
13
Humphrey PA, Scroggs MW, Roggli VL, Shelburne JD. Pulmo- nary carcinomas with a sarcomatoid element: An immunocyto- chemical and ultrastructural analysis. Hum Pathol 1988; 19:155- 165. Battifora H. Spindle cell carcinoma: Ultrastructural evidence of squamous origin and collagen production by the tumor cells. Cancer 1976; 37:2275-2282. Addis BJ, Corrin B. Pulmonary blastoma, carcinosarcoma and spindle-cell carcinoma: An immunohistochemical study of kera- tin intermediate filaments. ] Pathol 1985; 147:291-301. Barnard WG. Embryoma of lung. Thorax 1952; 7:299-301. Spencer H. Pulmonary blastoma. ] Pathol Bacteriol 1961;
Francis D, Jacobsen M. Pulmonary blastoma. Curr Top Pathol 1983; 73~265-294. Jacobsen M, Francis D. Pulmonary blastoma: A clinicopatholo- gical study of eleven cases. Acta Pathol Microbiol Scand [ A ] 1980;
Roth ]A, Elguezabal A. Pulmonary blastoma evolving into car- cinosarcoma. Am ] Surg Pathol 1978; 2:407-413. Razzuk MA, Urschel HC, Race GT, Arndt JH, Paulson DL. Car- cinosarcoma of the lung. ] Thorac Cardiouasc Surg 1971; 61:541- 546. Chaudhuri MR. Bronchial carcinosarcoma. ] Thorac Cardiouasc Surg 1971; 61:319-323. Jenkins BJ. Carcinosarcoma of the lung: Report of a case and review of the literature. Thorac Cardiouasc Surg 1968; 55:657- 662. Moore TC. Carcinosarcoma of the lung. Surgery 1961; 505386- 893. Love GL, Daroca PJ, Bronchogenic sarcomatoid squamous cell carcinoma with osteoclast-like giant cells. H i m Pathol 1983;
82:161-165.
88:151-160.
14:1004-1006.
386 CANCER January 25, 2992, Volume 69, No. 2
14.
15.
16.
17.
18.
19.
20.
21.
22.
23.
24.
25.
Hsu S-M, Raine L, Fanger H. Use of avidm-biotin peroxidase complex (ABC) in immunoperoxidase techniques: A comparison between ABC and unlabeled antibody (PAP) procedures. J His- tochem Cytochem 1981; 29:577-580. Mountain CF. A new international staging system for lung cancer. Chest 1986; (Suppl) 89:225-233. Ro JY, Ayala AG, Wishnow KI, Ord6iiez NG. Sarcomatoid blad- der carcinoma: Clinicopathologic and immunohistochemical study on 44 cases. Surg Pathol 1988; 1:359-374. Ro JY, Ayala AG, Sella A, Samuels ML, Swanson DA. Sarcoma- toid renal cell carcinoma: A clinicopathologic study of 42 cases. Cancer 1987; 59:516-526. Young RH. Carcinosarcoma of the urinary bladder. Cancer 1987;
Farrow GM, Harrison EG, Utz DC. Sarcomas and sarcomatoid and mixed malignant tumors of the kidney in adults: Part 111. Cancer 1968; 22:556-563. Zarbo RJ, Crissman JD, Venkat H, Weiss MA. Spindle-cell carci- noma of the upper aerodigestive tract mucosa: An immunohis- tologic and ultrastructural study of 18 biphasic tumors and com- parison with seven monophasic spindle-cell tumors. Am J Surg
Du Boulay CEH, Isaacson P. Carcinoma of the esophagus with spindle cell features. Histopathology 1981; 5:403-414. Piscioli F, Aldovini D, Bondi A, Eusebi V. Squamous cell carci- noma with sarcoma-like stroma of the nose and paranasal si- nuses: Report of two cases. Histopathology 1984; 8:633-639. Batsakis JG. “Pseudosarcoma” of the mucous membranes in the head and neck. J Laryngol Otol 1981; 95:311-316. Hams M. Spindle cell squamous carcinoma: Ultra-structural ob- servations. Histopathology 1982; 6:197-210. Bauer TW, Rostock RA, Eggleston JC, Baral E. Spindle cell carci- noma of the breast: Four cases and review of the literature. Hum
59~1333-1339.
Pathol 1986; 10~741-753.
Pathol 1984; 15:147-152.
26.
27.
28.
29.
30.
31.
32.
33.
34.
35.
36.
37.
Kaufman MW, Marti JR, Gallager HS, Hoehn JL. Carcinoma of the breast with pseudosarcomatous metaplasia. Cancer 1984;
Foulds L. The histological analysis of tumors. A critical review. A m J Cancer 1940; 39:l-24. Virchow R. In Die Krankhaften Geschwulste, vol. 2. Berlin: Au- gust Hirschwald, 1864-1865; 181 (cited by Humphrey et al.
Drury RAB, Stirland RM. Carcinosarcomatous tumours of the respiratory tract. J Pathol Bacteriol 1959; 77:543-554. Saphir 0, Vass A. Carcinosarcoma. A m J Cancer 1938; 33:331- 361. Minna JD, Pass H, Glastein E, Ihde DC. Cancer of the lung. In: DeVita VT, Hellman S, Rosenberg SA, eds. Cancer. Principles and Practice of Oncology, ed. 3. Philadelphia: JB Lippincott,
Auerbach 0, Garfinkel L, Parks VR. Histologic type of lung cancer in relation to smoking habits, year of diagnosis and sites of metastases. Chest 1975; 67:382-387. Ellis GL, Langloss JM, Heffner DK, Hyams VJ. Spindle-cell carci- noma of the aerodigestive tract: An immunohistochemical analy- sis of 21 cases. A m J Surg Patho[ 1987; 11:335-342. Geisinger KR, Dabbs DJ, Marshall RB. Malignant mixed miillerian tumors: An ultrastructural and immunohistochemical analysis with histogenetic considerations. Cancer 1987;
Kakizoe S, Kojiro M, Nakashima T. Hepatocellular carcinoma with sarcomatous change: Clinicopathologic and immunohisto- chemical studies of 14 autopsy cases. Cancer 1987; 59:310-316. Shannon RL, Grignon DJ, Ro JY, Ord6iiez NG, Mackay 8, Ayala AG. Sarcomatoid carcinoma of the prostate (Abstr). Lab lnvest 1989; 60:87. LiVolsi VA, Brooks JJ, Arendash-Durand B. Anaplastic thyroid tumors: Immunohistology. A m J Clin Pathol 1987; 87:434-442.
53: 1908-1917.
Hum Pathol 1988; 191155-165).
1989; 591-705.
59:1781-1790.
Copyright © 2022 FDOKUMEN




















