Lifecycle Series: Anthropometrics Transcript - Minnesota ...
Upload
independentCategory
view
1download
0
www.elsevier.com/locate/jpedsurg
Journal of Pediatric Surgery (2007) 42, E23–E29
t(11;19)(q21;p12~p13.11) and MECT1-MAML2 fusiontranscript expression as a prognostic marker in infantilelung mucoepidermoid carcinomaAlexandre Serraa,⁎, Hans K. Schackertb, B. Mohrc, Anja Weised,Thomas Liehrd, Guido Fitzea
aDepartment of Pediatric Surgery, University of Dresden, D-01307 Dresden, GermanybDepartment of Surgical Research, University of Dresden, D-01307 Dresden, GermanycDepartment of Internal Medicine, University of Dresden, D-01307 Dresden, GermanydInstitute of Human Genetics and Anthropology, University of Jena, Germany
⁎ Corresponding author. Tel.: +49 351E-mail address: alexandre.serra@uni
0022-3468/$ – see front matter © 2007doi:10.1016/j.jpedsurg.2007.04.031
AbstractBackground: Primary pulmonary mucoepidermoid carcinomas (MECs) are the third most frequentpulmonary malignant neoplasm in children, and new molecular diagnostics may prove useful indetermining the biologic course of such tumors.Methods: We analyzed the presence of a balanced t(11;19)(q21; p12~p13.11) and the MECT1-MAML2fusion transcript in a 9-year-old girl with mucoepidermoid lung carcinoma using conventionalcytogenetics, fluorescence in-situ hybridization, spectral karyotyping, high-resolution multicolorbanding, and reverse transcriptase–polymerase chain reaction.Results: We confirmed the t(11;19)(q21; p12∼p13.11) in the tumor. Molecular analysis of thetranslocation breakpoint confirmed the presence of the MECT1-MAML2 fusion transcript postulated tolead to an altered cyclic adenosine monophosphate signaling in MEC.Conclusions: Our data concur with previously reported cases, in which t(11;19) appears to be theprimary chromosomal aberration for pulmonary MEC in children, and that the MECT1-MAML2 fusiontranscript is associated with a better prognosis in MEC tumors.© 2007 Elsevier Inc. All rights reserved.
Index words:
Mucoepidermoidlung carcinoma;Cytogenetics;t(11;19)(q21;p12∼p13.11);
MECT1-MAML2fusion transcript
Mucoepidermoid carcinomas (MECs) may arise frommucinous cells in a wide range of different organs and arecharacterized by the presence of squamous, mucin-producing,and intermediate cells in variable proportions. Most MECsoccur in the major salivary glands, accounting for approxi-mately 21% to 29%ofmalignant salivary neoplasias [1,2]. Theremainder arise in minor salivary glands of the buccal mucosa,
458 4901; fax: +49 351 458 5343.klinikum-dresden.de (A. Serra).
Elsevier Inc. All rights reserved.
lips, retromolar region, tongue, and lung. Primary pulmonaryvariants are very rare in adults, whereas in children, theyconstitute approximately 9% of all primary malignant lungneoplasms, hence representing the third most frequent primarymalignancy of the lung in this age group [3,4].
The present study investigated cytogenetic and moleculargenetic abnormalities in an infantile MEC of the lung andidentified the newly described fusion transcript (andpotential oncogene), MECT1-MAML2 (MECT1, MEC trans-located 1, also known as transducer of regulated cyclicadenosine monophosphate [cAMP] response element–

E24 A. Serra et al.
binding 1 [CREB1] [TORC1] or Warthin and mucoepider-moid tumor translocation partner gene 1 [WAMPT1];MAML2, mastermindlike 2), which has been shown toencode a fusion transcript that acts as a coactivator of thecAMP signaling pathway and whose expression has beenlinked to the prognosis of MEC in children [5-7].
1. Materials and methods
1.1. Clinical summary
The patient was a 9-year-old girl who had a 1-year historyof persistent and therapy-refractory, low-grade microcyticanemia, as well as chronic fatigue and recurrent upper airwayinfections. Initial chest radiographs showed a lobar pneu-monia of the right middle lobe, unresponsive to antibiotictherapy. A thorax computed tomographic scan revealed aheterogeneous mass of the right middle lobe compressing thebronchial system. The histopathologic evaluation of biopsiestaken during the fibrobronchoscopy established the diag-nosis of a low-grade malignant MEC. The patient underwentsurgical resection of the right lower and middle lobes, andthe surgical specimen revealed a yellowish tumor 4 × 4 ×4 cm in size. Regional lymph nodes were not affected atsurgery. Viable tumor samples were processed for routinehistopathologic examination as well as for cell culture andcytogenetic and molecular genetic analyses. The post-operative course was uneventful, and in the follow-up,there were no signs of metastases or local recurrence [8].
1.2. Histopathology
For histopathologic examination, formalin-fixed andparaffin-embedded sections were stained with H&E. Addi-tional immunohistochemical studies (data not shown) wereperformed using antibodies against cytokeratin (CK)5/6(DAKO, Glostrup, Denmark), CK13 (PROGEN, Heidel-berg, Germany), CK14 (Novocastra, Newcastle Upon Tyne,United Kingdom), and CK 8/18 (Novocastra), according tostandard protocols.
1.3. Cell cultures
Immediately after the surgical resection of the carcinoma,tumor samples were isolated and processed according tostandard protocols. In brief, viable tumor samples wereminced into small fragments and digested in a collagenasepreparation (250 U/mL) for 1 hour at room temperature. Thecell suspension was then washed twice in Eagle ModifiedEagle Medium (MEM) and seeded in 25-cm2 flasks with thegrowth medium, 500 mL of which contained DulbeccoMEM/Ham's F12 (1:1; Invitrogen GmbH, Karlsruhe,Germany) supplemented with 10% inactivated fetal calfserum, 2 mmol/L L-glutamine, 2% nonessential amino acids
100× (Invitrogen GmbH, Germany), 25 μg/mL progesterone(Clonetics, Cambrex, Belgium), 50 mg/mL transferrin(Invitrogen), 0.5 mL GA-1000 gentamicin sulfate and0.5 mL amphotericin B (Clonetics), 10 μg/mL humanepidermal growth factor (Clonetics), and 10 mg/mL insulin(Clonetics). Cells were further grown in RPMI-1640Medium (Invitrogen) supplemented with 15% inactivatedfetal calf serum, 2 mmol/mL L-glutamine, 100 U/mLpenicillin, and 0.1 mg/mL streptomycin. For cytogeneticanalyses, cells were harvested after short-term culture andafter long cultivation for long-term culture. After colchicineexposure, cells were subjected to hypotonic treatment andfixation in methanol/acetic acid.
1.4. Chromosomal analyses
Freshly prepared chromosome preparations were bandedusing GTG- and GAG-banding techniques as describedelsewhere [9-11]. Metaphases were fully karyotyped accord-ing to Mitelman [12]. Hybridizations were done asrecommended by the manufacturer with the following DNAprobes: SkyPaint probe mixture (Applied Spectral Imaging,Migdal HaEmek, Israel), whole chromosome painting (WCP)19 (chromosome paints DNA probe; Abbott GmbH & CoKG, Wiesbaden, Germany), and LSI IGH/CCND1 (hybri-dizes to band 14q32 and to band 11q13; Abbott GmbH & CoKG). For the analysis of the results, a Spectra Cube Systemequipped with the software Skyview 1.5 (Applied SpectralImaging, GmbH, Mannheim, Germany) was used.
High-resolution multicolor-banding (MCB) based onmicrodissection-derived region-specific libraries for chro-mosomes 2, 10, 11, 14, and 19 was performed as previouslydescribed, including methods and MCB probe sets [13]. Awhole chromosome painting probe for chromosome 11 wasused additionally in one MCB experiment, according toSenger et al [14]. Metaphase spreads were analyzed using afluorescence microscope (Axioplan 2 mot, Carl-Zeiss Co,Jena, Germany) equipped with appropriate filter sets todiscriminate among a maximum of 5 fluorochromes and thecounterstain diaminophenylindol. Image capturing andprocessing were carried out using an Isis multicolorfluorescent in-situ hybridization (mFISH) imaging system(MetaSystems, Altlussheim, Germany) for MCB.
1.5. RNA isolation/reversetranscriptasepolymerase chain reaction
Messenger RNA (mRNA) was obtained directly fromperipheral blood leukocytes of the patient, from pellets fromthe tumor and control cell cultures, and from fresh tumor tissue(Prof Füzesi, Göttingen, Germany) using standard techniquesand the QuickPrep micro-mRNA Purification Kit fromAmersham Bioscience (Freiburg, Germany). ComplementaryDNAwas generated from mRNA by a reverse transcriptase–polymerase chain reaction (RT-PCR) approach, and specific

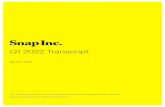
Fig. 1 Hematoxylin-eosin staining of the tumor. The pulmonaryMEC arose underneath the intact bronchial epithelium and showedsquamous, mucin-producing, and intermediate cells consistent witha grade 1 MEC.
E25t(11;19) in a child’s lung mucoepidermoid in carcinoma
cDNA fragments of the target genes were amplified using thecDNA primer pairs described. Reverse transcriptase–poly-merase chain reaction was conducted following standardtechniques using the following parameters: MgCl2, 1.5 μL;deoxynucleotide triphosphate (dNTP), 3 μL; Taq polymerase,0.1 μL; primers, 1.0 μL; target cDNA, 2.0 μL; and doubledistilled water (ddH2O), 13.9 μL. Data from RT-PCR sampleswere analyzed with a phosphorimager and the valuesnormalized to GAPDH. Polymerase chain reaction productswere gel-purified and sequenced using an automated ALFDNA sequencer (Amersham Pharmacia Biotech, Freiburg,Germany), and results were analyzed by basic local alignmentsearch tool (BLAST) search (http://www.ncbi.nlm.nih.gov/BLAST). All results were confirmed by repeated testing.
The following primers were selected:
MECT1: 5′-CAATCAGAAGCAGGCGGAGGAGAC-3′(sense)5′-GAGCGGGGAGGGGAAGTGGATGTT-3′(antisense)
MAML2: 5′-CACCGCCCCCACCAGACTATC-3′ (sense)5′-GGCCGGCCTTGTACATGTAGTTAG-3′(antisense)
MECT1-AML2 fusion transcript: 5′-CAATCAGAAG-CAGGCGGAGGAGAC-3′ (sense)5 ′ -CATGGCTGGGTGCGGGTTGTTA-3 ′(antisense)
Genbank Accession numbers:MECT1, AY040323;MAML2,AY040322;MECT1-MAML2 fusion transcript, AY040324.
2. Results
Gross examination of the surgical specimen revealed a40 × 40 × 40-mm large exophytic, yellowish white tumor in
the main bronchus of the midlobe of the right lung withmultifocal, subpleural chronic retention pneumonia. Micro-scopically, the tumor was composed of mucus-producingcells, intermediate cells, and small foci of squamous cellsconsistent with a grade 1 MEC (Fig. 1). Lymph nodemetastases were not detected. The postoperative tumorclassification was pT1, pN0, pMx, R0 (according to UnionInternationale Contre Le Cancer, 2002).
Conventional chromosomal analysis of tumor cellsrevealed the following karyotype: 43-46,XX,t(11;19)(q21;p13) [cp10]/41-46,XX [cp8].
Further molecular-cytogenetic techniques using conven-tional G-banding, spectral karyotyping, and MCB (Fig. 2) ontumor cells from long-term cell culture revealed a complexvariant of the classic t(11;19) with a pericentric inversion of11p11.2q21, interstitial deletion of 11q21q23.3, and terminaldeletion of 11p11.2pter, but a retained translocation betweenbands 11q21 and 19p13, resulting in the followingkaryotype: 44-45,XX.ish,der(2)t(2;14)(?q1?;q?11)[2],?+del(10)(pter-Nq25.2:),t(11;19) (11qter-N11q23.3::11p11.2-N11q21::19p12-N19pter),inc[cp6].
Furthermore, the long-term cultured cells had thefollowing additional chromosomal aberrations, which werenot detected in the fresh tumor samples:
1. A supernumerary deleted copy of chromosome 10, del(10)(pter-Nq25.2:).
2. An unbalanced translocation between chromosomes 2and 14, der(2)t(2;14)(?q1?;q?11), which was onlydetected in 2 metaphases.
Spectral karyotyping and MCB analyses of the controlcell line NCI-H292 also revealed the translocation t(11;19)[karyotype, t(11;19)(11qter-N11q23.3::11p11.2-N11q21::19p12-N19pter], which was genetically identical tothe translocation detected in the tumor (Fig. 3).
An RT-PCR showed the expression of both MECT1 andMAML2 in peripheral leukocytes from the patient(Fig. 4A). An RT-PCR on total RNA from the pulmonaryMEC (fresh tumor samples) and cell line NCI-H292 servingas positive control showed the presence of a specifictranscript. An RT-PCR on RNA from peripheral leukocytesand from the neuroblastoma cell line Vi-856 (serving asnegative controls) and from the pulmonary MEC cell linerevealed no specific transcript. Sequence analysis of the RT-PCR fragments verified and confirmed MECT1-MAML2fusion transcripts in both the pulmonary MEC tissue and inthe cell line NCI-H292 (Fig. 4B).
3. Discussion
We have observed significant chromosome abnormalitiesin the primary lung MEC of a 9-year-old child. Although fewsimilar pediatric cases have been reported to date, including

Fig. 2 Spectral karyotyping of the tumor cells subsequent to long-term cell culture. A, G-banded karyotype. B, Classified image of the samemetaphase. The arrows indicate the main abnormalities. Chromosomes 6, 19, and 21 were likely randomly lost. Note that the short-termcultured tumor cells showed the translocation t(11;19) as sole chromosomal aberration. The tumor karyotype of the long-term cultured cellswas determined to be: 44-45,XX.ish der(2)t(2;14)(?q1?;q?11)[2],?+del(10)(pter-Nq25.2:), t(11;19)(11qter-N11q23.3::11p11.2-N11q21::19p12-N19pter),inc[cp6].
E26 A. Serra et al.

Fig. 3 High-resolution multicolor banding analyses of the long-term tumor cells for chromosomes 11 (A) and 19 (B) and of the positivecontrol cell line NCI-H292 for chromosomes 11 (C) and 19 (D). Note the translocation t(11;19) in the control cell line [karyotype, t(11;19)(11qter-N11q23.3::11p11.2-11q21::19p12-N19pter], which was identical to the translocation detected in the tumor of the patient.
E27t(11;19) in a child’s lung mucoepidermoid in carcinoma
an 8-year-old-boy, a 3-year-old girl, a 6-year-old girl withlung MEC [15-17], and another 6-year-old female patientwith mucoepidermoid parotid adenocarcinoma [18], evenmore rare are cases of MEC with lymph node and bonemetastasis leading to death in children [19]. Accordingly, upto 83% of pulmonary MECs in adults are low-grade tumorswith an excellent prognosis, whereas the high-gradebronchial MEC has a poorer prognosis [20].
Several characteristics seem to contribute to this relatively“mild” course in MEC of the lung. In particular, the t(11;19)(q14∼21;p12∼13) constitutes a common aberration depend-ing on the primary site of the tumor, which is possiblyassociated with or responsible for the mucoepidermoidphenotype [16,21-23]. The karyotypic abnormalities in MEChave been classified into 2 different groups: (a) numericalaberrations including diverse chromosomal trisomies andmonosomies and (b) structural alterations of 11q—particu-larly t(11;19)(q14∼21;p12∼13), which are so frequent that ithas been considered the primary chromosomal abnormalityin MEC [24]. Accordingly, we have identified the transloca-tion t(11;19) in almost every metaphase studied in the tumor
cells as well as in a positive control cell line (NCI-H292).Regarding the possible effect of these translocations, Tononet al [5] postulated that t(11;19) might result in tumordevelopment because of the expression of a fusion transcriptoriginating from the 2 genes located at the breakpoints inboth chromosomes. This chimera MECT1-MAML2 was ableto in vitro activate the transcription of the Notch target geneHES1 independently of both Notch-ligand and CSL bindingsites. Because Notch signaling has been implicated in themaintenance of an undifferentiated state in stem cells, binarycell-fate decisions, and induction of differentiation, allimportant steps in the tumorigenesis, the expression of thefusion transcript and disruption of the Notch pathway couldbe held responsible for the development of the tumor [25].Similarly, Enlund et al [26] also reported that the fusiontranscript created by the translocation t(11;19) disrupted theNotch signaling pathway, resulting in an upregulation of theexpression of Notch target genes such as HES5. Subse-quently, the focus of studies has shifted from the Notchpathway to the cAMP signaling pathways because it has beenshown that MECT1 expression originates TORC1, a

Fig. 4 A, Messenger RNA expression ofMECT1 andMAML2 inperipheral blood leukocytes of the patient. B, Expression ofMECT1-MAML2 transcript chimera in the fresh tumor cells (tumorsample) and in the long-term tumor cell line (tumor cell line), in thepositive control NCI-H292 cell line (NCI-H292), and in theneuroblastoma Vi-856 cell line (Vi-856). Note that the fusiontranscript (MECT1-MAML2 chimera) is expressed in the freshtumor yet not in the long-term cell line.
E28 A. Serra et al.
transducer of regulated CREB protein, which potentlyinduces CREB1 target genes through a potent transcriptionactivation domain [6,7]. The authors concluded that TORCsrepresent a family of highly conserved CREB coactivatorsthat may control the potency and specificity of CRE-mediated responses, including tumorigenesis [6]. Accord-ingly, the putative mechanism for tumor developmentoriginated from or associated with t(11;19) involves thecomplex interaction of Mam proteins and the cAMPsignaling pathway because the expression of the MECT1-MAML2 fusion transcript has been shown to strongly inducetarget gene expression by CREB-mediated stimulation innormal and transformed cells [7,27]. The isolation of thefusion transcript in our patient and in the positive control(NCI-H292) cell line supports the hypothesis of MECdevelopment based on the t(11;19) resulting in MECT1-MAML2 fusion transcript expression. Interestingly, in a long-term cell culture, we have observed that the fusion transcript
was solely expressed in a positive control cell line (NCI-H292), although the cytogenetically detected t(11;19) waspresent in both cell lines (data not shown), and both MECT1andMAML2 were separately expressed. It is feasible that thelong growth time may have led to the negative findings ofMECT1-MAML2 fusion transcript in this sample because theexpression of many fusion genes, including this fusiontranscript, is usually very low.
The impact of t(11;19) on the clinical course of MEC isstill controversial. Generally speaking, low-grade tumorshave a higher incidence of the translocation, which has notyet been found in poorly differentiated MEC. Interestingly,all pulmonary MEC with 11q rearrangements were of low-grade malignancy. It remains speculative if the translocationt(11;19)(q21;p13) might represent a diagnostic marker forlow- to intermediate-grade MEC. Conversely, more recentstudies have determined that the MECT1-MAML2 fusionproduct is specific for MEC tumors and associated with asubset of tumors that have a more favorable prognosis basedon a rather protracted clinical course [28,29]. Some authorshave additionally demonstrated a significantly lower risk oflocal recurrence, metastases, and tumor-related deaths inMECT1-MAML2–positive tumors compared with fusion-negative tumors, which suggests that the molecular classi-fication of MEC based on the expression of the fusiontranscript may indeed be useful as a marker of prognosis andprediction of the biologic behavior [30]. Our case studysupports such conclusion because the patient has now been2.5 years tumor-free after the resection of the primary lesion.
In summary, we demonstrated several genetic abnormal-ities in an infantile MEC of the lung and correlated thefindings with the expression of a tumor-inducing fusionproduct, MECT1-MAML2. This study and data from otherstudies suggest that the translocation t(11;19)(q14∼21;p12∼13) and, more importantly, the consequent expressionof the MECT1-MAML2 fusion transcript serve as adiagnostic and prognostic marker for low- to intermediate-grade MEC, particularly in the lung. A larger casuistic,possibly in a multicenter study design, will be able tostatistically confirm the hypothesis that the expression of theMECT1-MAML2 fusion transcript is indeed associated with abetter prognosis in childhood MEC.
Acknowledgments
The authors would like to acknowledge Yvonne Kemnitz(Department of Pediatric Surgery, University of Dresden,Dresden, Germany), Felicitas Zachow (Department ofNeurosurgery, University of Dresden), and Ulrike Fitze(Department of Internal Medicine, University of Dresden)for the excellent technical assistance. We thank Dr MichaelHaase and Dr Katrin Friedrich (Department of Pathology,University of Dresden) for the histology samples. We aregrateful to Prof Dr Laszlo Füsezi (Department of Pathology,

E29t(11;19) in a child’s lung mucoepidermoid in carcinoma
University of Göttingen, Göttingen, Germany) for providingus RNA from MEC tumor samples from the patient.
References
[1] Satko I, Stanko P, Longauerova I. Salivary gland tumors treated inthe stomatological clinics in Bratislava. J Craniomaxillofac Surg2000;28(1):56-61.
[2] Ellis GL, Auclair PL. Tumors of the salivary glands. 1996 Atlas oftumor pathology, 3rd ed, vol. 17. Washington (DC): AFIP; 1996.
[3] Welsh JH, Maxson T, Jaksic T, et al. Tracheobronchialmucoepidermoid carcinoma in childhood and adolescence: casereport and review of the literature. Int J Pediatr Otorhinolaryngol1998;45(3):265-73.
[4] Granata C, Battistini E, Toma P, et al. Mucoepidermoid carcinoma ofthe bronchus: a case report and review of the literature. PediatrPulmonol 1997;23(3):226-32.
[5] Tonon G, Modi S, Wu L, et al. t(11;19)(q21;p13) translocation inmucoepidermoid carcinoma creates a novel fusion product thatdisrupts a Notch signaling pathway. Nat Genet 2003;33(2):208-13.
[6] Iourgenko V, Zhang W, Mickanin C, et al. Identification of a family ofcAMP response element–binding protein coactivators by genome-scale functional analysis in mammalian cells. Proc Natl Acad Sci U SA 2003;100:12147-52, 20037.
[7] Conkright M, Canettieri G, Screaton R, et al. TORCs: Transducers ofregulated CREB activity. Mol Cell 2003;12(2):413-23.
[8] Vogelberg C, Mohr B, Fitze G, et al. Mucoepidermoid carcinoma as anunusual cause for recurrent respiratory infections in a child. J PediatrHematol Oncol 2005;27(3):162-5.
[9] Stollmann B, Fonatsch CH, Havers W. Persistent Epstein-Barr virusinfection associated with monosomy 7 or chromosome 3 abnormalityin childhood myeloproliferative disorders. Br J Haematol 1985;60:183-96.
[10] Benn PA, Perle MA. Chromosome staining and banding techniques.In: Rooney DE, Czepulkowski BH, editors. Human cytogenetics, vol.I. New York: Oxford University Press; 1992. p. 95-6.
[11] Mohr B, Bornhäuser M, Thiede C, et al. Comparison of spectralkaryotyping and conventional cytogenetics in 39 patients with acutemyeloid leukemia and myelodysplastic syndrome. Leukemia 2000;14:1031-8.
[12] Mitelman F, editor. ISCN: 1995. An international system for humancytogenetic nomenclature. Basel: S. Karger; 1995.
[13] Liehr T, Heller A, Starke H, et al. Microdissection based highresolution multicolor banding for all 24 human chromosomes. Int JMol Med 2002;9(4):335-9.
[14] Senger G, Chudoba I, Plesch A. Multicolor-FISH—the identifica-tion of chromosome aberrations by 24 colors. BIOforum 1998;9:499-503.
[15] Anton-Pacheco J, Jimenez MA, Rodriguez-Peralto JL, et al.Bronchial mucoepidermoid tumor in a 3-year-old child. PediatrSurg Int 1998(7):524-5.
[16] Stenman G, Petursdottir V, Mellgren G, et al. A child with a t(11;19)(q14-21;p12) in a pulmonary mucoepidermoid carcinoma. VirchowsArch 1998;433:579-81.
[17] Kantar M, Cetingul N, Veral A, et al. Rare tumors of the lung inchildren. Pediatr Hematol Oncol 2002;19(6):421-8.
[18] Dahlenfors R, Wedell B, Rundcrantz H, et al. Translocation (11;19)(q14-21;p12) in a parotid mucoepidermoid carcinoma of a child.Cancer Genet Cytogenet 1995;79:188.
[19] Bellah R, Mahboubi S, Berdon W. Malignant endobronchial lesions ofadolescence. Pediatr Radiol 1992;22(8):563-7.
[20] Heitmiller RF, Mathisen DJ, Ferry JA, et al. Mucoepidermoid lungtumors. Ann Thorac Surg 1989;47(3):394-9.
[21] Johansson M, Mandahl N, Johansson L, et al. Translocation 11;19 in amucoepidermoid carcinoma of the lung. Cancer Genet Cytogenet1995;80:85-6.
[22] El-Naggar AK, Lovell M, Killiary AM, et al. A mucoepidermoidcarcinoma of minor salivary gland with t(11;19)(q21;p13.1) as the onlykaryoptypic abnormality. Cancer Genet Cytogenet 1996;87(1):29-33.
[23] Nordkvist A, Edstrom S, Mark J, et al. Multiple unrelated chromosomeabnormalities in a metastatic mucoepidermoid carcinoma of the parotidgland. Cancer Genet Cytogenet 1992;61:158-61.
[24] Nordkvist A, Gustafsson H, Juberg-Ode M, et al. Recurrentrearrangements of 11q14-22 in mucoepidermoid carcinoma. CancerGenet Cytogenet 1994;74(2):77-83.
[25] Radtke F, Raj K. The role of Notch in tumorigenesis: oncogene ortumor suppressor? Nat Rev Cancer 2003;3(10):756-67.
[26] Enlund F, Behboudi A, Andren Y, et al. Altered Notch signalingresulting from expression of a WAMTP1-MAML2 gene fusion inmucoepidermoid carcinomas and benign Warthin's tumors. Exp CellRes 2004;292(1):21-8.
[27] Coxon A, Rozenblaum E, Park YS, et al. Mect1-Maml2 fusiononcogene linked to aberrant activation of cyclic AMP/CREB regulatedgenes. Cancer Res 2005;65(16):7137-44.
[28] Okabe M, Myabe S, Nagatsuka H, et al. MECT1-MAML2 fusiontranscript defines a favorable subset of mucoepidermoid carcinoma.Clin Cancer Res 2006;12(13):3902-7.
[29] Winnes M, Enlund F, Mark J, et al. Is the MECT1-MAML2 genefusion specific for mucoepidermoid carcinomas? J Mol Diagnostics2006;8(3):394-6 [Correspondence].
[30] Behboudi A, Enlund F, Winnes M, et al. Molecular classification ofmucoepidermoid carcinomas—prognostic significance of theMECT1-MAML2 fusion oncogene. Genes Chromosomes Cancer2006;45:470-81.
Copyright © 2022 FDOKUMEN