Dietary and Non-Dietary Phytochemicals and Cancer - Unglue.it

1 23
Maternal and Child HealthJournal ISSN 1092-7875 Matern Child Health JDOI 10.1007/s10995-011-0842-5
Dietary Management of Infantile Colic: ASystematic Review
Marina Iacovou, Robin A. Ralston, JaneMuir, Karen Z. Walker & Helen Truby

1 23
Your article is protected by copyright and
all rights are held exclusively by Springer
Science+Business Media, LLC. This e-offprint
is for personal use only and shall not be self-
archived in electronic repositories. If you
wish to self-archive your work, please use the
accepted author’s version for posting to your
own website or your institution’s repository.
You may further deposit the accepted author’s
version on a funder’s repository at a funder’s
request, provided it is not made publicly
available until 12 months after publication.

Dietary Management of Infantile Colic: A Systematic Review
Marina Iacovou • Robin A. Ralston •
Jane Muir • Karen Z. Walker • Helen Truby
� Springer Science+Business Media, LLC 2011
Abstract Infantile colic, the cause of 10–20% of all early
paediatrician visits, can lead to parental exhaustion and
stress. A systematic review was conducted to examine
whether dietary change provides an effective therapy for
infantile colic. Six databases were searched from 1960, and
24 studies selected for inclusion. In breastfed infants, evi-
dence suggests that a hypoallergenic maternal diet may be
beneficial for reducing symptoms of colic. In formula-fed
infants, colic may improve after changing from a standard
cow’s milk formula to either a hydrolysed protein formula
or a soy-based formula. Fibre-supplemented formulae had
no effect. Removal of poorly digested carbohydrates from
the infant’s diet has promise, but additional clinical studies
must be conducted before a recommendation can be made.
Use of a universal definition to measure symptoms of
infantile colic and consistent analysis of urine and faecal
samples would improve the evidence in this area.
Keywords Infantile colic � Diet � Breastfed infants �Formula-fed infants
Background
Infantile colic appears in typically developing, healthy
infants [1] who commence unexplained inconsolable
crying episodes during the early weeks of life. These peak
around 6–8 weeks postpartum and spontaneously resolve
by 3–4 months [2]. ‘Colicky’ infants commonly present
with symptoms of excessive flatulence or frequent crying,
are very unsettled, fussy or irritable without a definite
explanation, or may show signs of pain (drawing up the
knees, arching the back) [2]. Infantile colic can be defined
by the ‘Wessel Criteria’: paroxysms of crying episodes,
lasting for more than 3 h per day, for three or more days
per week, and for three or more weeks [2, 3].
Infantile colic is the cause of 10–20% of all paediatrician
visits in the first 4 months of life [4, 5]. A systematic review
[6] has reported that sustained infant crying leads to parental
exhaustion, and has many deleterious consequences
including: difficulties with concentration, loss of patience,
ready frustration, feelings of incompetence, fear of harming
the child [6], and early cessation of breastfeeding [7]. In
addition, mothers becoming stressed due to infant crying
reduce face-to-face interaction with their child [8]. A sys-
tematic review and meta-analysis reported an association
between poor infant temperament and maternal postpartum
depression (effect size 0.31, 95% confidence interval (CI)
0.261–0.369) [9]. The risk of maternal depression is also
increased by infant crying (odds ratio 10.8, 95% CI
4.3–26.9) [10]. The disturbing combination of infant crying
with parental exhaustion and maternal postpartum depres-
sion can be a trigger for the serious physical abuse found
with Shaken Baby Syndrome [11–14].
While the aetiology of infantile colic is unknown, it
appears to relate to both the immaturity of the infant gut
and the composition of the infant’s diet [15, 16]. Current
treatment methods are diverse and controversial [17, 18],
and involve a range of behavioural, pharmaceutical, and
dietary strategies [2, 19–24]. Dietary interventions are one
of the most common treatment approaches and present an
M. Iacovou � R. A. Ralston (&) � K. Z. Walker � H. Truby
Department of Nutrition and Dietetics, Monash Medical Centre,
Southern Clinical School of Medicine, Monash University,
Block E, Level 5, 246 Clayton Rd, Clayton, VIC 3168, Australia
e-mail: [email protected]
J. Muir
Department of Medicine, Eastern Health Clinical School,
Monash University, Box Hill, VIC, Australia
123
Matern Child Health J
DOI 10.1007/s10995-011-0842-5
Author's personal copy

opportunity for simple, drug-free therapeutic management,
an obvious first choice for parents. As both breastfed and
formula-fed infants suffer from infantile colic [16], dietary
change must encompass both the maternal diet in breastfed
infants and change to infant formulae in formula-fed infants.
Two early systematic reviews [19, 20] reported prom-
ising results for several dietary treatments, but were both
conducted more than 10 years ago and included the same
randomised controlled trials (RCT). The present systematic
review examines more recent data in order to establish
whether dietary change can provide an effective therapy for
infantile colic in developed countries.
Methods
Search Methods
In June–July, 2010, six databases (OvidMedline, CINAHL
plus, AMED, Scopus, NUTRITIONnetBASE, Cochrane
library) were searched from 1960 using terms relating to the
question: Can dietary interventions be an effective form
of therapy in reducing the symptoms of infantile colic?
Unpublished studies and grey literature were not retrieved.
Search terms (Table 1) were grouped into five categories:
infantile colic, dietary interventions, breast milk, formula,
and infant. Synonyms and alternative words were sought
from current literature and a thesaurus. If a known study was
not retrieved, search terms were expanded and relevant
synonyms added.
Study Retrieval and Analysis
Retrieved citations were compiled in EndNote (version
X3). Titles/abstracts were assessed to determine if the full
article was relevant. Inclusion and exclusion criteria are
listed in Table 2. Studies were coded with the reason for
exclusion. Complete publications for all remaining studies
were obtained, read thoroughly, and re-evaluated. If
retained, the data was extracted and tabulated as summa-
rized in Table 3. If a study also examined a non-dietary
intervention, only the dietary intervention was included in
this review. The level of evidence of each included study
was determined using nationally-based guidelines [25],
while quality was evaluated as negative, neutral, or posi-
tive using a checklist [26].
After data extraction, the studies were categorised
according to intervention under the following headings:
changes to the maternal diet; use of hydrolysed milk pro-
teins, soy-based, or fibre-enriched formulae; and change to
carbohydrate. Studies of positive quality and higher evi-
dence studies were given greater importance. The NHMRC
body of evidence matrix [25] guided development of
summary statements.
Results
A total of 742 articles were retrieved from six database
searches. After review, 687 studies were excluded,
including duplicates, studies with an irrelevant outcome or
intervention, studies in a non-relevant population group, or
publications not reporting a study. The full publications
were sought for the remaining 55 studies (four were
unavailable). After reading 51 full papers, 27 were exclu-
ded as irrelevant, often due to type of intervention (e.g.
bottle flow variations). The remaining 24 studies included
in the final review were: two level I systematic reviews, 12
level II RCTs with 15–158 subjects, nine level III studies
with 6–115 subjects (five RCTs, three non-randomised
Table 1 Categories and search terms used for this systematic review examining the association between diet and symptoms of infantile colic
Colic Dietary interventions Breast milk Formula Infant
Colic Diet therapy Breast milk Bottle-fed Infant
Fussing Cow’s milk protein Human milk Milk Baby
Paroxysmal fussing Carbohydrates Milk Hypoallergenic formula Newborn
Wind FODMAPs Breastfeeding Formula Child
Crying Low-allergen Maternal diet Soy milk
Unsettled Maternal diet Mother’s diet
Irritable Solids
Abdominal cramp Early foods
Gastrointestinal Complimentary foods
Pain Wheat
Gut Nutrition
Gripe water
FODMAPs fermentable oligosaccharides, disaccharides, monosaccharides and polyols
Matern Child Health J
123
Author's personal copy

interventions, and one case–control study), and one level
IV cross-sectional study. The process of study exclusion is
given in Fig. 1. Table 3 summarises the 22 included pri-
mary studies that had a follow up period ranging from 3 h
to 30 days for varied dietary interventions. No studies
reported any side effects.
The two included systematic reviews [19, 20], con-
ducted over 10 years ago, were of positive quality. Based
on the same eight dietary RCTs, they both concluded that
use of a hypoallergenic or soy-based infant formula or the
provision of a hypoallergenic maternal diet for mothers of
breastfed infants reduced symptoms of colic, as defined by
duration of infant crying and fussing. The present review
includes these same eight RCTs, but adds nine new RCTs,
three intervention studies, one case–control study, and one
cross-sectional study.
Maternal Diet of Breastfed Infants
Six studies of breastfed infants have examined the rela-
tionship between maternal diet and symptoms of infantile
colic [17, 18, 27–30]. One high quality RCT (n = 90)
reported an absolute risk reduction [37% (95% CI
15–56%) when mothers changed from a control diet to a
hypoallergenic diet (eliminating dairy foods, eggs, peanuts,
tree nuts, wheat, soy, and fish) for seven days [18]. Two
earlier studies [17, 30] support this finding, but neither
separated the results for breastfed infants from results for
formula-fed infants fed hypoallergenic formula. The
hypoallergenic diet must also be well designed to exclude
all trigger foods. In a small RCT (n = 20) [27], elimination
of only cow’s milk from the mother’s diet for only two
days had no effect on the duration of colic in breastfed
infants. A poor quality intervention eliminating only dairy
foods, fish, and eggs from the maternal diet, although
continued for 30 days, had no effect on crying duration
[29]. A cross-sectional study reported [28] that maternal
consumption of cruciferous vegetables, cow’s milk, and
onions was associated with increased colic, while con-
sumption of chocolate and garlic had no effect. When both
level of evidence and study quality is considered, it appears
that changing the maternal diet to reduce the burden of
allergy-associated foods can provide some benefit in
reducing infantile colic in breastfed infants.
Hydrolysed Formulae
Thirteen studies have examined the use of either partially,
extensively, or completely hydrolysed infant formulae for
amelioration of infantile colic. In hydrolysed formulae,
whole milk proteins are altered to make them more readily
digested. Partially hydrolysed formulae are often used
for milk intolerances, while extensively and completely
hydrolysed formulae are more commonly prescribed for
milk allergies. In one high quality RCT [31], both a par-
tially hydrolysed formula and a soy-based formula were
shown to reduce colic symptoms after feeding for 14 days
(P \ 0.05). This improvement was sustained for at least an
additional 14 days. While no significant differences were
observed between the two formulae, neither was directly
compared with regular cow’s milk formula containing
intact proteins. A second study trialling an infant formula
containing partially hydrolysed milk proteins and prebiot-
ics supported these findings [15].
Five level II and four level III studies examining the
benefits of extensively hydrolysed infant formulae all
reported an improvement in symptoms. Comparing a
hydrolysed formula (n = 35) to a standard cow’s milk
formula over 7 days (n = 35), Arikan et al. [21] found
greater reduction in daily crying time in the hydrolysed
formula group (-2.22 h/day, P \ 0.001). Similarly, a
whey hydrolysate formula given for 7 days reduced crying
Table 2 Inclusion and exclusion criteria
Infants Mothers Intervention Type of publication
Inclusion criteria
Aged B 6 months Aged 18–45 years Any dietary intervention Randomised controlled trials
Healthy and typically developing Healthy In a developed country Cohort studies
Any feeding patterna Case–control studies
Cross-sectional studies
Exclusion criteria
Aged [6 months Aged \18 or [45 years Non-dietary intervention Editorials
Underlying medical condition Underlying medical condition Dietary or enzymatic supplementation Abstracts
On medication On medication Focused on taste only Commentaries
Enteral feeding In a developing country
a Any combination of breastfed, formula-fed, or solid food
Matern Child Health J
123
Author's personal copy

Ta
ble
3S
um
mar
yo
fin
clu
ded
stu
die
s
Ref
eren
ceS
tudy
des
ign
and
evid
ence
level
Popula
tion
char
acte
rist
ics
Defi
nit
ion
of
coli
c
Fee
din
g
type
Inte
rven
tion
Sam
ple
size
Len
gth
of
foll
ow
up
Outc
om
eR
esult
sQ
ual
ity
Hypoal
lerg
enic
mat
ernal
Die
t
Evan
s
[27]
RC
T(I
I)In
fants
wit
hco
lic
aged
3–18
wee
ks;
New
Zea
land
His
tory
of
per
sist
ent
cryin
gfo
r
no
reas
on
lead
ing
to
nurs
eor
physi
cian
dia
gnosi
s
of
coli
c
Excl
usi
vel
y
bre
astf
ed
Cro
ssover
:el
imin
atio
nof
cow
’s
mil
kfr
om
mat
ernal
die
tan
d
(1)
600
ml
cow
’sm
ilk
plu
s
soya
mil
k(I
som
il)
wit
hvan
illa
flav
our,
and
(2)
600
ml
soya
mil
kw
ith
flav
ouri
ng.
Quan
tity
of
mea
t,veg
etab
les,
fish
,eg
gs,
nuts
,fr
uit
,an
dch
oco
late
consu
med
by
moth
erw
as
reco
rded
20
Tw
o
trea
tmen
ts
giv
enin
2day
s
blo
cks
on
3
separ
ate
occ
asio
ns
(12
day
s
tota
l)
Dura
tion
and
rate
of
coli
c
reco
rded
by
moth
er
Mat
ernal
avoid
ance
of
cow
’sm
ilk
had
no
effe
ct.
Mat
ernal
consu
mpti
on
of
fruit
or
choco
late
was
asso
ciat
edw
ith
less
coli
c
(P\
0.0
5).
No
effe
ctof
mat
ernal
consu
mpti
on
of
mil
k,
veg
etab
les,
fish
,eg
gs,
or
nuts
.H
ighly
div
erse
mat
ernal
die
tw
asas
soci
ated
wit
h
more
coli
c(P
\0.0
5)
0
Hil
la[1
7]
RC
T(I
II)b
Infa
nts
wit
hco
lic
aged
4–16
wee
ks;
Mel
bourn
e,A
ust
rali
a
Wes
sel
crit
eria
Bre
astf
ed
and
form
ula
-
fed
Moth
ers
on
eith
er(1
)a
low
alle
rgen
die
tc,
or
(2)
aco
ntr
ol
die
t.B
ott
le-f
edin
fants
on
eith
er(1
)a
modifi
edC
MIF
(Enfa
lac)
,or
(2)
hypoal
lerg
enic
case
inH
IF
(Pre
ges
tim
il)
38
form
ula
-
fed
plu
s
77
bre
astf
ed
infa
nts
;54
moth
ers
on
low
alle
rgy
and
61
on
contr
ol
die
t
7day
sT
ota
ldis
tres
s
tim
e(m
in/d
ay)
reco
rded
by
moth
ers.
Red
uct
ion
of
tota
ldis
tres
s
tim
eby
25%
Res
ult
sfo
rbre
astf
edan
dfo
rmula
-
fed
infa
nts
wer
egro
uped
and
com
par
edto
contr
ols
.61%
inth
e
inte
rven
tion
gro
up
had
25%
dis
tres
sre
duct
ion
ver
sus
43%
in
the
contr
ol
gro
up:
adju
sted
OR
2.3
2(9
5%
CI
1.0
7–5.0
,
P=
0.0
3).
No
dif
fere
nce
bet
wee
n
bre
astf
edver
sus
form
ula
-fed
infa
nts
P
Hil
l[1
8]
RC
T(I
I)In
fants
wit
hco
lic
aged
\9
wee
ks;
Mel
bourn
e,A
ust
rali
a
Wes
sel
crit
eria
Excl
usi
vel
y
bre
astf
ed
Mat
ernal
die
tei
ther
(1)
low
alle
rgen
(excl
udin
gdai
ry,
eggs,
pea
nuts
,tr
eenuts
,w
hea
t,
soy
and
fish
),or
(2)
hab
itual
die
t(i
ncl
udin
ghig
hal
lerg
en
foods)
47
on
low
alle
rgen
die
t,43
on
hab
itual
die
t
7day
sD
aily
dura
tion
of
cryin
g/f
uss
ing
report
edby
moth
er.[
25%
reduct
ion
in
dura
tion
of
cryin
g/f
uss
ing
[25%
reduct
ion
of
coli
csy
mpto
ms
was
seen
in74%
infa
nts
wher
e
moth
erfo
llow
eda
low
alle
rgen
die
tver
sus
37%
infa
nts
wher
e
moth
erfo
llow
edhab
itual
die
t:
abso
lute
risk
reduct
ion
of
37%
(95%
CI
18–56%
,P
\0.0
01)
P
Lust
[28
]X
S(I
V)
Infa
nts
wit
han
dw
ithout
coli
cag
ed\
4m
onth
s
(mea
n2.8
month
s);
Unit
edS
tate
s
Fro
m
ques
tions
on
abdom
inal
cram
pin
g,
irri
tabil
ity,
and
inte
nse
cryin
g
Excl
usi
vel
y
bre
astf
ed
Ques
tionnai
reon
mat
ernal
consu
mpti
on
of
cruci
fero
us
veg
etab
les
(cab
bag
e,
cauli
flow
er,
bro
ccoli
,B
russ
els
spro
uts
),co
w’s
mil
k,
onio
n,
gar
lic,
and
choco
late
.
272
NA
RR
of
coli
cIn
take
of
C1
cruci
fero
us
veg
etab
le,
RR
1.6
(95%
CI
1.1
–2.4
).C
ow
’s
mil
k,
RR
2.0
(95%
CI
1.1
–3.5
);
onio
ns,
RR
1.7
(95%
CI
1.1
–2.5
);
choco
late
RR
1.5
(95%
CI
1.0
–2.2
);gar
lic
RR
1.2
(95%
CI
0.9
–1.6
).A
mounts
of
food
consu
med
not
report
ed.
P
Ogger
o
[29]
RC
T(I
II)b
Infa
nts
aged
3–12
wee
ks
adm
itte
dto
hosp
ital
for
sever
eco
lic;
Ital
y
Wes
sel
crit
eria
Excl
usi
vel
y
bre
astf
ed
Eli
min
atio
nof
mil
kan
dpro
duct
s
conta
inin
gm
ilk
pro
tein
s,fi
sh,
and
eggs
from
mat
ernal
die
t
16
30
day
sC
ryin
gdura
tion
report
edby
par
ents
62.5
%of
bre
astf
edin
fants
wit
h
moth
ers
on
hypoal
lerg
enic
die
ts
impro
ved
(not
signifi
cant)
N
Tau
bm
an
[30]
RC
T(I
I)In
fants
aged
\3
month
s
who
cry
[2
h/d
ay;
Unit
edS
tate
s
Cry
ing
[2
h/
day
due
to
poss
ible
abdom
inal
gas
or
an
unknow
n
cause
Form
ula
and
bre
ast
fed
Eit
her
(1)
die
tin
terv
enti
on:
case
in-b
ased
HIF
(Nutr
amig
en)
for
form
ula
-fed
infa
nts
,or
elim
inat
ion
of
mil
k
pro
duct
sfr
om
mat
ernal
die
t
for
bre
astf
edin
fants
,or
(2)
par
enta
lco
unse
llin
g
10
per
gro
up
9day
sM
ean
cryin
gti
me
per
day
report
edby
par
ents
Res
ult
sfo
rdie
tin
terv
enti
on
gro
up
(bre
astf
edan
dfo
rmula
-fed
infa
nts
)w
ere
gro
uped
and
com
par
edto
counse
llin
ggro
up.
Both
trea
tmen
tsre
sult
edin
reduct
ion
inm
ean
dai
lycr
yin
g
tim
e.A
fter
9day
s,th
e
counse
llin
ggro
up
had
agre
ater
reduct
ion
incr
yin
gti
me
than
the
die
tin
terv
enti
on
gro
up
(P\
0.0
2)
N
Matern Child Health J
123
Author's personal copy

Ta
ble
3co
nti
nu
ed
Ref
eren
ceS
tudy
des
ign
and
evid
ence
level
Popula
tion
char
acte
rist
ics
Defi
nit
ion
of
coli
c
Fee
din
gty
pe
Inte
rven
tion
Sam
ple
size
Len
gth
of
foll
ow
up
Outc
om
eR
esult
sQ
ual
ity
Par
tial
lyhydro
lyse
din
fant
form
ula
Ber
seth
[31]
RC
T(I
I)V
ery
fuss
yin
fants
aged
7–63
day
s
rece
ivin
gst
andar
d
cow
’sm
ilk
form
ula
;U
nit
ed
Sta
tes
Ver
yfu
ssy
or
extr
emel
y
fuss
y
Excl
usi
vel
y
form
ula
-fed
Eit
her
(1)
PH
IF
low
inla
ctose
(Enfa
mil
)or
(2)
SIF
(Soy
Enfa
mil
)
82
on
SIF
,76
on
PH
IF
28
day
sP
aren
tal
per
cepti
on
of
infa
nt
fuss
ines
s,
amount
of
gas
,num
ber
of
spit
ups,
hours
cryin
g,
stool
freq
uen
cy,
num
ber
of
bow
elm
ovem
ents
,
stool
consi
sten
cy
All
outc
om
esin
both
trea
tmen
t
gro
ups
reduce
dsi
gnifi
cantl
y
bet
wee
nbas
elin
ean
d14
day
s
(P\
0.0
5);
reduct
ions
wer
e
mai
nta
ined
to28
day
s.N
o
dif
fere
nce
bet
wee
ngro
ups
inan
y
outc
om
em
easu
res
exce
pt
stool
freq
uen
cy(m
ore
soli
dw
ith
SIF
(P\
0.0
5)
P
Sav
ino
[15]
RC
T(I
II)b
Infa
nts
wit
hco
lic
aged
\4
wee
ks;
Ital
y
Wes
sel
crit
eria
Excl
usi
vel
y
form
ula
-fed
New
form
ula
wit
h
par
tial
ly
hydro
lyse
d
whey
pro
tein
s
plu
spre
bio
tics
FO
San
dG
OS
62
on
‘new
’
form
ula
14
day
sR
educt
ion
of
full
-forc
ed
cryin
gep
isodes
last
ing
[40
min
report
edby
par
ents
Num
ber
of
coli
cep
isodes
/day
dec
reas
edfr
om
bas
elin
e
(5.9
9±
1.8
4)
today
14
(1.7
6±
1.6
0)
P
Exte
nsi
vel
yhydro
lyse
din
fant
form
ula
Ari
kan
[21]
RC
T(I
I)In
fants
wit
hco
lic
aged
4–12
wee
ks;
Turk
ey
Wes
sel
crit
eria
Excl
usi
vel
y
form
ula
-fed
Eit
her
:(1
)H
IFor
(2)
contr
ol.
No
bra
nd
nam
es
wer
epro
vid
ed.
The
HIF
is
assu
med
tobe
exte
nsi
vel
y
hydro
lyse
d
35
on
HIF
,35
on
contr
ol
7day
sR
educt
ion
inm
ean
tota
l
cryin
g(h
/day
)in
7day
sbef
ore
trea
tmen
tver
sus
7day
sduri
ng
trea
tmen
t
Cry
ing
tim
ew
asre
duce
daf
ter
7day
s
(2.6
9h/d
ay)
com
par
edto
bas
elin
e
(4.9
1h/d
ay)
inH
IFgro
up
(P\
0.0
01).
Gre
ater
reduct
ion
in
cryin
gh/d
ayin
HIF
gro
up
ver
sus
contr
ol
gro
up
(P\
0.0
01)
P
Fors
yth
[23]
RC
T(I
I)In
fants
wit
hco
lic
aged
\8
wee
ks;
Unit
edS
tate
s
Wes
sel
crit
eria
Excl
usi
vel
y
form
ula
-fed
Cro
ssover
:(1
)
case
in-b
ased
exte
nsi
vel
yH
IF
(Nutr
amig
en),
and
(2)
stan
dar
d
CM
IF
17
Alt
ernat
ing
4day
son
each
form
ula
,
repea
ted
twic
e
Chan
ge
incr
yin
g
beh
avio
ur;
day
-to-d
ay
var
iabil
ity
incr
yin
g
beh
avio
ur
Tota
lcr
yin
gti
me
incr
ease
daf
ter
swit
chto
CM
IFan
ddec
reas
ed
when
swit
ched
toex
tensi
vel
yH
IF
(P\
0.0
1);
the
effe
ctat
tenuat
ed
wit
hti
me
P
Hil
la
[17]
RC
T(I
II)b
Infa
nts
wit
hco
lic
aged
4–16
wee
ks;
Mel
bourn
e,
Aust
rali
a
Wes
sel
crit
eria
Bre
astf
edan
d
form
ula
-fed
Moth
ers
on
eith
er
(1)
alo
w
alle
rgen
die
tc,
or
(2)
aco
ntr
ol
die
t
38
form
ula
-fed
plu
s77
bre
astf
ed
infa
nts
;54
moth
ers
on
low
alle
rgy
and
61
on
contr
ol
die
t
7day
sT
ota
ldis
tres
sti
me
(min
/
day
)re
cord
edby
moth
er.
Red
uct
ion
of
tota
ldis
tres
sti
me
by
25%
Res
ult
sfo
rbre
astf
edan
dfo
rmula
-fed
infa
nts
wer
egro
uped
,an
d
com
par
edw
ith
contr
ols
.61%
on
the
inte
rven
tion
had
25%
dis
tres
s
reduct
ion
ver
sus
43%
of
contr
ols
:
adju
sted
OR
2.3
2(9
5%
CI
1.0
7–5.0
,P
=0.0
3).
No
dif
fere
nce
bet
wee
nbre
astf
edver
sus
form
ula
-
fed
infa
nts
P
Bott
le-f
edin
fants
on
eith
er(1
)a
modifi
edC
MIF
(Enfa
lac)
,or
(2)
hypoal
lerg
enic
case
inH
IF
(Pre
ges
tim
il).
Matern Child Health J
123
Author's personal copy

Ta
ble
3co
nti
nu
ed
Ref
eren
ceS
tudy
des
ign
and
evid
ence
level
Popula
tion
char
acte
rist
ics
Defi
nit
ion
of
coli
c
Fee
din
gty
pe
Inte
rven
tion
Sam
ple
size
Len
gth
of
foll
ow
up
Outc
om
eR
esult
sQ
ual
ity
Jakobss
on
[34]
RC
T(I
I)In
fants
wit
hse
ver
e
coli
cag
ed
2–8
wee
ks;
Sw
eden
Wes
sel
crit
eria
Excl
usi
vel
y
form
ula
-fed
Cro
ssover
:(1
)ca
sein
-bas
ed
exte
nsi
vel
yH
IFw
ith
48%
Efr
om
fat,
41%
Efr
om
carb
ohydra
te(A
lim
entu
m),
and
(2)
case
in-b
ased
exte
nsi
vel
yH
IFw
ith
35%
Efr
om
fat,
54%
Efr
om
carb
ohydra
te(N
utr
amig
en)
15
7day
sper
form
ula
Aver
age
dai
ly
cryin
gti
me
(h);
aver
age
dai
lycr
yin
g
inte
nsi
ty,
dis
turb
ed
slee
p(%
of
day
s)
report
edby
par
ents
Both
types
of
HIF
reduce
d
cryin
gti
me
from
bas
elin
e
(7.3
6±
1.3
2h/d
ay)
today
7
(Ali
men
tum
2.2
1±
0.4
0h/
day
(P\
0.0
1),
Nutr
amig
en
2.9
3±
0.7
0h/d
ay
(P\
0.0
1))
.N
odif
fere
nce
bet
wee
nfo
rmula
e
P
Loth
e[3
5]
RC
T(I
II)d
Infa
nts
aged
2w
eeks
to3
month
s
adm
itte
dto
hosp
ital
wit
h
sever
eco
lic;
Sw
eden
Par
oxysm
al
abdom
inal
pai
n,
sever
e
cryin
g
(sev
eral
h/d
ay),
abdom
inal
dis
tensi
on,
and
wis
hto
suck
leoft
en
Excl
usi
vel
y
form
ula
-fed
Cro
ssover
:(1
)C
MIF
(Enfa
mil
),an
d(2
)S
IF
(Pro
Sobee
).If
no
impro
vem
ent,
infa
nts
wer
e
giv
enca
sein
-bas
ed
exte
nsi
vel
yH
IF
(Nutr
amig
en)
60
7day
sper
form
ula
Pre
sence
/
abse
nce
of
coli
c
sym
pto
ms
report
edby
par
ents
29%
of
infa
nts
reco
ver
ed
sponta
neo
usl
yan
dbeg
anto
tole
rate
CM
IF.
18%
of
infa
nt’
ssy
mpto
ms
dis
appea
red
wit
hin
48
hw
ith
SIF
.In
53%
,sy
mpto
ms
did
not
impro
ve
wit
hS
IF—
wit
h
exte
nsi
vel
yH
IF,
all
wer
e
sym
pto
m-f
ree
wit
hin
48
h
P
Loth
e[3
3]
Inte
rven
tion
study
(III
)
Infa
nts
wit
hco
lic
aged
2–12
wee
ks;
Sw
eden
Wes
sel
crit
eria
Excl
usi
vel
y
form
ula
-fed
Cas
ein-b
ased
exte
nsi
vel
y
HIF
(Nutr
amig
en)
27
5day
sC
ryin
gti
me
(h/
day
)re
port
ed
by
par
ents
Cry
ing
tim
edec
reas
edw
hen
stan
dar
dC
MIF
(mea
n5.6
h/
day
)w
asre
pla
ced
wit
hH
IF
(mea
n0.7
h/d
ay)
(P\
0.0
01)
0
Luca
ssen
[32]
RC
T(I
I)In
fants
wit
hco
lic
aged
\6
month
s;
The
Net
her
lands
Wes
sel
crit
eria
Excl
usi
vel
y
form
ula
-fed
Eit
her
(1)
whey
-bas
ed
exte
nsi
vel
yH
IF(N
utr
ilon
Pep
ti)
or
(2)
stan
dar
d
CM
IF
20
on
HIF
,18
on
stan
dar
d
CM
IF
7day
sD
iffe
rence
in
the
reduct
ion
of
cryin
g
dura
tion
bet
wee
n
bas
elin
ean
d
day
7
Cry
ing
tim
edec
reas
edby
47
min
/day
more
wit
hH
IF
ver
sus
CM
IF(P
=0.0
4)
P
Ogger
o
[29]
RC
T(I
II)b
,dIn
fants
aged
3–12
wee
ks
adm
itte
dto
hosp
ital
for
sever
e
coli
c;It
aly
Wes
sel
crit
eria
Excl
usi
vel
y
form
ula
-fed
SIF
(Iso
mil
)giv
enfo
r48
h.
Ifsy
mpto
ms
conti
nued
,
case
in-b
ased
exte
nsi
vel
y
HIF
(Nutr
amig
en)
subst
itute
d
15
30
day
sC
ryin
g
dura
tion
report
edby
par
ents
13
(86.6
%)
of
15
infa
nts
not
resp
ondin
gto
soy
impro
ved
wit
hH
IF(P
\0.0
1)
N
Tau
bm
an
[30]
RC
T(I
I)In
fants
aged
\3
month
s
who
cry
[2
h/d
ay;
Unit
edS
tate
s
Cry
ing
[2
h/
day
due
to
poss
ible
abdom
inal
gas
or
an
unknow
n
cause
Form
ula
and
bre
ast
fed
Eit
her
(1)
die
tin
terv
enti
on:
case
in-b
ased
exte
nsi
vel
y
HIF
(Nutr
amig
en)
for
form
ula
-fed
infa
nts
,or
elim
inat
ion
of
mil
k
pro
duct
sfr
om
mat
ernal
die
tfo
rbre
astf
edin
fants
,or
(2)
par
enta
lco
unse
llin
g
10
per
gro
up
9day
sM
ean
cryin
g
tim
eper
day
report
edby
par
ents
Res
ult
sfo
rdie
tin
terv
enti
on
gro
up
(bre
astf
edan
dfo
rmula
-
fed
infa
nts
)w
ere
gro
uped
and
com
par
edto
counse
llin
g
gro
up.
Both
trea
tmen
ts
resu
lted
inre
duct
ion
inm
ean
dai
lycr
yin
gti
me.
Aft
er
9day
s,th
eco
unse
llin
ggro
up
had
agre
ater
reduct
ion
in
cryin
gti
me
than
the
die
t
inte
rven
tion
gro
up
(P\
0.0
2)
N
Matern Child Health J
123
Author's personal copy

Ta
ble
3co
nti
nu
ed
Ref
eren
ceS
tudy
des
ign
and
evid
ence
level
Popula
tion
char
acte
rist
ics
Defi
nit
ion
of
coli
c
Fee
din
gty
pe
Inte
rven
tion
Sam
ple
size
Len
gth
of
foll
ow
up
Outc
om
eR
esult
sQ
ual
ity
Com
ple
tely
hydro
lyse
din
fant
form
ula
Est
ep[3
7]
Inte
rven
tion
study
(III
)
Infa
nts
wit
h
exce
ssiv
ecr
yin
g
and
fuss
ing
aged
3.5
–7
wee
ks;
Unit
edS
tate
s
Wes
sel
crit
eria
Excl
usi
vel
y
form
ula
-fed
Com
ple
tely
HIF
(Neo
cate
)6
5day
sC
ryin
gan
dfu
ssin
g
tim
ere
port
edby
par
ents
Dai
lycr
yin
gan
dfu
ssin
gti
me
reduce
dby
21–64%
(mea
n45%
),
are
duct
ion
of
148
min
/day
from
bas
elin
e(P
\0.0
02)
P
Est
ep[3
6]
RC
T(I
II)d
Infa
nts
wit
h
exce
ssiv
ecr
yin
g
and
fuss
ing
aged
15–48
day
s;
Unit
edS
tate
s
Wes
sel
crit
eria
Bre
astf
ed
swit
ched
to
form
ula
-fed
Tem
pora
rily
taken
off
bre
ast
mil
kan
dgiv
en
com
ple
tely
HIF
(Neo
cate
)
64
day
sC
ryin
gan
dfu
ssin
g
tim
ere
port
edby
par
ents
Red
uce
dcr
yin
gti
me
wit
hin
2–4
day
sw
hil
eon
com
ple
tely
HIF
.C
ryin
gti
me
impro
ved
by
13–72%
(mea
n45%
)
(P=
0.0
41)
0
Soy-B
ased
Infa
nt
Form
ula
Ber
seth
[31]
RC
T(I
I)V
ery
fuss
yin
fants
aged
7–63
day
son
stan
dar
dC
MIF
;
Unit
edS
tate
s
Ver
yfu
ssy
or
extr
emel
y
fuss
y
Excl
usi
vel
y
form
ula
-fed
Eit
her
(1)
low
lact
ose
par
tial
lyH
IF(P
HIF
Enfa
mil
),or
(2)
SIF
(Soy
Enfa
mil
)
82
on
SIF
,
76
on
PH
IF
28
day
sP
aren
tal
per
cepti
on
of
infa
nt
fuss
ines
s,
amount
of
gas
,
num
ber
of
spit
ups,
hours
cryin
g,
stool
freq
uen
cy,
num
ber
of
bow
el
movem
ents
,st
ool
consi
sten
cy
All
outc
om
esw
ere
reduce
d
signifi
cantl
yfr
om
bas
elin
eto
day
14
inboth
trea
tmen
tgro
ups
(P\
0.0
5);
reduct
ions
wer
e
mai
nta
ined
today
28.
No
dif
fere
nce
sbet
wee
ngro
ups
in
any
outc
om
em
easu
res
exce
pt
stool
freq
uen
cy(m
ore
soli
dw
ith
SIF
(P\
0.0
5))
P
Cam
pbel
l
[38]
RC
T(I
I)In
fants
wit
hco
lic
aged
3–14
wee
ks;
Sco
tlan
d
Wes
sel
crit
eria
Excl
usi
vel
y
form
ula
-fed
Cro
ssover
:(1
)S
IF,
and
(2)
CM
IF
19
1w
eek
for
each
form
ula
Tim
ew
ith
coli
c
sym
pto
ms
(h/d
ay)
report
edby
par
ents
SIF
reduce
dco
lic
sym
pto
ms
(P\
0.0
1)
N
Loth
e[3
5]
RC
T(I
I)In
fants
aged
2w
eeks
to3
month
s
adm
itte
dto
hosp
ital
wit
h
sever
eco
lic;
Sw
eden
Par
oxysm
al
abdom
inal
pai
n,
sever
e
cryin
g
(sev
eral
h/d
ay),
abdom
inal
dis
tensi
on,
and
wis
hto
suck
leoft
en
Excl
usi
vel
y
form
ula
-fed
Cro
ssover
:(1
)C
MIF
(Enfa
mil
),an
d(2
)S
IF
(Pro
Sobee
).If
no
impro
vem
ent,
infa
nts
wer
egiv
enca
sein
-bas
ed
exte
nsi
vel
yH
IF
(Nutr
amig
en)
60
7day
sper
form
ula
Pre
sence
/abse
nce
of
sym
pto
ms
of
coli
c
report
edby
par
ents
29%
of
infa
nts
sponta
neo
usl
y
reco
ver
edan
dbeg
anto
tole
rate
CM
IF.
18%
of
sym
pto
ms
dis
appea
red
wit
hin
48
hof
SIF
P
Ogger
o
[29]
RC
T(I
II)b
Infa
nts
aged
3–12
wee
ks
adm
itte
dto
hosp
ital
for
sever
e
coli
c;It
aly
Wes
sel
crit
eria
Excl
usi
vel
y
form
ula
-fed
SIF
(Iso
mil
)fo
r48
h.
If
sym
pto
ms
conti
nued
,
case
in-b
ased
exte
nsi
vel
y
HIF
(Nutr
amig
en)
subst
itute
d
44
30
day
sC
ryin
gdura
tion
report
edby
par
ents
65.9
%im
pro
ved
wit
hS
IFN
Fib
re-e
nri
ched
infa
nt
form
ula
Tre
em
[39]
RC
T(I
I)In
fants
wit
hco
lic
aged
2–8
wee
ks;
Unit
edS
tate
s
Unex
pla
ined
fuss
ines
sor
cryin
g
for[
3h/
day
on
at
leas
t3
of
6
succ
essi
ve
day
s
Excl
usi
vel
y
form
ula
-fed
Cro
ssover
:(1
)fi
bre
supple
men
ted
SIF
(Iso
mil
,14.1
gdie
tary
fibre
/L)
and
(2)
pla
cebo
SIF
(sta
ndar
dIs
om
il,
3.1
gdie
tary
fibre
/L).
Max
imum
volu
me
of
form
ula
:1,0
80
ml/
day
27
9day
sper
form
ula
Aver
age
dai
ly
cryin
gti
me
(h/
day
);av
erag
e
dai
lycr
yin
gplu
s
fuss
ing
tim
e(h
/
day
)
No
dif
fere
nce
incr
yin
gor
cryin
g
plu
sfu
ssin
gti
me
(h/d
ay)
bet
wee
n
form
ula
e.S
mal
lre
duct
ion
in
cryin
g(-
32%
,P
\0.0
5)
and
cryin
g?
fuss
ing
tim
e(-
29%
,
P\
0.0
5)
wit
hth
efi
bre
-enri
ched
SIF
com
par
edto
bas
elin
e
P
Matern Child Health J
123
Author's personal copy

Ta
ble
3co
nti
nu
ed
Ref
eren
ceS
tudy
des
ign
and
evid
ence
level
Popula
tion
char
acte
rist
ics
Defi
nit
ion
of
coli
c
Fee
din
gty
pe
Inte
rven
tion
Sam
ple
size
Len
gth
of
foll
ow
up
Outc
om
eR
esult
sQ
ual
ity
Car
bohydra
teal
tera
tion
Cole
[41]
Inte
rven
tion
study
(III
)
Hea
lthy
infa
nts
aged
*6
month
s;
Unit
edS
tate
s
Not
exam
ined
for
coli
c
Excl
usi
vel
y
form
ula
-fed
Eit
her
(1)
120
ml
whit
e
gra
pe
juic
e(p
er120
ml:
0g
sorb
itol
0g
sucr
ose
,
8.8
gfr
uct
ose
,8.4
g
glu
cose
)or
(2)
pea
rju
ice
(per
120
ml:
2.4
g
sorb
itol,
1.1
gsu
crose
,
7.5
gfr
uct
ose
,2.7
g
glu
cose
)giv
enw
ithin
2m
inaf
ter
2h
fast
14
1.5
h%
tim
esp
ent
cryin
g
duri
ng
1.5
h
obse
rvat
ion
per
iod
No
dif
fere
nce
in%
cryin
gti
me
afte
rgra
pe
ver
sus
pea
rju
ice
P
Duro
[40]
Cas
eco
ntr
ol
(III
):co
lic
gro
up
and
non-c
oli
c
gro
up
Hea
lthy
infa
nts
aged
4–6
month
s;
Unit
edS
tate
s
Quan
tifi
ed
infa
nt
cryin
g
Form
ula
and
bre
astf
ed
Eit
her
(1)
120
ml
whit
e
gra
pe
juic
e(p
erdl:
7.5
g
fruct
ose
,7.1
gglu
cose
,
pH
3.2
5),
or
(2)
120
ml
apple
juic
e(p
erdl:
6.2
g
fruct
ose
,2.7
gglu
cose
,
0.5
gso
rbit
ol,
1.2
g
sucr
ose
,pH
3.6
0)
afte
r
2h
fast
.
30
tota
l:16
wit
hco
lic,
14
wit
hout
3h
BH
2ex
cret
ion;
cryin
gan
d
slee
pin
gti
me
Infa
nts
wit
hco
lic
fed
apple
juic
e
had
incr
ease
dB
H2
excr
etio
n
(P\
0.0
5)
and
incr
ease
dcr
yin
g
tim
e(P
\0.0
5)
ver
sus
infa
nts
wit
hout
coli
c.C
ryin
gan
d
slee
pin
gti
mes
wer
eunch
anged
inin
fants
fed
whit
egra
pe
juic
e
whet
her
wit
hco
lic
or
not
P
Sta
hlb
erg
[24
]
RC
T(I
I)In
fants
wit
hco
lic;
mea
nag
e
11.9
wee
ks
Not
defi
ned
Infa
nts
wea
ned
from
bre
ast
mil
k
Cro
ssover
:(1
)poole
d
bre
ast
mil
k,
(2)
poole
d
bre
ast
mil
kw
ith
hydro
lyse
dla
ctose
,(3
)
adap
ted
CM
IF(T
utt
eli)
,
and
(4)
adap
ted
CM
IF
wit
hhydro
lyse
dla
ctose
10
7day
sper
inte
r-
ven
tion
%of
day
sw
ith
coli
c;dai
ly
dura
tion
and
sever
ity
of
coli
c
report
edby
par
ents
No
signifi
cant
dif
fere
nce
s
(P[
0.0
5)
for
dai
lydura
tion
of
coli
cor
%day
sw
ith
coli
cfo
ran
y
trea
tmen
tgro
up,
for
bre
ast
ver
sus
form
ula
,or
for
lact
ose
ver
sus
hydro
lyse
dla
ctose
N
Excl
udin
gsy
stem
atic
revie
ws
BH
2bre
ath
hydro
gen
,C
HO
carb
ohydra
tes,
CI
confi
den
cein
terv
al,
CM
IFco
w’s
mil
kin
fant
form
ula
,d
day
,E
tota
ldie
tary
ener
gy,
FO
Sfr
uct
o-o
ligosa
cchari
des
,G
OS
gal
acto
-oli
gosa
cchar
ides
,H
IFhydro
lyse
din
fant
form
ula
,O
Rodds
rati
o,
PH
IFpar
tial
lyhydro
lyse
dfo
rmula
,R
CT
random
ised
contr
oll
edtr
ial,
RR
rela
tive
risk
,SIF
soy-b
ased
infa
nt
form
ula
Qual
ity:
Pposi
tive,
Oneu
tral
,N
neg
ativ
ea
Com
bin
edre
sult
sfo
rin
fants
fed
ahydro
lyse
dfo
rmula
and
bre
astf
edin
fants
wit
hm
oth
ers
consu
min
ga
low
alle
rgen
die
tb
Dat
ause
dw
asbas
edon
only
one
arm
of
the
study,
soev
iden
cele
vel
iseq
uiv
alen
tto
anin
terv
enti
on
study
cO
nly
rice
,buck
whea
t,ap
ple
,pea
r,w
ater
,w
eak
tea,
wea
kco
ffee
,pota
to,
pum
pkin
,zu
cchin
i,m
arro
w,
lett
uce
,ca
rrot,
cauli
flow
er,
squas
h,
lam
b,
bee
f,ch
icken
,vea
l,tu
rkey
,fi
sh,
dai
ry-f
ree
mar
gar
ine,
saffl
ow
eroil
,honey
,su
gar
,sa
lt,
and
pep
per
allo
wed
dN
ora
ndom
isat
ion
of
hydro
lyse
dfo
rmula
port
ion,
soev
iden
cele
vel
equiv
alen
tto
anin
terv
enti
on
study
Matern Child Health J
123
Author's personal copy

duration more than standard cow’s milk formula
(P = 0.04) [32]. As above, two studies that did not provide
separate data on formula-fed versus breastfed infants lend
support to these findings [17, 30]. Forsyth et al. [23]
alternated standard cow’s milk formula with a casein
hydrolysate formula for 4 days each over a total of
16 days. Total daily crying time increased on standard
formula but decreased on hydrolysed formula, although the
effect diminished after the third switch. Lothe et al. [33]
also reported reduced crying time when a casein hydroly-
sate formula replaced standard cow’s milk formula
(P \ 0.0001). When two extensively hydrolysed formulae
with differing carbohydrate and fat content were compared,
both proved effective in reducing crying times over 7 days
(P \ 0.01), indicating that change to carbohydrate and fat
content had no effect [34]. In two level III studies, exten-
sively hydrolysed formulae were given to infants with colic
after symptoms failed to improve with soy-based formula.
In each case, the hydrolysed formula provoked a significant
improvement [29, 35].
Two studies of level III evidence have examined the
effect of completely hydrolysed formula on daily crying
and fussing time. In a small study of only six infants, the
temporary replacement of breast milk with completely
hydrolysed formula reduced infants’ crying and fussing
time by 45% (P = 0.041) after 2–4 days [36]. Similarly,
when completely hydrolysed formula replaced usual infant
formulae in another six infants, the daily duration of crying
and fussing time was reduced (P \ 0.002) [37]. Overall,
the evidence strongly suggests that use of partially,
extensively, or completely hydrolysed infant formula can
be effective in reducing the symptoms of infantile colic in
formula-fed infants.
Soy-Based Formula
Three level II RCTs and one level III study have examined
the use of soy-based formula to improve symptoms of
infantile colic. As above, Berseth et al. [31] found that both
soy-based formula and partially hydrolysed formula
reduced symptoms of colic (P \ 0.05), each having similar
effect. Two poor quality RCTs also support this. In the first
[38], a soy-based formula reduced symptoms of colic
(P \ 0.01) relative to a standard cow’s milk formula after
feeding for 7 days. The other [29] reported a 65.9%
improvement in crying duration when feeding a soy-based
formula for only 48 h. In contrast, an older but higher
quality RCT [35] compared regular cow’s milk formula to
a soy-based formula, again over seven days, and reported
only an 18% improvement of symptoms with soy-based
formula. Overall, the evidence suggests that a soy-based
formula may improve symptoms of colic, although more
extensive trials are needed.
Fibre-Enriched Formula
A single level II crossover RCT has compared a soy-based
formula with and without supplementation with soy poly-
saccharide to increase fibre content [39]. After nine days on
each formula, no difference in crying and fussing time was
detected.
Carbohydrate Malabsorption
Three studies have examined the effect of poorly absorbed
carbohydrates on symptoms of infantile colic. Duro et al.
[40] challenged infants with or without colic with either
Total Returned
742
Excluded*
687
Included
55
Excluded*
31
Included
24
RCTs
17
Systematic reviews
2
Intervention studies
3
Case control studies
1
Cross-sectional studies
1
Outcome or intervention
6
Duplicate
3
Not a study
17
Population
1
Not found
4
Outcome or intervention
291
Duplicate
292
Not a study
35
Population
69
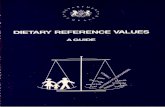
Fig. 1 Flow diagram depicting process of study selection and reasons for exclusion. RCT randomised controlled trial. *Stems below the
excluded box indicate reasons for exclusion
Matern Child Health J
123
Author's personal copy

apple or white grape juice. Apple juice has a high ratio of
fructose: glucose and contains sorbitol, and is therefore rich
in poorly absorbed carbohydrates. Conversely, the carbo-
hydrates in white grape juice, which has a low fructose:
glucose ratio and does not contain sorbitol, are readily
absorbed. After apple juice, infants with colic exhibited
increased breath hydrogen (P \ 0.05) and an increased
crying time (P \ 0.05) compared to infants without colic.
In contrast, when fed white grape juice, no differences in
breath hydrogen and crying time were apparent. Similarly,
Cole et al. [41] challenged healthy infants with either white
grape juice or pear juice (equivalent to apple juice above)
and reported no difference in crying time. This however,
may be a consequence of the fact that infants in this study
did not have colic. Although present evidence is limited,
the effect of poorly absorbed carbohydrates such as fruc-
tose and sorbitol could be targeted for future research in
colicky infants. In a third, small study (n = 10), hydroly-
sing lactose in either pooled breast milk or cow’s milk
formula before feeding to the infant had no effect on the
daily duration of colic [24].
Discussion
Evidence from this systematic review suggests that pro-
viding a hypoallergenic diet to the mother may ameliorate
colic in breastfed infants, while changing to a hydrolysed
protein formula may reduce colic in formula-fed infants.
As these dietary therapies are low risk interventions, these
could be offered as an option to mothers who wish to try
dietary manipulation in an attempt to alleviate colic
symptoms. However, expert nutritional guidance should be
sought as very restricted maternal diets have the potential
to be nutritionally inadequate. In addition, both the use of
hydrolysed milk formula and the use of a hypoallergenic
diet for the mother have cost implications that could be
problematic for low-income families. Advice to mothers
dealing with infantile colic should also include support and
reassurance by the medical team that this is a self-limiting
condition that infants tend to grow out of by 3–4 months of
age. There appears to be no advantage to changing the
macronutrient balance of an infant formula or adding die-
tary fibre, although soy-based formulae may be of benefit.
Removal of poorly digested carbohydrates from the
infant’s diet also has promise for treatment of infantile
colic, although additional clinical studies must be con-
ducted before any recommendation can be made.
Studies are needed to explore reasons why breastfed
infants get colic. Breast milk remains an optimal source for
infant nutrition and maturation of the infant gut [42]. It
contains proteins which aid micronutrient absorption or
enhance mucosal immunity; non-digestible carbohydrates
whose fermentation helps establish beneficial microbiota in
the infant bowel; a proper ratio of omega-3 to omega-6
polyunsaturated fatty acids; and a plethora of anti-
inflammatory factors [43, 44]. Breast milk clearly has a
capacity to change with time and in response to infant needs
[43], but little is known on how it responds to change in
maternal diet. Nevertheless, two studies providing level II
evidence and four studies of lower impact indicate potential
benefit of a hypoallergenic diet for breastfeeding mothers
whose infants have colic. However adhering to a strict
hypoallergenic diet may be difficult for mothers, particularly
within under-resourced communities. Additional studies are
now needed to identify the triggers in breast milk for infantile
colic and to explore potential mechanisms.
Does colic in formula-fed infants have a similar aetiol-
ogy to that in breastfed infants? To date, the answer to this
question remains unknown, as no studies have compared
colic in exclusively breastfed infants with that in formulae-
fed infants. For infants who are given formula and who
develop colic, present advice from the American Academy
of Pediatrics and the American Academy of Family Phy-
sicians does not support a formula change, considering that
parental counselling may be more effective [45]. This
advice however, is based on a single early study which was
not designed to examine the effectiveness of dietary change
but was instead designed to show the effectiveness of
counselling [30]. This present review has now identified
two systematic reviews and ten additional studies that
examine the use of hydrolysed infant formulae for treat-
ment of infantile colic, all of which report positive findings
clearly supporting the utility of hydrolysed formulae. What
remains unclear is whether a hydrolysed cow’s milk pro-
tein formula or a soy-based protein formula provides
greater benefit. A single study comparing the two types of
formulae [31], reported no difference in efficacy. Concerns
have been raised however, concerning the content of
phytoestrogenic isoflavones in soy formulae [46, 47]. The
optimum degree of hydrolysis for formulae used to treat
infantile colic is also unclear. No studies as yet compare
the effectiveness of completely hydrolysed, extensively
hydrolysed, and partially hydrolysed formulae.
Are there dietary extracts or supplements of benefit in
colic? Although this question is not addressed in this
review, two level II RCTs have indicated improvement in
colic when herbal tea has been given to colicky infants [21,
48]. Interestingly, although gripe water is a well-known
remedy for infantile colic that has been used since 1851
[22], no studies were retrieved that explore this as a pos-
sible treatment. It would be of benefit to compare the
effects of dietary change with such alternative treatments,
as well as programs for behavioural change, for example
training parents in calming or reassurance techniques [49],
or with the use of acupuncture [50].
Matern Child Health J
123
Author's personal copy

One strength of individual studies included in this sys-
tematic review was the consistency of their inclusion and
exclusion criteria. All ensured that both infants and
mothers were healthy and not medicated and that infants
were typically developing and born at full term. As it is
important to exclude lactose intolerance as a cause of
infantile colic, included studies would have benefited from
more consistent measurement of infant faeces [51]. Only
five studies [15, 24, 31, 34, 39] analysed infant stool
consistency. Although validated methods are available for
adults [52], examination of infant stool consistency varied
and often relied on subjective visual interpretation by
parents or researchers [31, 34]. Others, although measuring
transit time [39] or stool frequency [15], neglected to
examine stool consistency or collected stools only to
exclude illness [24]. Urine samples should also be routinely
collected to exclude urinary tract infection. This was done
in only two of the present 21 studies [34, 35].
It is often uncertain if treatment benefit attenuates with
time. However, the fact that colic spontaneously resolves
around 3–4 months precludes long-term studies because a
developmental bias may occur as the infant gut matures.
There are also many inherent difficulties, including ethical
issues, in conducting randomised studies in this vulnerable
population. The main outcome measure of most studies
was reduced crying duration, yet this was surprisingly
poorly defined. Although the well established ‘Wessel
criteria’ [3] were used in most (59%) studies to define
infantile colic for eligibility criteria, no standard measure
was applied to define colic as an outcome measure. Rather,
this outcome was variously presented as presence/absence
[35] or percentage reduction in symptoms of colic [17, 18],
reduced daily crying time [21, 30, 32–34, 39], or number of
crying episodes lasting [40 min [15] or [1 h [29]. While
some studies analysed crying time only, others combined
crying and fussing time, and another [37] analysed them
separately. There is a clear need for a standard, consistent,
and objective definition of a clinically important infant
crying duration and crying reduction specifically designed
for use in studies of infantile colic. As fussing is a very
subjective measure, a valid, reliable tool is needed to dif-
ferentiate among fussing, crying, and normal infant
behaviour before including fussing as an outcome.
Varied sources of bias occur in the studies surveyed. In
this field publication bias is likely as studies reporting
statistically significant results will be published more often.
Small sample size is also often a problem. Of the 12 level II
studies included here, six had a sample size of B 20. Bias
due to attrition is also a concern. For example, in one study
[32], 98 participants were recruited, but only 33 (34%)
completed. Recruitment for studies on infantile colic often
occurs predominantly at hospitals and paediatric clinics,
thus selecting a group that may not represent all infants
with colic. As some studies report an improvement in
colicky symptoms among infants in the control groups (in
one case by 37% [18]), a placebo effect is possible,
stressing the importance of study design. Many studies on
colic also arise through commercial links. Among 16
studies examining a formula-based intervention, most
acknowledged the company supplying the formula, and
many also acknowledged funding from infant food
manufacturers.
One of the strengths of the present review is the vigor-
ous and systematic nature of its methodology. Introduction
of bias was minimised by using the same data extraction
table and quality assessment checklist for each study.
Included studies were of high quality. Of the 12 level II
studies, eight were of positive, two were neutral and only
two were negative quality. Of the nine level III studies, six
were of positive quality. Both level of evidence and study
quality were considered when making conclusions, reduc-
ing the influence of lower quality studies. In addition, due
to rigorous searching of multiple databases and inclusion of
studies with evidence levels of IV and above, this sys-
tematic review is very comprehensive. One weakness is
that only one rather than two investigators analysed each
study. However, a second opinion was always sought
where there were aspects of doubt. As dietary interventions
and methods varied among studies, a meta-analysis could
not be conducted.
Conclusion
Varied dietary therapies have been investigated for treat-
ment of infantile colic, involving both changes to the
maternal diet and changes to infant formulae. Methodo-
logical inconsistencies are evident among studies. Use of a
universal definition to measure symptoms and consistent
methods for analysis of urine and faeces would improve
evidence. This systematic review suggests that in breastfed
infants, a hypoallergenic maternal diet may be beneficial
for reducing symptoms of infantile colic. However it is
acknowledged that a low hypoallergenic diet may be dif-
ficult to follow, particularly for an extensive length of time
and requires input from dieticians. In formula-fed infants,
the strongest evidence base supports the use of hydrolysed
formulae; there is some support for use of soy-based for-
mulae and no support for the use of fibre-supplemented
formulae. There is weak evidence supporting removal of
poorly digested carbohydrates from the infant’s diet. As
these dietary interventions are low risk, this evidence has
potential to impact current recommendations for the
treatment of infantile colic.
Conflict of interest The authors declare no conflicts of interest.
Matern Child Health J
123
Author's personal copy

References
1. Forsyth, B. W. C. (1985). Mothers’ perceptions of problems of
feeding and crying behaviors: a prospective study. AmericanJournal of Diseases of Children, 139, 269–272.
2. Jarman, R., & Sewell, J. (2000). Common behavioural and
developmental problems. In Paediatric handbook. Blackwell,
Oxford, pp 144–145.
3. Wessel, M. A., et al. (1954). Paroxysmal fussing in infancy,
sometimes called ‘‘colic’’. Pediatrics, 14, 421–434.
4. Brazelton, T. B. (1962). Crying in infancy. Pediatrics, 29,
579–588.
5. Lucassen, P. L. B. J., et al. (2001). Systematic review of the
occurrence of infantile colic in the community. Archives ofDisease in Childhood, 84, 398–403.
6. Kurth, E., et al. (2011). Crying babies, tired mothers: What do we
know? A systematic review. Midwifery, 27(2), 187–194.
7. Li, R., et al. (2008). Why mothers stop breastfeeding: mothers’
self-reported reasons for stopping during the first year. Pediatrics,122, S69–S76.
8. Papousek, M., & von Hofacker, N. (1998). Persistent crying in
early infancy: A non-trivial condition of risk for the developing
mother-infant relationship. Child: Care, Health and Develop-ment, 24(5), 395–424.
9. Beck, C. T. (1996). A meta-analysis of the relationship between
postpartum depression and infant temperament. NursingResearch, 45(4), 225–230.
10. Vik, T., et al. (2009). Infantile colic, prolonged crying and
maternal postnatal depression. Acta Paediatrica, 98, 1344–1348.
11. Barr, R. G. (2002). Changing our understanding of infant
colic. Archives of Pediatrics and Adolescent Medicine, 156,
1172–1174.
12. Barr, R. G., et al. (2006). Age-related incidence curve of hospi-
talized Shaken Baby Syndrome cases: Convergent evidence for
crying as a trigger to shaking. Child Abuse and Neglect, 30, 7–16.
13. American Academy of Pediatrics Committee on Child Abuse and
Neglect. (2001). Shaken Baby Syndrome: Rotational cranial
injuries—Technical report. Pediatrics, 108(1), 206–210.
14. Canadian Pediatric Society. (2001). Joint statement on Shaken
Baby Syndrome. Paediatrics & Child Health, 6(9), 663–667.
15. Savino, F., et al. (2006). Reduction of crying episodes owing to
infantile colic: A randomized controlled study on the efficacy of a
new infant formula. European Journal of Clinical Nutrition,60(11), 1304–1310.
16. Savino, F. (2007). Focus on infantile colic. Acta Paediatrica,96(9), 1259–1264.
17. Hill, D. J., et al. (1995). A low allergen diet is a significant
intervention in infantile colic: Results of a community-based
study. Journal of Allergy and Clinical Immunology, 96(6I),
886–892.
18. Hill, D. J., et al. (2005). Effect of a low-allergen maternal diet on
colic among breastfed infants: A randomized, controlled trial.
Pediatrics, 116(5), e709–e715.
19. Garrison, M. M., & Christakis, D. A. (2000). Early childhood:
colic, child development, and poisoning prevention: a systematic
review of treatments for infant colic. Pediatrics, 106(1 part 2),
184–190.
20. Lucassen, P. L., et al. (1998). Effectiveness of treatments for
infantile colic: Systematic review. British Medical Journal,316(7144), 1563–1569.
21. Arikan, D., et al. (2008). Effectiveness of massage, sucrose
solution, herbal tea or hydrolysed formula in the treatment of
infantile colic. Journal of Clinical Nursing, 17(13), 1754–1761.
22. Blumenthal, I. (2000). The gripe water story. Journal of the RoyalSociety of Medicine, 93, 172–174.
23. Forsyth, B. W. C. (1989). Colic and the effect of changing for-mulas: A double-blind, multiple-crossover study. Journal ofPediatrics, 115(4), 521–526.
24. Stahlberg, M. R., & Savilahti, E. (1986). Infantile colic and
feeding. Archives of Disease in Childhood, 61(12), 1232–1233.
25. National Health and Medical Research Council. (2009). NHMRCadditional levels of evidence and grades for recommendationsfor developers of guidelines, stage 2 consultation. Canberra,
Australia: NHMRC.
26. American Dietetic Association. (2008). ADA evidence analysismanual: Steps in the ADA evidence analysis process (4th ed.).
Chicago, IL: Scientific Affairs and Research, American Dietetic
Association.
27. Evans, R. W., et al. (1981). Maternal diet and infantile colic in
breast-fed infants. Lancet, 1(8234), 1340–1342.
28. Lust, K. D., et al. (1996). Maternal intake of cruciferous vege-
tables and other foods and colic symptoms in exclusively breast-
fed infants. Journal of the American Dietetic Association, 96(1),
46–48.
29. Oggero, R., et al. (1994). Dietary modifications versus dicyclo-
mine hydrochloride in the treatment of severe infantile colics.
Acta Paediatrica, 83(2), 222–225.
30. Taubman, B. (1988). Parental counseling compared with elimi-
nation of cow’s milk or soy milk protein for the treatment of
infant colic syndrome: A randomized trial. Pediatrics, 81(6),
756–761.
31. Berseth, C. L., et al. (2009). Clinical response to 2 commonly
used switch formulas occurs within 1 day. Clinical Pediatrics,48(1), 58–65.
32. Lucassen, P. L. B., et al. (2000). Infantile colic: Crying time
reduction with a whey hydrolysate: A double-blind, randomized,
placebo-controlled trial. Pediatrics, 106(6), 1349–1354.
33. Lothe, L., & Lindberg, T. (1989). Cow’s milk whey protein
elicits symptoms of infantile colic in colicky formula-fed infants:
A double-blind crossover study. Pediatrics, 83(2), 262–266.
34. Jakobsson, I., et al. (2000). Effectiveness of casein hydrolysate
feedings in infants with colic. Acta Paediatrica, 89(1), 18–21.
35. Lothe, L., et al. (1982). Cow’s milk formula as a cause of
infantile colic: A double-blind study. Pediatrics, 70(1), 7–10.
36. Estep, D. C., & Kulczycki, A., Jr. (2000). Colic in breast-milk-fed
infants: Treatment by temporary substitution of Neocate infant
formula. Acta Paediatrica, 89(7), 795–802.
37. Estep, D. C., & Kulczycki, A, Jr. (2000). Treatment of infant
colic with amino acid-based infant formula: A preliminary study.
Acta Paediatrica, 89(1), 22–27.
38. Campbell, J. P. M. (1989). Dietary treatment of infant colic: a
double-blind study. Journal of the Royal College of GeneralPractitioners, 39, 11–14.
39. Treem, W. R., et al. (1991). Evaluation of the effect of a fiber-
enriched formula on infant colic. Journal of Pediatrics, 119(5),
695–701.
40. Duro, D., et al. (2002). Association between infantile colic and
carbohydrate malabsorption from fruit juices in infancy. Pediat-rics, 109(5), 797–805.
41. Cole, C. R., et al. (1999). Consequences of incomplete carbo-
hydrate absorption from fruit juice consumption in infants.
Archives of Pediatrics and Adolescent Medicine, 153, 1098–
1102.
42. Piper, K. M., et al. (2007). The bioactive nature of human
breastmilk. Breastfeeding Reviews, 15(3), 5–10.
43. Walker, A. (2010). Breast milk as the gold standard for protective
nutrients. Journal of Pediatrics, 156(2 Suppl), S3–S7.
44. Lonnerdal, B. (2010). Novel insights into human lactation as a
driver of infant formula development. Nestle Nutrition WorkshopSeries Pediatrics Program, 66, 19–29.
Matern Child Health J
123
Author's personal copy

45. O’Connor, N. R. (2009). Infant formula. American Family Phy-sician, 79(7), 565–570.
46. Turck, D. (2007). Soy protein for infant feeding: what do we
know? Current Opinion in Clinical Nutrition & Metabolic Care,10(3), 360–365.
47. ESPGHAN Committee on Nutrition, et al. (2006). Soy protein
infant formulae and follow-on formulae: A commentary by the
ESPGHAN Committee on Nutrition. Journal of Pediatric Gas-troeterology and Nutrition, 42, 352–361.
48. Weizman, Z., et al. (1993). Efficacy of herbal tea preparation in
infantile colic. Journal of Pediatrics, 122(4), 650–652.
49. Shergill-Bonner, R. (2010). Infantile colic: practicalities of
management, including dietary aspects. Journal of Family HealthCare, 20(6), 206–209.
50. Landgren, K., et al. (2010). Acupuncture reduces crying in infants
with infantile colic: A randomised, controlled, blind clinical
study. Acupuncture in Medicine, 28(4), 174–179.
51. Nyeko, R., et al. (2010). Lactose intolerance among severely
malnourished children with diarrhoea admitted to the nutrition
unit, Mulago hospital, Uganda. BMC Pediatrics, 31(10), 1–9.
52. Whelan, K., et al. (2007). Kings stool chart. Kings College
London [cited Oct 2010]; Available from: http://www.kcl.ac.uk/
schools/biohealth/research/nutritional/stoolchart.
Matern Child Health J
123
Author's personal copy
Copyright © 2022 FDOKUMEN