
Reversal of Fibronectin and Opsonic Deficiency in Patients
10
Reversal of Fibronectin and Opsonic Deficiency in Patients A Controlled Study THOMAS M. SABA, PH.D., FRANK A. BLUMENSTOCK, PH.D., DHIRAJ M. SHAH, M.D., JOHN E. KAPLAN, PH.D., ESHIN CHO, M.S., WILLIAM SCOVILL, M.D.,* HOWARD STRATTON, PH.D.,t JONATHAN NEWELL, PH.D., MARC GOTTLIEB, M.D., NELL SEDRANSK, PH.D.,t ROBIN RAHM, M.D. Plasma fibronectin is an opsonic glycoprotein which augments reticuloendothelial phagocytic clearance of nonbacterial partic- ulates. We evaluated the influence of intravenous infusion of plasma cryoprecipitate on circulating immunoreactive fibronectin and associated opsonic activity at 0.5, 2.0, 4.0, 10, and 21 hr postinfusion in septic (n = 8) and nonseptic (n = 6) surgical and/or trauma patients with documented plasma fibronectin de- ficiency. The study was a randomized, double-blind, crossover clinical protocol in which fibronectin-poor (0.116 ± 0.025 mg/ ml) cryoprecipitate extracted plasma (placebo) was compared to fibronectin-rich (2.139 ± 0.161 mg/ml) plasma cryoprecipitate. Septic injured patients (149.37 ± 17.11 jg/ml) had lower (p < 0.05) plasma fibronectin levels than nonseptic injured patients (212.17 ± 7.14 jg/ml) and both were less (p < 0.05) than normal (330 ± 30 jg/ml). As tested in vitro with a peritoneal macrophage monolayer assay, cryoprecipitate manifested opsonic activity related to its fibronectin concentration. Intravenous in- fusion of fibronectin rich cryoprecipitate reversed both the im- munoreactive fibronectin and opsonic deficiency, while infusion of the placebo at a comparable total protein load did not reverse either deficient parameter. Reversal of fibronectin deficiency was more sustained in nonseptic injured patients as compared to septic injured patients. Thus, reversal of opsonic deficiency in septic and nonseptic injured patients is observed after infusion of plasma cryoprecipitate and not with infusion of fibronectin deficient plasma at comparable protein loads. Also, cryoprecip- itate extracted plasma may serve as an appropriate control so- lution for randomized studies evaluating the therapeutic value of fibronectin-rich plasma cryoprecipitate. FIBRONECTIN IS A large molecular weight dimeric gly- coprotein. It exists in a soluble form in blood and tissue fluids and in an insoluble form in basement mem- * Currently in the Department of Surgery at the University of Mary- land, Baltimore, Maryland. t Department of Mathematics at the State University of New York, Albany, New York. This study was supported by grant GM-21447 from the National Institute of General Medical Sciences. Reprint requests: Dr. Thomas M. Saba, Professor and Chairman, Department of Physiology, Albany Medical College of Union University, 47 New Scotland Avenue, Albany, NY 12208. Submitted for publication: May 30, 1983. From the Departments of Physiology and Surgery, Neil Hellman Medical Research Building, Albany Medical College of Union University, Albany, New York branes, extracellular matrices, and connective tis- sue.18'23'29'35 Fibronectin is identical to opsonic a2 surface binding (SB) glycoprotein3'26 or cold-insoluble globulin (CIg)'7 whose opsonic influence augments macrophage and leukocyte phagocytosis of nonbacterial particu- lates."" 134 Fibronectin has unique domains with high af- finity for collagen, fibrin, actin, Clq, and Staphylococcus aureus, as well as other molecules. '8'23'35 Its influence on particle phagocytosis coupled with its ability to augment cell-cell interaction and cell adhesion to a substratum suggests that fibronectin has opsonic as well as adhesive properties.29 Plasma fibronectin deficiency exists in trauma and burn patients, especially during invasive wound infection and/ or bacteremia postinjury.'6'25'31'33 Patients with dissemi- nated intravascular coagulation and organ failure also have very low plasma fibronectin levels.'9 Persistent fi- bronectin deficiency in the septic injured patient coexists with multiple organ failure, especially respiratory dis- tress.22'25'30'3",33 Since phagocytic host defense failure in the septic injured patient may be a contributing factor in the etiology of organ failure with sepsis, it has been suggested that reversal of plasma fibronectin deficiency may have value in the treatment of injured patients.25'29 Previous studies have reported that following the in- travenous infusion of fresh plasma cryoprecipitate into septic surgical or trauma patients there was an increase in opsonic activity expressed by plasma or serum har- vested from such patients.25'31 Accordingly, since cryo- precipitate is rich in plasma fibronectin (CIg), and since purified fibronectin augments phagocytosis,"l"l127 the re- versal of opsonic deficiency was attributed to the fibro- nectin content of cryoprecipitate.25 However, rapid al- 87
Transcript of Reversal of Fibronectin and Opsonic Deficiency in Patients

Reversal of Fibronectin and Opsonic Deficiency in Patients
A Controlled Study
THOMAS M. SABA, PH.D., FRANK A. BLUMENSTOCK, PH.D., DHIRAJ M. SHAH, M.D., JOHN E. KAPLAN, PH.D.,ESHIN CHO, M.S., WILLIAM SCOVILL, M.D.,* HOWARD STRATTON, PH.D.,t JONATHAN NEWELL, PH.D.,
MARC GOTTLIEB, M.D., NELL SEDRANSK, PH.D.,t ROBIN RAHM, M.D.
Plasma fibronectin is an opsonic glycoprotein which augmentsreticuloendothelial phagocytic clearance of nonbacterial partic-ulates. We evaluated the influence of intravenous infusion ofplasma cryoprecipitate on circulating immunoreactive fibronectinand associated opsonic activity at 0.5, 2.0, 4.0, 10, and 21 hrpostinfusion in septic (n = 8) and nonseptic (n = 6) surgicaland/or trauma patients with documented plasma fibronectin de-ficiency. The study was a randomized, double-blind, crossoverclinical protocol in which fibronectin-poor (0.116 ± 0.025 mg/ml) cryoprecipitate extracted plasma (placebo) was comparedto fibronectin-rich (2.139 ± 0.161 mg/ml) plasma cryoprecipitate.Septic injured patients (149.37 ± 17.11 jg/ml) had lower (p< 0.05) plasma fibronectin levels than nonseptic injured patients(212.17 ± 7.14 jg/ml) and both were less (p < 0.05) thannormal (330 ± 30 jg/ml). As tested in vitro with a peritonealmacrophage monolayer assay, cryoprecipitate manifested opsonicactivity related to its fibronectin concentration. Intravenous in-fusion of fibronectin rich cryoprecipitate reversed both the im-munoreactive fibronectin and opsonic deficiency, while infusionof the placebo at a comparable total protein load did not reverseeither deficient parameter. Reversal of fibronectin deficiencywas more sustained in nonseptic injured patients as comparedto septic injured patients. Thus, reversal of opsonic deficiencyin septic and nonseptic injured patients is observed after infusionof plasma cryoprecipitate and not with infusion of fibronectindeficient plasma at comparable protein loads. Also, cryoprecip-itate extracted plasma may serve as an appropriate control so-lution for randomized studies evaluating the therapeutic valueof fibronectin-rich plasma cryoprecipitate.
FIBRONECTIN IS A large molecular weight dimeric gly-coprotein. It exists in a soluble form in blood and
tissue fluids and in an insoluble form in basement mem-
* Currently in the Department of Surgery at the University of Mary-land, Baltimore, Maryland.
t Department of Mathematics at the State University of New York,Albany, New York.
This study was supported by grant GM-21447 from the NationalInstitute of General Medical Sciences.
Reprint requests: Dr. Thomas M. Saba, Professor and Chairman,Department of Physiology, Albany Medical College of Union University,47 New Scotland Avenue, Albany, NY 12208.
Submitted for publication: May 30, 1983.
From the Departments of Physiology and Surgery, NeilHellman Medical Research Building, Albany Medical
College of Union University, Albany, New York
branes, extracellular matrices, and connective tis-sue.18'23'29'35 Fibronectin is identical to opsonic a2 surfacebinding (SB) glycoprotein3'26 or cold-insoluble globulin(CIg)'7 whose opsonic influence augments macrophageand leukocyte phagocytosis of nonbacterial particu-lates."" 134 Fibronectin has unique domains with high af-finity for collagen, fibrin, actin, Clq, and Staphylococcusaureus, as well as other molecules.'8'23'35 Its influence onparticle phagocytosis coupled with its ability to augmentcell-cell interaction and cell adhesion to a substratumsuggests that fibronectin has opsonic as well as adhesiveproperties.29
Plasma fibronectin deficiency exists in trauma and burnpatients, especially during invasive wound infection and/or bacteremia postinjury.'6'25'31'33 Patients with dissemi-nated intravascular coagulation and organ failure alsohave very low plasma fibronectin levels.'9 Persistent fi-bronectin deficiency in the septic injured patient coexistswith multiple organ failure, especially respiratory dis-tress.22'25'30'3",33 Since phagocytic host defense failure inthe septic injured patient may be a contributing factorin the etiology of organ failure with sepsis, it has beensuggested that reversal of plasma fibronectin deficiencymay have value in the treatment of injured patients.25'29
Previous studies have reported that following the in-travenous infusion of fresh plasma cryoprecipitate intoseptic surgical or trauma patients there was an increasein opsonic activity expressed by plasma or serum har-vested from such patients.25'31 Accordingly, since cryo-precipitate is rich in plasma fibronectin (CIg), and sincepurified fibronectin augments phagocytosis,"l"l127 the re-versal of opsonic deficiency was attributed to the fibro-nectin content of cryoprecipitate.25 However, rapid al-
87

SABA AND OTHERS
terations of fibronectin as well as opsonic activity candevelop in the septic injured patient, which raises thepossibility that the increase in opsonic activity after cryo-precipitate infusion could have developed spontaneouslyor as a nonspecific event following the infusion of a largevolume of a protein-rich plasma fraction. While the initialclinical studies on reversal of fibronectin deficiency withcryoprecipitate infusion25 have been confirmed,5'22'30'3'all such patient studies were neither "blinded" nor "con-trolled" in that the temporal pattern of opsonic activityafter infusion ofa nonfibronectin enriched plasma fractionwas not studied. The present investigation was designedas a controlled study in which fibronectin-rich plasmacryoprecipitate was compared to fibronectin-poor cryo-precipitate extracted plasma which served as the placeboor control solution. This study was also designed to eval-uate the utility of using cryoprecipitate extracted plasmaas a control solution for future randomized, controlled,prospective clinical studies which will emphasize the in--fluence of cryoprecipitate infusion on multiple organfunction. In the present study, we evaluated the specificityof the fibronectin response to either plasma fraction aswell as the relationship of alterations of immunoreactivefibronectin to the opsonic activity as tested by bioassay.
Methods and Patients
Patients
Studies were performed on 14 surgical or trauma pa-tients. Entry into the study required the presence of tissueinjury due to either operation and/or trauma as well asfibronectin deficiency. Eight of these patients had doc-umented sepsis postsurgery or post-trauma, while six pa-tients were nonseptic at the time of study. Sepsis wasdefined as the existence of either a positive blood culture,invasive wound infection, or pneumonia. Informed con-sent was obtained in accordance with institutional policy.The protocol was approved by the Human Studies Com-mittee.
Experimental Protocol
The experimental design was that of a randomized,double-blind crossover clinical study. The primary in-vestigator and clinical staffinvolved in the blood samplingand/or patient care were "blinded" with regards to thenature of the solution being used. Within the crossoversequence, patients received either the cryoprecipitate first,followed 24 hr later by cryoprecipitate extracted plasma(placebo), or the placebo first, followed 24 hrs later bythe cryoprecipitate. Thus, all patients received both thecryoprecipitate and placebo over the approximate 48-hrexperimental interval. Plasma anticoagulated with EDTAand serum samples were obtained prior to entry in the
protocol (baseline), as well as at l/2, 2, 4, 10, and 21 hr(s)postinfusion of either cryoprecipitate or placebo. A 22-hr point after the first infusion was the baseline for thesecond infusion which began at 24 hr. The sequence wasrandomized utilizing a sealed card file system stratifiedaccording to both sex and age. Patients were categorizedas septic or nonseptic prior to the blind being "opened."
Electroimmunoassay of Fibronectin
Immunoreactive fibronectin in both plasma and serumwas measured by standard electroimmunoassay or rocketimmunoelectrophoresis utilizing monospecific antiserumto human fibronectin.4"16 3' For electroimmunoassay, thehuman fibronectin was purified by affinity chromatog-raphy utilizing gelatin-Sepharose'0 as previously docu-mented.2 Immunochemical purity of the fibronectin wastested by electroimmunoassay with unabsorbed, polyspe-cific antiserum, and homogeneity was ascertained by gra-dient polyacrylamide gel electrophoresis.2'3 Antiserum tohuman fibronectin used in the electroimmunoassay wasdeveloped in rabbits. Specificity of the antiserum wasdetermined by immunoelectrophoresis2'3 against affinitypurified human fibronectin and normal human plasmato verify the presence of a single precipitant arc.
Immunoturbidimetric Assay ofFibronectin
As an additional approach to measurement of plasmaand serum fibronectin, we also used the rapid immu-noturbidimetric assay as recently developed.24 Its utili-zation was important, since this assay requires only 10min for completion as opposed to 48 hr by electroim-munoassay. This allowed assessment of prevailing fibro-nectin levels on which to calculate replacement dosages.The immunoturbidimetric fibronectin assay (Biodynam-ics/BMC, Indianapolis, IN) is a kinetic immunologic assaybased on the interaction ofan antigen and an antibody.24In this assay, the purified immunoglobulin fraction fromsheep antiserum to purified human fibronectin and notwhole antiserum is utilized. The high affinity, monospe-cific antibody as well as calibrated fibronectin antigenstandards are available in the fibronectin kit purchasedcommercially. In the immunoturbidimetric assay, a 250-,ul aliquot of the antibody-buffer mixture was added tothe reaction cuvette with an automated micropipette sys-tem (Automated ABA-100 chemistry analyzer, AbbottDiagnostics, North Chicago, IL). Then, a 5-Ml sample ofeither serum or plasma to be assayed for fibronectin wasadded. At 1.0 min after addition of the antigen (serum,plasma, or purified standards) the initial extinction (El)was read using a 340- to 380-nm filter. A second extinction(E2) was read 10 min after initiation of the reaction. Theobserved difference (AE = E2-E,) between the two ex-tinctions was calculated and used to determine the fi-
88 Ann. Surg. * January 1984
FIBRONECTIN AND MACROPHAGE FUNCTION
bronectin concentration from the standard calibrationcurve.24
Peritoneal Macrophage Monolayer Assay
The opsonic activity of serum samples was assessedwith an adherent macrophage monolayer assay.' Serumand not plasma was used in this assay. This assay hasbeen previously compared to the standard liver slice op-sonic bioassay with experimental models of known op-sonic deficiency and shown to provide similar results.'Preparation ofthe monolayer as well as the gelatin coatingofthe test particles has been previously described in detail'and will be only highlighted for completeness. Briefly, ratperitoneal macrophages harvested 96 hrs after intraper-itoneal injection of 1% sodium caseinate were utilizedand 2 X 106 viable cells added per 16-mm well to developthe macrophage monolayer assay."" The target particleswere gelatinized 5'Cr labelled formalin-fixed sheep redblood cells (SRBC) suspended in Dulbecco's modifiedEagle's medium (DMEM) at a 4% hematocrit. The abilityfor fibronectin to augment internalization of gelatin-coated target particles by adherent peritoneal macrophageshas been confirmed by electron microscopy." The mac-rophage monolayer was incubated for 2.0 hr under hu-midified 5% C02-air in: 1.0 ml DMEM, 10 units of hep-arin, 20 ,l experimental serum, and 100 ul gelatinized5'Cr-labelled SRBC preparation. After 2 hr, the incubationmedia as well as the noningested SRBCs were removedby aspiration and the macrophage monolayers washedwith cold phosphate buffered saline (PBS). The mono-layers were then digested with 0.5 M NaOH and trans-ferred to scintillation tubes. Radioactivity was determinedwith an automated deep well gamma scintillation systemequipped with a 2-inch sodium iodide crystal. Blankscontaining macrophages and gelatinized 5'Cr-labelledSRBCs, but no added fibronectin or serum, were per-formed in each assay series, and uptake in the blanks wassubtracted to yield the net fibronectin mediated targetparticle uptake. Opsonic activity is expressed as the per-centage of injected target particle dose (%ID) removedper 2 X 106 macrophages. The dependency of opsonicactivity as determined by this bioassay on the presenceof fibronectin has been documented.'
Cryoprecipitate Preparation
Fresh human plasma cryoprecipitate (fibronectin-rich)was compared to cryoprecipitate-extracted plasma (fi-bronectin-poor) which served as the placebo control.Paired preparations were prepared specifically for thisstudy by the American Red Cross Blood Center in Albanyfrom fresh plasma obtained from the same donors. Thecryoprecipitate and/or cryoprecipitate-extracted plasmawas prepared from fresh plasma and packaged in com-
89
2000 1
2
"I...
2laC.)
0U'
2
i>
1000
500 1
400
300
200 F
100 F
0PLASMA
CRYOPRECIPITATE
Normal Plasm (33±303ig/ml)
-r+iCRYOPRECIPITATEEXTRACTED PLASMA
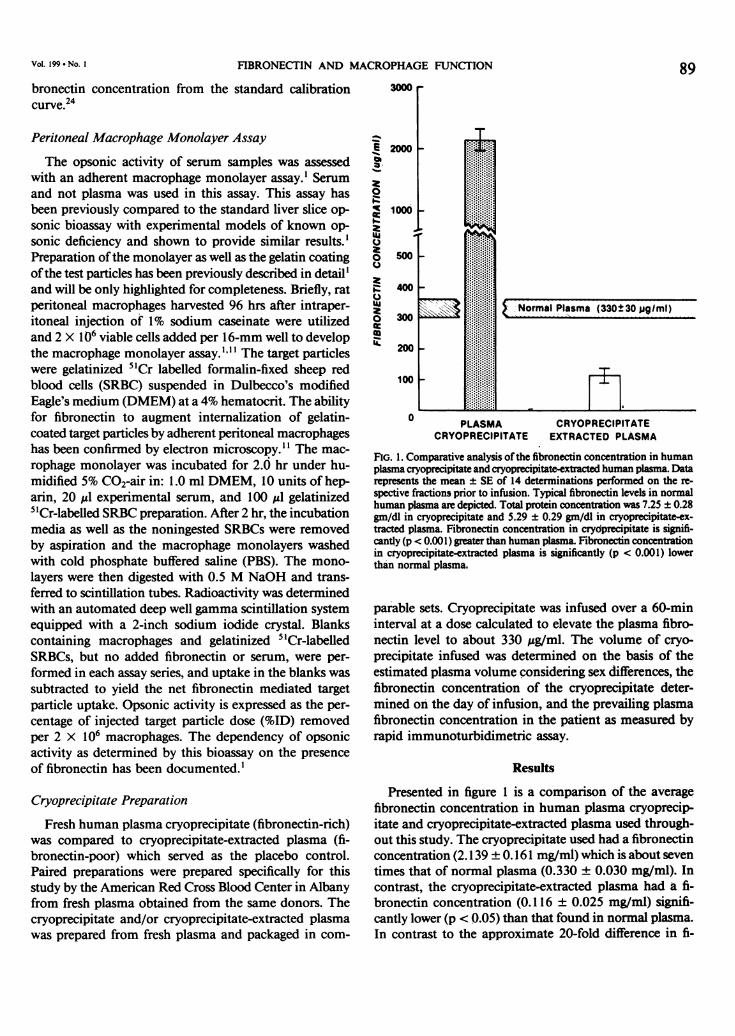
FIG. 1. Comparative analysis ofthe fibronectin concentration in humanplasma cryoprecipitate and cryoprecipitate-extracted human plasma. Datarepresents the mean ± SE of 14 determinations performed on the re-spective fractions prior to infusion. Typical fibronectin levels in normalhuman plasma are depicted. Total protein concentation was 7.25 ± 0.28gm/dl in cryoprecipitate and 5.29 ± 0.29 gm/dl in cryoprecipitate-ex-tracted plasma. Fibronectin concentration in crydprecipitate is signifi-cantly (p < 0.001) greater than human plasma. Fibronectin concentrationin cryoprecipitate-extracted plasma is significantly (p < 0.001) lowerthan normal plasma.
parable sets. Cryoprecipitate was infused over a 60-mininterval at a dose calculated to elevate the plasma fibro-nectin level to about 330 Ag/ml. The volume of cryo-precipitate infused was determined on the basis of theestimated plasma volume considering sex differences, thefibronectin concentration of the cryoprecipitate deter-mined on the day of infusion, and the prevailing plasmafibronectin concentration in the patient as measured byrapid immunoturbidimetric assay.
Results
Presented in figure 1 is a comparison of the averagefibronectin concentration in human plasma cryoprecip-itate and cryoprecipitate-extracted plasma used through-out this study. The cryoprecipitate used had a fibronectinconcentration (2.139 + 0. 161 mg/ml) which is about seventimes that of normal plasma (0.330 ± 0.030 mg/ml). Incontrast, the cryoprecipitate-extracted plasma had a fi-bronectin concentration (0.116 ± 0.025 mg/ml) signifi-cantly lower (p <0.05) than that found in normal plasma.In contrast to the approximate 20-fold difference in fi-
Vol. 199 * No. I
Ann. Surg. * January 1984
TABLE 1. Calculated Total Protein and Fibronectin Loads* Infusedinto Patients Given Plasma Cryoprecipitate or
Cryoprecipitate-Extracted Plasma
Totalt Protein Totalt FibronectinNo.
Infusate Studies (gm/infusion) (mg/infusion)
Plasmacryoprecipitate 14 11.32 ± 0.62 329.90 ± 25.90
(p >0.05) (p < 0.001)
Cryoprecipitate-extracted plasma 14 13.01 ± 0.44 29.80 ± 6.10
* Calculated as the volume of infusate administered times the total protein orfibronectin concentration. The average volume ofplasma cryoprecipitate was 154.35+ 8.56 ml. The average volume of cryoprecipitate-extracted plasma was 246.07+ 2.23 ml.
t The average total protein concentration was 7.25 ± 0.28 gm/dl in cryoprecipitateand 5.29 ± 0.29 gm/dl in cryoprecipitate-extracted plasma. The average fibronectinconcentration was 2.138 ± 0.161 mg/ml in cryoprecipitate and 0.1 16 ± 0.025 mg/ml in cryoprecipitate-extracted plasma.
bronectin concentration, the total protein concentrationwas 7.25 ± 0.28 gm/dl in plasma cryoprecipitate and 5.29+ 0.29 gm/dl in cryoprecipitate-extracted plasma. Thevolume of the placebo infusion was adjusted so that thetotal protein load given with either infusion was quitecomparable (Table 1).
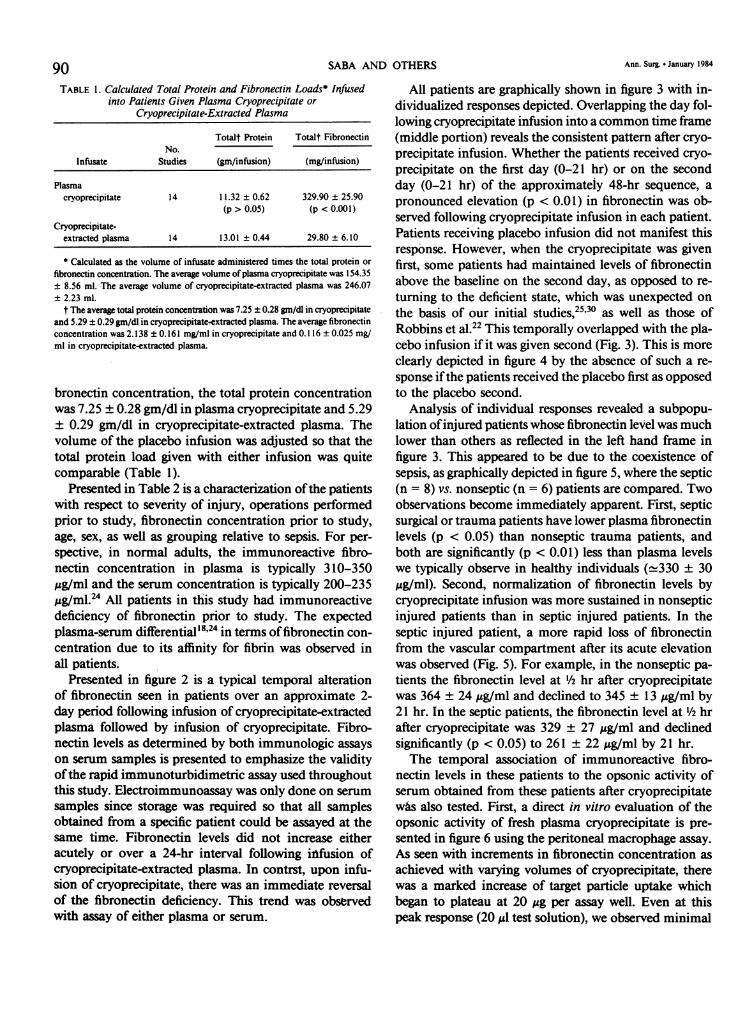
Presented in Table 2 is a characterization ofthe patientswith respect to severity of injury, operations performedprior to study, fibronectin concentration prior to study,age, sex, as well as grouping relative to sepsis. For per-spective, in normal adults, the immunoreactive fibro-nectin concentration in plasma is typically 310-350ug/ml and the serum concentration is typically 200-235,g/ml.24 All patients in this study had immunoreactivedeficiency of fibronectin prior to study. The expectedplasma-serum differential18'24 in terms offibronectin con-centration due to its affinity for fibrin was observed inall patients.
Presented in figure 2 is a typical temporal alterationof fibronectin seen in patients over an approximate 2-day period following infusion of cryoprecipitate-extractedplasma followed by infusion of cryoprecipitate. Fibro-nectin levels as determined by both immunologic assayson serum samples is presented to emphasize the validityofthe rapid immunoturbidimetric assay used throughoutthis study. Electroimmunoassay was only done on serumsamples since storage was required so that all samplesobtained from a specific patient could be assayed at thesame time. Fibronectin levels did not increase eitheracutely or over a 24-hr interval following infusion ofcryoprecipitate-extracted plasma. In contrst, upon infu-sion of cryoprecipitate, there was an immediate reversalof the fibronectin deficiency. This trend was observedwith assay of either plasma or serum.
All patients are graphically shown in figure 3 with in-dividualized responses depicted. Overlapping the day fol-lowing cryoprecipitate infusion into a common time frame(middle portion) reveals the consistent pattern after cryo-precipitate infusion. Whether the patients received cryo-precipitate on the first day (0-21 hr) or on the secondday (0-21 hr) of the approximately 48-hr sequence, apronounced elevation (p < 0.01) in fibronectin was ob-served following cryoprecipitate infusion in each patient.Patients receiving placebo infusion did not manifest thisresponse. However, when the cryoprecipitate was givenfirst, some patients had maintained levels of fibronectinabove the baseline on the second day, as opposed to re-turning to the deficient state, which was unexpected onthe basis of our initial studies,25'30 as well as those ofRobbins et al.22 This temporally overlapped with the pla-cebo infusion if it was given second (Fig. 3). This is moreclearly depicted in figure 4 by the absence of such a re-sponse ifthe patients received the placebo first as opposedto the placebo second.
Analysis of individual responses revealed a subpopu-lation ofinjured patients whose fibronectin level was muchlower than others as reflected in the left hand frame infigure 3. This appeared to be due to the coexistence ofsepsis, as graphically depicted in figure 5, where the septic(n = 8) vs. nonseptic (n = 6) patients are compared. Twoobservations become immediately apparent. First, septicsurgical or trauma patients have lower plasma fibronectinlevels (p < 0.05) than nonseptic trauma patients, andboth are significantly (p < 0.01) less than plasma levelswe typically observe in healthy individuals (-330 ± 30gg/ml). Second, normalization of fibronectin levels bycryoprecipitate infusion was more sustained in nonsepticinjured patients than in septic injured patients. In theseptic injured patient, a more rapid loss of fibronectinfrom the vascular compartment after its acute elevationwas observed (Fig. 5). For example, in the nonseptic pa-tients the fibronectin level at 1/2 hr after cryoprecipitatewas 364 ± 24 ;g/ml and declined to 345 ± 13 ,g/ml by21 hr. In the septic patients, the fibronectin level at 1/2 hrafter cryoprecipitate was 329 ± 27 ,Ag/ml and declinedsignificantly (p < 0.05) to 261 ± 22 ,ug/ml by 21 hr.The temporal association of immunoreactive fibro-
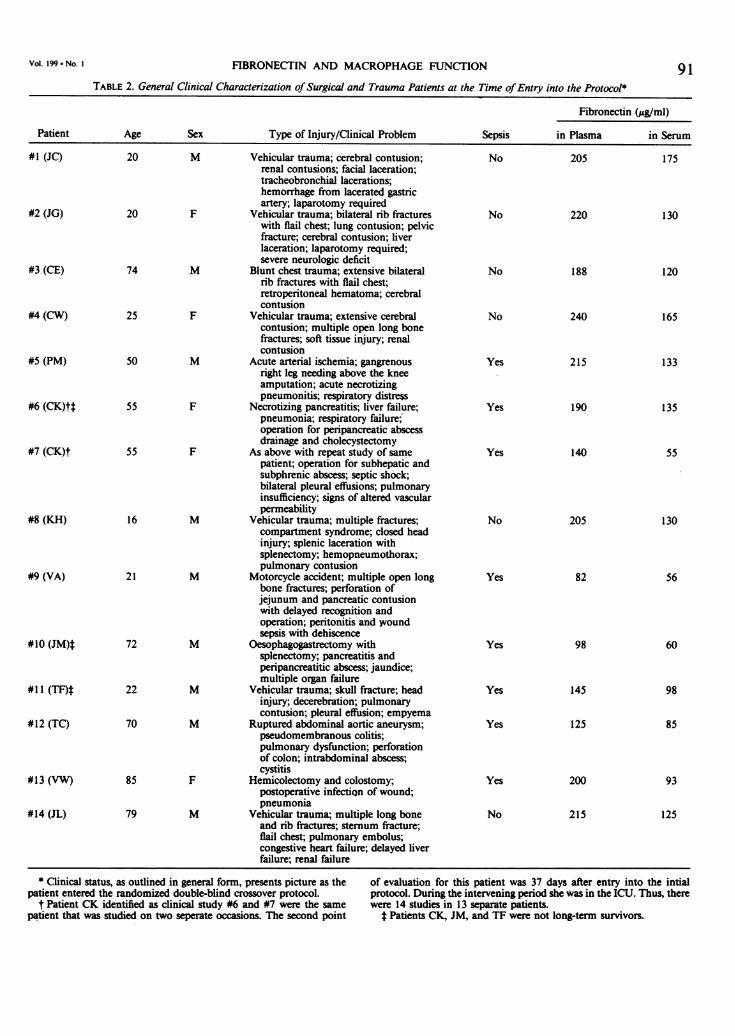
nectin levels in these patients to the opsonic activity ofserum obtained from these patients after cryoprecipitatewas also tested. First, a direct in vitro evaluation of theopsonic activity of fresh plasma cryoprecipitate is pre-sented in figure 6 using the peritoneal macrophage assay.As seen with increments in fibronectin concentration asachieved with varying volumes of cryoprecipitate, therewas a marked increase of target particle uptake whichbegan to plateau at 20 ,ug per assay well. Even at thispeak response (20 ,l test solution), we observed minimal
90 SABA AND OTHERS
FIBRONECTIN AND MACROPHAGE FUNCTION 91TABLE 2. General Clinical Characterization ofSurgical and Trauma Patients at the Time ofEntry into the Protocol*
Fibronectin (,ug/ml)Patient Age Sex Type of Injury/Clinical Problem Sepsis in Plasma in Serum
#1 (JC) 20 M Vehicular trauma; cerebral contusion; No 205 175renal contusions; facial laceration;tracheobronchial lacerations;hemorrhage from lacerated gastricartery; laparotomy required
#2 (JG) 20 F Vehicular trauma; bilateral rib fractures No 220 130with flail chest; lung contusion; pelvicfracture; cerebral contusion; liverlaceration; laparotomy required;severe neurologic deficit
#3 (CE) 74 M Blunt chest trauma; extensive bilateral No 188 120rib fractures with flail chest;retroperitoneal hematoma; cerebralcontusion
#4 (CW) 25 F Vehicular trauma; extensive cerebral No 240 165contusion; multiple open long bonefractures; soft tissue injury; renalcontusion
#5 (PM) 50 M Acute arterial ischemia; gangrenous Yes 215 133right leg needing above the kneeamputation; acute necrotizingpneumonitis; respiratory distress
#6 (CK)tt 55 F Necrotizing pancreatitis; liver failure; Yes 190 135pneumonia; respiratory failure;operation for peripancreatic abscessdrainage and cholecystectomy
#7 (CK)t 55 F As above with repeat study of same Yes 140 55patient; operation for subhepatic andsubphrenic abscess; septic shock;bilateral pleural effusions; pulmonaryinsufficiency; signs of altered vascularpermeability
#8 (KH) 16 M Vehicular trauma; multiple fractures; No 205 130compartment syndrome; closed headinjury; splenic laceration withsplenectomy; hemopneumothorax;pulmonary contusion
#9 (VA) 21 M Motorcycle accident; multiple open long Yes 82 56bone fractures; perforation ofjejunum and pancreatic contusionwith delayed recognition andoperation; peritonitis and woundsepsis with dehiscence
#10 (JM)* 72 M Oesophagogastrectomy with Yes 98 60splenectomy; pancreatitis andperipancreatitic abscess; jaundice;multiple organ failure
#11 (TF)t 22 M Vehicular trauma; skull fracture; head Yes 145 98injury; decerebration; pulmonarycontusion; pleural effusion; empyema
#12 (TC) 70 M Ruptured abdominal aortic aneurysm; Yes 125 85pseudomembranous colitis;pulmonary dysfunction; perforationof colon; intrabdominal abscess;cystitis
#13 (VW) 85 F Hemicolectomy and colostomy; Yes 200 93postoperative infection of wound;pneumonia
#14 (JL) 79 M Vehicular trauma; multiple long bone No 215 125and rib fractures; sternum fracture;flail chest; pulmonary embolus;congestive heart failure; delayed liverfailure; renal failure
* Clinical status, as outlined in general form, presents picture as the of evaluation for this patient was 37 days after entry into the intialpatient entered the randomized double-blind crossover protocol. protocol. During the intervening period she was in the ICU. Thus, there
t Patient CK identified as clinical study #6 and #7 were the same were 14 studies in 13 separate patients.patient that was studied on two seperate occasions. The second point t Patients CK, JM, and TF were not long-term survivors.
Vol. 199 * No. I

SABA AND OTHERS
&-i lmmunoturbidimrtric Assay (Plasma)v.0 Immunoturbidimetric Assay(Serum)
400 0-0 Electrolmmunossay (Serum)
300
@ 200
/~~~~~~~~~~~~~~~~...
c
Cryoprgclpltats PlasmaExtracted Plasma Cryoprecipitiat
4 .24 1.0 0.5 2 4 10 21 22 0.5 2 4 10 21
PRE-INFUSION POST-INFUSION (hr) POST-INFUSION (hr)
FIG. 2. Comparison of electroimmunoassay and immunoturbidimetricassay of fibronectin in serum (electroimmunoassay was not done onplaima samples). Plasma and serum concentrations of fibronectin inseptic trauma patient (VW), as well as their temporal alterations followingintravenous infusion of either plasma cryoprecipit#te or cryoprecipitate-extracted plasma is presented.
opsoniC activity by the cryoprecipitate extracted plasmawhen diluted and used in similar volumes (Fig. 6).
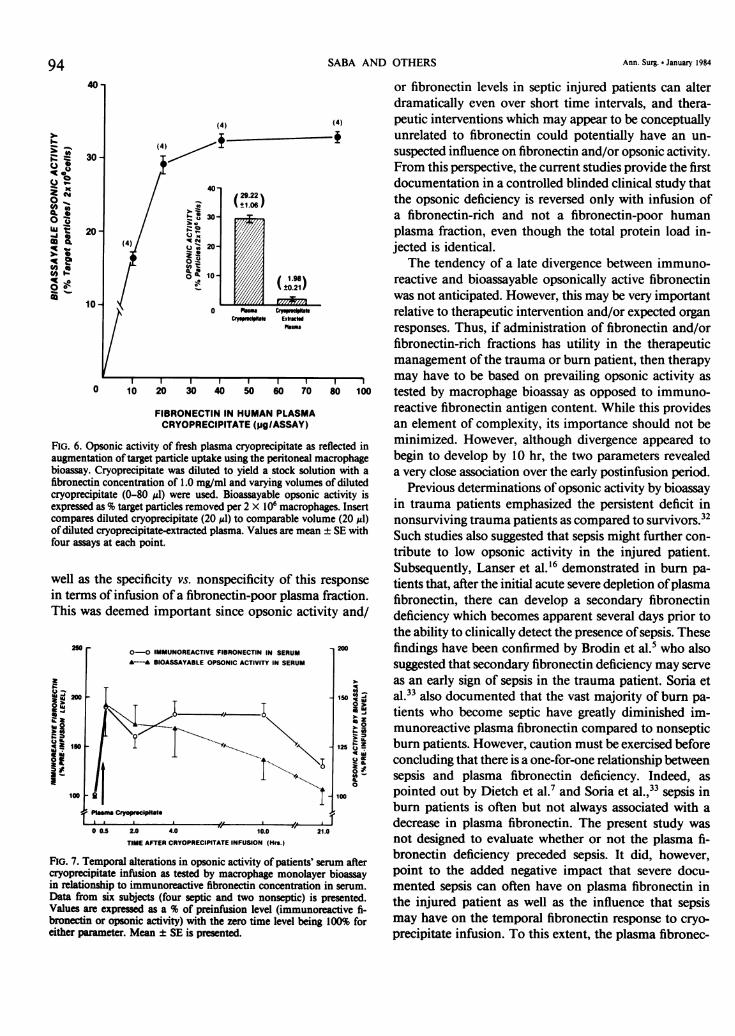
Figure 7 presents bioassayable and immunoreactivefibronectin prior to and within 4 hr of cryoprecipitate
450*
400
'aUk
0
!a
-a(a
350-
300-
250-
200-
150-
100-
50-B.-o 0.21 HRS-PI - - 0.21 HRS -..I.--- 0.21 HRS-.|
PLACEBO CRYOPRECIPITATEor
CRYOPRECIPITATE PLACEBO
FlG. 3. Temporal alterations of plasma fibronectin prior to and at ½/2,2, 4, and 21 hi(s) foliowing the infusion of fibronectin-rich plasmacryoprecipitate or placebo (cryoprecipitate-extracted plasma). Analysisintervals are over a 2-day period as portrayed (21-hr protocol = day).For all patients, the initial postcryoprecipitate infusion interval wasgraphkaliy depicte,d within the same window (middle portion) to portraythe consistent acute reversal of fibronectin deficiency. Each continuousline represents an individual patient study (n = 14). Samples from onepatienf(-) we)e not available beyond point indicated. Acute elevationof fibronectin after cryoprecipitate was highly significant (p < 0.01). Noigi ant increase was observed after placebo (cryoprecipitate-extractedplasma) infusion (left portion).
infusion using serum and not plasma in both assays. Thereis a very close association between the two parametersof opsonic activity of the serum and fibronectin levels inthe serum. Thus, acute elevation of fibronectin results inan immediate increased expression of opsonic activity byserum derived from such patients. However, quite un-expectedly the bioassayable opsonic activity appeared todecline sooner after cryoprecipitate, especially over 10-21 hr as compared to immunoreactive fibronectin. Com-parison of the early opsonic response seen with cryopre-cipitate to that observed after placebo (Fig. 8) clearlyemphasized the specificity of this response. There was no
significant (p < 0.05) increase in opsonic activity afterinfusion of the fibronectin-poor placebo. It should benoted, with reference to the small but potentially im-portant divergence of immunoreactive fibronectin andbioassayable fibronectin seen over the 21-hr period (Fig.7), that the peritoneal macrophage monolayer assay wasonly performed on samples available from 6 of the 14patients studied. Thus, firm conclusions as to the existenceof a divergence cannot be made. However, since thesesix individuals included both septic and nonseptic pa-tients, they are most likely representative of the entiregroup's response.
Discussion
The importance of nonspecific phagocytic defensemechanisms in modulating the host's response to trauma,burn, and septic shock has been previously emphasized.29Fibronectin appears to be an important humoral mod-ulator of the phagocytic clearance of nonbacterial par-ticulates such as fibrin/fibrinogen complexes, injured tis-sue collagenous debris, cytoskeletal debris, and denaturedproteins. Fibronectin also binds to Staphylococcus au-
reus14 and some evidence suggests augmentation of S.aureus phagocytosis by fibronectin under in vitro con-
ditions,'5 althovgh this aspect remains controversial.2'One form of fibronectin is soluble and found in plasma,lymph, and other tissue fluids. It manifests opsonicactivity"3'26 and a high affinity for denatured collagen,actin, and fibrin. A second form of fibronectin is insolubleat neutral pH and is widely distributed in the extracellularmatrix and associated basement membranes. It is sus-
pected to exert an adhesive role in vivo in maintainingcell-cell interaction and cell adhesion to a substratum.'2'35
Fibronectin deficiency early post-trauma or burn, as
well as during later periods of systemic sepsis, is welldocumented.'6'31'33 Subsequent gradual elevation in fi-bronectin levels has been documented during the recovery
from a septic interval in burn patients.'6 Liver Kupifer
cell clearance ofgelatin-coated particles from the vascularcompartment is closely correlated with endogenousplasma fibronectin concentrations.427 28 This is not cell
92 Ann. Surg. * January 1984

FIBRONECTIN AND MACROPHAGE FUNCTION
specific, in that blood monocytes, alveolar macrophages,polymorphonuclear leukocytes, as well as peritonealmacrophages will increase their uptake of test particlesin the presence of fibronectin' 1,34 as reviewed.'8,29The common identity of plasma fibronectin (cold-in-
soluble globulin) and opsonic a2 surface bindingglycoprotein3'26 formed the conceptual basis for utilizationofhuman plasma cryoprecipitate as an experimental mo-dality to reverse fibronectin deficiency in septic surgicaland trauma patients.25 An elevation in opsonic activityas tested with the liver slice assay was observed in theseinitial longitudinal patient studies.25'3' However, controlsinjected with a nonfibronectin-rich plasma fraction were
not done for comparison. Subsequent clinical studies
A. PLACEBO FIR8T-CRYOPRECIPITATE SECOND
4O0 r
300
200
cryoprecipitateExtracted Plasma
PlasmaCryoprecipitate
4 10 210 BL 0.5 2 4 10 21 22 0.5 2
TIME AFTER INFUSION (Hrs.)
5007
e
400-
0
2
°U 300-20cc
vq 200-
C,,
100
'1C
93
ASEPTIC PATIENTS0 NON-SEPTIC PATIENTS
I I I/IBASELINE 0.5 2.0 4.0 21
TIME AFTER CRYOPRECIPITATE (hrs)
FIG. 5. The influence of coexistent sepsis postsurgery or post-traumaon prevailing plasma fibronectin as well as the fibronectin response tocryoprecipitate infusion. The mean ± SE is presented for baseline plasmafibronectin in both the septic (149.37 ± 17.11 Ag/ml) patients (n = 8)and the nonseptic (212.17 ± 7.14 gg/ml) patients (n = 6). Prior tocryoprecipitate infusion, plasma fibronectin levels in both groups were
significantly (p < 0.01) less than normal (330 ± 30 Mg/ml) and significantly(p < 0.05) different from each other. In the septic group, each patientshowed a decline over the 21-hr period, which was significantly (p < 0.05)different than the pattern seen in the nonseptic patients.
3. CRYOPRECIPITArTE FIR8T-PLACEBO SECOND
400 r I
300
200 F
100Plasma
CryopreclpltateCryoprecipitale
Extracted Plasma
OLSL 0.5 2 4 10 21 22 0.5 2 4 10 21
TIME AFTER INFUSION (Nrs.)
FIG. 4. Plasma fibronectin levels in two typical patients (JM and CK),contrasting the temporal pattern as a function of the injection sequencefor plasma cryoprecipitate or placebo. Acute elevation of fibronectinwas observed after cryoprecipitate injection. Placebo did not elevatefibronectin (top graph) but a paradoxical high level ofplasma fibronectinwas seen when the placebo was given second (bottom graph), reflectiveof a secondary rise and/or maintained level seen after cryoprecipitatein many patients.
documented normalization of the peripheral vascular re-
sponse to an ischemic stimulus3' as well as an improve-ment in the ventilation-perfusion balance30 after infusionof fresh plasma cryoprecipitate into septic injured patients.Confirmatory reports by others have also provided ad-ditional radiologic, pulmonary, renal, and metabolic ev-
idence pointing to an improvement in organ function inseptic trauma patients with cryoprecipitate infusion.5 22The fact that deficiency of plasma fibronectin increasesthe degree of lung vascular injury observed with sepsisin sheep20 suggests that this may be an additional factorcontributing to the relationship of fibronectin deficiencyto respiratory distress with septic shock. Indeed, recentstudies by Soria et al.33 emphasize the association ofsevereplasma fibronectin deficiency to existence of pulmonaryfailure in burn patients.The present controlled study was a logical and necessary
extension of these previous clinical observations, whichwere not done with comparison to a placebo or controlsolution. Most important was whether or not the reversalof the immunoreactive fibronectin deficiency would ini-tiate a consistent reversal of the opsonic deficiency as
Vol. 199 * No. I
SABA AND OTHERS
)1.
C
-K P0
2 6,R0 Stoui8
co Ico _
30
20 -
10*
4) (4)
i ~ ~~ f
a.,7
40-{29.22(+i.06Z
30-
20-
~~~(±t0.211
0 Phm C IaIa
Crysp OUcill Extrwded
Rasma
0 10 20 30 40 50 60 70 80
FIBRONECTIN IN HUMAN PLASMACRYOPRECIPITATE (pg/ASSAY)
FIG. 6. Opsonic activity of fresh plasma cryoprecipitate as reflected inaugmentation of target particle uptake using the peritoneal macrophagebioassay. Cryoprecipitate was diluted to yield a stock solution with afibronectin concentration of 1.0 mg/ml and varying volumes of dilutedcryoprecipitate (0-80 Al) were used. Bioassayable opsonic activity isexpressed as % target particles removed per 2 X 106 macrophages. Insertcompares diluted cryoprecipitate (20 Al) to comparable volume (20 1)of diluted cryoprecipitate-extracted plasma. Values are mean ± SE withfour assays at each point.
well as the specificity vs. nonspecificity of this response
in terms of infusion of a fibronectin-poor plasma fraction.This was deemed important since opsonic activity and/
0-0 IMMUNOREACTIVE FIBRONECTIN IN SERUMA--A BIOASSAYABLE OPSONIC ACTIVITY IN SERUM
200 1500
mz
0
I~~~~~~~~~~~~~~~~~~~~~~~I
SI ~~~~~~~~~~~~0Plasm Cryoprcipltte
0 0.S 2.0 4.0 10.0 21.0
TIME AFTER CRYOPRECIPITATE INFUSION (Mrs.)
FIG. 7. Temporal alterations in opsonic activity of patients' serum aftercryoprecipitate infusion as tested by macrophage monolayer bioassayin relationship to immunoreactive fibronectin concentration in serum.Data from six subjects (four septic and two nonseptic) is presented.Values are expressed as a % of preinfusion level (immunoreactive fi-bronectin or opsonic activity) with the zero time level being 100% foreither parameter. Mean ± SE is presented.
or fibronectin levels in septic injured patients can alterdramatically even over short time intervals, and thera-peutic interventions which may appear to be conceptuallyunrelated to fibronectin could potentially have an un-
suspected influence on fibronectin and/or opsonic activity.From this perspective, the current studies provide the firstdocumentation in a controlled blinded clinical study thatthe opsonic deficiency is reversed only with infusion ofa fibronectin-rich and not a fibronectin-poor humanplasma fraction, even though the total protein load in-jected is identical.
The tendency of a late divergence between immuno-reactive and bioassayable opsonically active fibronectinwas not anticipated. However, this may be very importantrelative to therapeutic intervention and/or expected organ
responses. Thus, if administration of fibronectin and/orfibronectin-rich fractions has utility in the therapeuticmanagement of the trauma or burn patient, then therapymay have to be based on prevailing opsonic activity as
tested by macrophage bioassay as opposed to immuno-reactive fibronectin antigen content. While this providesan element of complexity, its importance should not beminimized. However, although divergence appeared tobegin to develop by 10 hr, the two parameters revealeda very close association over the early postinfusion period.
Previous determinations of opsonic activity by bioassayin trauma patients emphasized the persistent deficit innonsurviving trauma patients as compared to survivors.32Such studies also suggested that sepsis might further con-tribute to low opsonic activity in the injured patient.Subsequently, Lanser et al.'6 demonstrated in burn pa-tients that, after the initial acute severe depletion ofplasmafibronectin, there can develop a secondary fibronectindeficiency which becomes apparent several days prior tothe ability to clinically detect the presence ofsepsis. Thesefindings have been confirmed by Brodin et al.' who alsosuggested that secondary fibronectin deficiency may serveas an early sign of sepsis in the trauma patient. Soria etal.33 also documented that the vast majority of burn pa-tients who become septic have greatly diminished im-munoreactive plasma fibronectin compared to nonsepticburn patients. However, caution must be exercised beforeconcluding that there is a one-for-one relationship betweensepsis and plasma fibronectin deficiency. Indeed, aspointed out by Dietch et al.7 and Soria et al.,33 sepsis inburn patients is often but not always associated with adecrease in plasma fibronectin. The present study wasnot designed to evaluate whether or not the plasma fi-bronectin deficiency preceded sepsis. It did, however,point to the added negative impact that severe docu-mented sepsis can often have on plasma fibronectin inthe injured patient as well as the influence that sepsismay have on the temporal fibronectin response to cryo-precipitate infusion. To this extent, the plasma fibronec-
94 Ann. Surg. a January^ 1984
(4
FIBRONECTIN AND MACROPHAGE FUNCTION
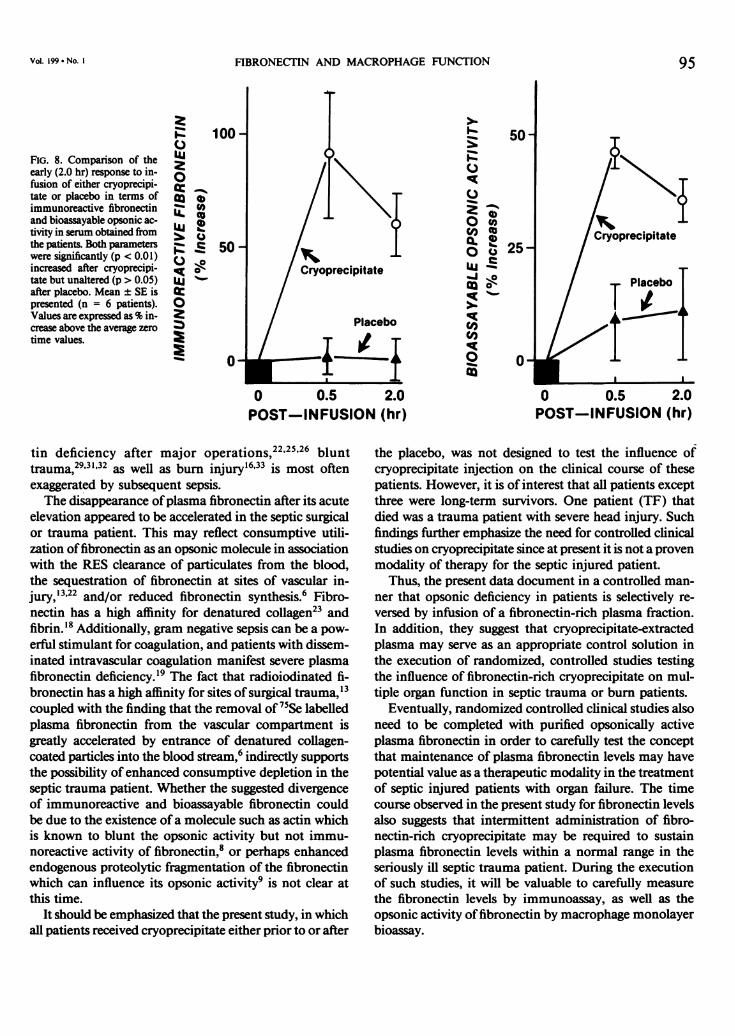
FIG. 8. Comparison of theearly (2.0 hr) response to in-fusion of either cryoprecipi-tate or placebo in terms ofimmunoreactive fibronectinand bioassayable opsonic ac-tivity in serum obtained fromthe patients. Both parameterswere significantly (p < 0.01)increased after cryoprecipi-tate but unaltered (p > 0.05)after placebo. Mean ± SE ispresented (n = 6 patients).Values are expressed as % in-crease above the average zerotime values.
o0t:-C.
co
0 0.5POST-INFUSION
tin deficiency after major operations,22'25'26 blunttrauma,29332 as well as burn injury 633 is most oftenexaggerated by subsequent sepsis.The disappearance ofplasma fibronectin after its acute
elevation appeared to be accelerated in the septic surgicalor trauma patient. This may reflect consumptive utili-zation offibronectin as an opsonic molecule in associationwith the RES clearance of particulates from the blood,the sequestration of fibronectin at sites of vascular in-jury,'22 and/or reduced fibronectin synthesis.6 Fibro-nectin has a high affinity for denatured collagen23 andfibrin.'8 Additionally, gram negative sepsis can be a pow-erful stimulant for coagulation, and patients with dissem-inated intravascular coagulation manifest severe plasmafibronectin deficiency.19 The fact that radioiodinated fi-bronectin has a high affinity for sites of surgical trauma,'3coupled with the finding that the removal of 75Se labelledplasma fibronectin from the vascular compartment isgreatly accelerated by entrance of denatured collagen-coated particles into the blood stream,6 indirectly supportsthe possibility ofenhanced consumptive depletion in theseptic trauma patient. Whether the suggested divergenceof immunoreactive and bioassayable fibronectin couldbe due to the existence of a molecule such as actin whichis known to blunt the opsonic activity but not immu-noreactive activity of fibronectin,8 or perhaps enhancedendogenous proteolytic fragmentation of the fibronectinwhich can influence its opsonic activity9 is not clear atthis time.
It should be emphasized that the present study, in whichall patients received cryoprecipitate either prior to or after
50
cO(u0 o 25-
Iaj'
Co0 0CO c
° 25-
2.0(hr)
95
0 0.5POST-INFUSION
2.0(hr)
the placebo, was not designed to test the influence ofcryoprecipitate injection on the clinical course of thesepatients. However, it is of interest that all patients exceptthree were long-term survivors. One patient (TF) thatdied was a trauma patient with severe head injury. Suchfindings further emphasize the need for controlled clinicalstudies on cryoprecipitate since at present it is not a provenmodality of therapy for the septic injured patient.
Thus, the present data document in a controlled man-ner that opsonic deficiency in patients is selectively re-versed by infusion of a fibronectin-rich plasma fraction.In addition, they suggest that cryoprecipitate-extractedplasma may serve as an appropriate control solution inthe execution of randomized, controlled studies testingthe influence of fibronectin-rich cryoprecipitate on mul-tiple organ function in septic trauma or burn patients.
Eventually, randomized controlled clinical studies alsoneed to be completed with purified opsonically activeplasma fibronectin in order to carefully test the conceptthat maintenance of plasma fibronectin levels may havepotential value as a therapeutic modality in the treatmentof septic injured patients with organ failure. The timecourse observed in the present study for fibronectin levelsalso suggests that intermittent administration of fibro-nectin-rich cryoprecipitate may be required to sustainplasma fibronectin levels within a normal range in theseriously ill septic trauma patient. During the executionof such studies, it will be valuable to carefully measurethe fibronectin levels by immunoassay, as well as theopsonic activity of fibronectin by macrophage monolayerbioassay.
Vol. 199 *, No. I

96 SABA AND OTHERS Ann. Surg. * January 1984
Acknowledgments
Utilization of the Albany Trauma Center (GM-15426) and the sec-retarial assistance of Mrs. Deborah Moran, Miss Susan Churan, andMrs. Maureen Davis are gratefully acknowledged.
References1. Blumenstock FA, Saba TM, Roccario E, et al. Opsonic fibronectin
after trauma and particle injection as determined by a peritonealmacrophage monolayer assay. J Reticuloendothel Soc 1981;30:61-71.
2. Blumenstock FA, Saba TM, Weber P. An affinity method for therapid purification ofopsonic a2SB glycoprotein from serum. AdvShock Res 1979; 2:55-71.
3. Blumenstock FA, Saba TM, Weber P, Laffin R. Biochemical andimmunological characterization of human opsonic a2-SB gly-coprotein: its identity with cold-insoluble globulin. J Biol Chem1978; 253:4287-4291.
4. Blumenstock FA, Weber P, Saba TM, Laffin R. Electroimmunoassayof alpha-2-opsonic protein during reticuloendothelial blockade.Am J Physiol 1977; 232:R80-R87.
5. Brodin B, Berghem L, Frigerg-Nielson S, et al. Fibronectin in thetreatment of septicemia-a preliminary report. In RugheimerE, Wawersik J, Zindler M, eds. Excerpta Medica. Hamburg,Germany: Seventh World Congress ofAnesthesiology, 1980; 504-505.
6. Deno DC, Lewis E, Saba TM. Dynamics of plasma fibronectinevaluated by isotopic disappearance kinetics. Fed Proc 1982;41:706.
7. Dietch EA, Gelder F, McDonald JC. The relationship between CIgdepletion and peripheral neutrophil function in rabbits and man.J Trauma 1982; 22:469-475.
8. Dillon BC, Estes J, Saba TM, et al. Actin-induced reticuloendothelialphagocytic depression as mediated by its interaction with fibro-nectin. Exp Molec Pathol 1982; in press. Abstract in J Res 1981;43a.
9. Ehrlich MI, Krushell JS, Blumenstock FA, Kaplan JE. Depressionof phagocytosis by plasmin degradation products of plasmin fi-bronectin. J Lab Clin Med 1981; 98:263-271.
10. Engvall E, Ruoslahti E. Binding of soluble form of fibroblast surfaceprotein, fibronectin, to collagen. Int J Cancer 1977; 20:1-5.
11. Gudewicz PW, Molnar J, Lai MZ, et al. Fibronectin mediated uptakeof gelatin-coated latex particles by peritoneal macrophages. JCell Biol 1980; 87:427-433.
12. Hynes RO, Yamada KM. Fibronectins: multifunctional modularglycoproteins. J Cell Biol 1982; 95:369-377.
13. Kaplan JE, Molnar J, Saba TM, Allen C. Comparative disappearanceand localization of isotopically labelled opsonic protein and sol-uble albumin following surgical trauma. J Reticuloendothel Soc1976; 20:375-384.
14. Kuusela P. Fibronectin binds to Staphylococcus aureus. Nature1978; 276:718-720.
15. Lanser ME, Saba TM. Fibronectin as a co-factor necessary for op-timal granulocyte phagocytosis of Staphylococcus aureus. J Re-ticuloendothel Soc 1981; 30:415-424.
16. Lanser ME, Saba TM, Scovill WA. Opsonic glycoprotein (plasmafibronectin) levels after burn injury: relationship to extent ofburn and development of sepsis. Ann Surg 1980; 192:776-782.
17. Mosesson MW, Umfleet RA. The cold-insoluble globulin ofhuman
plasma. I: Purification, primary characterization and relationshipto fibrinogen and other cold-insoluble fraction components. JBiol Chem 1970; 245:5728-5736.
18. Mosher DF. Fibronectin. Prog Hemost Thromb 1980; 5:111-151.19. Mosher DR, Williams EM. Fibronectin concentration is decreased
in plasma of severely ill patients with disseminated intravascularcoagulation. J Lab Clin Med 1978; 91:729-735.
20. Niehaus GD, Schumacker PT, Saba TM. Influence of opsonic fi-bronectin deficiency on lung fluid balance during bacterial sepsis.J Appl Physiol: Resp Envir Exer Physiol 1980; 49:693-699.
21. Proctor RA, Prendergast E, Mosher DF. Fibronectin mediated at-tachment ofStaphylococcus aureus to human neutrophils. Blood1982; 59:681-687.
22. Robbins AB, Doran JE, Reese AC, Mansberger AR. Cold-insolubleglobulin levels in operative trauma: serum depletion, woundsequestration, and biological activity. An experimental and clinicalstudy. Am Surg 1980; 46:663-672.
23. Ruoslahti E, Engvall E, Hayman E. Fibronectin: current conceptsof its structure and function. Collagen Res 1981; 1:95-128.
24. Saba TM, Albert WH, Blumenstock FA, et al. Evaluation of a rapidimmunoturbidimetric assay for opsonic plasma fibronectin insurgical and trauma patients. J Lab Clin Med 1981; 98:482-491.
25. Saba TM, Blumenstock FA, Scovill WA, Bernard H. Cryoprecipitatereversal of opsonic a2 surface binding glycoprotein deficiency inseptic surgical and trauma patients. Science 1978; 201:622-624.
26. Saba TM, Blumenstock FA, Weber P, Kaplan JE. Physiologic rolefor cold-insoluble globulin in systemic host defense: implicationsof its characterization as the opsonic a2SB glycoprotein. AnnNY Acad Sci 1978; 312:43-55.
27. Saba TM, Cho E. Reticuloendothelial systemic response to operativetrauma as influenced by cryoprecipitate or cold-insoluble globulintherapy. J Reticuloendothel Soc 1979; 26:171-186.
28. Saba TM, DiLuzio NR. Reticuloendothelial blockade and recoveryas a function of opsonic activity. Am J Physiol 1969; 216:197-205.
29. Saba TM, Jaffe E. Plasma fibronectin (opsonic glycoprotein): itssynthesis by vascular endothelial cells and role in cardiopulmonaryintegrity after trauma are related to reticuloendothelial function.Am J Med 1980; 68:577-594.
30. Scovill WA, Annest S, Saba TM, et al. Cardiovascular hemodynamicsafter opsonic a2 surface binding glycoprotein therapy in injuredpatients. Surgery 1979; 86:284-293.
31. Scovill WA, Saba TM, Blumenstock FA, et al. Opsonic a2 surfacebinding glycoprotein therapy during sepsis. Ann Surg 1978;188:521-529.
32. Scovill WA, Saba TM, Kaplan JE, et al. Deficits in reticuloendothelialhumoral control mechanisms in patients after trauma. J Trauma1976; 16:898-904.
33. Soria J, Soria C, Hourdille P, et al. Fibronectin level in burnstpatients-confrontation with the level of other factors of coag-ulation-clinical application. In Egbring R, Klingemann HG,eds. Factor XIII and fibronectin. Marburg, Germany: Die Med-izinische Verlagsgesellschaft mbH, 1983; 245-254.
34. Van De Water L III, Schroeder S, Crenshaw EB III, Hynes RO.Phagocytosis of gelatin-latex particles by a murine macrophageline is dependent on fibronectin and heparin. J Cell Biol 1981;90:32-39.
35. Yamada KM, Olden K. Fibronectins-adhesive glycoproteins of cellsurface and blood. Nature 1978; 275:179-184.




















