Family studies of IgA deficiency
10
Immunoflenetics21: 333-342, 1985 Im nlUllO= genetics © Springer-Verlag 1985 Family Studies of IgA Deficiency Alan N. Wilton, Trevor J. Cobain, and Roger L. Dawkins Departments of Clinical Immunology, Royal Perth Hospital and The Queen Elizabeth II Medical Centre, Perth, WesternAustralia Abstract. Seventeen immunoglobulin A (IgA)-deficient subjects and other members from 13 families were examined at HLA-A, B and DR, C4A, C4B, and Bf loci. Of the 29 independent haplotypes in the IgA-deficient subjects, 22 included deletions, duplications, or defects at the C4 or 21-hydroxylase loci. It is suggested that there may be a gene regulating serum IgA concentrations in this same region of chromosome 6. Three main supratypes explain most of the previously reported HLA associations with IgA deficiency. These are A1, Cw7, BS, C4AQO, C4B1, BfS, OR3, Bw65(14), C4A2, C4B1/2, BfS, and Bw57(17), C4A6, C4B1, BfS. All three are proposed to carry a gene for IgA deficiency, while other supratypes carrying the same B allele generally do not. Other supratypes possibly associated with IgA deficiency were also identified. A survey of about 150 individuals with at least 1 of the 3 main supratypes revealed only 2 IgA- deficient subjects, and these were among the 20 that had 2 of these supratypes. This suggests the possibility of a recessive mode of inheritance, with penetrance determined by another factor which is not major histocompatibility complex- linked. All the supratypes found in this group of IgA-deficient subjects would then carry the putative recessive allele for IgA deficiency. Introduction Selective immunoglobulin A (IgA) deficiency is the most common of the immuno- globulin deficiencies. Several surveys have estimated the prevalence of IgA deficiency in blood donors and community populations between 1/400 and 1/700 (Koistinen 1975, Johansson et al. 1968, Bachmann 1965, Oen et al. 1982, Leivers et al. 1978). Some studies report lower frequencies: 1/1000 (Cassidy et al. 1975), 1/1200 Address correspondenceto: AssociateProfessorR.L. Dawkins,Departmentof ClinicalImmunology, The Queen ElizabethII MedicalCentre,Nextlands, WesternAustralia6009.
-
Upload
universityofwesternaustralia -
Category
Documents
-
view
1 -
download
0
Transcript of Family studies of IgA deficiency

Immunoflenetics 21 : 333-342, 1985 Im nlUllO= genetics
© Springer-Verlag 1985
Family Studies of IgA Deficiency
Alan N. Wilton, Trevor J. Cobain, and Roger L. Dawkins
Departments of Clinical Immunology, Royal Perth Hospital and The Queen Elizabeth II Medical Centre, Perth, Western Australia
Abstract. Seventeen immunoglobulin A (IgA)-deficient subjects and other members from 13 families were examined at HLA-A, B and DR, C4A, C4B, and Bf loci. Of the 29 independent haplotypes in the IgA-deficient subjects, 22 included deletions, duplications, or defects at the C4 or 21-hydroxylase loci. It is suggested that there may be a gene regulating serum IgA concentrations in this same region of chromosome 6. Three main supratypes explain most of the previously reported HLA associations with IgA deficiency. These are A1, Cw7, BS, C4AQO, C4B1, BfS, OR3, Bw65(14), C4A2, C4B1/2, BfS, and Bw57(17), C4A6, C4B1, BfS. All three are proposed to carry a gene for IgA deficiency, while other supratypes carrying the same B allele generally do not. Other supratypes possibly associated with IgA deficiency were also identified. A survey of about 150 individuals with at least 1 of the 3 main supratypes revealed only 2 IgA- deficient subjects, and these were among the 20 that had 2 of these supratypes. This suggests the possibility of a recessive mode of inheritance, with penetrance determined by another factor which is not major histocompatibility complex- linked. All the supratypes found in this group of IgA-deficient subjects would then carry the putative recessive allele for IgA deficiency.
Introduction
Selective immunoglobulin A (IgA) deficiency is the most common of the immuno- globulin deficiencies. Several surveys have estimated the prevalence of IgA deficiency in blood donors and community populations between 1/400 and 1/700 (Koistinen 1975, Johansson et al. 1968, Bachmann 1965, Oen et al. 1982, Leivers et al. 1978). Some studies report lower frequencies: 1/1000 (Cassidy et al. 1975), 1/1200
Address correspondence to: Associate Professor R.L. Dawkins, Department of Clinical Immunology, The Queen Elizabeth II Medical Centre, Nextlands, Western Australia 6009.

334 A.N. Wilton et al.
(Natvig et al. 1971), and 1/3000 (Frommel et al. 1973). All these studies combined give an estimate of 1/600 prevalence. As well as occurring as sporadic cases, IgA deficiency is recognized as occurring as a familial trait (e. g., Oenet al. 1982), which suggests that there is a genetic basis for the disease. The structural gene for the heavy chain of immunoglobulin A is on chromosome 14 (Cox et al. 1982). IgA deficiency has been associated with alpha-1 antitrypsin deficiency, which is also on chromo- some 14 (Casterline et al. 1978), and aberrations of chromosome 18 (Grundbacher 1972). However, the most common associations reported are with alleles at loci in the major histocompatibility complex (MHC) on chromosome 6, which would appear a likely place for the regulatory site proposed by Natvig and co-workers (1971).
Increased frequencies of HLA-A1, A2, A19, A28, B5, B8, B13, BI 4, B17, B40 and DR3 have been reported in IgA-deficient subjects (HammarstrSm et al. 1984, Heikkila et al. 1984). A19, B17, and B40 were only increased in subjects suffering from upper respiratory tract infections. B13 was increased in subjects with very low but not completely absent IgA. A2 was increased in IgA-deficient epileptics on a particular drug regime. Combinations of these alleles have also been shown to be increased, e. g., A1, B8 (Heikkila et al. 1984, Ambrus et al. 1977) and B8, DR3, which also usually occurs with A1 (HammarstrSm and Smith 1983). IgA deficiency is also associated with autoimmune diseases such as systemic lupus erythematosus (SLE) and juvenile-onset diabetes mellitus (CMand and Bell 1978, Smith et al. 1978). These autoimmune diseases are also associated with the supratype A1, Cw7, B8, C4AQO, C4B1, BfS, DR3, DQ2 (Dawkins et al. 1983), suggesting that this is also the supratype associated with IgA deficiency. A second important supratype is predicted on the basis of increased frequencies of A28, and B14 and A28, B14 together (Cobain et al. 1983). The B14, C4A2, C4B1/2, BIT supratype, which carries a C4B duplication, is associated with 21-hydroxylase (21-OH) deficiency but the other common B14- containing supratypes B14, C4A3, C4B1, BfS, DR6 and B14, C4A3, B1, BfS, DR7 have not been associated with any diseases. The frequent occurrence of such combinations of rare alleles shows that such supratypes are highly conserved. Once the supratypes associated with the deficiency are identified, the presence of the disease gene may be predicted by the supratype, as is the case for 21-OH deficiency and its associated supratypes (Cobain et al. 1984, McCluskey et al. 1983).
Many reports give conflicting views as to the mode of inheritance of IgA deficiency. These range from autosomal recessive, and autosomal dominant with low penetrance, to multifactorial and polygenic (Oen et al. 1982). It is possible that the issue is confused by the existence of different supratypes carrying different alleles or genes for IgA deficiency, each with a different mode of expression, and also by the existence of transient forms of IgA deficiency (Cobain et al. 1981). We have attempted to define the supratypes that carry the gene for IgA deficiency from families with IgA-deficient members. We then examine the IgA concentrations in other unrelated subjects with these supratypes, which we predict also carry the disease gene, to determine the mode of expression of the gene.

Family Studies of IgA Deficiency 335
Materials and Methods
Subjects. Two groups of subjects were studied. Families with IgA-deficient members were "studied to identify the supratypes associated with IgA deficiency. Other individuals or families with supratypes of interest were studied to test models for the mode of inheritance and penetrance of the gene for IgA deficiency that is associated with these supratypes. From a survey of IgA concentrations in Western Australian blood donors and clinic patients being investigated for immunological disorders, a pool of over 80 IgA-deficient subjects who were not deficient for other immunoglobulins was found (Cobain et al. 1983). Families of 11 subjects from this pool were HLA-A, B, C, DR and C4 and Bftyped. Families of deficient subjects with A28 and/or B14 were particularly encouraged to participate to ensure that the B14 supratypes associated with IgA deficiency could be defined. Other families were chosen on the basis of availability. Families of two clinic patients with IgA concentrations consistently lower than normal were also examined. Some of the data on these families have been published in a preliminary report (Cobain et al. 1984). (a) Having defined some of the supratypes associated with IgA deficiency from these families, we searched other families on whom genotyping of all members had been completed for other reasons (e. g., bone marrow transplants, rheumatoid arthritis, insulin-dependent diabetes mellitus, kidney transplants) for the major supratypes of interest (see text). Families with more than one of the supratypes in family members were preferentially selected. Frozen serum samples were tested for IgA concentrations in 107 subjects from 25 families. Half the subjects carried one of the major IgA-associated snpratypes. (b) Twenty-nine diabetics with B8, C4AQO, C4B1, BfS, DR3 were tested. (c) One hundred and nine subjects from the Busselton study population who had IgA, HLA, and complement results were examined. (d) Four other subjects who were C4BQO homozygous were tested for IgA concentrations to test if C4B null homozygosity itself was associated with IgA deficiency.
IgA concentrations. Serum IgA concentrations were measured by rate nephelometry on a Beckman Automated Immunochemistry System. The 95700 reference range has been determined to be 0.65-3.4 g/1 in a local population. Subjects who had concentrations of less than 0.3 g/l, which is the lower limit of accurate measurement using this method, have been classed as IgA deficient. Many of these subjects had previously been shown to have less than 0.008 g/1 by radial immunodiffusion (Cobain et al. 1983). Subjects with serum IgA concentrations between 0.3 g/l and 0.65 g/1 have been classed as having low IgA concentrations.
HLA typing. HLA typing was performed using sera well characterized against cells typed in previous international workshops. HLA A, B, C typing was performed using the standard microlymphocytotox- icity method. DR typing was performed by a microcytotoxicity method using a nylon-wool-separated B-cell-enriched population (Danilovs et al. 1980), with additional T-cell depletion by rosette sedimentation.
Complement typing. The complement genes C4A and C4B were typed using a variation of the method of Awdeh and Alper (1980), i.e., immunofixation after electrophoresis of fresh plasma as described by McCluskey and co-workers (1983). Hemolytic overlays were used to distinguish between C4A and C4B alleles and densitometric ratios of C4A:C4B bands to detect C4 null alleles. Bftyping was performed by electrophoresis with immunofixation with antiserum to factor B (Alper et al. 1972).
Nomenclature. Supratypes are often referred to in this paper by giving the alleles at the HLA-B, C4A, C4B, and Bfloci in that order, e. g., 8,0,1,S represents HLA-B8, C4AQO, C4BI, BfS. Other unmentioned alleles may also be part of the supratype, e. g., 8.0, 1, S is invariably DR3 and usually AI. Duplications at the C4 loci are indicated by a slash between the alleles, e. g., 1/2 represents the C4B1/C4B2 duplication.
Results
Genotypes and supratypes in IgA deficiency. T h e g e n o t y p e s o f t h e 17 s u b j e c t s w i t h
I g A de f i c i ency f r o m 13 fami l ies a re g i v e n in T a b l e 1. S u b j e c t s T R E a n d C L E were
a d d e d t o t h e o r i g i n a l 11 fami l ies f r o m s u b j e c t g r o u p s a a n d b, r espec t ive ly . T h e

336 A.N. Wilton et al.
Table 1. Haplotypes in IgA-deficient subjects from 13 families show supratypes 8, 0, I, S; 17, 6, 1, S, and 14, 2, 1/2, S occur repeatedly
First haplotype Second haplotype
A B C 4 A C 4 B B f DR A B C4A C4B* B f DR
CLE SHA JAH HEA ADL
1 8 II 8
1 8 1 8 1 8 1 8
28 40 3 I S FEN 3 35 3/2 (0) F MIT 1 1 37 3 I F
2 29 44 0 I S LAW 2 44 3 1 S MCK 1 1-17 6 1 S TRE 32 117 6 1 S COO 1 1 117 6 1 S
2 26 44 3 1 F HOD 26 44 31 i S DAW 2 14 3 1 F
0 1 S 01 1 S 0 1 S 0 1 S 0 I S 0 1 S
3 1 1 8 0 - 28 14 31 3 28 44 3 3 (31) 40 3 3 28 40 3 3 3 114 2 4 3 114 2 1 (19) 1 14 2 (1) 33 114 2 3 33 114 2 5 28 114 2 7 28 114 2 7 1 1 8 0 (6) 2 60 0 7 2 60 0 (4) 11 51 01 6 (2) 51 0
1 S ] 3 1/2 S - 0 F 4 1 S 4 1 S 4 i /2 s 3 i /2 s 3 1/2 s i 1/2 S 1 1/2 s 1 1/2 S 5 1_/2 s 5 I S 3
2 S 6 2 S 6 I S (6) 1 S 5
Parentheses indicate the assignment needs to be confirmed. Other less likely possibilities may exist. * C4B1/2 duplication could not always be proven; some may be C4B2. I Assignment of the allele to this haplotype needs to be confirmed.
frequency of the various MHC alleles must reflect in part the method of ascertainment, but it is clear that there are many similarities between the 34 haplotypes identified in the 13 unrelated families.
At least five unrelated B14-containing haplotypes contain the entire B14, C4A2, C4B1/2, BfS supratype (denoted as 14, 2, 1/2, S). Synacthen stimulation tests on members of two families (FEN and LAW) show that the carriers of this supratype are heterozygous for 21-OH deficiency, which suggests that this supratype always has an allele for 21-OH deficiency (Cobain et al. 1984). Two of the six subjects with A28 have the A28, B14, C4A2, CB1/2, BfS, DR5 supratype and a third has A28, B14, C4B1/2 at least, with Uncertain alleles at C4A and DR. Excluding subjects TRE and CLE, there was no selection based on the presence of B8, but it is apparent that B8 is contained within the B8, C4AQO, C4R1, BfS, DR3 supratype (8, 0, 1, S).
In addition to the two supratypes defined above, there are further recurring combinations among the haplotypes shown in Table 1. For example, the B17, C4A6, C4B1, BfS supratype is present in three unrelated subjects usually with A1 and/or DR7. 44, 3, 1, S; 51, O, 1, S and 40, 3, 1, S also occur more than once in unrelated subjects. The alleles from another supratype, A2 and 60, O, 2, occur in a subject, WIL (not shown), who also has A32 and 7, 6, 1, but no family data are available. From Table 1 it is also apparent that 10 of the 17 cases with IgA deficiency have 2 rather than 1 of the 7 supratypes identified.

Family Studies of IgA Deficiency 337
Associated alleles in supratypes. In this group of IgA-deficient subjects, B8 is part of the 8, 0, 1, S supratype on each of 8 times that it occurs, and all three of the B17s occur as 17, 6, 1, S (Table 1). Nine of the ten Als occur with either 8, 0, 1, S or 17, 6, I, S and nine of the ten DR3s occur with 8, 0, 1, S or 14, 2, 1/2, S. B14 occurs 7 of 9 times as part of the 14, 2, 1/2, S. supratype. A28 occurs with several supratypes, but most commonly with 14, 2, 1/2, S.
IgA deficiency segregates with haplotypes. Family ADL (Table 2) contains at least three of the supratypes associated with IgA deficiency: (a) 8, 0,1, S, (b) 40, 3, 1, S, and (c) 14, 2, 1/2, S. In this family all three members who have two of these supratypes have IgA deficiency. The fourth haplotype appears identical with the 35, 2/3, O, F supratype in the IgA-deficient member of the FEN family (Table 1) and similar to haplotype b in the H O D family (Table 2), though in all cases it is difficult to demonstrate the C4BQO. This supratype may also carry an allele for IgA deficiency.
Family MIT (Table 2) has two IgA-deficient members, both of whom have the 14, 2,1/2, S supratypes. The other haplotype of one of the affected members includes C4AQO, C4B1, BfS, and DR3. This haplotype, c, may be a result of recombination with an 8, 0, 1, S, 3 haplotype. The B14 in this family and in family FEN is Bw65, which is equivalent to B14.2.
In family C O 0 (Table 2) the 17, 6, 1, S supratype appears in an IgA-deficient subject with 60, O, 2, S, which occurs in a second IgA-deficient subject and with the supratype 44, 3, 1, F that appears only once in the sample. The latter has a haplo- identical sibling who is not IgA deficient. Haplotype f in this family is most likely the 1, 8, 0, 1, S, 3 supratype. It occurs with 17, 6, I, S in subject H4 whose IgA concentration is 0.6 g/l, which is low but not deficient.
In family DAW (Table 2) the affected individual carries 14, 3,1, F and 51~ O, 1, S. Where 8, 0,1, S occurs with the first of these supratypes in this family, IgA deficiency is not evident. Densitometry suggests that the fourth supratype in this family (15, 3, 1, F) carries a duplication of C4A3, but this supratype is not associated with IgA deficiency.
In each of these families, every member who is IgA deficient or has low serum IgA concentrations has at least one of the three supratypes 14, 2, I/2, S, 17, 6, 1, S, and 8, 0, 1, S. Not every family member who has one of these supratypes has serum IgA concentrations that are lower than normal (Table 2).
Low IgA in families. The 8, 0, 1, S or 17, 6, 1, S supratypes also occurred in low IgA ( < 0.6 g/l) members of two other families studied (families M CD and ]FIN of Cobain et al. 1984). Low IgA concentration also has been demonstrated in the COO family with 17, 6, I, S and At , B8. 14, 2, 1/2, S and 8, 0,1, S occur in member II 3 of the FEN family who also has low IgA.
Relevance of complement alleles. Each of the above supratypes which are commonly associated with IgA deficiency contains unusual alleles at a C4 locus. The 14, 2, 1/2, S supratype contains the C4B duplication and the 8, 0, 1, S supratype contains a C4A null allele that is caused by a deletion (Carroll et al. 1984a). The third supratype, 17, 6,1, S, which is highlighted in Table 1, contains the C4A6 allele, which

~o
o~
r~o
~P
~
-~
0~
0~
~
-~
--,~ O
~
o
, B
~
-~
-.
o ~
~_
~.~
o
~
• ~'
~ ~
O~
~
o~
,~:
~."
~-]
~ o
~.~
.~,
p~
~'.
~1
~
, o
~
~ ~
~ ,~
.~
~,~
,~
~ d
._,~
~
~ d
.,
~
~-
~
~'
~,
~~
,~
~
'~
/ I
I L
I I
I ]
I ]
I I I I
I I
~
I I
I
~s~
I
~0
o8
o i o
.>
Z

Family Studies of IgA Deficiency 339
gives unique restriction fragment patterns (Palsdottir et al. 1983), indicating a difference at the DNA level.
C4A null alleles also occur on three supratypes other than 8, 0, 1, S (Table 1). Five subjects with IgA deficiency from four families have one of these supratypes. The C4A3/2 duplication with C4B null appears in one IgA-deficient subject, FEN, who also has 14, 2, 1/2, S. Another C4B null allele appears in the IgA-deficient subject JAH, who also has 8, 0, 1, S.
Other supratypes. The supratypes mentioned above account for all but three of the supratypes in the IgA-deficient subjects in Table 1. These three supratypes contain the complotype 3, I, F; two also have DR6.
IgA concentrations in subjects with 8, O, I, S; 17, 6, 1, S, and~or 14, 2, 1/2, S. None of the subjects from other families with only one of these three major supratypes was IgA deficient. In the Busselton population none of the 55 subjects 'with 1 of these supratypes was IgA deficient. Only one of the diabetics with 8, 0, 1, S was IgA deficient, and she was CLE, who is A1, 8, O, 1, S, DR3 homozygous. CLE was the only IgA-deficient subject among the 14 8, 0, 1, S homozygotes examined overall, and TRE was the only IgA-deficient among the six 17, 6,1, S/8, O, 1, S heterozygotes examined (including an HLA-identical sibling). Ten other C4AQO homozygotes and a total of 12 C4BQO homozygotes were tested; none was IgA deficient.
Discussion
HLA associations. The associations between IgA deficiency and A1, A28, B8, B14, B17 and DR3 which have been shown in previous studies (e. g., Cobain et al. 1983, Oen et al. 1982) are explicable in terms of only three supratypes: Al, B8, C4AQO. C4B1, BfS, DR3, A28, B14, C4A2, C4B1/2, BJS and AI, B17, C4A6, C4BI, BfS (Table 1). It is possible that there are other A28-containing supratypes associated with IgA deficiency. Associations with alleles such as AI and A28, which occur on several supratypes, are more likely to be detected than alleles that only occur on one, e. g., B14, B8, and B17. Accordingly, we suspect that some associations reported in earlier studies reflect the presence of a few supratypes which coincidentally have an allele in common, and that differences between earlier reports reflect the relative frequencies of the supratypes in the populations studied. A good example of this is the B40 association. In our sample, B40 occurs on two different supratypes: 40, 3, 1, S with DR4 and 60, O, 2, S.
Modes of inheritance. HLA-associated IgA deficiency has been presented as a dominant gene elsewhere (HammarstriSm and Smith 1983) because of the high frequency of a single supratype in the affected subjects. For a dominant gene, the penetrance would have to be very low to account for the high proportion of unaffected subjects with the IgA-associated supratypes, which are expected to have the IgA deficiency allele. (8, 0, 1, S is at a frequency of about 10% in Caucasian populations of Northern European descent.) In a sample of about 130 subjects with only one of the three major supratypes, none was IgA deficient. IgA deficiency was

340 A.N. Wilton et al.
found only in subjects with two of these supratypes. We have identified several supratypes associated with IgA deficiency and find that most affected subjects have two rather than one of these supratypes. These facts lead us to suggest that a preferable model is one with a recessive mode of inheritance for the MHC- associated gene, where the recessive allele is reasonably frequent (about 15~o) and present on many supratypes. Some of these supratypes will be rare and will not occur repeatedly in studies such as this with small sample sizes.
Penetrance is obviously not 100°(, since HLA-identical siblings are not always concordant (Table 2). Two subjects from the population survey were IgA deficient out of 20 subjects who were known to have two of three major supratypes, which suggests that penetrance is about 10~. The families presented here are consistent with the hypothesis that there is a second genetic factor, not linked to the MHC, which is required to produce IgA deficiency. On the data available we cannot distinguish whether the second gene is dominant or a common recessive. Even in the ADL family, where all members are likely to be homozygous for the HLA-linked IgA deficiency gene, either model would fit for the second locus. An environmental factor is also a possibility for the second factor. The families with members who have two of the three major supratypes and have low IgA concentrations suggest that the other factors may modify the extent of reduction of IgA concentration. Using the above estimates of frequency (15}/o) and penetrance (10~o), a prevalence of 1/440 would be expected for a. recessive trait. This rough estimate falls within the range generally reported in the literature: 1/400-1/700 (see Introduction).
Correlating supratypes to literature reports. Cleland and Bell (1978) report the HLA- A and B typing on a large family with IgA deficiency. Correlating the B typing in this family with the known IgA-associated supratypes gives the most likely supratypes in each individual, e. g., B8 is likely to be 8, 0, I, S, and B35 is likely to be 35, 3/2, O, F. Most of the B antigens in the IgA-deficient subjects, with the notable exception of B21, could be attributed to one of the supratypes in Table 1. This is also true of our own 50 IgA deficient subjects with only A and B typing, and another 66 from the literature (Buckley et al. 1977, Smith et al. 1978, HammarstrSm and Smith 1983, Oen et al. 1982). Two other IgA deficiency associated supratypes are also suggested by this data: a B13-containing supratype (B13 occurs in 7 of the 130), and a BT- containing supratype-possibly 7, 4, 2, S.
Recurring allelic combinations in the B to Bf region. The A and DR alleles associated with the 14; 2, 1/2, S supratype are somewhat variable. This suggests that the IgA deficiency gene is located close to the B, C4, and Bfgenes. The 8, 0, 1, S supratype is more common than the complete A1, B8, C4AQO, C4B1, BfS, DR3 supratype, again suggesting that the gene regulating serum IgA concentrations is close to C4. The complement types 0,1, S and 6,1, S also occur without their commonly associated B antigens.
Significance of C4B duplication and C4 null alleles. IgA deficiency and 21-OH deficiency are both associated with the Bw65(14), C4A2, C4B1/B2, BfS supratype (Cobain et al. 1984). Molecular cloning techniques have shown that the 21-0H genes are located very close to the C4 genes (Carroll et al. 1984b; see Fig. 1). Two 21-
Family Studies of IgA Deficiency 341
l ~ i l l CI I iu I
j t,,
5 " r- "l
~x t~ A A z~
O i I I I
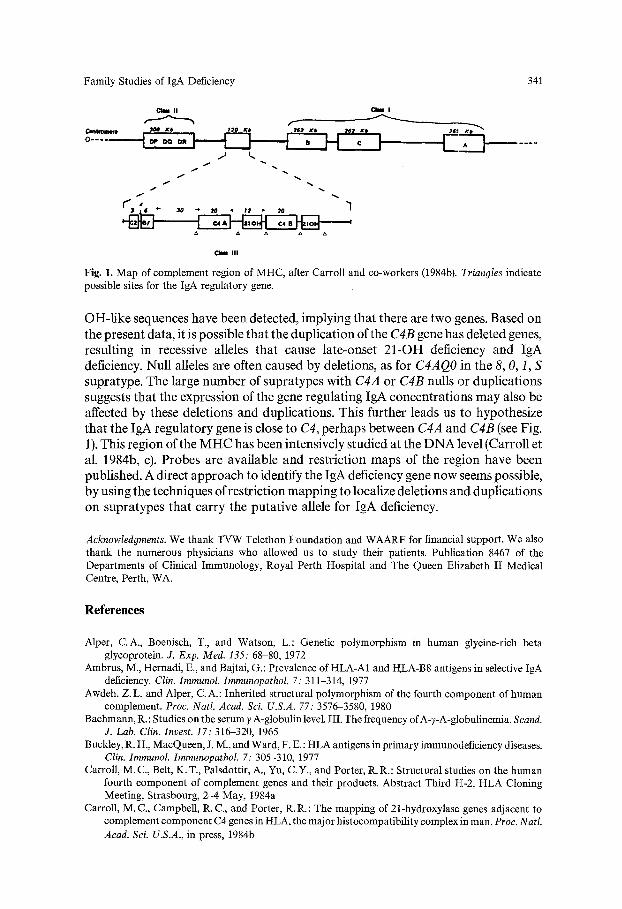
Fig. 1. Map of complement region of MHC, after Carroll and co-workers (1984b). Triangles indicate possible sites for the IgA regulatory gene.
OH-like sequences have been detected, implying that there are two genes. Based on the present data, it is possible that the duplication of the C4B gene has deleted genes, resulting in recessive alleles that cause late-onset 21-OH deficiency and IgA deficiency. Null alleles are often caused by deletions, as for C4AQO in the 8, 0, 1, S supratype. The large number of supratypes with C4A or C4B nulls or duplications suggests that the expression of the gene regulating IgA concentrations may also be affected by these deletions and duplications. This further leads us to hypothesize that the IgA regulatory gene is close to C4, perhaps between C4A and C4B (see Fig. 1). This region of the MHC has been intensively studied at the DNA level (Carroll et al. 1984b, c). Probes are available and restriction maps of the region have been published. A direct approach to identify the IgA deficiency gene now seems possible, by using the techniques of restriction mapping to localize deletions and duplications on supratypes that carry the putative allele for IgA deficiency.
Acknowledgments. We thank TVW Telethon Foundation and WAARF for financial support. We also thank the numerous physicians who allowed us to study their patients. Publication 8467 of the Departments of Clinical Immunology, Royal Perth Hospital and The Queen Elizabeth II Medical Centre, Perth, WA.
References
Alper, C.A., Boenisch, T., and Watson, L.: Genetic polymorphism in human glycine-rich beta glycoprotein. J. Exp. Med. 135: 68-80, 1972
Ambrus, M., Hernadi, E., and Bajtai, G.: Prevalence of HLA-A1 and RLA-B8 antigens in selective IgA deficiency. Clin. Immunol. Immunopathol. 7: 311-314, 1977
Awdeh, Z.L. and Alper, C.A.: Inherited structural polymorphism of the fourth component of human complement. Proc. Natl. Acad. Sci. U.S.A. 77: 3576-3580, 1980
Bachmann, R.: Studies on the serum 7 A-globulin level. III. The frequency of A-7-A-globulinemia. Scand. J. Lab. Clin. Invest. 17: 316-320, 1965
Buckley, R. H., MacQueen, J. M., and Ward, F. E.: HLA antigens in primary immunodeficiency diseases. Clin. Imrnunol. Immunopathol. 7: 305-310, 1977
Carroll, M.C., Belt, K.T., Palsdottir, A., Yu, C.Y., and Porter, R. R.: Structural studies on the human fourth component of complement genes and their products. Abstract Third H-2, HLA Cloning Meeting, Strasbourg, 2-4 May, 1984a
Carroll, M.C., Campbell, R. C., and Porter, R.R.: The mapping of 21-hydroxylase genes adjacent to complement component C4 genes in HLA, the major histocompatibility complex in man. Proc. Natl. Acad. Sci. U.S.A., in press, 1984b

342 A.N. Wilton et al.
Carroll, M.C., Campbell, R. C., Bentley, D. R., and Porter, R. R.: Class III region linking complement genes C4, C2 and factor B. Nature 307: 237-240, 1984c
Cassidy, J.T. and Nordby, G.L.: Human serum immunoglobulin concentrations; prevalence of immunoglobulin deficiencies. J. Allergy Clin. Immunol. 55: 35-48, 1975
Casterline, C.L., Evans, R., Battista, V.C., and Talamo, R.C.: Selective IgA deficiency and Pi ZZ- antitrypsin deficiency. Chest 73: 885-886, 1978
Cleland, L.G. and Bell, D.A.: The occurrence of systemic lupus erythematosus in two kindreds in association with selective IgA deficiency. J. Rheumatol. 5: 288-293, 1978
Cobain, T. J., Stuckey, M., French, M. A. H., and Dawkins, R. L.: Implications of transient and persistent IgA deficiency. Br. Soc. Immunol., summer meeting, 1981
Cobain, T.J., French, M. A. H., Christiansen, F.T., and Dawkins, R. L.: Association of IgA deficiency with HLA A28 and B14. Tissue Antigens 22: 151-154, 1983
Cobain, T. J., Stnckey, M. S., McCluskey, J., Wilton, A., Gedeon, A., Garlepp, M. J., Christiansen, F. T., Wilson, R. G., and Dawkins, R. L.: The co-existence of IgA deficiency and 21-hydroxylase deficiency marked by specific supratypes. Ann, N.Y Acad. Sci., in press, 1984
Cox, D.W., Markovic, V.D., and Teshima, I.E.: Genes for immunoglobulin heavy chains and for el- antitrypsin are localized to specific regions of chromosome 14q. Nature 297: 428-430, 1982
Danilovs, J. A., Ayoub, G. A., and Terasaki, P. I.: B-lymphocyte isolation by thrombin-nylon wool. In P. I. Terasaki (ed.): HistocompatibiIity Testing 1980, pp. 287-288, UCLA Tissue Typing Laboratory, Los Angeles, 1980
Dawkins, R. L. Christiansen, F. T., Kay, P. H., Garlepp, M. J., McCluskey, J., Hollingsworth, P. N., and Zilko, P. J. : Disease associations with complotypes, supratypes and haplotypes. Immm~ol. Rev. 70: 5- 22, 1983
Frommel, D., Moullec, J., Lambin, P., and Fine, J. M.: Selective serum IgA deficiency. Frequency among 15 200 French blood donors. Vox Sang. 25: 513-518, 1973
Grundbacher, F. J.: Genetic aspects of selective immunoglobulin A deficiency. J. Med. Genet. 9: 344.347, 1972
HammarstrSm, L. and Smith, C. I. E.: HLA A, B, C and DR antigens in immunoglobulin A deficiency. Tissue Antigens 21: 75-79, 1983
Hammarstr6m, L., Axelsson, U., Bjorkander, J., Hanson, L. A, Moller, A., and Smith. C. I. E.: HLA antigens in selective IgA deficiency: Distribution in healthy donors and patients with recurrent respiratory tract infections. Tissue Antigens 24: 35-39, 1984
Heikkila, M., Koistinen, J., Lohman, M., and Koskimies, S.: Increased frequency of HLA-A1 and -B8 in association with total lack, but not with deficiency of serum IgA. Tissue Antigens 23: 280-283, 1984
Johansson, S. G. O., Hogman, C.F., and Killander, J.: Quantitative immunoglobulin determination. Comparison of two methods. Estimation of normal levels and levels in personS lacking IgA and IgD. Acta Pathol. Microbiol. Scand. 74: 519-530, 1968
Koistinen, J.: Selective IgA deficiency in blood donors. Vox Sang. 29: 192-202, 1975 Leivers, S., Christiansen, F.T., French, M., and Davey, M. G.: Western Australian blood donors who
lack immunoglobulin A. Proc. Aust. Soc. Med. Res. 11: 47, 1978 McCluskey, J., Kay, P.H., Dawkins, R.L., Komori, K., Christiansen, F.T., and McCann, V.J.:
Association of specific MHC supratypes with rheumatoid arthritis and insulin dependent diabetes meUitus. Dis. Markers I: 197-212, 1983
Natvig, J. B., Harboe, M., Fausa, O., and Tviet, A.: Family studies individuals with selective absence of yA-globulin. Clin. Exp. Immunol. 8: 229-236, 1971
Oen, K., Petty, R.E., and Schroeder, M.C.: Immunoglobulin A deficiency; genetic studies. Tissue Antigens 19: 174-182, 1982
Palsdottir, A., Cross, S.J., Edwards, J.H., and Carroll, M.C.: Correlation between DNA restriction fragment length polymorphism and C4A6 protein. Nature 306: 615-616, 1983
Smith, W.I., Rabin, B.S., Huellmantel, A., Van Theil, D.H., and Drash, A.: Immunopathology of juvenile-onset diabetes mellitus. I. IgA deficiency and juvenile diabetes. Diabetes 27: 1092-1097, 1978
Received December 4, 1984; revised version received February 4, 1985