
Protein kinase inhibitors in the treatment of inflammatory and autoimmune diseases
10
Protein kinase inhibitors in the treatment of inflammatory and autoimmune diseases H. Patterson, R. Nibbs, I. McInnes and S. Siebert Institute of Infection, Immunity and Inflammation, College of Medicine, Veterinary and Life Sciences, University of Glasgow, Glasgow, UK Summary Protein kinases mediate protein phosphorylation, which is a fundamental component of cell signalling, with crucial roles in most signal transduction cascades: from controlling cell growth and proliferation to the initiation and regulation of immunological responses. Aberrant kinase activity is impli- cated in an increasing number of diseases, with more than 400 human dis- eases now linked either directly or indirectly to protein kinases. Protein kinases are therefore regarded as highly important drug targets, and are the subject of intensive research activity. The success of small molecule kinase inhibitors in the treatment of cancer, coupled with a greater understanding of inflammatory signalling cascades, has led to kinase inhibitors taking centre stage in the pursuit for new anti-inflammatory agents for the treat- ment of immune-mediated diseases. Herein we discuss the main classes of kinase inhibitors; namely Janus kinase (JAK), mitogen-activated protein kinase (MAPK) and spleen tyrosine kinase (Syk) inhibitors. We provide a mechanistic insight into how these inhibitors interfere with kinase signalling pathways and discuss the clinical successes and failures in the implementa- tion of kinase-directed therapeutics in the context of inflammatory and autoimmune disorders. Keywords: autoimmunity, novel biological therapies, protein kinases, signalling/signal transduction Accepted for publication 2 December 2013 Correspondence: S. Siebert, Institute of Infection, Immunity and Inflammation, College of Medicine, Veterinary and Life Sciences, University of Glasgow, 120 University Place, Sir Graeme Davies Building, Glasgow G12 8TA, UK. E-mail: [email protected] Introduction Inflammatory responses are generally initiated by the recog- nition of signals that convey evidence of pathogen invasion or tissue injury. This, in turn, initiates the activation of intracellular signalling cascades and subsequently results in increased expression of proinflammatory cytokine genes. When these inflammatory responses occur in the absence of overt infection, or when the responses persist despite reso- lution of the initial insult, these processes can become pathological and result in chronic inflammation. A wide spectrum of human diseases is associated with chronic inflammation and includes disorders such as pso- riasis, rheumatoid arthritis (RA) and multiple sclerosis (MS). A number of well-established immune modulatory drugs have been used in the clinic for the treatment of these inflammatory and autoimmune diseases; however, these therapies have several limitations. Most current first-line therapies are either non-selective immunosuppressive or cytotoxic drugs, which are associated with limited clinical efficacy and significant side effects [1–3]. Furthermore, many patients either do not respond adequately or become unresponsive to such therapies. There is therefore a large unmet need in the treatment of these patients, prompting the search for new drug targets for the treatment of these inflammatory-mediated diseases. As our understanding of the underlying inflammatory processes has advanced, increasingly sophisticated targeting of such pathways for therapeutic purposes has become a reality. An ideal therapeutic target would be a signalling molecule that plays an important role in the initiation of inflammatory responses but, in the context of other crucial cell mechanism-based events, is dispensable [4]. Much of the initial targeted therapeutic focus was on extracellular targets, with significant successes, including anti-tumour necrosis factor (TNF) and B cell-depleting therapies for RA and other inflammatory conditions. While undoubtedly sig- nificantly improving the treatment of these conditions, the current biological agents are not effective for all patients. Furthermore, even in those who respond, the majority have only a partial response with only a small minority achieving clinical remission. There therefore remains a significant Clinical and Experimental Immunology REVIEW ARTICLE doi:10.1111/cei.12248 1 © 2013 British Society for Immunology, Clinical and Experimental Immunology, 176: 1–10
Transcript of Protein kinase inhibitors in the treatment of inflammatory and autoimmune diseases

Protein kinase inhibitors in the treatment of inflammatory andautoimmune diseases
H. Patterson, R. Nibbs, I. McInnes andS. SiebertInstitute of Infection, Immunity and
Inflammation, College of Medicine, Veterinary
and Life Sciences, University of Glasgow,
Glasgow, UK
Summary
Protein kinases mediate protein phosphorylation, which is a fundamentalcomponent of cell signalling, with crucial roles in most signal transductioncascades: from controlling cell growth and proliferation to the initiation andregulation of immunological responses. Aberrant kinase activity is impli-cated in an increasing number of diseases, with more than 400 human dis-eases now linked either directly or indirectly to protein kinases. Proteinkinases are therefore regarded as highly important drug targets, and are thesubject of intensive research activity. The success of small molecule kinaseinhibitors in the treatment of cancer, coupled with a greater understandingof inflammatory signalling cascades, has led to kinase inhibitors takingcentre stage in the pursuit for new anti-inflammatory agents for the treat-ment of immune-mediated diseases. Herein we discuss the main classes ofkinase inhibitors; namely Janus kinase (JAK), mitogen-activated proteinkinase (MAPK) and spleen tyrosine kinase (Syk) inhibitors. We provide amechanistic insight into how these inhibitors interfere with kinase signallingpathways and discuss the clinical successes and failures in the implementa-tion of kinase-directed therapeutics in the context of inflammatory andautoimmune disorders.
Keywords: autoimmunity, novel biological therapies, protein kinases,
signalling/signal transduction
Accepted for publication 2 December 2013
Correspondence: S. Siebert, Institute of
Infection, Immunity and Inflammation, College
of Medicine, Veterinary and Life Sciences,
University of Glasgow, 120 University Place, Sir
Graeme Davies Building, Glasgow G12 8TA,
UK.
E-mail: [email protected]
Introduction
Inflammatory responses are generally initiated by the recog-nition of signals that convey evidence of pathogen invasionor tissue injury. This, in turn, initiates the activation ofintracellular signalling cascades and subsequently results inincreased expression of proinflammatory cytokine genes.When these inflammatory responses occur in the absence ofovert infection, or when the responses persist despite reso-lution of the initial insult, these processes can becomepathological and result in chronic inflammation.
A wide spectrum of human diseases is associated withchronic inflammation and includes disorders such as pso-riasis, rheumatoid arthritis (RA) and multiple sclerosis(MS). A number of well-established immune modulatorydrugs have been used in the clinic for the treatment of theseinflammatory and autoimmune diseases; however, thesetherapies have several limitations. Most current first-linetherapies are either non-selective immunosuppressive orcytotoxic drugs, which are associated with limited clinicalefficacy and significant side effects [1–3]. Furthermore,
many patients either do not respond adequately or becomeunresponsive to such therapies. There is therefore a largeunmet need in the treatment of these patients, promptingthe search for new drug targets for the treatment of theseinflammatory-mediated diseases.
As our understanding of the underlying inflammatoryprocesses has advanced, increasingly sophisticated targetingof such pathways for therapeutic purposes has become areality. An ideal therapeutic target would be a signallingmolecule that plays an important role in the initiation ofinflammatory responses but, in the context of other crucialcell mechanism-based events, is dispensable [4]. Much ofthe initial targeted therapeutic focus was on extracellulartargets, with significant successes, including anti-tumournecrosis factor (TNF) and B cell-depleting therapies for RAand other inflammatory conditions. While undoubtedly sig-nificantly improving the treatment of these conditions, thecurrent biological agents are not effective for all patients.Furthermore, even in those who respond, the majority haveonly a partial response with only a small minority achievingclinical remission. There therefore remains a significant
bs_bs_banner
Clinical and Experimental Immunology REVIEW ARTICLE doi:10.1111/cei.12248
1© 2013 British Society for Immunology, Clinical and Experimental Immunology, 176: 1–10

unmet need in the treatment of chronic inflammatoryconditions.
The drug development focus for inflammatory condi-tions has recently shifted more towards targeting intracellu-lar signalling pathways. Protein phosphorylation, conductedby protein kinases, represents a major type of post-translational modification and is a fundamental mechanismof cell signalling [5–8]. Protein kinases are therefore animportant class of intracellular enzymes that play a crucialrole in most signal transduction cascades, from controllingcell growth and proliferation to the initiation and regula-tion of immunological responses [5,9–12]. Protein kinases,also referred to as phosphotransferases, phosphorylate theirtarget proteins in cells by attaching phosphates covalently tothe side chains of serine, threonine or tyrosine residues(Fig. 1). More recently, the potential importance ofphosphorylation of histidine has also been recognized [13].A total of 518 kinase genes encoding kinase proteins havebeen identified in the human genome, referred to collec-tively as the kinome [14].
Despite being first described almost 60 years ago byBurnett and Kennedy [15], the general significance ofprotein phosphorylation was only appreciated fully in theearly 1980s (for a review, see [16]). Since then, the elucida-tion of protein kinase signalling cascades has been exponen-
tial [5], and includes the seminal studies by E. H. Fischerand E. G. Krebs, who were awarded the Nobel Prize in1992 for their discoveries concerning reversible proteinphosphorylation as a biological regulatory mechanism [17–19]. Kinases have subsequently been shown to play animperative role in the first steps of intracellular immune cellsignalling. For example, kinases are associated physicallywith the intracellular component of receptors on the cellsurface of T and B lymphocytes, and initiate intracellularsignalling cascades within these cells once such receptorshave engaged with their extracellular ligands [6]. Once itwas established that protein kinases were the fundamentaldrivers of inflammatory cell signalling, they were investi-gated as therapeutic targets for a variety of diseases.
Protein kinase inhibitors
More than 400 diseases have been associated either directlyor indirectly with protein kinases [20]. Thus protein kinasesare now considered to be one of the most important groupsof drug targets [10,21]. Kinases can be targeted by smallmolecular weight compounds which act to inhibit thephosphorylation of proteins, thus preventing their activa-tion [4]. These small molecule inhibitors can interferewith kinase activity by either: (i) blocking adenosinetriphosphate (ATP)-kinase binding, (ii) interfering withkinase–protein interactions or (iii) down-regulating kinasegene expression levels through the use of RNA interferencestrategies [20].
The success of kinase inhibitors in the treatment ofcancer showcased their therapeutic potential (for a review,see [22]). This success, coupled with a greater understand-ing of inflammatory signalling cascades, led to kinaseinhibitors taking centre stage in the pursuit for new anti-inflammatory agents for the treatment of immune-mediated diseases [23]. As such, a large body of researchand review literature has developed around protein kinasesand their inhibitors. In this review we describe the variousclasses of kinase targets, namely Janus kinase (JAK),mitogen-activated protein kinase (MAPK) and spleentyrosine kinase (SYK). We provide mechanistic insight intohow these inhibitors interfere with kinase signalling path-ways in the context of inflammatory and autoimmune dis-eases, as well as discussing the clinical successes and failuresin the implementation of kinase-directed therapeutics, andtheir potential in the treatment of inflammatory-mediateddiseases.
JAK family
Cytokines play essential roles in controlling all aspects ofimmune responses, including leucocyte differentiation anddevelopment, immunological tolerance and memory, andthey are also responsible for driving many immune-mediated diseases [24]. JAKs serve to transduce signals from
ATP ADP
P P P P
P
P
O
P
Protein kinase
Proteinphosphatase
Serine, threonineor tyrosine residue
Target proteinPhosphorylated
target protein
Aden-osine
Aden-osine
OH
Fig. 1. The catalytic cycle for protein phosphorylation by a protein
kinase. Protein kinases mediate the transfer of the γ-phosphate (P)
from adenosine triphosphate (ATP) to the hydroxyl group (OH) of a
serine, threonine or tyrosine residue of the targeted protein. This
phosphorylation acts as a ‘molecular switch’, which directly activates,
or inactivates, the functions of proteins. However, protein
phosphatases can oppose the kinase activities and reverse the effects of
phosphorylation, by catalysing the removal of the γ-phosphate from
the targeted protein (based on information taken from Grant [5];
Manning et al. [7]; Ubersax and Ferrell [8]).
H. Patterson et al.
2 © 2013 British Society for Immunology, Clinical and Experimental Immunology, 176: 1–10

cytokine receptors, in particular types I and II cytokinereceptors, which lack intrinsic kinase activity. Interferon(IFN) gene induction studies conducted in the early 1990sled to the discovery of the JAK–signal transducer and acti-vator of transcription (STAT) pathway, the major signallingcascade downstream from cytokine and growth factorreceptors [25,26]. This pathway consists of the JAK familyof non-receptor tyrosine kinases and the STAT family oftranscription factors [26]. A large number of cytokines(approximately 60) including IFN, colony-stimulatingfactors and interleukins (ILs) bind types I and II cytokinereceptors, which are associated constitutively with JAKs[27]. These JAKS are essential for cell signalling and uponligand binding the cytokine receptor dimerizes and triggersthe activation of the JAK–STAT signal transduction cascade[28–30].
The mammalian JAK family comprises four members:JAK1, JAK2, JAK3 and tyrosine kinase 2 (TYK2). They allshare a similar structure characterized by the presence ofseven JAK homology (JH) domains [26,31]. JAK1 and JAK3are responsible for the signal transduction of cytokinereceptors containing the IL-2 receptor common γ chain,thus mediating signalling by IL-2, IL-4, IL-7, IL-9, IL-15 andIL-21 cytokines that are essential for the development andmaturation of T lymphocytes (Table 1) [23,28,32]. Con-versely, JAK2 is associated with haematopoietic growthfactor receptors, as well as gp40-containing cytokine recep-tors [23]. JAK1, JAK2 and TYK2 are expressed ubiquitouslyin mammals, whereas JAK3 expression is limited mainly tohaematopoietically derived cells [30,33,34]. As such, JAK3 isimportant for leucocyte activation and proliferation;namely, natural killer (NK), T and B cells [35].
The importance of JAK signalling and its non-redundant,critical role in the initiation and regulation of inflammatoryimmune responses is best illustrated when JAKs are either
mutated or deleted in vivo (Table 1) [36,37]. As JAKs provedto be critical for both innate and adaptive immunity, thisfamily of protein kinases attracted significant attention as anew therapeutic target in inflammation and autoimmunedisease [33,38].
JAK inhibitors
Walker et al. reported that JAK3 expression, as well asSTAT-4, -5 and -6 expression, was increased in thesynovium of patients with RA, compared with normalsynovium [39]. This finding was confirmed in other studies,leading to selective inhibition of JAK kinases becoming atherapeutic strategy for the treatment of RA, as well as otherinflammatory-mediated diseases.
It soon became clear that inhibiting JAKs would blockmultiple aspects of cytokine signalling (Fig. 2). One of thefirst selective JAK inhibitors to be tested in humans andenter clinical trials was tofacitinib (formerly known asCP-690, 550). Tofacitinib, developed by Pfizer (New York,NY, USA), is a potent JAK1 and JAK3 antagonist, which alsoinhibits JAK2 to a lesser extent [28]. Preclinical studiesdemonstrated tofacitinib’s immunosuppressive effects invivo in animal models of transplantation and arthritis [40–43]. Thereafter, tofacitinib entered clinical trials which con-firmed its efficacy in RA [44,45]. Clinical studies have alsosuggested efficacy of tofacitinib in ulcerative colitis [46] andpsoriasis [47]. In November 2012, tofacitinib was approvedby the US Food and Drug Administration (FDA) for thetreatment of patients with active RA who have failedother disease-modifying anti-rheumatic drugs (DMARDs),thereby becoming the first oral kinase inhibitor approvedfor the treatment of this disease. However, the EuropeanMedicines Agency (EMA) did not approve tofacitinib forRA due to concerns about the overall safety profile of
Table 1. Functions of Janus kinases (JAKs) and the phenotypes of knock-out mouse models.
Kinase Cytokines requiring this JAK for signalling Knock-out mouse phenotype
JAK1 Cytokines whose receptors contain the IL-2 receptor common γ chain:
IL-2, IL-4, IL-7, IL-9, IL-15 and IL-21
Cytokines whose receptors contain the gp130 subunit (IL-6 family);
IL-6, IL-11, IL-33 LIF, OSM, CT-1, CNTF, CLC
IFNs
Embryonic lethal
JAK2 Cytokines whose receptors contain the gp130 subunit (IL-6 family);
IL-6, IL-11, IL-33 LIF, OSM, CT-1, CNTF, CLC
IL-3
IFN-γHormone-like cytokines: EPO, GH, PRL, TPO
Embryonic lethal
JAK3 Cytokines whose receptors contain the IL-2 receptor common γ chain:
IL-2, IL-4, IL-7, IL-9, IL-15 and IL-21
SCID; however viable and fertile
TYK2 IL-12
LPS
SCID; however viable and fertile.
Also susceptible to parasite infection
CLC: cardiotrophin-like cytokine; CNTF: ciliary neurotrophic factor; CT-1: cardiotrophin-1; EPO: erythropoietin; GH: growth hormone; IFN:
interferon; IL: interleukin; LIF: leukaemia inhibitory factor; LPS: bacterial lipopolysaccharide; OSM: oncostatin M; PRL: prolactin; SCID: severe com-
bined immunodeficiency; TPO: thrombopoietin.
Protein kinase inhibitors for inflammation
3© 2013 British Society for Immunology, Clinical and Experimental Immunology, 176: 1–10

tofacitinib, including unresolved concerns about the typeand risk of serious infections [48].
Despite its success in both preclinical studies and clinicaltrials, the exact mode of action of tofacitinib in the settingof autoimmune disease has yet to be ascertained fully[49,50]. Many of the cytokines that contribute to the patho-physiology of inflammatory-mediated autoimmune dis-eases signal through receptors associated with JAKs. It iswell established that autoreactive CD4+ T cells [T helper(Th) cells], namely Th1 and Th17 cells, and their cytokinescontribute to the pathophysiology of inflammation-mediated diseases such as RA and psoriasis [51–54]. Arecent study by Ghoreschi et al. demonstrated thattofacitinib suppresses the generation of pathogenic Th1 andTh17 cells by targeting JAK1 and JAK3 kinases in T cells[28]. The authors used in-vitro T cell assays and murinemodels of collagen-induced arthritis (CIA) to confirm thattofacitinib acts to interfere with multiple cytokine signallingpathways in T cells, including IL-6 and IFN-γ, to attenuatethe inflammatory response. Further studies will be requiredto validate which cytokines are blocked in patients undergo-ing tofacitinib treatment. The exact role and position oftofacitinib in the treatment pathway of inflammatory con-ditions remains unresolved, with studies under way tofurther evaluate its long-term safety in RA and its efficacy inother inflammatory immune-mediated diseases, includingpsoriasis, ankylosing spondylitis, juvenile idiopathic arthri-tis and ulcerative colitis [55].
A variety of other JAK inhibitors (Fig. 2) have sinceentered clinical trials for the treatment of RA and otherautoimmune disorders (Table 2). Ruxolitinib (INCB-018424), a JAK1 and JAK2 inhibitor already approved bythe FDA for treating patients with myelofibrosis, has shown
Cytokine
JAK1 JAK2 JAK1JAK3
GLPG-0634lestaurtinibtofacitinib
TofacitinibR-348
VX-509LY-3009104ruxolitinibtofacitinib
P P
IFN-γ IL-2
P
STAT-1 STAT-1
P
PNucleus P P P
STAT-1 STAT-1STAT-5 STAT-5
P P
STAT-5 STAT-5
Fig. 2. Example of Janus kinase (JAK) inhibitors blocking cytokine
signalling. Many cytokines exert their biological effects via the
JAK–signal transducer and activator of transcription (STAT) pathway.
As JAK inhibitors block JAK enzymes from initiating this signal
transduction cascade, they also interfere with cytokine signalling. A
variety of JAK inhibitors currently being evaluated in clinical trials
interfere with more than one JAK. However, selective JAK inhibitors
are also being developed.
Table 2. Janus kinase (JAK) inhibitors currently in development for inflammatory and autoimmune diseases.
Company Agent Target Indication Developmental status
Ambit Biosciences AC-430 JAK2† RA Preclinical studies
Symansis CEP-33779 JAK2† RA Preclinical studies
SLE Preclinical studies
Galapagos GLPG-0634 JAK1†, JAK2, Tyk2 RA Phase II
Cephalon Lestaurtinib (CEP-701) JAK2† Psoriasis Phase II
Incyte and Lilly LY-3009104 (INCB-28050) JAK1†, JAK2† RA Phase II
Incyte and Novartis Ruxolitinib (INCB-018424) JAK1†, JAK2† RA Phase II
Psoriasis Phase II
Rigel R-348 JAK3† RA Phase I
Pfizer Tofacitinib JAK3†, JAK2†, JAK1 RA FDA-approved (November 2012)
Psoriasis Phase III
IBD Preclinical studies
Vertex VX-509 JAK3† RA Phase II
†Denotes primary target of inhibitor. IBD: inflammatory bowel disease; RA: rheumatoid arthritis; SLE: systemic lupus erythematosus; FDA: Food
and Drug Administration.
H. Patterson et al.
4 © 2013 British Society for Immunology, Clinical and Experimental Immunology, 176: 1–10
promising results in Phase II clinical trials for RA as well asa topical treatment for psoriasis [56,57]. Other JAK inhibi-tors demonstrating efficacy in Phase II RA clinical trialsinclude GLPG-0634, a JAK1 inhibitor currently being devel-oped by Galapagos (Mechelen, Belgium), and VX-509, aselective inhibitor of JAK3 developed by Vertex Pharmaceu-ticals (Cambridge, MA, USA) [58].
As cytokines are a central component in the pathogenesisof inflammatory and autoimmune disorders, these smallmolecule JAK inhibitors have the potential for treating awhole range of these diseases in addition to RA.
MAPK family
Another family of protein tyrosine kinases that play animportant role in the regulation of fundamental biologicalprocesses are the mitogen-activated protein kinases(MAPKs). MAPKs are among the most ancient signaltransduction pathways, and are conserved from yeast tomammals [59,60]. MAPKs act by phosphorylating specificserine and threonine residues belonging to target proteins,and are key regulators of a wide range of cellular processes,including gene expression, proliferation, differentiation andprogrammed cell death [59,61–63].
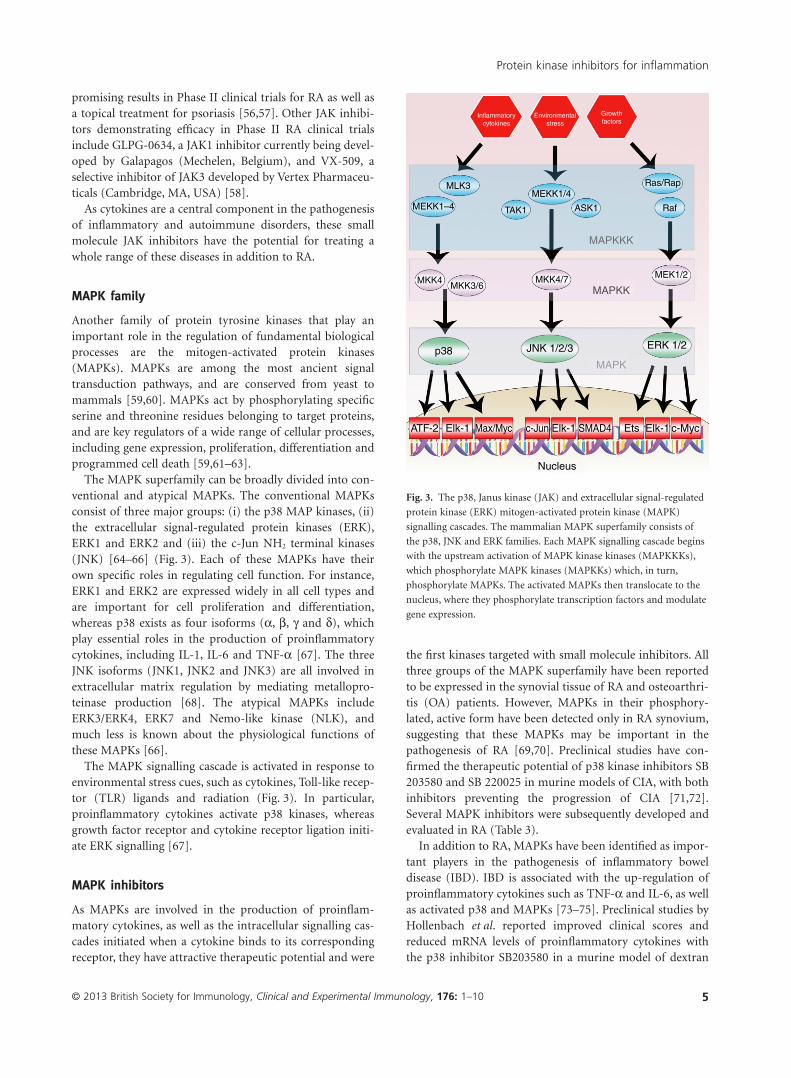
The MAPK superfamily can be broadly divided into con-ventional and atypical MAPKs. The conventional MAPKsconsist of three major groups: (i) the p38 MAP kinases, (ii)the extracellular signal-regulated protein kinases (ERK),ERK1 and ERK2 and (iii) the c-Jun NH2 terminal kinases(JNK) [64–66] (Fig. 3). Each of these MAPKs have theirown specific roles in regulating cell function. For instance,ERK1 and ERK2 are expressed widely in all cell types andare important for cell proliferation and differentiation,whereas p38 exists as four isoforms (α, β, γ and δ), whichplay essential roles in the production of proinflammatorycytokines, including IL-1, IL-6 and TNF-α [67]. The threeJNK isoforms (JNK1, JNK2 and JNK3) are all involved inextracellular matrix regulation by mediating metallopro-teinase production [68]. The atypical MAPKs includeERK3/ERK4, ERK7 and Nemo-like kinase (NLK), andmuch less is known about the physiological functions ofthese MAPKs [66].
The MAPK signalling cascade is activated in response toenvironmental stress cues, such as cytokines, Toll-like recep-tor (TLR) ligands and radiation (Fig. 3). In particular,proinflammatory cytokines activate p38 kinases, whereasgrowth factor receptor and cytokine receptor ligation initi-ate ERK signalling [67].
MAPK inhibitors
As MAPKs are involved in the production of proinflam-matory cytokines, as well as the intracellular signalling cas-cades initiated when a cytokine binds to its correspondingreceptor, they have attractive therapeutic potential and were
the first kinases targeted with small molecule inhibitors. Allthree groups of the MAPK superfamily have been reportedto be expressed in the synovial tissue of RA and osteoarthri-tis (OA) patients. However, MAPKs in their phosphory-lated, active form have been detected only in RA synovium,suggesting that these MAPKs may be important in thepathogenesis of RA [69,70]. Preclinical studies have con-firmed the therapeutic potential of p38 kinase inhibitors SB203580 and SB 220025 in murine models of CIA, with bothinhibitors preventing the progression of CIA [71,72].Several MAPK inhibitors were subsequently developed andevaluated in RA (Table 3).
In addition to RA, MAPKs have been identified as impor-tant players in the pathogenesis of inflammatory boweldisease (IBD). IBD is associated with the up-regulation ofproinflammatory cytokines such as TNF-α and IL-6, as wellas activated p38 and MAPKs [73–75]. Preclinical studies byHollenbach et al. reported improved clinical scores andreduced mRNA levels of proinflammatory cytokines withthe p38 inhibitor SB203580 in a murine model of dextran
MEKK1–4
MEKK1/4
MEK1/2
ERK 1/2JNK 1/2/3p38
ATF-2 Elk-1 Elk-1
Nucleus
Elk-1EtsSMAD4c-Jun c-MycMax/Myc
MLK3
MKK4MKK3/6
MKK4/7
TAK1 ASK1 Raf
MAPKKK
MAPKK
MAPK
Ras/Rap
Inflammatory
cytokines
Environmental
stress
Growth
factors
Fig. 3. The p38, Janus kinase (JAK) and extracellular signal-regulated
protein kinase (ERK) mitogen-activated protein kinase (MAPK)
signalling cascades. The mammalian MAPK superfamily consists of
the p38, JNK and ERK families. Each MAPK signalling cascade begins
with the upstream activation of MAPK kinase kinases (MAPKKKs),
which phosphorylate MAPK kinases (MAPKKs) which, in turn,
phosphorylate MAPKs. The activated MAPKs then translocate to the
nucleus, where they phosphorylate transcription factors and modulate
gene expression.
Protein kinase inhibitors for inflammation
5© 2013 British Society for Immunology, Clinical and Experimental Immunology, 176: 1–10

sulphate sodium (DSS)-induced experimental colitis [76].Early phase clinical trials with Semapimod (CNI-1493), ap38 kinase inhibitor, in Crohn’s disease appeared promis-ing, leading to further Phase III studies [77].
Despite their therapeutic appeal and promising earlyresults in RA and IBD, most subsequent clinical trials havegenerally failed due either to poor efficacy or toxicity [6].For example, the clinical trials of the p38 kinase inhibitorsBIRB-796 and VX-745 in RA were both terminated as aresult of adverse effects and associated toxicities, includinghepatotoxicity and other liver function abnormalities[67,78]. The placebo-controlled trial of semapimod wasineffective for the treatment of moderate to severe Crohn’sdisease [79]. It has been suggested that the side effects asso-ciated with MAPK inhibitors have prevented the use of suf-ficiently high enough therapeutic doses in the clinic,resulting in the termination of such trials due to inadequateefficacy [2,79]. Furthermore, it appears that the inhibitionof MAPKs may trigger compensatory mechanisms, asseveral clinical trials in RA resulted in a transient reductionin serum C-reactive protein (CRP) levels that were not sus-tained, suggesting that activation of alternative inflamma-tory pathways in RA patients diminished at the beginningof treatment, but then recovered 3 months later [80–82].One approach to overcome this may be to target upstreamsignalling kinases, such as the MAPKKs or the MAPKKKs,in these pathways (Fig. 3). However, the utility of MAPKinhibitors as anti-inflammatory therapies in the clinicalsetting remains unresolved, particularly with the emergenceof JAK and Syk inhibitors.
Syk
It is well established that classic immunoreceptors [i.e. B cellreceptors (BCRs), T cell receptors (TCRs) and Fc receptors(FcRs)] initiate signal transduction via relatively similarmechanisms [83]. These immunoreceptors all containimmunoreceptor tyrosine-based activation motifs (ITAMs),located on the cytoplasmic domains of transmembraneproteins on the receptors [84,85]. ITAMs are short peptidesequences with two tyrosine residues, which are rapidlyphosphorylated following receptor ligation which, in turn,induces the phosphorylation and recruitment of Syk or itsrelated homologue, zeta-chain-associated protein kinase 70
(ZAP-70). This signalling cascade is now referred to widelyas the central paradigm of immune cell signalling [83].
Syk is a 72 kDa cytosolic tyrosine kinase and belongs tothe family of non-receptor type protein tyrosine kinases[86]. Syk was first described by Taniguchi et al. [87] andlater identified as a critical signalling component requiredfor the activation and development of B cells, as well as formediating signalling through FcRs [88–90]. Syk is widelyexpressed in all haematopoietic cells and binds to the cyto-plasmic domains of BCRs, as well as FcRs expressed on avariety of cells, including B cells, mast cells and neutrophils[91]. In addition, Syk mediates signalling of other cellsurface receptors also found on non-haematopoietic cells,including β-integrins, receptors and TLR-4, as well as thecollagen receptor glycoprotein V1 [92–96]. Syk is imperativefor the initiation of signal transduction via these cell surfacereceptors and, as such, is especially important for orches-trating immune recognition receptors, as well asco-ordinating multiple downstream signalling pathways inleucocytes (Fig. 4). For example, Syk is associated with IgG(Fcγ) and IgE (FcεRI) receptors in granulocytes, and theactivation of these receptors results in degranulation andthe release of cytokines that contribute to allergic andproinflammatory responses [97].
Syk inhibitors
With Syk mediating the activation of sentinel cells (i.e. mastcells and macrophages), effector cells (i.e. neutrophils,eosinophils and basophils) and B cells, diseases such as RA,MS and SLE, where antibody-Fc receptor interactions arecentral to their pathogenesis, were identified as beingpotentially amenable to Syk suppression [98]. Severalstudies have suggested a role for Syk in the pathogenesis ofRA, with Syk expression up-regulated in the synovium ofpatients with RA compared to control OA synovium, andSyk mediating proinflammatory cytokine production(Fig. 4) [99,100]. These data suggested that Syk inhibitioncould potentially interfere with the inflammatory processesthat underlie RA, making Syk an attractive therapeutictarget in RA.
The first selective Syk inhibitor developed for treating RAwas fostamatinib (R788), an oral prodrug that is rapidlyconverted in vivo to a potent Syk inhibitor, known as R406.
Table 3. Mitogen-activated protein kinase (MAPK) inhibitors in clinical trials for inflammatory and autoimmune diseases.
Company Agent Target Indication Developmental status
Amgen AMG-548 p38α RA Terminated – liver toxicity
Boehringer Ingelheim Doramapimod (BIRB 796) p38 RA Terminated – liver and skin toxicities
Scios SCIO-323 p38α RA Terminated – skin toxicity
Sigma-Aldrich SB 220025 p38 RA Preclinical studies
Vertex VX-702 p38 RA Phase II completed
Ferring Pharmaceuticals Semapimod (CNI-1493) JNK and p38 Crohn’s disease Phase II completed
RA: rheumatoid arthritis; JNK: c-Jun NH2 terminal kinases.
H. Patterson et al.
6 © 2013 British Society for Immunology, Clinical and Experimental Immunology, 176: 1–10

R788 showed promising results in preclinical studies,suppressing inflammation and joint damage in antibody-mediated mouse models of arthritis and in a T cell-mediated rat model of RA [99,101]. The initial Phases I andII clinical trials for RA in humans suggested thatfostamatinib was well tolerated and efficacious, suppressingthe severity of arthritis and resulting in a sustained decreasein IL-6 and matrix metalloproteinase-3 (MMP-3) levels[102,103]. However, a separate concurrent study in a differ-ent RA population group (patients with an inadequateresponse to biological agents) failed to reach its primary
end-point [104]. Post-hoc analysis suggested that trialdesign could have adversely affected the observed outcomes[104,105]. However, the future of fostamatinib in RAremains unclear following the mixed therapeutic results inthe Phase III studies.
As Syk-dependent functions in both haematopoietic andnon-haematopoietic cells are central in the aetiology ofinflammatory disorders, Syk inhibitors may therefore stillprove to be efficacious in other immune diseases. MultipleSyk inhibitors are currently in clinical trials for the treat-ment of a variety of inflammatory-mediated diseases(Table 4). These trials include a Phase II clinical study of aninhaled Syk inhibitor, R343, for the treatment of allergicasthma, a chronic inflammatory disease of the airways[106]. Syk is essential for IgE receptor signal transduction inboth mast cells and basophils, resulting in the release ofproinflammatory mediators such as histamines, prostaglan-dins and cytokines [83]. R343 interrupts signal trans-duction via IgE receptors on mast cells, thus interferingwith the major inflammatory pathways underlying thepathogenesis of asthma [107].
Concluding remarks
The ultimate goal in the treatment of autoimmune diseasesis to suppress the pathological inflammatory componentand restore immunological self-tolerance, while preservingthe ability to mount an appropriate immune responseagainst invading pathogens. Protein kinases are the keydrivers of many inflammatory-mediated diseases and there-fore represent an important and promising class of thera-peutic targets in such disorders. The success of proteinkinase-directed therapies in the treatment of cancer hasspurred the search for small kinase inhibitors for the treat-ment of inflammatory and autoimmune diseases. To date,only a handful of kinase inhibitors have reached the stage ofFDA approval, while others have had mixed results in clini-cal trials. In addition to the above kinase inhibitors cur-rently undergoing clinical trials, inhibitors of other kinases,including JNK and ERK, have also been developed andawait testing in humans. It therefore remains to be deter-mined whether or not protein kinases will indeed turn outto be ‘the major drug targets of the 21st century’ [10], but
MEKKs
MMP-3
ERKs
IL-6
p38
Nucleus
Elk1ATFsc-Jun
c-Fos
Syk
JNK1
Fostamatinib
P
P
P
P
P
TN
F-R
2
Inflammation
Matrixdegradation
TNF-α
Fig. 4. Spleen tyrosine kinase (Syk)-mediated cytokine signalling and
Syk inhibitors. Syk inhibitors such as fostamatinib have been shown to
inhibit tumour necrosis factor (TNF)-α signalling both in vitro and in
vivo, therefore interfering with the production of proinflammatory
cytokine interleukin (IL)-6 and the enzyme matrix
metalloproteinase-3 (MMP-3) [active contributors to joint destruction
in rheumatoid arthritis (RA)].
Table 4. Spleen tyrosine kinase (SYK) inhibitors currently in development for inflammatory and autoimmune diseases.
Company Agent Indication Developmental status
Bayer BAY 61-3606 Allergic asthma Phase IV (FDA-approved)
Sigma-Aldrich ER-27319 Allergic diseases Preclinical studies
Tocris Bioscience
Astrazeneca and Rigel Fostamatinib (R788) RA Phase III – completed
Rigel R112 Allergic rhinitis Phase II – completed
Rigel R343 Allergic asthma Phase II
Rigel R348 Keratoconjunctivitis sicca Phase I – completed
RA: rheumatoid arthritis; FDA: Food and Drug Administration.
Protein kinase inhibitors for inflammation
7© 2013 British Society for Immunology, Clinical and Experimental Immunology, 176: 1–10

this should become more clear as our understanding of thebiology of these diseases and signalling pathways improves.
Disclosures
H. P. and R. N. have no conflicts of interest. I. M. hasreceived honoraria from Pfizer, Astra Zeneca, Galapagosand Vertex. S. S has received honoraria, speaker’s fees andconference sponsorship from Pfizer.
Acknowledgements
This paper is based on the dissertation submitted by H. P. aspart of her MScI Immunology degree in the University ofGlasgow.
References
1 Asadullah K, Volk H, Sterry W. Novel immunotherapies for pso-
riasis. Trends Immunol 2002; 23:47–53.
2 Balagué C, Kunkel SL, Godessart N. Understanding autoimmune
disease: new targets for drug discovery. Drug Discov Today 2009;
14:926–34.
3 Steinman L, Merrill JT, McInnes IB, Peakman M. Optimization of
current and future therapy. Nat Med 2012; 18:59–65.
4 Gaestel M, Mengel A, Bothe U, Asadullah K. Protein kinases as
small molecule inhibitor targets in inflammation. Curr Med Chem
2007; 14:2214–34.
5 Grant SK. Therapeutic protein kinase inhibitors. Cell Mol Life Sci
2009; 66:1163–77.
6 Kontzias A, Laurence A, Gadina M, O’Shea JJ. Kinase inhibitors in
the treatment of immune-mediated disease. F1000 Med Rep 2012;
4:5.
7 Manning G, Plowman GD, Hunter T, Sudarsanam S. Evolution of
protein kinase signaling from yeast to man. Trends Biochem Sci
2002; 27:514–20.
8 Ubersax JA, Ferrell JE Jr. Mechanisms of specificity in protein
phosphorylation. Nat Rev Mol Cell Biol 2007; 8:530–41.
9 Asadullah K, Gaestel M. Protein kinase inhibitors for the treat-
ment of inflammation – an overview. Antiinflamm Antiallergy
Agents Med Chem 2007; 6:3–4.
10 Cohen P. Protein kinases – the major drug targets of the twenty-
first century? Nat Rev Drug Discov 2002; 1:309–15.
11 Dar AC, Shoka KM. The evolution of protein kinase inhibitors
from antagonists to agonists of cellular signaling. Annu Rev
Biochem 2011; 80:769–95.
12 Shen K, Hines AC, Schwarzer D, Pickin KA, Cole PA. Protein
kinase structure and function analysis with chemical tools.
Biochim Biophys Acta 2005; 1754:65–78.
13 Klumpp S, Krieglstein J. Reversible phosphorylation of histidine
residues in proteins from vertebrates. Sci Signal 2009; 2:pe13.
14 Manning G, Whyte DB, Martinez R, Hunter T, Sudarsanam S. The
protein kinase complement of the human genome. Science 2002;
298:1912–34.
15 Burnett G, Kennedy EP. The enzymic phosphorylation of pro-
teins. J Biol Chem 1954; 211:969–80.
16 Cohen P. The origins of protein phosphorylation. Nat Cell Biol
2002; 4:E127–30.
17 Edelman AM, Blumenthal DK, Krebs EG. Protein serine/threonine
kinases. Annu Rev Biochem 1987; 56:567–613.
18 Fischer EH, Krebs EG. Relationship of structure to function of
muscle phosphorylase. Fed Proc 1966; 25:1511–20.
19 Krebs EG. The enzymology of control by phosphorylation. In:
Boyer PD, Krebs EG, eds. The enzymes: control by
phosphorylation Part A: general features: specific enzymes, vol. 17.
New York: Academic Press, 1986:3–20.
20 Melnikova I, Golden J. Targeting protein kinases. Nat Rev Drug
Discov 2004; 3:993–4.
21 Vlahovic G, Crawford J. Activation of tyrosine kinases in cancer.
Oncologist 2003; 8:531–8.
22 Zhang J, Yang PL, Gray NS. Targeting cancer with small molecule
kinase inhibitors. Nat Rev Cancer 2009; 9:28–39.
23 Lindstrom TM, Robinson WH. A multitude of kinases – which are
the best targets in treating rheumatoid arthritis? Rheum Dis Clin
North Am 2010; 36:367–83.
24 Kontzias A, Kotlyar A, Laurence A, Changelian P, O’Shea JJ.
Jakinibs: a new class of kinase inhibitors in cancer and autoim-
mune disease. Curr Opin Pharmacol 2012; 12:464–70.
25 Darnell JE Jr, Kerr IM, Stark GR. Jak–STAT pathways and tran-
scriptional activation in response to IFNs and other extracellular
signalling proteins. Science 1994; 264:1415–21.
26 Seavey MM, Dobrzanksi P. The many faces of Janus kinase.
Biochem Pharmacol 2012; 83:1136–45.
27 Leonard WJ. Role of Jak kinases and STATs in cytokine signal
transduction. Int J Hematol 2001; 73:271–7.
28 Ghoreschi K, Jesson MI, Li X et al. Modulation of innate and
adaptive immune responses by tofacitinib (CP-690, 550). J
Immunol 2011; 186:4234–43.
29 Pesu M, Candotti F, Husa M, Hofmann SR, Notarangelo LD,
O’Shea JJ. Jak3, severe combined immunodeficiency, and a new
class of immunosuppressive drugs. Immunol Rev 2005; 203:
127–42.
30 Yamaoka K, Saharinen P, Pesu M, Holt VE III, Silvennoinen O,
O’Shea JJ. The Janus kinases (Jaks). Genome Biol 2004;
5:253.
31 Stark GR, Kerr IM, Williams BR, Silverman RH, Schreiber RD.
How cells responds to interferons. Annu Rev Biochem 1998;
67:227–64.
32 Leonard WJ, O’Shea JJ. Jaks and STATs: biological implications.
Annu Rev Immunol 1998; 16:293–322.
33 Ghoreschi K, Laurence A, O’Shea JJ. Janus kinases in immune cell
signalling. Immunol Rev 2009; 228:273–87.
34 Rane SG, Reddy EP. JAK3: a novel JAK kinase associated with ter-
minal differentiation of hematopoetic cells. Oncogene 1994;
9:2415–23.
35 Kawamura M, McVicar DW, Johnston JA et al. Molecular cloning
of L-JAK, a Janus family protein–tyrosine kinase expressed in
natural killer cells and activated leukocytes. Proc Natl Acad Sci
USA 1994; 91:6374–8.
36 Levine RL, Pardanani A, Tefferi A, Gilliland DG. Role of JAK2 in
the pathogenesis and therapy of myeloproliferative disorders. Nat
Rev Cancer 2007; 7:673–83.
37 Macchi P, Villa A, Giliani S et al. Mutations of Jak-3 gene in
patients with autosomal severe combined immune deficiency
(SCID). Nature 1995; 377:65–8.
38 Pesu M, Laurence A, Kishore N, Zwillich SH, Chan G, O’Shea JJ.
Therapeutic targeting of Janus kinases. Immunol Rev 2008;
223:132–42.
H. Patterson et al.
8 © 2013 British Society for Immunology, Clinical and Experimental Immunology, 176: 1–10

39 Walker JG, Ahem MJ, Coleman M. Expression of Jak3, STAT1,
STAT4 and STAT6 in inflammatory arthritis: unique Jak3 and
STAT4 expression in dendritic cells in seropositive rheumatoid
arthritis. Ann Rheum Dis 2006; 65:149–56.
40 Changelian PS, Flanagan ME, Ball DJ et al. Prevention of organ
allograft rejection by a specific Janus kinase 3 inhibitor. Science
2003; 302:875–8.
41 Kudlacz E, Perry B, Sawyer P et al. The novel JAK-3 inhibitor
CP-690550 is a potent immunosuppressive agent in various
murine models. Am J Transplant 2004; 4:51–7.
42 Milici AJ, Kudlacz EM, Audoly L, Zwillich S, Changelian P.
Cartilage preservation by inhibition of Janus kinase 3 in two
rodent models of rheumatoid arthritis. Arthritis Res Ther 2008;
10:R14.
43 Paniagua R, Si MS, Flores MG et al. Effects of JAK3 inhibition
with CP-690,550 on immune cell populations and their functions
in nonhuman primate recipients of kidney allografts. Transplanta-
tion 2005; 80:1283–92.
44 Fleischmann R, Kremer J, Cush J et al. Placebo-controlled trial of
tofacitinib monotherapy in rheumatoid arthritis. N Engl J Med
2012; 367:495–507.
45 Burmester GR, Blanco R, Charles-Schoeman C et al. Tofacitinib
(CP-690, 550) in combination with methotrexate in patients with
active rheumatoid arthritis with an inadequate response to
tumour necrosis factor inhibitors: a randomised phase 3 trial.
Lancet 2013; 381:451–60.
46 Sandborn WJ, Ghosh S, Panes J et al. Tofacitinib, an oral Janus
kinase inhibitor, in active ulcerative colitis. N Engl J Med 2012;
367:616–24.
47 Strober B, Buonanno M, Clark JD et al. Effect of tofacitinib, a
Janus kinase inhibitor, on haematological parameters during 12
weeks of psoriasis treatment. Br J Dermatol 2013; 169:992–9.
48 European Medicines Agency. Pending EC decisions: Xeljanz.
2013. Available at: http://www.ema.europa.eu/ema/index.jsp?curl
=pages/medicines/human/medicines/002542/smops/Negative/
human_smop_000501.jsp&mid=WC0b01ac058008d7aa (accessed
1 October 2013).
49 Boy MG, Wang C, Wilkinson BE et al. Double-blind, placebo-
controlled, dose-escalation study to evaluate the pharmacologic
effect of CP-690, 550 in patients with psoriasis. J Invest Dermatol
2009; 129:2299–302.
50 Kremner JM, Bloom BJ, Breedveld FC et al. The safety and efficacy
of a JAK inhibitor in patients with active rheumatoid arthritis:
results of a double-blind, placebo-controlled phase IIa trial of
three dosage levels of CP-690,550 versus placebo. Arthritis Rheum
2009; 60:1895–905.
51 Damsker JM, Hansen AM, Caspi RR. Th1 and Th17 cells: adver-
saries and collaborators. Ann NY Acad Sci 2010; 1183:211–21.
52 Ghoreschi K, Thomas P, Breit S et al. Interleukin-4 therapy of pso-
riasis induces Th2 responses and improves human autoimmune
disease. Nat Med 2003; 9:40–6.
53 McInnes IB, Schett G. Cytokines in the pathogenesis of rheuma-
toid arthritis. Nat Rev Immunol 2007; 7:429–42.
54 Wilson NJ, Boniface K, Chan JR et al. Development, cytokine
profile and function of human interleukin 17-producing helper T
cells. Nat Immunol 2007; 8:950–7.
55 National Institute of Health – Clinical Trials.gov. Tofacitinib
search results. 2013. Available at: http://clinicaltrials.gov/ct2/
results?term=tofacitinib&Search=Search (accessed 1 October
2013).
56 Williams W, Scherle P, Shi J et al. A randomized placebo-
controlled study of INCB018424, a selective Janus kinase 1 & 2
(JAK1&2) inhibitor in rheumatoid arthritis. Arthritis Rheum
2008; 58:S431.
57 Mesa RA. Ruxolitinib, a selective JAK1 and JAK2 inhibitor for the
treatment of myeloproliferative neoplasms and psoriasis. IDrugs
2010; 13:394–403.
58 Spencer-Green G, Fan F, Frankovic B, Luo X, Hoock T, Damjanov
N. Dose ranging study of VX-509, an oral selective Jak3 inhibitor,
as monotherapy in patients with active rheumatoid arthritis (RA).
Arthritis Rheum 2011; 63:L3.
59 Dong C, Davis RJ, Flavell RA. MAP kinases in the immune
response. Annu Rev Immunol 2002; 20:55–72.
60 Widmann C, Gibson S, Jarpe MB, Johnson GL. Mitogen-activated
protein kinase: conservation of a three-kinase module from yeast
to human. Physiol Rev 1999; 79:143–80.
61 Kyriakis JM, Avruch J. Mammalian mitogen-activated protein
kinase signal transduction pathways activated by stress and
inflammation. Physiol Rev 2001; 81:807–69.
62 Schaeffer HJ, Weber MJ. Mitogen-activated protein kinases: spe-
cific messages from ubiquitous messengers. Mol Cell Biol 1999;
19:2435–44.
63 Wada T, Penninger JM. Mitogen-activated protein kinases in
apoptosis regulation. Oncogene 2004; 23:2838–49.
64 Chang L, Karin M. Mammalian MAP kinase signalling cascades.
Nature 2001; 410:37–40.
65 Davis RJ. Signal transduction by the JNK group of MAP kinases.
Cell 2000; 103:239–52.
66 Coulombe P, Meloche S. Atypical mitogen-activated protein
kinases: structure, regulation and functions. Biochim Biophys Acta
2007; 1773:1376–87.
67 Sweeney SE, Firestein GS. Mitogen activated protein kinase inhibi-
tors: where are we now and where are we going? Ann Rheum Dis
2006; 65:83–8.
68 Manning AM, Davis RJ. Targeting JNK for therapeutic benefit:
from junk to gold? Nat Rev Drug Discov 2003; 2:554–65.
69 Han Z, Boyle DL, Aupperle KR, Bennet B, Manning AM, Firestein
GS. Jun N-terminal kinase in rheumatoid arthritis. J Pharmacol
Exp Ther 1999; 291:124–30.
70 Schett G, Tohidast-Akrad M, Smolen JS et al. Activation, differen-
tial localization, and regulation of the stress-activated protein
kinases, extracellular signal-regulated kinase, c-JUN N-terminal
kinase, and p38 mitogen-activated protein kinase, in synovial
tissue and cells in rheumatoid arthritis. Arthritis Rheum 2000;
43:2501–12.
71 Badger AM, Bradbeer JN, Votta B, Lee JC, Adams JL, Griswold DE.
Pharmacological profile of SB 203580, a selective inhibitor of
cytokine suppressive binding protein/p38 kinase, in animal
models of arthritis, bone resorption, endotoxin shock and
immune function. J Pharmacol Exp Ther 1996; 279:1453–61.
72 Jackson JR, Bolognese B, Hillegass L et al. Pharmacological effects
of SB 220025, a selective inhibitor of P38 mitogen-activated
protein kinase, in angiogenesis and chronic inflammatory disease
models. J Pharmacol Exp Ther 1998; 284:687–92.
73 Brinkman BM, Telliez JB, Schievella AR, Lin LL, Goldfield AE.
Engagement of tumour necrosis factor (TNF) receptor 1 leads to
ATF-2 and p38 mitogen-activated protein kinase-dependent TNF-
alpha gene expression. J Biol Chem 1999; 274:30882–6.
74 Krautwald S. IL-16 activates the SAPK signalling pathway in CD4+macrophages. J Immunol 1998; 160:5874–9.
Protein kinase inhibitors for inflammation
9© 2013 British Society for Immunology, Clinical and Experimental Immunology, 176: 1–10

75 Tibbles LA, Woodgett JR. The stress-activated protein kinase path-
ways. Cell Mol Life Sci 1999; 55:1230–54.
76 Hollenbach E, Neumann M, Vieth M, Roessner A, Malfertheiner
P, Naumann M. Inhibition of p39 MAP kinase – and RICK/NF-
kappaB-signalling suppresses inflammatory bowel disease. FASEB
J 2004; 18:1550–2.
77 Hommes D, van den Blink B, Plasse T et al. Inhibition of stress-
activated MAP kinases induces clinical improvement in moderate
to severe Crohn’s disease. Gastroenterology 2002; 122:7–14.
78 Lee MR, Dominguez C. MAP kinase p38 inhibitors: clinical results
and an intimate look at their interactions with p38 protein. Curr
Med Chem 2005; 12:2979–94.
79 Dotan I, Rachmilewitz D, Schreiber S et al. A randomised
placebo-controlled multicentre trial of intravenous semapimod
HCI for moderate to severe Crohn’s disease. Gut 2010; 59:
760–6.
80 Cohen SB, Cheng TT, Chindalore V et al. Evaluation of
the efficacy and safety of pamapimod, a p38 MAP kinase
inhibitor, in a double-blind, methotrexate-controlled study of
patients with active rheumatoid arthritis. Arthritis Rheum 2009;
60:335–44.
81 Damjanov N, Kauffman RS, Spencer-Green GT. Efficacy, pharma-
codynamics, and safety of VX-702, a novel p38 MAPK inhibitor, in
rheumatoid arthritis: results of two randomized, double-blind,
placebo-controlled clinical studies. Arthritis Rheum 2009;
60:1232–41.
82 Genovese MC, Cohen SB, Wofsy D et al. A 24-week, randomized,
double-blind, placebo-controlled, parallel group study of the effi-
cacy of oral SCIO-469, a p38 mitogen-activated protein kinase
inhibitor, in patients with active rheumatoid arthritis. J
Rheumatol 2011; 38:846–54.
83 Mocsai A, Ruland J, Tybulewicz VLJ. The SYK tyrosine kinase: a
crucial player in diverse biological functions. Nat Rev Immunol
2010; 10:387–402.
84 Cambier JC. New nomenclature for the Reth motif (or ARH1/
TAM/ARAM/YXXL). Immunol Today 1995; 16:110.
85 Reth M. Antigen receptor tail clue. Nature 1989; 338:383–4.
86 Kurosaki T, Takata M, Yamanashi Y et al. Syk activation by the
Src-family tyrosine kinase in the B cell receptor signaling. J Exp
Med 1994; 179:1725–9.
87 Taniguchi T, Kobayashi T, Kondo J et al. Molecular cloning of a
porcine gene syk that encodes a 72-kDa protein-tyrosine kinase
showing high susceptibility to proteolysis. J Biol Chem 1991;
266:15790–6.
88 Kurosaki T. Regulation of B cell fates by BCR signaling compo-
nents. Curr Opin Immunol 2002; 14:341–7.
89 Sada K, Takano T, Yanagi S, Yamamura H. Structure and
function of Syk protein-tyrosine kinase. J Biochem 2001; 130:177–
86.
90 Turner M, Schweighoffer E, Colucci F, Di Santo JP, Tybulewicz
VL. Tyrosine kinase SYK: essential functions for immunoreceptor
signalling. Immunol Today 2000; 21:148–54.
91 Robak T, Robak E. Tyrosine kinase inhibitors as potential drugs
for B-cell lymphoid malignancies and autoimmune disorders.
Expert Opin Invest Drugs 2012; 21:921–47.
92 Chaudhary A, Fresquez TM, Naranjo MJ. Tyrosine kinase Syk
associates with Toll-like receptor 4 and regulates signaling in
human monocytic cells. Immunol Cell Biol 2007; 85:249–56.
93 Mocsai A, Zhou M, Meng F, Tybulewicz VL, Lowell CA. Syk is
required for integrin signalling in neutrophils. Immunity 2002;
16:547–58.
94 Takada Y, Aggarwal BB. TNF activates Syk protein tyrosine kinase
leading to TNF-induced MAPK activation, NF-kappaB activation,
and apoptosis. J Immunol 2004; 173:1066–77.
95 Watson SP, Auger JM, McCarty OJ, Pearce AC. GPVI and integrin
alphaIIb beta3 signaling in platelets. J Thromb Haemost 2005;
3:1752–62.
96 Willeke T, Schymeinsky J, Prange P, Zahler S, Walzog B. A role for
Syk-kinase in the control of the binding cycle of the beta2
integrins (CD11/CD18) in human polymorphonuclear
neutrophils. J Leukoc Biol 2003; 74:260–9.
97 Bhagwat SS. Kinase inhibitors for the treatment of inflam-
matory and autoimmune disorders. Purinergic Signal 2009;
5:107–15.
98 Wong BR, Grossbard EB, Payan DG, Masuda ES. Targeting Syk as
a treatment for allergic and autoimmune disorders. Expert Opin
Investig Drugs 2004; 13:743–62.
99 Braselmann S, Taylor V, Zhao H et al. R406, an orally available
spleen tyrosine kinase inhibitor blocks fc receptor signalling and
reduces immune complex-mediated inflammation. J Pharmacol
Exp Ther 2006; 319:998–1008.
100 Cha HS, Boyle DL, Inoue T et al. A novel spleen tyrosine
kinase inhibitor blocks c-Jun N-terminal kinase-mediated gene
expression in synoviocytes. J Pharmacol Exp Ther 2006; 317:
571–8.
101 Pine PR, Chang B, Schoettler N et al. Inflammation and bone
erosion are suppressed in models of rheumatoid arthritis follow-
ing treatment with a novel Syk inhibitor. Clin Immunol 2007;
124:244–57.
102 Weinblatt ME, Kavanaugh A, Burgos-Vargas R et al. Treatment of
rheumatoid arthritis with a Syk kinase inhibitor: a twelve-week,
randomized, placebo-controlled trial. Arthritis Rheum 2008;
58:3309–18.
103 Weinblatt ME, Kavanaugh A, Genovese MC, Musser TK,
Grossbard EB, Magilavy DB. An oral spleen tyrosine kinase (Syk)
inhibitor for rheumatoid arthritis. N Engl J Med 2010; 363:
1303–12.
104 Genovese MC, Kavanaugh A, Weiblatt ME et al. An oral Syk kinase
inhibitor in the treatment of rheumatoid arthritis: a three-month
randomized, placebo-controlled, phase II study in patients with
active rheumatoid arthritis that did not respond to biologic
agents. Arthritis Rheum 2011; 63:337–45.
105 Boers M. Syk kinase inhibitors for rheumatoid arthritis: trials and
tribulations. Arthritis Rheum 2011; 63:329–30.
106 National Institute of Health – Clinical Trials.gov. NCT01591044.
2013. Available at: http://clinicaltrials.gov/ct2/results?term=R343
&Search=Search (accessed 1 October 2013).
107 Norman P. A novel Syk kinase inhibitor suitable for inhalation:
R-343(?)-WO-2009031011. Expert Opin Ther Pat 2009; 19:
1469–72.
H. Patterson et al.
10 © 2013 British Society for Immunology, Clinical and Experimental Immunology, 176: 1–10




















