Orbital Diseases
389
-
Upload
khangminh22 -
Category
Documents
-
view
3 -
download
0
Transcript of Orbital Diseases


Surgical Atlas
o f
Orbital Diseases
System requirement:• Windows XP or above• Power DVD player (Software)• Windows media player 10.0 version or above• Quick time player version 6.5 or above
Accompanying DVD ROM is playable only in Computer and not in DVD player.Kindly wait for few seconds for DVD to autorun. If it does not autorun then please do the following:• Click on my computer• Click the DVD drive labelled JAYPEE and after opening the drive, kindly double click the file Jaypee
basm
ala
blog
(alw
ays o
rigin
al)

Subrahmanyam Mallajosyula MS, DO
Head, Dept of OphthalmologyBhaskar Medical College
Former Superintendent and ChiefDept of Oculoplastics and Orbital Services
Sarojini Devi Eye HospitalHyderabad, Andhra Pradesh, India
JAYPEE BROTHERS MEDICAL PUBLISHERS (P) LTDNew Delhi • Ahmedabad • Bengaluru • Chennai • Hyderabad • Kochi • Kolkata • Lucknow • Mumbai • Nagpur
®
Surgical Atlaso f
Orbital Diseases
basm
ala
blog
(alw
ays o
rigin
al)

Published byJitendar P VijJaypee Brothers Medical Publishers (P) LtdCorporate Office4838/24 Ansari Road, Daryaganj, New Delhi - 110002, India, Phone: +91-11-43574357Registered OfficeB-3 EMCA House, 23/23B Ansari Road, Daryaganj, New Delhi - 110 002, IndiaPhones: +91-11-23272143, +91-11-23272703, +91-11-23282021+91-11-23245672, Rel: +91-11-32558559, Fax: +91-11-23276490, +91-11-23245683e-mail: [email protected], Visit our website: www.jaypeebrothers.com
Branches2/B, Akruti Society, Jodhpur Gam Road SatelliteAhmedabad 380 015, Phones: +91-79-26926233, Rel: +91-79-32988717Fax: +91-79-26927094, e-mail: [email protected] Batavia Chambers, 8 Kumara Krupa Road, Kumara Park EastBengaluru 560 001, Phones: +91-80-22285971, +91-80-22382956, 91-80-22372664Rel: +91-80-32714073, Fax: +91-80-22281761 e-mail: [email protected] IIIrd Floor, Khaleel Shirazi Estate, Fountain Plaza, Pantheon RoadChennai 600 008, Phones: +91-44-28193265, +91-44-28194897, Rel: +91-44-32972089 Fax: +91-44-28193231 e-mail: [email protected]/1-3, 1st Floor, Balaji Building, Ramkote Cross Road,Hyderabad 500 095, Phones: +91-40-66610020, +91-40-24758498Rel:+91-40-32940929, Fax:+91-40-24758499 e-mail: [email protected]. 41/3098, B & B1, Kuruvi Building, St. Vincent RoadKochi 682 018, Kerala, Phones: +91-484-4036109, +91-484-2395739+91-484-2395740 e-mail: [email protected] Indian Mirror Street, Wellington SquareKolkata 700 013, Phones: +91-33-22651926, +91-33-22276404+91-33-22276415, Rel: +91-33-32901926, Fax: +91-33-22656075e-mail: [email protected] Market III, B-2, Sector-4, Faizabad Road, Indira NagarLucknow 226 016 Phones: +91-522-3040553, +91-522-3040554e-mail: [email protected] Amit Industrial Estate, 61 Dr SS Rao Road, Near MGM Hospital, ParelMumbai 400 012, Phones: +91-22-24124863, +91-22-24104532,Rel: +91-22-32926896, Fax: +91-22-24160828e-mail: [email protected]“KAMALPUSHPA” 38, Reshimbag, Opp. Mohota Science College, Umred RoadNagpur 440 009 (MS), Phone: Rel: +91-712-3245220, Fax: +91-712-2704275e-mail: [email protected]
USA Office1745, Pheasant Run Drive, Maryland Heights (Missouri), MO 63043, USA, Ph: 001-636-6279734e-mail: [email protected], [email protected]
Surgical Atlas of Orbital Diseases
© 2008, Jaypee Brothers Medical PublishersAll rights reserved. No part of this publication and DVD ROM should be reproduced, stored in a retrieval system, or transmitted in any form orby any means: electronic, mechanical, photocopying, recording, or otherwise, without the prior written permission of the editor and thepublisher.
This book has been published in good faith that the material provided by contributors is original. Every effort is made to ensure accuracy ofmaterial, but the publisher, printer and editor will not be held responsible for any inadvertent error(s). In case of any dispute, all legal mattersare to be settled under Delhi jurisdiction only.
First Edition: 2009ISBN 978-81-8448-394-9
Typeset at JPBMP typesetting unitPrinted at Ajanta Offset & Packagins Ltd., New Delhi
basm
ala
blog
(alw
ays o
rigin
al)

This book is dedicatedto
my family members, my teachers, my team membersand
my patients
basm
ala
blog
(alw
ays o
rigin
al)

basm
ala
blog
(alw
ays o
rigin
al)
Contributors
B Ranganadha Reddy MS
Professor and HeadDept of OtorhinolaryngiologyGandhi Medical CollegeHyderabad, India
Cat N Burkat MD
Assistant ProfessorOculoplastic Surgery ServiceDepartment of Ophthalmology and Visual SciencesUniversity of Wisconsin600 Highland AvenueMadison, WI 53792, USA
Christopher M Knapp BSc (Hons), FRC Ophth
Clinical LecturerDept of OphthalmologyUniversity of LeicesterLeicester Royal InfirmaryLeicester LEI 5 WW, UK
D Ravi Varma DM (Neuroradiology)
Consultant, Interventional and NeuroradiologistDept of RadiologyKrishna Institute of Medical SciencesHyderabad, India
Debraj Shome DO, DNB, FRCS (Glasgow), MNAMS, MS
Consultant, Department of Ophthalmicand Facial Plastic and Ocular OncologyAditya Jyot Eye Hospital Pvt LtdMumbai and Honorary ConsultantDept of Ocular OncologyAdvanced Center for Treatment Research andEducation in CancerTata Memorial CenterMumbai, India
Dinesh Selva MBBS (Hons), FRACS, FRANZCO
Professor and ChairmanSouth Australian Institute of OphthalmologyUniversity of Adelaide, Australia
Geeta K Vemuganti MD
DirectorOphthalmic Pathology ServiceLV Prasad Eye InstituteHyderabad, India
Golam Haider MS, FCPS
Associate ProfessorDept of Oculoplastics and Orbital ServicesNational Institute of OphthalmologyDhaka, Bangladesh
Jack Rootman MD, FRCSC
ProfessorDept of Ophthalmology and PathologyUniversity of British ColumbiaVancouver, Canada
Kahana Alon MD, PhD
Assistant ProfessorOculoplastic Surgery ServiceDepartment of Ophthalmology and Visual SciencesKellogg Eye Center, University of Michigan1000 Wall Street, Ann Arbor, MI 48105, USA
Kasturi Bhattacharjee MS, DNB, FRCS (Ed)
Senior Consultant and HeadDept of OrbitOphthalmoplastic and Reconstructive SurgeryShankaradeva NetralayaBeltola, Guwahati, Assam India
Kuldeep Raizada PhD
Head Dept of Ocular Prosthesis ServiceLV Prasad Eye InstituteHyderabad
Leaurence Brown FRC (Path)
Consultant HistopathologistDept of PathologyLeicester Royal InfirmaryLeicester LEI 5 WW, UK
basm
ala
blog
(alw
ays o
rigin
al)

viiiviiiviiiviiiviii Surgical Atlas of Orbital DiseasesSurgical Atlas of Orbital DiseasesSurgical Atlas of Orbital DiseasesSurgical Atlas of Orbital DiseasesSurgical Atlas of Orbital Diseases
M Chandrasekhara Reddy MS, MCh
Professor, Dept of NeurosurgeryGandhi Medical CollegeHyderabad, India
Mark J Lucarelli MD
Associate ProfessorOculoplastic Surgery ServiceDepartment of Ophthalmology and Visual SciencesUniversity of Wisconsin, 600 Highland AvenueMadison, WI 53792, USA
Modini Pandarpurkar MS
Assistant Professor of OphthalmologyFellow Oculoplastics and Orbital ServicesSarojini Devi Eye HospitalHyderabad, India
Mohd Ather MS
Assistant Professor of OphthalmologyOculoplastics and Orbital ServicesSarojini Devi Eye HospitalHyderabad, India
Mohd Javed Ali MS, FRCS, FRCGP
Fellow, Dept of Oculoplastics and Orbital ServicesSarojini Devi Eye HospitalHyderabad, India
Nancy Kim MD, PhD
Fellow, Oculoplastics and Orbital ServicesUniversity of Wisconsin Medical SchoolMadison, Wisconsin, USA
Peter J Dolman MD, FRCSC
Associate ProfessorDept of Oculoplastics and Orbital ServicesUniversity of British Columbia, Vancouver, Canada
Raghavan Sampath FRCS, FRC Ophth
Consultant Lid, Lacrimal and Orbit SurgeonDept of OphthalmologyLeicester Royal InfirmaryLeicester LEI 5 WW, UK
Ram Vaidhyanath FRCR
Consultant RadiologistDept of RadiologyLeicester Royal InfirmaryLeicester LEI 5 WW, UK
Raman Mittal DNB
ConsultantDept of Ophthalmic Plastic SurgeryOrbital Diseases and Ocular OncologyMGM Eye Institute, Raipur, India
Ramesh Murthy MD, FRCS
Senior ConsultantOculoplasty and Ocular Oncology Serviceand Pediatric Ophthalmologyand Strabismus ServiceLV Prasad Eye InstituteHyderabad, India
Ratnakar KS MD
HeadDept of PathologyGlobal HospitalHyderabad, India
Ravindra Mohan E MD, FRCS (Edin)
DirectorDept of Oculoplastics and Orbital ServicesShankara Netralaya, Chennai, India
Richard K Dortzbach MD, FACS
Professor EmeritusOculoplastic Surgery ServiceDepartment of Ophthalmology and Visual SciencesUniversity of Wisconsin600 Highland AvenueMadison, WI 53792, USA
Santosh G Honavar MD, FRCS
DirectorDept of OculoplasticsOrbital Services and Ocular OncologyLV Prasad Eye InstituteHyderabad, India
Subrahmanyam Mallajosyula MS, DO
Head, Dept of OphthalmologyBhaskar Medical CollegeFormer Superintendent and ChiefDept of Oculoplastics and Orbital ServicesSarojini Devi Eye HospitalHyderabad, India
Venkatesh C Prabhakaran MD
Clinical LecturerOculoplastic and Orbital DivisionSouth Australian Institute of Ophthalmologyand Department of PathologyUniversity of AdelaideAustralia
Vijay Anand P Reddy MD
Chief, Dept of Radiology and RadiotherapyApollo HospitalHyderabad, India
basm
ala
blog
(alw
ays o
rigin
al)

I became acquainted with Subrahmanyam Mallajosyula (Subbu) when he spent a period of time during 1998training with me as a fellow in orbit and oculoplastics at the University of British Columbia in Vancouver,Canada. At that time, he had been trained in India by some of the top surgeons and had furthered hispractical knowledge by visits and fellowships throughout the world. On a personal level, Subbu is anenergetic, kind and competent man driven by a strong desire to teach and to bring contemporary care tothose in great need. He has become a considerable force in aiding his colleagues in India with regard tooculoplastics and orbit. He is supported by his wife, Kalyani and family, all of whom are wedded to a deepcaring for humanity.
In the last three decades, advances in imaging, pathology, genetics, immunology and endocrinology,clinical evaluations have led to a consolidation of knowledge concerning diseases of the orbit. Coupled withsurgical innovations, these advances have led to a better understanding of the management of diseaseaffecting the orbit. There is, however, a need to bring together and simplify this knowledge in order toprovide practical and obtainable care in the developing order. Subbu has gathered a group of distinguishedand well-known orbital specialists as well as colleagues from India with vast, practical experience toaccomplish this goal. His hope is to target readers who are graduate students, residents of ophthalmology,fellows in oculoplastic and orbital services, and general ophthalmologists who encounter an oculoplasticproblem. This is an important and unique endeavour grounded in Subrahmanyam's long-time practice inpublic service in Hyderabad, where he has encountered the full range of orbital problems and challenges.He has brought to bear his skills, nurtured first in India and then through a range of travel and fellowshipsat some of the best orbital centers in the world. It is from these centers and from his wide collegial networkthat he has been able to produce this practical compendium of orbital knowledge. I believe his contributionwill not only further the orbital and oculoplastic services in India, Asia and Africa, but also it will bring anawareness of the vast experience in those areas to the rest of the world. The book is meant to provideprecise and succinct information on orbital disease, its evaluation and management. The emphasis is ofcourse on common disorders but also presents information on uncommon conditions backed up by caseillustrations.
As a mentor, colleague and author, I feel privileged to be a part of this enterprise.
Jack Rootman MD, FRCSC
ProfessorDepartment of Ophthalmology and Visual Sciences
Department of Pathology and Laboratory MedicineUniversity of British Columbia
Vancouver, British Columbia, Canada
Foreword
basm
ala
blog
(alw
ays o
rigin
al)

basm
ala
blog
(alw
ays o
rigin
al)

Preface
When I was a student, I often heard from my teachers saying "Proptosis is a Pandora's box". SurprisinglyI continue to hear it even today! Many a time I am asked to speak on the topic titled "Proptosis is a Pandora'sbox", and I always change it to "Is Proptosis still a Pandora's box?" It was so, in the past, when the onlyimaging available was orbital venography. The information of the orbital disease process obtained with itwas very meager. I salute my professor Dr. Vengala Rao, who used to perform orbitotomies in those days.It is the challenges he used to encounter, that stimulated me to take up this branch. Fortunately, advances inimaging techniques have made an immense contribution in the assessment of a case of proptosis, so thattoday, we know what we are dealing with. With careful clinical assessment, and knowledge in reading ofCT/MRI, we can even arrive at the histopathological diagnosis of majority of cases. Hence, surprises arevery few and far in between. Similarly, advances in histopathology and immunohistochemistry, anesthesia,chemo and radio therapy have made immense contributions in understanding and management of proptosis.The best example is Rhabdomyosarcoma. Today, nearly half the cases of proptosis can be managed by non-surgical methods or with very minor surgical procedures. I thankfully acknowledge the roles of Dr VengalaRao, my first teacher, Jack Rootman, Peter J Dolman, Brad Lemke and Mark J Lucarelli in furthering myunderstanding of orbital diseases.
The specialty of orbital diseases is very well advanced in North America and Europe, but not so in mostother countries. Availability of ophthalmic literatures authored by orbital surgeons from the developingcountries are very few. The idea of bringing this color atlas is to share two decades of my experience inorbital diseases. Though it is an atlas in principle, enough information is provided to understand theconditions and plan treatment strategies. It covers most of the common and some of the rare causes ofproptosis. With color illustrations, and case presentations, I tried to make this book interesting to read andalso to provide practical knowledge in clinical situations.
I thank all my contributing authors, who are internationally reputed, for their co-operation. The chaptersthey contributed were those in which they have a wealth of experience, viz. Jack Rootman on mesenchymaltumors, Peter J Dolman on thyroid associated orbitopathy (We rarely see such severe TAO in India ), MarkJ Lucarelli on anatomy and fractures of orbit.
I hope my efforts help shatter the myth that "proptosis is a Pandora's box". If this book inspires at leastsome ophthalmologists to pursue this specialty with more interest and vigor and blossom into efficientorbital surgeons, the purpose of this book is served. I truly believe that "What I do, you can also do" andwho knows you may do even better.
Subrahmanyam Mallajosyula15-05-2008Hyderabad
basm
ala
blog
(alw
ays o
rigin
al)

basm
ala
blog
(alw
ays o
rigin
al)

Acknowledgements
At the outset, I wish to acknowledge the significant roles played initially by my parents and then by mywife Rama, in my professional pursuits, which took a lot of time from my family and children Harsha andAahlad. I greatly appreciate their cooperation.
My teacher Dr. Kotagiri Vengala Rao was the first to introduce me to orbital surgery during my post-graduation. I still relish those memories. I thank Dr. Jeffrey Nerad for introducing me to Dr. Jack Rootman.I acknowledge the role of Dr. Jack Rootman, Peter J Dolman in fine tuning my skills—both clinical andsurgical. They are not only great teachers, but also wonderful human beings. My fellowship with them wasmade possible due to the financial assistance I received from them. I also thank the Orbis Inc. for awardingme the Ziegler's International Fellowship, which has part financed my fellowship at University of BritishColumbia, Vancouver. Similarly I thank the Association of Asian Indians in Ophthalmology for awardingthe competitive fellowship, which financed my training with Mark J Lucarelli, Brad Lemke and Richard KDortzbach at the University of Wisconsin, Madison. It was a great learning experience.
I thank all my contributing authors (and their supporting staff), who are all very eminent and highlyreputed, for sparing their time to make this book wonderful. I thank my fellow Dr. Mohd Javed Ali, for allhis assistance in proofreading. He is ever ready to help.
I wish to acknowledge the support and encouragement I received from Shri Jitendar P Vij, Chairmanand Managing Director, Mr Tarun Duneja, Director (Publishing) and Mr PS Ghuman, Sr Production Managerof M/s Jaypee Brothers Medical Publishers (P) Ltd. I also thank Mr Upinder, Mr Pankaj, Mr Ram Murti andMrs Seema Dogra of the same family (Jaypee) for their technical support.
basm
ala
blog
(alw
ays o
rigin
al)

basm
ala
blog
(alw
ays o
rigin
al)

Part One : Basic Concepts
1. Applied Anatomy of Orbit ................................................................................................................. 03Mark J Lucarelli, Nancy KimOrbital osteology 3; The periorbita 6; The orbital apex 6; The cavernous sinus 8; The globe 8; Theextraocular muscles 9; Lids 10; The lacrimal system 13; The nerves of the orbit 14; Vascular anatomy of theorbit: Arterial supply 17; Vascular anatomy of the orbit: Venous outflow 19; Paranasal sinuses 20;Conclusion 20
2. Clinical Approach to Proptosis ......................................................................................................... 23Subrahmanyam MallajosyulaPain 23; Progression 25; Proptosis 28; Axial proptosis 29; Measurement of proptosis 35; Pulsations 37;Pupil 41; Perception of color vision 41; Prism bar-cover test (PBCT) 42; Periorbital changes 45; Lid changes46; Conjunctival changes 48; Palpation 51; Auscultation 51; Evaluation of a case of proptosis 53
3. Imaging a Case of Proptosis: CT and MRI .................................................................................... 56Subrahmanyam Mallajosyula, Ravi VarmaEvaluation of a CT scan of orbit 58; Common mistakes 59; Bony orbit 60; Eyeball 65; Enlarged extraocularmuscle 69; Soft-tissue lesions 72; Lacrimal gland tumors 76; Cystic lesions of the orbit 78; Metastaticlesions 81; Contrast enhancement 83; 3-D reconstruction of the orbit 84
4. Role of Cytology in Orbital Lesions ................................................................................................ 85Geeta K Vemuganti, Anirban Bhaduri Fine needle aspiration/sampling techniques 85; Intraoperative-operative diagnosis by squash and imprintcytology 85; Squash/imprint cytology 85; Case illustrations 86
5. Pathology of the Orbital Diseases ................................................................................................... 97KS RatnakarClassification 97; Diagnosis of orbital tumors 98; Developmental lesions 98; Inflammatory lesions 100;Orbital infections 101; Cysticercosis 102; Neoplastic lesions 102; Benign tumors 103; Malignant tumors104; Metastasis 105; Grave's disease 106; Mucocele 106
Contents
basm
ala
blog
(alw
ays o
rigin
al)

xvixvixvixvixvi Surgical Atlas of Orbital DiseasesSurgical Atlas of Orbital DiseasesSurgical Atlas of Orbital DiseasesSurgical Atlas of Orbital DiseasesSurgical Atlas of Orbital Diseases
Part Two : Disease Patterns of Proptosis
6. Thyroid-Associated Orbitopathy.................................................................................................... 111Peter J DolmanIncidence and epidemiology 112; Risk factors and predictive variables 112; Pathogenesis 112; Course ofdisease 114; Clinical classification 114; The VISA classification 114; Vision/optic neuropathy 114;Inflammation/congestion 116; Strabismus/motility restriction 117; Appearance/exposure 117; Generalmanagement guidelines 118
7. Orbital Infections ............................................................................................................................... 120Shome debraj, Walinjkar Jaydeep, Mukherjee AngshumanRisk factors 121; Etiological causes of orbital infections 121; Bacterial infections 121; Fungal infections121; Parasitic infections 121; Protozoal infections 121; Diagnosis 121; Imaging studies 121; Emergencydepartment care 122; Further inpatient care 122; Case illustrations 123
8. Orbital Inflammatory Disease ........................................................................................................ 128E Ravindra Mohan, Moupia Goswami, Vinathi MutyalaOrbital amyloidosis 129; Sarcoidosis 130; Nonspecific orbital inflammatory syndrome (NSOIS) 131;Kimura’s disease 132; Wegener’s granulomatosis 132; Langerhan’s histiocytosis 133; Rosai-Dorfmandisease 133; Orbital xanthogranuloma 134; Case illustrations 134
9. Orbital Lymphoma ............................................................................................................................. 146Christopher Knapp, Ram Vaidhyanath, Laurence Brown, Raghavan SampathREAL classification 146; WHO classification of NHL 146; Modified Rye’s classification of Hodgkin’slymphoma 147; When to suspect lymphoma 147; When to suspect idiopathic orbital inflammatory disease148; Case illustrations 148
10. Vascular Lesions of Orbit ................................................................................................................ 151Subrahmanyam Mallajosyula, Mohd Javed AliMalformations 151; Lymphangioma 151; Orbital varices 152; Cavernous hemangioma 152; Othercongenital malformations 152; Sturge-Weber syndrome 152; Wyburn-Mason syndrome 153; Klippel-Trenaunay syndrome 153; Shunts 153; Carotid-Cavernous fistula 153; New growths 154; Capillaryhemangioma 154; Hemangiopericytoma 155; Angiosarcoma 155; Kaposi’s sarcoma 155;Hemangioendothelioma 155; Hemangioblastoma 155; Case illustrations 157
11. Orbital Tumors of Neurological Origin........................................................................................ 162Christopher M Knapp, Ram Vaidhyanath, Laurence Brown, Raghavan SampathOptic nerve glioma 162; Optic nerve meningioma 163; Orbital schwannoma (neurilemmoma) andneurofibroma 165; Case illustrations 166
12. Mesenchymal Tumors ....................................................................................................................... 170E Weis, J RootmanMesenchymal soft tissue tumors 170; Rhabdomyosarcoma 170; Rhabdomyoma 172; Leiomyoma 172;Leiomyosarcomas 172; Adipose tumors 172; Liposarcoma 174; Fibrous tissue tumors 174; Histiocytictumors 175; Fibrous histiocytoma 175; Malignant tumors of uncertain type 175; Rhabdoid tumor 175
basm
ala
blog
(alw
ays o
rigin
al)

13. Bone Tumors of Orbit ....................................................................................................................... 180Venkatesh C Prabhakaran, Dinesh SelvaClinical presentation 180; Osteoma 180; Fibrous dysplasia 181; Ossifying fibroma 182; Osteoblastoma183; Chondroma 183; Cholesterol granuloma 184; Aneurysmal bone cyst 184; Giant cell lesions 184;Osteogenic sarcoma 184; Chondrosarcoma 186; Mesenchymal chondrosarcoma 186; Ewing’s sarcoma186; Langerhan’s cell histiocytosis (LCH) 186; Intraosseous hemangioma 186
14. Tumors of Lacrimal Gland ............................................................................................................... 190Raman MittalClassification 190; Epithelial cyst (Dacryops) 190; Case illustrations 191; Pleomorphic adenoma 191;Adenoid cystic carcinoma 194
15. Cystic lesions of Orbit ...................................................................................................................... 199Golam Haider, Subrahmanyam Mallajosyula, Mohd Javed AliClassification 199; Dermoid and epidermoid cysts 200; Teratomas 201; Cephalocele 201; Microphthalmoswith cyst 202; Mucocele 202; Cysts of the optic nerve sheath 203; Hematic cyst 203; Simple cyst 204;Retention cyst 204; Lacrimal ductal cyst 204; Implantation cyst 205; Dacryocele 205
16. Parasitic Cysts of Orbit ..................................................................................................................... 207Subrahmanyam Mallajosyula, Mohd Ather, Modini PandarpurkarCysticercosis 207; Case illustrations 208; Hydatid cyst of orbit 217
17. Orbital Fractures ................................................................................................................................ 220Alon Kahana, Mark J Lucarelli, Cat N Burkat, Richard K DortzbachIntroduction 220; Anatomy 220; Imaging 226; Implant materials 227; General operative considerations229; Pediatric patients 231; Timing of surgery 231; Decision: repair or not repair 232; Floor fractures 233;Medial wall fractures 236; Lateral wall and zygomatico maxillary fractures 238; Late and secondaryfracture repair 238
18. Secondary and Metastatic Orbital Tumors ................................................................................. 244Kasturi Bhattacharjee, Harsha Bhattacharjee, Ganesh Kuri, Shyamanga BorooahOrbital extension of intraocular tumors 244; Orbital extension of retinoblastoma 244; Orbital extension ofmedulloepithelioma 246; Orbital extension of uveal melanoma 247; Orbital extension of lacrimal sactumors 250; Orbital extension of eyelid tumors 252; Basal cell carcinoma (BCC) 252; Sebaceous carcinomaof the eyelid 253; Squamous cell carcinoma of the eyelid 255; Malignant melanoma of eyelid 256; Orbitalextension of intracranial tumors 257; Orbital extension of conjunctival tumors 258; Squamous cellcarcinoma of the conjunctiva 258; Malignant Melanoma of the conjunctiva 259; Orbital extension oftumors of the nasal cavity and paranasal sinus 260; Orbital extension of nasopharyngeal tumor 262;Metastatic orbital tumors 263
ContentsContentsContentsContentsContents xviixviixviixviixvii
basm
ala
blog
(alw
ays o
rigin
al)

xviiixviiixviiixviiixviii Surgical Atlas of Orbital DiseasesSurgical Atlas of Orbital DiseasesSurgical Atlas of Orbital DiseasesSurgical Atlas of Orbital DiseasesSurgical Atlas of Orbital Diseases
Part Three : Management Strategies: Surgical
19. Decision Making ................................................................................................................................ 271Subrahmanyam MallajosyulaIntraconal lesion 273; Reese-Berke’s incision 273; Steps of Reese-Berke approach 274; Steps of superiorlidcrease incision 275; Apical conal lesions 279; Lesions of superior peripheral space 279; Thyroidassociated orbitopathy 285
20. Orbitotomies ........................................................................................................................................ 288Ramesh Murthy, Anirban Bhaduri, Vikas Menon, Santosh G HonavarGeneral principles 288; Approaches 289; Anterior orbitotomy 289; Swinging lower eyelid flap 289; Lateralorbitotomy 290; Stallard-Wright lateral orbitotomy 290; Transfrontal orbitotomy 291; Complications 291;Postoperative management 291; Case illustrations 291
21. Multidisciplinary Approach to Proptosis .................................................................................... 299Subrahmanyam Mallajosyula, B Ranganadha Reddy, M Chandrasekhar ReddySurgical anatomy 299; ENT approach to proptosis 300; Various etiological factors of proptosis in ENT300; Sinus diseases causing proptosis 301; Purulent infections 301; Extensive nasal polyposis 301;Mucormycosis 301; Allergic fungal sinusitis 301; Fronto- ethmoidal mucocele 302; Tumors of paranasalsinuses causing proptosis 302; Fibrous dysplasia 302; Hemangiopericytoma 302; Juvenile nasopharyngealangiofibroma 303; Squamous cell carcinoma 303; Rhabdomyosarcoma 303; Non-Hodgkin’s lymphoma303; Esthesio-neuroblastoma 304; Caldwell-Luc operation 304; Lateral rhinotomy/medial maxillectomy305; Total maxillectomy 306; Patterson’s operation 305; FESS 309; Neurosurgical approaches of proptosis309; Transcranial approach 311; Extracranial approach 309; Case illustrations 313
22. Orbital Exenteration .......................................................................................................................... 318Ramesh Murthy, Anirban Bhaduri, Sima Das, Santosh G HonavarIndications 318; Patient preparation 318; Surgical procedure 318; Types 319; Management of theexenterated socket 320; Prosthesis 320; Complications of exenteration 320; Case illustrations 321
23. Orbital Prosthesis............................................................................................................................... 327Kuldeep RaizadaTypes of prosthesis 327; Complete prosthesis 327; Factors that affect the fit of an orbital prosthesis 328;Preparation of the patient 328; Impression of the orbital defect 328; Casting 329; Sculpting 329; Moulding330; Using the desired material 331; Fabrications of ocular prosthesis 331; Assemble of prosthesis 331;Care of your prosthesis 331; Storing the prosthesis 332; Preventing mishaps 333
Part Four : Management Strategies: Nonsurgical
24. Medical Management of Proptosis ................................................................................................ 337Subrahmanyam Mallajosyula, Mohd Javed AliNonspecific inflammations of the orbit (NSOIS) 337; Specific inflammations of the orbit 338; Orbitalcellulitis 338; Rhino-orbital mucormycosis 338; Chronic granulomatous infections 338; Parasiticinfestations 338; Tolosa- Hunt syndrome 339; Capillary hemangioma 339; Acute intraorbital hemorrhageand emphysema 340; lymphoprolifarative and other neoplastic lesions 340; Case illustrations 340
basm
ala
blog
(alw
ays o
rigin
al)
25. Management of Ophthalmic Tumors: Role of Chemotherapy and Radiation Therapy .. 344Vijay Anand P Reddy, Nitin More, Ramesh Murthy, Anirban Bhaduri, Santosh G HonavarIntroduction 344; Ionizing radiation 344; Radiation therapy delivery methods 344; External beam radiation(teletherapy) 344; Internal radiation therapy (brachy therapy) 345; Plaque radiotherapy 346; Principles ofanti-neoplastic therapy 347; Capillary hemangioma 348; Basal cell and squamous cell carcinoma 348;Tumors of lacrimal gland 348; Malignant conjunctival tumors 349; Intraocular lymphoma 349;Retinoblastoma 349; Choroidal melanomas 349; Chemoreduction regimen 350; Oculor metastasis 352;Rhabdomyosarcoma 352; Orbital lymphoma 352; Grave’s ophthalmopathy 353; Optic nerve glioma 353;Optic nerve meningioma 353; Sequelae of radiation therapy 353
26. Carotid-Cavernous Fistulae: Role of Interventional Radiologist .......................................... 356D Ravi Varma, D Radhika VarmaPathophysiology 357; Clinical features 357; When to suspect CCF 359; Radiological investigations 359;Management of CCF 360; Direct CCF 360; Indirect CCF 363; Prognosis 363
27. Ocular and Systemic Associations of Proptosis ......................................................................... 366Subrahmanyam Mallajosyula, Mohd Javed AliCapillary hemangiomas 366; Neurofibromatosis 366; Craniofacial dysostosis 367; Encephalocele 367;Wegener’s granulomatosis 367; Wyburn-Mason syndrome 367; Hurler’s syndrome 368; Nonspecificorbital inflammation syndrome 368; Sclerosing inflammation of the orbit 368; Osteoma 368; Orbitalhamartoma (tuberous sclerosis) 368; Hemangioblastom 368
Index ..................................................................................................................................................... 369
ContentsContentsContentsContentsContents xixxixxixxixxix
basm
ala
blog
(alw
ays o
rigin
al)

basm
ala
blog
(alw
ays o
rigin
al)
basm
ala
blog
(alw
ays o
rigin
al)

Mark J Lucarelli, Nancy Kim
Applied Anatomy of OrbitApplied Anatomy of OrbitApplied Anatomy of OrbitApplied Anatomy of OrbitApplied Anatomy of Orbit
Figure 1.1: An axial view of the orbits demonstrating the dimen-sions and relationships between associated structures
Fundamental to the understanding of orbitalpathology and its surgical management is a soundworking knowledge of the anatomy of the normalorbit in three dimensions. The goal of this chapter isto review the location of critical ocular adnexal,orbital and related craniofacial structures and theanatomic relationships between them.
OVERVIEW
The orbit is defined as the bony cavity containingthe globe, extraocular muscles, fat, nerves and bloodvessels. Although the orbit is often described aspyramidal in shape, the space is actually pear-shaped,with its largest horizontal and vertical diameterslying 1 cm past the orbital rim and adjacent to theequator of the globe. Average orbital volume isapproximately 25-30 cc, of which the globe occupiesapproximately 7 cc of space. The lateral walls areoriented about 90° to one another and run 40 to 45mm in length to the apex. The medial walls of eachorbit run parallel to each other and measure 45 to 50mm in length. The optical axes themselves are alsoparallel to the course of the medial walls, rather thanthe diverging central axes of the orbits. Therefore,each globe is tonically held in adduction by theextraocular muscles to maintain ocular alignment.These relationships and other important dimensionsof the orbit are illustrated in Figure 1.1.
Orbital Osteology
The orbital rim is roughly in the shape of a spiral,with its starting and end points at the anterior andposterior lacrimal crests.1 There are seven bones
which make up the four orbital walls: the frontal,sphenoid (greater and lesser wings), ethmoid,lacrimal, maxillary, palatine, and zygomatic bones(Figure 1.2).
The roof of the orbit is comprised of the frontalbone anteriorly, and the lesser wing of the sphenoidbone posteriorly (Figure 1.3). The overall thicknessof the roof is significantly greater than that of eitherthe medial wall or orbital floor and is therefore,relatively resistant to fracture. Within the lesser winglies the optic foramen, through which the optic nerveexits the orbit via the optic canal. In about 30% ofindividuals, just above the frontosphenoid suture,lies the meningeal foramen through which therecurrent meningeal artery (a branch of the externalcarotid system) passes to anastomose with thelacrimal artery (a branch of the internal carotidsystem). This communication provides an importantpotential source of collateral blood flow to the orbit
1C H A P T E R
basm
ala
blog
(alw
ays o
rigin
al)

44444 Surgical Atlas of Orbital DiseasesSurgical Atlas of Orbital DiseasesSurgical Atlas of Orbital DiseasesSurgical Atlas of Orbital DiseasesSurgical Atlas of Orbital Diseases
Figure 1.2: An anterior-posterior view into the left bony orbit
Figure 1.3: The left orbital roof
basm
ala
blog
(alw
ays o
rigin
al)

Applied Anatomy of OrbitApplied Anatomy of OrbitApplied Anatomy of OrbitApplied Anatomy of OrbitApplied Anatomy of Orbit 55555
should its primary supply via the internal carotidsystem become disrupted. When the meningealforamen is absent, the middle meningeal arterycourses directly via the superior orbital fissure.2
Other important bony landmarks include the lacrimalgland fossa in the temporal roof and the trochlearfossa anteromedially. Just superolateral to thetrochlear fossa and at the medial one-third junctionof the superior rim, lies the supraorbital notch whichgives passage to supraorbital artery, vein, and nerve.In some individuals, this point of egress is completelyenclosed and appears as the supraorbital foramen.3
The medial wall includes the ethmoid, maxillary,and lacrimal bones, as well as the lesser wing of thesphenoid (Figure 1.4). Within the bony suture lineseparating the frontal from the ethmoid bone, thereare two important apertures, the anterior andposterior ethmoidal foramina. These foramina arethe exit points for the anterior and posteriorethmoidal arteries and nerves, respectively. Theanterior ethmoidal foramen is typically locatedapproximately 24 mm posterior to the orbital rimand the posterior ethmoidal foramen liesapproximately 36 mm posterior to the rim. The opticforamen, in turn, is located approximately 6 mmposterior to the posterior ethmoidal foramen. Theseforamina help the surgeon delineate the fronto-ethmoidal suture which is an important surgicallandmark for the roof of the ethmoid sinus, or foveaethmoidalis. The orbital roof slopes downward as ittravels medially. Medial to the orbital space, justbeyond the frontoethmoidal suture line, the foveaethmoidalis continues in a downward plane and ends
sagittally just above the nasal cavity and below theanterior cranial fossa at the cribriform plate. Bonydissection of the medial wall above the suture lineexposes the dura of the frontal lobe.
The ethmoid portion of the medial wall, thelamina papyracea, is extremely thin and is thus proneto fracture with trauma and to easily transmitinfection from the ethmoid air cells into the orbit assubperiosteal abscesses. The medial wall thickensagain in the area of the inferior suture between theethmoid and maxillary bones. This maxilloethmoidstrut4 provides support to the inferomedial orbitalwall and often survives trauma which fractures themore superior aspects of the wall. At the anterioraspect of the medial wall is the lacrimal sac fossa,bounded by the anterior and posterior lacrimalcrests. The anterior and posterior limbs of the medialcanthal tendon insert on the anterior and posteriorlacrimal crests, respectively.
The floor of the orbit consists of the maxillary,zygomatic and palatine bones. The maxillary boneforms the bulk of the floor while the zygomatic bonecontributes anterolaterally and the palatine bonecontributes to the posterior floor. A major landmarkin this area is the infraorbital groove, whichoriginates approximately 25-30 mm posterior to theorbital rim. The groove deepens and becomes anenclosed canal as it travels anteriorly within the floorto open again on the face of the maxillary bone atthe infraorbital foramen on the maxillary face, 4-6mm from the rim in adults.5 This pathway containsthe infraorbital neurovascular bundle which is easilyinjured by floor fractures or inadvertent surgicaldissection. Just medial to the infraorbital groove isthe thinnest portion of the maxillary bone. Not onlydoes this render the posteromedial part of the floorparticularly susceptible to blowout fractures, but italso provides an area where bone can be removedwith relative ease for inferior orbital decompression.The thicker, maxilloethmoid strut lies in the medialfloor and provides support for the orbital soft tissuesand the globe.4, 6 In the anteromedial floor, the bonynasolacrimal duct travels from the base of thelacrimal fossa in an inferior and usually slightlyposterolateral direction through the maxillary bonein the lateral nasal wall to empty into the inferiormeatus of the nose. The vector of the nasolacrimalduct shows considerable variability.Figure 1.4: Medial wall of the right orbit
basm
ala
blog
(alw
ays o
rigin
al)

66666 Surgical Atlas of Orbital DiseasesSurgical Atlas of Orbital DiseasesSurgical Atlas of Orbital DiseasesSurgical Atlas of Orbital DiseasesSurgical Atlas of Orbital Diseases
Figure 1.5: Lateral wall of the right orbit Figure 1.6: The left orbital apex
The lateral wall contains the zygomatic bone andthe greater wing of the sphenoid which separatesthe posterolateral orbit from the middle cranial fossa.The posterior borders of the lateral wall are definedby the superior and inferior orbital fissures. Theboundary between the lateral wall and roof is formedby the frontosphenoid suture, which transmits therecurrent meningeal artery. The anterior part of thelateral wall is comprised of the zygoma. Importantlandmarks in this region include the lateral orbitaltubercle, or Whitnall’s tubercle, which is the insertionpoint of the posterior head of the lateral canthaltendon, the lateral horn of the levator aponeurosis,the check ligament of the lateral rectus muscle, andLockwood’s ligament. The tubercle can be found justinside the orbital rim and approximately 11 mmbelow the frontozygomatic suture.7 The supero-anterior zygoma also contains the zygomatico-temporal and zygomaticofacial canals through whichbranches of the lacrimal artery and the lacrimal andzygomatic nerves pass (Figure 1.5).
The Periorbita
The periorbita refers to the tough, fibromembranouslining of the bony orbit which acts as a physical barrierto infection and provides a scaffold to which otherintraorbital connective tissues can attach. The regionsof greatest adherence between this sheath and boneare at the orbital rim, suture lines, bony fissures,trochlear fossa and the lacrimal crests. At the orbitalmargins, at the arcus marginalis, the periorbitathickens and gives rise to the orbital septum. Deepin the orbit, the periorbita continue through the
superior orbital fissure and optic canal to becomecontinuous with the dura. The potential space outsidethe periorbita is an important surgical plane. Accessto the orbital walls in decompression surgery, forexample, entails dissection between the bone and thisoverlying periosteal sheet.
The Orbital Apex
The orbital apex merits special attention, as the regionin which many critical orbital structures convergeand communicate with other important, periorbitalspaces (Figure 1.6). Cranial nerves II through VI,major orbital vessels, and all of the extraocularmuscles excluding the inferior oblique sit in tightproximity within the apex, and pathology in thisregion can produce profound deficits in vision andocular motility.8, 9
The apex is defined by only three walls; the flooris absent in the far posterior orbit.1 Major bonylandmarks include the superior orbital fissure,inferior orbital fissure, and the optic canal. Thesuperior orbital fissure divides the sphenoid into thegreater (lateral) and lesser (medial) wings and liesinferiorly and laterally to the optic foramen. Thisfissure measures approximately 20-22 mm in overalllength and is separated into superolateral andinferomedial sections by the tendon of the lateralrectus muscle. The superotemporal part of the fissurelies above the annulus of Zinn, the fibrous ringformed by the common origin of the rectus muscles.The lacrimal, frontal and trochlear nerves, and thesuperior ophthalmic vein pass through this region asthey traverse the apex. The inferomedial segment of
basm
ala
blog
(alw
ays o
rigin
al)

Applied Anatomy of OrbitApplied Anatomy of OrbitApplied Anatomy of OrbitApplied Anatomy of OrbitApplied Anatomy of Orbit 77777
the superior orbital fissure, also called the oculomotorforamen, is located inside the annulus and transmitsthe superior and inferior divisions of the oculomotornerve, the abducens nerve, sympathetic fibers, andthe nasociliary nerve, a terminal sensory branch ofthe ophthalmic division of the trigeminal nerve10-12
(Figure 1.7).The inferior orbital fissure bounds the greater
wing of the sphenoid, separating it from themaxillary bone inferomedially. This fissurecommunicates primarily with the pterygopalatinefossa (Figure 1.8). The maxillary branch of thetrigeminal nerve passes through the pterygopalatinefossa and subdivides into the infraorbital nervewhich, in turn, travels anteriorly into the orbit viathe infraorbital groove. The zygomatic nerve, anotherbranch of the maxillary branch of cranial nerve V,enters the orbit through the inferior orbital fissureto provide sensory innervation to lateral orbit andcheek after passing through the zygomaticofacialforamen. Also within the pterygopalatine fossa islocated the maxillary artery which gives rise to theinfraorbital artery, part of the neurovascular bundletraveling through the infraorbital groove. Para-sympathetic fibers originating from the pterygo-
palatine ganglion and terminating in the lacrimalgland are transmitted by the inferior orbital fissureas well.2 The inferior ophthalmic veins also pass fromthe orbit into the pterygoid plexus via the inferiororbital fissure.
The optic canal penetrates the superomedialorbital apex through the lesser wing of the sphenoidbone as the optic foramen. The canal is approximately6 mm in diameter and 8-10 mm in length and housesthe optic nerve and the ophthalmic artery. The canalruns along the upper, lateral wall of the anteriorsphenoid sinus and in the floor of the anterior cranialfossa.
Figure 1.7: The superior and inferior orbital fissures and associated apex structures of the right eye
Figure 1.8: Lateral cross-section of the orbit
basm
ala
blog
(alw
ays o
rigin
al)

88888 Surgical Atlas of Orbital DiseasesSurgical Atlas of Orbital DiseasesSurgical Atlas of Orbital DiseasesSurgical Atlas of Orbital DiseasesSurgical Atlas of Orbital Diseases
The Cavernous Sinus
The cavernous sinus is a large venous sinusposterior to the orbital apex contained within a duralcleft which is situated lateral to the sphenoid sinus(Figure 1.9). Its tributaries consist of the ophthalmic,cerebral middle meningeal, and pterygoid veins. Theleft and right cavernous sinuses communicate withone another via small channels which run superiorto the roof of the sphenoid sinus. Several criticalstructures pass through the cavernous sinus as theytravel into the orbit. The carotid siphon and thesympathetics which ride along on its sheath traversecentrally. In the lateral wall of the cavernous sinusarea embedded the oculomotor nerve, trochlearnerve, the ophthalmic and maxillary divisions of thetrigeminal nerve, and the abducens nerve. The opticnerves course superomedially to the cavernous sinus.The optic chiasm is formed just above the anterioraspect of the cavernous sinus.
As in the orbital apex, pathological processesinvolving the cavernous sinus such as the formationof carotid-cavernous fistulas, inflammation orinfection typically cause multiple cranial neuropathiesaffecting the eye.13 Further, because the right andleft cavernous sinuses are interconnected, diseaseprocesses extending posteriorly from the orbit onone side can spread to the other via these spaces.
The Globe
The average-size globe measures approximately23.5 mm in the horizontal meridian and 23 mm
vertically, with an anterior-posterior dimension ofabout 24 mm. Its overall volume is about 7cc. Theglobe is surrounded by a loose fascial sheath, orTenon’s capsule, which is interconnected to the scleraby fine fibrous bands. The potential space betweenthese layers is the episcleral space, and the areas ofgreatest adherence between them are approximately1.5 mm from the limbus anteriorly, and posteriorly,at the optic nerve sheath. Tenon’s capsule issuspended inside the orbit by interconnections withfine connective tissue septae within the surroundingorbital fat. This sheath must be traversed by thenerves and blood vessels which supply the globe.Likewise, the extraocular muscles must penetrateTenon’s layer to attach to the globe. As the musclespass from outside to inside the episcleral space tofuse with the sclera, Tenon’s capsule makesattachments with the intermuscular septum, a fibrousnetwork which encases and interconnects theextraocular muscles (Figure 1.10).14-18 Thus, followingenucleation, orbital implants that are placed withinTenon’s capsule may demonstrate a fair amount ofmotility even if they are not sutured to the extraocularmuscles themselves.18 The intermuscular septum andrectus muscles delineate the intraconal versusextraconal space.
Interconnections between the extraocular musclesheaths and the periorbita comprise the checkligaments. Superiorly, the check ligaments consist ofthe fascial complex surrounding the upper lidretractors, the superior rectus and levator palpebraemuscles.19 Similarly, the inferior check ligamentconsists of the muscle sheaths surrounding the lowerlid retractors, the inferior rectus and inferior oblique.
Figure 1.9: A cross-section of the cavernous sinus Figure 1.10: The extraocular muscles and intermuscular fascia
basm
ala
blog
(alw
ays o
rigin
al)

Applied Anatomy of OrbitApplied Anatomy of OrbitApplied Anatomy of OrbitApplied Anatomy of OrbitApplied Anatomy of Orbit 99999
Medially, the muscle sheath of the medial rectusinserts just inside the posterior lacrimal crest, to themedial orbital septum and caruncle to collectivelyform the medial check ligament. The analogous checkligament of the lateral rectus inserts onto the lateralorbital tubercle of Whitnall.7
The Extraocular Muscles
The four rectus muscles originate at the annulus ofZinn, within the orbital apex. Specifically, the superiorand medial recti originate adjacent to the lesser wingof the sphenoid, next to the optic canal. The inferiorrectus originates from a portion of the annulus whichextends from the body of the sphenoid bone to itsgreat wing. The lateral rectus has a bifid origin froma tendinous segment of the annulus which extendsacross the superior orbital fissure from the greaterto the lesser sphenoid wing and a more inferiorportion which extends directly from the greater wingitself.
The superior rectus lies just underneath thelevator palpebrae. Immediately beneath and medialto the superior rectus run the nasociliary nerve andophthalmic artery. The superior edge of the medialrectus travels just under these structures. From itsorigin at the annulus, the inferior rectus closelyfollows the floor of the orbit until reaching theanterior orbit, where it becomes separated from thefloor by the inferior oblique muscle as the lattercrosses from the medial to the lateral wall, and byfat. Medial and superior to the lateral rectus, is foundthe ciliary ganglion which is usually adherent to theintraorbital segment of the optic nerve.
The superior oblique muscle also begins alongthe annulus of Zinn, superomedially and extendsforward superiorly and along the junction betweenthe orbital roof and the medial orbital wall. As itcourses toward the anterior orbit, the muscle bellytransitions to a tendinous segment as it reaches thetrochlea, a pulley-like cartilaginous structure whichlies approximately 6-10 mm posterior to thesuperomedial orbital rim.20, 21 From this point, thetendon passes posterolaterally, making a 54° angle,to attach to the globe. It is this course which givesrise to the main actions of the superior oblique,namely intortion and depression of the globe withcontraction. During orbital surgery, caution to avoidinjuring the trochlea must be taken to avoid
subsequent scarring and restriction of superioroblique muscle action, or Brown’s syndrome.22
The inferior oblique, unlike the other extraocularmuscles, does not originate at the annulus, but fromthe periosteum of the anterior, inferomedial orbiton the maxillary bone. It courses posterolaterally,just beneath the inferior rectus to insert on theinferolateral globe, which gives rise to its mainactions: extortion and elevation of the globe. Thecapsulopalpebral fascia and Lockwood’s ligamentinterdigitate with the muscular fascia of the inferioroblique.
The extraocular muscles approximate a spiral inthe distance between their individual insertions andthe corneal limbus, the so-called spiral of Tillaux(Figure 1.11). Beginning with the medial rectus, eachsuccessive muscle inserts farther from the limbus.Although there is individual variation, the averagedistances are: medial rectus, 5.5 mm; inferior rectus,6.5 mm, lateral rectus, 6.9 mm, and superior rectus,7.7 mm.23
Innervation to the extraocular muscles is largelycarried by the oculomotor nerve (third cranial nerve),which supplies the medial, inferior, and superiorrectus muscles, the inferior oblique, as well as thelevator palpebrae superioris. The superior obliqueand lateral rectus receive innervation from the
Figure 1.11: Spiral of Tillaux
basm
ala
blog
(alw
ays o
rigin
al)

1010101010 Surgical Atlas of Orbital DiseasesSurgical Atlas of Orbital DiseasesSurgical Atlas of Orbital DiseasesSurgical Atlas of Orbital DiseasesSurgical Atlas of Orbital Diseases
trochlear nerve (fourth cranial nerve) and theabducens nerve (sixth cranial nerve), respectively.The blood supply to the muscles is carried bymuscular branches of the ophthalmic artery.
Lids
Understanding the general anatomy and dimensionsof the major eyelid landmarks is important in theevaluation of structural disease of the lids and inplanning surgical repair. The normal interpalpebralfissure height is 10-12 mm and the average length is28-30 mm. The distance between the upper lid creaseand lid margin measures approximately 8-11 mm atthe pupillary axis. The highest point of the upper lidcontour rests just nasal to the center of the pupil andthe upper lid margin is typically located 1-2 mm belowthe superior limbus in adults. The lateral canthalangle sits approximately 2 mm higher than the medialcanthus.
Both the upper and lower eyelids can be dividedinto the skin, orbicularis, orbital septum, orbital fat,lid retractors, tarsus, and conjunctiva. For descriptivepurposes, the layers can be grouped into the anterior
and posterior lamellae. The anterior lamella containslid structures which lie outside the orbit per se, and iscomprised of the skin and the orbicularis oculi(Figure 1.12).
The skin of the lids is the thinnest of the bodyand unlike skin elsewhere, has no subcutaneous fatlayer. The portion which lies anterior to tarsus isrelatively firmly attached to deeper structures whilethe preseptal portions are loosely connected. Anteriorto the margin, the skin contains the lash follicles withtheir associated sebaceous glands of Zeis and apocrineglands of Moll, as well diffusely distributed eccrinesweat glands.
The orbicularis muscle is a C-shaped complexof muscle fibers which functions to close the lids(Figure 1.13). It is divided into pretarsal, preseptaland orbital sections, all of which receive innervationfrom the facial nerve (seventh cranial nerve). Thepretarsal and preseptal parts of orbicularis areprimarily involved in involuntary closure of the lids,as elicited by the blink reflex. These fibers insert atthe medial canthal tendon as deep and superficialheads. A subset of pretarsal orbicularis fibers, alsocalled Horner’s muscle, inserts deep at the posteriorlacrimal crest as the deep limb of the medial canthal
Figure 1.12: A cross-section of the upper and lower lids Figure 1.13: The orbicularis oculi
basm
ala
blog
(alw
ays o
rigin
al)

Applied Anatomy of OrbitApplied Anatomy of OrbitApplied Anatomy of OrbitApplied Anatomy of OrbitApplied Anatomy of Orbit 1111111111
tendon, along the posterior aspect of the lacrimalsac and surround the canaliculi. These fibers arethought to provide a pumping action as they contractwhich facilitates tear drainage.24, 25 Horner’s muscleis also critical in maintaining close contact betweenthe posterior aspect of the lid and the globe. Theremaining pretarsal orbicularis inserts superficiallywithin the anterior limb of the medial canthal tendon.Laterally, slips from the upper and lower lid pretarsalorbicularis insert onto the lateral canthal tendonwhich in turn, inserts on the lateral orbital tubercle.Medially, the deep head of the preseptal orbicularisinserts into the fascia surrounding the lacrimal sacwhile the superficial head inserts onto the anteriorlimb of the medial canthal tendon.
The orbital orbicularis is chiefly responsible forforced lid closure, such as winking or in blep-harospasm. Medially, its insertions lie along theorbital rim and anterior medial canthal tendon. Asthey course laterally, these fibers overlie the zygomaand the elevators of the lateral mouth, thezygomaticus major and minor.
Underlying the pretarsal orbicularis and restinganterior to the tarsus is the muscle of Riolan whichconsists of small, horizontally oriented slips of muscle.These fibers appear grossly as the “gray line” of thelid margin which is posterior to the lash line andfunction to turn the lashes toward the eye duringblinking. The “gray line” is a useful landmark inaligning the wound edges in marginal lid lacerationrepair.
The septum, orbital fat and posterior lamella,which consists of the retractors, tarsus and con-junctiva, are considered to be intraorbital structures.The septum is comprised of tough fibrous connectivetissue arranged in sheets which originate from theperiosteum of the orbital rims at the arcus marginalis.This structure acts as an relative barrier between theorbit and lid in limiting the deep spread of superficialhemorrhage and infection. In the upper lid, theseptum fuses with the aponeurosis of the levatormuscle, the primary upper lid retractor muscle,approximately 2-5 mm above the superior tarsaledge.26 In the lower lid, the septum condenseswith the capsulopalpebral fascia as the two layersconverge toward the inferior edge of the lower tarsalplate.27
The orbital septum lies anterior to thepreaponeurotic orbital fat pads, which prolapseforward with any violation of the septum. As anatural consequence of aging, as the septum thinsand stretches, these fat pads tend to graduallyherniate anteriorly. In the upper lid, there are twodistinct fat pads, the medial and central fat pads.The medial pad can be distinguished by its relativelywhite color. The medial palpebral artery typicallyruns within this pocket and care should be taken toavoid inadvertent laceration or cauterization duringsurgery. Laterally, there is usually little fat in theupper lid. Instead, this space is usually filled by orbitallobe of the lacrimal gland.
The lower lids contain medial, central and lateralfat pads. The medial pad lies just medial to the inferioroblique and as in the upper lid, has a characteristicallywhite color and contains the lower palpebral artery.The central fat pad lies between the inferior obliquemuscle and a fascial band that separates it from thelateral fat pad. The latter extends to the inferior edgeof the lacrimal gland.28
The upper lid retractors consist of the levatormuscle which is innervated by cranial nerve III, andthe sympathetically innervated Müller’s muscle. Thelevator, which is the primary retractor, originatesfrom a point just above the annulus of Zinn, fromthe lesser wing of the sphenoid bone. The levatorcomplex includes a muscular component which isapproximately 40 mm long extending from its originon the lesser sphenoid wing just outside the annulusof Zinn, and the fibrous levator aponeurosis whichis 14-20 mm in length. As the muscular portioncourses forward in the orbit, it rides just above thesuperior rectus muscle and the two are inter-connected by interdigitated fibrous bands. As theyreach the equator of the globe, the levator broadensand transitions into its aponeurotic component.Medially and centrally, the aponeurosis inserts ontothe anterior tarsal surface and passes through theorbicularis to insert onto pretarsal skin. Theseinsertions create the upper lid crease. Medially, theaponeurosis separates into a single medial horn whichinserts into the posterior lacrimal crest and becomescontinuous with the medial canthal tendon complex.Similarly, the aponeurosis courses into a lateral hornwhich inserts into the lateral orbital tubercle, also
basm
ala
blog
(alw
ays o
rigin
al)

1212121212 Surgical Atlas of Orbital DiseasesSurgical Atlas of Orbital DiseasesSurgical Atlas of Orbital DiseasesSurgical Atlas of Orbital DiseasesSurgical Atlas of Orbital Diseases
called Whitnall’s tubercle, and becomes continuouswith the lateral canthal tendon complex (Figure 1.14).
The normal magnitude of upper lid elevation isapproximately 14-16 mm. Elevation of less than10-12 mm is usually abnormal. Elevation of less than5 mm is considered severe dysfunction and hasimportant implications in ptosis surgery. Because ofthe close apposition and fibrous interconnectionsbetween the levator and the superior rectus muscle,when the globe is elevated, the upper lid follows.This relationship is not passive, and the levator andsuperior rectus actually co-contract. Likewise, whenthe globe is depressed, both muscles relax togetherand the upper lid moves downward.29
At the transitional zone between the anteriormuscular component of the levator and itsaponeurosis is a fascial sleeve called Whitnall’sligament, or the superior transverse ligament. Thisband runs both over and beneath the levator at thispoint and behaves as a fulcrum point for the levatorwhere contraction of the muscular portion in thehorizontal plane becomes directed in the verticaldirection.30-32 However, Whitnall’s ligament is not astationary fulcrum,29 rather, it acts more as a swingingsuspender of the levator.31 Whitnall’s ligament alsoprovides mechanical support for the superior orbitalsoft tissues. Medially, this structure inserts withinthe fascial tissue surrounding the superior obliquetendon and the trochlea. Laterally, the ligamentinserts within the inner surface of the lateral wallinto the periorbita of the lacrimal gland fossa,approximately 10 mm above the lateral orbital
tubercle, or Whitnall’s tubercle. (Note that despitethe shared eponym, Whitnall’s ligament does notdirectly insert into Whitnall’s tubercle). Prior to itslateral insertion, the ligament courses across anddivides the lacrimal gland into a superior orbital lobeand an inferior palpebral lobe.30 (Figure 1.15).
Müller’s muscle is a secondary upper lid retractor,providing approximately 1-2 mm of elevation.It originates just deep to the levator aponeurosis atthe level of Whitnall’s ligament and is about 12-14mm in length. Muller’s muscle inserts at the superioredge of the tarsal plate. An important landmark for
Figure 1.14: The levator superioris complex,including Whitnall's ligament
Figure 1.15: The lacrimal gland and its relation to the levator superioris complex
basm
ala
blog
(alw
ays o
rigin
al)

Applied Anatomy of OrbitApplied Anatomy of OrbitApplied Anatomy of OrbitApplied Anatomy of OrbitApplied Anatomy of Orbit 1313131313
this structure is the peripheral vascular arcade whichlies between the levator aponeurosis and Müller’smuscle just above the tarsus. Injury to Müller’s orloss of sympathetic innervation, as occurs inHorner’s syndrome, causes a characteristic mild(1-2 mm) ptosis.33
In the lower lid, the retractor complex is calledthe capsulopalpebral fascia. This structure is acondensation of fibrous attachments to terminalmuscle slips from the inferior rectus which courseanteriorly to surround the inferior oblique muscleand fuse with its sheath. From this point, an importantcomponent of this fascial complex forms Lockwood’sligament, which extends across the width of theinferior orbit somewhat like a hammock, insertinglaterally at the lateral orbital tubercle and mediallyinto the medial canthal tendon and providing somesuspensory support to the orbital soft tissues.34
Anterior to Lockwood’s ligament, the capsulo-palpebral fascia send fibers into the inferiorconjunctival fornix (thus forming the suspensoryligament of the inferior fornix), while additionalfibers continue on to fuse with the septum and tofinally insert into the inferior border of the tarsalplate. As in the upper lid, the lower lid retractorswork in tandem with the inferior rectus to lower thelid with downgaze.
The analogous lower lid structure to Müller’smuscle in the upper lid is the inferior tarsal muscle.Loss of sympathetic innervation may cause a smallamount of “reverse ptosis” of the lower lid, elevatingthe inferior lid margin by approximately 1 mm aboveits usual resting position.33
The tarsal plates are comprised of denseconnective tissue that act at the structural skeletonof the lids. In both lids, the tarsi are 1 mm inthickness. In the upper lid, the tarsus is approximately10-12 mm in height at the pupillary axis, while thevertical extent of the lower tarsus is 4 mm. The tarsicontain the oil-producing meibomian glands whichopen on the margin, just posterior to the lash line. Inthe upper lid, approximately 2-3 mm from the tarsalmargin, lies the marginal arterial arcade. In the lowerlid this arcade typically lies within 1 mm of the lashes.Distichiasis is the abnormal growth of lashes fromthe meibomian gland orifices and may occur as acongenital anomaly or as an acquired state. In the
latter case, distichiasis is often a result of severechronic inflammation of the lids35.
At their medial and lateral borders, the tarsitaper. The upper and lower tarsi come together atthe canthus to form the deep lateral canthal tendon,which inserts just anterior to the lateral orbitaltubercle. Recall that the more superficial componentsof the lateral canthal tendon extend from the lateralpretarsal and preseptal orbicularis oculi muscles.Similarly, the medial aspects of the upper and lowertarsi contribute to the medial canthal tendon, withlarger, more superficial components which arise fromthe orbicularis oculi.
The conjunctiva comprises the most posteriorlayer of the lids. Basal tear flow is provided by theaccessory lacrimal glands of Krause in the upperconjunctival fornix, and the glands of Wolfring inthe lower fornix. Additional mucin-producing glandsare distributed within both the orbital and palpebralconjunctivae.
The Lacrimal System
The main lacrimal gland lies in the anterolateralorbital roof, within the lacrimal gland fossa of thefrontal bone, and measures roughly 20 × 12 × 5 mm.The gland is separated into a palpebral and an orbitallobe by the lateral levator aponeurosis. The primarysuspensory support for the main lacrimal gland comesfrom the Whitnall’s ligament.1 Damage to theligament leads to forward and downward prolapseof the gland in the orbit.36 Ducts from both lobespass through the palpebral lobe to empty into thesuperolateral fornix. Therefore, ideally, lacrimalgland biopsies should not be performed on thepalpebral lobe, since injury here may affect drainagefrom both lobes37 (Figure 1.15).
Innervation and blood supply are provided bythe lacrimal nerve and lacrimal artery, which enterthe gland posteriorly. Venous drainage occurs viathe lacrimal vein, which empties into the superiorophthalmic vein. Parasympathetic inputs originatefrom the lacrimal nucleus of the pons. Thesepreganglionic fibers pass through the geniculateganglion and then travel with the greater petrosalnerve to synapse eventually within the pterygo-palatine ganglion. These fibers then directly synapsein the lacrimal gland.38, 39 Additional postganglionic
basm
ala
blog
(alw
ays o
rigin
al)

1414141414 Surgical Atlas of Orbital DiseasesSurgical Atlas of Orbital DiseasesSurgical Atlas of Orbital DiseasesSurgical Atlas of Orbital DiseasesSurgical Atlas of Orbital Diseases
fibers traveling along branches of the maxillarydivision of the trigeminal nerve that converge withthe lacrimal nerve to enter the orbit also innervatethe lacrimal gland.40
Tears drain medially via the upper and lower lidpuncta, into the canaliculi, and into the lacrimal sac(Figure 1.16). The puncta are approximately0.3 mm in diameter. The initial segment of eachcanaliculus extends 2 mm perpendicular to the lidmargin then turns roughly 90° medially toward thecanthus. These horizontal canalicular segments areapproximately 8 mm in length. The lower canaliculusis typically slightly longer than its upper lidcounterpart. In 90% of individuals, the upper andlower canaliculi then fuse to form a 2 mm longcommon canaliculus which lies between the anteriorand posterior limbs of the medial canthal tendon andenters the lacrimal sac.41 The valve of Rosenmüller islocated at this junction and prevents the reflux oftears from the sac retrograde into the canaliculi. Thelengths of each component of the lacrimal drainagesystem become important when performing probingand irrigation to evaluate the patency of the outflowsystem.
The lacrimal sac sits within the lacrimal sac fossa.It is 12 mm long and its fundus lies 3-4 mm superiorto the valve of Rosenmüller.42 The sac lies just anteriorto the middle turbinate of the nose. The inferior sacis contiguous with the nasolacrimal duct whichcourses in the wall of the lateral nose and emptiesvia the valve of Hasner just below the inferiorturbinate. The valve of Hasner may be imperforatein young infants, and is the most common site ofnasolacrimal duct obstruction in this age group.
The Nerves of the Orbit
The optic nerve: The optic nerve (the second cranialnerve) is actually part of the central nervous system,extending directly from the brain into the orbit. Likethe rest of the central nervous system, the optic nerveis invested within a dural sheath and leptomeninges,surrounded by cerebrospinal fluid, and in part, iscovered with myelin. The fact that cerebrospinal fluidsurrounding the optic nerve communicates with thefluid surrounding the cerebrum and brainstem is thebasis for the seizures and life-threateningcardiopulmonary depression which can occur with
inadvertent perforation of the optic nerve sheathduring retrobulbar anesthesia.43
There are four major segments to the optic nerve,including the intracranial, intracanalicular, intra-orbital and the intraocular segments. Theintracanalicular segment of the optic nerve is tightlysurrounded by its dural sheath and tethered withinthe bone. Because of this, the intracanalicular segmentof the optic nerve is particularly susceptible to blunttrauma.44, 45 Once it passes through the optic foramen,the length of the intraorbital portion of the nerve isroughly 24-30 mm as it traverses the 20 mm or sodistance to the globe. Thus, the nerve has a slightlyserpentine course inside the orbit that allows formovement of the globe and some degree of proptosis.However, severe proptosis puts the nerve on stretch,described radiographically as “globe tenting”.46
The intraocular length of the nerve is approximately1 mm.
Sensory innervation of the orbit: Sensory innervationof the periorbital region is carried by the ophthalmicand maxillary divisions of the trigeminal nerve (fifthcranial nerve). Both branch from the trigeminalganglion which is located within the lateral wall ofthe cavernous sinus.
The ophthalmic branch further subdivides intothree segments: the frontal, lacrimal and nasociliarynerves. The frontal and lacrimal branches enter the
Figure 1.16: The lacrimal drainage system
basm
ala
blog
(alw
ays o
rigin
al)

Applied Anatomy of OrbitApplied Anatomy of OrbitApplied Anatomy of OrbitApplied Anatomy of OrbitApplied Anatomy of Orbit 1515151515
Figure 1.17: Lateral view of the orbit and major orbital sensory nerves
orbit in the superolateral part of the superior orbitalfissure, outside the annulus of Zinn. The frontal nervecourses through the extraconal fat and separates inthe anterior orbit into several smaller branchesincluding the supraorbital branch which supplies thescalp, forehead, upper lid, and conjunctiva. Thesupraorbital nerve exits via the supraorbital notchor foramen and should be carefully avoided duringdissection of the superior orbital rim. Injury to thedeep, lateral branches of the supraorbital nerve whichrun beneath the frontalis muscle, as can occur duringforehead lift surgery leads to scalp numbness to thevertex.47 The other major division of the frontalnerve, the supratrochlear nerve, exits just above thetrochlea to innervate parts of the lower forehead andmedial canthal region. The lacrimal nerve travels withthe lacrimal artery superolaterally in the extraconalspace, along the superior border of the lateral rectus(Figure 1.17). As it travels forward, it is joined byparasympathetic motor fibers within the orbit whichbegan within the nervus intermedius and which
supply the lacrimal gland, superolateral lid andconjunctiva.37
The nasociliary nerve enters the orbit via thesuperior orbital fissure within the annulus of Zinn,traversing just under the superior rectus muscle andover the optic nerve medially as it courses forwardin the orbit in association with the ophthalmic artery.In the posterior orbit, it subdivides into longposterior ciliary nerves which run medially andlaterally toward the globe, giving off sensory fiberswhich travel through the ciliary ganglion withoutsynapsing. The long ciliary nerves enter the scleraand continue forward, innervating the iris, corneaand ciliary muscles. Additional fibers from thenasociliary nerve travel superomedially and areresponsible for sensation from the nasal mucosa andthe skin on the medial tip of the nose via the anteriorethmoidal nerve. It is this branch which is responsiblefor Hutchinson’s sign in cases of herpes zosterophthalmicus. The final anterior branch of thenasociliary nerve is the infratrochlear nerve, which
basm
ala
blog
(alw
ays o
rigin
al)

1616161616 Surgical Atlas of Orbital DiseasesSurgical Atlas of Orbital DiseasesSurgical Atlas of Orbital DiseasesSurgical Atlas of Orbital DiseasesSurgical Atlas of Orbital Diseases
traverses the orbital septum inferior to the trochleato supply the medial eyelid skin, lacrimal sac andthe caruncle.
The maxillary division of the trigeminal nerveexits the middle cranial fossa via the foramenrotundum to enter the pterygopalatine fossa. Fromhere, the zygomatic branch enters the inferior orbitvia the inferior orbital fissure. It further subdividesinto the infraorbital, zygomaticotemporal, andzygomaticofacial nerves. The infraorbital nerve exitsthe orbit via the infraorbital notch or groove to supplythe skin of the lower lid, cheek and medial upper lip(Figure 1.2). Injury to this nerve by fracturesinvolving the orbital floor result in hypesthesia overthese areas. The zygomaticotemporal and zygo-maticofacial nerves provide sensory innervation tothe lateral brow and lateral cheek, respectively.
Motor innervation of the orbit: Motor innervationto the orbit involves the oculomotor, trochlear andabducens nerves, or the third, fourth and sixth cranialnerves, respectively. The oculomotor nerve exits thebrainstem medially, leaving its dural sheath to enterthe superolateral aspect of the cavernous sinus. Here,it divides into superior and inferior divisions whichboth pass into the orbit through the superior orbitalfissure, within the annulus of Zinn. The superiordivision sends branches to the levator muscle andsuperior rectus while the inferior division branchesinto three parts to supply the medial rectus, inferiorrectus and inferior oblique. The branch whichinnervates the inferior oblique also carries para-sympathetic fibers which synapse in the ciliaryganglion. Thus, injury due to surgery or trauma tothese inferior orbital structures can lead to an efferentpupillary defect and dilation.48
The trochlear nerve, the smallest and longest ofthe cranial nerves, arises from the dorsal midbrain,crosses the midline to emerge adjacent to the superiorcerebellar peduncle. It enters the cavernous sinusalong its lateral wall, reaching the orbit via thesuperior orbital fissure, above the annulus (along withthe frontal and lacrimal nerves). It travelsanteromedially above the levator just inferior to theperiorbita, and enters the superior oblique at themuscle belly’s posterior third. The trochlear nerve isunique among the cranial nerves. It is the only cranialnerve innervating an extraocular muscle which doesnot penetrate the intraconal surface of the muscle it
serves. It is also the smallest cranial nerve, has thelongest intracranial component, and is the onlycranial nerve to exit dorsally from the brainstem.For these reasons, it is also the most prone to injurywith closed head trauma.49
The abducens nerve originates from the pons andenters the cavernous sinus, initially following acourse within the sinus near the internal carotidartery before coursing laterally along the wall. Itpasses into the orbit via the intra-annular portion ofthe superior orbital fissure, running along the innersurface of the lateral rectus and piercing the musclebelly at its posterior one-third. The intracranialcourse of the abducens nerve turns sharply as itcrosses the petrosphenoidal ligament, making itparticularly prone to injury50, 51 with acute increases50
or decreases52 in intracranial pressure.Sympathetic innervation of the orbit: Sympathetics
to the orbit which supply the iris dilator, eyelidmuscle, eccrine sweat glands, and blood vesselsoriginate from the superior cervical ganglion. Thesefibers travel along the internal carotid artery, throughthe cavernous sinus and into the orbit along theophthalmic artery, via the superior orbital fissure.The sympathetics pass through the ciliary ganglion(located lateral to the optic nerve at the apex) withoutsynapsing.12
Parasympathetic innervation of the orbit: Para-sympathetics innervate the iris sphincter muscle,ciliary muscle, lacrimal gland and orbital bloodvessels to produce miosis, lacrimation and relaxationof vascular tone. These inputs originate in theEdinger-Westphal nucleus (third cranial nerve), thesalivatory nucleus via the nervus intermedius10
(the parasympathetic nerve fibers originating fromthe facial nerve), and the parasympathetic gangliasupporting the orbit. Preganglionic parasympatheticscourse with the oculomotor nerve, along its inferiordivision, and enter the orbit via the inferior orbitalfissure. These fibers run superficially in theoculomotor nerve as it exits the brainstem adjacentto the posterior communicating artery. Thus,aneurysms of the posterior communicating arterymay produce a third nerve palsy with an associateddilated pupil. These nerves synapse in the ciliaryganglion and enter the globe as the short posteriorciliary nerves.
basm
ala
blog
(alw
ays o
rigin
al)

Applied Anatomy of OrbitApplied Anatomy of OrbitApplied Anatomy of OrbitApplied Anatomy of OrbitApplied Anatomy of Orbit 1717171717
Figure 1.18: Lateral view of the orbit and major branches of the ophthalmic artery
The ciliary ganglion lies adjacent to the lateralaspect optic nerve at the orbital apex. The ganglionalso contains sympathetics that travel into the orbitvia the ophthalmic artery to reach the iris dilatorand ocular blood vessels, as well as sensory fibersfrom the nasociliary nerve which supply intraocularstructures. Neither the sympathetics nor the sensoryfibers synapse within the ganglion.
Preganglionic fibers from the facial nerve nucleuspass through the geniculate ganglion and then travelwith the greater petrosal nerve to eventually synapsewithin the pterygopalatine ganglion. These fiberscourse via the infraorbital fissure to the orbit anddirectly to the lacrimal gland.37, 38 Additionalpostganglionic fibers travel along branches of themaxillary division of the trigeminal nerve thatconverge with the lacrimal nerve to enter the orbit.
Vascular Anatomy of the Orbit: Arterial SupplyThe ophthalmic artery, the first intracranial branchfrom the internal carotid artery, provides most ofthe blood supply to the orbit and globe. Theophthalmic artery arises just as its parent vessel exitsthe cavernous sinus, just inferior to the optic nerveand posterior to the anterior clinoid process. Itimmediately joins the optic nerve along itsinferolateral surface, traveling within a commondural sheath, and entering the apex via the opticforamen.53, 54 Once inside the orbit, the artery crossesmedially and gives off its major apical branches(Figure 1.18).
The major intraconal vessels include the centralretinal artery, branches to the extraocular muscles,and the long and short posterior ciliary arteries. Thefirst branch of the ophthalmic artery is the central
basm
ala
blog
(alw
ays o
rigin
al)

1818181818 Surgical Atlas of Orbital DiseasesSurgical Atlas of Orbital DiseasesSurgical Atlas of Orbital DiseasesSurgical Atlas of Orbital DiseasesSurgical Atlas of Orbital Diseases
retinal artery. This vessel typically pierces the nerveinferomedially, at a point approximately 10 mm fromthe globe, and as it reaches the globe, gives off theend arteries to the retina. Branches to the extraocularmuscles show greater individual variation indistribution. Generally, these vessels run within themuscle belly or along their medial surfaces. As theycontinue to travel anteriorly with the muscles, theterminal branches of these arteries enter the globeat the tendinous muscle insertions, becoming theanterior ciliary arteries. These branches provideanastomoses with the long posterior ciliary arteriesto supply the iris, ciliary muscle and other anteriorintraocular structures. Because of this contributionof the muscular arteries to the anterior segment,disinserting more than two extraocular muscles fromthe globe during surgery at one time is generallyavoided.
Typically, there are two or three posterior ciliaryarteries which branch from the ophthalmic artery nearthe apex and run medially and laterally within theorbit. Some of these vessels divide into 15-20 shortposterior ciliary arteries which enter the posterioraspect of the sclera to supply the choroid and theoptic nerve head. Others, the two long posteriorciliary arteries, continue to travel anteriorly withinthe sclera, entering the globe medially and laterallyto supply the anterior segment and anastomosingwith terminal branches of the muscular arteries.
The major extraconal, apical branches of theophthalmic artery include the lacrimal and posteriorethmoidal arteries. The lacrimal artery, along withthe lacrimal nerve, runs above the superior borderof the lateral rectus to reach the lacrimal gland andlateral upper lid. It anastomoses with the middlemeningeal artery via the recurrent meningeal artery,and the temporal arteries. The posterior ethmoidalcourses medially, along the frontoethmoidal sutureto exit via the posterior ethmoid foramen where itgives off branches supplying the sinus and nasalmucosa and the frontal dura.54, 55
As the ophthalmic artery continues forward inthe orbit, it then gives rise to the anterior ethmoidalartery and finally, its terminal branches. The anteriorethmoidal vessel exits via the anterior ethmoidalforamen to supply frontal dura and ethmoid andfrontal sinus mucosa. Anastomoses from thiscirculation and branches of the external carotid
provide blood flow to the nose and septum. Thefrontoethmoidal suture, along which the anterior andposterior ethmoidal arteries and associated branchesof the nasociliary nerve run, is an important landmarkfor the roof of the ethmoid, or fovea ethmoidaliswhich lies just beyond this line. Penetration of themedial wall above this suture would allowcommunication between the anterior cranial fossa andthe orbit. Additionally, the posterior ethmoidalforamen characteristically lies 6 mm anterior to theoptic canal and 12 mm posterior to the anteriorethmoidal foramen.2
The terminal branches of the ophthalmic arteryare the supraorbital, supratrochlear, dorsal nasal andthe medial palpebral arteries. The supraorbital andsupratrochlear arteries provide the blood supply tothe forehead and medial lids, while the dorsal nasaland medial palpebral arteries supply the medial lidsand nose. The supraorbital artery travels above thelevator via the supraorbital notch or foramen andshould be carefully avoided during surgicaldissection of the orbital roof. All of these vesselsanastomose extensively with external carotidbranches to the face.
It is clear that there is great degree of collateralflow to the orbit and lids between the internal andexternal carotid circulation. Therefore, a review ofrelevant branches of the external carotid artery,namely branches of the maxillary artery, is alsoimportant. Superiorly, the superficial temporal arteryprovides blood supply to the forehead, anastomosingwith the circulation of the supraorbital andsuprotrochlear arteries. The angular artery providesanastomoses with the dorsal nasal and palpebralarteries medially. Within the orbit itself, thesphenopalatine artery, like the ethmoidal circulation,supplies the nasosinus mucosa and nasal septum. Thesuperficial branches of the infraorbital arteryanastomose with the inferomedial palpebral arteries,while the deeper branches anastomose with themuscular arteries. The anastomosis between thelacrimal artery and the middle meningeal artery hasalready been discussed. This occurs via the recurrentmeningeal artery, which enters the orbit through thesphenoid, through a foramen superolateral to thesuperior orbital fissure or directly via the fissureitself.2
basm
ala
blog
(alw
ays o
rigin
al)

Applied Anatomy of OrbitApplied Anatomy of OrbitApplied Anatomy of OrbitApplied Anatomy of OrbitApplied Anatomy of Orbit 1919191919
Figure 1.19: Venous drainage system of the orbit
Vascular Anatomy of the Orbit: VenousOutflow
The venous drainage pathways of the orbit runindependently of the arteries and are a completelyvalveless system. There are three major outflowsystems, involving the cavernous sinus, pterygoidplexus, and an anterior venous system which drainsvia the facial vein (Figure 1.19). The superiorophthalmic vein provides outflow from thesuperifical, superior periorbital and orbital regions,via the supraorbital, nasofrontal and angular veins.It can be divided into three segments as it runsanterior-posteriorly. The first segment coursesadjacent to the trochlea and along the medial edgeof the superior rectus. The second passes inferior tothe muscle and into the cone. This segment receivesthe ciliary and superior vortex veins from the globe.The third portion of the superior orbital vein travels
along the lateral edge of the superior rectus and exitsthe orbit via the extra-annular superior orbital fissureto drain into the cavernous sinus.
The inferior ophthalmic vein drains the inferiororbit, including tributaries from the inferior rectusand oblique muscles and from the inferior vortexveins. The inferior ophthalmic vein anastomoses witha branch of the superior ophthalmic vein. A portionof the outflow is directed into the pterygoid plexusand the rest directly into the cavernous sinus.Anteromedially, venous drainage occurs mainly viathe angular and facial veins. Because of the highdegree of anastamoses and absence of valves,some degree of venous obstruction can beredirected within the system. However, acutethromboses, particularly of the cavernous sinus, causemarked orbital congestion and subsequently,exophthalmos.
basm
ala
blog
(alw
ays o
rigin
al)

2020202020 Surgical Atlas of Orbital DiseasesSurgical Atlas of Orbital DiseasesSurgical Atlas of Orbital DiseasesSurgical Atlas of Orbital DiseasesSurgical Atlas of Orbital Diseases
Figure 1.20: Computed axial tomography illustrating the relationshipbetween the anterior cranial fossa, orbit and ethmoid sinus
Paranasal Sinuses
There are four pairs of paranasal sinuses: the frontal,ethmoid, sphenoid and maxillary sinuses whichdirectly neighbor the orbital roof, medial wall, andfloor. Knowledge of their anatomy is useful sincethese spaces can share disease processes with theorbit such as infection and tumors, and can alsoprovide surgical access to the orbit and lacrimalsystem.
The frontal sinus overlies the anterior portion ofthe orbital roof and drains into the frontonasal ductwhich travels though the anterior portion of theethmoid sinus (ethmoid infundibulum) to empty intothe middle meatus within the nose. This sinusdevelops in childhood and is usually difficult toappreciate radiographically until age 7 or so.Pneumatization is typically completed by earlyadulthood.56 The frontal sinus is a common site formucocele formation.57
The ethmoid sinuses lie between the medialorbital walls and immediately posterior to the nose.The lateral wall of this sinus is comprised of the verythin lamina papyracea, which is easily fractured insurgery or trauma, or compromised by local infection.A frequent source of orbital cellulitis is ethmoidsinusitis which spreads secondarily. The ethmoidroof, or fovea ethmoidalis, is located just beneaththe anterior cranial fossa and just medial to thefrontoethmoidal suture line within the orbit. Themost medial portion of the ethmoid roof is thecribriform plate, which overlies the nasal cavity(Figure 1.20). The sinuses themselves are comprisedof many individual, thin-walled air cells and can be
divided into three groups. The anterior and middleair cells drain into the middle meatus while theposterior air cells empty into the superior meatus ofthe nose. In performing dacryocystorhinostomy tocreate a passage between the lacrimal sac and nose,the ethmoid air cells are frequently encounteredextending anterior to the posterior lacrimal crest.58,59
The sphenoid sinuses are located midsagittallyand posterior to the ethmoid air cells. Like the frontalsinuses, they pneumatize relatively late in life anddo not reach full size until adolescence. Drainageoccurs via the sphenoethmoid recess located in theanterior sinus wall. Because the contents of the orbitalapex and nearby cavernous sinus exit the orbitthrough the sphenoid bone, the walls of the sphenoidlie in close proximity to a number of criticalstructures. Anteriorly and superolaterally, the opticnerve and intracavernous portion of the internalcarotid artery run along the lateral sinus walls. Severesphenoid sinusitis can therefore cause optic nerveinjury.60 Likewise, congenital dysplasia of thesphenoid, as can occur in neurofibromatosis type 1,can produce pulsatile proptosis.61, 62 The sphenoidsinus also provides a useful surgical approach to thepituitary fossa which is located posteriorly to thesinus.63
The maxillary sinus underlies the orbital floorand is the largest of the paranasal sinuses. Drainagefrom this sinus occurs via the maxillary ostium intothe middle meatus. The ostium is located high withinthe medial sinus wall, close to the level of the orbitalfloor. Thus, trauma to the orbital floor (i.e. orbitalfracture or inferomedial decompression) can obstructdrainage from the sinuses. Inside the medial wallsof the maxillary sinus, lie the bony nasolacrimalcanals. The posterior most aspect of the sinus extendsfrom the area of the infraorbital fissure, and theinfraorbital nerve and artery run along the maxillaryroof within the infraorbital canal. Behind themaxillary sinus is located the pterygopalatine fossaand the maxillary artery runs in its posterior wall.
Conclusion
The orbit and its surrounds represent a complexanatomical space, incorporating critical ocular, neural,and vascular structures. The purpose of this chapterhas been to provide an overview of orbital anatomy,as well as basic anatomy of the eyelids, lacrimal
basm
ala
blog
(alw
ays o
rigin
al)

Applied Anatomy of OrbitApplied Anatomy of OrbitApplied Anatomy of OrbitApplied Anatomy of OrbitApplied Anatomy of Orbit 2121212121
system, and paranasal sinuses. A detailedunderstanding of this anatomy is fundamental tooculoplastic surgery and the management of orbitaldisease.
REFERENCES
1. Whitnall SE. The Anatomy of the Human Orbit andAccessory Organs of Vision, 2nd ed. NewYork: OxfordUniversity Press; 1932.
2. Rootman J, Stewart B, Goldberg RA. Orbital Surgery: AConceptual Approach New York: Lippincott-Raven, 1995.
3. Webster RC. Supraorbital and supratrochlear notches andforamina: Anatomical variations and surgical relevance.Laryngoscope 1986;96:311.
4. Kim JW, Goldberg RA, Shorr N. The inferomedial orbitalstrut: An anatomic and radiographic study. Ophthal PlastReconstr Surg 2002;18:355-64.
5. Rose JG, Lucarelli MJ, Lemke BN. Lacrimal, orbital andsinus anatomy. In: Woog JJ, (Ed): Manual of EndoscopicLacrimal and Orbital Surgery. London: Elsevier, 2003.
6. Goldberg RA, Schorr N, Cohen M. The medial orbital strutin the prevention of post-decompression dystopia indysthyroid ophthalmopathy. Ophthalmic Plast ReconstrSurg 1992;8:32-34.
7. Whitnall S. On a tubercle on the malar bone, and on thelateral attachments of the tarsal plates. J Anat Physiol1911;45:426-32.
8. Yeh S, Foroozan R. Orbital apex syndrome. Curr OpinOphthalmol 2004;15:490-98.
9. Lenzi GL, Fieschi C. Superior orbital fissure syndrome: areview of 130 cases. Eur Neurol 1977;16:23-30.
10. Morard M, Tcherekayev V, deTribolet N. The superiororbital fissure: a microanatomical study. Neurosurgery1994;35:1087-93.
11. Jordan DR. The nervus intermedius. Arch Ophthalmol1993;111:1691.
12. Lyon D, Lemke BN, Wallow I, Dortzbach RK. Sympatheticnerve anatomy in the cavernous sinus and retrobulbarorbit of the cynomolgous monkey. Ophthalmic PlastReconstr Surg 1992;8:1-12.
13. Keane JR. Cavernous sinus syndrome. Analysis of 151 cases.Arch Neurol 1996;53:967-71.
14. Koornneef L. New insights in the human periorbitalconnective tissue: results of a new anatomic approach. ArchOphthalmol 1977;95:1269-73.
15. Koornneef L. Orbital septa: anatomy and function.Ophthalmology 1979;86:876-85.
16. Sutton J. The fascia of the human orbit. Anat Reconstr1920;18:141.
17. Dutton J. Atlas of Clinical and Surgical Orbital Anatomy.Philadelphia: WB Saunders Co; 1994.
18. Jones LT. A new concept of the orbital fascia and rectusmuscle sheaths and its surgical implications. Trans Am AcadOphthalmol Otolaryngol. 1968;72:755-64.
19. Fink W. An anatomical study of the check ligaments of thevertical muscles of the eyes. Am J Ophthalmol 1957;44:800-09.
20. Helveston E, Merriam W, Ellis F, Schelhamer R, Gosling G.The trochlea: a study of the anatomy and physiology.Ophthalmology 1982;89:124-33.
21. Sacks J. The shape of the trochlea. Arch Ophthalmol1984;102:932.
22. Neely K, Ernest J, Mottier M. Combined superior obliquepalsy and Brown’s syndrome after blepharoplasty. Am JOphthalmol 1990;109:347.
23. Apt L. An anatomic reevaluation of rectus muscleinsertions. Trans Am Ophthalmol Soc 1988;78:365.
24. Ahl NC, Hill JC. Horner’s muscle and the lacrimal system.Arch Ophthalmol. 1982;100:488-93.
25. Shinohara H, Kominami R, Yasutaka S, Taniguchi Y. Theanatomy of the lacrimal portion of the orbicularis oculimuscle (tensor tarsi or Horner’s muscle). Okajimas FoliaAnat Jpn 2001;77:225-32.
26. Meyer DR, Linberg JV, Wobig JL, McCormick SA. Anatomyof the orbital septum and tissues. Implications for ptosissurgery. Ophthal Plastic Reconstr Surg 1991;7:104-13.
27. Hawes MJ, Dortzbach RK. The relationship ofcapsulopalebral fascia with orbital septum of the lowereyelid: an anatomic study under magnification. JCraniofacial Surgery 2006;17:1118-20.
28. Castanares S. Blepharoplasty for herniated intraorbital fat:anatomical basis for a new approach. Plast Reconstr Surg1951;8:46-58.
29. Kikkawa DO, Lucarelli MJ, Shovlin JP, Cook BE, LemkeBN. Ophthalmic facial anatomy and physiology. In: Levine,MR, ed. Manual of Oculoplastic Surgery, third ed. NewYork: Butterworth Heinemann; 2003.
30. Whitnall S. On a ligament acting as a check to the action ofthe levator palpebrae superioris muscle. J Anat Physiol.1910;14:131.
31. Goldberg RA. Eyelid anatomy revisited: dynamic high-resolution images of Whitnall’s ligament and upper eyelidstructures with the use of a surface coil. Arch Ophthalmol.1992;110:1598.
32. Anderson R. Dixon R. The role of Whitnall’s ligament inptosis surgery. Arch Opthalmol 1979;97:705-07.
33. Walton KA, Buono LM. Horner syndrome. Curr OpinOphthalmol 2003;14:357-63.
34. Lockwood C. the anatomy of the muscles, ligaments,and fascia of the orbit, including an account of the capsuleof tenon, the check ligaments of the recti, and ofthe suspensory ligament of the eye. J Anat Physiol 1885;20:2-25.
35. Scheie HG, Albert DM. Distichiasis and trichiasis: originand management. Am J Ophthalmol 1966;61:718.
36. Lemke BN, Lucarelli MJ. Anatomy of the ocular adnexa,orbit, and related facial structures. In: Nesi, FA, Lisman,RD, Levine, MR, (Eds). Smith’s Ophthalmic Plastic andReconstructive Surgery. St. Louis: CV Mosby; 1998.
basm
ala
blog
(alw
ays o
rigin
al)

2222222222 Surgical Atlas of Orbital DiseasesSurgical Atlas of Orbital DiseasesSurgical Atlas of Orbital DiseasesSurgical Atlas of Orbital DiseasesSurgical Atlas of Orbital Diseases
37. Smith B, Petrelli R. Surgical repair of the prolapsed lacrimalgland. Ophthalmology 1978;96:113.
38. Ruskell G. The orbital branches of the pterygopalatineganglion and their relationship with internal carotid nervebranches in primates. J Anat 1970;106:323.
39. Ruskell G. The distribution of autonomic postganglionicfibers to the lacrimal gland in monkeys. J Anat 1971;109:229-42.
40. Dutton J. The lacrimal systems. In: Dutton, J. Atlas of Clinicaland Surgical Orbital Anatomy. Philadelphia: WB SaundersCo; 1994.
41. Tucker N, Tucker S, Linberg J. The anatomy ofthe common canaliculus. Arch Ophthalmol 1996;114:1231-34.
42. Groell R, Schaffler G, Uggowitzer M, Szolar D, Muellner K.CT: anatomy of the nasolacrimal sac and duct.Surg Radiol Anat. 1997;19:189-91.
43. Drysdale D. Experimental subdural retrobulbar injectionof anesthetic. Ann Ophthalmol 1984;16:716-19.
44. Anderson RL, Panje WR, Gross CE. Optic nerve blindnessfollowing blunt forehead trauma. Ophthalmology1982; 89: 445–55.
45. Sarkies N. Traumatic optic neuropathy. Eye 2004;18:1122–25.
46. Dalley R, Robertson W, Rootman J. Globe tenting: a sign ofincreased orbital tension. Am J Neuroradiol. 1984;10:181-86.
47. Knize D. A study of the supraorbital nerve. Plast ReconstrSurg 1995;96:564-69.
48. Hornblass A. Pupillary dilation in fractures of the floor ofthe orbit. Ophthalmic Surg 1979;10:44.
49. Mansour AM, Reinecke RD. Central trochlear palsy. SurvOphthalmol 1986;30:279-97.
50. Wall M, George D. Idiopathic intracranial hypertension. Aprospective study of 50 patients. Brain 1991;114:155-80.
51. Hanson RA, Ghosh S, Gonzalez-Gomez I, Levy ML, GillesFH. Abducens length and vulnerability? Neurology2004;62:33-36.
52. Insel TR, Kalin NH, Risch SC, Cohen RM, MurphyDL. Abducens palsy after lumbar puncture. N Engl J Med1980;303:703.
53. Hayreh SS. The ophthalmic artery. I. Origin andintracranial and intracanalicular course. Br J Ophthalmol1962;46:65-98.
54. Lang J, Kageyama I. The ophthalmic artery and itsbranches, measurements and clinical importance. SurgRadiol Anat 1990;12:83-90.
55. Ettl A, Kramer J, Daxter A, Koornneef L. High resolutionmagnetic resonance imaging of neurovascular orbitalanatomy. Ophthalmology 1997;104:869-77.
56. Zinreich SJ. Imaging of the nasal cavity and paranasalsinuses. Curr Opin Radiol 1992;4:112-16.
57. Rootman J. Disease of the Orbit. Philadelphia: JB Lippincott;1988.
58. Buus D, Tse D, Farris B. Ophthalmic complications of sinussurgery. Ophthalmology 1990;97:612-19.
59. Blaylock W. Moore C, Linberg J. Anterior ethmoidalanatomy facilitates dacryocystorhinostomy. ArchOphthamol 1990;108:1774-77.
60. Fujimoto N, Adachi-Usami E, Saito E, Nagata H. Optic nerveblindness due to paranasal sinus disease. Ophthalmologica1999;213:262-64.
61. Hunt JC, Pugh D. Skeletal lesions in neurofibromatosis.Radiology 1961;76:1–19
62. Mortada A: Pulsating exophthalmos with orbitalneurofibromatosis, Am J Ophthalmol 1967;64:462.
63. Kanter AS, Dumont AS, Asthagiri AR, Oskouian RJ, JaneJA, Laws ER. The transsphenoidal approach: a historicalperspective. Neurosurg Focus 2005;18:1-4.
basm
ala
blog
(alw
ays o
rigin
al)

Subrahmanyam Mallajosyula
Clinical ApproachClinical ApproachClinical ApproachClinical ApproachClinical Approachto Proptosisto Proptosisto Proptosisto Proptosisto Proptosis
Before we discuss about proptosis let me remind youthat we have to distinguish it from certain conditionswhich resemble proptosis (pseudo-proptosis) likeunilateral high myopia, buphthalmos, unilateral lidretraction, unilateral minimal ptosis of contralateraleye.
Though advances in imaging techniques haverevolutionized the diagnosis of orbital diseases,proper clinical evaluation of proptosis is still veryimportant because it gives us the insight into thedisease process and helps in evaluating the CT/MRIand arriving at a correct diagnosis. I follow the
9 “P”s, an extension of the 6 “P”s of Krohel’s. The9 Ps are: Pain, Progression (from history), Proptosis,Pulsations, Pupil, PBCT, Perception of color vision,Periorbital changes (inspection) and Palpation.
Pain: When severe pain is the presentingsymptom in proptosis, we have to consider thefollowing conditions: infection and inflammatorylesions like orbital cellulitis, orbital abscess(Figure 2.1), myocysticercosis, vascular conditionslike lymphangioma (Figure 2.2), high flowcarotid- cavernous fistula (Figure 2.3). Metastaticlesions (Figure 2.4) are also very painful.
Figure 2.4: Metastasis from thyroid carcinomaFigure 2.3: Carotid-cavernous fistula
Figure 2.2: LymphangiomaFigure 2.1: Orbital abscess
2C H A P T E R
basm
ala
blog
(alw
ays o
rigin
al)
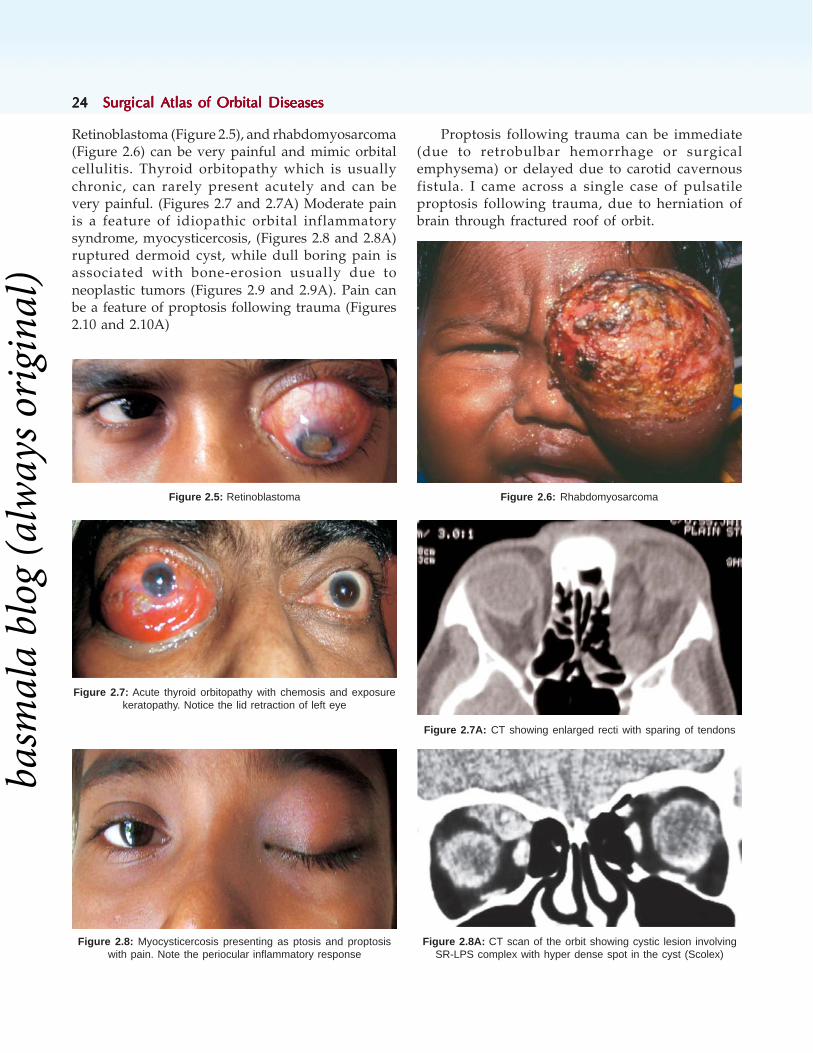
2424242424 Surgical Atlas of Orbital DiseasesSurgical Atlas of Orbital DiseasesSurgical Atlas of Orbital DiseasesSurgical Atlas of Orbital DiseasesSurgical Atlas of Orbital Diseases
Retinoblastoma (Figure 2.5), and rhabdomyosarcoma(Figure 2.6) can be very painful and mimic orbitalcellulitis. Thyroid orbitopathy which is usuallychronic, can rarely present acutely and can bevery painful. (Figures 2.7 and 2.7A) Moderate painis a feature of idiopathic orbital inflammatorysyndrome, myocysticercosis, (Figures 2.8 and 2.8A)ruptured dermoid cyst, while dull boring pain isassociated with bone-erosion usually due toneoplastic tumors (Figures 2.9 and 2.9A). Pain canbe a feature of proptosis following trauma (Figures2.10 and 2.10A)
Proptosis following trauma can be immediate(due to retrobulbar hemorrhage or surgicalemphysema) or delayed due to carotid cavernousfistula. I came across a single case of pulsatileproptosis following trauma, due to herniation ofbrain through fractured roof of orbit.
Figure 2.6: Rhabdomyosarcoma
Figure 2.7A: CT showing enlarged recti with sparing of tendons
Figure 2.8A: CT scan of the orbit showing cystic lesion involvingSR-LPS complex with hyper dense spot in the cyst (Scolex)
Figure 2.7: Acute thyroid orbitopathy with chemosis and exposurekeratopathy. Notice the lid retraction of left eye
Figure 2.5: Retinoblastoma
Figure 2.8: Myocysticercosis presenting as ptosis and proptosiswith pain. Note the periocular inflammatory response
basm
ala
blog
(alw
ays o
rigin
al)

Clinical Approach to ProptosisClinical Approach to ProptosisClinical Approach to ProptosisClinical Approach to ProptosisClinical Approach to Proptosis 2525252525
Progression: The onset of proptosis can be acute(hours to week), subacute (1 to 4 weeks) or chronic(more than 1 month). Acute proptosis can be due toinfections, inflammations, parasitic infestations,trauma, metastatic lesions or lymphangioma.Subacute presentation is common in inflammations,parasitic infestations or metastatic neoplasia.
(Figure 2.11) Chronic presentation is commonly dueto thyroid associated orbitopathy (Figure 2.12),orbital varices or benign neoplasia like cavernoushemangioma, (Figures 2.13 to 2.13B), Neurofibroma(Figures 2.14 to 2.14E), Schwannoma (Figures 2.15to 2.15B), Glioma of Optic Nerve, (Figures 2.16 to2.16C). Chronic presentation is characteristic of mostof the primary neoplasia of the orbit, both benignand malignant. However, if the presentation is lessthan 6 months, consider the possibility of a malignantlesion.
Figure 2.10A: After anterior orbitotomy showscomplete recovery. Vision improved to 20/30
Figure 2.10: Acute proptosis following Trauma. Notesevere chemosis, exposure keratitis with hypopyon
Figure 2.9A: CT scan orbit showing a mass in the fossa oflacrimal gland. Note the bony erosion and heterogenisity of themass (Adenoidcystic carcinoma of lacrimal gland)
Figure 2.9: Eccentric proptosis with globe pushed down.Note fullness of lacrimal gland region
Figure 2.11: Metastatic orbital lesion presenting subacutely.Note the inflammatory changes
Figure 2.12: Thyroid associated orbitopathy with chronic presenta-tion. Note the lid retraction and lateral flare of right upper lid. Note theabsence of congestion and edema
basm
ala
blog
(alw
ays o
rigin
al)

2626262626 Surgical Atlas of Orbital DiseasesSurgical Atlas of Orbital DiseasesSurgical Atlas of Orbital DiseasesSurgical Atlas of Orbital DiseasesSurgical Atlas of Orbital Diseases
Figure 2.13A: CT scan showing well encapsulated tumor(Cavernous hemangioma)
Figure 2.13B: Excised tumor
Figure 2.14B: Extension of tumor into superiorperipheral space pushing the globe down
Figure 2.13: Axial proptosis of left eye 3 yrs. Noticehow quiet was the globe
Figure 2.14A: CT shows a large well definedmass with bony expansion
Figure 2.14: M 52, RE proptosis since 3 yrs,Def. Vision 1yr. RAPD +, VA : 20/200
basm
ala
blog
(alw
ays o
rigin
al)

Clinical Approach to ProptosisClinical Approach to ProptosisClinical Approach to ProptosisClinical Approach to ProptosisClinical Approach to Proptosis 2727272727
Figure 2.15B: Excised tumor, proved to be schwannoma
Figure 2.14D: Spindle-cells of neurofibroma
Figure 2.14C: Well encapsulated tumor on gross exam
Figure 2.15: F 30, presented with proptosis of 3 yrs.Defective vision(20/800) RAPD +ve
Intermittent proptosis is usually due to idiopathicorbital inflammatory syndrome, lymphangioma
Figure 2.14E: Postoperative status recovery from proptosis. VAimproved to 20/40
Figure 2.15A: CT scan showing a well encapsulatedintraconal mass. Note the excavation of lateral wall
(Figure 2.17), orbital varices and myocysticercosis(in endemic areas). (Figure 2.18)
basm
ala
blog
(alw
ays o
rigin
al)

2828282828 Surgical Atlas of Orbital DiseasesSurgical Atlas of Orbital DiseasesSurgical Atlas of Orbital DiseasesSurgical Atlas of Orbital DiseasesSurgical Atlas of Orbital Diseases
Figure 2.18: CT scan showing an enlarged superior rectus musclewith a cyst showing hyper-dense spot within (Myocysticercosis)
Figure 2.16C: Postoperative status. No proptosis
Figure 2.16A: CT scan orbit showing optic nerve gliomawith cystic degeneration
Figure 2.17: Girl of 12 years presenting with recurrent episodes ofproptosis (3 in 5 yrs). Note the subconjunctival hemorrhage in theproptosed LE (Lymphangioma)
Figure 2.16B: Excised tumor
Figure 2.16: M 14 yrs, proptosis of right eye since 8 years.RAPD + Vision absent PL
Proptosis: Proptosis or protrusion of the eye balldepends on the location of the orbital lesion. A lesionin the intraconal space pushes the globe forwards tocause “axial proptosis” (Figures 2.19 to 2.19B), whereas a lesion in the peripheral surgical space pushesthe globe to the opposite side and causes “eccentric
proptosis.” However, since these surgical compart-ments are not strictly water-tight, a large intraconallesion can enter peripheral surgical space and causeeccentricity to an otherwise axial proptosis (Figure2.14 series).
basm
ala
blog
(alw
ays o
rigin
al)

Clinical Approach to ProptosisClinical Approach to ProptosisClinical Approach to ProptosisClinical Approach to ProptosisClinical Approach to Proptosis 2929292929
Axial proptosis: Lesion is in the intraconal space.In my experience the most common lesion ofintraconal space causing axial proptosis iscavernous hemangioma followed by Schwannoma,and neuro-fibroma. Optic nerve glioma andmeningioma of optic nerve sheath are important butnot very common lesions. Other lesions include orbitalvarix, lymphangioma. The most common intraconalcystic lesion is hydatid cyst (Figures 2.20 and2.20A).
One has to remember that most of the intraconallesions can compress optic nerve and lead to visualloss. Hence loss of vision in axial proptosis does notnecessarily mean that the patient had either opticnerve glioma or meningioma of optic nerve sheath.It can be due to any other lesion of intraconal spacelike hemangioma, schwannoma, neurofibroma,hydatid cyst or even idiopathic orbital inflammatorysyndrome. Optic nerve can also be compressed byenlarged extraocular muscles as in thyroid associatedorbitopathy.
Down and out proptosis is due to lesionsof superomedial space (pushing the globe downand out). Frontoethmoidal lesions are the mostcommon cause of such eccentric proptosis.Mucocele (Figures 2.21A to C), fungal granuloma,neoplastic lesions and fibrous dysplasia (Figures2.22A and B) are the common lesions. Lesions ofsupero-medial space like dermoids, hemangiomas canalso present with eccentric proptosis with globedisplaced down and out (Figures 2.23A and B).Osteoma of ethmoid (Figures 2.24A to E) is anotherrare cause.
Figure 2.19: Axial proptosis of left eye due to intraconal lesion
Figure 2.20: Intraconal hydatid cyst of orbit Figure 2.20A: Cyst excised with cryo after aspirating fluid
Figures 2.19A and B: CT scans of orbit showing intraconal tumor arising from optic nerve (Optic nerve glioma)
A B
basm
ala
blog
(alw
ays o
rigin
al)

3030303030 Surgical Atlas of Orbital DiseasesSurgical Atlas of Orbital DiseasesSurgical Atlas of Orbital DiseasesSurgical Atlas of Orbital DiseasesSurgical Atlas of Orbital Diseases
Figures 2.21A to C: Eccentric proptosis with the eyeball pushed down and out. Notice the gross outward displacementwith fullness in the superomedial aspect. CT scan shows a huge fronto-ethmoid mucocele
Figures 2.22A and B: Eccentric proptosis with globe pushed downand out due to fibrous dysplasia of frontal bone as demonstrated bythe CT scan (B)
A B
C
A
B
basm
ala
blog
(alw
ays o
rigin
al)

Clinical Approach to ProptosisClinical Approach to ProptosisClinical Approach to ProptosisClinical Approach to ProptosisClinical Approach to Proptosis 3131313131
Figures 2.23A and B: Coronal and axial sections of CT scan orbit showing a very large cystic lesion in the superomedial peripheral space(blue arrow), displacing the Globe (green pentagon) down and out. Compare the size of the cyst with that of opposite eyeball. Note the bonyexcavation of the roof and medial wall (red arrow). This is a case of Hydatid cyst of orbit
A B
Figures 2.24A to C: This young male of 22 yrs presented with recurrent, eccentric proptosis of right eye since 1year, and defective visionsince 3 months. He underwent surgery elsewhere for similar lesion 2 years back. Note the periocular fullness, and lateral displacement of theglobe. He had RAPD and the vision was 20/40. CT scan of orbits revealed a huge osteoma involving the ethmoid bone (arrow)
Figures 2.24D and E: Excised ivory osteoma. The postoperativerecovery was uneventful. The patient's vision improved to 20/20
A
B C
D
E
basm
ala
blog
(alw
ays o
rigin
al)
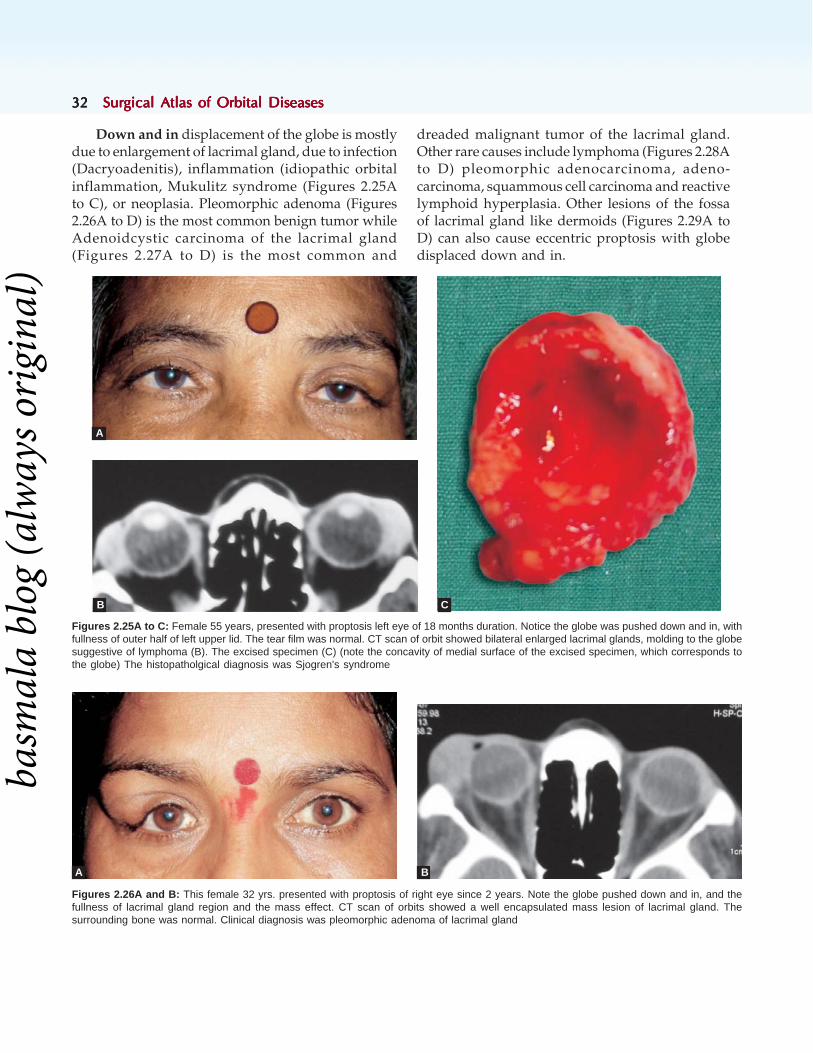
3232323232 Surgical Atlas of Orbital DiseasesSurgical Atlas of Orbital DiseasesSurgical Atlas of Orbital DiseasesSurgical Atlas of Orbital DiseasesSurgical Atlas of Orbital Diseases
Down and in displacement of the globe is mostlydue to enlargement of lacrimal gland, due to infection(Dacryoadenitis), inflammation (idiopathic orbitalinflammation, Mukulitz syndrome (Figures 2.25Ato C), or neoplasia. Pleomorphic adenoma (Figures2.26A to D) is the most common benign tumor whileAdenoidcystic carcinoma of the lacrimal gland(Figures 2.27A to D) is the most common and
dreaded malignant tumor of the lacrimal gland.Other rare causes include lymphoma (Figures 2.28Ato D) pleomorphic adenocarcinoma, adeno-carcinoma, squammous cell carcinoma and reactivelymphoid hyperplasia. Other lesions of the fossaof lacrimal gland like dermoids (Figures 2.29A toD) can also cause eccentric proptosis with globedisplaced down and in.
Figures 2.25A to C: Female 55 years, presented with proptosis left eye of 18 months duration. Notice the globe was pushed down and in, withfullness of outer half of left upper lid. The tear film was normal. CT scan of orbit showed bilateral enlarged lacrimal glands, molding to the globesuggestive of lymphoma (B). The excised specimen (C) (note the concavity of medial surface of the excised specimen, which corresponds tothe globe) The histopatholgical diagnosis was Sjogren's syndrome
Figures 2.26A and B: This female 32 yrs. presented with proptosis of right eye since 2 years. Note the globe pushed down and in, and thefullness of lacrimal gland region and the mass effect. CT scan of orbits showed a well encapsulated mass lesion of lacrimal gland. Thesurrounding bone was normal. Clinical diagnosis was pleomorphic adenoma of lacrimal gland
A B
A
B C
basm
ala
blog
(alw
ays o
rigin
al)
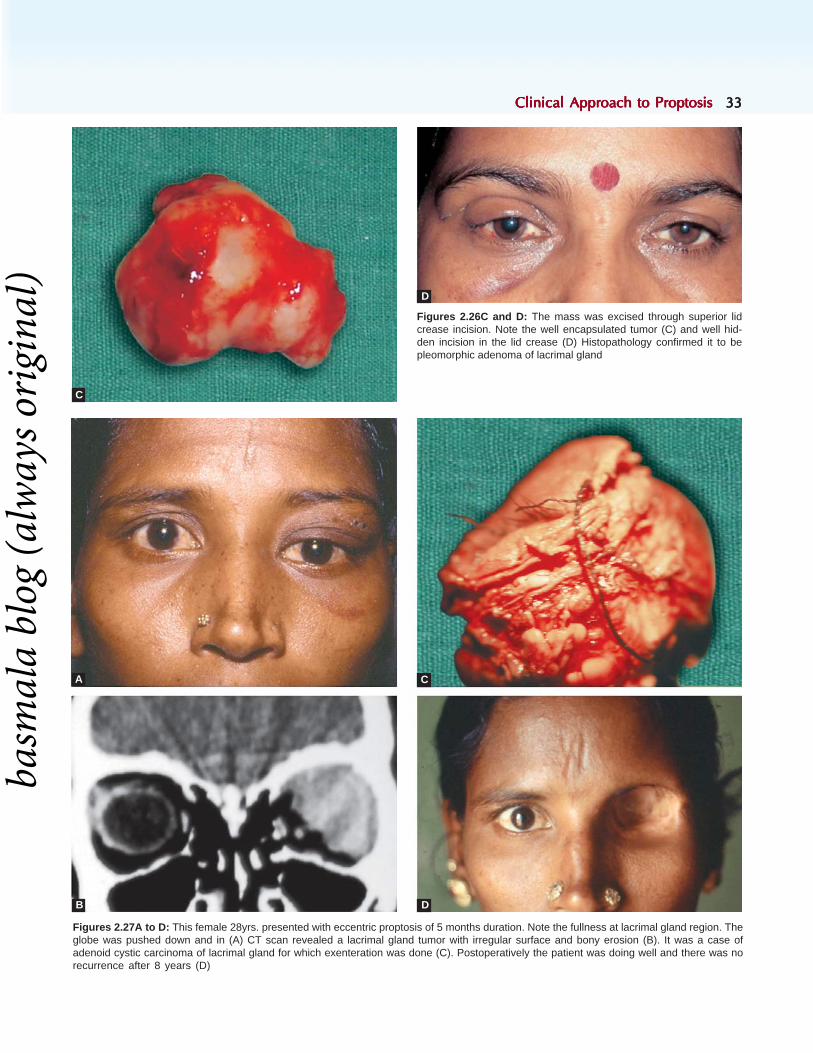
Clinical Approach to ProptosisClinical Approach to ProptosisClinical Approach to ProptosisClinical Approach to ProptosisClinical Approach to Proptosis 3333333333
Figures 2.26C and D: The mass was excised through superior lidcrease incision. Note the well encapsulated tumor (C) and well hid-den incision in the lid crease (D) Histopathology confirmed it to bepleomorphic adenoma of lacrimal gland
Figures 2.27A to D: This female 28yrs. presented with eccentric proptosis of 5 months duration. Note the fullness at lacrimal gland region. Theglobe was pushed down and in (A) CT scan revealed a lacrimal gland tumor with irregular surface and bony erosion (B). It was a case ofadenoid cystic carcinoma of lacrimal gland for which exenteration was done (C). Postoperatively the patient was doing well and there was norecurrence after 8 years (D)
C
D
A C
B D
basm
ala
blog
(alw
ays o
rigin
al)

3434343434 Surgical Atlas of Orbital DiseasesSurgical Atlas of Orbital DiseasesSurgical Atlas of Orbital DiseasesSurgical Atlas of Orbital DiseasesSurgical Atlas of Orbital Diseases
Figures 2.28A and B: Note the fullness of left upper lid with globepushed down and in (A). CT scan of orbit shows enlarged lacrimalgland, molding to the globe (B)
Figures 2.28C and D: The tumor was excised through Sub-browincision (C). Histopathology revealed it to be a case of lymphoma. 3days postoperative photo showing marked improvement from propto-sis (D)
A
B
C
D
basm
ala
blog
(alw
ays o
rigin
al)

Clinical Approach to ProptosisClinical Approach to ProptosisClinical Approach to ProptosisClinical Approach to ProptosisClinical Approach to Proptosis 3535353535
Figures 2.29A to D: Female 25 years, presented with eccentric proptosis of right eye since, 2 years, She had 2 episodes of pain andworsening of proptosis in the past 6 months. Note the fullness of the upper lid, and the globe which was pushed down and in (A) Axial andcoronal sections of the CT scan show a cystic lesion with variable consistency, situated at the fossa of lacrimal gland (B and C). Exciseddermoid cyst (D)
A
B
C D
Upward displacement of globe is due to eitheran extension of lesion of maxillary sinus into orbit(neoplasia, fungal granuloma or dumbbell dermoid)or lesions of inferior space like cavernoushemangioma, neurofibroma, schwannoma, cysticlesions like myocysticercosis involving inferior rectus(Figures 2.30A to C). Many a time lesions of maxillarysinus extend into frontoethmoidal sinuses, or nose.Anterior extension leads to fullness of cheek (Figures2.31A to C). It is my experience that orbital extensionof lesions from paranasal sinuses is a common causeof eccentric proptosis.
Measurement of proptosis is a very importantpart of evaluation of the patient. The displacementof the globe should be quantified in all the 3directions, anteroposterior (axial), horizontal andvertical axes. Naphzeiger’s test is a useful bedside
clinical test to detect mild proptosis (Figures 2.32Aand B). Ask the patient to look at a distant object,located at the same level as that of the patient’s eye.Stand behind the patient, and gently tilt the headbackwards and look down over the patient’s forehead.The proptosed eye appears ahead of the other.
Another simple bedside test to detect mildproptosis is with the help of a scale. Ask the patientto gently close the eyes, and keep a scale across theeye in contact with his forehead and cheek. Normallythere will be space between the scale and the closedlid. In the presence of proptosis this space isobliterated (Figures 2.33A and B).
Axial proptosis is best measured with Hertel'sexophthalmometer (Figure 2.34A). Leudde'sexophthalmometry is less accurate and inter-observervariation is more significant.
basm
ala
blog
(alw
ays o
rigin
al)

3636363636 Surgical Atlas of Orbital DiseasesSurgical Atlas of Orbital DiseasesSurgical Atlas of Orbital DiseasesSurgical Atlas of Orbital DiseasesSurgical Atlas of Orbital Diseases
Figures 2.30A to C: This female, 42 years in age, presented withproptosis left eye, which was displaced upwards (A). Note the masslesion in lower lid, which was transilluminant (B). This demoid cystwas removed through swinging lower lid approach. Note the minimalswelling of lower lid on 2nd postoperative day (C)
A
B
C
Figures 2.31A to C: This child presented with proptosis of right eye since 2 years. Note the fullness of cheek, and gross upward displacementof the globe due to lesion of the Maxillary sinus (A). CT scan of the orbit (B and C) revealed it to be ossifying fibroma. Note that the mass isinvolving the nasal cavity (red arrow) and the oral cavity (blue arrow)
A
B
C
basm
ala
blog
(alw
ays o
rigin
al)

Clinical Approach to ProptosisClinical Approach to ProptosisClinical Approach to ProptosisClinical Approach to ProptosisClinical Approach to Proptosis 3737373737
Hertel’s exophthalmometry consists of 2 footplates - one is fixed and the other sliding. Each footplate has a viewing mechanism (Figure 2.34B) wherethe eye being examined is seen in profile below ascale in millimeters (Figure 2.34D). There are 2 redlines for reference to avoid parallax error. Rest thefixed footplate on the anterior part of lateral wall ofright orbit and slide the other footplate on the scaletill it rests on the anterior part of lateral wall of leftorbit. Note the distance between the 2 foot platesfrom the scale. This is called the “Base Reading” (BR).It is very important to record the base reading sincethe exophthalmometry values change with basereading. In other words, if you take 2 readings onthe same patient one after the other with 2 differentbase readings, the values you get will be different.In fact the one with wider BR will give larger value!If you forget to note the BR, you can not accurately
To measure the horizontal displacement of theeye, put a mark on the center of root of the nose.Measure the distance from that point to the nasallimbus of the proptosed eye, with the other eye beingcovered. Repeat the same for the normal eye,covering the proptosed eye. The difference betweenthese two readings gives you the horizontaldisplacement (Figures 2.35A and B).
Vertical displacement is measured with the helpof 2 rulers. Hold the first scale in line with the lateralcanthi. Measure the distance from this scale to the6 O'clock limbus of each eye.
A larger reading of proptosed eye means thatthe globe is pushed inferiorly, and a lesser readingis obtained when the globe is displaced up (Figures2.36A and B).
Pulsations: Pulsations of globe in proptosis canbe either vascular pulsations or transmitted
Figures 2.32A and B: Naphzeiger’s test: Note the prominence ofleft eye (arrow). The right eye is not visible
Figure 2.33A: Note the space between the closedright eye and the scale in a normal eye
Figure 2.33B: Note the obliteration of space. The scale is incontact with the eyelid of proptosed left eye
compare results over a period of time. When once theBR is recorded, subsequent readings should be takenwith the same BR so that the results are comparable.
Another very important factor you have toremember is that while performing exophtha-lmometry, you should occlude the unexamined eyewith your thumb, (Figure 2.34C) so that the eye beingexamined comes to the primary position. Then onlythe readings are accurate.
A B
basm
ala
blog
(alw
ays o
rigin
al)

3838383838 Surgical Atlas of Orbital DiseasesSurgical Atlas of Orbital DiseasesSurgical Atlas of Orbital DiseasesSurgical Atlas of Orbital DiseasesSurgical Atlas of Orbital Diseases
Figure 2.34A: Hertel’s exophthalmometer: It consists of 2 footplates, one fixed (blue arrow) and another sliding (red arrow)which slides on a scale (green arrow). The distance between the 2 plates is the base reading (98 mm in this picture)
Figures 2.34C and D: Hertel's exophthalmometry. Note the unexamined right eye was occluded with the thumb, so that the eye being examined(left eye) is in the primary position. The scale reading of the anterior most part of the cornea seen in profile (green arrow) is the axial positionof the globe
C D
Figure 2.34B: Viewing system of each footplate. It has a red reference line in front (green arrow).Another redline (blue arrow) is seen throughthe prism. You have to align both the redlines into a single line to eliminate parallax error. The eye ball is seen in profile and its position is readfrom the scale (red arrow).
basm
ala
blog
(alw
ays o
rigin
al)

Clinical Approach to ProptosisClinical Approach to ProptosisClinical Approach to ProptosisClinical Approach to ProptosisClinical Approach to Proptosis 3939393939
Figures 2.36A and B: First Scale is held joining the lateral canthi and is the point of reference. The second scale measures the verticaldisplacement. Note that the proptosed left eye is displaced down and gives larger reading
A B
Figures 2.35A and B: Measurement of horizontal displacement of the eyeball. Ask the patient to fix at a distant object in the straight gaze,covering the unexamined eye. Measure the distance from the central point of reference on the root of nose (red arrow) to the nasal limbus;Compare the same with that of other eye. Lesser reading of the proptosed eye means that the globe was pushed medially (A: Central point ofreference drawn on the nose, B: Nasal limbus, C; Cover)
A B
pulsations. Vascular pulsations are due to increasedblood flow and is typically seen in Carotid-Cavernous Fistula (CCF). It is almost always seen inhigh-flow CCF (Figures 2.37A to C). The otherimportant causes include meningioma (Figures 2.38Ato C), orbital varix, aneurysms, etc. Transmittedpulsations are due to cerebral pulsations which aretransmitted due to bony deficiency as in
neurofibroma (Figures 2.39A and B). I have seen achild who presented with pulsatile proptosis due toherniation of frontal lobe of brain into orbit followingtrauma (Figures 2.40A and B).
To detect pulsations observe from a side. Subtlepulsations can be recognized while recording IOPwith an applanation tonometer.
basm
ala
blog
(alw
ays o
rigin
al)

4040404040 Surgical Atlas of Orbital DiseasesSurgical Atlas of Orbital DiseasesSurgical Atlas of Orbital DiseasesSurgical Atlas of Orbital DiseasesSurgical Atlas of Orbital Diseases
Figures 2.37A to C: Note the caput medusae of conjunctival con-gestion with limitation of abduction of left eye (A). She has a pulsatileproptosis, 3 months after head injury. The IOP was 28 mm of Hg. Bruitwas heard with the stethoscope (B). CT scan of orbit revealed a verygrossly enlarged superior ophthalmic vein (green arrow), typical ofcarotid cavernous fistula (C)
Figures 2.38A to C: This lady of 58 years, presented with pulsatileproptosis of right eye since 1 year (A). Note the temporal fullness,(blue arrow) which was showing pulsations (B), CT scan revealed amass from temporal lobe and involving the sphenoid wing with exten-sion in to orbit and the temple (C). Note the hyperostosis of Sphenoidbone (red arrow) This is a case of meningioma
A
C
B
A
B
C
basm
ala
blog
(alw
ays o
rigin
al)
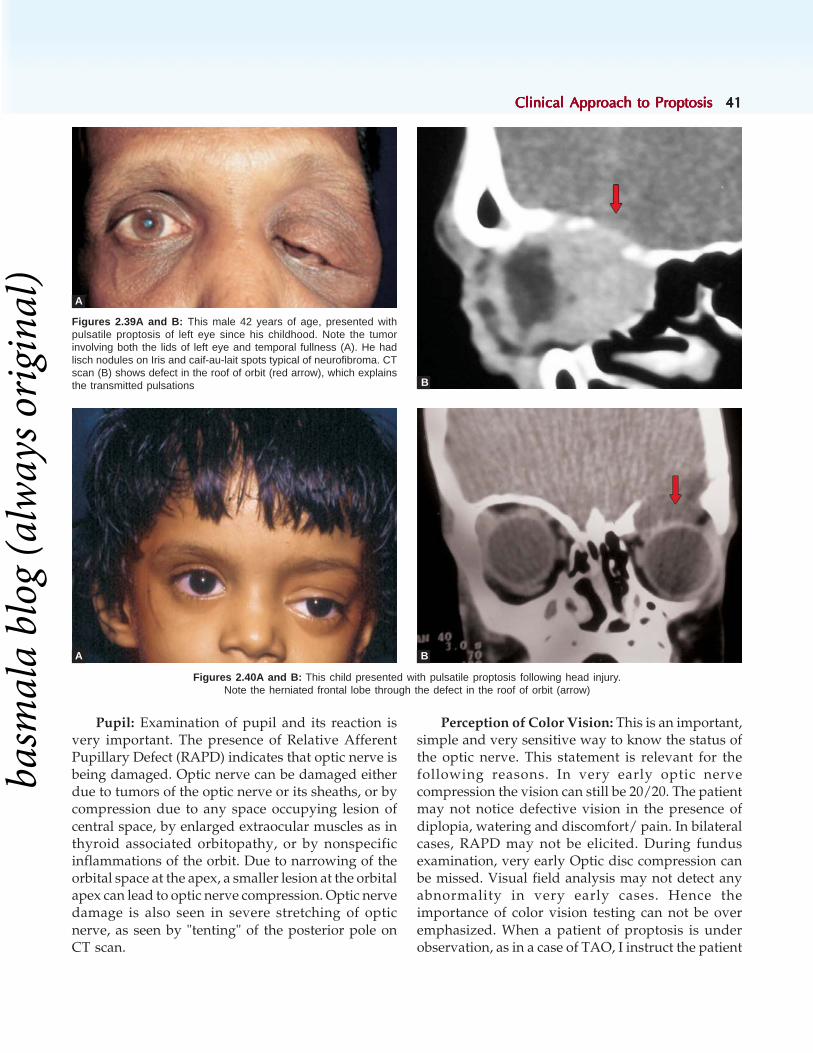
Clinical Approach to ProptosisClinical Approach to ProptosisClinical Approach to ProptosisClinical Approach to ProptosisClinical Approach to Proptosis 4141414141
Figures 2.39A and B: This male 42 years of age, presented withpulsatile proptosis of left eye since his childhood. Note the tumorinvolving both the lids of left eye and temporal fullness (A). He hadlisch nodules on Iris and caif-au-lait spots typical of neurofibroma. CTscan (B) shows defect in the roof of orbit (red arrow), which explainsthe transmitted pulsations
A
B
Figures 2.40A and B: This child presented with pulsatile proptosis following head injury.Note the herniated frontal lobe through the defect in the roof of orbit (arrow)
BA
Pupil: Examination of pupil and its reaction isvery important. The presence of Relative AfferentPupillary Defect (RAPD) indicates that optic nerve isbeing damaged. Optic nerve can be damaged eitherdue to tumors of the optic nerve or its sheaths, or bycompression due to any space occupying lesion ofcentral space, by enlarged extraocular muscles as inthyroid associated orbitopathy, or by nonspecificinflammations of the orbit. Due to narrowing of theorbital space at the apex, a smaller lesion at the orbitalapex can lead to optic nerve compression. Optic nervedamage is also seen in severe stretching of opticnerve, as seen by "tenting" of the posterior pole onCT scan.
Perception of Color Vision: This is an important,simple and very sensitive way to know the status ofthe optic nerve. This statement is relevant for thefollowing reasons. In very early optic nervecompression the vision can still be 20/20. The patientmay not notice defective vision in the presence ofdiplopia, watering and discomfort/ pain. In bilateralcases, RAPD may not be elicited. During fundusexamination, very early Optic disc compression canbe missed. Visual field analysis may not detect anyabnormality in very early cases. Hence theimportance of color vision testing can not be overemphasized. When a patient of proptosis is underobservation, as in a case of TAO, I instruct the patient
basm
ala
blog
(alw
ays o
rigin
al)

4242424242 Surgical Atlas of Orbital DiseasesSurgical Atlas of Orbital DiseasesSurgical Atlas of Orbital DiseasesSurgical Atlas of Orbital DiseasesSurgical Atlas of Orbital Diseases
to look at a bright red colored object with each eyeseparately on every sunday, and to report to meimmediately if he notices any change in brightnessof the color in one eye. If color vision is defective inthe proptosed eye, evaluate very carefully the pupilfor RAPD, do a very detailed fundus evaluation forthe presence of optic disc edema, pallor, presenceof opticociliary shunts, retinal/choroidal striae,retinal detachment. Visual field assessment ismandatory.
PBCT: Limitation of ocular motility in proptosisis mostly due to restrictive pathology as in thyroidassociated orbitopathy (Figures 2.41A and B),Idiopathic orbital inflammation (myositis component)(Figures 2.42A to D), myocysticercosis (Figures 2.43Aand B), and fungal granuloma (Figures 2.44A to C).Another important cause is CCF, wherein therestriction is paralytic in nature (Figures 2.45A toC). Large mass lesions can cause mechanicalrestriction. Limitation of ocular motility following
Figures 2.42A to D: Female 42 yrs., presented with subacute proptosis of left eye with pain and diplopia. Note the congestion of left eye andlimitation of abduction (A). CT scan showed enlarged medial rectus involving the tendon. A diagnosis of idiopathic orbital inflammatory syndromewas made. (Blue arrow) (B) She responded very well to systemic steroids. Note that the conjunctival congestion disappeared (C) andabduction restored to normal within 1 week (D)
A B
C D
Figures 2.41A and B: TAO: restricted elevation due to enlargedinferior rectus (arrow)
A
B
basm
ala
blog
(alw
ays o
rigin
al)

Clinical Approach to ProptosisClinical Approach to ProptosisClinical Approach to ProptosisClinical Approach to ProptosisClinical Approach to Proptosis 4343434343
trauma can be due to soft tissue edema, entrapmentof muscle or its sheath in orbital fracture and rarelydue to injury to the muscle itself. I came across arare cause wherein after trauma; the displaced boneitself caused limitation of motility (Figures 2.46A toD). I routinely quantify the ocular motility in degrees,just like Hirschberg's, so that it is easier to comparethe course of the disease over a long period.
When ocular motility is limited, I routinely doFDT (Forced Duction Test) and differentialtonometry to know whether it is due to restrictivepathology or paralytic. I prefer FDT to FGT(force generation test).In restrictive pathology FDTis positive and you feel resistance when you try tomove the globe in the direction of limitation.Elevation of intraocular pressure by more than 5 mm
Figures 2.43A and B: This young girl presented with proptosis ofleft eye since 4 weeks. She also complained of pain and diplopia.Note the fullness of upper lid, mild congestion of conjunctiva on themedial side and convergent squint. (A) CT scan of orbit revealedmyocysticercosis involving the superior oblique muscle. Note 2 cysts,one involving the muscle belly and the other the reflected tendon ofsuperior oblique (B)
A
B
Figures 2.44A to C: This elderly male, (A) an agricultural worker byoccupation, presented with gross proptosis with frozen globe (B).His vision was PL. Retropulsion was positive. FDT was positive in alldirections. CT scan of the orbit revealed a heterogenous mass lesionoccupying the entire orbit. Note the molding of the lesion to the globe(red arrow), the tenting of posterior pole (blue arrow) and involve-ment of anterior ethmoidal sinus. Histopathology showed it to be afungal granuloma (C)
A
B
C
basm
ala
blog
(alw
ays o
rigin
al)

4444444444 Surgical Atlas of Orbital DiseasesSurgical Atlas of Orbital DiseasesSurgical Atlas of Orbital DiseasesSurgical Atlas of Orbital DiseasesSurgical Atlas of Orbital Diseases
Figures 2.46C and D: Notice the congested blood vessels and the subtle under action of the lateral rectus of right eye (as evidenced bythe over action of medial rectus of left eye). (C) The diagnosis of A-V Fistula is confirmed by the engorged Superior ophthalmic vein (D)
Figures 2.46A and B: Male 27 yrs. presented with proptosis right eye, diplopia on dextroversion and pain of 2 weeks duration. He had aclosed head injury 3 months prior to the onset of proptosis. Notice mild congestion of proptosed right eye (A), better seen in the close-up of theeye (B)
Figures 2.45A to C: This girl presented with diplopia and restrictedmotility following trauma. Note subconjunctival hemorrhage in righteye. (A) FDT was positive. Clinical diagnosis was blowout fractureof floor of orbit with muscle entrapment. But CT scan of orbit revealedfracture roof of orbit with the bony spicule mechanically restrictingthe ocular motility. (B) Elevation restored to normal after removing thebony spicule (C)
B
A
C
A B
C D
basm
ala
blog
(alw
ays o
rigin
al)

Clinical Approach to ProptosisClinical Approach to ProptosisClinical Approach to ProptosisClinical Approach to ProptosisClinical Approach to Proptosis 4545454545
from the base pressure when the patient attempts tomove the globe in the direction of limitation ofmovement is significant. This occurs in restrictivepathology as the globe is compressed between theconstricting muscle and its opponent which can notrelax. Quantify the motility restriction, with PBCT(Prism Bar Cover Test) in different directions.This helps to know what is happening to theextraocular muscles, especially when you have tofollow a patient for a long time like thyroidassociated orbitopathy, and to decide if the patientbenefits with prescription of prisms.
Periorbital Changes: There are numerousperiorbital changes which help us in understandingthe pathology of the lesion and aid in clinicaldiagnosis. Some of these make the diagnosis very
obvious (like the lid retraction of thyroid associatedorbitopathy, Salmon patch of lymphoma, temporalfullness of sphenoid ridge meningioma) whileothers throw light into the disease process and itsactivity.
Temporal Fullness: This is very characteristic ofsphenoid wing meningioma, especially of lateral part(Figure 2.36) Sphenoid wing meningioma of lateralhalf typically presents as proptosis with fullness ofthe temple, which often exhibits pulsations. Sphenoidwing meningioma of medial half presents as proptosiswith restricted ocular motility (Figures 2.47A and B).Another very rare cause of temporal fullness is adumbbell dermoid (Figures 2.48A and B), in whicheyeball can move forwards on mastication due tocontraction of temporalis muscle.
Figures 2.48A and B: Dumble dermoid with temporal fullness. Note the fullness of temple and the medial displacement of the globe (A).CT scan shows dumble dermoid, extending into the temporal region with a big defect (blue arrow) in the lateral wall of the orbit (B)
A B
Figures 2.47A and B: Note proptosed left eye with restricted adduction. All movements other than abduction were restricted (A). CT scan oforbit revealed a heterogenous mass lesion with calcification, involving the temporal lobe, medial half of sphenoid wing. Note the hyperostosisof sphenoid bone (arrow), suggestive of meningioma (B)
A B
basm
ala
blog
(alw
ays o
rigin
al)

4646464646 Surgical Atlas of Orbital DiseasesSurgical Atlas of Orbital DiseasesSurgical Atlas of Orbital DiseasesSurgical Atlas of Orbital DiseasesSurgical Atlas of Orbital Diseases
Lid changes: The important lid changes includelid retraction, lid lag, sinuous lid margin, tumors ofthe lid (primary malignant tumors of the lid withsecondary orbital extension, primary vascularneoplasia with components of orbit and lid, ormultiple tumors involving the lids and orbit likeneurofibromatosis (Von Recklinghausen)).
Lid Retraction is the most common lid changeseen in thyroid associated orbitopathy. It can involveboth upper and lower eyelids. It is measured byrecording MRD values and subtracting the normalvalues (4 mm and 5 mm) from it. The lid retractionof TAO is due to over action of sympathetic system(Müller's muscle) and can also be due to hypotropiaand limitation of elevation, so that with the attemptto move the globe, the upper lid goes up and lidretraction worsens. The lid retraction can beunilateral or bilateral. As per the NOSPECSclassification, the lid retraction is classified as follows:mild if the lid margin is at limbus, moderate if up to
4 mm of sclera is seen and severe if > 4 mm of sclerais seen (Figures 2.49A to C). Usually in TAO, thecontor of lid is altered in that the highest point ofthe upper lid is at the lateral part (lateral flare).
Lid lag: Lid lag is the second most common lidchange in thyroid orbitopathy. It can be unilateralor bilateral. Lag-ophthalmos is a very importantfinding one has to look for. It can lead to exposurekeratopathy which in the early stages can presentwith pain and photophobia (Figures 2.50A and B).There may be associated defective vision. If thelagophthalmos is severe and prolonged, it can leadto frank corneal ulcer and even perforation. Henceit is very important to detect lag ophthalmos as earlyas possible and take remedial measures. To detectearly lagophthalmos, look from below (Figures 2.51Aand B). Severe lagophthalmos is usually seen in verygross proptosis which can be due to a very largebenign tumor, but more often due to faster growinglesions like metastatic lesions (Figures 2.52A to C).
Figures 2.49A to C: Lid retraction three grades in thyroid associated orbitopathy. Mild-upper lid is at the limbus (A)Moderate 2 mm of scleral show (B) More than 4 mm of scleral show (C)
A
B C
basm
ala
blog
(alw
ays o
rigin
al)

Clinical Approach to ProptosisClinical Approach to ProptosisClinical Approach to ProptosisClinical Approach to ProptosisClinical Approach to Proptosis 4747474747
Figures 2.52A to C: Mild lagophthalmos in a case of TAO (A), severe lagophthalmos in metastatic orbital lesion from carcinoma of thyroid(B). The elderly female (a case of hydatid cyst of orbit) had anterior staphyloma in her left eye due to perforated corneal ulcer (C)
A
B C
Figures 2.51A and B: Mild lagophthalmos may not be detected (A) unless examined from below (B)
A B
Figures 2.50A and B: Lag-lag: Unilateral (left eye) and bilateral in thyroid associated orbitopathy. Note a small corneal lesion at 6 O’ clock position due to exposure
A B
basm
ala
blog
(alw
ays o
rigin
al)
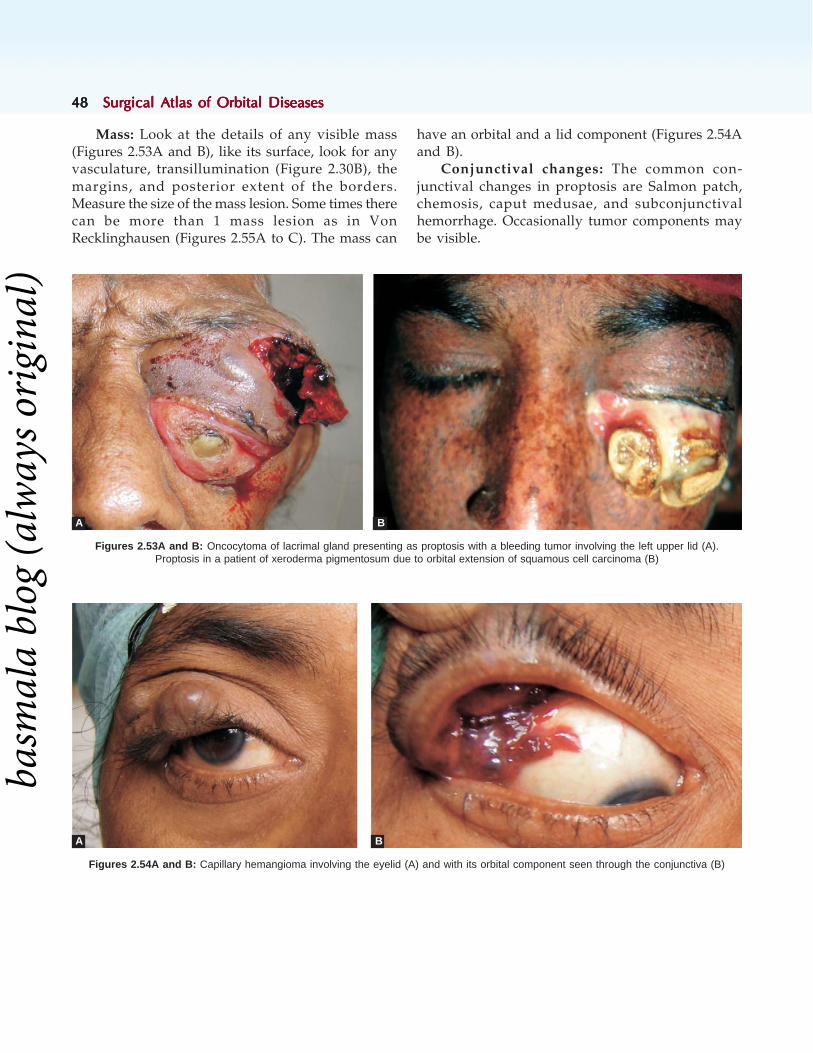
4848484848 Surgical Atlas of Orbital DiseasesSurgical Atlas of Orbital DiseasesSurgical Atlas of Orbital DiseasesSurgical Atlas of Orbital DiseasesSurgical Atlas of Orbital Diseases
Mass: Look at the details of any visible mass(Figures 2.53A and B), like its surface, look for anyvasculature, transillumination (Figure 2.30B), themargins, and posterior extent of the borders.Measure the size of the mass lesion. Some times therecan be more than 1 mass lesion as in VonRecklinghausen (Figures 2.55A to C). The mass can
have an orbital and a lid component (Figures 2.54Aand B).
Conjunctival changes: The common con-junctival changes in proptosis are Salmon patch,chemosis, caput medusae, and subconjunctivalhemorrhage. Occasionally tumor components maybe visible.
Figures 2.54A and B: Capillary hemangioma involving the eyelid (A) and with its orbital component seen through the conjunctiva (B)
B
Figures 2.53A and B: Oncocytoma of lacrimal gland presenting as proptosis with a bleeding tumor involving the left upper lid (A).Proptosis in a patient of xeroderma pigmentosum due to orbital extension of squamous cell carcinoma (B)
A B
A
basm
ala
blog
(alw
ays o
rigin
al)

Clinical Approach to ProptosisClinical Approach to ProptosisClinical Approach to ProptosisClinical Approach to ProptosisClinical Approach to Proptosis 4949494949
Figures 2.56A to C: Malignant lid tumors, when neglected, can extend into orbit as seen with the Meibomian Carcinoma lower eyelid ofright eye (A). Squamous cell carcinoma of right upper lid with orbital extension demonstrated in the CT scan (B and C)
Salmon patch is a pinkish, smooth mass, typicallyseen in the subconjunctival plane, either at the limbus,or fornix (Figures 2.57A to C). It is very typical oflymphoma. The lesion at the fornix, which is morecommonly seen, is due to the extension of the tumor,as it moulds to the adjacent globe and extendsanteriorly along the sub-tenon's plane and can extendupto the limbus. The isolated limbal mass is due toproliferation of the lymphocytes.
Caput medusae: Engorged blood vessels, typicallyaround the limbus are seen in AV malformations andfistula (Figures 2.58A and B). The engorgement isusually due to increased venous pressure due to A-V communication. It can be very subtle and can beeasily over looked by the novice. In high flow fistulathe caput medusae can be very significant and pointtowards the diagnosis. Some times it can beassociated with chemosis of conjunctiva.
Figures 2.55A to C: Neurofibromatosis can present either as Von Recklinghausen disease with multiple tumors on the eyelid (A),or as plexiform neurofibroma (B) involving the lid and orbit as seen in the CT scan (C)
A B C
A
B C
basm
ala
blog
(alw
ays o
rigin
al)

5050505050 Surgical Atlas of Orbital DiseasesSurgical Atlas of Orbital DiseasesSurgical Atlas of Orbital DiseasesSurgical Atlas of Orbital DiseasesSurgical Atlas of Orbital Diseases
Chemosis: Chemosis is divided into 3 grades,grade 1 is when the chemosed conjunctiva covers upto half the lid margin, grade 2 when it covers theentire lid margin and grade 3 when it overhangs thelid margin (Figures 2.59A to C). Conjunctival
chemosis can be because of active infections andinflammations like orbital cellulitis, orbital abscess,thyroid orbitopathy, or due to high flow arterio-venous communications, lymphangioma (Figures2.60A to C)
Figures 2.59A to C: Chemosis grade1 (covers upto half of lid margin) (A), grade 2 (covers upto entire length of lid margin) (B)and grade3 (overhangs the lid margin) (C)
A B C
Figures 2.58A and B: Caput medusae due to CCF (A). Note the grossly engorged superior ophthalmic vein(blue arrow) in the CT scan. Compare its size with the normal (red arrow)
A B
Figures 2.57A to C: Salmon patches of varying degrees presenting at the fornix and some extending up to limbus.Notice the typical color and also varying degrees of vasculature above them
A B C
basm
ala
blog
(alw
ays o
rigin
al)

Clinical Approach to ProptosisClinical Approach to ProptosisClinical Approach to ProptosisClinical Approach to ProptosisClinical Approach to Proptosis 5151515151
Subconjunctival hemorrhage is an importantfeature of lymphangioma, leukemia, trauma andbleeding diathesis. In a case of trauma, apartfrom associated ocular and systemic injuries,look for RAPD, retrobulbar hemorrhage andorbital fractures. If retrobulbar hemorrhage ispresent, do canthotomy and cantholysis (Figures2.61A and B).
Val salva: Increase in proptosis after Val salvamaneuver is typically due to Orbital Varix (Figures2.62A to C)
Examination of nasal cavity and oral cavity ismandatory, especially in the presence of paranasalsinus involvement (Figures 2.63A and B). It is mucheasier to get a biopsy done from these lesions toknow the nature of the lesion.
Other important periocular changes involvingcornea, ocular motility, pupil, visual acuity, fundusexamination, color vision were already mentionedearlier.
Palpation: Palpate the orbital margin, look forany palpable mass lesion and assess the orbitalpressure by retropulsion. While palpating the orbit,ask the patient to look in the direction in which youare palpating, so that the orbital septum is relaxed.Use the pulp of your finger to palpate the orbit forany mass. If a mass is palpable, note its consistency,tenderness, extent, surface, reducibility, posteriorextent. Assess the orbital tone by gently applyingpressure over the closed eyelids and pushing theglobe into the orbit. Compare the resistance offeredby the proptosed eye with that of the normal. Fromthis you can know if the orbital lesion is compressibleor unyielding mass.
Auscultation: In pulsatile proptosis, auscultatewith the bell of a stethoscope for any bruit. It istypically heard in high flow fistula.
Common causes of bilateral proptosis in childrenare congenital skeletal deformities, followed bylymphoma, leukemia and other lymphoproliferative
Figures 2.60A to C: Grade 3 chemosis in orbital cellulitis (A), carotid-cavernous fistula (B) and a case of lymphangioma (C)
A B C
Figures 2.61A and B: Acute proptosis with subconjunctival hemorrhage, and surgical emphysema following trauma (A). Note that theconjunctiva became flat after 2 snips were made into it to permit the escape of air. Lateral canthotomy and cantholysis was performed to drainthe retrobulbar hemorrhage (B)
A B
basm
ala
blog
(alw
ays o
rigin
al)

5252525252 Surgical Atlas of Orbital DiseasesSurgical Atlas of Orbital DiseasesSurgical Atlas of Orbital DiseasesSurgical Atlas of Orbital DiseasesSurgical Atlas of Orbital Diseases
Figures 2.62A to C: Female 21 years presented with proptosis of right eye since her childhood (A) She gives the history that the proptosisgets worse when ever she bends. Notice the increase in the amount of proptosis, fullness of upper lid, (B) and increasein the volume of the vascular component in a case of orbital varix (C)
Figures 2.63A and B: Nasal examination and oral examination can show the extension of lesions, especially if they arise from the Maxillarysinus. Note the visible mass in the left nostril (A) and the swelling of hard palate (B) which is the floor of maxillary sinus
A B C
A B
disorders. Other important secondary orbital lesionsthat cause bilateral involvement, though notnecessarily at the same time, include squamous cellcarcinoma of the conjunctiva associated withxeroderma pigmentosum, and neglected retino-blastoma. The most common cause of unilateralproptosis in children is dermoid cyst, followed byhemangiomas. Rhabdomyosarcoma is the mostcommon malignant lesion of pediatric age group. Inadults, the most common cause of proptosis, eitherunilateral or bilateral is thyroid associatedorbitopathy. Nonspecific orbital inflammation,granuloma (especially fungal granuloma involvingfrontoethmoid sinuses) and lymphomas are the othercommon bilateral lesions of orbit. However, thefrequency of these conditions can change from placeto place, depending upon the disease patterns of thoseareas. For example in India we see a lot of cases of
orbital myocysticercosis, which many of you in thewestern world might not have come across. Similarly,we rarely come across Wagener's granulomatosis,which is fairly common in the west. The diseasepresentations also can vary in different parts of theworld. When compared to the west, we in South Indiavery rarely come across severe thyroid orbitopathy.The incidence of infection due to tuberculosis is onthe rise because of HIV. So is the case with lymphoma.Thus the spectrum of orbital diseases is varied indifferent parts of the world (Table 2.1). With a goodknowledge of the disease patterns of the region anda good clinical work-up, a reasonable clinicaldiagnosis can be made most of the times. Advancesin investigative modalities like imaging (CT, MRI),histopathology (FNAC, IHC, Squash) come to ouraid to make a very accurate diagnosis, which goes along way in managing the case.
basm
ala
blog
(alw
ays o
rigin
al)

Clinical Approach to ProptosisClinical Approach to ProptosisClinical Approach to ProptosisClinical Approach to ProptosisClinical Approach to Proptosis 5353535353
Table 2.1: Etiology of proptosis in comparision with western literature (Incidence in percentage)Lesion Subrahmanyam Rootman Hendserson Richard Dallow
1578 3919 1376 1825
Systemic 12.2% 51.7% 3.8% 32 %Inflammatory 37.1% 8.6% 4.4% 13%Trauma 4.9% 4.9% — 2%Congenital 2.8% 4.9% 2.8% 2%Primary neoplasia 16.6% 14.3% 48.1% 6%Secondary neoplasia 1.9% 2.3% 19.5% 2%Metastatic lesions 1.3% 1.5% 8.1% 3%Vascular lesions 3.0% 4.6% 4.7% 6%Others 20.2% 7.2% 8.6% 34%
This table shows considerable difference in the etiology of proptosis, when I compared my series with 3 large series reportedfrom "clinical practice". I am not comparing with the reported series from pathology records, which have a strong bias towardsneoplastic lesions. Hence knowledge of disease pattern for the area, from which the patient has come, is very important. InIndia we come across compressive optic neuropathy due to thyroid associated orbitopathy very rarely, whereas at vancouverI noticed that its prevalence among the locals of Indian origin is similar to the caucasians. It may be due to the gross differencein the climatic conditions or the life style and needs to be investigated.
Evaluation of a Case of Proptosis
Name: Age: Sex:
Occupation: Address:
Regn. Number
Presenting complaints:
History of present illness:
Proptosis : Onset and Progression
Defective vision:
Double vision:
Pain scoring:
Trauma history:
Other history: (circle the one relevant): Thyroiddisease (Wt loss/gain, tremors, neck swellings,palpitations, others), sinusitis, aggravation withrespiratory infections, others .
Treatment historyPast History:(Circle the ones relevant)Thyroid disease HIV Any Medications /
anticoagulantsTuberculosis Diabetes Any SurgeriesSyphilis Hypertension Any known drug
reactions : List them
Family history:Personal history:General systemic examination:(circle the onesrelevant)Pulse: Pallor FrecklesBP: Icterus Neck SwellingsRR: Lymphadenopathy TremorsTemperature: Caif au lait spots
CVS:Respiratory System:Abdominal Examination:ENT Examination:ba
smal
a bl
og (a
lway
s orig
inal
)

5454545454 Surgical Atlas of Orbital DiseasesSurgical Atlas of Orbital DiseasesSurgical Atlas of Orbital DiseasesSurgical Atlas of Orbital DiseasesSurgical Atlas of Orbital Diseases
RE LEVisual acuityRefractionColor Vision:Visual fields (confrontation)Proptosis Proper:
Inspection:Compensatory head posture:Facial symmetry:Ocular symmetry:Any apparent mass description:
Eyelids• Position (MRD1 and MRD2):• Fullness• Contour• Movements/Lid Lag• Lagophthalmos• Mass lesion (describe if present)• Palpebral fissure height
Proptosis• Pulsations• MEASUREMENTS:• Hertel's (B.R……mm)• Horizontal• Vertical• Valsalva maneuver:• Periocular changes:
ConjunctivaCorneaAnterior chamberPupilLensFundusOcular motilityCover testPBCTIOPPalpation:Bony regularity:Temperature :Tenderness:Crepitus:Description of Mass:Thrill/ Reducibility:Retropulsion:
basm
ala
blog
(alw
ays o
rigin
al)
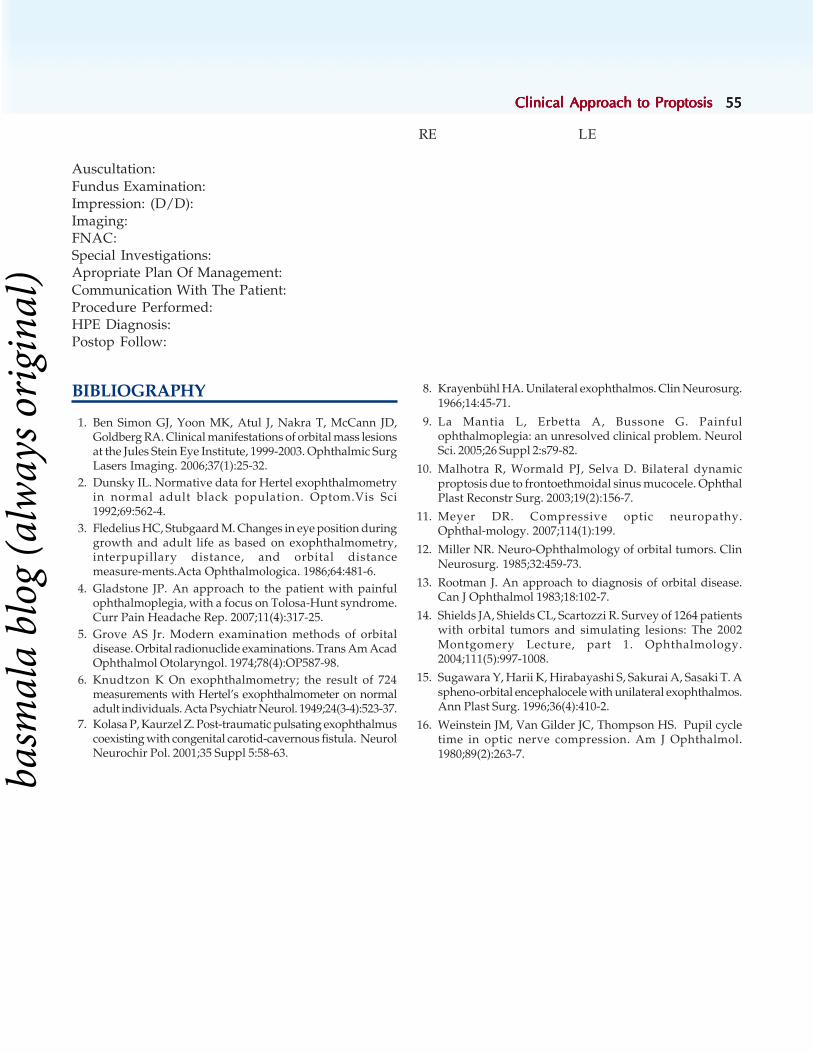
Clinical Approach to ProptosisClinical Approach to ProptosisClinical Approach to ProptosisClinical Approach to ProptosisClinical Approach to Proptosis 5555555555
BIBLIOGRAPHY
1. Ben Simon GJ, Yoon MK, Atul J, Nakra T, McCann JD,Goldberg RA. Clinical manifestations of orbital mass lesionsat the Jules Stein Eye Institute, 1999-2003. Ophthalmic SurgLasers Imaging. 2006;37(1):25-32.
2. Dunsky IL. Normative data for Hertel exophthalmometryin normal adult black population. Optom.Vis Sci1992;69:562-4.
3. Fledelius HC, Stubgaard M. Changes in eye position duringgrowth and adult life as based on exophthalmometry,interpupillary distance, and orbital distancemeasure-ments.Acta Ophthalmologica. 1986;64:481-6.
4. Gladstone JP. An approach to the patient with painfulophthalmoplegia, with a focus on Tolosa-Hunt syndrome.Curr Pain Headache Rep. 2007;11(4):317-25.
5. Grove AS Jr. Modern examination methods of orbitaldisease. Orbital radionuclide examinations. Trans Am AcadOphthalmol Otolaryngol. 1974;78(4):OP587-98.
6. Knudtzon K On exophthalmometry; the result of 724measurements with Hertel’s exophthalmometer on normaladult individuals. Acta Psychiatr Neurol. 1949;24(3-4):523-37.
7. Kolasa P, Kaurzel Z. Post-traumatic pulsating exophthalmuscoexisting with congenital carotid-cavernous fistula. NeurolNeurochir Pol. 2001;35 Suppl 5:58-63.
8. Krayenbühl HA. Unilateral exophthalmos. Clin Neurosurg.1966;14:45-71.
9. La Mantia L, Erbetta A, Bussone G. Painfulophthalmoplegia: an unresolved clinical problem. NeurolSci. 2005;26 Suppl 2:s79-82.
10. Malhotra R, Wormald PJ, Selva D. Bilateral dynamicproptosis due to frontoethmoidal sinus mucocele. OphthalPlast Reconstr Surg. 2003;19(2):156-7.
11. Meyer DR. Compressive optic neuropathy.Ophthal-mology. 2007;114(1):199.
12. Miller NR. Neuro-Ophthalmology of orbital tumors. ClinNeurosurg. 1985;32:459-73.
13. Rootman J. An approach to diagnosis of orbital disease.Can J Ophthalmol 1983;18:102-7.
14. Shields JA, Shields CL, Scartozzi R. Survey of 1264 patientswith orbital tumors and simulating lesions: The 2002Montgomery Lecture, part 1. Ophthalmology.2004;111(5):997-1008.
15. Sugawara Y, Harii K, Hirabayashi S, Sakurai A, Sasaki T. Aspheno-orbital encephalocele with unilateral exophthalmos.Ann Plast Surg. 1996;36(4):410-2.
16. Weinstein JM, Van Gilder JC, Thompson HS. Pupil cycletime in optic nerve compression. Am J Ophthalmol.1980;89(2):263-7.
RE LE
Auscultation:Fundus Examination:Impression: (D/D):Imaging:FNAC:Special Investigations:Apropriate Plan Of Management:Communication With The Patient:Procedure Performed:HPE Diagnosis:Postop Follow:
basm
ala
blog
(alw
ays o
rigin
al)

5656565656 Surgical Atlas of Orbital DiseasesSurgical Atlas of Orbital DiseasesSurgical Atlas of Orbital DiseasesSurgical Atlas of Orbital DiseasesSurgical Atlas of Orbital Diseases
Subrahmanyam Mallajosyula, Ravi Varma
Imaging a Case ofImaging a Case ofImaging a Case ofImaging a Case ofImaging a Case ofProptosis: CT and MRIProptosis: CT and MRIProptosis: CT and MRIProptosis: CT and MRIProptosis: CT and MRI
“Proptosis is a Pandora's box” was the most oftenquoted sentence in the past, and it was rightly so,since "surprises on the operation table" were quitefrequent. The surprises could be in the form ofpathology, localization and extent of the lesion. Theseproblems were too frequent for the occasional orbitalsurgeon. Hence, many a time in the past it was theteam effort—a team of neurosurgeon andophthalmologist—that used to perform surgery onevery case of proptosis. Advances in imagingtechniques have changed the scenario completely.With the advent of CT scan and later MRI we knowthe exact location of the lesion, the nature of the lesion(tumor or a cyst, encapsulated/ infiltrating, highlyvascular /less vascular, benign/malignant/metastatic). We can also very accurately predict thehistological nature of the lesion like glioma of theoptic nerve/meningioma of the optic nerve sheath/sphenoid ridge meningioma/ thyroid orbitopathy/cavernous hemangioma/ lymphangioma/ myocy-sticercosis/ myositis/lymphoma, etc. Hence thesurprises in proptosis were very rare now. After athorough clinical evaluation and imaging with CT,most often we know the nature and location of thelesion, which enables us to manage proptosis in asystematic way. We strongly believe that theadvances in imaging technologies have not only madethe diagnosis and management of proptosis morescientific, they have revived interest in thesubspecialty of orbital services.
The globe, conjunctiva and optic disc are theorbital structures amenable for direct examination.Pathology involving the rest of the orbital structures
needs imaging studies for optimal evaluation. Severalimaging techniques such as plain radiography,ultrasound, color Doppler, computed tomography(CT) and magnetic resonance imaging (MRI) areavailable for imaging orbital pathology. Eachtechnique has its own advantages and dis-advantages, and the information obtained from thesestudies is often complementary.
Plain radiography has been the only investigationavailable for orbital imaging for most of the lastcentury. Now, CT and MRI have largely replacedradiography, and skull X-rays are now performedonly in selected cases of facial fractures and to screenfor intraocular metallic foreign bodies before an MRexamination. Sonography is used largely in theevaluation of intraocular structures. Large masslesions in the orbit can also be visualized andcharacterized on sonography. Ultrasound combinedwith Duplex Doppler plays an important role in thenoninvasive evaluation of vascular pathologyinvolving the orbit. It can differentiate low flowlesions from high flow arteriovenous malformations.Though sonography is convenient and non-invasive,it suffers from limitations in the form of suboptimalvisualization of the posteriorly placed structures,nonvisualization of intracranial pathology and needfor expertise on part of the examiner.
The most widely used radiological investigationfor evaluation of the orbit is CT scan. It has theadvantages of being widely available, fast,inexpensive and relatively easy to interpret. Thetechnique is based on differential attenuation ofX-rays by tissues, where denser tissues attenuate
3C H A P T E R
basm
ala
blog
(alw
ays o
rigin
al)

Imaging a Case of Proptosis: CT and MRIImaging a Case of Proptosis: CT and MRIImaging a Case of Proptosis: CT and MRIImaging a Case of Proptosis: CT and MRIImaging a Case of Proptosis: CT and MRI 5757575757
more X-rays. Tissues can be characterized by theirattenuation values (also called Hounsfield units (HU)- named after the inventor of CT). The retro-orbitalfat imparts a natural contrast that aids in delineationof normal anatomy as well as pathology. On theHounsfield unit scale, air is defined as –1000 HU,pure water as 0 HU, and dense cortical bone as +1000HU. Retro-orbital fat usually measures –120 to –50HU, cerebrospinal fluid measures 0 to +10 HU, extra-ocular muscles measure +40 to +50 HU and brainmeasures +35 to +45 HU. CT scans of the orbit arebest obtained before and after intravenousadministration of iodinated contrast medium. Thinsections (2-3 mm) are required to delineate thepathology and differentiate it from the normal orbitalstructures. Imaging in both axial and coronal planesmay be required to optimally evaluate orbitalpathology. The images can be viewed in differentwindow settings to evaluate structures such as thesoft tissues on bony structures.
Modern day spiral CT and multidetector CTtechnology permit acquisition of the imaging data asa volume, within a few seconds so as to minimizemovement artifacts. It is now possible to acquireimages in several phases during and after intravenousadministration of contrast medium, that may beinstrumental in diagnosing vascular and other similarabnormalities of the orbit. In addition, postprocessing of spiral CT data yields extremely highresolution multiplanar reconstructions and 3-dimensional images, without the need for additionalexposure to radiation. CT scan images are taken withsoft tissue windows (to study the details of the globeand the soft tissue lesion) and bone windows (givethe details of the bone).
Though CT scan is considered as the work-horseof orbital imaging, it suffers from severaldisadvantages such as relatively low tissue contrastas compared to MRI, and severe degradation ofimage quality by dental fillings. Dose of radiation tothe lens, which is most sensitive organ in the bodyto radiation exposure, is a concern.
Unlike radiography and CT scan, MR imagingdoes not use ionizing radiation. Image productionin MRI is based on measurement of relaxationproperties of protons after excitation withradiofrequency energy. By altering the parametersof data acquisition, we can obtain several image
contrasts such as T1 weighted images, T2 weightedimages, proton density images, inversion recoveryimages, fat saturated images and gradient recalledimages.
MR imaging has several advantages over CT scansuch as superior soft tissue contrast, directmultiplanar capability and excellent visualization ofthe optic nerve and intracranial pathology.Availability of higher field strength magnets andsurface coils have significantly improved the imagequality in orbital imaging. However, the longacquisition times that degrade the image quality dueto movement artifacts and poor visualization of bonydetails and fractures still remain a significantimpediment in the use of MRI for orbital evaluation.Furthermore, MRI is contraindicated in patients withcardiac pacemakers and defibrillators, neurosti-mulators, metallic foreign bodies in the eye, and otherferromagnetic implants within the body.
Though, the signal pattern is highly dependantupon the specific imaging parameters used duringacquisition, in general the signal patterns of variousorbital and other related structures can be describedas follows:
T1 weighted T2 weighted Fat suppressed T1
Bone-cortex No signal No signal No signalBone-marrow Bright Bright DarkFat Very bright Bright Very darkMuscle Gray Gray GrayAqueous/ Dark Bright DarkVitreousLens Gray Gray GraySclera Gray Gray GrayCSF Dark Bright DarkBlood vessels No signal No signal No signalAir No signal No signal No signal
Currently, the information obtained on imagingstudies is complementary. The choice of imagingstudy should be based on the clinical presentationand the specific pathology being suspected. Further,the imaging techniques can be modified to specificallyaddress the pathology in question. Discussion withthe radiologist performing the imaging study goes along way in ensuring optimal imaging of the orbit.While ordering for the imaging, the decision dependsupon the nature of lesion. However I (MS), veryrarely, if at all ask for a plain X-ray of orbit. The
basm
ala
blog
(alw
ays o
rigin
al)

5858585858 Surgical Atlas of Orbital DiseasesSurgical Atlas of Orbital DiseasesSurgical Atlas of Orbital DiseasesSurgical Atlas of Orbital DiseasesSurgical Atlas of Orbital Diseases
information obtained from a plain X-ray is verylimited and grossly inadequate to understand thenature of the lesion and plan management(Figure 3.1).
My most preferred imaging modality is CT scanof Orbit, 2 mm slices of axial, coronal sections withsagittal reconstruction, with or without contrast.Contrast studies are ordered only when vascular ortumor pathology is suspected clinically. Otherwiseplain study alone is ordered. For example, in thyroidorbitopathy, plain study is asked for, contrast studyis not indicated. My preference for CT is because ofits easy availability, cost to the patient, easyinterpretation. I ask for an MRI only when I amdealing with a lesion of optic nerve or its sheathwhich account for 2 to 3% of all cases of proptosis.
Evaluation of a CT scan of orbit: Though thesoft tissue lesion attracts our attention, it is prudentto read the CT scan image in a systematic method,so that we don't miss any subtle changes, whichprovide very useful information.
The level of the scan: The orbital scans arenormally taken in a sequential order, from belowupwards for axial scans and from anterior toposteriorly in coronal scans. To know the level of
the scan in the axial sections, remember that themedial walls of the orbit are parallel in the midorbit(Figure 3.2). If they were not parallel, the level ofthe picture is either lower or upper. Look at anteriorand posterior parts of the picture. Anteriorly a flatnasal root and posteriorly the presence of brain tissueindicate that the scan was of upper part of the orbit(Figure 3.3). A prominent nose anteriorly, and thepresence of oropharynx posteriorly indicate that thepicture was of lower part of orbit (Figure 3.4). Theimportant structures of orbit at various levels areshown in Figures 3.5, 3.6 and 3.7.
Figure 3.3: Note the flat nasal root anteriorly
Figure 3.1: X-ray picture of orbit of a patient of proptosis. Theinformation obtained is very little. It is impossible to predict the natureof the lesion, and its exact location
Figure 3.2: Mid level: Note the medial
basm
ala
blog
(alw
ays o
rigin
al)

Imaging a Case of Proptosis: CT and MRIImaging a Case of Proptosis: CT and MRIImaging a Case of Proptosis: CT and MRIImaging a Case of Proptosis: CT and MRIImaging a Case of Proptosis: CT and MRI 5959595959
Figure 3.6: Axial CT scan at mid level of orbit showingimportant structures
Figure 3.5: Axial CT scan at lower level of orbitshowing important structures
Figure 3.4: Note the prominent nose anteriorly (blue arrow) andthe or opharynx posteriorly (yellow arrow). Normal anatomy of orbiton CT
Figure 3.7: Axial CT scan at upper level of orbit showingimportant structures
Common mistakes: We wish to discuss some ofthe common mistakes committed by the residentswhile interpreting the CT scan of the orbits. Theyare described with Figures 3.8 to 3.10.
How to read?• Anatomical location /level• Bony orbit
• Eye ball• Extra ocular muscles• Optic nerve• Soft tissue Lesions
— Borders / consistency• Hounsfield units• Contrast enhancement
basm
ala
blog
(alw
ays o
rigin
al)

6060606060 Surgical Atlas of Orbital DiseasesSurgical Atlas of Orbital DiseasesSurgical Atlas of Orbital DiseasesSurgical Atlas of Orbital DiseasesSurgical Atlas of Orbital Diseases
Figure 3.8: Discontinuity of optic nerve: Due to the sinuous course ofthe optic nerve, axial sections often show an apparent discontinuityof the optic nerve (Yellow arrow), which was misinterpreted in casesof trauma as avulsion by the residents
Figure 3.9: Cystic lesion abutting optic nerve: You can see a “cysticlesion” (yellow arrow) temporal to optic nerve (green arrow). Re-member that the optic nerve does not emerge from the most posteriorpart of the globe. The apparent "cyst" is in fact the eyeball itself! Thispatient had glioma of the right optic nerve (orange arrow)
Figure 3.11: Look at the bony “Excavation” with very smooth margins(yellow arrow) of the medial wall. This is due to increased orbitalpressure exerted by the lesion which is in contact with the bone. Thisdenotes a "chronic course” of a "benign lesion"
Bony Orbit
Excavation or molding (Figure 3.11) erosion, (Figures3.12 to 3.14) absence (Figure 3.15), hyperostosis(Figures 3.16A and B, 3.17) are the common changesin bony orbit.
Figure 3.12: Bony erosion and hypertrophy in a case of fungalgranuloma of orbit. Look at the “irregular” borders of the bone incomparison to the smooth borders of the excavation (Figure 3.11)Bony erosion is due to infiltration of the bone. It is commonly seen inmalignant lesions or fungal infections
Figure 3.10: Enlarged Optic canal is how most of the residents inter-preted A which is in fact enlarged inferior orbital fissure. Compare itssize with normal inferior orbital fissure (B) Remember that optic canalis seen at the level of anterior clinoid processes and you will be ableto see superior orbital fissure lateral to optic canal (Figure 3.6).
basm
ala
blog
(alw
ays o
rigin
al)

Imaging a Case of Proptosis: CT and MRIImaging a Case of Proptosis: CT and MRIImaging a Case of Proptosis: CT and MRIImaging a Case of Proptosis: CT and MRIImaging a Case of Proptosis: CT and MRI 6161616161
Figure 3.13: Sino-orbital mucormycosis. Note the involvement of sinus (yellow arrow),Orbit (Blue arrow) and brain (red arrow) with erosion of roof and medial walls of orbit
Figure 3.14: Fungal granuloma of the maxillary sinus with bony ero-sion (yellow arrows) Leading to extension into the ethmoid sinus,orbit and cheek Figure 3.15: Bony dehiscence: Dumbbell Dermoid involving maxillary
sinus and orbit. Note the absence of floor (yellow arrow). Note alsothe smooth excavation of the maxillary sinus and its expansion
Figures 3.16A and B: Note the hypertrophy (hyperostosis) of the Sphenoid bone (yellow arrow) In a case of sphenoidridge meningioma with extension to temporal region (green arrow). Note the intracranial component (red arrow)
BA
basm
ala
blog
(alw
ays o
rigin
al)

6262626262 Surgical Atlas of Orbital DiseasesSurgical Atlas of Orbital DiseasesSurgical Atlas of Orbital DiseasesSurgical Atlas of Orbital DiseasesSurgical Atlas of Orbital Diseases
Bony Lesions
Bony lesions include Osteoma (Figures 3.18A to C),fibrous dysplasia (Figure 3.19), Ossifying fibroma(Figures 3.20A and B). Subperiosteal hemorrhage(Figure 3.21) and subperiosteal abscess (Figures 3.22Ato C) are other common lesion frontoethmoidalmucoceles (Figures 3.23A and B), Angiofibroma fromsinuses (Figures 3.24A and B) are also seen fairlycommon. Fractures (Figures 3.25A and B, 3.26A andB) are quite frequent.
Figure 3.17: Hyperostosis and erosion of the sphenoid (yellow arrow)in a case of sphenoid ridge meningioma with intracranial component(red arrow), temporal fossa (green arrow) and orbital involvement(Blue arrow)
Figures 3.18A to C: Osteoma of the ethmoid bone involving the entire ethmoid, and leading to optic nerve compression. Seethe uniformly dense tumor with Hounsfield values similar to bone in both soft tissue windows (A) and bone window (B). Thetumor was excised through a modified Lynch incision (C)
A
B C
basm
ala
blog
(alw
ays o
rigin
al)

Imaging a Case of Proptosis: CT and MRIImaging a Case of Proptosis: CT and MRIImaging a Case of Proptosis: CT and MRIImaging a Case of Proptosis: CT and MRIImaging a Case of Proptosis: CT and MRI 6363636363
Figure 3.19: Fibrous dysplasia usually involves flat bones of face and hence orbital involvement is not uncommon. Imaging showsexpansion of the bone with thinning of the overlying cortex. A ‘ground-glass’ appearance is common on CT
Figures 3.20A and B: Ossifying fibroma Imaging shows a well circumscribed lesion eroding the bone with a scleroticmargin (yellow arrow) and foci of internal calcification (green arrow).
Figure 3.21: Sub-periosteal hemorrhage: Subperiosteal hemorrhage is less common than subperiosteal abscess. The periorbita can be seenclearly as a thickened membrane (yellow arrow). Note that the sinuses are clear in this film, unlike in subperiosteal abscess (red arrow) wherethe sinuses are involved (Figure 3.22)
A B
basm
ala
blog
(alw
ays o
rigin
al)

6464646464 Surgical Atlas of Orbital DiseasesSurgical Atlas of Orbital DiseasesSurgical Atlas of Orbital DiseasesSurgical Atlas of Orbital DiseasesSurgical Atlas of Orbital Diseases
Figures 3.22A to C: Sub-periosteal abscess, infection extending from the Fronto-ethmoidal sinuses (red arrow). Note the congestion andedema of the lids and peri-orbital region, chemosis and congestion of the conjunctiva apart from the eccentric proptosis. Periorbita (yellowarrow) could be well made out
Figures 3.23A and B: Fronto-ethmoidal mucocele is a very common cause of eccentric proptosis in which the globe is pushed down and out.You can see a very gross eccentric proptosis of left eye with fullness in the superomedial quadrant. The CT Scan shows a grossly enlargedfrontal sinus with mucosal thickness (yellow arrow)
Figures 3.24A and B: Angio fibroma arising from sinuses is not very rare. Note the huge tumor mass. Occupying the entire maxillary sinus,and distorting the orbital cavity. Its extension into the nose and the fullness of left cheek could be made-out. Also note the severe eccentricproptosis and corneal leucoma due to exposure
A B C
A B
A B
basm
ala
blog
(alw
ays o
rigin
al)

Imaging a Case of Proptosis: CT and MRIImaging a Case of Proptosis: CT and MRIImaging a Case of Proptosis: CT and MRIImaging a Case of Proptosis: CT and MRIImaging a Case of Proptosis: CT and MRI 6565656565
Figures 3.25A and B: Limitation of elevation of right eye with diplopia in upgaze following trauma while at play. Note the subconjunctivalhemorrhage. The FDT was positive. Clinical diagnosis of fracture floor of orbit with entrapment of inferior Rectus was made. But the CT scan(B) of orbit showed fracture roof of the orbit with the displaced fragment impinging on the globe and mechanically restricting its movement(yellow arrow)
Figures 3.26A and B: Fracture floor of orbit can either involve a large area (Red arrow- A) and may show hemorrhage in the sinus or may bevery tiny with trap-door mechanism and the typical "tear-drop" sign (yellow arrow- B). The rectus muscle may or may not be entrapped.Entrapment of the rectus with positive FDT and diplopia is one of the important indications for early surgery
Trauma: Trauma leading to orbital fractures(Figures 3.25A and B, 3.26A and B) is fairly commonand its incidence is on the raise in view of increasein road traffic accidents and violence in the society.Apart from traumatic optic neuropathy, diplopia isanother very important symptom. Persistentdiplopia due to entrapment of a rectus muscle andpositive FDT is one of the indications for surgery.
Eyeball: After examining the bony orbit, lookat the globe and its relation to the lesion. The lesionmay be soft and molding along the eyeball like alymphoma (Figure 3.27) The globe is pushed aheadby the lesion and also can alter its shape dependingon its consistency (Figures 3.28A and B). In Severeproptosis, tenting of posterior pole (Figure 3.29) canbe noticed.
BA
A B
basm
ala
blog
(alw
ays o
rigin
al)

6666666666 Surgical Atlas of Orbital DiseasesSurgical Atlas of Orbital DiseasesSurgical Atlas of Orbital DiseasesSurgical Atlas of Orbital DiseasesSurgical Atlas of Orbital Diseases
Figure 3.27: Molding: Look at the lesion which is molding along the globe, without altering its curvature (yellow arrow). This is very typicalof lesions which are soft like lymphoma. Molding can also be seen in fungal granuloma, adenoid cystic carcinoma of lacrimal gland
Figure 3.29: In severe proptosis, tenting of the globe with stretching of the optic nerve can occur. This also can contribute todefective vision. Look at the tenting of the posterior pole of the globe with loss of the normal curvature (yellow arrow)
Figures 3.28A and B: Firmer lesions indent the globe and can induce refractive errors. Compression of the globe by cystic lesion (Hydatid Cystfigure A yellow Arrow) and compression of the globe by tumor (schwannoma figure B, yellow Arrow). The intraconal lesions cause hyperopicshift in the refraction, by virtue of flattening the globe, while the lesions in the peripheral space cause astigmatism
A B
basm
ala
blog
(alw
ays o
rigin
al)

Imaging a Case of Proptosis: CT and MRIImaging a Case of Proptosis: CT and MRIImaging a Case of Proptosis: CT and MRIImaging a Case of Proptosis: CT and MRIImaging a Case of Proptosis: CT and MRI 6767676767
After examining the contour of the eyeball,(Figures 3.30 to 3.32) look at the intraocular contents.Retinoblastoma and uveal melanoma (Figures 3.33Ato D) are the most common intraocular tumors whichcan spread into the orbit and can cause secondary
proptosis. It is a routine practice to get a CT Scan oforbit in retinoblastoma. The tumor can be seen as anintraocular mass lesion with calcification. It can beconfined to the globe or can extend into the orbit,optic nerve or brain.
Figures 3.31A and B: This child had a painful proptosis of right eye. Note the gross proptosis with mild congestion, increase in the cornealdiameter, and amaurotic cat's eye reflex (A). The CT scan reveals intraocular masses with calcification (yellow arrow-B). in both the globes.Note the loss of integrity of the sclera with orbital extension (red arrow)
Figures 3.30A and B: Retinoblastoma; The typical amaurotic cat's eye reflex in the left eye( A) The intraocular mass withcalcification (yellow arrow–B) is very typical of retinoblastoma. The sclera looks normal
A B
A B
basm
ala
blog
(alw
ays o
rigin
al)
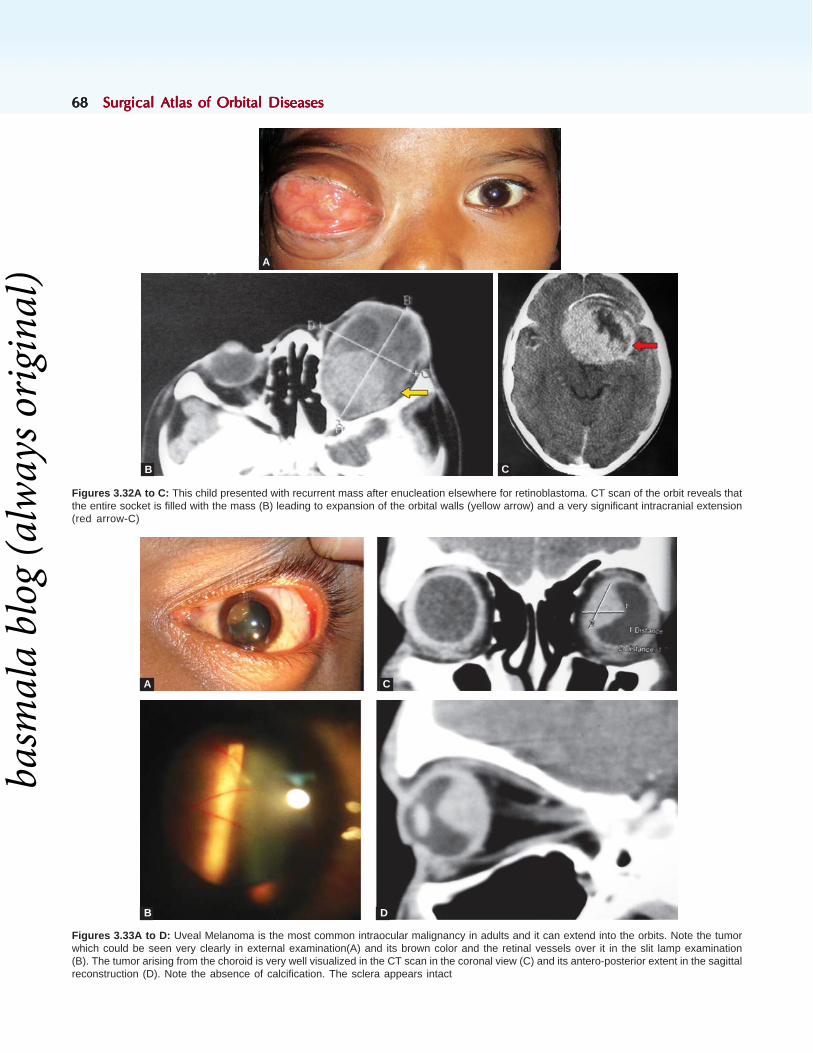
6868686868 Surgical Atlas of Orbital DiseasesSurgical Atlas of Orbital DiseasesSurgical Atlas of Orbital DiseasesSurgical Atlas of Orbital DiseasesSurgical Atlas of Orbital Diseases
Figures 3.32A to C: This child presented with recurrent mass after enucleation elsewhere for retinoblastoma. CT scan of the orbit reveals thatthe entire socket is filled with the mass (B) leading to expansion of the orbital walls (yellow arrow) and a very significant intracranial extension(red arrow-C)
Figures 3.33A to D: Uveal Melanoma is the most common intraocular malignancy in adults and it can extend into the orbits. Note the tumorwhich could be seen very clearly in external examination(A) and its brown color and the retinal vessels over it in the slit lamp examination(B). The tumor arising from the choroid is very well visualized in the CT scan in the coronal view (C) and its antero-posterior extent in the sagittalreconstruction (D). Note the absence of calcification. The sclera appears intact
A
B C
A
B
C
D
basm
ala
blog
(alw
ays o
rigin
al)

Imaging a Case of Proptosis: CT and MRIImaging a Case of Proptosis: CT and MRIImaging a Case of Proptosis: CT and MRIImaging a Case of Proptosis: CT and MRIImaging a Case of Proptosis: CT and MRI 6969696969
Enlarged extraocular muscle: Enlargedextraocular muscle (EOM) is the most commonfinding we come across on imaging in proptosis,followed by mass (tumor). This is because of highprevalence of myocysticercosis as cysticercosis isendemic in our area. The important causes ofenlarged extraocular muscle include thyroid
orbitopathy, (Figures 3.34A and 3.35A and B)myocysticercosis, (Figures 3.36A and B) idiopathicorbital inflammation (Figure 3.34B), rhabdomyo-sarcoma, lymphoma (Figures 3.39A to D), carotidcavernous fistula (Figures 3.37A and B to 3.38A andB), and metastasis. (Figures 3.40A to D).
Figures 3.34A and B: Thyroid associated orbitopathy (TAO) is the most common cause of enlarged extraocular muscle in most studies (A).Myositis due to idiopathic orbital inflammation (IOI) is also very common (B). Hence it is very important to differentiate these two conditions onimaging. The above pictures are very classical. In TAO, the tendon is spared and in myositis it is also involved. Contrast enhancement and onlylateral rectus muscle involvement can occur in IOI but not in TAO. Lacrimal gland and even fat can be involved in IOI, but not in TAO. Most oftenin TAO, the CT scan of the orbit reveals bilateral enlargement of extraocular muscles
Figures 3.35A and B: In TAO, enlarged extraocular muscle can compress the optic nerve and cause loss of vision. Note the grossly enlargedrecti muscles surrounding the optic nerve (red arrow) in the mid coronal sections of left orbit where as the optic nerve on the right side is freefrom compression. The posterior coronal sections reveal a severe compression of optic nerve on the left orbit. This patient had presented witha vision of 20/200 in left eye. Note that the floor and medial wall if orbit are reaching the posterior most part of the orbit, but not the zygoma.Hence in orbital decompression aimed to relieve optic nerve compression, I invariably include the medial wall or floor or both. I also excise orbitalfat. Lateral wall decompression is more for cosmetic purpose
A B
BA
basm
ala
blog
(alw
ays o
rigin
al)
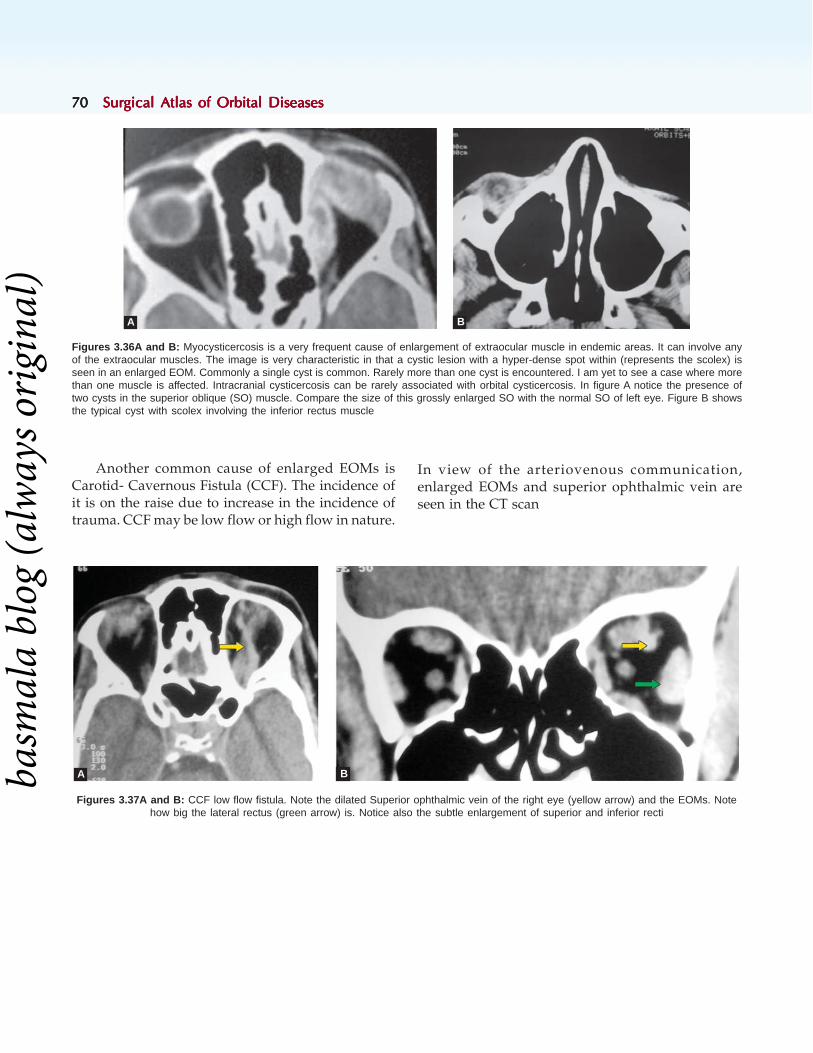
7070707070 Surgical Atlas of Orbital DiseasesSurgical Atlas of Orbital DiseasesSurgical Atlas of Orbital DiseasesSurgical Atlas of Orbital DiseasesSurgical Atlas of Orbital Diseases
Figures 3.36A and B: Myocysticercosis is a very frequent cause of enlargement of extraocular muscle in endemic areas. It can involve anyof the extraocular muscles. The image is very characteristic in that a cystic lesion with a hyper-dense spot within (represents the scolex) isseen in an enlarged EOM. Commonly a single cyst is common. Rarely more than one cyst is encountered. I am yet to see a case where morethan one muscle is affected. Intracranial cysticercosis can be rarely associated with orbital cysticercosis. In figure A notice the presence oftwo cysts in the superior oblique (SO) muscle. Compare the size of this grossly enlarged SO with the normal SO of left eye. Figure B showsthe typical cyst with scolex involving the inferior rectus muscle
Another common cause of enlarged EOMs isCarotid- Cavernous Fistula (CCF). The incidence ofit is on the raise due to increase in the incidence oftrauma. CCF may be low flow or high flow in nature.
In view of the arteriovenous communication,enlarged EOMs and superior ophthalmic vein areseen in the CT scan
Figures 3.37A and B: CCF low flow fistula. Note the dilated Superior ophthalmic vein of the right eye (yellow arrow) and the EOMs. Notehow big the lateral rectus (green arrow) is. Notice also the subtle enlargement of superior and inferior recti
A B
A Bbasm
ala
blog
(alw
ays o
rigin
al)

Imaging a Case of Proptosis: CT and MRIImaging a Case of Proptosis: CT and MRIImaging a Case of Proptosis: CT and MRIImaging a Case of Proptosis: CT and MRIImaging a Case of Proptosis: CT and MRI 7171717171
Figures 3.38A and B: CCF High-flow fistula: Compare the grossly enlarged superior ophthalmic vein (yellow arrow) and the huge enlargementof the inferior rectus muscle( green arrow) with the previous picture. The high flow CCF usually follows trauma, and clinically characterizedby pulsatile proptosis, caput medusae, chemosis, restricted ocular motility, gross retinal venous engorgement and secondary glaucoma
Figures 3.39A to D: Lymphoma: Lymphoma is characterized by a soft tissue lesion which typically molds around the globe (yellow arrow A,Band D). Salmon's patch is the typical presentation (C…green arrow). Some times enlarged EOMS can be seen in some sections of the CT scan(D…red arrow)
A B
A B
C D
basm
ala
blog
(alw
ays o
rigin
al)

7272727272 Surgical Atlas of Orbital DiseasesSurgical Atlas of Orbital DiseasesSurgical Atlas of Orbital DiseasesSurgical Atlas of Orbital DiseasesSurgical Atlas of Orbital Diseases
Figures 3.40A to D: Metastatic lesion from breast: This patient presented with painful proptosis of left eye (A) of 1 month duration. Sheunderwent mastectomy for carcinoma breast (B) 1 year back. CT scan of orbit shows enlarged lateral rectus muscle (C) associated witherosion of the lateral wall of the orbit (red arrow). Enlarged lateral rectus associated with bony erosion is a very common finding of CT scanof orbit in metastatic lesions, especially from breast and GIT. FNAC has confirmed the clinical diagnosis (D)
Soft-tissue Lesions
The clinical spectrum of primary soft tissue lesionsof the orbit is very varied. This is because of thevarious types of tissues that exist in the orbit. Thoughlesions of the optic nerve are not too common, theirimportance can not be over emphasized since theycan lead to loss of vision
The most frequent lesions of the optic nerve areglioma (Figures 3.41A and B, 3.42) and meningiomaof the optic nerve sheath (Figures 3.44A and B). Optic
nerve can also be involved in idiopathic orbitalinflammation (Figures 3.43A and B). It is veryimportant to know whether the intraconal lesion isarising from the optic nerve (meningioma or gliomaof optic nerve) or separate from it [cavernoushemangioma (Figures 3.45A to D), schwannoma(Figures 3.46A and B), etc]. Schwannoma (Figures3.46A and B) is another tumor from nerve tissues,which mimics closely cavernous hemangioma(Figures 3.45A to D).
A B
C D
basm
ala
blog
(alw
ays o
rigin
al)

Imaging a Case of Proptosis: CT and MRIImaging a Case of Proptosis: CT and MRIImaging a Case of Proptosis: CT and MRIImaging a Case of Proptosis: CT and MRIImaging a Case of Proptosis: CT and MRI 7373737373
Figure 3.42: The axial CT scan of orbit shows a very large intraconal mass with distinct borders, and is similar to the Figure 3.39. It howevershows distinctly cystic space (yellow arrow). It is a case of optic nerve glioma with cystic degeneration. Note the bony expansion, flatteningof the posterior pole of the globe
Figures 3.41A and B Optic Nerve Glioma: The axial section of CT scan shows spindle shaped tumor of the optic nerve with very distinctmargins. The coronal section shows a large intraconal tumor. Note that the optic nerve is not seen separately( red arrow). The margins are wellmade-out. There is no evidence of calcification and there is no contrast enhancement. These are the typical feature on imaging of a optic nerveglioma, which help in distinguishing it from meningioma of optic nerve sheath
Figures 3.43A and B: Optic nerve swelling (yellow arrow) as a part of idiopathic orbital inflammation.Note the enlarged medial rectus (green arrow). Note that the margins are indistinct
A B
A B
basm
ala
blog
(alw
ays o
rigin
al)

7474747474 Surgical Atlas of Orbital DiseasesSurgical Atlas of Orbital DiseasesSurgical Atlas of Orbital DiseasesSurgical Atlas of Orbital DiseasesSurgical Atlas of Orbital Diseases
Figures 3.44A and B Meningioma of Optic Nerve Sheath: Meningioma of the optic nerve sheath is more common than the optic nerveglioma. On imaging it is characterized by indistinct margins (blue arrow), calcification, "tram- track" appearance and contrast enhancement(yellow arrow). These features help in distinguishing this lesion from glioma of optic nerve. In the picture B, note the fluffy and indistinct marginswhich differ from the smooth and distinct margins of glioma. The hypodense spot in the center of the lesion is the optic nerve. The hyperdensespots along the optic nerve are due to calcification. Compare these figures with those of glioma to understand the differences between thesetwo lesions on imaging
Figures 3.45A to D: Cavernous Hemangioma is characterized by hyperdense lesion with well defined margins and very minimal contrastenhancement (green arrow). It is more commonly located in the intraconal space and lateral to optic nerve (yellow arrow). In coronal sectionthe mass can be seen separate from the optic nerve. Since most often the duration is very long (average 30 months), bony excavation of theorbit is very common. The excised tumor with very distinct borders is seen in C. Occasionally cavernous hemangioma may show calcifiedspots (D… yellow arrow) which represents the phleboliths. Note the subtle bony excavation of the lateral wall
A B
A B
C D
basm
ala
blog
(alw
ays o
rigin
al)

Imaging a Case of Proptosis: CT and MRIImaging a Case of Proptosis: CT and MRIImaging a Case of Proptosis: CT and MRIImaging a Case of Proptosis: CT and MRIImaging a Case of Proptosis: CT and MRI 7575757575
Figures 3.46A and B: Schwannoma is another common benign tumor and is characterized by very distinct margins. It is often of long durationand hence shows bony expansion. Note the gross axial proptosis of the left eye (A) and the large tumor with very clear cut margins in theintra-conal space, and excavation of the lateral wall (yellow arrow). Schwannomas rarely enhance on contrast
Neurofibroma involving the orbit can be plexiform or as a part of Von Recklinghausen disease (Figure3.47A to D).
Figures 3.47A to D Neurofibroma: Plexiform neurofibroma involving the orbit (AandB). Note the typical shape of the lesion and the imagingshowing the large tumor with indistinct margins involving the temple and the lid. Also note heterogenisity of the lesion. In Von Recklinghausendisease (C and D), the clinical picture with numerous nodular lesions is very distinctive. On imaging apart from proptosis and multiple tumors,dehiscence of the roof of orbit is common (C…yellow arrow), which results in pulsatile proptosis
A B
A B
C D
basm
ala
blog
(alw
ays o
rigin
al)

7676767676 Surgical Atlas of Orbital DiseasesSurgical Atlas of Orbital DiseasesSurgical Atlas of Orbital DiseasesSurgical Atlas of Orbital DiseasesSurgical Atlas of Orbital Diseases
Other vascular tumors like hemangioblastoma,hemangioendothelioma, hemangiopericytoma,angiosarcoma (Figures 3.48A to C), etc show onimaging a well defined mass lesion with contrastenhancement. Usually the clinical picture ischaracterized by shorter duration, mild pain/discomfort. The final diagnosis is by histopathology.Lymphangioma usually shows intralesionalhemorrhage (chocalate cyst).
Lacrimal gland tumors: The lacrimal glandlesions are common.Most common benign lesion ispleomorphic adenoma (Figures 3.49A to C) and themost common malignancy is adenoid cystic carcinoma(Figures 3.50A and B) which has a very poorprognosis. Clinically pleomorphic adenoma has a longduration, and painless. Shorter duration, often lessthan 6 months, and mild discomfort are frequent inadenoid cystic carcinoma. Usually pleomorphicadenoma is firm in consistency, and is non-tender.
Figures 3.48A to C: Angiosarcoma. This patient presented with painful proptosis of 3 months duration. Note the contrast enhancing masslesion with subtle indistinctness of posterior margins in the axial sections of the CT scan (C). The diagosis of angiosarcoma was confirmed onhistopathology and immuni-histochemistry
Figures 3.49A to C: Pleomorphic Adenoma: This patient presented with painless, gradually progressing proptosis of 18 months duration (A).Note that on imaging, the tumor is not molding, and is actually pushing the globe and indenting it. The downward and medial displacement of theglobe is very well made-out in the CT scan (C)
A B C
A
B C
basm
ala
blog
(alw
ays o
rigin
al)

Imaging a Case of Proptosis: CT and MRIImaging a Case of Proptosis: CT and MRIImaging a Case of Proptosis: CT and MRIImaging a Case of Proptosis: CT and MRIImaging a Case of Proptosis: CT and MRI 7777777777
Figures 3.50A and B: Adenoid Cystic Carcinoma: The duration of proptosis in this patient is 5 months. She presented with eccentric proptosisand pain. Imaging shows a hyperdense mass lesion of lacrimal gland, molding to the globe. This is because of the softer consistency of thetumor, and can mimic lymphoma of lacrimal gland
Lymphoma of lacrimal gland: (Figures 3.51 Aand B) is a soft lesion which moulds along theglobe.
Figures 3.51A and B: Lymphoma of Lacrimal Gland: The clinical presentation is characterized by the presence of Salmon's patch in thesuperior fornix (A). The CT scan shows a well defined enlargement of the lacrimal gland which is molding to the globe. Also note subtle bonyerosion of lateral wall of the orbit
BA
BA
Rhabdomyosarcoma: (Figures 3.52A to D) is themost common mesenchymal and malignant tumorof children. Superior Rectus muscle is most commonlyinvolved.
basm
ala
blog
(alw
ays o
rigin
al)

7878787878 Surgical Atlas of Orbital DiseasesSurgical Atlas of Orbital DiseasesSurgical Atlas of Orbital DiseasesSurgical Atlas of Orbital DiseasesSurgical Atlas of Orbital Diseases
Figures 3.52A to D: Rhabdomyosarcoma: This is a very common primary mesenchymal tumor of pediatric age group. The course can be rapidand some times very acute and mimic orbital cellulitis. The child (A) shows very gross proptosis with anterior staphyloma, while the child (C)shows less dramatic clinical picture. Note the fullness of the superior sulcus and eccentric proptosis with the eyeball pushed down in both thechildren. This is because the tumor involved superior rectus muscle (the most common EOM to be involved). Note the enlarged superior rectuswith distinct margins (B and D). Note also the subtle bony erosion in B, while bone shows expansion, not erosion. Contrast enhancement isobserved in these tumors. Biopsy confirms the diagnosis. The tumor responds very well to radiotherapy/chemotherapy
Cystic lesions of the orbit: A variety of cysticlesions occur in the orbit. They could be congenitalcysts like dermoid (Figures 3.53A and B), congenitalcystic eyeball, arachnoid cyst (Figures 3.56A and B),
parasitic cysts [cysticercosis (Figures 3.55A to C),hydatid cyst] (Figures 3.54A and B), cysticdegenerations (glioma), mucocele (Figure 3.57),lymphangioma.
Figures 3.53A and B: Dermoid Cyst is the most common cystic lesion of the orbit in most of the series, other than in areas endemic forcysticercosis. Dermoids are usually congenital, preseptal and involve the temporal region in children, while they are acquired, postseptal, andnasal in location (A) in adults. On imaging they show a cystic lesion with well defined margins. Some times, a part of the lesion can behyperdense, depending on its contents. Dumbbell -dermoids (B) are rare. Note the cystic lesion with an orbital component, and a temporalcomponent (yellow arrows), and the gap in the lateral wall of the orbit. Note also the smooth excavation of the lateral wall (blue arrow)
A B
C D
A B
basm
ala
blog
(alw
ays o
rigin
al)

Imaging a Case of Proptosis: CT and MRIImaging a Case of Proptosis: CT and MRIImaging a Case of Proptosis: CT and MRIImaging a Case of Proptosis: CT and MRIImaging a Case of Proptosis: CT and MRI 7979797979
Figures 3.54A and B: Hydatid Cyst: Hydatid cyst is not very common. It usually occurs in younger individuals, and is often intraconal inlocation. Hence visual symptoms, axial proptosis of few months duration and optic disc edema in a patient having pets, especially dogs shouldarouse clinical suspicion. CT scan of the orbit shows a thin walled, isodense cystic lesion (red arrow). It can grow to a very large size anddwarf the globe (yellow arrow: A and B). Note the large, thin walled cyst, pushing the eyeball inferolaterally. Compare the size of the cyst withthe eyeball. Also note the expansion of orbital walls. Because of such expansion of the orbital walls, and increased orbital volume, excision ofthe cyst leads to enophthalmos
Figures 3.55A to C: Cysticercosis: Orbital Myocysticercosis is common in endemic areas. Usually solitary cyst is seen, involving a single extraocular muscle. Restricted motility, diplopia associated with mild discomfort or pain are the important clinical features. Note the restrictedelevation of right eye (A). CT scan of orbit shows enlarged inferior rectus muscle (green arrow) with a cyst. Note the hyperdense spot in it(yellow arrow) which represents the scolex
Figures 3.56A and B: Arachnoid Cyst: Arachnoid cysts are very rare. Infants and young children with these congenital cysts present withpainless proptosis. CT scan of the orbit reveals a cyst associated with hydrocephalus. The Hounsfield units of the cyst are usually 5 to 10 units,similar to CCF. Note the severe flattening of the posterior pole of the eyeball (yellow arrow) by the cyst (green arrow) Also note the bonyexpansion of lateral and medial walls. Note the gross hydrocephalus (B white arrow)
A B
A B C
BA
basm
ala
blog
(alw
ays o
rigin
al)
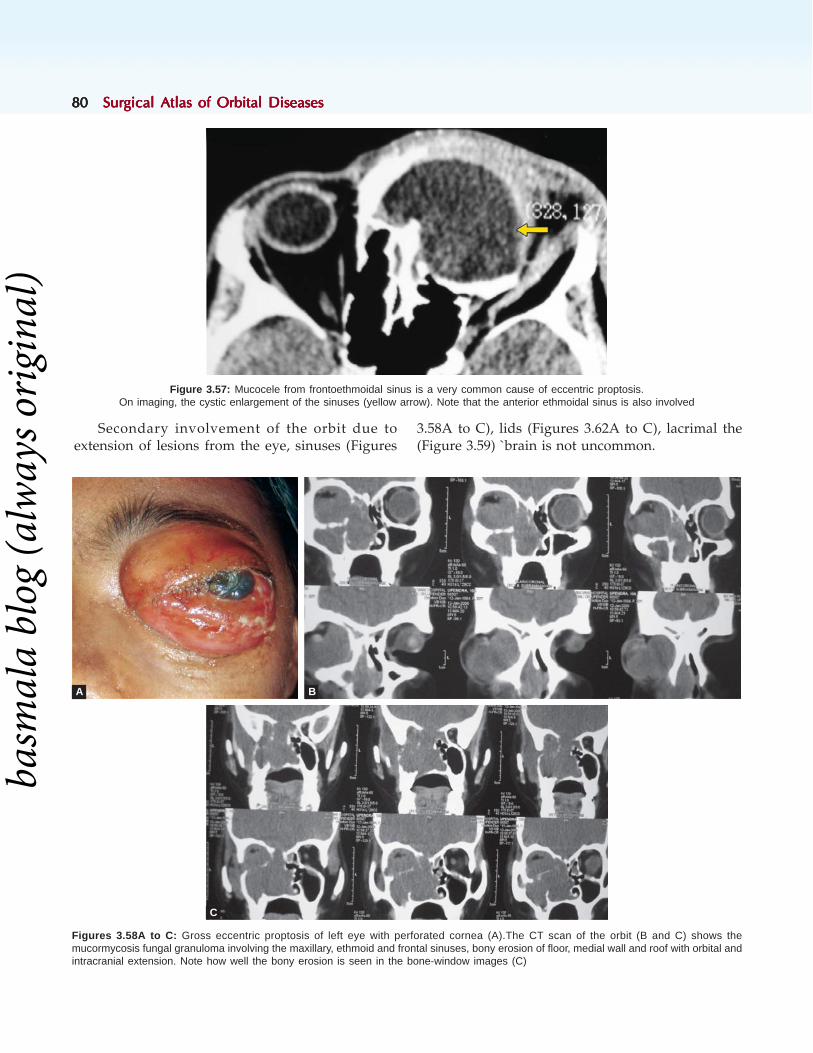
8080808080 Surgical Atlas of Orbital DiseasesSurgical Atlas of Orbital DiseasesSurgical Atlas of Orbital DiseasesSurgical Atlas of Orbital DiseasesSurgical Atlas of Orbital Diseases
Figure 3.57: Mucocele from frontoethmoidal sinus is a very common cause of eccentric proptosis.On imaging, the cystic enlargement of the sinuses (yellow arrow). Note that the anterior ethmoidal sinus is also involved
Secondary involvement of the orbit due toextension of lesions from the eye, sinuses (Figures
3.58A to C), lids (Figures 3.62A to C), lacrimal the(Figure 3.59) `brain is not uncommon.
Figures 3.58A to C: Gross eccentric proptosis of left eye with perforated cornea (A).The CT scan of the orbit (B and C) shows themucormycosis fungal granuloma involving the maxillary, ethmoid and frontal sinuses, bony erosion of floor, medial wall and roof with orbital andintracranial extension. Note how well the bony erosion is seen in the bone-window images (C)
A B
C
basm
ala
blog
(alw
ays o
rigin
al)
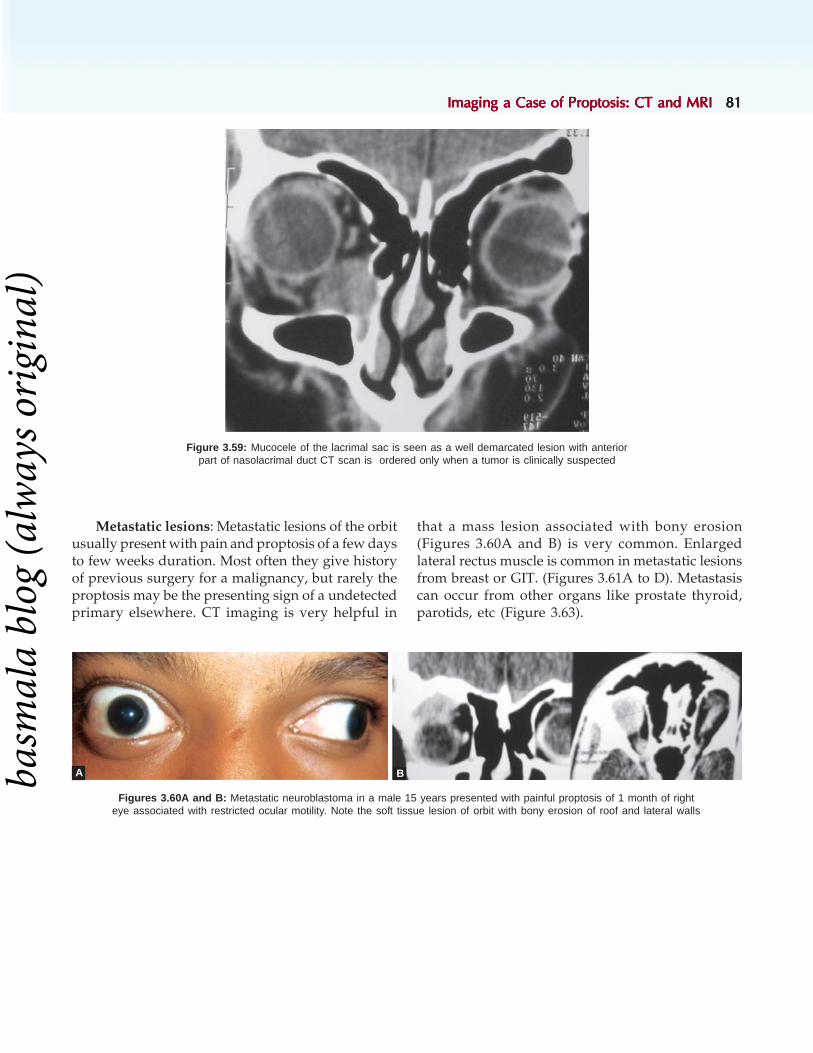
Imaging a Case of Proptosis: CT and MRIImaging a Case of Proptosis: CT and MRIImaging a Case of Proptosis: CT and MRIImaging a Case of Proptosis: CT and MRIImaging a Case of Proptosis: CT and MRI 8181818181
Figure 3.59: Mucocele of the lacrimal sac is seen as a well demarcated lesion with anteriorpart of nasolacrimal duct CT scan is ordered only when a tumor is clinically suspected
Metastatic lesions: Metastatic lesions of the orbitusually present with pain and proptosis of a few daysto few weeks duration. Most often they give historyof previous surgery for a malignancy, but rarely theproptosis may be the presenting sign of a undetectedprimary elsewhere. CT imaging is very helpful in
that a mass lesion associated with bony erosion(Figures 3.60A and B) is very common. Enlargedlateral rectus muscle is common in metastatic lesionsfrom breast or GIT. (Figures 3.61A to D). Metastasiscan occur from other organs like prostate thyroid,parotids, etc (Figure 3.63).
Figures 3.60A and B: Metastatic neuroblastoma in a male 15 years presented with painful proptosis of 1 month of righteye associated with restricted ocular motility. Note the soft tissue lesion of orbit with bony erosion of roof and lateral walls
A Bbasm
ala
blog
(alw
ays o
rigin
al)

8282828282 Surgical Atlas of Orbital DiseasesSurgical Atlas of Orbital DiseasesSurgical Atlas of Orbital DiseasesSurgical Atlas of Orbital DiseasesSurgical Atlas of Orbital Diseases
Figures 3.61A to D: Metastatic Carcinoma from right breast in a female of 45 years who presented with mild proptosis and periocular swellingof left eye since 1 month (A). She underwent radical mastectomy 2 years back (B). CT scan of orbits reveals enlarged lateral rectus (greenarrow) with bony destruction of lateral wall and the roof (C and D orange arrow). FNAC was positive for ductal carcinoma of breast. She wasreferred to oncologist for further management
Figures 3.62A to C: Secondary Involvemet From Lid Tumor in this elderly male who presented with a very large Basal cell carcinoma of theupper lid of 6 years duration. Note the huge upper lid tumor (A), and its orbital extension (B and C) evident in both coronal and sagittal sections
A B
C D
A
B C
Secondary orbital involvement can occur due to extension of tumors of eyelids (Figures 3.62A to C),intraocular tumors or intracranial tumors.
basm
ala
blog
(alw
ays o
rigin
al)

Imaging a Case of Proptosis: CT and MRIImaging a Case of Proptosis: CT and MRIImaging a Case of Proptosis: CT and MRIImaging a Case of Proptosis: CT and MRIImaging a Case of Proptosis: CT and MRI 8383838383
Figure 3.63: Adenoid cystic carcinoma of parotid gland with intracranial(red arrow) and orbital extension (green arrow). Also note the bony erosion
Figures 3.64A to D: Contrast enhancement of hemangioendothelioma (B when compared to A) and Lymphoma (D and C)
Contrast enhancement: Whenever I suspect avascular lesion or a tumor, I ask for contrast studies.Contrast enhancement shows that the tumor is veryvascular. It differentiates a cavernous hemangioma
from a hemangioendothelioma. When the tumors arevery strongly enhance on contrast as in the Figures3.64A to D, I will keep a unit of blood reserved atthe time of surgery.
A B
C D
basm
ala
blog
(alw
ays o
rigin
al)

8484848484 Surgical Atlas of Orbital DiseasesSurgical Atlas of Orbital DiseasesSurgical Atlas of Orbital DiseasesSurgical Atlas of Orbital DiseasesSurgical Atlas of Orbital Diseases
BIBLIOGRAPHY
1. Abou-Rayyah Y, Rose GE, Konrad H, Chawla SJ, MoseleyIF. Clinical, radiological and pathological examination ofperiocular dermoid cysts. Eye. 2002;16(5):507-12.
2. Arger PH The radiologic evaluation of unilateral proptosis.CRC Crit Rev Clin Radiol Nucl Med. 1974;5(1):43-67.
3. Char DH, Sobel D, Kelly WM, Kjos BO, Norman DMagnetic resonance scanning in orbital tumor diagnosis.Ophthalmology. 1985;92(10):1305-10.
4. Forbes G. Radiologic evaluation of orbital tumors. ClinNeurosurg. 1985;32:474-513.
5. Forbes GS, Sheedy PF 2nd, Waller RR. Orbital tumorsevaluated by computed tomography. Radiology.1980;136(1):101-11.
6. Hilal SK, Trokel SL. Computerized tomography of the orbitusing thin sections. Semin Roentgenol. 1977;12(2):137-47.
7. Klöppel R, Schulz HG, Ballin R, Lommatzsch P Value ofcomputed tomography in orbital tumors. Radiol Diagn(Berl). 1985;26(6):745-52.
8. Kokemueller H, Zizelmann C, Tavassol F, Paling T, GellrichNC A comprehensive approach to objective quantificationof orbital dimensions. J Oral Maxillofac Surg. 2008;66(2):401-7.
9. Trokel SL, Hilal SK Recognition and differential diagnosisof enlarged extraocular muscles in computed tomography.Am J Ophthalmol. 1979;87(4):503-12.
10. Urbanik A, Chojnacka I, Herman-Sucharska I, Jele?ska I,Brzozowska-Czarnek A. Computed tomography imagesof selected retrobulbar orbit tumors. Przegl Lek.2000;57(6):327-9.
11. Vignaud J, Hasso AN, Lasjaunias P, Clay C Orbital vascularanatomy and embryology. Radiology. 1974 ;111(3):617-26.
12. Wackenheim A, van Damme W, Kosmann P, BittighofferB. Computed tomography in ophthalmology. Densitychanges with orbital lesions. Neuroradiology.1977;13(3):135-8.
13. Wei R, Cai J, Wang H, Tao X, Zhu H, Zhou H. Analysis ofMRI and CT manifestations of paranasal sinuses andorbitocranial disorders with secondary exophthalmos.Zhonghua Yan Ke Za Zhi. 1999;35(3):200-2, 12.
14. Wende S, Aulich A, Nover A, Lanksch W, Kazner E,Steinhoff H, Meese W, Lange S, Grumme T. Computedtomography or orbital lesions. A cooperative study of 210cases. Neuroradiology. 1977;13(3):123-34.
15. Wende S, Kazner E, Grumme T The diagnostic value ofcomputed tomography in orbital diseases. A cooperativestudy of 520 cases. Neurosurg Rev. 1980;3(1):43-9.
3-D reconstruction of orbit: Orbital 3-Dreconstruction is ordered in severe orbital
fractures and also in congenital bone defects(Figures 3.65A and B).
Figures 3.65A and B: 3-D reconstruction of the orbit and periorbital regions is very useful in casesof trauma. Note how well the bony defect in the frontal bone and the cleft palate are seen
A B
basm
ala
blog
(alw
ays o
rigin
al)
Role of Cytology in Orbital LesionsRole of Cytology in Orbital LesionsRole of Cytology in Orbital LesionsRole of Cytology in Orbital LesionsRole of Cytology in Orbital Lesions 8585858585
Geeta K Vemuganti, Anirban Bhaduri
Role of CytologyRole of CytologyRole of CytologyRole of CytologyRole of Cytologyin Orbital Lesionsin Orbital Lesionsin Orbital Lesionsin Orbital Lesionsin Orbital Lesions
Cytologic diagnosis of lesions is one of the mainstayof diagnosis for lesions affecting various organs ofthe body. This speciality has made tremendousimpact even in ophthalmic pathology, an upcomingsubspeciality, which has been referred by FredrickJakobiec as “queen of subspecialities ofOphthlmology.” The techniques of obtainingspecimens of ocular cytology have undergone muchrefinement and with increasing reports of largerseries of cases, the learning curve has been crossedby many experts. In general, the techniques used fororbital lesions include: Fine needle aspiration ofpalpebral lesions, squash and imprint cytology offresh tissue for rapid intraoperative diagnosis.1-6 Thecytology specimens could also be subjected torecently emerging molecular tools of diagnosis,7-8 thusaiding in patient management.
Fine Needle Aspiration/Sampling TechniqueThe procedure for FNAC at any site in the body isthe same. The procedure can be done by thepathologist or the surgeon, directly under vision orunder guidance of CT. Usually there is no need ofany local anesthesia injection by this technique, exceptin children where a general anesthesia may bepreferred. The technique of obtaining the materialcould be a “sampling technique” wherein a 23 /24guage needle is introduced into the lesion andpushed in various directions within the lesion andgently withdrawn.9 By the capillary action, the cellsare drawn into the needle. This technique has alsobeen applied to ocular cytology.3,6 The advantagesof this technique are: It is easy, simple, lesshemorrhagic and causes less apprehension to the
patient. The cytologic material obtained by thismethod is usually adequate with minimum amountof hemorrhage. A few disadvantages of fine needleaspiration in general include inadequate material,hemorrhagic aspirate, bleeding at the site, especiallyfor highly vascular lesions. At our center, FNAC hasyielded diagnostic yield in more than 90% of cases.Tijl et al.10 reported the diagnostic yield of orbitalFNAB combined with clinical and radiologicalfeatures as 80%. Very rare potential complicationsinclude globe penetration, retrobulbar hemorrhage,diplopia and ptosis.11
Intraoperative-operative Diagnosis by Squashand Imprint CytologyThere is often a need for a reliable intraoperativediagnosis, specifically in situations where a definitivepreoperative tissue diagnosis is lacking and wherethe tissue diagnosis is likely to influence theimmediate surgical management.12 The establishedmethods of intraoperative diagnosis include frozensection diagnosis and intraoperative cytologicdiagnosis, each of which has its own merits anddemerits.
Squash or Imprint Cytology
The utility of imprint cytology in eye lesions wasfirst described by Fuchs for uveal melanoma in 1988.13
Imprint cytology of fresh unfixed tissue specimensand squash cytology of central nervous system lesionshave been extensively used in the last few decades,but rarely applied to ophthalmic pathology practice.The main indications for rapid intraoperativediagnosis are: a) Infiltrative lesions, suspected
4C H A P T E R
basm
ala
blog
(alw
ays o
rigin
al)

8686868686 Surgical Atlas of Orbital DiseasesSurgical Atlas of Orbital DiseasesSurgical Atlas of Orbital DiseasesSurgical Atlas of Orbital DiseasesSurgical Atlas of Orbital Diseases
malignant lesions or deeply located lesions where apreoperative tissue diagnosis is not available; b)Where there is a discrepancy between a preoperativeclinical diagnosis and the intraoperative findings and:c) Unusual clinical presentations with diagnosticdilemma.
Fresh unfixed tissue obtained at the time ofdiagnostic or excision biopsy can be used for makingsquash preparation and impressions on glass slides.The procedure for making squash or imprint smearsis usually based on the size, shape, consistency andcrushable properties of the tissue submitted. For soft,easy to spread tissues, tiny bit of the fresh tissue isplaced between two clean glass slides and gentlydrawn apart. For large firm specimens, the imprintsmears are prepared by touching the freshly cutsurface of the lesion with clean slides, avoidingsmearing to retain cell morphology. If the surface iscovered with blood or exudates, more number ofsmears is made, after gently wiping the surface clean.It is preferable to make a minimum of three slidesfor each case. It is advisable to preserve extraunstained smears for further tests like immuno-cytochemsitry or for any molecular studies in future.
These smears are either alcohol fixed for rapidhematoxylin and eosin staining, or fixed by air-dryingfor Diff-quick staining. A provisional cytologicdiagnosis can be made by the pathologist based onthe cellular and architectural features seen on smearsprepared from either or both techniques.
CASE ILLUSTRATIONS
Case 1
A 23-year-old female presented with swelling of leftupper lid for 2 months with occasional diplopia.Examination showed non-axial proptosis withdownward displacement of globe and fullness of theupper lid sulcus (Figure 4.1A). There was a firm,slightly tender nodular mass in the superolateralorbit. There was limited abduction of the left eye.CT scan shows a soft tissue mass in superolateralorbit, which could not be seen separate from thelateral rectus muscle (Figure 4.1B). Incision biopsywas done. Squash and imprint preparation shows apolymorphous population of inflammatory cellsconsisting of lymphocytes, neutrophils and also a feweosinophils (Figure 4.1C), suggestive of a nonspecific
orbital inflammatory disease. Permanent sectionsconfirmed the diagnosis.
Figures 4.1A to C: (A) Photograph shows the downward displace-ment of the left eye and fullness of the upper lid sulcus due to thepresence of a lacrimal gland mass (B) CT scan (coronal cut) showsa well-circumscribed, homogenous, extraconal, soft tissue mass inthe superolateral quadrant of mid-orbit, which is not seen separatefrom the lateral rectus muscle. There is no orbital fat streaking.(C) The squash smear shows a polymorphic population of cells con-sisting of lymphocytes, neutrophils, eosinophils. (Giemsa, x 500)
A
B
C
basm
ala
blog
(alw
ays o
rigin
al)

Role of Cytology in Orbital LesionsRole of Cytology in Orbital LesionsRole of Cytology in Orbital LesionsRole of Cytology in Orbital LesionsRole of Cytology in Orbital Lesions 8787878787
Case 2
A 12-year-old female presented with swelling of leftupper lid and cheek for 1 month. There was no historyof cough, hemoptysis, fever or weight loss. Therewas a soft, non-tender swelling in the superior orbit(Figure 4.2A). Preauriclar and submandibular lymphnodes of the left side were enlarged, firm, non-tender and mobile. CT scan showed a soft tissue massin superior orbit with bone destruction. Clinically, aprovisional diagnosis of adenoid cystic carcinoma ofthe lacrimal gland was made. FNAC from the orbitallesion and preauricular lymph node showedlymphocytic infiltrates, epithelioid granulomas andfew giant cells (Figure 4.2B). Extensive necrosis wasseen in some areas. Acid-fast bacilli staining of thesmears showed a few bacilli.
Case 3
A 70-year-old female presented with history ofpainful vision loss with drooping of the upper eyelidof the right eye for 1 month. Examination showedcomplete external ophthalmoplegia with ptosis,dilated and fixed pupil and optic atrophy (Figure4.3A). She was a diabetic on irregular treatment. CTscan showed a large, elongated cystic mass inposterior, superomedial orbit straddling intraconaland extraconal spaces and lying close to the opticnerve (Figure 4.3B). Differential diagnoses were: aparasitic cyst or cystic degeneration in a solid tumor.Preoperatively, an abscess was found, the wall wasexcised after draining the contents. Squash andimprint preparation of the walls showed chronicinflammatory cells and fibrosis with fungal filaments(Figure 4.3C). Cultures of the specimen confirmedaspergillosis.
Case 4
An 18-month-old male child presented with rightsided non-axial proptosis and temporal fossa fullness
Figures 4.2A and B: (A) Photograph shows narrowed palpebralaperture and fullness of left superior sulcus due to a soft mass in thesuperior orbit. (B) The squash smear show cluster of epitheloid cellswith slipper shaped nuclei (hematoxylon and eosin, × 200)
A
A
B
B
basm
ala
blog
(alw
ays o
rigin
al)

8888888888 Surgical Atlas of Orbital DiseasesSurgical Atlas of Orbital DiseasesSurgical Atlas of Orbital DiseasesSurgical Atlas of Orbital DiseasesSurgical Atlas of Orbital Diseases
of 15 days duration (Figure 4.4A). Peripheral bloodsmear was normal. CT scan showed an extraconal,well circumscribed soft tissue mass temporally withdestruction of the greater wing of sphenoid andextending into temporal fossa and middle cranialfossa (Figure 4.4B). Incision biopsy was done fromthe temporal fossa. The squash and imprint smearsshowed cellular infiltrates consisting of neutrophils,eosinophils, plasma cells and giant cells. In additionthere were large cells with moderate amount ofcytoplasm and large vesicular nucleus withprominent grooves and folds (Figure 4.4C). Frequentmultinucleated giant cells are seen. Tingible bodymacrophages and histiocytes with phagocytic activitywere noted. Based on the above features on squashand imprint smears, a provisional diagnosis ofeosinophilic granuloma was given which wasconfirmed on histology sections. Intralesionaltriamcinolone was injected and the lesion resolvedcompletely. Systemic workup included USGabdomen, skeletal survey, bone marrow biopsy andliver function tests were normal. Bone remodelingwas complete at 6 months.
Case 5
A 45-year-old male presented with progressiveprotrusion of the left eye for 3 months (Figure 4.5A)
Figures 4.3A to C: (A) Photograph shows complete ptosis on rightside. The patient had total external ophthalmoplegia with optic atrophyin the right eye. (B) Axial CT scan shows an elongated mass withcystic changes in the superomedial quadrant of the right orbit close tothe optic nerve and soft tissue mass or mucosal thickening in adjoiningethmoidal sinuses. (C) the smears shows prominent branching andseptate fungal filaments with inflammatory cells in the background(Giemsa, × 1000)
Figures 4.4A to C: (A) Photograph shows swelling and erythema ofthe right upper lid and fullness of the temporal fossa. (B) CT scan(axial cut) shows a homogenous, well-circumscribed, low intensitysoft tissue mass with destruction of the greater wing of sphenoid.The mass involves extraconal lateral orbit, temporal fossa and middlecranial fossa. (C) The squash smears are cellular with polymorphicpopulation of cells with multinucleated giant cells, neutrophils,eosinophils and histiocytes with prominent nuclear grooves andcleaves (hematoxylin and eosin, × 1000).
C
A
B
C
basm
ala
blog
(alw
ays o
rigin
al)

Role of Cytology in Orbital LesionsRole of Cytology in Orbital LesionsRole of Cytology in Orbital LesionsRole of Cytology in Orbital LesionsRole of Cytology in Orbital Lesions 8989898989
Figures 4.5A to C: (A) Photograph shows severe chemosis andnon-axial proptosis of the left eye. (B). CT scan (axial cut) shows awell defined irregular hypodense soft tissue mass in intraconal andextraconal spaces in the left orbit. (C) The smears show largemultinucleated giant cells with multiple lymphocytes, plasma cells withinthe cytoplasm of the histiocytes-called as emperipolesis, apathognomonic feature of Rosai-Dorfman disease ( Giemsa, × 500)
and non-tender, smooth, firm subcutaneous nodulesin left breast, upper abdomen and thigh for 2 months.CT scan showed a well defined soft tissue intraconaland extraconal mass in the left orbit (Figure 4.5B).He had a previous episode of proptosis on the sameside ten years ago, which was diagnosedhistopathologically as reactive lymphoid hyperplasiapreviously, which responded to local radiotherapyafter initial poor response to systemic steroids.Incision biopsy performed on the orbital mass twomonths ago showed sinus histiocytosis.
FNAC was performed from the breast andabdominal nodule at this presentation and smearsshowed high cellularity with a polymorphouspopulation of cells consisting of lymphocytes, plasmacells, histiocytes and neutrophils. A large number ofhistiocytic giant cells with abundant cytoplasmextended by the presence of intracytoplasmic plasmacells, lymphocytes and occasional neutrophils werepresent(Figure 4.5C). This feature, described asemperipolesis, confirmed that the subcutaneous nodules were a part of multifocal Rosai-Dorfman
Disease.
Case 6
A 48-year-old male presented with a swelling on thesurface of the right eye with prominence of that eyefor 6 months. Examination showed a pink fleshyconjunctival mass with intrinsic vessels (Figure 4.6A),axial proptosis and limitation of eye movements. CTscan showed a soft tissue mass moulding around theglobe and extending into the conjunctiva (Figure4.6B). Incision biopsy was done from the conjunctiva.Squash and imprint smears were cellular with amonomorphic population of lymphoid cells. Thesecells showed scant rim of cytoplasm and a roundnucleus with moderately coarse chromatin and smallnucleoli (Figure 4.6C). The biopsy confirmed a diffuselarge cell lymphoma, immuno-phenotypingsuggested a B cell lymphoma. Systemic workup didnot show any other focus of lymphoma. He wastreated with local external beam radiotherapy andwas doing well on last follow-up.
Case 7
A 65-year-old male presented with non-axial proptosisof right eye with inferomedial displacement for 15days. He also complained of low back ache for 3months. Firm, non-tender, fixed nodular mass inB
A
C
basm
ala
blog
(alw
ays o
rigin
al)

9090909090 Surgical Atlas of Orbital DiseasesSurgical Atlas of Orbital DiseasesSurgical Atlas of Orbital DiseasesSurgical Atlas of Orbital DiseasesSurgical Atlas of Orbital Diseases
Figures 4.6A to C: (A) A closeup photograph of the right eye showsthe pink fleshy conjunctival mass in the lateral bulbar conjunctiva withintrinsic vessels which seem to appear from and disappear into thetumor. This mass represents the conjunctival component of thelymphoma. There is also axial proptosis and limitation of eyemovements. (B) CT scan shows a soft tissue mass classically mouldingaround the globe and extending into the conjunctiva. (C) The smearsare cellular with monomorphic cells, with scant rim of cytoplasm anda moderately coarse chromatin patter. Note the absence of cohesion,cytoplasm and any differentiation. (Giemsa, x 500)
superolateral orbit with erosion of superior orbitalrim and temporal fullness (Figure 4.7A). CT scanshowed a soft tissue mass with bone destruction(Figure 4.7B). X-ray skull shows multiple punchedout lesions (Figure 4.7C), skeletal survey showsmultiple osteolytic lesions in long bones and spine.Cytology of the mass showed cellular smears with alarge number of plasma cells in varying stages ofdifferentiation (Figure 4.7D). Many bi-tri andmultinucleated forms were noted. The Giemsa
B
A
C
A
B
C
basm
ala
blog
(alw
ays o
rigin
al)

Role of Cytology in Orbital LesionsRole of Cytology in Orbital LesionsRole of Cytology in Orbital LesionsRole of Cytology in Orbital LesionsRole of Cytology in Orbital Lesions 9191919191
stained smears are helpful in identifying theamphophilic cytoplasm and a perinuclear halo. TheBone marrow shows 15-25% plasma cells in variousstages of differentiation.
Case 8
A 17-year-old male presented with gradual inferiordisplacement of right eye for three months andblurred vision following a trivial sports injury. Firm,fixed, slightly tender superomedial orbital massobserved. CT scan shows a soft tissue mass withpatchy enhancement in the superior orbit (Figure4.8A.) Peripheral blood smear was normal. Incisionbiopsy revealed a greenish yellow (chloroma) solidtumor in the peripheral surgical space. Squash imprintpreparations of tissues showed a monomorphicround cell tumor. However the characteristic featureis the pale staining nucleus, irregular nuclearmembrane, and pinkish cytoplasm. The Giemsastained smears are of great importance in confirmingthe blast like morphology with cytoplasmic granulesand sometime Auer rods can also be identified(Figures 4.8B and C), which confirms the diagnosisof leukemic deposits. Bone marrow biopsy wasnormal in this patient, at the time of orbitalpresentation suggesting the extramedullary leukemicdeposits.
Figures 4.7A to D: (A) Photograph shows fullness of upper lidsulcus and downward displacement of the right eye by an orbitalmass.(B). CT scan (axial cut) shows a well-circumscribed,homogenous, lobulated soft tissue mass in the orbit with bonedestruction and extension into the temporal fossa and middle cranialfossa. (C). Radiograph of skull (lateral view) shows multiple, punchedout osteolytic lesions in the skull bones. (D) The cytology smearshows multiple plasma cells with bi and multinucleated forms. Theamphophilic cytoplasm and the perinuclear halo is classical of plasmacell lineage ( Giemsa, × 500).
Figures 4.8A to C: (A) CT scan orbit (coronal cut) shows a well-circumscribed, homogenous, hypodense soft tissue mass, with nosurrounding bony changes, displacing the orbital contents inferiorly.(B) The smears show large cells with scant to moderate amount ofblue cytoplasm with lack of cohesion. (C) The higher magnificationshows the cytoplasmic Auer rod, confirming the diagnosis ofgranulocytic sarcoma (Giemsa, × 1000)
D
A
B
C
basm
ala
blog
(alw
ays o
rigin
al)

9292929292 Surgical Atlas of Orbital DiseasesSurgical Atlas of Orbital DiseasesSurgical Atlas of Orbital DiseasesSurgical Atlas of Orbital DiseasesSurgical Atlas of Orbital Diseases
Case 9A 6-year-old female presented with an increasingswelling below the left eye for 1 month, Onexamination, there was a firm mass in inferonasalorbit with non axial proptosis and superolateraldisplacement of the eye. CT scan showed a, well-circumscribed, smooth soft tissue extraconal massdisplacing adjacent medial rectus muscle and globe.The tumor was completely excised. Squash andimprint smears were highly cellular with irregularcells with marked pleomorphism of nuclei andcytoplasm. The cells with pink tongue likeprojections, spindle cells are helpful in suggestingRhabdomyoblastic differentiation (Figures 4.9A toD). The cells contained moderate to abundant amountof cytoplasm staining deep blue and containingoccasional small glycogen vacuoles. Few cells show
ill-defined relatively dense cytoplasmic inclusion.Tumor cells are found singly, but loose clusters alsoseen. Based on degree of myogenic differentiationAkhtar et al.14 divided Rhabdomyoblasts into 3categories—Early Rhabdomyoblasts are roundundifferentiated cells with high nuclear: Cytoplasmicratio. Intermediate Rhabdomyoblasts have relativelyabundant pale staining cytoplasm and one or moreirregular nuclei with occasional nucleoli. LateRhabdomyoblasts contain abundant cytoplasmstaining grayish blue and opaque. These cells varyfrom round to markedly elongated. Some cells showlocalized inclusion like grayish blue area withincytoplasm. The differential diagnosis include:Retinoblastoma, Burkitt's lymphoma, metastaticNeuroblastoma, PNET/Ewing's sarcoma andmyeloid leukemia can all present in orbit.
Figures 4.9A to D: (A) Photograph shows a swelling in the inferomedial orbit visible as a swelling in the lower lid and upward displacementof the globe. (B) CT scan, axial view shows a hyperdense mass in the medial orbit, indenting the globe. The mass is homogenous. (C) Thecytology smears show clumps of cells with pink cytoplasm. Note the presence of cells with tongue like projections a one pole of the cells.(Hematoxylin and eosin × 500) (D) The sections from the tumor show necrotic areas and large pink cells, characteristic of rhabdomyoblasts
A B
C D
basm
ala
blog
(alw
ays o
rigin
al)
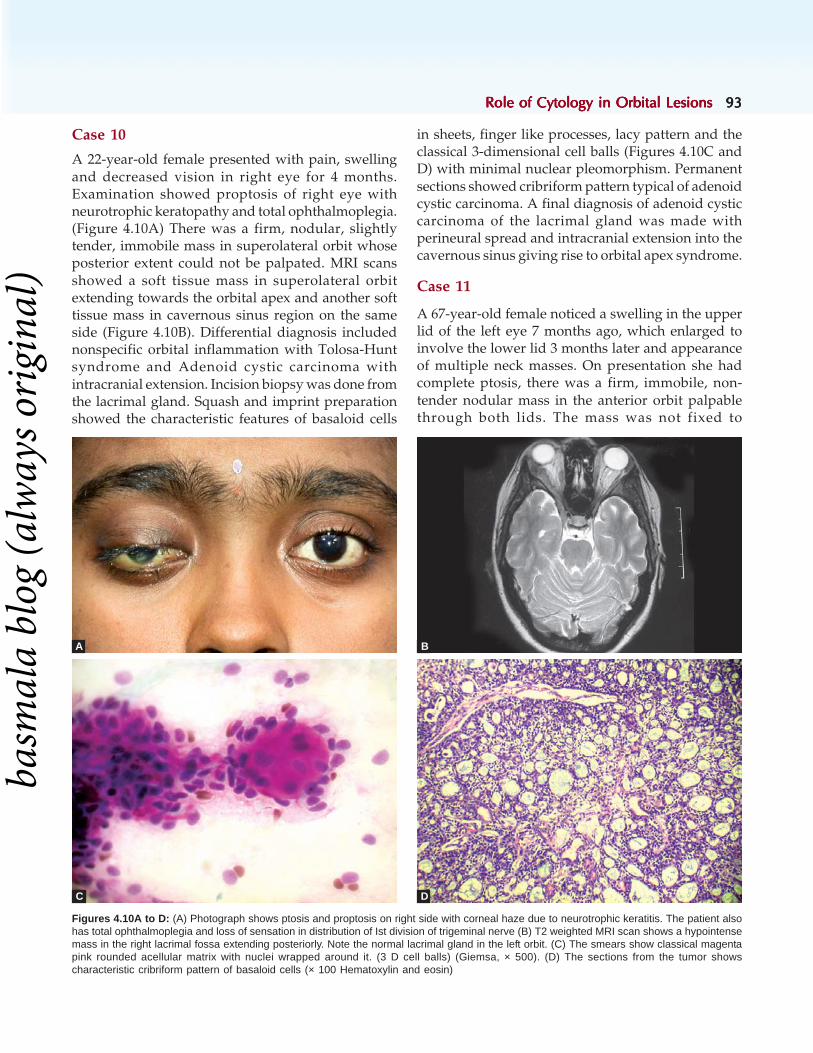
Role of Cytology in Orbital LesionsRole of Cytology in Orbital LesionsRole of Cytology in Orbital LesionsRole of Cytology in Orbital LesionsRole of Cytology in Orbital Lesions 9393939393
Case 10
A 22-year-old female presented with pain, swellingand decreased vision in right eye for 4 months.Examination showed proptosis of right eye withneurotrophic keratopathy and total ophthalmoplegia.(Figure 4.10A) There was a firm, nodular, slightlytender, immobile mass in superolateral orbit whoseposterior extent could not be palpated. MRI scansshowed a soft tissue mass in superolateral orbitextending towards the orbital apex and another softtissue mass in cavernous sinus region on the sameside (Figure 4.10B). Differential diagnosis includednonspecific orbital inflammation with Tolosa-Huntsyndrome and Adenoid cystic carcinoma withintracranial extension. Incision biopsy was done fromthe lacrimal gland. Squash and imprint preparationshowed the characteristic features of basaloid cells
in sheets, finger like processes, lacy pattern and theclassical 3-dimensional cell balls (Figures 4.10C andD) with minimal nuclear pleomorphism. Permanentsections showed cribriform pattern typical of adenoidcystic carcinoma. A final diagnosis of adenoid cysticcarcinoma of the lacrimal gland was made withperineural spread and intracranial extension into thecavernous sinus giving rise to orbital apex syndrome.
Case 11
A 67-year-old female noticed a swelling in the upperlid of the left eye 7 months ago, which enlarged toinvolve the lower lid 3 months later and appearanceof multiple neck masses. On presentation she hadcomplete ptosis, there was a firm, immobile, non-tender nodular mass in the anterior orbit palpablethrough both lids. The mass was not fixed to
Figures 4.10A to D: (A) Photograph shows ptosis and proptosis on right side with corneal haze due to neurotrophic keratitis. The patient alsohas total ophthalmoplegia and loss of sensation in distribution of Ist division of trigeminal nerve (B) T2 weighted MRI scan shows a hypointensemass in the right lacrimal fossa extending posteriorly. Note the normal lacrimal gland in the left orbit. (C) The smears show classical magentapink rounded acellular matrix with nuclei wrapped around it. (3 D cell balls) (Giemsa, × 500). (D) The sections from the tumor showscharacteristic cribriform pattern of basaloid cells (× 100 Hematoxylin and eosin)
BA
C D
basm
ala
blog
(alw
ays o
rigin
al)

9494949494 Surgical Atlas of Orbital DiseasesSurgical Atlas of Orbital DiseasesSurgical Atlas of Orbital DiseasesSurgical Atlas of Orbital DiseasesSurgical Atlas of Orbital Diseases
overlying skin. The lids were immobile and theconjunctival surface could not be inspected. The massextended beyond the lower orbital rim, onto thecheek. There was little blood on the lid margin andeyelashes were intact (Figure 4.11A). She also hadan enlarged preauricular lymph node on the sameside and bilateral neck glands in both anterior andposterior triangles. There were no other systemicabnormalities. CT scan showed a soft tissue massinvolving the lids and anterior orbit (Figure 4.11B).FNAC was done from the orbital mass and lymphnodes which showed large pleomorphic epithelialcells, seen in tissue fragments, small clumps as wellas singly. The cells show abundant vacuolatedcytoplasm and vesicular nucleus (Figure 4.11C). Inone of the smears, an Oil Red O staining was donewhich showed prominent bright orange red globuleswithin the cytoplasm of tumor cells (Figure 4.11D),
Figures 4.11A to D: (A) Photograph shows irregular swelling of both eyelids of left eye causing mechanical ptosis and extending beyond theinferior orbital rim. The lids could not be opened or everted for further examination. (B) CT scan shows a soft tissue mass involving the anteriororbit. (C) The smears show large epithelial cells with classical vacuolated cytoplasm. Note the presence of lymphocytes in the background(hematoxylin and eosin, x 500) (D) The Oil Red O staining fo the cytology smear shows the presence of bright orange fat deposits (Oil Red Ostaining, x 500)
thus confirming the diagnosis of sebaceous glandcarcinoma, with orbital invasion and regional lymphnode metastasis.
Case 12
A 45-year old male presented with a left upper liddroop and diplopia for 1 month. There was a firm,non-tender mass in lacrimal gland region,inferomedial displacement of the globe and limitationof elevation and abduction (Figure 4.12A). Fundusexamination showed choroidal folds and globeindentation. CT scan showed a soft tissue mass inlacrimal gland region with erosion of orbital roofand intracranial extension. Orbital part of the tumorwas removed through a lateral orbitotomy. TheSquash and imprint smears showed clumps of largepolygonal cells with abundant cytoplasm, cytoplasmicpink inclusions, a large vesicular nucleus with
A B
C D
basm
ala
blog
(alw
ays o
rigin
al)

Role of Cytology in Orbital LesionsRole of Cytology in Orbital LesionsRole of Cytology in Orbital LesionsRole of Cytology in Orbital LesionsRole of Cytology in Orbital Lesions 9595959595
prominent inclusion like nucleolus.(Figure 4.12B).Histology confirmed a metastatic carcinoma with atrabecular pattern, intracytoplasmic ropy secretions,osseous metaplasia and occasional cell with bile plugs(Figure 4.12C). Subsequently, the abdominalultrasound scan showed a well-defined mass in theright lobe of liver. Metastatic deposits from breast,lung, thyroid, hepatocellular carcinoma may be seenin the orbit and show similar appearance as seen inthe primary location. This is one of the importantindication of fine needle aspiration cytology of orbitallesions which influences the surgical management ofthe case.
In summary, it is important for theophthalmologists to apply cytology to ocular lesions
Figures 4.12A to C: (A) Photograph shows non-axial proptosis with downward displacement of the left globe and fullness of the upper lidsulcus. (B) The cytology smears show large plemorphic epithelial looking cells with vesicular nucleus and prominent nucleoli. Note thecytoplasmic eosinophilic inclusions, which was reported as metastatic carcinoma. (C) The permanent sections revealed the trabecular patternosseous metaplasia and bile plugs in few cells (hematoxylin and eosin, × 500)
REFERENCES
1. Orbit FNAC Burnier Jr. MN, Correia CP, McCartney ACE.Tumors of eye and ocular adnexae. In Fletcher CDM (Ed.):Diagnostic Histopathology of Tumors, (2nd ed) ChurchillLivingstone, Edinberg. 2000;2:1757.
2. Zajdela A, de Maublanc MA, Schlienger P, Haye C.Cytologic diagnosis of orbital and periorbital palpabletumors using fine needle sampling without aspiration.Diagn Cytopathol 1986;2:17-20.
3. Vemuganti GK, Naik MN, Honavar SG, Sekhar GC. Rapidintraoperative diagnosis of tumors of the eye and orbit bysquash and imprint cytology. Ophthalmology.2004;111:1009-15.
4. Wolska-Szmidt E, Jakubowska A, Krzystolik K, Chosia M.Fine needle aspiration biopsy and molecular analysis in
differential diagnosis of lymphoproliferative diseases ofthe orbit and eye adnexa. Pol J Pathol. 2004;55:51-7.
5. Schyberg E. Fine needle biopsy of orbital tumors. ActaOphthalmol 1975;125:11-2.
6. Font RL, Laucirica R, Ramzy I. Cytologic evaluation oftumors of the orbit and ocular adenexa: an analysis of 84cases studied by the "squash technique". Diagn Cytopathol1994;10:135-42.
7. Wolska-Szmidt E, Masiuk M, Krzystolik K, Chosia M. Flowcytometry in the diagnosis of lymphoproliferative lesionsof the orbit and eye adnexa in fine needle aspiration biopsy.Pol J Pathol. 2003;54:253-9.
8. Coupland SE, Heimann H, Bechrakis NE. Primaryintraocular lymphoma: a review of the clinical,histopathological and molecular biological features. GraefesArch Clin Exp Ophthalmol. 2004;242:901-13.
which can result in early diagnosis with less invasivetechniques, sometimes obviating the need for asurgery.
A C
B
basm
ala
blog
(alw
ays o
rigin
al)

9696969696 Surgical Atlas of Orbital DiseasesSurgical Atlas of Orbital DiseasesSurgical Atlas of Orbital DiseasesSurgical Atlas of Orbital DiseasesSurgical Atlas of Orbital Diseases
9. Koss LG. Diagnostic cytology and its histopatholoigc bases,(4th ed) Philadephia: JB Lippincott,1992;1-11.
10. Tijl JW, Koornneef L. Fine needle aspiration biopsy in orbitaltumours.Br J Ophthalmol. 1991;75:491-2.
11. Liu D. Complications of fine needle aspiration of the orbit.Ophthalmology 1985;92:1768-71.
12. Ackermann LV, Ramirez GA. Indications for and limitationsof frozen section diagnosis: A review of 1269 consecutivefrozen section diagnosis. Br J Surg 1959;46:336-50.
13. Fuchs U. Smear and imprint technique in malignant lesionsof the eye. Acta Ophthalmol ( Copenh) 1988;66:445-9.
14. Akhtar M, Ali MA, Bakry M, Huq M, Sackey K. Fine Needleaspiration Biopsy diagnosis of Rhabdomyosarcoma:Cytologic, histologic and ultra-structural correlations.Diagn Cytopathol 1992;8: 465-74.
basm
ala
blog
(alw
ays o
rigin
al)
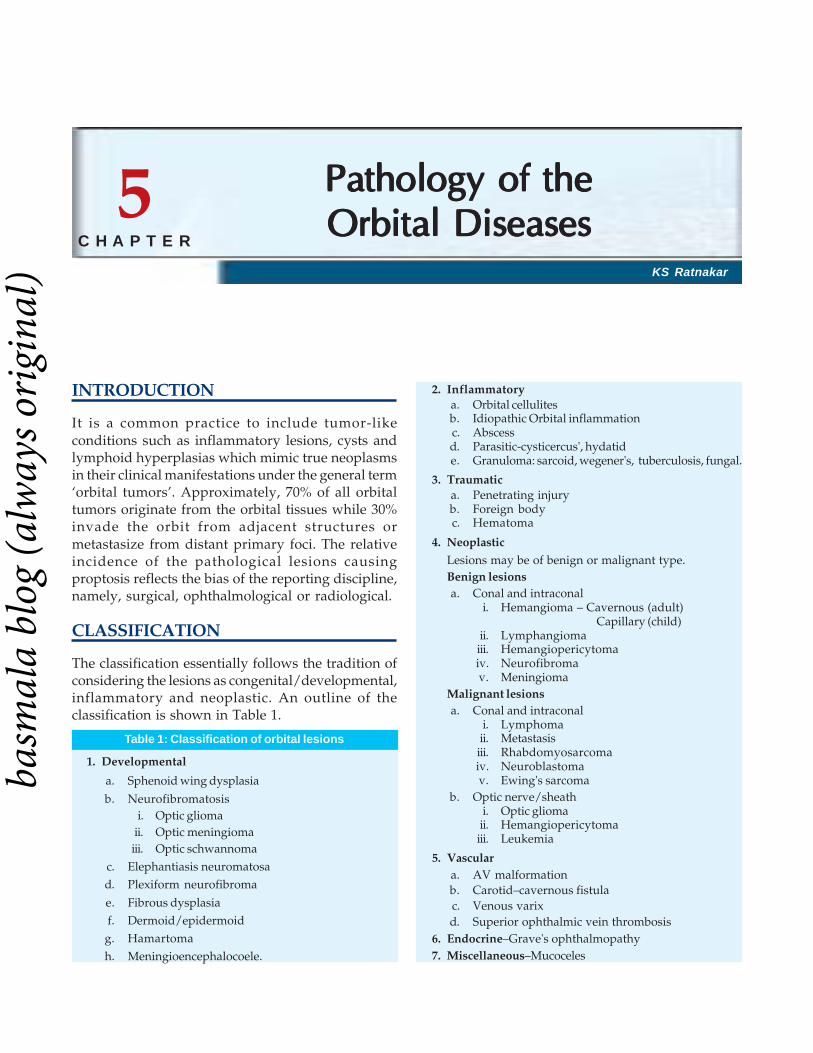
Pathology of the Orbital DiseasesPathology of the Orbital DiseasesPathology of the Orbital DiseasesPathology of the Orbital DiseasesPathology of the Orbital Diseases 9797979797
KS Ratnakar
Pathology of thePathology of thePathology of thePathology of thePathology of theOrbital DiseasesOrbital DiseasesOrbital DiseasesOrbital DiseasesOrbital Diseases
INTRODUCTION
It is a common practice to include tumor-likeconditions such as inflammatory lesions, cysts andlymphoid hyperplasias which mimic true neoplasmsin their clinical manifestations under the general term‘orbital tumors’. Approximately, 70% of all orbitaltumors originate from the orbital tissues while 30%invade the orbit from adjacent structures ormetastasize from distant primary foci. The relativeincidence of the pathological lesions causingproptosis reflects the bias of the reporting discipline,namely, surgical, ophthalmological or radiological.
CLASSIFICATION
The classification essentially follows the tradition ofconsidering the lesions as congenital/developmental,inflammatory and neoplastic. An outline of theclassification is shown in Table 1.
Table 1: Classification of orbital lesions
1. Developmental
a. Sphenoid wing dysplasia
b. Neurofibromatosisi. Optic glioma
ii. Optic meningiomaiii. Optic schwannoma
c. Elephantiasis neuromatosad. Plexiform neurofibroma
e. Fibrous dysplasiaf. Dermoid/epidermoidg. Hamartomah. Meningioencephalocoele.
2. Inflammatorya. Orbital cellulitesb. Idiopathic Orbital inflammationc. Abscessd. Parasitic-cysticercus', hydatide. Granuloma: sarcoid, wegener's, tuberculosis, fungal.
3. Traumatica. Penetrating injuryb. Foreign bodyc. Hematoma
4. Neoplastic
Lesions may be of benign or malignant type.Benign lesionsa. Conal and intraconal
i. Hemangioma – Cavernous (adult)Capillary (child)
ii. Lymphangiomaiii. Hemangiopericytomaiv. Neurofibromav. Meningioma
Malignant lesionsa. Conal and intraconal
i. Lymphomaii. Metastasisiii. Rhabdomyosarcomaiv. Neuroblastomav. Ewing's sarcoma
b. Optic nerve/sheathi. Optic gliomaii. Hemangiopericytomaiii. Leukemia
5. Vasculara. AV malformationb. Carotid–cavernous fistulac. Venous varixd. Superior ophthalmic vein thrombosis
6. Endocrine–Grave's ophthalmopathy7. Miscellaneous–Mucoceles
5C H A P T E R
basm
ala
blog
(alw
ays o
rigin
al)

9898989898 Surgical Atlas of Orbital DiseasesSurgical Atlas of Orbital DiseasesSurgical Atlas of Orbital DiseasesSurgical Atlas of Orbital DiseasesSurgical Atlas of Orbital Diseases
DIAGNOSIS OF ORBITAL TUMORS
Space occupying lesions, involving the orbit, producesymptoms and signs by compression, infiltrationand/or infarction of orbital structures. In the finalanalysis, the clinical presentation will result fromdisplacement and /or dysfunction of the globe, opticnerve, oculomotor nerve and blood vessels.
Proptosis: It is a common feature of all orbitaltumors, though its degree may vary. Those withinthe muscular cone, (e.g. optic glioma, hemangiomaand meningioma) usually produce axial proptosis, butthose outside the muscle cone, (e.g.dermoid, lacrimalgland tumor, neuroma) tend to push the eye oppositeto that of the lesion, to cause eccentric proptosis.
Optic neuropathy: Optic nerve involvement mayresult in: (a) Progressive visual loss associated withedema of disc. In many patients, however, visual lossmay be minimal and of delayed onset. In such cases,testing for color vision may reveal subtle defects evenwhen acuity is nearly normal, (b) Unilateral transientvisual loss which may occur in certain positions ofgaze and clears when the direction is changed, and(c) A specific triad may develop in chroniccompression of the optic nerve, namely loss of vision,swelling of disc which resolves into optic atrophyand appearance of optociliary shunt veins, (e.g. inspheno-orbital meningiomas).
Oculomotor paresis: The tumors located inorbital apex may involve oculomotor nerves in earlystage even before causing proptosis. Some tumorsmay involve one or two muscles, till late in thedisease. Diplopia produced by orbital masses maybe neurogenic or myogenic and rarely it may be acombination of both. The mechanical restoration ofocular mobility can be confirmed by performingcertain tests. Forced duction or traction test andintraocular pressure increase on looking in thedirection of gaze limitation are the tests of choicefor this purpose.
Pain: Most of the lesions are painless. Generally,pain is more frequent with malignant tumors. Lesionsthat involve cavernous sinuses and paranasal sinusesare usually painful.
Pupillary abnormalities: These abnormalities canoccur depending upon the involvement of theparasympathetic or sympathetic nerves, but this is
often marked by involvement of oculomotor nervepalsy.
DEVELOPMENTAL LESIONS
Sphenoid Wing Dysplasia
Pulsating exophthalmos results due to defectivedevelopment of sphenoid wing and roof of the orbit.About one-half of the cases are associated withneurofibromatosis. The lesion is evident in the earlyyears of life, starting with ptosis and thickening ofthe upper eyelid when it is associated withneurofibromatosis, followed by protrusion of the eyeball. The vision is spared till late. There is usually abulge in the temporal fossa. X-rays of the skull revealthe underlying bony deficits such as elevation ofsphenoid ridge, enlargment of the orbit, absence oftemporal line of the sphenoid wing, giving theappearance of an " empty orbit".
Neurofibromatosis
Neurofibromatosis involves the orbit either alone orin association with sphenoid dysphasia and producesa variety of orbital lesions in bony and soft tissuesegments.
The peripheral nerve sheath tumors arehistologically characterized by the presence ofpallisading spindle cells with micro or macrocysticchanges. The collagen content may vary. In plexiformtype, neurites in bundles may be seen within thestroma.
Case report: A 15-year-old boy presented withproptosis and diminished vision in the left eye. Intra-orbital soft tissue lesion was excised. He had inaddition bilateral acoustic neurinomas and intraduralneurofibroma in the lumbar region. The histologicalstudy revealed wavy spindle cells embedded in lose,fibrillary matrix. At places whirling bundles ofneuritis are noticed (Figure 5.1).
Meningioencephalocoeles
Sinonasal encephaloceles involve the medial orbitalwall and encroach into the orbit causinghypertelorism. The tissues include either meningesalone or brain parenchyma.
Case report: A 12-year-female has reported withproptosis, predominantly affecting the upper medial
basm
ala
blog
(alw
ays o
rigin
al)

Pathology of the Orbital DiseasesPathology of the Orbital DiseasesPathology of the Orbital DiseasesPathology of the Orbital DiseasesPathology of the Orbital Diseases 9999999999
aspect of left eye. Radiological examination includingCT scan and MRI revealed a cranial defect in theupper orbital wall with small cerebral parenchymaprotrusion into sac covered by meninges. Atoperation, CSF leakage was there and the sac contentsalong with contents are excised (Figure 5.2).
Dermoid and Epidermoids
These tumors result from embryonic ectodermalsequestration.
These are rare, found inside the orbit, and mostof them are located in the periorbital region.Dermoids and epidermoids have the samehistological features as seen elsewhere in the body.
Figure 5.1: Spindle cells showing wavy pattern in a case ofNeurofibroma. H and E × 400
Figure 5.2: Histological section showing Neuroglial elements in thewall of the Meningioencephalocoele. H and E × 400
Figure 5.3: Section showing cyst lined by epidermis with dermalappendages from a case of dermoid cyst H and E × 400
They are invariably benign and can be excised withease.
Case report: A 6-year-male child admitted withbulging at the root of nose along with fullness in theupper medial compartment of right eye. Radiologicalinvestigations showed a mass involving the anteriorbase of the frontal bone with orbital extension of thelesion (Figure 5.3).
Hamartoma
Hamartoma is a type of congenital lesion composedof tissues normal to the location. One type oftissue may be predominantly seen such as vasculartissue.
Fibrous Dysplasia
Fibrous dysplasia is a non-neoplastic disease of thebone that affects children and young adults.Craniofacial fibrous dysplasia is a benign conditionforming about 3% of all bone tumors. Dysplasia offrontal, sphenoid, ethmoid, zygomatic and maxillarybones may involve the orbit causing visualsymptoms. The symptoms may range fromprogressive visual loss to proptosis or orbitaldistortion. The lesion is usually painless. On plain X-rays the lesion appears as ground glass, milky andsclerotic and in most cases some areas of radiolucencymay be observed. Histological changes are consistentwith an arrest in the development of immaturewoven bone into more mature lamellar bone
basm
ala
blog
(alw
ays o
rigin
al)

100100100100100 Surgical Atlas of Orbital DiseasesSurgical Atlas of Orbital DiseasesSurgical Atlas of Orbital DiseasesSurgical Atlas of Orbital DiseasesSurgical Atlas of Orbital Diseases
embedded in cellular fibrous stroma. No osteoblasticrimming is seen around osseous islands. The wovenbone may appear as' Chinese figures' often describedto indicate their focal irregular pattern. The stromatends to be fibrous in older individuals (Figure 5.4).
INFLAMMATORY LESIONS
Orbital Cellulitis
Orbital cellulites can remain as a diffuse inflammationor progress to loculation to form an abscess. Thereis usually a profound disturbance of oculomotorfunctions, pain and constitutional symptoms.Occasionally, the abscess may become chronic andthe lesion may manifest like any begin spaceoccupying lesion. Pathology reveals diffusesuppurative inflammation composed of neutrophils.
Idiopathic Orbital Inflammation
Idiopathic orbital inflammation is the most commoncause of an intraorbital mass.
The condition is usually diagnosed clinically withclassic symptoms of painful proptosis and restrictionof extraocular muscle often unilateral. It is achallenging mimicker of an intraorbital neoplasm andis often a diagnosis by exclusion of other surgicallyremediable entities. The exact etiology is not known.Autoimmune response to antigen has beenimplicated. Perhaps the condition is multifactorial.IOI is often a diagnosis of exclusion of specific
etiologies. Every attempt has to be made to find thecause prior to labeling the condition as idiopathicorbital inflammation.
Lymphoid lesions of the orbit continue to poseproblems to the ophthalmologists and pathologistsas well. Despite increase in understanding andimproved methodology the diagnosis is often difficultand intrigues the treating surgeon.
The inflammatory lymphoid lesions which arealso called orbital idiopathic inflammation addfurther confusion to the understanding of the diseaseprocess.
Arnold and Becker (1972) and Hochheim (1900)first attempted to classify the lymphoid lesions ofthe orbit into four categories namely benignlymphoma, follicular lymphoma, lymphosarcomaand lymphatic leukemia. In these groups, the firsttwo possibly belong to the lesions of inflammatoryorigin. Blodi and Gass(1968) carefully analysed thenon-neoplastic lymphoid lesions and divided theminto follicular, diffuse lymphocytic and benignlymphocytic hyper plastic varieties. Morgan andHarry (1978) studied 98 cases of lymphoid lesionsand considered large number of cases that remainedconfined to the orbit are of inflammatory nature.These lesions have been termed by them aslymphocytic tumors of indeterminate nature.
These classifications in the present era ofmolecular markers, are unscientific and redundant.
Clinically, the inflammatory benign lymphoidlesions present with exophthalmos with conjunctivaledema, pain/inflammatory signs and occasionallywith palpable mass. There is no specific age or sexpredilection but appears to affect young adultspredominantly. Right eye appears to be involvedmore frequently than the left and small percentageis found to occur bilaterally. The duration of asymptomatology varies from less than a month toover several years. These tend to heal or improveover a period of time with steroids and/orantibiotics. Small but significant percentage of lesionsmay focally recur, but do not necessarily indicatemalignancy in all the cases. However, careful clinicalfollow-up is advised and a thorough systemicexamination. It is imperative to rule out anydisseminating malignant lymphoid lesions. Morganand Harry (1978) observed in over 25% of cases areassociated lymphoid malignancy elsewhere in the
Figure 5.4: Woven bone without osteoblast rimming in a case offibrous dysplasia H and E × 400
basm
ala
blog
(alw
ays o
rigin
al)

Pathology of the Orbital DiseasesPathology of the Orbital DiseasesPathology of the Orbital DiseasesPathology of the Orbital DiseasesPathology of the Orbital Diseases 101101101101101
body. This finding necessitates cautious thinking ofany lymphoid lesion in general.
However, Knowle et al. (1979) using moleculartechniques, made useful and important observationthat benign reactive lymphoid hyperplasias areimmunologically polyclonal whereas malignantlymphomas are monoclonal in nature.
The lymphoid lesions apparently looking benignmay present primarily in the orbit with its systemicinvolvement being observed at a later date. Thepathobiology cannot be clearly defined in the earlystages without application of molecular markers whichare rather defined. Hence the wisdom lies in carefulclinical and histological interpretation (Figure 5.5).
Orbital InfectionsAspergillosis
Aspergillosis is a fungal disease caused by aspergillusfumigatus, the most common causative species.Aspergillosis involving the orbit and cranial contentis rare. Paranasal sinus aspergillus infections areclassified as non-invasive and invasive types.
The invasive or fulminant type of aspergillosisoccurs primarily in immunologically compromisedindividuals. The clinical manifestations include arapidly progressive gangrenous necrosis ofthe mucoperiosteum, with destruction of nasalbones of the paranasal sinuses and orbital wall. Theremay be intracranial invasion. The orbital extension
is reflected by soft tissue densities extending fromthe sinuses especially the ethmoids into the orbitalcavity. Some degree of bone destruction is identifiedin combination with the fungal infiltrate.
The histology in acute form shows necrotisingvasculitis associated with soft tissue invasion byfungal filaments. In chronic form, there isgranulomatous reaction and fibrosis (Figure 5.6) Intraand extracellular aspergillus is demonstrable byfungus stains such as PAS and silver methanamine(Figure 5.7).
Case report: A 60-year diabetic reported withpainless proptosis of right eye of several weeksduration. There was restriction of ocular movementsin all directions. Orbital exploration revealed a toughsoft tissue lesion which resisted complete dissectionand excision. Histology showed many granulomascontaing foreign body giant cells containing fungalfilaments characteristic of aspergillous species.
Tuberculosis
Orbital tuberculosis is rare. In endemic areas,tuberculous infection should be considered as animportant entity in the aetiology of orbitalinflammation. Orbitomorphologically the lesionshows caseating coalescing granulomas. There maybe variable degree of fibrosis. Similar histoplasmosismay be encountered in brucellosis, histoplasmosis,sarcoidosis. Hence thorough clinical examination
Figure 5.5: Lymphoid aggregates with prominent germinal centersfrom a case of pseudo-lymphoma H and E × 400
Figure 5.6: Histological section showing foreign body type of giantcells in a granualomatous lesion. From case of Aspergilloma, orbit Hand E × 600
basm
ala
blog
(alw
ays o
rigin
al)

102102102102102 Surgical Atlas of Orbital DiseasesSurgical Atlas of Orbital DiseasesSurgical Atlas of Orbital DiseasesSurgical Atlas of Orbital DiseasesSurgical Atlas of Orbital Diseases
serological and/or cutaneous tests should beconducted for final diagnosis.
Cysticercosis
Cysticercosis of the orbit is very rare in the westernliterature, but Jacobiece and Font (1986) nath etal. (1977) documented nearly 24 cases in theliterature. Sarada et al. (1981) found one case inthe orbit among 50 cases of cysticercosis of the CNS.But in endemic areas orbital myocysticercosis isfairly common. They are usually managed with oralAlbendazole and prednisolone. Only anteriorlylocated cysticercosis is excised and is available forhistopathology (Figure 5.8). However, Murthy etal. (1990) reported on the use of ultrasound inpreoperative diagnosis.
Cysticercus cellulosae, histologically, whensectioned shows fibrocellular, reaction withpalisading histiocytes around the parasite. The wormmay get calcified in later stages. The cellular infiltratemay be dominated by eosinophils.
Neoplastic Lesions
Classification of orbital tumors is given in Table 2Benign tumors.
Table 2: Classification of orbital tumors
PrimaryI. Mesenchymal
a. Vascular: hemangioma, lymphangioma, heman-giopericytoma, hamangioendothelioma, Angiosar-coma, Kaposi’s sarcoma,
b. Lipoma, liposarcomac. Fibrous histiocytoma,d. Fibrosarcomae. Rhabdomyosarcomaf. Leiomyoma, sarcomag. Chondroma, chondrosarcomah. Giant cell tumor, osteosarcoma.
II. NeuralGlioma, neurilemmoma, neurofibroma, amputationneuroma.
III. Hemopoietic.Lymphoma, leukemia, myeloma.
IV. Lacrimal glandPlemorphic adenoma, adenoid cystic carcinoma.
V. MiscellaneousMeningioma, nonchromaffin paraganglioma, alveolarsoft part sarcoma, malignant melanoma.
SecondaryI. Direct extension
a. Intraocular tumors retinoblastoma, melanomab. Eyelid tumors basal, squamous, sebaceous
carcinoma, melanomac. Conjunctival squamous carcinoma, melanomad. Metastatic in children – neuroblastoma
In adults–Lung Ca, Breast Ca.
Figure 5.7: Fungal filaments of Aspergillus species. Silvermethanamine × 400
Figure 5.8: Cross-section of cysticercus. H and E × 400
basm
ala
blog
(alw
ays o
rigin
al)

Pathology of the Orbital DiseasesPathology of the Orbital DiseasesPathology of the Orbital DiseasesPathology of the Orbital DiseasesPathology of the Orbital Diseases 103103103103103
BENIGN TUMORS
Cavernous Hemangioma
The most common benign intraorbital tumor in theyoung and middle aged is cavernous hemangiomathat produces painless proptosis. It is common infemales and may enlarge during pregnancy.
Despite the mention that cavernous hemangiomais the most common benign intraorbital tumor, therehave not been many reports of a good series of thiscondition. Harris and Jacobiec (1979) could find 66cases recorded during a 40 year period from threecenters dealing specially with ophthalmic problems.Maroon and Kenerdell (1979) found five heman-giomas among 18 intraorbital tumors subjected tomicrosurgical treatment. The same authors reported17 hemangiomas among 300 cases of orbitaltumors seen from 1975 to 1982. Nath et al. (1977)found 12 cases among 120 cases of primary orbitaltumors.
Being a benign slow growing tumor, it causesprogressive often painless proptosis. As the lesion isusually situated behind the globe within the musclecone, it produces axial proptosis.
Despite the prominent protrusion of the eyeball,vision is preserved and movements of the eye arespared till late in the course. About half of the patientsin the series of Harris and Jacobiec(10979) hadblurred vision and only three of the 66 had diplopia.Neither bruit nor pulsations were present in any oftheir cases.
Microscopically, the lesion is composed of dilatedvascular channels. Some of the channels may containprominent smooth muscles when the lesions arecalled venous hemangiomas (Figure 5.9).
Capillary Hemangioma
Capillary hemangioma is a benign tumor thatmanifests usually in first five years of life and tendsto regress thereafter. It is generally single, brightred and smooth lesion. Histologically, capillaries ofsmall size are closely packed with no smooth musclein between (Figure 5.10).
Lymphangioma
There are no lymphatics in the orbit. However,lymphangiomas do occur here and account for 0.5 to3% of intraorbital tumors. It is commonly seen in
children and adolescents. Spontaneous hemorrhageinto the cyst leads to abrupt proptosis and formationof “chocolate cysts”. Lymphangioma occurs inextraconal location and presents with pain andproptosis. Infiltration of muscles and nerves of orbitalso occurs in this condition (Figure 5.11) .
Hemangiopericytoma
It is a rare lesion occurs in the fourth decade of life.It may be malignant in about 12% cases. The lesionconsists of increased number of thin-walled vascular
Figure 5.9: Histological section from a case of cavernoushemangioma, showing widely spaced vascular channels rimed byfibromuscular tissue. H and E × 400
Figure 5.10: Polypoidal tissue composed of proliferating vascularchannels embedded in a inflammatory and edematous stroma from acase of capillary hemangioma, pyogenic type. H and E × 400
basm
ala
blog
(alw
ays o
rigin
al)

104104104104104 Surgical Atlas of Orbital DiseasesSurgical Atlas of Orbital DiseasesSurgical Atlas of Orbital DiseasesSurgical Atlas of Orbital DiseasesSurgical Atlas of Orbital Diseases
channels with perivascular massing of pericytesseparated by tumor cells in a network of extracellularmaterial (Figure 5.12).
Meningiomas
Orbital meningiomas are of three types based on theirorigin—
1. Intracranial meningiomas which secondarilyinvade the orbit are the commonest.Meningiomas of the middle cranial fossaespecially those of sphenoid ridge are notoriousto cause proptosis. Meningiomas of the anteriorcranial fossa may invade the orbital roof. In
addition ectopic meningiomas arising from, forexample, the frontal sinus may encroach into theorbit.
2. Primary intraorbital meningiomas are raretumors which arise from the optic nerve. This isthe most difficult one to treat. Thedifferentiation between optic nerve gliomaand meningioma is an important clinicalproblem.
3. Those which have no apparent connection withthe optic nerve are occasionally found in theorbit. These probably arise from ectopicarachnoid cell nests in the orbit.
Intraorbital meningiomas are more commonin women than men. The average age of onsetis about 30 years. About 40% occur below 20years. The main clinical features are loss ofvision and progressive exopthalmos. Neuro-fibromatosis may be associated within16% of cases (Figure 5.13).
Malignant Tumors
RhabdomyosarcomaRhabdomyosarcoma is the most commonmalignant mesenchymal orbital neoplasm andmalignant orbital tumor in children. The average ageof onset is six years and the lesion is rare after 25years. The onset is rapid and the progressionsimulates cellulitis. Histologically, the tumors are of
Figure 5.11: Section showing dilated vascular channels with lym-phoid aggregates in the mural compartment from a case ofLymphagioma. H and E × 400
Figure 5.12: Histological section showing thin vascular channelswith oval to spindle cells oriented externally from a case ofHemangiopericytoma. H and E × 600
Figure 5.13: Section shows oval to polyhedral cells with vesicularnuclei and lightly acidophilic cytoplasm arranged in nests and whorls.There are scattered psammoma bodies, from a case of meningioma.H and E × 400
basm
ala
blog
(alw
ays o
rigin
al)

Pathology of the Orbital DiseasesPathology of the Orbital DiseasesPathology of the Orbital DiseasesPathology of the Orbital DiseasesPathology of the Orbital Diseases 105105105105105
three types (i) embryonal (ii) adult pleomorphic and(iii) alveolar.
Of these three types embryonal rhabdomyo-sarcoma is the most common type of malignanttumor. Structurally, tumors are composed of round,oval or stellate rhabdomyoblasts with mitosis inloose syncitium. Cells contain dense eosinophiliccytoplasm with striations.
Mortality rate is 40.6%. Prognosis is best in adultpleomorphic type and it is worst in alveolar type(Figures 5.14 and 5.15).
Adenoid Cystic Carcinoma
It occurs in adults of either sex in the fourthdecade of life. The lesion is relentlesslyprogressive, invading the adjacent tissues withcharacteristic tendency to spread along perineurallymphatics (Figure 5.16).
Lymphoma
Lymphomas in adults are encountered in 10%biopsies of orbital tumors. They are usually found inthe anterior orbit. About 25% of lymphomapresenting as NSOID may evolve into lymphomas.They are essentially B cell lymphomas. Orbitallymphomas may be the first manifestation of systemiclymphomas (Figure 5.17).
Histiocytoma
Malignant fibrous histiocytomas are rare, and morelethal lesions of orbit. These are common in olderage group. The origin of the tumor is from thehistiocytes,and the neoplastic histiocytes are bizarrewith areas of hemorrhage,necrosis and frequentmitosis. Focal or diffuse storiform patterncharacteristic of histiocytomas is discernible .
Metastasis
It accounts for 5% of orbital tumors. In children,neuroblastoma, ewing's and leukemia and in adults,carcinoma of bronchus and breast are the common
Figure 5.14: Cellular lesion showing spindle cells with acidophiliccytoplasm arranged in alveolar pattern in a case of alveolar rhab-domyosarcoma H and E × 400
Figure 5.15: Cellular lesion showing spindle cells with acidophiliccytoplasm arranged in alveolar pattern in a case of alveolar rhab-domyosarcoma. H and E × 600
Figure 5.16: Large cellular islands of basaloid cells with focal cysticpattern embedded in fibro vascular tissue. From a case of adenoidcystic carcinoma of the orbit. H and E × 400
basm
ala
blog
(alw
ays o
rigin
al)

106106106106106 Surgical Atlas of Orbital DiseasesSurgical Atlas of Orbital DiseasesSurgical Atlas of Orbital DiseasesSurgical Atlas of Orbital DiseasesSurgical Atlas of Orbital Diseases
primary sites. In about 50% of the cases the primaryremains unknown. Of all metastases 30% are orbitaland 70% ocular. The main symptoms are pain,proptosis and limitation of extraocular movements.Undifferentiated carcinomas arising in a paranasalsinus account for 4-9% of unilateral exophthalmos.The carcinoma of ethmoid most commonly involvesthe orbit. Pain, proptosis, restricted ocular motility,with ptosis occurring rapidly is a feature ofmalignancy of the orbit.
Optic Glioma
Optic glioma are primary tumors of the optic nerveand/or chiasma. They are usually low grade pilocyticastrocytomas which may appear fibroblastic due toinvasion of the leptomeninges (desmoplastic) orgelatinous with oligodendroglial component. Thoseof the optic nerve may be intraorbital or intracranial(Robertson and Broson, 1980; Alvord and Lofton, 1988).
Grave’s Disease
It is one of the most common causes of proptosiswhich mostly affects females. Lid retraction is anearly sign. These orbital signs may manifest at anystage of the endocrine dysfunction. Computedtomography and ultrasonography may reveal thecharacteristic thickening of extraocular muscleswithout evidence of mass lesion. The lesion is often
bilateral, though the patient may present when it isstill confined to one orbit. Microscopic examinationshows edema, lymphocytic infiltration sometimesforming follicles.
MISCELLANEOUS
Mucoceles
Mucoceles of the paranasal sinuses may requireneurosurgical attention when they involve the orbitand/or cranial contents. The most frequent site isthe frontal sinus.
Those involving the sphenoid and/or posteriorethmoidal sinuses are rare. Chen et al. (1986) andNugent(1970) reviewed 63 cases in whom visualimpairment was noted in 71% of the cases. Opticnerve damage may be caused by intracanalicularextension of the lesion with erosion of the canal walls.
Periorbital swelling, pain and displacement ofglobe are the frequent symptoms of frontal andethmoidal lesions. There may be a swelling over thefrontal sinus with crackling sensation on palpationdue to thinning of its anterior wall. Sphenoidal sinusmucoceles cause headache, peri or retroorbital painand ophthalmoplegias due to extension into theorbital apex and cavernous sinus (pompili et al. 1990).
Sellar involvement is seen frequently insphenoidal mucocele. Surgical intervention andexcision of the lesion is indicated to relieve pressureon the orbital contents.
The aetiology of mucoceles is multifactorial. Thebasic cause seems to be obstruction of the ostium ofthe sinus by a variety of causes such as inflammation,trauma, polyps, previous surgery, allergy and benignand malignant tumors. The exact precipitating factormay not be evident in many cases (Weber andMikulis, 1987).
Histological examination (HPE) revealsfragments of polypoid tissue lined by pseu-dostratified ciliated epithelium. The sub epithelialtissue is made up of loose stroma with pools of smallblood vessels and diffuse infiltration of mononuclearcells and prominent collections of eosinophilsembedded with calcific spicules.
Figure 5.17: Cellular lesion composed of monomorphic round cellswith dark nuclei and scant cytoplasm seen in nodular aggregatesform a case of orbital lymphoma. H and E × 400
basm
ala
blog
(alw
ays o
rigin
al)

Pathology of the Orbital DiseasesPathology of the Orbital DiseasesPathology of the Orbital DiseasesPathology of the Orbital DiseasesPathology of the Orbital Diseases 107107107107107
BIBLIOGRAPHY
1. Bakhshi S, Sidhu T: Pediatric orbital and ocular lymphomas,Pediatr Blood Cancer. 2008;50(4):940-1.
2. Bernardini FP, Bazzan M: Lymphoproliferative disease ofthe orbit, Curr Opin Ophthalmol. 2007;18(5):398-401.
3. Biswas J, Roy Chowdhury B, Krishna Kumar S, Lily ThereseK, Madhavan HN: Detection of Mycobacteriumtuberculosis by polymerase chain reaction in a case of orbitaltuberculosis, Orbit. 2001;20(1):69-74.
4. Butnor KJ, Cummings TJ. Pathologic quiz case: left eyeproptosis, ptosis, and blindness. Hemangiopericytoma ofthe orbit. Arch Pathol Lab Med. 2002;126(12):1555-6.
5. Cruz AA, Constanzi M, de Castro FA, dos Santos AC: Apicalinvolvement with fibrous dysplasia: implications for vision,Ophthal Plast Reconstr surg 2007;23(6):450-4.
6. Eddleman CS, Liu JK: Optic nerve sheath meningioma:current diagnosis and treatment, Neurosurg Focus.2007;23(5):E4.
7. Goisis M, Biglioli F, Guareschi M, Frigerio A, Mortini P:Fibrous dysplasia of the orbital region: current clinicalperspectives in ophthalmology and cranio-maxillofacialsurgery, Ophthal Plast Reconstr Surg. 2006;22(5):383-7.
8. Gordon LK: Orbital inflammatory disease: a diagnostic andtherapeutic challenge, Eye. 2006;20(10):1196-206.
9. Harris GJ, Jakobiec FA. Cavernous hemangioma of theorbit: A clincopathological analysis of sixty-six cases. In:Ocular and adnexal tumors. Birmingham, AL: Aesculapius,1978;741-81.
10. Honavar SG, Sekhar. G, Orbital Cysticercosis. Orbit 1998;17(4)271-84.
11. Kaur A, Kant S, Bhasker SK: Periorbital tuberculosis, Orbit.2007;26(1):39-42.
12. Lee V, Ragge NK, Collin JR. Orbitotemporal neuro-fibromatosis. Clinical features and surgical management,Ophthalmology. 2004;111(2):382-8.
13. Lin B, Looi A: Orbital lymphoma, Ophthalmology.2007;114(7):1423.
14. Malhotra R, Wormald PJ, Selva D. Bilateral dynamicproptosis due to frontoethmoidal sinus mucocele. OphthalPlast Reconstr Surg. 2003;19(2):156-7.
15. Nugent RA, Rootman J, Robertson WD, et al. Acute orbitalpseudotumors: AJNR 1981;2:431-6.
16. Perry SR, Rootman J, White VA. The clinical andpathological constellation of wegener's granulomatosis ofthe orbit. Ophthalmology 1997;104:683-94.
17. Pillai S, Malone TJ, Abad JC. Orbital tuberculosis. OphthalPlast Reconstr Surg 1995;11:27-31.
18. Rootman J, Hay E, Graeb D, et al. Orbital adenexallymphangiomas A spectrum of hemodynamicallyisolated vascular hamartomas. Ophthalmology.1986;93:1558-70.
19. Rootman J: Diseases of the orbit; A multidisciplinaryapproach. Lippincott Williams and Wilkins, (2nd Ed):455-506.
20. Selva D, White VA, O'Connell JX, Rootman J: Primary bonetumors of the orbit, Surv Ophthalmol. 2004;49(3)328-42.
21. Shields JA, Shields CL, Scartozzi R. Survey of 1264 patientswith orbital tumors and simulating lesions: The 2002Montgomery lecture, part 1. Ophthalmology. 2004;111(5):997-1008.
22. Siraj CA, Krishnan J, Nair RR, Girija AS: Invasiveaspergillosis producing painful ophthalmoplegia, J AssocPhysicians India. 2005;53:901-2.
23. Swamy BN, McCluskey P, Nemet A, Crouch R, Martin P,Benger R, Ghabriel R, Wakefield D: Idiopathic orbitalinflammatory syndrom: clinical features and treatmentoutcomes, Br J Ophthalmol. 2007;91(12):1667-70.
basm
ala
blog
(alw
ays o
rigin
al)

basm
ala
blog
(alw
ays o
rigin
al)

basm
ala
blog
(alw
ays o
rigin
al)

Peter J Dolman
Thyroid-AssociatedThyroid-AssociatedThyroid-AssociatedThyroid-AssociatedThyroid-AssociatedOrbitopathyOrbitopathyOrbitopathyOrbitopathyOrbitopathy
Figure 6.1: Axial CT scan of patient with asymmetric TAOdemonstrating right proptosis from marked enlargement of the rightorbital muscles and mild enlargement of the fat compartment. Comparethe affected right orbit with the normal left orbit
Figure 6.2A: Mild TAO in a young female with bilateral upper lidretraction (worse on the left side) and secondary ocular irritation andepiphora
Figure 6.2B: Same patient at the time of surgery following aposterior graded lowering of both upper eyelids
Introduction
Thyroid-associated orbitopathy (also known asGraves’ Orbitopathy, Graves’ Ophthalmopathy,Thyroid Eye Disease) is an immune-mediatedinflammatory disorder causing enlargement of theorbital muscles and fat (Figure 6.1).1,2 Its clinicalspectrum ranges from eyelid retraction and proptosiswith exposure complaints (Figure 6.2A) to moreserious problems such as orbital soft tissueinflammation (with discomfort, eyelid andconjunctival congestion and edema), extraocularmotility restriction, and loss of vision fromcompressive optic neuropathy (Figure 6.3A).3
Severe cases may result in lasting cosmeticdisfigurement and functional visual impairment.Quality of life studies have shown that it may have
6C H A P T E R
basm
ala
blog
(alw
ays o
rigin
al)

112112112112112 Surgical Atlas of Orbital DiseasesSurgical Atlas of Orbital DiseasesSurgical Atlas of Orbital DiseasesSurgical Atlas of Orbital DiseasesSurgical Atlas of Orbital Diseases
Figure 6.3A: Patient with severe manifestations of TAO: VISA Score:V = 1/1 (bilateral optic neuropathy with vision reduced to 20/100,20/80); I = 9/10 (pain at rest and movement, +2 chemosis, +1 eyelidedema, +1 caruncular edema, +1 conjunctival redness, +1 eyelidredness); S = 3/3 (motility restricted to less than 15° upgaze bilaterally);A = 3/3 (corneal ulceration, Hertel 26 mm bilaterally)
Figure 6.3B: Same patient following intravenous pulsedcorticosteroids, orbital decompression, and upper lid posteriorlowering. VISA Score: V = 0/1 (no optic neuropathy); I = 0/10; S = 1/3 (eyes aligned but restricted to 30° motility); A = 1/3, mild (someresidual upper eyelid deformity, Hertel 21 mm bilaterally)
more significant lifestyle consequences than chroniclung disease or diabetes mellitus.4
Incidence and Epidemiology
Thyroid-associated orbitopathy (TAO) is the mostcommon orbital disease in the Americas and Europe,with an annual incidence in females of approximately14 per 100,000 and approximately one-fifth that formales.5 Anecdotally, it may be less prevalent (orpossibly causes fewer severe complications) in Africaand South Asia. However, it does occur in all racesand ages, and is most common between the secondand sixth decades.6
Between 25-50% of patients with immune thyroiddiseases develop orbital involvement, and of those,5-10% may develop more severe consequences suchas severe inflammation and congestion, impairedmotility, or compressive optic neuropathy.7 A smallerpercentage may develop Graves’ lower limbdermopathy (pretibial myxedema, with depositionof subdermal hyaluronic acid), usually 1-2 yearsfollowing the onset of thyroid gland dysfunction andshortly following severe orbitopathy, and a smallersubset may develop acropachy (clubbing of thefingers).8
Risk Factors, Predictive Variables forDisease Severity and Associated ImmuneDisorders
Risk factors for developing TAO include smoking,life stressors, poorly controlled hypothyroidismfollowing radioactive iodine, and a positive familyhistory of orbitopathy.9,10
Predictive variables for developing more seriousconsequences of TAO include male gender,increasing age, smoking, and a rapid onset oforbitopathy.11
Cigarette smoking has been shown by numerousstudies to be correlated strongly with thedevelopment of TAO and a progressively higherincidence of smoking is seen with more severedisease.11-13
Patients with TAO have an increased probabilityof developing associated immune diseases, includingsuperior limbic keratitis (SLK), myasthenia gravis,diabetes mellitus, alopecia and vitiligo.14 Psychiatricconditions such as bipolar affective disorder andanxiety occur more frequently in patients withthyroid dysfunction and with TAO.
Pathogenesis
The pathologic hallmark of TAO is a lymphocyticinfiltration of orbital muscle and fat with expansionof these tissues from edema and deposition ofhyaluronic acid and other glycosaminoglycans.2
Patients exhibiting fat expansion alone may presentwith proptosis and lid retraction. Those with muscleenlargement and more inflammatory features maydevelop proptosis, periocular inflammatory features,and possible restriction of motility or strabismus iffibrosis develops (Figure 6.4). In a limited number
basm
ala
blog
(alw
ays o
rigin
al)

Thyroid-Associated OrbitopathyThyroid-Associated OrbitopathyThyroid-Associated OrbitopathyThyroid-Associated OrbitopathyThyroid-Associated Orbitopathy 113113113113113
Figure 6.4: Patient with TAO myopathy attempting to look up-wards.She had bilateral upgaze limitation, the right reaching 30° and the leftreaching 10°, based on the light reflexes on her cornea (VISAstrabismus score = 3/3)
Figure 6.5A: Coronal CT scan near apex showing bilateral opticnerve crowding. This patient had impaired central vision (20/70, 20/40), bilateral reduced color vision, and a right afferent pupil defect.VISA Score: V = 1/1 (optic neuropathy present)
Figure 6.5B: Axial CT scan of same patient showing adequate medialwall decompression into ethmoid sinuses and resolution of opticneuropathy (V = 0/1; central vision 20/20 both eyes)
of patients with severe myopathy, or with a narrowboney orbital apex, or with tight lids limiting anteriordisplacement of tissues, compression of the opticnerve may ensue (Figure 6.5A).
TAO is an immune-mediated disease which isstrongly associated with thyroid immune disorderssuch as Graves' disease or Hashimoto's thyroiditis.90% of patients with orbitopathy have a current orpast history of abnormal systemic thyroid hormonelevels, while others may develop abnormal levels inthe future. It is important to explain to patients thatthe orbitopathy is associated with, but not causedby, abnormal thyroid hormone levels, since patientsoften believe that the orbital disease should resolveonce a euthyroid state is reached.
Thyroid gland epithelial cells have surfacereceptors which bind thyroid stimulating hormone(TSH, thyrotropin), a hormone secreted in pulses bythe pituitary to control the release of thyroidhormone. In both Graves’ disease and Hashimoto'sthyroiditis, circulating thyrotropin-receptorantibodies (TSH-R Antibodies, TRAb) are presentwhich can bind to these same receptor sites, andinitiate and perpetuate the disease.2 At least threesubtypes of TRAb have been identified, presumedto arise from a small population of abnormalB-lymphocytes: (1) TSI (thyroid stimulatingimmunoglobulin), which causes hyperthyroidism;(2) blocking TRAb, which prevents TSH from bindingto thyroid cells and results in hypothyroidism;
(3) binding TRAb, which binds onto TSH receptorstransiently, and has little effect on overall thyroidhormone levels.
These circulating antibodies are thought to bemediators in orbitopathy as well, with the likelytarget being the orbital fibroblast.2 Orbital fibroblastsare present in extraocular muscle and in orbital fat.Orbital fibroblasts from patients with TAO haveincreased numbers of TSH-Receptors, which arethought to bind to circulating autoantibodies (TRAb),stimulating adipogenesis and deposition ofhyaluronic acid within orbital muscle and fat, thehistologic hallmark of TAO.
basm
ala
blog
(alw
ays o
rigin
al)

114114114114114 Surgical Atlas of Orbital DiseasesSurgical Atlas of Orbital DiseasesSurgical Atlas of Orbital DiseasesSurgical Atlas of Orbital DiseasesSurgical Atlas of Orbital Diseases
Orbital fibroblasts in patients with TAOhave also recently been shown to have anincreased number of receptors to “insulin-like growthfactor-1” (IGF-1 R), and serum from patients withTAO has been found to have circulating antibodiesdirected against IGF-1 receptors.15 Binding of IGF-1receptors has been shown to attract and activate T-lymphocytes and macrophages through inflam-matory mediators, which may be the mechanism ofinitiating and propagating the inflammatory andimmune cascade in TAO.16
Course of Disease
As with other immune disorders such as rheumatoidarthritis or Sjogren’s disease, TAO typically has aprogressive (active) inflammatory phase followed bya stable (inactive) postinflammatory phase. Thispattern of the disease was first described by Rundle,and the plot of orbital disease severity against timehas been called Rundle's curve.17,18 The steepness ofthe graph in the active phase reflects the acuity ofprogression, with a steeper slope often leading tomore serious sequellae.11
The duration of the active phase may last from6-18 months, during which the patient mayexperience inflammatory symptoms of orbitaldiscomfort, periocular and conjunctival edema andredness, and progression in proptosis, strabismus oroptic neuropathy. Management during this phase isaimed at modulating the immune response andreducing the inflammation, usually with the use ofsteroids, radiotherapy, or other immunosuppressiveagents, and hopefully limiting the destructiveconsequences of the active phase.
A useful analogy for patients is that theinflammatory phase is like a house on fire. Whileignited, efforts are made to staunch the flames orallow them to smolder if not too severe. Recons-truction is not carried out while the fire is still active.
Once the disease has become quiescent, surgerymay be offered to rectify damage resulting from theactive stage, including reducing proptosis, aligningmuscles, narrowing eyelid apertures, and debulkingfat pockets in the eyelids. This would be similar torepairs being carried out after the house fire wassuppressed.
Reactivation of disease is fairly uncommon,19
occurring in less than 5% of individuals, and is
sometimes associated with a major life stressor suchas a family death, divorce or loss of job.
Clinical Classification
One of the challenges in TAO is how to classify andgrade its various clinical manifestations so thatappropriate management can be instituted.
Most ophthalmologists are familiar withDr Werner’s NO SPECS classification that gradedvarious symptoms and signs associated with thedisease and assigned a global severity score.20 Whilethis has served as a useful mnemonic for the differentfeatures of TAO, it is weak in terms of definingmanagement and doesn't assess whether the diseaseis in the active or inactive, postinflammatory phase.
In 1989, Drs Mourits et al introduced a clinicalactivity score (CAS) to stage and grade theinflammatory phase of the disease.21
The VISA Classification
We have recently introduced the VISA classificationwhich is a clinical recording form designed for theoffice, and which separates the various clinicalfeatures of TAO into four parameters: V (vision, opticneuropathy); I (inflammation, congestion);S (strabismus, motility restriction); A (appearance,exposure).22
The basic visit form (Figure 6.6) includes the foursections recording historical symptoms on the leftand signs on the right. After each section is a progressrow (better, same, worse), recording both thepatient's and clinician's impression of the course ofthe disease since the last visit. The layout is designedto simplify data recording and possible later researchdata collation. Individual measurements may becompleted in as much or little detail as the clinicianchooses. At the end of the form is a summary gradefor the activity and severity for each of the fourdisease parameters and a space for investigations andmanagement plan.
On the first visit, the date and rate of onset ofboth the systemic and orbital symptoms should berecorded, since this may help predict the ultimateseverity of the inflammatory phase.a) Vision/optic neuropathy: The focus of thissection is to identify TAO optic neuropathy.The history includes visual blurring or colordesaturation and the progress and duration ofsymptoms.
basm
ala
blog
(alw
ays o
rigin
al)

Thyroid-Associated OrbitopathyThyroid-Associated OrbitopathyThyroid-Associated OrbitopathyThyroid-Associated OrbitopathyThyroid-Associated Orbitopathy 115115115115115
Figure 6.6: Follow-up VISA classification form
basm
ala
blog
(alw
ays o
rigin
al)

116116116116116 Surgical Atlas of Orbital DiseasesSurgical Atlas of Orbital DiseasesSurgical Atlas of Orbital DiseasesSurgical Atlas of Orbital DiseasesSurgical Atlas of Orbital Diseases
Objective measures of optic neuropathy includea loss in central visual acuity and color vision, anafferent pupil defect, and infrequently congestion orpallor of the optic nerve.
Ancillary testing includes coronal CT or MR Scansto confirm crowding of the orbital apex,standardized visual fields, and rarely VEP or opticnerve head photos. As a summary grade, VISA listsoptic neuropathy as present or absent since mostclinicians would attempt some treatment for thiscondition if present. The severity of the neuropathyis reflected in the individual measurements of centraland color vision.
My usual treatment for TAO optic neuropathyinitially is high dose corticosteroids either byintravenous route (1 gram Methyl-prednisolone over30 minutes on alternate days for 3 treatments) ororal route (100 mg prednisone daily on a taperingdose) with an expectation that vision should improvewithin days of therapy. In most cases, this treatmentwill cause incomplete or only temporary visualimprovement so that surgical decompression of themedial wall is required (through a Lynch,transcaruncular or endoscopic transethmoidalapproach) in order to relieve pressure morepermanently on the optic nerve at the crowded orbitalapex (Figure 6.5A and B).
I often arrange adjunctive radiotherapysubsequent to the decompression if the disease isactive to prevent further enlargement of the musclesand recurrence of neuropathy. Radiotherapy isadministered using a lateral port focused behind theglobe to minimize the risk of retinal or lens exposure;it is divided into 10 fractions of 200 rads over twoweeks23 and is contraindicated in diabetics becauseof the risk of inciting or aggravating retinopathy.24
Although radiotherapy remains controversial, it isstill widely used and many clinicians believe it isbeneficial for certain aspects of TAO, including opticneuropathy and significant inflammation.25 Successof therapy for TAO optic neuropathy from both aclinical or research standpoint is based on specificimproved measurements for central vision, colorvision and visual fields.b) Inflammation/congestion: Symptoms of ocularand periocular soft tissue inflammation includeorbital aching at rest or with movement, and eyelidor conjunctival swelling and redness.
The Clinical Activity Score (CAS) described andvalidated by Mourits and the AmsterdamOrbitopathy group assigns one point for each of thefollowing: orbital pain at rest, orbital pain withmovement, chemosis, caruncular edema, eyelidedema, conjunctival injection and eyelid injection.21
The VISA Inflammatory Score modifies the CASslightly by widening the grade for chemosis and lidedema from 0-2. Chemosis is graded as 1 if theconjunctiva lies behind the grey line of the lid and as2 if it extends anterior to the grey line (Figures 6.3Aand 6.7A). Lid edema is graded as 1 if it is presentbut not causing overhanging of the tissues, and as 2if it causes a roll in the lid skin including festoons inthe lower lid (Figures 6.3A and 6.7A). The worstscores from any of the four eyelids are recorded inthe inflammatory score table on the far right sectionof the table. The pain score is based on the patient'sreport of deep orbit discomfort rather than ocularsurface irritation (0 = no pain, 1 = pain withmovement, 2 = pain at rest). The additional gradingscores for chemosis and lid edema allow fordocumentation of more subtle changes ininflammatory features between visits. An additionalpoint is assigned for diurnal variation of symptoms,to reflect the variability in congestion typically seenduring the active phase.
Treatment of active inflammation in TAOdepends on its inflammatory score and evidence ofprogression. If the score is less than 4 out of 10, andthere is no deterioration based on history orsequential clinical examination, conservativemanagement is offered with reassurance, coolcompresses, nocturnal head elevation, and non-steroidal anti-inflammatories. In general, if theinflammatory grade is 5 or more, or if there issubjective or objective evidence of progression in theinflammation, more aggressive therapy should beconsidered, including oral or intravenouscorticosteroids, radiotherapy, and in refractory cases,immunosuppressive agents (Figures 6.3A and B, 6.7Aand B). Combination therapy is receiving increasingattention in severe, progressive cases 26, 27 and interestis also turning to new immunomodulatory agents,such as anti-tumor necrosis factor agents (etanercept,infliximab) or B-lymphocyte directed therapy(rituximab).28 The hope from greater understandingof the immunogenic mechanisms in this disease is to
basm
ala
blog
(alw
ays o
rigin
al)

Thyroid-Associated OrbitopathyThyroid-Associated OrbitopathyThyroid-Associated OrbitopathyThyroid-Associated OrbitopathyThyroid-Associated Orbitopathy 117117117117117
Figure 6.7A: Patient with severe active orbitopathy: V = 1/1 (opticneuropathy present); I = 10/10 (2/2 pain, 2/2 chemosis with conjunctivaoverlying eyelid margins, 2/2 eyelid edema of left lower eyelid, 1/1caruncular edema, 1/1 redness of conjunctiva, 1/1 redness of eyelid,1/1 progression in symptoms over past month)
Figure 6.7B: Same patient 2 days following 3 doses of intravenousmethyl-prednisolone with marked reduction in inflammatory signs.VISA Score: V = 1/1 optic neuropathy (improved vision, but still showingimpaired central and color vision); I = 4/10 (0/2 pain, 1/2 chemosiswith conjunctiva behind grey line of lower lid, 1/2 eyelid edema, withresolution of eyelid overhang, 0/1 caruncular edema, 1/1 conjunctivalredness, 0/1 eyelid redness, 1/1 diurnal variation)
identify markers of progressive, more severe diseaseso that earlier treatment and more specificimmunotherapy may be developed.c) Strabismus / motility restriction: The symptomsfor strabismus include a progression from nodiplopia, diplopia with horizontal or vertical gaze,intermittent diplopia in straight gaze, and constantdiplopia in straight gaze.
Ocular ductions can be graded from 0° to 45° infour directions using the Hirschberg principle: thepatient is asked to look as far as possible up, down,right and left while the observer points a bright lightat the eyes and studies the light reflex on the surfaceof the eye. If the light reflex hits the edge of thepupil, the eye has moved 15°, between the pupil edgeand the limbus, 30° and at the limbus, 45° (Figure6.4).
Strabismus can be measured objectively by prismcover testing in different gaze directions.
Ancillary testing includes using the Goldmannperimeter to quantify ocular ductions in fourdirections.29, 30 The patient keeps both eyes open andfollows the V4e light target, tapping a coin when theimage becomes double.
Management of strabismus depends on whetherthe orbitopathy is inflamed (measured in the previoussection) or if there is evidence of progression insymptoms and signs. If inflammation is present, thisis managed first, either with conservative treatmentor with anti-inflammatories or radiotherapy (Figure6.8A). During this stage, the strabismus can bemanaged with patching one eye or with Fresnelprisms. Once the inflammatory score has droppedto zero and there is no evidence of progression,management of strabismus might include prisms orsurgical alignment (Figure 6.8B).d) Appearance/exposure: Symptoms in this categoryinclude appearance concerns such as bulging of theeyes, eyelid retraction and fat pockets, as well asexposure complaints of foreign body sensation, glare,dryness or secondary tearing.
Objective measures of appearance change includeeyelid retraction (measured in millimeters), proptosis(measured with the Hertel exophthalmometer), anddocumentation of redundant skin and fat prolapse.Measures of exposure include corneal staining orulceration.
Photographs can document the appearancechanges.
Management of appearance and exposure changesdepend on the inflammatory stage of the disease.During the inflammatory phase (documentedprogression in any of the parameters or aninflammatory score > 5), lubricant drops and
basm
ala
blog
(alw
ays o
rigin
al)

118118118118118 Surgical Atlas of Orbital DiseasesSurgical Atlas of Orbital DiseasesSurgical Atlas of Orbital DiseasesSurgical Atlas of Orbital DiseasesSurgical Atlas of Orbital Diseases
Figure 6.8A: Patient with active TAO and strabismus (VISA Score:I = 7/10, S = 3/3, strabismus in primary gaze). Anti-inflammatory treat-ment was instituted and one eye was patched for comfort
Figure 6.8B: Once the disease had progressed into thepostinflammatory (inactive) phase, alignment surgery was performed:(VISA Score: V = 0/1; I = 0/10; S = 0/3, A = 0/3)
ointments can relieve ocular irritation. Rarely atarsorrhaphy or emergency orbital decompressionmay be required for severe exposure or cornealulceration. Once the inflammatory phase has settled,management for proptosis might include orbitaldecompression and for eyelid retraction may includeupper lid lowering from an anterior or posteriorapproach or lower lid elevation.31 These surgicalmeasures often relieve many of the exposurecomplaints (Figures 6.2A and B, 6.3A and B).e) Application of the VISA classification: The VISAClassification clusters the four functions disruptedby TAO in a logical sequence for recording andmanagement. Subjective input and reproducibleobjective measurements are recorded for each sectionand a global severity grade can be assigned for eachfunction. The subjective and objective progress and
tempo of disease can be documented to reflect diseaseactivity. The classification system has been validatedby showing that two clinicians could use the formsto assess patients independently with differentmanifestations of TAO and to choose similarmanagement plans.22 It is currently being assessedby members of the International Thyroid Eye DiseaseStudy (ITEDS) Group and further refinements andvalidation will be conducted. A common method ofdocumenting and classifying the disease parametersis critical for conducting multicenter clinical trials andto assess response to different therapies.
General Management Guidelines
Patients with TAO are often misdiagnosed initially,because the majority present with mild, nonspecificcomplaints such as tearing, irritation and lightsensitivity as a result of exposure from mild lidretraction. Occasionally mild inflammatory featuressuch as eyelid or conjunctival swelling may beinterpreted as allergies or viral infections. Many ofthese patients are frustrated with their medical careby the time the correct diagnosis has been reached.More serious manifestations of the disease such asmyopathy, proptosis and visual impairment generallydevelop rapidly and are more readily recognized.
Understanding what bothers the patient mostabout their condition helps to build rapport and toplan future management. Patients appreciatereassurance and education about the natural courseof TAO. Clarify that their endocrinologist and familypractitioner will work to control any thyroiddysfunction, and that while their orbitopathy maybe linked to thyroid immune disorders, a euthyroidstate does not necessarily lead to resolution of theorbitopathy. Emphasize that they can take positivesteps to help their condition by quitting smoking andrelieving stressors in their lives.
I take the time to explain what is predictableabout the disease, mentioning that the disease is self-limited, and that those with a mild presentation andyounger age are unlikely to progress to more seriouscomplications. For those with more seriouscomplications, I use the house-fire analogy to clarifythe two stages of orbitopathy, and the role of anti-inflammatory or immunomodulatory therapy in theactive phase and surgical reconstruction if necessaryin the postinflammatory stage. The internet providesa number of support groups and I also identify
basm
ala
blog
(alw
ays o
rigin
al)

Thyroid-Associated OrbitopathyThyroid-Associated OrbitopathyThyroid-Associated OrbitopathyThyroid-Associated OrbitopathyThyroid-Associated Orbitopathy 119119119119119
patients who I have treated who are willing to talkto newly diagnosed patients to allow sharing of theirexperiences.
REFERENCES
1. Bahn RS, Heufelder AE. Pathogenesis of Graves'Ophthalmopathy. N Engl J Med 1993;329(20):1468-75.
2. Garrity JA, Bahn RS. Pathogenesis of Graves'Ophthalmopathy: Implications for Prediction, Preventionand Treatment. Am J Ophthalmol 2006;142(1):147-53.
3. Rootman J, Dolman PJ. Thyroid Orbitopathy (Chapter 8)in: Diseases of the Orbit. A Multidisciplinary Approach.Hagerstown: Lippincott Williams & Wilings, 2003.
4. Gerding MN, Terwee CB, Dekker FW et al. Quality of lifein patients with Graves' Ophthalmopathy is markedlydecreased: measurement by the medical outcomes studyinstrument. Thyroid 1997;7(6):885-89.
5. Bartley GB. The epidemiologic characteristics and clinicalcourse of ophthalmopathy associated with autoimmunethyroid disease in Olmsted County, Minnesota. Trans AmOphthalmol Soc 1994;92:477-588.
6. Kendall-Taylor P, Perros P. Clinical presentation of thyroidassociated orbitopathy. Thyroid 1998;8:427-28.
7. Burch HB, Wartofsky L. Graves' Ophthalmopathy: currentconcepts regarding pathogenesis and management. EndocrRev 1993;14:747-93.
8. Fatourechi V, Pajouhi M, Fransway AF: Dermopathy ofGraves disease (pretibial myxedema). Review of 150 cases.Medicine (Baltimore) 1994;73(1):1-7.
9. Perros P, Kendall-Taylor P. Natural history of thyroid eyedisease. Thyroid 1998;8:423-25.
10. Bartalena L, Marcocci C, Bogazzi F, et al. Relation betweentherapy for hyperthyroidism and the course of GravesOphthalmopathy. N Engl J Med 1998;338:73-78.
11. Dolman PJ, Rootman J. Predictors of disease severity inthyroid-related orbitopathy. (Chap18) Orbital Disease.Present status and future challenges. Taylor and Francis,2005.
12. Prummel MF, Wiersinga WM. Smoking and risk of Graves'disease. JAMA 1993;269:479-82.
13. Pfeilschifter J, Ziegler R. Smoking and endocrineophthalmopathy: impact of smoking and current vs lifetimecigarette consumption. Clin Endocrinol (Oxf) 1996;45:477-81.
14. Cruz AA, Akaishi PM, Vargas MA, et al. AssociationBetween Thyroid Autoimmune Dysfunction and Non-Thyroid Autoimmune Diseases. Ophthalmic Plastic &Reconstr Surg 2007;23(2):104-08.
15. Pritchard J, Horst N, Cruikshank W, et al. Igs from patientswith Graves' disease induce the expression of T cellchemoattractants in their fibroblasts. J Immunol 2002; 168:942-50.
16. Pritchard J, Han R, Horst N, et al. Immunoglobulinactivation of T cell chemoattractant expression in fibroblastsfrom patients with Graves' disease is mediated throughthe insulin-like growth factor 1 receptor pathway. JImmunol 2003;170:6348-54.
17. Rundle FF. Development and course of exophthalmos andophthalmoplegia in Graves' disease with special referenceto the effect of thyroidectomy. Clin Sci 1945;5:177-94.
18. Rundle FF. Ocular changes in Graves' disease. QJM 1960;29:113-26.
19. Selva D, Chen C, King G. Late reactivation of thyroidorbitopathy. Clin & Exp Ophthalmol 2004;32(1),46-50.
20. Werner, SC. Classification of the eye changes of Graves'disease. American J Ophthalmology 1969;68:646-48.
21. Mourits MP, Prummel MF, Wiersinga WM, et al. Clinicalactivity score as a guide in the management of patientswith Graves' Ophthalmopathy. Clin Endocrinol 1997;47:9-22.
22. Dolman PJ, Rootman J. VISA Classification for Graves'Orbitopathy. Ophthal Plast Reconstr Surg. 2006;22(5):319-24.
23. Beckendorf V, Maalouf T, George J-L, et al. Place ofradiotherapy in the treatment of Graves' orbitopathy. Int JRadiation Oncology Biol Phys 1999;43:805-15.
24. Viebahn M, Marricks ME, Osterloh MD. Synergismbetween diabetic and radiation retinopathy: a case reportand review. Br J Ophthalmol 1991;75:29-32.
25. Cockerham KP, Mourits MPh, McNab AA, et al. Doesradiotherapy have a role in the management of thyroidorbitopathy? Debate. Br J Ophthalmol 2002;86:102-04.
26. Kahaly G, Schrezenmeir J, Krause U, et al. Ciclosporin andprednisone vs prednisone in treatment of Graves'Ophthalmopathy: a controlled, randomized andprospective study. Eur J Clin Invest 1986;16(5):415-22.
27. Bartalena L, Marcocci C, Chiovato L, et al. Orbital cobaltirradiation combined with systemic corticosteroids forGraves' Ophthalmopathy: comparison with systemiccorticosteroids alone. J Clin Endocrinol Metab 1983;56(6):1139-44.
28. Leandro MJ, Edwards JC, Cambridge G. Clinical outcomein 22 patients with rheumatoid arthritis treated with Blymphocyte depletion. Ann Rheum Dis 2002;61:883-88.
29. Gerling J, Lieb B, Kommerell G. Duction ranges in normalprobands and patients with Graves' ophthalmopathy,determined using the Goldmann perimeter. IntOphthalmol. 1998;21(4):213-21.
30. Dolman PJ, Kendler D, Rootman J. Measuring ocularexcursions in Graves' Orbitopathy. (Abst) InternationalCongress of Ophthalmology 2004.
31. Looi, A, Sharma B, Dolman PJ. A Modified PosteriorApproach for Upper Eyelid Retraction. Ophthalmic PlastReconst Surg 2006;22(6).
basm
ala
blog
(alw
ays o
rigin
al)

120120120120120 Surgical Atlas of Orbital DiseasesSurgical Atlas of Orbital DiseasesSurgical Atlas of Orbital DiseasesSurgical Atlas of Orbital DiseasesSurgical Atlas of Orbital Diseases
Shome Debraj, Walinjkar Jaydeep, Mukherjee Angshuman
Orbital InfectionsOrbital InfectionsOrbital InfectionsOrbital InfectionsOrbital Infections
Many disease processes such as cancers, infections,or inflammations present with overlapping clinicalmanifestations, because of the confined nature of theorbital space. Also, with the multitude of muscular,neurovascular, sensory, and glandular structureslocated close to each other in this space, preciseanatomic localization of various biologic processescan be difficult.
Orbital infections and inflammations present tothe clinician with similar findings: periorbital edema,erythema, proptosis, and pain. History and clinicalexamination determine the work-up required tobetter define the disease process. Orbital infectionscontinue to be associated primarily with diseases ofthe paranasal sinuses.1 Hemophilus influenza type Bis no longer a significant pathogen, because of aneffective vaccine.2 Fungal infections extending to theorbit are becoming more frequent, due to theincreased prevalence of immunocompromisedpatients.3
Infections of the orbit are uncommon, but theyare potentially devastating infections that can quicklyresult in blindness, meningitis, or death. Theemergency physician must make a rapid and accuratediagnosis and then quickly initiate therapy becausevisual loss is associated directly with the length oftime to definitive treatment.
Smith and Spencer4 classified orbital infectionsinto 5 tiers which were later modified by Chandleret al.5
• Group I — Preseptal cellulitis• Group II — Orbital cellulitis• Group III — Subperiosteal abscess
• Group IV — Orbital abscess• Group V — Cavernous sinus thrombosis.
This classification system does not necessarilyimply an order of disease progression; however, ithelps explain the physical signs and symptoms of thevarious infections and helps organize treatment plans.6
Orbital infections may be divided into preseptalcellulitis, in which infection is located anterior to theorbital septum (a thin sheet of fibrous tissue arisingfrom the periosteum of the orbital margin andinserting into the tarsal plates), and orbital cellulitis,in which there is infection of orbital tissues posteriorto the orbital septum.7 Preseptal cellulitis generallyresponds to oral antibiotics and rarely has importantsequelae. However, orbital cellulitis is a seriousinfection which may be complicated by abscessformation (subperiosteal, orbital, or brain),meningitis, septicemia, cavernous sinus thrombosis,and death. Although orbital cellulitis is related toethmoid sinusitis in 70-80% of cases8, it may alsodevelop after orbital or sinus trauma.9, 10 Prompt andappropriate management of patients with orbitalcellulitis or at risk of developing this minimises therisk of complications.10 The possible causes ofMortality/Morbidity following orbital cellulitis are:
• Cavernous sinus thrombosis• Brain abscess or meningitis• Permanent vision loss.
Demographic Profile
Sex• Males are affected slightly more often than
females.
7C H A P T E R
basm
ala
blog
(alw
ays o
rigin
al)

Orbital InfectionsOrbital InfectionsOrbital InfectionsOrbital InfectionsOrbital Infections 121121121121121
Age
• Orbital infections are more common in personsyounger than 19 years
• Orbital infections are more severe in adults.
Risk Factors
Past medical history significant for HIV, diabetes,immunosuppression, steroid use, renal disease, andtravel is important.
Chronologic relation with an insect sting, allergicreaction, or trauma may suggest etiologies that mimican orbital infection.
Etiological Causes of Orbital Infections
Bacterial infectionsBacteria, most commonly Streptococcus species, aswell as Staphylococcus aureus, Hemophilusinfluenzae, and anaerobes, cause the vast majorityof orbital infections.11
The incidence of Hemophilus influenzae type Bhas decreased since the early 1990s.2 In communitieswhere CAMRSA is prevalent, ophthalmologistsshould maintain high index of suspicion and obtainmicrobial cultures and sensitivity studies to helpguide antibiotic therapy for severe ophthalmicinfections.12
Fungal infectionsFungal infections are less common than bacterialinfections and occur more commonly in patients whoare immunocompromised (e.g., those with HIV ordiabetes). (Rhizopus, Mucor, Aspergillus)13
Phycomycosis, also known as mucormycosis, isthe most common and most virulent fungal diseaseinvolving the orbit. The specific fungal genus involvedis usually Mucor or Rhizopus. These fungi can involvethe blood vessel wall and produce thrombosingvasculitis.Therapeutic measures include controllingthe underlying metabolic abnormality, local surgicalexcision of infected tissues, and administration ofamphotericin B.14, 3
Parasitic infectionsParasitic diseases may be prevalent in endemic areas(e.g. Mediterranean, Eastern Africa, Australia,Middle East Asia, South America, Eastern Europe)and in travelers to these areas, such infections are
not uncommon. The causative organisms include Egranulosus, T solium,Trichinella spiralis and theOnchocerca.15
Protozol infectionsAlthough relatively uncommon, protozoal infections(most commonly with toxoplasma gondii) are seenin immunocompromised individuals.16
They have an increased likelihood for moresevere and atypical presentations; this highlights theneed for increased index of suspicion for HIVinfection as ocular or orbital disease may be the firstmanifestation of life-threatening systemictoxoplasmosis.
Diagnosis
The diagnosis of orbital infections includes thefollowing:
• A detailed history• Vision• Slit-lamp examination• Extraocular motility• Examination to document optic nerve function;
including pupillary function• Fundus examination• Resistance to retropulsion• Exophthalmometry: Hertel's exophthalmometry
is the gold standard.
Imaging Studies17
• Computed Tomography (CT) scan — A CT scanof the orbit, sinuses, and frontal lobe is essentialfor every patient showing signs of orbitalinvolvement. 2 mm cuts are ideal for the orbit.Both Axial and coronal scans shoud be carefullylooked at, to obtain a 3-dimensional perspective.
• Magnetic Resonance Imaging (MRI) — While aCT scan provides enough information in mostcases, a MRI scan may improve visualization ofcavernous sinus thrombosis.
• Ultrasonography (USG) B-scan — An USG B-scan is mostly supportive in role, due todifficulty in interpretation of posterior orbitallesions.
• X-rays — Waters, Caldwell, submental vertex,and lateral view are mainly of historical interest.
basm
ala
blog
(alw
ays o
rigin
al)

122122122122122 Surgical Atlas of Orbital DiseasesSurgical Atlas of Orbital DiseasesSurgical Atlas of Orbital DiseasesSurgical Atlas of Orbital DiseasesSurgical Atlas of Orbital Diseases
Other Tests
• Fiberoptic nasopharyngeal endoscopy:18 If anysuspicion of mucormycosis (i.e. elevated bloodglucose, leukemia, renal disease) exists,fiberoptic nasopharyngeal endoscopy should beperformed (usually, by an otolaryngologist) toseek evidence of black eschar formation.Endoscopy assisted transnasal drainage is alsouseful in cases with evidence of associated sinusinfections.
• Rapid plasma reagin (RPR), particularly in casesof insidious onset or with a history of syphilis.
• Cerebrospinal fluid (CSF) analysis for gram stain,cell count, cultures, and antigens may beconsidered in patients with associated centralnervous system signs.
Emergency Department Care
• Adults with preseptal cellulitis and no signs oforbital involvement can be discharged on oralantibiotics with close follow-up care.19
— Adults with orbital signs need admissionand IV antibiotics or antifungals are quicklyinitiated, under close supervision.
— Surgical intervention should be performedimmediately, in cases with CT evidence ofsubperiosteal or orbital abscess — fordrainage.19
— Surgical drainage is not always necessaryfor cellulitis; however, any patient withcompromised vision (20/60 or worse)should receive immediate surgery fordrainage and debridement.19
— Surgical drainage of abscesses (orbital orsubperiosteal) is considered, even withoutvisual loss. Drainage of sinuses should beconsidered in patients with associatedsinusitis.
— Some patients can be monitored for 48hours on IV antibiotics, with surgeryperformed for increasing proptosis,worsening visual acuity, or isolated muscleweakness. Surgery is performed after 48hours if fever continues or antibiotics fail.20
— Orbital drainage decreases intraorbitalpressure, decreases associated pressure onthe nerve and retinal circulation, creates a
potential path for further drainage (thewound is closed with spaced sutures) andprovides material for appropriately guidedantibiotic therapy. We recommend orbitaldrainage by a trained orbital specialist astissue in these cases are extremely vascular,friable and susceptible to damage.
— All children are admitted prior to initiatingtherapy21 even if they lack orbital signs-because children are deficient in IgG2 andare predisposed to bacteremia.
For orbital cellulitis, oxacillin or nafcillin can be usedwith the addition of ampicillin and sulbactam inchildren to cover H influenzae.21 Patients who areallergic to penicillin can use vancomycin, clindamycin,or chloramphenicol. More and more organisms incountries like India are becoming resistant toconventional antibiotics. Methicillicin resistantStaphylococcus Aureus (MRSA) strains are not onlyprevalent in the nosocomial environment but are alsofound in the community. MRSA orbital cellulitis canquickly progress to irreversible blindness, despiteantibiotic treatment.
— Alternatively, a cephalosporin (e.g. cefuroxime,cefoxitin, cefotetan) can be used alone.
— Nasal decongestants can be used to help drainthe sinuses.
— Concomitant steroid therapy, once clinicalimprovement is documented on antibiotics, isstarted to decrease inflammation associatedcollateral damage to tissue and edema, therebyfurther decreasing intraorbital pressure.
Further Inpatient Care
Underlying disorders, if present (e.g. hyper-glycemia, acidosis, infection, immunosuppression) arecorrected.
Consultations: Consultation with an ENTsurgeon or a neurosurgeon must be considered incases without improvement, or in cases withinvolvement of sinuses or the nervous system.
Necrotizing fascitis, Orbital Tuberculosis andCommunity Acquired MRSA (CAMRSA) inducedorbital cellulitis are rare entities in the spectrum oforbital infections. Although these infections are notso common, ophthalmologists should be well awareof these conditions, especially in endemic areas as
basm
ala
blog
(alw
ays o
rigin
al)

Orbital InfectionsOrbital InfectionsOrbital InfectionsOrbital InfectionsOrbital Infections 123123123123123
Figure 7.1A: Periocular necrotising fasciitis: External photograph ofpatient at presentation, showing left sided severe lid edema, erythemaand necrotic tissue with overlying skin scabs
Figure 7.1B: Periocular necrotising fasciitis: Slit lamp photograph ofthe left eye, in diffuse illumination (with upper eyelid retracted),showing periocular skin erythema and kerato-conjunctivitis
the morbidity and mortality of selected cases arereduced with prompt and appropriate antimicrobialtherapy. Keeping in mind this fact we find itappropriate to present the following case reports:
CASE ILLUSTRATIONS
Case 1
A 25-year-old systemically healthy male patientpresented with complaints of severe photophobia,redness, discharge, pain and severe swelling of thelids in the left eye, since 2 days. Past history wassignificant for a boil on the lower eyelid, 2 days ago.On examination, the best-corrected visual acuity was6/6 and 6/9, in the right and left eyes respectively.Right eye examination was unremarkable. The lefteye showed severe lid edema with scales on the skinand was diagnosed as having left sided periocularnecrotising fascitis with associated kerato-conjunctivitis (Figure 7.1A). The cornea showedmultiple marginal infiltrates. Photographicdocumentation of the anterior segment condition wasimpossible because of the severe photophobia.Extraocular movements were full. A conjunctivalswab and a periorbital skin swab were sent forculture and sensitivity. The corneal infiltrates werealso cultured on Blood agar and Sabouraud'sdextrose agar. The patient was seen by our infectiousdiseases expert and started on intravenous co-amoxiclav 1 gram twice daily, intravenous ceftriaxone1 gram twice daily and oral metronidazole 500 mgthree times daily, pending sensitivity reports. TopicalLotepred eye drops every 3 hourly and ciprofloxacin(0.3%) eye drops 6 times a day were started, in theleft eye.
On follow-up 2 days later, the patient wassymptomatically much better. The skin scabs hadfallen off, revealing violaceous, sub-epidermalnecrosis. The conjunctival inflammation had reducedand the corneal marginal infiltrates had almostdisappeared (Figure 7.1B). Culture and sensitivityresults showed Staphylococcus aureus, sensitive to theadministered medications. The culture plates forcorneal infiltrates showed negative growth and werediscarded after 3 weeks. The patient was sero-negative for HIV.
Five days later, the skin lesions had healed andthe conjunctivitis had resolved. Intravenous
antibiotics were stopped and the patient was startedon oral antibiotics for a week.
On final follow-up a month later, periocularskin discoloration was the only sequalae noted(Figure 7.2).
DiscussionNecrotising fascitis (NF) is a serious life threateningcondition, with reported mortality of more than 20%.The limbs, perineum and abdomen are frequentlyinvolved with facial involvement being rarelyinvolved. The organisms most closely linked to NFare Group A beta-hemolytic streptococci, thoughthese bacteria are isolated in only a minority of thecases.20
basm
ala
blog
(alw
ays o
rigin
al)

124124124124124 Surgical Atlas of Orbital DiseasesSurgical Atlas of Orbital DiseasesSurgical Atlas of Orbital DiseasesSurgical Atlas of Orbital DiseasesSurgical Atlas of Orbital Diseases
Figures 7.3A and B: Orbital tuberculosis manifesting with enophthalmos: External photograph of the face showing mild enophthalmos of theleft eye (left) and a coronal computed tomography scan showing an ill-defined anterior orbital mass located inferotemporally in the left orbit,with minimal contrast enhancement (right)
Periocular NF is reported to have a betterprognosis.22 Though reports of resolution of peri-ocular NF postsurgical debridement are common, adetailed Medline and Embase search revealed onlyone case report which was reported to resolve withconservative management.23 Infections in the peri-ocular region occur postsurgical procedures, posttrauma, postfurunculosis or even without anyantecedent cause.23
Ideally, a combination of intensive parenteralantimicrobial therapy and prompt surgicaldebridement of necrotic tissue should be performed.Intravenous pooled immunoglobulin and heparini-sation may also have beneficial roles by neutralisingsuper-antigen activity and aiding antibioticperfusion.24 Mild cases especially those restrictedto the eyelids alone may respond to medicaltherapy.23
We report the case of a 25-year-old male patientwho presented with periocular NF associated withkeratoconjunctivitis. We report this case to highlightthe successful conservative management of peri-
ocular NF and the hitherto unreported anteriorsegment involvement.
Case 2
A 60-year-old systemically healthy female wasreferred with a 2-month history of irritation in theleft eye associated with a mass in the lower lateralorbit. Her visual acuity was 20/20 in both eyes. Theright eye was unremarkable. The left eye was 2 mmenophthalmic by Hertels exophthalmometry butshowed no displacement (Figure 7.3A). Ocularmotility was full in range. There was a nontender,hard, lobulated mass measuring about 30 mm × 10mm in size in the inferior orbit, felt separate fromthe inferior orbital rim. The mass appeared to becontiguous with the globe. General physicalexamination including chest roentgenogram wasunremarkable.
Computed tomography scan showed an ill-defined extraconal anterior orbital mass locatedinferotemporal in the left orbit, with minimal contrastenhancement (Figure 7.3B). Differential diagnoses ofscirrhous breast cancer metastasis or sclerosingorbital pseudotumor were considered and a biopsywas performed by the inferior conjunctival fornicialapproach.
Histopathology revealed features of non-caseating granulomatous inflammation and fibrosis(Figure 7.4A). AFB was negative both by smear andculture. PCR for Mycobacterium tuberculosis DNAwas positive (Figure 7.4B). Orbital tuberculosis wasdiagnosed and the patient received four-drugcombination antitubercular therapy for 6 months. Theorbital mass completely regressed and there was nolocal recurrence at two years.
Figure 7.2: Periocular necrotising fasciitis: External photograph ofpatient, a month post presentation, showing healed skin lesions, withsymmetrical palpebral apertures
A B
basm
ala
blog
(alw
ays o
rigin
al)

Orbital InfectionsOrbital InfectionsOrbital InfectionsOrbital InfectionsOrbital Infections 125125125125125
Figures 7.4A and B: Orbital tuberculosis manifesting withenophthalmos: Histopathology of the orbital mass showing featuresof non-caseating granulomatous inflammation and fibrosis(hematoxylin and eosin, x 500) (left) and polymerase chain reactionof the specimen positive for mycobacterium tuberculosisdeoxyribonucleic acid (right)
Figure 7.5A: CAMRSA orbital cellulitis: External photograph of patient,showing severe right sided proptosis, with conjunctival chemosisand draining wound of the right upper eyelid
Discussion
Orbital tuberculosis is rare, even in endemiccountries.25 Erosion of a parenchymal pulmonarytuberculous focus in a blood or a lymph vessel maylead to dissemination of the organism; with systemicinvolvement.26 Orbital tuberculosis may involveorbital soft tissues, lacrimal gland, periosteum, andbones, and may extend to a contiguous paranasalsinus or intracranial cavity.25, 27 The disease course isgenerally slow and indolent.25,27 Clinical mani-festations include orbital tuberculoma and coldabscess presenting with proptosis, and orbitalosteomyelitis manifesting with discharging sinus andinflammation.25, 27 Orbital tuberculosis presents withproptosis and is not known to present withenophthalmos.28
Common manifestations of orbital tuberculosisare proptosis or discharging sinus. Our patient,however, presented with an orbital mass andenophthalmos. Orbital tuberculosis presents withproptosis and is not known to present withenophthalmos.25,27 Herein we report a case of orbitaltuberculosis presenting with an orbital mass andparadoxical enophthalmos.
Case 3
A 55-year-old systemically normal female patientpresented to us with right-sided sudden onset severeproptosis, pain and dimunition of vision, of 2 daysduration. Past history was significant for a boil onthe right upper eyelid, 2 days prior. The patient wason oral amoxicillin 750 mg three times daily, atpresentation.
On examination, the visual acuity was perceptionof light with inaccurate projection and 6/9 in the rightand left eyes respectively. The right eye was severelyproptotic, with greatly increased resistance toretropulsion. There was an upper lid wound, withpurulent drainage. The bulbar conjunctiva wasseverely chemosed, making the remaining slitlampexamination difficult (Figure 7.5A). Extraocularmovements were severely limited in all directionsof gaze. Left eye examination was unremarkable.
The patient was mildly febrile. Remainingsystemic examination was unremarkable. An orbitalComputed Tomography (CT) scan, routine bloodinvestigations and culture and urine examinationand culture were ordered. The blood and urineexamination reports were unremarkable, except formild leucocytosis. The CT scan showed a superiororbital mass suggestive of an abscess. The paranasalsinuses were clear of any obvious infection. Tentingof the ocular contents was seen on axial CT,suggestive of increased orbital pressure.
A superior orbitotomy for drainage of the abscesswas performed, under general anesthesia.2 millilitres of pus was drained and sent for cultureand antibiotic sensitivity testing and Pulsed field GelElectrophoresis (PFGE), which revealed CAMRSA,resistant to all antibiotics, except vancomycin,cotrimoxazole (trimethoprin/sulfamethoxazolecombination) and amikacin. The patient wasadmitted and started on intravenous vancomycin1 gram every 6 hours and intravenous amikacin1 gram daily, after consultation with our internist.The patient started improving three days posttherapy. Intravenous dexamethasone 4 mg every 8hours was started to decrease associatedinflammation. This was subsequently increased to
A B
basm
ala
blog
(alw
ays o
rigin
al)

126126126126126 Surgical Atlas of Orbital DiseasesSurgical Atlas of Orbital DiseasesSurgical Atlas of Orbital DiseasesSurgical Atlas of Orbital DiseasesSurgical Atlas of Orbital Diseases
Figure 7.5B: CAMRSA orbital cellulitis: External photograph, 3 monthspostorbitotomy, showing complete resolution of the condition andcomplete healing of the lid wound
8 mg every 8 hours, 2 days later. Serum creatinineand urea were monitored every 72 hours. Seven daysposttherapy, the vision had improved to 6/24 andthe ocular movements had normalized almostcompletely. However, lagophthalmos due to theearlier lid wound persisted. The patient wasdischarged on oral cotrimoxazole 960 mg every 12hours and oral steroids 60 mg every day. Theantibiotic was stopped a week later and steroidsgradually tapered.
At 3 months follow-up, the vision in the righteye was 6/9. The lid wound had completely healed(Figure 7.5B).
Discussion
Methicillin-resistant Staphylococcus aureus (MRSA)has been recognized as a cause of nosocomialinfections since the 1960s. Recently, MRSA infectionshave been reported among patients with no historyof hospitalization. These infections have affectedprison inmates, athletic teams, military recruits,children attending day care, and patients within noidentifiable risk group.29,30 Community acquiredMRSA (CAMRSA) is no longer a pathogen unique tocertain high-risk populations such as prison inmates.Most patients presenting in an outpatient setting withan MRSA soft-tissue infection are not linked to anydistinct high-risk group.30 These CAMRSA strainshave different genetic background and antibioticsusceptibility profiles than hospital strains. Despitetheir broader antibiotic susceptibility, in comparisonto hospital-acquired strains, CAMRSA strains cancause severe infections, such as necrotizingpneumonias, large soft-tissue abscesses, andnecrotizing fasciitis, in otherwise healthy patients.
CAMRSA causing orbital cellulitis is rare, butwith an increasing incidence.31
CAMRSA is geographically widespread, as it hasbeen reported in many regions of the US as well asEurope, Japan, and Australia.30, 31 Within the orbit;this infection is extremely virulent and being resistantto most antibiotics, causes severe damage.
We report a rapidly evolving orbital cellulitiscaused by CAMRSA. A rapidly evolving orbitalcellulitis with an abscess in an adult from any causeshould undergo prompt surgical drainage andtreatment with susceptible antibiotics. So in thisrespect a MRSA orbital cellulitis is no different. Thereal teaching point in this case is to include MRSA asa significant possible cause of the cellulitis and tostart empiric therapy that includes coverage forMRSA, until antibiotic susceptibilities come back. Itis further recommended to maintain suspicion forMRSA in community patients with possiblestaphylococcal infection, failing β-lactam classantibiotic therapy, to obtain culture and sensitivitystudies in cases of severe ophthalmic infections, andto be informed about the rates of MRSA in the localcommunity.
REFERENCES
1. Henning Bier, and Uwe Ganzer. Involvement of the orbitin diseases of the paranasal sinuses. Neurosurgical Review1990;13: 109-12.
2. Ambati BK, Ambati J, Azar N. Periorbital and orbital cellulitisbefore and after the advent of Haemophilus influenzaetype B vaccination. Ophthalmology 2000; 107: 1450-53.
3. Kronish JW, Jhonson TE, Gilberg SM, et al. Orbital infectionsin patients with human immunodeficiency virus infection.Ophthalmology 1996;103:1483-92.
4. Smith AF, Spencer JF. Orbital complications resulting fromlesions of the sinuses. Ann Otol Rhinol Laryngol 1948; 57:5-27.
5. Chandler JR, Langenbrunner DJ, Stevens ER: Thepathogenesis of orbital complications in acute sinusitis.Laryngoscope 1970; 80: 1414-28.
6. Uzcategui N, Warman R, Smith A, Howard CW. Clinicalpractice guidelines for the management of orbital cellulitis.J Pediatr Ophthalmol Strabismus 1998;35:73-79.
7. Givner, Laurence B. Periorbital versus orbital cellulitis.Concise Reviews Of Pediatric Infectious Diseases. PediatricInfectious Disease Journal 2002.21:1157-58.
8. Shovlin JP. Orbital infections and inflammations. Curr OpinOphthalmol. 1998; 9: 41-48.
basm
ala
blog
(alw
ays o
rigin
al)

Orbital InfectionsOrbital InfectionsOrbital InfectionsOrbital InfectionsOrbital Infections 127127127127127
9. Mannor G. Unusual orbital infections: Oculoplastic andorbital surgery. Current Opinion in Ophthalmology2000;11: 357-60.
10. Shuttleworth GN. (Clinical review)Orbital trauma.do notblow your nose. BMJ 1999;318:1054-55.
11. Wald ER. Periorbital and Orbital Infections. Pediatrics inReview 2004; 25: 312-20.
12. Jeyaratnam D, Reid C, Kearns A, Klein J. Communityassociated MRSA: an alert to paediatricians. Arch Dis Child2006; 91: 511-12.
13. Hendrickson RG, Olshaker J, Duckett O. Rhinocerebralmucormycosis: a case of a rare, but deadly disease. J EmergMed 1999;17:641-45.
14. Ferry AP, Abedi S. Diagnosis and management ofrhinoorbitalcerebral mucormycosis. A report of 16personally observed cases. Ophthalmology 1983;90:1096-104.
15. Mortada A. Orbital pseudo-tumors and parasitic infections.Bull Ophthalmol Soc Egypt 1968; 6: 393-9.
16. Mun-Wai L, Kee-Siew F, Li-Yang H, Wee-Kiak L. Opticnerve toxoplasmosis and orbital inflammation as initialpresentation of AIDS. Graefe's Archive for Clinical andExperimental Ophthalmology 2006;244:1542-44.
17. Luis Gorospe, Aránzazu Royo, Teresa Berrocal, Garcia-Raya P, Moreno P, Abelairas J. Imaging of orbital disordersin pediatric patients. European Radiology 2003;13:2012- 26.
18. Wendy L. Wright MS. Viral or Acute BacterialRhinosinusitis? Determining the Difference. The NursePractitioner: The American Journal of Primary Health Care2005;30:30-41.
19. D B Jones and P G Steinkuller. Strategies for the initialmanagement of acute preseptal and orbital cellulitis. TransAm Ophthalmol Soc. 1988;86:94-112.
20. Urschel JD. Necrotizing soft tissue infections. Postgrad MedJ 1999;75:645-49.
21. Donahue SP, Schwartz G. Preseptal and orbital cellulitis inchildhood. A changing microbiologic spectrum.Ophthalmology 1998; 105:1905-06.
22. Kronish JW, McLeish WM. Eyelid necrosis and periorbitalnecrotizing fasciitis. Report of a case and review of theliterature. Ophthalmology 1991; 98; 92-8.
23. Luksich JA, Holds JB, Hartstein ME. Conservativemanagement of necrotizing fasciitis of the eyelids.Ophthalmology 2002; 109; 2118-22.
24. Seal DV. Necrotizing fasciitis. Curr Opin Infect Dis 2001; 14:127-132.
25. Aggarwal D, Suri A, Mahapatra AK. Orbital tuberculosiswith abscess. J Neuro-Ophthalmol 2002; 22: 208-10.
26. Biswas J, Shome D. Choroidal tubercles in disseminatedtuberculosis diagnosed by the polymerase chain reactionof aqueous humor: a case report and review of the literature.Ocul Immunol Inflamm 2002;10: 293-98.
27. Sen DK. Tuberculosis of the orbit and lacrimal gland: aclinical study of 14 cases. J Pediatr Ophthalmol Strabismus1980;17:232-38.
28. Shome D, Honavar SG, Vemuganti GK, Joseph J. Orbitaltuberculosis manifesting with enophthalmos and causinga diagnostic dilemma. Ophthal Plast Reconstr Surg 2006;22: 219-21.
29. Weber JT. Community-associated methicillin-resistantStaphylococcus aureus. Clin Infect Dis 2005; 41: S269 - 72.
30. Rutar T, Chambers HF, Crawford JB, Perdreau-RemingtonF, Zwick OM, Karr M, Diehn JJ, Cockerham KP. Ophthalmicmanifestations of infections caused by the USA 300 cloneof community-associated methicillin-resistant Staphy-lococcus aureus. Ophthalmology 2006;113:1455-62.
31. Rutar T, Zwick OM, Cockerham KP, Horton JC. Bilateralblindness from orbital cellulitis caused by community-acquired methicillin-resistant Staphylococcus aureus. Am JOphthalmol 2005;140:740-2.
basm
ala
blog
(alw
ays o
rigin
al)
128128128128128 Surgical Atlas of Orbital DiseasesSurgical Atlas of Orbital DiseasesSurgical Atlas of Orbital DiseasesSurgical Atlas of Orbital DiseasesSurgical Atlas of Orbital Diseases
E Ravindra Mohan, Moupia Goswami, Vinathi Mutyala
Orbital Inflammatory DiseaseOrbital Inflammatory DiseaseOrbital Inflammatory DiseaseOrbital Inflammatory DiseaseOrbital Inflammatory Disease
The orbits represent a microcosm of the body interms of tissues present-muscle, adipose tissue, bloodvessels, nerves, skin and bone as also the eyeballwith its unique architecture, histology and spectrumof diseases affecting it. Inflammatory conditions ofthe orbit represent the commonest afflictions of theorbits and thyroid associated orbitopathy andinfections constitute the bulk of these.
Excluding the above causes of orbitalinflammation, the causative entities range fromvasculitis, like Wegener’s granulomatosis togranulomatous conditions like sarcoidosis and theentity of idiopathic orbital inflammation, earlierpopularly labelled as pseudotumor. As evident fromthe diversitry of underlying causes, the clinicalpicture, natural history, treatment and outcome ofthese conditions vary greatly.
The age profile of patients with orbitalinflammation also varies greatly, ranging from thepaediatric age group for juvenile xanthogranulomato adulthood, mostly the 3rd-5th decades of life forthe vast majority of inflammatory conditions. Orbitalinflammatory disorders are less common in theelderly, and must be diagnosed only after ruling outmetastatic disease and infections, by tissue diagnosisif needed.
Orbital inflammation affects both sexes and allraces across continents.
Broadly speaking, all patients with orbitalinflammation present with one or more of theinflammatory symptoms of pain, swelling around theeye, proptosis, double vision or reduced vision,redness or watering. Pain is a common symptom and
is variably described as dull, aching or throbbingand is poorly localized, with headache being acommon complaint. Periocular swelling andpuffiness, more pronounced in the mornings afterrising from sleep is not uncommon. While doublevision is reported by some of these patients, it is aprimary complaint only in a small proportion of thepatients and at times elicited only on examination.
Orbital disease, particularly resulting frominflammatory conditions is one of the few remainingareas in the practice of ophthalmology, wheredetailed and meticulous history taking still has animportant role and bearing on arriving at a diagnosis.Details of symptoms, associated systemic features,response to medications and side effects of treatmentare important areas which need to be probedcarefully. For example, merely knowing that apatient’s orbital symptoms improved on oral steroidsmay be inadequate to arrive at a diagnosis ofidiopathic orbital inflammation. If the details aresought, and suggest rapid relief starting withinhours, and near total resolution, one would be moredefinite in making the diagnosis.
Examination of a patient with orbitalinflammatory disease needs to be done withmeticulous attention to detail. Careful documentationincluding photographic documentation is invaluablein studying the natural history of an individualpatient’s condition as also in prognostication and intitrating medical therapy.
Close co-ordination with other specialiststreating a patient is clearly essential in themanagement of patients with orbital inflammatory
8C H A P T E R
basm
ala
blog
(alw
ays o
rigin
al)

Orbital Inflammatory DiseaseOrbital Inflammatory DiseaseOrbital Inflammatory DiseaseOrbital Inflammatory DiseaseOrbital Inflammatory Disease 129129129129129
conditions. In addition to primary care givers, likerheumatologists in managing a patient with avasculitic condition, other specialists often need tobe involved in care as the disease progresses orcomplications develop as a result of medical therapy,as in the need for orthopaedic care for asepticnecrosis of neck of femur developing from prolongedsystemic steroid therapy.
Overall, the disease entities covered in thischapter are diverse and may have little in commonexcept the propensity to produce orbitalinflammation. Achieving a precise diagnosis, byobtaining orbital tissue for diagnosis if needed, isvital. With present day techniques andinstrumentation, obtaining an adequate specimen forhistopathological and immunohistochemicaldiagnosis is safe. Except for cases where the diseaseis localized to a relatively inaccessible region of theorbit like the orbital apex, or resolves fully on medicaltherapy based on presumptive diagnosis, an incisionalbiopsy is essential to achieve diagnosis and rule outother causes for orbital inflammation likemasquerade syndrome related to malignant tumor.A fine needle aspiration biopsy is often inadequatefor the purpose.
The treatment of orbital inflammations remainscentred on the control of inflammation andprevention of the sequelae of persistent andprolonged inflammatory reaction. A host ofimmunosuppressive drugs like cyclosporine,methotrexate and cyclophosphamide are used inaddition to intravenous methylprednisolone and thewidely used oral steroid medications.
Surgery in patients with orbital inflammatorydisease is primarily to obtain tissue diagnosis.Surgical debulking of the involved orbital tissue israrely needed, and the use of destructive operationslike orbital exenteration is only in extremelydisfigured orbits with no visual potential andseverely troubling symptoms. Radiation therapy haslimited role.
Treatment of orbital inflammatory disease needsto be tailored and titrated to the individual diseaseentity and patient. Since inflammation often tendsto relapse and recur, long term follow-up is neededas also monitoring to assess for complications oforbital disease like ocular motility restriction orcomplications of therapy, like steroid induced cataract.
The prognosis for patients with orbitalinflammatory disease is variable and depends on theunderlying disease and its severity.
ORBITAL AMYLOIDOSIS
Amyloidosis refers to a heterogenous group ofdisorders of protein metabolism characterized by theextracellular deposition of abnormal insoluble proteinfibrils. Deposition of amyloid in the eye and itsadnexal structures may occur as part of systemicamyloidosis or as a localised form. Local orbitalamyloidosis is a rare condition, comprising only 4%of cases of local amyloidosis seen in the head andneck regions.1
Ocular findings in primary generalisedamyloidosis include purpura of the eyelids, whichcan frequently be the presenting sign; bilateral,symmetrical, small amyloid papules of the skin ofthe eyelids, nodules in the lids, ptosis; proptosis,globe displacement with or without visualimpairment, ophthalmoplegias or amyloidneuropathy affecting pupillary function or both andsubconjunctival hemorrhages.
Histologically the specimen shows fibrousconnective tissue and massive amyloid depositinfiltrated with lymphocytes, plasma cells, andforeign body giant cells. Amyloid deposits areidentified histologically by congo red staining(Figure 8.1) and viewing under polarized light whereamyloid deposits produce a distinctive ‘apple greenbirefringence’. The pathogenic mechanisms leadingto local tissue deposition of amyloid are not clear.The universal constituent of amyloid is the amyloidP component (AP). It is derived from normal
Figure 8.1: Congo red staining showing amyloid (Congo red x 200)
basm
ala
blog
(alw
ays o
rigin
al)

130130130130130 Surgical Atlas of Orbital DiseasesSurgical Atlas of Orbital DiseasesSurgical Atlas of Orbital DiseasesSurgical Atlas of Orbital DiseasesSurgical Atlas of Orbital Diseases
circulating plasma protein, serum amyloid Pcomponent (SAP). The isolated pure human SAPradiolabelled with I 123 is a highly specific tracer forall types of amyloidosis.2
The best method of orbital imaging is CT scan,for its ability to detect calcification whichdifferentiates it from other lesions. Radionuclide SAPscans help in anatomical localisation of amyloiddeposits.
Management of orbital amyloidosis is difficult.Standard treatment aims to reduce reproduction ofthe monoclonal immunoglobulin precursor viachemotherapy or radiotherapy or surgery of thelocalized lesion. Total excision is usually difficult andsurgery is aimed at debulking the mass withpreservation of palpebral gland of the lacrimal gland,levator and rectii muscles.
REFERENCES
1. Gean-Marton AD, Kirsh CFE, Vezina LG, et al. Focalamyloidosis of the head and neck: evaluation with CT andMR imaging. Radiology 1991;181:521-5.
2. Murdoch IE,Sullivan TJ, Moseley I, Hawkins PN, PepysMB, Tan SY, Gamer A, Wright JE. Primary localisedamyloidosis of the orbit. Br J Ophthalmol 1996;80:1083-6.
SARCOIDOSIS
Sarcoid (from the Greek ‘sark’ and ‘oid’ meaning“flesh-like”) or Besnier-Boeck disease or Schaumann’ssyndrome.
Sarcoidosis is an idiopathic chronic nonnecrotizing granulomatous multi-systemic diseasethat affects skin, brain, eyes, lungs, spleen, thyroid,and liver. It commonly affects young adults, whofrequently present with hilar lymphadenopathy, pulmonary infiltration, ocular and cutaneouslesions.
Ocular involvement manifests in 25-60% ofpatients with systemic sarcoidosis.1 The mostcommon ocular manifestation in sarcoidosis is uveitisand the most common orbital manifestation isdacryoadenitis, which is frequently bilateral.2 Othermanifestations include eyelid swelling and palpableeyelid masses, conjunctival nodules, retrobulbarmasses, proptosis, optic nerve, chiasma or sheathinvolvement, optic radiation infiltration, bonedestruction and rarely extraocular muscleinvolvement.
It is mainly a diagnosis of exclusion based onclinical picture, laboratory tests, biopsy andradiologic evidence. Up to 90 percent of patients withocular sarcoid have abnormal chest radiographs.Hilar lymphadenopathy is seen (Figures 8.2A andB). Lung biopsy by tracheobronchial fiber optictechniques is 90 percent accurate. Biopsy of anenlarged, potentially infiltrated lacrimal gland orconjunctival granuloma is an acceptable alternative.
Figures 8.2A and B: CT chest showing hilarlymphadenopathy in sarcoidosis
A
B
basm
ala
blog
(alw
ays o
rigin
al)

Orbital Inflammatory DiseaseOrbital Inflammatory DiseaseOrbital Inflammatory DiseaseOrbital Inflammatory DiseaseOrbital Inflammatory Disease 131131131131131
Typical histologic findings from biopsy includeaccumulation of T lymphocytes and mononuclearphagocytes, diffuse non-caseating epitheloidgranulomas and derangements of the normal tissuearchitecture. Infectious etiologies need to be excludedby culture and/or staining.
Corticosteroids are the mainstay of treatment insymptomatic cases. Severe symptoms are generallytreated with steroids. In cases of steroid intoleranceor resistance, steroid sparing agents such asazathioprine and methotrexate are often used.Cyclophosphamide has also been used. As thegranulomas are caused by collections of immunesystem cells, particularly T cells, there has been someearly indication of success using immuno-suppressants, interleukin 2 inhibitors or anti tumornecrosis factor-alpha treatment (such as infliximab).
Lofgren’s syndrome represents an acutepresentation with erythema nodosum, bilateral hilarlymphadenopathy and polyarthralgia. This entity hasa relatively good prognosis.
The combination of anterior uveitis, parotitis andfever is called uveoparotid fever and in associationwith cranial nerve palsies is referred to as Heerfordt-Waldenstrom syndrome.
REFERENCES
1. Hunter DG, Foster CS. Ocular manifestations of sarcoidosis.In: Albert DM, Jakobiec FA, eds. Principles and practice ofophthalmology. Philadelphia: WB Saunders, 1994; 443-50.
2. Jakobiec F, Bilyk JR, Font RL Non infectious orbitalinflammations. In: Spencer WH, editor. Ophthalmicpathology - An Atlas and Textbook. WB Saunders,Philadelphia, 1996; 2810-58.
NONSPECIFIC ORBITALINFLAMMATORY SYNDROME (NSOIS)
Nonspecific orbital inflammatory syndrome (NSOIS),commonly referred to as Idiopathic OrbitalInflammation, Orbital Pseudotumor is defined as abenign, non infective clinical syndrome characterizedby features of nonspecific inflammatory conditionsof the orbit without identifiable local or systemiccauses. Idiopathic orbital inflammation is the thirdmost common non infectious orbital disease,following Graves’s orbitopathy and lympho-proliferative diseases. It accounts for 4.7 to 6.3% oforbital disorders.1
Idiopathic orbital inflammation has highlyvariable clinical features, from a diffuse to very focalprocess targeting specific orbital tissues, such as thelacrimal gland, extraocular muscles, optic nerve andorbital fat. Presentations vary according to thespecific location and the degree of inflammation,fibrosis, and mass effect. Ptosis, chemosis, motilitydysfunction, and optic neuropathy may also befound. Entrapment, compression, and destruction oforbital tissues may occur in patients with extensivesclerosis. Unilateral presentation is typical, butbilateral presentations are not uncommon.
Radiological imaging studies allow tissuecharacterization and localization without surgicalintervention and thereby have become invaluablediagnostic tools. Computed tomography is thepreferred mode of imaging. Idiopathic orbitalinflammation is typically seen on CT scans as a focalor diffuse mass, usually poorly demarcated andenhancing with contrast. Common CT findings includeenhancement with contrast medium, infiltration ofretrobulbar fat, proptosis, extraocular muscleenlargement, muscle tendon or sheath enlargement,apical fat edema, optic nerve thickening, uveal-scleralthickening, edema of the Tenon capsule, and lacrimalgland infiltration. Tendons of the extraocular musclesmay be involved or spared.
The histopathological spectrum of idiopathicorbital inflammation is typically non diagnostic, wide,and diverse, ranging from the typical diffusepolymorphous infiltrate to the atypical granulo-matous inflammation, tissue eosinophilia, andinfiltrative sclerosis. In the absence of systemic fibroinflammatory, granulomatous, and vasculitic disease,these atypical presentations are considered to besubclasses of idiopathic orbital inflammation.2
NSOIS respond rapidly to high dose steroidtherapy in tapering doses but recurrences arecommon. In such cases, chemotherapy (e.g.methotrexate, cyclosporine) and low-dose radiation(e.g. 1500-2500 cGy EBRT) may be needed to controlthe inflammation.3
REFERENCES
1. Henderson JW: Orbital tumors, Newyork, Ravin press,1994, (3rd ed), pp 13-14; 47;317-411.
2. Root man J: The classification and management of acuteorbital pseudotumors: Ophthalmology 1982, 89;1040-48.
3. Leone C: Treatment protocol for orbital inflammatorydiseases; Ophthalmology 1985, 92; 1325-31.
basm
ala
blog
(alw
ays o
rigin
al)

132132132132132 Surgical Atlas of Orbital DiseasesSurgical Atlas of Orbital DiseasesSurgical Atlas of Orbital DiseasesSurgical Atlas of Orbital DiseasesSurgical Atlas of Orbital Diseases
KIMURA’S DISEASE
Kimura’s disease is a chronic inflammatory disorderof uncertain etiology which typically presents asmultiple cutaneous nodules in the head and neckregion particularly the preauricular regions. It wasfirst described in China in 1937 by Kim and Szeto aseosinophilic lymphogranuloma.1
Kimura’s disease is most commonly seen inpatients between 20-40 years of age with a strikingmale predominance and is endemic among theoriental population. It is characterized by a triad ofinsidious onset of painless subcutaneous nodules inthe head and neck region, blood and tissueeosinophilia and markedly elevated serumimmunoglobulin levels.2 In the orbit, presentation isin the form of proptosis, upper lid swelling andorbital masses usually in the lacrimal gland.
The histomorphology of Kimura’s nodule ischaracterized by intense infiltration of lymphocytes,vascular proliferation and plasma cells with a variablenumber of lymphoid follicles with germinal centers.Typically, there is a moderate to intense eosinophilicinfiltration mainly in a perivascular pattern.Immuohistochemical stains would typically show IgEreticular network in the germinal centers.3
Following initial presentation, surgical excisionand biopsy with debulking is the preferred mode oftreatment, but recurrence is common. Othertreatment options include radiation, systemiccorticosteroids, cyclosporine and pentoxyfylline.
REFERENCES
1. Kim HT, Szeto C. Eosinophilic hyperplasticlymphogranuloma, comparison with Mikulicz’s disease.Chin med J. 1937 23:699-700.
2. Hui PK, Chan JK, Ng CS, Kung IT, Gwi E.Lymphadenopathy of Kimura’s disease. Am J Surg Pathol.1989; 13:177-86.
3. Motoi M, Wahid S, Horie Y, Akagi T. Kimura’s disease:clinical, histological, and immunohistochemical studies.Acta Med Okayama.1992;46:449-55.
WEGENER’S GRANULOMATOSIS
Wegener’s granulomatosis (WG) is a fulminantsystemic disease of unknown aetiology consisting ofnecrotizing granulomatous vasculitis of the upper and
lower respiratory tracts, focal necrotizingglomerulonephritis, and systemic small vesselvasculitis involving multiple organ systems.
Incidence of ocular involvement in WG variesfrom 29 to 79%.1, 2 Ocular involvement can be eitherdue to an extension from the adjacent paranasalsinuses (contiguous) or as a result of focal vasculitis(noncontiguous).1,2 Presentation can be in the formof proptosis, dacryocystitis, scleritis with peripheralkeratopathy, kerato-conjunctivitis sicca, uveitis,retinitis, retinal vascular occlusions, exudative retinaldetachments, and optic neuritis.
Laboratory findings support or confirm thediagnosis of WG. In the active stage of the diseaseraised ESR and leucocytosis are seen. Chest X-rayand computerised tomography detect pulmonaryinvolvement. Routine urine analysis detects renalinvolvement. Serum antibodies against thecytoplasmic component of neutrophils and monocytes(cANCA) form a useful adjunct in the diagnosis ofWG. Indirect immunofluorescence is currently thestandard test for ANCA screening.3 Between 80%and 95% of all ANCA found in WG is cANCA.
Diagnosis is established by biopsy in orbital andparanasal sinus involvement. The characteristichistopathologic picture is that of necrotising vasculitisof the blood vessels, usually with granulomaformation in the surrounding infiltrates.
Management of WG requires a multisystemapproach. Oral corticosteroids along with a cytotoxicagent, of which cyclophosphamide is the mostefficacious, is the treatment of choice. Early treatmentwith cyclophosphamide and corticosteroids reducesboth ocular and systemic morbidity.
Exacerbations are common in the first two yearsafter diagnosis. In cases of remission, azathioprine,cyclosporine A and methotrexate may be used.
REFERENCES
1. Straatsma BR. Ocular manifestations of Wegener’sgranulomatosis. Am J Ophthalmol 1957; 144:789-99.
2. Bullen CL, Liesegang TJ, McDonald TJ, DeRemee RA. Ocularcomplications of Wegener’s granulomatosis.Ophthalmology 1983;90:279-90
3. Harman LE, Margo CE. Wegener’s granulomatosis. Surveyof Ophthalmology 1998; 42:458-80.
basm
ala
blog
(alw
ays o
rigin
al)
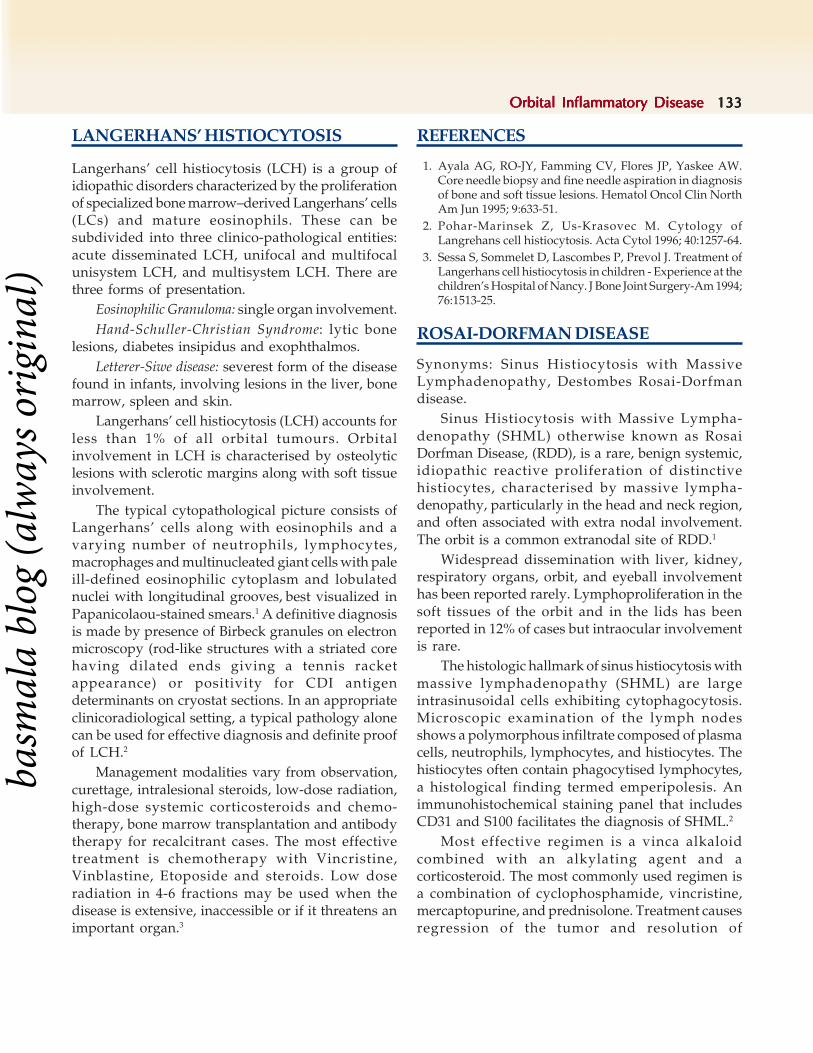
Orbital Inflammatory DiseaseOrbital Inflammatory DiseaseOrbital Inflammatory DiseaseOrbital Inflammatory DiseaseOrbital Inflammatory Disease 133133133133133
LANGERHANS’ HISTIOCYTOSIS
Langerhans’ cell histiocytosis (LCH) is a group ofidiopathic disorders characterized by the proliferationof specialized bone marrow–derived Langerhans’ cells(LCs) and mature eosinophils. These can besubdivided into three clinico-pathological entities:acute disseminated LCH, unifocal and multifocalunisystem LCH, and multisystem LCH. There arethree forms of presentation.
Eosinophilic Granuloma: single organ involvement.Hand-Schuller-Christian Syndrome: lytic bone
lesions, diabetes insipidus and exophthalmos.Letterer-Siwe disease: severest form of the disease
found in infants, involving lesions in the liver, bonemarrow, spleen and skin.
Langerhans’ cell histiocytosis (LCH) accounts forless than 1% of all orbital tumours. Orbitalinvolvement in LCH is characterised by osteolyticlesions with sclerotic margins along with soft tissueinvolvement.
The typical cytopathological picture consists ofLangerhans’ cells along with eosinophils and avarying number of neutrophils, lymphocytes,macrophages and multinucleated giant cells with paleill-defined eosinophilic cytoplasm and lobulatednuclei with longitudinal grooves, best visualized inPapanicolaou-stained smears.1 A definitive diagnosisis made by presence of Birbeck granules on electronmicroscopy (rod-like structures with a striated corehaving dilated ends giving a tennis racketappearance) or positivity for CDI antigendeterminants on cryostat sections. In an appropriateclinicoradiological setting, a typical pathology alonecan be used for effective diagnosis and definite proofof LCH.2
Management modalities vary from observation,curettage, intralesional steroids, low-dose radiation,high-dose systemic corticosteroids and chemo-therapy, bone marrow transplantation and antibodytherapy for recalcitrant cases. The most effectivetreatment is chemotherapy with Vincristine,Vinblastine, Etoposide and steroids. Low doseradiation in 4-6 fractions may be used when thedisease is extensive, inaccessible or if it threatens animportant organ.3
REFERENCES
1. Ayala AG, RO-JY, Famming CV, Flores JP, Yaskee AW.Core needle biopsy and fine needle aspiration in diagnosisof bone and soft tissue lesions. Hematol Oncol Clin NorthAm Jun 1995; 9:633-51.
2. Pohar-Marinsek Z, Us-Krasovec M. Cytology ofLangrehans cell histiocytosis. Acta Cytol 1996; 40:1257-64.
3. Sessa S, Sommelet D, Lascombes P, Prevol J. Treatment ofLangerhans cell histiocytosis in children - Experience at thechildren’s Hospital of Nancy. J Bone Joint Surgery-Am 1994;76:1513-25.
ROSAI-DORFMAN DISEASE
Synonyms: Sinus Histiocytosis with MassiveLymphadenopathy, Destombes Rosai-Dorfmandisease.
Sinus Histiocytosis with Massive Lympha-denopathy (SHML) otherwise known as RosaiDorfman Disease, (RDD), is a rare, benign systemic,idiopathic reactive proliferation of distinctivehistiocytes, characterised by massive lympha-denopathy, particularly in the head and neck region,and often associated with extra nodal involvement.The orbit is a common extranodal site of RDD.1
Widespread dissemination with liver, kidney,respiratory organs, orbit, and eyeball involvementhas been reported rarely. Lymphoproliferation in thesoft tissues of the orbit and in the lids has beenreported in 12% of cases but intraocular involvementis rare.
The histologic hallmark of sinus histiocytosis withmassive lymphadenopathy (SHML) are largeintrasinusoidal cells exhibiting cytophagocytosis.Microscopic examination of the lymph nodesshows a polymorphous infiltrate composed of plasmacells, neutrophils, lymphocytes, and histiocytes. Thehistiocytes often contain phagocytised lymphocytes,a histological finding termed emperipolesis. Animmunohistochemical staining panel that includesCD31 and S100 facilitates the diagnosis of SHML.2
Most effective regimen is a vinca alkaloidcombined with an alkylating agent and acorticosteroid. The most commonly used regimen isa combination of cyclophosphamide, vincristine,mercaptopurine, and prednisolone. Treatment causesregression of the tumor and resolution of
basm
ala
blog
(alw
ays o
rigin
al)

134134134134134 Surgical Atlas of Orbital DiseasesSurgical Atlas of Orbital DiseasesSurgical Atlas of Orbital DiseasesSurgical Atlas of Orbital DiseasesSurgical Atlas of Orbital Diseases
lymphadenopathy with minimal recurrence. Surgeryis indicated rarely, in life or function threateningsituations.
REFERENCES
1. Friendly DS, Font RL, Rao NA. Orbital involvement in‘sinus’ histiocytosis. Arch Ophthalmol 1977;95:2006–11.
2. Slone SP, Fleming DR, Buchino JJ. Arch Pathol Lab Med2003 Mar;127(3):341-4.
ORBITAL XANTHOGRANULOMA
Adult xanthogranulomatous diseases are non-Langerhans histiocytic disorders (type II) involvingthe ocular or orbital tissues and constitute a groupof entities with varying manifestations. They areadult onset xanthogranuloma (AOX), which isisolated with no systemic associations, adult onsetasthma with periocular xanthogranuloma (AAPOX),necrobiotic xanthogranuloma (NBX) and Erdheim-Chester disease (ECD). Juvenile xanthogranulomasusually present with skin or intraocular lesions andorbital involvement which is rare, occurs almostexclusively in children.1
Ocular involvement maybe in the form of eyelidor orbital mass, proptosis, orbital bone mass andextraocular muscle involvement,epibulbar mass,uveal mass, uveitis and rarely retinal and choroidalinvolvement. While the orbit or adnexalxanthogranuloma tends to be anterior in AOX,AAPOX, and NBX, it is often diffuse in ECD andleads to visual loss.
Diagnosis is confirmed by biopsy. Thecharacteristic appearance of xanthogranulomas onhistopathology is proliferation of histiocytes, plasmacells and lymphocytes with Touton giant cells thatstain positive for lipid. Touton giant cells aremultinucleate cells with the nuclei arranged in awreath around a nidus of eosinophilic cytoplasm andseparated from the cell membrane by a rim oftranslucent foamy cytoplasm.2 Necrosis (necrobiosis)with pallisading epitheliod histiocytes is mostly seenin NBX whereas large lymphoid aggregates withgerminal centers are often found in cases of AAPOX.ECD exhibits florid fibrosis with fewer follicles andmore dispersed lymphocytes and lipid ladenhistiocytes.
The clinical course is chronic and oftenprogressive. Various treatment modalities includelocal excision, periocular and systemic steroids,chemotherapy with low dose chlorambucil, nitrogenmustard, cyclophosphamide, melphalan, localradiation and plasma exchange.
REFERENCES
1. Zelger B, Cerio R, Orchard G, et al. Juvenile and adultxanthogranuloma. A histological and immunohisto-chemical comparison. Am J Surg Pathol 1994;18:126–35.
2. Murthy R, Honavar SG, Vemuganti GK, Naik M, BurmanS. Isolated giant xanthogranuloma of the orbit. Indian JOphthalmol [serial online] 2007 [cited 2007 Jul 22]; 55:156-58.
CASE ILLUSTRATIONS
Case 1
An 18-year-old female, presented with recurrentswelling of the right upper lid of 4 monthsduration.There was no history of pain, redness,diplopia or defective vision. A cystic mass was excisedelsewhere 8 months back, histopathology reportswere not available.
On examination, best corrected visual acuity inboth eyes was 6/6,N6. Ocular movements were fulland painless.There was fullness of the upper temporalpart of the right orbit. A firm to hard cord like masswas felt preseptally. The mass was adherent to thebone at the lateral canthus. (Figure 8.3) There wasno lymphadenopathy.
CT scan (Figure 8.4) showed enlarged mass, notseparate from lacrimal gland, surrounding the globe.It was heterogenous in density.
Figure 8.3: Showing fullness of upper temporalpart of the right orbit in a patient with sarcoidosis
basm
ala
blog
(alw
ays o
rigin
al)

Orbital Inflammatory DiseaseOrbital Inflammatory DiseaseOrbital Inflammatory DiseaseOrbital Inflammatory DiseaseOrbital Inflammatory Disease 135135135135135
Total excision of the mass was performedthrough anterior orbitotomy.Intraoperatively themass was found to be arising from the palpebral partof the lacrimal gland.
Histopathological examination revealed chronicgranulomatous inflammation with no evidence ofcaseation. Large amounts of granuloma withepitheloid cells and giant cells were observed,suggestive of sarcoidosis (Figure 8.5).
Special stain for fungus and acid fast bacilli werenegative.
Blood tests for serum calcium, phosphorus,proteins, angiotensin converting enzyme and serumlysozyme were within normal limits.
No systemic medications were started in viewof normal blood investigations.
The patient was asymptomatic and there was norecurrence during the postoperative follow up of twoyears.
Case 2
A male farmer, 45 years of age, presented withcomplaints of protrusion of right eyeball for the past2 months. His general health was good. Previousthyroid profile was normal.
Examination revealed best corrected visual acuityof 6/6p, N6 and 6/5, N6 in the right and left eyesrespectively. There was periocular fullness andinferior scleral show of 2 mm.The globe was pushedforwards by 9 mm,outwards by 3 mm and upwardsby 2 mm. Ocular motility was normal. There was norelative afferent papillary defect.There was increasedresistance to retropulsion (Figure 8.6). A firm masswas palpable in the inferomedial orbit, posteriorextent of which could not be felt.
Slit lamp examination of the anterior segment andintraocular pressure were within normallimits.Fundus examination revealed disc edema withno choroidal folds. CT scan revealed an illdefinedheterogenous mass lesion in the right inferomedialorbit extending upto the apex.Medial rectus andinferior rectus were included in the mass lesion(Figures 8.7 and 8.8). We did a right orbital biopsythrough a subciliary incision, with debulking of thetumor under general anesthesia. Intraoperatively aninfiltrating grey white firm mass was seen, which
Figure 8.4: CT scan showing anteriorly located heterogenousmass in the upper temporal quadrant in patient with sarcoidosis
Figure 8.5: Photomicrograph showing non-caeseatinggranulomas (Hematoxylin Eosin x 200)
Figure 8.6: Photograph showing periocular fullness, proptosis andscleral show in a patient with nonspecific inflammation of right orbit
basm
ala
blog
(alw
ays o
rigin
al)

136136136136136 Surgical Atlas of Orbital DiseasesSurgical Atlas of Orbital DiseasesSurgical Atlas of Orbital DiseasesSurgical Atlas of Orbital DiseasesSurgical Atlas of Orbital Diseases
was difficult to cut and hence was removedpiecemeal. Histopathological examination of thespecimen was consistent with a diagnosis of nonspecific inflammation with extensive fibrocollagenoustissue. In view of this finding,ultrasound abdomenwas done to rule out retroperitoneal fibrosis. ANCAtest was advised to rule out Wegener’s granulo-matosis. Both test reports were found to be withinnormal limits. Patient was started on tapering doseof oral steroids, starting with prednisolone50 mg/day, reducing it by 10 mg every 3 days andtab pentoxyfylline 400 mg TDS for one month
followed by 400 mg BD for one month. There wassignificant clinical improvement postoperatively withvision improving to 6/6, and complete resolution ofproptosis.
Case 3
A young female aged 15 years, presented with smallswelling in the upper outer quadrant of the left eyesince 2 years. The swelling was progressivelyincreasing in size. There was no pain, visualdisturbance or diplopia.
On examination, fullness of superotemporalregion with displacement of the globe downwardsand medially was seen (Figure 8.9). A soft to firmswelling with illdefined margins was palpable. It wascompressible, non reducible, non pulsatile and nontender. There was increased resistance toretropulsion. There was no lymphadenopathy.CT scan revealed well defined, heterogeneouslydense, non enhancing enlargement of lacrimal gland.(Figures 8.10A and B). We excised the mass in totothrough lateral orbitotomy. Histopathologyexamination revealed focal collection of chronicinflammatory cells with abundant fibrocollagenoustissue suggestive of nonspecific inflammation oflacrimal gland (Figure 8.11). Postoperatively, patientwas symptom free on follow up of 5 years.
Case 4
A 32-year-old female presented with complaints ofprotrusion, pain and redness in the right eyeassociated with progressive dimunition in vision since1 year.
On examination, the best corrected visual acuityin right eye was 2/60, N36. Marked lid edema and
Figure 8.7: Axial CT scan showing illdefined heterogenous masslesion extending upto apex in a patient with nonspecific inflammation
Figure 8.8: Coronal CT scan - Medial rectus and Inferior rectusmuscles involvement in the nonspecific inflammation of orbit
Figure 8.9: Photograph showing fullness of superotemporal regionwith downward displacement of the right globe in a patient withnonspecific inflammation of lacrimal gland
basm
ala
blog
(alw
ays o
rigin
al)

Orbital Inflammatory DiseaseOrbital Inflammatory DiseaseOrbital Inflammatory DiseaseOrbital Inflammatory DiseaseOrbital Inflammatory Disease 137137137137137
conjunctival congestion was seen, globe wasdisplaced forwards and downwards. Elevation andabduction of the globe was restricted. A palpablemass was felt in the superotemporal quadrant.Preauricular and submandibular lymphadenopathywas present on the same side. Ultrasound abdomenwas normal, FNAC showed reactive changes withmild eosinophilia. CT scan showed large extraconalorbital mass surrounding the globe all round,infiltrating the periocular structures (Figure 8.12). We
Figures 8.10A and B: Axial (A) and Coronal (B) sections of CT scan showing well defined, heterogeneously dense nonenhancingenlargement of lacrimal gland in a patient with nonspecific inflammation
Figure 8.11: Photomicrograph showing specimen of lacrimal glandwith chronic inflammatory cells surrounding it, suggestive ofinflammation of lacrimal gland (Hematoxylin Eosin x 100)
Figure 8.12: CT scan showing large extraconal orbital masssurrounding the globe and infiltrating the periocular structures in apatient with Kimura's disease
performed a lateral orbitotomy. Intraoperatively, themass was firm in consistency and was extensivelyinfiltrating the periorbital, lateral orbital and thelacrimal gland region extending upto the apex.
Histopathological report confirmed the diagnosisof angiolymphoid hyperplasia with eosinophilia
A B
basm
ala
blog
(alw
ays o
rigin
al)

138138138138138 Surgical Atlas of Orbital DiseasesSurgical Atlas of Orbital DiseasesSurgical Atlas of Orbital DiseasesSurgical Atlas of Orbital DiseasesSurgical Atlas of Orbital Diseases
(Kimura’s disease) (Figure 8.13). A course of systemicsteroids was given. Visual acuity improved to 6/6,N6 in the affected eye. She came back 4 months laterwith severe pain and headache, with massiveproptosis and keratinization of conjunctiva andcornea. Right eye had no perception of light. Patientwas referred to oncologist for chemotherapy andradiotherapy. The response was not satisfactory. Inview of the above, exenteration of the right orbitwas done. (Figure 8.14) Patient was fitted with aspectacle mounted prosthesis. Recurrence was seenthe form of tiny nodular subcutaneous lesions. CTscan evidence of orbital recurrence was seen in theform of soft tissue filling orbit (Figure 8.15). As thelesion was non malignant, it was decided to watchthe lesion for 6 months. Patient thereafter was lost
to follow up. This case shows that some of the benignorbital inflammations may be very aggressive andsevere disease may even necessitate orbitalexenteration.
Case 5
A male aged 41 years, presented with recurrent leftcheek swelling with protrusion of left eye since 5months. He had undergone partial maxillectomysurgery of the left side 1 year back.
On examination, his best corrected vision was6/9, N6 in both the eyes.Left proptosis with upwarddisplacement of the globe was seen. A firm to hardswelling was palpable in the left inferior orbit andcheek area. Elevation and depression of the left eyewas restricted. (Figure 8.16 ).No afferent papillarydefect was present. CT scan revealed soft tissue
Figure 8.13: CT scan post exenteration of thepatient with Kimura's disease
Figure 8.14: Appearance following orbital exenterationfor severe Kimura's disease
Figure 8.15: Photomicrograph showing blood vessels with scatteredeosinophils and lymphocytes in a patient with Kimura's disease(Hematoxylin Eosin x 200)
Figure 8.16: Photograph showing left proptosis, upward displacementof globe and fullness in periocular area in a patient with Wegener'sGranulomatosis
basm
ala
blog
(alw
ays o
rigin
al)

Orbital Inflammatory DiseaseOrbital Inflammatory DiseaseOrbital Inflammatory DiseaseOrbital Inflammatory DiseaseOrbital Inflammatory Disease 139139139139139
lesion in the left maxillary sinus with extraconalextension into the orbit (Figures 8.17A and B). TheCT scans showed evidence of partial resolution offindings following treatment with oral steroids(Figures 8.18A and B).
Histopathological examination showed depositsof fibrocollagenous tissue with areas of necrosis withvessel obstruction and dense collection of chronicinflammatory cells (Figure 8.19). A diagnosis ofWegener’s granulomatosis was kept in mind. Chest
Figures 8.17A and B: CT scan pre-treatment - showing soft tissue lesion due to Wegener'sGranulomatosis in the left maxillary sinus extending to left orbit
Figures 8.18A and B: CT scan, post-treatment with systemic steroids in a patient withWegener's Granulomatosis, showing partial resolution of the lesion
Figure 8.19: Photomicrograph showing diffuse inflammation with granulomatous reaction (giant cell formation).Arrow shows healed vasculitis. This is suggestive of Wegener's Granulomatosis (Hematoxylin Eosin x 100)
A B
A B
basm
ala
blog
(alw
ays o
rigin
al)

140140140140140 Surgical Atlas of Orbital DiseasesSurgical Atlas of Orbital DiseasesSurgical Atlas of Orbital DiseasesSurgical Atlas of Orbital DiseasesSurgical Atlas of Orbital Diseases
X-ray was normal. p ANCA and c ANCA wereborderline.Patient was evaluated by rheumatologistand based on clinical diagnosis of Wegener’sgranulomatosis, was started on oral steroids. Patienthad resolution of symptoms and decrease in swellingfollowing treatment.
Case 6
A male child aged 4 years was referred with CT scanof orbit as a case of malignant lacrimal gland tumor.He had painful swelling of right upper lid of 2 monthsduration and raised ESR. On examination, his bestcorrected vision was 6/18 in the right eye. Tender
swelling of the right upper lid, more on lateral aspectwas noticed (Figure 8.20). There was no proptosis.Ocular motility was normal.Rest of anterior segmentand fundus examination was normal. CT scan(Figures 8.21A and B) revealed an irregularheterodense mass in the lacrimal gland region,associated with lysis of lateral wall and temporal partof roof of orbit. With the presumptive diagnosis ofLangerhan cell histiocytosis, he underwent acomplete evaluation including bone marrow whichwas normal. Chest X-ray revealed interstitialpneumonia. An anterior orbitotomy revealedyellowish black material. Impression cytology andpermanent sections confirmed the diagnosis ofLangerhans cell histiocytosis. On pediatrician’sadvise, patient was started on oral prednisolone and6-Mercaptopurine. Patient has been free of symptomson a followup of 3 years.
Case 7
A male child aged 2 years presented withgradual onset of swelling in the right upper lid since3 months.There was sudden increase in swelling inthe last 2 days. On examination, a well circumscribed,non tender, firm lesion was palpable in the superiororbit.Posterior limit could not be felt (Figure 8.22).CT scan showed heterogenous soft tissue in the
Figure 8.20: Photograph showing swelling of the lateral part ofright upper eyelid in a patient with Langerhans’ cell histiocytosis
Figures 8.21A and B: CT scan shows an irregular heterodense mass in the lacrimal gland area associated withlysis of lateral wall and temporal part of roof of orbit in a patient with Langerhans’ cell histiocytosis
A B
basm
ala
blog
(alw
ays o
rigin
al)

Orbital Inflammatory DiseaseOrbital Inflammatory DiseaseOrbital Inflammatory DiseaseOrbital Inflammatory DiseaseOrbital Inflammatory Disease 141141141141141
Figure 8.22: Photograph showing swelling of the right upper eyelid in another patient with Langerhans’ cell histiocytosis
anterior superior aspect of the right orbit(predominantly preseptal) with lytic lesions in thetemporal bone (Figures 8.23A and B). Anteriororbitotomy with excision of mass was done. It wascream to black in colour and soft in consistency.Histopathological examination showed largecollection of histiocytes, in addition to lymphocytes,eosinophils, plasma cells and few multinucleatedgiant cells (Figure 8.24). He was treated withintravenous steriods followed by oral steroids forone month. There was complete resolution of massfollowing this. He was asymptomatic during twoyears of follow-up.
Figure 8.24: Photomicrograph showing numerous eosinophils andhistiocytes suggestive of Langerhans’ cell histiocytosis(x100,Hematoxylin Eosin)
Figures 8.23A and B: CT scan showing heterogenous soft tissue in the anterior superior aspect of the right orbit(predominantly preseptal) with lytic lesion in the temporal bone in a patient with Langerhans’ cell histiocytosis
A B
basm
ala
blog
(alw
ays o
rigin
al)

142142142142142 Surgical Atlas of Orbital DiseasesSurgical Atlas of Orbital DiseasesSurgical Atlas of Orbital DiseasesSurgical Atlas of Orbital DiseasesSurgical Atlas of Orbital Diseases
Figure 8.25: Photographs showing left proptosis, upward globedisplacement and fullness of the left side of the face in a patient withRosai-Dorfman disease
Figures 8.26A to D: MRI scans of the patient with Rosai-Dorfman disease shows illdefined extra and intraconal heterogenous mass lesion,isointense in T1 and hypointense in T2 weighted images with homogenous contrast enhancement. Inferior and lateral rectus muscles arethickened and displaced
A B
C D
Case 8
A 31-year-old female, presented with recurrentepisodes of swelling and prominence of left eye since8 months.She had been on steroids off and on. Onexamination, fullness of left side of face was seen.There was 4mm left axial proptosis. Firm irregularmass was palpable in the left inferior orbit.There wasno lymphadenopathy (Figure 8.25). MRI scan showeda huge fusiform retrobulbar mass (Figures 8.26A toD). Histopathological and immunochemistry studyof the biopsy specimen revealed features consistent
basm
ala
blog
(alw
ays o
rigin
al)

Orbital Inflammatory DiseaseOrbital Inflammatory DiseaseOrbital Inflammatory DiseaseOrbital Inflammatory DiseaseOrbital Inflammatory Disease 143143143143143
Figure 8.27: Photomicrograph showing histiocytes with lymphocytesand plasma cells in Rosai-Dorfman disease ( x 40, Hematoxylin Eosin)
Figure 8.28: Photograph showing downward displacement of righteyeball, with proptosis in a patient with Juvenile Xanthogranuloma
Figure 8.29: CT scan showing a large slightly hyperdense retrobulbarmass with excavation of medial wall in the patient with JuvenileXanthogranuloma
with Rosai Dorfman syndrome (Figure 8.27). Patientwas seen by oncologist who advised radiation to theorbit. Patient refused treatment and was lost tofollow-up. She came back one and a half years laterwith double vision and massive proptosis. There wasincreased retrobulbar resistance. Disc edema was seenon fundus evaluation. In view of the huge size of thelesion and the high dose of radiation that would berequired with its potential complications, it wasdecided to perform a surgical debulking.Intraoperatively, a firm grey tumor was seeninfiltrating the inferior orbit. Inferior rectus wasdensely adherent to it. Patient was advised taperingdose of oral steroids. Patient was free of symptomson 2 years of follow-up.
Case 9
A male child, age 1 year, presented with prominenceof right eye since last 20 days. There was no pain,redness, fever or weight loss. On examination, therewas downward displacement of right eyeball with 4mm proptosis (Figure 8.28). Resistance to retro-pulsion was felt. Restriction of elevation andabduction was seen. Fundus examination revealedmild disc edema with dilated tortuous retinal veins.CT scan revealed a large slightly hyperdenseretrobulbar mass with excavation of medial wall oforbit (Figure 8.29). The mass was removed piecemealby anterior orbitotomy. Histopathological exami-nation showed features of juvenile xanthogranuloma(Figure 8.30 ). He was started on tapering dose of
oral steroids. On 6 months followup, completeresolution of proptosis was seen. He wasasymptomatic at follow-up of 3 years.
Case 10
A young female of age 35 years, presented withpainless progressive protrusion of both eyes sincefive years. She had occasional double vision. Shehad been treated with oral steroids off and on withdramatic improvement in symptoms, and recurrenceon stopping the same. She had received anti
basm
ala
blog
(alw
ays o
rigin
al)

144144144144144 Surgical Atlas of Orbital DiseasesSurgical Atlas of Orbital DiseasesSurgical Atlas of Orbital DiseasesSurgical Atlas of Orbital DiseasesSurgical Atlas of Orbital Diseases
Figure 8.30: Photomicrograph shows numerous Toutan giant cells,(Hematoxylin Eosin × 40 ) suggestive of Xanthogranuloma
tuberculosis therapy earlier. She also reporteddryness of the mouth. On examination, her bestcorrected visual acuity was 6/36, N36 and 6/24, N6in the right and left eye respectively.Axial proptosiswas noted with firm palpable orbital masses in bothorbits, most prominent in the superonasalorbit.Ocular movements were restricted in allgazes.There was no lagophthalmos (Figure 8.31).
Slit lamp examination revealed reduced tearmeniscus, superficial punctuate keratopathy andposterior subcapsular cataract in both the eyes.Fundus examination revealed striae in the right eyeand choroidal folds in the left eye. Bilateral parotidenlargement was noted on both sides. Thus the
possibility of Sjogren’s syndrome with underlyingautoimmune disease was considered. CT scan of theorbit revealed bilateral diffuse illdefined extra andintraconal soft tissue with clumps of calcificationwithin (Figures 8.32A and B). Transeptal orbitalbiopsy was done under general anesthesia. Histo-pathological examination suggested xantho-granulomatous inflammation. Medical oncology anddermatology opinion was sought. In view of sideeffect of long term steroids, patient was started onoral anti-inflammatory drugs and steroid sparingimmunosuppressive therapy (Cyclophosphamide,Endoxan 50 mg daily), with biweekly monitoring ofWBC and platelet counts. Surgical debulking was not
Figure 8.31: Photograph showing bilateral proptosisin a patient with Xanthogranuloma orbit
Figures 8.32A and B: CT scan in the patient with Xanthogranuloma showing bilateral diffuse illdefined periocular, extraand intraconal soft tissue lesion. Extraocular muscles cannot be identified separately.Clumps of calcification noted
A B
basm
ala
blog
(alw
ays o
rigin
al)

Orbital Inflammatory DiseaseOrbital Inflammatory DiseaseOrbital Inflammatory DiseaseOrbital Inflammatory DiseaseOrbital Inflammatory Disease 145145145145145
considered in view of potential risks. Oral anti-inflammatory drugs had to be stopped after a monthdue to increase in dry eye symptoms. On last follow-up, patient was symptomatically better.The wasconsiderable decrease in proptosis and improvementof extraocular motility. Patient was symptomatic dueto dry eyes, but had much reduced proptosis andorbital symptoms.
ACKNOWLEDGEMENTS
We are grateful to Dr J Biswas and Dr S Krishna Kumar, OcularPathology Service, Sankara Nethralaya for their help with thephotomicrographs and Dr Veena Noronha, Radiology Service,Sankara Nethralaya for help in the interpretation of radiologic images.We are also grateful to Dr Nirmala Subramaniam, EmeritusProfessor of Oculoplasty, Sankara Nethralaya for providing someof the photographs.
basm
ala
blog
(alw
ays o
rigin
al)
146146146146146 Surgical Atlas of Orbital DiseasesSurgical Atlas of Orbital DiseasesSurgical Atlas of Orbital DiseasesSurgical Atlas of Orbital DiseasesSurgical Atlas of Orbital Diseases
Christopher s, Laurence Brown, Raghavan Sampath
Orbital LymphomaOrbital LymphomaOrbital LymphomaOrbital LymphomaOrbital Lymphoma
The Lymphoproliferative diseases, includingmalignant lymphoma, are not a single disease entitybut a collection of disorders ranging from benignreactive hyperplasia, atypical lymphocyte infiltrateto malignant lymphoma.1 Some consider idiopathicorbital inflammation (pseudotumor) as part of thelymphoproliferative disease spectrum.1 Approxi-mately 75% of patients with purely orbital lymphomawill develop systemic disease, whilst 1-5% of thosewith systemic disease will have orbital involvement.1
Overall orbital lymphoma accounts for less than 1%of all lymphoma.2 Interestingly those patients withatypical orbital lymphocytic infiltrate are at anincreased risk of systemic lymphoma.1
Various classifications of Lymphomas are invogue. They include the following:
Revised European American LymphomaClassification (REAL Classification)3
1. Leukemias and Lymphomas of B-cell Origin(Pan B CD 19,20+)
A. Indolent B-cell malignancies:(i) Small lymphocytic lymphoma
(ii) Hairy cell leukemia(iii) Follicular lymphomas(iv) Lymphoplasmacytoid lymphoma(v) Marginal zone lymphoma.
B. Aggressive B-cell malignancies:(i) Diffuse large cell lymphoma
(ii) Follicular large cell lymphoma(iii) Mantle cell lymphoma(iv) Burkitt's lymphoma(v) Plasmacytoma / Myeloma
2. Leukemias and Lymphomas of T-cell Origin(CD 2, 7+)
A. Indolent T-cell malignancies:(i) T-CLL
(ii) Cutaneous T-cell lymphoma (Sezarysyndrome)
B. Aggressive T-cell malignancies:(i) Peripheral T-cell NHL
(ii) Angioimmunoblastic T-cell lymphoma(iii) Intestinal T-cell lymphoma(iv) Adult T-ALL
WHO Classification of NHL1. B-cell Neoplasms
A. Precursor B-cell ALLB. Mature B-cell malignancies:
(i) B-cell CLL(ii) Plasmacytoma
(iii) Extranodal marginal B-cell lymphoma(iv) Mantle cell lymphoma(v) Follicular lymphoma
(vi) Diffuse large B-cell lymphoma(vii) Burkitt's lymphoma
(viii) B-cell promyelocytic leukemia(ix) Hairy cell leukemia(x) Lymphoplasmocytic lymphoma
(xi) Monocytoid B-cell lymphoma.2. T-cell Neoplasms
A. Precursor T-cell ALLB. Mature T-cell malignancies:
(i) Mycosis fungicides
9C H A P T E R
basm
ala
blog
(alw
ays o
rigin
al)

Orbital LymphomaOrbital LymphomaOrbital LymphomaOrbital LymphomaOrbital Lymphoma 147147147147147
(ii) Adult T-cell lymphoma(iii) Anaplastic or Null cell lymphoma(iv) Peripheral T-cell lymphoma, not
specified(v) T-cell prolymphocytic leukemia
(vi) Aggresive NK cell leukemia(vii) T-cell gruanular lymphocytic
leukemia.
Modified Rye's Classification of Hodgkin'sLymphoma4
1. CLASSIC HD:A. Lymphocyte-predominanceB. Nodular sclerosisC. Mixed cellularityD. Lymphocyte depletion.
2. Nodular Lymphocyte-predominant HDClinically it is difficult to differentiate the
malignant and non-malignant tumors since age, sex,presenting symptoms and radiographic findings aresimilar. Even utilising immunohistochemical andmolecular biology techniques it is difficult to separatethe conditions.1 Polymerase chain reaction is amethod of amplifying target genetic material in tissuesamples to identify a gene re-arrangement diagnosticof lymphoma. This is particularly useful when themicroscopic morphology resembles chronic inflam-mation, but the clinical presentation is suggestive oflymphoma.5
Orbital lymphoma is typically a non-HodgkinsB-cell lymphoma arising from mucosa-associatedlymphoid tissue (MALTOMA)1,6 and accounts forapproximately 10-15%1,7 of all orbital masses. Whenonly malignant masses are taken in to account, theyaccount for 55% of the lesions.1 Other types oflymphoma identified in the orbit include extranodalmarginal zone lymphoma (MZL), follicular (FL),diffuse large B-cell (DLBCL), mantle cell (MCL), B-cell chronic lymphocytic leukaemia (CLL)/smalllymphocytic lymphoma, peripheral T-cell lymphoma(PTCL) and natural killer cell lymphoma (NKCL).8
Orbital lymphoma tends to be a bilateral diseaseand can affect the conjunctiva, lacrimal gland, befound in the nasolacrimal duct, as well as intraconaland extraconal space.1,9 The orbital lesions tend topresent insidiously with painless proptosis in the sixth
decade,1,7,10 whilst visual impairment is relatively rareoccurring in only 13% of patients.7 It can rarelypresent like acute orbital inflammation or cellulitis.MZL has the lowest risk of accompanying extra-orbital disease and consequently, the lowest risk oflymphoma-associated death.3
Radiographically orbital lymphomas tend to behomogenious in nature and mould themselvesaround orbital structures such as the globe and opticnerve.1,9 Bone erosion is rare although bonedestruction can occur with aggressive tumors.7
Radiotherapy is an effective treatment for orbitalMALT lymphoma using doses in the order of30Gy.11,12 The 5 and 10 years survival rates for MALTlymphoma is 100% and 88%.12
Orbital inflammatory disease include a widespectrum of conditions ranging from idiopathicorbital inflammation to orbital involvement of specificsystemic inflammatory disorders such as Wegener’sgranulomatosis, sarcoidosis, systemic lupuserythematosus (SLE) or Tolosa Hunt syndrome.13 Inthe case of Wegener’s granulomatosis and sarcoidosisocular involvement occurs in approximately 50% ofaffected subjects. The inflammation may affectmultiple or localized orbital tissues and can involvethe sclera.13 Investigations are therefore guidedtowards identifying these specific diagnoses. Theseinclude a battery of blood tests including full bloodcount (FBC), urea and electrolytes (U&E), C reactiveprotein (CRP) and/or erythrocyte sedimentation rate(ESR), autoantibody screen, anti-nuclear antibodyscreen (ANA), ANCA, rheumatoid factor (RhF),thyroid function tests (TFT), thyroid peroxidiseantibody screen and serum ACE. Radiological testsinclude a chest X-ray, and orbital imaging (CT and/or MRI). An orbital ultrasound scan can be beneficial.
Where no underlying cause can be identified thediagnosis of idiopathic orbital inflammation can bemade.
When to Suspect Lymphoma• Age of onset: more common in the elderly• Insidious onset• Bilateral disease with no evidence of
indentation of the globe (choroidal folds)• Lacrimal gland involvement, lesions are typically
firm/rubbery on palpation
basm
ala
blog
(alw
ays o
rigin
al)

148148148148148 Surgical Atlas of Orbital DiseasesSurgical Atlas of Orbital DiseasesSurgical Atlas of Orbital DiseasesSurgical Atlas of Orbital DiseasesSurgical Atlas of Orbital Diseases
• Conjunctival involvement, lesions are typicallysalmon colored
• Orbital imaging will reveal the lesion to bemoulded around the globe.
When to Suspect Idiopathic OrbitalInflammatory Disease
• Onset is usually acute• Symptoms include; pain, erythema, proptosis,
diplopia and blurred vision• Involvement of the extraocular muscles and the
sclera (scleritis)• Differential diagnosis includes; orbital cellulitis,
a systemic inflammatory disease such asWegeners granulomatosis, sarcoidosis,polyarteritis nodosa and neoplasms such aslymphoma
• Investigations include; FBC, U & E, CRP,antibody screen, serum ACE, ANA, ANCA,RhF, thyroid function and thyroid peroxidaseantibodies
• Imaging; orbital CT and/or MRI scan,ultrasound scan to rule out scleritis and a chestX-ray where sarcoidosis is suspected.
CASE ILLUSTRATIONS
Case 1
A 52 years old diabetic female presented to the orbitclinic with enlargement of the left lacrimal gland.Examination revealed proptosis of 5 mm on the leftside, whilst oculomotility was full, there was noRAPD and funduscopy was unremarkable. Routinebloods were taken to rule out autoimmune conditionsand inflammatory conditions such as Wegner'sgranulomatosis, systemic lupus erythematosus (SLE),Sjorgren's syndrome, and sarcoidosis. These wereall negative. An urgent CT scan revealed a discretesoft tissue mass arising from the left lacrimal gland(Figure 9.1) extending in to the orbit and displacingthe lateral rectus muscle. The right orbit was normal.The differential diagnosis included plemorphicadenoma and lymphoma.
Excision biopsy via a lateral orbitotomy approachwas performed since pleomorphic adenoma wassuspected.
Initial examination of the biopsy specimenidentified a dense exudate of lymphoid cells formingprominent germinal centers. The appearance was
suggestive of reactive lymphoid change. Subsequentimmunohistochemistry identified T and B cellproliferation and in one specimen kappa light chainscould be identified. A low grade lymphoma wassuspected. Molecular genetics confirmed thediagnosis of low grade B cell lymphoma.
The wounds settled well postoperatively andvision was maintained at 6/9 in the left eye and 6/5in the right. A referral was made to the lymphomaservice for a course of radiotherapy. There was noevidence of systemic lymphoma. 40 Gy was given tothe right orbit in 20 fractions.
Postradiotherapy she suffered from a dry eyeand was prescribed lubricants. A combination ofradiation and diabetic retinopathy subsequentlydeveloped. However there was no evidence ofrecurrence at 6 years.
Case 2
A 31 years old male attended the eye casualty with a3 weeks history of bilateral orbital inflammation(Figure 9.2) and right sided proptosis (Figure 9.3).Visual acuity was 6/5 in both eyes and IOPs werenormal. Examination revealed bilateral conjunctivalchemosis, associated with reduced upgaze andabduction. Fundoscopy was unremarkable. Routinebloods were taken to rule out inflammatorydisorders. C-reactive protein and plasma viscositywere elevated as was the white cell count. An urgentMRI scan was arranged which revealed bilateralenlargement of the lacrimal glands (Figure 9.4)suggestive of lymphoma.
Urgent lacrimal gland biopsy was performed.Histology confirmed the diagnosis of Hodgkin’s
lymphoma and referral to the lymphoma service wasmade.
Figure 9.1: Left lacrimal gland enlargement
basm
ala
blog
(alw
ays o
rigin
al)

Orbital LymphomaOrbital LymphomaOrbital LymphomaOrbital LymphomaOrbital Lymphoma 149149149149149
Case 3
A 63 years old male was referred to the eye casualtywith a 3 month history of diplopia and right sidedproptosis. Onset had been gradual and visual acuitywas 6/9 in both eyes. Examination revealed 3 mm ofproptosis in the right eye which was associated withreduced ocularmotility in all directions of gaze.Intraocular pressure was normal and there was noevidence of an RAPD. Fundoscopy revealed evidenceof choroidal folds on the right although both discswere healthy. There was no associated ocular painor headache and there was no history of weight loss,fever or cough. He was an ex-smoker having stopped6 years previously. There was no significant pastmedical history. Routine bloods were taken to ruleout systemic causes. Urgent CT and MRI scans wereperformed, revealing orbital inflammation suggestiveof lymphoma.
An urgent orbital biopsy was performed within3 days and the patient started on a reducing dose ofsteroids postoperatively. Histology was inconclusive
revealing only chronic inflammation. Lymphoma wasstill suspected, and after a discussion with the patient,a more extensive orbital biopsy was performed.Histology was once again inconclusive, revealing onlyscant lymphoid exudates. Subsequent immun-ohistochemistry identified B and T cells. No evidenceof lymphoma was found.
Referral was made to the lymphoma team to ruleout systemic lymphoma. None was identified. Thepatient continues to be followed up.
Case 4
A 26 years old female presented to eye casualty witha three day history of right orbital swelling. Visualacuity was 6/9 in the right eye and 6/6 in the left.There was marked chemosis (Figure 9.5) andproptosis of the right eye associated with andreduced upgaze and adduction. Fundoscopy wasnormal and there was no evidence of papilloedema.No RAPD was noted. The patient was apyrexial. Adiagnosis of orbital cellulitis was made andappropriate treatment commenced. CT scan of theorbits revealed preseptal and orbital inflammationwith evidence of mild proptosis. The extraocularmuscles and optic nerve were normal and sinusesclear. There was no evidence of any abscessformation. An orbital ultrasound scan was normal.
Despite intravenous antibiotics no improvementin the symptoms was seen. Referral was made to theorbital service and idiopathic orbital inflammationdiagnosed. Routine bloods were taken to rule outsarcoidosis, Wegeners granulomatosis, and syphilis,along with an auto-antibody screen, full blood count,thyroid function tests and C-reactive protein screen(CRP). All these tests were normal other than anelevated CRP. Systemic steroids were commenced(Prednisolone 1mg/kg) along with a histamine H2receptor antagonist. Over the next few days thesymptoms and eye movements started to resolve.
Figure 9.2: Bilateral orbital inflammation
Figure 9.3: Right sided proptosis
Figure 9.4: Bilateral lacrimal gland enlargement
Figure 9.5: Right sided chemosis and lid edema
basm
ala
blog
(alw
ays o
rigin
al)

150150150150150 Surgical Atlas of Orbital DiseasesSurgical Atlas of Orbital DiseasesSurgical Atlas of Orbital DiseasesSurgical Atlas of Orbital DiseasesSurgical Atlas of Orbital Diseases
The patient was discharged home on a reducing doseof steroids. Urgent immunology and rheumatologyout patient appointments were arranged. Nounderlying immunological or rheumatologicalabnormalities were detected.
Three months following the initial episode, thepatient returned to eye casualty with a flare up inthe left eye, and then a further six months and twoyears later in the right eye. All episodes settled witha short course of systemic steroids. Biopsy isnormally recommended for all suspected idiopathicorbital inflammation but in this particular patient thefeatures were typical with no localising lesion so abiopsy wasn't performed.
Surgical Approach
Surgery is generally indicated to obtain tissue forhistology and to aid diagnosis of suspicious lesions.Incisional biopsy is the treatment of choice.
Incisional Biopsy
The lateral 1/2 of the upper lid skin crease is markedwith pen and extended down parallel to the lidmargin, level with the lateral canthus, where it isextended in a horizontal plane just past the orbitalrim. Local anesthetic is injected subcutaneously. Askin incision is made along line with a cuttingdiathermy. Both the palpebral and orbital parts ofthe lacrimal gland are identified and an incisionalbiopsy is made. Any other suspicious lesions are alsobiopsied and sent for histology.
The deep tissues are closed with 5.0 vicryl andskin closed with 6.0 prolene.
Suspicious visible conjunctival (bulbar andpalpebral) and sub-conjunctival lesions should alsobe biopsied.
A reducing dose of steroids is given for 18 daysalong with a histamine H2 receptor antagonist suchas ranitidine.
A head-light can be worn throughout theprocedure to ensure adequate illumination of theoperating field.
REFERENCES
1. Akansel G, Hendrix L, Erickson BA, et al. MRI patterns inorbital malignant lymphoma and atypical lymphocyticinfiltrates. Eur J Radiol 2005;53(2):175-81.
2. Norton AJ. Monoclonal antibodies in the diagnosis oflymphoproliferative diseases of the orbit and orbitaladnexae. Eye 2006;20(10):1186-8.
3. Jenkins C, Rose GE, Bunce C, et al. Histological features ofocular adnexal lymphoma (REAL classification) and theirassociation with patient morbidity and survival. Br JOphthalmol 2000;84(8):907-13.
4. Schnitzer B. Classification of lymphomas. CRC Crit RevClin Lab Sci. 1978;9(2):123-78. Review.
5. Coupland SE, Krause L, Delecluse HJ, et al. Lympho-proliferative lesions of the ocular adnexa. Analysis of 112cases. Ophthalmology 1998;105(8):1430-41.
6. White WL, Ferry JA, Harris NL, Grove AS, Jr Ocular adnexallymphoma. A clinicopathologic study with identificationof lymphomas of mucosa-associated lymphoid tissue type.Ophthalmology 1995;102(12):1994-2006.
7. Selva D, Rootman J, Crompton J Orbital lymphomamimicking optic nerve meningioma. Orbit 2004;23(2):115-20.
8. McKelvie PA, McNab A, Francis IC, Fox R, O'Day J Ocularadnexal lymphoproliferative disease: a series of 73 cases.Clin Experiment Ophthalmol 2001;29(6):387-93.
9. Sullivan TJ, Valenzuela AA Imaging features of ocularadnexal lymphoproliferative disease. Eye 2006;20(10):1189-95.
10. Demirci H, Shields CL, Shields JA, Honavar SG, MercadoGJ, Tovilla JC Orbital tumors in the older adult population.Ophthalmology 2002;109(2):243-8.
11. Bhatia S, Paulino AC, Buatti JM, Mayr NA, Wen BC. Curativeradiotherapy for primary orbital lymphoma. Int J RadiatOncol Biol Phys 2002;54(3):818-23.
12. Hasegawa M, Kojima M, Shioya M, et al. Treatment resultsof radiotherapy for malignant lymphoma of the orbit andhistopathologic review according to the WHO classification.Int J Radiat Oncol Biol Phys 2003;57(1):172-6.
13. Gordon LK Orbital inflammatory disease: a diagnostic andtherapeutic challenge. Eye 2006;20(10):1196-206.
basm
ala
blog
(alw
ays o
rigin
al)

Vascular Lesions of OrbitVascular Lesions of OrbitVascular Lesions of OrbitVascular Lesions of OrbitVascular Lesions of Orbit 151151151151151
Subrahmanyam Mallajosyula, Mohd Javed Ali
Vascular LesionsVascular LesionsVascular LesionsVascular LesionsVascular Lesionsof Orbitof Orbitof Orbitof Orbitof Orbit
To comprehend the vascular lesions of the orbit, itis very important to have embryological,pathological and clinical concepts very clear in mind.There have been numerous ways of classifying theselesions, the most common being to divide them intomalformations, shunts and new growths.1 Manyentities have been placed under these three headingswhich we will discuss in detail.
MALFORMATIONS
Malformations are present since the time of birth,though they may not manifest at that time. Flatendothelium lines their wall, and in contrast toneoplastic lesions, do not show any growth in-vitro.The orbital society has classified malformations as:2
a. No flow or hemodynamically isolatedmalformations. For example: Lymphangioma.
b. Venous flow malformations. For example:Varices.
c. Arterial flow malformations. For example:Cavernous hemangioma.
d. Other congenital malformations. For example:Phakomatosis.
Lymphangioma
These are benign vascular lesions seen usually in theearly childhood and commonly confused with orbitalvenous anomalies and hemangiomas. Though theyare hemodynamically isolated, they arborize the orbitand bleeding into their lumen causing chocolate cystis not very uncommon. Lymphangiomas often
enlarge during the upper respiratory infectionsprobably due to the inflammatory response of thelymphoid tissue within the lesion.3
Superficial lymphangiomas are lesions of the lidor conjunctiva, readily visible on inspection asmultiple serous or blood filled cysts. These are usuallypurely lymphatic in character. Indication formanagement is due to cosmetic reasons and can beremoved easily.4
Deep Lymphangiomas have in addition venousconnections and may cause slowly progressiveproptosis. They may present with increase in sizeduring upper respiratory infection. It can also presentwith sudden proptosis due to bleeding into its lumencausing a chocolate cyst. A significant number ofthese patients may present with signs of optic nervecompression like decreased visual acuity,dyschormatopsia, diminished contrast and lightbrightness sensitivity and visual field defects.
Imaging modalities used include Ultrasono-graphy, CT or MRI. Of these MRI is the diagnosticmodality of choice.1 USG demonstrates cystic massesin the retrobulbar space. CT shows low densitymasses in intra and extraconal compartments withminimal ring enhancement on contrast. No vascularcomponent is noted on angiography. MRI is usefulto delineate the lesions well and is also helpful intiming the chocolate cyst as being acute, subacute orchronic which may have clinical implications.5
Management is usually conservative sincespontaneous regression of the cysts is common.Surgery though ungratifying because of incomplete
10C H A P T E R
basm
ala
blog
(alw
ays o
rigin
al)

152152152152152 Surgical Atlas of Orbital DiseasesSurgical Atlas of Orbital DiseasesSurgical Atlas of Orbital DiseasesSurgical Atlas of Orbital DiseasesSurgical Atlas of Orbital Diseases
removal and recurrences, should still be carried onin the presence of signs of optic nerve compression.Carbon dioxide and contact Nd:YAG lasers are usefulsurgical adjuncts.6
Other recent modalities that are gainingupperhand in the initial management includes theuse of sclerosing agents. Many sclerosing agents inuse include Picibanil (OK-432)7,8 percutaneous ethanol9
and bleomycin.10 Certain other agents like 5% sodiummorrhuate11 and sodium tetradecyl sulfate,12
considered to be more effective by some for themanagement of low flow vascular lesions have beenrecommended as the first line therapy forlymphangiomas.11
Orbital Varices
Orbital varices are weakened, dilated segments oforbital venous system. Age at presentation variesfrom childhood to middle ages .Most of the casesare unilateral and upper nasal quadrant is thefavoured site. Clinical signs include visible lesions inthe eyelid or conjunctiva, or the patient may presentwith a non-pulsatile proptosis which is accentuatedwith increasing venous pressure like while straining,assuming a dependant posture like sitting with a headdown position or by a valsalva maneuver. Since theorbital venous channels are devoid of valves, areversible proptosis occurs.13 Rarely varices maythreaten the vision by optic nerve compression dueto acute hemorrhage or thrombosis. Chronic lesionsmay present as enophthalmos.14
Imaging modalities used include CT scan,Doppler ultrasonography and angiography. Dopplerdemonstrates the flow of blood. Rapid spiral CTduring valsalva maneuver shows characteristicenlargement of the engorged varix. Uniform contrastenhancement is seen. Sometimes phleboliths may alsobe seen. Angiography shows connection of the lesionto the venous system and completely fills upfollowing injection.1
Management is usually conservative. But in thepresence of signs of optic nerve compression, surgicalremoval is attempted .Complete removal is usuallynot possible since the lesions are friable,unencapsulated and bleed easily. Embolization usingcoils through a distal vein is another method todiminish symptoms.13
Cavernous Hemangioma
Cavernous hemangioma is the most common benignorbital tumor in adults predominantly affectingmiddle aged females. Most frequently it develops inthe intraconal space though it may also developelsewhere in the orbit.15
The patients present with slowly progressiveunilateral axial proptosis which may be associatedwith decreased visual acuity, hyperopia, optic nervecompression, optic disc edema, choroidal folds andgaze-evoked amarousis, raised intraocular pressureand strabismus. Bilateral cavernous hemangiomashave also been reported.16,17
Imaging modality used commonly is a CT scanwhich shows a well defined intraconal mass withsmooth margins that enhances either homogenouslyor inhomogenously with intravenous contrast.Sometimes small areas of calcification are seen.18 OnMRI the lesion is isointense and hyper intense to themuscle on T1 and T2 weighted images respectively.With Gadolinium contrast, the lesion fills uphomogenously.19
Management is surgical excision Lateralorbitotomy is the most common approach if the lesionis intraconal. Anterior orbital approaches are usefulfor extraconal lesions. Surgical removal is muchsimpler, since cavernous hemangiomas are wellencapsulated. Cryo is a very useful adjunct. In verylarge lesions, passing a suture through the lesionhelps in two ways, for exsanguination of the tumorreducing its size and to hold the tumor.
Other Congenital Malformations
Many other congenital malformations commonlytermed as phakomatosis and include 'Sturge-WeberSyndrome', 'Wyburn-Mason Syndrome', 'Klippel-Trenaunay Syndrome', 'Osler-Weber-RenduSyndrome' and many more rare malformations.1
Sturge-Weber Syndrome: It is also called asencephalofacial angiomatosis and is a sporadicphakomatosis that involves the leptomeninges, brainand eyes. Struge-Weber is characterized by a naevusflammeus or port wine stain over the area oftrigeminal nerve distribution, ipsilateral lepto-meningeal hemangiomas and contralateral seizuresand hemiparesis. Ophthalmological features
basm
ala
blog
(alw
ays o
rigin
al)

Vascular Lesions of OrbitVascular Lesions of OrbitVascular Lesions of OrbitVascular Lesions of OrbitVascular Lesions of Orbit 153153153153153
include ipsilateral episcleral hemangiomas, glaucomasand diffuse choroidal hemangioma and homonymoushemianopia.
Diffuse choroidal hemangioma gives acharacteristic 'tomato-catsup' fundus.20 Imagingmodalities like CT and MRI are used. CT scanmay show 'tramline markings' of cerebralcalcification.
Management includes the use of Erbium laser fornaevus flammeus, external beam radiotherapy fordiffuse choroidal hemangiomas and medical controlof intraocular pressure followed by a combinedtrabeculotomy-trabeculectomy for glaucoma.21
Wyburn-Mason Syndrome: This is a rare A-Vmalformation of retina, optic nerve head andposterior fossa involving a direct communicationbetween arteries and veins without the interveningcapillary bed. Orbits are occasionally involved withipsilateral portwine pigmented naevi over thetrigeminal course.1 CT scans may show enlarged opticcanal and bony orbit with a poorly defined enhancingmass.22
Klippel-Trenaunay Syndrome: This raresyndrome encompasses cutaneous hemangiomas,venous varicosities and bony and soft tissuehypertrophy of usually a single limb. Rarely is theorbit involved with vascular anomalies.23
SHUNTS
Carotid-Cavernous Fistula
As obvious from the name, it is an abnormalcommunication between the carotid artery and thecavernous sinus. The blood in the cavernous sinusbecomes arterialized thereby raising the venouspressure and at the same time the arterial perfusionsuffers. The fistula can be classified as 'direct orindirect', 'high flow or low flow ' and 'spontaneousor traumatic'. Barrow standardized the classificationin 1985.24
Trauma is the most common cause of direct ortype A fistulas usually seen in basal skull fractures.Indirect or type C, D, E, are due to congenitalanomalies or spontaneous rupture of the artery
secondary to aneurysm, atherosclerosis and severehypertension.
Clinical features include classical triad ofconjunctival chemosis, pulsatile proptosis and bruit.Bruit is best heard as a flushing noise with the bellof the stethoscope, reduced by ipsilateral carotidcompression in the neck. Other features includeptosis; increased intraocular pressure due to elevatedepiscleral pressure;25 anterior segment ischemiahallmarked by corneal edema, ischemic pseudoiritis,rubeosis iridis and cataract; ophthalmoplegia, mostfrequently affecting the 6th cranial nerve due to itsintracavernous location; diplopia Fundus examinationreveals dilated veins, optic disc edema andintraretinal hemorrhages.
Imaging modalities used are CT scan, MRI andangiography. CT scan shows enlarged superiorophthalmic vein, enlarged extraocular muscles andenlargement of the cavernous sinus.26 The definitetest in selective internal or external carotidangiography which will demonstrate the fistula andits hemodynamics.
Carotid cavernous fistulas are managed byinterventional radiologists.Usually these patients arefirst seen by an ophthalmologist/orbital surgeon whomakes the diagnosis and refers to interventionalradiologist for management. Management indicationsinclude secondary glaucomas, ophthalmoplegia,severe proptosis and intolerable bruit.27 Balloon/coils or surgical occlusion of the fistula isrecommended for the Type A. Balloon/coil can beintroduced either by an arterial or a venous route.
Barrow's types of carotid-cavernous fistulas24
Barrow Origin Vessels InvolvedType
Type A Trauma Internal carotid
Type B Spontaneous Meningeal branches of internalcarotid
Type C Spontaneous Meningeal branches of externalcarotid
Type D Spontaneous Meningeal branches of internaland external carotids.
basm
ala
blog
(alw
ays o
rigin
al)

154154154154154 Surgical Atlas of Orbital DiseasesSurgical Atlas of Orbital DiseasesSurgical Atlas of Orbital DiseasesSurgical Atlas of Orbital DiseasesSurgical Atlas of Orbital Diseases
Type B and C can be treated with selectiveembolization of a single feeder vessel whereas TypeD requires embolization of all the multiple feederchannels. Various complications of interventionalradiology like vascular perforations, hemorrhage andpermanent neurological deficit have been reported.28
New GrowthsNew growths can be further subdivided into'Hamartomas' and 'Neoplasms'. The hamartomas areexemplified by cavernous hemangiomas whereasthe neoplasms include 'hemangiopericytoma','Angiosarcoma', 'Kaposi Sarcoma', 'angiomyomas',etc.1
Capillary HemangiomaCapillary hemangiomas are hamartomascharacterized by growth of blood vessels along withproliferation of endothelium. These are commonbenign primary tumors of the orbit in children. Itusually presents in the first or second week afterbirth and enlarges during the first year of life, afterwhich they begin to involute. About 70% regress by7 years of age.
Clinical presentation are in the form ofstrawberry naevus when the hemangioma involvesthe lid. Involvement of the conjunctiva is importantfrom diagnostic point of view. Within the orbitanterior and superior quadrant of the orbit is afavoured site. Orbital lesions may present with aprogressive non-pulsatile proptosis, which mayincrease following straining and crying.29 Capillaryhemangiomas have important systemic implicationslike high output failure, 'Kasabach-Meritt Syndrome'(Anemia + thrombocytopenia + low coagulantfactors)30 and 'Maffuci Syndrome' (Hemangiomas +enchondromatosis).
Imaging modalities used include CT scan, MRIand angiography.
CT scans demonstrates moderately well definedlesion with finger like projections that may be presentin any orbital space. There is a moderate to intenseenhancement on contrast. Gadolinium enhanced T1wieghted images with fat suppression shows diffusehomogenous or heterogenous enhancement. Multiplefeeder vessels are seen on angiography.
Treatment is indicated when vision is threatenedby amblyopia as a result of anisometropia, ptosis orstrabismus.
Intralesional injection of steroids is the mostfrequently used method. Usually 40-80 mg oftriamcinolone with 25 mg of methylprednisolone isdirectly injected into the lesion.1 AlternativelyTriamcinolone 40 mg along with betamethasone4 mg can also be used. The tumor usually begins toregress in two weeks but if necessary injection maybe repeated after about two months. Earlyrecognition and prompt treatment with intralesionalsteroid prevents early occlusion amblyopia, butfollow-up and management of refractive amblyopiawith glasses and patching is necessary in the longerterm. Potential complications include skindepigmentation, fat atrophy, eyelid necrosis andrarely central retinal artery occlusion.
Systemic steroids are indicated for extensivelesions especially if associated with visceralinvolvement. Recommended dosage used is 1.5 to2.5 mg/kg prednisolone daily over a few weeks withtitration downward depending on response.1
Though steroids are effective in large majorityof patients, a recurrence is not infrequent. Recurrentor resistant cases are being treated with recombinantinterferon alpha-2a and 2b with variable results.31
Recent studies have demonstrated good efficacy ofinterferons when given subcutaneously in a dose of3 million units/m2. During clinical follow-updiagnostic ultrasound evaluation ( the depthdimension) proved helpful. One report suggestedhigh efficacy of treatment when a combination ofinterferon alpha-2a with a low dose ofcyclophosphamide.
In the presence of very large platelet-consuminglesions as seen with Kasabach-Meririt syndrome,systemic antifibrinolytics like aminocaproic acid ortranexemic acid are used.30
Surgical resection is carried out in cases wherevision is threatened or there is a failure of medicalmanagement. Surgery should be carried out underhypotensive anesthesia with constant hemostasisduring removal.32
basm
ala
blog
(alw
ays o
rigin
al)

Vascular Lesions of OrbitVascular Lesions of OrbitVascular Lesions of OrbitVascular Lesions of OrbitVascular Lesions of Orbit 155155155155155
HemangiopericytomaThese are uncommon vascular tumors of the orbitoccurring in the middle ages. They are divided intobenign and malignant based upon the histopathology.Clinical features include progressive painlessproptosis of usually less than one year duration,predominantly in the superior part of orbit.Hemodynamically there is rapid circulation withsignificant shunting of blood. CT and MRI showswell defined lesions with homogenous contrastenhancement.33 The microscopic features includecellular, myxoid and storiform components withspindle shaped pericytes, which stain positively withvimentin upon immunohistochemistry.34
Management includes careful and completeexcision. The tumor has a pseudocapsule and isnotorious for recurrences. Histologically benigntumors have been reported to metastasize. A veryaggressive local behavior may warrant anexenteration.35
AngiosarcomaAngiosarcomas are malignant tumors of theendothelial origin, with an affinity for the head andneck regions. Mostly affects males in 6-8th decadesof life. They are ill defined, multiple, involving theskin of the lids and the orbit.36 They may presentwith orbital apex syndrome and other neurologicaldeficits37 Since these tumors are aggressive, a widesurgical excision is adviced.
Kaposi's SarcomaKaposi sarcoma has generated considerable researchafter the advent of AIDS.38 Though it is reported tobe common in the western literature, we are yet tosee a single case. Ocular involvement is usually ofthe skin, lids or conjunctiva as reddish or purplelesions and rarely lacrimal gland is involved.39
Histologically vascular slit channels lined byendothelium are seen.
Management includes the use of chemotherapyand extended field radiotherapy.
Hemangioendothelioma
These are very rare tumors of the orbit. It is knownto affect all age groups with no age or sexprelidiction. Multifocality is present in 9-14% of thecases.40
It presents as a very rapidly enlarging mass withedema or erythema of overlying skin. The tumor ishighly vascular and bleeds significantly on biopsy.Unlike rhabdomyosarcoma, it has a mass effect ratherthan being invasive. Imaging modalities used areCT and MRI, which demonstrates lytic, multi-loculated, expansile lesions of the orbit.Histopathologically the tumor is composed ofirregular vascular elements lined with immatureendothelial cells with prominent anaplasia. Allhemangioendotheliomas are positive for at least oneendothelial marker. (CD31, CD34, factor VIII ).Management includes histological grading followedby treatment with radiotherapy, chemotherapy andsurgical removal.41
Hemangioblastoma
Hemangioblastoma is a rare tumor of the orbit. Itpresents with progressive proptosis which can be axialand abaxial as hemangioblatomas have been reportedboth from the recti muscles42 and optic nerve.43 Opticnerve hemangioblastomas are frequently familial,presents with visual loss and RAPD and are associatedwith infratentorial hemangioblastomas, angiomatosisretinae, and cysts of the abdominal viscera. CTand Magnetic resonance imaging reveals a well-enhanced mass, with an enlargement of optic canalin cases of optic nerve lesions. Management includessurgical removal with appropriate orbitotomyapproaches.43
basm
ala
blog
(alw
ays o
rigin
al)

156156156156156 Surgical Atlas of Orbital DiseasesSurgical Atlas of Orbital DiseasesSurgical Atlas of Orbital DiseasesSurgical Atlas of Orbital DiseasesSurgical Atlas of Orbital Diseases
Orb
ital
Vas
cula
r L
esio
ns
at a
Gla
nce
Nam
e of
the
lesi
onAg
eC
linic
al fe
atur
esIm
agin
g m
odal
ities
Man
agem
ent
Lym
phan
giom
aEa
rlyPr
ogre
ssiv
e pr
opto
sis
that
incr
ease
s w
ithU
SG, C
T an
d M
RI.
MR
I is m
odal
ity o
fC
onse
rvat
ive, S
clero
sing
agen
ts,
child
hood
uppe
r res
pira
tory
infe
ctio
ns, s
udde
n pr
op-
choi
ce a
s it
delin
eate
s th
e le
ison
wel
lSu
rgic
al w
ith a
djun
ctiv
e la
sers
tosi
s w
ith o
r with
out o
ptic
ner
ve c
ompr
essi
onan
d al
so h
elps
in ti
min
g th
e ch
ocol
ate
due
to b
leed
ing
into
the
lum
en (c
hoco
late
cys
t)cy
st
Orb
ital v
aric
esch
ildho
od to
Non
-pul
astil
e, re
vers
ible
pro
ptos
is, i
ncre
ases
CT,
Dop
pler
USG
and
ang
iogr
aphy
.C
onse
rvat
ive,
Em
boliz
atio
nm
iddl
e ag
ew
ith v
alsa
lva
man
euve
rPh
lebo
liths
may
be
obse
rved
on
CT
Surg
ical
rem
oval
Cav
erno
usM
iddl
e ag
esSl
owly
pro
gres
sive
uni
late
ral a
xial
pro
ptos
is,
CT
and
MR
I. W
ell d
efin
ed in
traco
nal
Surg
ical
exc
isio
n w
ith a
late
ral
hem
angi
oma
decr
ease
d vi
sion
, hyp
erop
ia, o
ptic
ner
ve c
om-
mas
s w
ith s
moo
th m
argi
ns a
ndor
bito
tom
y ap
proa
chpr
essi
on, c
horo
idal
fold
s an
d ga
ze e
voke
den
hanc
emen
t with
con
trast
amar
aosi
s
Car
otid
-Cav
erno
usVa
riabl
eC
onju
nctiv
al c
hem
osis
, pul
satil
e pr
opto
sis
with
CT,
MR
I and
ang
iogr
aphy
. Enl
arge
dIn
terv
entio
nal r
adio
logy
Bal
loon
fistu
laa
brui
t, an
terio
r seg
men
t isch
emia
and
gla
ucom
asu
perio
r oph
thal
mic
vei
n is
a fe
atur
e.or
coi
l em
boliz
atio
nD
efin
ite te
st is
ang
iogr
aphy
Cap
illary
hem
angi
oma
Ist y
ear o
fSt
raw
berry
nev
us o
n lid
s an
d co
njun
ctiv
a. N
on-
CT,
MR
I and
ang
iogr
aphy
. Fin
ger l
ike
Topi
cal, i
ntra
lesio
nal a
nd sy
stem
iclif
epu
lsat
ile p
ropt
osis
that
incr
ease
with
val
salv
apr
ojec
tions
into
the
orbi
t with
mod
erat
est
eroi
ds. I
nter
fero
ns a
nd c
yclo
-m
aneu
ver. A
dditi
onal
feat
ures
of a
ssoc
iate
dto
inte
nse
enha
ncem
ent o
n co
ntra
stph
osph
amid
e. S
urgi
cal e
xcis
ion
Kasa
back
-Mer
itt a
nd M
afuc
ci s
yndr
omes
Hem
angi
oper
icyto
ma
Mid
dle
ages
Pain
less
, pro
gres
sive
ecc
entri
c pr
opto
sis
CT
and
MR
I sho
ws
wel
l def
ined
lesi
ons
Car
eful
exc
isio
n. A
ggre
ssiv
eof
less
than
a y
ear d
urat
ion
with
hom
ogen
ous
cont
rast
enh
ance
men
ttu
mor
s re
quire
exe
nter
atio
n
basm
ala
blog
(alw
ays o
rigin
al)
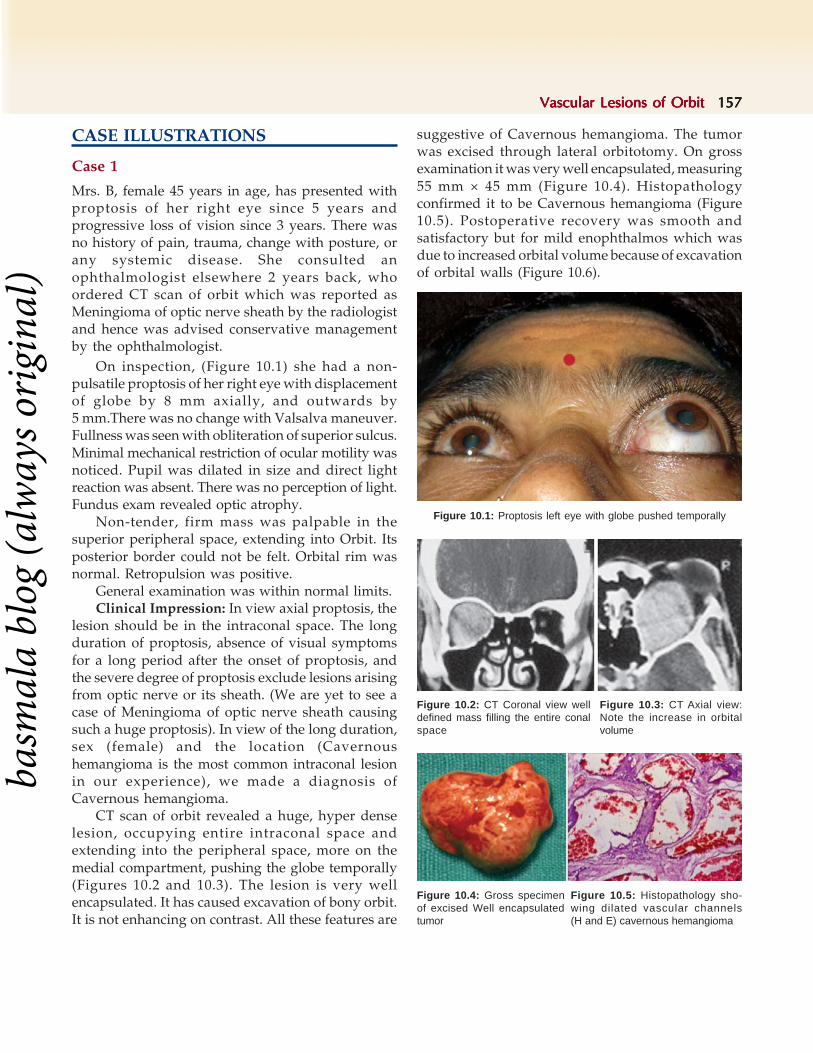
Vascular Lesions of OrbitVascular Lesions of OrbitVascular Lesions of OrbitVascular Lesions of OrbitVascular Lesions of Orbit 157157157157157
CASE ILLUSTRATIONS
Case 1
Mrs. B, female 45 years in age, has presented withproptosis of her right eye since 5 years andprogressive loss of vision since 3 years. There wasno history of pain, trauma, change with posture, orany systemic disease. She consulted anophthalmologist elsewhere 2 years back, whoordered CT scan of orbit which was reported asMeningioma of optic nerve sheath by the radiologistand hence was advised conservative managementby the ophthalmologist.
On inspection, (Figure 10.1) she had a non-pulsatile proptosis of her right eye with displacementof globe by 8 mm axially, and outwards by5 mm.There was no change with Valsalva maneuver.Fullness was seen with obliteration of superior sulcus.Minimal mechanical restriction of ocular motility wasnoticed. Pupil was dilated in size and direct lightreaction was absent. There was no perception of light.Fundus exam revealed optic atrophy.
Non-tender, firm mass was palpable in thesuperior peripheral space, extending into Orbit. Itsposterior border could not be felt. Orbital rim wasnormal. Retropulsion was positive.
General examination was within normal limits.Clinical Impression: In view axial proptosis, the
lesion should be in the intraconal space. The longduration of proptosis, absence of visual symptomsfor a long period after the onset of proptosis, andthe severe degree of proptosis exclude lesions arisingfrom optic nerve or its sheath. (We are yet to see acase of Meningioma of optic nerve sheath causingsuch a huge proptosis). In view of the long duration,sex (female) and the location (Cavernoushemangioma is the most common intraconal lesionin our experience), we made a diagnosis ofCavernous hemangioma.
CT scan of orbit revealed a huge, hyper denselesion, occupying entire intraconal space andextending into the peripheral space, more on themedial compartment, pushing the globe temporally(Figures 10.2 and 10.3). The lesion is very wellencapsulated. It has caused excavation of bony orbit.It is not enhancing on contrast. All these features are
suggestive of Cavernous hemangioma. The tumorwas excised through lateral orbitotomy. On grossexamination it was very well encapsulated, measuring55 mm × 45 mm (Figure 10.4). Histopathologyconfirmed it to be Cavernous hemangioma (Figure10.5). Postoperative recovery was smooth andsatisfactory but for mild enophthalmos which wasdue to increased orbital volume because of excavationof orbital walls (Figure 10.6).
Figure 10.2: CT Coronal view welldefined mass filling the entire conalspace
Figure 10.3: CT Axial view:Note the increase in orbitalvolume
Figure 10.4: Gross specimenof excised Well encapsulatedtumor
Figure 10.5: Histopathology sho-wing dilated vascular channels(H and E) cavernous hemangioma
Figure 10.1: Proptosis left eye with globe pushed temporally
basm
ala
blog
(alw
ays o
rigin
al)

158158158158158 Surgical Atlas of Orbital DiseasesSurgical Atlas of Orbital DiseasesSurgical Atlas of Orbital DiseasesSurgical Atlas of Orbital DiseasesSurgical Atlas of Orbital Diseases
Case 2
Mr. K, male, 32 years of age presented to us withpainless progressive proptosis of right eye since 3years. There was no history of defective vision, ordiplopia.
On examination (Figure 10.7) we noticed eccentricproptosis of the right eye, with fullness inferiorly.The proptosis was nonpulsatile. Ocular motility wasnormal. Pupil was normal. There was no RAPD.Vision was 20/20 and color vision was normal. CTscan showed a well defined lesion in the inferiorperipheral space with minimal contrast enhancementand bony excavation of the floor of the orbit(Figures 10.8 and 10.9), suggestive of Cavernoushemangioma.
Anterior inferior orbitotomy was performedthrough subciliary approach, and the tumor wasexsanguinated by passing a suture through thesubstance of it to shrink its size (Figure 10.10).This suture also helps in applying traction to assistthe excision of the tumor through a smallerincision .
The excised tumor was pinkish in color and wasvery well encapsulated. (Figure 10.11) The cut-sectionof the tumor (Figure 10.12) showed honey-comb likeappearance with blood oozing out from the entirecut surface. On histological examination theencapsulated mass was made-up of dilated vascularchannels, filled with blood (Figure 10.13), confirmingthe clinical diagnosis of Cavernous hemangioma. Thepatient recovered well (Figure 10.14). The proptosisdisappeared completely. His vision remained 20/20.The ocular motility was full.
Figure 10.6: Postoperative picture showing relief from proptosis
Figure 10.13: Dilated vascularchannels filled with blood
Figure 10.12: Cut section showinghoneycomb appearance with bloodoozing from it
Figure 10.10: Suture throughexsanguinated and shrinks Aidsexcision by traction
Figure 10.11: Well encapsulatedtumor
Figure 10.8: CT scan shows welldefined lesion in inferior space
Figure 10.9: CT scan well def-ined lesion with bony excavation
Figure 10.7: Eccentric proptosis with inferior fullness
basm
ala
blog
(alw
ays o
rigin
al)

Vascular Lesions of OrbitVascular Lesions of OrbitVascular Lesions of OrbitVascular Lesions of OrbitVascular Lesions of Orbit 159159159159159
There was no recurrence of the tumor. The pointsto consider in this case were the location of cavernoushemangioma in the inferior peripheral space, thepassing of suture through the hemangioma to bleedthe tumor and shrink its size, which facilitates toremove the tumor through a smaller incision. Cryois other wise an excellent tool to hold the tumorduring its dissection and removal.
Case 3
Mrs. J, a female 28 years of age, presented withhistory that her friends and family members werecommenting that her right eye was looking prominentsince 3 months (Figure 10.15). She had no pain anddid not complain of any visual disturbances. Pasthistory was significant in that she had convulsions 4years back and CT scan of brain showed 2 calcifiedlesions (Figure 10.16). She was on carbamazepine(Tegretol) since then. There was no relapse ofconvulsions. On clinical evaluation, she had 3 mm ofaxial and nonpulsatile proptosis, which did notincrease with Val-salva maneuver. The ocular motilitywas normal. The pupils were brisk and the visionwas 20/20. CT scan of orbit revealed a hyper-dense,contrast enhancing lesion of size 15 × 12 mm in theintraconal space (Figures 10.17A and B). In view ofthe short duration and contrast enhancement,provisional diagnosis of a vascular tumor likehemangioendothelioma/hemangiopericytoma wasconsidered. Lateral orbitotomy was performed andthe tumor was excised. Histopathology and Immuno-histochemistry revealed it to be hemangioblastoma.Further evaluation of the patient did not show any
other lesions in the posterior segment of the globes,brain or elsewhere. The calcified lesions are probablyintracranial hemangioblastoma and since they wereinactive, neurosurgeon did not contemplate excision.The patient has no recurrence during the past 3 yearsof follow-up (Figure 10.18).
Case 4
Miss P, female child of 6 years presented with acuteproptosis of 2 weeks duration associated with severepain and defective vision. There was no history oftrauma.She never had similar problem previously.
On examination she had a non-pulsatile, proptosisof 7 mm, associated with severe periocular fullness,chemosis grade III associated with subconjunctival
Figure 10.15: Axial proptosisof right eye
Figure 10.16: CT scan of brainshowing calcified lesions
Figures 10.17A and B: Axial and Coronal sections of CT orbit showingwell encapsulated Intraconal lesion with contrast enhancement
A B
Figure 10.18: Postoperative status showing complete recovery
Figure 10.14: One week postop, recovery from proptosis
basm
ala
blog
(alw
ays o
rigin
al)

160160160160160 Surgical Atlas of Orbital DiseasesSurgical Atlas of Orbital DiseasesSurgical Atlas of Orbital DiseasesSurgical Atlas of Orbital DiseasesSurgical Atlas of Orbital Diseases
hemorrhage, and restricted ocular motility in allgazes .Pupil was dilated. RAPD was present. Herbest corrected vision was 20/200. Retropulsion waspositive. Tenderness was present on palpation(Figure 10.19).
In view of acute onset associated with pain,chemosis, restricted motility, subconjunctivalhemorrhage and chemosis, in a child, Lymphangiomawas the clinical diagnosis. CT scan showed a contrastenhancing lesion with a huge hemorrhage in thelesion, supporting the clinical diagnosis (Figure10.20). Normally lymphangioma is managedconservatively since it is not possible to excise itcompletely and hence recurrence is very common.But in this child as the vision is being compromised,the parents were informed that though recurrence isvery common, surgery was to be performed to savevision. Antero-lateral orbitotomy was performed.About 6 cc of blood was aspirated from the lesion toshrink it and excised as much as possible (Figure10.21). The histopathology confirmed the diagnosisof lymphangioma (Figure 10.22). Postoperativerecovery was smooth and the vision improved to20/20 (Figure 10.23). After 3 years, she had a
recurrence which was surgically managed. There wasno recurrence in the 2 year postoperative follow-upafter second surgery.
REFERENCES
1. Rootman J: Diseases of the orbit; A multidisciplinaryapproach. Lippincott Williams and Wilkins, 2nd Edition:455-506.
2. Harris GJ Orbital vascular malformations: a consensusstatement on terminology and it clinical implications. Orbitalsociety. Am J Ophthalmol. 1999; 127:453-55.
3. Rootman J, Hay E, Graeb D, et al. Orbital adenexallymphangiomas. A spectrum of hemodynamically isolatedvascular hamartomas. Ophthalmology. 1986; 93:1558-70.
4. Pang P, Jakobiec FA, Iwamoto T, Hornblass A Smalllymphangiomas of the eyelids. Ophthalmology 1984;91:1278-84.
5. Kazim M, Kennerdell JS, Rothfus W, et al. Orbitallymphangioma: correlation of magnetic resonance imagesand intraoperative findings. Ophthalmology. 1992; 99:1588-94.
6. Harris GJ, Sakol PJ, Bonavolontu G, et al. An analysis of 30cases of orbital lymphangiomas: pathophysiologicalconsiderations and management recommendations.Ophthalmology. 1990; 97:1583-91.
7. C Luzzatto, P Midrio, Z Tchaprassian, M Guglielmi:Sclerosing treatment of lymphangiomas with OK-432. ArchDis Child 2000;82:316-318.
8. CM Giguere, NM Bauman, Y Sato, DK Burke, JH Greinwald,S Pransky, P Kelley, K Georgeson, and RJH Smith Treatmentof Lymphangiomas With OK-432 (Picibanil) Sclerotherapy:A Prospective Multi-institutional Trial Arch OtolaryngolHead Neck Surg, October 1, 2002; 128(10): 1137-44.
9. JP Deveikis. Percutaneous Ethanol Sclerotherapy forVascular Malformations in the Head and Neck Arch FacialPlast Surg, September 1, 2005; 7(5): 322-5.
Figure 10.19: Acute proptosiswith severe chemosis andperiocular swelling
Figure 10.20: CT scan of orbitshowing large cystic lesion inintraconal space extending tomedial peripheral space, andhemorrhage within
Figure 10.21: Blood beingdrawn from the lesionintraoperatively
Figure 10.22: Histopathologyshowing channels filled with lymph
Figure 10.23: Postoperative status. Proptosisdisappeared vision improved to 20/20
basm
ala
blog
(alw
ays o
rigin
al)

Vascular Lesions of OrbitVascular Lesions of OrbitVascular Lesions of OrbitVascular Lesions of OrbitVascular Lesions of Orbit 161161161161161
10. Mathur NN, Rana I, Bothra R, Dhawan R, Kathuria G,Pradhan T Bleomycin sclerotherapy in congenital lymphaticand vascular malformations of head and neck. Int J PediatrOtorhinolaryngol. 2005;69(1):75-80.
11. Schwarcz RM, Ben Simon GJ, Cook T, Goldberg RASclerosing therapy as first line treatment for low flowvascular lesions of the orbit. Am J Ophthalmol.2006;141(2):333-9.
12. Wojno TH Sotradecol (sodium tetradecyl sulfate) injectionof orbital. Lymphangioma. Ophthal Plast Reconstr Surg.1999;15(6):432-7.
13. Wright JE, Sullivan TJ, Garner A, et al. Orbital venousanomalies. Ophthalmology. 1997; 104:905-13.
14. Cline RA, Rootman J. Enophthalmos: a clinical review.Ophthalmology. 1984; 91:229-37.
15. Harris GJ, Jakobiec FA. Cavernous hemangioma of theorbit: A clincopathological analysis of sixty-six cases. In:Ocular and adnexal tumors. Birmingham, AL: Aesculapius,1978:741-81.
16. Fries PD, Char DH. Bilateral orbital cavernoushemangiomas. Br J Ophthalmol 1988; 72:871-3.
17. Sullivan TJ, Aylward GW, Wright JE, et al. Bilateral multipleCavernous hemangiomas of the orbit. Br J Ophthalmol.1992; 76:627-9.
18. Forbes GS, Sheedy PF, Waller RR. Orbital tumors evaluatedby Computer tomography. Radiology 1980;136:101-11.
19. Ohtsuka K, Hashimoto M, Akiba H. Serial dynamicmagnetic resonance imaging of orbital cavernoushemangioma. Am J Ophthalmol. 1997; 123:396-8.
20. Susac JO, Smith JL, Scelfo RJ The "tomato catsup" fundus inSturge-Weber syndrome. J Pediatr Ophthalmol Strabismus.1974; 92:69-70.
21. Phelps CD The pathogenesis of glaucoma in Struge-WeberSyndrome. Ophthalmology. 1978; 85:276-86.
22. Kim J, Kim OH, Suh JH, Lew HM Wyburn-Masonsyndrome: An unusual presentation of bilateral orbital andunilateral brain A-V malformations. Pediatr Radiol. 1998;28:161.
23. Good WV, Hoyt CS Optic nerve shadow enlargement inKlippel. Trenaunay-Weber syndrome. J Pediatr OphthalmolStrabismus. 1989; 26:288-9.
24. Barrow DL, Spector RH, Braun IF, et al. Classification andTreatment of spontaneous carotid-cavernous sinus fistulas.J Neurosurg 1985; 62:248-56.
25. Talusan ED, Fishbein SL, Shwartz B Increased pressure ofdilated episcleral veins with open angle glaucoma withoutexophthalmos. Ophthalmology. 1983; 90:257-65.
26. Vinuela F, Fox AJ, Debrun GM, et al. Spontaneous carotid-cavernous fistulas: clinical, radiological and therapeuticconsiderations. J Neurosurg. 184; 60:976-84.
27. Debrun GM, Vinuela F, Fox AJ, et al. Indications fortreatment and classification of 132 carotid-cavernousfistulas. Neurosurg. 1988; 22:285-9.
28. Lasjaunias P, Chiu M, Ter Brugge K, et al. Neurologicalmanifestations of intracranial dural arterio-venousmalformations. J Neurosurg 1986; 64:724-30.
29. Haik BG, Jakobiec FA, Ellsworth RM, Jones IS. Capillaryhemangioma of the lids and orbit: an analysis of the clinicalfeatures and therapeutic results in 101 cases. Ophthalmology1979; 86:760-92.
30. Neidhart JA, Roach RW. Successful treatment of skeletalhemangioma and Kasabach-Merritt syndrome withaminocaproic acid. Am J Med 1982; 73: 434-8.
31. Teske S, Ohlrich SJ, Gole G, et al. Treatment of orbitalcapillary hemangioma with interferon. Aust N Z JOphthalmol 1994; 22: 13-7.
32. Walker RS, Custer PL, Nerad JA. Surgical excision ofperiorbital capillary hemangiomas. Ophthalmology 1994;101:1333-40.
33. Kikuchi K, Kowada M, Sageshima M Orbitalhemangiopericytoma: CT MRI and angiographic findings.Comput Med Imaging Graph. 1994;18:217-22.
34. Croxatto JO, Font RL. Hemangiopericytoma of the orbit:A clinico-pathological study of 30 cases. Hum Pathol 1982;12:210-18.
35. Sullivan TJ, Wright JE, Wulc AE, et al. Hemangiopericytomaof the orbit. Aust N Z J Ophthalmol . 1992; 20:325-32.
36. Maddox JC, Evans HL. Angiosarcoma of skin and soft tissue:a Study of forty-four cases. Cancer 1981;48:1907-21.
37. Messmer EP, Font RL, McCary JA, Murphy D. Epithelioidangio-sarcoma of the orbit presenting as Tolosa-Huntsyndrome. A clinicopathological case report with reviewof literature. Ophthalmology 1983; 90:1414-21.
38. Holland GN, Gottlieb MS, Yee RD, et al. Ocular disordersassociated with a new severe acquired cellularimmunodeficiency syndrome. Am J Ophthalmol. 1982;93:393-402.
39. Kalinske M, Leone CR Jr Kaposi's sarcoma involving theeyelid and conjunctiva. Ann Ophthalmol. 1982; 14:497-9.
40. Arie R, Aylon YG, Don R Hemangioendothelioma of theorbit. Intl J Pediatric Otorhinolaryngology. 2006;1:188-91.
41. Lyon DB, Tang TT, Kidder TM Hemangioendothelioma ofthe orbital bone. Ophthalmol 1992. 99:1773-98.
42. Cockerham KP, Sachs DM, Cockerham GC, Hidayat AA,Brown HG Orbital hemangioblastoma arising in a rectusmuscle. Ophthal Plast Reconstr Surg. 2003 May;19(3):248-50.
43. Hotta H, Uede T, Morimoto S, Tanabe S, Hashi K, TakedaM. Optic nerve hemangioblastoma. Neurol Med Chir(Tokyo). 1989;29(10):948-52.
basm
ala
blog
(alw
ays o
rigin
al)

162162162162162 Surgical Atlas of Orbital DiseasesSurgical Atlas of Orbital DiseasesSurgical Atlas of Orbital DiseasesSurgical Atlas of Orbital DiseasesSurgical Atlas of Orbital Diseases
Christopher M Knapp, Ram Vaidhyanath, Laurence Brown, Raghavan Sampath
Orbital Tumors ofOrbital Tumors ofOrbital Tumors ofOrbital Tumors ofOrbital Tumors ofNeurological OriginNeurological OriginNeurological OriginNeurological OriginNeurological Origin
Optic Nerve Glioma
The first clinical report of optic nerve tumors wasby Antonio Scarpa in 1816, however it wasn't until1912 that Hudson described optic nerve gliomas andoptic meningiomas as separate lesions.1 These tumorsare relatively rare, accounting for less than 4% of allorbital tumors. Overall optic nerve gliomas accountfor 65%1,2 of optic nerve tumors and meningiomas35%.1 Optic nerve gliomas appear to be morefrequent in females, whereas for optic pathwaygliomas, there may be an equal sex distribution.2
Lesions typically become symptomatic in childhood.3
The mean age of presentation is 8.8 years with only10% presenting after 19 years of age.2 Most lesionsare sporadic although there is an association withneurofibromatosis (NF 1). Adult optic nerve gliomasmay behave like those presenting in childhood,3
however some may show an aggressive behavior,being clinically distinct from those seen in childhood.These patients are typically middle aged with a slightmale bias.3
Benign optic nerve gliomas are typically pilocyticastrocytomas originating from astrocytic glia and caninvolve the visual pathways anywhere from the opticnerve to the visual cortex.1,4 Histologically they arecomposed of delicate, hair-like elongated eosinophiliccells in an interwoven pattern. The nuclei may beround or oval. Mitoses are rare, but nuclear atypiamay be observed. Malignant change is very rare.The proliferating astrocytes in an optic gliomamay be associated with worm-like denselyeosiniophilic bodies, known as Rosenthal fibers,surrounded by hyalinized connective tissue, a
distinctive (but not diagnostic) feature of pilocyticastrocytomas.5 Orbital gliomas, particularly inpatients suffering from NF 1, can extend throughthe pia and arachnoid matter in to the subdural space.They tend to remain intradural, however whenincompletely excised can recur diffusely invadingadjacent orbital structures. Where the lesion hasspread to the subarachnoid space reactiveproliferation of fibrovascular and meningeothelialtissue can occur resulting in arachnoid hyperplasia,which can resemble an optic nerve sheathmeningioma.1 Two patterns of growth are identified,perineural (circumferential growth) and intraneuralgrowth. Perineural growth results from proliferatingastrocytes and fibrovascular tissue within the duralsheath, widening the epipial-subdural space andsubsequently compressing the optic nerve. Intra-neural growth results from growth of intra-axialastrocytes causing the subarachnoid space to beobliterated. Perineural growth appears to occur inpatients with NF1.1 Enlargement of optic gliomasoccurs by a combination of neoplastic cellproliferation, reactive arachnoid proliferation andaccumulation of PAS positive mucinous substance.Rapid growth can result from cystic degenerationor intra-lesional hemorrhage. Malignant change canoccur however this is extremely rare.1
Malignant optic nerve gliomas seen in adultsshow evidence of malignant astrocytomas and arethought to originate within the optic pathways.Extension is usually subpial along the optic pathwaysalthough can directly invade the substance of thebrain.1
11C H A P T E R
basm
ala
blog
(alw
ays o
rigin
al)

Orbital Tumors of Neurological OriginOrbital Tumors of Neurological OriginOrbital Tumors of Neurological OriginOrbital Tumors of Neurological OriginOrbital Tumors of Neurological Origin 163163163163163
Approximately 30-50% of benign optic gliomasare associated with neurofibromatosis type 1(NF 1)2, 4, the rest occur sporadically. The incidenceof optic nerve glioma in patients with NF 1 is 15-20%of which only about 20% have visual symptoms.1, 4
The presenting symptoms depend very much onthe location of the lesion. Those involvingpredominantly the intraorbital optic nerve presentwith proptosis, ocular motility abnormalities, visionloss and visual field loss. Intracranial tumorsincluding those involving the chiasm, tend to havereduced vision and endocrine abnormalitiesincluding precocious puberty.1-4 Fundoscopy mayreveal either optic atrophy or papilloedemadepending on the location of the lesion. Optocilliaryshunt vessels, central retinal vein occlusion andvenous stastis retinopathy are occasionally seen.1,3
Hemorrhage in to the tumor can result in acuteproptosis and sudden loss of vision.3
Investigation of optic nerve gliomas involvescomputerized tomography (CT) and magneticresonance imaging (MRI). The appearance of thelesion depends on whether the patient has NF 1 ornot. Fusiform swelling of the optic nerve is typicallyseen in patients without NF 1, whereas those withNF 1 tend to have more irregular nerves with areasof kinking or buckling.3 Cystic spaces mayoccasionally be seen representing mucinousaccumulations. With perineural growth patterns,there may be thickening of the dura with preservationof the compressed optic nerve, mimicking the tram-tracking seen in optic nerve sheath meningiomas.Calcification is a rare finding.1 MRI shows the lesionsto be hypointense on T1 weighted images, whereason T2 images the glioma tends to be hyperintense.3
Contrast enhancement and fat suppression techniquecan help to differentiate optic nerve meningiomasfrom gliomas, since arachnoid hyperplasia associatedwith gliomas does not enhance with gadolinium.1
Treatment options depend very much on thelocation and extent of the lesion. Most optic nervegliomas have an indolent growth pattern and canremain stable for many years, with somespontaneously regressing.1, 3 Those lesions confinedto the optic nerve show a mortality rate of 5% fromintracranial extension. Tumor resection is curative
whilst the lesion remains confined to the optic nerve.Lesions involving the chiasm have a mortality rateof approximately 28% from intracranial spread, whilsthypothalamic or 3rd ventricle involvement increasesthe mortality rate to more than 50% at 15 years.1
Patients with isolated optic nerve involvement andgood vision should be reviewed on regularly withrepeat serial MRI scans of the optic nerve. When thereare signs of posterior progression the lesion shouldbe excised en block.1 Those lesions confined to theoptic nerve in blind, painful or cosmeticallyunacceptable eyes should be considered for surgicalexcision.1,3,4 Optic nerve lesions extending to thechiasm or those primarily involving the chiasm oroptic tracks could be considered for chemotherapyor radiotherapy. Children 5-7 years and youngershould be treated with chemotherapy2,4 sinceradiotherapy at this age may result in damage to theendocrine system and affect the future intellectualdevelopment of the child.1,4 Children aged 10 andabove may be considered for radiotherapy usingvarious delivery techniques. Doses typically givenare in the range of 45 to 56 Gy given in 180cGyfractions.
Malignant glioma seen in adults is invariablyfatal.1 Neuro-imaging of an involved optic nerve isnon-specific and the condition shows a rapid rate ofprogression. Lesions affecting the proximal part ofthe optic nerve can progress to affect both eyes within5-6 weeks.3
Optic Nerve Meningioma
Optic nerve meningiomas account for one third ofprimary optic nerve tumors and were first identifiedas a pathological entity in 1835 by Jean Cruveilheir.It wasn't until 1912 that Hudson clearly differentiatedoptic nerve gliomas from meningiomas.6 Mostmeningiomas involving the orbit are extensions fromintracranial sites such as the sphenoidal wing(secondary optic nerve sheath meningiomas).Primary optic nerve meningiomas originate from thecap cells of the arachnoid surrounding the intraorbitalor intracanalicular portion of the optic nerve.3 Thetypical age at presentation is 40 years of age6,7 withbilateral cases presenting much earlier atapproximately 13 years of age.6 There is a small sexbias with 61% of cases occurring in females.6
basm
ala
blog
(alw
ays o
rigin
al)

164164164164164 Surgical Atlas of Orbital DiseasesSurgical Atlas of Orbital DiseasesSurgical Atlas of Orbital DiseasesSurgical Atlas of Orbital DiseasesSurgical Atlas of Orbital Diseases
Histologically most orbital meningiomas are ofthe meningiothelial or syncytial variety. The cells areeosinophilic with abundant cytoplasm and indistinctcell margins. The nuclei are small and vesicular withoccasional pseudoinclusions. Cells may be wrappedwith or without psammoma bodies in tight whorls.5
Approximately 90% of meningiomas involving theorbit originate from intracranial sites, primarily theolfactory groove and the sphenoidal ridge.6 Ectopiclesions have been described in the orbit, seeminglyindependent of the optic nerve, these may havedeveloped from orbital mesenchymal cells or maybe a case of mistaken identity, since lesions such asfibroxanthomas and hemangiopericytomas closelyresemble meningiomas.6
NF 1 is associated with optic nerve meningioma,although the relationship is no where near as high asfor optic nerve glioma. The incidence of NF 1 inpatients with optic nerve meningioma is 2%, whereasthe incidence of NF 1 in the general population is0.03-0.05%.6
The classical triad of clinical findings in opticnerve meningioma are visual loss, optic atrophy andoptociliary shunt vessels.3,6 The simultaneousoccurrence of these three findings is however rare.The most common finding is vision loss which cantake the form of visual obscurations. Other findingsare reduced color vision and visual field defects.3,6
Proptosis seems to follow the onset of visual loss,tending to be reasonably mild.3,7 It is thought to occurbecause tumor growth results in a straightening ofthe optic nerve and may also account for any ocularmotility defects with up gaze being most commonlyaffected.6,7 Orbital pain may occur. Examination mayreveal disc swelling although the only signs may beoptic atrophy. Optociliary shunts which present inless than one third of patients3,7 are shunts betweenthe retinal and choroidal circulations and thought tobe a result of a reopening of regressed vestigialembryonic retinociliary anastomoses.6 They may beseen in eyes with other causes of disc swelling. Thedisc swelling and central retinal vein congestion mayproceed the shunt vessels by 1-2 years becomingnoticeable as the swelling starts to resolve3 and thenregress as optic atrophy sets in.6
Meningiomas arise from meningothelial cellsalong the meninges. Large collections are known as
pachionian bodies or arachnoid bodies whereassmaller ones are known as arachnoid villi. Opticnerve meningiomas are thought to arise frommeningiothelial cap cells of the arachnoid villi.6 Twopatterns of growth are seen, a syncytial pattern inwhich polygonal cells are arranged in sheetsseparated by vascular trabeculae and a transitionalpattern where spindle cells are arranged in concentricwhorls. Mitoses are uncommon. Psammoma bodiesare occasionally seen in which calcium salts can bedeposited. Meningiomas may spread in thesubarachnoid spaces along paths of least resistance.They can extend in to the surrounding tissues3 andthe haversian canal system of bone resulting inhyperosteosis. They do not seem to invade the brainand are not associated with raised intracranialpressure or pituitary dysfunction.6 Growth is slowalthough may accelerate with pregnancy and resultsin compression of the optic nerve.6
Investigation involves CT and MRI imaging.Calcification when present is useful in distinguishingoptic nerve gliomas from meningiomas. Typically thelesions show 'tram-tracking' in which a thickenedoptic nerve sheath surrounds a central lucent opticnerve.3,6,7 On coronal views this is seen as a densering surrounding the central optic nerve.6 MRI withgadolinium enhancement is particularly sensitive indetecting meningiomas.7
Treatment options include surgery andradiotherapy, however observation is not un-reasonable since the mortality rate is low.7 Surgerymay be indicated for aggressive lesions however itis associated with a high degree of local recurrenceand orbital invasion. Typically surgical excisionresults in blindness, since the tumor and optic nerveoften share their blood supply.6,7 Decompression ofthe nerve has been attempted by opening the duralsheath, which in some cases can arrest the visualdeterioration.3,6 Fractionated radiotherapy with atotal of 40-54Gy given in divided doses seems to beeffective in stabilizing and in some cases improvevision, whilst at the same time limiting the risks ofoptic nerve or chiasm damage to less than 5%.3,7,8
Interestingly the tumor volume appears unchangedfollowing radiotherapy, despite an improvement inneurological function.8 The side effects of treatmentincluding headache, nausea and hair loss can be
basm
ala
blog
(alw
ays o
rigin
al)

Orbital Tumors of Neurological OriginOrbital Tumors of Neurological OriginOrbital Tumors of Neurological OriginOrbital Tumors of Neurological OriginOrbital Tumors of Neurological Origin 165165165165165
limited by fractionating the doses. Later side effectsinclude pituitary dysfunction, retinopathy, iritis andtemporal lobe atrophy.8 The risk of optic nerve orchiasm damage associated with high doses ofradiotherapy. When doses greater than 59Gy aregiven in fractions of less than 1.9Gy there is an 11%risk of injury whilst doses greater than 1.9Gy have a47% risk according to a University of Florida study.9
Low dose steroids at the time of radiotherapy maylimit damage from radiation induced peritumoredema.8 The risk of a second malignancy followingradiotherapy is 0-2% at 10-20 years.8 When a lesionis treated with a single dose of radiation thethreshold for injury is 8-10 Gy.8
Orbital Schwannoma (Neurilemmoma) andNeurofibroma
Schwannomas also known as neurilemmomasaccount for approximately 1-4% of orbital tumors,occurring most commonly in men between the secondand fifth decades.10,11 They occasionally arise fromthe optic nerve, probably originating from schwanncells of sympathetic nerves tightly adherent to theoptic nerve.3 More frequent sites are the other cranialnerves including the oculomotor, lacrimal, trigeminaland zygomaticotemporal nerves.10,11 The mostcommonly affected cranial nerve is the vestibularnerve.12
Schwannomas are slow growing lesions that donot invade surrounding tissues.11 Clinical featuresinclude proptosis and diplopia. Globe compressioncan induce a hypermetropic shift, whilst optic nervecompression results in reduced visual acuity.Malignant transformation is rare.10
Gross examination reveals a well encapsulatedyellowish grey lesion, with cysts containing clearfluid. Histologically schwannomas show two growthpatterns: Antoni A where densely packed spindle-shaped cells are arranged with palisaded nucleisometimes forming Verocay bodies, and Antoni Bwhere cells are separated by an abundant myxoidstroma with no alignment of nuclei. Mitoses areusually absent. The associated nerve may sometimesbe seen in one side of the lesion, in contrast to aneurofibroma where the originating nerve isexpanded by the lesion and cannot be seen. So-called"ancient schwannomas" may feature bizarre enlargedor multiple nuclei, but there are no malignant
connotations.10,13 The lesions may be very vascular,causing diagnostic confusion.
Surgery is the treatment of choice11 although it isassociated with usual risks of orbital surgeryincluding loss of sight. Recent advances in steriotacticradiosurgery and fractionated radiotherapy in thetreatment of vestibular schwannoma and non-vestibular schwannoma have achieved high levels oftumor growth control whilst preserving cranial nervefunction.12,14 Future advances may mean that thistreatment option could be used to treat and controlorbital schwannomas.3
Neuro-imaging reveals a homogenious lesion iso-intense with rest of the surrounding neural tissuemimicking other lesions such as optic nerve gliomas,cystic spaces are sometimes seen.3,11 Histopathologyis required to make a definitive diagnosis.10,11,15
Neurofibromas are another group of benignnerve sheath tumors which can occur in the orbitregion.16 In a retrospective review by Rose et al. in1991,17 looking at peripheral nerve tumors in the orbit,they found that 93% of these lesions were eitherschwannomas (neurilemmomas) or neurofibromas.In their series they found that most affected nervewas the first division of the trigeminal nerve.
Neurofibromas are typically associated withneurofibromatosis, although they can occur inisolation. Approximately 25 to 45% of all lesions arefound in the head and neck region.16 Other sitestypical affected by neurofibromas include the eyelids,the orbit and rarely the lacrimal sac.18
Clinically they tend to present with painlessproptosis and diplopia. Pain and altered sensationare rare.17
Grossly, the lesions appear as an encapsulatedfirm white mass. Histologically neurofibromas consistof wavy cells with basophilic nuclei.16
The treatment of choice is surgical excision. Evenwhen incompletely excised recurrence is low.17
When to Suspect an Orbital Tumor ofNeurological Origin
• Insidious onset• Proptosis typically axial• Symptoms may include: Pain with and without
eye movement, diplopia, blurring of vision,reduced color vision and increased hyper-metropia
basm
ala
blog
(alw
ays o
rigin
al)

166166166166166 Surgical Atlas of Orbital DiseasesSurgical Atlas of Orbital DiseasesSurgical Atlas of Orbital DiseasesSurgical Atlas of Orbital DiseasesSurgical Atlas of Orbital Diseases
• Fundoscopy may include: Unilateral disc swellingand choroidal folds
• Firmness of the globe to retropulsion.
Investigations• Bloods to rule out an inflammatory cause• Orbital imaging: CT and/or MRI imaging
preferably with contrast enhancement• Orbital biopsy where imaging is suspicious or
the diagnosis is in doubt.
CASE ILLUSTRATIONS
Case 1
A 2 years old child with Neurofibromatosis type 1was referred to the eye department by the pediatriconcology service following surgery for a cerebellarastrocytoma and hydrocephalus.
At presentation she had an unrelated rightconvergent strabismus for which she underwentconvergent squint surgery. Fundoscopy includingthe optic disc was unremarkable and there was noRAPD. There was no evidence of proptosis.
Routine MRI scans (Figures 11.1 and 11.2)revealed sub-clinical bilateral optic nervegliomas.
Over the following 8 years optic disc cuppingdeveloped, with the left disc being paler and morecupped. Color vision remained normal in both eyes.
Case 2
A 66 years old female presented to the orbit clinicwith a 6 months history of horizontal diplopia. Visualacuity was 6/9 in the right eye and 6/12 in the left.Ocular motility appeared normal however diplopiawas reported on dextroversion. There was proptosisof 4 mm on the left and a left relative afferentpapillary defect. Only 2 of 13 ishihara plates werecorrectly identified by the left eye whereas colorvision in the right eye was normal. There was noevidence of papilloedema, although the left disc wasslightly pale. Fundoscopy revealed signs of agerelated macular degeneration in both eyes. Routinebloods were taken.
Urgent MRI and CT scans were performed,revealing an intraconal soft tissue mass which involvedthe sphenoidal wing and extending intracranially tothe temporal lobe (Figure 11.3). The findings werestrongly suggestive of a meningioma. A subsequentCT scan showed evidence of hyperostosis of thesphenoidal wing, as well as bone loss in the posterior-lateral aspect of the orbit. The diagnosis of asphenoidal wing meningioma was made.
A neurosurgical referral was made and thepatient was offered the option of a craniotomy andsurgical debulking of the tumor. As there was noguarantee that this would improve her vision,surgery was declined. The condition is beingmanaged conservatively with regular clinic followup and routine repeat MRI scans.
Case 3
A 66 years old female was referred from a districthospital with retro-orbital pain. An MRI had revealed
Figure 11.1: Bilateral optic nerve glioma (axial view)
Figure 11.2: Bilateral optic nerve glioma involving the chiasm(coronal view) Figure 11.3: Left optic nerve meningioma
basm
ala
blog
(alw
ays o
rigin
al)

Orbital Tumors of Neurological OriginOrbital Tumors of Neurological OriginOrbital Tumors of Neurological OriginOrbital Tumors of Neurological OriginOrbital Tumors of Neurological Origin 167167167167167
an intraconal retrobulbar mass displacing the opticnerve superiorly, with no evidence of bonedestruction. Visual acuity was 6/9 in the right eyeand 6/6 in the left. Color vision slightly reduced inthe right eye, seeing 13 out of 15 ishihara plates, theleft was normal. A mild right RAPD was noted. Bothoptic discs were normal and there was no proptosis.A diagnosis of optic nerve meningioma was made.Following discussion with the patient and oncology/radiotherapy department a dose of 50.4 Gy was givenin 14 fractions to the orbit.
Subsequent MRI scans revealed a reduction inthe tumor following the radiotherapy. Aftertreatment the patient experienced a dry right eye,which was treated with lubricants, and there wasevidence of mild radiation retinopathy.
Case 4
A 74 years old female with a known optic nervemeningioma was referred to the orbital clinic with arecurrence of orbital symptoms and enlargement ofthe lesion. Visual acuity in the affected eye was NPL,whereas the right was 6/6. Proptosis was noted onthe left side. The left disc was atrophic and therewas marked chorioretinal atrophy. An MRI confirmedenlargement of the lesion with extension towardsthe orbital apex. Following discussion with thepatient a decision was made to debulk themeningioma via a lateral orbitotomy. Histologyconfirmed the diagnosis of a meningioma (Figures11.4 and 11.5).
Case 5
A 36 years old male attended the orbit clinicwith an 18 months history of worsening left sidedproptosis (Figure 11.6). Visual acuity was unaffected;left eye 6/6, right 6/5, although color vision wasslightly reduced, with only 11 out of 13 ishihara colorvision plates being correctly identified in the left eye.Color vision was normal in the right eye. The visualfield on the left showed generalized depression onthe left side although no relative afferentpapillary defect was identified. Oculomotorfunction was reduced on abduction and upgaze inthe left eye. Fundoscopy of both eyes was normalwith no evidence of papilloedema. The centralnervous system examination was unremark-able and there was no past medical history ofrelevance.
Figure 11.4: Low power meningioma H and E stain
Figure 11.5: High power meningioma H and E stain
Figure 11.6: Left sided proptosis
An urgent MRI scan of the orbits was arrangedidentifying a 2.5 cm rounded intraconal lesion whichwas enhanced following intravenous contrastadministration (Figure 11.7). The optic nerve, lateraland inferior rectus were displaced and that the lesionwas intraconal (Figure 11.8). The optic nerve wasseparate from the lesion. An MRI scan was also
basm
ala
blog
(alw
ays o
rigin
al)

168168168168168 Surgical Atlas of Orbital DiseasesSurgical Atlas of Orbital DiseasesSurgical Atlas of Orbital DiseasesSurgical Atlas of Orbital DiseasesSurgical Atlas of Orbital Diseases
Surgical Approach
Where orbital surgery is considered to obtain a tissuediagnosis or to debulk an orbital tumor, a lateralorbitotomy approach is chosen since this gives goodaccess to the retro-orbital spaces and any lesionsfound there. If there is evidence of intracranialextension, referral to a neurosurgeon is indicated, acraniotomy may be indicated.
Lateral Orbitotomy
A lateral orbitotomy approach is employed to biopsytumors arising in the anterior third of the orbit. Thelateral 1/3 of the skin crease is marked with pen andextended down parallel to the lid margin to a heightlevel with the lateral canthus. The line is thenextended laterally in a horizontal plane for 1½ cm.Local anesthetic is injected subcutaneously in thisregion. A skin incision is made along this line with acutting diathermy. The deep tissues are bluntdissected down to the periosteum. This is incisedwith the diathermy and the periosteum bluntdissected off the bone exposing the lateral wall fromthe frontozygomatic suture down to the lower borderof the lateral wall just above the opening of thezygomaticofacial foramen. At the orbital rim theperiobita is elevated off the internal aspect of thelateral wall of the orbit. The orbital contents aredisplaced nasally with a malleable retractor. Twoholes ½ cm apart and ¾ cm back from the orbitalmargin are drilled parallel to the orbital rim at thesuperior border of the exposed bone and 2 at thebottom. A gap of approximately 3 cm will existbetween the higher of the 2 lower holes and the lowerof the upper 2 holes. The lateral orbital wall is incisedwith a power saw between the drilled holes bothsuperiorly and inferiorly. The cuts extended forapproximately 2 cm in a radial direction to an areawhere the bone thins. A malleable retractor shouldbe used to protect the globe during this procedure.The section of bone is dissected off with forceps andstored in normal saline.
Once the lesion is identified care should be takento avoid the globe, optic nerve and rectus muscles,while incision biopsies are taken using a 15° bladeand forceps. Pupil reactions are monitoredthroughout the procedure. Hemostasis is achievedwith bipolar cautery. The lateral orbital wall isreplaced by threading 4.0 prolene through the
Figure 11.7: Left orbital schwannoma axial view
Figure 11.8: Left orbital schwannoma sagittal view
organized overall the MRI and CT findingssuggested the lesion was a possible cavernoushemangioma. An urgent excision biopsy wasarranged via a lateral orbitotomy approach.
Macroscopically the tumor was found to be cysticand wrapped around optic nerve. The lesion wasdebulked. As the surgery proceeded the pupilbecame fixed and dilated. No further debulking wasattempted and the wound closed.
Postoperatively the pupil gradually recoveredand vision remained 6/6.
Histopathological examination revealed thelesion to be a cystic Schwannoma.
Referral was made to the oncology service andthe tumor treated with radiotherapy.
basm
ala
blog
(alw
ays o
rigin
al)

Orbital Tumors of Neurological OriginOrbital Tumors of Neurological OriginOrbital Tumors of Neurological OriginOrbital Tumors of Neurological OriginOrbital Tumors of Neurological Origin 169169169169169
pre-holes at the orbital rim and tied in place. Thetissues are closed with 5.0 vicryl and skin closed with5.0 prolene. A reducing dose of steroids is given for18 days along with a histamine H2 receptor antagonistsuch as ranitidine.
A head-light is worn throughout the procedureto ensure adequate illumination of the operating field.Where a drain is used this can be removed thefollowing day.
REFERENCES
1. Dutton JJ. Gliomas of the anterior visual pathway. Surveyof Ophthalmology 1994;38(5):427-52.
2. Jahraus CD, NJ Tarbell. Optic pathway gliomas. PediatricBlood and Cancer 2006;46(5):586-96.
3. Miller NR. Primary tumours of the optic nerve and itssheath Eye 2004;18(11):1026-37.
4. Kaufman LM, O Doroftei. Optic glioma warrantingtreatment in children Eye, 2006. 20(10):1149-64.
5. Rosenblum MK, Bilbao JM Ang L Neuromucular systemChap 28 in Surgical Pathology Ed Rosai (9th ed) 2004;2:2461-682.
6. Dutton JJ. Optic nerve sheath meningiomas. Survey ofOphthalmology 1992;37(3):167-83.
7. Carrasco JR, RB Penne. Optic nerve sheath meningiomasand advanced treatment options. Current Opinion inOphthalmology 2004;15(5):406-10.
8. Melian E, WM Jay. Primary radiotherapy for optic nervesheath meningioma. Seminars in Ophthalmology,2004;19(3-4):130-40.
9. Parsons JT, et al. Radiation optic neuropathy aftermegavoltage external-beam irradiation: analysis of time-dose factors. International Journal of Radiation Oncology,Biology, Physics, 1994;30(4):755-63.
10. Subramanian N, et al. Cystic schwannoma of the orbitacase series Orbit 2005;24(2):125-29.
11. Tezer MS, et al. Schwannoma originating from theinfraorbital nerve: a case report. Auris Nasus Larynx 2006;33(3):343-5.
12. Pollock BE, RL Foote, SL Stafford. Stereotactic radiosurgery:the preferred management for patients with nonvestibularschwannomas? Int J Radiat Oncol Biol Phys, 2002;52(4):1002-7.
13. Rutherford SA, AT King. Vestibular schwannomamanagement: What is the 'best' option? Br J Neurosurg,2005;19(4):309-16.
14. Tsuzuki N, et al. Cystic schwannoma of the orbit: casereport. Surg Neurol, 2000;54(5):385-7.
15. Rosai J Soft Tissues Chap 25 in Surgical Pathology Ed Rosai(9th ed) 2004;2:2237-371.
16. Chua CN, Alhady M, Ngo CT, Swethadri GK, Singh A, TanS Solitary nasal neurofibroma presenting as compressiveoptic neuropathy. Eye 2006;20(12):1406-8.
17. Rose GE, Wright JE. Isolated peripheral nerve sheathtumours of the orbit Eye 1991;5(6)668-73.
18. Dailey RA, Sullivan SA, Wobig JL. Surgical debulking ofeyelid and anterior orbital plexiform neurofibromas bymeans of the carbon dioxide laser. American Journal ofOphthalmology, 2000;130(1):117-19.
basm
ala
blog
(alw
ays o
rigin
al)

170170170170170 Surgical Atlas of Orbital DiseasesSurgical Atlas of Orbital DiseasesSurgical Atlas of Orbital DiseasesSurgical Atlas of Orbital DiseasesSurgical Atlas of Orbital Diseases
E Weis, J Rootman
Mesenchymal TumorsMesenchymal TumorsMesenchymal TumorsMesenchymal TumorsMesenchymal Tumors
Mesenchymal Soft Tissue Tumors
Tumors that are believed to arise from mesenchymaltissues occur in multiple sites with variable biologicbehavior. In the orbit mesenchymal tissues includestriated and smooth muscle, fibrous tissue, fat,cartilage, and bone. Bone tumors are discussedseparately in Chapter 13. Despite orbital mesenchymearising from neural crest, lesions do not differ fromother locations in the body in which mesenchymaltissues arise from mesoderm. In our orbital centermesenchymal tumors account for 1.6% of orbitallesions and 9% of neoplasias; in children theyconstitute 5% of all disease and 19.4% of childhoodneoplasia.1
Striated Muscle TumorsRhabdomyosarcoma
EpidemiologyRhabdomyosarcoma accounts for approximately 20%of all soft-tissue sarcomas making it the mostcommon soft tissue sarcoma in children.2, 3 The headand neck is the principal location and the orbit thesecond most common site in the head and neck (themost common being the parameninges) accountingfor about 10% of all rhabdomyosarcomas.4-6
Rhabdomyosarcoma is thus the most commonprimary orbital malignancy of childhood. In our clinicit constitutes 1% of all orbital neoplasias, and 6% inchildren.1
It has occurred from birth to the seventh decade,but 70% present in the first decade with a mean ageof 8. The embryonal subtype affects mainly children,the alveolar mainly adolescents (median age 16), and
the much rarer anaplastic (pleomorphic) subtype mostcommonly presents in older people (median age is54).7-11 Embryonal rhabdoymyosarcoma is the mostcommon subtype accounting for 49% of allrhabdomyosarcomas and their predominance in theorbit is even greater since this subtype has apredilection for the orbit and parameninges.12
Most cases are sporadic although familial,congenital, and multiple tumors in the same patientincluding retinoblastoma have been reported.13 Mostevidence suggests that they arise from primitivemesenchyme and not from skeletal muscle as theycan develop in areas with no skeletal muscle.14
Presentation
The typical presentation is rapidly developingexophthalmos over weeks (mean of 5) with 60%presenting with signs of inflammation includingconjunctival and eyelid swelling.9,10,15 Two-thirds ofprimary orbital rhabdomyosarcoma present with amass in the superonasal quadrant.15,16
The differential diagnosis is that of a childhoodprogressive rapidly developing mass with or withoutinflammation: infantile hemangioma, lymphangioma,neuroblastoma, chloroma, cellulitis, and non-specificorbital inflammation.
Imaging
There are no specific radiologic findings inrhabdomyosarcoma.17 Local bone invasion has beenreported in 24% of cases,18 with destruction of theorbital wall without orbital expansion seen in 30%.15,19
CT imaging typically shows a homogeneous (92%)well-defined soft tissue mass without bone
12C H A P T E R
basm
ala
blog
(alw
ays o
rigin
al)

Mesenchymal TumorsMesenchymal TumorsMesenchymal TumorsMesenchymal TumorsMesenchymal Tumors 171171171171171
Figures 12.1A and B: This 11-year-old child presented with a 3-week history of swelling of the left upper lid associated with ptosis andintermittent diplopia. It was a nonpainful swelling. She had an interpalpebral fissure of 5 mm on the left compared to the right at 8 mm, with 3 mmdownward and 1 mm axial displacement of the left globe. This was associated with a 2 diopter left hypotropia in primary position, whichincreased to 6 diopters in upgaze. There was a solid, rubbery, palpable mass just behind the superior oblique tendon adjacent to the trochlea.On CT scan, there was a well-defined, homogeneous, hyperdense extraconal mass in the superomedial orbit displacing the eye and medialrectus muscle downward. The superior muscle group appeared displaced laterally. Because of the rapid development of this mass, anincisional biopsy was performed. Histopathologically, the mass was consistent with an embryonal rhabdomyosarcoma. Repeat investigationsrevealed no other evidence of tumor, and the patient underwent chemotherapy and radiotherapy. She is alive and well 17 years later withpseudophakos (20/25-2) and some enophthalmos
Table 1: The International classification ofRhabdomyosarcoma (1995)
Superior prognosis BotryoidSpindle cell
Intermediate prognosis Embryonal
Poor prognosis AlveolarUndifferentiated
Subtypes whose prognosis Rhabdomyosarcoma with
is not presently available rhabdoid features
destruction that takes up contrast in a moderate tomarked amount; rarely the mass is poorly definedas it invades surrounding structures. It is most oftenextraconal (87%), in the supero-nasal quadrant (66%),(Figures 12.1A and B) and may displace but doesnot appear to arise from the extraocular muscles.15,16,20
Invasion of the sinus is noted in 20%.15 Focalhemorrhage or necrosis may result in heterogeneity.17
MRI typically shows isointensity to skeletal muscleand hypointensity to orbital fat on T1, hyperintensityon T2 to orbital fat and muscle, decreased signalintensity on all pulse sequences, and moderate tomarked uptake of gadolinium.16,17,20
ClassificationThe International Classification of Rhabdo-myosarcoma combined previous histologicclassification schemes to provide a system based onprognosis.12 The Pleomorphic subtype was excludedfrom this classification system because of its rarityin children (Table 1). The WHO classification hasdivided rhabdomyosarcoma into embryonal,alveolar, and pleomorphic subtypes. The spindle celland botryoid are considered variants of theembryonal subtype.21 The alveolar subtype morecommonly presents in the inferior orbit.
ManagementBefore the 1960’s rhabdomyosarcoma was an almostuniformly fatal disease. Common metastatic sites
included the lung (66% of metastasis), lymph nodes,and bone marrow.22 Interestingly, lymph nodemetastasis is highly related to site of origin with lowerrates seen in orbital tumors.22 Since the developmentof combination therapy, including biopsy/conservative surgery, radiation, and multi-agentchemotherapy, the majority of children are nowsurviving.14 Survival is related to pre-treatmenttumor extension past the site of origin, size, nodalinvolvement, and metastasis at presentation.6
Anatomic site is related to prognosis with the orbithaving the best prognosis (92% survival).5,23,24
Histologic type, as previously mentioned, is alsoassociated with survival.12 (Table 1).
Management begins with pathologic confir-mation and staging. Two contrasting clinicalphiloshophies have emerged from the main clinicaltrial groups. The American Intergroup Rhabdo-
A B
basm
ala
blog
(alw
ays o
rigin
al)

172172172172172 Surgical Atlas of Orbital DiseasesSurgical Atlas of Orbital DiseasesSurgical Atlas of Orbital DiseasesSurgical Atlas of Orbital DiseasesSurgical Atlas of Orbital Diseases
myosarcoma Study Group (IRSG) have tended to bemore aggressive by utilizing routine radiotherapy,except for tumors that are totally excised, followedby prolonged chemotherapeutic regimes.25,26 Whereasthe European International Society of PediatricOncology (SIOP) have attempted to use short coursechemotherapy and have avoided surgery orradiotherapy if possible.27-29 The best treatment optionis likely somewhere between these two philo-sophies.30 The vast majority of recurrences occurwithin 3 years of presentation and can often betreated with chemotherapy and repeat excision. Incases with refractory orbital tumors, salvage surgeryhas been shown to be beneficial.31
Complications related to treatment includecataract (55-82%), dry eye (30-36%), radiationretinopathy (6%), and bony hypoplasia (24-59%)secondary to radiation induced damage.15,32
Secondary malignancies are rare (1.2-3%) and mostcommonly occur in patients who have receivedalkylating agents and radiation.15,33
Rhabdomyoma
Tumors of skeletal muscle differentiation are atypicalin that malignant are more common than the benign.Rhabdomyoma is a rare benign tumor that has hadonly 6 cases described in the orbit.34-38 Extracardiacrhabdomyomas are divided into 4 categories: adult,fetal, genital, and the rhabdomyomatous mesen-chymal hamartoma types. The adult and fetal typehave a predilection for the head and neck and therhabdomyomatous mesenchymal hamartoma occursmainly in the periorbital and perioral subcutaneoustissue in children.14 We have reported the only caseof rhabdomyomatous mesenchymal hamartomareported in the orbit.38 Tumor excision or debulkingwith observation have been described ifsymptomatic, since they can regress with time.39
Recurrences are extremely rare and are typicallyassociated with incomplete removal.
Very little has been written about the radiologicfindings of extracardiac rhabdomyoma.17 CT imagingdemonstrates an ill defined homogeneous lesion thatdoes not show signs of necrosis or hemorrhage withheterogeneous enhancement.37 The adjacent bone canbe remodelled secondary to pressure but destructionis absent.37 MRI demonstrates a well defined masssimilar to muscle on T1 and T2 weighted images withvariable enhancement patterns.37,40-42
Smooth Muscle Tumors
Smooth muscle tumors of the orbit are exceedinglyrare and can arise from Muller’s muscle and the smoothmuscle overlying the inferior orbital fissure.Leiomyoma is a benign slow growing lesion withthree distinct clinical groups: (1) leiomyomacutis, (2) deep dermal (genital leiomyomas), and(3) leiomyoma of deep soft tissue (musculoskeletal).14
The most common location for these tumors is thefemale genital tract.44 About 20 cases in the orbit havebeen reported with a mean age of presentation in theorbit of 36 years.43 Complete excision is the preferredtreatment, since they are not sensitive to radiation,and no orbital recurrences have been found withcomplete excision.43 Interestingly, regression iscommonly seen with leiomyomas in other body sites.14
Leiomyosarcomas are rapidly growing infiltra-tive malignancies that can vary in their naturalbehavior. They account for 5-10% of soft tissuesarcomas2,45,46, are more common in females, presentat a median age of 60,47 and they can occur in youngerindividuals who have received radiation therapy.48,49
Most commonly they are retroperitoneal, thus lesionsoutside this location are poorly understood; yetcertain differences have been consistently docu-mented. Extra-peritoneal location seems to have abetter prognosis with a 5 year survival ofapproximately 64% and equal gender incidence.45,50
Although extremely rare in the orbit exenteration isthe preferred treatment.51-55 Adjuvant chemotherapyand radiotherapy may be beneficial.56
Imaging of subcutaneous leiomyoma typicallyshow a well-defined mass on MR with T1 intensitysimilar to skeletal muscle and T2 displaying aheterogeneous high or mixed signal intensity.17 Deepleiomyomas often show calcification, T1 intermediatesignal intensity, T2 variable intensity, and markedcontrast enhancement.17 Leiomyosarcomas do notdisplay specific features on imaging. Hemorrhage,necrosis, and cystic change are common. Ahypervascular mass with arteriovenous shunting isoften seen on arteriography.17
Adipose Tumors
Despite fat making up the majority of the orbitalvolume and lipomas being the most common softtissue tumor in the body14, tumors arising fromadipose tissue in the orbit are rare. Lipomas should
basm
ala
blog
(alw
ays o
rigin
al)

Mesenchymal TumorsMesenchymal TumorsMesenchymal TumorsMesenchymal TumorsMesenchymal Tumors 173173173173173
Figures 12.2A to D: (A) This 21-year-old female noted a nonpainful, mildly tender swelling of the left lower lid for 2 years. There was nohistory or findings of increase in size with Valsalva maneuver and no ecchymotic episodes. On physical examination, the vision was normal.There was a soft palpable mass not attached to the underlying tissue with 2 mm of vertical displacement and 1.5 mm of relative enophthalmos.Ocular movements were normal. (B, C) CT scan demonstrated a well-delineated low-density lesion anteriorly (C-large arrow). The lesionappeared to be adjacent to orbital fat, which was of a higher density (C-small arrow). The lesion also appeared to cause bone excavationanteriorly (B-arrow). It was thought to be a lipomatous tumor. At the time of excision, a well-defined lipomatous mass was removed en bloc fromthe inferolateral orbit. (D) Histologically, it had the typical features of a lipoma. Reprinted with permission from Shah NB, Chang WY, White VA,et al. Orbital lipoma:2 cases and review of the literature. Ophthalmic Plastic and Reconstructive Surgery. 2007;23:203
be differentiated from prolapsed orbital fat sincethey are often well circumscribed, slightly moreyellow, and displace orbital structures.57 (Figures12.2A to D) They present commonly in mid-life, aremore frequent in men, are not related to race, andafter an initial growth phase typically do not changein size significantly.58,59 Lipomas are divided into deepand subcutaneous/superficial lesions which are muchmore common.
Lipomas are identical to subcutaneous fat on CTand MRI.17 In the orbit they can have lower densitythan the surrounding orbital fat simulating a cyst.57
When the tumor is encapsulated a low signal fibrouscapsule may be visualized on MR and CT.17
Nonencapuslated lipomas have been reported makingit difficult to localize them when adjacent to normalfat.67
A B
C D
basm
ala
blog
(alw
ays o
rigin
al)

174174174174174 Surgical Atlas of Orbital DiseasesSurgical Atlas of Orbital DiseasesSurgical Atlas of Orbital DiseasesSurgical Atlas of Orbital DiseasesSurgical Atlas of Orbital Diseases
Liposarcoma is one the most common soft tissuesarcomas of adult life,14 but is rare in the orbit.1,60
Thirty five cases have been reported in the literature,but misclassification is likely since our definition andpathological evaluation has improved over time.61,62
In orbital cases the average age was 64 years of agewith a female predilection.55 The most commonpresentation is painless proptosis with an 8 monthmean duration of symptoms.55 Three distinct entitieshave been described, each validated with cytogeneticevidence. In order of good to poor prognosis theyare: well-differentiated (adipocytic, sclerosing,inflammatory, spindle cell, and dedifferentiated),myxoid/round cell, and pleomorphic.14,63 In the orbitthe myxoid is the most common subtype.62 Unlikelipomas which are primarily subcutaneous in locationliposarcomas are primarily deep tumors; if they occursuperficially they are referred to as atypical and havean excellent prognosis since they are often amenableto complete surgical resection.64-66 It is generallybelieved that lipomas cannot transform intoliposarcomas; the distinction in location betweenlipomas and liposarcomas is the primary argumentcited as proof of this.14 Clinical and histopathologicdiagnosis can be difficult. Treatment involves surgicalexcision which typically involves exenteration,although well circumscribed cases have been resected.Liposarcomas of the orbit have a favorable prognosiswith no reports of a neoplasm, that meets today’shistopathological criteria for diagnosis, metastasizingand only one recurring locally.61,62
When a lesion with imaging characteristics similarto a lipoma with an adjacent non-fatty mass,liposarcoma should be added to the differentialdiagnosis. Liposarcomas vary from approximately a25-75% fatty component depending on their level ofdifferentiation.68 Liposarcomas also show calcificationin approximately 12% of cases which is more commonthan in lipomas.17 Few papers have described theimaging in the orbit. Jakobiec et al. described centrallucency due to fat seen on CT imaging resembling acystic structure.61 They also reported that theselesions commonly involved the extraocular musclesand one case was hyperintense on MRI T1 imaging.61
A single case report described unique characteristicsincluding an extraconal mass with MRI T2 imagingshowing hypointensity in comparison to cerebralcortex and light peripheral enhancement withgadolinium.54
Lesions shown to mimic fatty tumors on imaginginclude myxoid tumors, lesions associated with asubacute hematoma, muscle with fatty replacement,and tumors invading surrounding fat.17
Fibrous Tissue Tumors
Despite the large number of subtypes of fibroustumors, only a few have been reported in the orbit.Fibrosarcomas have been diagnosed much lesscommonly over time as our definition andpathological assessment has advanced.14 Recent serieshave found that they are slightly more common inmen69 and usually present in the early 40’s.70, 71
Recurrence is very common occurring inapproximately 45% with surgical margins being thebest predictor.69 Scott et al.’s series found thatrecurrence occurred in 79% of tumors withinadequate margins and in 18% of those treated withwide or radical excision.69 Five year metastasis ratesare around 63% and are typically to the lung, spine,and skull.69 A 5 years survival rate of approximately40% has been reported.69 These lesions are rare as aprimary tumor of the orbit but they can also invadefrom the nasal cavity or face. Exenteration or excisionwith wide local margins is recommended since theyare commonly incompletely removed. CT and MRimaging typically show an aggressively infiltratingorbital mass,72 however infantile lesions have beenreported to be well circumscribed.73
Solitary fibrous tumor classically occurs in thepleural lining of the lung, but has been describedthroughout the body including the orbit, adjacentnasal cavity and sinuses.14 Approximately 55 caseshave been reported in the orbit since its firstdescription there in 1994 with most cases beingbenign.74-76 It has been seen in all age groups, with amedian age of 50,77 and usually presents as a well-circumscribed yet unencapsulated lesion causinggradual proptosis.1 Pleural solitary fibrous tumor canvary greatly in its clinical characteristics andmalignancy on pathological assessment. Even less isknown about non-pleural solitary fibrous tumors.Approximately 10% of non-pleural lesions have beenshown to recur and metastases are very rare.78
Pathological assessment for atypical features wasfound to be a significant predictor of recurrence.78
Since these tumors are difficult to remove due toinvasion and they may undergo malignant trans-formation en bloc resection is recommended.79
basm
ala
blog
(alw
ays o
rigin
al)

Mesenchymal TumorsMesenchymal TumorsMesenchymal TumorsMesenchymal TumorsMesenchymal Tumors 175175175175175
Figures 12.3A and B: (A) This 34-year-old woman presented with ahistory of right upper lid swelling and ptosis over 1 year, which wasassociated with tearing, light sensitivity and occasional sharp pain.Physical examination findings were a palpable lacrimal gland on theright, bilateral reduced Schirmer's function, 3 mm of ptosis and 3 mmof proptosis. There was a soft nontender mass superolaterally, whichwas causing a 3 mm downward and 4 mm inward displacement aswell as indentation of the globe, leading to elevation of macula anddisc (B)
On CT the lesions are well circumscribed andtake up contrast intensely in a homogeneous or ringpattern,76 although one review suggests that contrastuptake is mild to moderate.72 With MRI these tumorsalso enhance intensely, commonly showing areas ofhemorrhage and T2 hypointensity.72
Histiocytic TumorsFibrous histiocytomaFibrous histiocytomas histologically and clinically canvary from a slowly developing benign to locallyaggressive fast growing malignant lesion. Foursubtypes have been described in order of frequency:storiform-pleomorphic, myxoid (myxoidfibro-sarcoma), giant cell (malignant giant cell tumor ofsoft parts), and inflammatory (xanthosarcoma,malignant xanthogranuloma).14 Benign fibroushistiocytoma most commonly affects the skin butapproximately 0.3% can occur in deeper locations suchas muscle tissue.80 Recurrence rates for benigncutaneous fibrous histiocytomas following excisionrange from 5-10%,14,81 with deeper tumors typicallypresenting as a much larger lesion more oftenresulting in incomplete resection and thus recurrencerates have been reported closer to 50%.82,83
Malignant fibrous histiocytomas are the mostcommon adult malignant soft tissue tumor in thebody.84 Font et al.’s orbital series found that 63%were benign, 26% were locally aggressive and 11%were malignant.82 They showed that if the tumor hadinfiltrative margins, hypercellular zones or both,recurrence rates were 57% compared to 31% in thosethat did not have these features.82 Typically they areslow-growing, firm, infiltrative, and present in theupper nasal quadrant with a mean age of 43 years.82
Common presenting symptoms include proptosis(60%), mass (46%), and decreased vision (25%) witha mean duration of symptoms of 29 months.82
Complete surgical excision is recommended. This istypically accomplished by removing the tumor alonealthough in some infiltrative cases this might not bepossible without exenteration. Recent large systemicseries have reported recurrence rates from 19-21%,metastasis, mostly to lung and bone, in 31-35%, and5 year survival rates from 65-70%.85-87 In contrast
ten year survival rates for orbital tumors is about90%.1,82
It can be difficult to differentiate fibrous fromother lesions.17,72 (Figures 12.3A and B) No specificultrasonic and CT imaging characteristics have beenfound (Figures 12.4A to E).88 Imaging is also highlyvariable related to amounts of collagen, necrosis,hemorrhage, and myxoid tissue but often displayshigh signal intensity on T2. Benign tumors aretypically well-circumscribed and may remodel bone,with malignant lesions typically having infiltratingmargins and bone destruction.72 Benign histio-cytomas are usually homogeneous on CT, and MRIT1 and T2 imaging, whereas malignant lesions havea more heterogeneous pattern.72 In some casesmalignant lesions may have a homogeneous CT andT1 image with a heterogeneous T2 image.72
Histopathology and immunohistiochemistry help inthe diagnosis (Figures 12.5A and B)
Malignant Tumors of Uncertain TypeRhabdoid tumor is a highly aggressive neoplasmprimarily seen in the kidney although it has beenreported in extrarenal sites including the centralnervous system and soft tissues including theorbit.14,89-96 Extrarenal sites have approximately a 15%survival, but there are too few reported cases in theorbit to come to a conclusion as to whether theybehave differently than other extrarenal sites. Of the7 described in the orbit 4 have died.
A Bbasm
ala
blog
(alw
ays o
rigin
al)

176176176176176 Surgical Atlas of Orbital DiseasesSurgical Atlas of Orbital DiseasesSurgical Atlas of Orbital DiseasesSurgical Atlas of Orbital DiseasesSurgical Atlas of Orbital Diseases
Figures 12.4A to E: (A, B) The ultrasound for the patient depicted a well-defined solid lacrimal mass indenting the globe. (C to E) CT scandemonstrated a well-defined, solid, enhancing, slightly bosselated mass that indents the globe and causes excavation of the adjacent lacrimalfossa. The mass appeared distinct from the lacrimal gland and enhanced to a greater degree
Figures 12.5A and B: The patient underwent an excision biopsy of the lesion, which at the time of surgery appeared yellow and soft. It wasexcised from the adjacent lacrimal gland. (A, B) Histologically, it was an encapsulated, somewhat myxomatous, vascular spindle cell lesion,which was negative for S100, keratin and epithelial membrane antigen but positive for smooth muscle antigen, vimentin and CD34. Thehistologic differential diagnosis included fibrous histiocytoma, myxoid tumor or leiomyoma
A B C
D E
A B
basm
ala
blog
(alw
ays o
rigin
al)

Mesenchymal TumorsMesenchymal TumorsMesenchymal TumorsMesenchymal TumorsMesenchymal Tumors 177177177177177
REFERENCES
1. Rootman, J, Diseases of the Orbit: A MultidisciplinaryApproach. 2nd ed. 2003, Philadelphia: Lippincott Williamsand Wilkins.
2. Russell, WO, et al. A clinical and pathological staging systemfor soft tissue sarcomas. Cancer, 1977;(4):1562-70.
3. Masson, JK and EH Soule, Embryonal rhabdomyo-sarcomaof the head and neck. Report on eighty-eight cases. Am JSurg, 1965;110(4):585-91.
4. Maurer, HM, et al., The Intergroup RhabdomyosarcomaStudy-I. A final report. Cancer, 1988;61(2):209-20.
5. Maurer, HM, et al., The Intergroup RhabdomyosarcomaStudy-II. Cancer, 1993;71(5):1904-22.
6. Crist W, et al., The Third Intergroup RhabdomyosarcomaStudy. J Clin Oncol, 1995;13(3):610-30.
7. Ashton, N and G Morgan, Embryonal sarcoma andembryonal rhabdomyosarcoma of the orbit. J Clin Pathol,1965;18(6):699-714.
8. La Quaglia, MP, et al., The effect of age at diagnosis onoutcome in rhabdomyosarcoma. Cancer, 1994;73(1):109-17.
9. Jones, IS, AB Reese, and J Kraut, Orbital rhabdo-myosarcoma. An analysis of 62 cases. Am J Ophthalmol,1966;61(4):721-36.
10. Jones, IS, AB Reese, and J Krout, Orbital rhabdo-myosarcoma: an analysis of sixty-two cases. Trans AmOphthalmol Soc, 1965;63:223-55.
11. Furlong, MA, T Mentzel, and JC Fanburg-Smith,Pleomorphic rhabdomyosarcoma in adults: aclinicopathologic study of 38 cases with emphasis onmorphologic variants and recent skeletal muscle-specificmarkers. Mod Pathol, 2001;14(6)595-603.
12. Newton, WA, Jr, et al., Classification of rhabdo-myosarcomas and related sarcomas. Pathologic aspects andproposal for a new classification—an IntergroupRhabdomyosarcoma Study. Cancer, 1995;76(6):1073-85.
13. Howard, GM and VG Casten, Rhabdomyosarcoma of TheOrbit In Brothers. Arch Ophthalmol, 1963;70:319-22.
14. Weiss, ww and JR Goldblum, Enzinger and Weiss’s SoftTissue Tumors (4th ed) 2001, ST. Louis: Mosby.
15. Shields, CL, et al., Clinical spectrum of primary ophthalmicrhabdomyosarcoma. Ophthalmology, 2001;108(12):2284-92.
16. Sohaib, SA, I Moseley, and JE Wright, Orbitalrhabdomyosarcoma—the radiological characteristics. ClinRadiol, 1998;53(5):357-62.
17. Krandsdorf, MJ and MD Murphrey, Imaging of Soft TissueTumors (2nd ed) 2006, Philadelphia: Lippincott Williamsand Williams.
18. Simmons, M and AK Tucker, The radiology of bone changesin rhabdomyosarcoma. Clin Radiol, 1978;29(1): 47-52.
19. Kirkpatrick, JA and MA Capitanio, Radiology of the orbitin infancy and childhood. Radiol Clin North Am, 1972;10(1):143-66.
20. Mafee, MF, E Pai, and B Philip, Rhabdomyosarcoma of theorbit. Evaluation with MR imaging and CT. Radiol ClinNorth Am, 1998;36(6):1215-27, xii.
21. Parham, DM and FG Barr, WHO classification of Tumors.Pathology and Genetics: Tumors of Soft Tissue and Bone.2002, Lyon, France: IARC Press. 146-49.
22. Raney, RB, Jr, et al., Disease patterns and survival rate inchildren with metastatic soft-tissue sarcoma. A report fromthe Intergroup Rhabdomyosarcoma Study (IRS)-I. Cancer,1988;62(7):1257-66.
23. Crist, WM, et al., Prognosis in children withrhabdomyosarcoma: a report of the intergrouprhabdomyosarcoma studies I and II. IntergroupRhabdomyosarcoma Committee. J Clin Oncol, 1990;8(3):443-52.
24. Newton, WA, Jr, et al., Histopathology of childhoodsarcomas, Intergroup Rhabdomyosarcoma Studies I andII: clinicopathologic correlation. J Clin Oncol, 1988;6(1):67-75.
25. Breneman, JC and ES Wiener, Issues in the local control ofrhabdomyosarcoma. Med Pediatr Oncol, 2000;35(2):104-9.
26. Baker, KS, et al., Benefit of intensified therapy for patientswith local or regional embryonal rhabdomyosarcoma:results from the Intergroup Rhabdomyosarcoma StudyIV. J Clin Oncol, 2000;18(12):2427-34.
27. Martelli, H, et al., Conservative treatment for girls withnonmetastatic rhabdomyosarcoma of the genital tract: Areport from the Study Committee of the InternationalSociety of Pediatric Oncology. J Clin Oncol, 1999;17(7):2117-22.
28. Baldini, EH, et al., Long-term outcomes after function-sparing surgery without radiotherapy for soft tissuesarcoma of the extremities and trunk. J Clin Oncol,1999;17(10):3252-9.
29. Oberlin, O, et al., Treatment of orbital rhabdomyosarcoma:survival and late effects of treatment—results of aninternational workshop. J Clin Oncol, 2001;19(1):197-204.
30. McDowell, HP, Update on childhood rhabdomyosarcoma.Arch Dis Child, 2003;88(4):354-7.
31. Mannor, GE, et al., Multidisciplinary management ofrefractory orbital rhabdomyosarcoma. Ophthalmology,1997;104(7)1198-201.
32. Raney, RB, et al., Late effects of therapy in 94 patients withlocalized rhabdomyosarcoma of the orbit: Report fromthe Intergroup Rhabdomyosarcoma Study (IRS)-III, 1984-1991. Med Pediatr Oncol, 2000;34(6)413-20.
33. Heyn, R, et al., Second malignant neoplasms in childrentreated for rhabdomyosarcoma. Intergroup Rhabdo-myosarcoma Study Committee. J Clin Oncol, 1993.11(2):262-70.
34. Knowles, DM, 2nd and FA Jakobiec, Rhabdomyoma of theorbit. Am J Ophthalmol, 1975;80(6):1011-8.
35. Di Sant’Agnese, PA and DM Knowles, 2nd, Extracardiacrhabdomyoma: a clinicopathologic study and review ofthe literature. Cancer, 1980;46(4):780-9.
basm
ala
blog
(alw
ays o
rigin
al)

178178178178178 Surgical Atlas of Orbital DiseasesSurgical Atlas of Orbital DiseasesSurgical Atlas of Orbital DiseasesSurgical Atlas of Orbital DiseasesSurgical Atlas of Orbital Diseases
36. Hatsukawa, Y, et al., Rhabdomyoma of the orbit in a child.Am J Ophthalmol, 1997;123(1):142-4.
37. Myung, J, et al, Rhabdomyoma of the orbit: a case report.Pediatr Radiol, 2002;32(8):589-92.
38. Mavrikakis, I, et al., Orbital mesenchymal hamartoma withrhabdomyomatous features. Br J Ophthalmol, 2007;91(5):692-3.
39. DiMario, FJ, Jr, et al., Evolution of cardiac rhabdomyomain tuberous sclerosis complex. Clin Pediatr (Phila), 1996;35(12):615-9.
40. Fukuda, Y, et al., Rhabdomyoma of the base of the tongue.J Laryngol Otol, 2003;117(6):503-7.
41. Metheetrairut, C, et al., Pharyngeal rhabdomyoma: aclinico-pathological study. J Otolaryngol, 1992;21(4):257-61.
42. Ho, VT and VM Rao, Recurrent adult-type pharyngealrhabdomyoma: MR appearance. AJR Am J Roentgenol,1992;159(5):1130-1.
43. Arat, YO, et al., Leiomyoma of the orbit and periocularregion: a clinicopathologic study of four cases. OphthalPlast Reconstr Surg, 2005;21(1):16-22.
44. Farman, AG, Benign smooth muscle tumours. S Afr Med J,1975;49(33):1333-40.
45. Gustafson, P, et al., Soft tissue leiomyosarcoma. Apopulation-based epidemiologic and prognostic study of48 patients, including cellular DNA content. Cancer,1992;70(1):114-9.
46. Hashimoto, H, et al., Leiomyosarcoma of the external softtissues. A clinicopathologic, immunohistochemical, andelectron microscopic study. Cancer, 1986;57(10):2077-88.
47. Shmookler, BM and DH Lauer, Retroperitonealleiomyosarcoma. A clinicopathologic analysis of 36 cases.Am J Surg Pathol, 1983;7(3):269-80.
48. Font, RL, S Jurco, 3rd, and RJ Brechner, Postradiationleiomyosarcoma of the orbit complicating bilateralretinoblastoma. Arch Ophthalmol, 1983;101(10):1557-61.
49. Folberg, R, et al., Orbital leiomyosarcoma after radiationtherapy for bilateral retinoblastoma. Arch Ophthalmol,1983;101(10):1562-5.
50. Farshid, G, et al., Leiomyosarcoma of somatic soft tissues:a tumor of vascular origin with multivariate analysis ofoutcome in 42 cases. Am J Surg Pathol, 2002;26(1):14-24.
51. Jakobiec, FA, et al., Leiomyoma and leiomyosarcoma ofthe orbit. Am J Ophthalmol, 1975;80(6):1028-42.
52. Wojno, T, RR Tenzel, and M Nadji, Orbital leiomyosarcoma.Arch Ophthalmol, 1983;101(10):1566-8.
53. Meekins, BB, JJ Dutton, and AD Proia, Primary orbitalleiomyosarcoma. A case report and review of the literature.Arch Ophthalmol, 1988;106(1):82-6.
54. Hou, LC, MA Murphy, and GA Tung, Primary orbitalleiomyosarcoma: a case report with MRI findings. Am JOphthalmol, 2003;135(3):408-10.
55. Lin, IC, et al., Primary orbital leiomyosarcoma. OphthalPlast Reconstr Surg, 2005;21(6):451-3.
56. Sturgis, EM and BO Potter, Sarcomas of the head and neckregion. Curr Opin Oncol, 2003;15(3):239-52.
57. Shah, NB, et al., Orbital lipoma: 2 cases and review ofliterature. Ophthal Plast Reconstr Surg, 2007;23(3):202-5.
58. Rydholm, A and NO Berg, Size, site and clinical incidenceof lipoma. Factors in the differential diagnosis of lipomaand sarcoma. Acta Orthop Scand, 1983;54(6):929-34.
59. Solvonuk, PF, et al., Correlation of morphologic andbiochemical observations in human lipomas. Lab Invest,1984;51(4):469-74.
60. Shields, JA, et al., Classification and incidence of space-occupying lesions of the orbit. A survey of 645 biopsies.Arch Ophthalmol, 1984;102(11):1606-11.
61. Jakobiec, FA, et al., Primary liposarcoma of the orbit.Problems in the diagnosis and management of five cases.Ophthalmology, 1989;96(2):180-91.
62. Cai, YC, et al., Primary liposarcoma of the orbit: aclinicopathologic study of seven cases. Ann Diagn Pathol,2001;5(5)255-66.
63. Fletcher, CDM, Diagnostic Histopathology of Tumors (2nded) CDM Fletcher. 2000, London: Churchill Livingstone.
64. Linehan, DC, et al., Influence of biologic factors andanatomic site in completely resected liposarcoma. J ClinOncol, 2000;18(8):1637-43.
65. Evans, HL, EH Soule, and RK Winkelmann, Atypical lipoma,atypical intramuscular lipoma, and well differentiatedretroperitoneal liposarcoma: a reappraisal of 30 casesformerly classified as well differentiated liposarcoma.Cancer, 1979;43(2):574-84.
66. Kindblom, LG, L Angervall, and AS Fassina, Atypicallipoma. Acta Pathol Microbiol Immunol Scand [A], 1982.90(1):27-36.
67. Roberts, CC, PT Liu, and TV Colby, Encapsulated versusnonencapsulated superficial fatty masses: a proposed MRimaging classification. AJR Am J Roentgenol, 2003;180(5):1419-22.
68. Kransdorf, MJ, et al., Imaging of fatty tumors: distinctionof lipoma and well-differentiated liposarcoma. Radiology,2002;224(1):99-104.
69. Scott, SM, et al., Soft tissue fibrosarcoma. A clinicopathologicstudy of 132 cases. Cancer, 1989;64(4):925-31.
70. Pack, GT and IM Ariel, Fibrosarcoma of the soft somatictissues; a clinical and pathologic study. Surgery, 1952;31(3):443-78.
71. Pritchard, DJ, et al., Fibrosarcoma of bone and soft tissuesof the trunk and extremities. Orthop Clin North Am, 1977.8(4):869-81.
72. Dalley, RW, Fibrous histiocytoma and fibrous tissue tumorsof the orbit. Radiol Clin North Am, 1999;37(1):185-94.
73. Lee, MJ, et al., Congenital-infantile fibrosarcoma: magneticresonance imaging findings. Can Assoc Radiol J, 1996;47(2):121-5.
basm
ala
blog
(alw
ays o
rigin
al)

Mesenchymal TumorsMesenchymal TumorsMesenchymal TumorsMesenchymal TumorsMesenchymal Tumors 179179179179179
74. Westra, WH, WL Gerald, and J Rosai, Solitary fibrous tumor.Consistent CD34 immunoreactivity and occurrence in theorbit. Am J Surg Pathol, 1994;18(10):992-8.
75. Cerda-Nicolas, M, et al., Solitary fibrous tumor of the orbit:morphological, cytogenetic and molecular features.Neuropathology, 2006;26(6):557-63.
76. Meyer, D and F Riley, Solitary fibrous tumor of the orbit: aclinicopathologic entity that warrants both a heightenedawareness and an atraumatic surgical removal technique.Orbit, 2006;25(1):45-50.
77. Dictor, M, et al., Myofibromatosis-like hemangio-pericytoma metastasizing as differentiated vascular smooth-muscle and myosarcoma. Myopericytes as a subset of“myofibroblasts”. Am J Surg Pathol, 1992;16(12):1239-47.
78. Vallat-Decouvelaere, AV, SM Dry, and CD Fletcher,Atypical and malignant solitary fibrous tumors inextrathoracic locations: evidence of their comparability tointra-thoracic tumors. Am J Surg Pathol, 1998;22(12):1501-11.
79. Bernardini, FP, et al., Solitary fibrous tumor of the orbit: isit rare? Report of a case series and review of the literature.Ophthalmology, 2003;110(7):1442-8.
80. Fletcher, CD, Benign fibrous histiocytoma of subcutaneousand deep soft tissue: a clinicopathologic analysis of 21 cases.Am J Surg Pathol, 1990;14(9):801-9.
81. Niemi, KM, The benign fibrohistiocytic tumours of the skin.Acta Derm Venereol Suppl (Stockh), 1970;50(63):Suppl 63:1-66.
82. Font, RL and AA Hidayat, Fibrous histiocytoma of theorbit. A clinicopathologic study of 150 cases. Hum Pathol,1982;13(3):199-209.
83. Franquemont, DW, et al., Benign fibrous histiocytoma ofthe skin with potential for local recurrence: a tumor to bedistinguished from dermatofibroma. Mod Pathol, 1990;3(2):158-63.
84. Enzinger, FM, Malignant fibrous histiocytoma 20 years afterStout. Am J Surg Pathol, 1986. 10 Suppl 1:43-53.
85. Salo, JC, et al., Malignant fibrous histiocytoma of theextremity. Cancer, 1999;85(8):1765-72.
86. Le Doussal, V, et al., Prognostic factors for patients withlocalized primary malignant fibrous histiocytoma: amulticenter study of 216 patients with multivariate analysis.Cancer, 1996;77(9):1823-30.
87. Zagars, GK, JR Mullen, and A. Pollack, Malignant fibroushistiocytoma: outcome and prognostic factors followingconservation surgery and radiotherapy. Int J Radiat OncolBiol Phys, 1996;34(5):983-94.
88. Jacomb-Hood, J and IF Moseley, Orbital fibroushistiocytoma: computed tomography in 10 cases and areview of radiological findings. Clin Radiol, 1991;43(2):117-20.
89. Haas, JE, et al., Ultrastructure of malignant rhabdoid tumorof the kidney. A distinctive renal tumor of children. HumPathol, 1981;12(7):646-57.
90. Sotelo-Avila, C, et al., Renal and extrarenal rhabdoid tumorsin children: a clinicopathologic study of 14 patients. SeminDiagn Pathol, 1986;3(2):151-63.
91. Stidham, DB, et al., Congenital malignant rhabdoid tumorof the orbit. J Aapos, 1999;3(5):318-20.
92. Walford, N, et al., Intraorbital rhabdoid tumour followingbilateral retinoblastoma. Histopathology, 1992;20(2):170-3.
93. Gunduz, K, et al., Malignant rhabdoid tumor of the orbit.Arch Ophthalmol, 1998;116(2):243-6.
94. Rootman, J, KF Damji, and JE Dimmick, Malignant rhabdoidtumor of the orbit. Ophthalmology, 1989;96(11): 1650-4.
95. Niffenegger, JH, et al., Adult extrarenal rhabdoid tumor ofthe lacrimal gland. Ophthalmology, 1992;99(4):567-74.
96. Gottlieb, C, et al., Congenital orbital and disseminatedextrarenal malignant rhabdoid tumor. Ophthal PlastReconstr Surg, 2005;21(1):76-9.
basm
ala
blog
(alw
ays o
rigin
al)
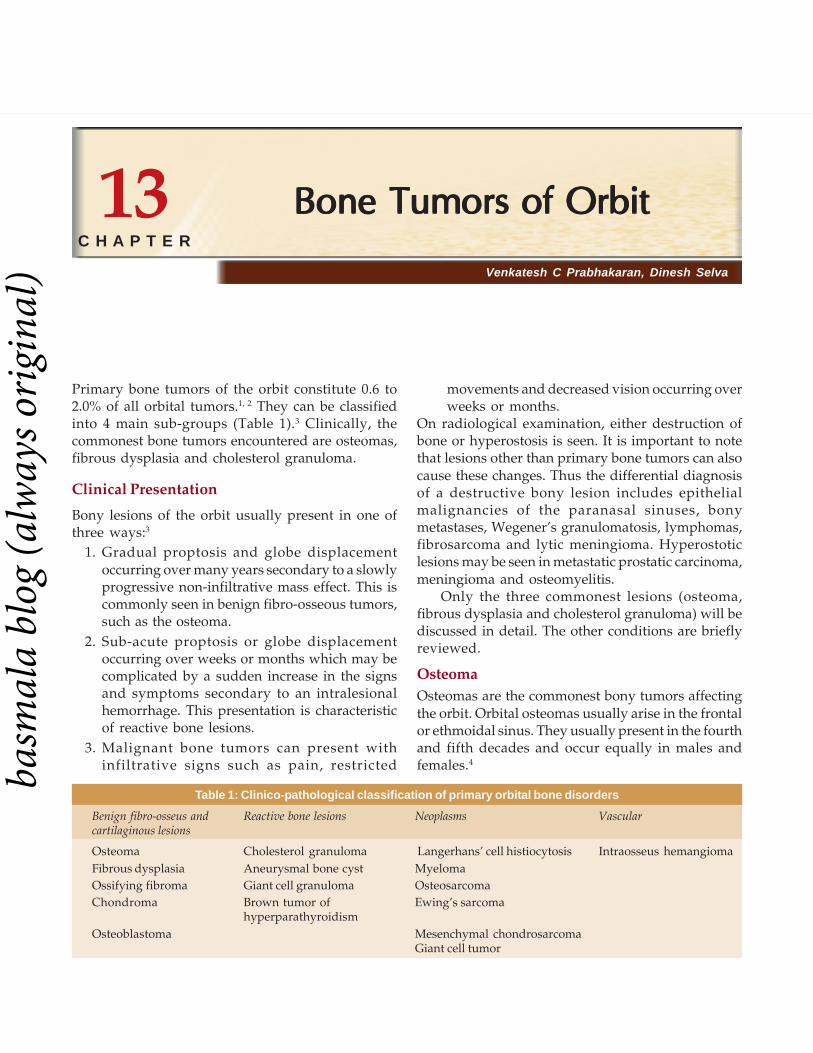
180180180180180 Surgical Atlas of Orbital DiseasesSurgical Atlas of Orbital DiseasesSurgical Atlas of Orbital DiseasesSurgical Atlas of Orbital DiseasesSurgical Atlas of Orbital Diseases
Venkatesh C Prabhakaran, Dinesh Selva
Bone Tumors of OrbitBone Tumors of OrbitBone Tumors of OrbitBone Tumors of OrbitBone Tumors of Orbit
Primary bone tumors of the orbit constitute 0.6 to2.0% of all orbital tumors.1, 2 They can be classifiedinto 4 main sub-groups (Table 1).3 Clinically, thecommonest bone tumors encountered are osteomas,fibrous dysplasia and cholesterol granuloma.
Clinical Presentation
Bony lesions of the orbit usually present in one ofthree ways:3
1. Gradual proptosis and globe displacementoccurring over many years secondary to a slowlyprogressive non-infiltrative mass effect. This iscommonly seen in benign fibro-osseous tumors,such as the osteoma.
2. Sub-acute proptosis or globe displacementoccurring over weeks or months which may becomplicated by a sudden increase in the signsand symptoms secondary to an intralesionalhemorrhage. This presentation is characteristicof reactive bone lesions.
3. Malignant bone tumors can present withinfiltrative signs such as pain, restricted
movements and decreased vision occurring overweeks or months.
On radiological examination, either destruction ofbone or hyperostosis is seen. It is important to notethat lesions other than primary bone tumors can alsocause these changes. Thus the differential diagnosisof a destructive bony lesion includes epithelialmalignancies of the paranasal sinuses, bonymetastases, Wegener’s granulomatosis, lymphomas,fibrosarcoma and lytic meningioma. Hyperostoticlesions may be seen in metastatic prostatic carcinoma,meningioma and osteomyelitis.
Only the three commonest lesions (osteoma,fibrous dysplasia and cholesterol granuloma) will bediscussed in detail. The other conditions are brieflyreviewed.
OsteomaOsteomas are the commonest bony tumors affectingthe orbit. Orbital osteomas usually arise in the frontalor ethmoidal sinus. They usually present in the fourthand fifth decades and occur equally in males andfemales.4
Table 1: Clinico-pathological classification of primary orbital bone disorders
Benign fibro-osseus and Reactive bone lesions Neoplasms Vascularcartilaginous lesions
Osteoma Cholesterol granuloma Langerhans’ cell histiocytosis Intraosseus hemangiomaFibrous dysplasia Aneurysmal bone cyst MyelomaOssifying fibroma Giant cell granuloma OsteosarcomaChondroma Brown tumor of Ewing’s sarcoma
hyperparathyroidismOsteoblastoma Mesenchymal chondrosarcoma
Giant cell tumor
13C H A P T E R
basm
ala
blog
(alw
ays o
rigin
al)

Bone Tumors of OrbitBone Tumors of OrbitBone Tumors of OrbitBone Tumors of OrbitBone Tumors of Orbit 181181181181181
Clinically, osteomas cause gradual proptosis andglobe displacement occurring over many years. Theremay be an associated headache and a bony mass isusually palpable in the superior or superomedialorbit. Obstruction of the sinus ostia may lead tosinusitis or mucocoele formation. Uncommonfeatures include acquired Brown’s syndrome, gaze-evoked amaurosis or pain, globe subluxation anderosion leading to orbital emphysema or CSFrhinorrhea. Osteomas of the sphenoid sinus, thoughrare, are important as they can cause an orbital apexsyndrome and optic atrophy.3
An important systemic association is Gardner’ssyndrome which is a phenotypic variant of the familialadenomatous polyposis syndrome. Gardner’ssyndrome is an autosomal dominant condition whosefeatures include colonic polyps, osteomas, andcongenital hypertrophy of the retinal pigmentepithelium (CHRPE). As the rate of malignanttransformation of the colonic polyps is very high,screening for Gardner’s syndrome (dilatedfunduscopic examination and gastroenterologistreferral) is recommended in patients withosteoma.5
On X-ray and CT scans, osteomas are extremelyradiodense, well circumscribed lesions, usuallyarising in the sinus and invading the orbit. Bonewindows on CT usually show a very dense peripherywith a more radiolucent center.
Histologically, osteomas are composed of lamellarbone with fibrovascular stroma. They are divided intothree types: ivory, compact and fibrous osteomasbased on the relative proportions of lamellar boneand fibrous stroma.6 The ivory osteomas areconsidered to be the most mature form of the lesion.However, there does not seem to be a correlationbetween clinical behavior and histological subtype.3
Asymptomatic osteomas are treatedconservatively, except when involving thesphenoidal sinus, as it is easier to remove a smalllesion before it encroaches on the optic canal.
When symptomatic, treatment is by surgicalexcision. Anterior lesions are removed via an anteriororbitotomy. A modified Lynch incision may be usedfor superomedial osteomas. Endoscopic techniquesmay also be used.7 Posterior lesions may require acombined orbitocranial approach. Recurrence is rare,even following partial removal.
CASE ILLUSTRATION (Figures 13.1A to D)
Fibrous Dysplasia
Fibrous dysplasia develops almost exclusively inchildren in the first two decades of life, though thedisease may progress well into adulthood. It is adeforming but not destructive disease of bone andis caused by proliferation of fibrous tissue andosteoid in medullary bone.
Three forms are described: monostotic fibrousdysplasia accounts for most cases of orbitalinvolvement; in polyostotic disease, deformities oflong bones occur together with skull lesions; andMcCune-Albright syndrome which is a triad ofpolyostotic fibrous dysplasia, sexual precocity andcutaneous pigmentation (with ‘coast of Maine’borders).
Most patients present with facial asymmetry,proptosis and globe displacement progressingover many years. Associated symptoms includediplopia, anosmia, hearing defects, nasal obstructionand epiphora.8 Increased intracranial pressure andcranial nerve palsies can also occur. Extensive diseaseresults in a deformed facies known as ‘leontiasisossea’.
Progressive disease can result in optic nervecompression. Acute compressive neuropathy mayoccur secondary to intralesional hemorrhage,sphenoidal sinus mucocoele or secondary aneurysmalbone cyst.3
Imaging shows expansion of the bone withthinning of the overlying cortex. A ‘ground-glass’appearance is common on CT. The disease usuallyaffects multiple orbital bones, extending across suturelines.
The main differential diagnosis is hyperostoticmeningioma, which occurs in an older age group,and is differentiated on imaging by the presence ofa soft tissue component.
Histopathology shows a loose, moderatelycellular fibrous stroma containing spicules ofwoven bone often with characteristic ‘C’ or‘Chinese character’ shapes. Osteoblastic activity isinconspicuous.6
As the natural history of the lesion is usually oneof slow progression, a conservative approach tomanagement is recommended, unless functional
basm
ala
blog
(alw
ays o
rigin
al)

182182182182182 Surgical Atlas of Orbital DiseasesSurgical Atlas of Orbital DiseasesSurgical Atlas of Orbital DiseasesSurgical Atlas of Orbital DiseasesSurgical Atlas of Orbital Diseases
Figures 13.1A to D: A 19-year-old male presented with a dull headache and a swelling in the region of the left upper lid. On clinical examination(A), fullness was noted above the left medial canthus with downward displacement of the globe. A bony-hard mass could be palpated in theleft superomedial orbit. Computed tomographic scan (B and C) revealed a highly circumscribed radio-opaque mass with a bosselated contouroccupying the frontal sinus and extending into the left superonasal orbit. The bone window settings (B and C) demonstrated the radiolucenttrabecular center surrounded by a dense periphery, characteristic of an osteoma. Surgical removal was performed using a stereotacticassisted sino-orbital approach. The sinus component was removed by a nasal endoscopic approach following a modified Lothrop procedure.The orbital component was drilled out through an external skin-crease approach. (D). The patient made an uneventful recovery followingsurgery
deficits develop. Surgical treatment requires amultidisciplinary craniofacial approach, with removalof as much of the affected bone as possible andreconstruction of the resulting defect in a singleoperation.9
CASE ILLUSTRATION (Figures 13.2A to D)
Ossifying Fibroma
This is a lesion peculiar to craniofacial bones. Themandible is the site of predilection but the orbit(usually the roof) may rarely be involved.6 It usually
presents in the first two decades of life with a veryslowly progressive displacement of the globe.Imaging shows a well circumscribed lesion erodingthe bone with a sclerotic margin and foci of internalcalcification.
Histopathology reveals trabeculae of bone andosteoid lined by osteoblasts in a cellular stroma.6 A‘psammomatoid’ variant is described, in whichossicles remniscent of psammoma bodies are seen.10
This variant shows more aggressive behavior andhas a greater risk of recurrence following incompleteexcision.
A B
C D
basm
ala
blog
(alw
ays o
rigin
al)

Bone Tumors of OrbitBone Tumors of OrbitBone Tumors of OrbitBone Tumors of OrbitBone Tumors of Orbit 183183183183183
Figures 13.2A to D: This 22-year-old female presented with progressive decrease of vision in the left eye. Clinical examination revealed facialbony asymmetry with prominent frontal ridges (A). On cutaneous examination (B), a large nevus with the so-called “coast of Maine” borderswas seen. Computed tomographic scan (C) showed extensive expansion of craniofacial bones extending across suture lines, with a “ground-glass” appearance. These features are consistent with a diagnosis of polyostotic fibrous dysplasia (McCune-Albright syndrome). As thedisease was causing visual compromise, left optic nerve decompression was performed via a craniotomy. Histology shows the typical C-shaped trabeculae of woven bone (D, arrow) set in a cellular fibrous stroma
It is important to distinguish ossifying fibromafrom fibrous dysplasia as the former lesion is moreaggressive, and left alone, inexorably enlarges andmay enter into the cranium. As incomplete excisionfrequently leads to recurrence6, complete surgicalexcision is the treatment of choice.
Osteoblastoma
This is a benign tumor composed of osteoblasts andis extremely rare in the orbit.11 It affects patients inthe second to third decades and presents with aslowly progressive proptosis and globe displacement.The reported cases have arisen from the roof and
ethmoid sinuses and imaging shows an osteolyticlesion larger than 1 cm with a sclerotic margin.Histologically, trabeculae of lamellar bone withosteoblastic rimming are seen. The histologicalappearance is indistinguishable from that of osteoidosteoma (a lesion seen in long bones and measuringless than 1 cm in diameter).6 Surgical excision is thetreatment of choice.
Chondroma
Chondromas are benign cartilaginous tumors thatmay rarely be encountered in the orbit, usually nearthe orbital rim or trochlea.12 Radiologically, they are
A B
C D
basm
ala
blog
(alw
ays o
rigin
al)

184184184184184 Surgical Atlas of Orbital DiseasesSurgical Atlas of Orbital DiseasesSurgical Atlas of Orbital DiseasesSurgical Atlas of Orbital DiseasesSurgical Atlas of Orbital Diseases
seen as dense, well circumscribed masses. Onhistology, they are composed of lobules of maturecartilage.13 Excision is curative.
Cholesterol GranulomaCholesterol granuloma is a foreign body responseto the presence of crystallized cholesterol. Itcommonly involves the middle ear and temporalbone, but the orbit may rarely be affected. In theorbit, it occurs almost exclusively in the superolateralfrontal bone.14, 15
Males in the fourth to fifth decades of life arepredominantly affected. The usual presentation is thatof a slowly progressive superolateral mass resultingin inferior globe displacement, proptosis and diplopiain upgaze. There may be associated headache or painand a history of trauma may be elicited in somepatients.
CT imaging demonstrates an osteolytic lesionexpanding and eroding the frontal bone andextending into the orbit and intracranially.14, 15 WithMRI, high signal intensities are seen on both T1 andT2 weighted images (similar to dermoid cysts).
Histology is characterised by the presence ofnumerous cholesterol clefts and an associated foreignbody giant cell reaction.
Curettage of the lesion via a percutaneousapproach is curative. An endoscope may be helpfulin visualizing areas behind the superior orbital rim.16
CASE ILLUSTRATION (Figures 13.3A to F)
Aneurysmal Bone Cyst
This cystic lesion of the bone is rare in the orbit andusually presents with a painless proptosis in thesecond decade of life.17 Sudden progression mayoccur following an intralesional hemorrhage. Imagingshows a destructive, expansile bony lesion usuallyinvolving the roof of the orbit. Curettage of the lesionis curative and histological examination shows bloodfilled fibrous spaces that lack an endothelial lining.Hemosiderin laden macrophages and bony trabeculaeare seen in the fibrous stroma surrounding thespaces.3
Giant Cell Lesions
A histological picture dominated by giant cells is seenin three different lesions: giant cell tumor, giant cellgranuloma and ‘brown tumor’ of hyperpara-thyroidism. Giant cell tumor or osteoclastoma isusually seen in epiphyses of long bones and affectspatients between the ages of 25-40 years.6 Ituncommonly involves the paranasal sinuses and cansecondarily impinge upon the orbit.6 Histology showsevenly scattered multinucleated giant cells containingbetween 10-100 nuclei. The stromal cells containnuclei resembling those of the giant cells.6 En blocexcision is usually curative.
Giant cell granuloma, also known as giant cellreparative granuloma, is a rare destructive lesion ofbone that presents with proptosis and globedisplacement.18 Headache and pain may also bepresent. In contrast to giant cell tumor, giant cellgranuloma is seen in younger patients (average age18.6 years) and on histology, the giant cells are sparseand unevenly distributed and reactive new boneformation may be seen.6 This lesion responds wellto curettage.
‘Brown tumor’ is histologically almostindistinguishable from giant cell granuloma.Clinically, however, it is associated with primary orsecondary hyperparathyroidism. The increasedosteoclastic activity leads to focal areas of boneresorption and hemorrhage. As treatment ofhyperparathyroidism usually results in spontaneoushealing of the bony lesion, it is important that a carefulclinical evaluation is performed in patients withhistology suspicious for ‘brown tumor’.19
Osteogenic Sarcoma
Osteogenic sarcoma of the orbit is rare and is seen inthe 4th and 5th decades of life in patients who haveusually undergone previous radiotherapy forretinoblastoma or fibrous dyplasia.6 Primary orbitalinvolvement is exceedingly rare.20 It develops rapidlyover a period of weeks to months and can presentwith proptosis, pain, diplopia and visual impairment.Imaging shows a mixed lytic and sclerotic mass withindistinct margins. Histology shows sarcomatous
basm
ala
blog
(alw
ays o
rigin
al)

Bone Tumors of OrbitBone Tumors of OrbitBone Tumors of OrbitBone Tumors of OrbitBone Tumors of Orbit 185185185185185
Figures 13.3A to F: This 50-year-old male presented with a 6-month history of right proptosis. Examination (A) showed 2 mm proptosis with3 mm inferior displacement of the right eye. Computed tomographic scan (B) revealed an osteolytic lesion involving the right superolateral frontalbone. On magnetic resonance imaging, the mass showed high signal intensity on the T1-weighted image (C). The T2-weighted image showeda similar appearance. Based on the clinical and radiological findings, a diagnosis of cholesterol granuloma was made. Anterior orbitotomy wasperformed through an upper lid skin crease incision (D). A friable mass was seen protruding from beneath the superior orbital rim (arrow) andthe lesion was curetted out. The portion of the lesion behind the superior orbital rim and abutting the dura was removed using endoscopicvisualization. Histology (E) showed the characteristic cholesterol clefts (arrow) surrounded by a granulomatous inflammation. The patientmade an excellent recovery (F)
cells in a stroma with foci of osteoid formation.6
Treatment is by preoperative chemotherapy followedby resection and postoperative chemotherapy.The prognosis for craniofacial lesions, however, ispoor.
A
B
C
D
E
F
basm
ala
blog
(alw
ays o
rigin
al)

186186186186186 Surgical Atlas of Orbital DiseasesSurgical Atlas of Orbital DiseasesSurgical Atlas of Orbital DiseasesSurgical Atlas of Orbital DiseasesSurgical Atlas of Orbital Diseases
Chondrosarcoma
These are slow-growing, non-metastasizing locallyaggressive tumors commonly arising in the paranasalsinuses and invading the orbit.13 Imaging reveals awell-defined osteolytic lesion with internal stippling.Multiple lobules of hypercellular cartilage withbinucleate cells in lacunae and mitotic figures are seenon microscopy. Treatment is by radical resection butcomplete removal may not be possible in thecraniofacial region and multiple recurrences may beseen.13
Mesenchymal Chondrosarcoma
This variant of chondrosarcoma has a predilectionfor the head and neck region. It may occur in thesoft tissues of the orbit, almost exclusively in femalesin the second and third decades of life.21 The clinicalcourse is rapid and patients present with proptosisand infiltrative effects of less than a year’s duration.Imaging shows a non-specific, irregular, mottled softtissue mass. On histology areas of poorly differ-entiated mesenchymal cells intermixed with lobulesof mature cartilage are seen. As metastasis, especiallyto the lungs, can occur, exenteration is the treatmentof choice.21
Ewing’s Sarcoma
This is a small round cell tumor of bone mainlyaffecting patients in the first two decades. Orbitalinvolvement is usually by metastases or spread fromadjacent areas (Ewing’s sarcoma is responsible for10% of pediatric orbital metastasis). Primary Ewing’ssarcoma of the orbit is exceedingly rare.22 Clinically,a rapidly developing non-axial proptosis is noted andimaging reveals expansile mass with bonedestruction. Microscopy shows a featureless smallround cell proliferation. PAS positive glycogengranules may be seen in the cytoplasm. Immuno-histiochemistry (for CD99) is helpful in making thediagnosis. Treatment is by chemotherapy followedby resection or radiotherapy.
MyelomaMultiple myeloma or solitary plasmacytoma mayinvolve the orbit, usually in patients older than 50years of age.23 Presentation is with subacute onset ofpain and proptosis. An osteolytic area with acontiguous soft tissue mass is seen on imaging.Histology shows sheets of malignant plasma cells.The orbital lesions are treated with radiotherapy andchemotherapy is used for systemic disease.
Langerhans’ Cell Histiocytosis (LCH)LCH results from an abnormal proliferation ofLangerhans’ cells- specialized histiocytic cellsnormally seen in the epidermis and characterised by‘racquet-shaped’ cytoplasmic granules (Birbeckgranules) on electron microscopy. One form of LCH,previously known as eosinophilic granuloma,preferentially affects the skull and presents as alocalized lytic lesion of bone. The disease is usuallyseen in young males and the children classicallypresent with proptosis secondary to a superolateralorbital lesion.24 On CT, a central radiolucent area withan enhancing rim is seen. Histologically, agranulomatous infiltrate with Langerhans’ cells andprominent eosinophils is observed. The treatmentof choice is curettage, though intralesional steroidinjections and low-dose radiotherapy have also beenused. An endoscopic aided curettage may achievecomplete removal of the lesion.
CASE ILLUSTRATION (Figures 13.4A to D)Intraosseous HemangiomaThis is a rare vascular tumor which presents as aslowly developing orbital mass, often associated withpain or tenderness.25 The frontal bone is usuallyaffected and on CT, a well-defined, radiolucent massthat expands the inner and outer tables of the boneis seen. Histologically, the lesions are hemangiomascomposed of thin-walled vascular spaces lined byendothelium. Treatment is by surgical excision of thelesion with a rim of normal bone. Preoperativeangiography should be performed.
basm
ala
blog
(alw
ays o
rigin
al)

Bone Tumors of OrbitBone Tumors of OrbitBone Tumors of OrbitBone Tumors of OrbitBone Tumors of Orbit 187187187187187
Figures 13.4A to D: This 5-year-old boy presented with a 3-week history of pre-septal cellulitis involving the left upper lid that had failed torespond to antibiotics (A). A computed tomographic scan revealed an irregular, osteolytic lesion involving the left frontal bone and extendingthrough the roof of the orbit into the anterior cranial fossa (B). This lesion was approached via an upper lid skin crease incision. The periosteumwas reflected off the roof of the orbit and endoscopic visualization was used to effect safe curettage of the entire lesion, including from areasabutting the dura (C); long arrow: superior orbital rim; short arrow: dura). Histology (D) showed a polymorphic inflammatory infiltrate withpredominance of eosinophils, characteristic of Langerhans cell histiocytosis. Staging showed this to be unifocal, unisystem disease and he hadno further treatment. There was no recurrence of the disease after a 3-year follow up (Figure 13.4D courtesy of Prof T.Y. Khong, Adelaide)
CASE ILLUSTRATION (Figures 13.5A to C)
A B
C D
A
basm
ala
blog
(alw
ays o
rigin
al)

188188188188188 Surgical Atlas of Orbital DiseasesSurgical Atlas of Orbital DiseasesSurgical Atlas of Orbital DiseasesSurgical Atlas of Orbital DiseasesSurgical Atlas of Orbital Diseases
Figures 13.5A to C: A 57-year-old female presented with a one-year history of a mass over the left forehead that was gradually increasingin size. She was otherwise asymptomatic. Examination revealed a bony mass over the left frontal-orbital region. Ophthalmic examinationrevealed a 2 mm inferior displacement of the left globe. A computed tomographic scan showed a mass lesion within the left frontal bone. Intensecontrast enhancement of the lesion was seen (A). Magnetic resonance demonstrated intermediate T1 and high T2 signal intensity (B). Biopsyof the mass was performed by the neurosurgeon and revealed an intraosseus cavernous hemangioma (C). Postoperative angiographyshowed that the lesion was supplied by the ethmoidal branches of the left ophthalmic artery and by the left middle meningeal artery. The supplywas too small for embolization and the patient has been under observation for the last 3 years, with no further symptoms
REFERENCES
1. Rootman J, Chang W, Jones D. Distribution and differentialdiagnosis of orbital disease. In: Rootman J, ed. Diseases ofthe orbit, 2nd ed. Philadelphia: Lippincott Williams andWilkins, 2003;53-84.
2. Shields JA, Bakewell B, Augsburger JJ, Flanagan JC.Classification and incidence of space-occupying lesions ofthe orbit: a survey of 645 biopsies. Arch Ophthalmol1984;102:1606-11.
3. Selva D, White VA, O’Connell JX. Primary bone tumors ofthe orbit. Surv Ophthalmol 2004;49:328-42.
4. Henderson JW. Fibro-osseus, osseus, and cartilaginoustumors of orbital bone. In: Henderson JW, ed. Orbitaltumors, 3rd ed. Philadelphia: Raven Press, 1994.
5. McNab AA,. Orbital osteoma in Gardner’s syndrome. AustNZ J Ophthalmol 1998;26:169-70.
6. Fu YS, Perzin KH. Nonepithelial tumors of the nasal cavity,paranasal sinuses and nasopharynx: a clinicopathologicstudy. II. Osseus and fibro-osseus lesions, includingosteoma, fibrous dysplasia, ossifying fibroma,osteoblastoma, giant cell tumor, and osteosarcoma. Cancer1974;33:1289-305.
7. Chen C, Selva D, Wormald PJ. Endoscopic modified lothropprocedure: an alternative for frontal osteoma excision.Rhinology 2004;42:239-43.
8. Katz BJ, Nerad JA. Ophthalmic manifestations of fibrousdysplasia. Ophthalmology 1998;105:2207-15.
9. Jackson IT, Hide TA, Gomuwka PK, et al. Treatment ofcranio-orbital fibrous dysplasia. J Maxillofac Surg1982;10:138-41.
10. Margo CE, Weiss A, Habal MB. Psammomatoid ossifyingfibroma. Arch Ophthalmol 1986;104:1347-51.
11. Leone CR, Lawton AW, Leone RT. Benign osteoblastomaof the orbit. Ophthalmology 1988;95:1554-8.
12. Jepson CM, Wetzig PC. Pure chondroma of the trochlea.Surv Ophthalmol 1966;11:656-9.
13. Fu YS, Perzin KH. Non-epithelial tumors of the nasal cavity,paranasal sinuses and nasopharynx: a clinicopathologicstudy. III. Cartilaginous tumors (chondroma, chondro-sarcoma). Cancer 1974;34:453-63.
14. Arat YO, Chaudhry IA, Boniuk M. Orbitofrontal cholesterolgranuloma: distinct diagnostic features and management.Ophthal Plast Reconstr Surg 2003;19:382-7.
15. McNab AA, Wright JE. Orbitofrontal cholesterolgranuloma. Ophthalmology 1990;97:28-32.
16. Selva D, Chen C. Endoscopic approach to orbitofrontalcholesterol granuloma. Orbit 2004;22:49-52.
17. Ronner HJ, Jones IS. Aneurysmal bone cyst of the orbit: areview. Ann Ophthalmol 1983;15:626-9.
18. Spraul CW, Wojno TH, Grossniklaus HE, Lang GK.Reparative giant cell granuloma with orbital involvement.Klin MonatsblAugenheilkd 1997;211:133-4.
19. Parrish CM, O’Day DM. Brown tumor of the orbit. ArchOphthalmol 1986;104:1199-202.
B C
basm
ala
blog
(alw
ays o
rigin
al)

Bone Tumors of OrbitBone Tumors of OrbitBone Tumors of OrbitBone Tumors of OrbitBone Tumors of Orbit 189189189189189
20. Parmar DN, Luthert PJ, Cree IA, et al. Two unusual osteogenicorbital tumors: presumed parosteal osteosarcomas of theorbit. Ophthalmology 2001;108:1452-6.
21. Guccion R, Font R, Enzinger F, Zimmerman L. Extraskeletalmesenchymal chondrosarcoma. Arch Pathol 1973;95:336.
22. Guzowski M, Tumuluri K, Walker DM, Maloof A. Primaryorbital Ewing sarcoma in a middle-aged man. Ophthal PlastReconstr Surg 2005;21:449-51.
23. Rodman HI, Font RL. Orbital involvement in multiplemyeloma: review of the literature and report of three cases.Arch Ophthalmol 1972;87:30-5.
24. Jordan DR, McDonald H, Noel L, Nizalik E. Eosinophilicgranuloma. Arch Ophthalmol 1994;111:134-5.
25. Relf S`J, Bartley GB, Unni KK. Primary orbital intraosseushemangioma. Ophthalmology 1991;98:541-7.
basm
ala
blog
(alw
ays o
rigin
al)
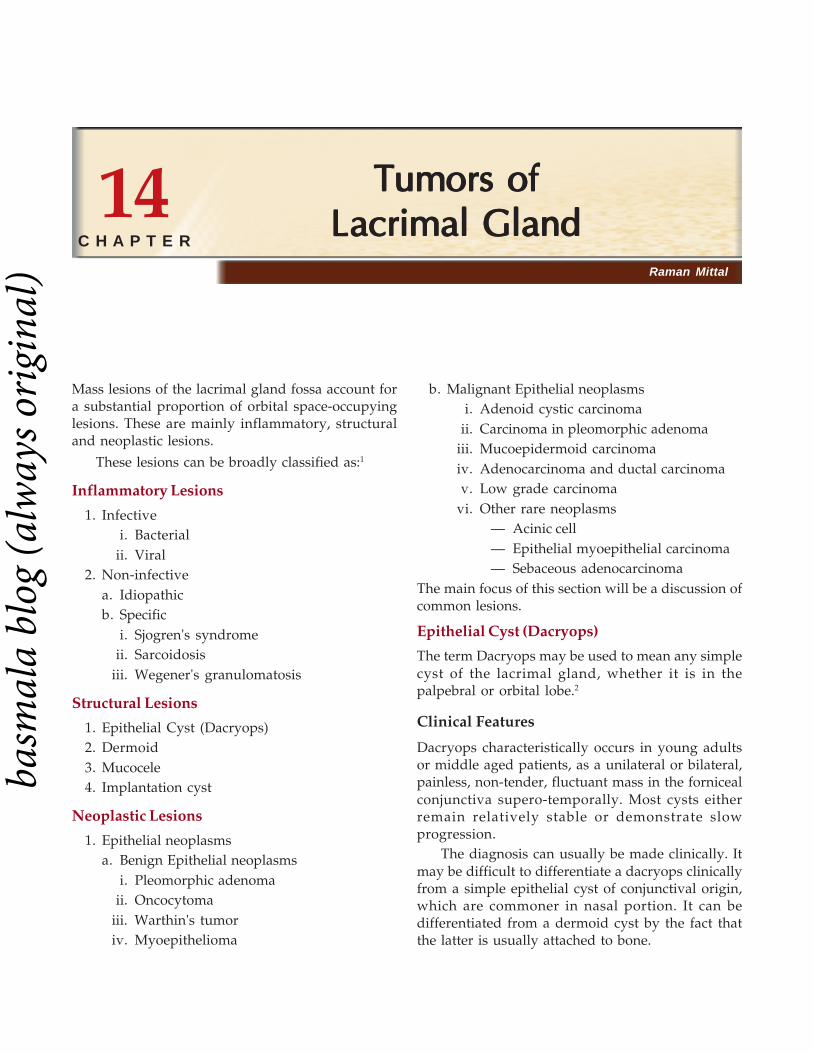
190190190190190 Surgical Atlas of Orbital DiseasesSurgical Atlas of Orbital DiseasesSurgical Atlas of Orbital DiseasesSurgical Atlas of Orbital DiseasesSurgical Atlas of Orbital Diseases
Raman Mittal
Tumors ofTumors ofTumors ofTumors ofTumors ofLacrimal GlandLacrimal GlandLacrimal GlandLacrimal GlandLacrimal Gland
Mass lesions of the lacrimal gland fossa account fora substantial proportion of orbital space-occupyinglesions. These are mainly inflammatory, structuraland neoplastic lesions.
These lesions can be broadly classified as:1
Inflammatory Lesions
1. Infectivei. Bacterial
ii. Viral2. Non-infective
a. Idiopathicb. Specific
i. Sjogren's syndromeii. Sarcoidosis
iii. Wegener's granulomatosis
Structural Lesions
1. Epithelial Cyst (Dacryops)2. Dermoid3. Mucocele4. Implantation cyst
Neoplastic Lesions
1. Epithelial neoplasmsa. Benign Epithelial neoplasms
i. Pleomorphic adenomaii. Oncocytoma
iii. Warthin's tumoriv. Myoepithelioma
b. Malignant Epithelial neoplasmsi. Adenoid cystic carcinoma
ii. Carcinoma in pleomorphic adenomaiii. Mucoepidermoid carcinomaiv. Adenocarcinoma and ductal carcinomav. Low grade carcinoma
vi. Other rare neoplasms— Acinic cell— Epithelial myoepithelial carcinoma— Sebaceous adenocarcinoma
The main focus of this section will be a discussion ofcommon lesions.
Epithelial Cyst (Dacryops)
The term Dacryops may be used to mean any simplecyst of the lacrimal gland, whether it is in thepalpebral or orbital lobe.2
Clinical Features
Dacryops characteristically occurs in young adultsor middle aged patients, as a unilateral or bilateral,painless, non-tender, fluctuant mass in the fornicealconjunctiva supero-temporally. Most cysts eitherremain relatively stable or demonstrate slowprogression.
The diagnosis can usually be made clinically. Itmay be difficult to differentiate a dacryops clinicallyfrom a simple epithelial cyst of conjunctival origin,which are commoner in nasal portion. It can bedifferentiated from a dermoid cyst by the fact thatthe latter is usually attached to bone.
14C H A P T E R
basm
ala
blog
(alw
ays o
rigin
al)

Tumors of Lacrimal GlandTumors of Lacrimal GlandTumors of Lacrimal GlandTumors of Lacrimal GlandTumors of Lacrimal Gland 191191191191191
Figures 14.1A and B: Mr V, with clear, cystic lesions(Dacryops) in both eyes
Pathology and Pathogenesis
Grossly, the classic dacryops is a round cyst thatcontains clear fluid (tears) and is lined by epithelium.The epithelium may consist of one or two layers ofrelatively flat cells similar to those found in a lacrimalgland duct, or it may be composed of nonkeratinizingstratified epithelium with goblet cells similar to thosein the conjunctiva. Normal lacrimal gland tissue isusually identified in the histologic specimen adjacentto the cyst.
It is believed that a dacryops results fromobstruction of one of the secretory ducts of thelacrimal gland.3 The obstruction results in progressivedilatation of the duct with formation of a thin walledcyst.
Management
When a dacryops is small and asymptomatic notreatment is necessary. If it is larger and symptomatic,it can be managed by simple aspiration. Aspirationcan lead to recurrence, so it is advisable to removethe lesion surgically using either a conjunctivalapproach or a lateral orbitotomy.
Prognosis
The prognosis for vision and life is excellent.Complications associated with a dry eye may occurif an excessive amount of lacrimal gland tissue andduct is removed.
CASE ILLUSTRATIONS
Case 1
Mr V, 47 years male, presented with complaints ofrecurring redness and itching in both eyes. The patienthad been diagnosed earlier as a case of allergicconjunctivitis and was treated accordingly. He alsohad small, round, non-tender, cystic lesions in thelacrimal gland area on both the sides. So the patientwas diagnosed to be a case of dacryops in both eyesand was advised excision. (Figures 14.1A and B).
Pleomorphic AdenomaPleomorphic adenoma is the most common benignepithelial tumor of the lacrimal gland. Typically theyoccur at a younger age (2nd-5th decades) thanmalignant tumors.
Clinical FeaturesThe characteristic presentation is of a slowlyprogressive (more than a year), painless proptosis,downward globe displacement and swelling ofthe upper lid, unassociated with inflammatorysigns or symptoms. Larger tumors may indent theglobe and cause blurring of vision and maycause diplopia. The common signs consist ofproptosis, usually non-tender, palpable mass inthe superotemporal quadrant, downward andinward globe displacement and sometimes restrictedupgaze. Fundus examination may show globeindentation in larger tumors and also choroidalfolds sometimes.
A
B
basm
ala
blog
(alw
ays o
rigin
al)

192192192192192 Surgical Atlas of Orbital DiseasesSurgical Atlas of Orbital DiseasesSurgical Atlas of Orbital DiseasesSurgical Atlas of Orbital DiseasesSurgical Atlas of Orbital Diseases
ImagingPleomorphic adenoma is best seen on CT scan.Usually a well circumscribed, homogenous orheterogenous, moderate to markedly enhancing softtissue mass lesion is seen in the area of lacrimal gland.The scans may show pressure indentation over globeand expansion of the lacrimal fossa, suggestingchronicity of the lesion, in most cases. The mass mayhave few hyperdense areas suggestive of calcification.Ultrasound may reflect the histologic pattern with ahighly reflective pseudocapsule, cystic spaces, and awell demarcated mass.
Pathology and PathogenesisThe pleomorphic adenoma of the lacrimal gland ischaracteristically firm, grayish-white, encapsulatedand bosselated mass on gross examination.Histologically, the tumor is composed of bothepithelial and mesenchymal elements. The epithelialelements take the form of ducts, cords and squamouspearls. The mesenchymal elements usually includemyxoid and chondroid tissue and sometimes osseoustissue. The diverse patterns of two componentsaccount for the name, pleomorphic adenoma. Animportant feature is the presence of microscopicnodular extensions into the pseudocapsule. This mayaccount for the tendency of the tumor to recur whenappropriate margins are not taken. The pathogenesisis not clear. It appears that both the cellular andstromal elements are derived from epithelial cellslining the acini and ducts.
ManagementIf there is a strong clinical suspicion of the lacrimalgland tumor being pleomorphic adenoma, on thebasis of slow growing lesion, and absence of pain,motility disturbance and bony expansion, then it isbest to excise the tumor completely without capsularrupture and without a prior incisional biopsy.Incomplete excision or capsular rupture may lead toa recurrence, sometimes with malignant trans-formation. Therefore, an incisional biopsy is probablycontraindicated if the diagnosis is strongly suspectedclinically.
The most appropriate approach is by a modifiedlateral orbitotomy. The important aspects are widesurgical exposure, excision of the periorbita, carefulmanipulation of the tumor to avoid rupture, removal
of a margin or adjacent tissue, and where possible,preservation of the uninvolved palpebral lobe(reducing the incidence of postoperative filamentarykeratopathy).
PrognosisThe prognosis of the patient with pleomorphicadenoma of the lacrimal gland is generally verygood. It is likely that greater attention to a completeen bloc excision will decrease the chance ofrecurrence and malignant transformation.
Case 2
Ms P, 20 years female, presented to me withprotrusion of the right eyeball for 1 year, associatedwith reduced visual acuity. She had graduallyincreasing non-axial proptosis of the right eyeball.As you see in the figure (Figure 14.2A) the eyeballwas displaced down and in. I could palpate a hard,non-reducible mass in the right supero-temporalorbit. There was neither tenderness nor any sign ofinflammation. The mass was not pulsatile. Theextraocular motility of right eye was restricted inupgaze, dextroelevation and dextroversion. Anteriorsegment of both the eyes were within normal limits,but the fundus of the right eye had folds of theinternal limiting membrane, suggesting indentationof the globe by tumor.
Her CT scan (Figures 14.3A and B) showed afairly well defined orbital mass in the area of lacrimalgland. The mass was indenting over the globe. Nobony erosions could be seen. The moulding of theorbital wall contours suggested chronic and benignnature of the lesion.
My clinical diagnosis was right lacimal glandtumor, most probably a pleomorphic.
Adenoma: I did lateral orbitotomy to excise offthe tumor completely. Cryoextraction of the tumorwas done. It was a well encapsulated grayish whitemass measuring 2.6 × 2 × 1.5 cm. (Figure 14.4A). Grossexamination of the cut section showed grayish andchalky white areas and also cystic areas filled withmucin material.
Histopathologic examination (Figure 14.4B)showed a dimorphic picture with epithelial andstromal cells in close proximation. There wereglandular and dilated cystic spaces lined by double
basm
ala
blog
(alw
ays o
rigin
al)

Tumors of Lacrimal GlandTumors of Lacrimal GlandTumors of Lacrimal GlandTumors of Lacrimal GlandTumors of Lacrimal Gland 193193193193193
Figures 14.3A and B: Axial and coronal sections of the CT scan showing fairly well defined orbital mass in the area of lacrimal gland
Figure 14.4A: Picture of the excised lacrimal gland tumor Figure 14.4B: Photomicrograph of pleomorphic adenoma (H and E stain)
Figure 14.2A: Ms P, Non-axial proptosis right eye Figure 14.2B: Well aligned eyes postoperatively
Figures 14.2A and B: Clinical picture of Ms P. Preoperative picture (A) showing non-axial proptosis of the right eyeball. Theglobe has been displaced downwards and inwards. Postoperative picture (B) showing that both the eyes are now well aligned
A B
A B
basm
ala
blog
(alw
ays o
rigin
al)

194194194194194 Surgical Atlas of Orbital DiseasesSurgical Atlas of Orbital DiseasesSurgical Atlas of Orbital DiseasesSurgical Atlas of Orbital DiseasesSurgical Atlas of Orbital Diseases
layered cuboidal cells with secretions in the lumen.Stroma consisted of basaloid cells with spindleappearance, indistinct cell borders with elongatedvesicular nucleus with stellate pattern. Therewas abundant myxoid matrix in between the stromalcells.
These all histopathologic features confirmed thediagnosis of Pleomorphic Adenoma of LacrimalGland, right orbit. Postoperatively, proptosisresolved completely (Figure 14.2B).
Case 3
Mr K, 50 years old male presented to us with severepain, swelling and redness of right periocular areafor 15 days. He gave the history of graduallyincreasing painful protrusion of the right eyeball forabout a month for which he underwent evisceration2 weeks back. On examination, I could palpate amoderate to hard mass filling the supero-temporaland temporal part of right orbit. The lids and adnexawere inflamed with conjunctival chemosis (Figure14.5A). CT scan orbit was done which showed a wellcircumscribed, soft tissue mass in the supero-lateralquadrant of right orbit (Figures 14.6A and B). Themass was mildly enhancing on contrast. There wereno bony erosions. A disfigured globe (S/Pevisceration) was seen. So, now clinically, thesequence of events that I thought was; the patienthad gradually progressing lacrimal gland tumor(most probably pleomorphic adenoma) which leadto severe proptosis with exposure keratopathy and/
or perforated corneal ulcer. The previous surgeonhad addressed the corneal complication byperforming evisceration, without tackling theprimary cause, i.e. lacrimal gland tumor.
I did lateral orbitotomy to excise off the tumorcompletely. Cryoextraction of the tumor wasperformed (Figure 14.7). Histopathologic exami-nation of this well encapsulated tumor showed cellsarranged in dimorphic pattern. The backgroundshowed myxoid stroma in between. These featureswere consistant with Pleomorphic Adenoma ofLacrimal Gland, right orbit. He was provided witha prosthesis after the postoperative edema subsidedand the patient was comfortable (Figure 14.5B).
Adenoid Cystic Carcinoma
Adenoid Cystic Carcinoma (ACC) is the mostcommon malignant epithelial tumor of the lacrimalgland. It has a tendency for bimodal occurrence i.e.more common in 2nd and 4th decades.
Clinical Features
The most important feature is a short duration ofonset, i.e. usually few months. Generally patients alsocomplain of having persisting pain, usually associatedwith paresthesia. Other clinical features include thosewhich are seen in other lacrimal gland tumors as well.To enumerate, these are; a mass lesion in supero-temporal quadrant, proptosis, downward and nasaldisplacement of the globe, ptosis and decreasedvisual acuity.
Figure 14.5A: Preoperative picture of Mr K. Note the Figure 14.5B: Postoperative appearance of patient withsuperior sulcus fullness readymade ocular prosthesis
basm
ala
blog
(alw
ays o
rigin
al)

Tumors of Lacrimal GlandTumors of Lacrimal GlandTumors of Lacrimal GlandTumors of Lacrimal GlandTumors of Lacrimal Gland 195195195195195
Figures 14.6A and B: Axial and coronal sections of CT scan orbit show a well defined masslocated at the lacrimal gland area of right orbit
Figure 14.7: Gross appearance of the lacrimal gland tumor (Pleo-morphic adenoma) along with a bone piece from lateral orbital wall
ImagingCT scan is the imaging modality of choice. Animportant feature (that differentiates many malignantlesion from a benign one) is bony erosions orosteolytic changes in the adjacent bone. Otherfeatures that help me to say that the lacrimal glandtumor is Adenoid Cystic Carcinoma are irregularmargins of the lesion and its extension towards theorbital apex. But on CT scan, the lesion may actuallyappear to be a well defined, solid and fairlyhomogenous and hence can be easily confused witha benign lesion. Presence or absence of calcificationdoesn't help much. In MRI, the T2 weighted images
may show the tumor as isointense to brain andextraocular muscles.
Pathology and PathogenesisOn gross examination, adenoid cystic carcinomas areusually grayish white, firm and may give a falseimpression of being circumscribed or pseudo-encapsulated. Histopathologically, ACC has solidareas or cords of malignant epithelial cells. It can bedivided into several histologic subtypes:
1. Cribriform (Glandular or Swiss cheese) pattern: Showsmultiple lobules with many small clear spaces,giving it a cribriform appearance.
2. Sclerosing variant: Consists of hyalinizedcylinders of connective tissue and elongatedepithelial cords, surrounded by a densehyalinized stroma.
3. Basaloid variant: Shows solid epithelial lobuleswith large basophilic nuclei and scantycytoplasm that resembles the lobules seen inbasal cell carcinoma.
4. Comedocarcinoma variant: Shows epithelial lobuleswith large foci of central necrosis.
5. Tubular (Ductal) variant: Is composed ofelongated and comma shaped epithelial tubuleslined by two or three layers of cells.
In practical terms, cribriform is the most commonpattern. Basaloid pattern is the least common but ismost aggressive and therefore has the worstprognosis.
A B
basm
ala
blog
(alw
ays o
rigin
al)

196196196196196 Surgical Atlas of Orbital DiseasesSurgical Atlas of Orbital DiseasesSurgical Atlas of Orbital DiseasesSurgical Atlas of Orbital DiseasesSurgical Atlas of Orbital Diseases
Figure 14.8: Clinical picture showing left eye enophthalmos withptosis status post lateral orbitotomy (Note eyebrow scar) Figure 14.9: Clinical picture 4 weeks after ptosis correction
ManagementThe mainstay of managing ACC remains completesurgical excision with adjuvant radiotherapy andchemotherapy. For very well defined lesions, localexcision with the adjacent bone removal should bedone; for not so well defined lesions, orbitalexenteration and for tumors that have extended intothe bone or soft tissues of the orbit, radical en blocorbitectomy by a multidisciplinary team should bedone. As it is difficult to ensure complete tumorexcision, surgery should be followed by adjuvantradical external beam radiotherapy. This EBRT mayprevent or delay local recurrence.
The role of local, regional or systemicchemotherapy remains unclear in what is essentiallyan indolent tumor. We used a combination ofcarboplatin or cisplatin with 5-fluorouracil ordoxorubicin in our patients as postoperative adjuvanttherapy.4 Among all the treatment options,chemotherapy has the greatest potential to eradicateoccult metastatic disease.
PrognosisWhat so ever we may do, the prognosis of adenoidcystic carcinoma remains dismal. The usual clinicalcourse of ACC is painful local and regional recurrencefollowed by distant metastasis, usually to the lungs.Tumor can recur even at a very late date (even 20years later). Most patients die within 5 years ofrecurrence.
Case 4
This patient Mrs B, 18 years old female, presentedto me with left blepharoptosis and mildenophthalmos. She gave the history of orbitotomydone elsewhere on left side for orbital tumor (as isevident from eyebrow scar in the picture) (Figure14.8), about 5 years back. Old CT scan report (CTscan films were not available) suggested inhomo-genous soft tissue mass in supero-lateral quadrantof left orbit. There was orbital fossa formationwithout bony erosions or intracranial extension. Shewas not aware of previous diagnosis nor was anyhistopathologic report available. I did TarsofrontalSling (Silicon rod sling) for her and advised her forCT scan orbits and regular follow up to rule out anytumor recurrence in future (Figure 14.9).
But the patient was lost to follow up for about18 months, and therefter reported with massiveproptosis and exposure keratopathy which had sub-acute onset (Figures 14.10A and B). CT scan done atthis stage revealed a large heterogenous mass in thesupero-lateral aspect of left orbit (Figures 14.11A andB). The mass was large enough to end just short oforbital apex. Roof of the left orbit appeared erodedat places but no obvious bony breach or intracranialextension was seen.
Clinical and radiological findings suggested thatI was dealing with a recurrence of Lacrimal GlandTumor, and that too a malignant one. I sent a
basm
ala
blog
(alw
ays o
rigin
al)

Tumors of Lacrimal GlandTumors of Lacrimal GlandTumors of Lacrimal GlandTumors of Lacrimal GlandTumors of Lacrimal Gland 197197197197197
Figures 14.10A and B: Patient presenting with massive proptosis and exposure keratopathy of left eye caused by a large lesion inlacrimal gland area
Figures 14.11A and B: Axial and Coronal sections of CT scan orbit show a large heterogenous mass located at the lacrimal glandarea of left orbit, ending just short of orbital apex. Note the bony erosions caused by the lesion
small tissue for cytology which strongly favored thediagnosis of Adenoid Cystic Carcinoma. Finally, I didlid sparing orbital exenteration (Figure 14.12A)and sent the specimen for histopathologic examination.
Histopathologic examination (Figure 14.12B)showed tumor cells arranged in cribriform pattern
with abundant mucoid matrix in extracellular spaces.The features were consistant with Adenoid CysticCarcinoma of lacrimal gland. The patient wasreferred to an oncologist to rule out systemicmetastasis and give adjuvant radiotherapy andchemotherapy.
A B
A B
basm
ala
blog
(alw
ays o
rigin
al)

198198198198198 Surgical Atlas of Orbital DiseasesSurgical Atlas of Orbital DiseasesSurgical Atlas of Orbital DiseasesSurgical Atlas of Orbital DiseasesSurgical Atlas of Orbital Diseases
Figures 14.12A and B: Exenterated specimen (A) showing cribriform pattern of adenoid cystic carcinoma (H and E stain) (B)
REFERENCES
1. Diseases of Orbit, Textbook, 2nd Edition, Rootman J,Lippincott Williams and Wilkins, Chapter - Neoplasia, Page344-45.
2. Bullock JD, Fleishman JA, Rosset JS: Lacrimal ductal cysts.Ophthalmol 1986;93:1355-60.
3. Smith S, Rootman J: Lacrimal ductal cysts. Presentationand management. Surv Ophthalmol 1986;30:245-50.
4. Muthy R, et al. Adenoid Cystic Carcinoma of theLacrimal Gland: Management and Outcome. (Unpublisheddata).
A B
basm
ala
blog
(alw
ays o
rigin
al)

Cystic Lesions of OrbitCystic Lesions of OrbitCystic Lesions of OrbitCystic Lesions of OrbitCystic Lesions of Orbit 199199199199199
Cystic Lesions of OrbitCystic Lesions of OrbitCystic Lesions of OrbitCystic Lesions of OrbitCystic Lesions of Orbit
Cystic lesions of the orbit are not uncommon. A trueorbital cyst is any closed cavity or sac within thebony orbital confines that is lined with epitheliumand contains a liquid or semisolid materials.1 Thecysts may be developmental or acquired.
Developmental cysts
• Dermoid / Epidermoid• Cytic teratomas• Encephalocele• Congenital cystic eye• Perioptic hygromas.
Acquired cysts
• Dacryops• Mucocele• Dacryocele or amniontocele• Hematic cyst• Simple retention cysts• Epithelial implantation cysts• Chocolate cysts• Parasitic cysts like cysticercosis and hydatid
cyst• Cystic degeneration of certain tumors like
lymphangiomas, optic nerve gliomas andschwannomas.
Another classification proposed by Shields JA andShields CL2 for pediatric cystic lesions of the orbit isas follows:
1. Cysts of surface epithelium: These are furtherdivided into:
• Simple epithelial cyst (Epidermal,conjunctival and apocrine gland cysts)
• Dermoid cysts (Epidermal and conjunctivalcysts).
2. Neural cysts: Further divided as:• Those associated with ocular maldevelop-
ment like congenital cystic eye andcolobomatous cyst.
• Those associated with brain and meningealtissues like cephalocele and optic nervemeningocele.
3. Secondary cysts: The most important secondarycyst is mucocele occurring in children secondaryto cystic fibrosis.
4. Inflammatory cysts: These include parasitic cystslike cysticercosis and hydatid cyst.
5. Noncystic lesions with cystic component: Theseinclude certain tumors like adenoid cysticcarcinoma, rhabdomyosarcomas and lymphan-giomas.
Parasitic encystment is more often aninflammatory granuloma. Hematic cysts are not linedwith epithelium but with a fibrous encapsulation ofblood or blood products. Malignant epithelialneoplasm that secondarily invades the orbit maydevelop central necrosis.
Parasitic cysts is being dealt as a separate chapterin this book. Cystic degeneration of tumors isdiscussed in their respective chapters.
Golam Haider, Subrahmanyam Mallajosyula, Mohd Javed Ali
15C H A P T E R
basm
ala
blog
(alw
ays o
rigin
al)

200200200200200 Surgical Atlas of Orbital DiseasesSurgical Atlas of Orbital DiseasesSurgical Atlas of Orbital DiseasesSurgical Atlas of Orbital DiseasesSurgical Atlas of Orbital Diseases
Figure 15.1: A 9 months old female child with cystic swelling inlower part of orbit
attached to the overlying skin. In adulthood dermoidcysts may have a more posterior location.7 Theposterior located cysts may be difficult to palpate.Proptosis and globe displacement are common. Longstanding dermoid in the superior orbit maycompletely erode the roof and become adherent toduramater. Rarely an orbital cyst may pass throughbony sutureline to extend intracranially or into thetemporal fossa. Pressure placed on the extracranialportion of such a bilobed cyst may be transmittedthrough the bony dehiscence into the orbit and is acause for the mastication proptosis reported byBullock.8
Less commonly, orbital inflammation may be thepresenting sign due to leakage of oil or keratin fromthe cysts.
Expansion of the dermoid cyst and inflammatoryresponse to leakage may results in an orbitalcutaneous fistula, usually following incompletesurgical removal.
Investigations
CT scan may show a heterogenous lesion with rimenhancement, calcification, fossa formation in thebone (Figure 15.2), bone erosion, bone sclerosis andintracranial extension.
MRI
Particularly important to see the cystic nature of thelesion when the cyst present as an inflammatoryorbitopathy with surrounding tissue reaction.
DERMOID AND EPIDERMOID CYSTS
Dermoid cysts are among the most commonperiorbital tumors presenting in childhood3,4
(Figure 15.1). Its, incidence is 33% of all orbital cysts.Dermoid and Epidermoid cysts are choriostomasthat arise from subcutaneous epidermal rests orepidermal tissues trapped along bony suture linesduring embryonic development.
These cysts are present congenitally and enlargeprogressively. The superficial cysts are symptomaticin childhood but deeper dermoid may not beclinically symptomatic till in adulthood. Theepidermoid enlarges and develops into a cyst linedwith stratified squamous epithelium, which usuallyis attached to the fronto-zygomatic suture supero-temporally or to the naso-frontal suture supero-nasally. If the cyst wall contains skin appendages suchas hair follicles, sweat glands or sebaceous glands,the cysts are termed as dermoid cyst.5
If skin appendages are absent, the cysts aretermed as epidermoid cyst.6 Preseptal orbitaldermoid cyst occurs most commonly in the area oflateral brow adjacent to fronto-zygomatic suture.Duane's experience is that these cysts have occurredwith equal frequency both nasally and temporally.Medial lesions in the infant should be distinguishedfrom congenital encephaloceles or amniontoceles.
The mass is painless, smooth, ovoid to round inshape and firm to rubbery in consistency (Figure15.4). It is immobile, being relatively attached to theperiostium of the underlying suture. But it is not
Figure 15.2: CT scan of left orbit showing cystic space inlower part of orbit
basm
ala
blog
(alw
ays o
rigin
al)

Cystic Lesions of OrbitCystic Lesions of OrbitCystic Lesions of OrbitCystic Lesions of OrbitCystic Lesions of Orbit 201201201201201
Figure 15.3: Inferior orbitotomy for complete removal of cyst
Figure 15.4: Dermoid cyst after removal
Figure 15.5: Case 5 days postoperatively
Treatment
Surgical excision is the treatment of choice. Superficialcyst in childhood can be excised through an incisiondirectly over the lesion or preferably through upperlid crease. A posteriorly located cyst may requiremore careful planning for an approach through ananterior or lateral orbital route9,10 (Figure 15.3).
Cysts located along the superior orbital roof withintracranial extension needs neurosurgical consul-tations and possible transcranial approach.11,12 It isimportant to keep the cyst wall intact during surgery.Intraoperative rupture with release of its contentsmay incite granulomatous inflammation. When aninadvertent rupture occurs operating area must beflooded with irrigating solution. Complete removalof the cyst wall is curative (Figures 15.4 and 15.5).Incomplete removal may lead to recurrence.9
TERATOMAS
Like dermoids teratomas are congenital tumor andchoristomas.13,14 Dermoid and epidermiod cysts aredeveloped from one germ layer but teratomas arisefrom two or more germ layers, including ectodermand endoderm or mesoderm or both.15 Tumors maypresent at any age, many at or shortly after birth.Elsewhere teratomas are common in the gonads,mediastinum and pineal area. More than 50 cases havebeen reported in the orbit.16,17
Histologically, the tissues are usually maturedand consist of ectoderm represented by keratinized
squamous epithelium and adnexal glandularstructures; mesoderm by fibrous tissue, cartilage, fat,muscle and or bone; endoderm by gastrointestinalmucosa and glandular tissue and neuroectoderm bymature brain.16,17
Indication for surgery is unacceptable cosmeticappearance to the patient. One should preserve theglobe whenever possible.18 Incomplete removal leadsto recurrence. Exenteration is sometimes preferredbecause of fear of malignancy.15
CEPHALOCELE
A congenital dehiscence in the bony cranium mayenable the meningeal tissue to herniate into the orbitforming cystic structure filled with CSF – an orbitalmeningocele. If brain protrudes inside the sac the
basm
ala
blog
(alw
ays o
rigin
al)

202202202202202 Surgical Atlas of Orbital DiseasesSurgical Atlas of Orbital DiseasesSurgical Atlas of Orbital DiseasesSurgical Atlas of Orbital DiseasesSurgical Atlas of Orbital Diseases
condition is termed as meningo-encephalocele. It maybe fronto-ethmoidal or sphenoidal.19,20
Presentation is usually during infancy andchildhood. It may present with pulsatile proptosis.Common site is superomedial aspect of the orbit. Themass is soft in consistency. The size of mass isincreased by straining, bending forward or weightlifting. The direction of proptosis is inferotemporal.It may present with enophthalmos due tocompression of orbital contents.21
Following conditions may be associated withencephalocele:22
1. Neurofibromatosis2. Hypertelorism3. Malar or orbital bone depression4. Optic atrophy5. Optic nerve coloboma6. Optic nerve glioma7. Microphthalmos8. Morning-glory syndrome.
Radiological Finding
CT scan may show defect in the anterior cranial fossa.3-dimensional coronal views can detect encephaloceleeasily. When associated with sphenoid bonedysplasia, enlargement of superior orbital fissure inplain film appear as "Bare orbit". CT scan may revealan enlarged middle cranial fossa. The temporal lobeof brain may herniate through the whole posteriororbit. Enlargement of pituitary fossa and optic canalmay be associated with these bony defects.22
Treatment
Surgical treatment is indicated in cases of exposureand lagophthalmos. Excision of small encephalocelethrough transfrontal craniotomy may be done. For alarger encephalocele, dural patching and bonegrafting can be done.22
MICROPHTHALMOS WITH CYST
Microphthalmos with orbital cyst result from thefailure of the choroidal fissure to close in embryo.This condition may be unilateral or bilateral. Thepresence of an orbital cyst may be beneficial forstimulating normal growth of the involved orbitalbone and eyelid. The cyst is lined internally by gliotic
retina and externally by fibrous envelop. The cystsare usually located in inferior orbit and cause thelower lid to bulge. In almost all cases resulting eye isdefective, smaller than normal and has an attachedcystic mass at birth.23,24
The cyst may be smaller or larger than the eye.Cyst is bluish in color and translucent, and maydisplace the globe. In contrast congenital cystic eyeresults from failure of optic vesicle to involute.The eye is filled with both solid and cystic form ofdysplastic neuroglial tissue.25 The cyst is connectedto the brain by an astrocytic filled stalk, but it doesnot communicate to the anterior ventricle.
Both microphthalmos with cyst and conge-nital cystic eye should be distinguished fromcystic teratoma and encephalocele by imagingstudies.26
Management of microphthalmos with cyst andcongenital cystic eye involves excision of the cystsand or globe along with abnormal neuroepithelialtissue.27 There has been a lot a work done on the useof sclerosing agents in such cysts. Ethanolamine oleatesclerotherapy may be an effective minimal inter-vention treatment option for cosmetic rehabilitationof patients with orbitopalpebral cyst associated withcongenital microphthalmos with no visualpotential.28,29
Each lesion is self centered and often an orbitalimplantation be placed and a prosthesis fitted to orbitin a satisfactory cosmetic effect. Sometimes removalof bone and reconstruction of the socket may be done.
MUCOCELE
Destruction of sinus ostium due to recurrentinflammation, trauma or intensive mucosal diseaseresult in a mucous filled sinus or mucocele which canexpand slowly to involve the orbital cavity. If thesinus is inflamed and the cyst contain pus or mucous,the term pyocele and mucopyocele respectively,apply. It may occur at any age, most common inbetween (40-70) years. Mucocele from frontal-ethmoidal sinus are most common. The enlargementof the mucocele is insidious, with proptosis anddisplacement of the globe being manifest inassociation with a palpable, smooth wall mass in theupper and inner quadrant of the orbit. Mucocele ofthe posterior orbit may present more insidiously with
basm
ala
blog
(alw
ays o
rigin
al)

Cystic Lesions of OrbitCystic Lesions of OrbitCystic Lesions of OrbitCystic Lesions of OrbitCystic Lesions of Orbit 203203203203203
a complaint of headache and orbital discomfort. Themucocele arises in the sphenoidal sinus andpostethmoidal air cells and may mimic retrobulbarneuritis, or cause ophthalmoplegia and ptosis byaffecting branches of 3rd cranial nerve along withaxial proptosis.30,31
The differential diagnosis of cystic medial orbitallesion must also include encephalocele with skull basedeformity.
Appearance of a typical mucocele on a CT scanincludes bowing of the sinus wall into the orbit, withattenuation or even erosion of bone with a cysticcavity. MRI shows highly variable signal intensities.
Treatment of mucocele is surgical for re-establishment of normal drainage, removal of thelining of the cyst. Frontal and ethmoidal mucoceleare approached sub-periosteally with elevation of anosteoplastic flap32; eradication and extirpation of alldiseased mucosa is done. Successful endoscopic sinusobliteration and or re-establishing sinus drainageprotects against recurrence.33 Sphenoidal sinusmucocele is approached intranasally. Neurosurgicalconsultation is indicated for those mucoceles withintracranial extension.34,35
CYSTS OF THE OPTIC NERVE SHEATH
Dilatation and expansion of the optic nerve sheathhas been observed in variety of neoplastic and non-neoplastic condition. Such a cystic growth in a opticnerve sheath filled with CSF has been perioptichygroma, arachnoid cyst of the optic nerve sheath,optic hydrops and meningocele.36,37 Most perioptichygromas present in patients between the ages of30-60yrs with complaints of headache and visualdisturbance. Optic nerve signs are defective vision,RAPD, optic disc edema, optic atrophy andvisual field defects. The cyst can be well delineatedin MRI with fat suppression technique andgadolinium contrast.
HEMATIC CYST
Hematic cyst refers to the accumulation ofhematogenous debris within a cavity lined withfibrous tissue but not epithelial or endothelialtissue.40,41
It can occur at any age. It should be distinguishedfrom endothelial-lined blood containing cyst such aschocolate cyst associated with lymphangioma, venousvarices and hemangioma. Hematic cysts areuncommon. Proptosis, globe displacement, motilitydisturbance may occur due to chronic hematic cyst(Figure 15.6). Spontaneous eyelid ecchymosis andedema may suggest this diagnosis. In acute casesthere may be decrease in vision, RAPD and choroidalfolds.42, 43
Hematic cyst may be due to trauma and anincompletely reabsorbed orbital hemorrhage, whereinthe presence of old blood and blood breakdownproduct incite a granulomatous inflammation andfibrous encapsulation. Others believe that a cyst arisesfrom bleeding within the bony diploes that breaksout into the peripheral space.44
Investigations
Plain film may show bony erosion when cyst arisesin the superior orbit and involve the orbital portionof the frontal bone. CT shows well-defined non-enlarging mass (Figure 15.7) having the same densityas the brain. On MRI T1 and T2 weighted signal hyperintensity are constant with blood.45
Treatment
Surgical evacuation of the cyst content, removal ofthe fibrous wall lining and establishment ofmeticulous hemostasis to prevent recurrence.Removal of one wall of the cyst often is all that isnecessary and all that is attached to the orbital tissuecan be left intact (Figures 15.8 and 15.9).
basm
ala
blog
(alw
ays o
rigin
al)

204204204204204 Surgical Atlas of Orbital DiseasesSurgical Atlas of Orbital DiseasesSurgical Atlas of Orbital DiseasesSurgical Atlas of Orbital DiseasesSurgical Atlas of Orbital Diseases
Simple Cyst
Simple cyst may include serous, retention andimplantation cyst. These are rare in the orbit but areslightly more common in the eyelid and conjunctiva.This cyst is lined by simple epithelium.
Retention CystIt originates in the glandular appendages of theconjunctiva and adnexal structure. Obstruction of theorifice of the lacrimal gland or accessory lacrimalgland from trauma or cicatrix may result in a thinwalled epithelium lined cyst in the superior fornixthat can cause mass effect.
Lacrimal Ductal CystIt arises often in the supero-lateral orbit and can beeasily seen by everting the upper lid. These arefrequently bilateral,46 they present as round lesionsoriginating from the palpebral portion of the lacrimalgland which protrudes into the superior fornix.Marsupialization may be preferable to completeexcision, because attempt to excise the cyst mayunnecessarily close the remaining lacrimal ductalcyst.47,48 Ductal cysts can rarely arise from accessorylacrimal glands.49
Figure 15.9: Postoperative appearance 3 weeks after the operation
Figure 15.8: Surgical approach for removal of hematic cyst
Figure 15.7: CT scan shows well defined mass in the orbital apex
Figure 15.6: A 15 year girl with cystic swelling inthe superior orbital region
basm
ala
blog
(alw
ays o
rigin
al)

Cystic Lesions of OrbitCystic Lesions of OrbitCystic Lesions of OrbitCystic Lesions of OrbitCystic Lesions of Orbit 205205205205205
Implantation CystIt arises from misplacement of surface epithelium intothe orbit as a result of trauma or surgery. It is difficultto eradicate due to variable depth. Removal of theentire cyst or electrodessication of the epithelial liningeffects a cure.50
DACRYOCELE
Distension of the nasolacrimal sac by entrappedmucoid material results in the formation of adacryocele due to obstruction of the nasolacrimalduct. A congenital dacryocele manifests at birth as afirm bluish swelling in the medial canthal area at orbelow the medial canthal tendon. Lacrimal sac is tenseand filled with mucous and dacryocystitis with orwithout cellulitis may be a frequent presentation.51
Surgical indications are dacryocystitis, cellulitis,recurrent dacryocystitis, difficulties in breathing inlarge nasal cyst, failure to respond to conservativetreatment. Difficulties in diagnosis of congenitaldacryocele include - encephalocele, mucocele,dermoid cyst, and capillary hemangioma. Congenitaldacryocele should be conservatively managedinitially and if there is no response probing shouldnot be delayed.52,53 Adult dacryocele needs dacryo-cysto-rhinostomy (DCR) surgery.53, 54
REFERENCES
1. Henderson JW, Farrow GM: Orbital Tumors, 2nd ed. NewYork, Brian C Decker, 1980.
2. Shields JA, Shields CL. Orbital cysts of childhoodclassification, clinical features and management. SurvOphthalmol. 2004;49(3):281-99.
3. Stefanyszyn MA, Handler SD, Wright JE: Pediatric orbitaltumors. Otolaryngol Clin North Am 1988;21:103.
4. Pfeiffer RL, Nicholl R J: Dermoid and epidermoid tumorsof the orbit. Arch Ophthalmol 1948;40:639.
5. Ahuja R, Azar NF. Orbital dermoids in children. SeminOphthalmol. 2006;21(3):207-11.
6. Yanoff M, Fine BS: Ocular Pathology: A Text and Atlas, 3rded. Philadelphia, JB L ippincott, 1989.
7. Rootman J: Diseases of the Orbit: A MultidisciplinaryApproach. Philadelphia, JB Lippincott, 1988.
8. Bullock JD, Bartley GB: Dynamic proptosis. Am JOphthalmol 1986;102:104.
9. Yen KG, Yen MT. Current trends in the surgicalmanagement of orbital dermoid cysts among pediatricophthalmologists. J Pediatr Ophthalmol Strabismus.2006;43(6):337-40; quiz 363-4.
10. Pryor SG, Lewis JE, Weaver AL, Orvidas LJ. Pediatricdermoid cysts of the head and neck. Otolaryngol HeadNeck Surg. 2005;132(6):938-42.
11. Srivastava U, Dakwale V, Jain A, Singhal M. Orbital dermoidcyst with intracranial extension. Indian J Ophthalmol.2004;52(3):244-6.
12. Yuen HK, Chong YH, Chan SK, Tse KK, Chan N, Lam DS.Modified lateral orbitotomy for intact removal of orbitaldumbbell dermoid cyst. Ophthal Plast Reconstr Surg.2004;20(4):327-9.
13. Duke-Elder S: System of Ophthalmology, Vol XIII, Normaland Abnormal Development: Part II. CongenitalDeformation. St. Louis, CV Mosby, 1963.
14. Levin ML, Leone CR Jr, Kincaid MC: Congenital orbitalteratomas. Am J Ophthalmol 1986;102:476.
15. Thomas J, Gregory L, Louis B. Orbital Neoplasm. Orbit,Eyelid and Lacrimal System. American Academy ofOphthalmology, 2004-2005;Section 7.64.
16. Lee GA, Sullivan TJ, Tsikleas GP, Davis NG Congenitalorbital teratoma. Aust N Z J Ophthalmol. 1997;25(1):63-6.
17. Gnanaraj L, Skibell BC, Coret-Simon J, Halliday W, ForrestC, DeAngelis DD. Massive congenital orbital teratoma.Ophthal Plast Reconstr Surg. 2005;21(6):445-7.
18. Chang DF, Dallow RL, Walton DS: Congenital orbitalteratoma: Report of a case with visual preservation. JPediatr Ophthalmol Strabismus 1980;17:88.
19. Mahapatra AK, Agrawal D. Anterior encephaloceles: aseries of 103 cases over 32 years. J Clin Neurosci.2006;13(5):536-9. Epub 2006 May 6.
20. Mahapatra AK, Suri A. Anterior encephaloceles: a study of92 cases. Pediatr Neurosurg. 2002;36(3):113-8.
21. Macfarlane R, Rutka JT, Armstrong D, Phillips J, Posnick J,Forte V, Humphreys RP, Drake J, Hoffman HJ.Encephaloceles of the anterior cranial fossa. PediatrNeurosurg. 1995;23(3):148-58.
22. Raman Sharma R, Mahapatra AK, Pawar SJ, Thomas C, Al-Ismaily M. Trans-sellar trans-sphenoidal encephaloceles:report of two cases. J Clin Neurosci. 2002;9(1):89-92.
23. Waring GO III, Roth AM, Rodrigues MM: Clinicopathologiccorrelation of microphthalmos with cyst. Am J Ophthalmol1976;82:714.
24. Lieb W, Rochels R, Gronemeyer U: Microphthalmos withcolobomatous orbital cyst: Clinical, histological,immunohistological, and electron microscopic findings. BrJ Ophthalmol 1990;74:59.
25. Chaudhry IA, Shamsi FA, Elzaridi E, Arat YO, Riley FC.Congenital cystic eye with intracranial anomalies: aclinicopathologic study. Int Ophthalmol. 2007;27(4):223-33.Epub 2007 Apr 24.
26. Brodic G E. Cystic Lesion of the Orbit In:Principle andPractice of Ophthalmology 2nd ed. WB SaundersCompany, 2000 pp 3072.
27. Doglietto F, Massimi L, Dickmann A, Tamburrini G,Caldarelli M, Di Rocco C. Microphthalmia andcolobomatous cyst of the orbit. Acta Neurochir (Wien).2006;148(10):1123-5. Epub 2006 Sep 8.
basm
ala
blog
(alw
ays o
rigin
al)

206206206206206 Surgical Atlas of Orbital DiseasesSurgical Atlas of Orbital DiseasesSurgical Atlas of Orbital DiseasesSurgical Atlas of Orbital DiseasesSurgical Atlas of Orbital Diseases
28. Naik MN, Murthy RK, Raizada K, Honavar SG.Ethanolamine oleate sclerotherapy in the management oforbito-palpebral cyst associated with congenitalmicrophthalmos. Am J Ophthalmol. 2005;139(5):939-41.
29. Naik MN, Honavar SG, Murthy RK, Raizada K, Thomas R.Ethanolamine Oleate Sclerotherapy Versus Simple CystAspiration in the Management of Orbitopalpebral CystAssociated With Congenital Microphthalmos. Ophthal PlastReconstr Surg. 2007;23(4):307-11.
30. Ajaiyeoba A, Kokong D, Onakoya A. Clinicopathologic,ophthalmic, visual profiles and management of mucoceles.J Natl Med Assoc. 2006;98(1):63-6.
31. Herndon M, McMains KC, Kountakis SE. Presentation andmanagement of extensive fronto-orbital-ethmoidmucoceles. Am J Otolaryngol. 2007;28(3):145-7.
32. Ulualp SO, Carlson TK, Toohill RJ. Osteoplastic flap versusmodified endoscopic Lothrop procedure in patients withfrontal sinus disease. Am J Rhinol. 2000;14(1):21-6.
33. Har-El G. Endoscopic management of 108 sinus mucoceles.Laryngoscope. 2001;111(12):2131-4.
34. Peral Cagigal B, Barrientos Lezcano J, Floriano Blanco R,García Cantera JM, Sánchez Cuéllar LA, Verrier HernándezA. Frontal sinus mucocele with intracranial and intraorbitalextension. Med Oral Patol Oral Cir Bucal. 2006;1;11(6):E527-30.
35. Shah A, Meyer DR, Parnes S. Management offrontoethmoidal mucoceles with orbital extension: isprimary orbital reconstruction necessary? Ophthal PlastReconstr Surg. 2007;23(4):267-71.
36. Harris GJ, Sacks JG, Weinberg PE, O'Grady RB: Cyst of theintraorbital optic nerve sheaths. Am J Ophthalmol1976;81:656.
37. Miller NR, Green WR: Arachnoid cysts involving a portionof the intraorbital optic nerve. Arch Ophthalmol1975;93:1117.
38. Moschos MM, Lymberopoulos C, Moschos M. Arachnoidcyst of the optic nerve: a case report. Klin MonatsblAugenheilkd. 2004;221(5):408-9.
39. Akor C, Wojno TH, Newman NJ, Grossniklaus HE.Arachnoid cyst of the optic nerve: report of two cases andreview of the literature. Ophthal Plast Reconstr Surg.2003;19(6):466-9.
40. Krohel GB, Wright JE: Orbital hemorrhage. Am JOphthalmol 1979;88:254.
41. Pearson PA, Rakes SM, Bullock JD: Letter: Clinicopathologicstudy of hematic cysts of the orbit. Am J Ophthalmol1986;102:804.
42. Milne HL 3rd, Leone CR, Kincaid MC, Brennan MW.Chronic hematic cyst of the orbit. Ophthalmology.1987;94(3):271-7.
43. Privat C, Bellamy J, Courthaliac C, Kinn T, Ravel A, MondieJ, Bacin F, Boyer L. Chronic hematic cyst of the orbit (orbitalsubperiosteal hematoma). J Radiol. 2000;81(7):811-4.
44. Cameron JD, Letson RD, Summers CG: Clinical significanceof hematic cyst of the orbit. Ophthalmic Plast ReconstrSurg 1988;4(2):95.
45. Kersten RC, Kersten JL, Bloom HR, Kulwin DR. Chronichematic cyst of the orbit. Role of magnetic resonanceimaging in diagnosis. Ophthalmology. 1988;95 (11):1549-53.
46. Tsiouris AJ, Deshmukh M, Sanelli PC, Brazzo BG. Bilateraldacryops: correlation of clinical, radiologic, andhistopathologic features. AJR Am J Roentgenol.2005;184(1):321-3.
47. Bullock JD, Fleishman JA, Rosset JS. Lacrimal ductal cysts.Ophthalmology. 1986;93(10):1355-60.
48. Brownstein S, Belin MW, Krohel GB, Smith RS, Condon G,Codere F. Orbital dacryops. Ophthalmology.1984;91(11):1424-8.
49. Khoury NJ, Haddad MC, Tawil AN, Ma'luf RN. Ductal cystsof the accessory lacrimal glands: CT findings. AJNR Am JNeuroradiol. 1999;20(6):1140-2.
50. Wuebbolt GE, Zuercher M, O'Donnell B, Collin R. Epithelialimplantation cysts of the upper eyelid after lid-loweringprocedures. Ophthalmology. 1993;100(9):1289-92.
51. Mansour AM, Cheng KP, Mumma JV, Stager DR, HarrisGJ, Patrinely JR, Lavery MA, Wang FM, Steinkuller PGCongenital dacryocele. A collaborative review.Ophthalmology. 1991;98(11):1744-51.
52. Schnall BM, Christian CJ Conservative treatment ofcongenital dacryocele. J Pediatr Ophthalmol Strabismus.1996;33(5):219-22.
53. O'Keefe M, Shaikh A, Bowell R, Lanigan B. Management ofcongenital dacryocele. Acta Ophthalmol (Copenh). 1994;72(1):122-3.
54. Rootman J. Disease of the Orbit : A MultidisciplinaryApproach. Philadelphia, JB Lippincott,1995;149.
basm
ala
blog
(alw
ays o
rigin
al)

Subrahmanyam Mallajosyula, Mohd Ather, Modini Pandarpurkar
Parasitic Cysts of OrbitParasitic Cysts of OrbitParasitic Cysts of OrbitParasitic Cysts of OrbitParasitic Cysts of Orbit
The prevalence of parasitic cysts of orbit varies greatlyin different regions of the world. For examplecysticercosis which is endemic in Asia, Latin Americaand Africa,1 is rare in North America and EuropeanCountries. Nearly 15% of proptosis we treat is due tocysticercosis! Hydatid is the next common parasiticcyst. However, in view of the wide spreadinternational travel, it is essential to know about theseconditions, as revealed by the fact that many cases ofneurocysticercosis were reported in USA.2,3
Cysticercosis: Cysticercosis is the larval form ofTaenia Solium. Man is the definitive host for TaeniaSolium. The larval form of cysticercosis occurs ininfested pig, which is the intermediate host.Cysticercosis occurs in humans when they takecontaminated food like improperly cooked oruncooked vegetables or through water.
Cysticercosis can involve many organs and sub-cutaneous tissues. Neurocysticercosis is verycommon. Extraocular cysticercosis is more frequentthan intraocular. We see 40-50 new cases of myo-cysticercosis per year while my vitreo-retinalcolleagues see 4-6 cases a year. Most often we seesolitary cysts. Multiple cysts or association withneurocysticercosis is rare.4,5 Very few cases of opticnerve involvement are reported.6,7,8
The clinical presentation of orbital cysticercosisis varied. The onset can be acute/sub-acute orintermittent. Pain and swelling can vary from severeto minimal. Ocular motility restriction and diplopiaare very common. FDT is positive. The horizontal rectiand superior rectus/LPS complex are commonly
involved. Most of the patients are young with anaverage age of 16.5 years. Myocysticercosis is the mostcommon cause of acquired ptosis in the age group of10-20 years in our series. A high degree of suspicionis needed to investigate and diagnose this condition.Anticysticercosis antibodies are positive in about 60%of cases. CT scan or Ultrasound B scan of orbit9,10 revealenlarged muscle with a cyst showing a hyper densespot within (which represents scolex). We prefer CTscan to B scan for the diagnosis, since we want to knowif there is associated neurocysticercosis.
If neurocysticercosis also coexists, we refer thepatient to neurologist. If there is no neurocysticercosis,we treat the patient with oral Albendazole 15 mg/kg.body.wt/ day in 2 divided doses for 4 weeks alongwith prednisolone. In those with severe inflammatorysigns, we prescribe Prednisolone at a dose of 2 mg/kg.body wt/ day and in others at 1 mg /kg.body wt/day, and will taper over a period of 4 weeks. We followthe patients with B scan, since it is less expensive andeasily available.
Awareness of the disease, high index of suspicionand imaging are necessary to diagnose this condition.When the disease is for several months, and is notdiagnosed and treated properly, the cyst migratesanteriorly . It can be seen in subtenon’s space, usuallyin relation to an extraocular muscle. Such cysts areexcised, which on histopathology show a highlyconvoluted membrane with scolex. These patients areinvestigated for the presence of cysticercosis elsewhereand treated acoordingly.Rarely spontaneous extrusionmay11 occur.
16C H A P T E R
basm
ala
blog
(alw
ays o
rigin
al)

208208208208208 Surgical Atlas of Orbital DiseasesSurgical Atlas of Orbital DiseasesSurgical Atlas of Orbital DiseasesSurgical Atlas of Orbital DiseasesSurgical Atlas of Orbital Diseases
When to suspect Myocysticercosis?Young patient (5-20 yrs)Stay/visit to endemic regionOnset: Acute/Subacute/IntermittentPain: Severe/moderateProptosis: Mild to moderate and eccentricOcular motility: Restricted, FDT positive,Diplopia commonSoft tissue changes: Severe/minimal.
Investigations
Serum Anticysticercosis: Positive in about 60% casesonly.Imaging: CT/MRI preferred; Enlarged extraocularmuscle with a cyst and scolex.
Treatment
Albendazole: 15mg/kg body wt/day in 2 divided doses× 4 weeks along with Prednisolone 1-2 mg/kg bodywt/ day, tapered over 4 weeks.
CASE ILLUSTRATIONS
Case 1
Miss S, an young girl of 16 years in age was referredto us with the history of pain and swelling of righteye since 2 days. She had a similar episode 2 weeksback for which the referring doctor treated her withsystemic antibiotics and she responded.
As you could see, (Figure 16.1) she presented withmarked swelling of both the lids of her right eye, upperlid being more severe. She complains of pain ofmoderate intensity. There is a slight raise of localtemperature, mild tenderness, minimal chemosis, mildproptosis and normal ocular motility (Figure 16.2).
We felt the chances of orbital infection are remotesince it is difficult to explain why an infection recursin such a short time in an otherwise healthy youngwoman. In view of the age, intermittency/ recurrence
in short time, symptoms not in proportion to the signs,myocysticercosis was our clinical diagnosis. Plain CTscan of Orbits revealed enlarged LPS-SR complex witha cyst and scolex (Figures 16.3 and 16.4), confirmingour clinical diagnosis.
She was treated with Albendazole 400 mg bid for4 weeks along with Prednisolone 90 mg/day (Her wt.was 45 kg) Since the inflammation was fairly severeas evidenced by severe edema of lids and markedlyenlarged. LPS-SR complex. We started her onPrednisolone at 2 mg/kg.body wt./day and taperedover a months time. The response was quite dramaticas you can see in the Figure 16.5 which was taken 1week after starting the medication.
Figure 16.3: Axial CT image shows enlargedLPS-SR complex enclosing a cyst
Figure 16.2: On elevating the eye lid, the eye looks normalbut for mild chemosis and minimal proptosis
Figure 16.1: Miss S, F16 presenting with severe edema of lids andswelling extending all round into periocular region of right eye
basm
ala
blog
(alw
ays o
rigin
al)
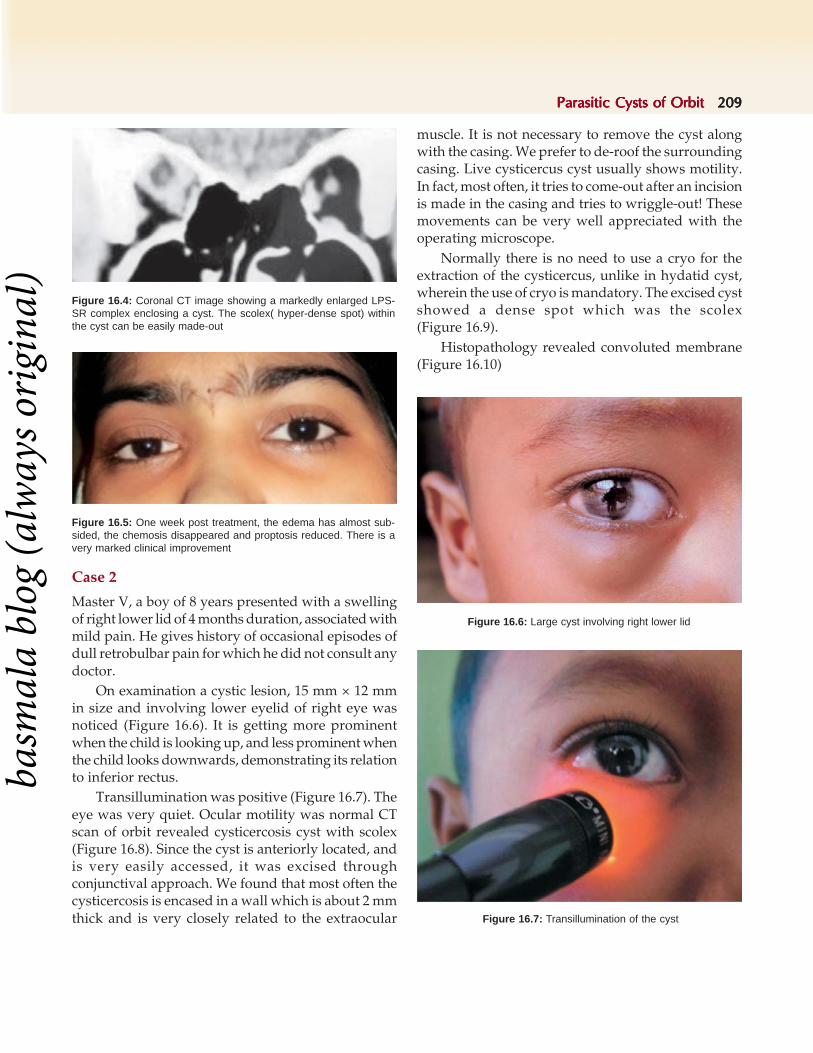
Parasitic Cysts of OrbitParasitic Cysts of OrbitParasitic Cysts of OrbitParasitic Cysts of OrbitParasitic Cysts of Orbit 209209209209209
Figure 16.4: Coronal CT image showing a markedly enlarged LPS-SR complex enclosing a cyst. The scolex( hyper-dense spot) withinthe cyst can be easily made-out
Figure 16.5: One week post treatment, the edema has almost sub-sided, the chemosis disappeared and proptosis reduced. There is avery marked clinical improvement
muscle. It is not necessary to remove the cyst alongwith the casing. We prefer to de-roof the surroundingcasing. Live cysticercus cyst usually shows motility.In fact, most often, it tries to come-out after an incisionis made in the casing and tries to wriggle-out! Thesemovements can be very well appreciated with theoperating microscope.
Normally there is no need to use a cryo for theextraction of the cysticercus, unlike in hydatid cyst,wherein the use of cryo is mandatory. The excised cystshowed a dense spot which was the scolex(Figure 16.9).
Histopathology revealed convoluted membrane(Figure 16.10)
Case 2
Master V, a boy of 8 years presented with a swellingof right lower lid of 4 months duration, associated withmild pain. He gives history of occasional episodes ofdull retrobulbar pain for which he did not consult anydoctor.
On examination a cystic lesion, 15 mm × 12 mmin size and involving lower eyelid of right eye wasnoticed (Figure 16.6). It is getting more prominentwhen the child is looking up, and less prominent whenthe child looks downwards, demonstrating its relationto inferior rectus.
Transillumination was positive (Figure 16.7). Theeye was very quiet. Ocular motility was normal CTscan of orbit revealed cysticercosis cyst with scolex(Figure 16.8). Since the cyst is anteriorly located, andis very easily accessed, it was excised throughconjunctival approach. We found that most often thecysticercosis is encased in a wall which is about 2 mmthick and is very closely related to the extraocular Figure 16.7: Transillumination of the cyst
Figure 16.6: Large cyst involving right lower lid
basm
ala
blog
(alw
ays o
rigin
al)

210210210210210 Surgical Atlas of Orbital DiseasesSurgical Atlas of Orbital DiseasesSurgical Atlas of Orbital DiseasesSurgical Atlas of Orbital DiseasesSurgical Atlas of Orbital Diseases
Case 3
Baby H, a girl of 8 years presented with painfuleccentric proptosis of left eye of 2 weeks duration. Onexamination fullness in supero-medial space with theglobe pushed down and out and severe tendernesswas present. Abduction was restricted (Figure 16.11).
In view of short duration, pain and inflammatorysigns, inflammatory /infective etiology wassuspected.
CT scan of the orbit revealed sub-periostealabscess with a cystic lesion within (Figure 16.12).
Careful examination revealed a white spot withinit representing scolex (Figure 16.13).
The subperiosteal abscess was drainedthrough superior Lynch incision. Along with pus,a cysticercosis cyst also was removed (Figures 16.14and 16.15). It is the first and the only case ofcysticercosis involving the subperiosteal space that weencountered. It is one of the rarest presentations of
Figure 16.10: Microphotograph showing convoluted membrane
Figure 16.9: Excised cyst showing hyper-dense spot
Figure 16.8: CT Orbits showing cyst with scolex
Figure 16.11: Eccentric proptosis with fullness andinflammatory signs
Figure 16.12: CT scan showing subperiosteal abscess with a cyst
basm
ala
blog
(alw
ays o
rigin
al)

Parasitic Cysts of OrbitParasitic Cysts of OrbitParasitic Cysts of OrbitParasitic Cysts of OrbitParasitic Cysts of Orbit 211211211211211
Figure 16.15: Excised cysticercosis
Figure 16.14: Incision mark on first postoperative day
Figure 16.13: Cyst with scolex
Figure 16.17: One month postoperative picture showing normalrestoration of movement
Figure 16.16: Microphotograph showingcysticercosis with suckers
cysticercosis and the only one to the best of ourknowledge and pub med search. The diagnosis wasconfirmed by histopathology (Figure 16.16).
The postoperative recovery was uneventful. Theocular motility was restored (Figure 16.17). Very faintincisional scar can be made out.
Case 4
Mrs V, female 32 years, presented with suddendiminution of vision of her right eye since 2 weeks,associated with mild pain. Examination revealed mildfullness of superior sulcus, RAPD, and normal ocularmotility. Optic disc was normal. Vision was 20/400(Figures 16.18, 16.19 and 16.20).
The possibility of retro bulbar neuritis was thoughtof. But to exclude any other pathology, CT imagingof orbit was performed which surprisingly revealed
basm
ala
blog
(alw
ays o
rigin
al)

212212212212212 Surgical Atlas of Orbital DiseasesSurgical Atlas of Orbital DiseasesSurgical Atlas of Orbital DiseasesSurgical Atlas of Orbital DiseasesSurgical Atlas of Orbital Diseases
cysticercosis involving the lateral rectus, abetting opticnerve at orbital apex (Figures 16.21 and 16.22). This isan unexpected diagnosis, since cysticercosis is rareafter 20 years, and presenting like retro bulbar neuritisis very unusual.
She was treated with oral Albendazole(15 mg/kg.body wt. in 2 divided doses /day) for 4 weeks andPrednisolone at a dose of 2 mg/kg.body wt./daytapered over a period of 4 weeks. This high dose ofprednisolone was used because of associated opticneuropathy.
The patient recovered very well. The patient'speriocular fullness disappeared. The pain subsided(Figure 16.23). Her vision improved to 20/30. However she had a inferior arcuate scotoma (Figure 16.24).
CT imaging after 4 months showed the presenceof a shrunken cyst and scolex could not be seen
Figure 16.22: Cyst abetting the optic nerve
Figure 16.23: Subsidence of periocular edema,recovery of vision to 20/30
(Figure 16.25), which means that the cyst died. Thepatient is doing well for the past 2 years.
This is a unique case scenario. Cysticercosis veryrarely causes a toxic optic neuropathy. It is rare after25 years of age. In fact at the age of 32 years, thispatient is the oldest patient of cysticercosis we havecome across so far. We never suspected the possibilityof cysticercosis in this patient, but the hunch to get aCT helped in making correct diagnosis and providecorrect treatment for this lady. We could restore hervision.
This case clearly illustrates that even those whoregularly come across cysticercosis can also miss acase, unless they are extra careful.
Figure 16.18: Shows mild periocular fullness. Her vision was 20/400. Pupil was dilated and sluggish with a significant RAPD
Figure 16.19: Showing normal abduction
Figure 16.20: Showing normal adduction
Figure 16.21: Cyst with hyper dense spot representing scolex,involving lateral rectus at the orbital apex
basm
ala
blog
(alw
ays o
rigin
al)

Parasitic Cysts of OrbitParasitic Cysts of OrbitParasitic Cysts of OrbitParasitic Cysts of OrbitParasitic Cysts of Orbit 213213213213213
Figure 16.25: CT after 4 months shows a cyst which is shrunkenand does not show the scolex
Case 5
Master R, a boy of 8 years presented with pain,proptosis, drooping of left upper eye lid, since 4 days,associated with headache and nausea and diplopia.
There was no history of convulsions, vomiting orfever (Figure 16.26).
On examination, periocular fullness, more onsuperior quadrant with eyeball pushed down,minimal congestion of conjunctiva, and restrictedocular motility in vertical gaze leading to verticaldiplopia were evident (Figure 16.27). The vision was20/20, pupil was normal and optic disc showed mildhyperemia with filling up of the cup. There were no
hemorrhages. Clinical diagnosis of myocysticercosisinvolving LPS-SR complex was made because ofpatients age, acute onset, with inflammatory signs,acquired ptosis, mild proptosis, and restricted ocularmotility. In view of headache, nausea and early discedema, the coexistence of neurocysticercosis wassuspected.
On imaging, of the orbit, (Figures 16.28 and 16.29)a markedly enlarged LPS-SR complex was noted.A large cystic lesion was seen in relation to thethickened muscles. Scolex was made out in the cyst.
Imaging of the brain confirmed our suspicion. Itrevealed the presence of a calcified cyst in the brainparenchyma (Figure 16.30) with normal architectureof the surrounding brain. Typical " Coin Lesions" withsurrounding edema of brain was noted in other parts(Figure 16.31). A total of 3 such active cysts were notedin the serial sections of the brain. The surroundingcerebral edema indicated that the cyst is live andactive. Anticysticercosis antibodies were positive at1.68 od units, as against the values of > 0.5 od unitstaken as positive. Most of the patients ofneurocysticercosis present with convulsions. Theunique features of this case are (1) absence ofconvulsions, (2) multiple cysts in the brain, three areactive and one is inactive, association of orbital andneurocysticercosis.
In view of associated neurocysticercosis the childwas referred to neurologist who treated him withAlbendazole, Prednisolone and Carbamazepam. Thechild recovered well. Six weeks after initiating thetreatment, the ptosis disappeared, and normal ocularmotility was restored.The optic disc edema subsidedcompletely. There was no recurrence during the last2 years of follow up (Figure 16.32).
Figure 16.24: Visual fields showing inferior arcuate scotoma
Figure 16.26: Periocular swelling, ptosis, mild eccentric proptosiswith the globe pushed down in a child of 8 yrs. Onset was acute
basm
ala
blog
(alw
ays o
rigin
al)
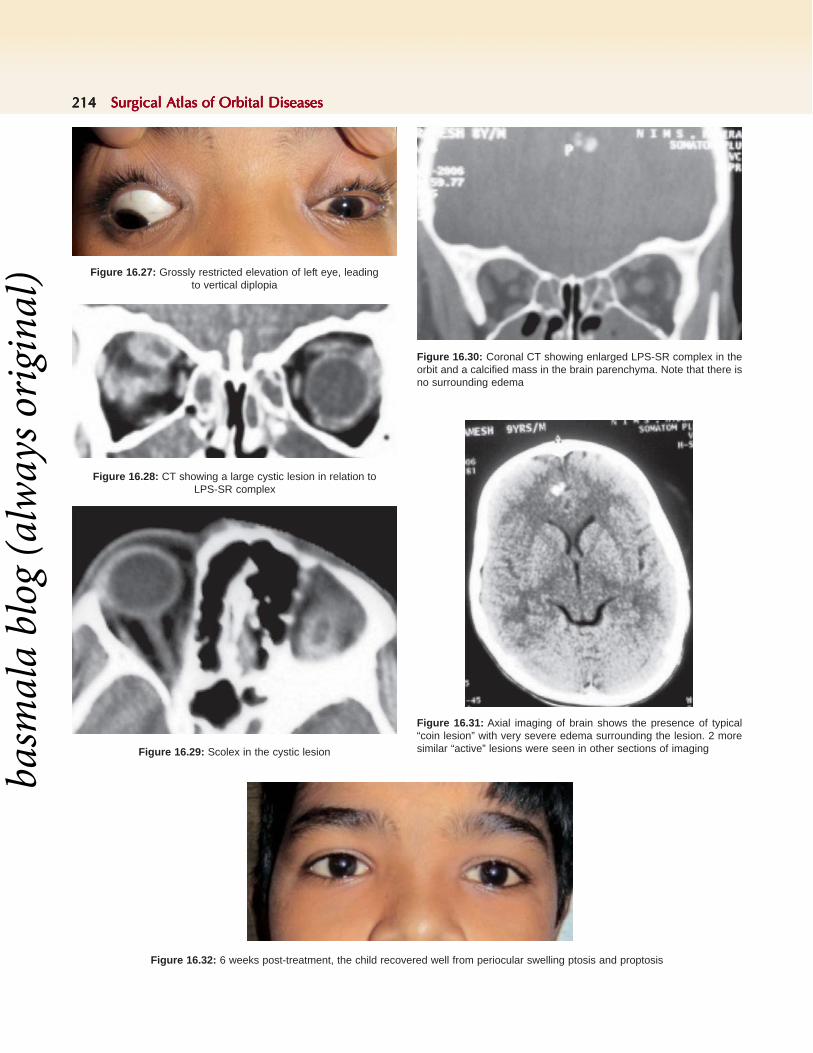
214214214214214 Surgical Atlas of Orbital DiseasesSurgical Atlas of Orbital DiseasesSurgical Atlas of Orbital DiseasesSurgical Atlas of Orbital DiseasesSurgical Atlas of Orbital Diseases
Figure 16.27: Grossly restricted elevation of left eye, leadingto vertical diplopia
Figure 16.28: CT showing a large cystic lesion in relation toLPS-SR complex
Figure 16.29: Scolex in the cystic lesion
Figure 16.30: Coronal CT showing enlarged LPS-SR complex in theorbit and a calcified mass in the brain parenchyma. Note that there isno surrounding edema
Figure 16.31: Axial imaging of brain shows the presence of typical“coin lesion” with very severe edema surrounding the lesion. 2 moresimilar “active” lesions were seen in other sections of imaging
Figure 16.32: 6 weeks post-treatment, the child recovered well from periocular swelling ptosis and proptosis
basm
ala
blog
(alw
ays o
rigin
al)

Parasitic Cysts of OrbitParasitic Cysts of OrbitParasitic Cysts of OrbitParasitic Cysts of OrbitParasitic Cysts of Orbit 215215215215215
Case 6
We wish to share our experience with a unique clinicalexperience.
Mr. S 18 years presented with a swelling on hisleft eye of 4 days duration. He is a college student,doing his graduation. He gives history of mild painand discomfort. There is no history of defective visionor diplopia. He noticed mild drooping of his left upperlid since 1 week, but did not pay attention due to hisapproaching examinations. However he noticed thismorning that the swelling has enlarged and thediscomfort has increased in intensity. His food habitsinclude eating road-side junk food, raw vegetables andgreen salads.
On examination (Figure 16.33) but for veryminimal fullness and 1 mm of ptosis of his leftupperlid,the rest looked normal. Ocular motility wasnormal (Figures 16.34 and 16.35).
On elevating the upper lid, a cyst measuring 12cm × 10 cm, and in relation to superior rectus wasseen. Surrounding conjunctiva was congested. This isthe typical appearance of cysticercosis in the sub-
Figure 16.33: Anterior segment looks almost normal
Figure 16.34: Note the cyst in relation to superior rectus muscle.Surrounding conjunctiva was congested
Figure 16.35: The ocular motility was normal. The elevation as youcan see here is full. He is orthophoric on cover test
Figure 16.36: Spontaneously extruded cysticercosis in a container
tenon's space. The cyst is always in relation to an extra-ocular muscle. Most often the surroundingconjunctiva shows congestion. Since the cyst was veryanteriorly placed, excision was planned and Mr. S wasadvised to come after 2 days to the operation roomfor excision of the cyst under local anesthesia. Heattended the operation room after 2 days, carrying asmall bottle in which he placed “something” that camefrom his affected eye that morning (Figure 16.36).
To our surprise the bottle contained cysticercosiscyst. This is an example of spontaneous extrusion.
Case 7
We are to share with you a very rare clinicalpresentation of cysticercosis, which we came acrossonly once so far. The patient, master D a young boyof 12 years, was a student of class 7, and was from a
basm
ala
blog
(alw
ays o
rigin
al)

216216216216216 Surgical Atlas of Orbital DiseasesSurgical Atlas of Orbital DiseasesSurgical Atlas of Orbital DiseasesSurgical Atlas of Orbital DiseasesSurgical Atlas of Orbital Diseases
village, 80 miles away. He was brought with a historyof sudden loss of vision of his left eye since 2 weeks.He complained of dull retro bulbar pain of 2 monthsduration. There was no history of trauma, fever orany other symptoms of systemic illness.
On examination, (Figure 16.37) there was mildproptosis of his left eye, which was more evident onNafzeiger’s (Figure 16.38). The ocular motility wasnormal. The pupil was dilated with a very significantRAPD. The vision was reduced to PL only.Retropulsion was mildly positive.
Fundus Examination revealed optic disc whichshows nasal hyperemia, and gross pallor on thetemporal side, with exudates, macular fan anddegenerative changes involving macula suggestive ofneuroretinitis (Figure 16.39).
This child was referred to us in view of proptosisof his left eye. The association between proptosis andneuroretinitis is very unusual and difficult to explain.The fundus picture was more like a neuroretinitisrather than disc edema.
We discussed about the possibilities of a fungalinfection extending from the sinuses with a vascularinvolvement, which could explain proptosis andsudden acute fall of vision (which is due to retinal
Figure 16.39: Severe macular changes including macular fan,exudates and pallor of optic disc
Figure 16.38: Proptosis of left eye is better appreciatedby Nafzeiger's test
Figure 16.37: Presents with sudden loss of vision of his left eyeFigure 16.40: Axial imaging of orbit shows a cyst in relation to optic
nerve. Scolex is seen very clearly
Figure 16.41: Cyst involving optic nerve. Scolex could be seen inthe center of the cyst
vascular obstruction) and could not explainneuroretinitis.
The possibility of cysticercosis was also discussed,but we were not for it as we did not come across sucha clinical presentation.
Imaging by CT scan of orbit showed a large cystin relation to the optic nerve and scolex could be veryclearly seen (Figures 16.40 and 16.41).
basm
ala
blog
(alw
ays o
rigin
al)

Parasitic Cysts of OrbitParasitic Cysts of OrbitParasitic Cysts of OrbitParasitic Cysts of OrbitParasitic Cysts of Orbit 217217217217217
Figures 16.42A and B: CT Scan of orbit showing a well encapsu-lated, intraconal Hydatid cyst (A) Severe proptosis and distorted globewith anterior staphyloma in a neglected case of Hydatid disease (B)
Anticysticercosis antibodies were positivewhich confirms the diagnosis of cysticercosis of opticnerve. The associated neuroretinitis was due to thesevere inflammatory response produced by the toxinsreleased, which was common with cysticercosis.
The child was treated with oral Albendazole andPrednisolone. Surgical excision of the cyst through theantero-lateral orbitotomy was not considered in viewof the severe irreversible damage already occurred,and the very poor visual prognosis. With treatment,proptosis disappeared, but his vision was absent PL.
Hydatid Cyst of Orbit
Hydatid cyst is another parasitic infestation of theorbit, less common than cysticercosis. It is caused byechinococcus granulosus or the dog tapeworm. Dogsare the primary hosts with sheep and cattle beingintermediary hosts. Humans are accidental hosts,acquiring infection by ingesting ova along with rawvegetables, contaminated water, or from direct contactwith dogs. Embryos pass across duodenal mucosa toliver through the portal veins. Liver, lungs, and brainare primarily affected. Orbital disease is seen in only1% of hydatid disease.12 Hydatid cysts form 0.3-5% ofall orbital diseases.13,14
Hydatid infestation commonly presents inchildren and young adults. Most of the patients arebelow 16 years.13 Rarely elderly people are affectedby this disease.
Proptosis is the most common presentation oforbital hydatidosis.14 Usually, the proptosis is of a fewmonths duration, associated with mild pain ordiscomfort. Hydatid cysts are commonly located inthe intraconal space. In our experience it is the mostcommon cystic lesion of intraconal space. Sinceintraconal space is the most common location, it canpresent with defective vision associated with RAPDand optic disc edema. Other causes of defective visionin hydatid cyst we came across include refractiveerrors and corneal perforation due to exposurekeratitis in one case. Other symptoms can beperiorbital pain, chemosis and headache.12 Diplopiadue to ocular motility restriction can be a raresymptom.15,16 In neglected and unattended longstanding cases, these cyst grow to a very large size,deforming the globe (Figure 16.42).17 Diagnosis is bya high index of suspicion especially in endemic areas,and investigations like CT scan orbit. Sometimes
orbital hydatid may be a part of disseminateddisease,18 with lung, liver and brain being commonlyinvolved and hence in every case of hydatid cyst,ultrasound of abdomen and CT scan of chest and brainwere advised.18,19
Investigations
• CBP- usually normal• Stool examination does not show ova or cysts• Casoni's intradermal test is positive in 75% of the
people13
• CIEP- Counter immunoelectrophoresis• Imaging techniques of importance are orbital
ultrasonography and CT scan.On ultrasound, diagnostic double wall sign is
confirmatory, spoke wheel pattern and water lily signare seen with cyst calcification.
CT scan shows well encapsulated cystic mass withcyst fluid showing attenuation values of 3-30 HU. Themass indents and deforms the globe. Calcification ofthe internal septa may be seen. We prefer CT scan ofthe orbit.
Microscopic analysis of the cyst fluid showsscolices and hooklets. The cyst wall is laminated andhas the characteristic "coats of an onion" appearance.
Management: We prefer surgical excision of thecyst by performing orbitotomy . The cyst wall is verythin and can rupture during surgery. Hence, toprevent it, after exposing the cyst, we prefer to aspiratethe contents, so that the cyst shrinks in size. Then itcan be very safely pulled out with the help of a cryo.Akon O. et al from Turkey20 have advocatedpercutaneous aspiration of the cyst under ultrasonicguidance, followed by injection of 15% of hypertonicsaline and reaspiration (PAIR technique). Theyshowed a decrease in cyst size by three months and amarked decrease to 0.5 ml. by 9 months.
Medical management of hydatid cysts andrecurrent cysts with Albendazole and Praziquantalhas also been tried.21
A B
basm
ala
blog
(alw
ays o
rigin
al)

218218218218218 Surgical Atlas of Orbital DiseasesSurgical Atlas of Orbital DiseasesSurgical Atlas of Orbital DiseasesSurgical Atlas of Orbital DiseasesSurgical Atlas of Orbital Diseases
Figure 16.43: Male 35 years presented with proptosis of right eye of 2years duration with mild pain and discomfort. Note the eccentricproptosis with the globe pushed down and out. Note also the fullnessof superior sulcus. His BCVA was 20/80
Figures 16.44A to C: CT scan of the orbit shows a very large cyst in the superior peripheral space, pushing the globe down and out
Figures 16.45A to C: The cyst was exposed through superior lid crease incision. Note the tense cyst, as it is protruding-out (A). About 10 ml ofthe fluid was aspirated, and the collapsed cyst was removed with a cryo(B) The diagnosis of hydatid cyst was confirmed by the laminar / onionpeel appearance
Figure 16.46: First postoperative day picture, showing clinicalimprovement
CASE ILLUSTRATION
Note the position of the globe which has come back to normal. Also there is marked improvement in the fullness of superior sulcus. Patient'svision improved to 20/30 in course of time
A B C
A B C
basm
ala
blog
(alw
ays o
rigin
al)

Parasitic Cysts of OrbitParasitic Cysts of OrbitParasitic Cysts of OrbitParasitic Cysts of OrbitParasitic Cysts of Orbit 219219219219219
REFERENCES
1. Del Brutto OH. “Neurocysticercosis: Updating in diagnosisand Treatment” Neurolgia, 2005;20(8):412-8.
2. Del la Garza Y, Graviss E A, Daver NG,Gambarin KJ,Shandera WX, Schanz PM, White AC Jr : “Epidemiologyof Neurocysticercosis in Houston, Texas” Am J Trop. Med.Hyg.2005;73(4):766-70.
3. Towas JM, Hoffmann CJ,: “Neurocysticercosis in Oregon:1995-2000” Emerg. Infect Dis 2004;10(3):508-10.
4. Pushker N, Bajaj MS, Balasubramanya R: “ DisseminatedCysticercosis involving Orbit, brain and sub-cutaneoustissue”J. Infect. 2005;51(5)e245-8.
5. Chadha V, Pandey PK, Chauhan D, Das s: “ Simultaneousintraocular and bilateral extraocular Muscle involvementin a case of disseminated Cysticercosis” Int.Ophthalmol2006;15.
6. Gulliani BP, Dadeya S, Malik KP, Jain DC : “BilateralCysticercosis of optic nerve” J Neurophthalmol 2001;21(3):217-8.
7. Bajaj MS, pushker N: “Optic nerve cysticercosis” ClinicalExperimental Ophthalmol; 2002;30(2);140-3.
8. Sudan R, Muralidhar R, Sharma P, “ Optic NerveCysticercosis: case report and review of currentmanagement” Orbit, 2005;24(2);159-62.
9. Sekhar GC, Honavar SG, “ Myocysticercosis Experiencewith imaging and therapy” Ophthalmol, 1999;106(12)2336-40.
10. Honavar SG, Sekhar CG, “ Ultrasonological Characteresticsof Extraocular Cysticercosis” Orbit 1998;17(4),271-84
11. Bansal RK, Gupta A,Grewal SP, Mohan K, “ Spontaneousextrusion of cysticercosis: Report of three cases”, Indian Jophthalmol,1992;40(2):59-60.
12. Turgut AT, Turgut M, Ko?ar U.: "Hydatidosis of the orbitin Turkey: results from review of the literature 1963-2001"Int Ophthalmol. 2004;25(4):193-200.
13. Xiao A, Xueyi C: "Hydatid cysts of the orbit in Xinjiang: areview of 18 cases", Orbit. 1999;18(3):151-55.
14. Gomez Morales A, Croxatto JO, Crovetto L, Ebner R;Hydatid cysts of the orbit. A review of 35 cases,Ophthalmology. 1988;95(8):1027-32.
15. Kiratli H, Bilgiç S, Oztürkmen C, Aydin O: Intramuscularhydatid cyst of the medial rectus muscle, Am J Ophthalmol.2003;135(1):98-9.
16. Jhn lCrompton, Prema V Iyer, David J Merry John Tomich,Llance V Perrett "Hydatid cyst: an unusual cause ofdiplopia" Australian and New Zealand Journal ofOphthalmology 13 (2), 195-203.
17. Rastogi A, Arora R, Chaturvedi K. Orbital hydatid cyst: anunusual presentation", Orbit. 1998;17(2):107-111.
18. Betharia SM, Pushker N, Sharma V, Avinash M, KashyapS: "Disseminated hydatid disease involving orbit, spleen,lung and liver". Ophthalmologica. 2002;216(4):300-4.
19. Andronikou S, Welman CJ, Kader E: "Classic and unusualappearances of hydatid disease in children" Pediatr Radiol.2002;32(11):817-28.
20. Akhan O, Bilgiç S, Akata D, Kiratli H, Ozmen MN:"Percutaneous treatment of an orbital hydatid cyst: a newtherapeutic approach" Am J Ophthalmol. 1998;125(6):877-9.
21. Sihota R, Sharma T:Albendazole therapy for arecurrent orbital hydatid cyst Indian J Ophthalmol.2000;48(2):142-3.
basm
ala
blog
(alw
ays o
rigin
al)

220220220220220 Surgical Atlas of Orbital DiseasesSurgical Atlas of Orbital DiseasesSurgical Atlas of Orbital DiseasesSurgical Atlas of Orbital DiseasesSurgical Atlas of Orbital Diseases
Alon Kahana, Mark J Lucarelli, Cat N Burkat, Richard K Dortzbach
Orbital FracturesOrbital FracturesOrbital FracturesOrbital FracturesOrbital Fractures
INTRODUCTION
The surgeon encounters orbital fractures in the acute,subacute and chronic settings. In each situation, thetreatment goals are similar-restoration of orbitalintegrity and volume. However, the nuances oftreatment can vary widely according to the specificsetting and injury. In this chapter, we will attemptto provide an overview of how we approach orbitalfractures in a variety of settings, and provide enoughreference materials to satisfy the need for additionalstudy.
ANATOMY
The adult human orbit has a volume of approximately30 ml, of which the globe accounts for approximately7 ml, or about 25%.1 It traditionally is said to beformed of 7 bones: maxillary, zygomatic, frontal,lacrimal, ethmoid (lamina papyracea), palatine, andthe sphenoid, although the greater and lesser wingsof the sphenoid develop independently duringembryogenesis [the alisphenoid (greater wing) andorbitosphenoid (lesser wing) bones].2 The optic canalis part of the lesser wing of the sphenoid.
Orbital bony strength is dependent on a seriesof dense bony buttresses that provide structuralintegrity and create a protective frame around theeye. Anteriorly are the frontomaxillary andfrontozygomatic buttresses. Posteriorly is thepterygomaxillary buttress (Figure 17.1).3-9 Orbitalfractures can be classified as blow-out fractures (norim involvement), and fractures that involve the rim
as part of La Forte II or III fractures. Fracturesinvolving the buttresses typically present with largerdisplacements. Alternatively, when the buttresses areintact, trapdoor-type fractures are more common.4
The anatomic landmarks of most fracturescorrelate with the bony anatomy (Figure 17.2). Floor
Figure 17.1: Orbitomaxillary buttresses. Nasomaxillary (medial),zygomaticomaxillary (lateral). Based on Gruss et al., 1986.Diagrammatic representation of the maxillary buttresses showing thetwo anterior buttresses (medial or nasomaxillary and lateral orzygomaticomaxillary) and the posterior buttress (pterygomaxillary).The relationship of these buttresses to the cranial base above, themandible below and the correct occlusion is seen
17C H A P T E R
basm
ala
blog
(alw
ays o
rigin
al)

Orbital FracturesOrbital FracturesOrbital FracturesOrbital FracturesOrbital Fractures 221221221221221
fractures often extend up to the infraorbital grooveand/or canal, since the thin bone of the floor abutsthe stronger bone of the canal. Posteriorly, floorfractures nearly always leave the most posteriorportion intact since it is part of the large and strongpalatine bone. Medially, floor fractures often leaveintact the inferomedial strut, a part of thefrontomaxillary buttress.10, 11 Medial wall fracturesoften end at the frontoethmoidal suture line: thelamina papyracea is very thin, whereas the frontalbone is thick and supported by the cribriform plate.Lateral wall fractures often occur as part of acomplex fracture involving the zygomatic arch andthe maxillary bone.
Orbital nerves and vascular bundles can oftenbe involved in orbital fractures, and serve asimportant landmarks (Figure 17.2). Since theinfraorbital nerve often abuts the floor fracture edge,it is commonly contused by the trauma but rarelysevered. Hence, hypoesthesia in the V2 distributionof the trigeminal nerve is very common followingorbital trauma, but such numbness typically resolves,at least partially, several weeks to months after injuryunless surgical repair causes further damage. Justposterior to where the infraorbital groove and canalmeet, a perforating branch of the infraorbital arteryis often encountered, which can cause significant
bleeding if not isolated and cauterized in the courseof surgical repair.12
The zygomatic bone contains foramina for boththe zygomaticofacial and the zygomaticotemporalnerves, branches of the V1 division of the trigeminalnerve. Overall, the area innervated by these nervesis small, and patients often tolerate hypoesthesiaassociated with injury to these nerves, which mayoccur from surgery as well as from the initial injury.
Injury to the infratrochlear, posterior ethmoidaland/or anterior ethmoidal neurovascular bundles areuncommon, but can be associated with significantbleeding. Superomedial orbital injury may also beassociated with damage to the trochlea, causingtorsional diplopia.
Orbital fractures can often cause ocular dys-motility. There are several general etiologies in theacute setting: direct muscle damage and/or edema,nerve damage, or muscle entrapment. The restrictioncaused by muscle entrapment often involves theorbital fibrous connective tissue complex, of whichthe extraocular muscle pulleys and septa are a part.13,14
Hence, herniation and entrapment of orbitalconnective tissue that is associated with anextraocular muscle can often cause a clinical pictureof entrapment even though the muscle itself is notincarcerated in the fracture. Such findings can often
Figure 17.2: An anterior-posterior view into the right bony orbit
basm
ala
blog
(alw
ays o
rigin
al)

222222222222222 Surgical Atlas of Orbital DiseasesSurgical Atlas of Orbital DiseasesSurgical Atlas of Orbital DiseasesSurgical Atlas of Orbital DiseasesSurgical Atlas of Orbital Diseases
be subtle. So a high index of suspicion is important(Figures 17.3A and B, and 17.4A to D).
Finally, the optic nerve enters the optic canal nearthe apex of the orbit. Blunt trauma can result in opticnerve injury through several mechanisms: collapseof the optic canal with crush injury to the nerve, injuryof perforating vessels to the optic nerve, hemorrhagewith compressive optic neuropathy, severing throughavulsion of the nerve, and direct injury to the globewith transmission of the impact posteriorly (Figures17.5 and 17.6).
EXAMINATION
A patient with orbital trauma requires a completehistory and ophthalmic examination, including adilated fundus examination. Any loss of con-sciousness should be documented, and the possibilityof an intraocular or intraorbital foreign body mustbe addressed. The possibility of an open globe shouldbe considered in every patient with orbital trauma,and an open globe must be ruled out prior to anyorbital evaluation and management. Loss of vision,dysmotility, hyphema, and 360° subconjunctivalhemorrhage are often associated with a rupturedglobe.
When the examination occurs in an intensive caresetting, as is often the case, exact history and a fullexamination cannot be obtained. In such a setting,early evaluation of the pupils, prior to sedation/analgesia-related miosis, is critical to identifying opticnerve trauma and a relative afferent pupillary defect(RAPD). Intraocular pressure should be measuredwith a handheld device, such as a Tonopen(Medtronic Ophthalmics, Minneapolis, MN, USA),
Figures 17.3A and B: Mild muscle entrapment. Patient is a 45 yearsold man who suffered a left blow-out fracture and experienceddiplopia in upgaze. He presented several weeks after his initial traumawith a CT scan taken shortly after the injury. Examination found mildrestriction of the left eye in upgaze. The CT scan showed left inferiorrectus rounding, consistent with muscle entrapment. He was onlyminimally symptomatic in upgaze with no diplopia in primary ordowngaze, and did not require surgical repair
and high intraocular pressure treated aggressively.In an alert patient with loss of vision and elevatedintraocular pressure, the possibility of a retrobulbarhemorrhage must be assessed, and when appropriate,a lateral canthotomy with cantholysis performedacutely. Particular attention must be given topatients who are on blood-thinning medications,such as warfarin, which can make an orbitalhemorrhage both more likely and more severe.Canthotomy incision is a simple and fairly benigntechnique for rapidly reducing vision-threateningorbital pressure, and the addition of a cantholysis canfurther improve the decompression.15 It is not rarefor patients with an orbital compartment syndrometo report improvement in vision within minutes of acanthotomy and cantholysis. Evacuation of an orbitalhematoma in the acute setting has been described,including a minimally invasive technique.16
While extraocular motility cannot be evaluatedin the sedated patient, radiologic suggestion ofentrapment should be further investigated withforced duction testing at the bedside, which thesedation facilitates (Figures 17.7A to E). It should be
A B
A
B
basm
ala
blog
(alw
ays o
rigin
al)

Orbital FracturesOrbital FracturesOrbital FracturesOrbital FracturesOrbital Fractures 223223223223223
Figures 17.4A to D: Severe entrapment with muscle pinching. Patient is a 19-year-old college student involved in a nightclub alteration, whoattributed his pain to swelling and bruising. One week later, when the swelling subsided, he continued to have pain and nausea with eyemovement, with significant diplopia. Examination revealed right inferior rectus restriction (A and B). CT showed pinching of an entrappedmuscle in a small minimally-displaced floor fracture (C). Urgent exploratory surgery found a dusky IR. After muscle release and fracture repair,he was instructed to patch his uninjured left eye and use his right eye to read and do homework. Over the next few weeks, motility recoveredto better than 80% of normal, with only minimal diplopia in extreme down and up-gaze (D)
C
D
basm
ala
blog
(alw
ays o
rigin
al)

224224224224224 Surgical Atlas of Orbital DiseasesSurgical Atlas of Orbital DiseasesSurgical Atlas of Orbital DiseasesSurgical Atlas of Orbital DiseasesSurgical Atlas of Orbital Diseases
Figures 17.5: Optic canal injury. Patient was a 12 years old involvedin an unhelmeted accident while riding an all terrain vehicle (ATV).She developed a left relative afferent pupillary defect. Maxiface CTscan revealed evidence of fractures (arrowhead) through thesphenoid sinus extending into the left optic canal, with a small airbubble located at the intracranial opening of the optic canal (arrow).
Figures 17.7A to E: Forced ductions—before (A to C) and after (D and E) repair. (A) Forced ductions before repair demonstrating verticalrestriction, (A to C) Forced ductions after floor fracture repair with release of entrapped inferior rectus muscle, demonstrating normal ductions(D and E)
A B
C D
E
Figures 17.6: Axial section of CT scan showing small air bubble(arrow) at the intracranial opening of optic canal. These subtle fracturefindings are a common occurrence in pediatric patients in whom thebones are malleable
basm
ala
blog
(alw
ays o
rigin
al)

Orbital FracturesOrbital FracturesOrbital FracturesOrbital FracturesOrbital Fractures 225225225225225
remembered that ductions may also be limited byorbital edema, so the ductions should be comparedwith one another. Often, the pupils cannot be dilatedbecause of the tenuous neurological state of thesepatients in the immediate postinjury period. In thesecases a direct ophthalmoscope may be used to viewthe vitreous and disc. A vitreous hemorrhage shouldbe noted and further investigated for a possiblerhegmatogenous retinal detachment using B-scanultrasound. Likewise, the presence of a cornealabrasion or a hyphema should be assessed and treated.
The evaluation of facial fractures is oftenperformed by a multi-disciplinary team, and it isimportant to communicate effectively with othermembers of that team. The orbital evaluation shouldinclude palpation of the rim for any step-offs, and ofthe periorbital region for crepitus (Figures 17.8Aand B). If the patient is alert, sensation in thetrigeminal distribution can be assessed. Hypoesthesiain the distribution of the V2 branch of the trigeminalsuggests an orbital floor fracture, but can also beassociated with nerve contusion and orbital edema.Hertel exophthalmometry is a useful indicator of the
risk of enophthalmos, and in our experience,the presence of 1.5 mm or more of enophthalmosin the acute posttrauma period suggests thatfurther enophthalmos may develop once swelling isreduced.
Additional structural and functional con-sequences of orbital fractures should be carefullyassessed. Attention should be given to integrity andsymmetry of the medial and lateral commissures.Zygomatic fractures can often cause lateral canthaldystopia (Figures 17.9A to D), whereas nasoethmoid
Figures 17.8A and B: Lateral canthal dystopia post-ZMC fracturerepair. Note the right lateral canthal dystopia. Patient had suffered amotor vehicle accident with right orbital fractures. His zygoma wasreduced to achieve alignment in 2 dimensions (rather than 3dimensions), with resultant enlargement of the orbital cavity. Hepresented to our clinic with enophthalmos and diplopia. Subsequentsurgical repair resolved his enophthalmos and diplopia
Figures 17.9A to D: Traumatic telecanthus (A). Patient suffered significant facial trauma following a fall, with severe comminuted nasoethmoidfractures along with maxillary and zygomatic fractures (B and C). Initial repair did not fully restore the anatomy of the medial canthus and shewas referred for a consultation. Intraoperatively, scar tissue was debulked and miniplate fixation was used to anchor the medial canthaltendon. Postoperatively, she has medial scleral show, and only 1mm of telecanthus (D)
A
C
B
D
A B
basm
ala
blog
(alw
ays o
rigin
al)

226226226226226 Surgical Atlas of Orbital DiseasesSurgical Atlas of Orbital DiseasesSurgical Atlas of Orbital DiseasesSurgical Atlas of Orbital DiseasesSurgical Atlas of Orbital Diseases
fractures can often cause telecanthus (Figures 17.10Aand B). Nasoethmoid fractures are also associatedwith damage to the nasolacrimal duct, leading to anincreased risk of posttraumatic epiphora.
Often, surgical repair of orbital fractures can bedelayed until a better examination can be performedand an informed consent can be obtained. In thissetting, useful adjuncts in the evaluation of diplopiaand ocular dysmotility are ocular alignment measure-ments of heterotropia, and the binocular visual field(also known as diplopia field) which uses theGoldmann perimeter to delineate the area of fusion.
IMAGING
Computed tomography (CT) scan without contrastcontinues to be the workhorse of orbital fractureimaging. A study including axial, coronal and sagittalcuts through the orbit is prefered.9, 17 Displacementshould be noted using the bone-window, whereasthe presence of soft-tissue herniation, including fatand muscle herniation, should be assessed using thesoft-tissue window. A careful and systematic reviewof the orbital bones is necessary in order to avoidmissing a small fracture that may be clinicallyrelevant. Once a fracture has been identified, theimaging study is carefully reviewed for other facialfractures, especially nasal, frontal, zygomatic arch,and mandibular fractures, as well as any fractures ofthe orbital buttresses. The orbital rim, inferomedialstrut, and the bony platforms at the edges of fractureare assessed. The repair of pan-facial fractures in mostcenters is coordinated with the rest of the traumateam in order to achieve the best possible outcomefor the patient. Of great import is the overall size of
the orbital fractures, as well as the extent ofdisplacement. We typically recommend surgicalrepair for orbital wall fractures that total more than50% of the size of the orbital floor, since suchfractures, when not repaired, can lead to significantenophthalmos.18 (Figures 17.11A to C).
Next, the soft-tissue windows should be carefullyexamined for herniation of fat and/or extraocularmuscle. However, it is important to emphasize thatmuscle entrapment is a clinical diagnosis, not aradiological diagnosis. The presence of retrobulbarhemorrhage should be noted, and its sizeapproximated. The appearance of the extraocularmuscles should be carefully noted for a roundingeffect (which may signify entrapment) or forenlargement that can be associated with a hematoma(Figure 17.3). If muscle entrapment is noted clinicallybut not supported radiologically, we recommend thatsurgical exploration be carefully considered.
Figures 17.11A to C: Enophthalmos. Three examples of clinically-apparent enophthalmos resulting from orbital trauma
Figures 17.10A and B: Naso-ethmoid comminuted fracture repairwith miniplates, and fixation of the medial canthal ligament to theminiplates. A nasal splint with silastic bolsters can facilitatereconstruction of the medial canthal architecture
A B
A
B
C
basm
ala
blog
(alw
ays o
rigin
al)

Orbital FracturesOrbital FracturesOrbital FracturesOrbital FracturesOrbital Fractures 227227227227227
IMPLANT MATERIALS
The choice of material for orbital fracture repair isbroad, and includes both autogenous tissues andalloplastic materials. Each has advantages anddisadvantages.19
Alloplastic implants are easily available, requiringno harvesting procedure with its associatedmorbidity. Several, such as titanium plates andporous polyethylene, have proven over time to bestrong and effective.20-24 The disadvantage ofalloplasts is that they do not completely integratewith the living orbital tissues, which can lead to earlyand late complications, including infection, exposureand/or extrusion. The bacterial load required toinfect an alloplastic implant can be lower by a factorof 10,000 than for an autogenous graft.25 Implantexposure can particularly pose a risk for infection. Inaddition, because the integration of even the bestalloplastic implants is incomplete, migration andexposure can occur, both in the early postoperativeperiod and as a late complication. Finally, when acomplication occurs with an alloplastic implant,management will often require removal of theimplant, which can be challenging.
Alloplastic materials include porous polyethylene(e.g. Medpor, Porex Surgical, Newnan, GA, USA),hydroxyapatite (e.g. Biocoral, Wilmington, DE,USA), titanium mesh (such as from KLS Martin,Tuttlinger, Germany; Stryker Craniomaxillofacial,Portage, MI, USA; Synthes Inc., West Chester, PA,USA), and nylon (such as Supramid, S. Jackson,Alexandria, VA).
Titanium is a strong, inert metal. It does notintegrate but can be easily fixated to the surroundingbones and can provide excellent support for orbitalstructures.23 If bone resorption occurs, it mayinfrequently require removal. Overall, titanium meshcan be an excellent choice for orbital fracture repairand has a significant track record of safety.24
However, in our experience, reoperations followingimplantation of titanium mesh are more difficult asfibrous scar tissue insinuates itself into the holes ofthe mesh (Figures 17.12A and B). Hence, titaniummesh is not our first choice in the repair of orbitalfloor fractures. In cases of severe obliteration of morethan one of the orbital walls, titanium mesh may bean excellent choice, owing to its ability to be shaped
and maintain the desired shape. The use of titaniummini-plates in the stabilization of orbital rim andbuttress fractures is a mainstay of fracture fixationtechniques.
Nylon sheets come in a variety of sizes and areeasy to use.26 Fixation can be achieved with a fibrinsealant (e.g. Tisseel, Baxter, Deerfield, IL, USA) or abiological glue (BioGlue, CryoLife, Kennesaw, GA,USA). However, late complications with nylon sheetsare not uncommon, and in particular, the capsule thatforms around the nylon sheet can spontaneouslyhemorrhage.27
Our preferred alloplastic implant material isporous polyethylene, which is strong, biocompatibleand can integrate well.20, 28-30 Medpor Barrier implants(Porex Surgical, Newnan, GA, USA), are porouspolyethylene plates that are coated with a thin, non-porous, high density polyethylene barrier that isheat-bonded to the porous material on one side. Thisbarrier is positioned toward the orbital tissues toreduce scarring and attachment of orbital tissues tothe plate.31 The barrier also has the added benefit ofstrengthening the sheet. Porous polyethyleneimplants can also be easily secured to the rim withscrews if necessary, either using a channel implantor directly through the porous polyethylene. Theyare malleable and can be cut into various sizes andshapes with a large Metzenbaum scissors. A newerversion of the porous polyethylene implant is theTITAN implant (Porex surgical), which can holdcurved shapes particularly well. This implant is well
Figures 17.12A and B: Titanium mesh with scarring. Patient is ayoung woman who was injured in a motor vehicle accident. Shesuffered severe ocular injuries that eventually resulted in anenucleation. In addition, she underwent floor fracture repair withtitanium mesh. Her implant motility was severely limited and shedeveloped significant enophthalmos with superior sulcus deformity.She was referred for an orbital consultation and underwent orbitalvolume augmentation. Intraoperatively, her inferior rectus andsurrounding orbital tissues were found to be tightly adherent to thetitanium mesh, with extensive scarring through the holes in the mesh.These were dissected off to free the orbital tissues from incarcerationin the titanium mesh
A B
basm
ala
blog
(alw
ays o
rigin
al)

228228228228228 Surgical Atlas of Orbital DiseasesSurgical Atlas of Orbital DiseasesSurgical Atlas of Orbital DiseasesSurgical Atlas of Orbital DiseasesSurgical Atlas of Orbital Diseases
suited for repair of large floor fractures andreconstructions that involve both the floor and themedial wall (such as loss of the inferomedial strut)(Figures 17.13A to D). The titanium mesh embeddedin the porous polyethylene contains holes throughwhich screws can be placed for improved fixation ifnecessary.
Autogenous bone grafts have a proven trackrecord of reliability, but require a harvestingprocedure unless a cadaveric bone graft is used. Givenrecent concerns with infectious agents and priondiseases, cadaveric bone grafts may be seen as lessdesirable to many patients. Fresh bone contains livingosteocytes and integrates well with the surroundingbones. When cranial bone is used, early integration
is achieved and minimal resorption is observed.32-34
This is most likely the result of the neural crest originof calvarial bone, which is shared with orbital bones.The neural crest-derived craniofacial bones formthrough intramembranous ossification, whereas themesodermal bones of the ribs and pelvis formthrough endochondral ossification.35, 36 Calvarial bonecan be harvested without the need for surgicalpreparation of a different body site (Figures 17.14Ato D). In addition, calvarial access can be hiddenbehind the hairline, and when a bicoronal approachis used for orbital fracture repair, the same exposurecan be used for harvesting the graft. A majordisadvantage of calvarial bone grafts is that despitethe overall safety of the harvesting procedure, the
Figures 17.13A to D : Medpor TITAN in complex fractures and orbital reconstructions. A: Posterior large medial wall fracture and Medpor TITANimplant prior to placement. The implant was cut to size, incorporating a notch for the inferior oblique. It was then bent and placed into position.A=anterior. P=posterior. S=superior. B: Even a large Medpor TITAN implant can be bent and will hold its shape. This patient underwent orbitalreconstruction following excision of sino-orbital squamous cell carcinoma that involved the inferomedial orbital bones. Fixation was achievedwith glutaraldehyde-crosslinked albumin adhesive (BioGlue, Cryolife Inc)
A
C
B D
basm
ala
blog
(alw
ays o
rigin
al)
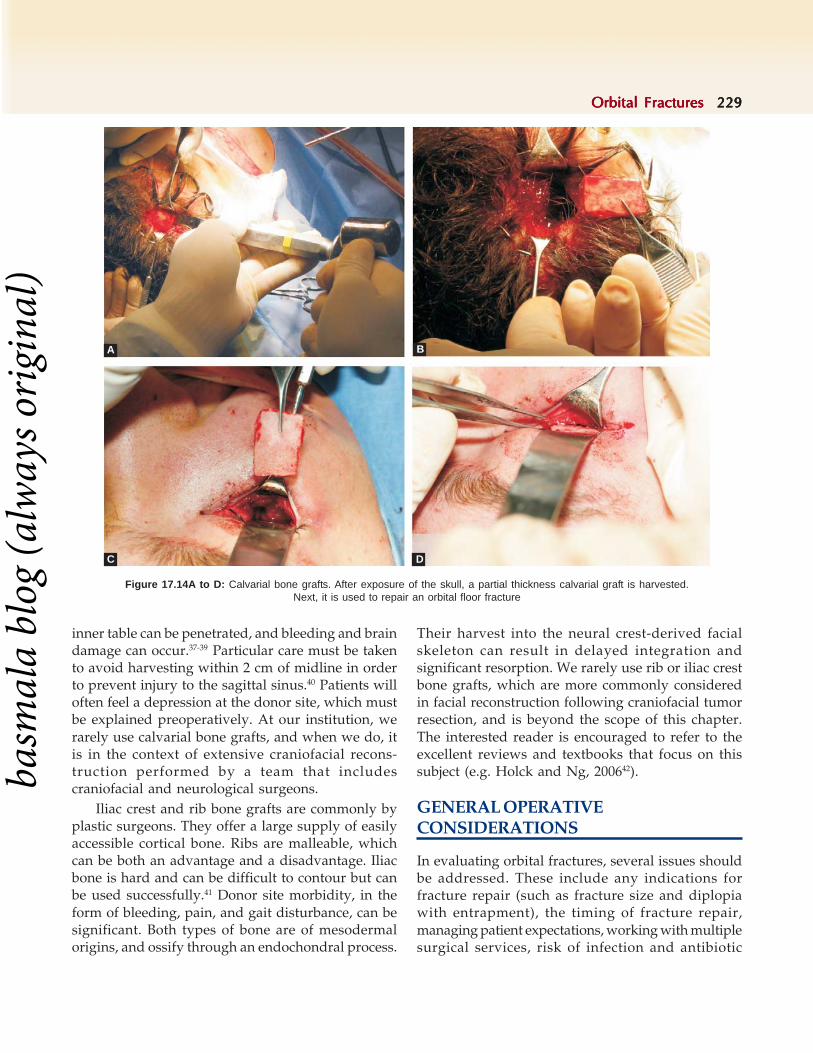
Orbital FracturesOrbital FracturesOrbital FracturesOrbital FracturesOrbital Fractures 229229229229229
Figure 17.14A to D: Calvarial bone grafts. After exposure of the skull, a partial thickness calvarial graft is harvested.Next, it is used to repair an orbital floor fracture
inner table can be penetrated, and bleeding and braindamage can occur.37-39 Particular care must be takento avoid harvesting within 2 cm of midline in orderto prevent injury to the sagittal sinus.40 Patients willoften feel a depression at the donor site, which mustbe explained preoperatively. At our institution, werarely use calvarial bone grafts, and when we do, itis in the context of extensive craniofacial recons-truction performed by a team that includescraniofacial and neurological surgeons.
Iliac crest and rib bone grafts are commonly byplastic surgeons. They offer a large supply of easilyaccessible cortical bone. Ribs are malleable, whichcan be both an advantage and a disadvantage. Iliacbone is hard and can be difficult to contour but canbe used successfully.41 Donor site morbidity, in theform of bleeding, pain, and gait disturbance, can besignificant. Both types of bone are of mesodermalorigins, and ossify through an endochondral process.
Their harvest into the neural crest-derived facialskeleton can result in delayed integration andsignificant resorption. We rarely use rib or iliac crestbone grafts, which are more commonly consideredin facial reconstruction following craniofacial tumorresection, and is beyond the scope of this chapter.The interested reader is encouraged to refer to theexcellent reviews and textbooks that focus on thissubject (e.g. Holck and Ng, 200642).
GENERAL OPERATIVECONSIDERATIONS
In evaluating orbital fractures, several issues shouldbe addressed. These include any indications forfracture repair (such as fracture size and diplopiawith entrapment), the timing of fracture repair,managing patient expectations, working with multiplesurgical services, risk of infection and antibiotic
A B
C D
basm
ala
blog
(alw
ays o
rigin
al)

230230230230230 Surgical Atlas of Orbital DiseasesSurgical Atlas of Orbital DiseasesSurgical Atlas of Orbital DiseasesSurgical Atlas of Orbital DiseasesSurgical Atlas of Orbital Diseases
coverage, orbital edema and the use of steroids,concomitant management of soft tissue injuries, theuse of blood thinning products, and elective versusurgent repair. Patients should be advised to avoidblowing their nose,43 and prescribed nasal saline spray2-4 times daily. Patients are instructed to keep theirhead elevated, and to use ice-cold compresses for 2-3 days. Any blood thinning medications, especiallyaspirin, clopidogrel (Plavix, Bristol-Myers Squibb) orwarfarin, should be discontinued in co-ordinationwith the prescribing internist. Other blood thinningproducts include non-steroidal anti-inflammatorydrugs, vitamin E, garlic, ginseng, and ginkgobiloba.44,45 With patients on warfarin, the prothrombintime should be checked in the early preoperativeperiod. Since an orbital hemorrhage can havecatastrophic effects on vision, care must be taken inoperating on anticoagulated patients.
Antibiotics
Orbital cellulitis is a serious but uncommoncomplication of orbital fractures.46 Practice patternsvary widely regarding the use of antibiotics in thecontext of orbital fractures. Multiple published studieshave shown that postoperative antibiotics do not alterthe rate of infection associated with orbital fractures,although good studies have not been performed.22,47,48
A randomized trial with 181 patients who underwentopen reduction and fixation of mandibular fracturesalso showed no advantage to postoperativeantibiotics.49 Risk factors for orbital infection in thecontext of orbital fractures include open fractures,sinusitis, and contaminated wounds.46 In thesesituations, we always give preoperative antibiotics,since preoperative administration of antibioticshas been shown to provide improved prophylaxis.50
In addition, in cases of frank wound contamination,we carefully treat the wounds with 5% Betadinesolution and irrigate the wound intraoperativelywith bacitracin solution. Our antibiotics of choice areCefazolin, Ampicillin-Sulbactam (Unasyn, Pfizer,NY, USA) or Clindamycin, with the latter twoproviding improved coverage of anaerobic micro-organisms.
The risk of antibiotic overuse cannot be over-emphasized. The human body is continuouslycolonized by bacteria that exist in steady-stateequilibrium in the context of the normal flora.Treatment with antibiotics alters the equilibrium,
which can potentially lead to the proliferation ofantimicrobial-resistant pathogenic organisms. Hence,overuse of antibiotics can cause an infection withresistant bacteria. We usually limit antibiotic usageto the preoperative setting, with administration priorto surgical incision in order to achieve significanttissue concentration at the surgical site intra-operatively. Postoperative antibiotics are given onlyif there are active signs of infection or if systemicsteroids are prescribed in the context of a higher riskof infection (as discussed below).
Steroids
Glucocorticoids can be extremely useful in theperioperative management of orbital fractures.51-53
However, their use can lead to complications,especially an increased risk of infection. Hence, anysteroid administration is done using a very rapidtaper regimen.
The most useful contexts of steroid usage are inthe preoperative assessment of extraocular musclefunction and in the prophylaxis of postoperativeemesis (which can cause implant movement andbacterial spread). In the preoperative setting, it issometimes difficult to distinguish between extra-ocular muscle contusion or edema and frank muscleentrapment. This distinction is important to makesince it can strongly influence the decision torecommend surgical exploration repair. Therefore,when there is significant dysmotility associated withmoderate to severe orbital edema, a small orbitalfracture and no obvious entrapment radiologically,we document the dysmotility with a binocular visualfield (also known as a diplopia field, performed withboth eyes open on a Goldmann Perimeter), andprescribe a rapid taper of Prednisone orMethylprednisolone over the course of 5-7 days. Atypical Prednisone taper for an adult would be 40,30, 20, 10, and 5 mg over the course of 5 days. Were-evaluate motility toward the end of the treatmentcourse (in 5-7 days) and reassess the need for surgicalintervention. In numerous cases, these exams willreveal significantly improved motility and nearresolution of diplopia, avoiding the need for surgicalexploration of a fracture that was otherwise too smallto warrant surgical repair.
Another context for prescribing a steroid taperis in children, who tend to swell more and scar faster.We try to operate on children earlier (within 1 week
basm
ala
blog
(alw
ays o
rigin
al)

Orbital FracturesOrbital FracturesOrbital FracturesOrbital FracturesOrbital Fractures 231231231231231
and in cases of severe restriction, even sooner). A-5day steroid taper can help control posttraumaticedema and facilitate early and safe surgery.
Intraoperative IV steroids can be very useful intwo respects: control of nausea, and expeditedresolution of postoperative edema and discomfort.In an adult, 8-10 mg of Dexamethasone are oftengiven by the anesthesiologist toward the end ofsurgery. Intraoperative steroid irrigation of the orbitis performed rarely, and usually in the context oflate repair of a scarred musculoseptal system.
Infrequently, a postoperative steroid taper isprescribed if severe edema is anticipated (e.g. laterepair of severely scarred orbit), or if edema wouldinterfere with the postoperative evaluation andpatient management (e.g. with extraocular motilityevaluation). However, there are no good studies todirect perioperative steroid use, and the potentialside effects must be fully considered.
Pediatric patients
Special attention must be given to nondisplacedfractures and floor fractures in pediatric patientssince muscle entrapment with frank muscle pinchingmay occur.54 Steroids will not only fail to resolve thedysmotility, but will also delay needed surgicalintervention, which can lead to irreversible muscleinjury. Such fractures have been termed "greenstick"fractures, and are the result of the fact that the facialbones of children have a higher cancellouscomposition and thinner cortices, resulting inincreased bone flexibility.55-58
At times, orbital floor fractures result in minimalsoft tissue injury, no orbital edema and noenophthalmos but severe dysmotility with entrap-ment, pain, and nausea. CT scanning may onlydemonstrate minimal tissue herniation and fracturedisplacement. This presentation has been termed"white eye syndrome."54, 59 Clinical signs of musclepinching and entrapment include restriction inupgaze, severe pain worsened by upgaze, andoculocardiac reflex induced by upgaze, which caninclude nausea, vomiting, bradycardia and/orsyncope.58, 60, 61 Timely management of fractures withmuscle pinching is essential in order to reduce therisk of irreversible muscle damage and strabismus,both in the pediatric and adult population. In patients
with White Eye Syndrome, surgical exploration andrepair must be carried out urgently. The examinationof a child who is in pain and distressed followingorbital trauma can be quite challenging, and thesurgeon must maintain a high level of suspicion,especially when the eye and orbit appear normal butthere may be a motility disturbance.
Timing of surgeryThe ideal timing of surgical exploration and repairdepends on the clinical findings, the overall medicalcondition of the patient, the radiographic evidenceand any concomitant injuries. Delayed repair has theadvantages of reduced swelling, a more thoroughpreoperative evaluation, and an increased opport-unity to establish a meaningful patient-doctorrelationship prior to any surgery. Early repair hasthe advantage of reduced fibrosis and scarring. Ingeneral, we prefer to repair orbital fractures within2 weeks of injury once the majority of post-traumaticedema has resolved.18, 60
There are several exceptions to this “2 week”guideline whereby early or late intervention wouldbe preferred. First, if the patient's overall medicalcondition is unstable, then medical stabilization musttake precedence. Second, if entrapment with musclepinching is encountered (often in children as part ofa White Eye Syndrome), urgent repair is advisablein order to reduce the risk of irreversible muscledamage. Third, when the optic nerve may becompromised, the status of the optic nerve shouldbe properly investigated prior to any orbital surgery.Otherwise, surgery may further compromise thealready-traumatized nerve, or the patient mayperceive the surgery as the cause of any optic nervedamage. The status of the globe and the possibilityof a retinal detachment must also be fullyaddressed prior to any orbital fracture surgery.Finally, if other surgical interventions are planned,coordinating care can be an overall advantage to thepatient by minimizing multiple inductions ofanesthesia.
Another softer exception to the 2-week rule isthe pediatric population. Children swell more, buttheir edema resolves faster. They heal and scar faster,and are more prone to greenstick fractures andmuscle pinching. Hence, expedited repair is oftenrecommended for children.
basm
ala
blog
(alw
ays o
rigin
al)

232232232232232 Surgical Atlas of Orbital DiseasesSurgical Atlas of Orbital DiseasesSurgical Atlas of Orbital DiseasesSurgical Atlas of Orbital DiseasesSurgical Atlas of Orbital Diseases
Decision: repair or not repair?Surgical repair of orbital fractures is a very safeprocedure when done appropriately. Nevertheless,surgery can cause complication.62, 63 The decision ofwhether to repair an orbital fracture is complex, andmust rely on the individual circumstances as well ason the experience of the surgeon. However, severalguidelines have been published that can be of greathelp in making a recommendation regarding surgicalrepair. These guidelines address the risk of post-traumatic enophthalmos,64 ocular dysmotility,diplopia, and facial deformity.
Fracture size correlates well with the risk of post-traumatic enophthalmos.18, 65 Hence, radiographicassessment of fracture size can be a critical part ofthe decision tree. There are several methods that havebeen advocated in the evaluation of post-traumaticenlargement of orbital volume. When the zygoma isnot involved, it is simplest to assess whether the sumof orbital floor and medial wall fractures constituteshalf of the floor or more. This algorithm is simple toexecute but does not take into account any lateralwall/ZMC fractures.65 Another method requiresmeasurement of the added volume caused by thefracture. This is determined by comparing thefractured orbit with the non-traumatized orbit.66-68
For example, using one algorithm, measurements thatreveal greater than 13% orbital volume enhancementwould lead to a recommendation for surgical repair.67
The weakness of this algorithm is that many patientssustain injury to both orbits, which precludes usefulcomparison.
Zygoma fractures can seriously complicate anyvolumetric assessment, since floor fractures are oftenpresent but get reduced once the ZMC fracture isreduced.65 Nevertheless, the rotation and/ordisplacement of a fractured zygoma can lead tosevere orbital volume changes, and incompletereduction of ZMC fractures can be a common causefor postoperative enophthalmos. ZMC reductionrequires special care since without three pointfixation, reduction may be incomplete although thefracture may appear well aligned along the orbitalrim. Rotation and orbital volume expansion can stilloccur and can often be hard to detect. Hence, three-point reduction of ZMC fractures with properfixation should be the goal of these surgicalrepairs.65,69,70
Ocular dysmotility and diplopia are debilitatingconsequences of orbital trauma. Ocular dysmotilitycan occur for several reasons, and it is the task of thesurgeon to distinguish between the etiologies inorder to make the appropriate recommendation.Posttraumatic extraocular muscle dysfunction canoccur as a result of muscle contusion, hematoma,fibrosis or avulsion, muscle entrapment with orwithout pinching, cranial nerve injury and muscleparesis, generalized orbital swelling, or contractureof the antagonist muscle. Muscle fibrosis orcontractures are later complications that must beprevented by proper management. However, attimes it can be very challenging to distinguishbetween ocular dysmotility with or withoutentrapment. Limitation in up-gaze with associatedpain and nausea can be telltale signs of muscleentrapment. In addition, CT scans can be particularlyhelpful in this task. Rounding of an extraocular muscleis often associated with entrapment. The radiologistand surgeon must be particularly cognizant of orbitaltissue herniation without frank muscle herniation:the herniated tissues may cause entrapment by virtueof their numerous fibrous attachments to a muscle.Such a fracture should be repaired.
Some surgeons advocate exploration and repairof orbital floor fractures for non-resolving infra-orbital hypoesthesia. However, a meta-analysis ofthe literature found little evidence to supportsuch a recommendation since the reportedsurgical outcomes were poor. However, if infra-orbital pain is worsening, exploration is probablywarranted.71-73
The decision to operate is complex and must beindividualized. Our preference is to operate within2 weeks of injury except in children, in which casesurgical repair would preferably take place within aweek. In cases with pinched muscles, urgent repairwithin 1-3 days of injury would be advocated. Whenorbital edema makes the evaluation difficult, a steroidtaper can be very helpful. When the examination isinconclusive, a re-examination is warranted and canbe critical to making the proper diagnosis andsurgical plan.
Irrespective of the type and location of thefractures, the goals of surgery are fundamentallysimilar: repositioning of herniated orbital tissues,

Orbital FracturesOrbital FracturesOrbital FracturesOrbital FracturesOrbital Fractures 233233233233233
reconstructing the orbital bony support, and restoringnormal orbital volume and structure.
FLOOR FRACTURES
Orbital floor fractures are common, and result fromblunt orbital trauma in which force is delivered tothe thin bones of the orbital floor, typically alongthe infraorbital canal. Often, an orbital floor fracturewill not involve the orbital rim, which is much thickerand stronger. In such an instance, the term "blow-out fracture" is often applied. The term was first usedby Smith and Regan in 1956 to describe orbitalfractures caused by striking the orbital rim with ahurling ball.74-76
The orbital floor is the shortest of the walls. Itconsists of the roof of the maxillary sinus with a smallcontribution posteriorly from the palatine bone, andcontains the infraorbital groove and canal. The edgeof the canal forms a weak spot in the floor structure.Hence, most floor fractures extend up to the canal,but the canal is often left mostly intact.
Concomitant displaced zygomatic fracturesshould be repaired first, since reduction and fixationof the ZMC fracture will often reduce the floorfracture as well.65 Floor fractures are often associatedwith medial wall fractures. When making thedecision to proceed with or forgo surgery, the totalwall area involved by the fracture, including the floorand medial wall, must be taken into account andaddressed.
The evaluation of a suspected floor fracture oftenrequires CT scanning with coronal sections, whichfacilitates the assessment of bone displacement andextraocular muscle findings. It must be emphasizedagain that muscle entrapment is a clinical diagnosis,which should be supported by the radiologicevidence but need not be.
Extraocular muscle entrapment in the context oforbital floor fractures is not uncommon.(Figure 17.4)However, the finding of muscle entrapment can besubtle, and a high level of suspicion must bemaintained (Figure 17.3). Tissue herniation is verycommon in the context of orbital floor blow-outfractures. All orbital tissues must be retrieved andrepositioned into the orbit at the time of repair;otherwise, tissue incarceration can lead to necrosisand permanent muscle dysfunction.
Our favored approach to the inferior orbit isthrough a transconjunctival approach.77-80 We usuallyavoid the lateral canthotomy and inferior cantholysis,but at times, when better exposure is required for alarger fracture, a tighter orbit, or more extensiveherniation, the canthotomy and cantholysis cangreatly aid in obtaining adequate exposure. Care mustbe taken to perform the exposure correctly to avoidpostoperative complications.81 The inferior fornix andlateral canthus are infiltrated with 2-3 ml of localanesthetic containing 1% Lidocaine, 0.25%Bupivicaine, and 1:100,000 dilution of epinephrine.The patient's face and any wounds are carefullyprepped with 5% Betadine solution, and steriledrapes are placed. We routinely place a lubricatedplastic corneal protective shield on the globe.
First, forced ductions are performed to assessfor muscle entrapment (Figure 17.7). Next, theassistant retracts the lower eyelid down with aDesmarres retractor. The surgeon uses a malleableretractor to sweep the orbital fat posteriorly anddrape the conjunctiva and lower lid retractors overthe inferior orbital rim (Figure 17.15A). The surgeonthen uses a monopolar electrocautery device with amicrodissection needle (such as the Colorado needle,Colorado biomedical, Evergreen, CO, USA) to cutthrough conjunctiva, lid retractors and orbital rimperiosteum to reveal the bony rim. The incision ismade inferiorly in the fornix (at least half waybetween the inferior edge of the tarsus and thedeepest part of the fornix) to help minimize cicatricialchanges (retraction or entropion) of the eyelidmargin (Figure 17.15B). We then use a Freer elevatorto lift the periorbita off of the orbital floor. Ourdissection is guided by the CT findings: the initialsub-periosteal dissection is performed away from thefracture and then brought to the fracture site. Thefracture edges are carefully defined and visualized.A malleable retractor is used to gently retract theglobe superiorly while the herniated orbital contentsare lifted back into the orbit using a Freer elevator.Often, the herniated tissues need to be bluntlyseparated from any early scars that form at the edgeof the fracture and in the maxillary sinus; this mustbe done slowly and carefully, taking care to avoidinjury to the infraorbital neurovascular bundle andthe perforating artery. The maxillary sinus is typicallywell visualized through the fracture (Figure 17.15C).
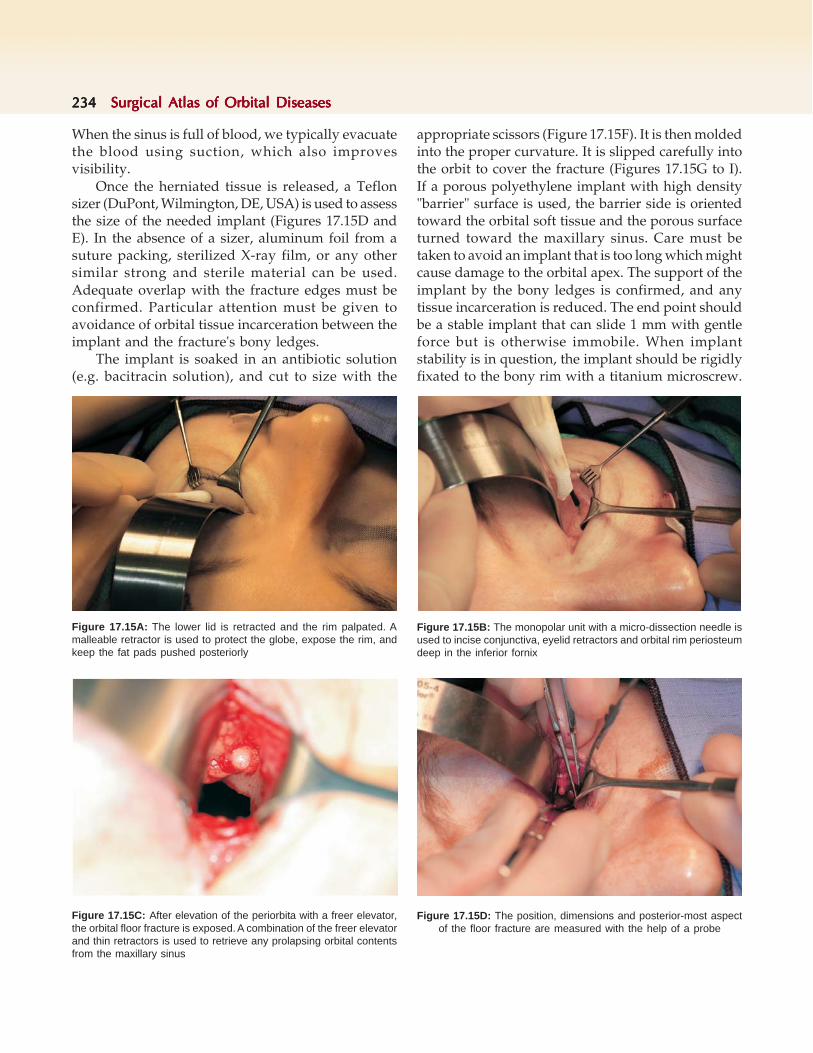
234234234234234 Surgical Atlas of Orbital DiseasesSurgical Atlas of Orbital DiseasesSurgical Atlas of Orbital DiseasesSurgical Atlas of Orbital DiseasesSurgical Atlas of Orbital Diseases
When the sinus is full of blood, we typically evacuatethe blood using suction, which also improvesvisibility.
Once the herniated tissue is released, a Teflonsizer (DuPont, Wilmington, DE, USA) is used to assessthe size of the needed implant (Figures 17.15D andE). In the absence of a sizer, aluminum foil from asuture packing, sterilized X-ray film, or any othersimilar strong and sterile material can be used.Adequate overlap with the fracture edges must beconfirmed. Particular attention must be given toavoidance of orbital tissue incarceration between theimplant and the fracture's bony ledges.
The implant is soaked in an antibiotic solution(e.g. bacitracin solution), and cut to size with the
appropriate scissors (Figure 17.15F). It is then moldedinto the proper curvature. It is slipped carefully intothe orbit to cover the fracture (Figures 17.15G to I).If a porous polyethylene implant with high density"barrier" surface is used, the barrier side is orientedtoward the orbital soft tissue and the porous surfaceturned toward the maxillary sinus. Care must betaken to avoid an implant that is too long which mightcause damage to the orbital apex. The support of theimplant by the bony ledges is confirmed, and anytissue incarceration is reduced. The end point shouldbe a stable implant that can slide 1 mm with gentleforce but is otherwise immobile. When implantstability is in question, the implant should be rigidlyfixated to the bony rim with a titanium microscrew.
Figure 17.15C: After elevation of the periorbita with a freer elevator,the orbital floor fracture is exposed. A combination of the freer elevatorand thin retractors is used to retrieve any prolapsing orbital contentsfrom the maxillary sinus
Figure 17.15A: The lower lid is retracted and the rim palpated. Amalleable retractor is used to protect the globe, expose the rim, andkeep the fat pads pushed posteriorly
Figure 17.15B: The monopolar unit with a micro-dissection needle isused to incise conjunctiva, eyelid retractors and orbital rim periosteumdeep in the inferior fornix
Figure 17.15D: The position, dimensions and posterior-most aspectof the floor fracture are measured with the help of a probe

Orbital FracturesOrbital FracturesOrbital FracturesOrbital FracturesOrbital Fractures 235235235235235
Figure 17.15E: A Teflon sizer is used to assesscoverage of the fracture
Figure 17.15F: Once the correct sizer is identified, the Medporimplant is cut to size
Figures 17.15G to I: The implant is placed on top of the fracture. Care must be taken not to incarcerate anyorbital tissues between the implant and the orbital floor
G
H I

236236236236236 Surgical Atlas of Orbital DiseasesSurgical Atlas of Orbital DiseasesSurgical Atlas of Orbital DiseasesSurgical Atlas of Orbital DiseasesSurgical Atlas of Orbital Diseases
Figure 17.15J: Once the implant is stable, the eyelid retractors arereapproximated using buried interrupted sutures
A screw can be placed right through the MedporBarrier implant or through the TITAN MTB implant.Some surgeons favor surgical glue for fixating theimplant temporarily. The Desmarres retractor is thenremoved, and the eyelid retractors sutured withburied, interrupted 7-0 polyglactin (Vicryl) sutureusing 3-point fixation (Figure 17.15H). Theconjunctiva is left unsutured.
When no bony ledge is present to support thefracture, cantilevering of the TITAN implant or aMedpor Channel plate over the rim can provide rigidfixation. Some surgeons favor titanium mesh in thissituation.
Other methods of fixation include the use of fibrinsealant (such as Tisseel, Baxter, Deerfield, IL, USA)and biological glue. BioGlue (CryoLife, Kennesaw,GA, USA) is a two-component glue, containingengineered bovine albumin in one tube and aglutaraldehyde solution in the other. When the twosubstances mix, the glutaraldehyde cross-linksalbumin molecules to each other and to thesurrounding proteins. Glutaraldehyde cross-linkingresembles a peptide bond, and hence can easily formcovalent bonds among proteins in contact with thechemical. When a porous implant is used, the albumininfiltrates through the pores as it gets cross-linked,resulting in strong biocompatible chemical bondingof the implant to the surrounding tissues. The use ofbiological glues and sealants is particularly usefulwhen implant stability is in question, yet the surgicalexposure is inadequate for complete rigid fixation(often because the globe should only be retractedgently and carefully).
MEDIAL WALL FRACTURES
Medial wall blowout fractures are common buthistorically were under-diagnosed because they canbe asymptomatic in the acute post-traumaticphase.4, 65 The nearly ubiquitous use of CT scanningin the United States in the evaluation of facial fractureshas made the diagnosis of medial fractures mucheasier.82 However, when CT is unavailable, theevaluating physician must maintain a high level ofsuspicion. Epistaxis can be associated with medialwall fractures because of tears in the sinus mucosa.The epistaxis is typically self-limited. Vision-threatening orbital hemorrhage can occur if theanterior or posterior ethmoidal vessels are injured.It is important to remind patients to avoid blowingtheir nose, since this can lead to orbital emphysemaand a compartment syndrome (Figures 17.16A andB).43, 83
The thin lamina papyracea constitutes most ofthe medial wall of the orbit, behind the posteriorlacrimal crest. The medial orbital wall is completedposteriorly by the lesser wing of the sphenoid, andanteriorly by the lacrimal bone. Both the sphenoidand the lacrimal bones are thicker. Hence, medialwall fractures occur because of the weakness of thethin lamina papyracea, and are typically localized atthe boundary between the lamina papyracea and oneof the thicker bones. Medial wall fractures commonlyoccur in the context of orbital floor blowout fractures,but can also occur in isolation.4, 26 They can also beassociated with nasal fractures, which can lead to
Figures 17.16A and B: Orbital/periorbital emphysema. Monocularpatient was assaulted with a blow to the left orbit. He presented tothe emergency department after blowing his nose, leading to severepain and reduced vision. In the ER, his intraocular pressure wasmeasured at 60 mm Hg. Emergent lateral canthotomy and inferiorcantholysis were performed, resulting in decompression of the orbit,restoration of vision and rapid decline in intraocular pressure to theteens. A CT scan following the cantholysis revealed air in the orbit.His lateral canthus was repaired 4 days later
A B

Orbital FracturesOrbital FracturesOrbital FracturesOrbital FracturesOrbital Fractures 237237237237237
telecanthus and possible damage to the nasolacrimaldrainage apparatus.84, 85
Described approaches to the medial wall fractureinclude a Lynch incision in the medial canthus, abicoronal incision, a medial upper lid crease incision,or a transconjunctival incision. However, ourpreferred approach is the transcaruncular incision.86-
88 When the medial wall fracture is large, or associatedwith a floor fracture, multiple incisions may benecessary, such as a secondary lower lid fornixincision.26, 89
The transcaruncular approach requires meticuloushemostasis in order to properly expose and visualizethe fracture,. Pinpoint cautery with a micro-dissectionneedle (e.g. Colorado needle, Colorado Biomedical,Evergreen, CO, USA) is very helpful, as is the use ofthrombin solution, absorbable gelatin sponge(Gelfoam, Pfizer), FloSeal (a combination of gelatinfoam and thrombin, Baxter) or 3% hydrogen peroxidesolution. Care must be taken with hydrogenperoxide, since it can inhibit tissue healing, and itsuse has been associated with air embolization.90-92
Good lighting is also important, and a head-mountedlight source is nearly always used in our cases.
Prior to initiating surgical repair, forced ductionsare performed to assess for muscle entrapment
(Figure 17.7). The transcaruncular approach beginswith infiltration of the medial fornix with localanesthetic containing 1:100,000 dilution of epine-phrine. An incision is made through the caruncleanterior to the plica semilunaris using Westcottscissors.86, 87 The incision is extended superiorly andinferiorly along the conjunctival fornices in order tocreate sufficient exposure and prevent uncontrolledtearing of the conjunctiva intraoperatively. Asufficient distance away from the canaliculi ismaintained. Curved Stevens tenotomy scissors arethen used to bluntly dissect along Horner's muscle,which inserts on the posterior lacrimal crest. Caremust be taken not to iatrogenically fracture the laminapapyracea just posterior to the crest, since this willmake subsequent elevation of the periorbita morechallenging. Once the posterior crest is exposed, theperiorbita is incised with a monopolar unit and amicrodissection needle. Achieving excellenthemostasis is critical at this point. Next, a Freerelevator is used to lift the periorbita anteriorly inorder to fully expose the posterior lacrimal crest. Theperiorbita is then lifted posteriorly to create a sub-periosteal dissection plane along the laminapapyracea (Figures 17.17A and B). The anteriorethmoidal neurovascular bundle is typically foundapproximately 24 mm posterior to the posteriorlacrimal crest, along the fronto-ethmoidal suture line.This neurovascular bundle is carefully and thoroughlycauterized with a bipolar cautery unit, and thendivided with the monopolar unit. The subperiostealdissection is then completed to fully expose thefracture.
Figure 17.17B: Inferior oblique isolation. The IO muscle may be taggedwith 6-0 polyglactin sutures and the origin disinserted to provide goodexposure
Figure 17.17A: Transcaruncular exposure of the left medial wallfollowing disinsertion of the inferior oblique muscle

238238238238238 Surgical Atlas of Orbital DiseasesSurgical Atlas of Orbital DiseasesSurgical Atlas of Orbital DiseasesSurgical Atlas of Orbital DiseasesSurgical Atlas of Orbital Diseases
If the fracture is very posterior, the posteriorethmoidal bundle may be encountered. In such cases,the posterior ethmoidal bundle should be carefullycauterized with the bipolar cautery to avoid intra-or postoperative hemorrhaging. The posteriorbundle is typically found approximately 12 mm fromthe anterior bundle, and on average only 6 mm fromthe optic canal.
After adequate hemostasis and exposure areachieved, herniated orbital tissues are retrieved andrepositioned into the orbit. The fracture size ismeasured, and implant properly sized. We havefound Teflon implant sizers to be very useful at thisstep. The implant is then placed over the fracture,ensuring that no orbital tissues are left incarcerated.When using a Medpor Barrier plate, the barrier sideshould be turned toward the orbit to reduce the riskof tissue scarring to the implant.
If the fracture extends inferiorly to involve theorbital floor, an inferior fornix transconjunctivalincision can be made to increase exposure. At times,the inferior oblique muscle must be disinserted fromits origin. At the end of the case, the oblique is thenreapproximated to its origin with 6-0 polyglactinsuture. The floor and medial wall fractures can berepaired with a single implant. For this, the MedporTITAN Barrier implant is ideal, since it can be moldedinto the required semi-cylindrical shape and willmaintain this shape. Such a large implant is betterplaced through the inferior fornix incision, and thenthe positioning adjusted through the caruncularincision. Some surgeons advocate multiple implantsthat can overlap, using very thin implants.26
Closing the transcaruncular incision involvesplacing one to three buried interrupted 6-0 fast-absorbing plain gut sutures to close the caruncularconjunctiva.
Medial wall fractures are particularly challengingto repair when they are part of a comminuted naso-ethmoid fracture.93 In these circumstances, post-traumatic telecanthus is common, and can be quitedisfiguring (Figure 17.9). Repair of the fracturedposterior lacrimal crest and stabilization of the medialcanthal tendon should be attempted during primaryrepair. Good exposure is critical, and when the naso-ethmoid fractures are part of panfacial trauma,a bicoronal approach has many merits.94 Transnasalwiring has been described for the repair of post-
traumatic telecanthus,93, 95 and may be necessary incombination with miniplate fixation when repairingseverely comminuted naso-ethmoid fractures.However, whenever possible, we favor miniplatefixation of the comminuted bones and the medialcanthal tendon (Figures 17.10A and B).96
LATERAL WALL ANDZYGOMATICO MAXILLARYFRACTURES
Fractures of the lateral wall of the orbit are common,and typically result from direct blunt trauma to thezygoma and lateral orbital rim. The zygomaarticulates with the sphenoid, maxillary, frontal andtemporal bones. Therefore, fractures of the zygomacan often disrupt the architecture of the entire region,and hence are often referred to as zygomaticomalarcomplex fractures (ZMC fractures). Importantly, theorbital floor is always fractured in the context of adisplaced zygomatic fracture, but will typically reduceonce the zygoma fracture is reduced.65
Numerous surgical approaches to the ZMCfracture have been described for open reduction,including transconjunctival,78, 97-99 intraoral,100 temporal(Gillies), brow incision and bicoronal flap. Inaddition, some surgeons advocate closed reductionor observation for non-comminuted and uncom-plicated zygoma fractures.101, 102 The approach to theZMC fracture is greatly aided by careful evaluationof the CT scan, and different classification systemshave been proposed in an effort to provide guidanceto proper preoperative planning. Whicheverapproach is chosen, a reduction of the zygoma shouldattempt to replace the zygoma back into its normalanatomic location. Because the zygoma can rotatearound an axis formed by the inferolateral orbitalrim, reduction of just the fronto-zygomatic andzygomatico-maxillary sutures is not sufficient: a thirdpoint of alignment should be confirmed in order toensure proper reduction and avoid late enoph-thalmos.65 Exploration of the lateral floor of the orbitcan greatly assist in the fracture reduction, as wellas help avoid orbital tissue incarceration betweenthe zygoma and the sphenoid bones.
When non-comminuted fracture displacement isnoted on examination and CT scans, we favor surgicalexploration and repair through a subconjunctival

Orbital FracturesOrbital FracturesOrbital FracturesOrbital FracturesOrbital Fractures 239239239239239
inferior fornix and lateral canthotomy approach.99
First, forced ductions are performed to assess forpossible muscle entrapment. The lateral canthus andinferior fornix are infiltrated with local anestheticcontaining 1:100,000 dilution of epinephrine, and alubricated plastic corneal protective shield is placedon the eye. A lateral canthotomy and inferiorcantholysis (and sometimes superior cantholysis, too),are performed to release the lateral canthalattachments and provide good exposure of the lateralrim. The lateral inferior fornix is then incised to revealthe inferolateral rim. The periosteum is incised alongthe entire exposed rim, and a freer elevator is usedto lift the periosteum and expose the rim from abovethe fronto-zygomatic suture down to below themaxillo-zygomatic suture and medially to theinfraorbital canal. When a depressed floor fractureis present, the inferior fornix incision can be carriedout medially to provide full exposure of the floor.
Next, the zygoma must be properly reduced andaligned along three points: the fronto-zygomaticsuture, the maxillo-zygomatic suture at the inferiorrim, and a third point that can be the zygomatic-sphenoid suture at the lateral orbital floor, thezygomatico-maxillary buttress, and/or the zygomaticarch.65, 69, 70, 99 The first two points ensure anterioralignment, whereas a third point ensures posterioralignment. Failure to achieve posterior alignment canpredispose to enophthalmos by enlarging theposterior orbital volume (Figure 17.8).
A useful tool in ZMC fracture alignment has beenthe T-bar screw, also known as the Carroll-Girardscrew (Walter Lorenz Surgical, Jacksonville, FL,USA).99, 103 This cork-screw-like instrument is screwedonto the thick bone at the malar eminence and usedto manipulate the zygoma into proper position(Figure 17.18A and B). This tool is particularly usefulin minimally-comminuted fractures, and allows forexceptional control of the zygoma through a small-incision approach. However, when severe com-minution exists without solid bone for placement ofthe screw, multiple incisions would be required toachieve complete reduction and rigid fixation.
Following reduction of the fracture, fixation isaccomplished using titanium miniplates. Forcedductions are performed again to ensure that noentrapment was caused by the fracture reduction.The lateral floor is explored to assess the zygomatico-
sphenoid suture. Next, the periosteum is sutured andthe lower lid retractors are reapproximated usingburied interrupted 7-0 polyglactin suture. The lateralcanthal tendon is resuspended to the periosteum atWhitnall's tubercle. If lower lid laxity is present,horizontal tightening is performed to reduce the riskof postoperative lower lid retraction. Placement of aFrost suture can be done in the presence ofconcomitant lower lid trauma and when the risk ofcicatricial ectropion is felt to be high.
LATE AND SECONDARYFRACTURE REPAIR
As far back as 1957, Smith and Regan made the pointthat "late cases are far more difficult to correct."74
Nevertheless, thirty years ago, many surgeonsadvocated observation and delay of surgery for allbut the most severe orbital fractures.104, 105 However,with the advent of CT scanning, an evolution inimplants and fixation devices, and greatly improvedsurgical techniques, primary repair has become thestandard of care for symptomatic or large orbitalfractures. Still, there are occasions when late repairof orbital fractures is still encountered. Some reasonsinclude lack of access to medical care followingtrauma, misdiagnosis, multiple medical problemspreventing timely repair, or a suboptimal repair thatrequires reoperation.
The goal of late fracture repair is the same as forearly repair, namely to restore orbital anatomy andreduce or eliminate any symptoms. Late repair isnearly always complicated by significant fibrosis andabnormal anatomy that can distort the normalanatomic landmarks. When dysmotility is a significantsymptom and its repair a main goal of the operation,
Figures 17.18A and B: The Carroll-Girard (T-bar) screw is a powerfultool for 3-dimensional control and manipulation of the zygomatic ormaxillary bones during orbital fracture repair. After drilling a smallguidance hole, the screw is positioned and attached to the T bar(Photos courtesy of Benjamin Marcus, MD, University of Wisconsin)
A B

240240240240240 Surgical Atlas of Orbital DiseasesSurgical Atlas of Orbital DiseasesSurgical Atlas of Orbital DiseasesSurgical Atlas of Orbital DiseasesSurgical Atlas of Orbital Diseases
good motility measurements are critical, as is theassistance of an expert in adult strabismus.Dysmotility that results from entrapment can becorrected when the muscle entrapment is reduced.However, if the dysmotility is the result ofirreversible muscle or nerve damage, further orbitalsurgery will not restore normal motility, and cancause a significant increase in orbital fibrosis inaddition to the risk of an unnecessary orbital surgery.Instead, strabismus surgery would be a better option.Hence, careful diagnosis of the underlying cause ofdysmotility is crucial. In our practice, we will obtaina CT scan to evaluate the bony anatomy, andoccasionally a dynamic MRI scan to evaluate the causeof dysmotility. In addition, we request a consultationfrom an expert in strabismus, and employ a team-oriented approach to caring for these patients.
A common reason for late surgical repair is severeenophthalmos (Figure 17.11). In a paper by Koo etal. (2006),64 clinically apparent enophthalmos wasfound when enophthalmos was measured at 3-4 mmor more. In such cases, patients must weigh theirsymptoms against the risks of surgical complications.It is important to emphasize that counseling andmanaging expectations are very important forachieving a result that is satisfactory to both thesurgeon and the patient.
Our approach to enophthalmos repair stressespre-operative counseling in order to clearly definewhat the patient desires and what we believe can beaccomplished safely. Our surgical techniqueemphasizes good exposure, optimized illumination,and meticulous hemostasis. We employ the sameincisions that we utilize for early fracture repair,namely the inferior fornix, lateral canthotomy/cantholysis, and transcaruncular incisions. Often, themain decision is whether to attempt reduction of ahealed fracture or to focus on the enophthalmos andprovide orbital volume augmentation through theuse of porous polyethylene implants. Given theadded risk of re-fracturing and reducing healedfractures, we usually opt for orbital volumeenhancement and accept the mild deformities thatmay be associated with poorly positioned but healedZMC fractures. For volume enhancement, we typicallyutilize porous polyethylene wedge implants that areshaped to reduce orbital volume or implantswith titanium that can be fixated at the orbital rim(Figure 17.19).
CONCLUSION
Orbital fractures are commonly encountered by theophathlmologist, otolaryngologist, and orbitofacialplastic surgeon. Proper treatment requires a completeophthalmic evaluation, systematic review of theradiographic evidence, and thoughtful surgicalplanning with careful attention to anatomic principles.The use of smaller and hidden incisions (particularlyconjunctival incisions) has made surgical treatmentof orbital fractures more esthetically satisfying whilereducing the risk of complications. The choice ofimplant materials has never been greater, providingthe surgeon with options that can be tailored to theneeds of the patients. While surgical repair of orbitalfractures has advanced considerably over the past50 years, there is no doubt that we will continue tosee innovations and further improvements in surgicaltechniques, to the continued benefit of our patients.
REFERENCES
1. Zide BM and Jelks GW, Surgical Anatomy of the Orbit. (1sted). 1985: Lippincott Williams & Wilkins 88.
2. Morriss-Kay GM. Derivation of the mammalian skull vault.J Anat 2001;199:143-51.
3. Manson PN, Hoopes JE, and Su CT. Structural pillars of thefacial skeleton: an approach to the management of Le Fortfractures. Plast Reconstr Surg 1980;66:54-62.
4. Burm JS, Chung CH, and Oh SJ. Pure orbital blowoutfracture: new concepts and importance of medial orbitalblowout fracture. Plast Reconstr Surg 1999;103:1839-49.
5. Sorni M, Guarinos J, and Penarrocha M. Implants inanatomical buttresses of the upper jaw. Med Oral PatolOral Cir Bucal 2005;10:163-8.
Figure 17.19: Medpor wedge implant. Orbital volume enhancementwill often require placement of space-occupying implants. The Medporwedge implant, which comes in both right-sided and left-sidedconfigurations, is a useful tool. Alternatively, multiple flat implants canbe stacked to achieve the appropriate amount of volume augmentation

Orbital FracturesOrbital FracturesOrbital FracturesOrbital FracturesOrbital Fractures 241241241241241
6. Kreutziger KL. Complex maxillofacial fractures:management and surgical procedures. South Med J 1982;75:783-93.
7. Karlan MS and Cassisi NJ. Fractures of the zygoma. Ageometric, biomechanical, and surgical analysis. ArchOtolaryngol 1979;105:320-7.
8. Gruss JS and Mackinnon SE. Complex maxillary fractures:role of buttress reconstruction and immediate bone grafts.Plast Reconstr Surg 1986;78:9-22.
9. Hopper RA, Salemy S, and Sze RW. Diagnosis of midfacefractures with CT: what the surgeon needs to know.Radiographics 2006;26:783-93.
10. Kim JW, Goldberg RA, and Shorr N. The inferomedialorbital strut: an anatomic and radiographic study. OphthalPlast Reconstr Surg 2002;18:355-64.
11. Goldberg RA, Shorr N, and Cohen MS. The medial orbitalstrut in the prevention of postdecompression dystopia indysthyroid ophthalmopathy. Ophthal Plast Reconstr Surg1992; 8: 32-4.
12. Rubin PA, Hatton MP, and Bilyk JR. Orbital perforatingbranch of the infraorbital artery: an important landmarkin orbital surgery. Ophthal Plast Reconstr Surg 2005; 21:447-9.
13. Koornneef L. Orbital septa: anatomy and function.Ophthalmology 1979; 86: 876-80.
14. Koornneef L and Zonneveld FW. Orbital anatomy, thedirect scanning of the orbit in three planes and their bearingson the treatment of motility disturbances of the eye afterorbital "blow-out" fractures. Acta Morphol Neerl Scand1985; 23: 229-46.
15. Yung CW, Moorthy RS, Lindley D, et al. Efficacy of lateralcanthotomy and cantholysis in orbital hemorrhage. OphthalPlast Reconstr Surg 1994; 10: 137-41.
16. Burkat CN and Lemke BN. Retrobulbar hemorrhage:inferolateral anterior orbitotomy for emergentmanagement. Arch Ophthalmol 2005; 123: 1260-2.
17. Schuknecht B and Graetz K. Radiologic assessment ofmaxillofacial, mandibular, and skull base trauma. Eur Radiol2005; 15: 560-8.
18. Hawes MJ and Dortzbach RK. Surgery on orbital floorfractures. Influence of time of repair and fracture size.Ophthalmology 1983; 90: 1066-70.
19. Wolfe SA. Autogenous bone grafts versus alloplasticmaterial in maxillofacial surgery. Clin Plast Surg 1982; 9:539-40.
20. Rubin PA, Bilyk JR, and Shore JW. Orbital reconstructionusing porous polyethylene sheets. Ophthalmology 1994;101: 1697-708.
21. Ozturk S, Sengezer M, Isik S, et al. Long-term outcomes ofultra-thin porous polyethylene implants used forreconstruction of orbital floor defects. J Craniofac Surg2005; 16: 973-7.
22. Villarreal PM, Monje F, Morillo AJ, et al. Porouspolyethylene implants in orbital floor reconstruction. PlastReconstr Surg 2002; 109: 877-85; discussion 886-7.
23. Gear AJ, Lokeh A, Aldridge JH, et al. Safety of titaniummesh for orbital reconstruction. Ann Plast Surg 2002; 48:1-7; discussion 7-9.
24. Ellis E, 3rd and Tan Y. Assessment of internal orbitalreconstructions for pure blowout fractures: cranial bonegrafts versus titanium mesh. J Oral Maxillofac Surg 2003;61: 442-53.
25. Nguyen PN and Sullivan P. Advances in the managementof orbital fractures. Clin Plast Surg 1992; 19: 87-98.
26. Su GW and Harris GJ. Combined inferior and medialsurgical approaches and overlapping thin implants fororbital floor and medial wall fractures. Ophthal PlastReconstr Surg 2006; 22: 420-3.
27. Custer PL, Lind A, and Trinkaus KM. Complications ofsupramid orbital implants. Ophthal Plast Reconstr Surg2003; 19: 62-7.
28. Choi JC, Sims CD, Casanova R, et al. Porous polyethyleneimplant for orbital wall reconstruction. J CraniomaxillofacTrauma 1995; 1: 42-9.
29. Bilyk JR, Rubin PA, and Shore JW. Correction ofenophthalmos with porous polyethylene implants. IntOphthalmol Clin 1992; 32: 151-6.
30. Romano JJ, Iliff NT, and Manson PN. Use of Medpor porouspolyethylene implants in 140 patients with facial fractures.J Craniofac Surg 1993; 4: 142-7.
31. Choi JC, Bstandig S, Iwamoto MA, et al. Porouspolyethylene sheet implant with a barrier surface: a rabbitstudy. Ophthal Plast Reconstr Surg 1998; 14: 32-6.
32. Tessier P, Kawamoto H, Matthews D, et al. Autogenousbone grafts and bone substitutes--tools and techniques: I.A 20,000-case experience in maxillofacial and craniofacialsurgery. Plast Reconstr Surg 2005; 116: 6S-24S; discussion92S-94S.
33. Tessier P. Autogenous bone grafts taken from the calvariumfor facial and cranial applications. Clin Plast Surg 1982; 9:531-8.
34. Kusiak JF, Zins JE, and Whitaker LA. The earlyrevascularization of membranous bone. Plast Reconstr Surg1985; 76: 510-6.
35. Zins JE and Whitaker LA. Membranous versusendochondral bone: implications for craniofacialreconstruction. Plast Reconstr Surg 1983; 72: 778-85.
36. Craft PD and Sargent LA. Membranous bone healing andtechniques in calvarial bone grafting. Clin Plast Surg 1989;16: 11-9.
37. Kline RM, Jr. and Wolfe SA. Complications associated withthe harvesting of cranial bone grafts. Plast Reconstr Surg1995; 95: 5-13; discussion 14-20.
38. Jackson IT, Adham M, Bite U, and Marx R. Update on cranialbone grafts in craniofacial surgery. Ann Plast Surg 1987;18: 37-40.
39. Jackson IT, Costanzo C, Marsh WR, and Adham M. Orbitalexpansion in plagiocephaly. Br J Plast Surg 1988; 41: 16-9.
40. Zins JE, Weinzweig N, and Hahn J. A simple fail-safe methodfor the harvesting of cranial bone. Plast Reconstr Surg 1995;96: 1444-7.

242242242242242 Surgical Atlas of Orbital DiseasesSurgical Atlas of Orbital DiseasesSurgical Atlas of Orbital DiseasesSurgical Atlas of Orbital DiseasesSurgical Atlas of Orbital Diseases
41. Kontio RK, Laine P, Salo A, et al. Reconstruction of internalorbital wall fracture with iliac crest free bone graft: clinical,computed tomography, and magnetic resonance imagingfollow-up study. Plast Reconstr Surg 2006; 118: 1365-74.
42. Holck DE and Ng JD, Eds. Evaluation and Treatment ofOrbital Fractures: A Multidisciplinary Approach. (1st ed.)2005, Saunders. 544.
43. Reeves DL, Lucarelli MJ, and Rose JG, Jr. Severesubcutaneous emphysema following orbital blowoutfracture. Ophthal Plast Reconstr Surg 2005; 21: 465-7.
44. Messina BA. Herbal supplements: Facts and myths--talkingto your patients about herbal supplements. J PerianesthNurs 2006; 21: 268-78; quiz 279-81.
45. Ang-Lee MK, Moss J, and Yuan CS. Herbal medicines andperioperative care. Jama 2001; 286: 208-16.
46. Ben Simon GJ, Bush S, Selva D, and McNab AA. Orbitalcellulitis: a rare complication after orbital blowout fracture.Ophthalmology 2005; 112: 2030-4.
47. Martin B and Ghosh A. Antibiotics in orbital floor fractures.Emerg Med J 2003; 20: 66.
48. Westfall CT and Shore JW. Isolated fractures of the orbitalfloor: risk of infection and the role of antibiotic prophylaxis.Ophthalmic Surg 1991; 22: 409-11.
49. Miles BA, Potter JK, and Ellis E, 3rd. The efficacy ofpostoperative antibiotic regimens in the open treatment ofmandibular fractures: a prospective randomized trial. J OralMaxillofac Surg 2006; 64: 576-82.
50. Classen DC, Evans RS, Pestotnik SL, et al. The timing ofprophylactic administration of antibiotics and the risk ofsurgical-wound infection. N Engl J Med 1992; 326: 281-6.
51. Flood TR, McManners J, el-Attar A, and Moos KF.Randomized prospective study of the influence of steroidson postoperative eye-opening after exploration of theorbital floor. Br J Oral Maxillofac Surg 1999; 37: 312-5.
52. Millman AL, Della Rocca RC, Spector S, et al. Steroids andorbital blowout fractures–a new systematic concept inmedical management and surgical decision-making. AdvOphthalmic Plast Reconstr Surg 1987; 6: 291-300.
53. Courtney DJ, Thomas S, and Whitfield PH. Isolated orbitalblowout fractures: survey and review. Br J Oral MaxillofacSurg 2000; 38: 496-504.
54. Jordan DR, Allen LH, White J, et al. Intervention withindays for some orbital floor fractures: the white-eyedblowout. Ophthal Plast Reconstr Surg 1998; 14: 379-90.
55. Koltai PJ, Amjad I, Meyer D, and Feustel PJ. Orbital fracturesin children. Arch Otolaryngol Head Neck Surg 1995; 121:1375-9.
56. Chandler DB and Rubin PA. Developments in theunderstanding and management of pediatric orbitalfractures. Int Ophthalmol Clin 2001; 41: 87-104.
57. Hatton MP, Watkins LM, and Rubin PA. Orbital fracturesin children. Ophthal Plast Reconstr Surg 2001; 17: 174-9.
58. Egbert JE, May K, Kersten RC, and Kulwin DR. Pediatricorbital floor fracture: direct extraocular muscleinvolvement. Ophthalmology 2000; 107: 1875-9.
59. Bansagi ZC and Meyer DR. Internal orbital fractures in thepediatric age group: characterization and management.Ophthalmology 2000; 107: 829-36.
60. Burnstine MA. Clinical recommendations for repair ofisolated orbital floor fractures: an evidence-based analysis.Ophthalmology 2002; 109: 1207-10; discussion 1210-1; quiz1212-3.
61. Grant JH, 3rd, Patrinely JR, Weiss AH, et al. Trapdoorfracture of the orbit in a pediatric population. Plast ReconstrSurg 2002; 109: 482-9; discussion 490-5.
62. Mauriello JA, Jr. Complications of orbital trauma surgery.Adv Ophthalmic Plast Reconstr Surg 1987; 7: 99-115.
63. Jordan DR, St Onge P, Anderson RL, et al. Complicationsassociated with alloplastic implants used in orbital fracturerepair. Ophthalmology 1992; 99: 1600-8.
64. Koo L, Hatton MP, and Rubin PA. When is enophthalmos"significant"? Ophthal Plast Reconstr Surg 2006; 22: 274-7.
65. Pearl RM. Treatment of enophthalmos. Clin Plast Surg 1992;19: 99-111.
66. Cooper WC. A method for volume determination of theorbit and its contents by high resolution axial tomographyand quantitative digital image analysis. Trans AmOphthalmol Soc 1985; 83: 546-609.
67. Raskin EM, Millman AL, Lubkin V, et al. Prediction of lateenophthalmos by volumetric analysis of orbital fractures.Ophthal Plast Reconstr Surg 1998; 14: 19-26.
68. Fan X, Li J, Zhu J, et al. Computer-assisted orbital volumemeasurement in the surgical correction of lateenophthalmos caused by blowout fractures. Ophthal PlastReconstr Surg 2003; 19: 207-11.
69. Rohner D, Tay A, Meng CS, et al. The sphenozygomaticsuture as a key site for osteosynthesis of theorbitozygomatic complex in panfacial fractures: abiomechanical study in human cadavers based on clinicalpractice. Plast Reconstr Surg 2002; 110: 1463-71; discussion1472-5.
70. Gruss JS, Van Wyck L, Phillips JH, and Antonyshyn O. Theimportance of the zygomatic arch in complex midfacialfracture repair and correction of posttraumaticorbitozygomatic deformities. Plast Reconstr Surg 1990; 85:878-90.
71. Burnstine MA. Clinical recommendations for repair oforbital facial fractures. Curr Opin Ophthalmol 2003; 14:236-40.
72. Boush GA and Lemke BN. Progressive infraorbital nervehypesthesia as a primary indication for blow-out fracturerepair. Ophthal Plast Reconstr Surg 1994; 10: 271-5.
73. Anderson AG, Frank TW, and Loftus JM. Fractures of themedial infraorbital rim. Arch Otolaryngol Head Neck Surg1988; 114: 1461-3.
74. Smith B and Regan WF, Jr. Blow-out fracture of the orbit;mechanism and correction of internal orbital fracture. AmJ Ophthalmol 1957; 44: 733-9.
75. Converse JM, Smith B, Obear MF, and Wood-Smith D.Orbital blowout fractures: a ten-year survey. Plast ReconstrSurg 1967; 39: 20-36.

Orbital FracturesOrbital FracturesOrbital FracturesOrbital FracturesOrbital Fractures 243243243243243
76. Converse JM and Smith B. Blowout fracture of the floor ofthe orbit. Trans Am Acad Ophthalmol Otolaryngol 1960;64: 676-88.
77. Tenzel RR and Miller GR. Orbital blow-out fracture repair,conjunctival approach. Am J Ophthalmol 1971; 71: 1141-2.
78. Tessier P The conjunctival approach to the orbital floor andmaxilla in congenital malformation and trauma. J MaxillofacSurg 1973; 1: 3-8.
79. Kushner GM Surgical approaches to the infraorbital rimand orbital floor: the case for the transconjunctivalapproach. J Oral Maxillofac Surg 2006; 64: 108-10.
80. Goldberg RA, Lessner AM, Shorr N, and Baylis HI. Thetransconjunctival approach to the orbital floor and orbitalfat. A prospective study. Ophthal Plast Reconstr Surg 1990;6: 241-6.
81. Westfall CT, Shore JW, Nunery WR, et al. Operativecomplications of the transconjunctival inferior fornixapproach. Ophthalmology 1991; 98: 1525-8.
82. Grove AS, Jr., Tadmor R, New PF, and momose KJ. Orbitalfracture evaluation by coronal computed tomography. AmJ Ophthalmol 1978; 85: 679-85.
83. Jordan DR, White GL, Jr., Anderson RL, and Thiese SM.Orbital emphysema: a potentially blinding complicationfollowing orbital fractures. Ann Emerg Med 1988;17:853-5.
84. Gruss JS, Hurwitz JJ, Nik NA, and Kassel EE. The patternand incidence of nasolacrimal injury in naso-orbital-ethmoid fractures: the role of delayed assessment anddacryocystorhinostomy. Br J Plast Surg 1985; 38:116-21.
85. Becelli R, Renzi G, Mannino G, et al. Posttraumaticobstruction of lacrimal pathways: a retrospective analysisof 58 consecutive naso-orbitoethmoid fractures. J CraniofacSurg 2004; 15: 29-33.
86. Garcia GH, Goldberg RA, and Shorr N. The transcaruncularapproach in repair of orbital fractures: a retrospectivestudy. J Craniomaxillofac Trauma 1998; 4: 7-12.
87. Shorr N, Baylis HI, Goldberg RA, and Perry JD.Transcaruncular approach to the medial orbit and orbitalapex. Ophthalmology 2000; 107: 1459-63.
88. Kim S, Helen Lew M, Chung SH, et al. Repair of medialorbital wall fracture: transcaruncular approach. Orbit 2005;24: 1-9.
89. Kim KS, Kim ES, and Hwang JH. Combined transcutaneoustransethmoidal/transorbital approach for the treatmentof medial orbital blowout fractures. Plast Reconstr Surg2006; 117: 1947-55.
90. Rees JE. Where have all the bubbles gone? An ode toHydrogen peroxide, the champagne of all wound cleaners.Accid Emerg Nurs 2003; 11: 82-4.
91. Miranda P, Cabrera A, Esparza J, and Jerez A. An oxygenembolism after hydrogen peroxide scalp infiltration. Caseillustration. J Neurosurg 2006; 104: 152.
92. Detorakis ET, Drositis I, Drakonaki EE, et al.Pneumocephalus and presumed meningitis followinginconspicuous penetrating periocular trauma. ActaOphthalmol Scand 2004; 82: 603-5.
93. Sargent LA and Rogers GF. Nasoethmoid orbital fractures:diagnosis and management. J Craniomaxillofac Trauma1999; 5: 19-27.
94. Shaw RC and Parsons RW. Exposure through a coronalincision for initial treatment of facial fractures. PlastReconstr Surg 1975; 56: 254-9.
95. Leipziger LS and Manson PN. Nasoethmoid orbitalfractures. Current concepts and management principles.Clin Plast Surg 1992; 19: 167-93.
96. Shore JW, Rubin PA, and Bilyk JR. Repair of telecanthusby anterior fixation of cantilevered miniplates.Ophthalmology 1992; 99: 1133-8.
97. Converse JM, Firmin F, Wood-Smith D, and FriedlandJA. The conjunctival approach in orbital fractures. PlastReconstr Surg 1973; 52: 656-7.
98. Nunery WR. Lateral canthal approach to repair of trimalarfractures of the zygoma. Ophthal Plast Reconstr Surg 1985;1: 175-83.
99. Chang EL, Hatton MP, Bernardino CR, and Rubin PA.Simplified repair of zygomatic fractures through atransconjunctival approach. Ophthalmology 2005; 112:1302-9.
100. Courtney DJ. Upper buccal sulcus approach tomanagement of fractures of the zygomatic complex: aretrospective study of 50 cases. Br J Oral Maxillofac Surg1999; 37: 464-6.
101. Zingg M, Laedrach K, Chen J, et al. Classification andtreatment of zygomatic fractures: a review of 1,025 cases.J Oral Maxillofac Surg 1992; 50: 778-90.
102. Honig JF and Merten HA. Classification system andtreatment of zygomatic arch fractures in the clinical setting.J Craniofac Surg 2004; 15: 986-9.
103. Kreutziger KL. Zygomatic fractures: reduction with theT-bar screw. South Med J 1992; 85: 1193-202.
104. Emery JM, Noorden GK, and Sclernitzauer DA. Orbitalfloor fractures: long-term follow-up of cases with andwithout surgical repair. Trans Am Acad OphthalmolOtolaryngol 1971; 75: 802-12.
105. Putterman AM, Stevens T, and Urist MJ. Nonsurgicalmanagement of blow-out fractures of the orbital floor.Am J Ophthalmol 1974; 77: 232-9.

244244244244244 Surgical Atlas of Orbital DiseasesSurgical Atlas of Orbital DiseasesSurgical Atlas of Orbital DiseasesSurgical Atlas of Orbital DiseasesSurgical Atlas of Orbital Diseases
Kasturi Bhattacharjee, Harsha Bhattacharjee, Ganesh Kuri, Shyamanga Borooah
Secondary and MetastaticSecondary and MetastaticSecondary and MetastaticSecondary and MetastaticSecondary and MetastaticOrbital TumorsOrbital TumorsOrbital TumorsOrbital TumorsOrbital Tumors
Figure 18.1: Bilateral retinoblastoma with orbital extension
Secondary orbital tumors are due to the extensionof a primary tumor into the orbit. The orbit may beaffected secondarily by tumors arising in the adjacentstructures. Such tumors commonly arise from theglobe, lids, conjunctiva, nasopharynx, paranasal sinus,and lacrimal sac. Intracranial tumors can also haveintraorbital extension. Several factors contribute tothe extension of tumors into the orbit. These includethe site of the primary tumor, aggressiveness of thetumor and adequacy of initial treatment.
Orbital Extension of Intraocular Tumors
This is more commonly seen in less developedcountries due to a delay in presentation for treatmentof a primary tumor. In more advanced countriessystems of ocular screening have reduced both themorbidity and mortality from these neoplasms.Though most intraocular tumors can invade the orbitif not managed aggressively and adequately,however higher frequency is encountered amongstretinoblastoma, medulloepithelioma and uvealmelanoma.1 Retinoblastoma and medulloepitheliomaare usually found in pediatric population whilstmelanomas are more common amongst adults.
Orbital Extension of Retinoblastoma
Retinoblastoma (RB) is the most common childhoodintraocular tumor. The incidence is approximately 1in 15,000 to 1 in 20,000 live births. Diagnosis andtreatment can salvage life. However, early diagnosiscan salvage not only the eye, but also sight. Indeveloped countries the mortality rate fromextraocular retinoblastoma is as low as 5 %, but thisincreases to over 90% in underdeveloped countries.2
Retinoblastomas generally remain within theglobe for a considerable duration of time. However,once they penetrate Bruch's membrane they becomehighly aggressive. With time this leads ontoextraocular spread. This may remain localized tothe soft tissues surrounding the eye or the orbit(Figure 18.1) or may extend via the optic nerve intothe brain (Figure 18.2) and meninges with subsequentseeding of the spinal fluid. Distant metastasis mayoccur through hematogenous spread involving thebones, bone marrow, liver, pancreas, kidney, spleen,lungs and gonads.
Extraocular extension of retinoblastoma into theorbit most commonly occurs through the peri-emissarial blood vessels. Extension also occursdirectly into the choroid and through erosion of theglobe. Once the tumor enters the orbit, it enters astate of neoplastic proliferation and rapidly developsinto an orbital mass. Spread of retinoblastoma into
18C H A P T E R

Secondary and Metastatic Orbital TumorsSecondary and Metastatic Orbital TumorsSecondary and Metastatic Orbital TumorsSecondary and Metastatic Orbital TumorsSecondary and Metastatic Orbital Tumors 245245245245245
the central nervous system usually occurs by directinvasion of the optic nerve and the subarachnoidspace by the tumor cells. Very rarely retinoblastomaof peripapillary choroid can egress into the centralnervous system via the posterior ciliary vessels.
Orbital invasion of retinoblastoma carries a poorprognosis and is a predictive factor of metastasis(Figures 18.3 and 18.4). Kapelman JE et al3 produceda multivariate analysis suggesting that orbitalinvasion and optic nerve invasion were the mosthighly predictive risk factors of death fromretinoblastoma.
The main goal of treatment for extraocularretinoblastoma is to extend survival and the diseasefree interval. Rootman J et al4 reported that only 9.4% of patients with orbital extension lived more than2 years after diagnosis. It was noted that orbitalextension of retinoblastoma was frequentlyassociated with distant metastasis. ZyguiskaManchowa H et al5 had reported 14 cases ofextraocular retinoblastoma or with recurrence ofwhich 78.6% had died.
Though there is no proven effective therapy forextraocular retinoblastoma, it should be managedwith aggressive chemotherapy and radiotherapy tothe orbit. When there is meningeal involvementcraniospinal irradiation and/or intrathecal chemo-therapy is indicated. However, often palliativetreatment is required if therapy is ineffective. Highlyindividualized aggressive therapy enhances longersurvival in patients with overt extraocularretinoblastoma (Figure 18.5). Chantada G hadreported use of neoadjuvant combination chemo-therapy followed by surgery in the form ofenucleation and/or resection of residual orbital tumormass and adjuvant chemotherapy and radiotherapy.6
Chemotherapy includes Vincristine, Etoposide,Carboplatin, Cyclophosphamide, Doxorubicin,Idorubicin, and Cisplatin.7 They reported that thistreatment regimen was highly efficacious for patientswith orbital extension of retinoblastoma.
Figure 18.2: CT brain of the child in figure 18.1 revealed a pinealomagiving a trilateral presentation of RB .Classic of hereditary type
Figure 18.3: Bilateral advanced retinoblastoma with extraocularextension involving the orbit and adnexae on the left side
Figure 18.4: Bilateral retinoblastoma. The child had undergone sixcycles of chemotherapy. The left eye was salvaged , however theright eye had undergone enucleation

246246246246246 Surgical Atlas of Orbital DiseasesSurgical Atlas of Orbital DiseasesSurgical Atlas of Orbital DiseasesSurgical Atlas of Orbital DiseasesSurgical Atlas of Orbital Diseases
Keralli H et al8 reported that exenterationfollowed by chemotherapy and radiotherapy doesnot prolong the survival of patients with massiveorbital involvement of intraocular retinoblastoma.
Orbital Extension of Medulloepithelioma
Intraocular medulloepithelioma of the ciliary bodyis a rare tumor occurring during the first decade oflife. This embryonal tumor usually arises from theneuroepithelium of the ciliary body.9 Rarely, it mayarise from iris, retina and optic nerve.10-12
Though the tumor tends to locally invade thesurrounding ocular structures, it can also extend intothe orbit and rarely metastasize. It can be classifiedas teratoid or nonteratoid medulloepithelioma.Medulloepithelioma that contains heterogenoustissues like skeletal muscle, cartilage and hair areclassified as teratoid.13,14
Histologically, medulloepithelioma consists oftwo cellular components: epithelial cords and afibrillar matrix. Epithelial cells are arranged inconvoluted patterns or in a circular pattern around alumen or more commonly as elongated, interlacingcords. Both pigmented and non-pigmented cells maybe present. More malignant tumors contain somevery poorly differentiated cells which may resemble
retinoblastoma cells. Medulloepithelioma forms astroma composed of loose, delicate fibrils withabundant ground substance resembling embryonicmesenchyme or myxoid tissue.
Clinically it presents with loss of vision, pain,photophobia, ciliary body or anterior chambermass,leucocoria and as proptosis in advanced cases(Figures 18.6 to18.9). Presence of a fleshy grey, pink,yellow or brown color mass with cystic areas in theciliary body region is very characteristic. Very oftenlens coloboma may be the only presenting signoccurring due to absent zonules.The tumor maypresent either as a solid or polycystic mass or as sheetbehind the lens, resembling a cyclitic membrane.Thecysts of the tumor may be free floating cysts or maysettle in anterior chamber or vitreous.The tumor maycontain heterogenous tisues like cartilage whichpresents like chalk particles as grey-white opacities.Complications are rubeosis, glaucoma (Buph-thalmos), cataract and retinal detachment. Malignantchanges of medulloepithelioma are rare. Thesechanges are characterized by increased pleomorphicand mitotic activity with areas of poorlydifferentiated neuroblastic cells or sarcomatouschanges with invasion of surrounding ocularstructures.15 Charif CM et al. reported a case of a 4years old child with malignant medulloepitheliomainvolving the sclera with extension into the orbitalfat.16 Though tumors predominantly occur inchildren, they can rarely present in adults. J MichaelJumper had reported a case of a 45 years old manwith invasive medulloepithelioma.17
Diagnosis is usually established by slit lampexamination along with radiological investigationslike ultrasound biomicroscopy, CT scan and MRI.Julian G Feijoo had reported characteristicultrasonographic features of medulloepitheliomawhich included echogenic heterogenicity of thetumor with presence of multiple cysts with stalk-likeprolongation of the surface.18 However diagnosis isconfirmed by histopathological examination and byimmunohistochemistry.
Treatment of choice is wide local excision. Inmalignant tumors enucleation is preferred. However,with extensive extraocular spread exenteration isperformed followed by chemotherapy.Role ofradiotherapy is palliative only.
Figure 18.5: Fundus photograph illustrating regressionof retinoblastoma following SALT

Secondary and Metastatic Orbital TumorsSecondary and Metastatic Orbital TumorsSecondary and Metastatic Orbital TumorsSecondary and Metastatic Orbital TumorsSecondary and Metastatic Orbital Tumors 247247247247247
Figures 18.6 to 18.9: Ciliary body medulloepithelioma with orbital extension. 5 years old boy presenting with buphthalmos and underwenttrabeculectomy initially elsewhere. 3 months following this presented to us with proptosis and orbital mass. On biopsy it was diagnosed asmedulloepithelioma which was confirmed by immunohistochemistry. The child underwent six cycles of chemotherapy and radiotherapyfollowed by total exenteration
Figure 18.6 Figure 18.7
Figure 18.8 Figure 18.9
Orbital Extension of Uveal Melanoma
Orbital involvement of uveal melanomas occur afterextrascleral extension of massive intraocular lesions.Although extraocular spread may present with itsown set of clinical problems, ultimately it is the distantmetastases which ultimately decide the long-termprognosis of the patient.
Uveal melanomas are a diverse group ofpigmented tumors originating in the iris, ciliary body
and most commonly the choroid. They are the mostcommon primary intraocular tumors with an annualincidence that varies worldwide. Melanomas tendto be more common in those of caucasian descentand tend to have increased incidence with decreasinglatitude suggesting that increased sun exposure maybe a factor in development. They predominate in theolder age group peaking in the sixth decade.19
Predisposing factors include ocular melanosis andmelanocytoma.

248248248248248 Surgical Atlas of Orbital DiseasesSurgical Atlas of Orbital DiseasesSurgical Atlas of Orbital DiseasesSurgical Atlas of Orbital DiseasesSurgical Atlas of Orbital Diseases
The tumors can be subclassified by histologicalcell type using the modified version of the prognosticcell type introduced by Callendar. Spindle A, spindleB, epithelioid and mixed types can be seen (Figures18.10A to G) with epithelioid cells having the worst
prognosis.20 Other prognostic factors include size ofthe primary and age of the patient at presentation.21
Recently, genetic mutations have also been notedincluding monosomy 3 and duplication ofchromosome 8q confer worse prognosis.
A B
C D
E F
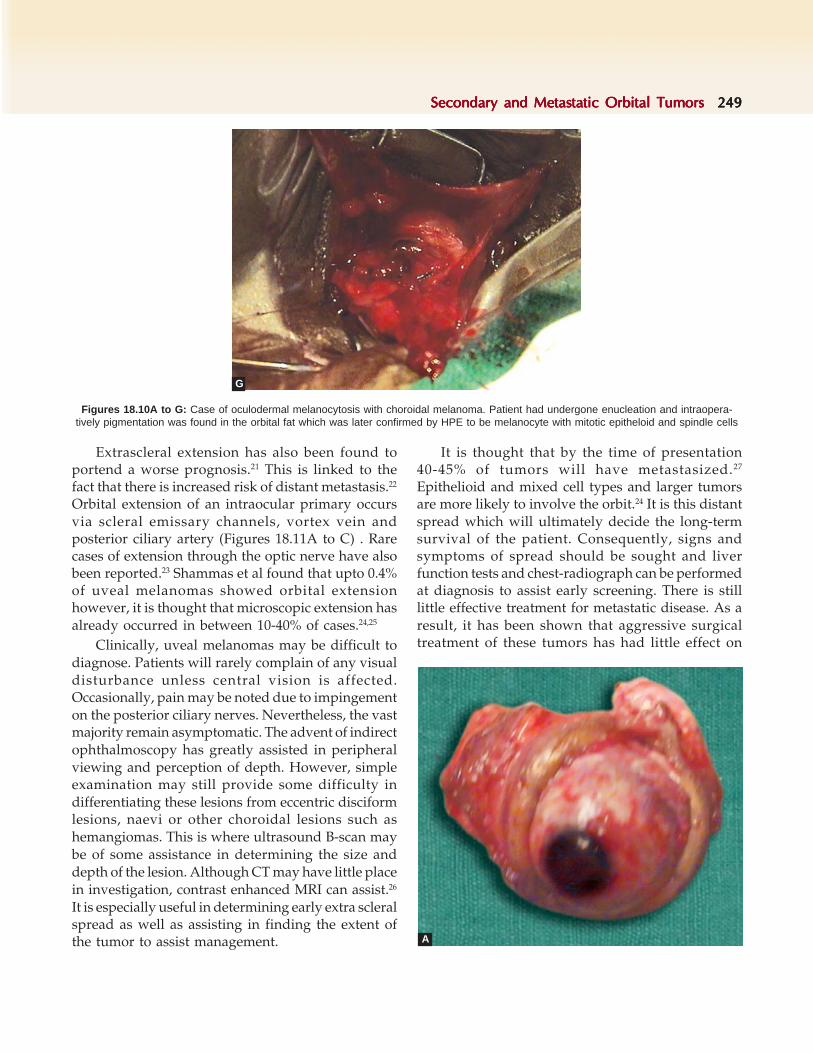
Secondary and Metastatic Orbital TumorsSecondary and Metastatic Orbital TumorsSecondary and Metastatic Orbital TumorsSecondary and Metastatic Orbital TumorsSecondary and Metastatic Orbital Tumors 249249249249249
Figures 18.10A to G: Case of oculodermal melanocytosis with choroidal melanoma. Patient had undergone enucleation and intraopera-tively pigmentation was found in the orbital fat which was later confirmed by HPE to be melanocyte with mitotic epitheloid and spindle cells
Extrascleral extension has also been found toportend a worse prognosis.21 This is linked to thefact that there is increased risk of distant metastasis.22
Orbital extension of an intraocular primary occursvia scleral emissary channels, vortex vein andposterior ciliary artery (Figures 18.11A to C) . Rarecases of extension through the optic nerve have alsobeen reported.23 Shammas et al found that upto 0.4%of uveal melanomas showed orbital extensionhowever, it is thought that microscopic extension hasalready occurred in between 10-40% of cases.24,25
Clinically, uveal melanomas may be difficult todiagnose. Patients will rarely complain of any visualdisturbance unless central vision is affected.Occasionally, pain may be noted due to impingementon the posterior ciliary nerves. Nevertheless, the vastmajority remain asymptomatic. The advent of indirectophthalmoscopy has greatly assisted in peripheralviewing and perception of depth. However, simpleexamination may still provide some difficulty indifferentiating these lesions from eccentric disciformlesions, naevi or other choroidal lesions such ashemangiomas. This is where ultrasound B-scan maybe of some assistance in determining the size anddepth of the lesion. Although CT may have little placein investigation, contrast enhanced MRI can assist.26
It is especially useful in determining early extra scleralspread as well as assisting in finding the extent ofthe tumor to assist management.
It is thought that by the time of presentation40-45% of tumors will have metastasized.27
Epithelioid and mixed cell types and larger tumorsare more likely to involve the orbit.24 It is this distantspread which will ultimately decide the long-termsurvival of the patient. Consequently, signs andsymptoms of spread should be sought and liverfunction tests and chest-radiograph can be performedat diagnosis to assist early screening. There is stilllittle effective treatment for metastatic disease. As aresult, it has been shown that aggressive surgicaltreatment of these tumors has had little effect on
G
A

250250250250250 Surgical Atlas of Orbital DiseasesSurgical Atlas of Orbital DiseasesSurgical Atlas of Orbital DiseasesSurgical Atlas of Orbital DiseasesSurgical Atlas of Orbital Diseases
survival and consequently management has tendedto be more conservative. Treatment is partly tailoredto the size and type of extrascleral extension. Plaqueradiotherapy has been shown to be effective againstflat or small nodular extensions, whereas with largernodular extension and recurrence external beamradiotherapy followed by exenteration can be used.Vortex vein involvement requires resection of thevortex vein followed by further enucleating orradiotherapy. Recently, brachytherapy has also beenproposed for as a substitute for radiotherapy. Earlyfindings suggest that the technique requires less timefor completion of treatment whilst delivering ahigher dose of radiation to the tumor.
Despite improving diagnosis and managementof melanoma, survival has improved little. Thus theaim is still to be able to diagnose these tumors priorto extrascleral extension.28
Orbital Extension of Lacrimal Sac TumorsOccurance of lacrimal sac tumor is very rare. Inmajority of patients they are epithelial in origin Theseepithelial tumors include squamous and transitionalcell papillomas, oncocytic adenomas and carcinomaslike transitional cell carcinoma, squamous cellcarcinoma, adenocarcinoma, adenoid cysticcarcinoma, mucoepidermoid carcinoma and poorlydifferentiated carcinoma.29,30 Amongst the non-epithelial tumor the most common is fibrous
histiocytoma followed by a variety of other tumorsincluding lymphoid tumor, malignant melanoma,hemangiopericytoma, neurofibroma, granulocyticsarcoma and lipoma.30 It has been found thatapproximately 55% of lacrimal sac tumors undergomalignant transformation.30 Though these tumors arelocally invasive, however at times it can invade theorbit and can also metastasize becoming lifethreatening.
The age of presentation of lacrimal sac tumorsdepend on the histologic pattern of the neoplasm.Benign tumors like papillomas are found in youngerage group. However, the malignant tumors are seenwithin 41-75 years of age.31 Ni C and co-worker hadreported that genetic and environmental factors mayplay a role in clinical presentation of lacrimal sactumor.32
The signs and symptoms are usually insidiouswith epiphora being the most common symptom andlacrimal sac mass as the most common presentingsign.
Histopathologically, lacrimal sac tumors areclassified as epithelial tumors and non-epithelialtumors. These tumors are either benign or malignant.The malignant tumors are found to arise either frompre-existing tumors or arise de novo.
The papillomas are the most common lacrimalsac tumors .According to their growth the papillomas
Figures 18.11A to C: Case of intraocular melanoma with extension to sclera and orbit. Patient had undergone exenteration and socketwas reconstructed with temporalis muscle transfer covered with split thickness skin graft
B C

Secondary and Metastatic Orbital TumorsSecondary and Metastatic Orbital TumorsSecondary and Metastatic Orbital TumorsSecondary and Metastatic Orbital TumorsSecondary and Metastatic Orbital Tumors 251251251251251
crest along the medial orbital wall, the nasolacrimalsac is usually not prominently identified onradiographic imaging (CT/MRI). Expansion oflacrimal sac fossa, destruction of bone, a massextending beyond the lacrimal sac suggest a lacrimalsac tumor. A chest X-ray, hematologic tests includingfull blood count with differential, ESR, renal andhepatic function tests, antineutrophil cytoplasmicantibody and leutic serology may be considered.Swabbing for microbiologic culture is essential in anulcerated lesion. Biopsy for histopathologicaldiagnosis is mandatory for treatment.
Traditionally, suspected lacrimal sac tumor ismanaged by dacryocystectomy with tissue biopsyand frozen section analysis (Figures 18.12A and B).This was followed by further treatment as requiredincluding radical resection, radiotherapy, orchemotherapy.
Nowadays, incisional biopsy is done in largeulcerative tumors to plan subsequent therapy.Following definitive histological examination, if noevidence of tumor is found, a DCR is performed. Ifthe only suggestion of a lacrimal sac tumor is a fillingdefect on DCG, a DCR and biopsy should beperformed. If the biopsy reveals a locally invasivetumor, nasal endoscopic monitoring is advised.Aggressive tumors are treated with radical surgeryor radiotherapy.
are subdivided as exophytic, inverted and mixed.However according to the histologic patterns,papillomas are classified as squamous cell papillomascharacterized by acanthotic, stratified squamousepithelium transitional cell papilloma with stratifiedcolumnar epithelium and mixed papilloma with amixture of squamous cell and transitional cell.Malignant transformation in the form of carcinomaslike squamous cell, transitional cell or adenocarcinoma seem to originate from the epithelial liningof the lacrimal sac. Other epithelial tumors areoncocytic adenomas and mucoepidermoid carcinoma.Oncocytic tumors are composed of special types ofepithelial cell called oncocytes due to their abundanteosinophilic cytoplasm. These tumors rarely undergometastasis. Mucoepidermoid carcinoma is a rareepithelial tumor of the lacrimal sac. These tumorsare composed of a mixture of different cells likemucus secreting cells, epidermoid cells and basal cells.Seven types of non-epithelial tumors of lacrimal sacare reported. The common amongst them are fibroushistiocytoma, lymphoma, melanoma and hemangio-opericytoma.30 In general, lacrimal sac tumorsare rarely life threatening. Distant metastasis can befatal.
A thorough history directed to pertinent clinicalfeatures is very important. A comprehensive ocularand systemic examination is necessary to assess thefirmness and location of the mass in relation to themedial canthal tendon. Careful examination to ruleout any punctal discharge and regional lymph-adenopathy and a complete nasal and sinusevaluation should be done.
Lacrimal function tests the rapidity of flow fromthe lacrimal sac. Benign tumors demonstrate outflowstenosis and carcinomas show complete obstruction.Dacryocystogram of a lacrimal sac tumor shows adiscrete mass with a filling defect or a distended sacshadow with uneven or mottled density of thecontrast media and some patency.
Computed tomography of orbit and sinuses isessential to outline the tumor and assess erosion orinvasion into nearby structures. Located within thelacrimal sac fossa, anterior to the posterior lacrimal
Figures 18.12: A case of lacrimal sac tumor which was laterdiagnosed as squamous cell carcinoma of lacrimal sac

252252252252252 Surgical Atlas of Orbital DiseasesSurgical Atlas of Orbital DiseasesSurgical Atlas of Orbital DiseasesSurgical Atlas of Orbital DiseasesSurgical Atlas of Orbital Diseases
Management varies as to the tumor origin. Forlacrimal sac neoplasms, surgery with adjuvantradiotherapy is advised. In lymphomas, chemo-therapy is the definitive treatment. For localizedepithelial and mesenchymal tumors, wide surgicalexcision is performed. Postoperative radiotherapyis recommended for malignant epithelial tumors.Further surgery and adjuvant radiotherapy isperformed for recurrent lesions.
For malignant melanomas extensive surgicalresection, radiotherapy or chemotherapy may delayrecurrence but survival remains poor.
A partially or totally irreducible lacrimal sacmucocele indicates an underlying neoplasm. This ismanaged by DCR followed by definitive therapydetermined by histology with biopsy if bone erosionis absent on CT. If radiology suggests malignancy,treatment is as outlined above.
Orbital Extension of Eyelid Tumors
Malignant eyelid tumors have the propensity ofaggressive growth and for metastasis necessitatingaggressive management.Though there are differenttypes of eyelid tumors, however epithelial tumorsare most common malignant eyelid tumors. Theseare usually slowly enlarging and destructive tumorswhich can invade the adnexal tissues and the orbit.
The clinical features of malignant eyelid tumorsare variable.Very often they present as chronicblepheritis or meibomianitis or as a lid mass.Theremay be associated loss of eyelashes or pitting ornotching of lid lamella.Presence of superficialtelengiectatic blood vessels on the surface of the massis characteristic of malignant eyelid tumors.Theimportant and common epithelial malignancies of theeyelid are basal cell carcinoma, squamous cellcarcinoma and sebaceous gland carcinoma.
Basal Cell Carcinoma (BCC)Basal cell carcinoma is the most common malignanteye lid tumor in Caucasians (80 to 90%), while itshares equal incidence with sebaceous gland andsquamous cell carcinoma in Japan and Asia (20 to40%).33,34 Its incidence is increasing worldwide.35
Incidence of BCC in caucasians is generally higher inmales than females. It occurs rarely before 20 yearsof age, but age specific incidence increases thereafterpeaking between 40 to 80 years with an average ageof onset of 48 years.
Independent risk factors for BCC include red hairand light skin color.36 Dynamic tanning and burningreaction to the skin is also a clear predisposing factor.37
Other risk factors include ionizing radiation, arsenicexposure, smoking history and patients with AIDS.38,39
Rare syndromes associated with BCC includealbinism, xeroderma pigmentosum, Gorlin'ssyndrome, milia, spina bifida and syndactyly.
The most frequent site of involvement is thelower lid (50 to 60%) and medial canthus (25 to 30%).Upper lid (15%) and lateral canthus (5%) are lessfrequently involved.39 In the early stages BCC appearsas a pearly, raised area, through which dilatedvessels are seen. They ultimately undergo ulcerationand present as destructive lesions which distort theeyelid anatomy. It has an indolent and painlesscourse. Histologically, BCC can be classified asnodulo-ulcerative (rodent ulcer), pigmented,morphea or sclerosing, superficial, keloidal andfibroepithelial variety (pinkuus tumor). It may causeloss of eyelash and mimic chronic infection of eyelidmargin. The nodular variety is the most common andit appears as a raised pearly nodule with telangectasiaand central ulceration. Histology shows nests of basalcells that originate from the basal cell layer of theepithelium with peripheral palisading. Morpheoformlesions are firm and slightly elevated with ill-definedmargins. Histology shows thin cords which radiateperipherally. Morpheoform is more aggressive thannodular tumor. BCC is a slow growing tumor and itis locally invasive. It rarely spreads to distal parts ofthe body.40 Reported incidence of metastasis is 0.0028to 0.55%.3 Choroidal invasion occurs at advancedstages with median survival of 3 years atpresentation. Orbital extension is usually found withinner canthal lesions (Figure 18.13). This is due todelayed presentation or treatment and multiplerecurrence following incomplete excision.
Surgical excision is the most common mode oftreatment, followed by curettage and cautery,cryosurgery and radiotherapy.41 Mohs micrographicsurgery as practised in many centers allow 100%freeing of excision margin. Micrographic surgeryallows 99% success rate with tumor removal bysmaller margin.42
Cryosurgery is suitable for superficial lid tumorsand gives 92% five years cure rate.43 Curettage isusually combined with cautery and usually requires

Secondary and Metastatic Orbital TumorsSecondary and Metastatic Orbital TumorsSecondary and Metastatic Orbital TumorsSecondary and Metastatic Orbital TumorsSecondary and Metastatic Orbital Tumors 253253253253253
multiple applications. A course of radiotherapy isadvocated for large tumors in older patients.
Photodynamic therapy and carbon dioxide lasershave emerged recently. Percutaneous delta amino-laevulinic acid is used with exposure to light in the620-670 nm range. The success rate of photodynamictherapy in superficial BCC is 92 to 100%.44 Othermodalities of treatment include intra-lesional andperilesional interferon α2 band 5-flurouracil.45,46
Management of basal cell carcinoma with orbitalinvasion should be very aggressive. Radical surgeryincludes wide excision under frozen section or Mohsmicrographic surgery technique. It may requireradical surgical procedures such as orbitalexenteration, bony removal and even craniotomy.
Sebaceous Carcinoma of the Eyelid
Sebaceous gland carcinoma has an incidence of 1-5%of all eyelid malignancies.2 It has a much higherprevalence amongst the Asians and especially thoseof Indian origin. It occurs with increasing frequencyin advancing age. The upper lid is most commonlyinvolved in approximately 2/3rd of cases, followedby lower lid involvement and rarely the caruncle.Sebaceous gland carcinoma of eyelids is aggressivewith a tendency for widespread metastasis. Clinicaldiagnosis at an early stage has a wide differential. Itmay masquerade as chronic blepharitis, blepharo-conjunctivitis, chalazion, keratoconjunctivitis or basalcell carcinoma.47 The blepharoconjunctivitisassociated with sebaceous gland carcinoma is due to
the characteristic intraepithelial or pagetoid spreadof the tumor which involves the basal layers of skinand mucous membrane in a radial fashion. It can alsopresent as thickening of the lid on the tarso-conjunctival border with areas of conjunctivalinjection.
Histopathologic features of sebaceous glandcarcinoma include the presence of cells of sebaceousorigin confirmed by lipid stains (oil red O) on freshtissue specimen. The tissue shows varying degreesof sebaceous differentiation and infiltration with lossof normal architecture of the gland which is replacedby pleomorphic cells with prominent vacuolatedcytoplasm with high mitotic activity. The degree ofdifferentiation starts from the periphery andprogresses towards the center. Differentiated cellsare vacuolated or foamy with slight basophiliccytoplasm. However, less differentiated tumor cellsare more deeply basophilic and are anaplastic.Minimally invasive tumors are composed of lobulesof varying sizes with minimal tumor extension.Invasive tumors are composed of diffuse cords ofcells with minimum lobule formation that extends tothe stroma. Rao and coworkers reported a histologicvariant of sebaceous gland carcinoma calledcomedocarcinoma in which the tumor lobulesundergo central areas of necrosis.48
Orbital extension of sebaceous gland carcinomahas an incidence varying from 6 to 35% and isassociated with a 70 % mortality rate. There is 70 %involvement of preauricular, cervical and sub-maxillary lymph nodes. Lymphatic spread of thetumor may occur to lung, liver, skull and brain. Theoverall 5 year mortality is approximately 15%.2
The management of sebaceous gland carcinomais surgical removal of the tumor under frozen section.Rarely, surgical extirpation enhances the long-termprognosis of the tumor (Figures 18.14A to C and18.15A to E).
Patients with widespread lid involvement ororbital extension require exenteration. These patientsrequire very close follow up with map biopsiesbecause of its multicentric presentation and pagetoidspread. Involvement of the adjacent lymphatic glandrequires radical resection. Role of radiotherapy inmanagement of sebaceous gland carcinoma is verylimited. Though the tumor is radiosensitive and
Figure 18.13: Basal cell carcinoma of eyelids with orbitalextension

254254254254254 Surgical Atlas of Orbital DiseasesSurgical Atlas of Orbital DiseasesSurgical Atlas of Orbital DiseasesSurgical Atlas of Orbital DiseasesSurgical Atlas of Orbital Diseases
Figure 18.14C: 2 months postoperative
Figure 18.14B: Lid Reconstruction with Cutler Beard surgery
Figure 18.14A: A case of sebaceous gland carcinoma
Figure 18.15A: A case of Sebaceous gland carcinoma presentingwith thickening of lower lid on the right side for 6 months
Figure 18.15B: Lid reconstruction with Hughes surgery
Figure 18.15C: 2 months postoperative

Secondary and Metastatic Orbital TumorsSecondary and Metastatic Orbital TumorsSecondary and Metastatic Orbital TumorsSecondary and Metastatic Orbital TumorsSecondary and Metastatic Orbital Tumors 255255255255255
responds to radiotherapy initially the recurrence rateis high. Thus radiotherapy is indicated in patients inwhom surgery is not possible.
Squamous Cell Carcinoma of the Eyelid
Squamous cell carcinoma is the second most commoncancer among whites.49,50 The relative incidence ofBCC to SCC varies from 13:1 to 40:1.51
Risk factors for developing squamous cellcarcinoma include increasing age,51 fair skin,49,50
history of sunlight exposure during childhood witha tendency to sunburns,52 PUV-A therapy,53,54 human
Figure 18.15D: 6 months later there was a mass in the orbit mediallyand HPE revealed a sebaceous gland carcinoma. This must haveoccurred due to incomplete removal of the primary tumor
Figure 18.15E: Secondary reconstruction was done with removal ofthe orbital mass along with excision of the medial part of the eyelidand medial canthus with reconstruction with forehead flap
papilloma virus55 exposure to ultraviolet radiation,56
immunodeficiency due to immunosuppressivesfollowing organ transplantation57 and exposure toarsenic.50 People with xeroderma pigmentosum, acondition characterized by defective DNA repairfollowing UV radiation damage to DNA andoculocutaneous albinism are also predisposed.58
Squamous cell carcinoma of the eyelid (Figure18.16) can arise de novo in relatively normal skin orfrom actinic keratosis.59,60 The mean age atpresentation is around 60 years and is found to behigher amongst the males.61 It shows a tendencytowards involving the lower lid and lid margin.50
Local spread of the tumor is more aggressive thanbasal cell carcinoma and it may also metastasize toregional lymph nodes (Figures 18.17A and B).50
The lesions present as firm hyperkeratoticpapules or plaques with erythema of the surroundingskin and induration; ulceration may be present.
The tumor may spread perineurally and this isassociated with a higher incidence of recurrence andmetastasis.50,62 Orbital involvement from squamouscell carcinoma may occur due to neglected, long-standing tumors63,64 and occurs in 2.5 to 5.9% ofcases.60,64 Presentation may be with pain or restrictionof globe movement.
Poorly differentiated carcinomas, those arisingfrom scars, tumor size > 2 cm and regional nodeinvolvement are associated with increased risk forrecurrence or death.65 Metastasis occurs in 1-21% ofeyelid SCC.66
Figure 18.16: Squamous cell carcinoma of the eyelid

256256256256256 Surgical Atlas of Orbital DiseasesSurgical Atlas of Orbital DiseasesSurgical Atlas of Orbital DiseasesSurgical Atlas of Orbital DiseasesSurgical Atlas of Orbital Diseases
Figures 18.17A and B: Extensive squamous cell carcinoma of the eyelid with extension into the conjunctiva and the orbit
Biopsy is required for confirmation of diagnosis.Usual treatment consists of the excision of the tumorwith monitoring of the margins by Moh's micro-graphy or frozen section. Local control with Moh s'surgery is 96.9% at 5 years.67
Radiotherapy may be preferred for patients whoare unable to tolerate surgery or who have inoperabletumors. The five year tumor control rate withradiotherapy was 93.3%. Irradiation was equallysuccessful in primary cases and in those recurrentfollowing surgery.68 Cryotherapy may be used fortumors of large size to reduce their vascularity andsize so that surgical excision and repair can be carriedout with better surgical and functional results. It isalso useful as a primary mode of therapy for smalltumors with a wide base or those situated at the lidmargin.69 Exenteration is required for tumorsextending to the orbit.70
Other eyelid tumors that can extend into the orbitare malignant melanoma of eyelid and Merkels celltumor.
Malignant Melanoma of Eyelid
Malignant melanoma of the eyelid is very rare. Itmay either arise denovo or from preexisting precursorlesions like lentigo maligna or Hutchinson's melanoticfreckle, dysplastic naevus and giant naevus. In thelast 10 years we had come across only 4 cases ofmelanoma of eyelid and only one case had orbitalextension (Figure 18.18). The relative risk ofmalignant melanomas is extremely low for Afro-Carrabian. Intra-orbital melanomas have the worst
survival experience.71 Based on the clinical andhistological features the cutaneous melanomas areclassified as superficial spreading, acral, nodular andlentigo melanoma. Of all the melanomas involvingthe eye and the adnexa, the melanomas involvingthe eyelid margins and conjunctiva have worseprognosis.72 Orbital extension of cutaneous or eyelidmelanomas constitute less than 1% of secondaryorbital tumors. Treatment is tailored to the size andextension of the tumor. The management ofmalignant melanoma of the eyelid is surgical removal
Figure 18.18: Eyelid melanoma with orbital extension
A B

Secondary and Metastatic Orbital TumorsSecondary and Metastatic Orbital TumorsSecondary and Metastatic Orbital TumorsSecondary and Metastatic Orbital TumorsSecondary and Metastatic Orbital Tumors 257257257257257
of the tumor under frozen section control. Rarely,surgical extirpation enhance the long-term prognosisof the tumor. Patients with widespread lidinvolvement or orbital extension requires exen-teration. Our case of malignant melanoma of theeyelid with orbital extension was managed by totalexenteration and socket reconstruction withtemporalis muscle transfer.
Orbital Extension of Intracranial Tumors
The orbit is very rarely invaded by tumors otherthan meningiomas from the intracranial cavity. As aresult this section will mainly focus on themanagement of meningiomas. Other tumors that doinvade the orbit include parasellar tumors such aspituitary tumors and craniopharyngiomas.1,2,73,74 Thesetend to involve the superior orbital fissure and opticnerve foramen resulting in compression of structuresat these sites.
Gliomas are the most common intracerebralmalignancy. However, they rarely involve the orbit.It is only the high grade and aggressive glioblastomamultiforme that may invade the orbital contentseither directly or via the foramina. Unfortunately,prognosis is poor for these tumors. External beamradiotherapy may temporarily halt growth andreduce short-term visual deterioration, but thistreatment is only palliative.3/75
Meningiomas account for approximately 18 % ofall intracranial neoplasms.4,76 Annual incidence isapproximately 2 per 10000 per year afflicting femalestwice as often as males.5,77 Meningiomas originatefrom the meningoepithelial cells of the arachnoid villi.Consequently, they tend to originate at sites wherethe arachnoid villi are present. These includeparasagittal regions, cavernous sinus and foramenmagnum. The sites of interest with regards to orbitalextension include the sphenoid wing, lamina cribrosaand tuberculum sella.6,78 There is still some debate asto the etiology of these tumors. Various theories havebeen proposed including trauma or viruses.However, as yet only ionizing radiation7,79 anddeletions of chromosome 22 have been accepted.8,80
The alterations of chromosome 22 mean that there isalso a link to neurofibromatosis type 2. It has alsobeen noted that some meningiomas expressprogesterone receptors and that there is apreponderance for meningiomas in female breast
cancer patients.9,81 Thus there may also be a hormonaldriving force towards growth.
Meningiomas have been classified into 15subtypes under the WHO classification system.10,82
94% are thought to be benign, 5% atypical and 1%malignant.11,83 As the majority are benign they mostlyexert their effects locally by compression or moredistantly through mass effect or raised intracranialpressure. Consequently, it is apparent that thestructures affected will be dependent on the site ofthe tumor.
Orbital invasion most commonly presents withearly unilateral painless visual loss. The visual loss isusually gradual, but in less than 5 % of cases may beacute.12,84 Other symptoms may include headache,nausea and diplopia. Examination may reveal opticatrophy or papilloedema (Figure 18.19A).
Meningiomas also display bone involvementshowing hyperostosis and less frequently lysis. Thiscan be visualized well with CT. MRI can be used todefine the involvement of local structures (Figure18.19B). With the increasing availability of 3dimensional reconstruction planning of therapy isnow much easier.
The aim of surgery is to completely excise thetumor (Figure 18.19C). If this is not possible thenaggressive debulking should be attempted with
Figure 18.19A: Intracranial meningioma with orbital extension

258258258258258 Surgical Atlas of Orbital DiseasesSurgical Atlas of Orbital DiseasesSurgical Atlas of Orbital DiseasesSurgical Atlas of Orbital DiseasesSurgical Atlas of Orbital Diseases
Figure 18.19B: CT scan showing a mass in the temporal fossa withextension into the orbit and shows hyperostosis of the temporalbone, sphenoidal bone and inferolateral orbital bones
Figure 18.19C: 1 week postoperative following removal of themeningioma by orbito-temporal approach
postoperative radiotherapy. A combined surgicalapproach can be performed with a neurosurgicalcraniotomy and an ophthalmic orbitotomy. Ideally,both neurosurgical and ophthalmic teams areinvolved, although increasingly excision is performedsolely by neurosurgeons. Orbitotomy sites vary withposition of extension of the meningioma into the orbit.Whilst craniotomies can be fronto-temporal,pterional, supraorbital ridge or subfrontal. For casesin which an operative approach may not be suitableexternal beam radiotherapy(EBRT) or IMRT can beapplied. Newer treatments such as chemotherapywith hydroxyurea seems to have achieved littlesuccess in tumor debulking.13/85 Whilst hormonaltherapy with anti-progesterone receptor agentsseems to have had some success with selectedtumors.14/86
Final success depends on recurrence. Therecurrence rate of meningiomas varies between 10and 20%. They may recur upto 20 years after initialexcision and yearly close follow up with CT scanningis advocated.15,87 Recurrence tends to yield largebulky tumors that affect local structures and requireextensive debulking thus resulting in an increasedmorbidity.
Orbital Extension of Conjunctival Tumors
Squamous cell carcinoma of the conjunctiva
The incidence of conjunctival squamous cell carcinomais 1-2.8 per100, 000.88 It affects the elderly with a meanage of 60 year. Over 70% of the patients are male.88,89
Sunlight exposure due to UV-B radiation90 is a riskfactor.91 HPV has also been implicated especially intypes 16 and 18.92,93 Ultraviolet induced mutations inTP53 have also been implicated. It occurs at a youngerage and is more aggressive in patients with immuno-suppression.
The lesion occurs commonly in the interpalpebralarea, with the majority being perilimbal. Thepresentation varies from a gelatinous mass or noduleto a flat patch of leukoplakia or a diffuse invasivelesion (Figure 18.20A).88,94 The commonest presentingsymptoms are red eye and ocular irritation.95
Squamous cell carcinoma mimicking sclerokeratitishas also been reported.
The tumor may involve the underlying sclera inone third of the cases with intraocular involvementin 11-13% and orbital invasion in 11-15% (Figure18.20B).87,95 Risk of orbital involvement may be higherwith mucoepidermoid variants.96 Impression

Secondary and Metastatic Orbital TumorsSecondary and Metastatic Orbital TumorsSecondary and Metastatic Orbital TumorsSecondary and Metastatic Orbital TumorsSecondary and Metastatic Orbital Tumors 259259259259259
Figure 18.20A: Conjunctival squamous cell carcinoma (SCC) with360° involvement of limbus
Figure 18.20B: Scleral necrosis and invasion by theconjunctival SCC
cytology may aid in the diagnosis by displayingkeratinized dysplastic cells, hyperkeratosis,syncytial-like groupings and prominent and largenucleoli.97 UBM can show intraocular extension ofconjunctival squamous cell carcinoma (Figure 18.20C).
Management of OSSN requires adequate excisionand careful follow up to monitor any recurrence.98
Recurrence following excision depends on histo-pathological grade of tumor and involvementof surgical margins.99,100 Cryosurgery, topical5-fluorouracil or mitomycin C treatment following
Figure 18.20C: UBM showing intraocular extension of conjunctival SCC in ciliary body region
surgical excision has been shown to decrease therecurrence rate.101,102 Topical interferon α2b has beenused in the treatment of presumed recurrent cornealand conjunctival intraepithelial neoplasia.103 Once theorbit is involved exenteration may be required.
Malignant Melanoma of the Conjunctiva
Malignant melanoma of the conjunctiva has anincidence of 0.2 to 0.8 per 1000 in whites104-106 andcomprises 2-3% of ocular tumors107,108 and is lesscommonly seen in the pigmented races.106 It has

260260260260260 Surgical Atlas of Orbital DiseasesSurgical Atlas of Orbital DiseasesSurgical Atlas of Orbital DiseasesSurgical Atlas of Orbital DiseasesSurgical Atlas of Orbital Diseases
higher probability of local relapse than favorablylocated (bulbar and limbal conjunctiva) tumors, lowerTNM grade, and excision plus adjuvant therapy.121,122
Orbital extension of malignant melanoma ofconjunctiva occurs far less frequently when comparedto intraocular melanomas in the ratio of 4:23.123
Treatment includes extensive tumor removal,cryotherapy and topical mitomyin C with amnioticmembrane allograft for diffuse conjunctival andcorneal melanoma arising from primary acquiredmelanosis (Figure 18.20B).124
As primary and adjuvant therapy, topicalmitomycin yielded an overall recurrence rate of50%.125 Survival rates were found to be worst forthose with intraorbital spread.107
Orbital Extension of Tumors of the Nasal Cavityand Paranasal Sinus
Malignant tumors of this region are a diverse groupof neoplasms. They are relatively rare and as a resultfew definitive studies have been performed intotheir management. The studies that have beenundertaken illustrate that prognosis and managementvary depending on the type and site of tumordiagnosed.
increasing preponderance with age109 and arises denovo or from a nevus. However, most commonly110
these develop from primary acquired melanosis(PAM) with atypia (Figure 18.21).111,112 The mostcommon site of origin is the limbus.104 Other sitesinclude the fornices, palpebral conjunctiva andcaruncle (Figures 18.21A and B).
Folberg R and Co-workers had reported that 50%of PAM with atypia may progress to malignantmelanoma.113-115 PAM appears as flat, patchypigmentation in the conjunctival epithelium and canremain dormant for years or show slow progressionor may wax and wane.116,117 Development ofthickening within areas of PAM may indicate invasivegrowth. However, a junctional nevus may beindistinguishable from PAM with atypia histo-logically. Junctional nevi are seen in childhood whilePAM occurs in middle-aged and elderly individuals.Biopsy of lesions that are widespread, large,thickened, dark, palpebral, unusually vascular orprogressive has been suggested.118
Conjuctival melanoma arising from pre-existingnevus119,120 may be characterized by change in color,nodularity or bleeding. The 10 year survival rate inone series was 77.7%. Unfavorable tumor location(palpebral conjunctiva, fornix, caruncle, cornealstroma, eyelid), age greater than 55 years, higherTNM category, tumor thickness more than 10 mm,high mitotic index and more epitheloid cells wereassociated with higher risk of tumor related death.Tumors with unfavorable location, higher TNMgrade, and excision alone as initial therapy had a
Figure 18.21A: Conjunctival malignant melanoma
Figure 18.21B: Postoperative total excision of conjunctival malignantmelanoma with application of cryotherapy to the conjunctival margins.5 years postoperative without any recurrence

Secondary and Metastatic Orbital TumorsSecondary and Metastatic Orbital TumorsSecondary and Metastatic Orbital TumorsSecondary and Metastatic Orbital TumorsSecondary and Metastatic Orbital Tumors 261261261261261
Growth is often large prior to symptoms fromthese tumors, partly due to the nature of the cavitiesfrom which they arise. Since only a thin bony wallseparates the nasal cavity and sinuses from importantstructures, invasion of nerves, brain and orbit arefrequent.
These tumors are more commonly found in maleswith 80% presenting between the ages of 45 and 85.There is an increased risk in people living indeveloping countries.126
Due to the non-specific nature of presentationdiagnosis is often difficult. Patients may present withnasal obstructive symptoms, rhinorrhea, epistaxisand less commonly pain. If the orbit is involved thenproptosis and ocular motility may be affecteddepending on the site of the original tumor. Visionis usually affected later unless the orbital apex isinvolved whilst conjunctival congestion may resultfrom a larger mass in the orbit. Thus when nasalsymptoms are persistent cases should be investigatedfurther. Endoscopy and more detailed radiographyhave indeed improved earlier pick up. The maxillarysinus is the most common site of primary tumororigin (55%) (Figure 18.22), followed by the nasalcavity (35%) and then the ethmoids (9%). Thesphenoidal and frontal sinuses are rarely involvedbut when they are they confer a poor prognosis.2,127
The majority of tumors are squamous cellcarcinomas (80%)127,128 with adenocarcinoma andadenoid cystic carcinoma making up the majority ofthe rest. The orbit is thus also most frequentlyinvaded by squamous cell carcinoma. Routes includethe foramina, perineural spread or direct invasionvia bony erosion. Lymphatic spread is however rare.
Squamous cell carcinomas most commonly arisefrom the turbinates. Consequently, they present morecommonly with signs of congestion and nasolacrimalduct obstruction. Up to 80 % have bony erosion ofthe orbit at the time of diagnosis.129 Nickel andchrome workers have a higher incidence of squamouscarcinomas.130 It is also increasingly thought thatsmoking is a risk factor for development of thesetumors.131 Biopsy is often important as the variousdifferent forms of squamous carcinoma conferdifferent modes of spread and hence affect prognosis.
Adenocarcinoma is more common in wood-workers and is linked to other chemicals for instancethose found in the leather tanning industry.132
The prognosis from these tumors varies withhistological grading. They commonly invade the baseof skull and the orbit affecting vital structures.However, distant metastasis is rare. Undifferentiatedcarcinomas have a very poor prognosis, usually beingpicked up at a late stage. Unlike squamous carcinomasthey are commoner in women than men. Small cellcarcinomas are similar to their lung counterparts andmay present with early proptosis, epistaxis andobstructive symptoms.
X-ray was the initial tool for diagnosis and isstill useful in determining location, size and presenceof bony erosion.129 However, it has now beensurpassed by computed tomography whichhighlights bony involvement. MRI T2 weighted helpsdifferentiate tumor from surrounding tissue andedema. Bowing of tumor-fat interface in fat saturatedimages gives a clue as to invasion. If this changesfrom smooth to irregular, invasion is far morelikely.133
Treatment of nasal and sinus tumors usually fallsbeyond the domain of ophthalmologists. Specialistsfrom the fields of head and neck surgery and maxillo-facial surgery provide the best hope for patients.Surgeons with skills in facial reconstruction may alsohelp the patients once treatment is completed. Thereis still some debate over the best modality oftreatment partly due to the lack of adequate research.However, in a recent meta-analysis, surgery aloneseemed to be better than combination with radiation.Worst of all appeared to be radiation alone.134 Oftenradiotherapy is given to help reduce the size of thetumor prior to surgery, however, as yet there is littleevidence that this improves long-term survival. Thus,surgery with wide local margins still seems to bepreferred for low stage cancers and surgery withsome adjunctive radiotherapy used for higher stagecancers. Different approaches have been used to gainaccess dependent on the size and position of thetumor. Recently, endoscopic approaches have beenused to reduce postoperative morbidity withcomplete transnasal resections, although this is stilla developing field.135 Another area of debate is therole of exenteration with orbital involvement. Studieshave shown that preservation of the eye has notaffected survival rates.136 Indeed if adequatereconstruction is performed a good functionaloutcome can be achieved in up to 90% of cases.137

262262262262262 Surgical Atlas of Orbital DiseasesSurgical Atlas of Orbital DiseasesSurgical Atlas of Orbital DiseasesSurgical Atlas of Orbital DiseasesSurgical Atlas of Orbital Diseases
Figure 18.22: Carcinoma of maxillary sinus with involvement ofparanasal sinus,nasal cavity, the orbit and surrounding adnaxaeleading to extreme lateral displacement of the right orbit
However, we recommend orbital exenteration withinvolvement of the orbital apex, extraocular muscles,bulbar conjunctiva and sclera.Radiotherapy has beenused for some time in the treatment of head andneck tumors. However, high doses of radiation arerequired for successful treatment. Since the tumorsare found close to structures that are highlyradiosensitive, morbidity is often high followingtreatment. In a review of 48 patients treated withcurative radiotherapy 33% developed unilateralblindness whilst 4 developed bilateral blindnesssecondary to optic nerve damage.138 However,irradiation can be used in rarer instances whencervical lymph node spread has occurred.
Chemotherapy is usually reserved for certaintypes of tumor. These include lymphoma, neuro-endocrine, enthesioneuroblastoma and undifferent-iated carcinomas. The trouble in the past has beenthe systemic side effects. However, increasingly alocal approach has been attempted with some success.
Prognosis from a recent review suggests anoverall survival of around 40%. Prognosis varied withsite and type of lesion. Nasal fared better thanethmoidal which in turn had better survival thanmaxillary. There was also a worse prognosis forfrontal and sphenoidal involvement due to increasedinvasion of the brain and dura. Glandular carcinomashad a better prognosis than squamous carcinomas.134
Other studies have shown that although orbitalinvolvement is not detrimental per se, and deeporbital involvement leads to a poorer survival, hencethe advice for exenteration when these tissues dobecome involved.139/140
Orbital Extension of Nasopharyngeal Tumor
Although nasopharnygeal tumors are found in closeproximity to those of the nasal cavity, they have analtogether different pattern of presentation partlybecause of the vast lymphatic network present in theregion. They are almost a distinct entity affecting agenerally younger age group, between 45-55. Thereis a higher incidence amongst males with the highestincidence amongst the southern Chinese populations.Here 15-30 males per 100,000 are diagnosed with thecondition per year. However, in other parts of theworld the disease is relatively rare. There is thoughtto be a genetic element as the risk continues to remainhigh even in second generation Chinese emigrantsdespite the change of environment factors.141/142
Epstein-Barr virus has been implicated as theenvironmental agent as carcinoma cells have beenfound to contain viral DNA.143 Changes in the makeup of these cells are thought to result in squamouscell carcinoma. Unlike nasal tumors they are far morelikely to incur systemic spread.
Patients tend most commonly to present with aneck mass secondary to regional lymphnodemetastasis. This is often linked with dysphagia. Othersymptoms include nasal symptoms such as rhinorrheaand nasal congestion, auditory problems such ashearing loss, fullness and recurrent otitis media. Ifthe orbit is involved then symptoms may includeproptosis, reduced vision, ocular motility disordersand pain. The orbit is rarely involved and is usuallyaffected later than other structures.144 Direct invasionthrough bone is rare. However, common routesinclude pterygopalatine fossa, inferior orbital fissureand then secondarily through the paranasal sinuses.Either CT or MRI can be used to help detect thepathway of tumor entry into the orbit.145
Unlike nasal and paranasal sinus tumors surgeryplays only a minor role in the management of thesetumors, because local metastatic spread is alreadylikely to have occurred. Thus radiotherapy is theprimary treatment modality for orbital invasion.Chemotherapy is used as an adjunctive treatment for

Secondary and Metastatic Orbital TumorsSecondary and Metastatic Orbital TumorsSecondary and Metastatic Orbital TumorsSecondary and Metastatic Orbital TumorsSecondary and Metastatic Orbital Tumors 263263263263263
advanced regional metastasis or more distant spread.Recent reviews of cases have shown that orbitalinvolvement confers a particularly bad prognosis. The5 years survival of a recent case series ofnasopharyngeal cancer with orbital extension wasonly 28%.146
Metastatic Orbital TumorsMetastasis to the orbit occurs secondary tohematological spread of a primary tumor. Of all theorbital cases 1.5 to 3.3 % are metastatic of which 7 %cases are bilateral. In the pediatric age group, thecommon primaries include neuroblastoma, Wilm'stumor and Ewing's sarcoma. In adults, the commonprimary sites for metastatic tumors to the orbit arefrom breast, prostate, lung, gastrointestinal tract,kidney and cutaneous melanoma. Most commonly,the patient has a known primary tumor. The mostcommon malignancies that metastasize to the orbitare carcinoma of the breast in females and carcinomaof the lung in males.147,148 Metastases to the orbit havealso been reported to occur from carcinoma ofthe tongue, pancreas, gallbladder, cervix, penis,urinary bladder, thyroid intestinal carcinoid, renalcell carcinoma and carcinosarcoma of the parotidgland.149-157
Orbital metastasis may also be the firstmanifestation of a systemic malignancy. Metastasesto fat and bone are twice as common than muscle.Usually the primary tumor is known except in aboutone quarter of patients. Certain carcinomas likemelanoma and breast carcinoma are likely to have aknown primary.
Average survival is approximately 9 months fromthe orbital presentation. The first manifestation ofsymptoms due to orbital metastasis usually occursafter a mean period of 31-64 months after diagnosisof primary disease, but tumors such as breast cancerand thyroid cancer have a longer delay (3-5 years).Melanoma is intermediate (2 years) and those fromthe lung and gastrointestinal tract are diagnosedshortly before or after orbital presentation. The meanage of the patients was 64 years in one study.147
These tumors present similarly to othersinvolving the orbit. Symptoms include lid swelling,red eye, pain, proptosis and diplopia and signsinclude incomitant strabismus with diplopia,blepharoptosis, decreased vision, proptosis and a
palpable mass.158,159 However, motility disturbanceout of proportion to the proptosis is characteristic ofan orbital metastatic tumor. Unusually, enophthalmoshas been reported with schirrous carcinomas of thebreast whilst metastases from the prostate to the orbitare usually osteoblastic in nature.160,161 Renal cellcarcinoma has a tendency to induce hemorrhage andconsequently it may initially be difficult todifferentiate from orbital hematoma.156 Diagnosis ofmetastatic origin follows simple lines. Site of theoriginal tumor may also be ascertained withsymptoms and signs suggestive of other systemsbeing involved. Investigations may include non-specific tests such as carcinoembryonic antigen (CEA)which is elevated in metastatic disease of the bowel.Other specific tests may be refined with regards tothe primary tumor suspected. Both CT and MRI havea place in management. Both hyperostotic andspiculated CT appearances have been described.147,149
MRI may assist in soft tissue differentiation and toassess spread. Ultimately, however, a fine needleaspiration biopsy may be required to confirm thediagnosis in situations where an orbitotomy is notpossible.162
The survival rate of these patients is poor andconsequently treatment is mainly palliative and isaimed at providing symptomatic relief163 withradiotherapy, hormonal therapy, chemotherapy andsurgery depending on the type and stage of thedisease.
REFERENCES
1. Zeynel A,karcioglu,Hadjistilianuo D. Orbital tumors :Diagnosis and Treatment 257.
2. Rootman J: Diseases of the orbit: A multidisciplinaryapproach (2nd ed): Lippincott Williams and Wilkins,Philadelphia, PA, 324.
3. Kapelman JE, Mc Lean IW, Rosenberg SH: multivariateanalysis of risk factors for metastasis in retinoblastomatreated by enucleation. Ophthalmology: 1987; 94: 371-7.
4. Rootman J, Lilsworth RM, Hofbaurve J, Ketcher D: orbitalextension of retinoblastoma: a clinicopathologic study. CanJ Ophthalmol, 1978;13(2): 72-80.
5. Zyguiska- Machowa H, Macujeuski Z, Sadowska M:Orbital invasion and recurrence of retinoblastoma: KlinOczna. 1991;93 (1): 19-20.
6. Chautada G, Jandino A, Corsak S, Manzitha J, RosiawskiE, Schwartzman E: treatment of overt extraocularretinoblastoma: Med Paediatr Oncol; 2003; 40(3): 158-61.

264264264264264 Surgical Atlas of Orbital DiseasesSurgical Atlas of Orbital DiseasesSurgical Atlas of Orbital DiseasesSurgical Atlas of Orbital DiseasesSurgical Atlas of Orbital Diseases
7. Namaune F, Doz F, Tangley ML, et al: high dosechemotherapy with carboplatin, etoposide andcyclophosphamide followed by a haematopoetic stem cellrescue in patients with high risk retinoblastoma. A SFOPand SFGM study. European Journal of cancer. 1997;33(14);2368-75.
8. Keralli H, Belgic S, Ozerdem U: management of massiveorbital involvement of intraocular retinoblastoma.
9. Hemsmann N, Steform F H: Medullooepithelioma of theciliary body: Acta Ophthalmol 1991: 69: 398-401.
10. Myron Y, Ben S F: Ocular pathology. (3rd ed) 1989; 50411. Llyod WC 3rd,O'Hara M: Malignant teratoid Medullo-
epithelioma: clinical-echographic- histopathologiccorrelation: JAAPOS 2001: 5: 395-7.
12. O'Keepe M, Fulcher T, Kelly P, Luv W, Dudges J:Medulloepithelioma of the Optic nerve head: Archives ofOphthalmology .1997: 115; 1325-27.
13. Shields JA, Eagle RC Jr, Shields CL, Singh AD, Robitaille J.Pigmented Medulloepithelioma of the ciliary body. ArchOphthalmol 2002; 120: 207-10.
14. Brougthon WL, Zimerman LE. A clinicopathologic studyof 56 cases of intraocular Medulloepithelioma. Am JOphthalmol 2000; 130:364-6.
15. Pradhan SB, Adhikari RC, Shrestha B, Sayami G, Dali S,Shrestha HG: Malignant teratoid Medulloepithelioma ineye. Kathmandu University Medical Journal. 2003:1:42-4.
16. Charif Chefchaouni M, El Bakkali M, Abdellah H, El AmartiA, Benchrifa F, Saidi O, Berraho A: Medulloepithelioma ofthe ciliary body- a case report. J Fr Ophthalmol. 2000;23(2):165-9.
17. J Michael Jumper, Devron H Char, Edward L Howes Jr,Daniel G Bitner: Neglected malignant Medulloepitheliomaof the eye: Orbit. 1999: 18:1 37-43.
18. Julian Garcia- Feijoo et al. Medulloepithelioma of the ciliarybody-ultrasonographic biomicroscopic findings. JUltrasound Med. 2005: 24: 247-50.
19. Collaborative ocular melanoma study group: enucleationradiation of large choroidal melanoma I: Characteristicsof patients enrolled. Am J Ophthalmol 1998;125(6): 767-78.
20. Mclean IW, Zimmerman LE, Evans RM: Reappraisal ofCallender's spindle a type of malignant melanoma ofchoroids and ciliary body Am J Ophthalmol 1978;86(4):557-64.
21. Polito E, Leccisotti A Primary and secondary melanomas:A clinical and prognostic study. Ophtal Plast Reconstr Surg1995;11: 169-81.
22. Hungerford J. Prognosis in ocular melanoma. Br J Ophthal1989; 73: 689-90.
23. Saadati H, Calvano C and Diba R. Orbital and optic chiasmalextension of uveal melanoma. Ophthal Plast Reconstr Surg2004;20(5) 387-90.
24. Shammas HF, Blodi FC. Orbital extension of choroidaland ciliary body melanomas. Arch Ophthalmol 1977; 95:2002-5.
25. Shields CL, Shields JA, Yarian DL Augsberger JJ.Intracranial extension of choroidal melanoma via th eopticnerve. Br J Ophthal 1987; 71: 172-6.
26. Recsan Z, Karlinger K, Fodor M et al. MRI for theevaluation for scleral invasion and extrascleral extensionof uveal melanomas. Clinical radiology 2002; 57: 371-6.
27. Collaborative ocaular melanoma study group. The COMSrandomized trial of iodine 125 brachytherapy for choroidalmelanoma III: Initial mortality findings: COMS no.18 ArchOphthalmol 2001;119:969-82.
28. Lin KL, Tena LB, Finger PT Orbital brachytherapy forextrascleral extension of choroidal melanoma. BR JOphthalmol. 2006;90:1438-39.
29. McNab AA, Mc Kelmme P, malignant melanoma oflacrimal sac complicating primary acquired melanosis ofthe conjunctiva.Ophthalmic Surg Lasers 1997; 28;501.
30. Stefanyszy MA, Hidayat AA, Peer JJ, Flanagan JC; Lacrimalsac tumours: Ophthal plastic reconstr surg: 1994. Sept; 10(3): 169-84.
31. Ryan SJ, Font RL: Primary epithelial neoplasms of thelacrimal sac. Am J Ophthalmol 1973: 76: 73-88.
32. Ni C, D' Amico DJ, Fan CQ, Kuo PK: Tumours of thelacrimal sac. A clinicopathologic analysis of 82 cases. IntOphthalmol clin 1982: 22: 121-40.
33. Haward J Loff; Landa N:Malignant eyelid lisions:Ophthalmic hyper guide; section: oculoplastics; 2006:1-6.
34. Takamura H; Yamashita H: Clinicopathological analysisof malignant eyelid tumor cases at Yamagata hospital:Statistical comparision of tumor incidence in Japan andother countries; Japanese journal of Ophthalmology: Vol49, No 5, 2005;349-54.
35. Lear J T, Harvy I, de Barkar D: Basal cell carcinoma: Journalof the Royal Society of Medicine, 1998;91:585-8.
36. Kricker A, Armstrong B K, English D R : Sun exposureand non melanocytic skin cancer . Cancer Causes Control1994;5(4):367-92.
37. Vitasa B C, Taylor H R, Strickland P T et al, Associationnon melanoma skin cancer and actinic keratosis withcumulative solar ultraviolate exposure in Marylandwatermen:cancer 1990:65;2811-17.
38. Wojne T H: The association between cigarette smokingand basal cell carcinoma of eyelid in woman : Ophthalplast reconstr surg.1999;15(6),390-2.
39. Shield C L, basal cell carcinoma of the eyelid : IntOphthalmol Clinic, 1993;33:124.
40. Lo J, Snow S, Reinzer G: Metastatic basal cell carcinoma:Report of 12 cases with a review of literature, J Am AcadDematol, 1991;24,715-19.
41. Motley R J, Gouldf D J, Douglas W S, Sympson N B:Treatment of basal cell carcinoma by dermatologist in theUK, Br J Dermatol, 1995;132: 437-40.
42. Mak A S, Poom A M Leung C Y et all, Audit of basal cellcarcinoma in Princess Margarat Hospital, Hong Kong :Usefulness of frozen section examination in surgicaltreatment: Scand J Plast Reconstr Surg Hand Surg1995;29:149-52.

Secondary and Metastatic Orbital TumorsSecondary and Metastatic Orbital TumorsSecondary and Metastatic Orbital TumorsSecondary and Metastatic Orbital TumorsSecondary and Metastatic Orbital Tumors 265265265265265
43. Tuppurainen K, Cryotherapy for eyelid and peri ocularbasal cell carcinomas: Outcome in 166 cases over an 8 yrperiod, Graefes Arch Clin Exp Ophthalmol 1995;233:205-8.
44. Salache S J. Status of curettage and desiccation in thetreatment of primary basal cell carcinoma.J Am AcadDermatol 1984;10:285-7.
45. Chimenti S, Peris K, Di Cristofaro S et al. Use ofrecombinant interferon alpha 2b in the treatment of basalcell carcinoma. Dermatology 1995;190:214-17.
46. Miller BH, Shavin J S, Cognetta A, et al . Non surgicaltreatment of basal cell carcinoma with intralesional 5FU/Epinephrin injectable gel: J Am Acad Dermatol 1997;36:72-7.
47. Hagedoorn A: Paget's disease of the eyelid associated withcarcinoma: Br J Ophthalmol 1937;21: 234-41.
48. Rao NA, McLean IW, Zimmerman LE: Sebaceouscarcinomam of the eyelids and caruncle: correlation ofhistopathologic features with prognosis. In Jacobiek F(ed);Ocular and adnexal tumours. Birmingham, AL, 1978; 461-76.
49. Johnson TM, Rowe DE, Nelson BR, Swanson NA.Squamous cell carcinoma of the skin (excluding lip andoral mucosa). J Am Acad Dermatol 1992;26:467-84.
50. Reifler DM, Hornblass A. Squamous cell carcinoma of theeyelid. Surv Ophthalmol 1986;30:349-65.
51. Kwitko ML, Boniuk M, Zimmerman LE. Eyelid tumourswith reference to lesions confused with squamous cellcarcinoma. I. Incidence and errors in diagnosis. ArchOphthalmol 1963;69:693-7.
52. Suchniak JM, Baer S, Goldberg LH. High rate of malignanttransformation in hyperkeratotic actinic keratoses. J AmAcad Dermatol 1997;37:392-4.
53. Stern RS, Laird N, Melski J, Parrish JA, Fitzpatrick TB,Bleich HL. Cutaneous squamous-cell carcinoma in patientstreated with PUVA. N Engl J Med 1984;310:1156-61.
54. Forman AB, Roenigk HH Jr, Caro WA, Magid ML. Long-term follow-up of skin cancer in the PUVA-48 cooperativestudy. Arch Dermatol 1989;125:515-9.
55. McGregor JM, Proby CM. The role of papillomaviruses inhuman non-melanoma skin cancer. Cancer Surv1996;26:219-36.
56. Fears TR, Scotto J. Estimating increases in skin cancermorbidity due to increases in ultraviolet radiationexposure. Cancer Invest 1983;1:119-26.
57. Jensen P, Hansen S, Møller B, et al. Skin cancer in kidneyand heart transplant recipients and different long-termimmunosuppressive therapy regimens. J Am AcadDermatol 1999;40:177-86.
58. Kraemer KH, Lee MM, Scotto J. Xerodermapigmentosum: cutaneous, ocular, and neurologicabnormalities in 830 published cases. Arch Dermatol1987;123:241-50.
59. Dinehart SM, Nelson-Adesokan P, Cockerell C, et al.Metastatic cutaneous squamous cell carcinoma derivedfrom actinic keratosis. Cancer 1997;79:920-3.
60. Marks R, Rennie G, Selwood TS, et al. Malignanttransformation of solar keratoses to squamous cellcarcinoma. Lancet 1988;1:795-6.
61. Donaldson M J, Sullivan T J, Whitehead K J, et al. Squamouscell carcinoma of the eyelids. Br J Ophthalmol 2002;86:1161-5.
62. Guidelines of care for cutaneous squamous cell carcinoma:Committee on Guidelines of Care, Task Force onCutaneous Squamous Cell Carcinoma. J Am AcadDermatol 1993;28:628-31.
63. Rathbun JE, Beard C, Quickert MH. Evaluation of 48 casesof orbital exenteration. Am J Ophthalmol 1971;72:191-1.
64. Howard GR, Nerad JA, Carter KD, et al. Clinicalcharacteristics associated with orbital invasion ofcutaneous basal cell and squamous cell tumors of theeyelid. Am J Ophthalmol. 1992;113(2):123-33.
65. Mullen JT, Feng L, Xing Y, et al. Invasive Squamous CellCarcinoma of the Skin: Defining a High-Risk Group.Annals of Surgical Oncology. 2006;13:902-9.
66. Loeffler M, Hornblass A. Characteristics and behavior ofeyelid carcinoma. Ophthalmic Surg 1990;21:513-8.
67. Abide JM, Nahai F, Bennett RG. The meaning of surgicalmargins. Plast Reconstr Surg 1984;73:492-7.
68. Fitzpatrick PJ, Thompson GA, Easterbrook WM. Basal andsquamous cell carcinoma of the eyelids and their treatmentby radiotherapy. Int J Radiat Oncol Biol Phys.1984;10(4):449-54.
69. Govind A, Lamba PA. Cryo surgery for lid tumors. IndianJ Ophthalmol 1988;36:165-7.
70. Rathbun JE, Beard C, Quickert MH. Evaluation of 48 casesof orbital exenteration. Am J Ophthalmol 1971:72:191-1.
71. Keller AZ. Histology, survivorship and related factors inthe epidemiology of eye cancers. Am JEpidemiol.1973;97(6): 386-93.
72. Keller AZ. Histology, survivorship and related factors inthe epidemiology of eye cancers. Am JEpidemiol.1973;97(6): 386-93.
73. Berezin M, Gutman I, Tadmor R et al Malignantprolactinoma. Acta Endocrinol 1992;127 :476-80.
74. Demaerel P, Mosely IF, Scaravilli F. Recurrentcraniopharyngioma invading the orbit, cavernous sinusand skull base: a case report Neuroradiology 1993;35:261-3.
75. Lawton AW, Karesh JW. Intracranial glioblastomainvading the orbit. Archives of ophthalmol 1986;104:806.
76. Rachlin JR, Rosenblum ML: Etiology and biology ofmeningiomas. Al-Mefty O(ed) Meningiomas. New York:Raven.
77. Bondy M, Ligon BL. Epidemiology and etiology ofintracranial meningioma. Journal Neurooncol 1996;29(3)197-205.
78. Chou SM, Miles JM. The pathology of meningiomas. Al-Mefty O(ed) Meningiomas. New York: Raven.
79. Pollak L, Walach N, Gur R, Schiffer J. Meningiomas afterradiotherapy for tinea capitis. Tumori 1998;84:65-8.
266266266266266 Surgical Atlas of Orbital DiseasesSurgical Atlas of Orbital DiseasesSurgical Atlas of Orbital DiseasesSurgical Atlas of Orbital DiseasesSurgical Atlas of Orbital Diseases
80. Lekanne Deprez RH, Riegman PH, van Drunen E et al.cytologenic, molecular genetic and pathological analysesin 126 meningiomas. J neuropathol Exp Neurol 1995;54:224-35.
81. Markopoulos C, Sampalis F, Givalos N Gogas H.Association of breast cancer with meningioma. Eur J SurgOncol 1998;24:332-4.
82. Louis DN, Scheithauer BW, Budkha H et al: Meningiomas,in Kleihues P, Cavenee WK (Eds): Pathology and geneticsof tumours of the Nervous sytem. Lyon :IARC Press 200176-84.
83. Kleihues P, Burger PC, Scheithauer BW. Histological typingof tumours of the central nervous system.(2nd ed) Berlin, Germany: Springerverlag, 1993.
84. Wilson WB, Gordon M, Lehman RA : Meningiomasconfined to the optic canal and foramina. Surg Neurol1979; 12: 21-8.
85. Newton HB, Slivka MA, Tevens C. Hydroxyureachemotherpay for unresectable or residual meningioma.Journal of neuro-oncology 2000; 49(2):165-70.
86. Markwalder TM, Gerber HA, Waelti et al.Hormonotherapy of meningiomas with medroxy-progesterone acetate. Immunohistochemicaldemonstration of the effect of medroxyprgesterone acetateon growth fractions of meningioma cells using themonoclonal antibody KI67. Surg Neurol 1988; 30: 97-101.
87. Jaaskelainen J: Seemingly complete removal ofhistologically benign meningioma: Late recurrence rateand factors predicting recurrence in 657 patients. Amultivariate analysis. Surg Neurol 1986;26: 461-69.
88. Lee GA, Hirst LW. Incidence of ocular surface dysplasia inmetropolitan Brisbane. Arch Ophthalmol 1992;110:525-7.
89. McKelvie PA, Daniell M, McNab S, et al. Squamous cellcarcinoma of the conjunctiva: a series of 26 cases. BJO2002;86:168-73.
90. Odrich MG, Jakobiec FA, Lancaster WD, et al. A spectrumof bilateral squamous conjunctival tumors associated withhuman papillomavirus type 16. Ophthalmology1991;98:628-35[Medline].
91. Lauer SA, Malter JS, Meier R. Human papillomavirus type-18 in conjunctival intraepithelial neoplasia. Am JOphthalmol 1990;110:23-7[Medline].
92. McDonnell JM, McDonnell PJ, Sun YY. Humanpapillomavirus DNA in tissues and ocular surface swabsof patients with conjunctival epithelial neoplasia. InvestOphthalmol Vis Sci 1992;33:184-9[Abstract/Free Full Text].
93. Saegusa M, Takano Y, Hashimura M, et al. HPV type-16in conjunctival and junctional papilloma, dysplasia, andsquamous cell carcinoma. Pathol J Clin 1995;48:1106-10[Abstract].
94. Grossniklaus HE, Green WR, Luckenbach M, et al.Conjunctival lesions in adults. Cornea 1987;6:87-116.
95. Tunc M, Char DH, Crawford B, et al. Intraepithelial andinvasive squamous cell carcinoma of the conjunctiva:analysis of 60 cases. Br J Ophthalmol 1999;83:98-103.
96. TE Johnson, KF Tabbara, RG Weatherhead, et al.Secondary squamous cell carcinoma of the orbit. ArchOphthalmol.1997; 115 (1).
97. Nolan GR, Hirst LW, Bancroft BJ. The cytomorphology ofocular surface squamous neoplasia by using impressioncytology. Cancer. 2001; 25;93(1):60-7.
98. Lee GA, Hirst LW. Retrospective study of ocular surfacesquamous neoplasia. Aust N Z J Ophthalmol.1997;25(4):269-76.
99. Tabin G, Levin S, Snibson G, et al. Late recurrences andthe necessity for long-term follow-up in corneal andconjunctival intraepithelial neoplasia. Ophthalmology.1997;104(3):485-92.
100. Lee GA, Hirst LW. Ocular surface squamous neoplasia.(Review) Surv Ophthalmol 1995;39:429-50.
101. Peksayar G, Altan-Yaycioglu R, Onal S. Excision andcryosurgery in the treatment of conjunctival malignantepithelial tumours. Eye. 2003;17(2):125-6.
102. Chen C, Louis D, Dodd T, Muecke J. Mitomycin C as anadjunct in the treatment of localised ocular surfacesquamous neoplasia. Br J Ophthalmol. 2004; 88(1):17-8.
103. Boehm MD, Huang AJ: Treatment of recurrent coarnealand conjunctival intraepithelial neoplasia with topicalinterferon alpha 2b. Ophthalmology, vol 11, issue 9, 1755-61.
104. Seregard S. Conjunctival melanoma. Surv Ophthalmol.1998;42:321-50.
105. Yu GP, Hu DN, McCormick S, et al. Conjunctivalmelanoma: is it increasing in the United States? Am JOphthalmol. 2003;135:800-6.
106. Jakobiec FA. Conjunctival melanoma. Arch Ophthalmol.1980;98:1378-84.
107. Keller AZ. Histology, survivorship and related factors inthe epidemiology of eye cancers. Am J Epidemiol 1973;97:386-93.
108. Char DH. The management of lid and conjunctivalmalignancies. Surv Ophthalmol. 1980; 24:679-89.
109. Tuomaala S, Eskelin S, Taarkanen A, et al. Population-based assessment of clinical characteristics predictingoutcome of conjunctival melanoma in whites. InvOphthalmol Vis Sci. 2002;43(11):3399-408.
110. Demirci H, Shields CL, Shields JA. Malignant melanomaarising from unusual conjunctival blue nevus. ArchOphthalmol. 2000; 118:1581-84.
111. Seregard S, Kock E Conjunctival melanoma in Sweden1969-91. Acta Ophthalmol. 1992;70:289-96.
112. Folberg R, McLean IW, Zimmerman LE. Conjunctivalmelanosis and melanoma. Ophthalmology. 1984;91:673-8.
113. Folberg R. Melanocytic lesions of the conjunctiva. In:Spencer WH. Ophthalmic Pathology: An Atlas andTextbook. (4th ed) Philadelphia, Pa: WB Saunders Co; 1996.
114. Folberg R,McLean IW,Zimmerman LE. primary acquiredmelanosis of the conjunctiva. Hum Pathol. 1985;16:129-35.

Secondary and Metastatic Orbital TumorsSecondary and Metastatic Orbital TumorsSecondary and Metastatic Orbital TumorsSecondary and Metastatic Orbital TumorsSecondary and Metastatic Orbital Tumors 267267267267267
115. Folberg R, McLean IW,Zimmerman LE Malignantmelanoma of the conjunctiva. Hum Pathol. 1985;16:136-43.
116. Shields JA, Shields CL Melanocytic tumors. In: Atlas ofconjunctival and eyelid tumors. Philadelphia: LippincottWilliams and Wilkins 1999:243-65.
117. Jakobiec FA, Folberg R, Iwamoto T Clinicopathologiccharacteristics of premalignant and malignant melanocyticlesions of the conjunctiva. Ophthalmology. 1989;96:147-66.
118. Gloor P, Alexandrakis G. Clinical characterization ofprimary acquired melanosis. Invest Ophthalmol Vis Sci.1995; 36 :1721-9.
119. Brownstein S, Henry M, Bernardo AI. Malignantmelanoma of the conjunctiva after 11 years. CanJ Ophthalmol. 1979; 14(2):142-6.
120. Shields CL, Fasiudden A, Mashayekhi A, et al. ConjunctivalNevi. Clinical Features and Natural Course in 410Consecutive Patients. Arch Ophthalmol. 2004;122:167-75.
121. Werschnik C, Lommatzsch P K. Long-term Follow-up ofPatients With Conjunctival Melanoma. American Journalof Clinical Oncology. 2002;25(3):248-55.
122. Paridaens ADA, McCartney ACE, Minassain DC et al.Orbital exenteration in 95 cases of primary conjunctivalmelanoma. Br J Ophthalmol. 1994;78(7):520-8.
123. Henderson JW Orbiyal tumors, (3rd ed). New york: RavenPress.1994.
124. Shields CL, Shields JA, Armstrong T. Management ofconjunctival and corneal melanoma with surgical excision,amniotic membrane allograft, and topical chemotherapy.Am J Ophthalmol. 2001;132(4):576-8.
125. Madhavi Kurli, Paul T. Finger. Topical mitomycinchemotherapy for conjunctival malignant melanoma andprimary acquired melanosis with atypia: 12 years'experience. Graefe's Arch Clin Exp Ophthalmol. 2005;243(11): 1108-14.
126. Carrau RL, Myers EN: Neoplasms of the nose andparanasal sinuses. In: Bailey BJ et al(Eds.) Head and necksurgery-otolaryngology (3rd ed), Lippincott, williams andWilkins 2001.
127. Cody DT, Lawrence WD: Neoplasms of the nasal cavity.In: Cummings CW et al. (Eds) Otolarygngology- Headand neck surgery. Mosby 1999.
128. Barnes L, Eveson J, Reichart P, et al. World HealthOrganisation classification of tumours: pathology andgenetics - head and neck tumours. IARC press 2005.
129. Weber AL, Stanton AC. Malignant tumors of the paranasalsinuses: radiologic, clinical and histopathologic evaluationof 200 cases. Head neck surg 1984;6:761-76.
130. Pedersen E, Hogetveit AC, Andersen A. Cancer of therespiratory organs among workers at a nickel refinery inNorway. Int J Cancer 1973;12:32-41.
131. Benninger MS. The impact of cigarette smoking andenvironmental tobacco smoke on nasal and sinus disease:a review of the literature. Am J Rhinol 1999;13: 435-8.
132. Acheson ED. Adenocarcinoma of the nasal cavity andsinuses in England and Wales. Br J Ind Med 1972; 29:21-30.
133. Sievers KW, Greess H, Baum U et al. Paranasal sinus andnasopharynx CT and MRI. Eur J Radiol 2000;33:185-202.
134. Dulguerov P, Jacobsen MS, Allal AS et al. Nasal andparanasal sinus carcinoma: are we making progress? Aseries of 220 patients and a systematic review. Cancer2001;92:3012-9.
135. Banhiran W, Casiano RR. Endoscopic sinus surgery forbenign and malignant nasal and sinus neoplasm. CurrOpin Otolaryngol Head Neck Surg 2005; 13:50-4.
136. Scott MW, Levine PA, Cantrell RW. Preservation of theeye in the treatment of sinonasal malignant neoplasmswith orbital involvement: A confirmation of the originaltreastise.
137. Imola MJ, Schramm VL: Orbital preservation in thesurgical management of sinonasal malignancy.Laryngoscope 2002;112:1357-65.
138. Parsons JT, Mendenhall WM, Mancuso AA et al. Malignanttumours of the nasal cavity and ethmoid and sphenoidsinuses. Int J Radiat Oncol Biol Phys 1988;14:11-22.
139. Suarez C, Liorente JL, Fernandez De Leon R et al.Prognostic factors in sinonasal tumors involving theanterior skull base. Head Neck 2004;26:136-44.
140. Iannetti G, Valentini V, Rinna C et al. Ethmoido-orbitaltumours: our experience. J Cran fac surg 2005;16:1085-91.
141. Chew CT. Nasopharynx (the postnasal space). In KerrAG, Mackay IS, Bull TR (Ed) Scott-Brown's otolaryngology.(5th ed) 1987. Butterworths.
142. Vokes EE, Liebowitz DN, Weichselbaum RR:Nasopharyngeal carcinoma. Lancet 1997;350: 1087-91.
143. Tsai ST, Jin YT, Mann RB, et al: Epstein-Barr virus detectionin nasopharyngeal tissues of patients with suspectednasopharyngeal carcinoma. Cancer 1998;82:1449-53.
144. Hsu MM, Tu SM. Nasopharyngeal carcinoma in Taiwan,clinical manifestation and results of therapy. Cancer1983;52:362-8.
145. Luo CB, Teng MMH, Chen SS et al. Orbital invasion innasopharyngeal carcinoma: evaluation with computedtomography and magnetic resonance imaging. Chin medJ 1998;61:382-8.
146. Hsu WM, Wang AG. Nasopharyngeal carcinoma withorbital invasion. Eye 2004;18:833-8.
147. Goldberg RA. Rootman J, Cline RA. Tumors metastatic tothe orbit: A changing picture. Surv Ophthalmol. 1990;35:1-24.
148. Ferry A, Font RL. Carcinoma metastatic to the eye andorbit:I. A clinicopathologic study of 227 cases. ArchOphthalmol. 1974;92:276-86.
149. Gonzales CM, Kuzel T, Carter MA Metastaticadenocarcinoma of the prostate to the orbit J Urol 1997;157: 625-7.
150. Maheswari GK, Baboo HA, Gopal U, Wadhwa MKCarcinoma of the tongue presenting as orbital metastasis.Turkish Journal of Cancer. 2002. 32(4,F).
151. Geetha N, Chandralekha B, Kumar A, et al.Carcinoma ofthe pancreas presenting as an orbital tumour: a casereport. American Journal of clinical Oncology. Cancerclinical trials. 21(5):532-3.

268268268268268 Surgical Atlas of Orbital DiseasesSurgical Atlas of Orbital DiseasesSurgical Atlas of Orbital DiseasesSurgical Atlas of Orbital DiseasesSurgical Atlas of Orbital Diseases
152. Misra A, Misra S, Chaturvedi A, Srivastava PK. Case report.Orbital metastasis from gall bladder carcinoma. Br J radiol.2002;75(889);72-3.
153. Lee HM, Choo CT, Poh WT.Ornital metastasis fromcarcinoma of cervix. Br J Ophthalmol. 1997;81:329.
154. Filho APS, Odashiro AN, Pereira PR, Buloushi A, CodereF, Burnier MN. Orbital metastasis of urinary bladdercarcinoma: A Clinicopathological Report and Review ofthe Literature. Orbit. 2005;24(4):269-71.
155. Borota OC, Kloster R, Lindal S. Carcinoid tumourmetastatic to the orbit with infiltration to the extraocularorbital muscle. APMIS.2005;113:135-9.
156. Hart RH, Luthert PJ, Rose GE. Renal cell carcinomamasquerading as recurrent orbital hematoma. Orbit. 2005;24(4):281-4.
157. Orbital Metastasis and Intraocular Invasion of MalignantMixed tumour (Carcinosarcoma) of the Parotid Gand in aChild. Arch Ophthalmol. 2004;122(1):114-8.
158. Shields CL, Shields JA, Peggs M. Tumours metastatic tothe orbit. Ophthal Plast Reconstr Surg. 1988;4(2):73-80.
159. Holland D, Maune S, Kovacs G, Behrendt S. Metastatictumours of orbit: A retrospective study. Orbit.2003;22(1):15-24.
160. Chang BYP, Cunniffe G, Hutchinson C. Enophthalmosassociated with primary breast carcinoma. Orbit.2002;21(4):307-10.
161. Shields CL, Shields JA, Brotman HK, Carvalho C, Eagle RDJr. Cancer metastatic to the orbi:the 2000 Robert M Curtislecture. Ophthal Plast Reconstr Surg. 2001;17:346-54.
162. Dresner SC, Kennerdell JS, Dekker A. Fine needleaspiration biopsy of metastatic orbital tumours. SurvOphthalmol. 1983;27(6).
163. Tijl J, Koornneef L, Eijpe A et al. Metastatic tumours to theorbit-management and prognosis. Grefe's Arch Clin ExpOphthalmol.1992; 230(6):527-30.


270270270270270 Surgical Atlas of Orbital DiseasesSurgical Atlas of Orbital DiseasesSurgical Atlas of Orbital DiseasesSurgical Atlas of Orbital DiseasesSurgical Atlas of Orbital Diseases

Decision MakingDecision MakingDecision MakingDecision MakingDecision Making 271271271271271
Subrahmanyam Mallajosyula
Decision MakingDecision MakingDecision MakingDecision MakingDecision Making
The etiology of proptosis is multifactorial. As weknow it can be congenital, or acquired due to variouscauses like infections both nonspecific and specificbacterial like tuberculosis,1-4 sarcoidosis,5-7 fungalinfections, inflammations, parasitic infestations,vascular malformations, primary orbital tumorsarising from various tissues like nerves and theirsheaths, vascular tissues, mesenchymal, lympho-proliferative, bony lesions apart from secondaryinvolvement from the globe, paranasal sinuses andthe brain. Metastatic lesions from breast,8 thyroid,prostate, GIT and other primary lesionselsewhere9-12 were documented in the literature.Involvement of Orbit in generalized lym-phoproliferative lesions like systemic lymphomas,leukemia is very well known. It is really surprisingto know the wide variety of pathology that caninvolve such a small structure as orbit. It is not anexaggeration that in the orbit one can come acrossalmost all the types of pathology that can involvehuman body.
With such a wide spectrum of pathological lesionscausing proptosis, it is natural that the managementstrategies also vary. The options include observationand reassurance, medical management, surgery,radiotherapy and chemotherapy. The surgicalprocedures include biopsy, debulking, excision oftumor/mass/cyst through various surgicalapproaches, multi-speciality approaches along withENT/Neurosurgeon, and exenteration.The decisiondepends upon accurate diagnosis of the nature ofthe lesion (infective/cystic/tumor: benign/malignant/Secondary/metastatic) and its locationand extent (intraconal/peripheral space/extension
to paranasal sinuses/intracranial extension).A detailed clinical evaluation, and imaging with CTscan/MRI of Orbit usually give us enoughinformation to plan proper management strategy.Other investigations like serology, FNAC13,14, Squashand IHC (Immuno-Histochemistry) are useful aidsin establishing the diagnosis and planning themanagement. In this chapter I am outlining thedifferent management strategies and which to choosefrom. The details of the management procedures aredescribed in the following chapters.
Medical management is indicated when proptosisis due to orbital cellulitis, orbital myocysticercosis,idiopathic orbital inflammation, most cases of thyroidassociated orbitopathy (the drug-trial for TAO is wellknown), Wegener's granulomatosis, tuberculosis ofthe orbit, fungal granulomas, in other words in allthe inflammatory and infective conditions. However,drain an orbital or sub-periosteal abscess, along withsystemic antibiotics. The role of medical managementis discussed in a separate chapter.
Chemotherapy and radiotherapy have a greatrole in the management of rhabdomyosarcoma,lymphoma and other lymphoproliferative diseases,retinoblastoma. They can also be used occasionallyin thyroid orbitopathy, idiopathic orbital inflam-mation. They are helpful in the treatment of othermalignancies like adenoid cystic carcinoma oflacrimal gland, secondary and metastatic lesions.These were discussed in a separate chapter.
For me, it is always very important to get at anaccurate diagnosis as early as possible, so that I amnot missing any serious condition. That is why, evenin a case of clinically suspected orbital cellulitis, I get
19C H A P T E R

272272272272272 Surgical Atlas of Orbital DiseasesSurgical Atlas of Orbital DiseasesSurgical Atlas of Orbital DiseasesSurgical Atlas of Orbital DiseasesSurgical Atlas of Orbital Diseases
Figures 19.1A and B: FNAC showing malignant cells in whorl pattern,suggestive of neuroblastoma. The details are better seen in highermagnification. This patient presented with painful proptosis andrestricted ocular motility. CT scan revealed a mass lesion with bonyerosion. Diagnosis of metastatic neuroblastoma was made from FNAC
Figures 19.2A and B: FNAC showing cells with large, peripheralnucleus and vacuolated cytoplasm arranged in clusters, frommetastatic ductal carcinoma of breast leading to proptosis
Figures 19.3A to C: Typical Salmon's patch of lymphoma arising from the upper fornix (A) and lower fornix (B).Biopsy is indicated for histopathological confirmation (C)
a CT scan as early as possible to make sure that I amnot missing other conditions like rhabdomyosarcoma,retinoblastoma which can occasionally present asorbital cellulitis. The CT scan also informs me if thereis an abscess which I have to drain, or it is only orbitalcellulitis which I can manage medically.
When the diagnosis is not definite, I prefer to doa biopsy and get a histopathological diagnosis. Thetissue diagnosis can be by way of FNAC (Figures19.1A and B and 19.2A and B), biopsy or intra-operative Squash smear examination. However Ipersonally don't perform FNAC on a lacrimal glandtumor. Instead I wish to excise the tumor in toto andplan further treatment depending on thehistopathological diagnosis.
Biopsy is indicated for histopathologicalconfirmation of clinical diagnosis (Figures 19.3A toC) as in lymphoma, meningioma of optic nervesheath, rhabdomyosarcoma, so that the patient canbe referred to an oncologist. Biopsy is also indicatedwhen the clinical diagnosis is not definite (Figures19.4A to E).
When I am planning excision of the tumor, theapproach depends on its location. If it is involvingsurrounding structures like PNS, or brain, it will bea multispeciality approach. However, FESS(Functional endoscopic sinus surgery) is the best wayto manage fronto-ethmoid mucocele. If the tumor isconfined to the orbit, it will be dealt with by mealone, the only exception being a small apical lesion,for which I prefer a transcranial approach.
The orbital approaches to proptosis are lateralorbitotomy approaches and anterior orbitotomyapproaches. The anterior orbitotomy approaches arefurther divided into cutaneous approaches andconjunctival approaches. When choosing a procedureI consider the surgical exposure and also the cosmeticresult. Though I wish to hide the scar and give thebest cosmetic result, adequate surgical exposure ofthe lesion is of paramount importance, which can notbe over-emphasized. I advise the beginners and theoccasional orbital surgeons to choose simplerprocedures first, and as they gain experience, theycan perform other complicated procedures. I wish
BA
A B
A B C

Decision MakingDecision MakingDecision MakingDecision MakingDecision Making 273273273273273
Figures 19.4A and B: This patent presented with painful proptosisof 1 month duration.He had exposure Keratitis and his vision was 20/400. Note the severe swelling, tarsorrhaphy for exposure keratitis,and chemosed conjunctiva. The CT scan shows a heterogenouslesion surrounding the optic nerve. Radiologist reported it asmeningioma. The past history was significant that he had discontinuedtreatment for tuberculosis.Since this type of acute/subacutepresentation is unusual for meningioma, I thought of infective pathology( tuberculosis) and wanted to confirm the diagnosis by a biopsy
Figures 19.4C to E: When lateral orbitotomy was performed (C) a pinkish mass was found around the optic nerve, which was biopsied. Thehistopathology showed it to be non-Hodgkins B-cell lymphoma (D) He was referred to an oncologist and he responded very well to radio-therapy (E)
Figures 19.5A and B: Lateral Orbitotomy incisions in frontal (A) andlateral (B) views. Stallard-Wright (yellow), Reese- Berke (White) andsuperior lid crease incision (pink)'
to emphasize that usually there are more than oneoption, and the procedure chosen varies from onesurgeon to other, depending upon the individual'spreference.
Intraconal Lesion: Lateral orbitotomy isindicated for intraconal lesions and lacrimal glandlesions. There are different approaches; the mostcommonly performed are Stallard-Wright'sprocedure, Reese-Berke's procedure and superior lid-crease incision (Figures 19.5A and B). Each has itsown merits. I will outline these approaches, before Idiscuss my preferences.
Stallard-Wright's incision starts at the lateral thirdto half, beneath the eyebrow, up to the lateral endof the brow, and then descends vertically along thelateral border of the orbit, and extends horizontallyalong the crow's feet .Thus it has two horizontalincisions, one at the level of sub-brow, and the other
at crow's feet, which are well hidden. But the verticalcomponent of the incision leaves a visible scar. Theadvantages of the incision include a very large andadequate area of surgical exposure to deal with hugetumors. The other advantage is that the lateralcanthus is not disturbed.
Reese-Berke’s incision (Figures 19.6A to 19.9B)is a horizontal incision that starts from the lateralcanthus and extends 4-5 cm horizontally along thecrow's feet. This incision gives a very good exposureto deal with most of the tumors. The scar is verywell hidden in the crow's feet and surgical scar isnever an issue. The only disadvantage is that thelateral canthus is disturbed and needs to bereconstructed at the end of the surgery. For those ofyou who are routinely doing oculoplastic procedures,this is neither difficult, nor time consuming. In thosesituations where the patient had a long standing andprominent proptosis, you may even do lateral tarsalstrip at the time of reconstruction of the lateralcanthus and correct horizontal laxicity of the lid.
Superior lid crease incision (Figures 19.10A to19.11C) is another excellent approach, where in theincision is along the lid crease, and then extends alongthe crow's feet. The entire incision is very wellhidden, so that the scar is not visible. It also gives avery adequate exposure. The lateral canthus is notdisturbed. However, damage to Levator PalpebraeSuperioris leading to ptosis is a known complication.
A B
C D E
A B

274274274274274 Surgical Atlas of Orbital DiseasesSurgical Atlas of Orbital DiseasesSurgical Atlas of Orbital DiseasesSurgical Atlas of Orbital DiseasesSurgical Atlas of Orbital Diseases
Steps of Reese-Berke Approach
Figures 19.7A and B: Zygoma was exposed (A), cuts were made above and below and the zygoma wasbeing removed with a rounger (B)
Figures 19.6A and B: Steps of lateral orbitotomy Reese-Berke's incision. Traction suture was applied tolateral rectus (A). Horizontal incision made from the lateral canthus (B)
Figures 19.8A and B: Periosteum was incised, and reflected (A). Lateral Rectus was identified. Tractionsuture applied earlier helps in its identification. Lateral rectus was retracted away from the tumor (B)
A B
A B
A B

Decision MakingDecision MakingDecision MakingDecision MakingDecision Making 275275275275275
Figures 19.9A and B: The tumor was removed with the help of cryo (A). After securing hemostasis, the Zygoma was replaced in its placeand secured. Drain is placed in a separate stab incision and not in the original incision. This gives a better scar. The wound is closed in layers
Steps of Superior Lidcrease Incision
Figures 19.11A to C: The lateral wall is exposed (A), which has been removed. Periosteum was incised.The tumor was exposed (B), dissected, and removed with the help of a cryo (C)
A B C
Figures 19.10A to C: The incision is along the lid crease and extends horizontally along the crow's foot (A and B).Carefully dissect up to the septum, and approach the lateral wall (C)
A CB
A B

276276276276276 Surgical Atlas of Orbital DiseasesSurgical Atlas of Orbital DiseasesSurgical Atlas of Orbital DiseasesSurgical Atlas of Orbital DiseasesSurgical Atlas of Orbital Diseases
Figures 19.13A to C: Another patient with a prominent proptosis of right eye due to a large neurofibroma, excised through Reese-Berke'sincision. Note that the incisional scar is very well hidden in the crow's feet
I believe that a scar on the face is a cosmeticblemish. I wish to perform the orbitotomy leavingas minimal scar as possible. The scar induced by thevertical component of Stallard-Wright's incision isof concern, and I wish to avoid it. Hence it was morethan 2 decades since I performed Stallard-Wrightsincision. My routine is Reese-Berke's approach.It gives adequate exposure to deal with most of thetumors (Figures 19.12A to 19.13C). If the tumor istoo big, then I perform superior lid creaseincision. The scar induced in these two proceduresis very well hidden and patient's satisfaction is veryhigh.
However it is very important to remember thatintraconal tumor can be excised by lateral orbitotomy
approach, only if it is lateral to optic nerve. If thetumor is medial to optic nerve, it cannot be excisedthrough lateral orbitotomy as the optic nerve canget damaged. In these situations, antero-lateralorbitotomy is preferred (Figures 19.14A to 19.21B).Hence the importance of assessing the relationshipof the tumor with optic nerve in coronal sections ofCT scan cannot be over-emphasized.
In antero-lateral orbitotomy, lateral orbitotomyis performed to get space and better surgicalexposure. 180° peritomy is performed, the medialrectus is disinserted, the globe is retracted laterallyand the tumor is removed between the globe andthe retracted medial rectus. Then the medial rectusis reattached.
Figures 19.12A to D: Note the gross proptosis of right eye in this female, due to a very large cavernous hemangioma occupyingmost of the orbit, as shown in the CT scan imaging. Such a large tumor could be excised through Reese-Berke's incision excised tumor (C) andpostoperative recovery (D)
A B
C D
A B C
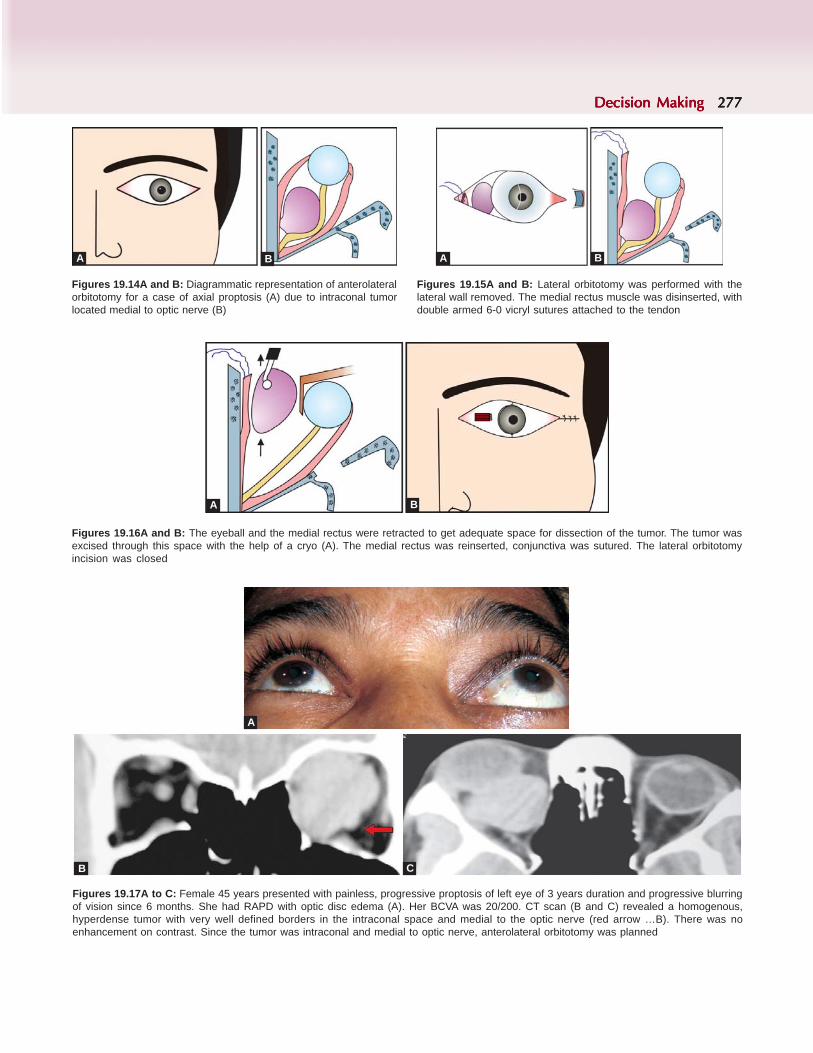
Decision MakingDecision MakingDecision MakingDecision MakingDecision Making 277277277277277
Figures 19.14A and B: Diagrammatic representation of anterolateralorbitotomy for a case of axial proptosis (A) due to intraconal tumorlocated medial to optic nerve (B)
Figures 19.15A and B: Lateral orbitotomy was performed with thelateral wall removed. The medial rectus muscle was disinserted, withdouble armed 6-0 vicryl sutures attached to the tendon
Figures 19.16A and B: The eyeball and the medial rectus were retracted to get adequate space for dissection of the tumor. The tumor wasexcised through this space with the help of a cryo (A). The medial rectus was reinserted, conjunctiva was sutured. The lateral orbitotomyincision was closed
Figures 19.17A to C: Female 45 years presented with painless, progressive proptosis of left eye of 3 years duration and progressive blurringof vision since 6 months. She had RAPD with optic disc edema (A). Her BCVA was 20/200. CT scan (B and C) revealed a homogenous,hyperdense tumor with very well defined borders in the intraconal space and medial to the optic nerve (red arrow …B). There was noenhancement on contrast. Since the tumor was intraconal and medial to optic nerve, anterolateral orbitotomy was planned
A B A B
A B
A
B C

278278278278278 Surgical Atlas of Orbital DiseasesSurgical Atlas of Orbital DiseasesSurgical Atlas of Orbital DiseasesSurgical Atlas of Orbital DiseasesSurgical Atlas of Orbital Diseases
Figures 19.18A to C: Lateral orbitotomy was performed with Reese-Berke's incision. The Zygoma was removed, and periorbita incised tofacilitate moving the globe laterally (A). 180° peritomy was performed medially from12 to 6 o'clock position. Medial Rectus muscle was identified(B), and disinserted after applying 6-O vicryl sutures (C)
Figures 19.19A and B: The globe is retracted laterally, and the disinserted medial rectus medially to getadequate surgical space (S…A). By careful dissection in this space, the tumor was identified (T…B)
Figures 19.20A and B: The tumor was dissected carefully from the surrounding structures andwas removed carefully with the help of a cryo (A and B)
CA B
A A
A B

Decision MakingDecision MakingDecision MakingDecision MakingDecision Making 279279279279279
Apical conal lesions are better approached throughtranscranial approach with the help of a neurosurgeon.This was discussed in the concerned chapter.
Imaging studies tell us if we are dealing withoptic nerve glioma or meningioma of optic nervesheath. I prefer to follow closely a case of optic nerveglioma with imaging every 6 months and performsurgery only if the eye has become blind or the tumoris nearing the orbital apex. For meningioma, I dolateral orbitotomy and take a biopsy for histo-pathological confirmation (which is mandatory here)before referring for radiotherapy.
Lesions of Superior Peripheral Space: Anteriororbitotomy approaches are normally used for theselesions, the exception being lateral orbitotomy forlacrimal gland tumors. However I am excisinglacrimal gland tumors, up to moderate size throughanterior orbitotomy approaches.
For tumors of the superior peripheral andsubperiosteal spaces, both subciliary and superiorlidcrease incisions give very good surgical exposure(Figures 19.22A and B). However the surgical scar isbetter camouflaged in the lid crease and hence is mypreferred procedure (Figures 19.23A to 19.31C).
Figures 19.21A and B: The medial rectus muscle was anchored to its original incision (A). The conjunctiva wassutured into its place (B). The lateral orbitotomy wound was closed as usual
A B
Figures 19.22A and B: Superior Anterior orbitotomy incisions, subciliary (white) andLid-crease (yellow) incisions
A B

280280280280280 Surgical Atlas of Orbital DiseasesSurgical Atlas of Orbital DiseasesSurgical Atlas of Orbital DiseasesSurgical Atlas of Orbital DiseasesSurgical Atlas of Orbital Diseases
Figures 19.23A to C: Female 38 years, presented with proptosis of left eye of 2 years duration. Note that the globe is pushed down and in,with fullness of superior sulcus (A). CT scan of the orbit revealed lacrimal gland tumor pushing the globe down and in (B) Excavation of thelateral wall of orbit could be seen (C)
Figures 19.25A and B: The lacrimal gland mass was removed with the help of cryo (A). Theexcised tumor is shown in B
A
Figures 19.24A and B: Lid-crease incision was made (A), the septum was identified andreflected from the orbital rim (B)
A B
A B
B C

Decision MakingDecision MakingDecision MakingDecision MakingDecision Making 281281281281281
Figures 19.26A and B: Female 18 years, presented with progressive, painless proptosis of right eye since 8 years. Note the severeproptosis of right eye with the eyeball pushed down and out. Note also the bluish mass lesion in the right upper lid (A and B)
A B
Figures 19.27A and B: CT scan of the orbit shows multilobulated lesion, occupying most of the intraconalspace, pushing the optic nerve infero-laterally, and extending from the apex to the upper eyelid
Figures 19.28A and B: Superior lid-crease incision was chosen, since if needed, it could be converted to lateralorbitotomy also. Note the tumor (T) on either side of the superior oblique (S.O) tendon. The tendon of superioroblique was outlined yellow to facilitate recognition
A B
A B

282282282282282 Surgical Atlas of Orbital DiseasesSurgical Atlas of Orbital DiseasesSurgical Atlas of Orbital DiseasesSurgical Atlas of Orbital DiseasesSurgical Atlas of Orbital Diseases
Figure 19.30: The excised tumor (Cavernous hemangioma)
Figures 19.29A and B: The tumor was excised carefully, withoutdamaging the superior oblique, with the help of cryo (A). Note that thesuperior oblique tendon is intact (B), and also the cavity formed afterthe excision of the tumor
A
Subcaruncular incision is popular for thyroiddecompression of medial wall, since it gives accessto ethmoid sinus. The scar is never an issue withtransconjunctival approaches.
Figures 19.31A to C: A patient with cavernous hemangioma located in the anterior part of superior peripheral space being excised in totothrough superior lid crease incision. The incision in this situation can be smaller (A) The tumor is seen in B. Look how well the incision iscamouflaged in the lid crease (C) in the figure taken immediately after completion of surgery. The surgery was performed under localanesthesia
Figures 19.32A and B: Lynch Incision (white line) and transconjunctival approaches(subcaruncular incision blue line and subconjunctival peritomy incision redline)
A B C
For lesions of medial peripheral space,the approaches can be percutaneous Lynchincision or transconjunctival incisions (Figures 19.32Aand B).
A
B
B

Decision MakingDecision MakingDecision MakingDecision MakingDecision Making 283283283283283
Lesions of inferior peripheral space, can beapproached either through the skin or conjunctiva(Figures 19.35A and B).
Subciliary is more popular of the skin approaches.It still leaves a scar, which is mostly cosmetically
However, the beginner finds it a little difficultwith these approaches. Lynch incision is simpler, anda better procedure for the beginner.If the lesion is
large, Lynch incision is my choice (Figures 19.33A to19.34B).
Figures 19.33A and B: Eccentric proptosis of right eye (A) progressing for the past 3 years. He has RAPD and optic disc edema. CT scan,revealed a huge osteoma of ethmoid (B) Since the tumor is very large, the only practical approach is transcutaneous, modified Lynch incision
acceptable. However, trans-conjunctival approachesare without a visible scar (Figures 19.36A to 19.38B).Swinging lower eyelid approach causes a scar whichis hidden in the crow's feet.
Figures 19.34A and B: The osteoma being removed through a modified Lynch incision (A) The excised osteoma is seen in (B)
A B
Figures 19.35A and B: The approaches for inferior peripheral space can be cutaneous like Subciliary incision (yellow line), or conjunctivalapproach. The swinging lower lid approach (Pink line) is a combine of both skin and conjunctival approaches and gives adequate room forsurgery
A B
BA
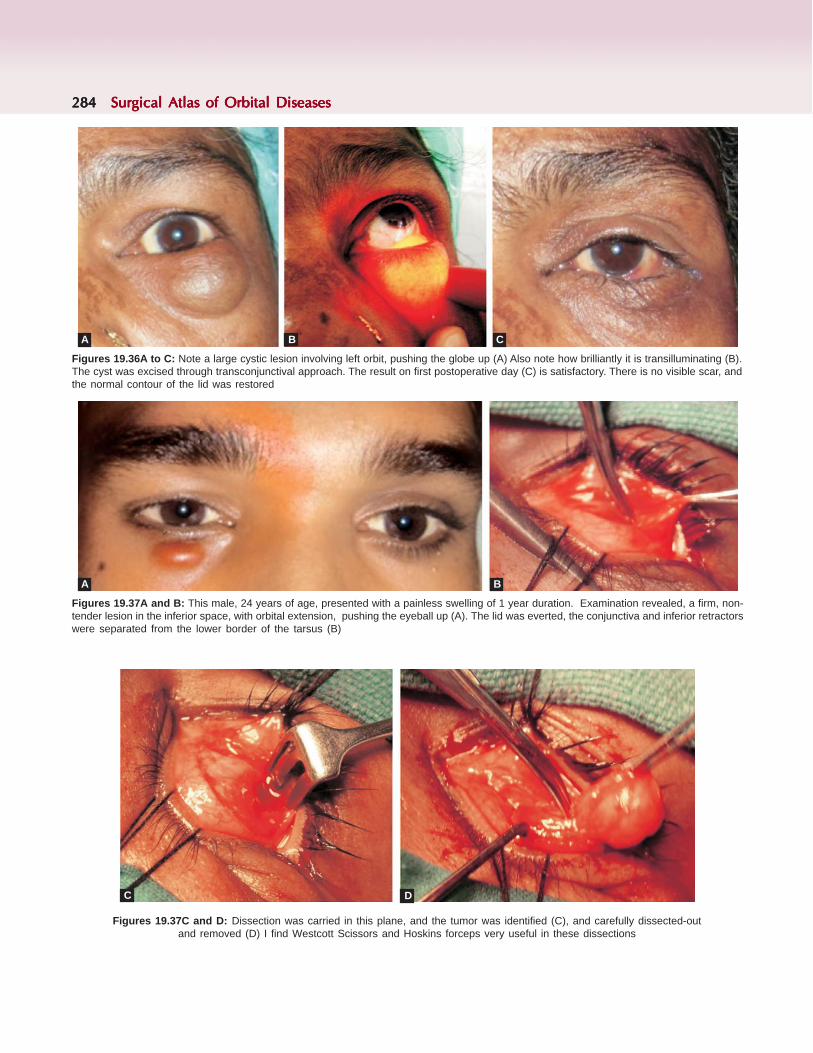
284284284284284 Surgical Atlas of Orbital DiseasesSurgical Atlas of Orbital DiseasesSurgical Atlas of Orbital DiseasesSurgical Atlas of Orbital DiseasesSurgical Atlas of Orbital Diseases
Figures 19.36A to C: Note a large cystic lesion involving left orbit, pushing the globe up (A) Also note how brilliantly it is transilluminating (B).The cyst was excised through transconjunctival approach. The result on first postoperative day (C) is satisfactory. There is no visible scar, andthe normal contour of the lid was restored
A B C
Figures 19.37A and B: This male, 24 years of age, presented with a painless swelling of 1 year duration. Examination revealed, a firm, non-tender lesion in the inferior space, with orbital extension, pushing the eyeball up (A). The lid was everted, the conjunctiva and inferior retractorswere separated from the lower border of the tarsus (B)
A B
Figures 19.37C and D: Dissection was carried in this plane, and the tumor was identified (C), and carefully dissected-outand removed (D) I find Westcott Scissors and Hoskins forceps very useful in these dissections
C D

Decision MakingDecision MakingDecision MakingDecision MakingDecision Making 285285285285285
Swinging lower eye lid approach is one of myfavorite procedures for large lesions in peripheralsurgical space, for optic nerve decompression inthyroid associated orbitopathy, and orbitalfloor fractures. The advantages include anexcellent exposure of field of surgery, possibility of3-wall decompression and very minimal scar(Figures 19.39A to 19.43B).
Thyroid associated orbitopathy: In India, I find theclinical presentation of thyroid orbitopathy lessaggressive than in western reports. This is the sameobservation of almost all my colleagues in India.However, I came across many Indians at Vancouverwhose presentation of thyroid associated orbitopathy
was as severe as in the Caucasians. The weatherconditions or the life style may be the reason for thisdifference and requires a systematic evaluation.
In thyroid orbitopathy, steroids are indicatedwhen the patient has inflammatory symptoms ordiplopia. Optic nerve compression is anotherindication, before surgical decompression isperformed. Radiotherapy with linear accelerators innon-diabetics patients is an option when theinflammatory signs and symptoms are controlledwith steroids. Surgery is usually in stages,decompression followed next by muscle surgery forsquint/diplopia, and then lid surgery forblepharochalasis/lid retraction.
Figures 19.38A and B: The conjunctiva and the inferior retractors are carefully reattached to the lower border oftarsus with interrupted, 6-0 Vicryl buried sutures (A) Note that the normal contour of the lid was restored on thefirst postoperative day. Note also that the position of the globe is back to normal, and there was no scar. Thissurgery can be performed comfortably under local anesthesia
A B
Figures 19.39A and B: Female 55 years presented with bilateral proptosis of 6 months and defective vision of 3months. She is hypothyroid and diabetic and has typical features of thyroid associated orbitopathy. Her BCVA was20/200 20/400, and has severe optic disc edema
A B

286286286286286 Surgical Atlas of Orbital DiseasesSurgical Atlas of Orbital DiseasesSurgical Atlas of Orbital DiseasesSurgical Atlas of Orbital DiseasesSurgical Atlas of Orbital Diseases
Figures 19.40A and B: CT scan of the orbits showed gross enlargement of the inferior, medial andsuperior recti, sparing the tendons. Note the bilateral apical compression, which is evident in both axialand coronal sections
B
Figures 19.41A and B: She underwent bilateral 3 wall decompression along with excision of fat(about 6 cc) from each orbit by swinging lower eyelid approach
A
BFigures 19.42A and B: Note the gross difference between the preoperative (A) and postoperative(B) conditions. Note that the postoperative scar after swinging lower eyelid approach is practicallynot visible. The patient's vision improved to 20/20 and 20/30
BA
A

Decision MakingDecision MakingDecision MakingDecision MakingDecision Making 287287287287287
Figures 19.43A and B: The visual fields of right eye before(A) and after(B) orbital decompres-sion showing marked improvement
BA
REFERENCES
1. Kaur A, Agrawal A : "Orbital tuberculosis - an interestingcase report", Int Ophthalmol. 2005;26(3):107-9.
2. Shome D, Honavar SG, Vemuganti GK, Joseph J. "Orbitaltuberculosis manifesting with enophthalmos and causinga diagnostic dilemma" Ophthal Plast Reconstr Surg. 2006;22(3):219-21.
3. Aversa do Souto A, Fonseca AL, Gadelha M, Donangelo I,Chimelli L, Domingues FS, "Optic pathways tuberculomamimicking glioma: case report" Surg Neurol. 2003;60(4):349-53.
4. Aggarwal D, Suri A, Mahapatra AK, "Orbital tuber-culosis with abscess" J Neuroophthalmol. 2002;22(3):208-10.
5. Mavrikakis I, Rootman J.: "Diverse clinical presentations oforbital sarcoid", Am J Ophthalmol. 2007;144(5):769-77.
6. Biswas J, Krishnakumar S, Raghavendran R, Mahesh L: Lidswelling and diplopia as presenting features of orbitalsarcoid"Indian J Ophthalmol. 2000;48(3):231-3.
7. Segal EI, Tang RA, Lee AG, Roberts DL, Campbell GA:"Orbital apex lesion as the presenting manifestation ofsarcoidosis"J Neuroophthalmol.2000;20(3):156-8.
8. Ahmad SM, Esmaeli B. "Metastatic tumors of the orbitand ocular adnexal" Curr Opin Ophthalmol. 2007;18(5):405-13.
9. Sivagnanavel V, Riordan-Eva P, Jarosz J, Portmann B,Buxton-Thomas M; "Bilateral orbital metastases from aneuroendocrine tumor" J Neuroophthalmol.2004;24(3):240-2.
10. Bakri SJ, Krohel GB, Peters GB, Farber MG: " Spermaticcord leiomyosarcoma metastatic to the orbit" Am JOphthalmol. 2003;136(1):213-5.
11. McCulley TJ, Yip CC, Bullock JD, Warwar RE, Hood DL:"Cervical carcinoma metastatic to the orbit", Ophthal PlastReconstr Surg. 2002;18(5):385-7.
12. Mohadjer Y, Wilson MW, Fuller CE, Haik BG: "Primarypelvic telangiectatic osteosarcoma metastatic to both orbits",Ophthal Plast Reconstr Surg. 2004;20(1):77-9.
13. Heerema A, Sudilovsky D: "Mucinous adenocarcinoma ofthe ovary metastatic to the eye: report of a case withdiagnosis by fine needle aspiration biopsy", Acta Cytol.2001;45(5):789-93.
14. Saikia B, Dey P, Saikia UN, Das A : "Fine needle aspirationcytology of metastatic scalp nodules", Acta Cytol.2001;45(4):537-41.

288288288288288 Surgical Atlas of Orbital DiseasesSurgical Atlas of Orbital DiseasesSurgical Atlas of Orbital DiseasesSurgical Atlas of Orbital DiseasesSurgical Atlas of Orbital Diseases
Ramesh Murthy, Anirban Bhaduri, Vikas Menon, Santosh G Honavar
General PrinciplesBefore undertaking any surgery in the orbit, athorough knowledge of the normal eyelid and orbitalanatomy is essential. In addition we always evaluateevery case starting with a thorough history,meticulous examination, imaging and laboratoryinvestigations. This helps us to arrive at a differentialdiagnosis. As a general rule, an excisional biopsy isindicated for well circumscribed lesions or thosewhich are benign, while an incisional biopsy isperformed for a lesion which is suggestive ofmalignancy or inflammation.
Thorough understanding of CT and MRI is a mustand we must emphasize that familiarity with surgicalapproaches is essential. One should observe and assistorbital surgeries before one embarks into thisindependently.
One should also understand the instrumentationneeded for this surgery. When using electric sawsone needs to ensure safety of the patient's eyeball aswell as of the surgeon and the team. Protectiveglasses should be worn along with face masks toprevent inadvertent spillage of blood and bonefragments. Use of retractors is required to provideadequate exposure. One also needs to be careful notto exert pressure on the globe when using theretractors. Wright's and malleable ribbon retractorsare used not only to expose the tissues but also toprotect the surrounding tissues. Proper illuminationand adequate magnification is essential to visualizethe orbital structures.1
The key to safe surgery is good surgical exposure.The surgical incision should be of adequate length.This can be supplemented by traction sutures at
OrbitotomiesOrbitotomiesOrbitotomiesOrbitotomiesOrbitotomies
appropriate locations. While cosmesis is desirable,safe and adequate surgical access is the aim. Patienceis required when dissecting lesions in the orbit.Gentle blunt dissection is performed using a Freerelevator or lens spatulas to separate the orbital massfrom the surrounding tissues. Repositioning of theretractors is essential as the dissection proceeds. Inorder to perform dissection, the blunt tipped Westcotttenotomy scissors is used. The little finger is a usefulinstrument to palpate the lesion and perform bluntdissection. Gentle counter traction is needed whendissecting an orbital mass. A cryoprobe can be usedto hold the mass and pull it gently while dissectionis going on.2
Adequate hemostasis needs to be ensured duringorbital surgery. Hypotensive anesthesia is advan-tageous. However the anesthetist should bring backthe blood pressure to normal following surgery, toensure adequate intraoperative hemostasis. Bipolarcautery should be used in the orbit. When the sourceof bleed cannot be identified, simple packing withgauze should be performed. Indirect pressure overthe closed lids is also useful. Bone wax or gel foamsoaked in thrombin can also be used to stem bleedingduring orbital surgery.
For an accurate pathological diagnosis, it isnecessary to obtain a sample of adequate size,representing the lesion and undamaged by cauteryor surgical instrumentation. Routine samples areusually sent in formalin. If a fresh sample needs tobe sent or frozen section analysis is required, it isbest to inform the pathologist beforehand. Therequisition form sent to the pathologist should havedetailed clinical findings.
20C H A P T E R

OrbitotomiesOrbitotomiesOrbitotomiesOrbitotomiesOrbitotomies 289289289289289
Approaches
Many approaches can be used to gain access to theorbit.3 The various types of incisions are demon-strated in Figure 20.1.The approaches can be
1. Anterior orbitotomya. Approach to the superior orbit
— Benedict incision4
— Upper lid crease incision— Byron Smith lid split incision5
b. Approach to the inferior orbit— Mc Cord swinging lower lid incision6
— Subciliary incisionc. Approach to the medial orbit
— Lynch incision— Gull wing incision— Transcaruncular incision
2. Lateral orbitotomy3. Transnasal endoscopic approach4. Transantral or Calwell–Luc approach5. Transfrontal orbitotomy.
Anterior Orbitotomy
This approach is useful for anterior orbital lesions,for the drainage of hematomas and abscesses andincision biopsy of posteriorly placed orbital lesions.
For superior lesions a transcutaneous approachthrough the upper lid skin crease leaves a less visiblescar. However approach thorough the lower lid skincan leave an unsightly scar. The Byron Smith lid splitincision which can be used to access largesuperomedial lesions is not very popular.
A Lynch incision can be used to approach themedial subperiosteal space. A transcaruncularapproach is also useful and may be combined with alateral orbitotomy.
For inferior orbital lesions a lower eyelidtransconjunctival approach is the least disfiguring.
Swinging Lower Lid Flap
The first step is to make a mark on the skinhorizontally at the lateral canthus. A bridle suture isplaced through the inferior rectus muscle and then amosquito artery forceps is applied to the lateralcanthus along the skin mark to provide hemostasiswhen the incision is made. The skin is then incisedwith a Bard parker knife or a Colorado needle. Aftercutting the lateral canthus, inferior cantholysis isperformed. Two 4/0 silk traction sutures are passedthrough the lower lid margin through the grey lineof the lower lid. The traction sutures are secured toprovide exposure. A conjunctival incision is thenmade at the inferior border of the tarsus or slightlylower starting laterally and then extending itmedially. The plane between the orbicularis muscle
Figure 20.1: Various surgical approaches for orbit

290290290290290 Surgical Atlas of Orbital DiseasesSurgical Atlas of Orbital DiseasesSurgical Atlas of Orbital DiseasesSurgical Atlas of Orbital DiseasesSurgical Atlas of Orbital Diseases
and the orbital septum is dissected to the inferiororbital margin. Further traction sutures can be placedthrough the conjunctiva and inferior retractors toimprove visualization. A Desmarre's retractor canbe used to give traction and expose the tissues. Theperiosteum or septum is then opened. With the helpof retractors the lesion is exposed and bluntdissection performed to separate the lesion andperform a biopsy. Adequate hemostasis is ensured.The edges of the periosteum are sutured with 6.0vicryl interrupted sutures. The conjunctiva is closedwith interrupted 6/0 vicryl sutures and the lateralcanthotomy is repaired by using 6/0 prolene suturesto secure the tarsus to the lateral orbital periosteum.Closure is performed in 2 layers with 6/0 vicryl forthe soft tissues and 6/0 prolene for the skin.Antibiotic ointment is instilled and a pressuredressing is applied. The steps of this technique havebeen demonstrated in Figures 20.2A to Q.
Lateral Orbitotomy
This is a useful technique for lesions in the intraconalspace and lesions lateral to the optic nerve. Inaddition this is useful for large lesions anywhere asthis can be combined with other approaches to allowthe globe to be moved laterally for increasing surgicalexposure. The Berke-Reese incision disturbs thelateral canthus and leaves a less satisfactory scar.7
The modified Stallard Wright approach is a goodapproach. We are presently using a lid creaseapproach which gives aesthetically pleasing results.
Stallard-Wright Lateral Orbitotomy8
The first step is to pass 4/0 silk sutures below theinsertions of the lateral and superior rectus musclesand form a loop. This is tied to get a hold on themuscle and for identifying the muscle as surgeryprogresses to avoid any inadvertent damage to themuscles. An incision is made on the skin. The incisionstarts from just below the lateral aspect of the browand ends in a rhytid over the anterior zygomaticarch. The skin incision is made with a no. 11 Bard-Parker blade. Under stretch and lifting the tissues,the subcutaneous tissues are dissected down to theperiosteum using a radiofrequency monopolar probe.As this dissection proceeds, one must ensure thatadequate hemostasis is achieved by using a bipolarcautery. Multiple 4/0 silk traction sutures are placed
to gain exposure. The periosteum is exposed overthe whole lateral orbital margin. The periosteum iscut with a monopolar probe about 4 mm behind theorbital rim starting superiorly and ending inferiorlyjust above the zygomatic arch. Relaxing incisions needto be given to the periosteum. The periosteum is thenreflected. The periorbita is also lifted away from theorbital bone upto the anterior one third of the orbit.This has to be performed with care to avoid anybreach. The zygomaticotemporal and zygo-maticofacial vessels may bleed and may need to becauterized. The temporalis muscle also needs to beseparated laterally and reflected. This muscle is veryvascular and adequate hemostasis needs to beensured. Incision lines are made on the bone about 3mm above the frontozygomatic suture superiorly andjust above the zygomatic arch inferiorly. ADesmarre's retractor is placed to pull the skin andsubcutaneous tissue laterally and a lid guard is placedinside the orbit to protect the contents of the orbit.Using an oscillating saw, cuts are made along theincision lines on the bone. Irrigation is performed asthe saw is being used. Drill holes may be made onboth sides adjacent to the bone cut. Once the cutshave been made, the bone fragment is held with abone rongeur and moved back and forth until itfractures posteriorly. It is then removed and wrappedin wet saline gauze. The bone can be further nibbledwith a bone punch or removed with a burr for furtherexposure. Hemostasis is essential especially in theregion of the temporal fossa. Bone wax may be usedto cover any bleeding points in the bone. A T shapedincision is made in the periorbita. This is done witha no 15 Bard Parker blade or a blunt tipped Westcotttenotomy scissors. The incision is then extendedcircumferentially. A nick is made posteriorly and theperiorbita at the cut edges is grasped and gentlyspread apart to extend the cut posteriorly. Dissectionof the orbital mass is performed by blunt dissection.Location of the orbital mass can be confirmed bygentle palpation. Wrights retractors and malleableretractors are used to gently retract the globe andkeep the orbital fat away from the area of dissection.Hemostasis is achieved by bipolar forceps. The pupilis checked at regular intervals.9 A cryoprobe can beused to aid delivery of the lesion. If it is anencapsulated lesion, dissection is performed close tothe capsule using a Freer elevator. Once the orbital

OrbitotomiesOrbitotomiesOrbitotomiesOrbitotomiesOrbitotomies 291291291291291
surgery has been completed, the periorbita can beclosed with 6/0 interrupted vicryl sutures. The bonefragment may be replaced and either a wiringthrough the holes is performed or the cut edges arestuck with cyanoacrylate glue. The periosteum is thenclosed with 6/0 vicryl sutures. The subcutaneoustissues are apposed with 6/0 vicryl sutures and theskin is closed with 6/0 prolene continuous sutures.Intravenous steroids are preferably given at the endof the procedure. A suction drain may or may not beplaced. A pressure dressing is placed after applyingantibiotic ointment. The steps of this technique havebeen demonstrated in Figures 20.3A to S.
Transcarcuncular Approach
This approach through the conjunction for medialorbital lesions is technically difficult but can givebetter cosmesis than a skin approach. This can becombined with a lateral orbitotomy for greaterexposure.
Transnasal Endoscopic Approach and Tran-santral Approach
This is best performed by or with the assistance ofan ENT surgeon and is especially useful for biopsyof lesions near the orbital apex or arising from thesinuses. This is also a useful approach to remove anybone fragments that may be impinging on the opticnerve following an orbital fracture. This is useful forinferior lesions especially those arising predominantlyfrom the maxillary or ethmoidal sinuses forperforming a biopsy of these lesions.10
Transfrontal Orbitotomy11-13
This approach is performed to access lesions at theorbital apex. A team approach including aneurosurgeon is needed. There are potentialcomplications in this procedure especially ptosis andextraocular muscle palsy.
A bicoronal flap is created. The frontal bone flapis hinged laterally, still attached to the temporalismuscle and pericranium. This provides good exposureof the medial, superior and lateral orbital apex. If thelesion is confined to the orbit, an extradural approachis undertaken. For orbital lesions extending into thecranium, an intradural approach is needed. The orbitalroof is removed, keeping the periorbita intact. Thefrontal nerve is an important landmark, which runs
anteroposteriorly over the levator muscle. Entry intothe orbit is made medially avoiding the area of thesuperior orbital fissure. The orbital roof is recons-tructed by using an alloplastic material or using theinner table of the frontal bone flap.
Complications
This is a major surgery and there can becomplications.14
1. Vasculara. Bleedingb. CRVO, BRVOc. Vitreous hemorrhaged. Short posterior ciliary artery occlusion
2. Neural/Musculara. Corneal anesthesiab. Internal ophthalmoplegiac. Extraocular muscle paresisd. Lateral rectus adhesione. Ptosisf. Optic neuropathyg. CSF leakh. hypoesthesia
Postoperative Management
The patient is advised bed rest with the head elevatedand advised not to strain to prevent increase in thevenous pressure. Steroids and anti-inflammatorymedication is prescribed. Systemic antibiotics maybe prescribed. The vision, pupil, ocular motility andfundus is assessed.
CASE ILLUSTRATIONS
Case 1
(Swinging lower lid incision of McCord)A 7-year-old girl presented with complaints of a
palpable mass below right eye, graduallyincreasing in size over 3 months (Figure 20.2A).Clinically a firm to hard mass was palpable in theanterior inferior orbit (arrow indicates theinferomedial orbital mass) (Figure 20.2B). The masswas immobile and non-tender. The mass was causingsuperior displacement of the globe. Anterior segmentand fundus examination were normal except forindentation effect of the mass on the globe, seeninferiorly. There was no limitation of ocularmovements.

292292292292292 Surgical Atlas of Orbital DiseasesSurgical Atlas of Orbital DiseasesSurgical Atlas of Orbital DiseasesSurgical Atlas of Orbital DiseasesSurgical Atlas of Orbital Diseases
CT scans showed an ill defined, hyperdense,extraconal mass in the inferomedial quadrant of theorbit with indentation of the globe and distortion ofthe medial wall of the orbit (Figure 20.2B).
Excision biopsy of the mass was planned and wasdone through an anterior orbitotomy approach usinga swinging eyelid incision and the mass was removedcompletely (Figures 20.2C to Q).
Steps of Surgery
Figure 20.2A: A 7-year-old girl presented with a mass below theright eye (arrow) with history of gradual increase in size over 3months
Figure 20.2B: CT scan (coronal section) revealed an ill definedhyperdense, inferior orbital mass in the right orbit (arrow)
Figure 20.2C: 4/0 silk sutures are passed through the lower lidmargin, one near the lateral canthus and one centrally
Figure 20.2D: Mark is made on the skin horizontally at the lateralcanthus and a lid speculum is placed. An artery forceps is used tocrush the tissues along the mark
Figure 20.2E: A lateral canthotomy is performed with scissors
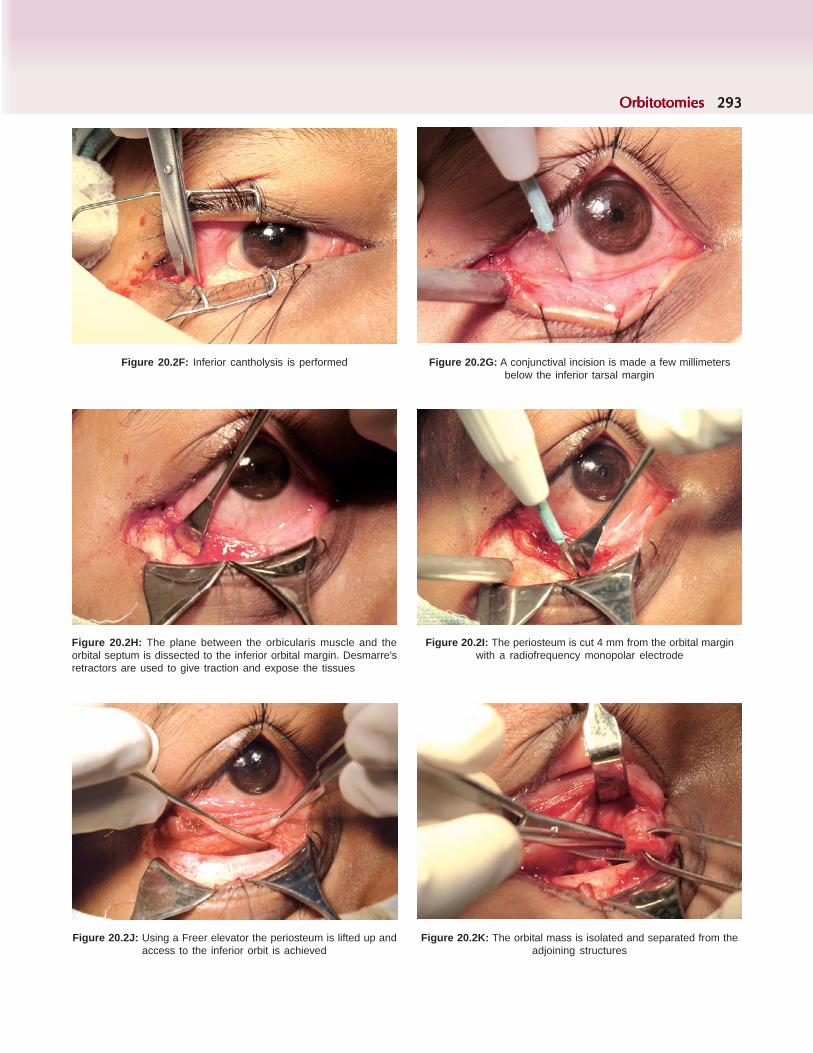
OrbitotomiesOrbitotomiesOrbitotomiesOrbitotomiesOrbitotomies 293293293293293
Figure 20.2F: Inferior cantholysis is performed Figure 20.2G: A conjunctival incision is made a few millimetersbelow the inferior tarsal margin
Figure 20.2H: The plane between the orbicularis muscle and theorbital septum is dissected to the inferior orbital margin. Desmarre'sretractors are used to give traction and expose the tissues
Figure 20.2I: The periosteum is cut 4 mm from the orbital marginwith a radiofrequency monopolar electrode
Figure 20.2J: Using a Freer elevator the periosteum is lifted up andaccess to the inferior orbit is achieved
Figure 20.2K: The orbital mass is isolated and separated from theadjoining structures

294294294294294 Surgical Atlas of Orbital DiseasesSurgical Atlas of Orbital DiseasesSurgical Atlas of Orbital DiseasesSurgical Atlas of Orbital DiseasesSurgical Atlas of Orbital Diseases
Figure 20.2N: The edges of the periosteum are sutured with 6/0vicryl interrupted sutures
Figure 20.2O: The conjunctiva is closed with interrupted 6/0 vicrylsutures and the lateral canthotomy is repaired by using 6/0 prolenesutures to secure the tarsus to the lateral orbital periosteum
Figure 20.2M: The cut edges of the periosteum are then isolatedFigure 20.2L: A pink firm well defined mass was removedfrom the inferior orbit
Figure 20.2P: Closure is performed in 2 layers with 6/0 vicryl forthe soft tissues and 6/0 prolene for the skin
Figure 20.2Q: One week post surgery, there is minimal lid edema andthe wound is well apposed. Histopathological examination revealed itwas a degenerated parasitic cyst with chronic inflammation andcalcification. The child had an uneventful recovery thereafter

OrbitotomiesOrbitotomiesOrbitotomiesOrbitotomiesOrbitotomies 295295295295295
Case 2
(Modified Stallard Wright orbitotomy)A 30-year-old female presented with gradually
increasing protrusion of the left eye for one yearassociated with diplopia followed by progressive lossof vision, watering, redness and pain in the eye. Onclinical examination, she had severe non-axialproptosis measuring 12 mm with lateral displacementof the globe (Figure 20.3A). There was protrusion oforbital fat through the orbital septum. The mass waspalpable and seemed to encompass the globe. It wasfirm in consistency, with mild tenderness. There wassevere restriction of eye movements, lagophthalmosand exposure keratopathy. Fundus examinationshowed a pale optic disc with blurred margins and
collateral vessels on the disc. CT scan showed anirregular intraconal mass; optic nerve could not beseen separately (Figures 20.3B and C). The massshowed specks of intralesional calcification and wascausing distortion of the globe and medial orbitalwall indicative of a large optic nerve sheathmeningioma. Incision biopsy was done through asubbrow incision which confirmed the diagnosis ofmeningioma. As there was no optic canal orintracranial extension, it was decided that debulkingof the mass would restore the eye to its naturalposition although the eye was blind. Debulking wassubsequently done through a lateral orbitotomyapproach (modified Stallard-wright incision).
Steps of Surgery
Figure 20.3A: A 30-year-old lady presented with progressiveproptosis of the left eye with downward and lateral displacement ofthe globe
Figure 20.3B: CT scan (coronal section) showed a large, irregular,hyperdense mass behind the left globe
Figure 20.3C: CT scan (axial section) showed the ill definedmass occupying most of the left orbit (arrow) Figure 20.3D: A mark is made on the skin for the S shaped incision

296296296296296 Surgical Atlas of Orbital DiseasesSurgical Atlas of Orbital DiseasesSurgical Atlas of Orbital DiseasesSurgical Atlas of Orbital DiseasesSurgical Atlas of Orbital Diseases
Figure 20.3G: The periosteum is cut with a monopolar probe about 4mm behind the orbital rim starting superiorly and ending inferiorly justabove the zygomatic arch
Figure 20.3H: The periosteum is then reflected. The periorbita is alsolifted away from the orbital bone upto the anterior one third of the orbit
Figure 20.3E: The skin incision is made with a no 11 Bard Parkerblade. The incision starts from just below the lateral aspect of thebrow and ends in a rhytid over the anterior zygomatic arch
Figure 20.3F: Under stretch and lifting the tissues, thesubcutaneous tissue is dissected down to the periosteum
Figure 20.3I: The temporalis muscle is separated from the underlying bone using a bipolar cautery

OrbitotomiesOrbitotomiesOrbitotomiesOrbitotomiesOrbitotomies 297297297297297
Figure 20.3J: Incision lines are made on the bone about 3 mm abovethe frontozygomatic suture superiorly and just above the zygomaticarch inferiorly. A Desmarre's retractor is placed to pull the skin andsubcutaneous tissue laterally and a lid guard is placed inside the orbitto protect the contents of the orbit. Using an oscillating saw, cuts aremade along the incision lines on the bone. Irrigation is performed asthe saw is being used
Figure 20.3K: Once the cut have been made, the bone fragment isheld with a bone rongeur and moved back and forth until it fracturesposteriorly
Figures 20.3L and M: T shaped incision is made in the periorbita with a blunt tipped Westcott scissors
Figure 20.3N: The cut edges of the periorbita are grasped andgently spread apart to extend the cut posteriorly
Figure 20.3O: Retractors are used to keep the orbital fat away anddissection of the mass is performed by blunt dissection
L M

298298298298298 Surgical Atlas of Orbital DiseasesSurgical Atlas of Orbital DiseasesSurgical Atlas of Orbital DiseasesSurgical Atlas of Orbital DiseasesSurgical Atlas of Orbital Diseases
Figure 20.3P: A reddish friable firm mass wasremoved from the orbit
Figure 20.3Q: The periorbita is closed withinterrupted 6/0 vicryl sutures
Figure 20.3R: The subcutaneous tissue is apposed with 6/0 vicrylsutures
Figure 20.3S: The skin is closed with continuous 6/0 prolenesuture. The patient was doing well at last follow-up
REFERENCES
1. Wright JE et al. Continuous monitoring of the visual evokedresponse during intraorbital surgery. Trans OphthalmolSoc UK. 1973;93:311.
2. Putterman A, Goldberg MF Retinal cryoprobe in orbitaltumour management. Am J Ophthalmol 1975;80:88.
3. Leone CR Surgical approaches to the orbit. Ophthalmology1979;86:930.
4. Benedict WL Surgical treatment of tumours and cysts ofthe orbit. Eleventh de Schweinitz lecture. Am J Ophthalmol1949;32:763-73.
5. Smith B The anterior surgical approach to orbital tumours.Trans Am Acad Ophthalmol Otolaryngol 1966;70:607-11.
6. Mc Cord CD Jr Orbital decompression for Graves' disease.Exposure through lateral canthal and inferior fornixincision. Ophthalmology 1981;88:533-41.
7. Berke RN Modified Kronlein operation. AMA ArchOphthalmol 1954;51:609-32.
8. Wright JE Surgical exploration of the orbit. TransOphthalmol Soc UK 1979;99:238-40.
9. Simonton JT, Garber PF, Ahl N Margins of safety in lateralorbitotomy. Arch Ophthalmol 1977;95:1229-31.
10. Maroon JC, Kennerdell JS. Microsurgical approach to orbitaltumours. Clin Neurosurg 1979;26:479-89.
11. Shucart W Transfrontal approach to the orbit. In HornblassA(ed): Tumours of the Ocular Adnexa and Orbit St Louis,CV Mosby, 1979.
12. Love JG, Benedict WL Transcranial removal of intraorbitaltumours. JAMA 1945;121:777-84.
13. Schurmann K, Oppel O. Transfrontal orbitotomy as amethod of operation in retrobulbar tumours. Klin MonatsblAugenheikld 1961;139:130-59.
14. Long JC, Ellis PP Total unilateral visual loss following orbitalsurgery. Am J Ophthalmol 1971;71:218-20.

Subrahmanyam Mallajosyula, B Ranganadha Reddy, M Chandrasekhar Reddy
Multidisciplinary ApproachMultidisciplinary ApproachMultidisciplinary ApproachMultidisciplinary ApproachMultidisciplinary Approachto Proptosisto Proptosisto Proptosisto Proptosisto Proptosis
Introduction
The orbit is located between the facial structures,paranasal sinuses and the skull base. Some of thebony walls that separate the orbit and the paranasalsinuses are very thin. Orbit is in direct communicationwith brain through the optic canal. Variouspathological lesions extend from these surroundingstructures in to the orbit and vice versa. Rarely thelesion can involve the sinuses, orbit and the brain,like sino-orbito-cranial mucormycosis. Thus orbit isan area of interest for several other surgicalspecialties like ENT specialist and neurosurgeon.Ophthalmic surgeons can deal with orbit by a numberof direct orbital approaches. ENT surgeons can gainaccess to pathological conditions arising with in theair sinuses through percutaneous approaches, oralcavity or endonasal endoscopic approaches.Neurosurgeons can access to those tumors thatinvade both the intracranial and orbital space. Adetailed discussion of these lesions is beyond thescope of this book. However we review the variousENT and neurological lesions that may present withproptosis and outline various surgical approachestowards managing these lesions.
Surgical Anatomy
The orbital cavity is a 30 ml pear shaped; four walledstructure. The central axis of the orbit and the visualaxis of the globe are separated by 23 degrees.
The medial wall is formed by the lacrimal andethmoidal bones along with body of the sphenoidbone.
Lateral wall of the orbit is formed by zygomaticbone and greater wing of sphenoid, floor is formedzygomatic, maxillary and palatine bones and roof isformed by horizontal portion of the frontal bone andby the lesser wing of the sphenoid bone.
The optic canal: A tubular cavity lying in thedeepest portion of the orbit enters the cranial cavitymedial to the anterior clinoid process. The optic canalmeasures an average 5 to 10 mm long, 4.5 mm wideand 5 mm in height.
The thickness of the medial wall of the optic canalis an important surgical consideration in thetransethmoidal and transsphenoidal approaches tothe canal. In about 12% of cases the medial wall ofthe optic canal is bordered not by the sphenoid sinusbut by a posterior or superior ethmoidal air cell. Theinclination angle of the optic canal relative to itssurroundings is practically important concern.
For the superior orbital fissure, through whichthe intracranial duramater joins the periorbita, medialmargin is formed by the lesser wing of the sphenoidand greater wing of sphenoid forms the lateralmargin.
Optic nerve has a flattened longitudinal shape,measure approximately 4 × 6 mm. As it entersthe cranial end of the optic canal, it is circular and5 mm in diameter, and continues to the globe as a6 × 4 mm vertically oval structure.
The intracranial pia and arachnoid accompaniesthe nerve from the chiasm and both fuse at the globe.There are loose trabeculations in the subarachnoidspace.
21C H A P T E R

300300300300300 Surgical Atlas of Orbital DiseasesSurgical Atlas of Orbital DiseasesSurgical Atlas of Orbital DiseasesSurgical Atlas of Orbital DiseasesSurgical Atlas of Orbital Diseases
The annulus of Zinn forms the tendinous insertionof the extraocular muscle cone at the apex. It spansthe superior orbital fissure creating an intraconal andextraconal compartment of the fissure, dissecting thestructures that run through it.
ENT APPROACH TO PROPTOSIS
The paraorbital region represents the paranasal airsinuses surrounding the orbit. Tumors of the orbitand paraorbital region sometimes distort the naturalarchitecture of the eye. Although proptosis may seemto be primarily the concern of the ophthalmologist,because of the close proximity of the orbit and paranasal sinuses and various connecting fissures andforamina between the two, many ENT lesions maypresent with proptosis.
Various Etiological Factors of Proptosis in ENTThere are various etiological factors of interest tothe otolaryngologists, which can cause proptosis.Diseases can be classified as follows:
a. Diseases of the orbit caused by the inflammationin Paranasal sinuses.
b. Tumors of the orbito-sinual-region.c. Diseases of the lacrimal apparatus secondary to
sinonasal diseases.
a. Infection and inflammation
A variety of inflammatory and infective sinonasalconditions may impinge on the orbit; the commonestof which are as follows:
1. Acute purulent sinusitis2. Gross polyposis-particularly when it begins at
an early age3. Fungal infections4. Mucocele-commonest is frontoethmoidal
mucocele.
b. Tumors of the orbito–sinual disease
The Paranasal sinuses tumors are classified into benignand malignant.
Benign Paranasal sinus tumorA. Epithelial tumors:
1. Papilloma 2. Inverting papilloma 3. Tumors of minor salivary glands
B. Angiomatous tumors:1. Juvenile nasopharyngeal angiofibroma2. Hemangiopericytoma3. Lymphangioma
C. Mesenchymal tumors:1. Fibrous dysplasia2. Osteomas
D. Odontogenic tumors: AmeloblastomaE. Neurogenic tumors
1. Schwannoma2. Neurofibroma
Malignant paranasal sinus tumorsA. Epithelial tumors
1. Squamous cell carcinoma2. Adenoid cystic carcinoma3. Esthesioneuroblastoma4. Malignant melanoma of sinonasal tract
B. Lymphoreticular tumors:1. Lymphoma–Non-Hodgkin's2. Extramedullary plasmacytoma
C. Mesenchymal tumors:1. Osteogenicsarcoma2. Rhabdomyosarcoma3. Fibrosarcoma4. Chondrosarcoma
c. Diseases of the lacrimal apparatus
1. Chronic dacryocystitis2. Tumors of the lacrimal apparatus
Clinical Manifestations and EvaluationThe most common problems the patients complainedare
a. Proptosisb. Nasal obstructionc. Epistaxisd. Reduced visione. Facial swellingf. Nasal dischargeg. Redness of eyeh. Diplopia
After thorough ENT clinical examination the patientspresented with following manifestations.
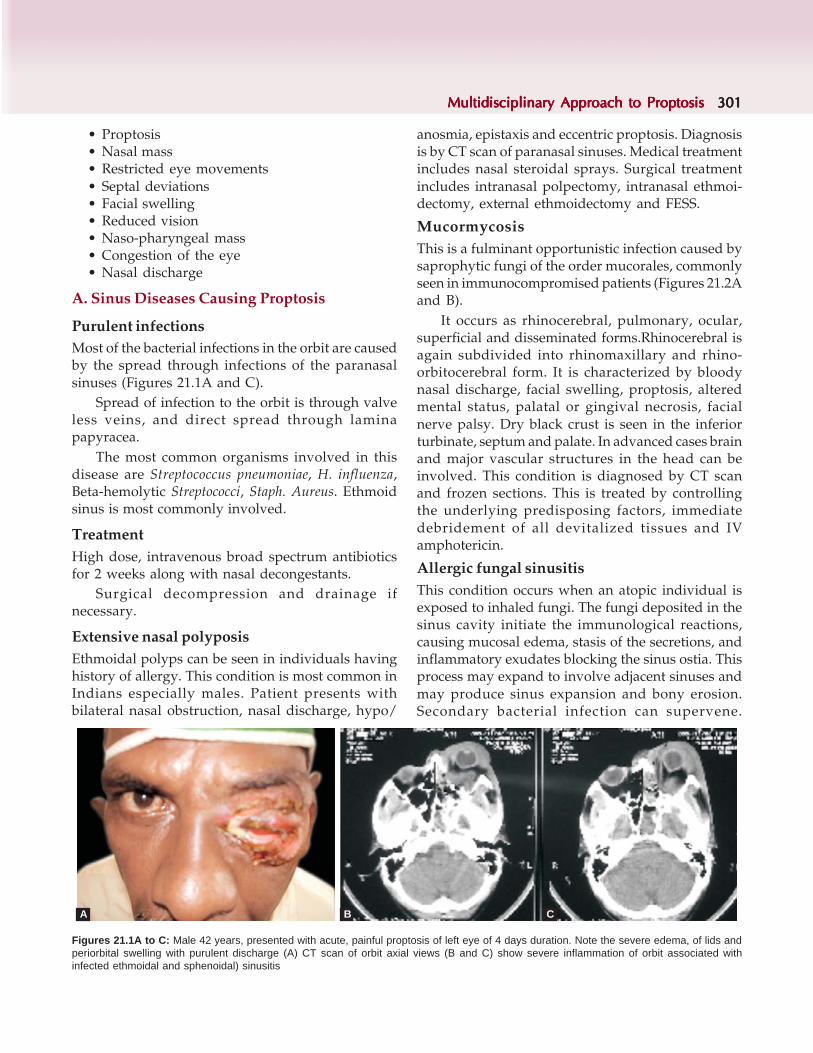
Multidisciplinary Approach to ProptosisMultidisciplinary Approach to ProptosisMultidisciplinary Approach to ProptosisMultidisciplinary Approach to ProptosisMultidisciplinary Approach to Proptosis 301301301301301
Figures 21.1A to C: Male 42 years, presented with acute, painful proptosis of left eye of 4 days duration. Note the severe edema, of lids andperiorbital swelling with purulent discharge (A) CT scan of orbit axial views (B and C) show severe inflammation of orbit associated withinfected ethmoidal and sphenoidal) sinusitis
• Proptosis• Nasal mass• Restricted eye movements• Septal deviations• Facial swelling• Reduced vision• Naso-pharyngeal mass• Congestion of the eye• Nasal discharge
A. Sinus Diseases Causing Proptosis
Purulent infectionsMost of the bacterial infections in the orbit are causedby the spread through infections of the paranasalsinuses (Figures 21.1A and C).
Spread of infection to the orbit is through valveless veins, and direct spread through laminapapyracea.
The most common organisms involved in thisdisease are Streptococcus pneumoniae, H. influenza,Beta-hemolytic Streptococci, Staph. Aureus. Ethmoidsinus is most commonly involved.
TreatmentHigh dose, intravenous broad spectrum antibioticsfor 2 weeks along with nasal decongestants.
Surgical decompression and drainage ifnecessary.
Extensive nasal polyposisEthmoidal polyps can be seen in individuals havinghistory of allergy. This condition is most common inIndians especially males. Patient presents withbilateral nasal obstruction, nasal discharge, hypo/
anosmia, epistaxis and eccentric proptosis. Diagnosisis by CT scan of paranasal sinuses. Medical treatmentincludes nasal steroidal sprays. Surgical treatmentincludes intranasal polpectomy, intranasal ethmoi-dectomy, external ethmoidectomy and FESS.
MucormycosisThis is a fulminant opportunistic infection caused bysaprophytic fungi of the order mucorales, commonlyseen in immunocompromised patients (Figures 21.2Aand B).
It occurs as rhinocerebral, pulmonary, ocular,superficial and disseminated forms.Rhinocerebral isagain subdivided into rhinomaxillary and rhino-orbitocerebral form. It is characterized by bloodynasal discharge, facial swelling, proptosis, alteredmental status, palatal or gingival necrosis, facialnerve palsy. Dry black crust is seen in the inferiorturbinate, septum and palate. In advanced cases brainand major vascular structures in the head can beinvolved. This condition is diagnosed by CT scanand frozen sections. This is treated by controllingthe underlying predisposing factors, immediatedebridement of all devitalized tissues and IVamphotericin.
Allergic fungal sinusitisThis condition occurs when an atopic individual isexposed to inhaled fungi. The fungi deposited in thesinus cavity initiate the immunological reactions,causing mucosal edema, stasis of the secretions, andinflammatory exudates blocking the sinus ostia. Thisprocess may expand to involve adjacent sinuses andmay produce sinus expansion and bony erosion.Secondary bacterial infection can supervene.
A B C
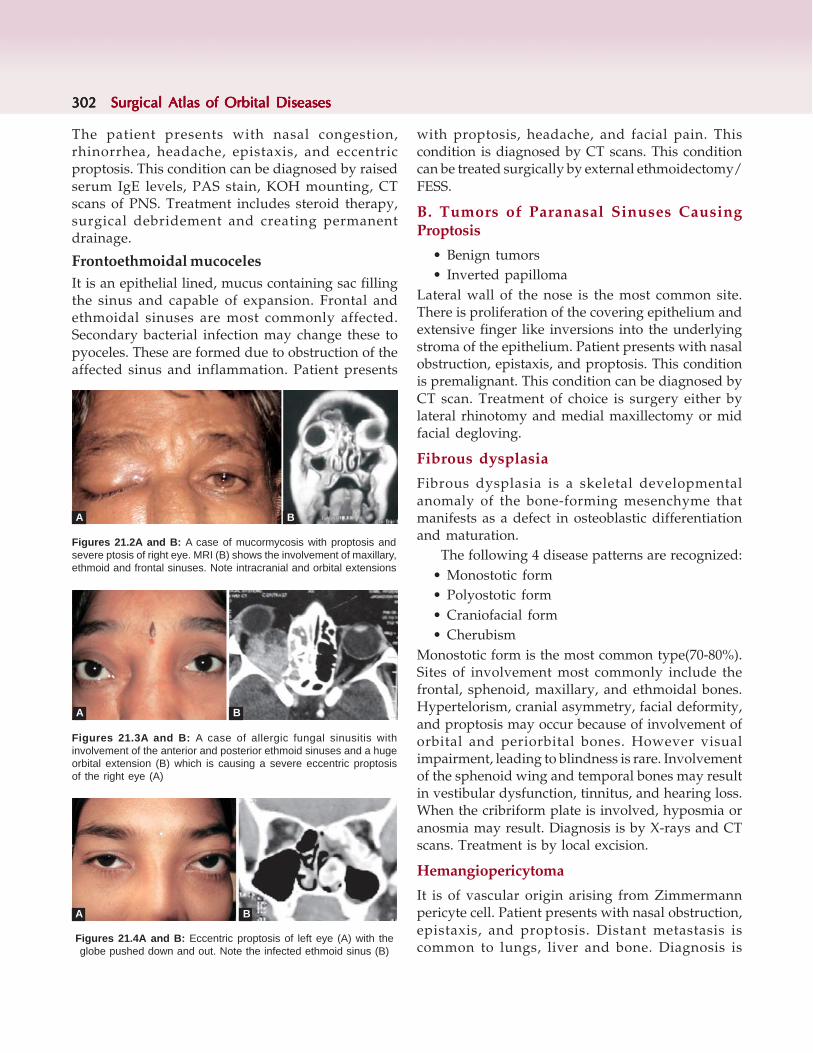
302302302302302 Surgical Atlas of Orbital DiseasesSurgical Atlas of Orbital DiseasesSurgical Atlas of Orbital DiseasesSurgical Atlas of Orbital DiseasesSurgical Atlas of Orbital Diseases
with proptosis, headache, and facial pain. Thiscondition is diagnosed by CT scans. This conditioncan be treated surgically by external ethmoidectomy/FESS.
B. Tumors of Paranasal Sinuses CausingProptosis
• Benign tumors• Inverted papilloma
Lateral wall of the nose is the most common site.There is proliferation of the covering epithelium andextensive finger like inversions into the underlyingstroma of the epithelium. Patient presents with nasalobstruction, epistaxis, and proptosis. This conditionis premalignant. This condition can be diagnosed byCT scan. Treatment of choice is surgery either bylateral rhinotomy and medial maxillectomy or midfacial degloving.
Fibrous dysplasia
Fibrous dysplasia is a skeletal developmentalanomaly of the bone-forming mesenchyme thatmanifests as a defect in osteoblastic differentiationand maturation.
The following 4 disease patterns are recognized:• Monostotic form• Polyostotic form• Craniofacial form• Cherubism
Monostotic form is the most common type(70-80%).Sites of involvement most commonly include thefrontal, sphenoid, maxillary, and ethmoidal bones.Hypertelorism, cranial asymmetry, facial deformity,and proptosis may occur because of involvement oforbital and periorbital bones. However visualimpairment, leading to blindness is rare. Involvementof the sphenoid wing and temporal bones may resultin vestibular dysfunction, tinnitus, and hearing loss.When the cribriform plate is involved, hyposmia oranosmia may result. Diagnosis is by X-rays and CTscans. Treatment is by local excision.
Hemangiopericytoma
It is of vascular origin arising from Zimmermannpericyte cell. Patient presents with nasal obstruction,epistaxis, and proptosis. Distant metastasis iscommon to lungs, liver and bone. Diagnosis is
The patient presents with nasal congestion,rhinorrhea, headache, epistaxis, and eccentricproptosis. This condition can be diagnosed by raisedserum IgE levels, PAS stain, KOH mounting, CTscans of PNS. Treatment includes steroid therapy,surgical debridement and creating permanentdrainage.
Frontoethmoidal mucocelesIt is an epithelial lined, mucus containing sac fillingthe sinus and capable of expansion. Frontal andethmoidal sinuses are most commonly affected.Secondary bacterial infection may change these topyoceles. These are formed due to obstruction of theaffected sinus and inflammation. Patient presents
Figures 21.4A and B: Eccentric proptosis of left eye (A) with theglobe pushed down and out. Note the infected ethmoid sinus (B)
Figures 21.3A and B: A case of allergic fungal sinusitis withinvolvement of the anterior and posterior ethmoid sinuses and a hugeorbital extension (B) which is causing a severe eccentric proptosisof the right eye (A)
Figures 21.2A and B: A case of mucormycosis with proptosis andsevere ptosis of right eye. MRI (B) shows the involvement of maxillary,ethmoid and frontal sinuses. Note intracranial and orbital extensions
A B
A B
A B

Multidisciplinary Approach to ProptosisMultidisciplinary Approach to ProptosisMultidisciplinary Approach to ProptosisMultidisciplinary Approach to ProptosisMultidisciplinary Approach to Proptosis 303303303303303
Figures 21.6A to C: Note the pinkish tumor in the right nostril. CT scan shows a hyperdense lesion filling the entireethmoidal sinuses and extending into the right orbit (B and C)
swelling in the bridge of nose, CSF rhinorrhea, signsof raised intracranial involvement. Diagnosis is bybiopsy, and imaging with CT scan and MRI.Treatment includes surgery, radiotherapy and chemo-radiotherapy. Surgery includes lateral rhinotomy andmedial maxillectomy, partial maxillectomy, total andextended maxillectomy and craniofacial dislocation.
Adenoid cystic carcinomaThese arise from minor salivary glands of the nose.These grow very aggressively and have perivascularand perineural spread. Patients die of distantmetastasis. Diagnosis is by biopsy. Treatment includessurgical resection with postoperative radiation.
RhabdomyosarcomaMost common soft tissue tumor of childhood. Patientpresents with proptosis, visual impairment, painlessfacial swelling, nasal obstruction, and epistaxis.Diagnosis is by biopsy, CT scan, bone marrowexamination. Treatment includes radical surgery,radiotherapy and chemotherapy.
Non-Hodgkin's lymphomaThese are commonly seen in elderly males. B-celllymphomas are much more common than T-celllymphomas. The maxillary and ethmoid sinuses aremost commonly involved. Patient presents with nasalobstruction, epistaxis, proptosis, infraorbitalanesthesia, facial swelling. Histopathologicalevaluation, including immunohistochemistry ofbiopsy specimen is diagnostic. If it is plasmacytomathen serum electrophoresis should be done.Treatment includes surgical resection, radiation andchemotherapy.
confirmed by histopathological examination.Treatment is by radiotherapy followed by wide localexcision.
Juvenile nasopharyngeal angiofibroma
It is a highly vascular, benign but biologicallyaggressive tumor originating in the nasopharynxexclusively seen in adolescent males. This tumor hasboth vascular and fibrous elements. Patient presentswith nasal obstruction, epistaxis, facial deformity,proptosis, and headache. Biopsy is contraindicated.Investigations required are CT scan with contrast,and MRI angiogram. Preoperative embolization isuseful. Treatment includes lateral rhinotomy withmedial maxillectomy, transpalatine with or withouttrans- antral approach, mid facial degloving.
Malignant TumorsSquamous cell carcinomaMaxillary sinus is the most commonly involved. It isseen in elderly males. Patients present with nasalobstruction, mass in the nasal cavity, epistaxis, facialswelling, altered facial sensation. If mass involvesethmoids then patient presents with proptosis,
Figures 21.5A and B: Eccentric proptosis of left eye (A) due toangiofibroma. CT scan shows the tumor involving the sinus and thenasal cavity (B)
A B
A B C

304304304304304 Surgical Atlas of Orbital DiseasesSurgical Atlas of Orbital DiseasesSurgical Atlas of Orbital DiseasesSurgical Atlas of Orbital DiseasesSurgical Atlas of Orbital Diseases
EsthesioneuroblastomaAlso known as olfactory neuroblastoma orneuroendocrine tumor, this arises in the upper partof nasal cavity from stem cells of neural crest origin.Patient presents with mass in the nasal cavity,epistaxis, proptosis. It is a slow growing tumor whichmay become large and destructive. Biopsy andusing specific tumor markers is the diagnostictool. Treatment includes surgical resection andradiation.
Various approaches for tumor removal• Caldwell-luc operation• Lateral rhinotomy• Trans palatal approach to remove postnasal
tumors• Intranasal ethmoidectomy• External ethmoidectomy: Lynch-Howarth
procedure• Patterson's operation• Maxillectomy:
— Medial— Partial— Total— Extended
• Craniofacial approach• Functional endoscopic sinus surgery
Caldwell-Luc operation
Incision extends from canine ridge, runs laterally for3.5-4 cm parallel to the teeth.
The soft tissues are incised down to bone.Using a periosteum elevator, the bony anterior
wall of the antrum is exposed.Using a 5 mm Jenkin's gouge, a sliver of anterior
wall is elevated and removed with forceps. The bonyopening is enlarged with Hajek's sphenoidal punchforceps.
The antral mucosa is incised and the contents areexamined.
After surgery the cavity is packed with BIPP.
Jansen-Horgan operationAfter performing the Caldwell-Luc operation theposterior ethmoidal cells are opened through theantrum. This is achieved by pushing a closedTilley-Henckle forceps in an upward, medial andposterior direction at the upper and inner angle ofthe antrum.
The opening is enlarged with suitable punchforceps to allow adequate exenteration of theposterior and middle ethmoid cells. Great care isnecessary in enlarging the opening as it may damagecribriform plate or optic nerve.
Intranasal ethmoidectomy
Under general anesthesia the polypus bearing areaof the nose is exposed and the polypoid masses areremoved with Henckel's forceps. The remainingpieces of polypoid mucosa are removed with Citelli'supturned forceps, which is also used in uncappingthe ethmoidal bulla and for removing every visibletrace of edematous mucosa from the air cells.
External Ethmoidectomy
Lynch-Howarth's operationUnder general anesthesia a slightly curved incision,medial to, and concave towards the medial canthusof the eye is made. The periosteum is elevated to
Figures 21.7A and B: Caldwell-Luc operation Figure 21.8: Jansen-Horgan procedure
A B
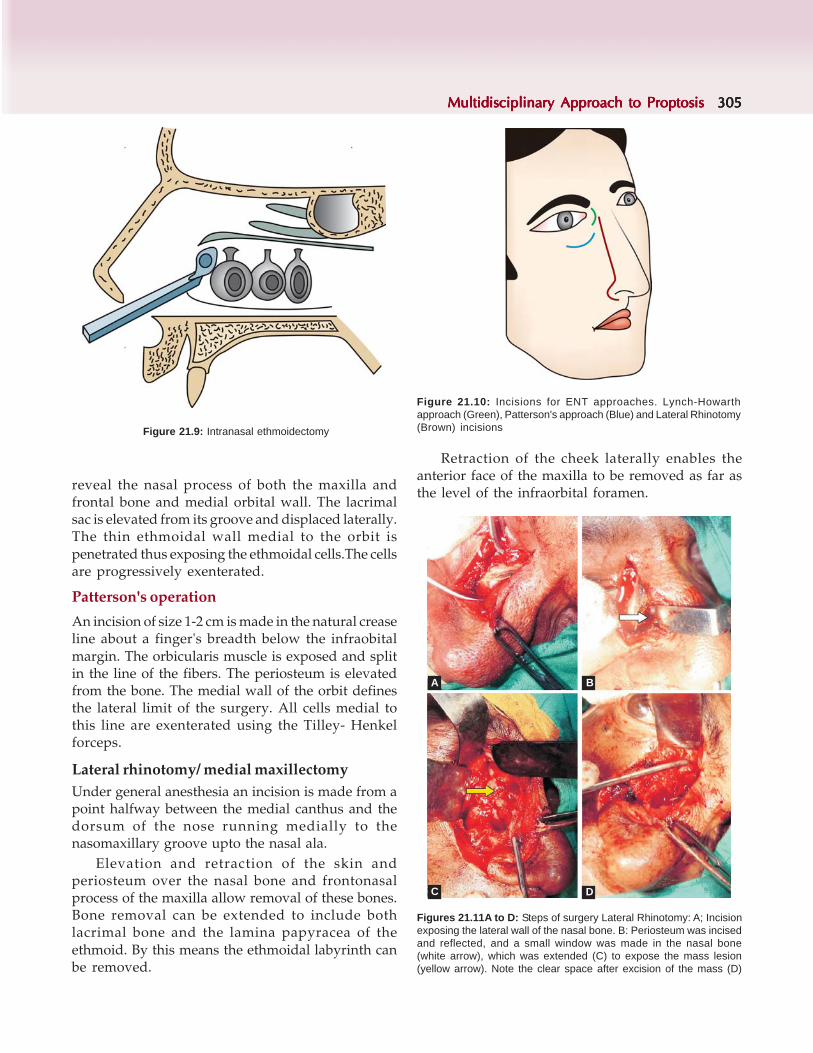
Multidisciplinary Approach to ProptosisMultidisciplinary Approach to ProptosisMultidisciplinary Approach to ProptosisMultidisciplinary Approach to ProptosisMultidisciplinary Approach to Proptosis 305305305305305
reveal the nasal process of both the maxilla andfrontal bone and medial orbital wall. The lacrimalsac is elevated from its groove and displaced laterally.The thin ethmoidal wall medial to the orbit ispenetrated thus exposing the ethmoidal cells.The cellsare progressively exenterated.
Patterson's operation
An incision of size 1-2 cm is made in the natural creaseline about a finger's breadth below the infraobitalmargin. The orbicularis muscle is exposed and splitin the line of the fibers. The periosteum is elevatedfrom the bone. The medial wall of the orbit definesthe lateral limit of the surgery. All cells medial tothis line are exenterated using the Tilley- Henkelforceps.
Lateral rhinotomy/ medial maxillectomyUnder general anesthesia an incision is made from apoint halfway between the medial canthus and thedorsum of the nose running medially to thenasomaxillary groove upto the nasal ala.
Elevation and retraction of the skin andperiosteum over the nasal bone and frontonasalprocess of the maxilla allow removal of these bones.Bone removal can be extended to include bothlacrimal bone and the lamina papyracea of theethmoid. By this means the ethmoidal labyrinth canbe removed.
Retraction of the cheek laterally enables theanterior face of the maxilla to be removed as far asthe level of the infraorbital foramen.
Figure 21.10: Incisions for ENT approaches. Lynch-Howarthapproach (Green), Patterson's approach (Blue) and Lateral Rhinotomy(Brown) incisions Figure 21.9: Intranasal ethmoidectomy
Figures 21.11A to D: Steps of surgery Lateral Rhinotomy: A; Incisionexposing the lateral wall of the nasal bone. B: Periosteum was incisedand reflected, and a small window was made in the nasal bone(white arrow), which was extended (C) to expose the mass lesion(yellow arrow). Note the clear space after excision of the mass (D)
A B
C D

306306306306306 Surgical Atlas of Orbital DiseasesSurgical Atlas of Orbital DiseasesSurgical Atlas of Orbital DiseasesSurgical Atlas of Orbital DiseasesSurgical Atlas of Orbital Diseases
Total Maxillectomy
A Weber-Fergusson skin incision is marked outstarting at the philtrum of the lip and going upto thecolumella. The incision is continued round the marginof the ala of the nose and up, along the lateral wallof the nose to the medial corner of the eye, turninglaterally in a rounded fashion to go 5 mm below thelid margin on the lower lid. The remainder of theincision is intraoral and follows the alveolar buccalsulcus, around the maxillary tuberosity and acrossthe palate at the junction of the soft palate withposterior end of hard palate. The final incision isslightly lateral to the midline to join the originalincision in the region of the upper first incisor tooth.Facial skin is elevated. Clearance of the orbit shouldbe done first. If the orbital contents are left in situthey can be elevated. Then ethmoid labyrinth shouldbe exenterated. The bony orbital floor is divided with
an osteotome. The upper part of the maxilla is freed.Then hard palate is separated from the soft palate.Then the medial and lateral pterygoid plates areremoved to separate the posterior wall of the maxilla.Then the free maxilla bone is separated from themucosal fibers and muscle fibers.
Figures 21.12A and B: The external markings for incision (A), andin the oral cavity for total maxillectomy
Figures 21.13A to D: External marking for the incision (A) intraoral incision made and the cheek flap reflected (B)Anterior wall of the maxilla exposed (C), which was opened and the fungal granuloma excised (D)
A B
A B
C D

Multidisciplinary Approach to ProptosisMultidisciplinary Approach to ProptosisMultidisciplinary Approach to ProptosisMultidisciplinary Approach to ProptosisMultidisciplinary Approach to Proptosis 307307307307307
Craniofacial ApproachPreliminary temporary tarsorraphies are made toprotect the cornea.
The classical lateral rhinotomy incision iscontinued upto forehead either in the midline or in aprominent frown crease. The soft tissues aredissected off the underlying facial bones. Theperiosteum of frontal bone is carefully elevated anddissected laterally. The window craniotomy iscreated. Dura is carefully separated.
Then the dissection is extended to encompassboth ethmoids and the anterior wall of the sphenoidsinus. The specimen is finally freed by dividing theperpendicular plate of the ethmoid. The laminapayracea, anterior wall of the sphenoid and medialantral wall must all be removed.
Trans palatal approach to remove postnasaltumors
Under general anesthesia, a curved incisionbowed forwards is made between the maxillarytuberosities, keeping internal to the greater palatineforamen.
If the operation is performed for the removal ofthe tumor which extends forward into the nasalcavity, the incision should be carried more anteriorly.The incision is deepened through mucosa andperiosteum. The mucosa on the upper surface of thepalate is divided transversely and postnasal space isexamined. Depression of the soft palate with aretractor will give adequate exposure of the postnasalspace.
Figures 21.16A and B: After removing the lateral wall of the nose,the part of the tumor in the nasal cavity and ethmoid sinus wasexcised by the ENT surgeon
Figures 21.14A to C: Incision for cranio-facial approach (A), which is indicated when the lesioninvolves the sinuses, nasal cavity, orbit and the brain as seen in the CT scan images (B and C)
A B C
A B
Figures 21.15A and B: Incisions similar to lateral Rhinotomy, andexposure of the nasal bone
A B

308308308308308 Surgical Atlas of Orbital DiseasesSurgical Atlas of Orbital DiseasesSurgical Atlas of Orbital DiseasesSurgical Atlas of Orbital DiseasesSurgical Atlas of Orbital Diseases
Figures 21.17A to D: The incision is extendedby the neurosurgeon, onto the fore-head andthe horizontal part of it is behind the hair-line.The Frontal bone is exposed (A) Bur-holes aremade (B) and the frontal bone is removed as aflap(C), exposing the dura covering the brain.The frontal sinus was exposed (D)
Figures 21.18A to D: Note the frontal sinuscomponent (yellow arrow) and the intracranialcomponent (white arrow) of the mass (A) Theentire mass could be visualized (green arrow)after removing the overlying bone (B). The masswas excised. The incision was closed inlayers with interrupted sutures (C). Thepreoperative condition with eccentric proptosisis seen in (D)
A B
C D
C D
A B

Multidisciplinary Approach to ProptosisMultidisciplinary Approach to ProptosisMultidisciplinary Approach to ProptosisMultidisciplinary Approach to ProptosisMultidisciplinary Approach to Proptosis 309309309309309
Functional endoscopic sinus surgery( FESS)
During the past decade and half, FESS has becomemore popular and is increasingly used to treat lesionsof the sinuses with orbital extension, and for orbitaldecompression surgeries as in Thyroid AssociatedOrbitopathy. It can also be very safely used forbiopsy, debulking or excising the mass lesion. Theprocedure is safe, gives a very good access to all thesinuses without a surgical scar.
Removal of disease and relevant contact areaswhile conserving normal mucosa without exposingbony margins and preserving normal anatomy tothe extent possible is the advantage, with restorationof ventilation and restoration of mucociliarytransport.
Figure 21.19: Incisions for transpalatal approach
Figures 21.20A and B: Bony ostium is made in the medial wall oforbit and fat is being removed (white arrow A). Note how big a bonyostium can be made in the medial wall of the orbit for decompressionof orbit in thyroid associated orbitopathy
Lateral orbitotomy Kronlein, 1889Rowbotham, 1949Krayenbuhl, 1967Stalard, 1947Berke, 1953Brihaye, 1968Kennerdell & Maroon, 1976
Anterior orbitotomy Knapp, 1847Benedict, 1949
Transethamoidal orbitotomy Niho, 1961Frontal trans-sinusoidal Colohan, 1941Inferior orbitotomy Davis, 1940Transcranial approachesSub frontal Dandy, 1941
Housepain, 1969Frontolateral Naffziger, 1948Frontoorbital Tym, 1961
Birhaye, 1968Jane, 1982
Frontotemporo-orbital Kennerdell & Maroon, 1976Pterional Hamby, 1982
Neurosurgical Approach to Proptosis
The first known craniotomy for an intraorbital tumorproducing proptosis was performed by Durante inRome in 1887.
The choice of various approaches to the orbitrequires that the surgeon has a perfect knowledgeof the orbital pathology and a thorough knowledgeof the diverse surgical approaches as well as theiradvantages, indications, limitations and contra-indications.
Various surgical approaches to the orbit may bedivided into two groups: Extracranial approach andtranscranial approach.
Extracranial approach
Because of its outline, the orbit has five sides,each of which may be used to reach the orbitalcontents.
1. The anterior surgical approach, anteriororbitotomy can be performed through theeyelids or the conjunctiva.
2. The orbitonasal route approach is termed transe-thmoidal orbitotomy.
3. Transmaxillary orbitotomy through the inferiororbital wall.
4. Temporal orbitotomy or external lateralapproach through the temporal fossa.
5. Transcranial or transcranial orbitotomy throughthe superior wall.
A B

310310310310310 Surgical Atlas of Orbital DiseasesSurgical Atlas of Orbital DiseasesSurgical Atlas of Orbital DiseasesSurgical Atlas of Orbital DiseasesSurgical Atlas of Orbital Diseases
The temporal and superior or transfrontalapproaches are of surgical interest in neuro-surgery.
Transcranial approach to the orbit is the mostcomplex and demanding route.
Indications
• Cranio-orbital disease• Sphenoid wing or anterior fossa meningiomas with
orbital extension• Fronto-orbital fibrous dysplasia• Chondroma• Chondrosarcoma• Epidermoid cyst• Osteoma• Aneurysmal bone cyst• Primary intraorbital tumors-those arising in the
orbital apex or in the superointernal quadrant ofthe orbit.
• Optic nerve sheath meningiomas• Optic nerve glioma• Neurinoma• Intraconal cavernous hemangioma• Inflammatory pseudotumors• Perioptic metastases• Vascular malformations• Lymphangioma
In addition, two wall transcranial decompressionand extended pterional orbital decompression hasbeen tried in the management of gravesophthalmopathy.
Supraorbital Craniotomy
Under general anesthesiaSupine position with head slightly extended to allowseparation of the frontal lobe from the orbital roofby the gravity. The sagittal axis of the skull is rotated10° toward the contralateral side.
Incision-hemicoronal or bicoronal skin incisionA cutaneous flap is raised and dissected from thepericranium and from the temporal muscleaponeurosis, including the superior branch of thefacial nerve in the folded planes.
The most anterior portion of the temporal muscleis dissected and the burr hole is made in the temporal
fossa behind the zygomatic process of the frontalbone, exposing the dura of the anterior fossa in itsupper portion and the periorbita in its lower portionboth separated by the orbital roof.
A second opening is made immediately abovethe orbital rim in the superointernal angle outsidethe glabella. Standard precautions are requiredbecause of presence of frontal sinus. Both openingsmay be connected with the craniotome, otherwise,third frontal burr hole is made equidistant from thefirst two and approximately 4 to 5 cm from the orbitalroof. From the lateral burr hole a Gigli saw is passedtoward the lateral rim which is then sectioned. Fromthis same opening the duramater and the periorbitaare protected with small spatulas the orbital roof issectioned with the chisel directed toward the midline.From the medial frontal opening the superior orbitalrim and the orbital roof was sectioned with the chiseldirected laterally and posteriorly toward theosteotomy previously performed. The frontal boneflap is then easily raised together with the superiororbital rim and the anterior and wider sector of theorbital roof, exposing the frontal duramater andperiorbita.
It is necessary to complete bone resection of theorbital roof and the upper margin of the optic canalin apical tumors.
The surgical microscope and self retainingretractors are placed with only minimal frontaldisplacement. An anteroposterior incision is mademedially to the levator palpebraris muscle in theperiorbita. Next, the inner and superior rectusmuscles are explored by microsurgical technique untilthe optic nerve is located. This method carries theleast risk of causing irreversible ophthalmoplegia.
In optic nerve gliomas, the nerve is oftenextremely thickened in its distended meningealcoverings, showing regular contours. In these casesthe lesion is dissected laterally, the anterior portionfrom behind the eyeball and the posterior one at thelevel of the annulus of Zinn, followed by opening ofthe frontobasal dura to explore the optic nerve alongits intracranial course. The nerve is then resectedfrom the prechiasmatic level toward the optic canal,including the foraminal portion.
In sheath meningiomas presenting as diffusethickening the dural sheath may be opened anteroposteriorly and the tumor may be dissected jointly

Multidisciplinary Approach to ProptosisMultidisciplinary Approach to ProptosisMultidisciplinary Approach to ProptosisMultidisciplinary Approach to ProptosisMultidisciplinary Approach to Proptosis 311311311311311
with the invaded sheath by following thesubarachnoid space. In few cases particularly inlesions located anteriorly sight preservation isachieved provided that careful dissection is carriedout and vascularization is spared in the nerve andretina. When the tumoral mass is large and notclearly restricted to the nerve course, exhibits micronodular infiltration of the muscles at the apex, theeye is most likely amaurotic.Thus it is advisable toresect this type of mass with the nerve. In such casesit is essential to perform intracranial exploration ofthe optic nerve which may be surrounded by thetumor extending through the optic canal.
In neurinomas and cavernous hemangiomas,once the lesion has been located and may be removedin toto because of attachment to critical structures isunusual. In rare cases of hour glass neurinomasextending toward the middle cranial fossa combinedintracranial and intraorbital procedure is required.
Transcranial approach with resection of theorbital roof
Tumors invading or arising from the orbital roofdemand a technique different from the one used forpurely intraorbital lesions.
Frontal or frontotemporal craniotomy is doneaccording to the lesion extension. When markedhyperostosis is present, the procedure begins withgradual resection of the pathological bone withburrs, drills and gouges. It is often necessary tocontinue bone resection toward the roof and lateralorbital wall leaving the orbital contents amplyexposed. In purely osseous lesions this stage
ends with total removal of the lesion.The final stepis to perform plastic reconstruction of the resecteddura with pericranium.The roof and the lateral wallof the orbit is reconstructed with methyl-methacrylate.
Summary
The choice of the most suitable surgical approach fororbital tumors is made on the basis of tumor location,size, and apparant site of origin, propagation routeand probable histological type.
Superior orbitotomy is indicated in fronto-ethmoidal mucoceles, dermoid cyst and lacrimalgland tumors.
Lateral orbitotomy is indicated in cavernoushemangiomas, neurinomas, inflammatory pseudotumors and metastasis.
Inferior orbitotomy is less frequently usedapproach in rare lesions such as lymphomas andmetastasis.
Transantral approach is indicated for tumorsoriginating from ethmoid cells and maxillary sinus.Larger lesions require extended approaches forexample superolateral and inferolateral according totumor topography and used for large hydatid cystor huge cavernous hemangiomas.
Transcranial approach is indicated for cranioorbital meningiomas of the sphenoid wing, and withanterior cranial fossa disease with orbital extension.The transcranial route is the only one that allowsdecompression of the optic canal and intracranialexploration of the optic nerve along its prechiasmaticcourse.
Figures 21.21A and B: Axial proptosis of right eye in a male of 35 years (A) due to Schwannoma. Note that the well defined tumor ispartly in the orbit and partly in the brain (arrow) as it is extending through superior orbital fissure
A B
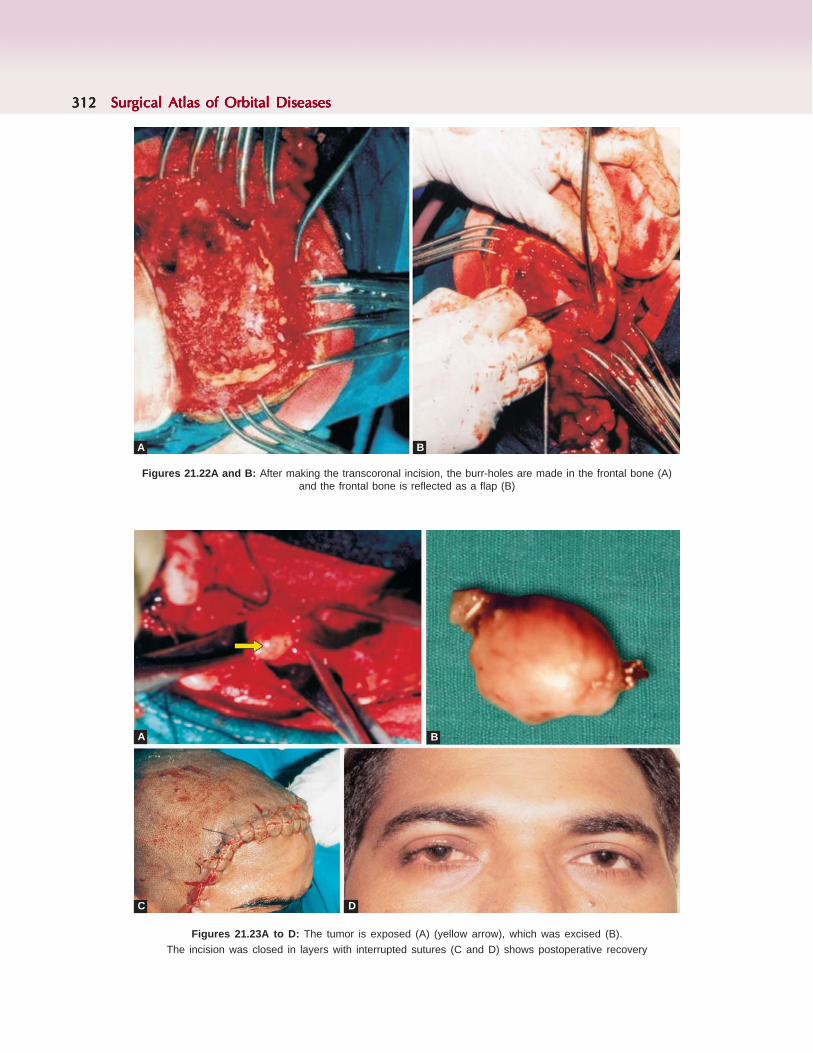
312312312312312 Surgical Atlas of Orbital DiseasesSurgical Atlas of Orbital DiseasesSurgical Atlas of Orbital DiseasesSurgical Atlas of Orbital DiseasesSurgical Atlas of Orbital Diseases
Figures 21.22A and B: After making the transcoronal incision, the burr-holes are made in the frontal bone (A)and the frontal bone is reflected as a flap (B)
Figures 21.23A to D: The tumor is exposed (A) (yellow arrow), which was excised (B).The incision was closed in layers with interrupted sutures (C and D) shows postoperative recovery
A B
A B
C D

Multidisciplinary Approach to ProptosisMultidisciplinary Approach to ProptosisMultidisciplinary Approach to ProptosisMultidisciplinary Approach to ProptosisMultidisciplinary Approach to Proptosis 313313313313313
CASE ILLUSTRATIONS
Case 1Female 48 years (Figure 21.24A) presented witheccentric proptosis of 2 years duration, and defectivevision since 2 months. She gives history of recurrentepisodes of sinusitis. On examination, she hadeccentric proptosis of left eye with the globe pushedup (6 mm), outwards (7 mm) and forwards by7 mm.The ocular motility was restricted mildly in alldirections. Pupil showed RAPD, and her BCVA was20/60 and color vision was 6/17. Fullness of leftcheek was noted. CT scan of orbit (Figures 21.24B
Figure 21.24A to C: Note the eccentric proptosis of left eye with fullness of left cheek. CT scan of orbit (B and C) showed a large, hyperdenselesion filling entire maxillary sinus (yellow arrow) with orbital extension (green arrow) and extension in front of maxilla into cheek (red arrow).Note how the optic nerve (white arrow) was pushed by the mass
and C) showed a large, hyperdense lesion fillingentire maxillary sinus, with orbital extension.Extension in front of maxilla into cheek was found.The optic nerve was pushed by the mass. In view ofrecurrent sinusitis, involvement of the sinuses, fungalgranuloma was the clinical diagnosis. The lesion wasdebulked through a modified lateral rhinotomyincision, along with my ENT colleague. The orbitalcomponent was debulked through the horizontalincision, exposing the floor of the orbit. She receivedamphotericin-B for the fungal granuloma. Her visionimproved to 20/30, and there was no recurrence inthe past 4 years.
Figures 21.25A to C: The lesion in front of the maxilla was exposed (white arrow A) and excised through a modified lateral rhinotomy incision.Then the anterior wall of maxilla was opened, the mass was exposed (yellow arrow B) and removed. The orbital component was debulkedthrough the horizontal incision, exposing the floor of the orbit. At the end of the surgery (C) note the concavity in the cheek due to excision ofthe mass in the cheek
A B C
A B C

314314314314314 Surgical Atlas of Orbital DiseasesSurgical Atlas of Orbital DiseasesSurgical Atlas of Orbital DiseasesSurgical Atlas of Orbital DiseasesSurgical Atlas of Orbital Diseases
Case 2Female of 16 years presented with eccentric proptosisof left eye since 1 year and blurring of vision since1 month. She was an agricultural worker. She had aneccentric proptosis of left eye with the eyeball pushedup and out (Figure 21.26A). Ocular motility wasrestricted in elevation and abduction pupil showedRAPD in the left eye. Her BCVA was 20/40. CT scan(Figures 21.26B and C) showed a mass lesion of the
maxillary and ethmoid sinuses, with bony destructionand orbital extension. Since most of the orbital floorwas destroyed, we planned for a swinging lowereyelid approach, which gives adequate exposure tothe floor of orbit (Figure 21.27A) and the mass wasdebulked (B). Postoperative recovery was good (C).However there was significant enophthalmos. Sheimproved with antifungal drugs and there was norecurrence during 3 years follow-up.
Figures 21.26A to C: This female of 16 years presented with eccentric proptosis of left eye since 1 year and blurring of vision since1 month.Left eye was pushed up and out (A). CT scan showed a mass lesion of the maxillary and ethmoid sinuses, with bony destruction and orbitalextension (B and C)
Figures 21.27A to C: Swinging lower eyelid approach, which gives adequate exposure to the floor of orbit (roof of maxilla A) and themass was debulked (B). Postoperative recovery was good. Note the minimal scar (C)
A B C
A B C
Case 3
A 22 years male presented with complaints of leftsided nasal obstruction since 5 months, bleeding fromthe left nasal cavity since 4 months, swelling overthe left cheek since 3 months and protrusion of theleft eye since 3 months. On anterior rhinoscopicexamination a pinkish mass was seen in the left nasalcavity extending into the posterior choana which wasobserved in the posterior rhinoscopy. There was a
proptosis of the left eye (Figure 21.28A). Ocularmovements and vision were normal. CT scan showeda space occupying lesion arising in the left maxillarysinus which is extending into the nasal fossa causingdisplacement of inferior and medial walls of the orbits/o neoplasm (Figure 21.28B). The mass was excisedthrough the Moure's lateral rhinotomy approach.Histopathology showed it to be nasopharyngealangiofibroma (Figure 21.28C and D).

Multidisciplinary Approach to ProptosisMultidisciplinary Approach to ProptosisMultidisciplinary Approach to ProptosisMultidisciplinary Approach to ProptosisMultidisciplinary Approach to Proptosis 315315315315315
Figures 21.28A and B: Eccentric proptosis of left eye with the globepushed up. Note the fullness below the lower eyelid (A) CT scan (B)shows a hyperdense mass with contrast enhancement, involving themaxillary sinus, extending into the nasal cavity. Note the bonyexpansion of the sinus, leading to proptosis
Figures 21.28C and D: Histopathology showing a picture of vascularspaces with less stroma of fibrous tissue (C) suggestive of Angio-fibroma (D) shows postoperative picture with recovery from proptosis
Figures 21.29A and B: Eccentric proptosis of right eye (A) with theglobe pushed laterally and down. Note the fullness of superior sulcus.CT scan (B) shows a large, heterogenous lesion involving the ethmoidsinuses, with bony expansion
Case 4
Boy of 2 years was brought with complaints of rightsided nasal obstruction since 2 months, protrusionof the right eye since 1 month and watering of theright eye since 1 month (Figure 21.29A). On anteriorrhinoscopic examination a grayish mass was seen inthe right nasal cavity. Right eye was proptosed.Ocular movements were normal. CT scan (Figure21.29B) revealed a well defined, non enhancing lesionin the right anterior ethmoidal air cells with centralhyperdense component causing expansion of adjacent
A B
C D
A B
bony structures and proptosis of the right eye. Themass was excised through medial orbitotomyapproach and the mass was sent for HPE whichshowed infected granuloma (Figures 21.30A and B).
Case 5
Male 15 years, presented with complaints of left sidednasal obstruction since 5 months and protrusion ofthe left eye since 3 months (Figure 21.31A). Onanterior rhinoscopic examination a grayish whitemass was seen in the left nasal cavity. There waseccentric proptosis of the left eye. Ocular movementsand visual acuity were normal. CT scan showed alarge well defined soft tissue lesion seen in the regionof the ethmoidal air cells on the left side extendinginto left nasal cavity and sphenoid sinus. The lesionwas surrounded by thick irregular sclerotic bonymargins and there was expansion of the bony outlinesinto the left orbit causing proptosis, suggestive offibrous dysplasia. In view of his symptoms andcosmetic considerations, the mass was excisedthrough external ethmoidectomy approach.Histopathology confirmed the diagnosis of fibrousdysplasia (Figures 21.32A and B).
Figures 21.30A and B: Excised mass (A) and the earlypostoperative recovery (B)
Figures 21.31A and B: Note the eccentric proptosis with the globepushed outwards (A) CT scan revealed an expansile lesion of theethmoid bone (B) with sclerotic margins, heterogenisity and cysticspaces within, suggestive of fibrous dysplasia
A B
A B

316316316316316 Surgical Atlas of Orbital DiseasesSurgical Atlas of Orbital DiseasesSurgical Atlas of Orbital DiseasesSurgical Atlas of Orbital DiseasesSurgical Atlas of Orbital Diseases
Case 6
Female 34 years, presented with proptosis of righteye of 6 months duration, and defective vision since1 month. She had axial proptosis of 5 mm and
downward displacement by 4 mm (Figure 21.33A).RAPD was observed. Her BCVA was 20/30 in righteye. The past history was significant in that she hadconvulsions 2 years back, and was usinganticonvulsants since then CT scan of the orbitrevealed an intraconal, heterogenous, apical masswith very distinct margins (Figures 21.33B and C).The CT scan of brain (Figures 21.34A to C) showedcalcified lesions without any surrounding edema inthe frontal and occipital cortex. The possibility ofhemangioblastoma was considered. Fundusexamination was normal. In view of the apicallocation, a transcranial approach (A) was performed(Figures 21.35A and B). Histopathology confirmedit to be hemangioblastoma. There was no recurrencein the 2 years follow-up.
Figures 21.32A and B: Microphotography showing well demarcatedislands of cartilage with interwoven fibro-osseous tissue, suggestiveof fibrous dysplasia (A) The early postoperative recovery withimprovement in proptosis is evident (B)
Figures 21.33A to C: Female 34 years, with proptosis of right eye of 6 months duration, and defective vision since 1 month. She had axialproptosis of 5 mm and downward displacement by 4 mm (A). CT scan of the orbit revealed an intraconal, heterogenous, apical mass with verydistinct margins (B and C)
A B
A
B C

Multidisciplinary Approach to ProptosisMultidisciplinary Approach to ProptosisMultidisciplinary Approach to ProptosisMultidisciplinary Approach to ProptosisMultidisciplinary Approach to Proptosis 317317317317317
Figures 21.34A to C: The CT scan of brain showed calcified lesions without any surrounding edema in the frontal and occipital cortex
Figures 21.35A and B: In view of the apical location, a transcranialapproach (A) was performed. Histopathology confirmed it to behemangioblastoma. Postoperative figure (B) showing completerecovery
BIBLIOGRAPHY
1. Atallah N (1981) osteomas of the paranasal sinuses, journalof laryngology and otology.
2. Balasingam V, Noguchi A, McMenomey SO, Delashaw JBJr Modified osteoplastic orbitozygomatic craniotomy.Technical note J Neurosurg. 2005;102(5):940-4.
3. Bordley, JE nad Bosley, mucoceles of the frontal sinus,annals of otology, rhinology and laryngology.
4. Canalis RL, ethmoidal mucocele. Archives of otolary-ngology.
5. Cheesman AD Lund, Cranio facial resection for tumors ofnasal cavity and paranasal sinuses.
6. Doxanas MT Clinical Orbital Anatomy.7. Eichel the intranasal ethmoidectomy procedures.8. Fearon BEdwards orbital- facial complications of sinusitis
in children.9. Freedman HM (1979) complications of intranasal
ethmoidectomy.10. Fu JD, Zhao JW, Yin DL, Liu HC, Qiu E, Zhang JL, Zhang
TM. Surgical treatment of fibrous dysplasia of the skullwith neuro-navagation .Zhonghua Yi Xue Za Zhi.2004;17;84(10):808-12. Chinese.
11. Goisis M, Biglioli F, Guareschi M, Frigerio A, Mortini PFibrous dysplasia of the orbital region: current clinicalperspectives in ophthalmology and cranio-maxillofacialsurgery. Ophthal Plast Reconstr Surg. 2006;22(5):383-7.
A B C
A B
12. Harrison DFN (1971) surgical anatomy of maxillary andethmoid sinuses.
13. Harrison DFN (1980) The ENT surgeon looks at the orbit,journal of laryngology and otology.
14. Harrison DFN (1981) Surgical approach to the medial orbitalwall. Annals of otology,rhinology and laryngology.
15. Harrison DFN (1987) juvenile angiofibroma, archives ofotolaryngology-head and neck surgery.
16. Hejazi N, Hassler W, Offner F, Schuster A. Cavernousmalformations of the orbit: a distinct entity? A review ofown experiences. Neurosurg Rev. 2007;30(1):50-4;discussion 54-5. Epub 2006.
17. Howard and Lund, the midfacial degloving approach tosinonasal disease, journal of laryngology and otology.
18. Howard, DJ Lund reflections on the management ofadenoid cystic carcinoma of nasal cavity and paranasalsinuses. Otolaryngology 93.
19. Hubert (1937) orbital infections due to nasal sinusitis, NewYork journal of medicine37.
20. Korinth MC, Ince A, Banghard W, Gilsbach JM. Follow-upof extended pterional orbital decompression in severeGraves’ ophthalmopathy. Acta Neurochir (Wien).2002;144(2):113-20; discussion 120.
21. Linnet J, Hegedus L, Bjerre PK. Neurosurgical treatmentof patients with severe thyroid-associated ophtha-lmopathy. Transcranial two-wall orbital decompressionUgeskr Laeger. 2002;6;164(19):2505-8. Danis
22. Lloyd(1988) Diagnostic imaging of nose and paranasalsinuses.
23. Lund, tomors of paranasal cavities, Oto-Rhino-Laryngology45.
24. Natvig K and Larsen, mucoceles of paranasal sinuses,Journal of Laryngolog and Otology.
25. Reisch R, Perneczky A. Ten-year experience with thesupraorbital subfrontal approach through an eyebrow skinincision. Neurosurgery. 2005;57(4 Suppl):242-55; discussion242-55.
26. Rontal (1979) Surgical anatomy of the orbit, annals ofOtology, Rhinology and Laryngology 88.
27. Schramm, Orbital complications of sinusitis, Otolary-ngology, 86.
28. Zizmor(1968) cysts and benign tumors of the paranasalsinuses,, seminars in Roentgenology.3

318318318318318 Surgical Atlas of Orbital DiseasesSurgical Atlas of Orbital DiseasesSurgical Atlas of Orbital DiseasesSurgical Atlas of Orbital DiseasesSurgical Atlas of Orbital Diseases
Ramesh Murthy, Anirban Bhaduri, Sima Das, Santosh G Honavar
Orbital ExenterationOrbital ExenterationOrbital ExenterationOrbital ExenterationOrbital Exenteration
Exenteration refers to removal of the eyeball alongwith the orbital contents. This disfiguring anddestructive procedure is reserved for the treatmentof life-threatening conditions where otherapproaches have failed.
The first mention of orbital exenteration was400 years ago by Bartische in his treatise on eyediseases.1 He described partial exenteration.Extensive orbital exenteration was describedby Golovine, Nowikoff and Filatov in the early1900s.2
Indications
We usually perform this procedure in the followingsituations.
1. Malignanciesa. Primary orbital lesions like extensive
adenoid cystic carcinoma of the lacrimalgland
b. Intraocular lesions like orbital extension ofretinoblastoma, choroidal melanoma
c. Orbital extension of periocular malignanciesi. Carcinoma of the paranasal sinuses
ii. Eyelid tumorsiii. Skin malignancies
2. Infections like sino-orbital mucormycosis andother fungal infections.
3. Relative indicationsa. Severe orbital contracture with inability to
wear a prosthesisb. Neurofibromatosis with orbital deformity
c. Orbital meningioma and lymphangiomacausing disfiguring proptosis
d. Recalcitrant orbital inflammations unres-ponsive to other treatment modalities
Patient PreparationThe patient needs to understand the need for such adestructive surgery and the gross disfigurementcaused by the procedure. We also counsel our patientsextensively that their facial appearance can never berestored to what it was before. However, an orbitalprosthesis can restore appearance to an acceptableextent, although it will never provide eyelid or ocularmotility. Psychological help is sometimes sought whenwe feel that the patient may not be able to withstandthe consequences of the surgery.
Surgical ProcedureWe always perform the procedure under generalanesthesia. In the rare situation when this is notpossible, local anesthesia can also be used with 2%lignocaine with 1:200,000 adrenaline given as aretrobulbar injection and followed by injectionsaround the orbital rim and in addition withinfraorbital, nasociliary and frontal nerve blocks. Forevery patient we have a pint of blood ready fortransfusion if required. In addition hypotensiveanesthesia is used for all the cases. We also ensurethat the cauteries are working well and have sufficientgauze on table to control bleeding.
The skin is marked all around with a methyleneblue marker. A 4-0 silk suture is passed through theeyelid skin and orbicularis to exit from the tarsal
22C H A P T E R

Orbital ExenterationOrbital ExenterationOrbital ExenterationOrbital ExenterationOrbital Exenteration 319319319319319
plate at the lid margin and then passed similarlythrough the tarsal plate and skin and tied to securethe lids together. This suture is left long to providetraction during the procedure.
A lid sparing exenteration is less disfiguring thana total exenteration. In such a case we make theincision a short distance away from the lid margin.If however there is involvement of the lid, the incisionis made just inside the orbital rim. The skin incisionis made with a 11 no. Bard Parker knife, startinginferiorly and progressing laterally, superiorly andmedially. The superonasal quadrant is approachedlast as it bleeds extensively. If the lid skin is beingspared, it is dissected along with orbicularis to reachthe periosteum of the orbital rim. Once the lid skinis cut, the underlying tissues can then be cut with amonopolar cautery.
The periosteum is cut 6 millimetres or so fromthe orbital rim and then elevated using a periostealelevator. The sharp end of the periosteal elevator isused to separate it from the orbital rim and the bluntend for the intraorbital portion. The attachments inthe region of the medial and lateral canthal tendonand the trochlea are lifted off from the underlyingbone. The neurovascular bundle entering throughthe infraorbital and supraorbital foramen is usuallycauterised before cutting it. We separate the
periorbita from the bone superiorly, laterally andinferiorly first using the blunt end of the periostealelevator or a lens spatula. The periorbita is firmlyattached to the bone near the orbital rim and looselywithin the bony orbit. Medially the lacrimal sac iselevated and cut near the nasolacrimal duct.Occasionally if there is a suspicion of tumor spreadthrough the nasolacrimal duct we remove bone inthat region using the Kerrison's rongeur. In cases oftumors where there is bone involvement, we removeall the involved bone. If such a step is pre-empted,then occasional help from a neurosurgeon for tumorsextending superiorly and sometimes our ENTcolleague especially for sino-orbital mucormycosisis sought.
Once we reach the orbital apex, we are wary ofthe vessels that might bleed before we finally removeall the contents of the orbit. We clamp the tissuesnear the apex with a curved artery forceps beforecutting the apical stump. For visualization, we use alid spatula to push the contents to one side. Bleedingcan be a problem and we use a strong cautery tostem it. Bone wax is needed for the occasionalrecalcitrant bleeder. We wait for the blood pressureto return to normal before we close the lid skin (ifperforming a lid sparing exenteration). We useabsorbable 6-0 vicryl for the underlying tissues and
Types
Type Contents removed Contents preserved Final appearance Complications
Anterior exenteration/ Globe, posterior lamella of Periorbita, posterior Shallow socket, • Delayed healingextended enucleation eyelid, conjunctival sac orbital contents immobile eyelids present • Immobile ill fitted prosthesis
Lid sparing exenteration/ Orbital contents including Anterior lamina of theSubtotal exenteration periosteum of orbital walls eyelid including skin and Deep orbit. Residual skin • Hematoma behind the skin
Eyelid margins some orbicularis muscle and orbicularis edges flapssutured together forming • Necrosis of skin flapsa smooth lining
Total exenteration/ Orbital contents, Bare orbital bones with Spectacle mounted prost- • Sino-orbital fistulaEyelid sacrificing periorbita and lids or without a skin graft hesis can be fitted after • CSF leak
the healing is complete • Hematoma formation.• Keratinization of the skin
graft causing a malodoroussocket
• Infection
Radical exenteration Dissection involves Frontal bone replaced, Cavity can be filled with • Exposure of intracranialparanasal sinuses, cavity covered with myocutaneous vascular contents and associatedface, jaw, palate, myocutaneous vascular flaps or a maxillofacial complicationsskull base. flap with vascular prosthesis can be used • Poor cosmesis
anastomosis to close the palatal defectalong with split skin graft.

320320320320320 Surgical Atlas of Orbital DiseasesSurgical Atlas of Orbital DiseasesSurgical Atlas of Orbital DiseasesSurgical Atlas of Orbital DiseasesSurgical Atlas of Orbital Diseases
6-0 prolene continuous suture for the skin. If the lidskin has been removed, the socket is packed withBetadine soaked gauze.
We give the patient systemic antibiotics and anti-inflammatory medication and give a pressure patchfor 2 days. On the third day following surgery weremove the patch and perform daily aspiration ofthe contents ( in lid sparing) or cleaning and packingin total exenteration.
Management of the Exenterated SocketIt is important to note that the primary objective ofexenteration is to remove all disease. Even afterexenteration, the patient needs to be monitoredcarefully clinically or by imaging for any recurrence.
Spontaneous GranulationThis has to be performed when the surgical excisionhas been radical and the lid skin excised. In thesecases we leave the remaining skin to line the socketand pack the socket with gauze soaked in Betadineas a pressure pack and for about 2 weeks with regularchanging of dressings in the hospital, or by the patientat home. The entire socket is allowed to heal bygranulation. Of course the advantage of this is thefact that any recurrent disease can be identified easily.However the healing is a slow process.
Skin GraftingPartial thickness skin grafts have been in vogue for along time since they were popularized by Wheeler.4
Using a dermatome, skin is harvested from a nonhair bearing area such as the inner thigh andabdomen. The graft is then fitted to the exenterationcavity, trimmed and sutured using 6-0 prolenesutures. Slits are made to facilitate drainage andprevent collection of fluid underneath. Healingusually takes 6 weeks, following which the patient isfitted with prosthesis.5
Skin FlapsThis is my preferred technique where the lid skin isspared and used to close the cavity. Postsurgerypressure patch is placed and aspiration of the socketis performed daily for a week to remove anycollection of fluid. Once the healing is complete, asmooth surface is achieved over which prosthesis canbe placed easily.
Myocutaneous Flaps
Other techniques like temporalis muscle trans-position, forehead, cheek, pectoralis flaps have alsobeen described.6-9
Prosthesis
Exenteration prosthesis is our preferred techniqueof managing the cosmetic issues followingexenteration, which is discussed as a separate chapterin the book.
Complications of Exenteration
Bleeding can be life threatening especially during thesurgery and adequate support from the anestheticteam is a must. In addition blood for transfusionshould be available. One should have a good cauterymachine.
Socket infection can occur and needs to bemanaged by systemic and local antibiotics. Any gapein the sutured wound should be closed if possible orin the presence of infection should be allowed togranulate spontaneously.
Recurrence of the primary disease can occur andhence monitoring at regular intervals postsurgery isessential.
CASE ILLUSTRATIONS
Case 1
A 51-year-old female presented with pain andswelling of the left eye for 15 days. She had a historyof gradual loss of vision in the left eye for 2 yearsfollowed by gradual protrusion of that eye for 1 year.On examination, there was proptosis of the left eye,with swelling of the lids and ptosis (Figure 22.1A).On lifting the ptotic lid, a brown, firm perilimbalnodule was seen next to an opaque cornea (Figure22.1B). There was complete restriction of eyemovements. CT scan of the orbit showed a soft tissuemass filling the orbit almost upto the apex (Figures22.1C and D). The globe contour was distorted andno normal orbital structures were recognizable. Adiagnosis of uveal melanoma with secondary orbitalextension was made. There was no lymphadenopathyin the head and neck region. Systemic workup wasdone which did not reveal any systemic metastasis.
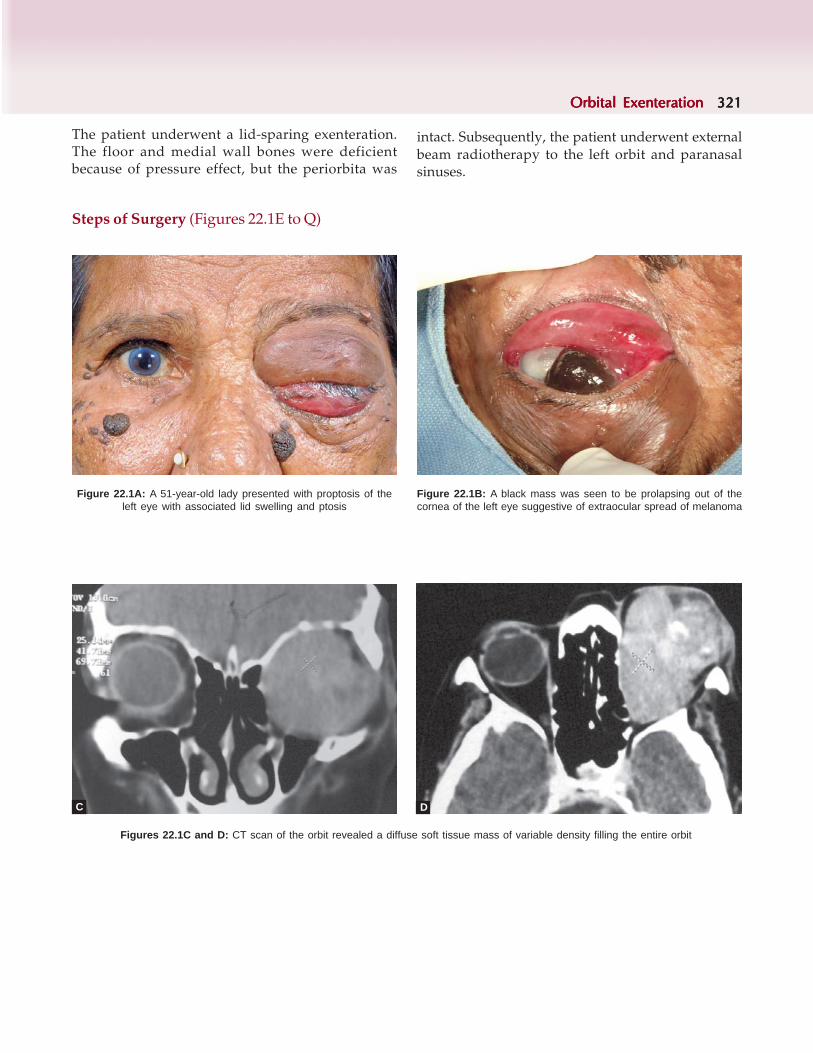
Orbital ExenterationOrbital ExenterationOrbital ExenterationOrbital ExenterationOrbital Exenteration 321321321321321
Figures 22.1C and D: CT scan of the orbit revealed a diffuse soft tissue mass of variable density filling the entire orbit
The patient underwent a lid-sparing exenteration.The floor and medial wall bones were deficientbecause of pressure effect, but the periorbita was
intact. Subsequently, the patient underwent externalbeam radiotherapy to the left orbit and paranasalsinuses.
C D
Steps of Surgery (Figures 22.1E to Q)
Figure 22.1B: A black mass was seen to be prolapsing out of thecornea of the left eye suggestive of extraocular spread of melanoma
Figure 22.1A: A 51-year-old lady presented with proptosis of theleft eye with associated lid swelling and ptosis

322322322322322 Surgical Atlas of Orbital DiseasesSurgical Atlas of Orbital DiseasesSurgical Atlas of Orbital DiseasesSurgical Atlas of Orbital DiseasesSurgical Atlas of Orbital Diseases
Figure 22.1E: The skin was marked on both the upper and lowerlids to identify the site of incision
Figure 22.1F: A rolled up wet cotton gauze was placed over theconjunctiva. A 4-0 silk suture is passed through the eyelid skin andorbicularis to exit from the tarsal plate at the lid margin and thenpassed similarly through the tarsal plate and skin and tied to securethe lids together
Figure 22.1G: 3 such sutures are passed and the ends kept longfor traction during the procedure
Figure 22.1H: The skin incision is made with a 11 no. Bard Parkerknife, starting inferiorly and progressing laterally, superiorly and medially
Figure 22.1I: In a lid sparing exenteration, the skin incision is madea short distance away from the lid margin
Figure 22.1J: The underlying tissues are retracted and cut with aradiofrequency monopolar cautery

Orbital ExenterationOrbital ExenterationOrbital ExenterationOrbital ExenterationOrbital Exenteration 323323323323323
Figure 22.1K: The skin and subcutaneous tissues are incised up tothe level of the periosteum
Figure 22.1M: The periorbita is separated from the bone superiorly,laterally and inferiorly first using the blunt end of the periosteal elevatoror a lens spatula. The periorbita is firmly attached to the bone near theorbital rim and loosely within the bony orbit. Medially the lacrimal sacis elevated and cut near the nasolacrimal duct
Figure 22.1N: Near the orbital apex, the tissues are clamped with acurved artery forceps before cutting the apical stump
Figure 22.1O: The exenterated contents are dark brown in colorsuggestive of a melanoma
Figure 22.1P: 6/0 vicryl sutures are used to suture thesubcutaneous tissue once hemostasis has been achieved
Figure 22.1L: The periosteum is cut about 6 mm from the orbital rimand elevated using the periosteal elevator

324324324324324 Surgical Atlas of Orbital DiseasesSurgical Atlas of Orbital DiseasesSurgical Atlas of Orbital DiseasesSurgical Atlas of Orbital DiseasesSurgical Atlas of Orbital Diseases
Figure 22.1Q: The skin is closed with 6/0 prolene Figure 22.2A: A 40-year-old male presented to us with progres-sive proptosis of the left eye of 4 months duration
Figures 22.2B and C: CT scan revealed the presence of a fairly welldefined uniformly isodense intraconal mass between the medial rectusand optic nerve
Case 2
A 40-year-old male presented to us with eccentricprotrusion (outward and lateral displacement) of theleft eye which was gradually increasing for last 4months (Figure 22.2A). A non-tender mass, firm tohard in consistency was palpable deep in the superiorand nasal part of left orbit. There was no apparentnasal or paranasal sinus pathology. On presentation,he had best corrected visual acuity of 6/7.5 and 6/12in right and left eyes respectively. Ocular movementsin the left eye were grossly restricted; adductionmore than abduction. Anterior segment examinationwas unremarkable in both eyes. Fundus in the righteye was normal and in the left eye showed presenceof early disc edema. The patient was non-diabeticand non-hypertensive. Ultrasound B scan of the lefteye revealed diffuse thickening of medial rectus withmaximum diameter being 14.3 mm. CT scan showedpresence of a fairly well defined, uniformly isodense,intraconal mass located between medial rectus andoptic nerve. Medial rectus could not be appreciatedseparately from the mass posteriorly (Figures 22.2Band C). An excision biopsy by a lid split medialorbitotomy approach was done. Postoperatively hisproptosis was reduced but the vision in left eye wasreduced to PL with inaccurate projection of rays, andhe had grade 1 relative afferent pupillary defect.
Histopathology of the biopsy specimen showedpresence of giant cells and elongated budding fungalfilaments. Microbiological evaluation confirmed adiagnosis of aspergillosis.
C
B

Orbital ExenterationOrbital ExenterationOrbital ExenterationOrbital ExenterationOrbital Exenteration 325325325325325
Figure 22.2D: 4 months later the patient came back with exacerbationof proptosis and a firm palpable mass in the medial canthal region
4 months later the patient came back withexacerbation of proptosis with a firm mass palpablein the medial canthal region (Figure 22.2D).Exophthalmometry readings were 19 and 30 mm inthe right and left eye respectively. He had no visionin the left eye at this visit. CT scan showed a solidmass, which was filling almost the entire orbitalcavity; extraocular muscles could not be made outseparately from the mass (Figures 22.2E and F). Themass could be seen extending up to the superiororbital fissure. Lateral wall of orbit showedexcavation of bone. Contiguous middle cranial fossaand paranasal sinuses appeared uninvolved.Lid sparing exenteration was done in view ofextensive nature of disease.
Figures 22.2E and F: CT scan axial (E) and coronal (F) sections revealed a hyperdense mass filling most of the orbit
Figure 22.2G: Periodic acid schiff (PAS) stain (400×) showed thepresence of dark filaments confirming the diagnosis of aspergillusflavus
Figure 22.2H: Gomori’s methanamine silver (GMS) stain showed ofdark filaments aspergillus flavus
E F

326326326326326 Surgical Atlas of Orbital DiseasesSurgical Atlas of Orbital DiseasesSurgical Atlas of Orbital DiseasesSurgical Atlas of Orbital DiseasesSurgical Atlas of Orbital Diseases
Figure 22.2I: 3 months postsurgery the skin wound had healedand the patient did not show any signs of recurrence
Histopathology of the exenterated specimenrevealed multiple septate branching fungalfilaments within the giant cells and stroma. Therewas no definite evidence of vascular invasion. Therewas no involvement of the globe. Microbiologyconfirmed the presence of Aspergillus flavus [Figure22.2G periodic acid schiff (PAS) stain showing thedark filaments and Figure 22.2H Gomori'smethanamine silver (GMS) stain showing the darkfilaments against a green background] in theexenterated orbit.
The patient was maintained on oral antifungalsand was stable with no recurrence till last follow up3 months postsurgery (Figure 22.2I).
REFERENCES
1. Bartische G Ophthalmodouelia, das ist Augendiest.Dresden, Matthes Stockwell, 1583; 217-19.
2. Golovine SS Orbitosinus exenteration. Ann Ocul1909;141:413-31.
3. Nowikoff V Extirpation of the orbit. Lyon Chir 1927; 26:17-27.
4. Wheeler JM The use of epidermic graft in plastic eye surgery.Internat Clin 1922; 3:292-300.
5. Shields JA, Shields CL, Demirci H, Honavar SG, Singh ADExperience with eyelid-sparing orbital exenteration: the2000 Tullos O. Coston Lecture. Ophthal Plast Reconstr Surg2001;17(5):355-61.
6. Donahue PJ, Liston SL, Falconer DP, Manlove JC.Reconstruction of orbital exenteration cavities. The use ofthe latissimus dorsi myocutaneous free flap.ArchOphthalmol. 1989; 107(11):1681-3.
7. Uusitalo M, Ibarra M, Fulton L, Kaplan M, Hoffman W, LeeC, Carter S, O'Brien J. Reconstruction with rectus abdominismyocutaneous free flap after orbital exenteration inchildren. Arch Ophthalmol. 2001; 119(11):1705-9.
8. Bonavolonta G Frontalis muscle transfer in thereconstruction of the exenterated orbit.Adv OphthalmicPlast Reconstr Surg. 1992; 9:239-42.
9. Arlyan S, Cuono CB.Use of the pectoralis majormyocutaneous flap for reconstruction of large cervical, facialor cranial defects. Am J Surg. 1980;140(4):503-6.

Orbital ProsthesisOrbital ProsthesisOrbital ProsthesisOrbital ProsthesisOrbital Prosthesis 327327327327327
Kuldeep Raizada
Orbital ProsthesisOrbital ProsthesisOrbital ProsthesisOrbital ProsthesisOrbital Prosthesis
INTRODUCTION
Loss of an eye has a very traumatic effect. It leads toloss of self belief, can make the patient and familyvery depressed. Eye to eye contact is very importantin conversation, which is usually lost if the personhas a very disfiguring eye or an empty socket. Theyseek aesthetic improvement in their cosmeticappearance. Patient's rehabilitation with prosthesisis very challenging, especially when it is a facialprosthesis where a natural looking prosthesis is thefinal goal.
Orbital prosthesis and ocular prosthesis deal withthe fabrication of an artificial substitute for differentkind of orbital deformities, which can be due todiseases, surgery, trauma or congenital malformation.Several cases of devastating facial injuries, incurredin battle, were treated in the early nineteenth centurywith indigenous appliances and these reconstructiveprocedures gave definite push to the field of facialreplacement.1 Great strides in the field have beenmade in the past decades.
Orbital Prosthesis
Orbital prosthesis is meant for the face to improvethe cosmetic appearance of the individuals and mostoften it is required in conditions where there is anadditional loss of periocular tissues like eyelids,eyelashes and eyebrows.3 While fabricating an orbitalprosthesis utmost care should be taken to not onlyreplace lost periocular tissue but also to match themin terms of color and texture to the surroundingtissues and the fellow orbit.
Types of Prosthesis
• OrbitalComplete– Spectacle mounted prosthesis– Adhesive retained prosthesis– Magnetic retained prosthesis
Partial– Adhesive retained prosthesis
Complete prosthesis: means prosthesis with not onlyan ocular prosthesis but also it contains eye lids, eyebrow and eye lashes, to restore the normal anatomicalappearance to the patient.
On the basis is retention it can be furtherclassified.1-4,8
Spectacle mounted prosthesis: is used in conditionswhere surface remains moist and a silicon prosthesisis not going to stay. A facial prosthesis made up ofacrylic can be attached to spectacle, can be an optionfor such kind of cases.
Adhesive retained prosthesis: in conditions wheresurface is dry and a silicon prosthesis is going tostay. A facial prosthesis made up of medical gradesilicon can be attached externally in such cases.
Magnetic retained prosthesis: this is fabricated in avery special situation where patient had radicalorbital exenteration. The surface is provided withthe support of magnetic anchors that helps inretaining the prosthesis.
Partial prosthesis: described in literature earlier forthe nasal and auricular prosthesis. Recently Raizadaet al.5-6 described the method of fabricating the partialorbital prosthesis where at first a custom made ocular
23C H A P T E R

328328328328328 Surgical Atlas of Orbital DiseasesSurgical Atlas of Orbital DiseasesSurgical Atlas of Orbital DiseasesSurgical Atlas of Orbital DiseasesSurgical Atlas of Orbital Diseases
prosthesis is placed and later on the lower eyelidsare designed using the medical grade silicon and thenit can be retained with epithane.
Factors that Affect the Fit of an OrbitalProsthesis
There are many factors that affect the fit of an orbitalprosthesis.It is important to evaluate the orbitaldefect and later on choosing the modalities ofretaining the orbital prosthesis.
1. If the orbit had an incidence of tumors, thereshould be no recurrence.
2. The surface should be well healed; there shouldbe no edema, or infected external surface if thecase is of open defects like in the cases of radicalorbital exenteration.
3. If it is a case of orbital trauma and severedeformity like lid coloboma, they may benefitwith partial upper or lower lids prosthesis.
4. If the patient had extensive damage to the orbitalcavity, a glue based prosthesis will be interferingwith patient eyelids and may not be verycomfortable. Such cases may be eitherconsidered for blepharorrhaphy or else anspectacle mounted orbital prosthesis withvaulted back surface.
5. If the patients have ocular disfigurement in thelower lids due to the extensive trauma and lidscannot be constructed, a partial prosthesis withintegrated lower lids can be fabricated.
In this chapter I shall be discussing the techniqueof fabricating orbital prosthesis (a hybrid type as acomplex prosthesis is made up of two differentmaterials, so called as hybrid prosthesis).
There are many steps involved but the followingsteps involved fabricating an orbital prosthesis areof more concern:
• Preperation of the patient• Impression• Casting• Sculpting• Moulding• Coloring• Using the desired material• Fabrication of ocular prosthesis.
Preparation of the Patient
This is a very important step as patient needs tounderstand what we are going to do. A propercounselling about the whole procedure makes thepatient very calm, and make the work verycomfortable. I believe that the more the patientunderstands, the better he co-operates. Explain tothe patient the whole procedure using the otherpatient's pictures or illustrations. You can now askthe patient to lay down on a couch or bed in orderto make patient completely relaxed as this is verytiring because the whole procedure takes about 30to 45 minutes.
Impression of the Orbital Defect
Impression is taken while the patient is lying in thesupine position. Vaseline is applied on the places ofeyebrows, eyelashes as well as in the raw area of thedefect if present.
There are many ways to take an impression.Many people believe that only defective sideimpression makes work much easier, but I believethat taking the impression of the whole face givesbetter pictures, hence forth I prefer to take theimpression of both sides of the face so as to obtainaccurate information about the defective as well asnormal side too.
We make use of hydrophilic colloid as the basicmaterial of taking the impression of the orbital cavity.It is not only just an impression material that isneeded but you also require the reinforcing materialssuch as metal clips, gauge piece and the final layer ofcasting stone.
Prior to taking an impression of the defect, it isessential to tell the patient about the type ofimpression you are going to take as some time thedefects are open as in case of radical exenteration,and slight mistakes give really a hard time. By usingthe base plate wax and adhesives like micropore tape,mark the boundary of defect. Use Vaseline on thearea of the eye lashes and eyebrow, so that whiletaking out, the impression comes out easily. (Figures23.1A to C)
Figure 23.1E : This is a lateral view showing howthe base plate wax and micropore adhesive makes aboundary of the defect and make easier to take an

Orbital ProsthesisOrbital ProsthesisOrbital ProsthesisOrbital ProsthesisOrbital Prosthesis 329329329329329
Figures 23.1A to L: (A) patient with front view and left orbital exenteration (B) base plate wax boundary to hold the impression material(C) front view with base plate wax boundary in place with applied vaseline on the face (D) front view with the placement of hydrophilic colloidand reinforce material (E) lateral view shows the use of adhesive tape on the boundary of base plate wax (F) placements of uniform layer ofdie-stone (G) placement of tiny reinforce material so that while taking out the impression cast should not break (H) placement of a gauge pieceon the same (I) after removal of cast from the cavity called negative impression (J) on the negative impression after placing layers of die-stone(K) once the die-stone is set, you can see the differentiation zone of these two (L) after separation of the two-piece
impression. Use the hydrophilic colloid in the ratioof 1:1 with water and after mixing thoroughly withthe flat spatula, pour it first on the defect area andlater in the surrounding tissues (Figure 23.1D). Usethe reinforcing materials to make the impression sothat while putting the second layer of die stone, itgets adhered to the surface and makes a stableimpression (Figure 23.1F).
As hydrophilic colloid gets set very fast it isrecommended that mix the die stone in ratio of 1:1with water and pour above the hydrophilic colloidmaterial. Meanwhile use the reinforcing material tomake the die-stone mechanically strong (Figure 23.1G).
We prefer to use even gauze piece over the dyestone (Figure 23.1H), so that it get integrated withdye-stone. In about 10 minutes the die-stone getsset and exothermic reactions starts and we use mildwater on the surface so that it remains cool. Oncethe die-stone is set, ask the patient to squeeze theface and remove the impression which is called asnegative impression (Figure 23.1I).
Casting
Casting is replicating a negative impression topositive impression, and this will reflect the defectof the patient. Stablize the impression material usingthe clay or sand box and slowly pour the mixture ofdye-stone, step by step. Let it set for its optimal timeof about 15 minutes (depends on the type of dyestone used), (Figures 23.1J to L shows the junctionline of dye-stone and hydrophilic colloid from whereyou can separate the negative and positiveimpression). Remove dye-stone cast at the junctionline slowly from the hydrophilic colloid and this willrepresent the patients deformity (Figures 23.1I andL). You should always compare the impression ofthe defected area and the patient's actual orbitaldefect. Once you are sure then only proceed ahead.(Figure 23.2A).
Sculpting
Use the tinfoil of 0.01 mm on the defect to make themodel easier to take out from the cast and to check
A B C D
E F G H
I J K L

330330330330330 Surgical Atlas of Orbital DiseasesSurgical Atlas of Orbital DiseasesSurgical Atlas of Orbital DiseasesSurgical Atlas of Orbital DiseasesSurgical Atlas of Orbital Diseases
Figures 23.2A to O: (A) positive case from the impression of the face (B) use of tin foil so that model can be taken out with out distortion (C)Use of the base plate wax a base on the top of the thin tin foil (D) placement of an ocular prosthesis, front view looking at the Purkenje's images(E) eye lids after attaching the lump of wax and carved with the metal spatula (F) lateral view of the same patient on the normal side (G) lateralview of the same patient on the affected side (H) placement of final wax model on the face (I) use of computer programme Adobe Photoshopto make the grid and analyse further, in order to get a better symmetry (J) final wax model placed on the positive cast of the impression (K) investof the wax model in the metal flask using the die-stone (L) once the die-stone is set, apply thin layer of "Cold Mould Seal" so that mould can beopen (M) once the thin layer of the "Cold Mould Seal" is dried second layer of die-stone is also poured in the metal flask (N) open the mould, seethat how beautifully the mould opens up (O) do remove the all wax from mould using the hot water and soap
it on the patient face (Figure 23.2B). There are variouskinds of materials used such as clay, waxes or, directsilicon for sculpting model. We prefer to start theprocedure with the base plate wax as it has propertyof moulding into desired shapes (Figure 23.2C).
Now we need to choose an ocular prosthesis forthe same anterior curvature of the patient, preferablya flatter one when you have shallow defect of theorbit (Figure 23.2D). By using the Purkinje's imagesof the fellow eye and measuring the inter pupillarydistance (distance from the mid line of face to thecenter of the fellow eye) to locate the exact cornealreflex and even the use of hurtle exophthalmometerfor assessing the exact amount of proptosis helpsgreatly in fabrication. Once satisfied with the cornealposition, I use the thin strip of the base plate wax tosculpt the eyelids. It is preferable to see the patient'sface from all angles so that when prosthesis isfabricated, it should meet the criteria of having equalamount of elevation from the base of the orbit(Figures 23.2E to H).
I also take the pictures of the patient with thefinal sculpted model and download in the computer,
using the 'Adobe Photoshop 6.0' as graphicalvisualization makes it much easier to correct furtherthe lids alignment, and to create a better symmetry(Figure 23.2I). Once I am done with these all steps Iagain go back and check the sculpted model andcompare to the patient's defect, use the desirespectacle frame and cut in that fashion (Figure 23.2J).
Moulding
Making a two-piece mould is not a very complicatedjob, but of course making a mould is an art. Once thewax model is finished, apply the vaseline on the rearside of the prosthesis in order to get a smoothmoulded surface. Mix die-stone in a ratio of 1: 1 withwater. Use the vibrating unit to remove all the airbubbles and pour the mixture of die-stone and waterin to a metal flask, apply some of the mixture on theback side of the model in case of any undercuts andthen invest this model in the metal flask. Look verycarefully as some of the dye-stone may be fast settingbecause before it sets you need to remove the excessmaterial from the mould surface and check if anyundercuts are there, as presence of undercuts in the
A B C D E
F G H I J
K L M N O

Orbital ProsthesisOrbital ProsthesisOrbital ProsthesisOrbital ProsthesisOrbital Prosthesis 331331331331331
Figures 23.3A to J: (A) mould shows smooth surface without pit and holes ideal for using the silicon (B) place the ocular prosthesis in the eyecavity groove (C) use the cynoacarylate glue to fix this in same place (D) shows the silicon from factor II and intrinsic colors (E) shows thesteering of silicon along with flock and intrinsic colors in the silicon (F) using the thin cellophane sheet and checking the final color with patientskin tone (G) shows the room temperature cured prosthesis (H) indicated the rough edge of the prosthesis (I) fabrication of an ocularprosthesis (J) final finished prosthesis
mould will finally affect the quality of prosthesis.Once the stone is set, apply the separating media(from DPI) and pour the other in the same fashion.Once the mould is set, open it very carefully andremove the wax model from the mould, clean it withthe hot water and reapply the separating media(Figures 23.2K to 23.2O). Now your mould is readyfor pouring the desired material.
Using the Desired Material
Attach the prosthesis to the stone moulds in itsoriginal position. Using the cynoacrylate, fix theprosthesis into its curvature so that it remains in sameposition as done while sculpting (Figures 23.3A toC). Till this step everything is common, and nowyou have to decide which type of prosthesis you arelooking for.
Here I describe the making of silicon prosthesis.I mix MDX4210 with Dow corning silicon in 1:1 alongwith combinations of artist colors and dyes, try tomatch the shades of the patient skin and add moreflocking so that it give much better skin appearance.I usually prefer intrinsic coloring MDX4210. As it getsset, pour into the moulds and take out all the airbubbles. Now close it from back to front, so that incase any air bubble remains, it will come on the backof the prosthesis and can be later taken care by doingthe patch work (Figures 23.3D to F).
Cure the silicon at room temperature under highpressure. Once the silicon is cured, open the mouldsand you have the prosthesis ready in your hand.Trim the extra margins using the 3M (Factor II)trimming wheels in a tapering fashion, so that it
mingles well with the surrounding tissues.Sometimes one may need an extra touch up to thecolors to make the appearance better (Figures 23.3Gand H).
Fabrications of Ocular Prosthesis
Make the mould of same prosthesis,7 locate the Irisposition and make a fresh mould, paint an iris buttonof the same curvature as the fellow eye andpolymerize with the white base using the pressurizedcuring unit. Once it is cured, open the mold, createthe blood vessels using the cotton rayon threads.Paint the scleral shades using dry earth pigments andcure with the clear layer of PMMA. Trim the extraportions, polish and insert into the patient orbitalprosthesis, attached the eye lashes and eyebrows(Figure 23.3I).
Assemble the ProsthesisOnce you are done with fabrication of ocularprosthesis and the facial prosthesis, your ocular piececan go very easily in the cavity that has been formedin place of dummy prosthesis.
Attach the eyelashes on the upper lid and lowerlids. If needed some external coloring can be donein order to look better (Figure 23.3J). Once satisfied,you have to instruct the patient regarding the use ofthe prosthesis.
Care of Your Prosthesis
Preparing Your Skin and Your Prosthesis1. Repeatedly practice positioning your prosthesis
without adhesive to ensure accurate placement.
A B C D E
F G H I J

332332332332332 Surgical Atlas of Orbital DiseasesSurgical Atlas of Orbital DiseasesSurgical Atlas of Orbital DiseasesSurgical Atlas of Orbital DiseasesSurgical Atlas of Orbital Diseases
2. Wash and thoroughly dry your hands and skinwhere your prosthesis is to be placed.
3. Clean your prosthesis with a soft, bristledtoothbrush, mild soap, (e.g. Ivory liquid) andwarm water.
Applying Your Prosthesis1. If adhesive is used, it should be applied with
cotton tipped swab by evenly spreading a thinlayer of the adhesive along the outer edges ofthe backside of your prosthesis according to themanufacturer's instructions.
2. Allow the adhesive to reach its properreapplication state depending on the type ofadhesive used (e.g. dried clear for Pros-Aide).
3. Using a mirror, carefully position and press yourprosthesis onto your skin to ensure good contact.
Removing Your Prosthesis1. Remove your prosthesis from skin on a daily
basis to keep your tissues healthy and to maintainhygiene. Grasp the thickest edge of yourprosthesis and gently remove it very slowly soas not to tear the edges or irritate your skin.
2. If necessary, use a moist washcloth over thesurface of the prosthesis to loosen adhesive fromyour skin.
Cleaning Your Prosthesis
1. If adhesive was used, remove it gently rollingthe adhesive off the prosthesis (starting fromthe center to the outer edges) with yourfingertips, using gauze or textured cloth.Soaking the prosthesis in a cup of warm waterhelps to soften adhesive and makes it easier toremove.
2. Clean the prosthesis with a soft, bristledtoothbrush, mild soap (e.g. Ivory), and warmwater.
3. Remove any traces of adhesive or oil by gentlywiping the tissue side with a gauze or soft-textured cloth moistened with rubbing alcohol.Repeat this step using a gauze or soft-texturedcloth moistened with Listerine on the backsideof the prosthesis.
4. If your prosthesis has an ocular component,remove and clean it with soap and water. Theocular component should NOT be cleaned withrubbing alcohol. Place a drop of mineral oil onthe eye and shine it once a week. Replace theeye carefully and adjust the location bysqueezing the prosthetic eyelids together.
5. If your prosthesis is retained with magnets,clips, or plastic buttons, take care to cleanaround each fixture with a soft, bristled brush,soap and water.
Cleaning Your Skin
1. Wash your face with soap and water afterremoving the prosthesis and remove any residueof adhesive from the skin. Avoid the use ofharsh solvents such as benzene or xylene.
2. Apply a moisturizing lotion on nightly basis torestore natural body oils.
3. Report any areas of inflammation or irritationto the office or clinic.
Color Changes
1. Avoid smoking, as it will stain prosthesisyellow.
2. Avoid prolonged exposure to sunlight, whichcan cause color dissolution and weakening ofthe prosthetic material.
3. Avoid the use of strong solvents, such as benzeneand xylene, which can cause dissolution andweakening of the prosthetic material.
Storing the Prosthesis
1. Store the prosthesis in a dry, inconspicuous butsafe place (for example, a bedside table drawer).Keep it out of the reach of children and animals.
2. If you have an orbital prosthesis, store it in anupright position.
Figures 23.4A and B: (A) patient with left orbital exenteration due toBasal cell carcinoma of the left eye (B) patient with silicon glue onprosthesis in place, further cosmetic appearance improved with simplepair of glasses
A B

Orbital ProsthesisOrbital ProsthesisOrbital ProsthesisOrbital ProsthesisOrbital Prosthesis 333333333333333
Preventing Mishaps
1. Avoid extreme temperature changes, which cancause adhesive to fail.
2. Carry extra-adhesive and pre-packaged alcohol-soaked cotton balls in a small plastic bag.
3. Avoid placing the prosthesis in purses or pocketsclose to items such as ink pens and makeup thatcould stain it.
4. If adhesive are prescribed, be careful not to spillthe adhesive bottle. To prevent evaporation,keep the lid tightened when not in use.
CONCLUSION
In majority of cases facial prosthesis restores thecosmetic appearance as well as self confidence(Figures 23.4A and B). However, the patient shouldbe educated and motivated to use the prosthesis andmaintain it properly. A cosmetic rehabilitationwithout the proper counselling is not effective.Overall a facial prosthesis remains an option inminority of cases.
REFERENCES
1. Prince JH, A short history of the development of artificialeyes. In: Ocular prosthesis. E and S Livingstone Ltd,Edinburgh, 1946:6-7.
2. Jackson, IT, Tolaman, DE, Desjardins, RP,Branemark, PI: Anew method for fixation of external prosthesis, PlastReconst. Surg. 1986;77:668-72.
3. Raizada K, Murthy R, Honavar SG. Ocular prosthesis withlower lid augmentation for disfigured lids followingchemical burns. Journal of Ophthalmic Prosthesis J Ophth.Prosth. Volume II PP 24-6.
4. Raizada K, D Deepa Rani, Naik M, Honavar SG, Journal ofFacial and Somato Prosthesis. Post Enucleation SocketSyndrome: an ocularist View, Journal of Facial andSomatoprosthesis, 2005;1-12.
5. Yeatts RP. The esthetics of orbital exenteration.Am JOphthalmol. 2005;139(1):152-3.
6. Bulbulian AH. Prosthetic reconstruction of the exenteratedorbit. In: Facial Prosthetics. Charles C Thomas, Springfield,IL, 1973: 48-63.
7. Jahrling RC. Contracted socket following enucleation aftermultiple surgical procedures. Problems and treatment ofenucleation, evisceration, exposure. IntercontinentalMedical book corporation 1974:12;27-9.
8. Bulbian AH, Facial Prosthetics, method of retention of facialprosthesis 364.



Subrahmanyam Mallajosyula, Mohd Javed Ali
Medical ManagementMedical ManagementMedical ManagementMedical ManagementMedical Managementof Proptosisof Proptosisof Proptosisof Proptosisof Proptosis
Some of you may be surprised to know that nearlyhalf the cases of proptosis can be managed withoutsurgery. This is because of the advances in diagnosticand therapeutic interventions made in the past fewdecades which made medical managements morescientific, evidence based and safer. Many patientsof proptosis obviously are to benefit from theseadvances. We are confident that most of the activeorbital surgeons across the globe agree with thisstatement.
Many etiological factors involved in proptosis cannow be safely managed medically. This chapteroutlines the standard protocols and recent trendsinvading this arena. The role of medical managementin thyroid orbitopathy, and the role of chemotherapywere dealt in detail in separate chapters and hencenot included in this.
Let us consider the medical management in thefollowing headings:
• Nonspecific inflammations of the orbit• Specific inflammations of the orbit• Vascular lesions• Structural lesions• Lymphoproliferative and other neoplastic
lesions.1
NONSPECIFIC INFLAMMATIONS OFTHE ORBIT (NSOIS)
Based upon the location of inflammation the non-specific orbital inflammation or idiopathic orbitalinflammation can present as five entities : Myositic,
lacrimal, anterior, diffuse and apical. Apart fromclinical presentation, imaging is very helpful indiagnosis. NSOIS is usually acute or subacute in onsetand painful. It is usually unilateral, and occasionallybilateral. Rarely it is recurrent. The visual symptomsinclude diplopia, and defective vision. HistologicallyNSOIS is characterized by polymorphous infiltrations.
Nonspecific Myositic Inflammation
This is the most common presentation in ourexperience. We manage patients presenting as a singlemuscle disease with nonsteroidal anti-inflammatorydrugs and low dose corticosteroids. Recurrence isunlikely in them. Patients presenting with multiplemuscle disease, are prone to recurrences. We treatthem more aggressively with oral Prednisolone 2mg/kg body weight tapered over 4-6 weeks or withintravenous methyl prednisolone2 pulse therapy.Patients with recalcitrant disease requireimmunosuppressives. Such patients were found tobenefit from methotrexate in a dose of 15-25 mg perweek3 usually marked clinical response is evidentwithin a week. Those cases which fail to respond tothe drugs warrant a biopsy to exclude a lymphoma.
Nonspecific Lacrimal InflammationNonspecific dacryoadenitis should prompt asuspicion for systemic disease where a percutaneousbiopsy is recommended first. Management includesmoderate doses of steroids such as 1mg/kg oralprednisolone which can be tapered over 4-6 weeks.Majority of nonspecific dacryoadenitis resolves over6-12 weeks.
24C H A P T E R

338338338338338 Surgical Atlas of Orbital DiseasesSurgical Atlas of Orbital DiseasesSurgical Atlas of Orbital DiseasesSurgical Atlas of Orbital DiseasesSurgical Atlas of Orbital Diseases
Specific Inflammations of the Orbit
These are the most common etiological factors inproptosis for which medical management iscommonly carried out. Therapeutic options inmanagement of inflammations are ever expandingnot only because biologically targeted agents arebecoming increasingly available that can act onspecific segments of inflammatory cascades but alsobecause of advances in our understanding ofetiopathogenesis.
Orbital CellulitisThis is the most common cause of painful proptosis,acute in onset and most often unilateral. The principlesof management of a case of orbital cellulitis are controlof infection by the use of appropriate antibiotics,preventions of ocular as well as nonocularcomplications, surgical drainage when necessary andcareful follow up. We insist on imaging on anemergency basis in every case of orbital cellulitis fortwo reasons : (1) To make sure that we are not missingother neoplastic lesions like Rhabdomyosarcoma,Retinoblastoma which clinically mimic orbitalcellulitis (2) To plan the course of action: We prefersurgical drainage of orbital or sub-periosteal abscess.In the absence of abscess, medical management ispreferred. The patient should be carefully monitoredduring the treatment for any threat of loss of vision,and clinical response to the drugs. From ourexperience and also from the literature we wish toemphasize that there is a great difference in theprognosis and hence management strategies of orbitalcellulitis in children and adults. Usually in childrenunder the age of 9 years the infection is by a singleaerobic organism such as pneumococci4 and respondto medical management, the threat to affect vision israre and surgery is rarely needed. In contrast adultsharbor polymicrobial infection and the threat to visionis common and hence drainage is frequently requiredin addition to systemic antibiotics.5
Orbital cellulitis secondary to sinusitis is knownto harbour organisms like Strep pneumoniae, Hinfluenzae, Bacteroids and anaerobic cocci. Recom-mended antibiotics include third generationcephalosporins like cefotaxime, ceftriaxone andcefuroxime. Alternatively piperacillin withtaxobactum or ticarcillin with clavulanate can be used.Orbital cellulitis secondary to trauma or foreign-body
are known to be harbouring organisms like S aureus,S epidermidis, Streptococci and anerobes. Recom-mended antibiotics for such cases includeVancomycin along with third generation cephalo-sporins or imipenem1 Imaging with a CT or a MRIcan accurately monitor the progress and effect oftreatment. Septic thrombosis of cavernous sinuseither due to spread from contiguous structures orsepticemia demands prompt recognition andtreatment with broad spectrum antibiotics asdiscussed above for optimal clinical outcome.
Rhino-orbital MucormycosisThis is one of the very harmful infections and canlead to death. It is almost always associated withuncontrolled diabetes mellitus and usually withketoacidosis.6-8 Once the diagnosis is establishedbased on clinical findings, microscopic fungalexamination and culture, a multidisciplinary approachis commonly practiced. Diabetes should be managedsimultaneously. Following wide excision ofdevitalized tissue, the area is daily irrigated withamphotericin. Systemic treatment with amphotericinis also recommended. Some believe in the usefulnessof hyperbaric oxygen for such cases.9
Chronic Granulomatous InfectionsSince the advent of AIDS, incidence of certaingranulomatous infections of importance in proptosislike tuberculosis and syphilis is on a rise.
Orbital involvement in tuberculosis is usually bydirect invasion from sinuses or hematologicaldissemination. Periostitis, cold abscess and orbitaltuberculomas are well recognized lesions.10 In doubtfulcases PCR is helpful. Orbital involvement is diagnosedwith a high index of suspicion and aspiration biopsy.Systemic anti-tuberculous drugs are recommended incoordination with a chest physician.
Though literature says that syphilis is on a risewith immunosuppressive syndromes, we are yet tocome across a case of syphilis with orbital involve-ment. Periostitis, acute and chronic inflammations arerecognized lesions. Systemic antibiotic therapy usuallywith penicillins is useful in resolution of the disease.
Parasitic InfestationsCysticercosis, echinococcosis and trichinosis arecommon parasitic etiological factors in the causationof proptosis.

Medical Management of ProptosisMedical Management of ProptosisMedical Management of ProptosisMedical Management of ProptosisMedical Management of Proptosis 339339339339339
Cysticercosis is caused by C.cellulosae, thelarval form of tapeworm, Taenia solium. Though orbitis considered to be a rare site in the west, manyreports in the literature suggests that orbitalinvolvement is most frequent among Asians.11 Oncediagnosis is established with the help of imaging andserology, systemic albendazole (15 mg/kg) alongwith steroids (prednisolone 1-2 mg/kg) for a periodof four weeks is found to be effective11 If there isevidence of associated neurocysticercosis, treatmentis with steroids (prednisolone 1mg/kg) andpraziquantel 50 mg/kg in three divided doses for aperiod of 15 days. Association between orbitalmyocysticercosis and neurocysticercosis is not verycommon. We prefer to refer these patients to aneurologist for in-patient treatment since there is arare possibility of generalized seizures. The responsecan be monitored and progress can be documentedwith imaging.
Echinococcosis or hydatid cyst as it iscommonly called is an intestinal infestation of dogs.Orbital cysts are seen in 1% of echinococcosis.Systemic albendazole has been found to be effectivein resolving the cyst.15 Steroids are recommendedfor violent inflammatory reactions following ruptureof the cyst during aspiration or attempted surgicalremoval16 Certain studies have shown high efficacyin disease resolution when combination ofpraziquantel with albendazole12-14 is used.
Trichinosis occurs as cysts in extraocular muscles,which may show evidence of calcification on imaging.Treatment recommended include systemic thia-bendazole along with steroids to reduceinflammation. Personally we have no experience aswe are yet to come across a case of trichinosis withorbital involvement.
VasculitisVasculitis or angiitides as some may call it is a clinicalsyndrome that encompasses acute or chronicinflammation of vessels with vaso-obliterative signsand symptoms17 Most common vasculitis that involvethe orbit include Wegener's granulomatosis andPolyarteritis nodosa. Diagnosis is usually establishedby imaging, biopsy with a histopathologicalexamination and specially for wegener's a serologicalexamination in the form of C-ANCA15 Dramaticimprovement is noticed when systemic steroids arecombined with an alkylating agent like cyclo-
phosphamide.21,22 Recent studies have suggested arole of anti-TNFs (tumor necrosis factors) likeInfliximab and Etanercept. The development of novelapproaches focusing on blockade of specific moleculesincluding TNF alpha is awaited.22 Another novelapproach that is showing promise in the managementof refractory Wegener's and C-ANCA relatedvasculitis is the use of Rituximab, a chimeric anti-CD20 monoclonal antibody.23,24
Tolosa-Hunt SyndromeThis nonspecific granulomatous inflammation thoughrare is nevertheless an important differential diagnosisof apical orbital inflammations. The clinical course ismarked by remissions and recurrences. SPIR MRI(spectral presaturation with inversion recovery MRI)has been recommended for diagnosis1 Managementincludes a high dose of systemic steroids which oftenproduces a dramatic clinical improvement. SPIR MRIbefore and after corticosteroids have been found tobe useful in some studies for definite diagnosis andmonitoring of the disease.1
Vascular Lesions
Capillary Hemangioma
Treatment is indicated when vision is threatened byamblyopia as a result of anisometropia, ptosis orstrabismus.
Intralesional injection of steroids is the mostfrequently used method. Usually 40-80 mg oftriamcinolone with 25 mg of methylprednisolone isdirectly injected into the lesion.1 AlternativelyTriamcinolone 40 mg in combination 4 mgbetamethasone can be used. The tumor usually beginsto regress in two weeks but if necessary injectionmay be repeated after about two months. Earlyrecognition and prompt treatment with intralesionalsteroid prevents amblyopia exanopsia, but follow-up and management of refractive amblyopia withglasses and patching is necessary in the longer term.Potential complications include skin depigmentation,fat atrophy, eyelid necrosis and rarely central retinalartery occlusion.
Systemic steroids are indicated for extensivelesions specially if associated with visceralinvolvement. Recommended dosage used is1.5 mg/kg to 2.5 mg/kg Prednisolone daily over afew weeks with titration downward depending onresponse.1

340340340340340 Surgical Atlas of Orbital DiseasesSurgical Atlas of Orbital DiseasesSurgical Atlas of Orbital DiseasesSurgical Atlas of Orbital DiseasesSurgical Atlas of Orbital Diseases
Though steroids are effective in large majorityof patients, a recurrence is not infrequent. Recurrentor resistant cases are being treated with recombinantinterferon alpha-2a and 2b with variable results16
Recent studies have demonstrated good efficacy ofinterferons when given subcutaneously in a dose of3 million units/m2. During clinical follow-updiagnostic ultrasound evaluation ( the depthdimension) proved helpful. One report suggestedhigh efficacy of treatment when a combination ofinterferon alpha-2a with a low dose of cyclo-phosphamide.17
In the presence of very large platelet-consuminglesions as seen with Kasabach-Meririt syndrome,systemic antifibrinolytics like aminocaproic acid ortranexemic acid are used.18
Structural Lesions
Acute Intraorbital Hemorrhage and EmphysemaPost-traumatic fractures, soft tissue injury, contusionsand retrobulbar blocks may be associated with acuterise in intraorbital pressure as blood is trapped inconfined spaces. The effects of such rapid rise in thepressure include optic nerve ischemia and retinalhypoperfusion. The optic nerve head maydemonstrate arterial pulsations. Hence theimportance of prompt recognition and earlymanagement cannot be overemphasized. Thoughsevere visual threat is a surgical emergency, formoderate degrees of orbital tension, treatmentincludes 500 mg of acetazolamide i.v., and mannitol1-2 ml/kg i.v over 30 minutes has been advocated.1,19
Orbital emphysema is another cause of acuteorbital tension and is almost always secondary totrauma. This rarely requires decompression as theair tends to absorb rapidly. Though most of thepatients are managed with antibiotics, prophylacticuse is usually not required for clean wounds.20
Lymphoproliferative and Other NeoplasticLesions
These disorders encompasses a wide range of clinicalsyndromes. The advent of immunodiagnostics andmolecular techniques had a profound effect on betterunderstanding of pathogenesis and therapeutic
advances. Among the lymphoproliferative lesions,reactive lymphoid hyperplasia appears to be steroidsensitive as it responds to moderate doses ofPrednisolone. Failure to respond to steroids can bemanaged by cytotoxic agents and low doseradiotherapy.1
Another clinicopathological entity; the indeter-minate lymphoproliferative lesions are steroidresistant and may require treatment with immuno-supressives or radiotherapy.1 The widespread useof chemotherapy for lympho-proliferative lesions andother neoplastic conditions is being dealt in detail ina separate chapter.
CASE ILLUSTRATIONS
Case 1Mrs.K, female 54 years presented with acute, painfulproptosis of left eye of 5 days duration. She hadsevere pain, nausea and mild fever. There was a verysevere edema of the lids and periorbital edema(Figure 24.1A). The upper lid had complete ptosis.On everting the upper lid, the globe was found to beproptosed. The conjunctiva was congested andchemosed. Ocular motility was restricted (Figures24.1B and C).CTscan showed orbital cellulitis withoutany abscess. She was given intravenous (Amoxicillinand clavilanic acid) and Metronidazole, with whichshe showed a marked improvement within 5 days.She was relieved from pain, proptosis reduced, andthe ptosis improved markedly( Figure 24.1D) Theconjunctival chemosis and congestion improved andthe ocular motility restored to normal (Figures 24.1Eand F).
Figure 24.1 A: Female 54 years presented with acute, painful prop-tosis of left eye. Note the severe edema of the lid and periorbitaledema, and the gross ptosis

Medical Management of ProptosisMedical Management of ProptosisMedical Management of ProptosisMedical Management of ProptosisMedical Management of Proptosis 341341341341341
Figures 24.1B and C: On elevating the lid, note the conjunctival congestion and chemosis.Note the restricted ocular motility both in adduction (B) and abduction (C)
Figures 24.1E and F: Note the restoration of ocular motility both in adduction (E) and abduction (F)
Figure 24.1D: After medical management, note the improvement in the edemaof the lids, ptosis, chemosis and congestion of the conjunctiva
Case 2
Female 17 years, presented with proptosis of righteye associated with mid pain since 1 month. Therewas no history of trauma, defective vision ordiplopia. Examination revealed mild proptosis of theright eye with fullness of right upper lid in thesupero-temporal region (Figure 24.2A). CTscan of
the orbit revealed enlarged lacrimal gland moldingto globe (Figure 24.2 B). The possibility of lymphomawas thought off. FNAC and immunohistochemistrywere negative for lymphoma. Hence, a diagnosis ofnonspecific orbital inflammation, involving thelacrimal gland was made; the girl was treated withsystemic steroids to which she responded well(Figure 24.2C).
B C
E F

342342342342342 Surgical Atlas of Orbital DiseasesSurgical Atlas of Orbital DiseasesSurgical Atlas of Orbital DiseasesSurgical Atlas of Orbital DiseasesSurgical Atlas of Orbital Diseases
CT scan revealed inflammation at the apex of theorbit (Figures 24.3E and F) with mild enlargementof superior ophthalmic fissure. In view of subacuteonset, associated pain, restricted ocular motility anddefective vision, a diagnosis of superior ophthalmicfissure syndrome was made, and he was treated withsystemic steroids. The patient responded very well.The vision improved from 20/200 to 20/30 in afortnights time.
Figure 24.2 A: Note the fullness at the supero-temporal region of theright upper lid, with mild displacement of the globe and minimal ptosis
Figure 24.2B: Coronal section of CT scan of orbit showingenlarged lacrimal gland molding to the globe
Figure 24.2C: One week after oral prednisolone, note the improve-ment in the fullness of the supero-temporal region of the right upperlid, and in ptosis
Case 3
Male 28 years presented with proptosis of right eye,subacute in onset and associated with mild pain anddefective vision( Figure 24.3A) On examination, hehad mild proptosis associated with ptosis, andrestricted ocular motility (Figures 24.3B to D). Figure 24.3D: Note the restricted abduction in the right eye
Figure 24.3C: Note the restricted depression in the right eye
Figure 24.3B: Note the restricted adduction in the right eye
Figure 24.3A: Male 28 years, presented with severe ptosis of rightupper eye lid and mild proptosis of right eye

Medical Management of ProptosisMedical Management of ProptosisMedical Management of ProptosisMedical Management of ProptosisMedical Management of Proptosis 343343343343343
REFERENCES
1. Rootman J: Diseases of the orbit ; A multidisciplinaryapproach. Lippincott Williams and Wilkins, (2nd ed): 455-506.
2. Nugent RA, Rootman J, Robertson WD, et al. Acute orbitalpseudotumors: AJNR 1981;2:431-6.
3. Hemady R, Tauber J, Foster CST. Immunosuppressivedrugs in immune and inflammatory ocular disease. SurvOphthalmol 1991;35:369-85.
4. Donahue SP, Schwartz G. Preseptal and orbital cellulitis inchildhood: a changing microbiologic spectrum.Ophthalmology 1998; 105:1902-6.
5. Harris GJ. Subperiosteal abcess of orbit. Age as a factor inthe bacteriology and response to treatment. Ophthal-mology 1994;101:585-95.
6. Ameen M, Arenas R, Martinez-Luna E, Reyes M, ZacariasR: The emergence of mucormycosis as an importantopportunistic fungal infection: five cases presenting to atertiary referral center for mycology. Int J Dermatol. 2007Apr;46(4):380-4.
7. Bhadada S, Bhansali A, Reddy KS, Bhat RV, Khandelwal N,Gupta AK : Rhino-orbital-cerebral mucormycosis in type 1diabetes mellitus, Indian J Pediatr. 2005;72(8):671-4.
Figures 24.3E and F: CT scan, Axial and sagital sections of the orbitshow a hyperdense lesion abutting the optic nerve at the orbital apex.Its margins are indistinct. Axial section of the CT shows enlargedsuperior ophthalmic fissure
8. Nithyanandam S, Jacob MS, Battu RR, Thomas RK, CorreaMA, D'Souza O. Rhino-orbito-cerebral mucormycosis. Aretrospective analysis of clinical features and treatmentoutcomes Indian J Ophthalmol. 2003;51(3): 231-6.
9. Ferry AP, Abedi S. Diagnosis and management of rhino-orbitocerebral mucormycosis. A report of 16 personallyobserved cases. Ophthalmology 1983;90:1096-104.
10. Pillai S, Malone TJ, Abad JC. Orbital tuberculosis. OphthalPlast Reconstr Surg 1995;11:27-31.
11. Honavar SG, Sekhar.G, Orbital Cysticercosis. Orbit 1998;17(4): 271-84.
12. Srivastava VK, Srivastava A, Singhal KC. Albendazoletherapy in orbital cysticercosis. Ind J Physiol Pharmacol1996; 40:265-66.
13. Richards KS, Morris DL Effect of albendazole on humanhydatid cysts: an ultrastructural study. HPB Surg 1990; 2:105-13.
14. Gomez MA, Croxatto JO, Crovetto L, Ebner R. Hydatidcysts of the orbit. A review of 35 cases. Ophthalmology1998; 95:1027-32.
15. Perry SR, Rootman J, White VA. The clinical andpathological constellation of wegener's granulomatosis ofthe orbit. Ophthalmology 1997; 104:683-94.
16. Nolle B, Coners H, Duncker G. ANCA in ocularinflammatory disorders. Adv Exp Med Biol 1993;336:305-7.
17. Teske S, Ohlrich SJ, Gole G, et al. Treatment of orbitalcapillary hemangioma with interferon. Aust N Z JOphthalmol 1994; 22: 13-7.
18. Neidhart JA, Roach RW. Successful treatment of skeletalhemangioma and Kasabach-Merritt syndrome withaminocaproic acid. Am J Med 1982; 73: 434-8.
19. Rootman J, Stewart B, Goldberg RA. Orbital Surgery:A conceptual approach. Philadelphia: Lippincott-Raven,1995.
20. Fleishman JA, Beck RW, Hoffman RO. Orbital emphysemaas an ophthalmologic emergency. Ophthalmology 1984;91:1389-91.
21. Selamet U, Kovaliv YB, Savage CO, Harper L. ANCA-associated vasculitis: new options beyond steroids andcytotoxic drugs. Expert Opin Investig Drugs. 2007;16(5):689-703.
22. Svozilkova P, Rihova E, Brichova M, Diblik P, Kuthan P,Poch T. Infliximab in the treatment of Wegener'sgranulomatosis: case report. Cesk Slov Oftalmol.2006;62(4):280-6.
23. Tamura N, Matsudaira R, Hirashima M, Ikeda M, TajimaM, Nawata M, Morimoto S, Kaneda K, Kobayashi S,Hashimoto H, Takasaki Y. Two cases of refractoryWegener's granulomatosis successfully treated withrituximab.
24. White ES, Lynch JP Pharmacological therapy for Wegener’sgranulomatosis. Drugs. 2006;66(9):1209-28.
E
F

344344344344344 Surgical Atlas of Orbital DiseasesSurgical Atlas of Orbital DiseasesSurgical Atlas of Orbital DiseasesSurgical Atlas of Orbital DiseasesSurgical Atlas of Orbital Diseases
Vijay Anand P Reddy, Nitin More, Ramesh Murthy, Anirban Bhaduri, Santosh G Honavar
Management of OphthalmicManagement of OphthalmicManagement of OphthalmicManagement of OphthalmicManagement of OphthalmicTumors: Role of ChemotherapyTumors: Role of ChemotherapyTumors: Role of ChemotherapyTumors: Role of ChemotherapyTumors: Role of Chemotherapy
and Radiation Therapyand Radiation Therapyand Radiation Therapyand Radiation Therapyand Radiation Therapy
INTRODUCTION
Ocular Oncology deals with the diagnosis, surgicaland nonsurgical management of tumors involvingthe eyelids, external ocular surfaces, intraocularstructures and the orbit. Ocular tumors invariablyare managed by multidisciplinary team of ocularsurgeon and an oncologist experienced in thetreatment of such tumors.
Radiation Oncology is the clinical and scientificdiscipline devoted to the management of patientswith cancer and other diseases with ionizingradiation alone or combined with other modalitieslike surgery and chemotherapy. The aim of radiationtherapy is to deliver a precisely measured dose ofradiation to a defined tumor volume with minimaldamage to surrounding healthy tissue.
Radiation used for cancer treatment is calledionizing radiation because it forms ions in the cellsof the tissues it passes through, as it dislodgeselectrons from atoms. Ions are atoms that haveacquired an electric charge through the gain or lossof an electron. This can kill cells or change genes.Other forms of radiation, such as radio waves,microwaves, and light waves are called non-ionizing.They have lower energy and hence can not ionizecells.
Ionizing radiation is of two major types
a. Non-particle Photons (X-rays and γ-rays), whichare most widely used.
b. Particle radiation (electrons, protons, neutrons).The common types of radiation used for cancertreatment are:
1. High-energy photons come from radioactivesources such as cobalt, cesium, or a machinecalled a linear accelerator. This is by far the mostcommon type of radiation treatment in usetoday.
2. Electron beams produced by a linear acceleratoror beta particle emitting radioactive source likeStrontium and Ruthenium. They are used fortumors close to a body surface, e.g. skin,conjunctiva and sclera.
3. Protons are a newer form of treatment. Protonsare parts of atoms that cause little damage totissues they pass through but have maximumeffect at the end of their path. This means thatproton beams may be able to deliver moreradiation to the cancer while causing fewer sideeffects to normal tissues nearby. Although it isused routinely for certain types of ocular andbrain tumors, it still needs more study in others.
4. Neutrons are used for some cancers of the head,neck, and prostate. They can sometimes behelpful when other forms of radiation therapydo not work especially when the tumor hasanoxic zones.
Radiation therapy delivery methods are asfollows:
1. External Beam Radiation (Teletherapy): It isthe most widely used type of radiation therapy.The radiation is focused from machine outsidethe body onto the area affected by the cancer.This type of radiation is most often given byeither radioactive source like cobalt or cesiumor with linear accelerators (Figure 25.1). The
25C H A P T E R

Management of Ophthalmic Tumors: Role of Chemotherapy and Radiation TherapyManagement of Ophthalmic Tumors: Role of Chemotherapy and Radiation TherapyManagement of Ophthalmic Tumors: Role of Chemotherapy and Radiation TherapyManagement of Ophthalmic Tumors: Role of Chemotherapy and Radiation TherapyManagement of Ophthalmic Tumors: Role of Chemotherapy and Radiation Therapy 345345345345345
radiation is aimed at the tumor, but also affectsthe normal tissue it passes through on its wayinto and out of the body. External beamradiation allows large areas of the body to betreated and allows treatment of more than onearea such as the primary tumor and nearbylymphnodes. External radiation is usually givenin daily treatments, 5 days per week overseveral weeks.
2. Internal Radiation Therapy (Brachytherapy):It is also known as brachytherapy, which meansshort-distance therapy. With this method,radioactive sources are placed directly into thetumor or into a cavity close to the tumor. Theadvantage of brachytherapy is the ability todeliver a high dose of radiation to a small area.It is useful in situations that require a high doseof radiation. The main types of internal radiationare:a. Interstitial radiation: The radiation source is
placed directly into or next to thetumor using small pellets, wires, tubes, orcontainers. For example, carcinoma tongue(Figures 25.2A and B).
b. Intracavitary radiation: A container ofradioactive material is placed in a cavity ofthe body such as the vagina, nasopharynx.
c. Surface (mould): Radiation sources are placedover the tissue to be treated, e.g. Ca hard palate.
d. Plaque Brachytherapy: Concave shapedradioactive plaque is placed over the sclerafor ocular melanomas, retinoblastoma, etc(Figure 25.3A).
e. Intraluminal: Sources are placed in a lumen,e.g. carcinoma esophagus.
f. Intravascular: A single source is placed intosmall or large arteries such as coronary arteryfor prevention of stent restenosis.
Based on the duration of treatment, brachytherapyis classified as:
a. Permanent (low dose rate) Brachy therapy: Dose isdelivered over the lifetime of the source untilcomplete decay.
b. Temporary (high dose rate): Dose is delivered overa short period of time and the sources areremoved after the prescribed dose has beenreached.
Figure 25.1: Teletherapy machine for externalbeam radiation therapy Figure 25.2A and B: Interstitial brachytherapy
A
B

346346346346346 Surgical Atlas of Orbital DiseasesSurgical Atlas of Orbital DiseasesSurgical Atlas of Orbital DiseasesSurgical Atlas of Orbital DiseasesSurgical Atlas of Orbital Diseases
Radiation therapy may be used alone or incombination with other cancer treatments, such aschemotherapy or surgery. In some cases, a patientmay receive more than one type of radiation therapy.
External Radiotherapy in Ocular Tumors
Linear accelerators equipped with both photon andelectron facility and multileaf collimators (MLC) aremainly used for the external radiation therapy oforbital tumors where multiple radiation beams arefocused on the tumor. Simulator with all theparameters similar to linear accelerator but capableof only diagnostic X-rays is used for radiationtherapy planning. It simulates the beams of theexternal radiotherapy machines before the patient isbeing taken for the actual treatment.
Conventionally radiation therapy planning iscarried out by immobilizing the patient in treatmentposition and a CT scan is done in the treatmentposition with the immobilization in place. The imagesare transferred to the computerized treatmentplanning system. The tumor volume and the criticalstructures are delineated by the radiation oncologistand then the medical physicist plans the various beamangles and energies and gives various treatmentoptions. The optimal plan is selected by the radiationoncologist and the patient is simulated according tobony landmarks visible under fluoroscopy and thedata given by the treatment planning system. Thecomputerized scan is invariably being used in allorbital tumors and the 3-dimensional conformalradiation therapy (3D-CRT) is planned.
All the efforts in the development of radiationtherapy techniques are directed towards properinclusion of tumor in the target volume and to sparethe surrounding normal tissues. Intensity modulatedradiation therapy (IMRT) is newer form of externalradiation therapy that is capable of obtaining desireddose distribution in irregular and concave shapessparing the adjoining critical organs like optic chiasmand pituitary gland.
Plaque Radiotherapy
A radioactive plaque is a device that can be used todeliver a high dose of radiation precisely andselectively to a tumor and negligible dose to thesurrounding structures. It is made with radioactiveCobalt, Ruthenium, Iridium, Palladium or Iodinesealed within. Plaques come in various shapesand sizes ranging from 10 to 25 mm in diameter(Figure 25.3B).
The procedure is done under anesthesia.Preoperative assessment of the lesion: location, sizeand thickness are measured by means of ultrasoundB scan and the details are given to the ocularradiation oncologist. The radiation oncologist alongwith the radiation medical physicist plans thetreatment with the help of computerized automateddosimetry software. An appropriate plaque, theradiation dose, dose rate and treatment time isselected. The treatment time may vary from 24 to 96hours based on type and size of tumor. This processneeds expertise of a radiation therapist and aradiation physicist well versed in brachytherapy.
Figure 25.3A: Radioactive plaques for intraocular tumorsFigure 25.3B: Ruthenium 106 plaque being placed on the eye for a
choroidal melanoma

Management of Ophthalmic Tumors: Role of Chemotherapy and Radiation TherapyManagement of Ophthalmic Tumors: Role of Chemotherapy and Radiation TherapyManagement of Ophthalmic Tumors: Role of Chemotherapy and Radiation TherapyManagement of Ophthalmic Tumors: Role of Chemotherapy and Radiation TherapyManagement of Ophthalmic Tumors: Role of Chemotherapy and Radiation Therapy 347347347347347
Fig. 25.4: Cell cycle
After obtaining a proper consent the patient is takenfor the operative procedure. The concave shapeddummy plaque similar to the radioactive plaque isplaced and checked and then the radioactive plaqueis placed and sutured in place (Figure 25.4). Patientis placed in isolation till the entire period ofradiotherapy. The plaque is removed underanesthesia after the required dose of radiation isdelivered.
Indications of plaque brachytherapy are asfollows:
1. Retinoblastoma measuring < 16 mm in basaldiameter and < 8 mm in thickness a primarytreatment, as an adjuvant to chemoreduction,and for failure of focal therapy.
2. Primary treatment for most medium-sized andsome large choroidal and ciliary bodymelanomas in an eye with salvageable vision.
3. Choroidal hemangioma.4. Choroidal metastasis.5. Extensive retinal capillary hemangioma.
Cell Cycle and the Principles of Anti-neoplasticTherapy
It is important to understand the growth pattern oftumor cells that affect the overall biological behaviorof tumor and response to anti-neoplastic therapy,either radiation or cytotoxic chemotherapy. Cell cycle
is composed of four distinct phases. The G1 phaseconsists of cells that have recently completed divisionand are committed to continued proliferation. Aftera variable period of time, these cells begin tosynthesize DNA, marking the beginning of the Sphase. After DNA synthesis is complete, the end ofthe S-phase is followed by the premitotic rest intervalcalled the G2 phase. Finally, chromosomecondensation occurs and the cells divide during themitotic M phase. Resting diploid cells that are notactively dividing are described as being in the G0phase.
Ionizing radiation generally affects the neoplasticcells those are in synthetic and mitotic phase wherethe DNA of the cell is damaged either temporarilyor permanently, causing subsequent cell death.Radiation therapy is usually delivered in multiplefractions to target the tumor cells which were inresting phase during earlier fraction of radiation.
Similarly, some anticancer agents induce theircytotoxic effects during specific phases of the cellcycle. Chemotherapeutic agents are used either assingle agent or in the combination of different agents.Combination chemotherapy agents are selectedaccording to different mechanism of action to havesynergistic effect and with different toxicity profile.Cumulative doses of individual drugs are typicallylow in combination chemotherapy regimens,potentially minimizing the long-term toxicity andimproving the therapeutic ratio.
Management of Ophthalmic Tumors
Ocular tumors with proptosis as the first symptomarise from eyelid and lacrimal gland, orbital softtissues, optic nerve and orbital bones. Prominent onesamong those are squamous and basal cell carcinomaof eyelid, rhabdomyosarcoma, non-hodgkin'slymphoma, optic nerve glioma, meningioma andidiopathic orbital inflammation. Occasionally,retinoblastoma in advanced stage could present withproptosis of eye.
Tumors of the Eyelid
Most eyelid masses are benign tumors such as skinsquamous cell papilloma, melanocytic nevus orcongenital and acquired cysts. Common malignanttumors of eyelid include basal cell and squamous cellcarcinoma.

348348348348348 Surgical Atlas of Orbital DiseasesSurgical Atlas of Orbital DiseasesSurgical Atlas of Orbital DiseasesSurgical Atlas of Orbital DiseasesSurgical Atlas of Orbital Diseases
Capillary Hemangioma
It is the most common pediatric eyelid tumor. It maybe a component of Hippel-Lindau syndrome orSurge-Weber syndrome. The natural history oflesion is spontaneous regression over 3 to 4 years,therefore usually these lesions are observed.Indications of treatment are obstruction of the vision,amblyopia, ulceration of the eyelid due to vascularcompression. Steroids are the first line of treatment.Radiation therapy is reserved until other treatmentmethods have failed. Low energy photons orelectrons are used in dose of 500 to 750 cGy in 2-3fractions or fractionated low dose to a total of 1600to 2000 cGy.1
Basal Cell and Squamous Cell Carcinoma
Basal cell carcinoma (BCC) represents 90% ofmalignant eyelid tumors. Its four morphological typesare the nodular, ulcerative, pigmented and themorpheaform tumor. It mostly involves the lowereyelid. More likely to affect fair skinned personswith high solar exposure. It may be mistaken for achalazion or chronic blepharitis. Complete excisionwith frozen section control of tumor margins usingcryo is the standard treatment for localized tumors.Larger lesions are treated with definitive surgeryand appropriate reconstruction.
Squamous cell carcinoma (SCC) is the second mostcommon malignancy of the eyelids. Sun exposure isthe most important factor in developing SCC of theskin. It may occur in previously normal appearingskin or more commonly arises from a pre-existinglesions like actinic keratoses, skin damaged byionizing radiation or xeroderma pigmentosum.Unlike BCC of the eyelid, SCC can be an aggressivetumor and has the potential to invade the orbit,metastasize to lymph nodes and distant sites.
Primary excision is curative for small lesions inbasal cell and squamous cell carcinoma of eyelid.Irradiation could be used for unresectable andrecurrent basal cell carcinoma. It also could be usedas an alternative to surgery with more than 90% ofcure rate if patient prefers radiation therapy oversurgery. Cryotherapy could be used for recurrentlesions; usually in medial canthus. Orbitalexenteration is reserved for deep invasive lesions.Radiation dose of 50 to 60 Gy should be delivered
with low energy X-rays or electrons with appropriateshielding of lens.2
Sebaceous Carcinoma
Ocular sebaceous carcinoma is a very rare butaggressive tumor, most commonly occurs in patients60 to 80 years of age although the range is from earlychildhood through the nineties. It usually arises fromthe meibomian glands followed by glands of Zeissand caruncle. It may be multicentric resulting in localrecurrences. The incidence appears to be somewhatgreater in women and in Asian population.3
General principle of treatment is wide excision(with 5 to 6 mm surgical margins) with either frozensection or permanent section control as primarymanagement of sebaceous carcinoma.4 Map biopsiesof eyelids and conjunctiva should be carried out.Radiotherapy provides acceptable cosmesis both forprimary treatment and for treatment of recurrentdisease. Somewhat higher irradiation dosages in therange of 60 to 65 Gy in six to seven weeks arerecommended, and the control rates are in the rangeof 80 to 90% or better.5
Tumors of Lacrimal Gland
Epithelial tumors of lacrimal gland could be benign,e.g. pleomorphic adenoma (benign mixed tumor) ormalignant, e.g. adenoid cystic carcinoma orpleomorphic adenocarcinoma (malignant mixedtumor). On imaging, pleomorphic adenoma appearsas round to ovoid superotemporal orbital mass whichmay cause bony indentation, without bone erosion.Malignant tumors have irregular margin, often withadjoining bone destruction.
Complete excision of mass (excisional biopsy) iscurative for pleomorphic adenoma. Incompleteexcision can lead to recurrence and malignanttransformation.
Malignant tumors should be completely excisedif possible. Routinely postoperative radiation therapyto a dose of 5000 to 6000 cGy is delivered. In locallyadvanced lacrimal gland carcinoma, neoadjuvantchemotherapy with cisplatin and 5-fluorouracilfollowed by surgery and postoperative radiationtherapy is given. Results of intracarotidchemotherapy with Cisplatin and Doxorubicinfollowed by surgery and radiation therapy areencouraging6,7

Management of Ophthalmic Tumors: Role of Chemotherapy and Radiation TherapyManagement of Ophthalmic Tumors: Role of Chemotherapy and Radiation TherapyManagement of Ophthalmic Tumors: Role of Chemotherapy and Radiation TherapyManagement of Ophthalmic Tumors: Role of Chemotherapy and Radiation TherapyManagement of Ophthalmic Tumors: Role of Chemotherapy and Radiation Therapy 349349349349349
Malignant Conjunctival Tumors
Squamous cell carcinoma is the most common primarymalignant tumor of conjunctiva, manifests usually asa fleshy vascularized mass at the limbus. Conjunctivaltumors are treated by complete excision biopsy withfrozen section control of tumor margins andcryotherapy of the tumor bed. Reconstruction canbe done then by simple closure, conjunctival graftingor amniotic membrane transplant.
Primary or adjunctive use of local treatment withsome chemotherapeutic agents such as Mitomycin-C, 5- Flourouracil and Interferon alpha 2-b have beenreported. In some diffuse radiosensitive tumors suchas lymphoma, fractionated external beam radio-therapy or application of a radioactive plaque maybe employed.
Intraocular Tumors
Intraocular tumors arise from iris, choroid, retina oroptic nerve head. Iris masses could be melanocyticas nevus and melanoma, granuloma, hemangioma,leiomyoma, lymphoma, metastases, and extensionfrom a ciliary body tumor. Choroidal melanoma isthe most common intraocular tumor in adults. Othercommon intraocular pigmented tumors include opticnerve head melanocytoma, retinal pigmentepithelium adenoma and combined hamartoma ofretina and retinal pigment epithelium. Choroidal non-pigmented masses include amelanotic melanoma,uveal granuloma, lymphoma, osteoma and choroidalmetastases. Retinal non-pigmented masses includeretinoblastoma and toxocara granuloma.
Choroidal Melanomas
Small Lesions <1.5 mm height without high riskfactors like juxta papillary location, presence ofsubretinal hemorrhage, presence of orange pigmentare closely observed. Lesions of 1.5 to 10 mm heightare treated according to its location. Peripheral lesionsare locally excised. Central and mid peripheral lesionswith size < 4 mm are treated with trans-pupillarythermotherapy (TTT). Lesions with > 4 mm of sizeare treated with plaque therapy or external radiationtherapy with photons or protons. Lesions of >10 mmin height are treated with enucleation or externalradiation therapy.
Ruthenium-106 is currently the most commonlyused isotope for plaque radiotherapy of choroidal
melanomas, although cobalt-60, Iodine-125, iridium-192, strontium-90, and palladium-103 have also beenused. Modern techniques for plaque brachytherapyinvolve suturing a shielded plaque containing seedsof the radioactive isotope to the sclera.8,9 This remainsin place for a specified number of days in order todeliver the proper dose of radiation. Most mela-nomas are treated with a calculated apex dose of 70to 85 Gy.10
Intraocular Lymphoma
This is a rare variety of non-Hodgkin's lymphoma,large cell lymphoma being the most commonhistology. Uveal tract, retina, vitreous or optic nervesare usually involved. Vitreoretinal involvement isusually associated with central nervous systemlymphoma. Diagnosis is usually done by vitreousbiopsy. Usually they do not have systemicmanifestation. Recommended treatment is externalradiation therapy to a dose of 3600 to 4000 cGy at1.8-2 Gy fractions.11
Retinoblastoma
For over 100 years or longer the treatment ofintraocular retinoblastoma has been enucleation.Various forms of radiation treatment have been usedin the management of retinoblastoma since WorldWar II. The goal of radiation has been to destroy thetumour, save the eye, and maximise visual potential.Since the radiation in the paediatric age group hasits potential long-term side effects newer modalitieslike chemotherapy has been attempted. Since theintroduction of platinum and etoposide basedchemotherapy there has been tremendousimprovement in tumor control and survival.
Current standard treatment options forretinoblastoma include the following:
1. Cryotherapy: used in addition to radiation or inplace of photocoagulation for lesions smallerthan 4 disc diameters in the anterior portion ofthe retina.
2. Photocoagulation: occasionally used alone withsmall tumors. It is used for posteriorly locatedtumors that are smaller than 4 disc diameters,distinct from the optic nerve head and macula,and without involvement of large nutrientvessels or choroid involvement in patients withearly-stage disease (in addition to radiation

350350350350350 Surgical Atlas of Orbital DiseasesSurgical Atlas of Orbital DiseasesSurgical Atlas of Orbital DiseasesSurgical Atlas of Orbital DiseasesSurgical Atlas of Orbital Diseases
therapy) or when there is limited recurrencefollowing radiation therapy. Thermotherapydelivered via infrared radiation is an alternativeto laser photocoagulation.12
3. Chemoreduction: Systemic chemotherapy is usedto reduce tumor volume with intraoculartumors making them suitable for treatment withcryotherapy or photocoagulation.13,14 Factorssuch as tumor location (macula), patient age,and tumor size correlate with responsivenessto chemotherapy.15,16 Most tumors are treatedwith combination chemotherapy, Inj.Vincristine,Inj. Etoposide and Inj. Carboplatin. The dose ofthese drugs depends on the age, stage and theintention of treatment, either chemoreductionor adjuvant chemotherapy (Table 1). They alsorequire additional local therapy. Overall, theresponse rate is highest for tumors that areunilateral or unifocal and without vitreousseeding.
4. Subtenon (subconjunctival) chemotherapy:Carboplatin is administered by the treatingophthalmologist into the subconjunctival space.This modality is undergoing testing in phase Iand II trials and is generally used in conjunctionwith systemic chemotherapy and localophthalmic therapies for retinoblastoma withvitreous seeding. This approach offers somepromise in this group of patients.17,18
5. Surgery (enucleation) is usually undertakenwhen unilateral disease is massive and there isno expectation that useful vision can bepreserved. Careful examination of the enu-cleated specimen by an experienced pathologist
is necessary to determine whether high-riskfeatures for metastatic disease are present.Postoperative external radiation therapy isindicated in the presence of optic nerveextension to transection, scleral infiltration andextrascleral extension. Systemic standardchemotherapy for six cycles is indicated foranterior chamber seeding, infiltration of iris,ciliary body infiltration, massive choroidalinfiltration or optic nerve extension beyondlamina cribrosa. High dose chemotherapy for 6cycles is used in patients with combinedchoroidal infiltration and optic nerve extensionbeyond lamina cribrosa or with scleralinfiltration. High dose chemotherapy for 12cycles is used in patients with extrascleralextension and optic nerve extension totransection. Vincristine, doxorubicin, andcyclophosphamide, or vincristine, carboplatin,and etoposide are the drugs in different doseschedules as described in (Tables 2 and 3).Intrathecal methotrexate is given if CSF ispositive or there is radiological evidence ofintracranial extension.
6. External beam radiotherapy: Retinoblastoma isgenerally a radiosensitive tumor. Presently, witheffective chemotherapy drugs the indications forradiotherapy are minimized to avoid the lateeffects of radiotherapy, like facial deformitiesand second malignancies. External beamradiotherapy is a method of delivering wholeeye irradiation to treat advanced retinoblastoma,particularly when there is diffuse vitreousseeding. Presently, the indications of externalradiotherapy are residual disease after chemo-
Table 1: Chemoreduction regimen
Standard dose regimen
Inj. Vincristine 1.5 mg/m2 (0.05 mg/kg for children </= 36 months of age; max 2 mg) Day 1
Inj. Etoposide 150 mg/m2 (5 mg/kg for children </= 36 months of age) Day 1+2
Inj. Carboplatin 560 mg/m2 (18.6 mg/kg for children </= 36 months of age) Day 1
High dose chemotherapy
Inj. Vincristine 1.5 mg/m2 (0.05 mg/kg for children </= 36 months of age; max 2 mg) Day 1
Inj. Etoposide 250 mg/m2 (12 mg/kg for children </= 36 months of age) Day 1+2
Inj. Carboplatin 750 mg/m2 (28 mg/kg for children </= 36 months of age Day 1

Management of Ophthalmic Tumors: Role of Chemotherapy and Radiation TherapyManagement of Ophthalmic Tumors: Role of Chemotherapy and Radiation TherapyManagement of Ophthalmic Tumors: Role of Chemotherapy and Radiation TherapyManagement of Ophthalmic Tumors: Role of Chemotherapy and Radiation TherapyManagement of Ophthalmic Tumors: Role of Chemotherapy and Radiation Therapy 351351351351351
Table 4: Management of extraocular retinoblastoma
a. Baselins CT scan or MRI; bone marrow and CSFcytology
b. Intrathecal methotrexate if CSF is positive or there isradiological evidence of intracranial extension
c. High dose chemotherapy for minimum three cycles andreassess
d. Enucleation and continue high dose chemotherapy for6-12 cycles and external beam radiation therapy (seepost-enucleation protocol)
e. If systemic metastasis at the time of presentation,modify timing of local therapy depending on the extentof tumor.
Table 5: Post-enucleation adjuvant treatment protocol
a. Systemic standard chemotherapy for 6 cycles for1. anterior chamber seeding,2. infiltration of iris,3. ciliary body infiltration,4. massive choroidal infiltration5. optic nerve extension beyond lamina cribrosa.
b. High dose chemotherapy for 6 cycles in patients with1. combined choroidal infiltration2. optic nerve extension beyond lamina cribrosa or3. with scleral infiltration. High dose chemotherapy for
12 cycles is used in patients with extrascleral extensionand optic nerve extension to transection.
c. High dose chemotherapy for 12 cycles in patients with1. extrascleral extension2. optic nerve extension to transection.
Extraocular disease may be localized to the soft tissuessurrounding the eye or to the optic nerve beyondthe margin of resection. However, further extensionmay occur into the brain and meninges withsubsequent seeding of the spinal fluid, as well asdistant metastatic disease involving the lungs, bones,and bone marrow. High dose chemotherapy for 3 to6 cycles are given and disease is reassessed.Enucleation is performed followed by orbital externalbeam radiation therapy. Further, high dosechemotherapy is continued for total 12 cycles. Inextraorbital retinoblastoma, palliative therapy withradiation (including craniospinal irradiation whenthere is meningeal involvement) and/or intrathecalchemotherapy with methotrexate, cytarabine, andhydrocortisone, plus supportive care have been used(Tables 4 and 5).
therapy and local therapy, diffuse vitreousseeds, recurrent after chemotherapy, postenucleation (Scleral involvement, extraocularextension, optic nerve involvement). External-beam radiation with dose ranges from 3,500 to4,600 cGy. Special expertise is very essential totreat pediatric ocular and orbital tumors. Newermethods of delivering external-beam radiationare being used in an attempt to reduce adverselong-term effects. This includes intensity-modulated radiation therapy (IMRT),stereotactic radiation therapy, and proton-beamradiation therapy.19
7. Brachytherapy with radioactive plaques. Theseare radioactive plaques in concave shapes, eitherbeta or gamma emitting. The commonly usedradioactive sources are Iodine125, Gold,Iridium192 and Ruthenium106. Ruthenium and125I plaque therapy is preferred because of itsfavorable physical properties.20,21 They are usedfor either focal unilateral presentations orrecurrent disease following previous external-beam radiation. Indications of brachytherapyare lesion < 16 mm in basal diameter, < 8 mm inthickness, adjuvant to chemo reduction, failureof local therapy.
Table 2: Management of intraocular retinoblastomagroup I to IV-B
a. Focal therapy alone when appropriateb. Standard chemoreduction × 6 cycles + appropriate
sequential focal therapyc. Chemocryotherapy at each cycled. Standard chemoreduction × 12 cycles, when suboptimal
regression with chemotherapy at 6 cycles and RT is notfeasible (e.g. age < 1year)
e. Alternative chemotherapy regimen or RT when there isno regression after 3 cycles of standard chemotherapyor recurrence during chemotherapy.
Table 3: Management of intraocular retinoblastomagroup V-A and V-B
a. Unilateral – Primary enucleationb. Bilateral–High dose chemotherapy × 6 cycles +
appropriate sequential focal therapyc. Chemocryotherapy at each cycled. Periocular Carboplatin augmentation for group V-Be. High dose chemoreduction × 12 cycles when suboptimal
regression with chemotherapy at 6 cycles and RT is notfeasible (e.g. age < 1year)

352352352352352 Surgical Atlas of Orbital DiseasesSurgical Atlas of Orbital DiseasesSurgical Atlas of Orbital DiseasesSurgical Atlas of Orbital DiseasesSurgical Atlas of Orbital Diseases
With emerging dose-intensive chemotherapyregimens and the use of high-dose chemotherapywith autologous stem cell rescue, clinical trials areongoing to improve the dismal outcome for thisrelatively small group of patients. The agents usedin the past included vincristine, cyclophosphamide,and doxorubicin; although they produce an initialresponse, overall survival has been less than optimal.Carboplatin, ifosfamide, and etoposide have shownmore promise for remission and may be used inconjunction with high-dose chemotherapy followedby stem cell rescue. Patients presenting withextensive non-CNS metastases have been treatedsuccessfully with myeloablative chemotherapy withstem cell rescue.
Ocular Metastasis
Intraocular metastasis is now considered the mostcommon malignancy of the eye. The frequency ofocular metastasis varies significantly among primarysites. Ocular metastasis, and particularly choroidalmetastasis, can precede the diagnosis of the primarymalignancy. Lung cancer is the most common primarytumor (35 and 41%) detected in patients with noneoplasm at the time of ocular diagnosis followedby breast cancer, leukemia, lymphoma, multiplemyeloma and sarcoma. Rarely metastases frommalignancies of prostate, cervix, thyroid, skin, GItract and kidney can occur.
A number of options are available for the therapyof ocular metastasis, including observation,chemotherapy, photocoagulation, cryosurgery,surgical resection, or radiotherapy. The specifictherapy chosen for a patient is an individualizedprocess that considers the clinical condition of thepatient. The most commonly applied treatment isexternal-beam radiotherapy. In general, 30 to 40 Gyin 10 to 20 fractions could be considered a standardcourse of radiotherapy. For patients with a long lifeexpectancy, a higher total dose with lower dose perfraction can be considered.
Orbital Tumors
Pediatric primary orbital masses include dermoidcyst, capillary hemangioma and lymphangioma,inflammatory lesions, lymphocytic and leukemicinfiltrates, and pilocytic astrocytoma of the opticnerve, rhabdomyosarcoma and primary neuro-ectodermal tumor or Ewing's sarcoma. In adults, the
most common localized tumors of the orbit includecavernous hemangioma, fibrous histiocytoma,schwannoma, orbital pseudotumor, Grave's ophthal-mopathy and hemangiopericytoma. The mostcommon lacrimal gland tumors include pleomorphicadenoma and adenoid cystic carcinoma.
Rhabdomyosarcoma
Orbital rhabdomyosarcoma is treated with com-bination of chemotherapy and radiation therapy afterlocal excision or biopsy. Chemotherapy is usuallygiven for 2 to 3 cycles prior to the initiation ofradiation therapy, with the exception of patients withparameningeal disease and evidence of meningealextension in whom radiation therapy generallybegins as soon as possible. Vincristine,cyclophosphamide, doxorubicin, actinomycin-D,ifosfamide and etoposide are the drugs used for thetreatment of RMS. Radiation therapy is effective forachieving local control of tumor for patients withmicroscopic or gross residual disease followingbiopsy, initial surgical resection, or chemotherapy.The radiation therapy dose depends predominantlyon the extent of disease following the primarysurgical resection. Patients with completely resectedtumors (group I) of embryonal histology do wellwithout radiation therapy but radiation therapybenefits patients with group I tumors with alveolaror undifferentiated histology.22-24 In general, patientswith microscopic residual disease (group II) receiveradiation therapy to approximately 4,100 cGy.25
Patients with gross residual disease (group III) shouldreceive radiation dose of 5,040 cGy. The treatedvolume should be determined by the extent of tumorat diagnosis prior to surgical resection and prior tochemotherapy. A margin of 2 cm is generally used,including clinically involved nodes. Precautionsshould be taken to limit the dose to the lens, cornea,lacrimal gland, and optic chiasm.
Orbital Lymphoma
Most of the orbital lymphomas are confined to theorbit and are of low grade. Patient needs a stagingworkup (CBP, chest X-ray, USG abdomen, or CT scanof chest and abdomen, serum LDH, Bone marrowbiopsy and CSF cytology) to rule out systemiclymphoma. Radiotherapy is a well-establishedtreatment modality for orbital lymphoma. Primarychemotherapy has minimal efficacy in localized low-

Management of Ophthalmic Tumors: Role of Chemotherapy and Radiation TherapyManagement of Ophthalmic Tumors: Role of Chemotherapy and Radiation TherapyManagement of Ophthalmic Tumors: Role of Chemotherapy and Radiation TherapyManagement of Ophthalmic Tumors: Role of Chemotherapy and Radiation TherapyManagement of Ophthalmic Tumors: Role of Chemotherapy and Radiation Therapy 353353353353353
grade orbital lymphoma and thus is not advocatedas a first-line treatment. There have been numerousseries advocating low dose radiation for treatmentof orbital lymphomas. In general, radiation dose of3000 cGy is recommended for low grade lymphomasand 4000-4500 cGy for intermediate gradelymphomas.26,27 If it is associated with systemicdisease, it is treated with chemotherapy constitutingcyclophosphamide, doxorubicin, vincristine andprednisolone for 6 cycles followed by local radiationtherapy.
Idiopathic Orbital Inflammation (IOI)
Idiopathic Orbital Inflammation could be inflam-matory, reactive lymphoid hyperplasia or atypicallymphoid hyperplasia. Corticosteroids have been therecommended initial drug (prednisone 1 mg/kg/d),Recently, antimetabolites (azathioprine, metho-trexate, and leflunomide), T-cell inhibitors(cyclosporine and tacrolimus), and alkylating agents(cyclophosphamide and chlorambucil) were shownto be useful in the management of NSOI in differentseries.28 Use of low-dose external beam radiation2000 cGy demonstrated a 50 to 80% efficacy in aprevious series.29
Grave's Ophthalmopathy
Severe exophthalmos may occur in some patientswith thyrotoxicosis with involvement of extraocularmuscles. Indications for therapy are corneal exposurewhich may cause corneal ulceration that progress toscarring, optic nerve compression. CT scan showsthickened extraocular muscles. Steroids and diureticsare the first-line treatment, administered for 2 weeks.Radiation dose of 2000 cGy in 10 fractions providesgood symptomatic relief avoiding the need forfurther steroid therapy or surgical decompression.30
Optic nerve Meningioma
The diagnosis of optic nerve meningioma is usuallypresumptive and based on the appropriate clinicalpicture supported by appropriate neuroimaging.Biopsy is not routinely advocated, as surgicalintervention carries significant morbidity andmortality. Patients often undergo reimaging at 3months, and they are followed radiographically at 6to 12 month intervals after the disease has stabilized.Treatment strategy should be individualized.
Radiation therapy is recommended as soon as serialexamination documents a new decline in acuity and/or visual field. Tumor enlargement without loss ofvisual function, as determined by serial imaging, mayalso provide an indication for radiotherapy.Recommended dose of radiation therapy is5400 cGy.31 It should preferably be delivered viafractionated, 3-dimensional stereotactic and IMRTtechniques that provide the most precise conformalapplication of the dose to affected tissues.Theoretically, this approach should reduce the riskof side effects to surrounding radiosensitive ocularand neural tissues.
Optic Nerve Glioma
Chemotherapy is the first-line treatment, followedby radiation if chemotherapy fails. Standardchemotherapy for optic-pathway gliomas consists ofvincristine and carboplatin, whereas second-linetherapy is often thioguanine, procarbazine, andvincristine.32 When these fail, chemotherapeuticagents used in other progressive low-grade gliomascan be considered. These include cyclophosphamide,topotecan, and oral VP-16.Stabilization or improve-ment in visual function and tumor size is considereda response to treatment. Surgery has a limited role.Biopsies are performed when clinical and radiologicfeatures are atypical. Radiation therapy dose above5000 cGy is required for tumor control. Optic-nervegliomas should be operated upon only when grosslyproptotic and the eye is blind or near blind. In largeseries from the Mayo Clinic with a median follow-up time of 10 years, patients with glioma confined tothe optic nerve survived almost twice as long as thosewith involvement of optic chiasm.33
Sequelae of Radiation Therapy34-38
Postradiotherapy complications can be classified asacute (usually occurring within 3 months of treatment)or late (occurring many months to years aftercompletion of treatment). Acute lesions generallyaffect rapidly proliferating cells, and most can bereversed by appropriate medical management. Suchacute effects involving the ocular anterior segmentinclude blepharitis, conjunctivitis, and keratitis.However, residual stromal lesions and interstitialfibrosis may follow. Late effects are primarily causedby permanent vascular damage and resultant

354354354354354 Surgical Atlas of Orbital DiseasesSurgical Atlas of Orbital DiseasesSurgical Atlas of Orbital DiseasesSurgical Atlas of Orbital DiseasesSurgical Atlas of Orbital Diseases
Table 6: Radiation effects on the eye and orbital tissues
Eye lashes and Eyelid Spared by megavoltage (Cobalt, LA)Becomes thinner; function not alteredLash loss at 40–60 GyTelangiectasia at 55 Gy
Lacrimal system Dryness in 8-25% pts at 30 to 45 GyDryness in all pts over 4-8 yrs at >55 GyAtrophy at 50–60 GyStenosis at 65–75 Gy
Lens E B R T Single dose 2 Gy -CataractFractionated 8 Gy Cataract in 33% of pts> 11 Gy – Cataract in 100% of pts< 50 Gy – Cataract; vision not impaired> 60 Gy – Vision impairing cataracts
Plaque 50 Gy at limbus 33% cataracts
Conjunctiva Conjunctivitis at 55–75 GyTelangiectasia at 30 Gy
Cornea Superficial keratitis- edema, epithelialdefects at 30–50GySevere keratitis – Ulcer, scarring, perforation> 60Gy
Retina 40-60 Gy – retinopathy 10%> 60 Gy – retinopathy 30%CRA thrombosis may lead to edema andpallor of optic disc, retinal hemorrhages,blindness in 2-3 years
Optic nerve Neuropathy at >55 Gy
ischemia. Retinopathy, cataract, and optic neuro-pathy are examples of such late effects. (Table 6)Keratoconjunctivitis sicca, another late sequela toradiotherapy, may often be clinically nonmanifest orinsignificant but can result in ulcerative thinning andcorneal perforation.
Eyelid and periorbital skin radiation effects canbe acutely controlled with topical corticosteroids,wound debridement, and antibiotic therapy.Occasionally, reconstructive surgery is indicated totreat lid deformities. Patients should be encouragedto wear ultraviolet protective sunscreens and avoidusing harsh soaps and lotions.
Nasolacrimal duct occlusion may require siliconeintubation or dacrycryocysto-rhinostomy, whereassevere lacrimal punctal stenosis may necessitate aconjunctivo-dacryocystorhinostomy.
Severe noninfectious inflammation may requirea short course of corticosteroid therapy, butindiscriminate use of steroids should be avoidedbecause it can promote extracellular matrix
breakdown. Prolonged ocular surface inflammationor ulceration frequently requires prophylacticantibiotics. Artificial tears and ointments areindicated for dry eye relief. It is important torecognize that the irradiated cornea often has a poorcapacity to heal, despite neovascularization, becauseof the degree of epithelial toxicity. Mild punctatekeratopathy needs aggressive lubrication. Tearreplacement therapy with nonpreserved artificialtears and ointments facilitates epithelial woundhealing.
Infected corneal ulcers require prompt diagnosticand therapeutic measures, with initiation of broad-spectrum antibiotics modified as needed on cultureand susceptibility results. Although hydrophilic softcontact lenses can be used as protective bandagingto promote corneal healing, they may not be welltolerated in severe dry eyes; furthermore, they mayincrease the risk of an infection in patients whoare often additionally immunosuppressed bychemotherapy. Gas-permeable glued-on contactlenses have been used to treat radiation-inducedkeratitis effectively, but experience with this islimited. If necessary, a conjunctival flap can controlsevere pain caused by persistent corneal defects.
REFERENCES
1. Jacobeic FA, Jones IS. Vascular tumours, malformationsand degenerations. In: Duan TD, ed. Clinicalophthalmology, vol 2. Hagerstown, MD: Haper and Row,1976;1-40.
2. Fitzpatrick PJ, Thompson GA, Easterbrook WM, Gallie BL,Payne DG. Basal and squamous cell carcinoma of the eyelidsand their treatment by radiotherapy. Int J Radiat OncolBiol Phys. 1984;10(4):449-54.
3. Luxenberg MN. Sebaceous gland carcinoma. ArchOphthalmol 1988;106:119.
4. Tan KC, Lee ST, Cheah ST. Surgical treatment of sebaceouscarcinoma of eyelids with clinico-pathological correlation.Br J Plast Surg 1991;44:117-21.
5. Pardo FS, Wang CC, Albert D, et al. Sebaceous carcinomaof the ocular adnexa: radiotherapeutic management. Int JRadiat Oncol Biol Phys 1989;17:643-7.
6. Meldrum ML, Tse DT, Benedetto P. Neoadjuvantintracarotid chemotherapy for treatment of advancedadenocystic carcinoma of the lacrimal gland. ArchOphthalmol. 1998;116(3):315-21.
7. Tse DT, Benedetto P, Dubovy S, Schiffman JC, Feuer WJ.Clinical analysis of the effect of intraarterial cytoreductivechemotherapy in the treatment of lacrimal gland adenoidcystic carcinoma. Am J Ophthalmol. 2006.

Management of Ophthalmic Tumors: Role of Chemotherapy and Radiation TherapyManagement of Ophthalmic Tumors: Role of Chemotherapy and Radiation TherapyManagement of Ophthalmic Tumors: Role of Chemotherapy and Radiation TherapyManagement of Ophthalmic Tumors: Role of Chemotherapy and Radiation TherapyManagement of Ophthalmic Tumors: Role of Chemotherapy and Radiation Therapy 355355355355355
8. Journée-de Korver JG,Keunen JEE. Thermotherapy in themanagement of choroidal melanoma. Prog Retin Eye Res.2002;21:303- 17.
9. Shields CL, Cater J, Shields JA. Combined plaqueradiotherapy and transpupillary thermotherapy forchoroidal melanoma: tumor control and treatmentcomplications in 270 consecutive patients. Arch Ophthalmol.2002;120:933-40.
10. Nath R, Anderson LL, Luxton G, et al. Dosimetry ofinterstitial brachytherapy sources: recommendations of theAAPM Radiation Therapy Committee Task Group No 43.American Association of Physicists in Medicine. Med Phys.1995;22:209-34.
11. Jorge E Freire, Luther W. Brady. Jerry A. Shields, Carol L.Shields, Eye and Orbit, Principles and practice of RadiationOncology, (4th ed), 2004;876-96.
12. Shields CL, Santos MC, Diniz W, et al.: Thermotherapy forretinoblastoma. Arch Ophthalmol 1999;117 (7): 885-93.
13. Friedman DL, Himelstein B, Shields CL, et al.Chemoreduction and local ophthalmic therapy forintraocular retinoblastoma. J Clin Oncol 18 (1): 12-7, 2000.
14. Shields CL, Honavar SG, Meadows AT, et al.Chemoreduction plus focal therapy for retinoblastoma:factors predictive of need for treatment with external beamradiotherapy or enucleation. Am J Ophthalmol 2002;133(5): 657-64.
15. Lumbroso L, Doz F, Urbieta M, et al.: Chemothermo-therapy in the management of retinoblastoma.Ophthalmology 2002;109(6):1130-6.
16. Gombos DS, Kelly A, Coen PG, et al.: Retinoblastomatreated with primary chemotherapy alone: the significanceof tumour size, location, and age. Br J Ophthalmol 2002;86(1): 80-3.
17. Abramson DH, Frank CM, Dunkel IJ: A phase I/II study ofsubconjunctival carboplatin for intraocular retinoblastoma.Ophthalmology 1999;106(10):1947-50.
18. Villablanca JG, Jubran R, Murphree AL: Phase I study ofsubtenon carboplatin I with systemic high dosecarboplatin/etoposide/vincristine (CEV) for eyes withdisseminated intraocular retinoblastoma (RB). [Abstract]Proceedings of the XIII Biannual Meeting of ISGED and theX International Symposium on Retinoblastoma, 2001, FortLauderdale, Fla. USA.
19. Krasin MJ, Crawford BT, Zhu Y, et al.: Intensity-modulatedradiation therapy for children with intraocularretinoblastoma: potential sparing of the bony orbit. ClinOncol (R Coll Radiol) 2004;16 (3): 215-22.
20. Shields CL, Shields JA, Cater J, et al.: Plaque radiotherapyfor retinoblastoma: long-term tumor control and treatmentcomplications in 208 tumors. Ophthalmology2001;108(11):2116-21.
21. Merchant TE, Gould CJ, Wilson MW, et al.: Episcleral plaquebrachytherapy for retinoblastoma. Pediatr Blood Cancer2004;43(2):134-9.
22. Maurer HM, Beltangady M, Gehan EA, et al.: The IntergroupRhabdomyosarcoma Study-I. A final report. Cancer1988;61(2):209-20.
23. Maurer HM, Gehan EA, Beltangady M, et al.: The IntergroupRhabdomyosarcoma Study-II. Cancer 1993;71 (5):1904-22.
24. Wolden SL, Anderson JR, Crist WM, et al.: Indications forradiotherapy and chemotherapy after complete resectionin rhabdomyosarcoma: A report from the IntergroupRhabdomyosarcoma Studies I to III. J Clin Oncol 1999;17(11):3468-75.
25. Raney R, Hays D, Tefft M, et al.: Rhabdomyosarcoma andthe undifferentiated sarcomas. In: Pizzo PA, Poplack DG,Eds.: Principles and Practice of Pediatric Oncology.Philadelphia: JB Lippincott, 1989;635-58.
26. Esik O, Ikeda H, Mukai K, Kaneko A. A retrospectiveanalysis of different modalities for treatment of primaryorbital non-Hodgkin's lymphomas. Radiother Oncol 1996;38:13-8.
27. Jorge E Freire, Luther W. Brady. Jerry A. Shields, Carol L.Shields, Eye and Orbit, Principles and practice of RadiationOncology, (4th ed) 2004;876-96.
28. Cockerham KP, Hong SH, Browne EE: Orbitalinflammation. Curr Neurol Neurosci Rep 2003;3:401-9.
29. Smitt MC, Donaldson SS: Radiation therapy for benigndisease of the orbit. Semin Radiat Oncol 1999;9:179-89.
30. Sandler HM, Rubenstein JH, Fowble BL, Sergott RC, SavinoPJ, Bosley TM, Results of radiotherapy for thyroidophthalmopathy. Int J Radiat Oncol Biol Phys.1989;17(4):823-7.
31. Tsao MN, Hoyt WF, Horton J, et al. Improved visualoutcome with definitive radiation therapy for optic nervesheath meningioma. Int J Radiat Oncol Biol Phys.1991;45S:324-25.
32. Jahraus CD, Tarbell NJ. Optic pathway gliomas. PediatrBlood Cancer 2006;46:586-96.
33. Rush JA, Younge BR, Campbell RJ, et al. Optic glioma:long-term follow-up of 85 histopathologically verified cases.Opthalmology 1982;89:1213-9.
34. Brady LW, Shields J, Augsburger J et al. Complicationsfrom radiotherapy to the eye. Front Radiat Ther Oncol1989;23:238-50.
35. Servodido CA, Abramson DH. Acute and long-term effectsof radiation to the eye in children. Cancer Nurs 1993; 16:371-81.
36. Merriam GR, Szechtzer A, Focht EF. Theeffects of ionizingradiations to the eye. Front Radiat Ther Oncol 1972; 6:346-85.
37. Monroe AT, Bhandare N, Morris CG, Mendenhall WM.Preventing radiation retinopathy with hyperfractionation.Int J radiat Oncol Biol Phys 2005; 61: 856-64.
38. Bhandare N, Monroe AT, Morris CG et al. Does alteredfractionation influence therisk of radiation-induced opticneuropathy? Int J radiat Oncol Biol Phys 2005;62:1070-7.

356356356356356 Surgical Atlas of Orbital DiseasesSurgical Atlas of Orbital DiseasesSurgical Atlas of Orbital DiseasesSurgical Atlas of Orbital DiseasesSurgical Atlas of Orbital Diseases
D Ravi Varma, D Radhika Varma
Carotid-Cavernous Fistulae:Carotid-Cavernous Fistulae:Carotid-Cavernous Fistulae:Carotid-Cavernous Fistulae:Carotid-Cavernous Fistulae:Role of InterventionalRole of InterventionalRole of InterventionalRole of InterventionalRole of Interventional
RadiologistRadiologistRadiologistRadiologistRadiologist
The cavernous segment of the carotid artery is unique,as it is the only anatomical location in the body wherean artery is completely surrounded by a venousstructure. Carotid-cavernous fistulae (CCF) arespontaneous or acquired communications betweenthe carotid artery and the cavernous sinus withoutan intervening capillary bed. The arterial supply tothese lesions may come from the internal carotidartery (ICA), from the dural branches of externalcarotid artery (ECA), or from both. The cavernoussinus, being at the crossroads of the cranial and facial
Figure 26.1: Arterial and venous anatomy around the cavernous sinus
venous circulations, has rich communications withthe facial veins through the superior and inferiorophthalmic veins, with the transverse and sigmoidsinuses through the superior and inferior petrosalsinuses, with the cerebral cortical veins through thesphenoparietal sinus and with the pterygoid plexus(Figure 26.1). Thus these lesions can have a widerange of clinical presentations, the severity of whichis dependent not only on the volume of flow acrossthe fistula site, but also on the adequacy andpreferred pathway of venous drainage.
1. Common carotid artery,2. Internal carotid artery,3. External carotid artery,4. Dural branches of external carotid artery supplying the
cavernous sinus,5. Cavernous segment of internal carotid artery,6. Dural branches of internal carotid artery (meningio-
hypophyseal trunk and inferior cavernous sinus artery),7. Cavernous sinus,8. Superior petrosal sinus,9. Inferior petrosal sinus,
10. Superior ophthalmic vein,11. Inferior ophthalmic vein,12. Facial vein,13. Pterygoid venous plexus,14. Sphenoparietal sinus,15. Superior sagittal sinus,16. Deep venous system,17. Transverse sinus,18. Sigmoid sinus,19. Internal jugular vein.
26C H A P T E R

Carotid-Cavernous Fistulae: Role of Interventional RadiologistCarotid-Cavernous Fistulae: Role of Interventional RadiologistCarotid-Cavernous Fistulae: Role of Interventional RadiologistCarotid-Cavernous Fistulae: Role of Interventional RadiologistCarotid-Cavernous Fistulae: Role of Interventional Radiologist 357357357357357
The widely used system to classify CCF is based ontheir angioarchitecture. Barrow in 1985 classifiedthese lesions based on their arterial supply1 (Figures26.2A to C). Type A CCF are direct fistulae betweenthe ICA and the cavernous sinus, and are mostcommonly secondary to trauma. Type B, type C andtype D CCFs, are low flow indirect fistulae wheremultiple microfistulae are located within the wall ofthe cavernous sinus and drain into it. The arterialsupply to these lesions may originate from the duralbranches of ICA (Type B), dural branches of ECA(Type C) or from dural branches of ICA and ECA(Type D). (The salient features differentiating directand indirect CCF are depicted in Table 1).
PATHOPHYSIOLOGY
The elevated pressure in the cavernous sinus leadsto dramatic orbital changes as the superior andinferior orbital veins are devoid of valves. Thoughmost obvious manifestations of CCF are reflected inthe eye, we should not forget to look for other lessevident changes which may be vital clues to thediagnosis, or may result in disaster if overlooked.
Symptoms such as headache may indicate elevationof cerebral cortical venous pressure and mayresult in potentially fatal complications such ascerebral edema, intracerebral or subarachnoidhemorrhage. The pathophysiological mechanismsbehind the common clinical symptoms are detailedin Figure 26.3.
Clinical Features
CCF that have principal drainage into the superiorand inferior ophthalmic veins, present withpredominant orbital symptoms.2 Though mostpatients have orbital symptoms on the same side asthe fistula, we have seen several patients withunilateral CCF in whom the orbital symptoms werepresent on the contralateral side, or even on bothsides, depending on the available paths of venousdrainage (Figure 26.2C). The symptoms and clinicalsigns of CCF and their relative incidence are listedin Table 2.2,5
The clinical signs may be difficult to differentiatefrom other sequelae of craniocerebral trauma suchas orbital hematomas and cranial nerve injuries. Thereshould be a high index of suspicion when a patient
Figures 26.2A to C: Barrow classification of CCF
(A) Type A CCF: Internal carotid angiogram in lateral projection reveals opacification of cavernous sinus (arrow) and retrograde flow in thesuperior ophthalmic vein (double arrow), through a rent in the arterial wall. Note that there is immediate opacification of the entirecavernous sinus and superior ophthalmic vein during the arterial phase as is common with these high flow lesions
(B) Type B CCF: Internal carotid angiogram in lateral projection reveals opacification of cavernous sinus (double arrow) through small duralbranches (arrow) arising from the cavernous segment of internal carotid artery. In these lesions, there is a significant delay inopacification of the cavernous sinus and its draining veins – suggesting a slow flow across the fistula
(C) Type C CCF: Right external carotid angiogram in frontal projection reveals opacification of the right and left cavernous sinuses (arrows)through multiple small dural branches of the middle and accessory meningeal arteries (double arrow). Though the CCF was located onthe right side, this middle aged lady was symptomatic in the left eye as the predominant venous drainage was through the left superiorophthalmic vein.Type D CCF has arteriovenous fistulae with supply from dural branches of internal and external carotid arteries
A B C

358358358358358 Surgical Atlas of Orbital DiseasesSurgical Atlas of Orbital DiseasesSurgical Atlas of Orbital DiseasesSurgical Atlas of Orbital DiseasesSurgical Atlas of Orbital Diseases
presents with orbital symptoms after a head injury.The low flow at the shunt and nonspecific nature ofsymptoms makes indirect CCF even more difficultto diagnose. A useful clinical test to identify these
Figures 26.3: Pathophysiology of CCF
lesions is to look for reduction of symptomswith digital compression of the carotid artery in theneck.
Table 1: Comparison of direct and indirect CCF
Direct Indirect
Sex prediliction Male (Higher incidence of trauma) Commoner in femaleEtiology — Trauma (commonest) — Spontaneous (commonest)
— Ruptured cavernous ICA aneurysm — Cause unknown— Surgical trauma — Predisposing factors— Ehler’s Danlos syndrome • Cavernous sinus thrombosis— Fibromuscular dysplasia • Pregnancy— Arterial dissection • Trauma— Idiopathic • Sphenoid sinusitis
Pathology Rent in the wall of the cavernous segment Abnormal small dural arterio-venous shunts in the wall ofof internal carotid artery the cavernous sinus
Hemodynamics Usually high flow Usually low flowArterial supply and Barrow Cavernous segment of ICA — Dural branches of ICA (Type B)Classification Type (Type A) — Dural branches of ECA (Type C)
— Combination of dural branches of ECA and ICA (Type D)Symptoms May be abrupt following trauma or may Usually insidious onset, with slow progression
present after a delay of days or weeks.Usually progress rapidly.
Spontaneous closure Extremely rare May be achieved in 34-60% by conservative management

Carotid-Cavernous Fistulae: Role of Interventional RadiologistCarotid-Cavernous Fistulae: Role of Interventional RadiologistCarotid-Cavernous Fistulae: Role of Interventional RadiologistCarotid-Cavernous Fistulae: Role of Interventional RadiologistCarotid-Cavernous Fistulae: Role of Interventional Radiologist 359359359359359
Table 2: When to suspect CCFPast History• Craniocerebral trauma• Cavernous sinus thrombosis• Connective tissue disorders
Symptoms Signs• Swollen red eye • Proptosis• Orbital pain • Ptosis• Diplopia • Chemosis• Progressive vision loss • Cranial nerve palsies• Headache • Elevated intraocular pressure• Pulsatile tinnitus • Papilledema
• Optic nerve atrophy
Rare presentations• Neurological deficits• Intraparenchyma / Subarachnoid bleed• Epistaxis
CASE ILLUSTRATION (Figure 26.4)
Radiological InvestigationsIn a patient with clinical features of CCF, contrastenhanced CT scan is most often adequate to confirmthe diagnosis. In addition to the characteristic orbitaland cavernous sinus features (Figures 26.5A to C),skull base fractures and bony spicules aredemonstrated. Though CT angiography, MRI andMR angiography (Figures 26.6A to C) elegantlydemonstrate the abnormality, they add little in termof diagnosis or treatment planning, as the exact siteof fistula and hemodynamics of flow across it are
Figure 26.4: Clinical features of CCF. Mr. P (same patient as in Figure26.2A) was referred to us with proptosis of left eye that progressedover 4 months following a road traffic accident. Note the proptosis,orbital congestion and conjunctival chemosis. He had elevatedintraocular pressure and had lost vision in the left eye. As is commonin most patients with CCF, his presenting complaints were limited tothe orbit. Only on specific queries, he admitted that he often heard apulsatile "whooshing" sound in the left ear and that he had severeheadaches that appeared after the head injury
Figures 26.5A to C: CT scan findings in CCF Plain (A) and contrast enhanced (B) axial CT scans of the orbit in a 24-year-man with post-traumatic direct CCF, reveal proptosis (arrow), enlarged extraocular muscles (arrow heads) and prominent cavernous sinus (double arrow)on the left side. Dilatation of the superior ophthalmic vein (double arrowhead) should be specifically looked for in such cases (B) as it may bethe only indicator of an underlying vascular abnormality. This characteristic appearance has been termed as the "Hockey stick" sign.
Coronal CT scan (C) in another patient with post-traumatic direct CCF, reveals enlarged extraocular muscles (arrow heads) and dilatedsuperior ophthalmic vein (arrow) in the right eye. In subtle cases, comparison with the normal structures in the contralateral orbit will help inidentification
A B C
rarely demonstrated. Duplex Doppler studies of theorbit are useful in follow-up of lesions that are onconservative management or have undergone partialocclusion.
Definitive planning of treatment requires digitalsubtraction angiography with selective injections ofthe internal and external carotid arteries on eitherside. Information regarding the arterial supply, siteand size of the fistula, volume of flow across thefistula, patency of cavernous sinus, pattern of venousdrainage and adequacy of collateral circulation at thecircle of Willis can be obtained on this study.

360360360360360 Surgical Atlas of Orbital DiseasesSurgical Atlas of Orbital DiseasesSurgical Atlas of Orbital DiseasesSurgical Atlas of Orbital DiseasesSurgical Atlas of Orbital Diseases
Figures 26.6A to C: MR and MR Angiographic features of CCF. 21-year-old man with history of head injury presented with pulsatile proptosis.Axial T2 (A) and T1 (B) weighted MR scans of the brain reveal dilatation of the superior ophthalmic vein (arrow) and prominence of cavernoussinus (double arrow) on left side. On MRI, high velocity blood flow produces "flow voids" within blood vessels that usually appear black on allsequences.
Basal projection of MR Angiogram (C) reveals flow from the left internal carotid artery (arrow) into the left cavernous sinus (double arrow).The cavernous sinus is seen to drain into inferior petrosal sinuses (arrow head) and superior ophthalmic veins (double arrowhead) on eitherside
A B C
Management of CCFManagement of CCF must start with treating itssecondary manifestations such as glaucoma.Aggressive medical management of the elevatedintraocular pressure with adrenergic blockers oracetazolamide should be started while definitivetreatment should be directed towards closing thefistula. Surgical measures such as lateral canthotomyor tarsorrhaphy may be used to decompress the orbitand to prevent exposure keratopathy.
Direct CCFHigh flow lesions such as Type A CCF usuallyprogress rapidly and may result in vision loss,ophthalmoplegia, elevated intracranial pressure andintracranial hemorrhage. Spontaneous thrombosis isextremely rare and these lesions must be managedwithout delay. The indications of emergencytreatment4 of CCF are listed in Table 3.
Surgical ligation of the carotid artery isineffective in treating these lesions and may infactworsen the neurological symptoms, as the fistulasteals blood from the intracranial circulation. On theother hand, endovascular management seals off thefistula and preserves the patency of the carotid artery.
Table 3: Indications for emergency management of CCF
Clinical features• Epistaxis• Elevated intracranial pressure• Progressive proptosis• Diminishing visual acuity• Intraocular pressure > 40 mm Hg• Transient ischemic attacks
Imaging features• Presence of cortical venous drainage• Pseudoaneurysm / cavernous sinus varix
Occlusion of the fistula using silicone or latexdetachable balloons is the treatment of choice fordirect CCF3 (Figures 26.7A to F). These balloons arenegotiated through the rent in the wall of the artery,into the cavernous sinus and are inflated so as toseal off the fistula. After confirming satisfactoryposition of the balloon and verifying the patency ofthe carotid artery, the balloon is detached (Figures26.8A to L). Though these balloons eventually deflate,they occlude the fistula long enough to causethrombosis within the fistula and cavernous sinus.Transarterial balloon embolization has been reportedto be successful in 80-90% of cases.

Carotid-Cavernous Fistulae: Role of Interventional RadiologistCarotid-Cavernous Fistulae: Role of Interventional RadiologistCarotid-Cavernous Fistulae: Role of Interventional RadiologistCarotid-Cavernous Fistulae: Role of Interventional RadiologistCarotid-Cavernous Fistulae: Role of Interventional Radiologist 361361361361361
Figures 26.7A to F: Technique of detachable balloon embolization of CCF. The delivery catheter (A) is 165 cm long. The stiff proximal shaft is0.86 mm in diameter while the distal supple part is 0.57 mm in diameter. (B) The valve of the detachable balloon is threaded onto the tip of thedelivery catheter and the assembly (C) is introduced into the carotid artery. Once the balloon crosses the fistula and enters the cavernoussinus, it is inflated by injecting contrast medium into the hub (D), so that the balloon takes the shape of the cavernous sinus (E) and occludes theorifice of the fistula. Once satisfactory occlusion of the fistula is achieved, the balloon is detached by gentle traction on the delivery catheter (F)
Figures 26.8B and C: His brain CT (B) revealed a prominent superior ophthalmic vein (double arrowheads) on right side. Diagnostic rightinternal carotid angiogram (C) showed opacification of cavernous sinus (bold arrow), with absent flow into distal branches of internal carotidartery. From the cavernous sinus, blood was seen to flow retrogradely through the superior ophthalmic vein (double arrowheads) into theorbit, into the inferior petrosal sinus (long arrow) and into cortical veins (double arrows). As he had high flow towards the orbit and significantflow into the cortical veins, we planned emergency endovascular management. Such large hole direct CCF are best treated with trans-arterialembolization using detachable balloons
B C
Figure 26.8A: 29-year-old man who was operated for a traumaticextradural hematoma, presented 8 months later, with proptosis, diplopiaand right sided headache. He had loud bruit on auscultation over theright orbit. Note the ptosis, proptosis and lateral deviation of eyeballon the right side

362362362362362 Surgical Atlas of Orbital DiseasesSurgical Atlas of Orbital DiseasesSurgical Atlas of Orbital DiseasesSurgical Atlas of Orbital DiseasesSurgical Atlas of Orbital Diseases
Figures 26.8D and E: We threaded a detachable balloon (9 x 14 mm size) onto a delivery catheter (D)and introduced the assembly (arrow) through a guiding catheter (arrow heads) into the internal carotid artery (E)
D E
Figures 28.8F to H: We negotiated the balloon across the orifice of the fistula and placed it in the cavernous sinus (arrow head). We slowlyinflated the balloon with contrast medium, with frequent check angiograms (F). On complete inflation of the balloon, though we could achievecessation of flow in the cortical veins, flow persisted in the superior ophthalmic vein as seen on check angiogram (G) and follow-up Dopplerstudy (H)
Figures 26.8I and J: We negotiated another detachable balloon (arrow head) through the fistula into the anterior part of the cavernous sinus(I) and inflated it so that flow in the superior ophthalmic vein was arrested (J). The ophthalmic artery (arrow) and intracranial branches ofinternal carotid artery (arrow heads) are seen to fill now
F G H
I J

Carotid-Cavernous Fistulae: Role of Interventional RadiologistCarotid-Cavernous Fistulae: Role of Interventional RadiologistCarotid-Cavernous Fistulae: Role of Interventional RadiologistCarotid-Cavernous Fistulae: Role of Interventional RadiologistCarotid-Cavernous Fistulae: Role of Interventional Radiologist 363363363363363
Figures 26.8K and L: In the weeks following the embolization we confirmed the absence of flow in the superior ophthalmic vein on follow-up Doppler studies of the orbit (K). Though Doppler gives us information only about the orbital component of CCF, it is an inexpensive and reliablemodality to confirm the efficacy of treatment. Plain radiograph of the skull performed a month after treatment (L) showing the two balloonswithin the cavernous sinus
Indirect CCF
In contrast, indirect CCF are low flow lesions andusually progress slowly. These lesions must becarefully followed up with periodic clinicalexamination, measurement of intraocular pressureand angiographic studies as required. Specialattention should be paid to changes in theangioarchitecture and quantum of flow onangiography. Patients with visual deterioration,elevated intraocular pressure, obtrusive diplopia,intolerable bruit or headache and malignant proptosiswith exposure keratopathy require definitivemanagement. Table 1 summarizes and comparesdirect and indirect CCF.
Indirect CCF have multiple tiny arterovenousshunts in the wall of the cavernous sinus. These areusually embolized using polyvinyl alcohol particles,which not only mechanically occlude the lumen ofthe fistulae, but also incite an inflammatory reactionin the vessel wall (Figures 26.9A to F). Owing to the
multiplicity of the microfistulae and their propensityto parasitize additional arterial supply afterembolization, these lesions are relatively difficult toeliminate. Cure rates of 60-80% have been reportedin literature.
Occlusion of the cavernous sinus using detachablecoils is another treatment option in cases where theabove techniques fail. Extremely soft platinum coilsare introduced into the cavernous sinus througharterial or venous routes, so as to completely occludeits lumen. Complications such as transient cranialnerve palsies usually resolve over a few months.Permanent complications occur in less than 5% of cases.
Prognosis
With advances in imaging techniques and develop-ment of newer interventional techniques, consistentlygood results are being achieved in the managementof CCFs. The key to effective management of theselesions however, is early diagnosis by maintaining ahigh index of suspicion.
K L

364364364364364 Surgical Atlas of Orbital DiseasesSurgical Atlas of Orbital DiseasesSurgical Atlas of Orbital DiseasesSurgical Atlas of Orbital DiseasesSurgical Atlas of Orbital Diseases
Figures 26.9D and E: The feeders were embolized using polyvinyl alcohol particles (D) and (E)
D E
Figure 26.9F: Postembolization check angiogram shows absence of opacification of the fistulae and cavernous sinus
Figures 26.9A to C: Diagnostic left external carotid angiogram in frontal (A) and lateral (B) projections, reveal multiple arteriovenous fistulae(arrows) along the wall of the left cavernous sinus. Selective angiogram of the feeders (C) shows the fistulae and opacification of thecavernous sinus (arrow) as well as superior ophthalmic vein (arrow heads)
A B C

Carotid-Cavernous Fistulae: Role of Interventional RadiologistCarotid-Cavernous Fistulae: Role of Interventional RadiologistCarotid-Cavernous Fistulae: Role of Interventional RadiologistCarotid-Cavernous Fistulae: Role of Interventional RadiologistCarotid-Cavernous Fistulae: Role of Interventional Radiologist 365365365365365
REFERENCES
1. Barrow D, Spector R, Braun I, et al. Classification andtreatment of spontaneous carotidcavernous sinus fistulas.J Neurosurgery 1985; 62: 248-56.
2. Debrun GB, Lacour P, Fox AJ, et al. Traumaticcarotid-cavernous fistulas: etiology, clinical presentation,diagnosis, treatment, results. Semin Intervent Radiol 1987;4:242-8.
3. Higashida RT, Halbach VV, Tsai FY, et al. Interventionalneurovascular treatment of traumatic carotid andvertebral artery lesions. Results in 234 cases. AJR 1986; 153:577-82.
4. Halbach VV, Hieshima GB, Higashida RT, et al. Carotid-cavernous fistulae; Indications for urgent treatment. AJR1987; 149: 587-93.
5. de Keizer R. Carotid-cavernous and orbital arteriovenousfistulas: ocular features, diagnostic and hemodynamicconsiderations in relation to visual impairment andmorbidity. Orbit 2003; 22: 121-42.

366366366366366 Surgical Atlas of Orbital DiseasesSurgical Atlas of Orbital DiseasesSurgical Atlas of Orbital DiseasesSurgical Atlas of Orbital DiseasesSurgical Atlas of Orbital Diseases
Subrahmanyam Mallajosyula, Mohd Javed Ali
Ocular and SystemicOcular and SystemicOcular and SystemicOcular and SystemicOcular and SystemicAssociations of ProptosisAssociations of ProptosisAssociations of ProptosisAssociations of ProptosisAssociations of Proptosis
Some orbital lesions are known to have other ocularfeatures and also associated with other lesionselsewhere in the body. It is always essential to havea knowledge of these conditions, so that we caninvestigate accordingly and detect the disease in avery early stage and sometimes in asymptomaticstage,and help the patient. If needed we shouldrefer them to the respective specialists to preventcomplications and ensure overall care of thepatient.
In this chapter an attempt is made to list ocularand systemic associations of common orbitaldisorders presenting with proptosis. Some others likeleukemia, lymphomas are dealt with separatelyelsewhere in this book.
Capillary Hemangiomas
(a) Ocular features: Strawberry nevus of the lids,proptosis, ptosis, astigmatism, amblyopia, opticatrophy and exposure keratitis.
(b) Systemic associations:• Kasabach-Merritt syndrome (multiple
capillary hemangiomas + thrombocyto-penia)
• Mafucci syndrome (multiple capillaryhemangiomas + multiple enchondro-matosis)
• Phaces syndrome (posterior fossamalformations, hemangiomas, arterialanomalies, coarctation of the aorta, eyeabnormalities and sternum abnormali-ties).1,2
Neurofibromatosis
(a) Ocular features: Eyelid neurofibromas,prominent corneal nerves, glaucoma, Lischnodules, congenital ectropion uveae, irismamillations, choroidal naevi, retinalastrocytomas, optic nerve gliomas, optic nervemeningiomas and spheno-orbital encephalocelewith pulsating proptosis.
(b) Systemic associations: Chiasmal tumors,hypopituitarism, spinal and gastrointestinalneurofibromas, pheochromocytoma, juvenilexanthogranuloma, capillary hemangioma, Wilms’tumor, rhabdomyosarcoma, scoliosis, macro-cephaly, aqueductal stenosis and seizures.3,4
Diagnostic Criteria for NF-1NF 1 is diagnosed if 2 or more of the following groupof seven conditions are met
• Six or more caif-au-lait spots > 5 mm indiameter in prepubescents or > 15 mm in post-pubescents
• Two or more neurofibromas or one plexiformneurofibroma
• Axillary or inguinal freckling• Optic N glioma• Two or more Lisch’s nodules• Sphenoid bone dysplasia or thinning of long bone
cortex, with or without pseudoarthrosis• First degree relative with NF-1.
[Source: NIH Consensus development conference. ArchNeurol. 1988;45:575-580]
27C H A P T E R

Ocular and Systemic Associations of ProptosisOcular and Systemic Associations of ProptosisOcular and Systemic Associations of ProptosisOcular and Systemic Associations of ProptosisOcular and Systemic Associations of Proptosis 367367367367367
Neurofibroma type 2FeaturesMeningioma, glioma, schwannoma, vestibularschwannoma, posterior subcapsular lenticularopacities, hamartoma of retina and retinal pigmentepithelium.
NF2: Criteria for DiagnosisPresence of any one of the following features:
Bilateral vestibular schwannomaFirst degree relative with NF2 plus unilateral
vestibular schwannoma < 30 years.First degree relative with NF2 plus any 2 of the
following:• Meningioma• Glioma• Schwannoma• Juvenile posterior subcapsular
lenticular opacities• Juvenile cortical cataract.
[Source: National Institute of Health ConsensusDevelopment Conference Neurofibromatosis: ConferenceStatement. Arch Neurol 1988,45:,575-78.]
Diagnostic evaluation for NF2: MRI forneurological and neuro-otologic evaluation ismandatory, since nearly 90% of NF2 exhibit bilateralvestibular schwannomas.10
Thyroid Orbitopathy (Grave’s disease)
( a ) Ocular features: Lid retraction, chemosis,proptosis, superior limbic Keratoconjunctivitis,keratoconjunctivitis sicca, diplopia, opticneuropathy and choroidal folds.
(b) Systemic associations: Thyroid acropachy,plummer nails, tremors, fatigue, tachycardia,atrial fibrillation, pretibial myxoedema, alopecia,vitiligo, high output failure and myastheniagravis.
Craniofacial DysostosisCrouzon Syndrome( a ) Ocular features: Proptosis, hypertelorism,
V pattern exotropia, hypertropia, optic atrophy,exposure keratitis, megalocornea, glaucoma,colobomas, aniridia and blue sclera.
(b) Systemic associations: Wide cranium, midfacialhypoplasia, parrot-beak nose, frog facies,
mandibular prognathism and acanthosisnigricans.5,6
Apert Syndrome(a) Ocular features: Shallow orbits, proptosis,
hypertelorism, exotropia, antimongoloid slant,exposure keratitis, optic atrophy, keratoconus,congenital glaucoma and ectopia lentis.
(b) Systemic associations: Oxycephaly, midfacialhypoplasia, low set ears, high arched palate, cleftpalate, syndactyly, mental handicap andanomalies of the heart, lungs and kidney.5,6
Encephalocele
(a) Ocular features: Pulsatile proptosis, dystopia,medial canthal swelling, microphthalmos,colobomas and morning glory syndrome.
(b) Systemic associations: Neurofibromatosis,hypertelorism, broad nasal bridge and cleftpalate.7
Wegener’s Granulomatosis
(a) Ocular features: Nasolacrimal duct obstruction,dacryocystitis, scleritis, peripheral ulcerativekeratitis, nonspecific orbital inflammatorydisease and occlusive retinal periarteritis.
(b) Systemic associations: Necrotizing granulomasof upper respiratory tract, necrotizing glomeru-lonephritis, perforation of nasal septum, saddleshaped nasal deformity, nasal-paranasal fistulae,vasulitis of the spleen and adrenals, polyneuritisand meningioencephalitis.7
Wyburn-Mason Syndrome
(a) Ocular features: Arterio-venous malformationsof the conjunctiva, lids and retina, orbital A-Vmalformations causing proptosis and bruit,vitreous hemorrhage and neovascular glaucoma.
(b) Systemic associations: A-V malformations of theCNS causing headaches and seizures, cranialnerve palsies, motor and sensory deficits.7
Langerhans Cell Histiocytosis
(a) Ocular features: Proptosis, ptosis, periorbitalswelling, localized pain.
(b) Systemic associations: Osteolytic lesions ofskull, ribs and long bones, diabetic insipidus andsoft tissue lesions of liver and spleen.8

368368368368368 Surgical Atlas of Orbital DiseasesSurgical Atlas of Orbital DiseasesSurgical Atlas of Orbital DiseasesSurgical Atlas of Orbital DiseasesSurgical Atlas of Orbital Diseases
Hurler’s Syndrome(a) Ocular features: Corneal clouding,
papilloedema, shallow orbits causing proptosis.(b) Systemic associations: Stiff joints, coarse face,
chest deformities, dwarfism, hepatospleno-megaly and deafness.9
Nonspecific Orbital Inflammation Syndrome• Crohn's disease,• Systemic lupus erythematosus• Rheumatoid arthritis• Myasthenia gravis• Ankylosing spondylitis.
Sclerosing inflammation of the orbit• Riedel's thyroiditis• Mediastinal fibrosis• Sclerosing cholangitis• Fibrosis of parotid gland, lacrimal gland and
lung.
Osteoma• Gardner's syndrome (Familial polyposis of
large bowel, plus osteoma of skull or jaw plusepidermal and subcutaneous cysts)
• Turcot Syndrome (Familial adenomatouspolyposis plus CNS gliomas).
Fibrous dysplasiaMcCune-Albright syndrome (ployostotic fibrousdysplasia + sexual precocity + cutaneous pigmentation).
Orbital Hamartoma (tuberous sclerosis)Ocular : Retinal hamartomaVisceral : Pulmonary lymphangiomatosis
Renal angiolipomaCardiac rhabdomyoma
Skin : Facial angiofibromaCNS : Intracranial astrocytomas, ependymoma
Hemangioblastoma
Von Hippel- Lindau's disease• Retinal hemangioblastoma• Cerebellar and spinal hemangioblastoma• Renal cell carcinoma• Pheochromocytoma• Others: Pancreatic tumors, cystadenoma of
epididymis.
REFERENCES
1. Haik BG, Karcioglu ZA, Gordon RA, Pechous BP. Capillaryhemangioma. Surv Ophthalmol. 1994;38:399-426.
2. Kushner BJ. Hemangiomas. Arch Ophthalmol. 2000;118:835-36.
3. Beauchamp GR. Neurofibromatosis type 1 in children.Trans Am Ophthalmol soc. 1995;93:445-72.
4. Listernick R, Charrow J, Greenwald MJ, et al. Natural historyof optic pathway tumors in children with neurofibro-matosis type 1. J Pediatr.1994;125:63-66.
5. Cohen MM. The child with multiple birth defects. 2nded.New york:Oxford 1997:178-96.
6. Gorlin RJ, Cohen MM, Levin LS. Syndromes of the headand Neck. 3rd ed. Newyork Oxford; 1990.
7. Kanski JJ. Clinical Ophthalmology:A systematic approach.6th ed. Butterworth - Heinemann. 2007.
8. Huang F, Arceci R. The histiocytoses of infancy. SeminPerinatol 1999;23:319-31.
9. AAO. Pediatric Ophthalmology and strabismus. Section 6.Ocular findings in inborn errors of metabolism. AAOpublication 2006.
10. Arun D Singh, Bertil F Damato,, Jacob Pe'er, A. LinnMurphee, Julian Perry: Clinical Ophthalmic oncology, firstedition, 2007 Saunders Elsevier,Philadelphia.

IndexIndexIndexIndexIndex
A
3-D reconstruction of orbit 84Adenoid cystic carcinoma 194
clinical features 194imaging 195management 196pathology and pathogenesis 195
basaloid variant 195comedocarcinoma variant 195cribriform (glandular or swiss-
cheese) pattern 195sclerosing variant 195tubular (ductal) variant 195
prognosis 196Angiosarcoma 76Applied anatomy of orbit 3
cavernous sinus 8extraocular muscles 9globe 8lacrimal system 13lids 10nerves of the orbit 14
optic nerve 14parasympathetic innervation of the
orbit 16sensory innervation of the orbit 14sympathetic innervation of the
orbit 16orbital apex 6orbital osteology 3periorbita 6
Auscultation 51
B
Basal cell and squamous cell carcinoma348
B-cell lymphoma 174Benign tumors of orbit 103
capillary hemangioma 103
cavernous hemangioma 103hemangiopericytoma 103lymphangioma 103meningiomas 104
Bone tumors of orbit 180case-illustration 181
aneurysmal bone cyst 184cholesterol granuloma 184chondroma 183chondrosarcoma 186Ewing's sarcoma 186fibrous dysplasia 181giant cell lesions 184Langerhans cell histiocytosis (lCH)
186mesenchymal chondrosarcoma 186myeloma 186ossifying fibroma 182osteoblastoma 182osteogenic sarcoma 184
clinical presentation 162clinico-pathological classification of
primary orbital bone disorders 180osteoma 180
Bony lesions 62Bony orbit 60
C
Capillary hemangioma 348Carotid-cavernous fistula 39Carotid-cavernous fistulae 356
direct CCF 360indirect CCF 363management of CCF 360pathophysiology 357
clinical features 357prognosis 363radiological investigations 359
Cell cycle and the principles of anti-neoplastic therapy 347
Cephalocele 201
radiological finding 202treatment 202
Choroidal melanomas 349Classification of orbital tumors 102
primary 102hemopoietic 102lacrimal gland 102mesenchymal 102miscellaneous 102neural 102
secondary 102direct extension 102
Cystic lesions of the orbit 78Cysts of the optic nerve sheath 203Cytology smear 91
D
Dacryocele 205Decision making 271
apical conal lesions 279intraconal lesion 273lesions of superior peripheral space 279thyroid associated orbitopathy 285
Dermoid and epidermoid cysts 200investigations 200
MRI 200treatment 201
Developmental lesions of orbit 98dermoid and epidermoids 99fibrous dysplasia 99hamartoma 99meningioencephalocoeles 98neurofibromatosis 98sphenoid wing dysplasia 98
Diagnosis of orbital tumors 98oculomotor paresis 98optic neuropathy 98pain 98papillary abnormalities 98proptosis 98
Duplex Doppler 56
370370370370370 Surgical Atlas of Orbital DiseasesSurgical Atlas of Orbital DiseasesSurgical Atlas of Orbital DiseasesSurgical Atlas of Orbital DiseasesSurgical Atlas of Orbital Diseases
E
Enlarged extraocular muscle 69ENT approach to proptosis 300
etiological factors 300clinical manifestation and evaluation
300diseases of the lacrimal apparatus
300infection and inflammation 300tumors of the orbito-sinual disease
300Epithelial cyst (dacryops) 190
clinical features 190management 191pathology and pathogenesis 191prognosis 191
Etiology of proptosis 53Evaluation of a case of proptosis 53External radiotherapy in ocular tumors
346
F
Functional endoscopic sinus surgery(FESS) 309
G
Graves’ ophthalmopathy 353
H
Hand-Schuller-Christian syndrome 133Hematic cyst 203
investigations 203treatment 203
Hertel's exophthalmometer 35Hertel's exophthalmometry 37Hutchinson's sign 15Hydatid cyst of orbit 217
investigations 217management 217
I
Idiopathic orbital inflammation (IOI) 353Inflammatory lesions of orbit 100
orbital cellulitis 100idiopathic orbital inflammation 100orbital infections 101
aspergillosis 101cysticercosis 102neoplastic lesions 102tuberculosis 101
Internal radiation therapy (brachy-therapy) 345
Intraocular lymphoma 349Intraocular tumors 349
K
Kilppel-Trenaunary syndrome 153Kimura's disease 132
L
Lacrimal gland tumors 76Langerhans histiocytosis 133Letterer-Siwe disease 133Leudde's exophthalmometry 35Lid retraction 46Lymphoma of lacrimal gland 77Lynch-Howarth's operation 304
M
Malignant conjunctival tumors 349Malignant tumors of orbit 104
adenoid cystic carcinoma 105Graves disease 106histiocytoma 105lymphoma 105metastasis 105optic glioma 106rhabdomyosarcoma 104
Management of ophthalmic tumors 347Medical management of proptosis 337
nonspecific inflammations of the orbit(NSOIS) 337
chronic granulomatous infections338
nonspecific lacrimal inflammation337
nonspecific myositic inflammation337
orbital cellulitis 338parasitic infestations 338rhino-orbital mucormycosis 338specific inflammations of the orbit
338structural lesions 340Tolosa-Hunt syndrome 339vascular lesions 339vasculitis 339
Meningioma of optic nerve sheath 74Mesenchymal tumors 170
histiocytic tumors 175fibrous histiocytoma 175
malignant tumors of uncertain type175rhabdoid tumor 175
mesenchymal soft tissue tumors 170striated muscle tumors 170
rhabdomyoma 172rhabdomyosarcoma 170
Microphthalmos with cyst 202Mucocele 202Müller's muscle 46
N
Neurofibroma 75Neurosurgical approach to proptosis 309Non-Hodgkin's lymphoma 147Nonspecific orbital inflammatory
syndrome (NSOIS) 131
O
Ocular and systemic associations ofproptosis 366capillary hemangiomas 366
systemic associations 366ocular features 366
craniofacial dysostosis 367apert syndrome 367crouzon syndrome 367encephalocele 367fibrous dysplasia 368hemangioblastoma 368Hurler's syndrome 368Langerhans cell histiocytosis 367nonspecific orbital inflammation
syndrome 368orbital hamartoma (tuberous
sclerosis) 368osteoma 368sclerosing inflammation of the orbit
368Wegener's granulomatosis 367Wyburn-Mason syndrome 367
diagnostic criteria for NF-1 366neurofibroma type 2 367
criteria for diagnosis 367diagnostic evaluation 367features 367
neurofibromatosis 366ocular features 366systemic associations 366
thyroid orbitopathy 367Ocular metastasis 352Optic nerve glioma 353Optic nerve meningioma 353Orbital amyloidosis 129Orbital diseases 97
classification 97developmental 97endocrine 97
IndexIndexIndexIndexIndex 371371371371371
inflammatory 97miscellaneous 97neoplastic 97traumatic 97vascular 97
Orbital exenteration 318complications of exenteration 320indications 318management of the exenterated socket
320myocutaneous flaps 320patient preparation 318prosthesis 320skin flaps 320skin grafting 320spontaneous granulation 320surgical procedure 318types 319
anterior exenteration 319lid sparing exenteration 319radical exenteration 319total exenteration 319
Orbital fractures 220anatomy 220examination 222floor fractures 233general operative considerations 229
antibiotics 230decision repair or not repair 232timing of surgery 231
imaging 226implant materials 227late and secondary fracture repair 239lateral wall and zygomatico-maxillaryfractures 238
Orbital infections 120demographic profile 120diagnosis 121emergency department care 122etiological causes 121
bacterial infections 121fungal infections 121parasitic infections 121protozoal infections 121
imaging studies 121risk factors 121
Orbital lymphoma 146modified Rye's classification of
Hodgkin's lymphoma 147classic HD 147nodular lymphocyte-predominant
HD 147revised European American
lymphoma classification (REALclassification) 146leukemias and lymphomas of T-cell
origin 146
WHO classification of NHL 146B-cell neoplasms 146T-cell neoplasms 146
Orbital lymphoma 352Orbital prosthesis 327
assemble the prosthesis 331casting 329fabrications of ocular prosthesis 331impression of the orbital defect 328moulding 330preparation of the patient 328sculpting 329types 327
adhesive retained prosthesis 327magnetic retained prosthesis 327partial prosthesis 327spectacle mounted prosthesis 327
using the desired material 331Orbital tumors 352Orbital tumors of neurological origin 162
optic nerve glioma 162optic nerve meningioma 163orbital schwannoma (neurilemmoma)
and neurofibroma 165Orbital xanthogranuloma 134Orbitotomies 288
approaches 289general principles 288lateral orbitotomy 290Stallard-Wright lateral orbitotomy 290swinging lower lid flap 289transcarcuncular approach 291transfrontal orbitotomy 291
complications 291postoperative management 291
transnasal endoscopic approach andtransantral approach 291
P
Parasitic cysts of orbit 207investigations 208treatment 208
Patterson's operation 305Perception of color vision 41Peripheral surgical space 91Plaque radiotherapy 346Pleomorphic adenoma 191
clinical features 191imaging 192management 192pathology and pathogenesis 192prognosis 192
Pleomorphic adenoma 76Proptosis 28
axial proptosis 29
down and in displacement of the globe32
down and out proptosis 29measurement of proptosis 35upward displacement of globe 35
Pulsations of globe 37
R
Radiation therapy delivery methods 344Reese-Berke's incision 273Retinoblastoma 349
treatment 349chemoreduction 350cryotherapy 349photocoagulation 349subtenon (subconjunctival)
chemotherapy 350surgery (enucleation) 350
Rhabdomyosarcoma 77, 352Role of cytology in orbital lesions 85
fine needle aspiration/samplingtechnique 85
intraoperative-operative diagnosis bysquash and imprint cytology 85
squash or imprint cytology 85Rosai Dorfman disease 133
S
Sarcoidosis 130Sebaceous carcinoma 348Secondary and metastatic orbital tumors
244malignant melanoma of eyelid 256metastatic orbital tumors 263orbital extension of conjunctival
tumors 258malignant melanoma of the
conjunctiva 259squamous cell carcinoma of the
conjunctiva 258orbital extension of eyelid tumors 252orbital extension of intracranial tumors
257orbital extension of intraocular tumors
244orbital extension of lacrimal sac tumors
250orbital extension of medulloepithe-
lioma 246orbital extension of nasopharyngeal
tumors 262orbital extension of retinoblastoma
244orbital extension of tumors of the nasal
cavity and paranasal sinus 260

372372372372372 Surgical Atlas of Orbital DiseasesSurgical Atlas of Orbital DiseasesSurgical Atlas of Orbital DiseasesSurgical Atlas of Orbital DiseasesSurgical Atlas of Orbital Diseases
orbital extension of uveal melanoma247
sebaceous carcinoma of the eyelid 253squamous cell carcinoma of the eyelid
255Sequelae of radiation therapy 353Sinus diseases causing proptosis 301
allergic fungal sinusitis 301extensive nasal polyposis 301frontoethmoidal mucoceles 302mucormycosis 301purulent infections 301treatment 301
Soft-tissue lesions 72Sphenoid wing meningioma 45Steps of Reese-Berke's approachSteps of superior lid crease incision 275Sturge-Weber syndrome 152Subconjunctival hemorrhage 51
T
Teratomas 201Thyroid-associated orbitopathy 111
course of disease 114incidence and epidemiology 112management guidelines 118pathogenesis 112risk factors 112visa classification 114
appearance/exposure 117application of the visa classification
118
inflammation/congestion 116strabismus/motility restriction 117vision/optic neuropathy 114
Transcranial approach with resection ofthe orbital roof 311
Transpalatal approach to removepostnasal tumors 307
Trauma 65Tumors of lacrimal gland 348Tumors of paranasal sinuses causing
proptosis 302fibrous dysplasia 302hemangiopericytoma 302juvenile nasopharyngeal angio-
fibroma 303malignant tumors 303
adenoid cystic carcinoma 303esthesioneuroblastoma 304non-Hodgkin's lymphoma 303rhabdomyosarcoma 303squamous cell carcinoma 303
various approaches for tumorremoval 304Caldwell-Luc operation 304external ethmoidectomy 304intranasal ethmoidectomy 304Jansen-Horgan operation 304lateral rhinotomy/medial maxillec
tomy 305total maxillectomy 306
Tumors of the eyelid 347
V
Val salva 51Vascular anatomy of the orbit 17
arterial supply 17outflow 19paranasal sinuses 20venous 19
Vascular lesions of orbit 151malformations 151
cavernous hemangioma 152lymphangioma 151orbital varices 152other congenital malformations 152
shunts 153angiosarcoma 155capillary hemangioma 154carotid-cavernous fistula 153hemangioblastoma 155hemangioendothelioma 155hemangiopericytoma 155Kaposi's sarcoma 155new growths 154
Vascular pulsations 39Von Recklinghausen disease 75
W
Wegener's granulomatosis 132Whitall's tubercle 12Wyburn-Mason syndrome 153