
Cytokine inhibitors in autoimmune disease
19
Cytokine Inhibitors in Autoimmune Disease Ana Luisa Weckmann and Jorge Alcocer-Varela The cytokine network participates in the modulation of the immune system. Furthermore, the formation of the cytokine-receptor complex, as well as the transcription, translation, secretion, or degradation of cytokines interfere with the functions of cytokines. Cytokine inhibitors include antagonists, soluble receptors, cytokine-binding proteins, and cytokines that block other cytokines. In autoimmune diseases, an abnormal production of proinflammatory cyto- kines, or a reduced inhibition of their actions, may lead to an imbalance. The main cytokine inhibitors include interleukin-1 receptor antagonist (IL-lra), soluble IL-1 receptor (slL-1R), soluble TNF-~ receptors (soluble TNF-Rs), and certain cytokines, such as IL-4, TGFI~, and IL-10. The combination of cytokine inhibitors is a potential therapeutic approach in the treatment of immuno- inflammatory diseases. The nonspecific effects of immunosuppressive drugs are improved by using inhibitors with more specific actions on the functions of proinflammatory cytokines. Semin Arthritis Rheum 26:539-557. Copyright © 1996 by W.B. Saunders Com- pany INDEX WORDS: Cytokine antagonists; IL-lra; soluble TNF receptors; autoimmu- nity. C YTOKINES MEDIATE profound biologi- cal effects. Their multiple activities are regulated mainly at the level of their secretion by expression of their receptors, by the concomi- tant action of several cytokines, and by the occurrence of inhibitory proteins and specific carrier molecules. 1 The biological activity of cytokines depends on the proportion of cyto- kines and inhibitory molecules. 2 Cytokines are involved in some pathophysiological states be- cause of excessive production or inadequate inhibition. Defective control of certain T cell clones and their cytokines may lead to excessive production of proinflammatory cytokines, along with inadequate inhibition of their effects, which may contribute to the chronicity of disease. 3 CYTOKINE INHIBITORS Factors that are able to inhibit certain cyto- kines are found in biological fluids or superna- tants of cell cultures, called inhibitors, that generally show specific action on cytokines. Cytokine inhibitors may be classified as follows: (1) Nonpeptidic molecules. They may interfere with cytokine synthesis, receptor binding, or signal transduction. (2) Soluble receptors. They may neutralize and prevent extravascular es- cape. (3) IL-lra/mutated cytokines. They pre- vent induction of signal transduction via recep- tors. (4) Autoantibodies. They may neutralize and also may enhance complement-mediated killing of cells expressing membrane-bound or surface-receptor-bound cytokines. 4 Nonpeptidic molecules are considered the ideal antagonists because of their small size and oral activity. Of these, the only effective antago- nist has been isothiazolone A, which interferes with interleukin-5 (IL-5) binding to its receptor. Also, certain cytokines may antagonize the effects of other cytokines. Inhibitors may func- tion at different levels: by interfering with the cytokine-receptor complex, and thus inhibiting signal transduction; by altering transcription or translation processes; by interfering with secre- tion or degradation of cytokines, or by neutraliz- ing their ligand (Table 1). From the Department of Immunology and Rheumatology, Insfituto Nacional de la Nutrici6n Salvador Zubirdn, Mexico City, Mexico. Address reprint requests to JorgeAlcocer- Varela, MD, Depart- ment of Immunology and Rheumatology, Instituto Nacional de la Nutrici6n Salvador Zubir6n, Vasco de Quiroga 15, 14000 Mdxico, D.F., Mdxico. Copyright © 1996 by W.B. Saunders Company 0049-0172/96/2602-000255.00/0 Seminar, s in Arthritis and Rheumatism, Vo126, No 2 (October), 1996: pp 539-557 539
-
Upload
independent -
Category
Documents
-
view
3 -
download
0
Transcript of Cytokine inhibitors in autoimmune disease

Cytokine Inhibitors in Autoimmune Disease
Ana Luisa Weckmann and Jorge Alcocer-Varela
The cytokine network participates in the modulation of the immune system. Furthermore, the formation of the cytokine-receptor complex, as well as the transcription, translation, secretion, or degradation of cytokines interfere with the functions of cytokines. Cytokine inhibitors include antagonists, soluble receptors, cytokine-binding proteins, and cytokines that block other cytokines. In autoimmune diseases, an abnormal production of proinflammatory cyto- kines, or a reduced inhibition of their actions, may lead to an imbalance. The main cytokine inhibitors include interleukin-1 receptor antagonist (IL-lra), soluble IL-1 receptor (slL-1R), soluble TNF-~ receptors (soluble TNF-Rs), and certain cytokines, such as IL-4, TGFI~, and IL-10. The combination of cytokine inhibitors is a potential therapeutic approach in the treatment of immuno- inflammatory diseases. The nonspecific effects of immunosuppressive drugs are improved by using inhibitors with more specific actions on the functions of proinflammatory cytokines. Semin Arthritis Rheum 26:539-557. Copyright © 1996 by W.B. Saunders Com- pany
INDEX WORDS: Cytokine antagonists; IL-lra; soluble TNF receptors; autoimmu- nity.
C YTOKINES MEDIATE profound biologi- cal effects. Their multiple activities are
regulated mainly at the level of their secretion by expression of their receptors, by the concomi- tant action of several cytokines, and by the occurrence of inhibitory proteins and specific carrier molecules. 1 The biological activity of cytokines depends on the proportion of cyto- kines and inhibitory molecules. 2 Cytokines are involved in some pathophysiological states be- cause of excessive production or inadequate inhibition. Defective control of certain T cell clones and their cytokines may lead to excessive production of proinflammatory cytokines, along with inadequate inhibition of their effects, which may contribute to the chronicity of disease. 3
CYTOKINE INHIBITORS
Factors that are able to inhibit certain cyto- kines are found in biological fluids or superna- tants of cell cultures, called inhibitors, that generally show specific action on cytokines. Cytokine inhibitors may be classified as follows: (1) Nonpeptidic molecules. They may interfere with cytokine synthesis, receptor binding, or signal transduction. (2) Soluble receptors. They may neutralize and prevent extravascular es- cape. (3) IL-lra/mutated cytokines. They pre-
vent induction of signal transduction via recep- tors. (4) Autoantibodies. They may neutralize and also may enhance complement-mediated killing of cells expressing membrane-bound or surface-receptor-bound cytokines. 4
Nonpeptidic molecules are considered the ideal antagonists because of their small size and oral activity. Of these, the only effective antago- nist has been isothiazolone A, which interferes with interleukin-5 (IL-5) binding to its receptor. Also, certain cytokines may antagonize the effects of other cytokines. Inhibitors may func- tion at different levels: by interfering with the cytokine-receptor complex, and thus inhibiting signal transduction; by altering transcription or translation processes; by interfering with secre- tion or degradation of cytokines, or by neutraliz- ing their ligand (Table 1).
From the Department of Immunology and Rheumatology, Insfituto Nacional de la Nutrici6n Salvador Zubirdn, Mexico City, Mexico.
Address reprint requests to Jorge Alcocer- Varela, MD, Depart- ment of Immunology and Rheumatology, Instituto Nacional de la Nutrici6n Salvador Zubir6n, Vasco de Quiroga 15, 14000 Mdxico, D.F., Mdxico.
Copyright © 1996 by W.B. Saunders Company 0049-0172/96/2602-000255.00/0
Seminar, s in Arthritis and Rheumatism, Vo126, No 2 (October), 1996: pp 539-557 539
540 WECKMANN AND ALCOCER-VARELA
Table 1: Mechanisms of Action of Cytokine Inhibitors
1. Interference with the cytok ine/receptor complex
format ion (signal transduction inhibit ion)
2. Interference with transcription or translation
3, Interference with cytokine secretion or degrada-
t ion
AUTOIMMUNE DISEASES AND CYTOKINE INHIBITORS
Within an inflammatory environment, the net effect of cytokines depends on the balance between cytokines, inhibitors, cell surface recep- tors, and their relative expression. 5 Overproduc- tion of cytokines in autoimmune inflammatory diseases is characterized by increased produc- tion of natural inhibitors of cytokines, such as soluble receptors and antagonists.
For the treatment of autoimmune diseases, immunosuppressive drugs are used, such as antimetabolites, corticosteroids, or cyclosporin A. These drugs inhibit the production of several cytokines, but they display nonspecific effects. Therefore, attempts have been made to develop therapeutic agents able to block specifically the synthesis, release or actions of cytokines. 5
Knowledge of the existence of natural mecha- nisms for the preservation of cytokine homeosta- sis may lead to the use of natural immunomodu- lating agents for therapeutic treatment of inflammatory disorders. The study of the role of cytokines and other mediators of chronic inflam- mation offers a new immunopharmacological approach for treatment, by using recombinant human proteins that function as anticytokines, which neutralize the effects of inflammation mediators.
IL-1 INHIBITORS
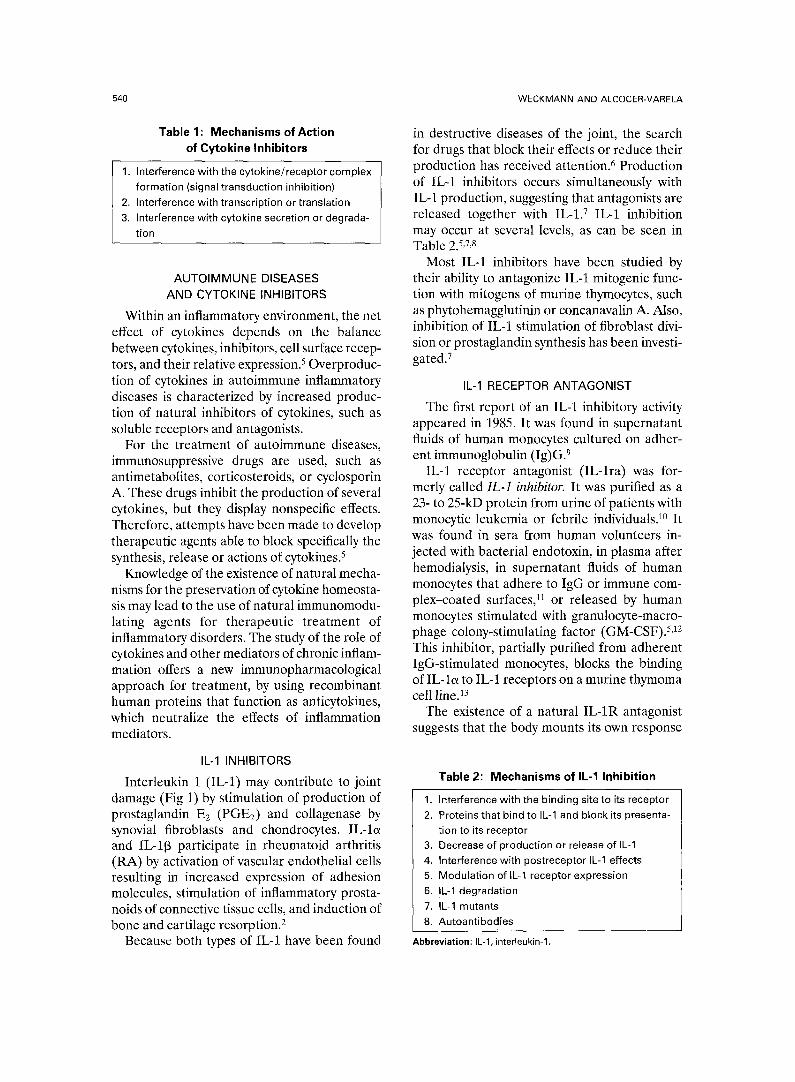
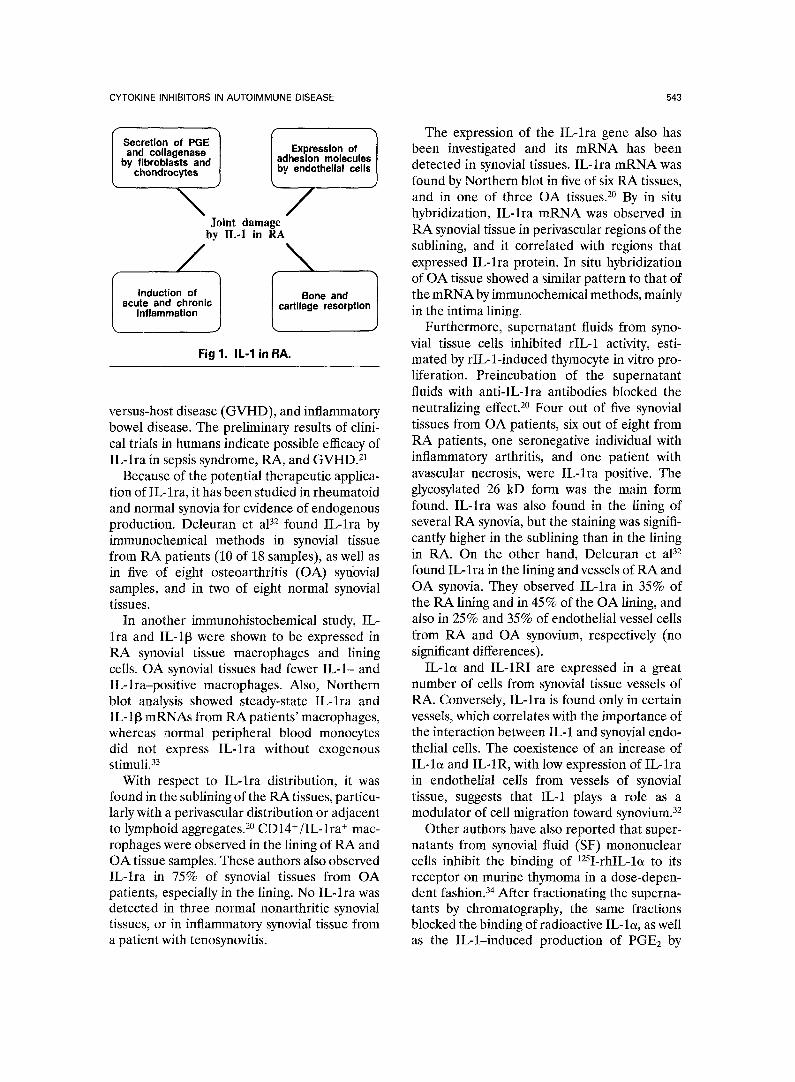
Interleukin 1 (IL-1) may contribute to joint damage (Fig 1) by stimulation of production of prostaglandin E2 (PGE2) and collagenase by synovial fibroblasts and chondrocytes. IL-lo~ and IL-113 participate in rheumatoid arthritis (RA) by activation of vascular endothelial cells resulting in increased expression of adhesion molecules, stimulation of inflammatory prosta- noids of connective tissue cells, and induction of bone and cartilage resorption. 2
Because both types of IL-1 have been found
in destructive diseases of the joint, the search for drugs that block their effects or reduce their production has received attention. 6 Production of IL-1 inhibitors occurs simultaneously with IL-1 production, suggesting that antagonists are released together with IL-1. v IL-1 inhibition may occur at several levels, as can be seen in Table 2. 5,7,8
Most IL-1 inhibitors have been studied by their ability to antagonize IL-1 mitogenic func- tion with mitogens of murine thymocytes, such as phytohemagglutinin or concanavalin A. Also, inhibition of IL-1 stimulation of fibroblast divi- sion or prostaglandin synthesis has been investi- gated. 7
IL-1 RECEPTOR ANTAGONIST
The first report of an IL-1 inhibitory activity appeared in 1985. It was found in supernatant fluids of human monocytes cultured on adher- ent immunoglobulin (Ig)G. 9
IL-1 receptor antagonist (IL-lra) was for- merly called IL-1 inhibitor. It was purifed as a 23- to 25-kD protein from urine of patients with monocytic leukemia or febrile individuals. 1° It was found in sera from human volunteers in- jected with bacterial endotoxin, in plasma after hemodialysis, in supernatant fluids of human monocytes that adhere to IgG or immune com- plex-coated surfaces, 11 or released by human monocytes stimulated with granulocyte-macro- phage colony-stimulating factor (GM-CSF). 5,12 This inhibitor, partially purified from adherent IgG-stimulated monocytes, blocks the binding of IL-la to IL-1 receptors on a murine thymoma cell line. ~3
The existence of a natural IL-1R antagonist suggests that the body mounts its own response
Table 2: Mechanisms of IL-1 Inhibition
1. Interference with the binding site to its receptor
2. Proteins that bind to IL-1 and block its presenta-
t ion to its receptor 3, Decrease of product ion or release of IL-1
4. Interference with postreceptor IL-1 effects
5. Modulat ion of IL-1 receptor expression 6. IL-1 degradat ion
7. IL-1 mutants
8. Autoant ibodies
Abbreviation: IL-1, interleukin-1.

CYTOKINE INHIBITORS IN AUTOIMMUNE DISEASE 541
against inflammation, and that IL-lra synthesis is a natural component for the resolution of the disease process. 6
IL-lra, also called IRAP (IL-1 receptor an- tagonist protein), was purified from the superna- tant fluids of phorbol myristate acetate (PMA)- stimulated myelomonocytic line U937, by several size exclusion chromatographic steps and high- pressure liquid chromatography (HPLC).14
IL-lra binds to IL-1 receptors and competes with IL-loL or IL-l[3, but it has no agonist activity, so that IL-lra is a ligand with pure antagonist activity. All three forms of IL-1 bind to IL-1 receptors in a similar fashion, but IL-lra may lack the secondary interactions necessary to trigger cell responses. It binds better to IL-1RI than to IL-1RII, 15 and it has the same affinity as IL-1 but it does not induce any biological response. 8 It does not activate any protein kinase normally activated by IL-1,16 and it is not internalized after its binding to IL-1RI. 6
IL-lra is synthesized as a propeptide of 177 amino acids, with a leader sequence of 25 amino acids. The mature protein has 152 amino acids and an N glycosylation site. 8 Glycosylation is not necessary for its inhibitory activity. 5,11 The amino acid sequence of IL-lra has 26% to 30% homol- ogy with IL-I[3 and 19% with IL-la. The identi- cal amino acids shared by the three proteins may be important for binding to the receptor, and the shared sequences of IL-la and IL-l[3 that differ from those of IL-lra may be crucial for IL-lra antagonist action. The similarities between IL-lra and IL-1 indicate that IL-lra belongs to the IL-1 gene family.
The pure protein has an isoelectric point of 5.0 and weighs 18 to 25 kD. Its sequence is identical to that of IL-lra cloned in human mononuclear cells. 17 IL-lra may be a glyco- sylated, 22- to 25-kD molecule, or a nonglyco- sylated, 17-kD molecule. IL-lra is conserved among different species, because rat IL-lra and mouse IL-lra are 75% and 77% identical to the human inhibitor. ~8
IL-lra is produced by monocytes and diverse tissue macrophages, including alveolar macro- phages of patients with interstitial pulmonary disease, synovial macrophages of patients with RA, as well as by in vitro-derived macro- phages. 19 It is produced also by neutrophils, keratinocytes, and epithelial cells. 8 IL-lra gene
expression has been found in normal skin, lymphoid tissues, and malignant endometrial tumors. 20
There are two structural variants of monocyte IL-lra in keratinocytes and other epithelial cells. 21,22 One is slL-lra, secretory IL-lra, which has a leader sequence and is produced by monocytes, neutrophils, and other cells. The other is icIL-lra or intracellular IL-lra, which lacks a leader sequence, and remains intracellu- lar in keratinocytes and other epithelial cells; fibroblasts or alveolar macrophages produce both simultaneously. 23,24 The roles of sIL-lra and icIL-lra in normal physiology or in host defense mechanisms remain unclear.
Either phorbol myristate acetate (PMA) or GM-CSF, added to several human myelomono- cytic cell lines, or human monocytes and macro- phages stimulated by IgG produce IL-lra. 25 Adherent IgG induces peripheral blood mono- cytes to secrete IL-lra, and the IgG F(ab') fragment does not. These findings support the hypothesis of a role of Fc-/R in IL-lra produc- tion. Also, peripheral blood macrophages and neutrophils secrete IL-lra in response to anti- Fc-yRII, suggesting that Fc~RI and Fc~RII play an important role in IL-lra production. 26
IL-lra blocks multiple IL-l-induced ef- fects. 6'27'28 The availability of recombinant IL- lra has allowed the study of its IL-1 inhibition in several animal models of acute or chronic dis- eases, where it has been found to reduce the effects shown in Tables 3 and 4. Nevertheless, IL-lra must have a 10- to 500-fold excess amount over IL-1 to inhibit 50% of IL-1 re- sponses in vitro and in vivo. 21,27
The crystal structure of IL-lra has been resolved to 0.21-nm resolution. 29 IL-lra has the same fold as IL-loL and IL-I[3, consisting of 12 [3 sheets that form a barrel of six sheets, closed at an end by 3 [3 hairpin loops. Cys69 and Cysll6 are bound by a disulfide bond. Mutagenesis studies show that there are putative interactions of IL-lra and IL-1 receptor that are structurally conserved and rigid. This allows for specific interactions with the IL-1 receptor.
A five-allele polymorphism has been shown in intron 2 of the IL-lra gene, localized in human chromosome 2q, due to a variable number of tandem repeats of 86 bp. 3° By polymerase chain reaction (PCR) analysis, the allelic frequencies

542
Table 3:IL-1 Effects Inhibited by IL-lra
Rabbit or mice death by endotoxin, LPS, or Esch- erichia coil
Septic shock induced by Klebsiella pneumoniae in rats
Hemodynamic shock and tissue damage in rabbits and baboons, byEcoli
Brain malaria in mice Circulating and spinal fluid IL-6 Hypoglycemia in mice Acute-phase proteins in mice Neutrophilia in mice Inflammation in animal models of sepsis, GVHD,
RA, asthma Severity and onset of arthritis in rats Collagen-induced arthritis in mice Onset of spontaneous diabetes in BB rats Proliferation of chronic myelogenous leukemia cells Accumulation of neutrophils during inflammatory
peritonitis in mice Experimental enterocolitis in rats Pulmonary inflammation by LPS in rats
Abbreviations: IL.1, interleukin-1 ; IL-lra, interleukin-1 receptor antagonist; LPS, lipopolysaccharide; IL-6, interleukin-6; GVHD, graft-versus-host disease; RA, rheumatoid arthritis; BB, BB rats, a strain of Wistar-derived rats that frequently develop spontane- ous insulin-dependent diabetes mellitus.
of the polymorphism were found in a control population (allele 2 = 23%), in patients with psoriasis I (allele 2 = 35.5%, increased in 50%), and in patients with psoriasis II (allele 2 = 2.7%, significantly decreased). An increase of 50% has also been observed in allele 2 in other inflammatory diseases such as discoid lupus erythematosus, dermatitis herpetiformis, and atopic eczema. In contrast with these inflamma- tory skin diseases, the allelic frequencies in RA and juvenile rheumatoid arthritis have been the same as in the control population.
Recently, 30 families, each with multiple psoriatic cases, have been studied using the intragenic tandem repeat sequence polymor- phism within the IL-lra gene. 31 The data show exclusion of linkage with IL-lra that extends by a minimal genetic distance of 1 cM. Therefore, the IL-lra gene is not an important genetic determinant for psoriasis susceptibility. The authors are in search of linked loci in these families, and they suggest the use of microsatel- lite genetic mapping to study the yet-unraveled pathogenesis of several diseases.
WECKMANN AND ALCOCER-VARELA
IL-1RA IN RHEUMATOID ARTHRITIS
Cytokines have an important role in rheuma- toid synovitis. Antigen-presenting cells that ex- press class II HLA are stimulated by GM-CSF, and they activate T lymphocytes to release interferon-~ (IFN-,/) and other cytokines. These cytokines stimulate macrophages to synthesize and release IL-1, tumor necrosis factor-~ (TNF- ~), and IL-6.
IL-1 constitutes an essential piece of the complex network of cytokines that participates in RA perpetuation. Macrophages produce IL-1 and TNF-a, which stimulate type B synoviocytes to proliferate and release metalloproteinases, GM-CSF, and other factors.
With the stimulus of IL-1, TNF-a, and IL-6, synovial fibroblasts and chondrocytes secrete enzymes, such as collagenase and other neutral proteases (Fig 2). Thus, cartilage, bone, and periarticular structures are damaged. 5
IL-lra may play a role in the pathophysiology of RA, because its messenger RNA (mRNA) has been found in synovial lining cells and in perivascular lymphoid aggregates. IL-lra may modify some animal models of acute arthritis, but not others. 19 The administration of IL-lra blocks the effects of ]L-1 in some animal models of septic shock, inflammatory arthritis, graft-
Table 4: Actions Blocked In Vitro by IL-lra
Lymphocyte proliferation Collagenase and PGE2 production by rabbit chon-
drocytes or synovial cells PGE2 synthesis by fibroblasts Bone resorption in mice and rats Cartilage matrix degradation Increase of adhesion molecules mRNA of human
umbilical vein endothelial cells Adhesion of endothelial cells to neutrophils and
eosinophils Synthesis of IL-1, TNF, IL-6, and GM-CSF by mono-
cytes Nitric oxide production by smooth muscle IL-8 production by mononuclear cells stimulated
with LPS or IL-1
Abbreviations: IL-lra, interleukin-1 receptor antagonist; PGE2, prostaglandin E2; mRNA, messenger RNA; IL-1, interleukin-1; TNF, tumor necrosis factor; IL-6, interleukin-6; GM-CSF, granu- Iocyte-macrophage colony-stimulating factor; IL-8, interleu- kin-8; LPS, lipopolysaccharide.
CYTOKINE INHIBITORS IN AUTOIMMUNE DISEASE 543
i m
by fibroblasts and
I
Secretion of PGE ~ Expression of "~ and collagenase I adhesion molecules[
chondrocytes ~by endothelial cel,s ~
\ / Joint damage
by IL-1 in RA
/ \ I
Induction of I Bone and acute and chronic [ cartilage resorption
Inflammation J
Fig 1. IL-1 in RA.
versus-host disease (GVHD), and inflammatory bowel disease. The preliminary results of clini- cal trials in humans indicate possible efficacy of IL-lra in sepsis syndrome, RA, and GVHD. 21
Because of the potential therapeutic applica- tion of IL-lra, it has been studied in rheumatoid and normal synovia for evidence of endogenous production. Deleuran et aP 2 found IL-lra by immunochemical methods in synovial tissue from RA patients (10 of 18 samples), as well as in five of eight osteoarthritis (OA) synovial samples, and in two of eight normal synovial tissues.
In another immunohistochemical study, IL- lra and IL-113 were shown to be expressed in RA synovial tissue macrophages and lining cells. OA synovial tissues had fewer IL-1- and IL-lra-positive macrophages. Also, Northern blot analysis showed steady-state IL-lra and ]L-113 mRNAs from RA patients' macrophages, whereas normal peripheral blood monocytes did not express IL-lra without exogenous stimuli. 33
With respect to IL-lra distribution, it was found in the sublining of the RA tissues, particu- larly with a pcrivascular distribution or adjacent to lymphoid aggregates. 2° CD14+/IL-lra + mac- rophages were observed in the lining of RA and OA tissue samples. These authors also observed IL-lra in 75% of synovial tissues from OA patients, especially in the lining. No IL-lra was detected in three normal nonarthritic synovial tissues, or in inflammatory synovial tissue from a patient with tenosynovitis.
The expression of the IL-lra gene also has been investigated and its mRNA has been detected in synovial tissues. IL-lra mRNA was found by Northern blot in five of six RA tissues, and in one of three OA tissues. 2° By in situ hybridization, IL-lra mRNA was observed in RA synovial tissue in perivascular regions of the sublining, and it correlated with regions that expressed IL-lra protein. In situ hybridization of OA tissue showed a similar pattern to that of the mRNA by immunochemical methods, mainly in the intima lining.
Furthermore, supernatant fluids from syno- vial tissue cells inhibited rIL-1 activity, esti- mated by rIL-l-induced thymocyte in vitro pro- liferation. Preincubation of the supernatant fluids with anti-IL-lra antibodies blocked the neutralizing effect. 2° Four out of five synovial tissues from OA patients, six out of eight from RA patients, one seronegative individual with inflammatory arthritis, and one patient with avascular necrosis, were IL-lra positive. The glycosylated 26 kD form was the main form found. IL-lra was also found in the lining of several RA synovia, but the staining was signifi- cantly higher in the sublining than in the lining in RA. On the other hand, Deleuran et aP 2 found IL-lra in the lining and vessels of RA and OA synovia. They observed IL-lra in 35% of the RA lining and in 45% of the OA lining, and also in 25% and 35% of endothelial vessel cells from RA and OA synovium, respectively (no significant differences).
IL-lc~ and IL-1RI are expressed in a great number of cells from synovial tissue vessels of RA. Conversely, IL-lra is found only in certain vessels, which correlates with the importance of the interaction between IL-1 and synovial endo- thelial ceils. The coexistence of an increase of IL-loL and IL-1R, with low expression of IL-lra in endothelial cells from vessels of synovial tissue, suggests that IL-1 plays a role as a modulator of cell migration toward synovium. 32
Other authors have also reported that super- natants from synovial fluid (SF) mononuclear cells inhibit the binding of 12SI-rhlL-lo~ to its receptor on murine thymoma in a dose-depen- dent fashion. 34 After fractionating the superna- tants by chromatography, the same fractions blocked the binding of radioactive IL-lo~, as well as the IL-l-induced production of PGE2 by

544 WECKMANN AND ALCOCER-VARELA
fibroblasts. The IL-1 inhibitor obtained from these supernatant fluids had a molecular weight of 21.5 kD, similar to that of the urine-derived inhibitor or to rhIL-lra.
To investigate the possible role of IL-lra in RA, IL-lra and IL-1 protein levels in SF samples from patients with active RA or with a variety of other inflammatory and noninflammatory ar- thropathies were measured, using sensitive and specific sandwich enzyme-linked immunosor- bent assays (ELISAs). IL-1 was undetectable in all SF samples analyzed; however, IL-lra levels were elevated in more than 80% of the RA SF samples and correlated with the SF neutrophil (PMN) concentrations. In this work, 3s cultured SF PMN were shown to produce small amounts of IL-lra and may be one source of this mol- ecule within the SF.
The production of IL-la, IL-113, and IL-lra by freshly isolated and cultured synovial tissue cells from RA and OA patients, also has been assessed by ELISAs. 36 The concentrations of IL-1 and IL-lra in OA samples were similar to those of RA samples. Perhaps this is because equal numbers of OA and RA cells were used in the experiments, which would correct for the lesser number of cells normally found in intact OA tissue sections. 36 The amounts of IL-1 and IL-lra produced were low in freshly isolated cell lysates, and increased during culture. The ratios of IL-lra to total IL-I in RA plus OA (overall) were 1.2 in fresh cell lysates, 1.8 in 3-day cell lysates, and 3.6 in culture supernatant fluids. In spite of IL-lra production, IL-1 activ- ity persisted in synovial tissue supernatant fluids in this work. There was an increase of IL-1 production combined with a decrease of IL-lra production by synovial tissue cells. When icIL- lra and sIL-lra mRNAs were studied by reverse- transcription polymerase chain reaction (RT- PCR), icIL-lra mRNA was found to be more abundant than sIL-lra mRNA in fibroblastlike synoviocytes and unfractionated synovial tissue cells from RA patients. The high icIL-lra:sIL- lra mRNA ratio in fibroblastlike synoviocytes correlated with the lack of IL-lra secretion by these cells. 36
Different studies have shown that IL-I~ and IL-lra have different regulatory patterns of production. Certain factors, such as soluble IgG or GM-CSF, enhance IL-lra production with- out stimulating that of IL- 113.3v,38
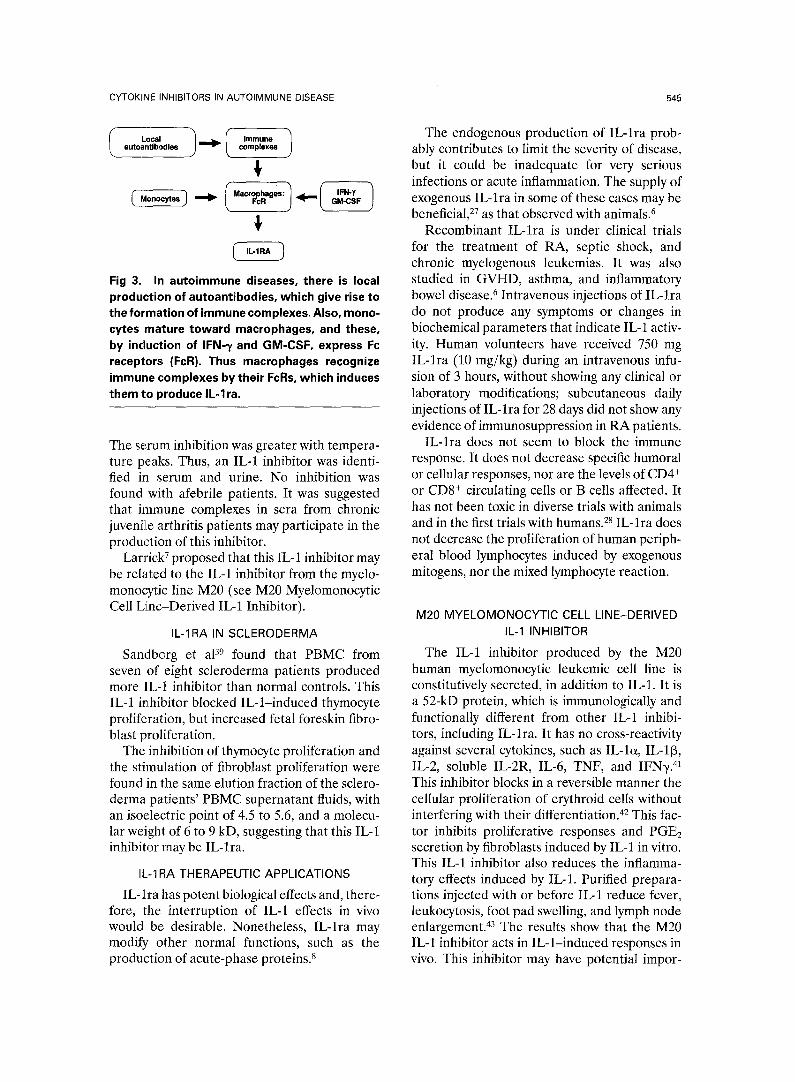
As monocytes mature and become macro- phages in culture, their IL-1 production de- creases and their IL-lra production increases. Thus, tissue macrophages are an important source of IL-lra 5 (Fig 3). Synovial macrophages of RA or OA are the main IL-lra-expressing cells, z°
The finding of simultaneous production of IL-l[3 and IL-lra by synovial macrophages in RA indicates that the same cells participate in joint destruction, by the production of IL-l[3, and in autocrine and paracrine modulation of this destruction, through IL-lra. 33
There is a paradox in the amount of synovial inflammation observed in synovial tissue from RA patients, in spite of the presence of IL-lra. This IL-lra may be a relatively weak inhibitor of the biological activity of IL-1, and it is needed in excess to function. The production of inhibitory activity of IL-1 by rheumatoid synovium macro- phages may be a natural control mechanism. It is possible that the persistent active synovitis is attributable to inadequate synthesis of antago- nists, and not to excessive production of ago- nists. 5
IL-1RA IN JUVENILE ARTHRITIS
Sandborg et a139 reported no IL-1 inhibitory activity from supernatant fluids of peripheral blood mononuclear cells (PBMC) of chronic juvenile rheumatoid arthritis patients. Con- versely, Prieur et al 4° observed a decrease of IL-1 activity in serum and urine from general- ized chronic juvenile arthritis febrile patients.
FIbrobl~
IFN-7 and ~ ~~b~l , T Cell other ~ ~ \
~1 ) Maerophage - - ~ ) Antigen
presenting Artlcula cell cartilage ~ ) roe~.
between T cells, macro- Fig 2. Interactions phages, antigen-presenting cells, and cytokines within synovium that contribute to joint damage (see text).
CYTOKINE INHIBITORS IN AUTOIMMUNE DISEASE 545
( .o. ) i,=o. ) autoantlbodles ~ complexes
_ .
Fig 3. In autoimmune diseases, there is local production of autoantibodies, which give rise to the formation of immune complexes, Also, mono- cytes mature toward macrophages, and these, by induction of IFN-x and GM-CSF, express Fc receptors (FcR). Thus macrophages recognize immune complexes by their FcRs, which induces them to produce IL-lra.
The se.rum inhibition was greater with tempera- ture peaks. Thus, an IL-1 inhibitor was identi- fied in serum and urine. No inhibition was found with afebrile patients. It was suggested that immune complexes in sera from chronic juveni]le arthritis patients may participate in the production of this inhibitor.
Larrick 7 proposed that this IL-1 inhibitor may be related to the IL-1 inhibitor from the myelo- monocytic line M20 (see M20 Myelomonocytic Cell Line-Derived IL-1 Inhibitor).
IL-1RA IN SCLERODERMA
Sandborg et aP 9 found that PBMC from seven of eight scleroderma patients produced more IL-1 inhibitor than normal controls. This IL-1 inhibitor blocked IL-l-induced thymocyte proliferation, but increased fetal foreskin fibro- blast proliferation.
The inhibition of thymocyte proliferation and the stimulation of fibroblast proliferation were found Jin the same elution fraction of the sclero- derma patients' PBMC supernatant fluids, with an isoelectric point of 4.5 to 5.6, and a molecu- lar weight of 6 to 9 kD, suggesting that this IL-1 inhibitor may be IL-lra.
IL-1RA THERAPEUTIC APPLICATIONS
IL-lra has potent biological effects and, there- fore, the interruption of IL-1 effects in vivo would be desirable. Nonetheless, IL-lra may modify other normal functions, such as the production of acute-phase proteins. 8
The endogenous production of IL-lra prob- ably contributes to limit the severity of disease, but it could be inadequate for very serious infections or acute inflammation. The supply of exogenous IL-lra in some of these cases may be beneficial, 27 as that observed with animals. 6
Recombinant IL-lra is under clinical trials for the treatment of RA, septic shock, and chronic myelogenous leukemias. It was also studied in GVHD, asthma, and inflammatory bowel disease. 6 Intravenous injections of IL-lra do not produce any symptoms or changes in biochemical parameters that indicate IL-1 activ- ity. Human volunteers have received 750 mg IL-lra (10 mg/kg) during an intravenous infu- sion of 3 hours, without showing any clinical or laboratory modifications; subcutaneous daily injections of IL-lra for 28 days did not show any evidence of immunosuppression in RA patients.
IL-lra does not seem to block the immune response. It does not decrease specific humoral or cellular responses, nor are the levels of CD4 + or CD8 + circulating cells or B cells affected. It has not been toxic in diverse trials with animals and in the first trials with humans. 28 IL-lra does not decrease the proliferation of human periph- eral blood lymphocytes induced by exogenous mitogens, nor the mixed lymphocyte reaction.
M20 MYELOMONOCYTIC CELL LINE-DERIVED IL-1 INHIBITOR
The IL-1 inhibitor produced by the M20 human myelomonocytic leukemic cell line is constitutively secreted, in addition to IL-1. It is a 52-kD protein, which is immunologically and functionally different from other IL-1 inhibi- tors, including IL-lra. It has no cross-reactivity against several cytokines, such as IL-I~, IL-1[3, IL-2, soluble IL-2R, IL-6, TNF, and IFN-/. 41 This inhibitor blocks in a reversible manner the cellular proliferation of erythroid cells without interfering with their differentiation. 4~ This fac- tor inhibits proliferative responses and PGE2 secretion by fibroblasts induced by IL-1 in vitro. This IL-1 inhibitor also reduces the inflamma- tory effects induced by IL-1. Purified prepara- tions injected with or before IL-1 reduce fever, leukocytosis, foot pad swelling, and lymph node enlargement. 43 The results show that the M20 IL-1 inhibitor acts in IL-l-induced responses in vivo. This inhibitor may have potential impor-

546 WECKMANN AND ALCOCER-VARELA
tance as an antiinflammatory or immune regula- tory factor.
The injection of IL-1 increases the levels of corticosterone and fibrinogen, which decreases by the IL-1 inhibitor derived from M20 cells. 44 Also, this inhibitor reverses the reduction of zinc and iron levels and the increase of copper levels in plasma attributable to IL-1, and this could have a favorable influence on the inflam- matory process.
SOLUBLE IL-1 RECEPTOR
Certain soluble cytokine receptors function as cytokine inhibitors; they originate from the extracellular domains of membrane receptors, and lack the transmembrane and cytoplasmic domains. 1,45 Their affinities for cytokines are generally identical to those of the membrane receptors.
Cytokine receptors can be classified into fami- lies and subfamilies, 4 as shown in Table 5. There are two soluble forms of the IL-1 receptors, sIL-1RI and slL-1RII. They are generated by proteolysis of the extracellular domains. Soluble IL-1RI found in normal serum binds IL-lra with higher affinity than IL-loL or IL-113, whereas sIL-1RII seems to bind IL-I[3 better. 46 This has been confirmed with the use of immobilized
Table 5: Classification of Cytokine Receptors
Families Ligands
Class I (Hematopoiet ic
receptors)
Common chain IL-6, CNTF, OSM, LIF,
(gp 130) IL-11
13-Chain IL-3, IL-5, GM-CSF ~-Chain IL-2, IL-4, IL-7, (IL-13,
IL-15)
Class II IFN receptors IFN
Ig superfamily recep- IL-1, CSF-1, Steel factor, tors FIt3L
TNF-like receptors TNF, NGF, CD27L, CD30L, CD40L
G-prote in-coupled Chemokines
receptors
Abbreviations: IL, interleukin; CNTF, ciliary neurotrophic factor; OSM, oncostatin M; LIF, leukemia inhibitory factor; GM-CSF, granulocyte-macrophage colony-stimulating factor; IFN, inter- feron; CSF-1, colony-stimulating factor 1; F153L, ligand of the fms-like tyrosine kinase; L, ligand; NGF, nerve growth factor. From Debets and Savelkouh Immunol Today 15:455-458, 1994.
slL-1RII, 47 wherein this receptor was shown to bind IL-113 with higher affinity than IL-loL or IL-lra. IL-l[3 had a slower dissociation rate from the receptor.
IL-1RII can either be shed spontaneously or by in vitro induction, probably involving prote- olysis. Shedding may be a kind of feedback signaling, because sIL-1RII is an antagonist of IL-I[3 .4
Several studies have shown that slL-1Rs have an inhibitory function in the homeostasis of IL-1 and thus may be added to the list of proteins with potential applications as IL-1 inhibitors, s Soluble IL-1R has been found in plasma and SF, and it is produced by activated PBMC. This soluble receptor binds to IL-l[3 but not to IL-lo~ or IL-lra (it may be sIL-1RII).
Human IL-lra binds to both human IL-1RI and IL-1RII on cell surfaces, although with 100-fold greater avidity to IL-1RI. IL-lra may bind preferentially to soluble IL-1RI and not at all to soluble IL-1RII. 21
Because sIL-1RI and sIL-1RII bind avidly to IL-lra and IL-113, respectively, their presence in human fluids might hinder the accurate detec- tion of the ligands. 47 The slL-1RI levels in SF from RA patients correlate inversely with IL- lra levels, which is compatible with the finding that slL-1RI binds to IL-lra avidly and preferen- tially over IL-lo~ or IL-113. Thus, sIL-1RI may bind IL-lra in the SF in vivo.
In the same study, IL-I[3 was not detected in SF from RA patients, which may have been attributable to the high levels of slL-1RII ob- served in the same fluids. The authors suggested that the highly variable reported levels of IL-I[3 in different studies may be caused by the effects of sIL-1RII on the detection assays. The produc- tion or administration of sIL-1RI might prefer- entially decrease the antiinflammatory effects of IL-lra.
There is a "double-edged sword" phenom- enon when soluble receptors are used, because they may antagonize as well as agonize certain functions. For example, in a murine model of alloreactivity, sIL-4R renders the allograft a prolonged survival, but sIL-4R does not block IL-4-induced IgE synthesis. Therefore, the ra- tio between sIL-4R and IL-4 is very important when considering sIL-4R therapeutic applica- tions. 4 In spite of an antagonist activity of soluble cytokine receptors, these can also act as

CYTOKINE INHIBITORS IN AUTOIMMUNE DISEASE 547
agonists, because they may form complexes with the ligand and function as carrier molecules.
The importance of soluble cytokine receptors is illustrated by several viruses. For example, cowpox and vaccinia viruses encode a protein in their open reading frame that is homologous to the extracellular domain of the slL-1RII. 48 Also, some pox viruses encode proteins that bind to TNF, and cytomegaloviruses encode proteins that bind to chemokines. 4 The cowpox virus Crma protein inhibits the IL-l[3 converting enzyme. 49 This protein may have therapeutic potential. 2
OTHER IL-1 INHIBITORS
In addition to IL-lra, other IL-1 inhibitors are: (1) uromodulin found in urine from preg- nant women, which is a glycosylated form of the Tamm-Horsfall protein (THP). It binds to IL-1 and TNF and other cytokines. 7 THP is a major protein component of urine. Uromodulin, a concavalin A (Con-A)-binding fraction of THP, inhibits T cell activation. Lambert et al so re- ported that THP inhibits the cytotoxicity of TNF-a in vitro, but THP may interact with the cells or with the extracellular matrix; (2) c~-2- macroglobulin, which is not specific because it binds to IL-1, IL-2, IL-6, and platelet-derived growth factor (PDGF). It does not seem to interfere with IL-1 binding or activation, and it may function by promoting the activity of cer- tain cytokines, and by inhibiting others; (3) corticosteroids, which suppress IL-1 transcrip- tion and synthesis when added before transcrip- tion is triggered; and (4) e~-melanocyte-stimulat- ing factor, which efficiently inhibits multiple IL-1 effects, such as fever, hyperalgesia, neutro- philia, and PGE2 synthesis.
Table 6: TNF-~ Properties
Induction of in vitro production of collagenase and
PGE2 by synovial fibroblasts and chondrocytes
Stimulation of bone resorption and fibrobtast prolif-
eration
Stimulation of IL-1 and GM-CSF production by RA synovial mononuclear cells
Increased potential tissue damage by IL-1
Abbreviations: TNF-c~, tumor necrosis factor-c~; PGE2, prosta- glandin E2; IL-1, interleukin-1; GM-CSF, granulocyte-macro- phage colony-stimulating factor; RA, rheumatoid arthritis.
TUMOR NECROSIS FACTOR
Tumor necrosis factor-~ (TNF-~) is a cyto- kine produced primarily by monocytes and mac- rophages. It is found in cells of the synovial membrane and in interstitial macrophages. Mononuclear cells from joints of RA patients produce TNF-e~. 51 It shares many properties with IL-1, 5 such as those shown in Table 6. TNF-a, alone or combined, also regulates the expression of HLA class II molecules and of adhesion molecules (integrins and selectins), so that its blockade may be beneficial in RA.
TNF-c~ synthesis and secretion can be in- duced when T lymphocytes are cultured with anti-CD2 antibodies. Also, the activation of T cells with a combination of anti-CD2 monoclo- nal antibodies (MAbs) increases the expression of the p75-kD TNF-oL receptor, and minor changes are observed in the expression of the p55-kD TNF-c~ receptor. Thus, the CD2 activa- tion pathway may have a role in the regulation of the TNF-cdTNFR system in T lymphocytes. CD2 may be an alternative pathway for the regulation of the cytokine network that modu- lates T cell function, s2
The following may block the production or biological activities of TNF-oL: (1) PGE= at high concentrations suppresses lipopolysaccharide (LPS)-induced TNF-a mRNA accumulation; (2) corticosteroids suppress the increase of endotoxin-induced TNF-c~ mRNA; (3) soluble TNF-a receptors block the TNF-e~-induced pro- duction of PGE2 by dermal fibroblasts and synovial cells, and that of collagenase by syno- vial cells, and also inhibit the respiratory burst in neutrophils.
SOLUBLE TNF RECEPTORS
TNF-~ inhibitors have been isolated from urine of healthy subjects and febrile patients, and from supernatants of rheumatoid SF cells in culture. These molecules are soluble forms of the two TNF-e~ receptors. The extracellular fragments of both receptors may be shed and inhibit the biological effects of TNF-~. 8 Soluble TNF receptor also has been found in sera of patients with cancer, and this receptor blocks the in vitro binding and activity of TNF-c~.
The soluble TNF-a receptors are TNFRI or p55, and TNFRII or p75. They are also called TNF-binding proteins I and II, or sTNFR[3 (TNF-R55-BP) and sTNFRc~ (TNF-R75-BP),

548 WECKMANN AND ALCOCER-VARELA
respectively. 8 Both are members of a family of receptors that comprise the nerve factor recep- tor and CD40. They are found in plasma from normal subjects and are increased in both plasma and SF from RA patients. The in vitro use of these inhibitors suppresses murine fibroblast cytotoxicity induced by murine or human TNF- 0~. 53
The TNF-Rs on synovial mononuclear cells are shed to constitute soluble receptors; such receptors may then act as natural inhibitors within the joint. 54 TNF-R75-BP is shed from T cells, which are abundant within RA joints, or from B cells. 45 TNF-R55-BP may be shed from macrophages, fibroblasts, and epithelial cells.
Both soluble TNF receptors bind to TNF-a, and to a lesser extent to TNF-[~. 45 They have greater affinity for TNF-a than membrane TNFR. 1
TNFR protein and mRNA have been found in normal PBMC, which increased with activa- tion elicited by phytohemagglutinin or IL-2. Synovial membrane or fluid resting cells of patients with RA have TNFR mRNA (p55 and p75). Synovial membrane resting cells from OA patients also have TNFR mRNA. s4
Brennan et a154 have reported, as shown in Table 7: (1) a significant increase of TNF-Rp75 on synovial membrane mononuclear cells of RA patients, compared with normal PBMC; (2) that TNF-Rp75 was increased, although not signifi- cantly, in SF mononuclear cells of RA patients (this receptor was significantly increased in CD3 ÷ T cells from SF, compared with blood cells); (3) that TNF-Rp75 was not increased on
Table 7: Expression of TNF-Rp75 on Mononuclear Cells From Peripheral Blood, Synovial Fluid, or Synovial Membrane of
Normal Subjects, RA Patients, or OA Patients
Mononuclear TNF.Rp75
Cells Normal RA OA
Peripheral b lood + + ND
Synovial f luid ND +, 1' 1' * ND
Synovial membrane ND 1̀ 1" +
NOTE. +, present; 1' 1' *, significant increase in synovial fluid CD3 ~ T cells vs. PBMC from one RA patient; 1' 1', significant increase vs. normal PBMC. Abbreviations: TNF, tumor necrosis factor; RA, rheumatoid arthritis; OA, osteoarthritis; ND, not determined; PBMC, periph- eral blood mononuclear cells. Data from Brennan et al. 54
Table 8: Expression of TNF-Rp55 on Mononuclear Cells From Peripheral Blood, Synovial Fluid, and Synovial Membrane of
Normal Subjects, RA Patients, and OA Patients
Mononuclear TNF-Rp55
Cells Normal RA OA
Peripheral blood + + ND Synovial fluid ND + ND Synovial membrane ND I" 1" 1"
NOTE. +, present; ~, nonsignificant increase vs. normal PBMC I', significant increase vs. normal PBMC.
Abbreviations: TNF, tumor necrosis factor; RA, rheumatoid arthritis; OA, osteoarthritis; ND, not determined; PBMC, periph- eral blood mononuclear cells. Data from Brennan et al. 54
the surface of PBMC of RA patients, or on synovial membrane mononuclear cells of OA patients.
With regard to TNF-Rp55, Table 8 summa- rizes that: (1) TNF-Rp55 was increased on synovial membrane mononuclear cells of RA patients, compared with normal PBMC; (2) TNF-Rp55 was not increased on PBMC, nor on SF mononuclear cells of RA patients; (3) TNF- Rp55 was increased, but without significant levels on synovial membrane mononuclear cells of OA patients.
With respect to soluble receptors, increased levels of both TNF-R55-BP and TNF-R75-BP have been found in sera from RA and OA patients compared with healthy individuals. 4s Levels of both soluble receptors were higher in RA sera than in OA sera. Also, both soluble TNFRs were significantly higher in SF from RA patients than in fluids from OA or seronegative arthropathies.
When SF and sera levels from RA patients were compared, the former were significantly higher, which suggests that there is a local production of TNFR within the joint. No corre- lation was found between TNF-R and soluble TNFR levels.
Moreover, Cope et a145 observed that SF from RA or OA patients blocked TNF-a cytotoxicity in 80% and 26%, in vitro, respectively. This inhibition could be reverted if the SF was preincubated with monoclonal antibodies di- rected to both TNFRs.
Nevertheless, in spite of the detection of augmented TNFR levels in SF from RA pa- tients, such levels were inadequate for complete

CYTOKJNE INHIBITORS IN AUTOIMMUNE DISEASE 549
neutralization of TNF-a. If the TNF-a activity was further blocked, the process of joint destruc- tion would probably be abrogated. Therefore, the development of clinical trials of anti-TNF-oL therapy may be promising. 45
After treatment of six RA patients with prednisolone and sulfasalazine, a shift of the serum levels of TNFR was observed after 6 weeks. TNFR and C-reactive protein levels and the e~Tthrocyte sedimentation rate decreased, whereas hemoglobin increased with treat- ment. 45
Plasma concentrations of soluble TNF recep- tors were measured in patients with systemic lupus erythematosus (SLE), progressive sys- temic sclerosis (PSS), and mixed connective tissue disease (MCTD)Y Both types of soluble TNF receptors in SLE and PSS patients, and p75 soluble TNF receptor in MCTD patients, were significantly increased compared with con- trols. Plasma concentrations of both soluble receptors showed a high correlation in the three groups of patients. Sera of patients neutralized TNF-~ cytotoxicity, and in the presence of anti-TNF receptor monoclonal antibodies, these sera were not able to inhibit TNF-a cytotoxicity. In one patient with SLE, autoantibodies against the p75 TNF receptor were found. These auto- antibodies did not interfere with the binding to TNF, but they may affect the balance between TNF-e~ and its antagonists.
In another study, 53 SLE patients and 140 healthy subjects were tested for soluble TNF receptors. Both types were significantly higher in 46 of the SLE patients compared with con- trols. Levels of soluble TNF receptors may be useful markers of SLE activity. The incidence and the extent of the increase of these receptors correlated with disease activity more than the titers of anti-dsDNA antibodies. 56
The therapeutic use of soluble TNFRs has the disadvantage of exhibiting a short half-life within the circulation. TNF-R-BPs half-lives may be improved by recombinant DNA technol- ogy. 8 The TNF-R-BP may be fused to other molecules to form chimeric proteins. For ex- ample, the fusion of TNF-R55-BP to the human IgG C3 chain has been achieved, to constitute the TNF-R55-BP/h~/3 chimeric molecule. This was accomplished by inserting the extracellular portion of TNF-R55-BP in the hinge region of the lgG. Also, the covalent union between
TNF-R55-BP and the CH2 and CH3 domains of a murine IgG1 has been accomplished. These two chimeric proteins are bivalent antagonists of TNF, which have a long half life; in mice, these TNF-binding proteins persisted 20 to 30 hours, longer than soluble TNF-Rs' half-lives. 57
ANTI-TNF-oL MONOCLONAL ANTIBODIES
There are natural autoantibodies to cytokines that are found in serum. 4 Among them, there are autoantibodies that react with IL-loL, IL-6, IFNa, and IL-10. They are frequently of IgG1 or IgG4 isotype. Some bind with no specificity to TNF-cq 1L-2, IL-4, and IL,8. Autoantibodies against IL-I[3, IL-lra, IL-3, IFN-[3, or IFN--/ have not been found. The therapeutic applica- tions of intravenous preparations of anticyto- kine antibodies should be considered cau- tiously, because antibodies such as anti-IL-le~ or anti-IL-6 may be antagonistic or agonistic. 4
There is a hierarchy in the cytokine network in RA. TNF-~ can be blocked with specific monoclonal antibodies to reduce the produc- tion of other cytokines, such as IL-1, GM-CSF, and IL-8. 58
Anti-TNF-a monoclonal antibodies have been tested in a model of collagen type II-induced arthritis in mice. The administration of a neutral- izing monoclonal anti-TNF antibody to DBA/1 mice suppresses the clinical manifestations of collagen II-induced arthritis. 59 The hamster anti-murine TNF monoclonal antibody TN3.19.2 significantly diminished inflammation and tis- sue destruction when administered to these mice. 6° It has also been shown that the adminis- tration of anti-TNF-eL MAbs to mice transgenic for the TNF-oL human gene prevents the devel- opment of arthritis. 61
A high-affinity chimeric monoclonal anti- TNF-oL antibody (human IgG1, mouse Fv), with neutralizing activity, has been administered to ten RA patients by intravenous injection. 58 All patients showed clinically beneficial effects along with a reduction of acute-phase protein levels, erythrocyte sedimentation rate, and rheuma- toid factors.
This antibody has been evaluated for safety and efficacy in the treatment of 20 RA pa- tients. 62 It was safe and well-tolerated, with both clinical and laboratory improvement. The Ritchie Articular Index decreased from a me- dian of 28 at zero time to 6 by week 6 of

550 WECKMANN AND ALCOCER-VARELA
treatment; the swollen joint count decreased from 18 to 5 in the same period; IL-6 levels decreased from 60 pg/mL (range, 18 to 500) to 40 pg/mL (range, 0 to 210) at week 2. Thus, anti-TNF-a may be a useful therapeutic agent in RA.
A randomized double-blind study in which a single infusion of 1 or 10 mg/kg of the anti- TNF-a MAb cA2 was given to RA patients, was compared with placebo. 63 The cA2, a chimeric human/murine MAb of IgG1K isotype, neutral- izes cytotoxicity mediated by TNF-a. The Pau- lus index, a combination of six clinical, observa- tional, and laboratory variables, was used to assess RA activity. 63 The achievement at week 4 of a Paulus 20% response was the primary endpoint. Only 8% of placebo patients re- sponded, whereas 44% of patients treated with 1 mg/kg cA2 (P = .0083) and 79% of those treated with 10 mg/kg cA2 (P < .0001) did. More than half of the high-dose cA2 patients improved by 50% using the Paulus criteria (P = .0005). These results were the first evi- dence that specific cytokine blockade can be effective in the treatment of RA.
The same authors repeated treatment of two to four cycles with the same chimeric MAb, 64 but this time the dose was 20 mg/kg in cycle 1 (in two to four infusions) and 10 mg/kg in a single infusion for cycles 2 to 4. The seven patients responded to treatment cycle 1 and showed repeated responses after cycles 2 to 4. The magnitude of the response was maintained. The median Paulus 20% response duration after treatment with 20 mg/kg in cycle 1 was 12 weeks (interquartile range, 8 to 17.4). The duration after treatment with 10 mg/kg was 9 weeks (range, 1 to 19.1) in cycle 2, 8 weeks (3.2 to 12.5) in cycle 3, and 8 weeks (1.6 to 15.2) in cycle 4 (P > .05 compared with cycle 1). Thus, regular treatment with cA2 may achieve long- term disease suppression.
Four patients developed human anti-chi- meric A2 antibody responses, specific for the murine portion of cA2. Two patients were successfully retreated despite this problem. The development of antiglobulin responses to cA2 may be prevented by combination therapy with traditional immunosuppressive drugs. The long- term safety of anti-TNF-~t remains to be rigor-
ously examined so that the risk of infection and other complications can be assessed. 65
Sequential knee synovial biopsies in a small number of patients before and after treatment with cA2 showed a reduction in cellularity. 65 This effect was accompanied by a reduction in the expression of the adhesion molecule E-selectin in vascular endothelium, and by a reduction in circulating soluble E-selectin lev- els. Possibly anti-TNF-a deactivates vascular endothelium and reduces cell migration. Alter- natively, by binding of cA2 to cell-associated TNF-oL and mediating cell lysis through comple- ment fixation or antibody-dependent cell cyto- toxicity, the population of activated macro- phages and polymorphs was reduced.
A study of cell-mediated immune responses of six RA patients treated with anti-TNF (cA2) included the proliferative responses of PBMCs to several mitogens and soluble antigens. 66 Re- sponses to all mitogens were notably impaired before treatment, but increased within 7 days of therapy. All stimulation indices increased after beginning cA2 treatment, and the clinical scores improved. The authors concluded that treat- ment with anti-TNF restored immunosup- pressed patients toward normal, which may have clinical importance in diseases in which inhibition of TNF is beneficial.
With respect to the effect of the isotype of the chimeric anti-TNF-a antibodies, the selection of the therapeutic antibodies may be important. In a rabbit model of human TNF-induced pyrexia, a human/murine chimeric IgG4 anti- human TNF-c~ MAb inhibited pyrexia in a dose-dependent manner, whereas an IgG1 iso- type caused marked pyrexia that indicated an immune complex-mediated response. In experi- mental septic shock in mice, treatment with an IgG1 hamster/routine chimeric anti-murine TNF MAb resulted in 90% survival by 72 hours, whereas an IgG2a variant resulted in 10% survival by 72 hours. The differences were not attributable to pharmacokinetic characteristics of these MAbs. Thus, the isotype can affect the result of the efficacy of anti-TNF-a chimeric MAbs. 67
There is an sTNF-R-Ig construct that antago- nizes TNF-o~ in an animal model of inflamma- tory lung disease? This construct prevented neutrophil infiltration in alveoli. Also, an

CYTOKINE INHIBITORS IN AUTOIMMUNE DISEASE 551
sIFN'yR-Ig construct has been used in animal models of SLE or multiple sclerosis. NZB/WF1 mice spontaneously develop an SLE-like syn- drome. The injection of slFNTR-Ig delayed kidney damage and mortality and prevented the onset of membrane-proliferative glomerulone- phritis, the infiltration of T cells and macro- phages into the kidney, the synthesis of IFN7 and TNF-~, and the expression of major histo- compatibility complex (MHC) class II mol- ecules, ICAM-1, VCAM-1, and IFN,/R on the tubular epithelium and the glomerular cells. The treatment also delayed the production of autoantibodies against dsDNA.
INTERFERON--y
IFN--/is a well-known antagonist of IL-4 in B lymphocytes, by blocking the IL-4-induced ex- pression of MHC class II antigens and CD23, as well as IgG1 and IgE secretion. In addition, IFN--/-induced IgG2a secretion is blocked by IL-4. These effects are not caused by competi- tive binding to surface receptors. 1
Although it is difficult to find IFN--/in syno- vial supernatants, it is produced by T cell clones derived from synovium or SF of RA patients. IFN--/induces HLA-DR expression, proinflam- matory cytokine production, and inhibition of IL-10 production by monocytes. Because IL-10 blocks DR expression, antigen presentation, and production of proinflammatory cytokines, the blocking effect of INF-~/over IL-10 produc- tion may promote autoimmune disease)
There is a mutual antagonism between IFN-,/ and TNF-R for B-type synoviocytes of RA or OA patients68: (1) TNF-o~ inhibits IFN-y- induced DR expression; (2) IFN-y blocks TNF- R-induced synoviocyte proliferation; (3) IFN-y blocks TNF-o~-induced collagenase production; (4) IFN-~ inhibits TNF-oL-induced GM-CSF production.
Conversely, IFN--/ is strongly inhibited by IL-4 and IL-10, and it blocks IL-10 production. The reciprocal inhibitory effect of IFN-,/ and IL-10 over each other's production may explain their lack of secretion in RA synovium, when the cells that secrete them are in close proxim- ity. 3
There is probably a defective control mecha- nism in RA resulting in low IFN-y production.
The lack of IFN-~ within the synovium may help increased TNF-e~ perform its proinflammatory effects. The benefits of IFN-~/as therapy have been modest, probably because IFN--y is able to induce DR in macrophages and does not antago- nize the IL-1 effects. 68
The use of parenteral IFN--/in RA has been moderately successful, and its slight antiinflam- matory effect may include its ability to block synoviocyte TNF-e~-mediated activation. 2°
A prospective study of a 2-year-follow-up of the use of subcutaneous rlFN--/in 70 patients with RA showed that it was well tolerated. Fifty-seven percent of patients after 1 year, and 38% after 2 years, were able to continue treat- ment, 69 and those who tolerated it benefited clinically. After 2 years, 65% of the patients discontinued the use of rlFN-y.
IFN-e~ induced an increase of circulating levels of IL-lra in healthy humans and in patients with hepatitis C, 12 hours after subcuta- neous injection. 7° IFN-,/induced an increase in circulating IL-lra in patients with renal cell carcinoma. Daily injections maintained en- hanced levels. Also, in vitro production of IL-lra by PBMC of healthy individuals was induced by incubation of the cells with INF-e~ or IFN-y. The induction was dose-dependent, and was higher with IFN-m In such diseases where IFN is injected daily, IL-lra levels can probably be maintained.
In addition to an induced increase in IL-lra production by IFN-c~ and IFN-% these cyto- kines also inhibit IL-113 spontaneous production and induction by LPS stimulated synovial mac- rophages of RA patients.
Because both IFNs increased IL-lra in blood, it was not established if IL-lra was an interme- diate of IFN for the inhibition of the cytokines. At least IFN-R induces endogenous IL-lra, which might contribute to certain effects in- duced by IFN. 7°
INTERLEUKIN-4
Interleukin-4 (IL-4) seems to exhibit a coordi- nated antiinflammatory action. 2 It exerts differ- ent effects on cytokines, according to cell type, mode of activation, and type of culture. In synoviocytes, IL-4 blocks IL-l-induced PGE2 and GM-CSF, but increases IL-6 production. 3
552
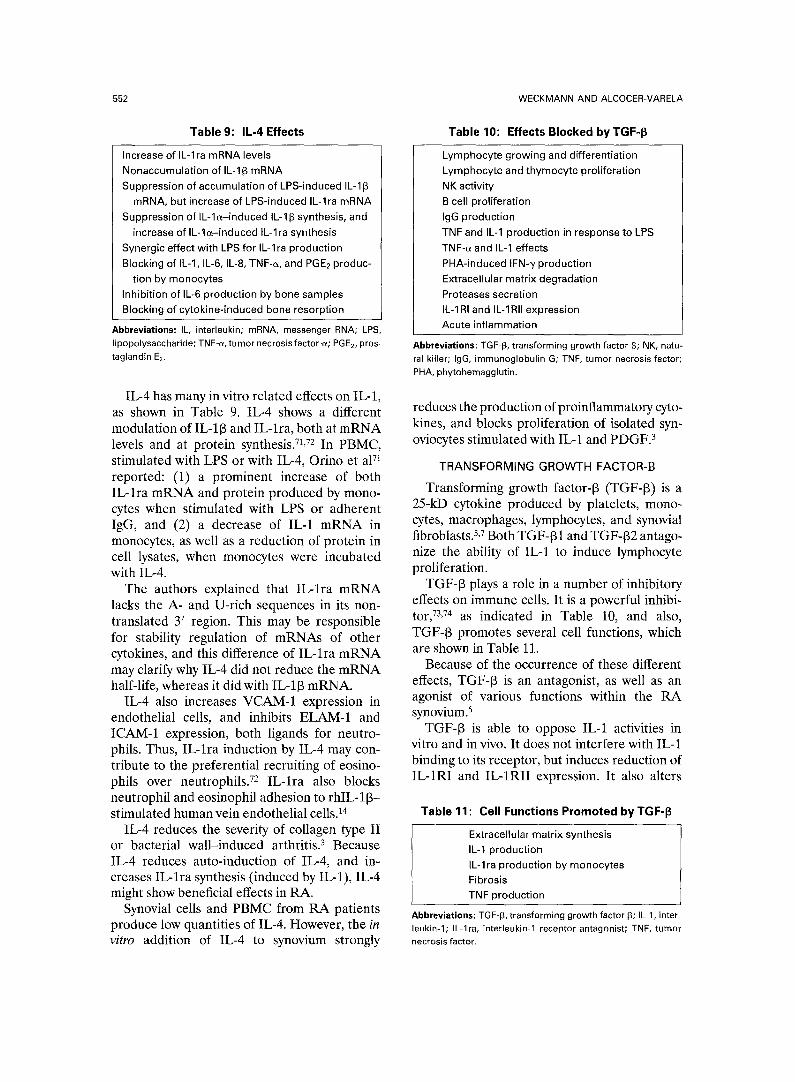
Table 9 : IL -4 Effects
Increase of IL-lra mRNA levels Nonaccumulation of IL-113 mRNA Suppression of accumulation of LPS-induced IL-113
mRNA, but increase of LPS-induced IL-lra mRNA Suppression of IL-le-induced IL-113 synthesis, and
increase of IL-ls-induced IL-1 ra synthesis Synergic effect with LPS for IL-lra production Blocking of IL-1, IL-6, IL-8, TNF-a, and PGE2 produc-
tion by monocytes Inhibition of IL-6 production by bone samples Blocking of cytokine-induced bone resorption
Abbreviations: IL, interleukin; mRNA, messenger RNA; LPS, lipopolysaccharide; TNF-cc, tumor necrosis factor-e; PGE2, pros- taglandin E2.
IL-4 has many in vitro related effects on IL-1, as shown in Table 9. IL-4 shows a different modulation of IL-l[3 and IL-lra, both at mRNA levels and at protein synthesis. 71,72 In PBMC, stimulated with LPS or with IL-4, Orino et a171 reported: (1) a prominent increase of both IL-lra mRNA and protein produced by mono- cytes when stimulated with LPS or adherent IgG, and (2) a decrease of IL-1 mRNA in monocytes, as well as a reduction of protein in cell lysates, when monocytes were incubated with IL-4.
The authors explained that IL-lra mRNA lacks the A- and U-rich sequences in its non- translated 3' region. This may be responsible for stability regulation of mRNAs of other cytokines, and this difference of IL-lra mRNA may clarify why IL-4 did not reduce the mRNA half-life, whereas it did with IL-113 mRNA.
IL-4 also increases VCAM-1 expression in endothelial cells, and inhibits ELAM-1 and ICAM-1 expression, both ligands for neutro- phils. Thus, IL-lra induction by IL-4 may con- tribute to the preferential recruiting of eosino- phils over neutrophils. 72 IL-lra also blocks neutrophil and eosinophil adhesion to rhIL-l[3- stimulated human vein endothelial cells. 14
IL-4 reduces the severity of collagen type II or bacterial wall-induced arthritis. 3 Because IL-4 reduces auto-induction of IL-4, and in- creases IL-lra synthesis (induced by IL-1), IL-4 might show beneficial effects in RA.
Synovial cells and PBMC from RA patients produce low quantities of IL-4. However, the in vitro addition of IL-4 to synovium strongly
WECKMANN AND ALCOCER-VARELA
Table 10: Effects Blocked by TGF-~
Lymphocyte growing and differentiation Lymphocyte and thymocyte proliferation NK activity B cell proliferation IgG production TNF and IL-1 production in response to LPS TNF-a and IL-1 effects PHA-induced IFN--y production Extracellular matrix degradation eroteases secretion IL-1RI and IL-1RII expression Acute inflammation
Abbreviations: TGF-13, transforming growth factor 13; NK, natu- ral killer; IgG, irnmunoglobulin G; TNF, tumor necrosis factor; PHA, phytohemagglutin.
reduces the production of proinflammatory cyto- kines, and blocks proliferation of isolated syn- oviocytes stimulated with ]L-1 and PDGF. 3
TRANSFORMING GROWTH FACTOR-B
Transforming growth factor-[3 (TGF-[3) is a 25-kD cytokine produced by platelets, mono- cytes, macrophages, lymphocytes, and synovial fibroblasts. 5,7 Both TGF-[3 1 and TGF-t32 antago- nize the ability of IL-1 to induce lymphocyte proliferation.
TGF-13 plays a role in a number of inhibitory effects on immune cells. It is a powerful inhibi- tor, 73,74 as indicated in Table 10, and also, TGF-13 promotes several cell functions, which are shown in Table 11.
Because of the occurrence of these different effects, TGF-[3 is an antagonist, as well as an agonist of various functions within the RA synovium. 5
TGF-13 is able to oppose IL-1 activities in vitro and in vivo. It does not interfere with IL-1 binding to its receptor, but induces reduction of IL-1RI and IL-1RII expression. It also alters
Table 11: Cell Functions Promoted by TGF-13
Extracellular matrix synthesis IL-1 production IL-lra production by monocytes Fibrosis TNF production
Abbreviations: TGF-13, transforming growth factor 13; IL-1, inter- leukin-1; iL-lra, interleukin-1 receptor antagonist; TNF, tumor necrosis factor.

CYTOKINE INHIBITORS IN AUTOIMMUNE DISEASE 553
IL-l-induced functions, such as collagenase production by synovial cells, thymocyte and lymphocyte proliferation, and chondrocyte acti- vation. 75
When murine normal hematopoietic progeni- tor cells were treated with IL-3, IL-1R expres- sion increased, but when these cells were then treated with TGF-[3, IL-1R expression was re- duced. 75 This reduction was also observed in several[ murine myeloid and lymphoid progeni- tor cell lines, and in human and murine bone marrow.
Because TGF-[3 is able to induce IL-1 mRNA in monocytes, and also to reduce IL-1R expres- sion, the receptor inhibition prevents the cells from responding to IL-1. This explains how TGF-[3, minimizes inflammatory responses and promotes the repair process. 75
In addition, TGF-13 is able to induce IL-lra expression in monocytes. 74,76 Supernatant fluids of monocytes kept in culture with TGF-[3 blocked IL-1 binding to its receptor. When these supernatants were precipitated with anti- IRAP (anti-IL-lra) monoclonal antibodies, Western blot analysis of the precipitates, with another anti-IRAP antibody, showed a 25-kD band, which corresponded to IRAP. TGF-[3 also induces IRAP mRNA in PBMC.
According to the aforementioned, TGF-[3 fulfills a role as an antiinflammatory cytokine, whereas 1L-1 and TNF show proinflammatory effects, s
With regard to TGF-[3 and TNF-~, these two cytokines are mutual antagonists. For example, the injection of TGF-[3 or anti-TNF-~ antibody protects rats against collagen type II-induced arthritis. In contrast, TNF-a or anti-TGF-[3 antibody injection enhances this arthritis. 76
There are high levels of TGF-[3 in synovial effusions from RA patients, whereas OA pa- tients have lower levels, s Rheumatoid synovial tissue produces TGF-[3 in vitro, and TGF-[3 mRNA is found in synovial macrophages and fibroblasts of RA patients. Thus, TGF-[3 may have clinical applications for the control of autoimmune diseases. 73
Kuruvilla et a173 studied the effect of TGF-13 injection on the induction of experimental aller- gic encephalomyelitis (EAE) in mice. Daily intraperitoneal injections during 2 weeks de- layed, but did not suppress, the development of
EAE. TGF[3-1 injections prevented spontane- ous recurring attacks of EAE. The authors also reported the results of TGF-131 injections in mice several weeks after the onset of collagen- induced arthritis. The course of the disease was not modified, but anti-collagen type 11 antibody titers were significantly reduced in mice treated for 4 days.
Histopathological joint changes decreased considerably when TGF-[31 was injected on days 14 through 18, or 28 through 32, after immunization with collagen. Neither hyperpla- sia of the lining membrane cells nor accumula- tion of mononuclear cells or connective tissue was observed.
INTERLEUKIN-10
Interleukin-10 (IL-10) is produced by human T cell clones, peripheral blood T and B acti- vated cells, monocytes, and Epstein-Barr virus- transformed B cell lines. IL-10 and IL-4 have similar effects on cytokine expression by mono- cytes. IL-10 blocks monocyte production of IL-loL, IL-l[3, IL-6, IL-8, TNF-~, GM-CSF, and G-CSF, after activation with LPS. This cytokine displays outstanding modulating effects of im- mune and inflammatory responses, because of its ability to decrease MHC class II expression and to block proinflammatory cytokine produc- tion by monocytes. Because IL-10 has inhibitory regulating effects on proinflammatory cyto- kines, which participate in chronic and acute inflammation in autoimmune diseases such as RA, SLE, and Sj6gren's syndrome (SS), likely IL-10 is a strong inhibitor of inflammation. 77,78
IL-10 has been difficult to detect in rheuma- toid synovium supernatants, despite the great number of monocytes in RA synovium. Incuba- tion of synovium with IL-10 reduces proinflam- matory cytokine production, although its effect is not as potent as that observed with IL-4. It appears that IL-10 serves mainly as a suppressor of immune functions, and that IL-4 has antiin- flammatory actions, 3 because IL-10 inhibits the effects of several proinflammatory cytokines, 77 and IL-4 increases IL-lra mRNA and decreases IL-1 mRNA in PBMC. 71
The production of IL-10 mRNA and protein by PBMC from SLE, RA, and SS patients is increased when compared with normal sub- jects. 78 Interleukin-10 is mainly produced by B

554 WECKMANN AND ALCOCER-VARELA
lymphocytes and monocytes. T lymphocytes con- tributed scantily to IL-10 production in these patients. The results indicate an IL-10 gene dysregulation.
In a recent study of 11 RA and 17 OA synovial membranes, IL-10 protein was sponta- neously produced. 79 Also, IL-10 mRNA was found in synovial tissues of five of five RA patients, and in four of five OA patients. IL-10 also was observed by immunohistological stain- ing in the lining layer of the synovial membrane, and double staining showed that monocytes and T cells produced this cytokine.
Interestingly, when IL-10 was blocked with an anti-IL-10 MAb, the production of TNF-~ and IL-I[3 by synovial membrane cultures increased significantly. The addition of exogenous IL-10 to synovial membrane cultures inhibited the production of TNF-oL and IL-113. Blocking of IL-1 (with IL-lra), or of TNF-c~ (with anti- TNF-~ antibody), decreased IL-10 production. Therefore, it seems that IL-10, IL-lra, and soluble TNFRs participate in an antiinflam- matory response in RA, by blocking proinflam- matory cytokines. The authors suggested that there is a relative deficit in IL-10 production in RA.
MUTATED CYTOKINES
A mutant form of IL-4, in which the tyrosine residue at position 124 is replaced by aspartic acid, blocks IL-4 and IL-13-induced B cell proliferation, and IgG4 and IgE synthesis, when the cells are costimulated with anti-CD40 MAb. IL-4 mutants therefore may be useful in the treatment of atopy. There are also mutant forms of GM-CSF that fail to bind to the GM-CSF-R and antagonize GM-CSF activity. 4
FUTURE APPROACHES WITH ANTAGONISTS
Multiple data supports the use of anticyto- kines as therapeutic agents, but the develop- ment of projects to test them has been slow. The most promising are IL-lra, soluble IL-1R, and soluble TNFRs. 57 Also, monoclonal antibodies against cytokines and their receptors have been tested, 2 and TGF-131 also has possible therapeu- tic application. 73
Parenteral administration of cytokine recep- tor antagonists has been suggested, because it not only exerts a beneficial therapeutic effect at the site of inflammation, but also interacts with many other cytokine-dependent functions.
The combination of a cytokine receptor an- tagonist (such as IL-lra) with a binding protein (such as slL-1R) represents one of the best therapeutic approaches. This is based on the fact that the binding of a cytokine molecule (in the example, IL-1) to its membrane receptor may be prevented both by directly blocking its receptor with the antagonist and by cytokine binding to the soluble receptor. New strategies must improve treatment of immunoinflam- matory diseases in a more specific fashion than current disease-modifying anti-rheumatic drugs (DMARDs). 8
Because of redundancy of the cytokine net- work in RA, inhibition of only one cytokine may be insufficient. As IL-1 and TNF-~ display similar effects, inhibiting only one would not have a meaningful impact, whereas therapy against both would have a greater probability of success. The combination of sTNFR or IFN--/ (against TNF-a) with IL-lra (against IL-1) has been suggested, z° The possible deficit of IL-10
11.-4
s y i TNF-cc IL-1RI, IL.1RII
IL-10 ~RA IL.1
Fig 4. Future approaches with antagonists. The use of several cytokines, such as IFN--/, IL-4, TGF-13, IL-2, IL-6, and IL-10, may enhance IL-lra production, which would block IL-1. Further- more, TGF-~ may inhibit IL-1RI and IL-1RII expres- sion. Simultaneously, IFN~ would block TNF-Q, along with soluble TNF receptors. White arrows indicate induction; black arrows indicate inhibi- tion.

CYTOKINE INHIBITORS IN AUTOIMMUNE DISEASE 555
production in RA suggests that this cytokine is a feasible therapeutic agent, 79 because IL-10 in- duces IL-lra and sTNF-R from monocytes.
Also, the recent finding of the IL-2 and IL-6 induction of IL-lra and soluble TNFR produc- tion in cancer patients 8°,8a leads to the use of several cytokines (Fig 4) that may enhance the production of both antagonists. This would indirectly dampen IL-1- and TNF-u-induced inflammatory effects.
With respect to targeted immunotherapy, the use of a fusion toxin, which is a synthetic protein
that comprises the diphtheria toxin sequence, has proved to be a potential immune response modifier in RA. s2 When this fusion toxin (termed DAB486IL-2) was administered to DMARDs- resistant RA patients, clinical improvement was observed. The use of this protein is based on the differential expression of high-affinity IL-2R on activated T lymphocytes, so that these ceils may be targets of DAB486IL-2 cytotoxicity. Neverthe- less, the number of patients in this phase I-II trial was small, and no persistent decrease of circulating T cells was shown.
REFERENCES 1. Fernfindez-Botran R: Soluble cytokine receptors: Their
role in immunoregulation. FASEB J 5:2567-2574, 1992 2. Duff GW: Cytokines and anti-cytokines. Br J Rheuma-
to132:15-20, 1993 3. Miossec P: Acting on the cytokine balance to control
auto-immunity and chronic inflammation. Eur Cytokine Netw 4:245-251, 1993
4. Debets R, Savelkoul FJ: Cytokine antagonists and their potential therapeutic use. Immunol Today 15:455-458, 1994
5. Arend WP, Dayer JM: Cytokines and cytokine inbibi- tors or antagonists in rheumatoid arthritis. Arthritis Rheum 33:305-315, 1990
6. Dinarello CA, Thompson RC: Blocking IL-I: Interleu- kin 1 receptor antagonist in vivo and in vitro. Immunol Today 12:404-410, 1991
7. Larrick JW: Native interleukin-I inhibitors. Immunol Today 10:61-66, 1989
8. Dayer JM, Fenner H: The role of cytokines and their inhibitors in arthritis. Bailli6re's Clin Rheumatol 6:485-516, 1992
9. Arend WP, Joslin FG, Massoni R J: Effects of immune complexes on production by human monocytes of interleu- kin 1 or an interleukin 1 inhibitor. J Immunol 134:3868- 3875, 1985
10. Seckinger P, Lowenthal JW, Williamson K, et al: A urine inhibitor of interleukin-1 activity that blocks ligand binding. Jr Immunol 139:1546-1549, 1987
11. Hannum CH, Wilcox CJ, Arend WP, et al: Interleu- kin-1 receptor antagonist activity of a human interleukin-1 inhibitor. Nature 343:336-340, 1990
12. Dinarello CA: Interleukin-1 and interleukin-1 antago- nism. Blood 77:1627-1652, 1991
13. Schur PH, Chang DM, Baptiste P, et al: Human monocytes produce IL-1 and an inhibitor of IL-1 in re- sponse to two different signals. Clin Immunol Immuno- patho157:45-63, 1990
14. Carter DB, Deibel MR, Dunn CJ, et al: Purification, cloning, expression, and biological characterization of an interleukin-1 receptor antagonist protein. Nature 344:633- 638, 1990
15. Granowitz EV, Clark BD, Mancilla J, et al: Interleu-
kin-1 receptor antagonist competitively inhibits the binding of interleukin-1 to type II interleukin-1 receptor. J Biol Chem 266:14147-14150, 1991
16. Dripps DJ, Brandhuber BJ, Thompson RC, et al: Interleukin-1 (IL-1) receptor antagonist binds to the 80- kDa IL-1 receptor but does not initiate IL-1 signal transduc- tion. J Biol Chem 266:10331-10336, 1991
17. Eisenberg SP, Evans RJ, Arend WP, et al: Primary structure and functional expression from complementary DNA of a human interleukin-1 receptor antagonist. Nature 343:341-346, 1990
18. Eisenberg SP, Brewer MT, Verderber E, et al: IL-1 receptor antagonist (IL-lra) is a member of the IL-1 gene family: Evolution of a cytokine control mechanism. Proc Natl Acad Sci U S A 88:5232-5236, 1991
19. Arend WP: Interleukin 1 receptor antagonist: A new member of the Interleukin 1 family. J Clin Invest 88:1445- 1451, 1991
20. Firestein GS, Berger AE, Tracey DE, et al: IL-1 receptor antagonist protein production and gene expression in rheumatoid arthritis and osteoarthritis synovium. J Immu- nol 149:1054-1062, 1992
21. Arend WP: Interleukin-1 receptor antagonist. Adv Immuno154:167-227, 1993
22. Henderson B: Therapeutic modulation of cytokines. Ann Rheum Dis 54:519-523, 1995
23. Haskill S, Marting G, Van Le L, et al: cDNA cloning of an intracellular form of the human interleukin-1 receptor antagonist associated with epithelium. Proc Natl Acad Sci U S A 88:3681-3685, 1991
24. Biegler CF, Norris DA, Weston WL, et al: Interleu- kin-1 receptor antagonist production by human keratino- cytes. J Invest Dermatol 98:34-44, 1992
25. Mazzei GJ, Bernasconi L, Lewis C, et al: Human granulocyte-macrophage colony-stimulating factor plus phor- bol myristate acetate stimulate a promyelocytic cell line to produce an IL-1 inhibitor. J Immuno120:683-689, 1990
26. Chang DM: Cellular signals for the induction of human interleukin-1 receptor antagonist. Clin Immunol Immunopathol 74:23-30, 1995
27. Arend WP, Welgus HG, Thompson RC, et al: Biologi- cal properties of recombinant human monocyte-derived

556 WECKMANN AND ALCOCER-VARELA
interleukin-1 receptor antagonist. J Clin Invest 85:1694- 1697, 1990
28. Thompson RC: IL-1 receptor antagonist in arthritis and arthritis models. Clin Exp Rheumatol 11:$169, 1993
29. Schreuder HA, Rondeau JM, Tardif C, et ah Refined crystal structure of the interleukin-1 receptor antagonist: Presence of a disulfide link and a cis-proline. Eur J Biochem 227:838-847, 1995
30. Blakemore AIF, McDonagh AJG, Messenger AG, et al: Genetics of interleukin 1 receptor antagonist in inflam- matory skin diseases. J Invest Dermatol 100:522, 1993
31. Rosbotham JL, Barker JN, Trembath RC: Exclusion of interleukin-1 receptor antagonist as a primary disease determinant for psoriasis (letter). J Invest Dermatol 104: 306, 1995
32. Deleuran BW, Chu CQ, Field M, et al: Localization of interleukin lc~ (IL-lc0, type 1 IL-1 receptor and interleu- kin 1 receptor antagonist protein in the synovial membrane and cartilage/pannus junction in rheumatoid arthritis. Br J Rheumato131:801-809, 1992
33. Koch AE, Kunkel SL, Chensue SW, et al: Expression of Interleukin-1 and Interleukin-1 receptor antagonist by human rheumatoid synovial tissue macrophages. Clin Immu- nol Immunopathol 65:23-29, 1992
34. Roux-Lombard P, Modoux C, Vischer T, et al: Inhibitors of interleukin 1 activity in synovial fluids and in cultured synovial fluid mononuclear cells. J Rheumatol 19:517-523, 1992
35. Malyak M, Swaney RE, Arend WP: Levels of synovial fluid interleukin-1 receptor antagonist in rheumatoid arthri- tis and other arthropathies: Potential contribution from synovial fluid neutrophils. Arthritis Rheum 36:781-789, 1993
36. Firestein GS, Boyle DL, Yu C, et al: Synovial interleu- kin-1 receptor antagonist and interleukin-1 balance in rheumatoid arthritis. Arthritis Rheum 37:644-652, 1994
37. Arend WP, Smith MF Jr, Janson RW, et al: IL-1 receptor antagonist and IL-I[3 production in human mono- cytes are regulated differently. J Immunol 147:1530-1536, 1991
38. Poutsiaka DD, Clark BD, Vannier E, et al: Produc- tion of interleukin-1 receptor antagonist and interleukin-l[3 by peripheral blood mononuclear cells is differentially regulated. Blood 78:1275-1281, 1991
39. Sandborg CI, Berman MA, Andrews BS, et al: Increased production of an interleukin-1 inhibitor with fibroblast stimulating activity by mononuclear cells from patients with scleroderma. Clin Exp Immunol 66:312-319, 1986
40. Prieur AM, Kaufmann MT, Griscelli C, et al: Specific interleukin-1 inhibitor in serum and urine of children with systemic juvenile chronic arthritis. Lancet 2:1240-1242, 1987
41. Peritt D, Flechner I, Yanai P, et ah The M20 IL-1 inhibitor. II. Biological characterization. J Immunol Meth- ods 155:167-174, 1992
42. Fibach E, Rigel M, Peled T, et al: The effect of human myelomonocytic leukemic cell line (M20) derived IL-1 inhibitor on human erythroid cell development. Leuk Lymphoma 15:327-332, 1994
43. Barak V, Peritt D, Yanai P, et al: In vivo anti
inflammatory effects of the M20 IL-1 inhibitor: I. Effects on acute inflammatory parameters. Biotherapy 6:263-270, 1993
44. Barak V, Gorodetsky R, Weidenfeld J, et al: In vivo anti-inflammatory effects of the M20 IL-1 inhibitor: II. Effects on serum reactants. Biotherapy 6:271-277, 1993
45. Cope A, Aderka D, Doherty M, et al: Soluble tumour necrosis factor (TNF) receptors are increased in the sera and synovial fluids of patients with rheumatic diseases. Arthritis Rheum 35:1160-1169, 1992
46. Dower SK, Wignall JM, Schooley K, et al: Retention of ligand binding activity by the extracellular domain of the IL-1 receptor. J Immunol 142:4314, 1989
47. Arend WP, Malyak M, Smith MF Jr, et al: Binding of IL-lc~, IL-113, and IL-1 receptor antagonist by soluble IL-1 receptors and levels of soluble IL-1 receptors in synovial fluids. J Immunol 153:4766-4774, 1994
48. Spriggs MK, Hruby DE, Maliszewski CR, et al: Vaccinia and cowpox viruses encode a novel secreted interleukin-1 binding protein. Cell 71:145, 1992
49. Ray CA, Black RA, Kronheim SR, et al: Viral inhibition of inflammation: cowpox virus encodes an inhibi- tor of the interleukin-l[3 converting enzyme. Cell 69:597- 604, 1992
50. Lambert C, Brealey R, Steele J, et al: The interaction of Tamm-Horsfall protein with the extracellular matrix. Immunology 79:203-210, 1993
51. Buchan G, Barret K, Turner M, et al: Interleukin-1 and tumor necrosis factor mRNA expression in rheumatoid arthritis: Prolonged production of IL-lm Clin Exp Immunol 73:499, 1988
52. Santis AG, Campanero MR, Alonso JL, et al: Regula- tion of tumor necrosis factor (TNF)-e~ synthesis and TNF receptors expression in T lymphocytes through the CD2 activation pathway. Eur J Immuno122:3155-3160, 1992
53. Seckinger P, Zhang JH, Hauptmann B, et al: Charac- terization of a tumor necrosis factor alpha inhibitor: Evi- dence of immunological cross-reactivity with the TNF receptor. Proc Natl Acad Sci U S A 87:5188-5192, 1990
54. Brennan FM, Gibbons DL, Mitchell T, et al: En- hanced expression of TNF receptor mRNA and protein in mononuclear cells isolated from rheumatoid arthritis syno- vial joints. Eur J Immuno122:1907-1912, 1992
55. Heilig B, Fiehn C, Brockhaus M, et al: Evaluation of soluble tumor necrosis factor (TNF) receptors and TNF receptor antibodies in patients with systemic lupus erythem- atosus, progressive systemic sclerosis, and mixed connective tissue disease. J Clin Immunol 13:321-328, 1993
56. Aderka D, Wysenbeek A, Engelmann H, et al: Correlation between serum levels of soluble tumor necrosis factor receptor and disease activity in systemic lupus ery- thematosus. Arthritis Rheum 36:1111-1120, 1993
57. Fenner H: Strategies for the clinical development of anti-cytokines. Clin Exp Rheumatol 11:$183-S184, 1993
58. Maini RN, Brennan FM, Williams R, et al: TNFc~ in rheumatoid arthritis and prospects of anti-TNF therapy. Clin Exp Rheumatol 11:S173-S175, 1993 (suppl 8)
59. Sheehan KCK, Ruddle NH, Schreiber RD: Genera- tion and characterization of hamster monoclonal antibodies that neutralize murine tumour necrosis factors. J Immunol 142:3884-3893, 1989
60. Williams RO, Feldmann M, Maini RN: Anti-tumour

CYTOKINE INHIBITORS IN AUTOIMMUNE DISEASE 557
necrosis; factor ameliorates joint disease in murine collagen- induced arthritis. Proc Natl Acad Sci U S A 89:9784-9788, 1992
61. Keffer J, Probert L, Cazlaris H, et al: Transgenic mice expressing human tumour necrosis factor: A predictive genetic model of arthritis. EMBO J 10:4025-4031, 1991
62. Elliott M J, Maini RN, Feldmann M, et al: Treatment of rheumatoid arthritis with chimeric monoclonal antibod- ies to tumor necrosis factor ~. Arthritis Rheum 36:1681- 1690, 19'93
63. Elliott M J, Maini RN, Feldmann M, et al: Ran- domised double-blind comparison of chimeric monoclonal antibody to tumour necrosis factor alpha (cA2) versus placebo in rheumatoid arthritis. Lancet 344:1105-1110, 1994
64. Elliott MJ, Maini RN, Feldmann M, et al: Repeated therapy with monoclonal antibody to tumour necrosis factor alpha (cA2) in patients with rheumatoid arthritis. Lancet 344:1125-1127, 1994
65. Maini RN, Elliott MJ, Brennan FM, et al: Beneficial effects of tumour necrosis factor-alpha (TNF-a) blockade in rheumatoid arthritis. Clin Exp Immunol 101:207-212, 1995
66. Cope AP, Londei M, Chu NR, et al: Chronic expo- sure to tumor necrosis factor (TNF) in vitro impairs the activation of T cells through the T cell receptor/CD3 complex: Reversal in vivo by anti-TNF antibodies in pa- tients with rheumatoid arthritis. J Clin Invest 94:749-760, 1994
67. Suitters A J, Foulkes R, Opal SM, et al: Differential effect of isotype on efficacy of anti-tumor necrosis factor alpha chimeric antibodies in experimental septic shock. J Exp Med 179:849-856, 1994
68. Alvaro-Gracia JM, Zvaifler NJ, Firestein GS: Cyto- kines in chronic inflammatory arthritis. V. Mutual antago- nism between IFN-gamma and TNF-alpha on HLA-DR expression, proliferation, collagenase production and GM- CSF production by rheumatoid arthritis synoviocytes. J Clin Invest 86:1790-1798, 1990
69. Cannon GW, Emkey RD, Denes A, et al: Prospective two-year follow-up of recombinant interferon-gamma in rheumatoid arthritis. J Rheumatol 17:304-310, 1990
70. Tilg H, Mier JM, Vogel W, et al: Induction of circulating IL-1 receptor antagonist by IFN treatment. J Immunol 150:4687-4692, 1993
71. Orino E, Sone S, Nii A, et al: IL-4 up-regulates IL-1
receptor antagonist gene expression and its production in human blood monocytes. J Immunol 149:925-931, 1992
72. Vannier E, Miller LC, Dinarello CA: Coordinated antiinflammatory effects of interleukin 4: Interleukin 4 supresses interleukin 1 production but up regulates gene expression and synthesis of interleukin 1 receptor antago- nist. Proc Natl Acad Sci USA 89:4076-4080, 1992
73. Kuruvilla AP, Shah R, Hochwald GM, et al: Protec- tive effect of transforming growth factor 131 on experimental autoimmune diseases in mice. Proc Nail Acad Sci U S A 88:2918-2921, 1991
74. Turner M, Chantry D, Katsikis P, et al: Induction of the interleukin 1 receptor antagonist protein by transform- ing growth factor-beta. Eur J Immuno121:1635-1639, 1991
75. Dubois CM, Ruscetti FW, Palaszynski EW, et al: Transforming growth factor 13 is a potent inhibitor of interleukin 1 (IL-1) receptor expression: Proposed mecha- nism of inhibition of IL-1 action. J Exp Med 172:737-744, 1990
76. Brennan FM, Feldmann M: Cytokines in autoimmu- nity. Curr Opin Immunol 4:754-759, 1992
77. de Waal Malefyt R, Abrams J, Bennet B, et al: Interleukin-10 inhibits cytokine synthesis by human mono- cytes: An autoregulatory role of IL-10 produced by mono- cytes. J Exp Med 174:1209-1220, 1991
78. Llorente L, Richaud-Patin Y, Fior R, et al: In vivo production of interleukin-10 by non-T cells in rheumatoid arthritis, Sj6gren's syndrome, and systemic lupus erythema- tosus: A potential mechanism of B lymphocyte hyperactivity and autoimmunity. Arthritis Rheum 37:1647-1655, 1994
79. Katsikis PD, Chu CQ, Brennan FM, et al: Immuno- regulatory role of interleukin 10 in rheumatoid arthritis. J Exp Med 179:1517-1527, 1994
80. Tilg H, Trehu E, Atkins MB, et al: Interleukin-6 (IL-6) as an anti-inflammatory cytokine-induction of circu- lating IL-1 receptor antagonist and soluble tumor necrosis factor receptor-p55. Blood 83:113-118, 1994
81. Tilg H, Shapiro L, Vannier ED, et al: Induction of circulating antagonists to IL-1 and TNF by IL-1 administra- tion and their effects on IL-2-induced cytokine production in vitro. J Immunol 152:3189-3198, 1994
82. Sewell KL, Parker KC, Woodworth TG, et al: DAB486IL-2 fusion toxin in refractory rheumatoid arthritis. Arthritis Rheum 36:1223-1233, 1993




















