
Prolactin, immunoregulation, and autoimmune diseases
12
Seminars in ARTHRITIS AND RHEUMATISM VOL 20, NO 5 APRIL 1991 Prolactin, Immunoregulation, and Autoimmune Diseases By Luis J. Jara, Carlos Lavalle, Antonio Fraga, Celso Gbmez-Sanchez, Luis H. Silveira, Pindaro Martinez-Osuna, Bernard F. Germain, and Luis R. Espinoza Cells of the immune system synthesize prolactin and express mRNA and receptors for that hor- mone. lnterleukin 1, interleukin 6, y interferon, tumor necrosis factor, platelet activator factor, and substance P participate in the release of prolactin. This hormone is involved in the patho- genesis of adjuvant arthritis and restores immu- nocompetence in experimental models. In vitro studies suggest that lymphocytes are an impor- tant target tissue for circulating prolactin. Prolac- tin antibodies inhibit lymphocyte proliferation. Prolactin is comitogenic with concanavalin A and induces interleukin 2 receptors on the sur- face of lymphocytes. Prolactin stimulates orni- thine decarboxylase and activates protein ki- nase C, which are pivotal enzymes in the differentiation, proliferation, and function of lym- phocytes. Cyclosporine A interferes with prolac- tin binding to its receptors on lymphocytes. Hyperprolactinemia has been found in patients with systemic lupus erythematosus. Fibromyal- From the Division of Rheumatology, Department of lntmwl Medicine, DiGon of Endocrinology, Department of Internal M&c&, Universir): of South Florida College ofMedicine, Tampa, FL, and the Rheumatic Diseases Unit, Hospital de Especial- idades, Centro Medico La Raza, IMSS, Mexico, DF, Mexico. Luis J. Jara, MD: Research Fellow, Division of Rheumatol- oa, Department of Internal Medicine, University of South Florida College of Medicine, and Rheumatic Diseases Unit. Hospital de Especialides, Centro Medico La Raza, IMSS, Mexico; Carlos Lavalle, MD, FACP: Rheumatic Diseases Unit. Hospital de Especialidades, Centro Mexico La Raza. IMSS, Mexico; Antonio Fraga, MD, FACP: Rheumatic Diseases Unit, Hospital de Especialidades, Centro Medico La Raza. IMMS, Mexico; Celso Gbmez-SBnchez, MD: Professor of Medicine, Div&ion of Endocrinology, Department of Inter- nal Medicine. Universitvof South Florida College of Medicine: gia, rheumatoid arthritis, and low back pain patients present a hyperprolactinemic response to thyrotropin-releasing hormone. Experimental autoimmune uveitis, as well as patients with uveitis whether or not associated with spondy- loarthropathies, and patients with psoriatic ar- thritis may respond to bromocriptine treatment. Suppression of circulating prolactin by bro- mocriptine appears to improve the immunosup- pressive effect of cyclosporine A with signifi- cantly less toxicity. Prolactin may also be a new marker of rejection in heart-transplant patients. This body of evidence may have an impact in the study of rheumatic disorders, especially connec- tive tissue diseases. A role for prolactin in autoim- mune diseases remains to be demonstrated. Copyright o 1991 by W.B. Saunders Company INDEX WORDS: Prolactin; autoimmunity; immu- noregulation. Luis H. Silveira, MD: Research Fellow, Do&ion of Rheuma- tology, Department of Internal Medicine, University of South Florida College of Medicine; Pindaro Martinez-Osuna, MD: Research Fellow, Division of Rheumatology, Department of Internal Medicine, University of South Florida College of Medicine; Bernard F. Germain, MD: Professor of Medicine, Division of Rheumatology, Department of Internal Medicine, Unrversity of South Florida CoIlege of Medzcitte: Luis R. Espinoza, MD: Professor ofMedicine, Division of Rheumatol- ogy? Department of Internal Medicine. Untver.sity of South Florida College of Medicine. Address reprint requests to Luis R. Espinoza. MD, LSU Medical Center, Section of Rheumatology, 1542 Tulane Ave, New Orleans, LA 70112-2822. Copytight o 1991 by W. B. Saunders Cornpan! 0049.0172/9112005-0001$5.0010 Semw~ars ,n Arthrifjs and Rheumatism, Vol20. No 5 (April), 1991: pp 273.284 273
-
Upload
independent -
Category
Documents
-
view
0 -
download
0
Transcript of Prolactin, immunoregulation, and autoimmune diseases

Seminars in
ARTHRITIS AND RHEUMATISM VOL 20, NO 5 APRIL 1991
Prolactin, Immunoregulation, and Autoimmune Diseases
By Luis J. Jara, Carlos Lavalle, Antonio Fraga, Celso Gbmez-Sanchez, Luis H. Silveira,
Pindaro Martinez-Osuna, Bernard F. Germain, and Luis R. Espinoza
Cells of the immune system synthesize prolactin and express mRNA and receptors for that hor- mone. lnterleukin 1, interleukin 6, y interferon, tumor necrosis factor, platelet activator factor, and substance P participate in the release of prolactin. This hormone is involved in the patho- genesis of adjuvant arthritis and restores immu- nocompetence in experimental models. In vitro studies suggest that lymphocytes are an impor- tant target tissue for circulating prolactin. Prolac- tin antibodies inhibit lymphocyte proliferation. Prolactin is comitogenic with concanavalin A and induces interleukin 2 receptors on the sur- face of lymphocytes. Prolactin stimulates orni- thine decarboxylase and activates protein ki- nase C, which are pivotal enzymes in the differentiation, proliferation, and function of lym- phocytes. Cyclosporine A interferes with prolac- tin binding to its receptors on lymphocytes. Hyperprolactinemia has been found in patients with systemic lupus erythematosus. Fibromyal-
From the Division of Rheumatology, Department of lntmwl Medicine, DiGon of Endocrinology, Department of Internal M&c&, Universir): of South Florida College ofMedicine, Tampa, FL, and the Rheumatic Diseases Unit, Hospital de Especial- idades, Centro Medico La Raza, IMSS, Mexico, DF, Mexico.
Luis J. Jara, MD: Research Fellow, Division of Rheumatol- oa, Department of Internal Medicine, University of South Florida College of Medicine, and Rheumatic Diseases Unit. Hospital de Especialides, Centro Medico La Raza, IMSS, Mexico; Carlos Lavalle, MD, FACP: Rheumatic Diseases Unit. Hospital de Especialidades, Centro Mexico La Raza. IMSS, Mexico; Antonio Fraga, MD, FACP: Rheumatic Diseases Unit, Hospital de Especialidades, Centro Medico La Raza. IMMS, Mexico; Celso Gbmez-SBnchez, MD: Professor of Medicine, Div&ion of Endocrinology, Department of Inter- nal Medicine. Universitv of South Florida College of Medicine:
gia, rheumatoid arthritis, and low back pain patients present a hyperprolactinemic response to thyrotropin-releasing hormone. Experimental autoimmune uveitis, as well as patients with uveitis whether or not associated with spondy- loarthropathies, and patients with psoriatic ar- thritis may respond to bromocriptine treatment. Suppression of circulating prolactin by bro- mocriptine appears to improve the immunosup- pressive effect of cyclosporine A with signifi- cantly less toxicity. Prolactin may also be a new marker of rejection in heart-transplant patients. This body of evidence may have an impact in the study of rheumatic disorders, especially connec- tive tissue diseases. A role for prolactin in autoim- mune diseases remains to be demonstrated. Copyright o 1991 by W.B. Saunders Company
INDEX WORDS: Prolactin; autoimmunity; immu- noregulation.
Luis H. Silveira, MD: Research Fellow, Do&ion of Rheuma- tology, Department of Internal Medicine, University of South Florida College of Medicine; Pindaro Martinez-Osuna, MD:
Research Fellow, Division of Rheumatology, Department of Internal Medicine, University of South Florida College of Medicine; Bernard F. Germain, MD: Professor of Medicine, Division of Rheumatology, Department of Internal Medicine, Unrversity of South Florida CoIlege of Medzcitte: Luis R.
Espinoza, MD: Professor ofMedicine, Division of Rheumatol- ogy? Department of Internal Medicine. Untver.sity of South Florida College of Medicine.
Address reprint requests to Luis R. Espinoza. MD, LSU Medical Center, Section of Rheumatology, 1542 Tulane Ave, New Orleans, LA 70112-2822.
Copytight o 1991 by W. B. Saunders Cornpan! 0049.0172/9112005-0001$5.0010
Semw~ars ,n Arthrifjs and Rheumatism, Vol20. No 5 (April), 1991: pp 273.284 273
274 JARA ET AL
T HE NEUROENDOCRINE and immune systems are intimately linked and involved
in bidirectional communication. A complete regulatory loop between the immune and neu- roendocrine systems has been postulated.’ Cells of the immune system express mRNA of adreno- corticotropic hormone, growth hormone (GH), thyroid stimulating hormone, and prolactin (PRL).’ In addition, they also synthesize these hormones3 and have receptors for all of them.4 The central nervous system cells have receptors for cytokines, ie, interleukin 1 (IL-l), and cyto- kines are synthesized by brain astrocytes and microglial cells.5,6
protein consisting of about 25% a-helix, 33% p turn, and 8% random coil.‘”
PRL has an important role in the regulation of immune function.7 It has the ability to pro- mote cell growth and/or differentiation in sev- eral tissues and also functions as an immunostim- ulator.’ Hyperprolactinemia has recently been demonstrated in men and pregnant women with systemic lupus erythematosus (SLE). Clinical observations and experimental studies suggest that PRL may be important in the pathogenesis of SLE and possibly of other autoimmune diseases.‘,”
This review discusses the interactions be- tween PRL and the immune system and its association with SLE as well as other autoim- mune diseases.
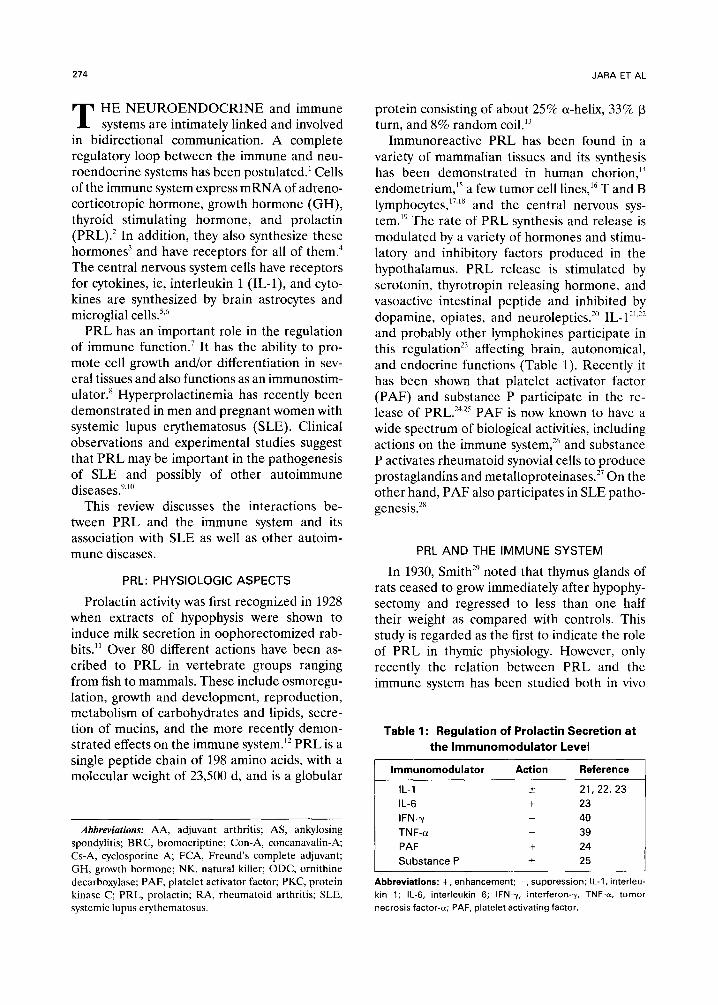
Immunoreactive PRL has been found in a variety of mammalian tissues and its synthesis has been demonstrated in human chorion,” endometrium,” a few tumor cell lines,16 T and B lymphocytes,‘7,‘8 and the central nervous sys- tem.19 The rate of PRL synthesis and release is modulated by a variety of hormones and stimu- lator-y and inhibitory factors produced in the hypothalamus. PRL release is stimulated by serotonin, thyrotropin releasing hormone, and vasoactive intestinal peptide and inhibited by dopamine, opiates, and neuroleptics.2” IL-l”,” and probably other lymphokines participate in this regulation2’ affecting brain, autonomical, and endocrine functions (Table 1). Recently it has been shown that platelet activator factor (PAF) and substance P participate in the re- lease of PRL.24,2” PAF is now known to have a wide spectrum of biological activities, including actions on the immune system,26 and substance P activates rheumatoid synovial cells to produce prostaglandins and metalloproteinases.27 On the other hand, PAF also participates in SLE patho- genesis.”
PRL AND THE IMMUNE SYSTEM
PRL: PHYSIOLOGIC ASPECTS
Prolactin activity was first recognized in 1928 when extracts of hypophysis were shown to induce milk secretion in oophorectomized rab- bits.” Over 80 different actions have been as- cribed to PRL in vertebrate groups ranging from fish to mammals. These include osmoregu- lation, growth and development, reproduction, metabolism of carbohydrates and lipids, secre- tion of mucins, and the more recently demon- strated effects on the immune system.‘* PRL is a single peptide chain of 198 amino acids, with a molecular weight of 23,500 d, and is a globular
In 1930, Smith” noted that thymus glands of rats ceased to grow immediately after hypophy- sectomy and regressed to less than one half their weight as compared with controls. This study is regarded as the first to indicate the role of PRL in thymic physiology. However, only recently the relation between PRL and the immune system has been studied both in vivo
Table 1: Regulation of Prolactin Secretion at
the lmmunomodulator Level
Abbreviations: AA, adjuvant arthritis; AS, ankylosing
spondylitis; BRC, bromocriptine; Con-A, concanavalin-A;
G-A, cyclosporine A, FCA, Freund’s complete adjuvant;
GH, growth hormone; NK, natural killer; ODC, ornithine
decarboxylase; PAF, platelet activator factor; PKC, protein kinase C; PRL, prolactin; RA, rheumatoid arthritis; SLE,
systemic lupus erythematosus.
lmmunomodulator
IL-I
IL-6
IFN-y
TNF-(Y
PAF
Substance P
Action Reference
?I 21, 22, 23
+ 23
_ 40
_ 39
+ 24
* 25
Abbreviations: +, enhancement: -, suppression; IL-l, interleu-
kin 1; IL-6, interleukin 6; IFN-y, interferon-y, TNF-u, tumor
necrosis factor-a; PAF, platelet activating factor.
PROLACTIN, IMMUNOREGULATION, AND AUTOIMMUNITY
(experimental models and clinical observation) and in vitro.
PRL. and Adjuvant Arthritis
In rats, Freund’s complete adjuvant (FCA) injected at the base of the tail induces an arthritic disease (adjuvant arthritis; AA) and there is a great amount of evidence suggesting that it is the result of an aberrant immune response.” Other abnormalities that may de- velop include balanitis, mild conjunctivitis, and uveitis. This picture is very similar to Reiter syndrome in humans.31
Nagy and Berczi reported that PRL, GH, and placental lactogen are potent in restoring the immune reactivity of hypophysectomized ani-
mals,32-34 and the treatment of rats with the dopaminergic ergot alkaloid bromocriptine (BRC) inhibited the following immune reac- tions: contact sensitivity skin reaction to dinitro- chlorobenzene, AA, experimental allergic en- cephalitis, and antibody formation to sheep red blood cells and bacterial lipopolysaccharide. These results suggest that BRC suppresses im- munity by inhibition of PRL.35,36 Neidhart and Larson studied the neuroendocrine response during FCA-induced immune stimulation, par- ticularly the release of endogenous pituitary hormones. The activity of ornithine decarbow- lase (ODC), the first enzyme involved in poly- amine biosynthesis, was used in this study as a biological marker of the stimulation of different parts of the central nervous system, the pituitary gland, and lymphoid tissues following immune stimulation. The circadian rhythms of pituitary ODC activity and plasma PRL level, 3 to 4 days
275
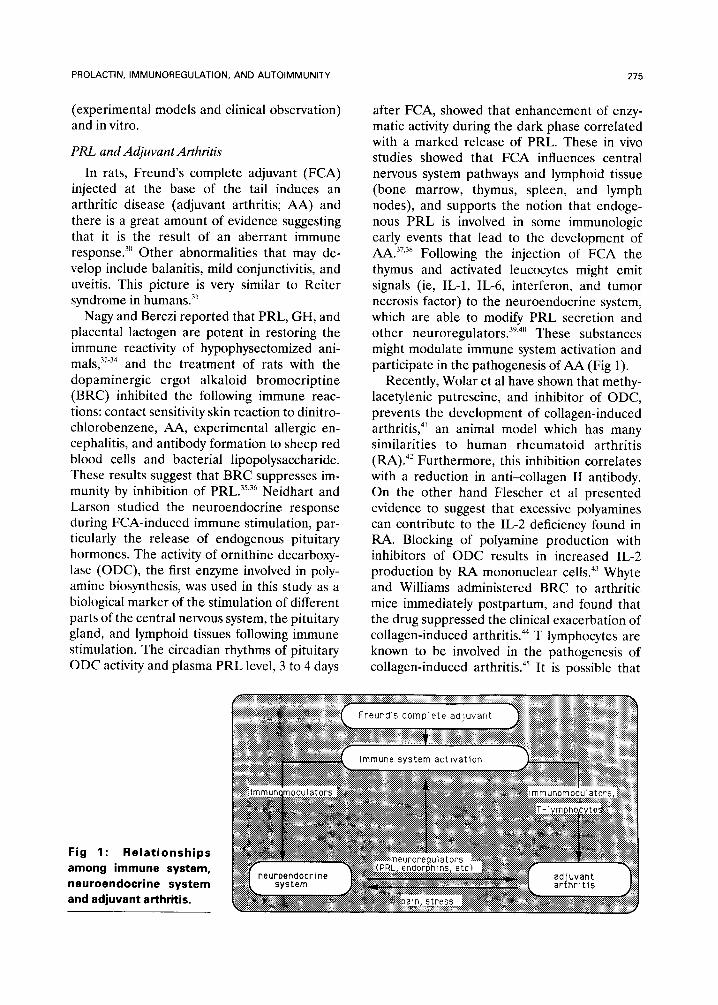
after FCA, showed that enhancement of enzy- matic activity during the dark phase correlated with a marked release of PRL. These in vivo studies showed that FCA influences central nervous system pathways and lymphoid tissue (bone marrow, thymus, spleen, and lymph nodes), and supports the notion that endoge- nous PRL is involved in some immunologic early events that lead to the development of AA.37.38 Following the injection of FCA the thymus and activated leucocytes might emit signals (ie, IL-l, IL-6, interferon, and tumor necrosis factor) to the neuroendocrine system, which are able to modify PRL secretion and other neuroregulators.39,4” These substances might modulate immune system activation and participate in the pathogenesis of AA (Fig 1).
Recently, Wolar et al have shown that methy- lacetylenic putrescine, and inhibitor of ODC, prevents the development of collagen-induced arthritiq4’ an animal model which has many similarities to human rheumatoid arthritis (RA).42 Furthermore, this inhibition correlates with a reduction in anti-collagen II antibody. On the other hand Flescher et al presented evidence to suggest that excessive polyamines can contribute to the IL-2 deficiency found in RA. Blocking of polyamine production with inhibitors of ODC results in increased IL-2 production by RA mononuclear cells4’ Whyte and Williams administered BRC to arthritic mice immediately postpartum, and found that the drug suppressed the clinical exacerbation of collagen-induced arthritis.44 T lymphocytes are known to be involved in the pathogenesis of collagen-induced arthritis.45 It is possible that
Fig 1: Relationships
among immune system, neuroendocrine system and adjuvant arthritis.
276 JARA ET AL
the ability of T lymphocytes to respond to antigenic stimulation may be mediated by PRL through the interaction with ODC activity, lead- ing to an excessive polyamine production and IL-2 deficiency. In this regard, recently, Yu- Lee* has shown that ODC mRNA levels and various growth-related genes in cultured T-cells (Nb2 T lymphoma cells) are stimulated by PRL.
PRL and Lymphocyte Function
Bernton et al in 1988 examined the T cell- dependent induction of activated tumoricidal macrophages in mice infected with either Myco- bacterium bovis (strain BCG) or Listeria monocy- togenes (LM) or inoculated with killed Propioni- bactetium acnes (PA). In this study, mice were treated with BRC and such treatment pre- vented T-cell dependent induction of macro- phage tumoricidal activity after the intraperito- neal injection with either BCG, LM, or PA. Concomitant treatment with bovine PRL re- versed this effect. Of the multiple events leading to macrophage activation in vivo, the produc- tion by T lymphocytes of y-interferon was the most impaired in BRC-treated mice. The criti- cal influence of pituitary PRL release on main- tenance of lymphocyte function and on lympho- kine-dependent macrophage activation suggests that in mice lymphocytes are an important target tissue for circulating PRL.47
In studies designed to evaluate the in vitro effects of exogenous PRL on lymphocyte prolif- eration with serum-free and serum supple- mented media, Hartmann et a14” were unable to find conditions where the addition of PRL to either culture system significantly affected pro- liferative responses. Surprisingly, when antisera to PRL were added to neutralize PRL (as a negative control) a profound inhibition of cell proliferation resulted. Antibodies to other pitu- itary hormones did not have any effect. Such inhibition appears specific for both murine and human growth factor-dependent cells and in- volved failure of anti-PRL treated lymphoid cells to respond to growth factors, as opposed to altered production of autocrine growth factors, namely IL-2 and IL-4. Thus, antibodies to PRL appear to block an event occurring in the Gl to S phase transition of these cell lines that consti- tutively express growth factor receptors. Collec- tively, these data indicate that lymphocytes
synthesize a cross-immunoreactive PRL-like pro- tein (ir-PRL) and that ir-PRL is required for normal proliferation in response to mitogen or growth factors.
Recent evidence supports a role for PRL in the mitogenesis of T lymphocytes. At subopti- ma1 concentrations of concanavalin-A (Con-A), the addition of rat PRL to murine splenocytes resulted in a dose-dependent increase in mito- genesis.17 Therefore, PRL is comitogenic with Con-A. In this sense, Mukherjee et a149 have shown recently that PRL induces IL-2 receptors on the surface of lymphocytes in vitro. Spleno- cytes from rats incubated in the presence of PRL responded to synthetic IL-2 by dividing. Preincubation of PRL with PRL antiserum markedly reduced the subsequent incorpora- tion levels of radiolabeled thymidine, whereas preincubation with GH antiserum was without effect. The IL-Zinduced proliferative response of PRL-treated lymphocytes implied that PRL induced IL-2 receptors on the cell surface. This was confirmed directly by flow cytometric analy- sis of PRL-treated lymphocytes stained with an antirat IL-2 receptor (anti-TAC) antibody. While these data offer little insight into an understanding of the mechanism(s) by which PRL might exert its IL-2 effect, this finding shows that PRL by itself is mitogenic.
PRL,: A New Cytokine (?)
PRL has been shown to be a mitogenic agent for Nb2 T lymphoma cells. Shiu et a150 demon- strated that these cells possess receptors that bind only PRL. In 1983, Russell et al showed that cyclosporine, an immunosuppresssive agent used in human organ transplantation5’ and re- cently in autoimmune diseases,” blocks PRL- stimulated ODC activity in lymphocyte-contain- ing tissues of the rat such as the thymus and spleen.53 The induction of increased ODC activ- ity is an integral event regulating lymphocyte differentiation, proliferation, and function.” Subsequently, Russell et al reported the pres- ence of PRL receptors on T, B, and monocytic cells of human peripheral blood and spIeen,5i.56 the estimated receptor number was 360 per cell. The specific binding of PRL to lymphocytes can be enhanced or blocked by cyclosporine depend- ing on the concentration of the drug. Adminis- tration of cyclosporine A (Cs-A) also rapidly

PROLACTIN, IMMUNOREGULATION, AND AUTOIMMUNITY
increased the serum PRL level in rats fourfold as compared with the control values within 1 hour of injection; such elevation could be blocked by BRC. This study suggests a role for PRL in the mechanism(s) of the immunosup- pressive action of Cs-A.
The discovery of PRL receptors on T and B lymphocytes suggested that immunomodulation by PRL was a primary response to the hormone and opened the door to exploration of the ability of PRL to directly affect cells of the immune system. It is known that these cells as well as many others have specific receptors for PRL (Table 2).
In 1986, Hiestand et a15’ provided evidence for the involvement of PRL in the maintenance of T cell immune competence. Their data showed that a reduction of serum PRL levels by BRC led to a decrease of lymphocyte responsive- ness toward antigenic stimulation in rats. This phenomenon was observed both in vitro (mixed lymphocyte reaction) and, more importantly, in vivo (graft v host reaction). Dot blot hybridiza- tion showed that cytoplasmic RNA (mRNA) from lymphocytes hybridized with both PRL and GH cDNA probes. This study suggests that the ability of T lymphocytes to respond fully to antigenic stimulation may depend on the pres- ence of PRL of pituitary origin bound to recep- tors on their outer membrane. On presentation of antigen these lymphocytes then produce a secondary signal in the form of a PRL/GH-
277
related polypeptide that can amplify either the response of the same cell to produce lympho- kines (autocrine action) or the mitogenic re- sponse of neighboring lymphocytes (exocrine action), or both. Binding of antigens or mito- gens to their cell surface receptors induces a secondary signal. In the same way as other immunomodulators, PRL can amplify the re- sponse of immune cells.5x
In 1987, Montgomery et al” showed that lymphocytes may produce a PRL-like protein, In this study the cell subset(s) responsible for the production of this PRL-like molecule was not identified. However, Con-A is a T cell- specific mitogen and the production of PRL bioactivity paralells the course of Con-A- induced proliferation, suggesting that this PRL- like factor is produced by this lymphocyte sub- set. The PRL-like material has a molecular mass of 46 kd, different from that of the anterior pituitary PRL entity in mice, which is 24 kd, and it has a peptide map homology similar to murine pituitary PRL. Di Mattia et al and Gellersen et al’x.ss have shown that PRL is synthesized by a human B-lymphoblastoid cell line (IM-9-P) and is indistinguishable from pituitary human PRL. These authors also demonstrate that PRL secre- tion in this line is regulated by dexamethasone but not by other hormones known to modulate PRL secretion in the pituitary or decidua.
The proliferative action of PRL on T lympho- cytes may be a complex interaction between two
Table 2: Prolactin Receptors in the Cells of the Immune System and in Some Tissues
I. Immune system:
macrophages T-lymphocytes
B-lymphocytes
natural killer cells
II. Endocrine system:
anterior pituitary
adrenal
pancreas (islets of Langerhans)
ovary
testis
mammary glands
Ill. Centralnervous system:
brain
IV. Others:
prostate
uterus
kidney
liver
skeletal muscle
lung
erythrocyte
aorta
lymphoma (T-cell derived)
mastocytoma (mast cells?)
Adapted from Russell DH. New aspects of prolactin and immunity: A lymphocyte-derived prolactin-like product and nuclear protein
kinase C activation. Trends Pharmacol Sci 1989;10:40-44

278 JARA ET AL
factors: the level of circulating PRL from the anterior pituitary (endocrine action), and the ability of activated T and B cells to divide and produce a PRL-like factor with possible auto- crine (on the same cell that produces them) and paracrine (on neighboring cells) actions. So far, the lymphocyte PRL-like substance appears to be a novel PRL variant and a new cytokine.
PRL and Protein Kinase C
The mitogenic activation of resting T lympho- cytes involves two distinct cellular events: the synthesis of IL-2 and the synthesis and expres- sion of IL-2 receptors. It is therefore significant that an immediate consequence of T cell activa- tion is the phosphorylation of a wide range of proteins on serine (Ser), threonine (Thr), and tyrosine (Tyr) residues.60 Briefly, when antigen interacts with T-cell receptors (or when mito- gens such as phytohemagglutinin or Con-A interact with T cell plasma membrane recep- tors) the following cascade of molecular events is thought to occur. Phospholipase C in the endoplasmic reticulum is activated, which in turn increases phosphoinositol turnover to pro- duce diacylglycerol and inositol triphosphate. The latter stimulates the release of bound calcium from the endoplasmic reticulum to produce an increase in the concentration of cytosolic-free calcium. The increased free cal- cium activates calmodulin which, together with diacylglycerol, activates protein kinase C (PKC), a crucial enzyme in the regulation of cellular function and growth including the cells of the immune system.61
Evidence from a number of cell types and tissues, such as vascular smooth muscle,6’ sug- gests that the intracellular action of PRL in- volves the activation of PKC. Also, Buckley et aVj3 have found that addition of PRL to purified rat liver nuclei and splenocyte nuclei results in a rapid activation by several 100-fold of PKC. This dose-dependent effect was blocked by a rat anti-PRL-receptor monoclonal antibody and by anti-PRL antiserum. The time course (3 min- utes) for PRL activation of PKC in splenic nuclei is similar to that reported for antibodies directed against Ia and immunoglobulin anti- gens and for CAMP on nuclear PKC activity in intact murine B lymphocytes.64 The observation of receptor-mediated activation of PKC in the
nucleus suggests that unoccupied PRL recep- tors are present in isolated nuclei. The implica- tions of this study are important for our under- standing of the nuclear function of polypeptide hormones such as PRL and its interaction with the immune system, ie, it is possible that PRL induction of IL-2-R on rat splenic lymphocytes might be explained by PKC activation.
PRL. and Natural Killer Cells
Forni et al”’ in 1983 demonstrated that de- struction of the tubero-infundibular region of the hypothalamus led to a persistently abro- gated natural killer (NK) activity in mice. These observations suggest that neuroendocrine mech- anisms play a relevant role in the control of NK activity. Gerli et alhh in 1986 studied human NK cell activity in 11 BRC-treated and 23 untreated hyperprolactinemic women and in 63 age- matched healthy women using a “Cr-release assay. NK cell activity was significantly reduced in untreated hyperprolactinemic patients with respect to normal subjects, but therapy with BRC restored NK cell function of patients to the levels of normal controls, suggesting that hyperprolactinemia is also immunosuppressive. However, Matera et al” studied the functional state of native NK cells in a large group of patients with hyperprolactinemia of functional or tumoral origins with no radiological demon- stration of hypothalamic damage and their re- sults showed that the NK activity from patients with hyperprolactinemia is not different from that of normal subjects. Alarc&-Segovia et al have found decreased NK function in hyperpro- lactinemia (personal communication, 1986). Re- cently, Matera et aY have shown that highly purified NK cells express binding sites for PRL (660 receptors per cell). At concentrations cor- responding to the therapeutic range, Cs-A in- duced a complete inhibition of PRL binding. By contrast, very low concentrations increased PRL binding to more than 100% of control levels. These data strongly support the idea of a close relation between PRL and NK cell lineage in humans.
PROLACTIN, IMMUNE SYSTEM, AND DISEASE
There are a number of observations in hu- mans that may indicate that PRL does indeed influence the immune system in both health and
PROLACTIN, IMMUNOREGULATION, AND AUTOIMMUNITY 279
disease. Thyroid autoimmunity was evaluated in 92 hyperprolactinemic patients, 4 of whom had acromegaly. High titers of thyroglobulin and microsomal antibodies were found in 1 acrome- galic and in 12 women with either adenomatous or idiopathic hyperprolactinemia.h4 Ishibashi and Yamaji”’ examined antithyroid antibodies in
sera from 73 erythroid patients with prolacti- noma and 40 patients with acromegaly. Statisti- cal analysis showed that the occurrence of both positive antimicrosomal antibody and antithyro-
globulin antibody was significantly higher in prolactinoma women than in normal and in
acromegalic women. In five women, both anti- bodies disappeared after BRC therapy and six of nine prolactinoma patients had a higher B
cell population. These results suggest that hyper- prolactinemia is associated with a higher inci-
dence of positive antithyroid antibodies, which may be consequent to nonspecific stimulation by PRL of B lymphocyte function. Vidaller et al, ” in 1986 studied the function of peripheral
blood lymphocytes from four patients with tu- moral hyperprolactinemia and normal ovarian
function before and after PRL levels were normalized by treatment with BRC. Lympho-
cytc responses were suppressed to Con-A or pokeweed mitogen and to a lesser extent to
phytohemagglutinin. The spontaneous Con-A induced suppression and production of IL-2 was low in two patients and was increased after drug
treatment. All these findings give insight on the immunomodulatory role of PRL in vivo. Some of these abnormalities, such as B lymphocyte stimulation, with overproduction of antibodies, decreased response to mitogens and lowered
suppression and production of IL-2, have been demonstrated in SLE patients.7’.71
PRL also was measured in 13 untreated and 42 treated patients suffering from celiac disease. Increased PRL values were found in four of the five untreated men, whereas the eight untreated women had normal levels. PRL was elevated in
all 35 patients responding favorably to a gluten- free diet. In contrast. significantly lower PRL levels were found in seven patients not respond- ing to the diet.”
In 1987, Lavalle et al” described increased basal levels of serum PRL in men with SLE. Serum PRL levels were above normal limits in seven of eight patients studied (P < .Ol). It is of
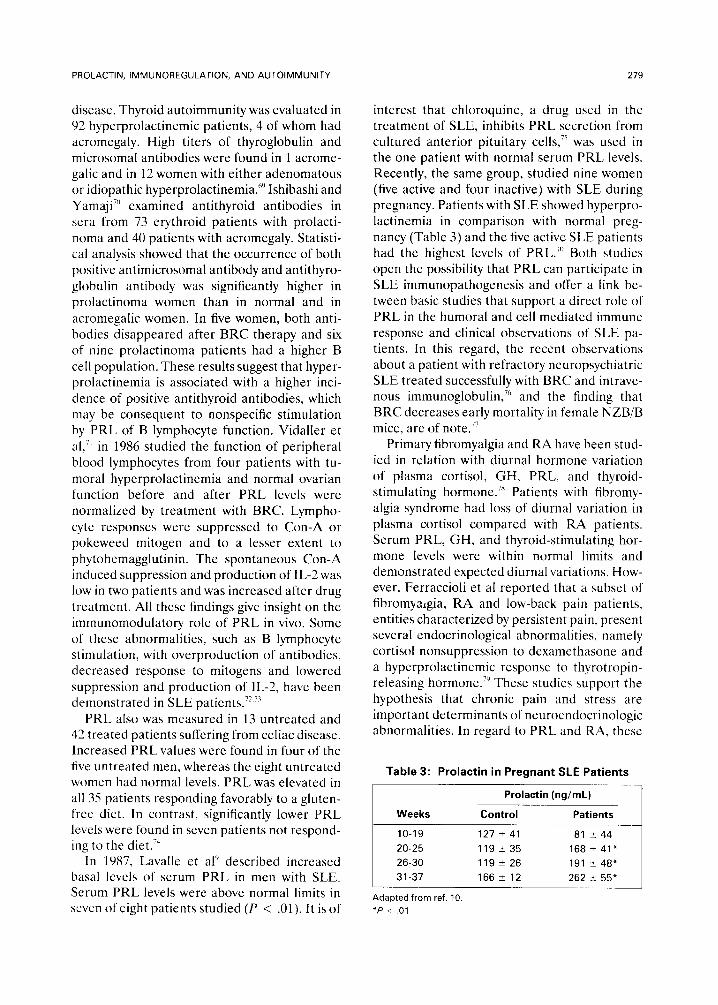
interest that chloroquine, a drug used in the treatment of SLE, inhibits PRL secretion from cultured anterior pituitary cells,‘5 was used in the one patient with normal serum PRL levels. Recently, the same group, studied nine women (five active and four inactive) with SLE during pregnancy. Patients with SLE showed hyperpro- lactinemia in comparison with normal preg-
nancy (Table 3) and the five active SLE patients had the highest levels of PRL.“’ Both studies open the possibility that PRL can participate in SLE immunopathogenesis and offer a link be- tween basic studies that support a direct role of PRL in the humoral and cell mediated immune
response and clinical observations of SLE pa- tients. In this regard, the recent observations about a patient with refractory neuropsychiatric SLE treated successfully with BRC and intrave- nous immunoglobulin,7h and the finding that BRC decreases early mortality in female NZB/B mice, are of note.77
Primary fibromyalgia and RA have been stud- ied in relation with diurnal hormone variation
of plasma cortisol, GH, PRL. and thyroid- stimulating hormone.” Patients with fibromy-
algia syndrome had loss of diurnal variation in plasma cortisol compared with RA patients. Serum PRL, GH, and thyroid-stimulating hor- mone levels were within normal limits and demonstrated expected diurnal variations. How- ever, Ferraccioli ct al reported that a subset of fibromyalgia, RA and low-back pain patients, entities characterized by persistent pain, present several endocrinological abnormalities, namely
cortisol nonsuppression to dexamethasone and a hyperprolactinemic response to thyrotropin- releasing hormone.“’ These studies support the
hypothesis that chronic pain and stress are important determinants of neuroendocrinologic abnormalities. In regard to PRL and RA, these
Table 3: Prolactin in Pregnant SLE Patients
Prolactin (ng/mL)
Weeks Control Patients -___
10-19 127 2 41 81 244
20-25 119k35 168 2 41*
26-30 119 2 26 191 t 48*
31-37 166 k 12 262 rt 55*
Adapted from ref. 10. *P < .Ol
280 JARA ET AL
results also support the notion of a close rela- tion between the neuroendocrine and immune systems. In 1985, Hedner and Bynke reported
four patients with endogenous iridocyclitis treated with BRC for hyperprolactinemia, galac- torrhea, and Parkinson disease and found allevi-
ation of the iridocyclitis.8” Of interest three of these patients had spondyloarthopathies: two
with ankylosing spondylitis (AS) and one with Reiter syndrome. Recently, ovarian function
was studied in women with AS and PRL level was found normal in all 17 patients.81 The levels of PRL in Reiter syndrome, psoriatic arthritis,
and other reactive arthritides are unknown. Determination of PRL values in these disorders is of interest because in AA, an excellent model
of reactive arthritis3’ several studies have shown hyperprolactinemia.”
Palestine et al demonstrated the effect of PRL suppression by BRC in combination with lower doses of Cs-A on experimental autoim-
mune uveitis.82 BRC plus low-dose Cs-A led to marked decreases in the incidence of experimen- tal autoimmune uveitis and anti-S antigen anti-
body titers as well as in the lymphocyte prolifer- ative assay. This study suggests that BRC can
enhance the immunosuppression of low-dose Cs-A and supports the idea that PRL has a role
in the immunosuppresive action of CS-A.‘~ Re- cently, the same group” demonstrated that the administration of Cs-A, Cs-A plus BRC, or BRC, results in down regulation of antinuclear autoantibody levels of PRL in patients with
uveitis. The levels of PRL were determined in these patients and the mean serum prolactin level was 5.4 ngimL. After therapy with BRC,
the mean serum prolactin level was less than 2.0 ng/mL in all patients.84 Dougados et alX5 investi-
gated the effect of BRC in 6 of the 12 Cs-A- treated RA patients previously reported. The addition of BRC did not potentiate Cs-A effi-
cacy since no significant clinical improvement was observed and there was no reduction in
Cs-A daily dosage, except in one patient. The small number of patients studied, however, and the low BRC dosage used preclude any definite conclusion. In contrast, of 35 psoriatic arthritis patients who were systematically treated with increasing doses of BRC, starting at 2.5 mg up to 30 mg per day, significant remission was observed in 77%.8h
Larson et al, and Carrier et a18’-“” proposed
PRL as a new marker of rejection in heart- transplant patients. This marker seems a partic- ularly useful predictor because its plasma con- centration increased between 2 and 8 days before rejection episodes. In support of this idea, Wilner et al” studied the effect of hypopro- lactinemia induced by a new drug, CQP 201- 403, a dopamine agonist, on the survival of heterotopic cardiac allografts and the ability of peripheral blood lymphocytes to respond in vitro to plant mitogens. CQP treatment greatly enhanced the immunosuppressive effect of Cs-A on graft survival and on in vitro lymphocyte function. The authors concluded that modula- tion by PRL may be a useful adjunct to Cs-A immunosuppression. Suppression of circulating PRL levels with BRC also improved the immu- nosuppressive effect of Cs-A, thereby lowering the frequency of early acute rejection as well as infection after cardiac transplantation.”
CONCLUSIONS AND PROSPECTS
The studies reviewed here support a link between PRL, the immune system, and autoim- mune diseases. The implications of this link are numerous, ranging from understanding patho- physiologic mechanisms to developing new clin- ical therapies. The main findings can be summa- rized as follows. (1) Cells of the immune system can synthesize PRL and other biologically ac- tive neuroendocrine peptide hormones. (2) PRL receptors are present on normal T, B, NK-cells and on monocytes. (3) PRL play a role in the development of adjuvant arthritis and restores immunocompetence in experimental models. (4) In vitro lymphocyte functions are decreased in hypoprolactinemia and are restored by PRL. (5) PRL stimulates ODC and thereby poly- amine synthesis in many tissues, including tis- sues of the immune system. (6) PRL can acti- vate PKC, a pivotal enzyme in many cellular functions and cell growth regulation, including the immune system. (7) Cs-A interferes with PRL binding to its receptors on lymphocytes. (8) Hyperprolactinemia has been shown in a subset of SLE patients. (9) Experimental autoim- mune uveitis and patients with uveitis, whether or not associated with spondyloarthropathies, may respond to BRC. This drug has been used successfully in psoriatic arthritis patients and in a single patient with SLE. (10) Suppression of circulating PRL by BRC appears to improve the

PROLACTIN, IMMUNOREGULATION, AND AUTOIMMUNITY 281
immunosuppressive effect of Cs-A with signifi- cantly less toxicity.
The evidence accumulated may have an im-
pact in the study of rheumatic disorders, espe- cially in connective tissue diseases. In this re-
gard, a number of pertinent questions emerge. (1) What is the prevalence of hyperprolactine- mia in patients with connective tissue diseases? (2) What is the relation among altered PRL levels, clinical activity, and expression of im- mune response, ie, antinuclear antibodies? (3) Is there an abnormality in immune cells PRL- receptors, as well as in the synthesis and secre- tion of PRL by T and B lymphocytes, of these patients? Does PRL influence receptors and synthesis of lymphokines of SLE patients? (4) Does PRL alter proliferation of SLE patients lymphocytes? (5) Is the response to PRL modi- fied in patients with reactive arthritis and uve- itis. in a similar way to that seen in AA? (6) Is
the combination of low-dose Cs-A plus BRC useful in the treatment of these diseases? (7) What is the role of hyperprolactinemia in clini- cal reactivation of SLE-pregnancy?
We believe the interaction between the im- mune and neuroendocrine systems is altered in patients with autoimmune diseases. The im- mune system fails to discriminate appropriately between self- and non-self-antigens, conse-
quently generating both specific and nonspecific responses against the antigens. Lymphokines and other stimulators are necessary to activate self-reactive T cells. In this context, immuno- logic signals (ie, IL-1 and other immunomodula- tors) can directly affect the neuroendocrine
system, by their receptors, and produce the release of hormones (ie, PRL, neurotransmit- ters, or growth factors). These neuroregulators exert direct influences over immunological
functions also by their receptors on T and B lymphocytes; therefore, hyperactive cells of the immune system produce more neuro and immu- nomodulators and complete a two-way humoral interaction between the immune and neuroen- docrine systems. A combination of cytokines and neuromodulators may function in an addi- tive, synergistic, or antagonistic manner on the immune-neuroendocrine system. This in-vivo activation signal leads to hyperactivity of B lymphocytes and exhausts the T cells, so they appear activated by cell surface markers al- though they are functionally depressed, and as a consequence they have an abnormal production of lymphokines. On the other hand, the neuroen- docrine axis may have a defective response to inflammatory stimuli and contribute to the sus- ceptibility to autoimmune diseases. In support of this concept, Sternberg et al have shown that Lewis strain rats have a defective hypothalamic response to inflammatory stimuli, resulting in a blunted corticosterone response from the adre- nal gland.“’ The defect appears to lie in the regulation of synthesis of mRNA for corticotro- pin-releasing hormone.q3 New ideas and investi-
gations for further confirmation of these studies are necessary, but regardless of their results, interaction between the neuroendocrine and immune systems will have a major impact on our understanding of the physiology, diagnosis, and therapy of connective tissue diseases.
REFERENCES
I. Blalock JE. Smith EM: A complete regulatory loop
between the immune and neuroendocrine systems. Fed
Proc 44: 108-111. 1985
2. Weigent DA. Blalock JE: Interactions between the
neuroendocrine and immune systems: Common hormones
and receptors. Immunol Rev 100:79-108, 1987 3. Khansari D, Mm-go A, Faith R: Effects of stress on the
immune system. Immunol Today 11:170-175, 1990
4. Bhalla AK: Hormones and the immune response. Ann
Rheum Dis 48: l-6, 1989
5. Plats-Salaman C: Immunomodulators and feeding
regulation: A humoral link between the immune and
nervous system. Brain Behav lmmun 3:193-213, 1989
h. Fontana A, Frei K, Bodmer S, et al: Immune-mediated
encephalitis on the role of antigen-presenting cells in brain tissue. Immunol Rev 100:185-201, 1987
7. Berczi I, Nagy E: The effect of prolactin and growth
hormone on hemolymphopoietic tissue and immune func-
tion. in Berczi 1, Kovacs K (eds): Hormones and Immunity.
Lancaster MTP Press. 1987. pp 145-171
8. Russell DH: New aspects of prolactin and immunity: A
lymphocyte-derived prolactin-like product and nuclear pro-
tein kinase C activation. Trends Pharmacol Sci 10:40-44.
1989
9. Lavalle C, Loyo E, Paniagua R et al: Correlation study
between prolactin and androgens in male patients with
systemic lupus erythematosus. J Rheumatol l-4:268-272,
1987
10. Fraga A, Jara L, Graef A, et al: Prolactin and gonadal
hormones in pregnant SLE patients. Arthritis Rheum.
32:S24, 1989 (abstr)
11. Stricker P, Grueter F: Action du lobe anterieur
del’hyphophysesur la montee laiteuse. CR Sot Biol (Par)
99: 1978-1980, 1928
12. Lamberts SWJ. Mac Leod RM: Regulation of prolac-
282 JARA ET AL
tin secretion at the level of the lactotroph. Physiol Rev
70:279-318, 1990
13. Nicoll CS, Mayer GL, Russell SM: Structural fea-
tures of prolactin and growth hormones that can be related
to their biological properties. Endocr Rev 7:169-203, 1986
14. Golander A, Hurley T, Barret J, et al: Prolactin
synthesis by human chorion decidual tissue: a possible
source of amniotic fluid prolactin. Science 202:311-313,
1978
15. Maslar IA, Riddick DH: Prolactin production by
human endometrium during the normal menstrual cycle.
Am J Obstet Gynecol135:751-754,1979
16. Rosen SW, Weintraub BD, Aaronson SA: Non-
random ectopic protein production by malignant cells: Direct evidence in vitro. J Clin Endocrinol Metab 50:834-
841,198O
17. Montgomery D, Zukoski C, Shah G, et al: Concanava-
lin A-stimulated murine splenocytes produce a factor with
prolactin-like bioactivity and immunoreactivity. Biochem
Biophys Res Commun 145:692-698,1987
18. DiMattia G, Gellersen B, Bohnet H, et al: A human
B-lymphoblastoid cell line produces prolactin. Endocrinol-
ogy 122:2508-2517, 1988
19. De Vito WJ: Distribution of immunoreactive prolac-
tin in the male and female rat brain: Effects of hypophysec-
tomy and intraventricular administration of colchicine.
Neuroendocrinology 47:87-99, 1989
20. Fluckiger E, Del Pozo E, van Werder K: Control of
prolactin secretion, in Fluckiger E, Del Pozo E, von Werder
K (eds): Prolactin, Physiology, Pharmacology and Clinical
Findings. Berlin, Germany, Springer-Verlag, 1982, pp 24-41
21. Bernton EW, Beach JE, Holaday JW, et al: Release
of multiple hormones by a direct action of interleukin-1 on
pituitary cells. Science 238:519-521, 1987
22. Schettini G, Lorio T, Meucci 0, et al: Interleukin-1-B
modulation of prolactin secretion from rat anterior pituitary
cells: involvement of adenylate cyclase activity and calcium
mobilization. Endocrinology 126:1435-1441, 1990
23. Yamaguchi M, Matsuzaki N, Hirota K, et al: Interleu-
kin 6 possibly induced by interleukin ll3 in the pituitary
gland stimulates the release of gonadotropins and prolactin.
Acta Endocrinol (Copenh) 122:201-205, 1990
24. Camoratto AM, Grandison L: Platelet-activating fac-
tor stimulates prolactin release from dispersed rat anterior
pituitary cells in vitro. Endocrinology 124:1502-1506, 1989
25. Arisawa M, Snyder G, Yu WH, et al: Physiologically
significant inhibitory hypothalamic action of substance P on
Prolactin release in the male rat. Neuroendocrinology
52122-27, 1990
26. Braquet P, Touqui L, Shen TY, et al: Perspectives in
platelet-activating factor research. Pharmacol Rev 39:97-
145,1987
27. Lotz M, Carson DA, Vaughan JH: Substance P
activation of rheumatoid synoviocytes: Neural pathway in pathogenesis of arthritis. Science 235:893-895, 1987
28. Tetta C, Bussolino F, Modena V, et al: Release of
platelet-activating factor in systemic iupus erythematosus.
Int Arch Allergy Appl Immunol91:244-256, 1990
29. Smith PE: The effect of hypophysectomy upon the
involution of the thymus in the rat. Anat Ret 47:119-129,
1930
30. Van Eden W, Holoshitz J, Cohen I: Antigenic mim-
icry between mycobacteria and cartilage proteoglycans: the
model of adjuvant arhtritis. Concepts Immunopathol4:144-
170,1987
31. Wilder RL: Animal models of reactive arthritis, in
Espinoza L, Goldenberg D, Arnett F, et al (eds): Infections
in the rheumatic diseases. Philadelphia, PA, Grune-
Stratton, 1988, pp 311-316
32. Nagy E, Berczi I: Immunodeficiency in hypophysecto-
mized rats. Acta Endocrinol (Copenh) 89:530-537. 1978
33. Berczi I, Nagy E, Kovacs K, et al: Regulation of
humoral in rats by pituitary hormones. Acta Endocrinol
(Copenh) 98:506-513,198l
34. Nagy E, Berczi I, Friesen HG: Regulation of immu-
nity in rats by lactogenic and growth hormones. Acta
Endocrinol (Copenh) 102:351-357, 1983
35. Nagy E, Berczi I, Wren G, et al: Immunomodulation
by bromocriptine. Immunopharmacology 6:231-243, 1983
36. Spangelo BL, Hall NR, Ross PC, et al: Stimulation of
in vivo antibody production and concanavalin-A-induced
mouse spleen cell mitogenesis by prolactin. Immunopharma-
cology 14:11-20, 1987
37. Neidhart M: Bromocriptine microcapsules inhibit
ornithine decarboxylase activity induced by Freund’s com-
plete adjuvant in lymphoid tissues of male rats. Endocrinol-
ogy 125:2846-2852, 1989
38. Neidhart M, Larson DF: Freund’s complete adjuvant
induces ornithine decarboxylase activity in the central
nervous system of male rats and triggers the release of
pituitary hormones. J Neuroimmunol26:97-105, 1990
39. Gaillard RC, Turnill D, Sappino P, et al: Tumor
necrosis factor inhibits the hormonal response of the
pituitary gland to hypothalamic releasing factors. Endocri-
nology 127:101-106, 1990
40. Vankelecom H, Carmeliet P, Heremans H. et al:
Interferon-I inhibits stimulated adrenocorticotropin, prolac-
tin, and growth hormone secretion in normal rat anterior
pituitary cell cultures. Endocrinology 126:2919-2926, 1990
41. Wolar JA, Logan D, Bowlin T: Methylacetylenic
putrescine (MAP), an inhibitor of polyamine biosynthesis.
prevents the development of collagen-induced arthritis.
Cell Immunol 125:498-507, 1990
42. Courtenay JS, Dallman MJ, Dayan AD, et al: Immu-
nization against heterologous type II collagen induces
arthritis in mice. Nature 283:666-668, 1980
43. Flescher E, Bowlin T, Ballester A, et al: Increased
polyamines may downregulate interleukin 2 production in
rheumatoid arthritis. J Clin Invest 83:1356-1352,1989
44. Whyte A, Williams RO: Bromocriptine suppresses
postpartum exacerbation of collagen-induced arthritis. Ar-
thritis Rheum 31:927-928, 1988
45. Holmdahl R, Klareskog L, Rubin K, et al: T lympho- cytes in collagen II-induced arthritis in mice: Characteriza-
tion of arthritogenic collagen II-specific T-cell lines and
clones. Stand J Immunol22:295-306, 1985
46. Yu-lee L: Prolactin stimulates transcription ofgrowth-
related genes in Nb2 T Lymphoma cells. Mol Cell Endo-
crinol68:21-28, 1990
47. Bernton EW, Meltzer MS, Holaday JW: Suppression
of macrophage activation and T-lymphocyte function in hypoprolactinemic. Science 239:401-404,1988
PROLACTIN, IMMUNOREGULATION, AND AUTOIMMUNITY 283
4X. Hartmann DP, Holaday JW, Bernton EW: Inhibition
of lymphocyte proliferation by antibodies to prolactin.
FASEB J 3:2194-2202, 1989
4Y. Mukherjee P, Mastro A, Hymer WC: Prolactin induc-
tion of interleukin-2 receptors on rat splenic lymphocytes.
Endocrinology 126:88-94, 1990
50. Shiu RPC. Elsholtz HP, Tanaka T, et al: Receptor-
mediated mitogenic action of prolactin in a rat lymphoma
cell line. Endocrinology 113:159-165, 1983
5 I, Cohen DJ. Loertscher R, Rubin MF, et al: Cyclospo-
rine: A new immunosuppressive agent for organ transplan-
tation. Ann Intern Med 101:667-682, 1984
52. Schnider R (ed): Cyclosporin in autoimmune disease.
First International Symposium, Basle, March 18-20. Springer
Verlag, Berlin, New York, Tokyo, Sept 1985
5.3. Russell DH, Larson DF, Womble JR, et al: Cyclo-
sporin A inhibits ornithine decarboxylase induction in
kidney in response to prolactin, growth hormone and
insulin. Physiologist 26:A-13, 1983
53. Klimpel CR, Byus CV, Russell DH, et al: Cyclic
AMP dependent protein kinase activation and the induc-
tion of ornithine decarboxylase during lymphocyte mitogen-
esis. J lmmunol 123:817-824, 1979
55. Russell DH, Matrisian L, Kibler R, et al: Prolactin
receptors on human lymphocytes and their modulation by
cyclosporine. Biochem Biophys Res Commun 121:899-906.
1084
5f). Russell DH, Kibler R, Matrisian L et al. Prolactin
receptors on human T and B lymphocytes: Antagonism of
prolactin binding by cyclosporine. J Immunol 134:3027-
3031.1985
57. Hiestand PC, Mekler P, Nordann R, et al: Prolactin
as a modulator of lymphocyte responsiveness provides a
possible mechanism of action for cyclosporine. Proc Nat1
Acad Sci USA 83:2599-2603, 1986
5X. Dinarello CA. Mier JW: Lymphokines. N Engl J Med 3 17:940-945, I987
5Y. Gellersen B. DiMattia, Friensen HG, et al: Regula-
tion of prolactin secretion in the human B-lymphoblastoid
cell line IM-9-P3 by dexamethasone but not other regulators
of pituitary prolactin secretion. Endocrinology 125:2853-
2861. 198’)
60. Wedner HJ, Bass G: Tyrosine.phosphorylation of a
66,000 Mr soluble protein in lectin-activated human periph-
eral blood T lymphocytes. J Immunol 136:4226-4231, 1986
61. Shaw LM: Advances in cyclosporine pharmacology,
measurement. and therapeutic monitoring. Clin Chem 35:
129’). 1308. 1989
62. Sauro MD. Buckley AR, Russell DH, et al: Prolactin
stimulation of protein kinase C activity in rat aortic smooth
muscle. Life Sci 44:1787-1792, 1989
63. Buckley A. Crowe P. Russell DH: Rapid activation of
protein kinase C in isolated rat liver nuclei by prolactin, a
known hepatic mitogen. Proc Nat1 Acad Sci USA X5:8649- 8653. 198X
64. Russell DH, Zorn NE, Buckley AR, et al: Prolactin
and known modulators of rat splenocytes activate nuclear protein kinase C. European J Pharmacol 188:139-152. 1990
65. Forni CT, Bindoni M, Santoni A, et al: Radiofre-
quency destruction of the tuberoinfundibolar region of
hypotalamus permanently abrogates NK cell activity in
mice. Nature 306:181-184, 1983
66. Gerli R, Rambotti P, Nicoletti I, et al: Reduced
number of natural killer cells in patients with pathological
hyperprolactinemia. Clin Exp Immunol64:399-406. 1986
67. Matera L, Ciccarelli E, Cesano A, et al: Natural killer
activity in hyperprolactinemic patients. Immunopharmacol-
ogy 18:143-146, 1989
68. Mater-a L, Muccioli G, Cesano A, et al: Prolactin
receptors on large granular lymphocytes: dual regulation by
cyclosporin A. Brain Behav Immun 2:1-10, 1988
69. Ferrari C, Boghen M, Paracchi A. et al: Thyroid
autoimmunity in hyperprolactinaemic disorders. Acta Endo-
crinol (Copenh) 104:35-41, 1983
70. Ishibashi M, Yamaji T: Immunological abnormalitied
with hyperprolactinemia. The Endocrine Society. 71 An-
nual meeting, pp 407, 1989 (abstr)
71. Vidaller A, Llorente L, Larrea F, et al: T-cell
dysregulation in patients with hyperprolactinemia: Effect of
bromocriptine treatment. Clin Immunol lmmunopathol
38337.343, 1986
72. Alcocer-Varela J, Alarcon-Segovia D: Decreased
production of and response to interleukin 2 by cultured
lymphocytes from patients with systemic lupus erythemato-
sus. J Clin Invest 69:1388-1392, 1982
73. Kammer GM, Stein RL: T lymphocyte immune
dysfunctions in systemic lupus erythematosus. J Lab Clin
Med 115:273-282, 1990
74. Stevens FM, McCarthy CF, Craig A: Is prolactin
trophic to the intestine in coeliac disease? Gut 19:A992, 1978
75. Conconi MV, Walker AM: Chloroquine affects pro-
lactin secretion and Golgi morphology in the mammotroph.
Endocrinology. 114:725-734, 1984
76. Rabinovich CE, Schanberg LE, Kredich DW: Intrave-
nous immunoglobulin and bromocriptine in the treatment
of refractory neuropsychiatric systemic lupus erythemato-
sus. Arthritis Rheum 33:R22, 1990 (abstr)
77. McMurray R, Keisler D, Walker S: Bromocriptine
(Br) decreases early mortality in female NZBl’w mice.
Arthritis Rheum 33:R30, 1990 (abstr)
78. McCain G, Tilbe KS: Diurnal hormone variation in
fibromyalgia syndrome: A comparison with rheumatoid
arthritis. J Rheumatol 16:154-157, 1989 (suppl 19)
79. Ferraccioli G, Cavalieri F, Salaffi F, et al: Neuroendo-
crinologic findings in primary fibromyalgia (soft tissue
chronic pain syndrome) and in other chronic rheumatic
conditions (rheumatoid arthritis, low back pain). J Rheuma-
to1 17:869-873, 1990 (editorial)
80. Hedner LP, Bynke G: Endogenous iridocyclitis re- lieved during treatment with bromocriptine. Am J Ophthal-
mol 100:618-619, 1985
81. Jimenez-Balderas FJ, Tapia-Serrano R, Madero-
Cervera J. et al: Ovarian function studies in active ankylos-
ing spondylitis in women. Clinical response to estrogen
therapy. J Rheumatol 17:497-502, 1990
82. Palestine AG, Muellenberg-Coulombre CG, Kim
MK, et al: Bromocriptine and low dose cyclosporine in the
treatment of experimental autoimmune uveitis in the rat. J Clin Invest 79:1078-1081. 1987
83. Blank M, Palestine A, Nussenblatt R, et al: Down- regulation of autoantibody levels of cyclosporine and bro-

JARA ET AL
mocriptine treatment in patients with uveitis. Clin Immunol
ImmunophatoI54:87-97, 1990
84. Palestine AG, Nussenblatt RB, Gelato M: Therapy
for human autoimmune uveitis with low-dose cyclosporine
plus bromocriptine. Transplant Proc 20:131-135, 1988
85. Dougados M, Duchesne L, Amor B: Bromocriptine
and cyclosporine A combination therapy in rheumatoid
arthritis. Arthritis Rheum 31:1333-1334, 1988 (letter)
86. Weber G, Frey H: Zur behandlung der Psoriasis
arthropathica mit Bromocriptin. Z Hautkr 61:1456-1466,
1986
87. Larson DF, Copeland JG, Russell DH: Prolactin
predicts cardiac allograft rejection in cyclosporine immuno-
suppressed patients. Lancet 2:53, 1985 (letter)
88. Carrier M, Emery RW, Wild-Mobley J, et al: Prolac-
tin as a marker of rejection in human heart transplantation.
Transplant Proc 19:3442-3443, 1987
89. Carrier M, Russell DH, Cork RC, et al: Analysis of
risk factors for acute allograft rejection after heart transplan-
tation. J Heart Transplant 9:372-375,199O
90. Wilner M, Ettenger R, Koyle M, et al: The effect of
hypoprolactinemia alone and in combination with cyclospo-
rine on allograft rejection. Transplantation 49:264-267,199O
91. Carrier M, Wild J, Pelletier C, et al: Bromocriptine as
an adjuvant to cyclosporine immunosuppression after heart
transplantation. Ann Thorac Surg 49:129-32, 1990
92. Sternberg EM, Hill JM, Chrousos GP, et al: Inflam-
matory mediator-induced hypothalamic-pituitary-adrenal
axis activation is defective in streptococcal cell wall arthritis-
susceptible Lewis rats. Proc Nat1 Acad Sci USA 86:2374-
2378, 1989
93. Sternberg EM, Scott Young III W, Bernardini R: A
central nervous system defect in biosynthesis of corticotropin-
releasing hormone is associated with susceptibility to strep-
tococcal cell wall-induced arthritis in Lewis rats. Proc Nat1
Acad Sci USA 86:4771-4775, 1989




















