Posttraumatic Refractory Intracranial Hypertension and Brain Herniation Syndrome: Cerebral...
8
Hindawi Publishing Corporation BioMed Research International Volume , Article ID , pages http://dx.doi.org/.// Clinical Study Posttraumatic Refractory Intracranial Hypertension and Brain Herniation Syndrome: Cerebral Hemodynamic Assessment before Decompressive Craniectomy Edson Bor-Seng-Shu, 1 Wellingson Silva Paiva, 1 Eberval G. Figueiredo, 1 Yasunori Fujimoto, 2 Almir Ferreira de Andrade, 1 Erich Talamoni Fonoff, 1 and Manoel Jacobsen Teixeira 1 Division of Neurological Surgery, Hospital das Clinicas, University of Sao Paulo School of Medicine, Eneas Aguiar Street, Oce , Sao Paulo, SP, Brazil Department of Neurosurgery, Osaka University Graduate School of Medicine, Osaka, Japan Correspondence should be addressed to Wellingson Silva Paiva; [email protected] Received July ; Accepted October Academic Editor: Joachim Oertel Copyright © Edson Bor-Seng-Shu et al. is is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited. Background. e pathophysiology of traumatic brain swelling remains little understood. An improved understanding of intracranial circulatory process related to brain herniation may have treatment implications. Objective. To investigate the cerebral hemodynamic changes associated with brain herniation syndrome due to traumatic brain swelling. Methods. Nineteen head-injured patients with evidence of refractory intracranial hypertension and transtentorial herniation were prospectively studied. Cerebral hemodynamic assessment by transcranial Doppler (TCD) ultrasonography was performed prior to decompressive craniectomy. Patients and their cerebral hemispheres were classied according to TCD-hemodynamic patterns, and the data correlated with neurological status, midline shi on CT scan, and Glasgow outcome scale scores at months aer injury. Results. A wide variety of cerebral hemodynamic ndings were observed. Ten patients (.%) presented with cerebral oligoemia, patients (.%) with cerebral hyperemia, and patients with nonspecic circulatory pattern. Circulatory disturbances were more frequently found in the side of maximal cerebral swelling than in the opposite side. Pulsatility index (PI) values suggested that ICP varied from acceptable to considerably high; patients with increased PI, indicating higher microvascular resistance. No correlation was found between cerebral hemodynamic ndings and outcome. Conclusions. ere is a marked heterogeneity of cerebral hemodynamic disturbances among patients with brain herniation syndrome. 1. Introduction e pathophysiology of traumatic brain swelling remains little understood to date; as a consequence, there are few therapeutic options to control this condition and a number of patients develop increased intracranial pressure (ICP), brain ischemia, and herniation [–]. To our knowledge, there are no studies concerning disturbances of intracranial circulation associated with the process of brain herniation and refractory intracranial hyper- tension due to severe traumatic brain swelling. An improved understanding of intracranial circulatory process related to this condition may have treatment implications. e objective of this study was to investigate the cerebral hemodynamic changes associated with refractory elevated ICP and brain herniation syndrome due to traumatic brain swelling. e relationships between such cerebral hemo- dynamic patterns and the patients’ outcome, as well as between cerebral hemodynamic patterns and computerized tomography (CT) scan ndings, were also veried. 2. Clinical Material and Methods .. Study Design and Patient Enrollment. Traumatic brain injury (TBI) patients with clinical and tomographic signs of
-
Upload
independent -
Category
Documents
-
view
2 -
download
0
Transcript of Posttraumatic Refractory Intracranial Hypertension and Brain Herniation Syndrome: Cerebral...

Hindawi Publishing CorporationBioMed Research InternationalVolume !"#$, Article ID %&"'"(, % pageshttp://dx.doi.org/#".##&&/!"#$/%&"'"(
Clinical StudyPosttraumatic Refractory Intracranial Hypertension andBrain Herniation Syndrome: Cerebral Hemodynamic Assessmentbefore Decompressive Craniectomy
Edson Bor-Seng-Shu,1 Wellingson Silva Paiva,1
Eberval G. Figueiredo,1 Yasunori Fujimoto,2 Almir Ferreira de Andrade,1
Erich Talamoni Fonoff,1 and Manoel Jacobsen Teixeira1
! Division of Neurological Surgery, Hospital das Clinicas, University of Sao Paulo School of Medicine, "## Eneas Aguiar Street,O$ce %&'(, &#%&)&!& Sao Paulo, SP, Brazil
"Department of Neurosurgery, Osaka University Graduate School of Medicine, Osaka, Japan
Correspondence should be addressed to Wellingson Silva Paiva; [email protected]
Received !) July !"#$; Accepted #% October !"#$
Academic Editor: Joachim Oertel
Copyright © !"#$ Edson Bor-Seng-Shu et al. *is is an open access article distributed under the Creative Commons AttributionLicense, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properlycited.
Background.*e pathophysiology of traumatic brain swelling remains little understood. An improved understanding of intracranialcirculatory process related to brain herniationmay have treatment implications.Objective. To investigate the cerebral hemodynamicchanges associated with brain herniation syndrome due to traumatic brain swelling.Methods. Nineteen head-injured patients withevidence of refractory intracranial hypertension and transtentorial herniation were prospectively studied. Cerebral hemodynamicassessment by transcranial Doppler (TCD) ultrasonography was performed prior to decompressive craniectomy. Patients andtheir cerebral hemispheres were classi+ed according to TCD-hemodynamic patterns, and the data correlated with neurologicalstatus, midline shi, on CT scan, and Glasgow outcome scale scores at - months a,er injury. Results. A wide variety of cerebralhemodynamic +ndings were observed. Ten patients (&!.%%) presented with cerebral oligoemia, $ patients (#&.'%) with cerebralhyperemia, and - patients with nonspeci+c circulatory pattern. Circulatory disturbances were more frequently found in the sideof maximal cerebral swelling than in the opposite side. Pulsatility index (PI) values suggested that ICP varied from acceptableto considerably high; patients with increased PI, indicating higher microvascular resistance. No correlation was found betweencerebral hemodynamic +ndings and outcome.Conclusions.*ere is a marked heterogeneity of cerebral hemodynamic disturbancesamong patients with brain herniation syndrome.
1. Introduction
*e pathophysiology of traumatic brain swelling remainslittle understood to date; as a consequence, there are fewtherapeutic options to control this condition and a number ofpatients develop increased intracranial pressure (ICP), brainischemia, and herniation [#–!$].
To our knowledge, there are no studies concerningdisturbances of intracranial circulation associated with theprocess of brain herniation and refractory intracranial hyper-tension due to severe traumatic brain swelling. An improvedunderstanding of intracranial circulatory process related tothis condition may have treatment implications.
*e objective of this study was to investigate the cerebralhemodynamic changes associated with refractory elevatedICP and brain herniation syndrome due to traumatic brainswelling. *e relationships between such cerebral hemo-dynamic patterns and the patients’ outcome, as well asbetween cerebral hemodynamic patterns and computerizedtomography (CT) scan +ndings, were also veri+ed.
2. Clinical Material and Methods
".!. Study Design and Patient Enrollment. Traumatic braininjury (TBI) patients with clinical and tomographic signs of

! BioMed Research International
intracranial hypertension and brain herniation due to uncon-trollable brain swelling forwhomdecompressive craniectomywas indicated and in whom transcranial Doppler (TCD)ultrasonography had been performed were prospectivelyenrolled. Exclusion criteria were penetrating head injuries,Glasgow Coma Scale (GCS) score of $ associated withbilaterally +xed and dilated pupils, and impossibility toassess cerebral circulation by TCD ultrasonography. Patientswith multisystem trauma were not excluded. Demographic,clinical, and radiological datawere collected for every patient.*is study was approved by our research ethics committeeand conducted according to the Declaration of Helsinkiprinciples.
".". Management Protocol. All patients were managed by astandard regimen based on the guidelines of the AmericanCollege of Surgeons (Advanced Trauma Life Support) andof the American Association of Neurological Surgeons asdescribed in our previous report [)]. A,er stabilization of res-piratory and circulatory functions, patients with neurologicaldeterioration and clinical signs of brain herniation and raisedICP underwent urgent computerized tomography (CT) scansof the brain. Routine ICPmonitoringwas not intended in thisprotocol.
".). Clinical and Tomographic De*nitions of Brain Herniation.Clinical evidence of cerebral herniation syndrome consistedof neurological deterioration characterized by decrease inGCS score and/or dilation of pupils that were unresponsiveto light, unilaterally or bilaterally, in conjunction with CTevidence of brain herniation characterized by severe di.usebrain swelling or predominantly unilateral di.use brainswelling associatedwithmass e.ect, a shi,ofmidline cerebralstructures >&mm, and/or obliteration of perimesencephaliccisterns. Patients with persisting GCS score of $ and/or bilat-erally +xed and dilated pupils did not undergo decompressivecraniectomy and were excluded.
".%. Assessment Technique of Cerebral Hemodynamics. *eneurosurgical team was oriented to maintain their routinepractice, without waiting for the arrival of TCD physician toavoid any delay in the patients’ treatment. In most instances,TCD measurements were obtained, while the patient waitedto go into the operating theater (one case) or while theanesthesiologist prepared the patient in the operating room.
*e middle cerebral artery (MCA) and the distal seg-ment of the extracranial internal carotid artery (ICA) wereinsonated using a portable !MHz pulsed TCD device (Pio-neer TC !"!" EME; Nicolet Biomedical, Madison, WI) viatemporal and submandibular ultrasound windows, respec-tively. *e MCA and extracranial ICA blood /ow variablesthat were recorded and analyzed included the mean velocity(the time mean of the peak velocities over the course offour cardiac cycles) and the pulsatility index (PI = [systolicvelocity ! diastolic velocity]/mean velocity).
Physiological data, including hematocrit, arterial bloodcarbon dioxide and oxygen pressures, body temperature, and
systemic arterial blood pressure, were documented in eachTCD study.
".#. De*nition of TCD Hemodynamic Patterns. ElevatedTCD /ow velocities have been found in both cerebralvasospasm and hyperemia. Given that the extracranial ICAis not involved in the spasm process, /ow velocity changeswithin this artery are associated with changes in CBF ratherthan with changes in arterial diameter [!)–!%]. ExtracranialICA /ow velocity can be considered as an index of CBF sinceelevated /ow velocity in the extracranial ICA is associatedwith increased /ow volume to the brain [!)–!']. Lindegaardratio (LR), de+ned as the ratio of MCA mean /ow velocityto extracranial ICA mean /ow velocity, can di.erentiatecerebral vasospasm from hyperemia [!&]. In hyperemia,both extracranial ICA and MCA mean /ow velocities areincreased, and the LR remains <$. In the present study, MCAmean /ow velocities >#"" cm/second in conjunction with LR<$ were de+ned as indicative of cerebral hyperemia, whileMCA mean /ow velocities <)" cm/second were de+ned asindicative of cerebral oligoemia. MCA mean /ow velocitiesbetween )" and 100 cm/second along with LR <$ wereconsidered as nonspeci+c hemodynamic pattern.
".+. Categorization of Patients by Cerebral Hemodynamic Pat-terns. Patients with hyperemia in both cerebral hemispheresor hyperemia in one cerebral hemisphere and nonspeci+ccirculatory pattern in another hemisphere were considered aspresenting cerebral hyperemia. On the other hand, patientswith oligoemia in both cerebral hemispheres or oligoemiain one cerebral hemisphere and nonspeci+c hemodynamicpattern in the opposite hemisphere were de+ned as havingcerebral oligoemia. Patients with hyperemia in one cerebralhemisphere and oligoemia in the contralateral hemispherewere grouped separately.
".'. Data Collection. Information on age, gender, date ofaccident, time intervals between the accident and hospitaladmission and between admission and surgical treatment,mechanism of injury, neurological status (GCS score andpupil response) at admission, before, and a,er decompressivecraniectomy, shi, degree of midline cerebral structures,associated intracranial lesions, length of hospital stay, andoutcomewere registered. Outcomewas evaluated at -monthsa,er injury by Glasgow Outcome Scale (GOS) score. Patientswith good recovery (GOS score of &) or with moderatedisability (GOS score of )) were considered as presentingfavorable outcome, while patients with severe disability (GOSscore of $) or in a vegetative state (GOS score of !) or thosewho died (GOS score of #) were de+ned as having unfavorableoutcome.
".,. Statistical Analysis. Data were reported as means ±standard deviations.*eMann-WhitneyU test, theWilcoxonrank-sum test, and the Fischer exact test were performed.Spearman correlation coe0cients were calculated whenappropriate.*e tests were considered statistically signi+cantat a probability value <"."&.

BioMed Research International $
3. Results
).!. Patient Characteristics. Nineteen patients with severetraumatic brain swelling and evidence of elevated ICP andtranstentorial herniation were included. *e mean age ofthe patients was 33 ± 14 years (range #%–-$ years). *erewere #$ males and - females. Admission GCS scores rangedfrom ) to #$, with a median of %. During TCD examinations,GCS scores ranged from ) to #! (median -). Twenty percentof patients had a hypotensive insult at hospital admission.All patients had clinical and tomographic signs of cerebralherniation. Two patient subgroups were formed. *e +rstgroup included ( patients without focal lesions, in whomsevere traumatic brain swelling accompanied by therapy-resistant signs of brain herniation required decompressivecraniectomy.*e second group included #" patients who hada space-occupying hematoma (contusion hemorrhage andextradural or subdural hematoma) that had been removed inan initial operation, and developed a,erwards severe brainswelling concomitant with signs of transtentorial herniation.Demographic, clinical, and imaging features for each patientwere summarized in Table #.
).". CBF Velocity Measurements and PI. Mean /ow velocitiesin the MCA ranged widely from ' to #)$ cm/s. *e averageMCA mean /ow velocities were 53 ± 38 cm/s and 51 ±26 cm/s, respectively, in the most swollen cerebral hemi-sphere and in the contralateral hemisphere. *e MCA PIvaried from ".-# to %."(; the average MCA PI was 1.85 ± 1.56in the most swollen hemisphere and #.%$, contralaterally. Allpatients with MCA mean /ow velocity < 40 cm/s presentedPI >#."", and those with MCA mean /ow velocity >#"" cm/spresented PI <".-$.*e LR was <$ in all cases.
).). Classi*cation of Patients and -eir Cerebral HemispheresbyHemodynamic Patterns. Tenpatients (&!.%%)were consid-ered as having cerebral oligoemia, $ patients (#&.'%) met thecriteria for cerebral hyperemia, and - patients ($#.&%) werefound to present nonspeci+c circulatory pattern. No patientswere found to have hyperemia in one cerebral hemisphereand oligoemia in the opposite hemisphere (Table !).
In the most swollen cerebral hemisphere, &!.-% of thepatients presentedMCAmean /ow velocities<)" cm/s (cere-bral oligoemia), $-.(% between )" and #"" cm/s (nonspe-ci+c hemodynamic pattern), and #".&% >#"" cm/s (cerebralhyperemia). In the opposite side, #%.-% of the patients hadMCA mean /ow velocities <)" cm/s (cerebral oligoemia),%-.&% between )" and #"" cm/s (nonspeci+c hemodynamicpattern), and &.(% >#"" cm/s (cerebral hyperemia) (Table !).Abnormal hemodynamic patterns were more frequentlyfound in the most swollen cerebral hemisphere than in theopposite hemisphere (-$.#% versus !$.&%, resp.) (" < 0.05).).%. Cerebral Hemodynamic Patterns and Outcome. No cor-relation was found between cerebral hemodynamic patternsand other variables such as preoperative GCS score, thedegree ofmidline cerebral structures shi, on preoperative CTscan, GOS scores at - months a,er injury, and neurologicalrecovery according to favorable (good recovery andmoderate
2
10
7
1
3
13
0
2
4
6
8
10
12
14
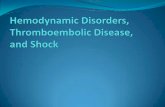
Most swollen cerebral hemisphereContralateral cerebral hemisphere
Oligoemia(MCA BFV <
40 cm/s)
Hyperemia(MCA BFV >100 cm/s
and LR <3)
Nonspeci!c(MCA BFV = 40 cm/s–
100 cm/s)
F12345 #: Hemodynamic patterns in the most swollen cerebralhemisphere and in the contralateral hemisphere (number of patientsversus hemodynamic pattern in TCD). LR: Lindegaard ratio; MCA:middle cerebral artery; BFV: blood /ow velocity; TCD: transcranialDoppler ultrasonography; All patients presented LR <$.disability) or unfavorable outcome (severe disability, vegeta-tive state, or death) at -months followup.
4. Discussion
%.!. Overview of Results. We report a series of #( patients withtraumatic brain swelling and evidence of increased ICP andbrain herniation, refractory to clinical measures, in whomcerebral hemodynamic assessment by TCD ultrasonographywas performed prior to decompressive craniectomy. Partic-ipants and their cerebral hemispheres (the side of maximalcerebral swelling and the opposite side) were categorizedaccording to TCD hemodynamic patterns, and the +ndingscorrelated with preoperative GCS score, degree of midlinecerebral structures shi, on preoperative CT scan, GOS scoresat -months a,er injury, and --month follow-up neurologicaloutcome based on favorable or unfavorable recovery. To ourknowledge, this is the +rst study that systematically evaluatedthe cerebral blood circulation of patients with traumaticbrain swelling leading to uncontrollable raised ICP and brainherniation syndrome. Patients with severe brainstem injury(GCS score of $ and/or bilaterally +xed and dilated pupils)were excluded from this study; therefore, this investiga-tion refers to patients eligible for treatment. We showed awide diversity of cerebral hemodynamic +ndings, rangingfrom severe oligoemia to hyperemia. Ten patients (&!.%%)presented with cerebral oligoemia, $ patients (#&.'%) withcerebral hyperemia, and - patients ($#.&%) with nonspeci+ccirculatory pattern (Table !). Hemodynamic abnormalitieswere more frequently found in the side of maximal cere-bral swelling than in the opposite side (-$% versus !$%,resp.) (Figure #). PI values suggested that ICP varied fromacceptable to considerably high; patients with increased PI,indicating high microvascular resistance, tended to have

) BioMed Research International
T6785#:Summaryo
fpatien
ts’demograph
ic,clinical,a
ndradiologica
ldata! .
Case
no.
Age(yrs),Sex
Lesio
nsop
erated
atho
spita
ladm
ission
Intervalfro
madmissionto
TCD
GCS
score
Pupils
Midbrain
cisterns
Midlin
eshi,on
CT(m
m)
Side
ofmaxim
alcerebralsw
elling
CHP
--MoGOS
score
#-$,F
-ho
urs
-Un
equal
Absent
#!Right
Oligoemia
#!
#',M
)ho
urs
-Un
equal
Absent
#-Right
Non
speci+c
#$
!',M
-days
-Un
equal
Absent
(Le,
Oligoemia
&)
$(,F
%hou
rs-
Unequal
Absent
##Right
Hyperem
ia$
&!',M
$hou
rs%
Unequal
Absent
#&Right
Oligoemia
)-
!&,M
)days
-Un
equal
Absent
#!Right
Oligoemia
$%
#(,F
ICH
!)ho
urs
-Un
equal
Right
Non
speci+c
)'
!',F
!hou
rs-
Unreactiv
eAb
sent
(Le,
Oligoemia
)(
!!,M
!hou
rs-
Unequal
Absent
#)Right
Hyperem
ia!
#"!&,F
-days
&Un
equal
Absent
'Right
Oligoemia
###
$",M
ICH
!days
-Un
equal
Absent
#%Right
Oligoemia
##!
!%,M
SDH
'days
-Un
equal
Absent
#!Right
Non
speci+c
&#$
#%,M
SDH
$days
#"Un
equal
Absent
&Le,
Hyperem
ia)
#)$(,M
EDH
$days
#!Un
equal
Right
Oligoemia
)#&
-#,F
ICHSD
H$d
ays
(Un
equal
Absent
##Le,
Oligoemia
!#-
&#,M
ICH
)days
(Un
equal
Absent
#(Le,
Non
speci+c
$#%
)$,M
SDH
$days
-Un
equal
Absent
!"Le,
Non
speci+c
##'
)-,M
SDH
(days
)Un
equal
Absent
#"Right
Oligoemia
!#(
!$,M
ICH
#day
-Un
reactiv
eAb
sent
#&Le,
Non
speci+c
$! EDH
:extradu
ralh
ematom
a;GCS
:Glas
gowCo
maS
cale;
GOS:Glas
gowOutcomeS
cale;
ICH:traum
aticcontusionalintracerebralhemorrhage;SD
H:sub
duralh
ematom
a;Un
equal:un
equal,atlea
ston
ereactive;
Unreactiv
e:un
reactiv
ebilaterally;C
HP:
cerebralhemod
ynam
icpatte
rns.

BioMed Research International &
T6785 !: Number of patients according to cerebral hemodynamicpatterns.
Hemodynamic patterns No. of patientsHyperemia $ (#&.'%)Oligoemia #" (&!.%%)Nonspeci+c - ($#.&%)
cerebral oligoemia, whereas those with decreased PI, re/ect-ing low microvascular resistance, tended to have cerebralhyperemia. No correlation was found between preoperativecerebral hemodynamic patterns and GOS scores at -monthsa,er injury and neurological recovery according to favorable(good recovery and moderate disability) or unfavorableoutcome (severe disability, vegetative state, or death) at -months followup.
%.". Methodological Issues. A potential criticism of our studyis the absence of ICPmeasurements, quantitative estimationsof CBF, cerebral arteriovenous oxygen di.erence, cerebralmetabolic rate of oxygen consumption, and biochemicalmarkers for cerebral ischemia. However, in our department,we have used clinical monitoring,measurements by noninva-sivemethods, and serial imaging.We have used ICPmonitor-ing only in selected cases with +ndings suggestive of intracra-nial hypertension in the neurosonograhic assessment.
*e management of severe TBI without ICP monitoringin all patients has been con+rmed in the recent study byChesnut et al. [!)], presenting the bene+t of ICP monitoringfor the outcome in randomized prospective trial. Measuringof the other physiological variables also requires the use ofinvasive cerebral and jugular venous catheters, aswell as time-consuming procedures that are di0cult to justify in patientswith neurological deterioration and evidence of uncontrol-lable intracranial hypertension and brain herniation. TCDstudy cannot provide quantitative blood /ow data, such as/ow rate, expressed inmL/min, or tissue perfusion, expressedin mL/#"" g of brain tissue/min [$, )]; however, blood /owvelocities in the cerebral arteries allow detection of cerebralhyperemia, oligoemia, and vasospasm [!&–!']. Despite thelimitations of TCD ultrasonography, its noninvasiveness andthe possibility of rapid real-time acquisition of intracranialhemodynamic data made this study possible.
For interpreting the results of TCD ultrasonography, itis necessary to consider the possibility that both cerebralhyperemia (elevated CBF) and vasospasm usually occurmore noticeably as of ! days a,er injury [#!, !']. Blood/ow velocities >#"" cm/second should be interpreted withcaution given that high blood /ow velocities in the cerebralarteries can be found in hyperemia as well as in vasospasm[!&–!%]; LR was used in our study to di.erentiate hyperemiafrom vasospasm [!-].
Our results failed to demonstrate a correlation betweencerebral hemodynamic patterns and GOS scores at -monthsa,er injury and between cerebral hemodynamic patterns andneurological recovery according to favorable or unfavorableoutcomes at - months followup, although this fact doesnot mean that those correlations cannot exist because of
the limitations of this investigation which include smallpatient sample, heterogeneous characteristics of the patientpopulation, coexistence of several prognostic factors, and thecomplexity of the brain’s hemimetabolic phenomena.
%.). Previous Investigations. In the Morgalla et al.’s seriescomprising $$ head-injured patients who underwent decom-pressive craniectomy, preoperative TCD ultrasonographydisclosed high resistance CBF pattern in !)% of patients,systolic spikes in #!% of patients, systolic /ow pattern withabsent diastolic /ow in &%% of patients, and normal TCD/ow pattern in #!% of patients [!(]. *ese data indicateoccurrence of cerebral oligoemia and nonspeci+c circulatorypattern in the setting of refractory raised ICP and brainherniation, which are quite intuitive and understandable.Although the characterization of TCD /ow velocities was notthe purpose of the study and there was no description ofcerebral hyperemia in this series [!(], these data also revealeda wide variability in cerebral hemodynamic presentationswhich are in line with our +ndings. On the other hand, itis reasonable to accept the occurrence of cerebral hyperemiain patients with uncontrollable increased ICP and brainherniation, as seen in our series. Kelly et al. [$", $#] performeda physiological strati+cation of TBI patients based on CBFand ICP measurements and described +ve subgroups ofpatients, each exhibiting relatively unique clinical coursesand outcomes: (#) hyperemia without intracranial hyper-tension, (!) hyperemia with intracranial hypertension andfavorable outcome, ($) cerebral vasoparalysis and hyper-emia with intracranial hypertension and poor outcome (ourpatients), ()) intracranial hypertension without hyperemia(our patients), and (&) normal ICP without hyperemia.
Interestingly, Morgalla et al. [!(, $!] have consideredTCD studies as an important adjunct in decision making,monitoring cerebral hemodynamic deterioration to systolic/ow pattern (with absent diastolic /ow) in some cases. Inour series, TCD data were not a deciding factor for surgicaldecompression, which was indicated based on clinical andCT +ndings compatible with raised ICP and brain herniation.We were afraid of waiting for the cerebral diastolic /owto cease since at this time CPP is certainly quite impairedand the indication of surgical treatment may be too latefor some patients [)]. Another option to measure hemody-namic changes in severe TBI patients is contrast-enhancedultrasonography (CEU). Heppner et al. [$$] have used thistechnique for noninvasive evaluation of cerebral perfusion inpatients with traumatic brain injury and to assess the e.ect ofdecompressive surgery on cerebral perfusion as measured byCEU. *e authors studied with TBI undergoing decompres-sive craniectomy and concluded that this ultrasonographymethod has potential for the intraoperative and bedsideassessment of cerebral perfusion in patients with TBI.
%.%. Implications for Treatment. Current therapeutic strategyconcerning CBF management in head-injured patients is toavoid states of critical cerebral hyperemia and oligoemia[), $), $&]. In theory, the former can lead to further increasein cerebral blood volume, vasogenic edema, and the risk

- BioMed Research International
of intracerebral bleeding, while the latter can induce cere-bral ischemia and infarction. Both states can worsen brainswelling and intracranial hypertension. For these reasons,decompressive craniectomy as the sole treatment could beinsu0cient in these cases [), $-]. E.orts must be made tomaintain adequate cerebral hemodynamics, preferably cou-pled with metabolism, avoiding signi+cant cerebral hyper-emia and oligoemia. Factors that can aggravate cerebralhyperemia such as hypercapnia, anemia, arterial bloodhypertension, increased cardiac output, hypervolemia, andcerebral metabolic crisis, among others, must be investi-gated and corrected if possible. In contrast, factors that canintensify cerebral oligoemia, such as hypocapnia, arterialblood hypotension, decreased cardiac output, hypovolemia,dehydration, and raised ICP must be ruled out and treatedwhen appropriate. Factors that increase cerebral metabolicactivity, such as hyperthermia and seizures, must be kept inmind, irrespective of cerebral hemodynamic pattern, whetherhyperemia or oligoemia. Despite not being demonstrated inour series, some patients can present with hemodynamicpattern suggestive of cerebral hyperemia in one hemisphereand oligoemia in the other [$&]. Treatment of these patients,mainly if both hyperemia and oligoemia are critically severe,may be challenging. Triple-H therapy or surgical decompres-sion indicated for treating cerebral oligoemia is clearly notsuitable for the hemisphere with hyperemia. Such patientsshould be monitored closely with multimodal fashion toachieve a middle ground whereby correction of cerebralhypoperfusion does not cause signi+cant worsening of con-tralateral cerebral hyperemia [$&]. For the future, in additionto CBF and ICP management, treatment at the biochemicallevel can be devised to manage brain swelling associated withposttraumatic cerebral metabolic crisis [$-, $%]. Althoughthere is no evidence to support the routine use of surgicaldecompression to reduce unfavorable outcomes in severe TBIand refractory high ICP, decompressive craniectomyhas beenthe treatment of choice [#–), -–(, ##–#&, #%–!$, !(, $!, $', $(].
5. Conclusions
*ere is a considerable heterogeneity of cerebral hemody-namic +ndings among individuals with refractory intracra-nial hypertension and brain herniation syndromedue to trau-matic brain swelling, and also between their cerebral hemi-spheres.*ese +ndings are in accordance with previous pub-lications on TBI, which demonstrated cerebral heterogene-ity in terms of circulation, pressure autoregulation, criticalclosing pressure, oxygenation, andmetabolism.*is supportsthe concept of heterogeneous nature of the pathophysiologyof the TBI and of the patients’ outcomes, suggesting thattherapeutic measures should be planned individually. *erecognition of posttraumatic cerebral hemodynamic patternsand their signi+cances is potentially useful for devising morespeci+c therapeutic strategies.
Conflict of Interests
*ere is no con/ict of interests and no +nancial disclosure inthis study.
References
[#] B. Aarabi, D. C. Hesdor.er, E. S. Ahn, C. Aresco, T. M. Scalea,and H. M. Eisenberg, “Outcome following decompressivecraniectomy for malignant swelling due to severe head injury,”Journal of Neurosurgery, vol. #"), no. ), pp. )-(–)%(, !""-.
[!] Y.-H. Bao, Y.-M. Liang, G.-Y. Gao, Y.-H. Pan, Q.-Z. Luo, and J.-Y. Jiang, “Bilateral decompressive craniectomy for patients withmalignant di.use brain swelling a,er severe traumatic braininjury: a $%-case study,” Journal of Neurotrauma, vol. !%, no. !,pp. $)#–$)%, !"#".
[$] E. Bor-Seng-Shu, M. J. Teixeira, R. Hirsch, A. F. De Andrade,and R. Marino Jr., “Transcranial doppler sonography in twopatients who underwent decompressive craniectomy for trau-matic brain swelling: report of two cases,” Arquivos de Neuro-Psiquiatria, vol. -!, no. $, pp. %#&–%!#, !"").
[)] E. Bor-Seng-Shu, R. Hirsch, M. J. Teixeira, A. F. De Andrade,and R. Marino Jr., “Cerebral hemodynamic changes gauged bytranscranial Doppler ultrasonography in patients with post-traumatic brain swelling treated by surgical decompression,”Journal of Neurosurgery, vol. #"), no. #, pp. ($–#"", !""-.
[&] A. F. deAndrade,W. S. Paiva, R. L.O. deAmorim et al., “Contin-uous ventricular cerebrospinal /uid drainage with intracranialpressure monitoring for management of posttraumatic di.usebrain swelling,” Arquivos de Neuro-Psiquiatria, vol. -(, no. #, pp.%(–'), !"##.
[-] D. James Cooper, J. V. Rosenfeld, L. Murray et al., “Decom-pressive craniectomy in di.use traumatic brain injury,”-e NewEngland Journal ofMedicine, vol. $-), no. #-, pp. #)($–#&"!, !"##.
[%] A. Daboussi, V. Minville, S. Leclerc-Foucras et al., “Cerebralhemodynamic changes in severe head injury patients under-going decompressive craniectomy,” Journal of NeurosurgicalAnesthesiology, vol. !#, no. ), pp. $$(–$)&, !""(.
['] B. M. Eberle, B. Schnuriger, K. Inaba, J. Peter Gruen, D.Demetriades, and H. Belzberg, “Decompressive craniectomy:surgical control of traumatic intracranial hypertension mayimprove outcome,” Injury, vol. )#, no. (, pp. '()–'(', !"#".
[(] L.H.Chi,M.W.Chee,K. L.Kah, I.Ng, andT.A. Beng, “Cerebraloxygenation, vascular reactivity, and neurochemistry followingdecompressive craniectomy for severe traumatic brain injury,”Journal of Neurosurgery, vol. #"', no. &, pp. ()$–()(, !""'.
[#"] K. Hu,M.-T. Lo, C. K. Peng et al., “Nonlinear pressure-/ow rela-tionship is able to detect asymmetry of brain blood circulationassociated with midline shi,,” Journal of Neurotrauma, vol. !-,no. !, pp. !!%–!$$, !""(.
[##] J. Jagannathan, D. O. Okonkwo, A. S. Dumont et al., “Outcomefollowing decompressive craniectomy in children with severetraumatic brain injury: a #"-year single-center experience withlong-term follow up,” Journal of Neurosurgery, vol. #"-, no. ), pp.!-'–!%&, !""%.
[#!] P. Kan, A. Amini, K. Hansen et al., “Outcomes a,er decompres-sive craniectomy for severe traumatic brain injury in children,”Journal of Neurosurgery, vol. #"&, no. &, pp. $$%–$)!, !""-.
[#$] E. Bor-Seng-Shu andM. J. Teixeira, “Brain vasospasm a,er headinjury,” Journal of Neurosurgery, vol. #"-, no. ), pp. %!'–%$",!""%.
[#)] W. Qiu, C. Guo, H. Shen et al., “E.ects of unilateral decom-pressive craniectomy on patients with unilateral acute post-traumatic brain swelling a,er severe traumatic brain injury,”Critical Care, vol. #$, no. -, p. R#'&, !""(.
[#&] T. Reithmeier, M. Lohr, P. Pakos, G. Ketter, and R.-I. Ernestus,“Relevance of ICP and ptiO! for indication and timing of

BioMed Research International %
decompressive craniectomy in patients with malignant brainedema,” Acta Neurochirurgica, vol. #)%, no. (, pp. ()%–(&!, !""&.
[#-] T. S. Skoglund, C. Eriksson-Ritzen, C. Jensen, and B. Rydenhag,“Aspects on decompressive craniectomy in patients with trau-matic head injuries,” Journal of Neurotrauma, vol. !$, no. #", pp.#&"!–#&"(, !""-.
[#%] J. F. Soustiel, G. E. Sviri, E. Mahamid, V. Shik, S. Abeshaus, andM. Zaaroor, “Cerebral blood /ow and metabolism followingdecompressive craniectomy for control of increased intracranialpressure,” Neurosurgery, vol. -%, no. #, pp. -&–%!, !"#".
[#'] M. F. Stiefel, G. G. Heuer, M. J. Smith et al., “Cerebraloxygenation following decompressive hemicraniectomy for thetreatment of refractory intracranial hypertension,” Journal ofNeurosurgery, vol. #"#, no. !, pp. !)#–!)%, !"").
[#(] A. Taylor,W. Butt, J. Rosenfeld et al., “A randomized trial of veryearly decompressive craniectomy in children with traumaticbrain injury and sustained intracranial hypertension,” Child’sNervous System, vol. #%, no. $, pp. #&)–#-!, !""#.
[!"] I. Timofeev, M. Czosnyka, J. Nortje et al., “E.ect of decom-pressive craniectomy on intracranial pressure and cerebrospinalcompensation following traumatic brain injury,” Journal ofNeurosurgery, vol. #"', no. #, pp. --–%$, !""'.
[!#] T.Ucar,M.Akyuz, S. Kazan, andR. Tuncer, “Role of decompres-sive surgery in the management of severe head injuries: prog-nostic factors and patient selection,” Journal of Neurotrauma,vol. !!, no. ##, pp. #$##–#$#', !""&.
[!!] E. C. Wang, B. T. Ang, J. Wong, J. Lim, and I. Ng, “Characteri-zation of cerebrovascular reactivity a,er craniectomy for acutebrain injury,” British Journal of Neurosurgery, vol. !", no. #, pp.!)–$", !""-.
[!$] R. F. Williams, L. J. Magnotti, M. A. Croce et al., “Impact ofdecompressive craniectomy on functional outcome a,er severetraumatic brain injury,” -e Journal of Trauma, vol. --, no. -,pp. #&%"–#&%-, !""(.
[!)] R. M. Chesnut, G. Petroni, and C. Rondina, “Intracranial-pressure monitoring in traumatic brain injury,” -e New Eng-land Journal of Medicine, vol. $-', no. #', pp. #%&#–#%&!, !"#$.
[!&] J. H. Lee, N. A. Martin, G. Alsina et al., “Hemodynamicallysigni+cant cerebral vasospasm and outcome a,er head injury:a prospective study,” Journal of Neurosurgery, vol. '%, no. !, pp.!!#–!$$, #((%.
[!-] K.-F. Lindegaard, H. Nornes, S. J. Bakke, W. Sorteberg, and P.Nakstad, “Cerebral vasospasm diagnosis by means of angiogra-phy and blood velocity measurements,” Acta Neurochirurgica,vol. #"", no. #-!, pp. #!–!), #('(.
[!%] N. A. Martin, R. V. Patwardhan, M. J. Alexander et al., “Char-acterization of cerebral hemodynamic phases following severehead trauma: hypoperfusion, hyperemia, and vasospasm,” Jour-nal of Neurosurgery, vol. '%, no. #, pp. (–#(, #((%.
[!'] M. Oertel, W. J. Boscardin, W. D. Obrist et al., “Posttraumaticvasospasm: the epidemiology, severity, and time course of anunderestimated phenomenon: a prospective study performed in!(( patients,” Journal of Neurosurgery, vol. #"$, no. &, pp. '#!–'!), !""&.
[!(] M. H. Morgalla, B. E. Will, F. Roser, andM. Tatagiba, “Do long-term results justify decompressive craniectomy a,er severetraumatic brain injury? Clinical article,” Journal of Neuro-surgery, vol. #"(, no. ), pp. -'&–-(", !""'.
[$"] D. F. Kelly, R. K. Kordestani, N. A. Martin et al., “Hyperemiafollowing traumatic brain injury: relationship to intracranialhypertension and outcome,” Journal of Neurosurgery, vol. '&, no.&, pp. %-!–%%#, #((-.
[$#] D. F. Kelly, N. A. Martin, R. Kordestani et al., “Cerebral blood/ow as a predictor of outcome following traumatic brain injury,”Journal of Neurosurgery, vol. '-, no. ), pp. -$$–-)#, #((%.
[$!] M. H. Morgalla, L. Krasznai, R. Buchholz et al., “Repeateddecompressive craniectomy a,er head injury in children: twosuccessful cases as result of improved neuromonitoring,” Surgi-cal Neurology, vol. )$, no. -, pp. &'$–&(", #((&.
[$$] P. Heppner, D. B. Ellegala, M. Durieux, J. A. Jane Sr., and J.R. Lindner, “Contrast ultrasonographic assessment of cerebralperfusion in patients undergoing decompressive craniectomyfor traumatic brain injury,” Journal of Neurosurgery, vol. #"), no.&, pp. %$'–%)&, !""-.
[$)] E. Bor-Seng-Shu, W. S. Kita, E. G. Figueiredo et al., “Cerebralhemodynamics: concepts of clinical importance,” Arq Neurop-siquiatr, vol. %", no. &, pp. $&!–$&-, !"#!.
[$&] E. Bor-Seng-Shu andM. J. Teixeira, “Brain vasospasm a,er headinjury,” Journal of Neurosurgery, vol. #"-, no. ), pp. %!'–%$",!""%.
[$-] E. Bor-Seng-Shu, M. De Lima Oliveira, and M. J. Teixeira,“Traumatic brain injury and metabolism,” Journal of Neuro-surgery, vol. ##!, no. -, pp. #$&#–#$&$, !"#".
[$%] P. Vespa, D. L. McArthur, J. Alger et al., “Regional heterogeneityof post-traumatic brain metabolism as studied by microdial-ysis, magnetic resonance spectroscopy and positron emissiontomography,” Brain Pathology, vol. #), no. !, pp. !#"–!#), !"").
[$'] E. Bor-Seng-Shu, E. G. Figueiredo, R. L. Amorim et al.,“Decompressive craniectomy: a meta-analysis of in/uences onintracranial pressure and cerebral perfusion pressure in thetreatment of traumatic brain injury,” Journal of Neurosurgery,vol. ##%, no. $, pp. &'(–&(-, !"#!.
[$(] E. Bor-Seng-Shu, E. G. Figueiredo, E. T. Fono. et al., “Decom-pressive craniectomy and head injury: brainmorphometry, ICP,cerebral hemodynamics, cerebral microvascular reactivity, andneurochemistry,” Neurosurgical Review, vol. $-, no. $, pp. $-#–$%", !"#$.

Submit your manuscripts athttp://www.hindawi.com
Hindawi Publishing Corporationhttp://www.hindawi.com Volume 2013
Oxidative Medicine and Cellular Longevity
Hindawi Publishing Corporation http://www.hindawi.com Volume 2013Hindawi Publishing Corporation http://www.hindawi.com Volume 2013
The Scientific World Journal
,QWHUQDWLRQDO�-RXUQDO�RI
(QGRFULQRORJ\+LQGDZL�3XEOLVKLQJ�&RUSRUDWLRQKWWS���ZZZ�KLQGDZL�FRP
9ROXPH�����
ISRN AnesthesiologyHindawi Publishing Corporationhttp://www.hindawi.com Volume 2013
OncologyJournal of
Hindawi Publishing Corporationhttp://www.hindawi.com Volume 2013
PPARRe sea rch
Hindawi Publishing Corporationhttp://www.hindawi.com Volume 2013
OphthalmologyJournal of
Hindawi Publishing Corporationhttp://www.hindawi.com Volume 2013
ISRN AllergyHindawi Publishing Corporationhttp://www.hindawi.com Volume 2013
BioMed Research International
Hindawi Publishing Corporationhttp://www.hindawi.com Volume 2013
ObesityJournal of
Hindawi Publishing Corporationhttp://www.hindawi.com Volume 2013
ISRN AddictionHindawi Publishing Corporationhttp://www.hindawi.com Volume 2013
Hindawi Publishing Corporationhttp://www.hindawi.com Volume 2013
Computational and Mathematical Methods in Medicine
ISRN AIDSHindawi Publishing Corporationhttp://www.hindawi.com Volume 2013
Clinical &DevelopmentalImmunology
Hindawi Publishing Corporationhttp://www.hindawi.com
Volume 2013
Diabetes ResearchJournal of
Hindawi Publishing Corporationhttp://www.hindawi.com Volume 2013
Evidence-Based Complementary and Alternative Medicine
Volume 2013Hindawi Publishing Corporationhttp://www.hindawi.com
Hindawi Publishing Corporationhttp://www.hindawi.com Volume 2013
Gastroenterology Research and Practice
Hindawi Publishing Corporationhttp://www.hindawi.com Volume 2013
ISRN Biomarkers
Hindawi Publishing Corporationhttp://www.hindawi.com Volume 2013
MEDIATORSINFLAMMATION
of