Model-Based Seizure Detection for Intracranial EEG Recordings
10
IEEE TRANSACTIONS ON BIOMEDICAL ENGINEERING, VOL. 59, NO. 5, MAY 2012 1419 Model-Based Seizure Detection for Intracranial EEG Recordings R. Yadav, Student Member, IEEE, M. N. S. Swamy, Fellow, IEEE, and R. Agarwal ∗ , Member, IEEE Abstract—This paper presents a novel model-based patient- specific method for automatic detection of seizures in the in- tracranial EEG recordings. The proposed method overcomes the complexities in the practical implementation of the patient-specific approach of seizure detection. The method builds a seizure model (set of basis functions) for a priori known seizure (the template seizure pattern), and uses the statistically optimal null filters as a building block for the detection of similar seizures. The process of modeling the template seizure is fully automatic. Overall, the detection method involves the segmentation of the template seizure pattern, rejection of the redundant and noisy segments, extraction of features from the segments to generate a set of models, selection of the best seizure model, and training of the classifier. The trained classifier is used to detect similar seizures in the remaining data. The resulting seizure detection method was evaluated on a total of 304 h of single-channel depth EEG recordings from 14 patients. The system performance is further compared to the Qu–Gotman patient-specific system using the same data. A significant improve- ment in the proposed system, in terms of specificity, is observed over the compared method. Index Terms—Automatic seizure detection, EEG, epilepsy, sta- tistically optimal null filters (SONFs). I. INTRODUCTION E PILEPSY is a chronic condition of the brain characterized by an enduring propensity to generate epileptic seizures that are different for each individual and contribute to disability and impaired quality of life. It has significant economic im- plications in terms of healthcare needs, premature deaths, and lost work production [1]–[3]. The primary diagnostic tool in the epilepsy is the EEG, in which the epileptic seizures become apparent as rhythmic discharges, often coinciding with or at times even preceding the earliest observable changes in behav- ior. Seizure detection helps in the accurate diagnosis of epilepsy and may be used to warn or abort an ongoing seizure [4]. Since Manuscript received July 29, 2011; revised November 12, 2011 and January 6, 2012; accepted February 6, 2012. Date of publication February 22, 2012; date of current version April 20, 2012. This work was supported in part by the Natural Sciences and Engineering Research Council (NSERC) of Canada under Grant A-7739. Asterisk indicates corresponding author. R. Yadav and M. N. S. Swamy are with the Center for Signal Processing and Communications (CENSIPCOM), Department of Electrical and Computer Engineering, Concordia University, Montreal, QC H3G 1M8, Canada (e-mail: [email protected]; [email protected]). ∗ R. Agarwal is affiliated with the Center for Signal Processing and Com- munications (CENSIPCOM), Department of Electrical and Computer Engi- neering, Concordia University, Montreal, QC H3G 1M8, Canada (e-mail: [email protected]). Color versions of one or more of the figures in this paper are available online at http://ieeexplore.ieee.org. Digital Object Identifier 10.1109/TBME.2012.2188399 the time of seizure occurrence is unknown, the monitoring peri- ods range from days to weeks generating a huge amount of data. Seizures are identified in the voluminous EEG data by visual inspection, which is time consuming, tiresome, and prone to errors. Thus, automatic seizure detection is warranted to aid in the rapid review of the voluminous EEG data [4], [5]. One popular design approach for automatic seizure detection is based on determining the boundaries between seizure and nonseizure EEG features by complex discrimination systems in which large training data are utilized. Detection techniques de- veloped by this approach are commonly referred to as generic seizure detection methods, and perform poorly due to the high inter-individual EEG variability [5], [6]. It is generally consid- ered difficult to design a single method that can detect all types of seizures in all patients [7]. The recurring nature of seizures within a patient opens pos- sibilities to overcome the poor performance of the generic de- tectors. It is observed that in most of the patients, one or two and sometimes more types of seizures tend to occur repeat- edly. In these cases, the electrographic seizure activity within each type is similar, though not identical [8]. It is possible to train a patient-specific seizure detector utilizing the information extracted from a previously identified template seizure for the patient under consideration. Detection schemes based on this design approach report significantly improved detection perfor- mance over the generic schemes [8]–[10]. In addition to the im- proved detection performance, patient-specific techniques play a pivotal role in defining and understanding the epileptogenic area that can possibly lead to improved surgical treatment [2], [6], [11]–[15]. Even though the patient-specific schemes demonstrate im- proved performance over the generic seizure detection methods, they are not practical. The main limiting factors in all patient- specific seizure detectors are 1) supervised selection of the tem- plate seizure; 2) supervised selection of the nonseizure EEG (or a set of nonseizure EEG patterns); and 3) supervised train- ing of the classifier. Another fundamental problem in seizure detection methods (generic as well as patient specific) is in de- tecting seizures that have subtle changes in the amplitude [4], [5], [10]. This problem is also evident in the visual detection of seizures. Addressing some of these limitations will lead to a more practical solution in the design of patient-specific seizure detectors. We present a novel method that addresses two of the three aforementioned limitations, notably, the supervised selection of nonseizure EEG and supervised training of the classifier. More- over, our method is capable of accurately detecting seizures that evolve with subtle changes in the EEG amplitude. Initial results of parts of the overall method have been presented at the IEEE 0018-9294/$31.00 © 2012 IEEE
Transcript of Model-Based Seizure Detection for Intracranial EEG Recordings

IEEE TRANSACTIONS ON BIOMEDICAL ENGINEERING, VOL. 59, NO. 5, MAY 2012 1419
Model-Based Seizure Detection for IntracranialEEG Recordings
R. Yadav, Student Member, IEEE, M. N. S. Swamy, Fellow, IEEE, and R. Agarwal∗, Member, IEEE
Abstract—This paper presents a novel model-based patient-specific method for automatic detection of seizures in the in-tracranial EEG recordings. The proposed method overcomes thecomplexities in the practical implementation of the patient-specificapproach of seizure detection. The method builds a seizure model(set of basis functions) for a priori known seizure (the templateseizure pattern), and uses the statistically optimal null filters as abuilding block for the detection of similar seizures. The processof modeling the template seizure is fully automatic. Overall, thedetection method involves the segmentation of the template seizurepattern, rejection of the redundant and noisy segments, extractionof features from the segments to generate a set of models, selectionof the best seizure model, and training of the classifier. The trainedclassifier is used to detect similar seizures in the remaining data.The resulting seizure detection method was evaluated on a total of304 h of single-channel depth EEG recordings from 14 patients.The system performance is further compared to the Qu–Gotmanpatient-specific system using the same data. A significant improve-ment in the proposed system, in terms of specificity, is observedover the compared method.
Index Terms—Automatic seizure detection, EEG, epilepsy, sta-tistically optimal null filters (SONFs).
I. INTRODUCTION
E PILEPSY is a chronic condition of the brain characterizedby an enduring propensity to generate epileptic seizures
that are different for each individual and contribute to disabilityand impaired quality of life. It has significant economic im-plications in terms of healthcare needs, premature deaths, andlost work production [1]–[3]. The primary diagnostic tool inthe epilepsy is the EEG, in which the epileptic seizures becomeapparent as rhythmic discharges, often coinciding with or attimes even preceding the earliest observable changes in behav-ior. Seizure detection helps in the accurate diagnosis of epilepsyand may be used to warn or abort an ongoing seizure [4]. Since
Manuscript received July 29, 2011; revised November 12, 2011 and January6, 2012; accepted February 6, 2012. Date of publication February 22, 2012;date of current version April 20, 2012. This work was supported in part by theNatural Sciences and Engineering Research Council (NSERC) of Canada underGrant A-7739. Asterisk indicates corresponding author.
R. Yadav and M. N. S. Swamy are with the Center for Signal Processingand Communications (CENSIPCOM), Department of Electrical and ComputerEngineering, Concordia University, Montreal, QC H3G 1M8, Canada (e-mail:[email protected]; [email protected]).
∗R. Agarwal is affiliated with the Center for Signal Processing and Com-munications (CENSIPCOM), Department of Electrical and Computer Engi-neering, Concordia University, Montreal, QC H3G 1M8, Canada (e-mail:[email protected]).
Color versions of one or more of the figures in this paper are available onlineat http://ieeexplore.ieee.org.
Digital Object Identifier 10.1109/TBME.2012.2188399
the time of seizure occurrence is unknown, the monitoring peri-ods range from days to weeks generating a huge amount of data.Seizures are identified in the voluminous EEG data by visualinspection, which is time consuming, tiresome, and prone toerrors. Thus, automatic seizure detection is warranted to aid inthe rapid review of the voluminous EEG data [4], [5].
One popular design approach for automatic seizure detectionis based on determining the boundaries between seizure andnonseizure EEG features by complex discrimination systems inwhich large training data are utilized. Detection techniques de-veloped by this approach are commonly referred to as genericseizure detection methods, and perform poorly due to the highinter-individual EEG variability [5], [6]. It is generally consid-ered difficult to design a single method that can detect all typesof seizures in all patients [7].
The recurring nature of seizures within a patient opens pos-sibilities to overcome the poor performance of the generic de-tectors. It is observed that in most of the patients, one or twoand sometimes more types of seizures tend to occur repeat-edly. In these cases, the electrographic seizure activity withineach type is similar, though not identical [8]. It is possible totrain a patient-specific seizure detector utilizing the informationextracted from a previously identified template seizure for thepatient under consideration. Detection schemes based on thisdesign approach report significantly improved detection perfor-mance over the generic schemes [8]–[10]. In addition to the im-proved detection performance, patient-specific techniques playa pivotal role in defining and understanding the epileptogenicarea that can possibly lead to improved surgical treatment [2],[6], [11]–[15].
Even though the patient-specific schemes demonstrate im-proved performance over the generic seizure detection methods,they are not practical. The main limiting factors in all patient-specific seizure detectors are 1) supervised selection of the tem-plate seizure; 2) supervised selection of the nonseizure EEG(or a set of nonseizure EEG patterns); and 3) supervised train-ing of the classifier. Another fundamental problem in seizuredetection methods (generic as well as patient specific) is in de-tecting seizures that have subtle changes in the amplitude [4],[5], [10]. This problem is also evident in the visual detectionof seizures. Addressing some of these limitations will lead to amore practical solution in the design of patient-specific seizuredetectors.
We present a novel method that addresses two of the threeaforementioned limitations, notably, the supervised selection ofnonseizure EEG and supervised training of the classifier. More-over, our method is capable of accurately detecting seizures thatevolve with subtle changes in the EEG amplitude. Initial resultsof parts of the overall method have been presented at the IEEE
0018-9294/$31.00 © 2012 IEEE

1420 IEEE TRANSACTIONS ON BIOMEDICAL ENGINEERING, VOL. 59, NO. 5, MAY 2012
Fig. 1. Illustration of temporal evolution of seizure on a single-channel EEGthat is observed as changing piecewise stationary rhythms as seizure continues.
meetings [16]–[18]. The method operates in two modes: trainingand testing. In the training mode, the system builds the seizuremodel and trains the classifier. In the testing mode, the classifierdetects seizure similar to a priori known seizure by tracking andmatching the time evolution of the seizure. The time evolutionof the seizure is the sequence of occurrence of the piecewise sta-tionary rhythms in the seizure. This novel approach allows theaccurate identification of recurring seizures and significantly re-duces false detections due to artifacts and nonepileptic rhythms.Furthermore, the proposed system performance is compared tothe Qu–Gotman patient-specific system [8] using the same data.
The remaining paper is organized as follows. Problem state-ment is described in Section II. Section III presents the model-based seizure detection system. Section IV presents the resultfrom the proposed system on 14 patient data and is compared tothe popular Qu–Gotman patient-specific system [8]. Results arediscussed in Section V and conclusions are drawn in Section VI.
II. PROBLEM STATEMENT
We assume seizure to be a narrowband signal in comparisonto the disproportionately large background EEG and define theproblem as the detection of rhythmic narrowband seizure ac-tivity, s(n), from the observed EEG consisting of signal andnoise, x(n) = s(n) + n(n). It is important to note that therhythmic narrowband seizure activity evolves as the seizure pro-gresses over time. In other words, a seizure is composed of shortpiecewise stationary rhythmic discharges that change from onerhythm to another as the seizure evolves [8], [13], [14], [19].Fig. 1 illustrates the temporal progression of a seizure in shortpiecewise stationary rhythms. The problem can be redefined asthe detection of these rhythms, i.e., the template seizure s(n)consists of a set components, s1(n), s2(n), . . . sN (n), with aspecific order of temporal occurrence.
We propose a model-based seizure detection system usingthe statistically optimal null filters (SONFs). SONF is a novelapproach for solving the problem of enhancement or suppres-sion of narrowband signals of short duration by combining themaximum signal-to-noise (SNR) ratio and least-squares (LS)optimization criteria [20]. Its intrinsic property is the ability to
track signals rapidly leading to a more practical processing ofshort-duration signals and has been shown to be equivalent tothe well-known Kalman filter, but with a much simpler imple-mentation [21]. Since the SONF is a linear time-varying filter,it can be implemented as a set of N parallel branches—one toestimate each seizure component without significantly increas-ing the computational cost. Parallel SONF branches becomeadvantageous to track the temporal occurrence of the individualseizure components that can further improve the detection speci-ficity. That is, the false detections due to nonepileptic rhythmicdischarges that have intrinsic characteristics similar to some ofthe seizure components can be minimized. This is possible be-cause an epileptic seizure is observed to evolve with sustaineddominant rhythms in short bursts as shown in Fig. 1, whilenormal EEG rhythms do not typically evolve [2], [17]. SONFsrequire a priori knowledge of the signal components or the basisfunctions constituting the signals to be estimated.
III. METHOD
A. Data Selection
The intracranial EEG data used in this study were acquiredwith the Harmonie System (Stellate System Inc., Montreal,Canada) from the Epilepsy Telemetry Unit at the Montreal Neu-rological Institute and Hospital (MNI/MNH). The data werefiltered between 0.5 and 70 Hz, prior to digitization at the sam-pling rate of 200 Hz. All patients had stainless steel depth EEGelectrodes of nine contacts that were surgically placed inside thebrain. There was no prescreening of the patients other than therequirement that they had at least three electrographic seizuresduring the monitoring sessions. For each patient, five sections ofrecordings, approximately 4–7 h each, were extracted such thatthree sections had at least one seizure each, one section duringwakefulness without seizures, and one without seizures duringsleep. Prior to sectioning, a trained EEG specialist using a bipo-lar montage scored all data for seizures. Since in some patients,seizures are only present in a single channel (focal seizures),we considered a single-channel evaluation of the patient data.Visual inspection of the first seizure section facilitated the se-lection of the single channel for analysis. For a patient withseizures occurring simultaneously on the multiple channels, weselected the channel in which the seizure is the most prominent.The selected channel is used to evaluate all data for the givenpatient. Data from 15 patients, originally collected betweenAugust 1998 and June 2004 for another study [5], were consid-ered for the design and development of the proposed algorithm.Data of one patient were rejected because it was not possible toclearly define the onset and the end of seizures. Thus, the datafrom 14 patients with over 304 h of EEG are used in this study.
For each patient, the first occurring seizure in one of the threeseizure sections is used as the template seizure pattern (TPAT )for the training of the proposed system. TPAT is the first 60 sor the complete seizure if it lasts less than 60 s. The trainingdata automatically include 30 s of EEG preceding the seizuretemplate.The trained detector is used to detect all other seizuresfor the given patient. In the literature, there exists a plethoraof patient-independent seizure detection methods while only a
YADAV et al.: MODEL-BASED SEIZURE DETECTION FOR INTRACRANIAL EEG RECORDINGS 1421
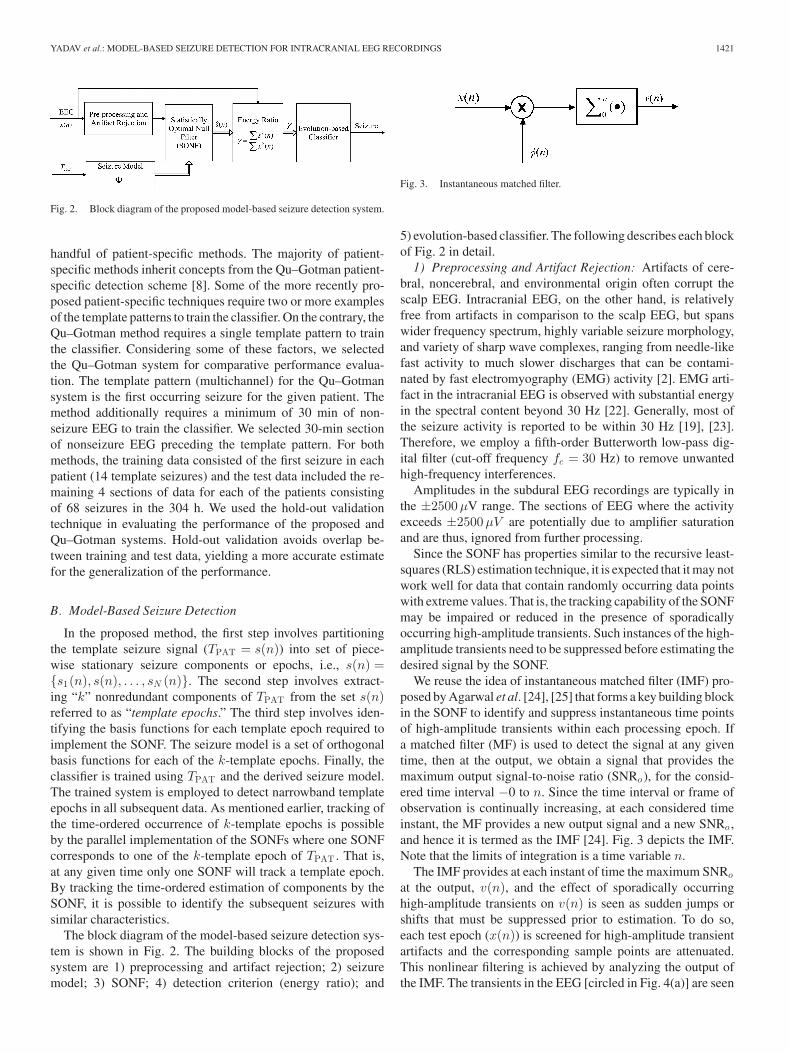
Fig. 2. Block diagram of the proposed model-based seizure detection system.
handful of patient-specific methods. The majority of patient-specific methods inherit concepts from the Qu–Gotman patient-specific detection scheme [8]. Some of the more recently pro-posed patient-specific techniques require two or more examplesof the template patterns to train the classifier. On the contrary, theQu–Gotman method requires a single template pattern to trainthe classifier. Considering some of these factors, we selectedthe Qu–Gotman system for comparative performance evalua-tion. The template pattern (multichannel) for the Qu–Gotmansystem is the first occurring seizure for the given patient. Themethod additionally requires a minimum of 30 min of non-seizure EEG to train the classifier. We selected 30-min sectionof nonseizure EEG preceding the template pattern. For bothmethods, the training data consisted of the first seizure in eachpatient (14 template seizures) and the test data included the re-maining 4 sections of data for each of the patients consistingof 68 seizures in the 304 h. We used the hold-out validationtechnique in evaluating the performance of the proposed andQu–Gotman systems. Hold-out validation avoids overlap be-tween training and test data, yielding a more accurate estimatefor the generalization of the performance.
B. Model-Based Seizure Detection
In the proposed method, the first step involves partitioningthe template seizure signal (TPAT = s(n)) into set of piece-wise stationary seizure components or epochs, i.e., s(n) ={s1(n), s(n), . . . , sN (n)}. The second step involves extract-ing “k” nonredundant components of TPAT from the set s(n)referred to as “template epochs.” The third step involves iden-tifying the basis functions for each template epoch required toimplement the SONF. The seizure model is a set of orthogonalbasis functions for each of the k-template epochs. Finally, theclassifier is trained using TPAT and the derived seizure model.The trained system is employed to detect narrowband templateepochs in all subsequent data. As mentioned earlier, tracking ofthe time-ordered occurrence of k-template epochs is possibleby the parallel implementation of the SONFs where one SONFcorresponds to one of the k-template epoch of TPAT . That is,at any given time only one SONF will track a template epoch.By tracking the time-ordered estimation of components by theSONF, it is possible to identify the subsequent seizures withsimilar characteristics.
The block diagram of the model-based seizure detection sys-tem is shown in Fig. 2. The building blocks of the proposedsystem are 1) preprocessing and artifact rejection; 2) seizuremodel; 3) SONF; 4) detection criterion (energy ratio); and
Fig. 3. Instantaneous matched filter.
5) evolution-based classifier. The following describes each blockof Fig. 2 in detail.
1) Preprocessing and Artifact Rejection: Artifacts of cere-bral, noncerebral, and environmental origin often corrupt thescalp EEG. Intracranial EEG, on the other hand, is relativelyfree from artifacts in comparison to the scalp EEG, but spanswider frequency spectrum, highly variable seizure morphology,and variety of sharp wave complexes, ranging from needle-likefast activity to much slower discharges that can be contami-nated by fast electromyography (EMG) activity [2]. EMG arti-fact in the intracranial EEG is observed with substantial energyin the spectral content beyond 30 Hz [22]. Generally, most ofthe seizure activity is reported to be within 30 Hz [19], [23].Therefore, we employ a fifth-order Butterworth low-pass dig-ital filter (cut-off frequency fc = 30 Hz) to remove unwantedhigh-frequency interferences.
Amplitudes in the subdural EEG recordings are typically inthe ±2500μV range. The sections of EEG where the activityexceeds ±2500μV are potentially due to amplifier saturationand are thus, ignored from further processing.
Since the SONF has properties similar to the recursive least-squares (RLS) estimation technique, it is expected that it may notwork well for data that contain randomly occurring data pointswith extreme values. That is, the tracking capability of the SONFmay be impaired or reduced in the presence of sporadicallyoccurring high-amplitude transients. Such instances of the high-amplitude transients need to be suppressed before estimating thedesired signal by the SONF.
We reuse the idea of instantaneous matched filter (IMF) pro-posed by Agarwal et al. [24], [25] that forms a key building blockin the SONF to identify and suppress instantaneous time pointsof high-amplitude transients within each processing epoch. Ifa matched filter (MF) is used to detect the signal at any giventime, then at the output, we obtain a signal that provides themaximum output signal-to-noise ratio (SNRo ), for the consid-ered time interval −0 to n. Since the time interval or frame ofobservation is continually increasing, at each considered timeinstant, the MF provides a new output signal and a new SNRo ,and hence it is termed as the IMF [24]. Fig. 3 depicts the IMF.Note that the limits of integration is a time variable n.
The IMF provides at each instant of time the maximum SNRo
at the output, v(n), and the effect of sporadically occurringhigh-amplitude transients on v(n) is seen as sudden jumps orshifts that must be suppressed prior to estimation. To do so,each test epoch (x(n)) is screened for high-amplitude transientartifacts and the corresponding sample points are attenuated.This nonlinear filtering is achieved by analyzing the output ofthe IMF. The transients in the EEG [circled in Fig. 4(a)] are seen

1422 IEEE TRANSACTIONS ON BIOMEDICAL ENGINEERING, VOL. 59, NO. 5, MAY 2012
Fig. 4. Impact of high-amplitude transients on the tracking ability of theSONF. (a) Estimate s(n) from the observed signal x(n) using SONF in thepresence of transient (enclosed in the ellipse). (b) Estimate s(n) of the observedsignal x(n) after filtering the observed transients. (c) IMF output (vk (n)) ofthe kth branch of the SONF for the two cases.
as sudden jump/shift in the output of the IMF (vk (n)) [circledin Fig. 4(c)] of the kth branch of the SONF.
The filtering process involves first removing linear trends inv(n). This is achieved by applying the first difference opera-tor. Let V be detrended v(n), a random variable of unknowndistribution with expected mean μ and variance σ2 . Then forany real number b > 0, Chebyshev’s inequality is defined asP (|V − μ| ≥ bσ) ≤ 1
b2 . Assuming that a relatively small per-centage of outliers (high-amplitude transients) are contained inx(n), then outliers are the sample points outside the boundary,bσ, i.e., sample points 3σ (where b = 3) away from the mean areconsidered to be due to the high-amplitude transients [17], [26].The amplitudes of the corresponding sample points are atten-uated by the empirically determined factor of 75% [17]. Thefiltered x(n) and its estimate ˆs(n) are shown in Fig. 4(b), whichclearly reflect suppression of the high-amplitude transients. Thefiltered x(n) is processed by the SONF for seizure detection.
2) Seizure Model: In the training mode for each patient data,the proposed system develops a seizure model for the a pri-ori known template seizure. The fully automated process ofmodeling TPAT involves 1) segmentation of TPAT into piece-wise stationary segments; 2) identification and rejection of re-dundant epochs resulting from the segmentation of TPAT ; and3) modeling of each remaining template epoch.
STFT-based segmentation: In the original work [16], the tem-plate pattern was visually segmented into 6 s epochs. As a fixedlength of the epochs may not be ideal for all types of seizures, wedetermine the length of the epochs using adaptive segmentation.The process is automated by introducing a short-time Fouriertransform (STFT)-based segmentation technique to identify thestationary sections [18]. The Fourier transform of the templatepattern is computed for sliding data frames of 2 s with a stepsize (τ ) of 0.25 s. The dominant rhythm frequency Fm in eachdata frame is defined as the frequency with maximum power:
Fm = maxf
{X(f)} (1)
where X(f) is the discrete Fourier transform and m denotesthe maximum power. The resulting set is a new discrete time
Fig. 5. STFT-based segmentation of TPAT . (a) 60 s long TPAT is shownalong with the evolution of dominant (peak) frequency Fm in (b). The epochsidentified by the adaptive segmentation algorithm in TPAT are enumerated.
series of the dominant frequency with a sampling interval of τ asshown in Fig. 5(b). The changes in the dominant rhythm of TPATare observed as a change in Fm (τ). The points of change in thedominant frequencies are identified as segmentation boundariesgiven by
gτ = |Fm (τ) − Fm (τ − 1)| < Δ (2)
where Δ(= 0.25) is the tolerance threshold defined as the max-imal allowable change in two consecutive Fm samples [18].
Segmented epochs shorter than 2 s are rejected. By doing so,we retain only the epochs with sustained dominant rhythm. Thelength of the basis functions is set as the average duration ofall the template epochs. The length of the sliding test windowrequired in the SONF is set equal to the length of the basisfunction.
In the example of Fig. 5, TPAT is segmented into a set ofseven stationary epochs (p = 7), E = {E1 , E2 , . . . , E7} basedon constant dominant rhythm frequency, Fm . Some epochs({E1 , E2}, {E3 , E4}, and {E5 , E6 , E7}) in this set repre-sent the same dominant rhythms. It is also possible that some ofthe epochs may be due to noise. Such epochs must be eliminatedprior to the construction of the seizure model.
Rejection of artifacts and redundant epochs in TPAT : A sim-ple approach to keep one of the several epochs with the samedominant rhythm is possible by examining the dominant fre-quency. Alternatively, cross-validation techniques can be ex-plored to identify and reject redundant epochs. We use the latterto identify and reject redundant epochs. The idea is to use thepth template epoch to derive a model for use in the SONF toprocess the remaining p − 1 template epochs. The detectionthreshold is set by running the pth epoch through the newlyderived SONF and is one-third of the maximum of energy ratio(γp ) computed by taking the energy ratio of the estimated andinput epoch (pth). From the remaining p − 1 epochs, all epochsdetected by the pth model are observed to be similar. The epochwith the highest energy ratio is retained as one of the templateepoch to model the seizure. The process is repeated until allepochs are unique. Epochs due to noise consist of a mixture offrequencies without any sustained rhythm. As a result, the detec-tion threshold obtained using the corresponding model, and the
YADAV et al.: MODEL-BASED SEIZURE DETECTION FOR INTRACRANIAL EEG RECORDINGS 1423
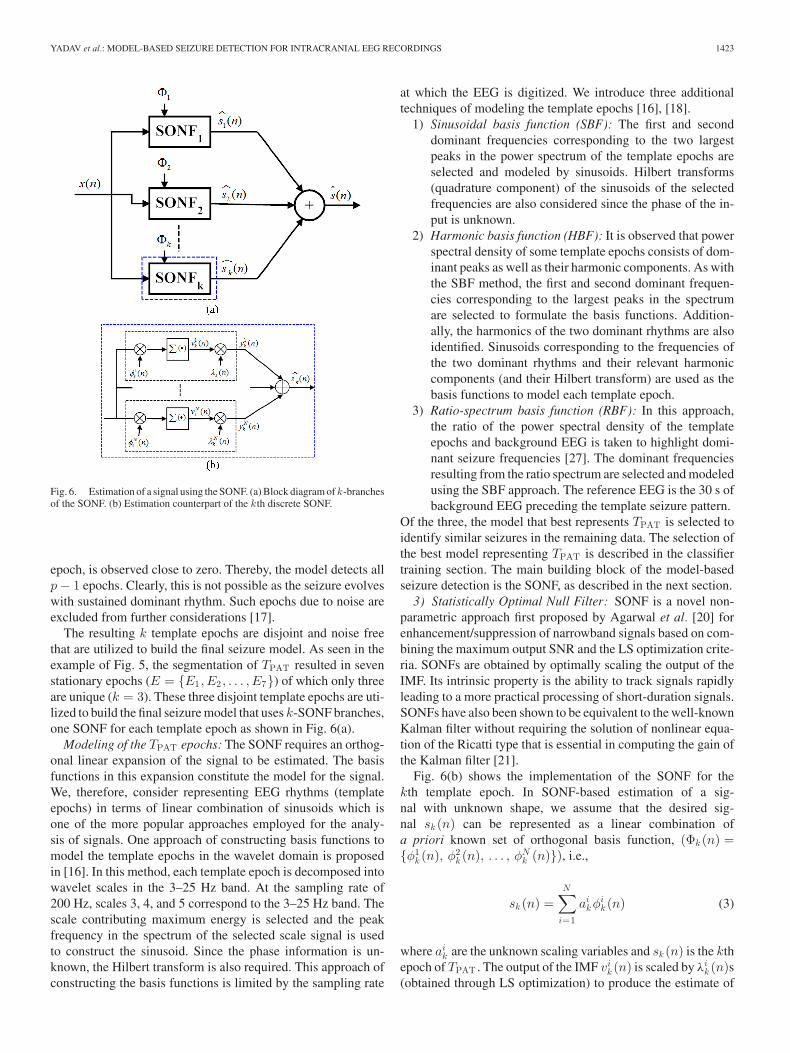
Fig. 6. Estimation of a signal using the SONF. (a) Block diagram of k-branchesof the SONF. (b) Estimation counterpart of the kth discrete SONF.
epoch, is observed close to zero. Thereby, the model detects allp − 1 epochs. Clearly, this is not possible as the seizure evolveswith sustained dominant rhythm. Such epochs due to noise areexcluded from further considerations [17].
The resulting k template epochs are disjoint and noise freethat are utilized to build the final seizure model. As seen in theexample of Fig. 5, the segmentation of TPAT resulted in sevenstationary epochs (E = {E1 , E2 , . . . , E7}) of which only threeare unique (k = 3). These three disjoint template epochs are uti-lized to build the final seizure model that uses k-SONF branches,one SONF for each template epoch as shown in Fig. 6(a).
Modeling of the TPAT epochs: The SONF requires an orthog-onal linear expansion of the signal to be estimated. The basisfunctions in this expansion constitute the model for the signal.We, therefore, consider representing EEG rhythms (templateepochs) in terms of linear combination of sinusoids which isone of the more popular approaches employed for the analy-sis of signals. One approach of constructing basis functions tomodel the template epochs in the wavelet domain is proposedin [16]. In this method, each template epoch is decomposed intowavelet scales in the 3–25 Hz band. At the sampling rate of200 Hz, scales 3, 4, and 5 correspond to the 3–25 Hz band. Thescale contributing maximum energy is selected and the peakfrequency in the spectrum of the selected scale signal is usedto construct the sinusoid. Since the phase information is un-known, the Hilbert transform is also required. This approach ofconstructing the basis functions is limited by the sampling rate
at which the EEG is digitized. We introduce three additionaltechniques of modeling the template epochs [16], [18].
1) Sinusoidal basis function (SBF): The first and seconddominant frequencies corresponding to the two largestpeaks in the power spectrum of the template epochs areselected and modeled by sinusoids. Hilbert transforms(quadrature component) of the sinusoids of the selectedfrequencies are also considered since the phase of the in-put is unknown.
2) Harmonic basis function (HBF): It is observed that powerspectral density of some template epochs consists of dom-inant peaks as well as their harmonic components. As withthe SBF method, the first and second dominant frequen-cies corresponding to the largest peaks in the spectrumare selected to formulate the basis functions. Addition-ally, the harmonics of the two dominant rhythms are alsoidentified. Sinusoids corresponding to the frequencies ofthe two dominant rhythms and their relevant harmoniccomponents (and their Hilbert transform) are used as thebasis functions to model each template epoch.
3) Ratio-spectrum basis function (RBF): In this approach,the ratio of the power spectral density of the templateepochs and background EEG is taken to highlight domi-nant seizure frequencies [27]. The dominant frequenciesresulting from the ratio spectrum are selected and modeledusing the SBF approach. The reference EEG is the 30 s ofbackground EEG preceding the template seizure pattern.
Of the three, the model that best represents TPAT is selected toidentify similar seizures in the remaining data. The selection ofthe best model representing TPAT is described in the classifiertraining section. The main building block of the model-basedseizure detection is the SONF, as described in the next section.
3) Statistically Optimal Null Filter: SONF is a novel non-parametric approach first proposed by Agarwal et al. [20] forenhancement/suppression of narrowband signals based on com-bining the maximum output SNR and the LS optimization crite-ria. SONFs are obtained by optimally scaling the output of theIMF. Its intrinsic property is the ability to track signals rapidlyleading to a more practical processing of short-duration signals.SONFs have also been shown to be equivalent to the well-knownKalman filter without requiring the solution of nonlinear equa-tion of the Ricatti type that is essential in computing the gain ofthe Kalman filter [21].
Fig. 6(b) shows the implementation of the SONF for thekth template epoch. In SONF-based estimation of a sig-nal with unknown shape, we assume that the desired sig-nal sk (n) can be represented as a linear combination ofa priori known set of orthogonal basis function, (Φk (n) ={φ1
k (n), φ2k (n), . . . , φN
k (n)}), i.e.,
sk (n) =N∑
i=1
aikφi
k (n) (3)
where aik are the unknown scaling variables and sk (n) is the kth
epoch of TPAT . The output of the IMF vik (n) is scaled by λi
k (n)s(obtained through LS optimization) to produce the estimate of
1424 IEEE TRANSACTIONS ON BIOMEDICAL ENGINEERING, VOL. 59, NO. 5, MAY 2012
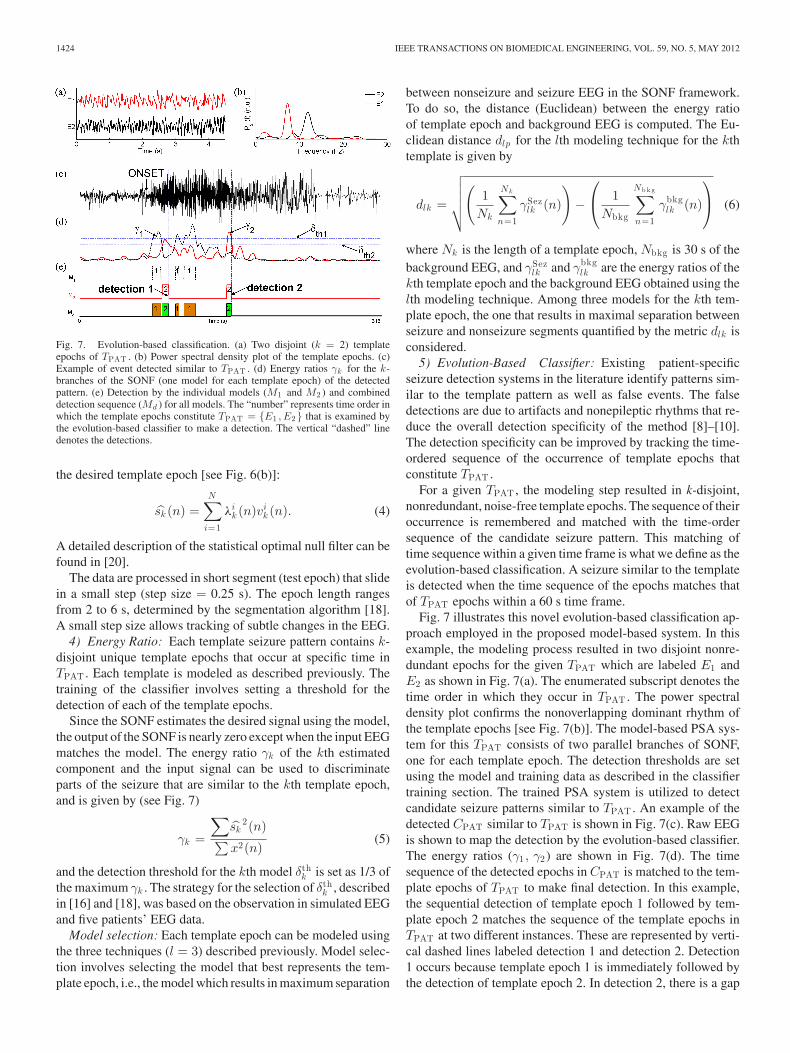
Fig. 7. Evolution-based classification. (a) Two disjoint (k = 2) templateepochs of TPAT . (b) Power spectral density plot of the template epochs. (c)Example of event detected similar to TPAT . (d) Energy ratios γk for the k-branches of the SONF (one model for each template epoch) of the detectedpattern. (e) Detection by the individual models (M1 and M2 ) and combineddetection sequence (Md ) for all models. The “number” represents time order inwhich the template epochs constitute TPAT = {E1 , E2} that is examined bythe evolution-based classifier to make a detection. The vertical “dashed” linedenotes the detections.
the desired template epoch [see Fig. 6(b)]:
sk (n) =N∑
i=1
λik (n)vi
k (n). (4)
A detailed description of the statistical optimal null filter can befound in [20].
The data are processed in short segment (test epoch) that slidein a small step (step size = 0.25 s). The epoch length rangesfrom 2 to 6 s, determined by the segmentation algorithm [18].A small step size allows tracking of subtle changes in the EEG.
4) Energy Ratio: Each template seizure pattern contains k-disjoint unique template epochs that occur at specific time inTPAT . Each template is modeled as described previously. Thetraining of the classifier involves setting a threshold for thedetection of each of the template epochs.
Since the SONF estimates the desired signal using the model,the output of the SONF is nearly zero except when the input EEGmatches the model. The energy ratio γk of the kth estimatedcomponent and the input signal can be used to discriminateparts of the seizure that are similar to the kth template epoch,and is given by (see Fig. 7)
γk =
∑sk
2(n)∑
x2(n)(5)
and the detection threshold for the kth model δthk is set as 1/3 of
the maximum γk . The strategy for the selection of δthk , described
in [16] and [18], was based on the observation in simulated EEGand five patients’ EEG data.
Model selection: Each template epoch can be modeled usingthe three techniques (l = 3) described previously. Model selec-tion involves selecting the model that best represents the tem-plate epoch, i.e., the model which results in maximum separation
between nonseizure and seizure EEG in the SONF framework.To do so, the distance (Euclidean) between the energy ratioof template epoch and background EEG is computed. The Eu-clidean distance dlp for the lth modeling technique for the kthtemplate is given by
dlk =
√√√√√(
1Nk
Nk∑
n=1
γSezlk (n)
)−
⎛
⎝ 1Nbkg
Nb k g∑
n=1
γbkglk (n)
⎞
⎠ (6)
where Nk is the length of a template epoch, Nbkg is 30 s of thebackground EEG, and γSez
lk and γbkglk are the energy ratios of the
kth template epoch and the background EEG obtained using thelth modeling technique. Among three models for the kth tem-plate epoch, the one that results in maximal separation betweenseizure and nonseizure segments quantified by the metric dlk isconsidered.
5) Evolution-Based Classifier: Existing patient-specificseizure detection systems in the literature identify patterns sim-ilar to the template pattern as well as false events. The falsedetections are due to artifacts and nonepileptic rhythms that re-duce the overall detection specificity of the method [8]–[10].The detection specificity can be improved by tracking the time-ordered sequence of the occurrence of template epochs thatconstitute TPAT .
For a given TPAT , the modeling step resulted in k-disjoint,nonredundant, noise-free template epochs. The sequence of theiroccurrence is remembered and matched with the time-ordersequence of the candidate seizure pattern. This matching oftime sequence within a given time frame is what we define as theevolution-based classification. A seizure similar to the templateis detected when the time sequence of the epochs matches thatof TPAT epochs within a 60 s time frame.
Fig. 7 illustrates this novel evolution-based classification ap-proach employed in the proposed model-based system. In thisexample, the modeling process resulted in two disjoint nonre-dundant epochs for the given TPAT which are labeled E1 andE2 as shown in Fig. 7(a). The enumerated subscript denotes thetime order in which they occur in TPAT . The power spectraldensity plot confirms the nonoverlapping dominant rhythm ofthe template epochs [see Fig. 7(b)]. The model-based PSA sys-tem for this TPAT consists of two parallel branches of SONF,one for each template epoch. The detection thresholds are setusing the model and training data as described in the classifiertraining section. The trained PSA system is utilized to detectcandidate seizure patterns similar to TPAT . An example of thedetected CPAT similar to TPAT is shown in Fig. 7(c). Raw EEGis shown to map the detection by the evolution-based classifier.The energy ratios (γ1 , γ2) are shown in Fig. 7(d). The timesequence of the detected epochs in CPAT is matched to the tem-plate epochs of TPAT to make final detection. In this example,the sequential detection of template epoch 1 followed by tem-plate epoch 2 matches the sequence of the template epochs inTPAT at two different instances. These are represented by verti-cal dashed lines labeled detection 1 and detection 2. Detection1 occurs because template epoch 1 is immediately followed bythe detection of template epoch 2. In detection 2, there is a gap
YADAV et al.: MODEL-BASED SEIZURE DETECTION FOR INTRACRANIAL EEG RECORDINGS 1425
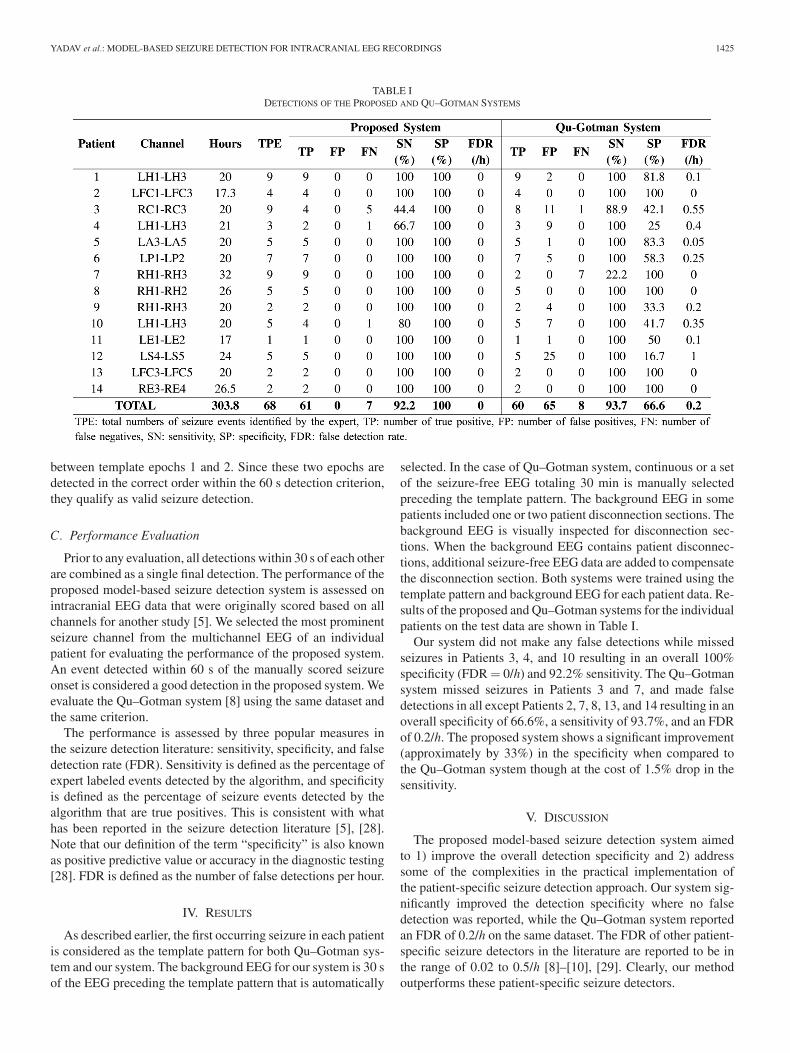
TABLE IDETECTIONS OF THE PROPOSED AND QU–GOTMAN SYSTEMS
between template epochs 1 and 2. Since these two epochs aredetected in the correct order within the 60 s detection criterion,they qualify as valid seizure detection.
C. Performance Evaluation
Prior to any evaluation, all detections within 30 s of each otherare combined as a single final detection. The performance of theproposed model-based seizure detection system is assessed onintracranial EEG data that were originally scored based on allchannels for another study [5]. We selected the most prominentseizure channel from the multichannel EEG of an individualpatient for evaluating the performance of the proposed system.An event detected within 60 s of the manually scored seizureonset is considered a good detection in the proposed system. Weevaluate the Qu–Gotman system [8] using the same dataset andthe same criterion.
The performance is assessed by three popular measures inthe seizure detection literature: sensitivity, specificity, and falsedetection rate (FDR). Sensitivity is defined as the percentage ofexpert labeled events detected by the algorithm, and specificityis defined as the percentage of seizure events detected by thealgorithm that are true positives. This is consistent with whathas been reported in the seizure detection literature [5], [28].Note that our definition of the term “specificity” is also knownas positive predictive value or accuracy in the diagnostic testing[28]. FDR is defined as the number of false detections per hour.
IV. RESULTS
As described earlier, the first occurring seizure in each patientis considered as the template pattern for both Qu–Gotman sys-tem and our system. The background EEG for our system is 30 sof the EEG preceding the template pattern that is automatically
selected. In the case of Qu–Gotman system, continuous or a setof the seizure-free EEG totaling 30 min is manually selectedpreceding the template pattern. The background EEG in somepatients included one or two patient disconnection sections. Thebackground EEG is visually inspected for disconnection sec-tions. When the background EEG contains patient disconnec-tions, additional seizure-free EEG data are added to compensatethe disconnection section. Both systems were trained using thetemplate pattern and background EEG for each patient data. Re-sults of the proposed and Qu–Gotman systems for the individualpatients on the test data are shown in Table I.
Our system did not make any false detections while missedseizures in Patients 3, 4, and 10 resulting in an overall 100%specificity (FDR = 0/h) and 92.2% sensitivity. The Qu–Gotmansystem missed seizures in Patients 3 and 7, and made falsedetections in all except Patients 2, 7, 8, 13, and 14 resulting in anoverall specificity of 66.6%, a sensitivity of 93.7%, and an FDRof 0.2/h. The proposed system shows a significant improvement(approximately by 33%) in the specificity when compared tothe Qu–Gotman system though at the cost of 1.5% drop in thesensitivity.
V. DISCUSSION
The proposed model-based seizure detection system aimedto 1) improve the overall detection specificity and 2) addresssome of the complexities in the practical implementation ofthe patient-specific seizure detection approach. Our system sig-nificantly improved the detection specificity where no falsedetection was reported, while the Qu–Gotman system reportedan FDR of 0.2/h on the same dataset. The FDR of other patient-specific seizure detectors in the literature are reported to be inthe range of 0.02 to 0.5/h [8]–[10], [29]. Clearly, our methodoutperforms these patient-specific seizure detectors.

1426 IEEE TRANSACTIONS ON BIOMEDICAL ENGINEERING, VOL. 59, NO. 5, MAY 2012
Fig. 8. Template pattern and a missed seizure by the proposed model-basedseizure detection system in Patient 3 (channels: RC1–RC3).
Although the patient-specific seizure detectors show im-proved sensitivity and FDR over the generic methods, theyare not practical. The main limiting factors are 1) selectionof the template seizure pattern; 2) selection of the backgroundEEG; and 3) supervised training of the classifier. We overcomethese challenges in the patient-specific seizure detection ap-proach by using a novel model-based scheme with the SONFsas the building blocks. The SONF is a simplified implemen-tation of the Kalman filter and can track narrowband signalsburied in noise [20], [21]. The idea is to detect short-durationdominant rhythms of the seizure for which SONFs becomepractical. Adaptive modeling and unsupervised classifier train-ing are some of the key attributes of this new system. Unlikethe multiresolution-based detectors, our system is not limited bythe sampling rate. Additionally, seizures with minimal changein the EEG amplitude are reported to be generally very diffi-cult to detect by experts as well automatic seizure detectors.The proposed method is capable of detecting such seizures. Westudied the proposed system’s ability to detect low-amplitudeseizures using simulated data in [17]. Patient 7 is one such ex-ample that had very low amplitude seizures, and low amplitudeis one possible reason for missing seizures in this patient by thecomparison system.
The proposed system resulted in no false detections whilemissing five out of nine seizures in Patient 3, one out of threeseizures in Patient 4, and one out of five seizures in Patient10. An example of the template pattern and a missed seizureby the proposed system for Patient 3 (channels: RC1–RC3)is shown in Fig. 8. The initial few seconds of the templatepattern contains the mixed frequency characteristics (4–34 s)that later evolve into rhythmic activity. The missed seizure issimilar to the mixed seizure part of the template seizure in theinitial few seconds (6–20 s), but did not continue to evolve intothe rhythmic part. On careful examination of the four derivedtemplate epochs for these patient data, it is observed that thefirst template epoch corresponded to the mixed frequency part,while the other three template epochs came from the rhythmicpart of the template pattern (TPAT ). The proposed system is
designed to detect seizures when the candidate seizures matchthe time-ordered occurrence of the template epochs in TPAT .All missed seizures of this patient did not meet this criterion.Clearly, the missed seizure does not match the template seizure.
Since the first 20 s of all seizures in this patient were verysimilar, we tested the idea of using only the first 20 s of thetemplate pattern to build the seizure model. However, this wasnot successful as a minimum of two disjoint template epochscould not be found. Our method is designed to detect seizuresevolving with sustained dominant rhythms. Therefore, it is not asurprise that the seizures that do not evolve with sustained dom-inant rhythms were not detected. In contrast, the Qu–Gotmansystem detected majority of the seizures for this patient but at thecost of 11 false detections. Similarly, the missed seizure in bothPatients 4 and 10 did not match the evolution pattern similar tothe template seizure pattern. The Qu–Gotman system detectedall seizures in Patient 4 at the cost of several false detectionsresulting in 100% sensitivity and at the cost of much lower speci-ficity (25%). The Qu–Gotman system detected all seizures inPatient 10 with no false detection. On the other hand, the Qu–Gotman system missed seven out of nine seizures in Patient 7while our system detected all of them with no FDs. The likelycause for missing seizures in this patient is the very low EEGamplitude. Additionally, the missed seizures by the Qu–Gotmansystem did not evolve similarly to the multichannel templateseizure within first 20 s. The epileptic discharge propagationthrough the brain structures may not be precisely reproduciblephenomena at all the times [13], [30]. The seizures can go un-detected by the Qu–Gotman system due to spatial and temporalconstraints which require the seizure onsets to occur in thesame channel as those of the template seizure [8]. An exampleof training data and a missed seizure by the Qu–Gotman systemis shown in Fig. 9. Clearly, in this example, the test seizure inchannels other than RH1–RH3 was of low amplitude and didnot evolve in the same manner as the template seizure. Sincethere are no spatial constraints in our system, it was capable ofdetecting low amplitude seizures.
Majority of false detections made by the Qu–Gotman sys-tem were brief rhythmic bursts (<4–6 s). These short rhythmicdischarge did not evolve similarly to the template seizure pat-tern, and hence was not detected by our system, resulting insignificantly improved detection specificity.
Isolating precisely reproducible phenomena in EEG signalsremains a difficult task and is vitally important to highlightpossible pathways of the epileptic discharge propagation [13],[30]. It is anticipated that there are typically one, two (andsometimes more) types of seizures in each patient. The aimof the proposed method is to detect a seizure that matches thetemplate seizure. If it is known that different brain structuresmay be involved at different times in the seizure generation,then it will be necessary to have the knowledge of each type ofseizure. In a single-channel configuration, this can be achievedby presenting an example of each type of seizure to build amodel, and detect subsequent similar seizures in the remainingdata.
The reproducibility of electrographic seizures as recordedintracerebrally may not always hold true [13], [30]. Patient 3

YADAV et al.: MODEL-BASED SEIZURE DETECTION FOR INTRACRANIAL EEG RECORDINGS 1427
Fig. 9. Example of the 20 s of template seizure pattern (a) and a missed seizure by the comparison system that was detected by the proposed system.
(see Fig. 8) is an example of this where several missed seizuresdid not evolve similarly to the template seizure on the selectedchannel. Seizures in this patient would still have not been de-tected even on the inclusion of multichannel information. How-ever, we observed variable seizure patterns evolving on otherchannels in some patients. If other channels are considered (aswould be done in a practical implementation of the method),variable seizures would certainly have been detected. One pos-sible extension of the current approach to multichannel scenariocan be developed by 1) finding the template epochs across theselected channels; 2) removing the redundant epochs; 3) findspatiotemporal sequence; and 4) then looking for similar se-quence in the remaining data. A match to one of the temporalsequences of variable seizures would certainly get detected inone of the channels, thereby improving the detection sensitivityof the method. This is considered as part of future work.
In general, the nonstationary, nonlinear, and chaotic nature ofthe EEG signals makes their analysis challenging. Thus, the firststep in the analysis of EEG signals typically involves automaticdecomposition of the EEG into stationary or quasi-stationarysegments, which has been a continuing subject of research formany years and has resulted in several application-specific seg-mentation techniques. A detailed description of some of the pop-ular EEG segmentation techniques can be found in [30]–[33].We have developed a new adaptive segmentation techniquebased on the STFT to facilitate unsupervised modeling. Thissegmentation technique works well for long rhythmic seizures.However, as with other systems, our system too has limitations.The limitation is in the modeling of nonrhythmic mixed fre-quency seizures and short-duration seizures as it fails to detectthese kinds of seizures.
The extension of the proposed method for the scalp EEGwould require inclusion of additional artifact management.This is because the scalp EEG is generally affected by ar-tifacts to a greater degree than the intracranial EEG. Sincethe proposed method examines the sequential occurrences ofspecific rhythmic discharges, rhythmic artifact may not be aproblem as it will not satisfy the stringent criterion of the se-quential occurrences. However, movement, electro-oculogram,electrocardiogram, and electromyogram artifacts must be re-moved to ensure that components representing EEG activity arepreserved [34].
VI. CONCLUSION
We present a novel fully automated patient-specific seizuredetection method that is based on the idea that epileptic seizuresof one or more types tend to recur within each patient. Piece-wise sustained rhythms of each seizure type are modeled fromthe a priori known template seizure pattern. Resulting modelformulates the required kernel for the SONF to detect similarseizures in subsequent EEG recordings. The process of buildinga dedicated seizure detection method for each seizure type (tem-plate seizure) is fully automated. We assessed the performanceof the detection on 14 patient recordings and showed sensitivitygreater than 92% without any false detections. Comparison toone of the seminal patient-specific seizure detection methods,on the same data, showed greatly improved performance. Theseresults suggest that the proposed seizure detection method canbe a candidate for clinical use. The results are encouraging andwarrant a larger multicenter validation study for wide clinicaluse.
ACKNOWLEDGMENT
The authors would like to thank Stellate Systems, Montreal,Canada, for providing the intracerebral EEG data used in thisstudy.
REFERENCES
[1] J. Engel and T. A. Pedley, Epilepsy: A Comprehensive Textbook.Baltimore, MD: Williams & Wilkins, Jan. 1998.
[2] F. H. Lopes da Silva and E. Niedermeyer, Electroencephalography: BasicPrinciples, Clinical Applications, and Related Fields. Baltimore, MD:Williams & Wilkins, 2005.
[3] T. Dua, H. M. de Boer, L. L. Prilipko, and S. Saxena, “Epilepsy care in theworld: Results of an ILAE/IBE/WHO global campaign against epilepsysurvey,” Epilepsia, vol. 47, pp. 1225–1231, Jul. 2006.
[4] R. Meier, H. Dittrich, A. Schulze-Bonhage, and A. Aertsen, “Detectingepileptic seizures in long-term human EEG: A new approach to automaticonline and real-time detection and classification of polymorphic seizurepatterns.,” J. Clin. Neurophysiol., vol. 25, pp. 119–131, Jun. 2008.
[5] S. Grewal and J. Gotman, “An automatic warning system for epilepticseizures recorded on intracerebral EEGs,” Clin. Neurophysiol., vol. 116,no. 10, pp. 2460–2472, 2005.
[6] S. B. Wilson, M. L. Scheuer, C. Plummer, B. Young, and S. Pacia, “Seizuredetection: Correlation of human experts,” Clin. Neurophysiol., vol. 114,no. 11, pp. 2156–2164, 2003.
[7] J. Mitra, J. R. Glover, P. Y. Ktonas, A. T. Kumar, A. Mukherjee,N. B. Karayiannis, J. D. Frost, R. A. Hrachovy, and E. M. Mizrahi, “A mul-tistage system for the automated detection of epileptic seizures in neonatal

1428 IEEE TRANSACTIONS ON BIOMEDICAL ENGINEERING, VOL. 59, NO. 5, MAY 2012
electroencephalography,” J. Clin. Neurophysiol., vol. 26, pp. 218–226,Aug. 2009.
[8] H. Qu and J. Gotman, “A patient-specific algorithm for the detectionof seizure onset in long-term EEG monitoring: Possible use as a warn-ing device,” IEEE Trans. Biomed. Eng., vol. 44, no. 2, pp. 115–122,Feb. 1997.
[9] A. Shoeb, H. Edwards, J. Connolly, B. Bourgeois, S. T. Treves, and J.Guttag, “Patient-specific seizure onset detection,” Epilepsy Behav., vol. 5,no. 4, pp. 483–498, 2004.
[10] A. S. Zandi, M. Javidan, G. A. Dumont, and R. Tafreshi, “Automatedreal-time epileptic seizure detection in scalp EEG recordings using analgorithm based on wavelet packet transform,” IEEE Trans. Biomed.Eng., vol. 57, no. 7, pp. 1639–1651, 2010.
[11] S. B. Wilson, M. L. Scheuer, R. G. Emerson, and A. J. Gabor, “Seizure de-tection: Evaluation of the reveal algorithm,” Clin. Neurophysiol., vol. 115,pp. 2280–2291, Oct. 2004.
[12] S. B. Wilson, “A neural network method for automatic and incrementallearning applied to patient-dependent seizure detection,” Clin. Neuro-physiol., vol. 116, pp. 1785–1795, Aug. 2005.
[13] F. Wendling, J.-J. Bellanger, J.-M. Badier, and J.-L. Coatrieux, “Extrac-tion of spatio-temporal signatures from depth EEG seizure signals basedon objective matching in warped vectorial observations,” IEEE Trans.Biomed. Eng., vol. 43, no. 10, pp. 990–1000, Oct. 1996.
[14] F. Wendling, M. B. Shamsollahi, J. M. Badier, and J. J. Bellanger, “Time-frequency matching of warped depth-EEG seizure observations,” IEEETrans. Biomed. Eng., vol. 46, no. 5, pp. 601–605, May 1999.
[15] D. Cosandier-Rimele, J.-M. Badier, P. Chauvel, and F. Wendling, “Aphysiologically plausible spatio-temporal model for EEG signals recordedwith intracerebral electrodes in human partial epilepsy,” IEEE Trans.Biomed. Eng., vol. 54, no. 3, pp. 380–388, Mar. 2007.
[16] L. Shi, R. Agarwal, and M. N. S. Swamy, “Model-based seizure detectionmethod using statistically optimal filters,” in Proc. IEEE Eng. Med. Biol.Soc. Conf., 2004, vol. 1, pp. 45–48.
[17] R. Yadav, R. Agarwal, and M. N. S. Swamy, “A new improved model-based seizure detection using statistically optimal null filter,” in Proc.IEEE Eng. Med. Biol. Soc. Conf., 2009, pp. 1318–1322.
[18] R. Yadav, R. Agarwal, and M. N. S. Swamy, “STFT-based segmentation inmodel-based seizure detection,” in Proc. IEEE Can. Conf. Electr. Comput.Eng., 2007, pp. 729–732.
[19] J. Gotman, “Automatic detection of seizures and spikes,” Clin. Neuro-physiol., vol. 16, no. 2, pp. 130–40, 1999.
[20] R. Agarwal, E. I. Plotkin, and M. N. S. Swamy, “Statistically optimal nullfilter based on instantaneous matched processing,” Circuits, Syst., SignalProcess., vol. 20, no. 1, pp. 37–61, 2001.
[21] R. Agarwal, E. I. Plotkin, and M. N. S. Swamy, “Statistically optimal nullfilters: Kalman equivalence,” in Proc. IEEE Int. Conf. Acoust., Speech,Signal Process., 2000, vol. 1, pp. 173–176.
[22] B. W. McMenamin, A. J. Shackman, L. L. Greischar, and R. J.Davidson, “Electromyogenic artifacts and electroencephalographic infer-ences revisited,” Neuroimage, vol. 54, pp. 4–9, Aug. 2010.
[23] M. E. Saab and J. Gotman, “A system to detect the onset of epilepticseizures in scalp EEG,” Clin. Neurophysiol., vol. 116, no. 2, pp. 427–442,2005.
[24] R. Agarwal, E. I. Plotkin, and M. N. S. Swamy, “Statistically optimal nullfilters for processing short record length signals,” in Proc. IEEE Int. Symp.Circuits Syst., 1995, vol. 3, pp. 2277–2280.
[25] R. Agarwal, E. I. Plotkin, and M. N. S. Swamy, “Recursive implementationof statistically-optimal null filters,” in Proc. IEEE Int. Symp. Circuits Syst.,1996, vol. 2, pp. 245–248.
[26] B. G. Amidan, T. A. Ferryman, and S. K. Cooley, “Data outlier detec-tion using the Chebyshev theorem,” in Proc. IEEE Aerosp. Conf., 2005,pp. 3814–3819.
[27] S. M. Haas, M. G. Frei, and I. Osorio, “Strategies for adapting automatedseizure detection algorithms,” Med. Eng. Phys., vol. 29, no. 8, pp. 895–909, 2007.
[28] T. Pietila, S. Vapaakoski, U. Nousiainen, A. Varri, H. Frey, V. Hakkinen,and Y. Neuvo, “Evaluation of a computerized system for recognition ofepileptic activity during long-term EEG recording,” Electroenceph. Clin.Neurophysiol., vol. 90, no. 6, pp. 438–443, 1994.
[29] G. R. Minasyan, J. B. Chatten, M. J. Chatten, and R. N. Harner, “Patient-specific early seizure detection from scalp electroencephalogram,” J. Clin.Neurophysiol., vol. 27, pp. 163–178, Jun. 2010.
[30] F. Wendling, J. M. Badier, P. Chauvel, and J. L. Coatrieux, “A methodto quantify invariant information in depth-recorded epileptic seizures,”Electroenceph. Clin. Neurophysiol., vol. 102, no. 6, pp. 472–85, 1997.
[31] R. Agarwal, J. Gotman, D. Flanagan, and B. Rosenblatt, “Automatic EEGanalysis during long-term monitoring in the ICU,” Electroenceph. Clin.Neurophysiol., vol. 107, no. 1, pp. 44–58, 1998.
[32] N. Amir and I. Gath, “Segmentation of EEG during sleep using time-varying autoregressive modeling,” Biol. Cybern., vol. 61, no. 6, pp. 447–455, 1989.
[33] J. S. Barlow, “Methods of analysis of nonstationary EEGs, with emphasison segmentation techniques: A comparative review,” J. Clin. Neurophys-iol., vol. 2, pp. 267–304, Jul. 1985.
[34] P. LeVan, E. Urrestarazu, and J. Gotman, “A system for automatic artifactremoval in ictal scalp EEG based on independent component analysis andBayesian classification,” Clin. Neurophysiol., vol. 117, pp. 912–927,Apr. 2006.
R. Yadav (S’04) received the B.Sc. degree in physicsand the M.Sc. degree in electronics both from theD.D.U. Gorakhpur University, Gorakhpur, India, in1998 and 2000, respectively. He is currently work-ing toward the Ph.D. degree in electrical engineeringfrom the Concordia University, Montreal, Canada.
He is also currently a Research Scientist at theLeap Medical Inc., Montreal. His research inter-ests include biomedical signal processing and pat-tern recognition with emphasis on their applicationto neural signals for critical care and neuroscience
research, and neural prosthesis.
M. N. S. Swamy (S’59–M’62–SM’74–F’80) re-ceived the B.Sc. (Hons.) degree in mathematicsfrom Mysore University, Mysore, India, in 1954, theDiploma degree in electrical communication engi-neering from the Indian Institute of Science, Ban-galore, India, in 1957, and the M.Sc. and Ph.D. de-grees in electrical engineering from the University ofSaskatchewan, Saskatoon, SK, Canada, in 1960 and1963, respectively.
He is currently a Research Professor and holder ofthe Tier I Chair in Signal Processing in the Depart-
ment of Electrical and Computer Engineering, Concordia University, Montreal,Canada, where he served as the Founding Chair of the Department of ElectricalEngineering from 1970 to 1977 and then as Dean of Engineering and ComputerScience from 1977 to 1993. He is the author or coauthor of over 300 journalarticles, six books and holds five patents. His research interests include audio,video, image, VLSI and biomedical signal processing.
Dr. Swamy is the recipient of many awards including the Education awardand the Guillemin best paper award given by the IEEE CAS Society. He servedas President of the IEEE_CAS Society in 2004, and as the E.I.C. of IEEE Trans.on Circuits and Systems-Part I during 2001–02.
R. Agarwal (M’88) received the M.A.Sc. and Ph.D.degrees both in electrical engineering from Concor-dia University, Montreal, Canada, in 1991 and 1995,respectively.
He is currently the Vice President of Researchand Development and Chief Technology Officer atLeap Medical Inc., Montreal, Canada, and is an Ad-junct Associate Professor at the Concordia Univer-sity. His research interests include biomedical signalprocessing (particularly pattern detection in the EEGof epileptic patients, analysis of polysomnograms,
ICU EEG monitoring, and evoked potentials), statistical signal processing, andsignal detection and estimation.