
Cranial particulate bone graft ossifies calvarial defects by osteogenesis
Upload
independentCategory
view
1download
0
Acta Neurochirurgica 78, 123-132 (1985) : A c t a . - 7 7 - - . Ndurochlrurglca �9 by Springer-Veflag 1985
Primary Cranial and Intracranial Chondrosarcoma A S u r v e y
M. Hassounah l, O. A1-Mefty 2, M. Akhtar 3, J. R. Jinkins 4, and J. L. Fox 2
1Division of Neurosurgery, The University of Alberta, Edmonton, Alberta, Canada, Departments of 2Neurosciences, 3 Pathology, and 4 Radiology, King Faisal Specialist Hospital and Research Centre, Riyadh, Saudi Arabia
Summary
Fifty cases of intracranial and cranial chondrosarcoma were reviewed in the world literature including two of our own. These were analyzed relevant to their histological subgroup, site of origin, age and sex incidence, calcification and vascularity, recurrence, and metastases. The analysis was done in order to clarify points in the diagnosis, management, and prognosis of this rare tumour. The mesenchymal subtype is a more malignant form with a higher tendency for recurrence, metastasis, and increased vascularity.
Keywords: Myxochondrosarcoma; mesenchymal chondrosar- coma; cranial tumour; infratemporal approach.
Introduction
O n l y 0 .16% o f all c ran ia l a n d i n t r a c r a n i a l les ions are
c a r t i l a g i n o u s t u m o u r s . C h o n d r o s a r c o m a cons t i t u t e s
a b o u t 14% o f these c h o n d r o m a t o u s t u m o u r s 6. M o r t 31
in 1899 r e p o r t e d one ear ly case o f i n t r a c r a n i a l m y x o -
c h o n d r o s a r c o m a . N o su rge ry was d o n e a t t ha t t ime,
a n d the p a t i e n t d ied s o m e years a f t e r the onse t o f
s y m p t o m s . L i c h t e n s t e i n a n d Be rns t e in 28 in 1959 in t ro -
d u c e d the t e r m m e s e n c h y m a l c h o n d r o s a r c o m a , dif-
f e r en t i a t i ng it h i s to log ica l ly f r o m o t h e r c h o n d r o m a t o u s
t u m o u r s .
W e su rveyed 48 cases o f p r i m a r y i n t r a c r a n i a l and
c ran ia l c h o n d r o s a r c o m a in the w o r l d l i t e r a tu re 2 - 3, 5, 6, 8, 9,11,12,15-18, 20- 22, 24, 25, 27 - 47 a n d desc r ibe two m o r e cases
o f p r i m a r y c ran i a l c h o n d r o s a r c o m a . C h o n d r o s a r c o m a
o r i g i n a t i n g f r o m the o rb i t a n d the p a r a n a s a l sinuses,
s e c o n d a r y m e t a s t a t i c c h o n d r o s a r c o m a , a n d c h o n d r o s -
a r c o m a s a s soc i a t ed wi th Ol l i e r ' s d isease o r M a f f u z z i ' s
s y n d r o m e are exc luded in these stat is t ics .
Illustrative Cases
Case 1. A 33-year-old female presented on February t6, 1983 with a 20 months' history of headache, pain behind the right ear, nausea
and vomiting. She had blurring of vision for four months. There was no history of head trauma. On physical examination she was awake, alert, and orientated. There was bilateral papilloedema. Hearing was normal in both ears. The rest of the cranial nerves were intact. There was some difficulty in doing tandem walking but no other cerebellar signs or nystagmus were present.
Skull X-rays showed a large calcified lesion in the right posterior fossa. Computed tomography (CT) of the head revealed a calcified posterior fossa mass on the right with invasion from the right temporal and occipital bones (Fig. 1). The mass was avascular on cerebral angiography. With a microsurgical technique gross total removal was obtained through combined posterior fossa and in- fratemporal approaches. The tumour, located extradurally, was attached to the dura.
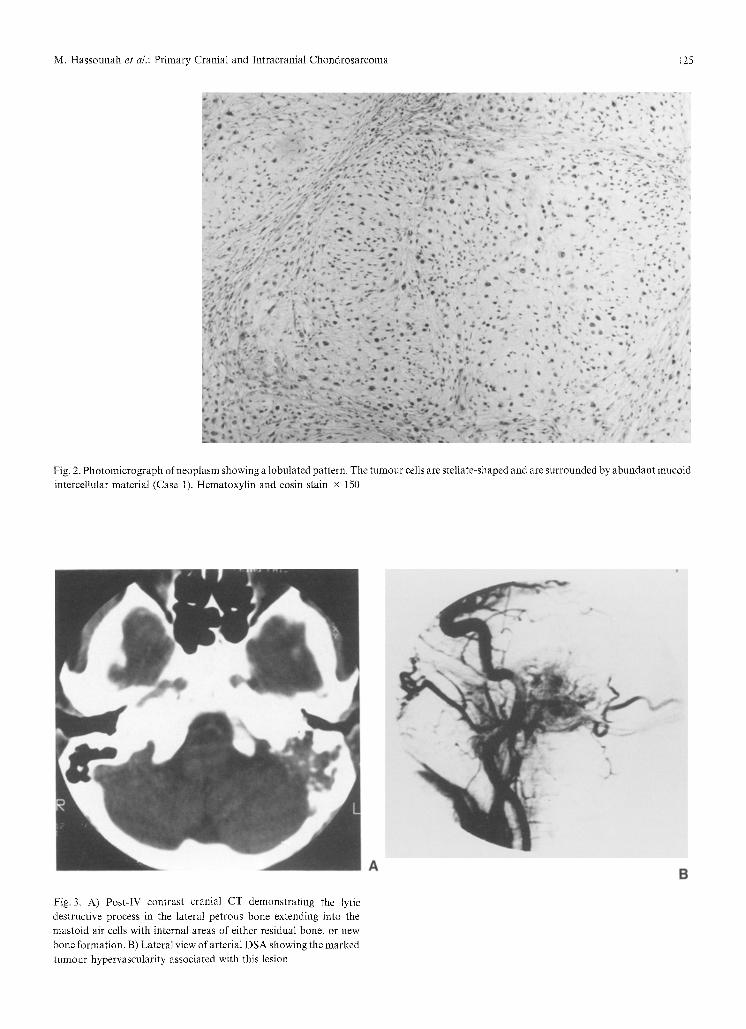
The tumour weighed 28 grams; measured approximately 5 x 4 x 3.5 cm; and consisted of soft, gelatinous, bluish and white tissue with occasional fragments of bone. Microscopically the tumour was composed of irregular and stellate-shaped cells with abundant myxoid stroma. The cytoplasm contained fine vacuolations and varied from scarcity to abundance. Nuclei, which were moderately hyperchromatic, were round to slightly irregular in shape and contained occasional mitotic figures. The neoplasm had a prominent lobular pattern (Fig. 2). Bony trabeculi were scattered within the tumour. The histological diagnosis was myxochondrosarcoma.
Postoperatively, a bone scan and metastatic workup failed to show extracranial involvement. The patient received 5,400 rads of high voltage X-radiation to the tumour bed. No further surgery or adjuvant chemotherapy was recommended. After three years the patient has shown no evidence of recurrence, clinically or radiologi- cally, and is quite well.
Case 2. A 65-year-old male, who had had a leftsided hearing loss and pain in the left ear for 5 years, underwent a left exploratory tympanotomy in another institution six weeks prior to his admission on June 13, 1984 at our hospital. The procedure was terminated because of profuse bleeding from the meatal incision. A tentative diagnosis of glomus jugulare tumour was made. There was no subsequent bleeding or otorrhea from the left ear, no pulsatile tinnitus, and no history of head trauma.
On examination there was a mass behind the left tympanic membrane. Audiometry revealed complete hearing loss in the left ear. The rest of the cranial nerves and neurological examinations were normal. Skull X-rays were normal. CT scan of the head demonstrated

124 M. Hassounah et al.: Primary Cranial and Intracraniai Chondrosarcoma
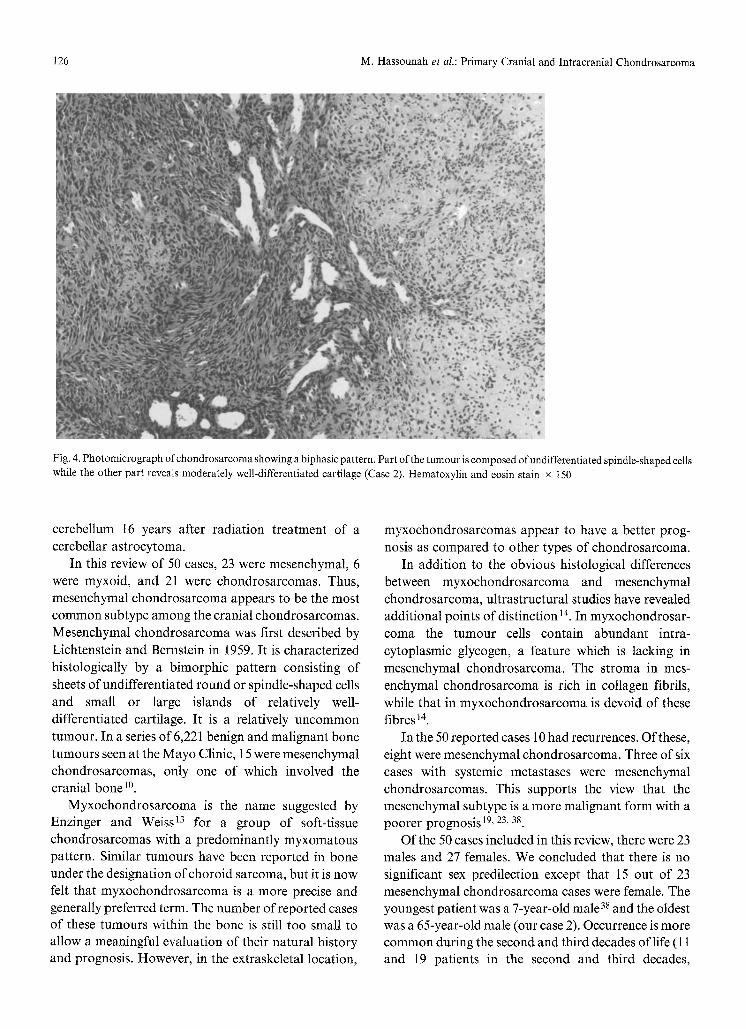
a large, enhancing lesion involving the left petrous pyramid and part of the mastoid bone and jugular foramen (Fig. 3A). Cerebral angiogram demonstrated a highly vascular tumour on the left at the base of the skull (Fig. 3B).
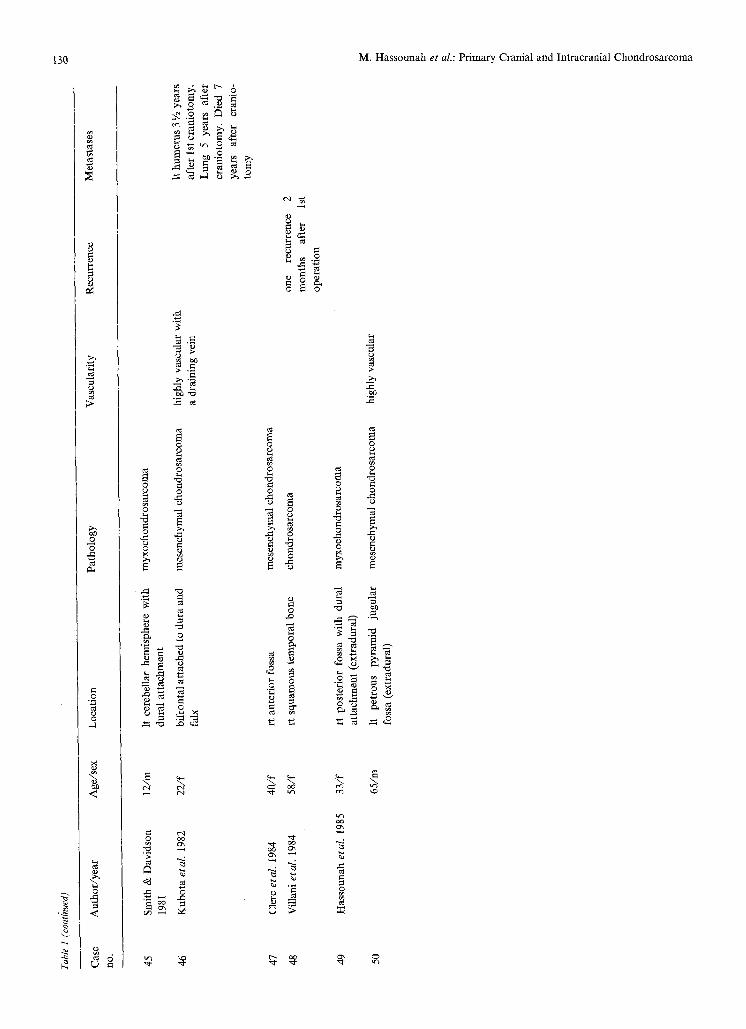
With microsurgical methods the tumour was totally removed through an infratemporal approach. The surgical specimen consisted of multiple fragments of bone, together measuring approximately 3 x 1 x 1 cm. Microscopic examination revealed bone extensively replaced by a malignant neoplasm containing a biphasic morpholog- ical pattern. Part of the tumour was composed of undifferentiated spindle-shaped cells with variable vascularity while other parts contained islands of moderately well-differentiated cartilaginous tissue (Fig. 4). The histological diagnosis was mesenchymal chondrosarcoma.
A metastatic workup done postoperatively failed to show any evidence of metastasis. Chemotherapy or radiation therapy was not recommended due to the low mitotic activity of the tnmour and because the tumonr was totally removed. Except for a partial facial paresis, the patient remains well 10 months after operation.
Discussion
Pr imary crania l and in t rac ran ia l c h o n d r o s a r c o m a is
a rare ma l ignan t neoplasm. The cl inical and pa tho log-
ical features o f 50 cases are summar ized in Tab. 1. The
exact site o f or igin in m a n y o f the cases is deba tab le
or unclear . I t appea r s tha t a b o u t ha l f o f the
c r an i a l / i n t r ac r an i a l c h o n d r o s a r c o m a s arise a long the
base o f the skull where the c h o n d r o c r a n i u m was fo rmed
f rom fusion o f a n u m b e r o f separa te cart i lages. Ossifi-
ca t ion occur red in la ter deve lopment . Bone des t ruc t ion
of ten seen by roen tgenog rams in this a rea also suggests
or igin f rom the chond roc ran ium.
Origin f rom a m e m b r a n o u s bone ( squamous por -
t ion o f the t e m p o r a l bone) was r epor t ed by Vil lani 44.
W h e n the tu rnou t has a t t a chmen t or invaded the falx,
t en tor ium, or dura l sinuses, the du ra is t hough t to be
the site o f origin. The meningea l f ibroblas ts which line
the undersur face o f the du ra and a r achno id were
t hough t by Alpers 1 to give rise to the car t i lag inous
tumours . In a rare case o f c h o n d r o s a r c o m a o f the
four th ventr icle descr ibed by Scot t 39, the tu rnou t was
pos tu l a t ed to have ar isen f rom the choro id plexus. This
ex t r a - ske le t a l or igin is best expla ined by the bel ief tha t
mesenchymal c h o n d r o s a r c o m a s arise f rom pr imi t ive
mul t i -po ten t i a l mesenchymal cells 14, 2s, 3s Bernstein
e t a l . 7 r epor ted a case o f c h o n d r o s a r c o m a o f the
Fig. 1. A) Lateral skull showing the irregular, ill-defined calcifica- tions overlying the posterior fossa. B) Axial section through the posterior fossa demonstrating the hypodense mass with internal areas of classic "popcorn" calcifications. C) Section at higher level again showing the typical calcifications within the hypodense tumour stroma
M. Hassounah et al.: Primary Cranial and Intracranial Chondrosarcoina 125
Fig. 2. Photomicrograph of neoplasm showing a lobulated pattern. The tumour cells are stellate-shaped and are surrounded by abundant mucoid intercellular material (Case 1). Hematoxylin and eosin stain x 150
Fig. 3. A) Post-IV contrast cranial CT demonstrating the lyric destructive process in the lateral petrous bone extending into the mastoid air cells with internal areas of either residual bone, or new bone formation. B) Lateral view of arterial DSA showing the marked tumour hypervascularity associated with this lesion
126 M. Hassounah e t al.: Primary Cranial and Intracranial Chondrosarcoma
Fig. 4. Photomicrograph of chondrosarcoma showing a biphasic pattern. Part of the tumour is composed of undifferentiated spindle-shaped cells while the other part reveals moderately well-differentiated cartilage (Case 2). Hematoxylin and eosin stain x 150
cerebellum 16 years after radiation treatment of a cerebellar astrocytoma.
In this review of 50 cases, 23 were mesenchymal, 6 were myxoid, and 21 were chondrosarcomas. Thus, mesenchymal chondrosarcoma appears to be the most common subtype among the cranial chondrosarcomas. Mesenchymal chondrosarcoma was first described by Lichtenstein and Bernstein in 1959. It is characterized histologically by a bimorphic pattern consisting of sheets of undifferentiated round or spindle-shaped cells and small or large islands of relatively well- differentiated cartilage. It is a relatively uncommon tumour. In a series of 6,221 benign and malignant bone tumours seen at the Mayo Clinic, 15 were mesenchymal chondrosarcomas, only one of which involved the cranial bone 10
Myxochondrosarcoma is the name suggested by Enzinger and Weiss 13 for a group of soft-tissue chondrosarcomas with a predominantly myxomatous pattern. Similar tumours have been reported in bone under the designation of choroid sarcoma, but it is now felt that myxochondrosarcoma is a more precise and generally preferred term. The number of reported cases of these tumours within the bone is still too small to allow a meaningful evaluation of their natural history and prognosis. However, in the extraskeletal location,
myxochondrosarcomas appear to have a better prog- nosis as compared to other types of chondrosarcoma.
In addition to the obvious histological differences between myxochondrosarcoma and mesenchymal chondrosarcoma, ultrastructural studies have revealed additional points of distinction 14. In myxochondrosar- coma the tumour cells contain abundant intra- cytoplasmic glycogen, a feature which is lacking in mesenchymal chondrosarcoma. The stroma in mes- enchymal chondrosarcoma is rich in collagen fibrils, while that in myxochondrosarcoma is devoid of these fibres 14.
In the 50 reported cases 10 had recurrences. Of these, eight were mesenchymal chondrosarcoma. Three of six cases with systemic metastases were mesenchymal chondrosarcomas. This supports the view that the mesenchymal subtype is a more malignant form with a poorer prognosis 19, 23, 38
Of the 50 cases included in this review, there were 23 males and 27 females. We concluded that there is no significant sex predilection except that 15 out of 23 mesenchymal ehondrosarcoma cases were female. The youngest patient was a 7-year-old male 38 and the oldest was a 65-year-old male (our case 2). Occurrence is more common during the second and third decades of life (11 and 19 patients in the second and third decades,

Tab
le 1
. P
rim
ary
Cra
nial
and
lnt
racr
ania
l C
hond
rosa
rcom
a
Cas
e A
utho
r/ye
ar
Age
/sex
L
ocat
ion
Pat
holo
gy
Vas
cula
rity
R
ecur
renc
e M
etas
tase
s n
o.
c)
1 M
ort
1899
28
/m
para
sell
ar
2 L
icht
enst
ein
22/f
pa
riet
al b
one
& B
erns
tein
195
9
3 D
ahli
n &
H
ende
rson
44
/f
1962
4 H
ardy
et a
L 19
66
42/f
5 R
aski
nd &
Gra
nt 1
966
48/1
6 B
erkm
en &
Bla
tt 1
968
26/f
7 M
inag
i &
New
ton
61/1
" 19
69
8 A
ndri
anja
tovo
et
aL
14/f
19
70
9 W
u &
Lap
i 19
70
18/t"
10
Sal
vado
r et
a[.
197i
24
/1'
11
17/f
12
Tak
ahas
hi e
tal.
19
71
47/f
13
Lee
dham
&
S
was
h 22
/m
1972
14
Roy
eta
].
1972
32
/m
rt p
arie
tal
sell
ar &
par
asel
lar
rt f
ront
al l
obe
rt f
ront
otem
poro
pari
etal
(e
xtra
dura
l)
para
sell
ar,
mid
fos
sa &
pe
trou
s ti
p
post
erio
r fo
ssa
atta
ched
to
du
ra (
subd
ural
)
It f
ront
opar
ieta
l ar
ea,
inva
d-
ing
dura
and
bon
e
skul
l
occi
put
it m
iddl
e &
po
ster
ior
foss
ae
(ext
radu
ral)
It p
etro
us b
one
rt p
arie
to-o
ccip
ital
att
ache
d to
te
ntor
ium
myx
ocho
ndro
sarc
oma
mes
ench
ymal
cho
ndro
sarc
oma
mes
ench
ymal
cho
ndro
sarc
oma
chon
dros
arco
ma
mes
ench
ymal
cho
ndro
sarc
oma
chon
dros
arco
ma
chon
dros
arco
ma,
w
ell-
diff
eren
- ti
ated
mes
ench
ymal
cho
ndro
sarc
oma
mes
ench
ymal
cho
ndro
sarc
oma
mes
ench
ymal
cho
ndro
sarc
oma
mes
ench
ymal
cho
ndro
sarc
oma
chon
dros
arco
ma
chon
dros
acro
ma
chon
dros
arco
ma
high
ly v
ascu
lar
4 re
curr
ence
s in
6
year
s
3 re
curr
ence
s,
died
ab
out
16
mon
ths
afte
r 1s
t op
erat
ion.
W
ith
each
su
bse-
qu
ent
rese
ctio
n th
e tu
mou
r ap
pear
ed
mor
e m
edul
lary
and
an
apla
stic
T 3
and
fem
oral
con
- dy
le
9 ye
ars
afte
r cr
anio
tom
y. D
ied
12
year
s af
ter
cran
io-
tom
y
spin
al c
ord
by C
SF
. L
ung
by
bloo
d st
ream
Q
9.
~w
�9
O 8 ~0

Tabl
e 1
(con
tinu
ed)
Cas
e A
utho
r/ye
ar
Age
/sex
L
ocat
ion
Pat
holo
gy
Vas
cula
rity
R
ecur
renc
e M
etas
tase
s
nO
.
15
Wag
a et
al.
197
2 51
/f
fron
topa
riet
al, i
nvad
ing
falx
&
chon
dros
arco
ma
tum
our
stai
n on
e re
curr
ence
2
rt
atri
um,
live
r,
both
sup
erio
r &
inf
erio
r sa
g-
mon
ths
afte
r op
era-
pa
ncre
as,
kidn
eys
&
itta
l si
nuse
s ti
on,
scar
im
plan
ta-
adre
nal.
D
ied
11
tion
and
met
asta
sis
mon
ths
afte
r op
era-
ti
on
16
Guc
cion
eta
l.
1973
19
/m
It p
arie
tal
regi
on a
ttac
hed
to
dura
17
Her
skow
itz
&
23/m
sp
heno
id b
one
& f
loor
of a
nte-
E1
Gam
maI
197
3 ri
or f
ossa
18
Lyn
ch &
Uri
buru
197
3 13
/m
rt f
ront
al w
ith
dura
l at
tach
- m
ent
19
Nau
fal
1973
, G
acek
27
/f
rt p
etro
us a
pex
1975
rt
mid
dle
& p
oste
rior
fos
sa
20
Set
h &
Sin
gh 1
973
32/m
rt
m
iddl
e cr
ania
l fo
ssa
(ext
radu
ral)
21
E1-
Gin
di e
tal.
19
74
23/m
It
tem
poro
pari
etal
wit
h du
ral
atta
chm
ent
22
Seh
acte
r et
al.
197
5 58
/m
It t
empo
ral
foss
a
23
23/m
rt
par
asel
lar
24
61/f
It
mid
dle
foss
a &
pet
rous
ape
x
25
Scot
t et
al.
19
76
39/m
fo
urth
ven
tric
le
26
Bah
r &
Gay
ler
1977
24
/m
rt C
P a
ngle
& j
ugul
ar f
ossa
(e
xtra
dura
l)
27
35/m
rt
pa
rasa
gitt
al,
atta
ched
to
sa
gitt
al s
inus
28
Alv
ira
& M
cLau
rin
21/f
It
fro
ntop
arie
tal
area
I9
78
Llo
yd 1
979
29
Cia
nfri
glia
eta
l.
1978
20
/t"
It m
iddl
e fo
ssa
(ext
radu
ral)
30
Sch
eith
auer
&
40/m
co
nvex
ity
wit
h du
ral
atta
ch-
Rub
inst
ein
i978
m
ent
mes
ench
ymal
cho
ndro
sarc
oma
chon
dros
arco
ma
mes
ench
ymal
cho
ndro
sarc
oma
myx
ocho
ndro
sarc
oma
mes
ench
ymal
cho
ndro
sarc
oma
chon
dros
arco
ma
chon
dros
arco
ma
chon
dros
arco
ma
ehon
dros
arco
ma
myx
ocho
ndro
sarc
oma
chon
dros
arco
ma
chon
dros
arco
ma
chon
dros
arco
ma,
low
gra
de
chon
dros
arco
ma
chon
dros
arco
ma
vasc
ular
high
ly v
ascu
lar
one
recu
rren
ce
in
one
year
one
recu
rren
ce,
22
mon
ths
afte
r op
era-
ti
on
It f
emur
& I
t pe
lvis
8
mon
ths
afte
r cr
anio
tom
y
m-*
o P~
o

31
32
33
34
35
36
37
38
39
40
41
42
43
44
Zuc
ker
& H
oro
up
ian
19
78
Rol
lo e
tal.
19
79
Her
os e
tal.
198
0
Kob
ayas
hi e
tal.
19
80
Gro
ssm
an &
Dav
is
1981
Gro
ssm
an &
Dav
is
1981
Sui
t et
al.
1982
Gro
ssm
an &
Dav
is
1981
Sui
t et
al.
1982
Gac
ek 1
975
Hos
hino
eta
l.
1981
17/f
7/m
I9/m
ll/m
26
/f
33/m
23/1
"
26
/f
ll/f
27/m
24/m
24/m
31/f
13/f
ante
rior
fo
ssa
wit
h du
ral
atta
chm
ent
rt
mid
fo
ssa
wit
h du
ral
atta
chm
ent
It
occi
pita
l,
atta
ched
to
su
peri
or
surf
ace
of
the
tent
oriu
m
It o
ccip
ital
lob
e an
d ce
rebe
l-
lum
, ari
ses
fro
m th
e te
ntor
ium
bila
tera
l fr
onto
pari
etal
, pa
ra-
sagi
ttal
It
sphe
noid
win
g w
ith
dura
l at
tach
men
t
rt
pari
etal
w
ith
dura
l at
tach
men
t
It
cere
bell
ar
hem
isph
ere,
no
dura
l at
tach
men
t
bipa
riet
al,
para
sagi
ttal
it p
aras
ella
r &
ret
rose
llar
rt
para
sell
ar
proj
ecti
ng
into
sp
heno
id s
inus
rt p
aras
ella
r
It p
etro
us b
on
e an
d po
ster
ior
foss
a
rt t
empo
ropa
riet
al
mes
ench
ymal
ch
on
dro
sarc
om
a
mes
ench
ymal
ch
on
dro
sarc
om
a
mes
ench
ymal
ch
on
dro
sarc
om
a re
sem
bles
AV
M
mes
ench
ymal
ch
on
dro
sarc
om
a va
scul
ar
mes
ench
ymal
ch
on
dro
sarc
om
a
mes
ench
ymal
ch
on
dro
sarc
om
a
mes
ench
ymal
ch
on
dro
sarc
om
a
mes
ench
ymal
ch
on
dro
sarc
om
a
mes
ench
ymal
ch
on
dro
sarc
om
a
cho
nd
rosa
rco
ma
cho
nd
rosa
rco
ma
cho
nd
rosa
rco
ma
my
xo
cho
nd
rosa
rco
ma,
low
gr
ade
mes
ench
ymal
ch
on
dro
sarc
om
a
rese
mbl
es A
VM
tum
ou
r st
ain
one
recu
rren
ce
3 ye
ars
afte
r op
era-
ti
on.
Die
d 7
year
s af
ter
oper
atio
n
one
recu
rreu
ce
6 m
on
ths
afte
r 1s
t op
erat
ion
2 re
curr
ence
s ov
er 3
ye
ars
2 re
curr
ence
s, a
t 13
&
16
year
s af
ter
1st
oper
atio
n.
Die
d 18
ye
ars
afte
r 1s
t op
erat
ion
supr
acla
vicu
lar
7 �8
9 ye
ars
afte
r I s
t op
erat
ion.
L 2
, 1 t
7th
ri
b, r
t ti
bia
8 �8
9 yea
rs
afte
r 1 s
t o
per
atio
n
o g~ g2
o g
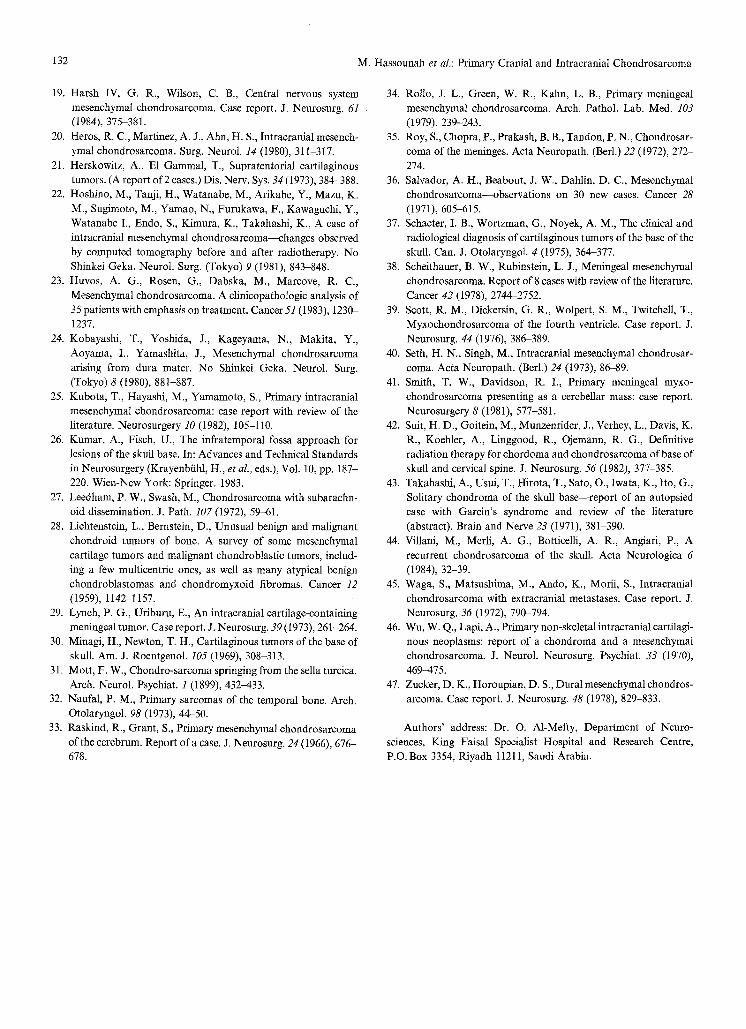
Tabl
e 1
(con
t&ue
d)
Cas
e 1
10
.
Aut
hor/
year
A
ge/s
ex
Loc
atio
n P
atho
logy
V
ascu
lari
ty
Rec
urre
nce
Met
asta
ses
45
46
47
48
49
50
Sm
ith
&D
avid
son
19
81
Kub
ota
etal
. 19
82
Cle
rc e
tal.
198
4
Vil
lani
eta
l. 1
984
Has
soun
ah e
tal.
19
85
12/m
22/f
40/f
58/f
33/f
65/m
It c
ereb
ella
r he
mis
pher
e w
ith
dura
l at
tach
men
t
bifr
onta
l att
ache
d to
dur
a an
d fa
lx
rt a
nter
ior
foss
a
rt s
quam
ous
tem
pora
l bo
ne
rt p
oste
rior
fos
sa w
ith
dura
l at
tach
men
t (e
xtra
dura
l)
It
petr
ous
pyra
mid
ju
gula
r fo
ssa
(ext
radu
ral)
myx
ocho
ndro
sarc
oma
mes
ench
ymal
cho
ndro
sarc
oma
mes
ench
ymal
cho
ndro
sarc
oma
chon
dros
arco
ma
myx
ocho
ndro
sarc
oma
mes
ench
ymal
cho
ndro
sarc
oma
high
ly v
ascu
lar
wit
h a
drai
ning
vei
n
high
ly v
ascu
lar
one
recu
rren
ce
2 m
onth
s af
ter
1st
oper
atio
n
It h
umer
us 3
~A y
ears
af
ter
1 st c
rani
otom
y.
Lun
g 5
year
s af
ter
cran
ioto
my.
D
ied
7 ye
ars
afte
r cr
anio
- to
my
O
g~
o

M. Hassounah et al.: Primary Cranial and Intracranial Chondrosarcoma 131
respectively). The dura t ion o f symptoms is usually long
and insiduous, the longest being 20 years 5.
Nineteen out o f 34 (56%) patients with reported
radiological studies showed some form of calcification
o f the tumour on skull X-ray or CT scan of the head.
C h o n d r o s a r c o m a ranges in vascularity f rom avascular
which is the more common, to a highly vascular
neoplasm (10 out o f 34 cases, or 29%). Eight out o f the
10 vascular neoplasms were mesenchymal types. Heros
etal . 2~ suggested preoperat ive radiat ion therapy or
embolizat ion in lesions so vascular they resemble
arter iovenous malformat ions .
There is a general agreement that radical resection is
the t reatment o f choice for chondrosa rcoma of the
cranium. When the tumour is localized in the temporal
bone, the infra temporal approach described by K u m a r and Fisch 26 is quite useful. Adjunct radiotherapy and
chemotherapy could be added. The beneficial effect of
radiat ion therapy has been occasionally documented by
compar ing CT scans before and after treatment: a 26%
reduct ion in the volume o f the tumour and an increased
density (approaching that o f bone) o f the entire t umour has been reported 22. Minagi and Newton 3~ also de-
scribed extensive, coarse calcification following radia- t ion therapy. Suit e ta l . 42 achieved local control with
p ro ton beam therapy in some cases. Harsh and Wilson 19 concluded that i rradiat ion and chemotherapy
should be considered even when patients have a long disease-free period after radical excision. Huvos et al. 23
noted there appeared to be a histological subtype o f
mesenchymal chondrosa rcoma which is characterized
by undifferentiated, small cells and which responds to a
combina t ion o f chemotherapy and irradiation.
Twenty percent o f the cases have shown evidence o f recurrence 2 months to 13 years after the first opera-
tion. One patient survived two recurrences in 18 years, this being the longest reported survival o f a patient
with chondrosa rcoma 24. Extracranial metastasis o f
chondrosa rcoma occurred in 12% of the 50 cases reviewed. The blood stream is the main route. A m o n g
the six cases whose neoplasms metastasized four
tumours were vascular and two tumours were of u n k n o w n vascularity. There was no relationship be-
tween metastasis and dural sinus a t tachment o f the
pr imary tumour . There is some correlat ion between the frequency of mitotic figures and the likelihood of recurrence and metastasis 38. Finally, according to
Arlen e ta l . 4, chondrosa rcomas of the head and neck
occur in younger patients and their growth pat tern is less aggressive in compar i son with those o f the peri-
pheral chondrosarcomas .
Acknowledgement
The authors would like to acknowledge Ms. Virginia D. Lacson for her secretarial assistance in the preparation of this manuscript.
References
1. Alpers, B. J., Cerebral osteochondroma of dural origin. Ann. Surg. 101 (1935), 27-37.
2. Alvira, M. M., McLaurin, R. L., Asymptomatic subdural chondrosarcoma. Case report. J. Neurosurg. 48 (1978), 825-828.
3. Andrianjatovo, J., Semette, D., Maspetiol, R., Nystagmus de type central. Premier signe r6v~lateur d'un chondrosarcome du trou occipital. Ann. Oto-Laryng. (Paris) 87 (1970), 279-286.
4. Arlen, M., Tollefsen, H. R., Huvos, A. G., Marcove, R. C., Chondrosarcoma of the head and neck. Am. J. Surg. 120 (1970), 456-460.
5. Bahr, A. L., Gayler, B. W., Cranial ehondrosarcomas. Report of four cases and review of the literature. Radiology 124 (1977), 151-156.
6. Berkmen, Y. M., Blatt, E. S., Cranial and intracrania! cartilagi- nous tumours. Clin. Radiol. 19 (1968), 327 333.
7. Bernstein, M., Perrin, R. G., Platts, M. E., Simpson, W. J., Radiaton-induced cerebellar chondrosarcoma. Case report. J. Neurosurg. 61 (1984), i74-177.
8. Cianfriglia, F., Pompili, A., Occhipinti, E., Intracranial malign- ant cartilaginous tumours. Report of two cases and review of literature. Acta Neurochir. (Wien) 45 (1978), 163-175.
9. Clerc, D., R6my, Ph., Salli6re, D., Mikol, J., Georges, B., Bisson, M., Massias, P., Ost6omalacie vitamino-r6sistante, syndrome de fanconi et chondrosarcome m6senchymateux m~ning6. Revue du Rhumatisme 51 (1984), 101-104.
10. Dahlin, D. C., Mesenchymal chondrosarcomas. In: Bone Tumors. GeneraI Aspects and Data on 6,221 Cases, Third ed., pp. 218-225. Springfield, Ill.: Ch. C Thomas. 1978.
11. Dahlin, D. C., Henderson, E. D., Mesenchymal chondrosar- coma. Further observations on a new entity. Cancer 15 (1962), 410-417.
12. E1-Gindi, S., Abd-E1-Hafeez, M., Salama, M., Extracranial skeletal metastases from an intracranial meningeal chondrosar- coma. Case report. J. Neurosurg. 40 (1974), 651-653.
13. Enzinger, F. M., Weiss, S. W., Extraskeletal myxoid chondrosar- coma. In: Soft Tissue Tumors, pp. 705-712. St. Louis-Toronto- London: C.V. Mosby Co. 1983.
14. Fu, Y. S., Kay, S., A comparative ultrastructural study of mesenchymal chondrosarcoma and myxoid chondrosarcoma. Cancer 33 (1974), 1531-1542.
15. Gacek, R. R., Diagnosis and management of primary tumors of the petrous apex. Ann. Otol. Rhinol. Laryngol. 84 (1975), 1-20.
16. Grossman, R. I., Davis, K. R., Cranial computed tomographic appearance of chondrosarcoma of the base of the skull. Radi- ology 141 (1981), 403M08.
17. Guccion, J. G., Font, R. L., Enzinger, F. M., Zimmerman, L. E., Extraskeletal mesenchymal chondrosarcoma. Arch. Pathol. 95 (1973), 336-340.
18. Hardy, J., Bertrand, C., Maltais, R., Robert, F., Thierry, A., Volumineux chondro-sarcome calcifi6 de la r~gion sellaire. Ex~r6se trans-sph~no]/dale sous contrSle radioscopique t61gvis& Neuro-Chirurgie (Paris) 12 (1966), 491-502.
132 M. Hassounah et al.: Primary Cranial and Intracranial Chondrosarcoma
19. Harsh IV, G. R., Wilson, C. B., Central nervous system mesenchymal chondrosarcoma. Case report. J. Neurosurg. 61 (1984), 375-381.
20. Heros, R. C., Martinez, A. J., Alan, H. S., Intracranial mesench- ymal chondrosarcoma. Surg. Neurol. 14 (1980), 311-317.
21. Herskowitz, A., E1 Gammal, T., Supratentorial cartilaginous tumors. (A report of 2 cases.) Dis. Nerv. Sys. 34 (1973), 384-388.
22. Hoshino, M., Tanji, H., Watanabe, M., Arikabe, Y., Mazu, K. M., Sugimoto, M., Yamao, N., Furukawa, F., Kawaguchi, Y., Watanabe I., Endo, S., Kimura, K., Takahashi, K., A case of intracranial mesenchymal chondrosarcoma---changes observed by computed tomography before and after radiotherapy. No Shinkei Geka. Neurol. Surg. (Tokyo) 9 (1981), 843-848.
23. Huvos, A. G., Rosen, G., Dabska, M., Marcove, R. C., Mesenchymal chondrosarcoma. A clinicopathologic analysis of 35 patients with emphasis on treatment. Cancer 51 (I 983), 1230- 1237.
24. Kobayashi, T., Yoshida, J., Kageyama, N., Makita, Y., Aoyama, I., Yamashita, J., Mesenchymal chondrosarcoma arising from dura mater. No Shinkei Geka. Neurol. Surg. (Tokyo) 8 (1980), 881-887.
25. Kubota, T., Hayashi, M., Yamamoto, S., Primary intracranial mesenchymal chondrosarcoma: case report with review of the literature. Neurosurgery 10 (1982), 105-110.
26. Kumar, A., Fisch, U., The infratemporal fossa approach for lesions of the skull base. In: Advances and Technical Standards in Neurosurgery (Krayenbfihl, H., et al., eds.), Vol. 10, pp. 187- 220. Wien-New York: Springer. 1983.
27. Leedham, P. W., Swash, M., Chondrosarcoma with subarachn- oid dissemination. J. Path. 107 (1972), 59-61.
28. Lichtenstein, L., Bernstein, D., Unusual benign and malignant chondroid tumors of bone. A survey of some mesenchymal cartilage tumors and malignant chondroblastic tumors, includ- ing a few multicentric ones, as well as many atypical benign chondroblastomas and chondromyxoid fibromas. Cancer 12
(1959), 1142-1157. 29. Lynch, P. G., Uriburu, E., An intracranial cartilage-containing
meningeal tumor. Case report. J. Neurosurg. 39 (1973), 261-264. 30. Minagi, H., Newton, T. H., Cartilaginous tumors of the base of
skull. Am. J. Roentgenol. 105 (1969), 308-313. 31. Mott, F. W., Chondro-sarcoma springing from the sella turcica.
Arch. Neurol. Psychiat. I (1899), 432-433. 32. Naufal, P. M., Primary sarcomas of the temporal bone. Arch.
Otolaryngol. 98 (1973), 44-50. 33. Raskind, R., Grant, S., Primary mesenchymal chondrosarcoma
of the cerebrum. Report of a case. J. Neurosurg. 24 (1966), 676- 678.
34. Rollo, J. L., Green, W. R., Kahn, L. B., Primary meningeal mesenchymal chondrosarcoma. Arch. Pathol. Lab. Med. 103
(1979), 239-243. 35. Roy, S., Chopra, P., Prakash, B. B., Tandon, P. N., Chondrosar-
coma of the meninges. Acta Neuropath. (Berl.) 22 (1972), 272- 274.
36. Salvador, A. H., Beabout, J. W., Dahlin, D. C., Mesenchymal chondrosarcoma--observations on 30 new cases. Cancer 28 (1971), 605-615.
37. Schacter, I. B., Wortzman, G., Noyek, A. M., The clinical and radiological diagnosis of cartilaginous tumors of the base of the skull. Can. J. Otolaryngol. 4 (1975), 364-377.
38. Scheithauer, B. W., Rubinstein, L. J., Meningeal mesenchymal chondrosarcoma. Report of 8 cases with review of the literature. Cancer 42 (1978), 2744-2752.
39. Scott, R. M., Dickersin, G. R., Wolpert, S. M., Twitchell, T., Myxochondrosarcoma of the fourth ventricle. Case report. J. Neurosurg, 44 (1976), 386-389.
40. Seth, H. N., Singh, M., Intracranial mesenchymal chondrosar- coma. Acta Neuropath. (Berl.) 24 (1973), 86-89.
41. Smith, T. W., Davidson, R. I., Primary meningeal myxo- chondrosarcoma presenting as a cerebellar mass: case report. Neurosurgery 8 (1981), 577-581.
42. Suit, H. D., Goitein, M., Munzenrider, J., Verhey, L., Davis, K. R., Koehler, A., Linggood, R., Ojemann, R. G., Definitive radiation therapy for chordoma and chondrosarcoma of base of skull and cervical spine. J. Neurosurg. 56 (1982), 377-385.
43. Takahashi, A., Usui, T., Hirota, T., Sato, O., Iwata, K., Ito, G., Solitary chondroma of the skull base--report of an autopsied case with Garcin's syndrome and review of the literature (abstract). Brain and Nerve 23 (1971), 381-390.
44. Villani, M., Merli, A. G., Botticelli, A. R., Angiari, P., A recurrent chondrosarcoma of the skull. Acta Neurologica 6 (1984), 32-39.
45. Waga, S., Matsushima, M., Ando, K., Morii, S., Intracranial chondrosarcoma with extracranial metastases. Case report. J. Neurosurg. 36 (1972), 790-794.
46. Wu, W. Q., Lapi, A., Primary non-skeletal intracranial cartilagi- nous neoplasms: report of a chondroma and a mesenchymal chondrosarcoma. J. Neurol. Neurosurg. Psychiat. 33 (1970), 469-475.
47. Zucker, D. K., Horoupian, D. S., Dural mesenchymal chondros- arcoma. Case report. J. Neurosurg. 48 (1978), 829-833.
Authors' address: Dr. O. A1-Mefty, Department of Neuro- sciences, King Faisal Specialist Hospital and Research Centre, P.O. Box 3354, Riyadh 11211, Saudi Arabia.
Copyright © 2022 FDOKUMEN




















