Minimal Access Cranial Suspension Lift: A Modified S-Lift
13
Cosmetic Minimal Access Cranial Suspension Lift: A Modified S-Lift Patrick Tonnard, M.D., Alexis Verpaele, M.D., Stan Monstrey, M.D., Ph.D., Koen Van Landuyt, M.D., Philippe Blondeel, M.D., Ph.D., Moustapha Hamdi, M.D., and Guido Matton, M.D. Gent, Belgium There is a strong trend at hand toward less dramatic facial rejuvenation surgery. Most of the authors’ patients want a cosmetic improvement but not at the cost of pro- longed disfigurement or a high risk of complications. In 1999, a very simple but effective rhytidectomy technique, termed an S-lift, was described in the literature and was adopted by the authors. Its basic principle is the suspen- sion of sagging facial features by a strong, permanent purse-string suture. The procedure is performed with the patient under local anesthesia. Significant modifications were applied to the incision, to the purse-string suture anchoring site, and to the direction and shape of the skin excision. The authors named the modified procedure the minimal access cranial suspension lift to specifically de- scribe the concept of the technique. Through an inverted L-shaped preauricular incision with extension below the sideburn, a limited skin undermining is performed. Two strong, permanent purse-string sutures are woven into the superficial musculoaponeurotic system tissues in a vertical U and an oblique O shape, initiating from a strong an- chorage in the deep temporal fascia at the level of the helical crus. Tying these sutures produces a very powerful vertical correction of descended facial features that acts mainly on the jowls and the upper neck. The procedure can be extended by continuing the dissection over the malar fat pad, placing a third vertical purse-string suture with strong action on the nasolabial groove, and vertically repositioning the midfacial volumes. During 20 months, pleasing results and a very low complication rate were obtained in 88 consecutive patients with a mean age of 55 1 /2 years. In this article, the authors provide a detailed description of the anesthetic and surgical technique, a demonstration of the results in different patient age cat- egories, and a discussion comparing the minimal access cranial suspension lift with other types of facial rejuvena- tion procedures. (Plast. Reconstr. Surg. 109: 2074, 2002.) Most patients consulting for facial rejuvena- tion have their own opinion about the desired result and the extent of the operation. This may be strongly different from the vision of the plastic surgeon, who may be inclined to pro- pose a comprehensive facial rejuvenation treat- ment. Most European patients want to look younger without evidence of their having had a face lift. Some patients refuse to have the plas- tic surgeon operate on their eyebrows or eye- lids. During consultation for facial rejuvena- tion, most patients demonstrate a maneuver that they have repeatedly performed in front of the mirror: they push the skin of the mandib- ular angle and the zygomatic region cranially (Fig. 1). To fulfill the wish of these patients, the S-lift, an operation that was originally pro- posed by Saylan, 1 has been redesigned. The term S-lift is confusing and refers only to the S-shaped skin pre-excision, which belongs to the originally described technique and which was abandoned by us because it was not surgi- cally sound. Therefore, we renamed the mod- ified procedure the minimal access cranial sus- pension lift (MACS lift) to specifically describe the concept of the technique. MATERIALS AND METHODS The MACS lift is performed as an outpatient procedure with the patient under local anes- thesia and minimal sedation. A total of 2.5 mg of midazolam is given intramuscularly before preparation and draping. This provides a com- fortable relaxation, without diminished con- sciousness. Tumescent infiltration with local anesthesia is provided with a 22-gauge spinal needle by using a diluted solution of 0.3% lidocaine, 1:650,000 adrenalin, and 2 mEq of sodium bicarbonate 2 (Table I). The same solu- tion is used for any ancillary procedure, such as liposuction of the submental region, upper or lower blepharoplasty, lipofilling, or laser resur- From the Coupure Centre for Plastic Surgery, Gent, the Department of Plastic and Reconstructive Surgery, University Hospital Gent, and the Coupure Centrum voor Plastische Chirurgie. Received for publication May 14, 2001; revised August 6, 2001. 2074
-
Upload
independent -
Category
Documents
-
view
3 -
download
0
Transcript of Minimal Access Cranial Suspension Lift: A Modified S-Lift

Cosmetic
Minimal Access Cranial Suspension Lift:A Modified S-LiftPatrick Tonnard, M.D., Alexis Verpaele, M.D., Stan Monstrey, M.D., Ph.D., Koen Van Landuyt, M.D.,Philippe Blondeel, M.D., Ph.D., Moustapha Hamdi, M.D., and Guido Matton, M.D.Gent, Belgium
There is a strong trend at hand toward less dramaticfacial rejuvenation surgery. Most of the authors’ patientswant a cosmetic improvement but not at the cost of pro-longed disfigurement or a high risk of complications. In1999, a very simple but effective rhytidectomy technique,termed an S-lift, was described in the literature and wasadopted by the authors. Its basic principle is the suspen-sion of sagging facial features by a strong, permanentpurse-string suture. The procedure is performed with thepatient under local anesthesia. Significant modificationswere applied to the incision, to the purse-string sutureanchoring site, and to the direction and shape of the skinexcision. The authors named the modified procedure theminimal access cranial suspension lift to specifically de-scribe the concept of the technique. Through an invertedL-shaped preauricular incision with extension below thesideburn, a limited skin undermining is performed. Twostrong, permanent purse-string sutures are woven into thesuperficial musculoaponeurotic system tissues in a verticalU and an oblique O shape, initiating from a strong an-chorage in the deep temporal fascia at the level of thehelical crus. Tying these sutures produces a very powerfulvertical correction of descended facial features that actsmainly on the jowls and the upper neck. The procedurecan be extended by continuing the dissection over themalar fat pad, placing a third vertical purse-string suturewith strong action on the nasolabial groove, and verticallyrepositioning the midfacial volumes. During 20 months,pleasing results and a very low complication rate wereobtained in 88 consecutive patients with a mean age of551⁄2 years. In this article, the authors provide a detaileddescription of the anesthetic and surgical technique, ademonstration of the results in different patient age cat-egories, and a discussion comparing the minimal accesscranial suspension lift with other types of facial rejuvena-tion procedures. (Plast. Reconstr. Surg. 109: 2074, 2002.)
Most patients consulting for facial rejuvena-tion have their own opinion about the desiredresult and the extent of the operation. Thismay be strongly different from the vision of theplastic surgeon, who may be inclined to pro-
pose a comprehensive facial rejuvenation treat-ment. Most European patients want to lookyounger without evidence of their having had aface lift. Some patients refuse to have the plas-tic surgeon operate on their eyebrows or eye-lids. During consultation for facial rejuvena-tion, most patients demonstrate a maneuverthat they have repeatedly performed in front ofthe mirror: they push the skin of the mandib-ular angle and the zygomatic region cranially(Fig. 1). To fulfill the wish of these patients,the S-lift, an operation that was originally pro-posed by Saylan,1 has been redesigned. Theterm S-lift is confusing and refers only to theS-shaped skin pre-excision, which belongs tothe originally described technique and whichwas abandoned by us because it was not surgi-cally sound. Therefore, we renamed the mod-ified procedure the minimal access cranial sus-pension lift (MACS lift) to specifically describethe concept of the technique.
MATERIALS AND METHODS
The MACS lift is performed as an outpatientprocedure with the patient under local anes-thesia and minimal sedation. A total of 2.5 mgof midazolam is given intramuscularly beforepreparation and draping. This provides a com-fortable relaxation, without diminished con-sciousness. Tumescent infiltration with localanesthesia is provided with a 22-gauge spinalneedle by using a diluted solution of 0.3%lidocaine, 1:650,000 adrenalin, and 2 mEq ofsodium bicarbonate2 (Table I). The same solu-tion is used for any ancillary procedure, such asliposuction of the submental region, upper orlower blepharoplasty, lipofilling, or laser resur-
From the Coupure Centre for Plastic Surgery, Gent, the Department of Plastic and Reconstructive Surgery, University Hospital Gent, and theCoupure Centrum voor Plastische Chirurgie. Received for publication May 14, 2001; revised August 6, 2001.
2074

facing of the central portion of the face. Whenperforming a MACS procedure separately, anaverage of 30 ml of this infiltration solution isused on each side of the face. At least 10 min-utes is allowed for adequate blanching of theinfiltrated skin. During this time, a closed-suction lipectomy of the submental area is per-formed in more than 95 percent of cases. Thisis done in the supraplatysmal plane with a2.5-mm spatula-tip cannula. Suction of the sub-platysmal region or the jowls is never per-formed. There are two types of MACS lifts: thesimple and the extended.
Simple MACS Lift
An inverted L-shaped preauricular incisionstarts at the most caudal end of the earlobe, is
directed upward, following the earlobe crease,crosses the incisura intertragica perpendicu-larly, makes a little indentation to go on thetragal rim, follows the anterior border of thehelical crus, further follows the hairline in thenon–hair-bearing recess in front of the ear,and then turns anteriorly along the inferiorlimit of the sideburn. A limited skin flap isundermined in an oval area extending from 1cm above the zygomatic arch to the mandibu-lar angle caudally and about 5 cm in the ante-rior direction (Fig. 2, left). Undermining of theskin flap is performed with face-lift scissors inthe spreading mode. Because of the tumescentinfiltration, a natural subcutaneous plane canbe found by simply spreading the scissors in aplane parallel to the skin. One centimeter infront of the anterior margin of the helical crusand 1 cm cranially to the zygomatic arch, anadditional injection of local anesthesia is givendown to the temporal bone. With pointed irisscissors in a spreading mode, the deep tempo-ral fascia is exposed over about 0.5 cm2, takingcare not to injure the superficial temporalvessels.
A first purse-string suture is made with 2-0Prolene monofilament on a big needle (V7
TABLE IAnesthetic Solution for Tumescent Infiltration in Minimal
Access Cranial Suspension Lift
100 ml of 0.9% sodium chloride solution20 ml of 2% lidocaine solution0.2 mg of adrenalin2 ml of 8.4% sodium bicarbonate
(0.3% lidocaine, adrenalin 1:650,000)
FIG. 1. (Left) Typical maneuver of patients between 40 and 50 years old in response to beingasked what they expect from a lifting procedure: They push the region of the mandibular anglecranially to correct the sagging in the lower third of the face. (Right) Typical maneuver of patientsolder than 50 years in reply to the same question: They push the region of the mandibular angleand the zygoma cranially to correct the sagging of the lower and middle third of the face.
Vol. 109, No. 6 / MINIMAL ACCESS CRANIAL SUSPENSION LIFT 2075

needle, Ethicon, Inc., Somerville, N.J.). Thefirst bite is taken deep down to the temporalbone (to be sure that the deep temporal fasciais included) in a craniocaudal direction (Fig. 2,right). The needle usually exits at the pretragalarea. The purse-string suture is continued in anarrow U-shape, first in a craniocaudal direc-tion, descending in front of the ear from thefirst bite down to the mandibular angle, mak-ing a U-turn, and returning 1 cm anteriorly ina parallel cranial direction to the startingpoint. A firm amount of parotid fascia in thecranial part and of platysma in the caudal partis taken with every bite of the needle. Thepurse-string suture is then tied under maxi-mum tension, exerting vertical traction on theplatysma, which causes strong elevation of thewhole anterior neck region. Seven knots aretied on this monofilament suture. The knot isburied in the soft tissue to prevent it frombeing visible or palpable through the skin.
A second purse-string suture is started at thesame point and is directed in an angle of about30 degrees anterior to the original verticalpurse string in a more open, oval shape tocorrect the jowling and the marionettegrooves. The suture is carried to the edge ofthe undermined area and then taken back tothe starting point (Fig. 2, right). After tying thissuture under maximum tension, a very effec-tive elevation of the jowls is seen. At this mo-ment, some dimpling will be seen at the limitsof the undermined skin, which is corrected by
freeing the retracted skin with scissors. Theexcess skin is redraped in a pure cranial direc-tion, marked, and resected. The skin is suturedunder strong vertical tension with five subcuta-neous sutures of 4-0 Vicryl. There is no tractionin the horizontal direction. The preauricularincision is sutured under minimal tension. Theearlobe, which is pulled cranially by puttingvertical tension on the skin flap, is simply setback without tension as a little transpositionflap. This avoids the risk of creating an unnat-ural, pulled-down earlobe.3 Sometimes a smalldog-ear will appear behind the earlobe. Toavoid a scar behind the ear, it is not resected.The patient is informed preoperatively aboutthe possibility of this small dog-ear and aboutits spontaneous disappearance within 2months. A small Penrose drain is inserted inthe lowest part of the incision at the earlobe,and a further closure of the skin is performedwith 5-0 Vicryl subcutaneously and with 5-0 and6-0 nylon continuous and interrupted skin su-tures. Ice cooling is applied for 2 hours afterthe procedure, and a light compressive dress-ing is left on for 1 day. The patient can leavethe office 2 hours after surgery. The dressingand Penrose drain are removed the next day,and the patient can shower and wash his or herface and hair from then on. During the first 24hours after surgery, patients are allowed to takelimited amounts of soft food together with oralantibiotics and pain medication (paraceta-mol). All patients are offered the opportunityof having daily facial lymphatic drainage mas-sage during one week, starting on postopera-tive day 4. All sutures are removed at day 7.
Extended MACS Lift
To enhance the effect on the nasolabialgroove and to lift the malar fat pad4 and themidface, the incision is extended along theanterior border of the temporal hairline (Fig.3, left). The subcutaneous undermining is ex-tended over the area of the malar fat pad anda third, narrow, U-shaped purse-string suture isplaced between the anterior part of the deeptemporal fascia and the malar fat pad (Fig. 3,right). By putting tension on this suture, anobvious flattening of the nasolabial groove andraising of the malar fat pad will result. Thismodification was designed in August of 2000.
A simple MACS lift is performed in approx-imately 11⁄2 hours. An extended MACS lift takes2 hours. Table II summarizes the modificationsmade to the originally described S-lift and the
FIG. 2. (Left) Preoperative marking of the preauricularand infracapillary incision (solid line) for the minimal accesscranial suspension lift. The dotted line indicates the extent ofundermining, and the arrow indicates the vector of traction.(Right) Minimal access cranial suspension lift. Position of thevertical, narrow purse-string suture and the 30-degreeoblique, wide purse-string suture on the nonunderminedsuperficial musculoaponeurotic system, with anchoring tothe deep temporal fascia. Sutures performed with 2-0Prolene.
2076 PLASTIC AND RECONSTRUCTIVE SURGERY, May 2002

similarities between it and the simple and ex-tended MACS lifts.
RESULTS
Between December of 1999 and June of2001, 88 MACS lifts were performed (81women, seven men). The mean age was 551⁄2years, ranging from 38 to 82 years (Figs. 4through 9). The simple MACS lift was per-formed on 54 patients, and the extendedMACS lift on 34 patients. All procedures wereperformed with the patient under local anes-thesia, with minimal sedation, and in an officesetting, except for four patients with a historyof medical disorders (hypertension, thrombo-embolic history). The operations for these fourpatients occurred with the patient under localanesthesia, with sedation given by an anesthe-siologist, and in a hospital setting. During thefirst 3 days, all patients experienced markedbut bearable pain in the temporal region and alimitation of mouth opening. This was proba-bly caused by the traction on the temporalfascia by the purse-string sutures. All patientsshowed a temporary swelling of the cranialportion of the sternocleidomastoid region thatdisappeared within 2 weeks. Most of the pa-tients were able to return to their normal ac-tivities 1 week after surgery with the help ofsome camouflaging makeup. On postoperativeday 14, all patients were able to go out withoutany makeup. Patients in whom an extendedMACS lift was performed showed a few more
days of swelling in the malar area. There wereno demands for surgical removal of dog-earsbehind the earlobe because they all disap-peared within 2 months after surgery. Patientsatisfaction was very high. In all patients, thedesired correction of the aging facial featureswas obtained and remained stable for the ex-tent of our follow-up. From a surgical point ofview, the short operating time, pleasing results,quick recovery period, and absolute absence ofmajor complications were considered very im-portant advantages of this procedure. Two he-matomas had to be evacuated: one at the endof the surgery and one 8 hours postoperatively,in a very active man who went to work imme-diately after surgery. The resulting scars wereinconspicuous. The effect of the surgery can beconsidered stable, as demonstrated in our pa-tient with the longest follow-up of 18 months(Fig. 9).
DISCUSSION
Facial aging is caused by a multitude of fac-tors: the years of gravitational pull on the softtissues between the skin and the facial skele-ton, loss of elasticity of the skin caused byintrinsic and extrinsic factors, possible facialdeflation caused by fat atrophy,5,6 or even bonyresorption.7,8 These different possibilities ex-plain the multitude of therapeutic approach-es.9–17 One can rejuvenate the skin by usingresurfacing techniques, lifting the sagged softtissues, augmenting deflated areas with autolo-gous or other materials, or combining differ-ent procedures. The MACS lift, as describedabove, is fundamentally a pure antigravita-tional lifting procedure that will suspend thesagging soft tissues of the face and neck, to-gether with the adhering skin, in a verticaldirection into the place where they previouslybelonged. When counseling candidates for fa-cial rejuvenation, most of them make a maneu-ver with the fingertips on the mandibular angleor the malar region, pushing the skin and thefacial soft tissues in an upward direction (Fig.1). Therefore, any technique that works in acaudocranial vertical direction will have a vi-sual anti-aging effect, whether it is a lateralremoval of the superficial musculoaponeuroticsystem (SMAS),12 a cranial suspension withpurse-string sutures,1 a subperiosteal open14 orendoscopic approach,9 or a deep-plane face-lifttechnique.16 In contrast to the most frequentlyproposed classic face lifts,10 which all have a
FIG. 3. (Left) Extended minimal access cranial suspensionlift. Preoperative marking of the preauricular and infracap-illary incision, which is extended along the temporal hairline,with supplementary undermining of the malar region anddifferent vectors of traction (arrows) on the midface soft tis-sues. (Right) Extended minimal access cranial suspension lift.Position of a third narrow purse-string suture, in addition tothe two purse-string sutures described in Figure 2, betweenthe anterior part of the deep temporal fascia and the malarfat pad.
Vol. 109, No. 6 / MINIMAL ACCESS CRANIAL SUSPENSION LIFT 2077

strong lateral vector of displacing soft tissues,the MACS lift is a pure vertical-vector face lift.
In recent years, the tendency has been to-ward less invasive techniques in facial rejuvena-tion surgery. Baker17 showed an evolution inhis face-lift techniques from extended classicdissections toward minimal incision techniquesand from a lateral pull to more cranially di-rected displacement of the soft tissues. Also,Finger18 proposed minimal skin and SMAS dis-sections, in combination with subperiostealmidface lifts, and demonstrated stable and nat-ural results with minimal postoperativemorbidity.
The ultimate determinant of a successfulrhytidectomy is a happy patient.17 Listening toour patients’ desires is essential to be able tofulfill them. Therefore, we believe the idealfacial rejuvenation procedure is an interven-tion with a visible but natural change, withminimal risks, minimal morbidity, and mini-mal social discomfort. Offering the MACS liftas a safe outpatient office procedure is wel-comed with great enthusiasm because of thestrong resistance to hospital admission of mostcosmetic surgery candidates and their reluc-tance to pay hospital expenses.
Subperiosteal procedures can produce dra-matic changes with beautiful long-term re-sults,9,14,15 but patients sometimes have swellingthat remains for 6 months. Also, by raising theperiosteum, tissue is moved to a position whereit has never been. Indeed, the periosteum isthe only anatomic structure that stays fixed tothe bone over an entire life. With the MACS
procedure, the sagging soft tissues are broughtback to their original position with a simplesuturing technique placed directly in the ptotictissue.
With Baker,17 we share the disappointmentabout the morbidity and the poor long-termresults of anterior corset platysmaplasty.19–21 Bypulling strongly on the lateral part of theplatysma at the mandibular angle in a cranialdirection, platysmal bands will disappear inmost cases. We limited our indications for an-terior platysmaplasty to the few cases in whichthe platysmal bands did not disappear withupward traction on the platysma in the regionof the mandibular angle. The combination ofmoderate-to-aggressive fine-needle liposuctionof the submental region with a strong cranialsuspension of the platysma and SMAS, as donein the MACS procedure, offers a simple andvaluable alternative.
In a classic face lift, the retroauricular andoccipital incision is used to create the posteriorpart of the skin flap. The traction on this flapin the oblique upward direction basically onlyredrapes skin and has little or no rejuvenatingeffect. Most of the skin resection in a classicface-lift design is done in the occipital region,producing the classic problems of hairline dis-placement or noticeable pretrichial scars, aproblem that was never encountered in ourpatient group.
The horizontal limb of the MACS-lift inci-sion enables us to excise a large amount offacial skin in a vertical direction without eleva-tion of the hairline.22–24 The extension of this
TABLE IIComparison of the Original S-Lift Technique with the Described Simple and Extended Minimal Access Cranial Suspension
(MACS) Lifts
S-Lift Simple MACS Lift Extended MACS Lift
Pre-excision of skin No pre-excision of skin No pre-excision of skinS-shaped skin incision, crossing the
non–hair-bearing skin at the helicalroot
Inverted L-shaped skin incisionfollowing lower border of sideburn
Inverted L-shaped skin incision followinglower border of sideburn and extendingalong anterior temporal hairline
Oval-shaped skin undermining Oval-shaped skin undermining Oval-shaped skin undermining withextension over malar fat pad
Vertical U-shaped and oblique O-shaped purse-string sutures onSMAS
Vertical U-shaped and oblique O-shaped purse-string sutures onSMAS
Vertical U-shaped and oblique O-shapedpurse-string sutures on SMAS and obliqueU-shaped purse-string suture betweenmalar fat pad and deep temporal fascia
Purse-string suture fixation toperiosteum of the zygomatic arch
Purse-string suture fixation to deeptemporal fascia
Purse-string suture fixation to deep temporalfascia
Skin redraping at 45-degree angle Customized skin excision afterredraping in vertical direction
Customized skin excision after redraping invertical direction
Skin redraping behind earlobe No skin incision behind earlobe No skin incision behind earlobeEffect on anterior neck and jowls Effect on anterior neck and jowls Effect on anterior neck, jowls, midface, and
nasolabial fold
SMAS, superficial musculoaponeurotic system.
2078 PLASTIC AND RECONSTRUCTIVE SURGERY, May 2002

incision in a pretrichial cephalic directionmakes action on the midface possible in theextended MACS lift. After meticulous closure
of this incision, very inconspicuous scars can beobtained.
The sagging of the midface can be treated
FIG. 4. (Above, left and right) Three-quarter and profile views of a 45-year-old woman withmoderate jowls and moderate central anterior neck skin laxity. No visible platysmal bands. (Below,left and right) One-year postoperative results, with correction of the jowls and neck laxity aftera simple minimal access cranial suspension procedure and minimal liposuction of the submentalarea.
Vol. 109, No. 6 / MINIMAL ACCESS CRANIAL SUSPENSION LIFT 2079

through different approaches. A lateral ap-proach was suggested by Hamra,16,25 Stuzin etal.,26 Owsley and Fiala,4 and Connell andSemlacher.27 Hester et al.28 described a morevertical approach through a lower eyelid inci-sion. A subperiosteal approach, introduced by
Tessier,14 was recently modified by Little.15
Byrd and Andochick29 used the endoscopethrough the temporal approach, and Yarem-chuk30 recently proposed a combination of dif-ferent approaches. Disappointed by the highcomplication rate of lower eyelid approaches28
FIG. 5. (Above, left and right) Three-quarter and profile views of a 56-year-old woman withmarked jowls, marionette grooves, and a heavy, fatty neck with clearly visible platysmal bands.(Below, left and right) Results 14 months after a simple minimal access cranial suspension lift withextended liposuction of the anterior neck and upper blepharoplasty. Note the correction of thejowls, marionette grooves, cervicomental angle, and the nice volumetric augmentation of thezygomatic region.
2080 PLASTIC AND RECONSTRUCTIVE SURGERY, May 2002
and the long recovery period of subperiostealmidface14,15,29 elevation, we decided to use thelateral approach. An extra U-shaped purse-string suture is placed between the anterior
part of the deep temporal fascia and the malarfat pad to lift the whole midface with anoblique to an almost vertical vector.
The debate between limited and extended
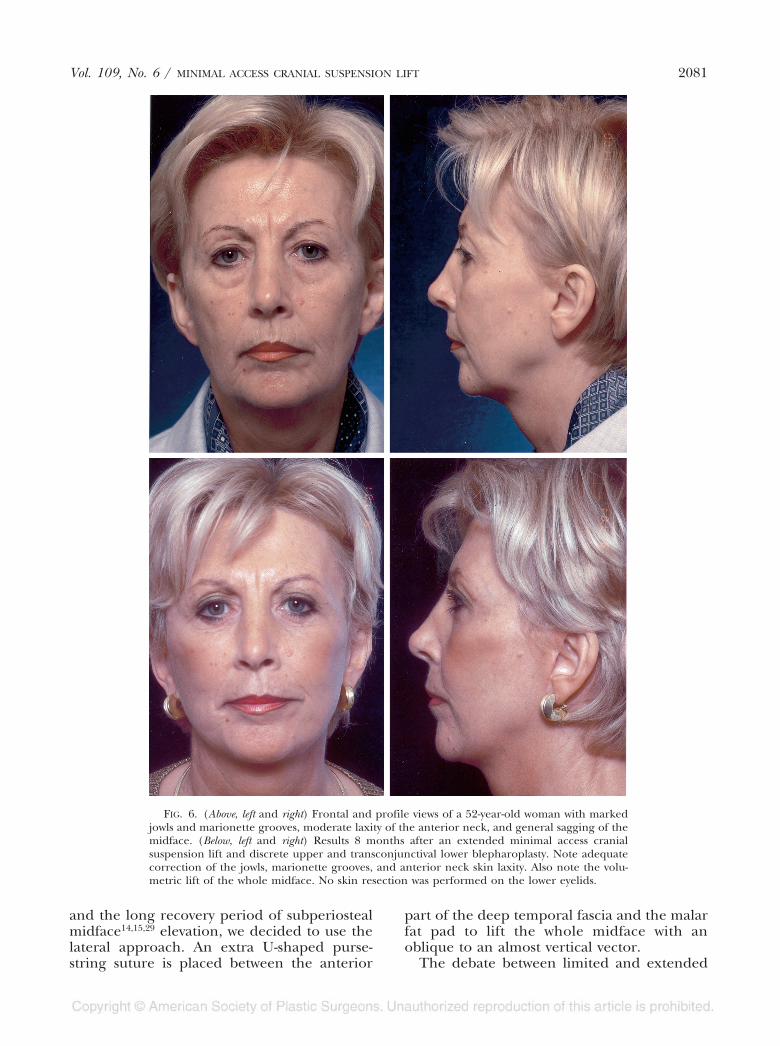
FIG. 6. (Above, left and right) Frontal and profile views of a 52-year-old woman with markedjowls and marionette grooves, moderate laxity of the anterior neck, and general sagging of themidface. (Below, left and right) Results 8 months after an extended minimal access cranialsuspension lift and discrete upper and transconjunctival lower blepharoplasty. Note adequatecorrection of the jowls, marionette grooves, and anterior neck skin laxity. Also note the volu-metric lift of the whole midface. No skin resection was performed on the lower eyelids.
Vol. 109, No. 6 / MINIMAL ACCESS CRANIAL SUSPENSION LIFT 2081

undermining of the facial skin is ongoing.Some authors are convinced that extensive un-dermining and radical skin resection leads tobetter and more long-lasting results.31 Beauti-
ful anatomic studies about the retaining liga-ments of the face have been published, to-gether with the statement that these ligamentsare to be divided to be able to resect more
FIG. 7. (Above, left and right) Three-quarter and profile views of a 60-year-old man with markedjowls, marionette grooves, laxity of the anterior neck skin with marked platysmal bands, andgeneral sagging of the midface. (Below, left and right) Results 11 months after extended minimalaccess cranial suspension lift and discrete upper blepharoplasty. Note adequate correction of thejowls, marionette grooves, and anterior neck skin laxity without platysmaplasty. There is a nicevolumetric rejuvenation of the midface area. No lower eyelid surgery was performed.
2082 PLASTIC AND RECONSTRUCTIVE SURGERY, May 2002

skin.32–34 But why should we transect the onlysupporting structures of the skin?
Concerning the stability of the results, werealize that 18 months of follow-up is short, butover that period the results have been as goodand as stable as in classic SMAS-lift techniques.
Because the original S-lift procedure as de-scribed by Saylan1 has some illogical stepsagainst elementary plastic surgery principles, alot of skepticism was raised about this interven-tion. Some surgeons compare this procedurewith a technique described in 1919 by Passot,35
FIG. 8. (Above, left and right) Frontal and three-quarter views of a 61-year-old woman with verymarked jowls, marionette grooves, laxity of the anterior neck skin with marked platysmal bands,general laxity of the facial skin, and excessive periorbital and lower eyelid rhytides. (Below, leftand right) Early postoperative results (4 months) after extended minimal access cranial suspen-sion lift, upper blepharoplasty, and erbium laser resurfacing of the perioral and lower eyelid area.Note the absence of erythema shortly after erbium resurfacing.
Vol. 109, No. 6 / MINIMAL ACCESS CRANIAL SUSPENSION LIFT 2083
merely consisting of an S-shaped excision ofpreauricular skin without any undermining,but the purse-string sutures do much morethan that.
The original Saylan S-lift design was modi-fied as follows. The S-shaped pre-excision of
skin was abandoned. First, one can never tellhow much skin must be removed at the end ofthe operation; second, after pre-excision ofskin, the surgeon is forced to manipulate andpull during the surgery on skin that will besutured at the end. Purse-string sutures are
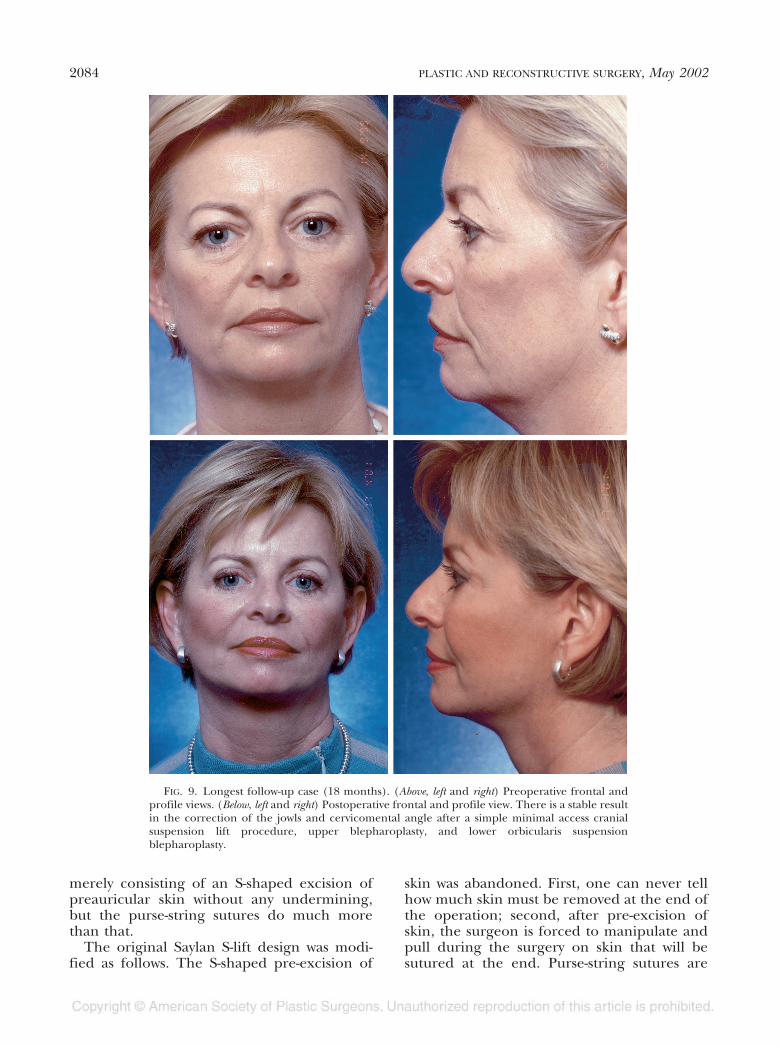
FIG. 9. Longest follow-up case (18 months). (Above, left and right) Preoperative frontal andprofile views. (Below, left and right) Postoperative frontal and profile view. There is a stable resultin the correction of the jowls and cervicomental angle after a simple minimal access cranialsuspension lift procedure, upper blepharoplasty, and lower orbicularis suspensionblepharoplasty.
2084 PLASTIC AND RECONSTRUCTIVE SURGERY, May 2002
anchored to the rigid deep temporal fasciarather than to the fragile periosteum of thezygomatic arch. Skin redraping is performed ina vertical direction instead of an oblique direc-tion at a 45-degree angle (Table II).
The advantages of a MACS lift comparedwith classical lifting techniques are a quick pro-cedure, local anesthesia, no hospital admis-sion, a short recovery period, and an inconspic-uous, short scar without raising of the temporalor occipital hairline. Perhaps most impor-tantly, it is a safe procedure.36,37 Facial nerveinjury and skin slough are unlikely to occur,and hematoma and postoperative numbnessare significantly reduced. Also, the combina-tion of centrofacial laser resurfacing and aMACS lift can be performed with great safety.38
Finally, the results seem to be very pleasing andnatural, eliminating the classic face-lift stigma-ta,3 thanks to the limited incision and emphasison vertical tissue displacement.
CONCLUSIONS
The original S-lift technique as described bySaylan1 has been modified by the authors intoa procedure that is called the MACS lift. Theprocedure is performed under local anesthe-sia, with minimal sedation, in an office-basedpractice. A simple MACS lift takes no longerthan 11⁄2 hours and mainly affects the lowerthird of the face. The extended MACS lift alsoaffects the middle third of the face and can beperformed in 2 hours. The core principle ofthe MACS procedure is putting strong, non-resorbable purse-string sutures on nonunder-mined SMAS and anchoring it to a fixed andrigid temporal fascia. This produces effectiveand stable elevation and traction on the SMASthat is transmitted to other regions in the face,such as the jowls, the malar fat pad, or thenasolabial grooves. Skin resection is principallydone in the temporal area after vertical trac-tion and redraping. Both procedures producehighly satisfactory results for the surgeon andfor the patient. The importance of this newtechnique is that it is essentially a vertical-vector face lift that works principally in anantigravitational direction.
Patrick L. Tonnard, M.D.Coupure Centre for Plastic SurgeryCoupure Rechts 164 C-DB-9000 [email protected]
REFERENCES
1. Saylan, Z. The S-lift: Less is more. Aesthetic Surg. J. 19:406, 1999.
2. Schoen, S. A., Taylor, C. O., and Owsley, T. G. Tumes-cent technique in cervicofacial rhytidectomy. J. OralMaxillofac. Surg. 52: 344, 1994.
3. Franco, T. Face-lift stigmas. Ann. Plast. Surg. 15: 379,1985.
4. Owsley, J. Q., and Fiala, T. G. Update: Lifting the malarfat pad for correction of prominent nasolabial folds.Plast. Reconstr. Surg. 100: 715, 1997.
5. Coleman, S. R. Facial recontouring with lipostructure.Clin. Plast. Surg. 24: 347, 1997.
6. Donofrio, L. M. Fat distribution: A morphologic studyof the aging face. Dermatol. Surg. 26: 1107, 2000.
7. Pessa, J. E. An algorithm of facial aging: Verification ofLambros’s theory by three-dimensional stereolithog-raphy, with reference to the pathogenesis of midfacialaging, scleral show, and lateral suborbital trough de-formity. Plast. Reconstr. Surg. 106: 479, 2000.
8. Pessa, J. E. The potential role of stereolithography inthe study of facial aging. Am. J. Orthod. DentofacialOrthop. 119: 117, 2001.
9. Ramirez, O. M., and Pozner, J. N. Subperiosteal mini-mally invasive laser endoscopic rhytidectomy: TheSMILE facelift. Aesthetic Plast. Surg. 20: 463, 1996.
10. Miller, T. A. Face lift: Which technique? Plast. Reconstr.Surg. 100: 501, 1997.
11. Baker, T. J., and Stuzin, J. M. Personal technique of facelifting. Plast. Reconstr. Surg. 100: 502, 1997.
12. Baker, D. C. Lateral SMASectomy. Plast. Reconstr. Surg.100: 509, 1997.
13. Owsley, J. Q. Face lift. Plast. Reconstr. Surg. 100: 514,1997.
14. Tessier, P. Subperiosteal face-lift. Ann. Chir. Plast. Esthet.34: 193, 1989.
15. Little, J. W. Three-dimensional rejuvenation of the mid-face: Volumetric resculpture by malar imbrication.Plast. Reconstr. Surg. 105: 267, 2000.
16. Hamra, S. T. Composite rhytidectomy. Plast. Reconstr.Surg. 90: 1, 1992.
17. Baker, D. C. Minimal incision rhytidectomy (short scarface lift) with lateral SMASectomy: Evolution and ap-plication. Aesthetic Surg. J. 21: 14, 2001.
18. Finger, E. R. A 5-year study of the transmalar subperi-osteal midface lift with minimal skin and superficialmusculoaponeurotic system dissection: A durable,natural-appearing lift with less surgery and recoverytime. Plast. Reconstr. Surg. 107: 1273, 2001.
19. Feldman, J. J. Corset platysmaplasty. Plast. Reconstr.Surg. 85: 333, 1990.
20. Knize, D. M. Limited incision submental lipectomy andplatysmaplasty. Plast. Reconstr. Surg. 101: 473, 1998.
21. Fuente del Campo, A. Midline platysma muscular over-lap for neck restoration. Plast. Reconstr. Surg. 102: 1710,1998.
22. Noël, A. La Chirurgie Esthétique: Son Rôle Social. Paris:Masson et Cie, 1926.
23. Rees, T. Aesthetic Plastic Surgery. Philadelphia: Saunders,1980.
24. Lewis, C.M. Preservation of the female sideburn. Aes-thetic Plast. Surg. 8: 91, 1984.
25. Hamra, S. T. The zygorbicular dissection in composite
Vol. 109, No. 6 / MINIMAL ACCESS CRANIAL SUSPENSION LIFT 2085

rhytidectomy: An ideal midface plane. Plast. Reconstr.Surg. 102: 1646, 1998.
26. Stuzin, J. M., Baker, T. J., Gordon, H. L., and Baker, T. M.Extended SMAS dissection as an approach to midfacerejuvenation. Clin. Plast. Surg. 22: 295, 1995.
27. Connell, B. F., and Semlacher, R. A. Contemporarydeep layer facial rejuvenation. Plast. Reconstr. Surg.100: 1513, 1997.
28. Hester, T. R., Codner, M. A., and McCord, C. D. The“centrofacial” approach for correction of facial agingusing the transblepharoplasty subperiosteal cheek-lift.Aesthetic Surg. Q. 16: 51, 1996.
29. Byrd, H. S., and Andochick, S. E. The deep temporallift: A multiplanar, lateral brow, temporal, and upperface lift. Plast. Reconstr. Surg. 97: 928, 1996.
30. Yaremchuk, M. J. Subperiosteal and full-thickness skinrhytidectomy. Plast. Reconstr. Surg. 107: 1045, 2001.
31. Pitman, G. H. Minimal incision rhytidectomy (shortscar face lift) with lateral SMASectomy: Evolution andapplication (Commentary). Aesthetic Surg. J. 21: 14,2001.
32. Furnas, D. W. The retaining ligaments of the cheek.Plast. Reconstr. Surg. 83: 11, 1989.
33. Furnas, D. W. Strategies for nasolabial levitation. Clin.Plast. Surg. 22: 265, 1995.
34. Stuzin, J. M., Baker, T. J., and Gordon, H. L. The re-lationship of the superficial and deep facial fascias:Relevance to rhytidectomy and aging. Plast. Reconstr.Surg. 89: 441, 1992.
35. Passot, R. La chirurgie esthétique des rides du visage.Presse Med. 27: 258, 1919.
36. Baker, D. C. Complications of cervicofacial rhytidec-tomy. Clin. Plast. Surg. 10: 543, 1983.
37. Matarasso, A., Elkwood, A., Rankin, M., and Elkowitz, M.National plastic surgery survey: Face lift techniquesand complications. Plast. Reconstr. Surg. 106: 1185,2000.
38. Fulton, J. E., Saylan, Z., Helton, P., Rahimi, A. D., andGolshani, M. The S-lift facelift featuring the U-su-ture and O-suture with skin resurfacing. Dermatol. Surg.27: 18, 2001.
2086 PLASTIC AND RECONSTRUCTIVE SURGERY, May 2002