
Giant cranial base tumours
6
Acta Neurochir (Wien) (1994) 129:121-126 =Acta Ncurochirurgica Springer-Verlag 1994 Printed in Austria Giant Cranial Base Tumours Sh. Pomeranz, F. Umansky, J. Elidan, E. Ashkenazi, A. Valarezo, and M. Shalit Departments of Neurosurgery and Otolaryngology, Hadassah University Hospital, Jerusalem, Israel Summary Thirty-three patients with giant (diameter/> 4.5 cm) cranial base tumours who underwent surgery at the Hadassah Hospital over the last ten years are described. Twenty-three of the patients had me- ningiomas, 4 neurinomas, one giant cell tumour, one haemangio- pericytoma, and 4 had malignant meningiomas. Four tumours were at the cerebellopontine angle, 9 within the anterior cranial fossa, 8 petroclival, 8 on middle fossa floor, and 4 along the sphenoid ridge. The average pre-operative symptom duration was 31 months, range 3 180 months. Nineteen patients had a radical tumour resection, 10 subtotal, and 4 a partial resection on an average 1.7 operations per patient. The mean follow-up period from the first operation was 39 months (range 2-120). There was no mortality peri-operatively or during the follow-up period. The mean pre-operative Karnofsky score was 68 and at the last follow-up 76. There was no correlation between histology and degree of resection, complications, or status at last follow-up. The best resections (92% radical) and outcome (mean Karnofsky 92) with the least number of operations (mean 1.4) were in the anterior fossa and along the sphenoid wing. The patients requiring the most operations (mean 2.1), having the smallest percentage of radical resections (25%) and the least favourable outcomes (mean Karnofsky 52) were those with petroclivai tumours. Patients with giant cranial base tumours have a good overall long-term prognosis, but especially those with petroclival tumours challenge us to improve our techniques. Keywords. Cerebellopontine angle; cranial base tumour; me- ningioma; neurinoma; microsurgery. Introduction The resection of cranial base tumours is a major surgical challenge due to the location of the tumours underneath the brain, their vicinity to critical structures such as the brain stem, cranial nerves, and cerebral vessels, and the problem of cerebrospinal fluid leakage following surgery. It is clear that of the cranial base tumours, those that are of giant dimensions increase the surgical difficulties, and more than one operation is often required for their resection. Sekhar 11 defined giant cranial base tumours as those with a "tumour equivalent diameter" of at least 4.5 cm, based on the maximal imaging (CT or MRI) diameter in each di- mension (X, Y, and Z) and the derived diameter being defined as (X x y x Z)l/3. Only singular publications have appeared describing giant cranial base tumours 2' 4, s, 10, 13, 14 and to the best of our knowledge, no large series describing such tu- mours has been published. This is in spite of the fact that certain cranial base tumours, such as olfactory groove meningiomas, typically attain extensive dimensions 6, 8. It is known that extensive highly-ma- lignant cranial base tumours have a poor prognosis 9, 12 In this report 33 patients with giant cranial base tumours, benign and of low-grade malignancy, who underwent surgery at the Hadassah Hospital over the last ten years, are described and analysed. Materials and Methods Approximately 420 patients with cranial base tumours who un- derwent surgery at the Hadassah Hospital neurosurgery department during the last ten years were reviewed and 33 patients with giant tumours (diameter above 4.5 cm, as defined by Sekhar ~) were found. Table 1. Location of Giant Base Tumours (Total of 33) Location No. of patients Anterior fossa, bilateral 9 Sphenoid wing 4 Middle fossa floor 8 Cerebellopontine angle 4 Petrous bone, petroclival, clival 8
-
Upload
independent -
Category
Documents
-
view
1 -
download
0
Transcript of Giant cranial base tumours

Acta Neurochir (Wien) (1994) 129:121-126 =Acta Ncurochirurgica �9 Springer-Verlag 1994 Printed in Austria
Giant Cranial Base Tumours
Sh. Pomeranz, F. Umansky, J. Elidan, E. Ashkenazi, A. Valarezo, and M. Shalit
Departments of Neurosurgery and Otolaryngology, Hadassah University Hospital, Jerusalem, Israel
Summary Thirty-three patients with giant (diameter/> 4.5 cm) cranial base
tumours who underwent surgery at the Hadassah Hospital over the last ten years are described. Twenty-three of the patients had me- ningiomas, 4 neurinomas, one giant cell tumour, one haemangio- pericytoma, and 4 had malignant meningiomas. Four tumours were at the cerebellopontine angle, 9 within the anterior cranial fossa, 8 petroclival, 8 on middle fossa floor, and 4 along the sphenoid ridge.
The average pre-operative symptom duration was 31 months, range 3 180 months.
Nineteen patients had a radical tumour resection, 10 subtotal, and 4 a partial resection on an average 1.7 operations per patient.
The mean follow-up period from the first operation was 39 months (range 2-120). There was no mortality peri-operatively or during the follow-up period. The mean pre-operative Karnofsky score was 68 and at the last follow-up 76. There was no correlation between histology and degree of resection, complications, or status at last follow-up.
The best resections (92% radical) and outcome (mean Karnofsky 92) with the least number of operations (mean 1.4) were in the anterior fossa and along the sphenoid wing. The patients requiring the most operations (mean 2.1), having the smallest percentage of radical resections (25%) and the least favourable outcomes (mean Karnofsky 52) were those with petroclivai tumours.
Patients with giant cranial base tumours have a good overall long-term prognosis, but especially those with petroclival tumours challenge us to improve our techniques.
Keywords. Cerebellopontine angle; cranial base tumour; me- ningioma; neurinoma; microsurgery.
Introduction
The resection of cranial base tumours is a major surgical challenge due to the location of the tumours underneath the brain, their vicinity to critical structures such as the brain stem, cranial nerves, and cerebral vessels, and the problem of cerebrospinal fluid leakage following surgery. It is clear that of the cranial base tumours, those that are of giant dimensions increase the surgical difficulties, and more than one operation
is often required for their resection. Sekhar 11 defined giant cranial base tumours as those with a " tumour equivalent diameter" of at least 4.5 cm, based on the maximal imaging (CT or MRI) diameter in each di- mension (X, Y, and Z) and the derived diameter being defined as (X x y x Z)l/3.
Only singular publications have appeared describing giant cranial base tumours 2' 4, s, 10, 13, 14 and to the best
of our knowledge, no large series describing such tu- mours has been published. This is in spite of the fact that certain cranial base tumours, such as olfactory groove meningiomas, typically attain extensive dimensions 6, 8. It is known that extensive highly-ma- lignant cranial base tumours have a poor prognosis 9, 12
In this report 33 patients with giant cranial base tumours, benign and of low-grade malignancy, who underwent surgery at the Hadassah Hospital over the last ten years, are described and analysed.
Materials and Methods
Approximately 420 patients with cranial base tumours who un- derwent surgery at the Hadassah Hospital neurosurgery department during the last ten years were reviewed and 33 patients with giant tumours (diameter above 4.5 cm, as defined by Sekhar ~) were found.
Table 1. Location of Giant Base Tumours (Total of 33)
Location No. of patients
Anterior fossa, bilateral 9 Sphenoid wing 4 Middle fossa floor 8 Cerebellopontine angle 4 Petrous bone, petroclival, clival 8
122 Sh. Pomeranz etal.: Giant Cranial Base Tumours
The primary initial clinical presentation of these tumours was an organo-mental syndrome in 10 patients, disequilibrium in 8, cranial nerve dysfunction in 8, and variations of hemiparesis in 7 patients.
The anatomical location of these tumours is presented in Table 1, showing a proportionate representation witin all three cranial fossas. There was a correlation between the tumour location and the primary symptoms: anterior fossa tumours primarily presented with an or- gano-mental syndrome and posterior fossa tumours largely presented with disequilibrium and/or cranial nerve deficits.
The mean Karnofsky functional score 7 (on a scale of 0-100, 70 = threshold of independent function with minimal assistance) of the patients was 68. The presenting symptom duration ranged from 3-180 months, the average being 31 months. The patients' ages ranged from 16 to 86, the mean being 52 years.
The evaluation of the patients included computerized tomog- raphy with thin slices and bone windows of the involved region. Over the last five years MRI was included as part of the evaluation. In 17 of the patients encasement or a significant invagination of cranial base blood vessels into the tumour was noted at the initial imaging so that a cerebral angiogram was performed. During the last two years three patients with prominent internal carotid artery involvement in the tumour underwent HmPAO nuclear brain scans without and with balloon test occlusion of the artery 3. The purpose of this examination is to pre-operatively evaluate the patient's tol- erance to sacrifice of the internal carotid artery.
The surgical approaches were conventional: uni or bilateral fron- tal craniotomies for anterior fossa floor tumours, frontotemporal craniotomies for sphenoid wing and middle fossa tumours, and a suboccipital craniectomy for posterior fossa turnouts. Five of the large petroclival tumours were resected by multiple stage surgery, via the middle and posterior fossa. Three tumours were resected via a combined infra- and supratentorial approach. The surgical aim was to attain a complete or maximal resection while attempting to maintain optimal integrity of vital structures. Follow-up surgery was performed to complete tumour resection or for recurrent tumour.
Radical tumour resection was defined as the combination of no tumour visualized via the operative microscope at the completion of surgery, no evidence of tumour histologically at the resection edges, no evidence of tumour on postoperative imaging, and no tumour recurrence during follow-up. Subtotal resection was defined as at least 90% of the tumour volume removed as judged on post- operative imaging as compared to the pre-operative imaging. Partial tumour resection was defined as less than 90% of the tumour volume removed as judged on imaging.
Following tumour resection, reconstruction of the surgical site was primarily performed with the purpose of preventing cerebro- spinal fluid leakage and possible ensuing infection. Fat, muscle, and fascia were taken from the thigh, abdomen or scalp and utilized to fill voids created by the tumour resection, block passages to the facial sinuses, and ensure good closure of the operative wound. Free mi- crovascular grafts were not used in this series. An important vas- cularized rotation flap which was utilized in subfrontal resections was the bifrontal pericranium laid on the anterior fossa floor to separate the cranial space from the underlying ethmoid sinuses and nasal cavity.
Results
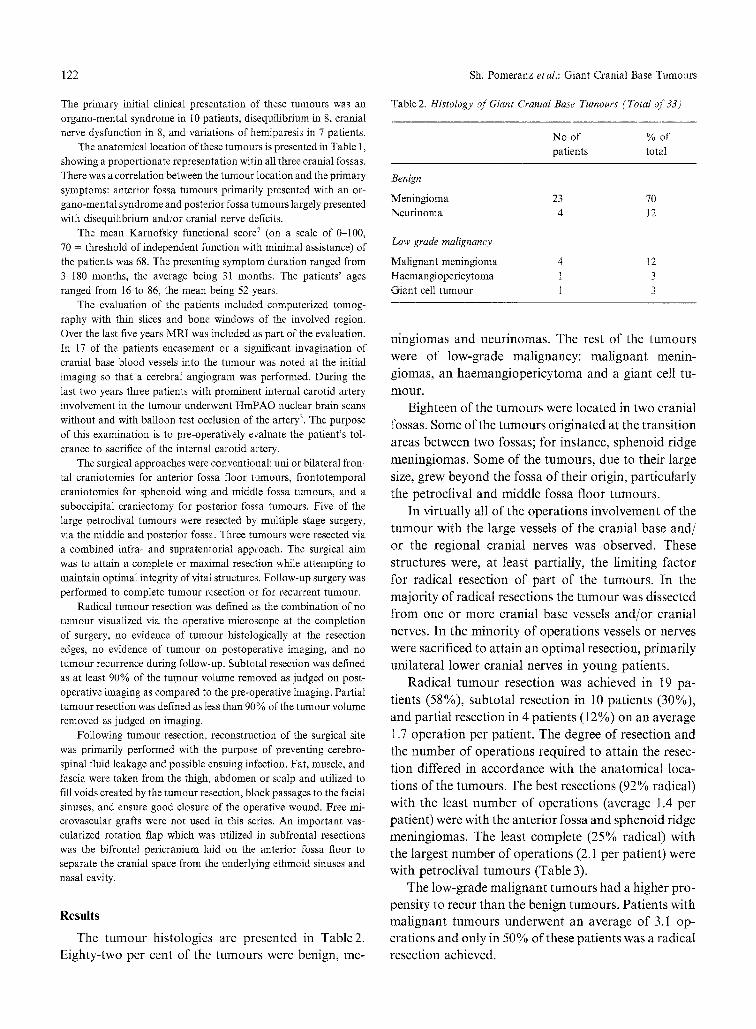
The t u m o u r histologies are presented in Table2.
Eighty-two per cent of the tumours were benign, me-
Table 2. Histology of Giant Cranial Base Tumours (Total of 33)
No of % of patients total
Benign
Meningioma 23 70 Neurinoma 4 12
Low grade malignancy
Malignant meningioma 4 12 Haemangiopericytoma 1 3 Giant cell tumour 1 3
n ingiomas and neur inomas . The rest of the tumours
were of low-grade mal ignancy: ma l ignan t menin-
giomas, an haemangioper icy toma and a giant cell tu-
mour .
Eighteen of the tumours were located in two cranial
fossas. Some of the tumours originated at the t ransi t ion
areas between two fossas; for instance, sphenoid ridge
meningiomas. Some of the tumours , due to their large
size, grew beyond the fossa of their origin, part icularly
the petroclival and middle fossa floor tumours.
In virtually all of the operat ions involvement of the
t u m o u r with the large vessels of the cranial base and/
or the regional cranial nerves was observed. These
structures were, at least partially, the l imiting factor
for radical resection of part of the tumours . In the
major i ty of radical resections the t u m o u r was dissected
from one or more cranial base vessels and /or cranial
nerves. In the minor i ty of operat ions vessels or nerves
were sacrificed to at ta in an opt imal resection, primari ly
uni lateral lower cranial nerves in young patients.
Radical t u m o u r resection was achieved in 19 pa-
tients (58%), subtotal resection in 10 patients (30%),
and partial resection in 4 patients (12%) on an average
1.7 operat ion per patient. The degree of resection and
the n u m b e r of operat ions required to a t ta in the resec-
t ion differed in accordance with the anatomical loca-
t ions of the tumours . The best resections (92% radical)
with the least n u m b e r of operat ions (average 1.4 per
patient) were with the anter ior fossa and sphenoid ridge
meningiomas. The least complete (25% radical) with
the largest n u m b e r of operat ions (2.1 per patient) were
with petroclival tumours (Table 3).
The low-grade mal ignan t tumours had a higher pro-
pensity to recur than the benign tumours . Patients with
ma l ignan t tumours underwent an average of 3.1 op-
erations and only in 50% of these patients was a radical
resection achieved.

Sh. Pomeranz et al.: Giant Cranial Base Tumours
Table3. Resection and Outcome of 33 Giant Cranial Base Tumours
Location/ Mean # % of Karnofsky score at tumour type operations/pt. Total
resection pre-op last follow-up
All 1.7 58 68 76 Anterior fossa + 92 69 92
sphenoid wing 1.4 PetroclivaI 2.1 29 70 52 Malignant 3.1 50 78 80
Table 4. Complications Following 56 Operations on 33 Patients with Giant Cranial Base Tumours
No. of cases
Infections
Meningitis 4 Brain abscess 1 Wound infection 3 Pneumonia, sepsis, urinary infection 10
Intracranial complications
Symptomatic brain oedema 6 Tumour bed haematoma 2 Hemiparesis 2 MCA infarct 1 Facial nerve deficit 4 Extra-ocular nerve deficit 3 Lower cranial nerve deficit 3
Extracranial complication
Symptomatic cardiac arrhythmia Gastric bleeding requiring gastrectomy Deep vein thrombosis
123
at other sites. Eleven patients had significant clinical
worsening of their b ra in funct ion and ten pat ients had
decreased funct ion of an impor t an t cranial nerve, at
least for several mon ths following surgery. At the last
follow-up, the mean Karnofsky score was 76, a sig-
nif icant rise relative to the pre-operative average score
of 68.
It can be seen from Table 3 that the best funct ional
results were in pat ients with anter ior fossa and sphenoid
ridge tumours , and the least favourable outcomes were
with petroclival tumours . The mean Karnofsky score
for pat ients with ma l ignan t tumours , at last follow-up,
was 80.
Illustrative Cases
1. Malignant meningioma. This 38-year-old woman had under- gone three subtotal resections of the tumour in the petrous region over seven years and had undergone teleradiotherapy. She was hos- pitalized now due to intractable left facial pain. Computerized tom- ography (Fig. 1) and magnetic resonance (Fig. 2) demonstrated a widespread petrous tumour extending into the middle and posterior fossas and the neck. Via an arched retro-auricular incision a subtotal resection was performed. Total resection was limited by widespread tumour infiltration of the internal carotid artery within the petrous bone and in the upper neck, the petrous bone itself having been subtotalty resected. The trigeminal nerve was seen to be widely in- filtrated by tumour and was transected at its emergence from the brain stem. The patient awoke readily at the completion of surgery with no facial pain, but with several complications: following surgery the vocal cord, which was paretic pre-operatively, became paralysed, requiring teflon injection of the cord. Repeated aspirations required a gastrostomy, from which the patient was weaned over several months. A pelvic abscess causing high fever was drained. Malab- sorption of cerebrospinal fluid (Fig. 3) was treated by a shunt from
The follow-up period in this series ranged from 2 -
120 months , with an average of 39 months . The mean
follow-up for ma l ignan t tumours was 75 months . It is
possible that the difference in follow-up time between
the benign and mal ignan t tumours is at least a part ial
explanat ion for the greater n u m b e r of operat ions that
pat ients with ma l ignan t tumours underwent . Three of
the four ma l ignan t mening iomas were histologically
diagnosed as benign at the initial operat ion.
There was no morta l i ty either peri-operatively or
dur ing the follow-up in this series. No t surprisingly,
the postoperat ive complicat ion rate was significant, as
can be seen in Table 4.
There were 8 infections at the operative site and 10 Fig. 1. Axial computerized tomography with contrast of the petrous bone malignant meningioma of patient 1

124 Sh~ Pomeranz etal.: Giant Cranial Base Tumours
2. Benign meningioma. This 50-year-old woman was hospitalized due to progressive dementia and paraparesis to the degree that she was unable to stand, and left arm paresis. MRI (Fig. 4) demonstrated a bifrontal tumour originating from the region of the tuberculum sella and invading the ethmoid sinuses. The pericallosal arteries were partially encased by tumour. Via a bifrontal craniotomy total re-
Fig. 2. Coronal magnetic resonance image of the malignant me- ningioma of patient 1 demonstrating the tumour extent intracranially and in the neck
Fig. 4. Axial computerized tomography with contrast enhancement at the level of the orbita of patient 2 pre-operatively. Tumour spread to the ethmoidal sinuses and partial encasement of the pericallosal arteries can be seen
Fig. 3. Axial computerized tomography following surgery of patient 1. The degree of resection can be seen. The turnout bed is full of fluid and the skin flap is elevated by cerebrospinal fluid under pres- sure. This finding was treated by a shunt to the peritoneum.
the tumour bed to the peritoneum. The patient, now at 20 months after surgery was no evidence of tumour regrowth, is at home with no facial pain and a Karnofsky score of 70.
Fig. 5. Axial computerized *omography at the level of the orbita of patient 2 following tumour resection. The frontal periosteal rotation flap partially filling the ethmoidal sinuses can be seen

Sh. Pomeranz etal.: Giant Cranial Base Tumours 125
section of the tumour was performed, including the parts from within the sinuses and from around the arteries. To avoid a CSF leak from the sinuses a bifrontal periosteal flap was rotated under the frontal bones and laid on the medial portion of the floor of both frontal fossas (Fig. 5). The postoperative course was uneventful, except for a dramatic improvement in the dementia and triparesis. The patient, is now 18 months after surgery with a Karnofsky score of 90 (versus 40 pre-operatively), and has no evidence of tumour.
Discussion
One of the critiques o f con tempora ry published se-
ries o f operated cranial base tumours is that they have
not wi ths tood the test o f time: a follow-up perspective o f 1 ~ 1 5 years is needed to evaluate the significant risk
o f cranial base surgery as opposed to the usually in-
dolent growth of these tumours . The present series is quite open to such critique: the mean patient follow-
up of 39 months is a relatively short time in compar ison
to the pre-operative mean symptom durat ion o f 31 months. All the more so when 42% of the patients did
not have a radical resection and 18% had m a l i g n a n t
tumours. Nevertheless, an interim result can be a mile-
stone: a point of perception as to what has been ac-
complished and where the trend leads.
Almost 40% of these patients had anterior fossa
f loor or sphenoid wing tumours , and they had an ex- cellent radical resection rate o f 92% with a dramat ic
clinical improvement , as demonst ra ted by the mean
Karnofsky score rise f rom 69 to 92. Even if some of
these patients have a future recurrence, it should be
detected early at foi low-up and have a good chance for a safe and total resection.
Overall, 58% of the patients have had no intra- or
postoperat ive evidence o f t umour up to their last fol- low-up. A n y recurrence in this group would probably
be slow-growing and potentially resectable (obviously this group significantly overlaps the group with ante-
rior fossa tumours). The significant numeric size of this
series with no mortal i ty at over 3 years o f follow-up
should be an encouraging statistic to the surgeon and patient under taking the t reatment o f a giant cranial base tumour .
Though the poor overall radical resection rate (25%)
and clinical outcome (Karnofsky score decrease peri- operatively f rom 70 to 52) o f the eight petroclival tu-
mours is discouraging; due to this poor outcome, sta- tistically this subgroup will p robably have little effect on the overall ou tcome of the whole series as time progresses. Considering the known difficulties with pe- troclival tumours 1, the initiation o f this series 10 years ago, and that several surgeons were involved in treating
these patients, it is not surprising that the outcome is
suboptimal. As individual surgeons gain experience in
the complex approaches to these petroclival tumours
it is hoped and expected that the outcome will improve. Though anterior fossa tumours typically reach large
dimensions, it is impressive that so many petroclival
tumours attain such a giant size with a reasonably functional clinical status o f the patient.
Another critique o f this series is that it is a very
"mixed bag" anatomical ly and prognostically. A sig-
nificant unification does exist in that all o f the tumours
were o f the cranial base, were o f giant proport ions, and were either benign or o f low-grade malignancy. It
is interesting that three o f the four malignant menin-
giomas were diagnosed histologically at the initial op- eration as benign.
It is selfevident that the t reatment o f giant cranial
base tumours is a major challenge to bo th surgeon and
patient. The results o f this series o f 33 giant cranial base tumours are encouraging overall, but highlight
the need to improve our skills, especially with those
tumours that have so far been difficult to resect safely,
such as giant petroclival meningiomas.
References
1. Bricolo AP, Turazzi S, Talacchi A, Cristofori L (1992) Micro- surgical removai of petroclival meningiomas: a report of 33 patients. Neurosurgery 31:813-828
2. Denecke HJ (1978) Surgery of extensive tumors of the petrosal bone and lateral skull base region. Laryngol Rhinol Otol (Stuttg) 57:287-290
3. Eckard DA, Purdy PD, Bonte FJ (1992) Temporary Balloon Occlusion of the carotid artery combined with brain blood flow imaging as a test to predict tolerance prior to permanent carotid sacrifice. AJNR 13:1565-69
4. Gulya AJ, Glasscock ME, Jackson CG, Pensak ML, Harris PF, Bond A (1986) Skull-base surgery: operative refinements. Oto- laryngol Head Neck Surg 94:315-321
5. Hanakita J, Imataka K, Hanada H (1984) A case of a huge neurofibroma expanding extra and intracranially through the enlarged jugular foramen. No Shinkei Geka 12:109-113
6. Kadis GN, Mount LA, Ganti SR (1979) The importance of early diagnosis and treatment of the meningiomas of the planum sphenoidale and tuberculum sella: a retrospective study of 105 cases. Surg Neurol 12:367-371
7. Karnofsky DA, Burchenal JH (1949) The clinical evaluation of chemotherapeutic agents in cancer. In: Macleod CM (ed) Eval- uation of chemotherapeutic agents. Columbia University Press, New York, pp 191-205
8. Mirimanoff RO, Bosoretz DE, Lingood RM, Ojemann RG, Martuza RL (1985) Meningioma, analysis of recurrence and progression following neurosurgical resection. J Neurosurg 62: 18-24
9. Pomeranz S, Sekhar LN, Janecka IP, Hirsch B, Ramasastry S (1993) Classification, technique, and results of surgical resection

126 Sh. Pomeranz etaL: Giant Cranial Base Tumours
ofpetrous bone tumors. In: Sekhar LN, Janecka IP (eds) Surgery of cranial base tumors. Raven, New York, pp 317-336
10. Pomeranz S, Sekhar L, Sen C, Snyderman C, Hirsch B (1991) Total petrous bone resection as an approach to intradural cranial base tumors. American Association of Neurological Surgeons, New Orleans, April 1991, Abstract
11. Sekhar LN, Jannetta PJ, Burkhart LE, Janosky JE (1990) Me- ningiomas involving the clivus: a six-year experience with 41 patients. Neurosurgery 27:764-781
12. Sekhar LN, Pomeranz S, Janecka IP, Hirsch B, Ramasastry S (1992) Temporal bone tumors: a report of 20 cases. J Neurosurg 76: p 578-587
13. Sekhar LN, Pomeranz S, Sen CN (199l) Extradural petrous bone and petroclival neoplasms. Acta Neurochir (Wien) [Suppl] 53:183 192
14. Sekhar LN, Schramm VL, Jones NF (1987) Subtemporal-pre- auricular infratemporal fossa approach to large lateral and pos- terior cranial base neoplasms. J Neurosurg 67:488-499
Correspondence: Shlomo Pomeranz, M.D., Neurosurgery De- partment, Hadassah University Hospital, Ein Karem, Jerusalem, Israel.




















