Ecological correlates to cranial morphology in leporids (Mammalia, Lagomorpha)
Upload
independentCategory
view
0download
0
EXPERIMENTAL
Cranial Particulate Bone Graft Ossifies CalvarialDefects by Osteogenesis
Aladdin H. Hassanein,M.D., M.M.Sc.
Praveen R. Arany, Ph.D.,M.D.S., M.M.Sc.
Rafael A. Couto, B.A.James E. Clune, M.D.Julie Glowacki, Ph.D.
Gary F. Rogers, M.D., J.D.,M.B.A.
John B. Mulliken, M.D.Arin K. Greene, M.D.,
M.M.Sc.
Boston, Mass.
Background: Cranial particulate bone graft heals inlay calvarial defects and canbe harvested as early as infancy. The purpose of this study was to test thehypothesis that particulate bone promotes ossification primarily by osteogenesis.Methods: Freshly harvested particulate bone, devitalized particulate bone, andhigh-speed drilled bone dust from rabbit calvaria were assayed for metabolic activity(resazurin) and viable osteoblasts (alkaline phosphatase). A rabbit cranial defectmodel was used to test the effect of devitalizing particulate bone on in vivo ossifi-cation. A parietal critical-size defect was created and managed in three ways: (1) noimplant (n � 6); (2) particulate bone implant (n � 6); and (3) devitalized par-ticulate bone implant (n � 6). Micro–computed tomographic scanning was usedto measure ossification 16 weeks later; histology also was studied.Results: Particulate bone contained more viable cells (0.94 percent transmit-tance per milligram) compared with devitalized particulate bone (0.007 per-cent) or bone dust (0.21 percent) (p � 0.01). Particulate bone had greateralkaline phosphatase activity (0.13 �U/�g) than devitalized particulate bone(0.000) or bone dust (0.06) (p � 0.01). Critical-size defects treated with par-ticulate bone had more ossification (99.7 percent) compared with devitalizedparticulate bone implants (42.2 percent) (p � 0.01); no difference was foundbetween devitalized particulate bone and the control (40.8 percent) (p � 0.9).Conclusions: Particulate bone graft contains living cells, including osteoblasts,that are required to heal critical-size cranial defects. These data support thehypothesis that particulate bone promotes ossification primarily byosteogenesis. (Plast. Reconstr. Surg. 129: 796e, 2012.)
Reconstruction of pediatric calvarial defects isdifficult. The use of alloplastic materialsgenerally is not indicated because they do not
fully osseointegrate and can become unstable withcranial growth.1 Autologous rib and iliac grafts re-sorb and cause donor-site morbidity.2–4 Split cranialbone is preferred for inlay cranioplasty but is difficultto harvest in children younger than 5 years becauseof the underdeveloped diploe.5
One option for overcoming the limited supplyof autologous bone in children is to use cranialparticulate bone graft. This material may be har-vested in infancy, before a diploic space has
formed. Using a hand-turned brace and bit, piecesof bone can be obtained from the ectocortical orendocortical surface. We previously have shownthat particulate graft repairs nonhealing, critical-size defects experimentally6 and clinically.7–10 Themechanism by which particulate graft ossifies crit-ical-size defects, however, is unknown.
Bone autografts heal primarily by two mech-anisms, depending on their architecture: osteogen-esis (direct ossification by osteoblasts within thegraft) and/or osteoconduction (ingrowth of adja-cent bone into the implant).11,12 Cancellous graftshave a large surface area–to–volume ratio, whichfacilitates revascularization, diffusion of recipient-site nutrients, and osteogenesis. Cortical grafts areresistant to rapid neovascularization; cells on theinterior do not survive, and the dense scaffold isrepopulated by ingrowth of living tissue.11,12 Al-
From the Department of Plastic and Oral Surgery, Children’sHospital Boston, Harvard Medical School; the Program inOral and Maxillofacial Pathology, Harvard School ofDental Medicine; and the Department of Orthopedic Sur-gery, Brigham and Women’s Hospital, Harvard MedicalSchool.Received for publication July 16, 2011; accepted November21, 2011.Copyright ©2012 by the American Society of Plastic Surgeons
DOI: 10.1097/PRS.0b013e31824a2bdd
Disclosure: The authors have no financial interestto declare in relation to the content of this article.
www.PRSJournal.com796e

though osteoinduction (differentiation of host mes-enchymal cells into osteoblasts) may be involved inautograft healing, demineralization is requiredfor osteoinductive matrix to have activity.13–16
Because the morphology of corticocancellousparticulate graft is similar to cancellous bone, wehypothesized that particulate graft contains viablecells that are responsible for healing. The purposeof this study was to determine whether autologouscalvarial particulate bone graft ossifies inlay cra-nioplasty defects primarily by osteogenesis.
MATERIALS AND METHODS
Histologic Analysis and Vital Assays ofBone Grafts
This study was approved by the Animal Useand Care Committee at Children’s Hospital Bos-ton. Subperiosteal exposure of the frontal andparietal bones of an adult, New Zealand Whiterabbit was performed, and particulate bone (700mg) was harvested from the calvaria with a hand-driven Hudson brace and 16-mm D’Errico crani-otomy bit (Codman & Shurtleff, Inc., Raynham,Mass.).6 Bone dust (350 mg), which does not healcritical-size cranial defects,6 was used as a control;it was procured with an electric pen drive and4-mm egg burr (Synthes, Inc., West Chester, Pa.).Particulate bone and bone dust were divided into35-mg aliquots. One-half of the particulate bonewas devitalized by two freeze-thaw cycles (–20°Cfor 18 hours and then room temperature for 6hours), followed by five deep freeze-thaw cycles(–80°C for 18 hours and then room temperaturefor 6 hours).17 Freeze-thawing was chosen as thedevitalization method because it does not alter theextracellular matrix or graft morphology.18 Sam-ples from all three graft types were fixed in 4%paraformaldehyde, decalcified, and embedded inparaffin, and 5-�m sections were stained with he-matoxylin and eosin.
Resazurin, an oxidation-reduction indicatorof living cells, was used to assess graft viability.Metabolically active cells reduce blue dye to a redfluorescent resorufin (Alamar Blue; Invitrogen,Inc., Carlsbad, Calif.).19,20 One milliliter of resa-zurin was added to each of five aliquots of partic-ulate bone, devitalized particulate bone, and bonedust. The mixtures were incubated in the dark at37°C for 2 hours. Absorption was measured usinga microplate reader at 570 nm and analyzed withKC4 software (BioTek Instruments, Inc., Win-ooski, Vt.). These data were normalized to dryweights (per milligram of graft) following 3 days
of lyophilization (FreeZone; Labconco, Inc., Kan-sas City, Mo.).
An assay for alkaline phosphatase was used tomeasure osteoblastic activity.21,22 One milliliter oflysis buffer (50 mM Tris HCl and 0.1% TritonX-100, pH 9.5) was added to five aliquots of par-ticulate bone, devitalized particulate bone, andbone dust, that were then lysed with sonication.One hundred microliters of 4-methylbelliferylphosphate (4-MUP Substrate System; Sigma-Al-drich, Inc., St. Louis, Mo.) was added to 20 �l ofeach sample for 25 minutes at 37°C. A standardcurve was run for each assay with human placentalalkaline phosphatase (Sigma-Aldrich). Fluores-cence was measured using a microplate readerwith excitation/emission at 365/450 nm and an-alyzed with KC4 software (BioTek). Fluorescenceunits were normalized to the amount of protein(in microunits per microgram) in each sample.Protein was determined with the bicinchoninicacid assay reagent according to the manufactur-er’s protocol (Pierce BCA Protein Assay Kit;Thermo Fisher Scientific, Inc., Waltham, Mass.).23
Animal ModelA rabbit calvarial critical-size defect model was
used to test the effect of particulate bone graftdevitalization on in vivo ossification.6 EighteenNew Zealand White rabbits aged 16 to 18 monthsunderwent subperiosteal exposure of the frontaland parietal bones through a coronal incision(Fig. 1). A 17 � 17-mm defect in the parietal bonesof 12 animals was made using an osteotome whilepreserving the underlying dura. Particulate bonegraft was harvested from the frontal bones using ahand-driven Hudson brace and 16-mm D’Erricocraniotomy bit (Codman & Shurtleff).6 In groupI (n � 6), the particulate bone was discarded andno implant was placed into the defect. In group II(n � 6), the particulate bone was placed into theparietal defect. In group III (n � 6), particulatebone first was harvested and devitalized; at a sec-ond operation, the parietal defect was created andfilled with the devitalized particulate bone. Beforeclosure, fibrin sealant was placed over the critical-size defect in all three groups (Tisseel; BaxterHealthcare Corporation, Deerfield, Ill.).6 Sixteenweeks postoperatively, rabbits were studied withmicro–computed tomography (Siemens Micro-CAT II Small Animal Imaging System; SiemensMedical Solutions USA, Inc., Malvern, Pa.). Ossi-fication was determined based on computed to-mographic densitometry using Amira software(Visage Imaging, Inc., San Diego, Calif.) and pre-
Volume 129, Number 5 • Ossification of Calvarial Defects
797e

sented as the percentage of the critical-size defectthat had ossified (1 – residual defect area/originaldefect area � 100). The parietal bones were ex-cised, and hematoxylin and eosin staining was per-formed to evaluate osseous healing of the grafts.
Statistical AnalysisPower analysis indicated that a sample size of
six rabbits in each group provided a 90 percentpower to detect a 25 percent difference in ossifi-cation (SD, 10 percent) using analysis of variance(nQuery Advisor 7.0; Statistical Solutions, Saugus,Mass.). Data are presented as medians with inter-quartile ranges (25th to 75th percentile). Differ-
ences between absorption/fluorescence and ossi-fication of critical-size defects were compared withthe Kruskal-Wallis test. Two-tailed values of p �0.05 were considered significant. Statistical anal-ysis was performed with GraphPad Prism (Graph-Pad Software, Inc., La Jolla, Calif.).
RESULTSHistologic Analysis and Vital Assays of BoneGrafts
Fresh particulate bone exhibited osteocyte-filled lacunae, whereas the lacunae were empty indevitalized particulate bone (Fig. 2). Bone dustshowed occasional osteocytes with predominantly
Fig. 1. Rabbit inlay cranioplasty model. (Above, left) Exposed frontal and parietalbones. (Above, right) Particulate bone procured from frontal bone with a hand-drivenbrace and bit. (Below, left) A 17 � 17-mm parietal critical-size defect and partial-thick-ness particulate bone donor site. (Below, right) Graft placed into critical-size defect.
Plastic and Reconstructive Surgery • May 2012
798e

vacant lacunae and areas of darkened staining andaltered lamellar structure consistent with thermalinjury. Particulate bone had more viable cells byresazurin assay (0.94 percent transmittance permilligram; interquartile range, 0.78 to 1.63 per-cent) than devitalized particulate bone (0.007 per-cent; interquartile range, 0.004 to 0.017 percent)or bone dust (0.21 percent; interquartile range,0.19 to 0.54 percent) (p � 0.01); bone dust ex-hibited greater viability than devitalized particu-late bone (p � 0.01) (Table 1). Particulate bonehad more alkaline phosphatase activity (0.13 �U/�g; interquartile range, 0.11 to 0.23) than devi-talized particulate graft (0.000; interquartilerange, 0.000 to 0.006) or bone dust (0.06; inter-
quartile range, 0.03 to 0.08) (p � 0.01); bone dusthad elevated alkaline phosphatase activity com-pared with devitalized particulate bone (p � 0.01).
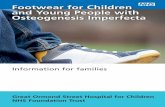
Repair of Cranial DefectsSixteen weeks after inlay cranioplasty, defects
treated with particulate bone were closed, whereasthose managed with no implant or with devitalizedparticulate bone were not healed (Fig. 3). Micro–computed tomography demonstrated that defectsfilled with particulate bone (group II) had greaterossification (99.7 percent; interquartile range,98.2 to 100 percent) than those with devitalizedparticulate bone (group III) (42.2 percent; inter-
Fig. 2. Comparison of cranial bone grafts. (Above) Gross images show that nondevitalized and devitalized particulate boneappear similar and are larger than bone dust. (Below) Histologic evaluation illustrates that particulate bone and devitalizedparticulate bone have equivalent architecture, in contrast to bone dust. Particulate bone contains lacunae that are osteocyte-filled; devitalized particulate bone has empty lacunae. Bone dust demonstrates occasional osteocytes with predominantlyempty lacunae; dark staining and altered lamellar architecture indicate thermal injury (hematoxylin and eosin; original mag-nification, �400).
Table 1. Comparison of Bone Graft Viability and Osteoblast Activity (n � 5 per Group)
ParticulateBone (IQR)
Devitalized ParticulateBone (IQR) Bone Dust (IQR) p*
Viability (resazurin, % transmittance/mg) 0.94 (0.78–1.63) 0.007 (0.004–0.017) 0.21 (0.19–0.54) 0.01Osteoblast activity (alkaline phosphatase, �U/�g) 0.13 (0.11–0.23) 0.000 (0.000–0.006) 0.06 (0.03–0.08) 0.01IQR, interquartile range.*Kruskal-Wallis test.
Volume 129, Number 5 • Ossification of Calvarial Defects
799e
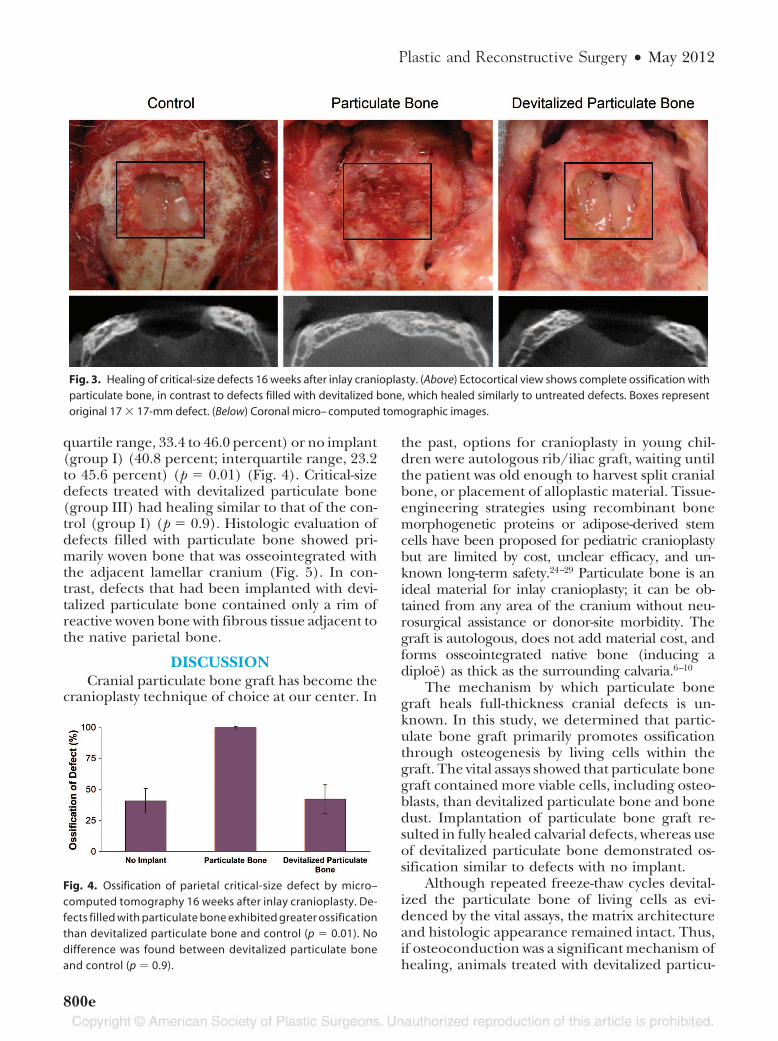
quartile range, 33.4 to 46.0 percent) or no implant(group I) (40.8 percent; interquartile range, 23.2to 45.6 percent) (p � 0.01) (Fig. 4). Critical-sizedefects treated with devitalized particulate bone(group III) had healing similar to that of the con-trol (group I) (p � 0.9). Histologic evaluation ofdefects filled with particulate bone showed pri-marily woven bone that was osseointegrated withthe adjacent lamellar cranium (Fig. 5). In con-trast, defects that had been implanted with devi-talized particulate bone contained only a rim ofreactive woven bone with fibrous tissue adjacent tothe native parietal bone.
DISCUSSIONCranial particulate bone graft has become the
cranioplasty technique of choice at our center. In
the past, options for cranioplasty in young chil-dren were autologous rib/iliac graft, waiting untilthe patient was old enough to harvest split cranialbone, or placement of alloplastic material. Tissue-engineering strategies using recombinant bonemorphogenetic proteins or adipose-derived stemcells have been proposed for pediatric cranioplastybut are limited by cost, unclear efficacy, and un-known long-term safety.24–29 Particulate bone is anideal material for inlay cranioplasty; it can be ob-tained from any area of the cranium without neu-rosurgical assistance or donor-site morbidity. Thegraft is autologous, does not add material cost, andforms osseointegrated native bone (inducing adiploe) as thick as the surrounding calvaria.6–10
The mechanism by which particulate bonegraft heals full-thickness cranial defects is un-known. In this study, we determined that partic-ulate bone graft primarily promotes ossificationthrough osteogenesis by living cells within thegraft. The vital assays showed that particulate bonegraft contained more viable cells, including osteo-blasts, than devitalized particulate bone and bonedust. Implantation of particulate bone graft re-sulted in fully healed calvarial defects, whereas useof devitalized particulate bone demonstrated os-sification similar to defects with no implant.
Although repeated freeze-thaw cycles devital-ized the particulate bone of living cells as evi-denced by the vital assays, the matrix architectureand histologic appearance remained intact. Thus,if osteoconduction was a significant mechanism ofhealing, animals treated with devitalized particu-
Fig. 3. Healing of critical-size defects 16 weeks after inlay cranioplasty. (Above) Ectocortical view shows complete ossification withparticulate bone, in contrast to defects filled with devitalized bone, which healed similarly to untreated defects. Boxes representoriginal 17 � 17-mm defect. (Below) Coronal micro– computed tomographic images.
Fig. 4. Ossification of parietal critical-size defect by micro–computed tomography 16 weeks after inlay cranioplasty. De-fects filled with particulate bone exhibited greater ossificationthan devitalized particulate bone and control (p � 0.01). Nodifference was found between devitalized particulate boneand control (p � 0.9).
Plastic and Reconstructive Surgery • May 2012
800e

late bone would have been expected to ossify in amanner similar to those with fresh particulatebone implants. Without viable cells, the size of thedevitalized particulate bone graft pieces likely wastoo small to withstand resorption and thus couldnot serve as a scaffold for bony ingrowth.6
In addition to osteogenesis, it is possible thatother factors may influence particulate bone grafthealing. Although particulate bone may containosteoinductive proteins, the graft is unlikely tocause osteoinduction because it is not demineral-ized. Demineralization of bone is required for os-teoinduction to occur in heterotopic sites.13–16
Recent experimental evidence suggests that cir-culating progenitor cells may contribute to ossifi-cation of calvarial defects.30,31
Bone dust commonly is described as finepieces of bone generated by a power-driven toolfor drilling burr holes or while harvesting splitcranial bone.6,32–42 We chose bone dust as a controlfor the vital assays because, although bone dust isprocured from the same donor site as particulategraft, it does not heal inlay cranioplasty defects.6The greater viability of particulate bone comparedwith bone dust may be attributable to thermal injury.During the procurement of bone dust, cells may besubjected to excessive heat from the high-speed drill.Because particulate bone is harvested with a slow,hand-driven brace and bit, osteoblasts are not dam-aged by heat and thus can survive procurement andtransfer to the recipient bed. Bone dust containedmore viable cells, including osteoblasts, than devi-talized particulate bone, yet bone dust does not healcritical-size defects.6 This finding suggests that there
may be a minimal threshold for the number of viablecells required for bony particles to ossify by osteo-genesis. Another possibility is that bone dust maypossess adequate osteogenic potential, but the smallsize of the particles facilitates resorption by macro-phages, in contrast to the larger pieces of particulategraft, which are more resistant to phagocytosis.6
CONCLUSIONSThis study shows that particulate bone graft
contains living cells, including osteoblasts. Afterdevitalization, particulate bone no longer healscritical-size calvarial defects. Thus, the primarymechanism by which particulate bone graft ossi-fies inlay cranioplasty defects is by osteogenesisfrom cells within the graft.
Arin K. Greene, M.D., M.M.Sc.Department of Plastic and Oral Surgery
Children’s Hospital Boston300 Longwood Avenue
Boston, Mass. [email protected]
ACKNOWLEDGMENTThe authors thank the Kresge Laboratory for Pedi-
atric Imaging Research (Children’s Hospital Boston) foruse of the micro–computed tomography and image-pro-cessing software.
REFERENCES1. Gosain AK, Chim H, Arneja JS. Application-specific selection
of biomaterials for pediatric craniofacial reconstruction: De-veloping a rational approach to guide clinical use. Plast Re-constr Surg. 2009;123:319–330.
Fig. 5. Histologic evaluation of grafted cranial defects 16 weeks postoperatively (hematoxylin and eosin;original magnification, �20). (Left) Particulate bone has healed the critical-size defect and osseointegratedwith the adjacent lamellar cranium. (Right) Devitalized particulate bone demonstrates reactive woven boneand fibrous tissue adjacent to the native parietal bone.
Volume 129, Number 5 • Ossification of Calvarial Defects
801e

2. Zins JE, Whitaker LA. Membranous versus endochondralbone: Implications for craniofacial reconstruction. Plast Re-constr Surg. 1983;72:778–785.
3. Laurie SW, Kaban LB, Mulliken JB, Murray JE. Donor-sitemorbidity after harvesting rib and iliac bone. Plast ReconstrSurg. 1984;73:933–938.
4. Tessier P, Kawamoto H, Posnick J, Raulo Y, Tulasne JF, WolfeSA. Complications of harvesting autogenous bone grafts: Agroup experience of 20,000 cases. Plast Reconstr Surg. 2005;116(Suppl):72S–73S; discussion 92S–94S.
5. Koenig WJ, Donovan JM, Pensler JM. Cranial bone graftingin children. Plast Reconstr Surg. 1995;95:1–4.
6. Clune JE, Mulliken JB, Glowacki J, et al. Inlay cranioplasty:An experimental comparison of particulate graft versus bonedust. Plast Reconstr Surg. 2010;126:1311–1319.
7. Greene AK, Mulliken JB, Proctor MR, Rogers GF. Primarygrafting with autologous cranial particulate bone preventsosseous defects following fronto-orbital advancement. PlastReconstr Surg. 2007;120:1603–1611.
8. Greene AK, Mulliken JB, Proctor MR, Rogers GF. Pediatriccranioplasty using particulate calvarial bone graft. Plast Re-constr Surg. 2008;122:563–571.
9. Gao LL, Rogers GF, Clune JE, et al. Autologous cranial partic-ulate bone grafting reduces the frequency of osseous defectsafter cranial expansion. J Craniofac Surg. 2010;21:318–322.
10. Rogers GF, Greene AK, Mulliken JB, Proctor MR, RidgwayEB. Exchange cranioplasty using autologous calvarial par-ticulate bone graft effectively repairs large cranial defects.Plast Reconstr Surg. 2011;127:1631–1642.
11. Motoki DS, Mulliken JB. The healing of bone and cartilage.Clin Plast Surg. 1990;17:527–544.
12. Rogers GF, Greene AK. Autogenous bone graft: Basic scienceand clinical implications. J Craniofac Surg. 2012;23:323–327).
13. Mulliken JB, Glowacki J. Induced osteogenesis for repair andconstruction in the craniofacial region. Plast Reconstr Surg.1980;65:553–560.
14. Glowacki J, Altobelli D, Mulliken JB. Fate of mineralized anddemineralized osseous implants in cranial defects. Calcif Tis-sue Int. 1981;33:71–76.
15. Glowacki J. A review of osteoinductive testing methods andsterilization processes for demineralized bone. Cell TissueBank. 2005;6:3–12.
16. Glowacki J, Zhou S, Mizuno S. Mechanisms of osteoinduc-tion/chondroinduction by demineralized bone. J CraniofacSurg. 2009;20(Suppl 1):634–638.
17. Zaleske D, Peretti G, Allemann F, et al. Engineering a joint:A chimeric construct with bovine chondrocytes in a devital-ized chick knee. Tissue Eng. 2003;9:949–956.
18. Urist MR, Dowell TA, Hay PH, Strates BS. Inductive sub-strates for bone formation. Clin Orthop Rel Res. 1968;59:59–96.
19. Nakayama GR, Caton MC, Nova MP, Parandoosh Z. Assess-ment of the Alamar Blue assay for cellular growth and via-bility in vitro. J Immunol Methods 1997;204:205–208.
20. Moursi AM, Winnard PL, Winnard AV, Rubenstrunk JM,Mooney MP. Fibroblast growth factor 2 induces increasedcalvarial osteoblast proliferation and cranial suture fusion.Cleft Palate Craniofac J. 2002;39:487–496.
21. Sodek J, Berkman FA. Bone cell cultures. Methods Enzymol.1987;145:303–324.
22. Byers BA, Pavlath GK, Murphy TJ, Karsenty G, Garcia AJ.Cell-type-dependent up-regulation of in intro mineralizationafter overexpression of the osteoblast-specific transcriptionfactor RUnx2/Cbfa1. J Bone Miner Res. 2002;17:1931–1944.
23. Tuszynski GP, Murphy A. Spectrophotometric quantitationof anchorage-dependent cell numbers using the bicin-choninic acid protein assay reagent. Anal Biochem. 1990;184:189–191.
24. Cowan CM, Shi YY, Aalami OO, et al. Adipose-derived adultstromal cells heal critical-size mouse calvarial defects. NatBiotechnol. 2004;22:560–567.
25. Dudas JR, Marra KG, Cooper GM, et al. The osteogenicpotential of adipose-derived stem cells for the repair of rabbitcalvarial defects. Ann Plast Surg. 2006;56:543–548.
26. Smith DM, Afifi AM, Cooper GM, Mooney MP, Marra KG,Losee JE. BMP-2-based repair of large-scale calvarial defectsin an experimental model: Regenerative surgery in cranio-plasty. J Craniofac Surg. 2008;19:1315–1322.
27. Kinsella CR Jr, Cray JJ, Durham EL, et al. Recombinanthuman bone morphogenetic protein-2-induced craniosyn-ostosis and growth restriction in the immature skeleton. PlastReconstr Surg. 2011;127:1173–1181.
28. Kinsella CR, Bykowski MR, Lin A, et al. BMP-2-mediatedregeneration of large-scale cranial defects in the canine: Anexamination of different carriers. Plast Reconstr Surg. 2011;127:1865–1873.
29. Levi B, James AW, Nelson ER, et al. Acute skeletal injury isnecessary for human adipose-derived stromal cell-mediatedcalvarial regeneration. Plast Reconstr Surg. 2011;127:1118–1129.
30. Levi B, James AW, Nelson ER, et al. Studies in adipose-derived stromal cells: Migration and participation in repairof cranial injury after systemic injections. Plast Reconstr Surg.2011;127:1130–1140.
31. Wang XX, Allen RJ Jr, Tutela JP, et al. Progenitor cell mo-bilization enhances bone healing by means of improvedneovascularization and osteogenesis. Plast Reconstr Surg.2011;128:395–405.
32. Davini V, Rivano C, Borzone M, Tercero E. Bone dust andadhesive material for closing bony breaches of the skull: Anew method. J Neurosurg Sci. 1981;25:117–119.
33. Tessier P. Autogenous bone grafts taken from the calvariumfor facial and cranial applications. Clin Plast Surg. 1982;9:531–538.
34. Jackson IT, Pellett C, Smith JM. The skull as a bone graftdonor site. Ann Plast Surg. 1983;11:527–532.
35. Jackson IT, Adham M, Bite U, Marx R. Update on cranialbone grafts in craniofacial surgery. Ann Plast Surg. 1987;18:37–40.
36. Jackson IT, Sullivan C, Shiele UU. A simple bone dust col-lector. Plast Reconstr Surg. 1988;81:967–969.
37. Craft PD, Sargent LA. Membranous bone healing and tech-niques in calvarial bone grafting. Clin Plast Surg. 1989;16:11–19.
38. Fukuta K, Har-Shai Y, Collares MV, Herschman BR, PersianiRJ, Jackson IT. The viability of revascularized calvarial bonegraft in a pig model. Ann Plast Surg. 1992;29:136–142.
39. Ilankovan V, Jackson IT. Experience in the use of calvarialbone grafts in orbital reconstruction. Br J Oral Maxillofac Surg.1992;30:92–96.
40. O’Broin ES, Morrin M, Breathnach E, Allcutt D, Earley MJ.Titanium mesh and bone dust calvarial patch during cra-nioplasty. Cleft Palate Craniofac J. 1997;34:354–356.
41. Sheikh BY. Simple and safe method of cranial reconstructionafter posterior fossa craniectomy. Surg Neurol. 2006;65:63–66.
42. Malhotra G, Gupta A, Jackson IT. Collection of bone dust: Anew technique. Plast Reconstr Surg. 2009;123:58e–59e.
Plastic and Reconstructive Surgery • May 2012
802e
Copyright © 2022 FDOKUMEN