
ON A MULTILEVEL KRYLOV METHOD FOR THE HELMHOLTZ EQUATION PRECONDITIONED BY SHIFTED LAPLACIAN

Journal of Pharmacological and Toxicological Methods xxx (2008) xxx–xxx
JPM-05808; No of Pages 6
Contents lists available at ScienceDirect
Journal of Pharmacological and Toxicological Methods
j ourna l homepage: www.e lsev ie r.com/ locate / jpharmtox
ARTICLE IN PRESS
Original article
Measuring left ventricular function in thenormal, infarcted andCORM-3-preconditionedmouse heart using complex admittance-derived pressure volume loops
James E. Clark a,⁎, Anil Kottam b, Roberto Motterlini c, Michael. S. Marber a
a Kings College London, Cardiovascular Division, London, SE1 7EH, UKb Scisense Inc. London, Ontario, Canada N6E 3A1c Department of Drug Discovery and Development, Italian Institute of Technology, Genova, Italy
⁎ Corresponding author. Department of Cardiology, KCL,Hospital, London SE17EH, UK. Tel.: +44 20 71880966; fax:
E-mail address: [email protected] (J.E. Clark).
1056-8719/$ – see front matter © 2008 Elsevier Inc. Alldoi:10.1016/j.vascn.2008.10.007
Please cite this article as: Clark, J. E., et al., Musing complex admittanceerived pressure...
a b s t r a c t
a r t i c l e i n f oArticle history:
Introduction:Miniaturiz Received 20 October 2008Accepted 30 October 2008Available online xxxxKeywords:MouseHeartMethodsVentricular functionAdmittanceConductanceInfarction
ed conductance catheters have been successfully applied tomeasure left ventricular(LV) function in themouse to assess cardiac or pharmacological interventions. Complex admittance, in contrast toexistingmethods using conductance catheters, produces an estimate of the parallel admittance of cardiacmusclethat can be used to correct themeasurement in real-time. The aimof this studywas to validate the use of complexadmittance to assess LV function in normal and infarcted hearts.Methods: Using a single conductance catheter,we directly compared measures of LV function using a specially developed admittance system (ADVantage™system) and a traditional conductance-derived pressure–volume (PV) system. We subjected mice to focalmyocardial ischaemia-reperfusion injury while measuring cardiac function to determine the ability of the newsystem to distinguish between normal, and dysfunctional LV, contractile performance. Results: LV pressure–volume loops from complex admittance is a reproducible and reliable method of determining LV function,producing data similar to that of the conductance catheter. Our data suggest that theADVantage™ systemrecordslarger systolic LV cavity volumes when compared to the traditional conductance system in the same animal. Inaddition, we demonstrate marked LV dysfunction following coronary artery occlusion and reperfusion which isameliorated using CORM-3, a cardioprotective agent that liberates carbon monoxide (CO). Conclusion: TheADVantage™ system is both effective and reproducible in measuring LV function and dysfunction in the mouse,without the need for complicated interventions to calibrate themeasurements. Thismaymark theway toward anaccurate assessment of murine cardiac function.
© 2008 Elsevier Inc. All rights reserved.
1. Introduction
The need for interrogation of murine cardiac function is vital forstudies designed to investigate therapies that modify cardiac contrac-tility or to manipulate pathologies such as cardiac remodelling ormyocardial infarction (MI). Any system used to examine cardiac functionshould be accurate, reproducible andwith low inter-user variation, all ofwhich are problematic in mice due to their small size and rapid heartrate. Over thepast fewdecades a numberof strategies havebeen adoptedto address this requirement including echocardiography, magneticresonance imaging and conductance volumetry (Balaban & Hampshire,2001; Feldmanet al., 2000;Georgakopoulos et al.,1998; James,Hewett, &Robbins, 1998; Rottman, Ni, & Brown, 2007; Wei et al., 2007). Of these,conductance catheters have emerged as a cost-effective platform for invivo characterisation of instantaneous pressure–volume loops to assessLV function (Pacher, Nagayama, Mukhopadhyay, Batkai, & Kass, 2008;Wei, Valvano, Feldman, & Pearce, 2005). One major limitation of single
The Rayne Institute, St Thomas'+44 20 71880970.
rights reserved.
easuring left ventricular func, Journal of Pharmacological a
frequency conductancemeasurements is that they cannot account for theinherent conductance of the myocardium which can result in over-estimation of the blood volume of the ventricle (Baan et al., 1984).Numerous strategies have been employed to overcome this inadequacy,such as hypertonic saline bolus injection and dual frequency excitation(Baan et al., 1984; Georgakopoulos & Kass, 2000a; Uemura et al., 2002).However, the necessary additional calibration steps often increase thevariability and introduce further errors in the measurements (Nielsenet al., 2007; Yang et al., 2001).
In an effort to overcome these shortcomings, a complex admittancebased technique was developed which produces an estimate of theparallel admittance of cardiac muscle that can be used to correct themeasurement in real-time (Raghavan et al., 2004). The corrected signalconsists of blood conductance which, when calibrated to end systolicand end diastolic blood conductance and aortic flow, can accuratelydetermine pressure–volume loops inside the LV on a beat-by-beat basiswithout the need for further calibration (Kottam et al., 2006; Raghavanet al., 2004). This new system, now in production (ADVantage™ system,Scisense Inc., London, Canada)was used tomeasure LV function in naïvemouse hearts and directly compared to data derived from traditionalconductance measurements.
tion in the normal, infarcted and CORM-preconditioned mouse heartnd Toxicological Methods (2008), doi:10.1016/j.vascn.2008.10.007
2 J.E. Clark et al. / Journal of Pharmacological and Toxicological Methods xxx (2008) xxx–xxx
ARTICLE IN PRESS
A requirement of any system to interrogate LV function is the abilityto discriminate between normal and abnormal function. Recentstudies have revealed the potent cardioprotective properties of thewater-soluble carbon monoxide-releasing molecule, CORM-3, inisolated preparations and in vivo studies (Chatterjee 2004; Clarket al., 2003; Foresti et al., 2004; Guo et al., 2004). In the present study,we used this molecule to elicit protection in an in vivo model of MI inorder to examine the efficacy of the ADVantage™ system to measurecardiac function.
The aim of this study, therefore, was to determine whether a novelmethod of PV loop acquisition, complex admittance, using the ADVan-tage™ system could be used to determine left ventricular function underresting conditions and after ischaemia reperfusion injury in the mouse.
2. Materials and methods
2.1. Experimental animals
All animal experiments were carried out in accordance with HomeOffice regulations as detailed in the Home Office Guidance on the
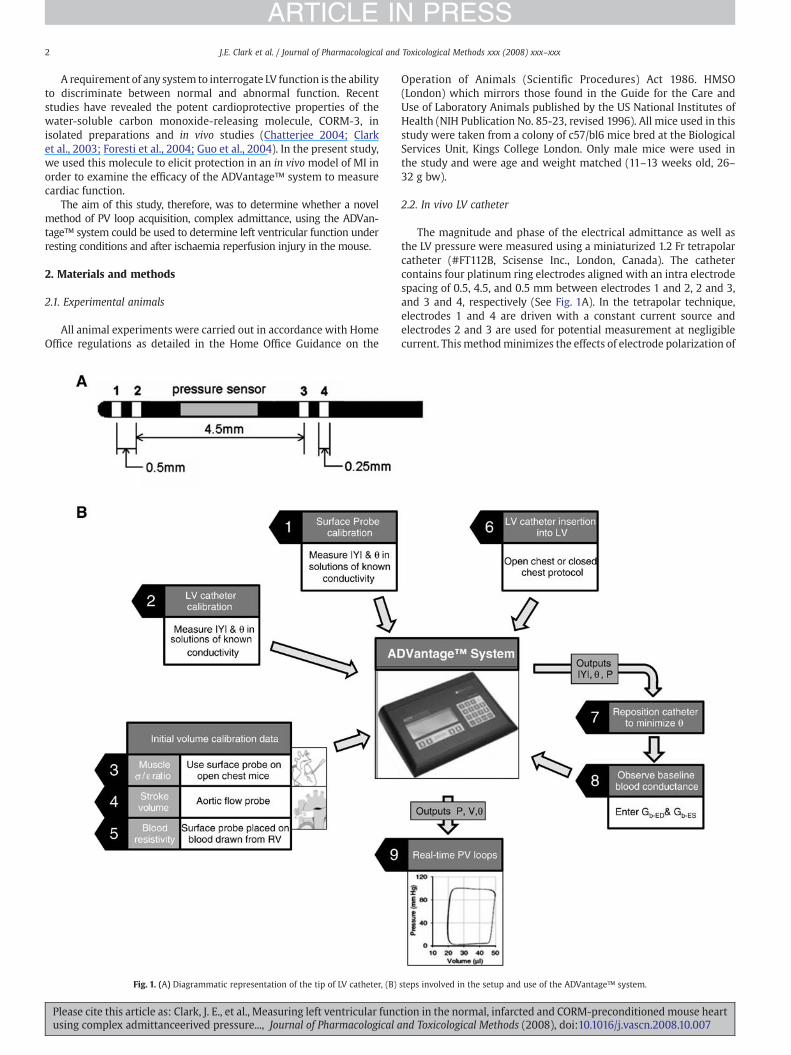
Fig. 1. (A) Diagrammatic representation of the tip of LV catheter, (B)
Please cite this article as: Clark, J. E., et al., Measuring left ventricular funcusing complex admittanceerived pressure..., Journal of Pharmacological a
Operation of Animals (Scientific Procedures) Act 1986. HMSO(London) which mirrors those found in the Guide for the Care andUse of Laboratory Animals published by the US National Institutes ofHealth (NIH Publication No. 85-23, revised 1996). All mice used in thisstudy were taken from a colony of c57/bl6 mice bred at the BiologicalServices Unit, Kings College London. Only male mice were used inthe study and were age and weight matched (11–13 weeks old, 26–32 g bw).
2.2. In vivo LV catheter
The magnitude and phase of the electrical admittance as well asthe LV pressure were measured using a miniaturized 1.2 Fr tetrapolarcatheter (#FT112B, Scisense Inc., London, Canada). The cathetercontains four platinum ring electrodes aligned with an intra electrodespacing of 0.5, 4.5, and 0.5 mm between electrodes 1 and 2, 2 and 3,and 3 and 4, respectively (See Fig. 1A). In the tetrapolar technique,electrodes 1 and 4 are driven with a constant current source andelectrodes 2 and 3 are used for potential measurement at negligiblecurrent. Thismethodminimizes the effects of electrode polarization of
steps involved in the setup and use of the ADVantage™ system.
tion in the normal, infarcted and CORM-preconditioned mouse heartnd Toxicological Methods (2008), doi:10.1016/j.vascn.2008.10.007

Fig. 2. Method for inducing reversible ischaemia (A and B) using a hanging weightsystem. (C) Surgical access is through a small left-sided lateral thoracotomy. Bars areraised to cause ischaemia and lowered for reperfusion.
3J.E. Clark et al. / Journal of Pharmacological and Toxicological Methods xxx (2008) xxx–xxx
ARTICLE IN PRESS
the measurement electrodes (van Oosterom, de Boer, & van Dam,1979). The pressure sensor is located between electrodes 2 and 3.
2.3. Surface probe
A tetrapolar surface probe (Scisense Inc., London, Canada) placedon the epicardial surface of the heart (above the LV) was used todetermine myocardial conductivity and permittivity. This is used forreal time calculation and removal of parallel conductance, which hasbeen shown to vary during the cardiac cycle (Wei et al., 2007). Theelectrode spacing on the probe ensures that the electric fieldpenetrates only the muscle and not the underlying blood pool(Kottam & Pearce, 2004). The surface probe was also used to measurethe blood resistivity at the end of the experiment by placing the probeon the surface of mouse blood collected in a vial immersed in a waterbath at 37 °C.
2.4. Instrumentation
Real-time pressure volume loops were obtained using theADVantage™ system (Scisense Inc, Canada) which uses an ultra-miniature admittance catheter described earlier to measure LVpressure and admittance. The use of complex electrical admittanceto determine real time LV volume has been described by Kottam et al.(2006). The non linear conductance-to-volume conversion equationhas been described by Wei et al. (2005). The various steps involved inthe setup and use of the ADVantage™ system is illustrated in Fig. 1B.The admittance catheter and surface probe calibrations wereperformed by measuring admittance magnitude and phase in salinesolutions of known conductivities. The conductivity values werechosen to cover the range of expected effective conductivities forblood and muscle (1000 to 10,000 μS/cm, or 0.1 to 1.0 S/m) at 37 °C.
2.5. Comparing conductance with admittance measurements of LVfunction
In order to compare the two methods of determining LV function,mice (n=16) were anaesthetized with isoflurane by passive inhalationand placed supine on a thermostatically-controlled heating pad tomaintain rectal temperature at 37±0.3 °C, intubated under directvision and ventilated under isoflurane anaesthesia (1.5% v/w/) in 100%oxygen at a respiratory rate of 110 min−1 and a tidal volume of 225 µlmin−1 (Ventilator—Hugo Sachs Elektronic MiniVent Type 845,Germany). An ultra-miniature conductance catheter (Scisense Inc.,London, Canada) was inserted into the left ventricle via a smalldiaphragmotomy through the apex of the heart. The catheter wasconnected to the ADVantage™ system and PV loopswere recorded at arate of 1000 samples/s using a multi-channel acquisition system(Powerlab, ADInstruments, UK). By observing the phase angle signal inreal time during the positioning of the catheter the user could movethe catheter to position the catheter on, or as close to as possible, thecentreline of the LV cavity.
The catheter was then connected to a Millar Aria MPVS system(Millar Instruments, Texas, USA) and PV loops were acquired aspreviously described by conductance (Burkhoff, Mirsky, & Suga, 2005;Clark et al., 2007; Tam et al., 2005). The catheter had been calibratedfor the conductance system prior to the experiment using the cuvettemethod according to the manufacturer's instructions and describedpreviously (Pacher et al., 2008). Parallel conductance (Vp) wasascertained by intravenous injection of a small amount (5–10 µl) ofhypertonic saline (15% NaCl w/v). Volume correction was performedby measuring aortic flow in the ascending aorta using a miniatureultrasonic aortic flow probe (Transonic Systems inc., USA). In bothcases, to ascertain the pressure–volume relationship under differentpreload conditions, the inferior vena cava (IVC) was transientlyoccluded using blunt-ended forceps.
Please cite this article as: Clark, J. E., et al., Measuring left ventricular funcusing complex admittanceerived pressure..., Journal of Pharmacological a
2.6. Infarction study
For the second part of the study, a similar surgical approach wasused to access the LV as described above. Coronary artery occlusionwas achieved using the hanging weight system as previouslydescribed (Eckle et al., 2006). Following left side lateral thoracotomy,a length of 8-0 nylon suture was carefully placed around the leftanterior descending (LAD) coronary artery, passed through a smalllength of 1.5 mm PE-10 tube and attached to a length of 5-0 suture.20 min baseline measurements were taken followed by administra-tion of CORM-3 (50 µmol kg−1 bw freshly dissolved in sterile saline,n=7) or vehicle (saline, n=6) via the jugular vein, followed by a 15minincubation period. PV loops using the ADVantage™ system wererecorded throughout the procedure. The suture was directed over twohorizontally mounted movable metal rods, and masses of 1 g eachwere attached to both ends. By elevation of the rods the masses aresuspended and the suture placed under controlled tension to occludethe LAD with a defined and constant pressure. LAD occlusion wasverified by paleness of the area at risk, with the colour of the LADperfusion zone changing from bright red to violet indicating cessationof blood flow. Reperfusionwas achieved by lowering the rods until themasses lay on the operating pad and the tension of the ligature wasrelieved. Reperfusion was verified by the equivalent criteria used toverify occlusion. Mice were excluded from further analysis if all threecriteria were not met at met at the start of coronary occlusion andwithin 15 min of reperfusion. During coronary artery occlusion,temperature and humidity of the heart surface were maintained bycovering the heart with the pectoralis minor muscle flap and bysealing the thoracotomy with a 0.9% (w/v) saline wet gauze. Regionalischaemia was induced for 30 min followed by 120 min reperfusion(Eckle et al., 2006; Fisher & Marber, 2002) (Fig. 2).
tion in the normal, infarcted and CORM-preconditioned mouse heartnd Toxicological Methods (2008), doi:10.1016/j.vascn.2008.10.007
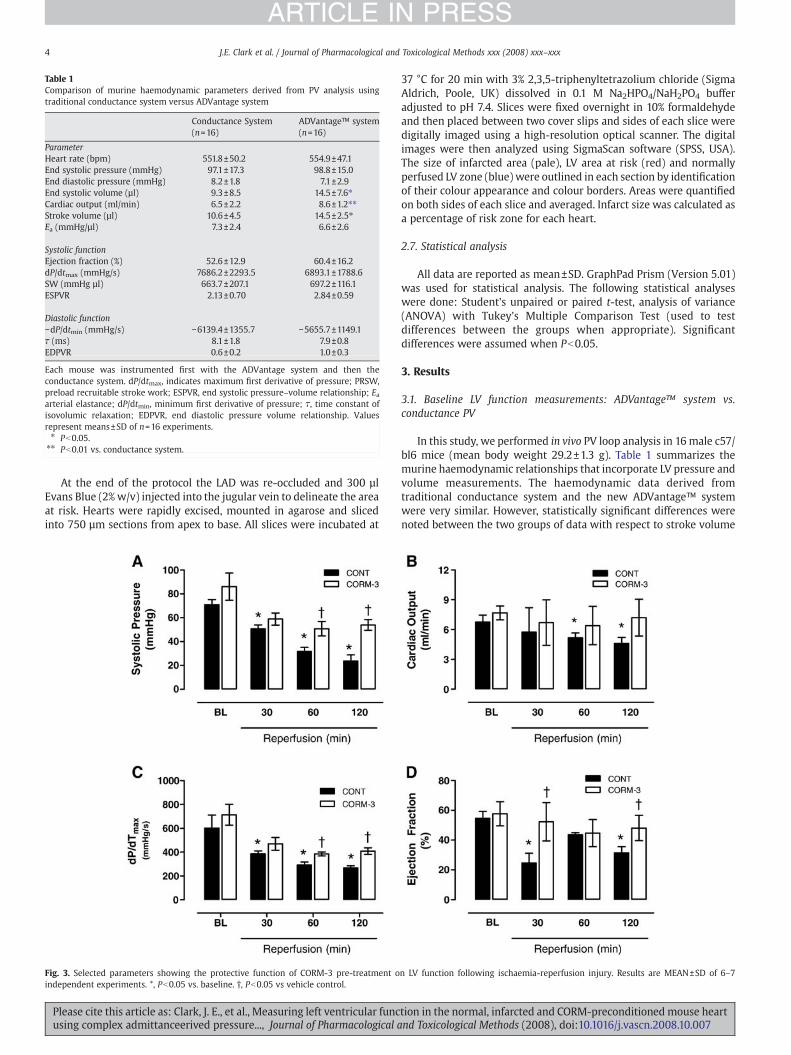
Table 1Comparison of murine haemodynamic parameters derived from PV analysis usingtraditional conductance system versus ADVantage system
Conductance System(n=16)
ADVantage™ system(n=16)
ParameterHeart rate (bpm) 551.8±50.2 554.9±47.1End systolic pressure (mmHg) 97.1±17.3 98.8±15.0End diastolic pressure (mmHg) 8.2±1.8 7.1±2.9End systolic volume (µl) 9.3±8.5 14.5±7.6⁎Cardiac output (ml/min) 6.5±2.2 8.6±1.2⁎⁎Stroke volume (µl) 10.6±4.5 14.5±2.5⁎Ea (mmHg/µl) 7.3±2.4 6.6±2.6
Systolic functionEjection fraction (%) 52.6±12.9 60.4±16.2dP/dtmax (mmHg/s) 7686.2±2293.5 6893.1±1788.6SW (mmHg µl) 663.7±207.1 697.2±116.1ESPVR 2.13±0.70 2.84±0.59
Diastolic function−dP/dtmin (mmHg/s) −6139.4±1355.7 −5655.7±1149.1τ (ms) 8.1±1.8 7.9±0.8EDPVR 0.6±0.2 1.0±0.3
Each mouse was instrumented first with the ADVantage system and then theconductance system. dP/dtmax, indicates maximum first derivative of pressure; PRSW,preload recruitable stroke work; ESPVR, end systolic pressure–volume relationship; Eaarterial elastance; dP/dtmin, minimum first derivative of pressure; τ, time constant ofisovolumic relaxation; EDPVR, end diastolic pressure volume relationship. Valuesrepresent means±SD of n=16 experiments.⁎ Pb0.05.⁎⁎ Pb0.01 vs. conductance system.
4 J.E. Clark et al. / Journal of Pharmacological and Toxicological Methods xxx (2008) xxx–xxx
ARTICLE IN PRESS
At the end of the protocol the LAD was re-occluded and 300 µlEvans Blue (2% w/v) injected into the jugular vein to delineate the areaat risk. Hearts were rapidly excised, mounted in agarose and slicedinto 750 µm sections from apex to base. All slices were incubated at
Fig. 3. Selected parameters showing the protective function of CORM-3 pre-treatment oindependent experiments. *, Pb0.05 vs. baseline. †, Pb0.05 vs vehicle control.
Please cite this article as: Clark, J. E., et al., Measuring left ventricular funcusing complex admittanceerived pressure..., Journal of Pharmacological a
37 °C for 20 min with 3% 2,3,5-triphenyltetrazolium chloride (SigmaAldrich, Poole, UK) dissolved in 0.1 M Na2HPO4/NaH2PO4 bufferadjusted to pH 7.4. Slices were fixed overnight in 10% formaldehydeand then placed between two cover slips and sides of each slice weredigitally imaged using a high-resolution optical scanner. The digitalimages were then analyzed using SigmaScan software (SPSS, USA).The size of infarcted area (pale), LV area at risk (red) and normallyperfused LV zone (blue) were outlined in each section by identificationof their colour appearance and colour borders. Areas were quantifiedon both sides of each slice and averaged. Infarct size was calculated asa percentage of risk zone for each heart.
2.7. Statistical analysis
All data are reported as mean±SD. GraphPad Prism (Version 5.01)was used for statistical analysis. The following statistical analyseswere done: Student's unpaired or paired t-test, analysis of variance(ANOVA) with Tukey's Multiple Comparison Test (used to testdifferences between the groups when appropriate). Significantdifferences were assumed when Pb0.05.
3. Results
3.1. Baseline LV function measurements: ADVantage™ system vs.conductance PV
In this study, we performed in vivo PV loop analysis in 16male c57/bl6 mice (mean body weight 29.2±1.3 g). Table 1 summarizes themurine haemodynamic relationships that incorporate LV pressure andvolume measurements. The haemodynamic data derived fromtraditional conductance system and the new ADVantage™ systemwere very similar. However, statistically significant differences werenoted between the two groups of data with respect to stroke volume
n LV function following ischaemia-reperfusion injury. Results are MEAN±SD of 6–7
tion in the normal, infarcted and CORM-preconditioned mouse heartnd Toxicological Methods (2008), doi:10.1016/j.vascn.2008.10.007
5J.E. Clark et al. / Journal of Pharmacological and Toxicological Methods xxx (2008) xxx–xxx
ARTICLE IN PRESS
(SV), end systolic volume and cardiac output (CO) which were allsignificantly higher in the ADVantage™ data set and their respectivestandard deviations were less.
3.2. LV function following MI: cardioprotective actions of CORM-3
Having established that the Advantage™ system was capable ofgeneratingphysiological data (above)with highfidelity our next aimwasto determine whether the same system was able to determine thechanges in LV function following MI with or without prior treatmentwith a cardioprotective agent. Many studies have described the use ofconductance catheters to determine LV function following myocardialischaemia with, or without, reperfusion (Clark et al., 2007; Lips et al.,2004; Shioura, Geenen, & Goldspink, 2007; Winter et al., 2008);therefore, in the interest of minimizing the number of mice used in thepresent study we used only the ADVantage™ system to assess LVfunction in a mouse model of myocardial infarction. Apart from a smalldecrease in systolic pressure immediately subsequent to CORM-3administration (data not shown) there were no other recorded effects
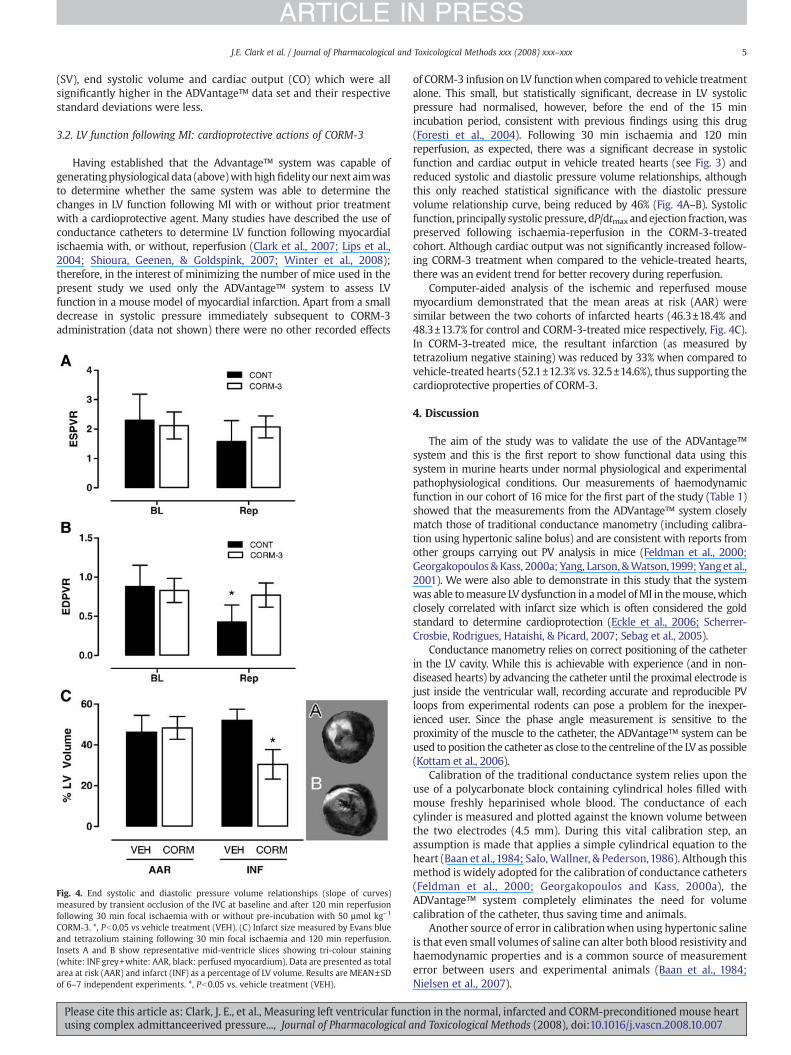
Fig. 4. End systolic and diastolic pressure volume relationships (slope of curves)measured by transient occlusion of the IVC at baseline and after 120 min reperfusionfollowing 30 min focal ischaemia with or without pre-incubation with 50 µmol kg−1
CORM-3. *, Pb0.05 vs vehicle treatment (VEH). (C) Infarct size measured by Evans blueand tetrazolium staining following 30 min focal ischaemia and 120 min reperfusion.Insets A and B show representative mid-ventricle slices showing tri-colour staining(white: INF grey+white: AAR, black: perfused myocardium). Data are presented as totalarea at risk (AAR) and infarct (INF) as a percentage of LV volume. Results are MEAN±SDof 6–7 independent experiments. *, Pb0.05 vs. vehicle treatment (VEH).
Please cite this article as: Clark, J. E., et al., Measuring left ventricular funcusing complex admittanceerived pressure..., Journal of Pharmacological a
of CORM-3 infusion on LV functionwhen compared to vehicle treatmentalone. This small, but statistically significant, decrease in LV systolicpressure had normalised, however, before the end of the 15 minincubation period, consistent with previous findings using this drug(Foresti et al., 2004). Following 30 min ischaemia and 120 minreperfusion, as expected, there was a significant decrease in systolicfunction and cardiac output in vehicle treated hearts (see Fig. 3) andreduced systolic and diastolic pressure volume relationships, althoughthis only reached statistical significance with the diastolic pressurevolume relationship curve, being reduced by 46% (Fig. 4A–B). Systolicfunction, principally systolic pressure, dP/dtmax andejection fraction,waspreserved following ischaemia-reperfusion in the CORM-3-treatedcohort. Although cardiac output was not significantly increased follow-ing CORM-3 treatment when compared to the vehicle-treated hearts,there was an evident trend for better recovery during reperfusion.
Computer-aided analysis of the ischemic and reperfused mousemyocardium demonstrated that the mean areas at risk (AAR) weresimilar between the two cohorts of infarcted hearts (46.3±18.4% and48.3±13.7% for control and CORM-3-treated mice respectively, Fig. 4C).In CORM-3-treated mice, the resultant infarction (as measured bytetrazolium negative staining) was reduced by 33% when compared tovehicle-treated hearts (52.1±12.3% vs. 32.5±14.6%), thus supporting thecardioprotective properties of CORM-3.
4. Discussion
The aim of the study was to validate the use of the ADVantage™system and this is the first report to show functional data using thissystem in murine hearts under normal physiological and experimentalpathophysiological conditions. Our measurements of haemodynamicfunction in our cohort of 16 mice for the first part of the study (Table 1)showed that the measurements from the ADVantage™ system closelymatch those of traditional conductance manometry (including calibra-tion using hypertonic saline bolus) and are consistent with reports fromother groups carrying out PV analysis in mice (Feldman et al., 2000;Georgakopoulos &Kass, 2000a; Yang, Larson, &Watson,1999; Yanget al.,2001). We were also able to demonstrate in this study that the systemwas able tomeasure LV dysfunction in amodel ofMI in themouse,whichclosely correlated with infarct size which is often considered the goldstandard to determine cardioprotection (Eckle et al., 2006; Scherrer-Crosbie, Rodrigues, Hataishi, & Picard, 2007; Sebag et al., 2005).
Conductance manometry relies on correct positioning of the catheterin the LV cavity. While this is achievable with experience (and in non-diseased hearts) by advancing the catheter until the proximal electrode isjust inside the ventricular wall, recording accurate and reproducible PVloops from experimental rodents can pose a problem for the inexper-ienced user. Since the phase angle measurement is sensitive to theproximity of the muscle to the catheter, the ADVantage™ system can beused to position the catheter as close to the centreline of the LV as possible(Kottam et al., 2006).
Calibration of the traditional conductance system relies upon theuse of a polycarbonate block containing cylindrical holes filled withmouse freshly heparinised whole blood. The conductance of eachcylinder is measured and plotted against the known volume betweenthe two electrodes (4.5 mm). During this vital calibration step, anassumption is made that applies a simple cylindrical equation to theheart (Baan et al., 1984; Salo,Wallner, & Pederson,1986). Although thismethod is widely adopted for the calibration of conductance catheters(Feldman et al., 2000; Georgakopoulos and Kass, 2000a), theADVantage™ system completely eliminates the need for volumecalibration of the catheter, thus saving time and animals.
Another source of error in calibrationwhen using hypertonic salineis that even small volumes of saline can alter both blood resistivity andhaemodynamic properties and is a common source of measurementerror between users and experimental animals (Baan et al., 1984;Nielsen et al., 2007).
tion in the normal, infarcted and CORM-preconditioned mouse heartnd Toxicological Methods (2008), doi:10.1016/j.vascn.2008.10.007

6 J.E. Clark et al. / Journal of Pharmacological and Toxicological Methods xxx (2008) xxx–xxx
ARTICLE IN PRESS
In addition, there is controversy in the literature relating to thecontribution of the myocardium (parallel conductance) during thecardiac cycle (Baan et al., 1984; Georgakopoulos et al., 1998; Georgako-poulos & Kass, 2000b; Lankford, Kass, Maughan, & Shoukas, 1990), butrecent compelling evidence suggests that parallel conductance variesbetween end-systole and end-diastole (Wei et al., 2007). Measurementof LV haemodynamic function using complex admittance eliminates theneed for saline bolus injection or other interventions since thesimultaneous measurement of magnitude and phase angle candetermine the instantaneous parallel myocardial contribution to thetotalmeasured admittance throughout the cardiac cycle. This effectivelyremoves errors resulting fromparallel conductancevariationwithphaseof the cardiac cycle and haemodynamic effects of hypertonic saline.
When the acquired values for stroke volume (SV), cardiac output(CO) and end systolic pressure in the two systems are compared, theADVantage™ system consistently recorded significantly higher valueswith a smaller associated standard deviation (variability, see Table 1). Itis likely that this is directly related to omitting the estimation of parallelconductance for calibrating the LV volume using hypertonic saline.
Although every effort was made in this study to reduce dehydra-tion of the animal blood volume loss between the two measurements,this cannot be completely excluded as an explanation for the reducedsystolic volume, SV and CO measurements. Although not addresseddirectly in this study, this may suggest that the new technology mayaid in the reduction of group sizes for certain studies and thereforeprovide a more cost effective solution for assessing LV function.
Left anterior descending (LAD) coronary artery ligation is the preferredand acceptable model of infarction and heart failure in mice (Fisher &Marber, 2002; Michael et al., 1995). In this study the ADVantage™ systemperformed well when assessing LV function following infarction.Significant reductions in systolic pressure, dP/dtmax and ejection fractionand cardiac output were measured which were attenuated (at 120 minreperfusion) in the mice pre-treated with CORM-3, these data show asimilar cardioprotective effect to those shownpreviously although inpriorstudies CORM-3 was administered at the time of reperfusion (Guo et al.,2004).
Assessment of LV function by micro conductance manometry isbecoming commonplace in rodent models of cardiac dysfunction. Theuse of complex admittance represents a technological advance allowingfor accurate and reproducible assessment of left ventricular functionwithout the need for complex interventions to ensure calibration.
Acknowledgement
JEC is funded by the British Heart Foundation (FS/06/026).
References
Baan, J., van der Velde, E. T., de Bruin, H. G., Smeenk, G. J., Koops, J., van Dijk, A. D., et al.(1984). Continuous measurement of left ventricular volume in animals and humansby conductance catheter. Circulation, 70(5), 812−823.
Balaban, R. S., & Hampshire, V. A. (2001). Challenges in small animal noninvasiveimaging. ILAR Journal, 42(3), 248−262.
Burkhoff, D., Mirsky, I., & Suga, H. (2005). Assessment of systolic and diastolicventricular properties via pressure–volume analysis: A guide for clinical, transla-tional, and basic researchers. American Journal of Physiology Heart and CirculatoryPhysiology, 289(2), H501−H512.
Chatterjee, P. K. (2004). Water-soluble carbon monoxide-releasing molecules: Helpingto elucidate the vascular activity of the ‘silent killer’. British Journal of Pharmacology,142(3), 391−393.
Clark, J. E., Flavell, R. A., Faircloth, M. E., Davis, R. J., Heads, R. J., & Marber, M. S. (2007). Post-infarction remodeling is independent of mitogen-activated protein kinase kinase 3(MKK3). Cardiovascular Research, 74(3), 466−470.
Clark, J. E., Naughton, P., Shurey, S., Green, C. J., Johnson, T. R., Mann, B. E., et al. (2003).Cardioprotective actions by a water-soluble carbon monoxide-releasing molecule.Circulation Research, 93(2), e2−e8.
Eckle, T., Grenz, A., Kohler, D., Redel, A., Falk, M., Rolauffs, B., et al. (2006). Systematicevaluation of a novel model for cardiac ischemic preconditioning in mice. AmericanJournal of Physiology Heart and Circulatory Physiology, 291(5), H2533−H2540.
Feldman, M. D., Erikson, J. M., Mao, Y., Korcarz, C. E., Lang, R. M., & Freeman, G. L. (2000).Validation of a mouse conductance system to determine LV volume: Comparison to
Please cite this article as: Clark, J. E., et al., Measuring left ventricular funcusing complex admittanceerived pressure..., Journal of Pharmacological a
echocardiography and crystals. American Journal of Physiology. Heart and CirculatoryPhysiology, 279(4), H1698−H1707.
Fisher, S. G., & Marber, M. S. (2002). An in vivo model of ischaemia-reperfusion injuryand ischaemic preconditioning in the mouse heart. Journal of Pharmacological andToxicological Methods, 48(3), 161−169.
Foresti, R., Hammad, J., Clark, J. E., Johnson, T. R., Mann, B. E., Friebe, A., et al. (2004).Vasoactive properties of CORM-3, a novel water-soluble carbon monoxide-releasingmolecule. British Journal of Pharmacology, 142(3), 453−460.
Georgakopoulos, D., & Kass, D. A. (2000). Estimation of parallel conductance by dual-frequency conductance catheter in mice. American Journal of Physiology Heart andCirculatory Physiology, 279(1), H443−H450.
Georgakopoulos, D., & Kass, D. A. (2000). Estimation of parallel conductance by dual-frequency conductance catheter in mice. American Journal of Physiology Heart andCirculatory Physiology, 279(1), H443−H450.
Georgakopoulos,D.,Mitzner,W.A., Chen, C.H., Byrne, B. J.,Millar, H.D., Hare, J.M., et al. (1998).In vivo murine left ventricular pressure–volume relations by miniaturized conductancemicromanometry. American Journal of Physiology, 274(4 Pt 2), H1416−H1422.
Guo, Y., Stein, A. B.,Wu,W. J., Tan,W., Zhu, X., Li, Q. H., et al. (2004). Administration of a CO-releasing molecule at the time of reperfusion reduces infarct size in vivo. AmericanJournal of Physiology Heart and Circulatory Physiology, 286(5), H1649−H1653.
James, J. F., Hewett, T. E., & Robbins, J. (1998). Cardiac physiology in transgenic mice.Circulation Research, 82(4), 407−415.
Kottam, A., & Pearce, J. A. (2004). Electric field penetration depth of myocardial surfacecatheters and the measurement of myocardial resistivity. Biomedical SciencesInstrumentation, 40, 155−160.
Kottam, A. T., Porterfield, J., Raghavan, K., Fernandez, D., Feldman,M.D., Valvano, J.W., et al.(2006). Real time pressure–volume loops in mice using complex admittance:Measurement and implications. Conference Proceedings of the IEEE Engineering inMedicine and Biology Society, 1, 4336−4339.
Lankford, E. B., Kass, D. A., Maughan,W. L., & Shoukas, A. A. (1990). Does volume catheterparallel conductance vary during a cardiac cycle? American Journal of Physiology, 258(6 Pt 2), H1933−H1942.
Lips, D. J., Bueno, O. F., Wilkins, B. J., Purcell, N. H., Kaiser, R. A., Lorenz, J. N., et al. (2004).MEK1-ERK2 signaling pathway protects myocardium from ischemic injury in vivo.Circulation, 109(16), 1938−1941.
Michael, L. H., Entman, M. L., Hartley, C. J., Youker, K. A., Zhu, J., Hall, S. R., et al. (1995).Myocardial ischemia and reperfusion: A murine model. American Journal ofPhysiology, 269(6 Pt 2), H2147−H2154.
Nielsen, J.M., Kristiansen,S. B., Ringgaard, S.,Nielsen,T. T., Flyvbjerg,A., Redington,A.N., et al.(2007). Left ventricular volume measurement in mice by conductance catheter:Evaluation and optimization of calibration. American Journal of Physiology Heart andCirculatory Physiology, 293(1), H534−H540.
Pacher, P., Nagayama, T., Mukhopadhyay, P., Batkai, S., & Kass, D. A. (2008). Measurementof cardiac function using pressure–volume conductance catheter technique in miceand rats. Nature Protocol, 3(9), 1422−1434.
Raghavan, K., Wei, C. L., Kottam, A., Altman, D. G., Fernandez, D. J., Reyes, M., et al.(2004). Design of instrumentation and data-acquisition system for complexadmittance measurement. Biomedical Sciences Instrumentation, 40, 453−457.
Rottman, J. N., Ni, G., & Brown, M. (2007). Echocardiographic evaluation of ventricularfunction in mice. Echocardiography, 24(1), 83−89.
Salo, R. W., Wallner, T. G., & Pederson, B. D. (1986). Measurement of ventricular volumeby intracardiac impedance: Theoretical and empirical approaches. IEEE Transactionson Biomedical Engineering, 33(2), 189−195.
Scherrer-Crosbie, M., Rodrigues, A. C., Hataishi, R., & Picard, M. H. (2007). Infarct sizeassessment in mice. Echocardiography, 24(1), 90−96.
Sebag, I. A., Handschumacher, M. D., Ichinose, F., Morgan, J. G., Hataishi, R., Rodrigues, A. C.,et al. (2005). Quantitative assessmentof regionalmyocardial function inmice by tissueDoppler imaging: Comparisonwith hemodynamics and sonomicrometry. Circulation,111(20), 2611−2616.
Shioura, K.M., Geenen, D. L., & Goldspink, P. H. (2007). Assessment of cardiac functionwiththe pressure–volume conductance system following myocardial infarction in mice.American Journal of Physiology Heart and Circulatory Physiology, 293(5), H2870−H2877.
Tam, C. W., Husmann, K., Clark, N. C., Clark, J. E., Lazar, Z., Ittner, L. M., et al. (2005).Enhanced vascular responses to adrenomedullin in mice overexpressing receptor-activity-modifying protein 2. Circulation Research, 98(2), 262−270.
Uemura, K., Sugimachi, M., Shishido, T., Kawada, T., Inagaki, M., Zheng, C., et al. (2002).Convenient automated conductance volumetric system. Japanese Journal of Physiology,52(5), 497−503.
van Oosterom, A. F., de Boer, R. W., & van Dam, R. T. (1979). Intramural resistivity ofcardiac tissue. Medical & Biological Engineering & Computing, 17(3), 337−343.
Wei, C. L., Valvano, J. W., Feldman, M. D., Nahrendorf, M., Peshock, R., & Pearce, J. A.(2007). Volume catheter parallel conductance varies between end-systole and end-diastole. IEEE Transactions on Biomedical Engineering, 54(8), 1480−1489.
Wei, C. L., Valvano, J. W., Feldman, M. D., & Pearce, J. A. (2005). Nonlinear conductance–volume relationship for murine conductance catheter measurement system. IEEETransactions on Biomedical Engineering, 52(10), 1654−1661.
Winter, E. M., Grauss, R. W., Atsma, D. E., Hogers, B., Poelmann, R. E., van der Geest, R. J.,et al. (2008). Left ventricular function in the post-infarct failing mouse heart bymagnetic resonance imaging and conductance catheter: A comparative analysis.Acta Physiologica (Oxf), 194(2), 111−122.
Yang, B., Larson, D. F., Beischel, J., Kelly, R., Shi, J., & Watson, R. R. (2001). Validation ofconductance catheter system for quantification of murine pressure–volume loops.Journal of Investigative Surgery, 14(6), 341−355.
Yang, B., Larson, D. F., & Watson, R. (1999). Age-related left ventricular function in themouse: Analysis based on in vivo pressure–volume relationships. American Journalof Physiology, 277(5 Pt 2), H1906−H1913.
tion in the normal, infarcted and CORM-preconditioned mouse heartnd Toxicological Methods (2008), doi:10.1016/j.vascn.2008.10.007
Copyright © 2022 FDOKUMEN




















