
Management of spinal dural arteriovenous fistulae with emphasis on an endovascular approach
6
Clinical Neurology and Neurosurgery 125 (2014) 81–86 Contents lists available at ScienceDirect Clinical Neurology and Neurosurgery journal homepage: www.elsevier.com/locate/clineuro Review Management of spinal dural arterio-venous fistulas. Report of 12 cases and review of literature Sherif Rashad, Mohamed Abdel-Bary, Waseem Aziz, Tamer Hassan ∗ Department of Neurosurgery, Alexandria University School of Medicine, Alexandria, Egypt article info Article history: Received 4 May 2014 Received in revised form 29 June 2014 Accepted 20 July 2014 Available online 27 July 2014 Keywords: Arteriovenous fistula Myelopathy Spinal arteriovenous fistula Spinal vascular malformation abstract Introduction: Spinal cord arteriovenous malformations and fistulae are rare vascular lesions than can lead to myelopathy that is at many instances overlooked during diagnosing the cause of progressive myelopathy and weakness. Treatment options involve either endovascular embolization, surgical dis- connection or a combination of both. This study aims to evaluate various treatment methods for sDAVFs and the outcome of these methods. Methods: This study involved 12 patients suffering from symptoms attributed to spinal dural arteriove- nous fistulas; 11 were male and one was a female patient, with ages ranging between 50 years and 71 years. All patients presented with progressive spastic paraparesis of varying grades, and 6 had sphincter disturbances prior to treatment. Patients were evaluated by Aminoff-Logue motor disability scale. Results: Three were managed by endovascular embolization and 9 by surgical disconnection. Three patients showed full recovery after treatment, 7 patients showed no change in their neurological status following treatment, and 2 patients showed partial recovery after treatment. Conclusion: Spinal AVF is a rare curable cause of spinal myelopathy if managed promptly. Good angiog- raphic studies prior to treatment decision are a must, in order to plan the best approach according to the angioarchitecture of the fistula whether it will allow endovascular embolization or will surgery be more feasible. © 2014 Elsevier B.V. All rights reserved. Contents 1. Introduction .......................................................................................................................................... 81 2. Materials and methods ............................................................................................................................... 82 3. Results ................................................................................................................................................ 83 3.1. Patient examples .............................................................................................................................. 83 4. Discussion ............................................................................................................................................ 84 5. Conclusion ............................................................................................................................................ 86 References ............................................................................................................................................ 86 1. Introduction Spine and spinal cord vascular lesions are rare vascular lesions, only representing 1–2% of the vascular neurologic pathologies [1], Abbreviations: AVF, arterio-venous fistula; sdAVF, spinal dural arterio-venous fistula. ∗ Corresponding author. Tel.: +20 3 5439341/111 2244524; fax: +20 3 5424756. E-mail addresses: [email protected], [email protected] (T. Hassan). with spinal dural AVF being the most common representing 80% of the spinal vascular malformation [2–5]. Spinal dural AVFs classically present by progressive spas- tic motor weakness, other symptoms include sensory deficits, sphincter disturbances and back pain [3,6–9] with some patients presenting acutely due to hemorrhage or due to Foix-Alajouanine syndrome [6,7]. The pathophysiology of symptoms is typically venous hypertension from shunting of the arterial blood into the valveless venous system of the spinal cord, which causes a decrease in the arterial supply, arterial steal and ischemia, leading to progres- sive necrotizing myelopathy that, if not treated, is non-reversible [1,6,10,11]. http://dx.doi.org/10.1016/j.clineuro.2014.07.028 0303-8467/© 2014 Elsevier B.V. All rights reserved.
Transcript of Management of spinal dural arteriovenous fistulae with emphasis on an endovascular approach

R
Mc
SD
a
ARRAA
KAMSS
C
1
o
fi
(
h0
Clinical Neurology and Neurosurgery 125 (2014) 81–86
Contents lists available at ScienceDirect
Clinical Neurology and Neurosurgery
journa l homepage: www.e lsev ier .com/ locate /c l ineuro
eview
anagement of spinal dural arterio-venous fistulas. Report of 12ases and review of literature
herif Rashad, Mohamed Abdel-Bary, Waseem Aziz, Tamer Hassan ∗
epartment of Neurosurgery, Alexandria University School of Medicine, Alexandria, Egypt
r t i c l e i n f o
rticle history:eceived 4 May 2014eceived in revised form 29 June 2014ccepted 20 July 2014vailable online 27 July 2014
eywords:rteriovenous fistulayelopathy
pinal arteriovenous fistulapinal vascular malformation
a b s t r a c t
Introduction: Spinal cord arteriovenous malformations and fistulae are rare vascular lesions than canlead to myelopathy that is at many instances overlooked during diagnosing the cause of progressivemyelopathy and weakness. Treatment options involve either endovascular embolization, surgical dis-connection or a combination of both. This study aims to evaluate various treatment methods for sDAVFsand the outcome of these methods.Methods: This study involved 12 patients suffering from symptoms attributed to spinal dural arteriove-nous fistulas; 11 were male and one was a female patient, with ages ranging between 50 years and 71years. All patients presented with progressive spastic paraparesis of varying grades, and 6 had sphincterdisturbances prior to treatment. Patients were evaluated by Aminoff-Logue motor disability scale.Results: Three were managed by endovascular embolization and 9 by surgical disconnection. Threepatients showed full recovery after treatment, 7 patients showed no change in their neurological status
following treatment, and 2 patients showed partial recovery after treatment.Conclusion: Spinal AVF is a rare curable cause of spinal myelopathy if managed promptly. Good angiog-raphic studies prior to treatment decision are a must, in order to plan the best approach according to theangioarchitecture of the fistula whether it will allow endovascular embolization or will surgery be morefeasible.© 2014 Elsevier B.V. All rights reserved.
ontents
1. Introduction . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 812. Materials and methods . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 823. Results . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 83
3.1. Patient examples . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 834. Discussion . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 845. Conclusion . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 86
References . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 86
. Introductionwith spinal dural AVF being the most common representing 80% ofthe spinal vascular malformation [2–5].
Spine and spinal cord vascular lesions are rare vascular lesions,nly representing 1–2% of the vascular neurologic pathologies [1],
Abbreviations: AVF, arterio-venous fistula; sdAVF, spinal dural arterio-venousstula.∗ Corresponding author. Tel.: +20 3 5439341/111 2244524; fax: +20 3 5424756.
E-mail addresses: [email protected], [email protected]. Hassan).
ttp://dx.doi.org/10.1016/j.clineuro.2014.07.028303-8467/© 2014 Elsevier B.V. All rights reserved.
Spinal dural AVFs classically present by progressive spas-tic motor weakness, other symptoms include sensory deficits,sphincter disturbances and back pain [3,6–9] with some patientspresenting acutely due to hemorrhage or due to Foix-Alajouaninesyndrome [6,7]. The pathophysiology of symptoms is typicallyvenous hypertension from shunting of the arterial blood into thevalveless venous system of the spinal cord, which causes a decrease
in the arterial supply, arterial steal and ischemia, leading to progres-sive necrotizing myelopathy that, if not treated, is non-reversible[1,6,10,11].
8 y and
brtw
mwa
2
bwypt
s[
swa
TA
M
2 S. Rashad et al. / Clinical Neurolog
Surgery is widely accepted as a treatment option for dural AVF,eing technically easy and carrying a low morbidity and low recur-ence rates. Advances in endovascular techniques and therapy ledo the increasing number of patients being treated by embolizationith good outcomes increasingly being reported [3,5,6,12–14].
In this article we report our experience with the diagnosis andanagement of 12 cases of spinal dural arterio-venous fistulas,ith review of the literature covering the diagnosis, management
nd outcome of this rare vascular pathology.
. Materials and methods
This study included 12 patients, managed for spinal fistulasetween 2006 and 2013 for spinal dural AVFs (Table 1). Patientsere all males, except 1, with age ranging from 50 years to 71
ears, with median age of 56 years. All patients presented withrogressive spastic motor weakness with or without sphincter dis-urbances.
Clinical evaluation: Patients were evaluated by Aminouff-Lougecore at the time of hospitalization and at follow-up (Tables 1 and 2)15].
Diagnostic workup: Upon clinical suspicion of the presence ofpinal vascular pathology patients were evaluated by MRI with andithout contrast. Typical features of spinal fistulae were present in
ll cases as signal voids, cord hyperintensity on T2 images, and cord
able 1ll cases included in the study.
No Age Sex Presentation Diagnosis Tr
1 61 M Paraplegia, myelopathy,sphincter disturbances
Left dural AVF at D9 Su
2 71 M Progressive spasticparaparesis, sphincterdisturbances
Right dural AVF at D12 Enw
3 50 M Progressive spasticparaparesis
Left dural AVF at D10 Enaninrigdi
4 54 M Progressive spasticparaparesis, sphincterdisturbances
Right dural AVF at D11 Su
5 67 M Progressive spasticparaparesis, sphincterdisturbances
Right dural AVF at L5(origination from rightlateral sacral arteryfrom right internal iliacartery)
Su
6 54 M Progressive spasticparaparesis
Left dural AVF at D9 Su
7 50 M Progressive weakness,paraplegic, sphincterdisturbances
Right dural AVF at D10 Su
8 50 M Spastic paraplegia,sphincter disturbances
Left dural AVF at D9 Enwfro
9 60 F Spastic paraparesis,sphincter disturbances
Right dural AVF at S1(origination from rightlateral sacral arteryfrom right internal iliacartery)
Su
10 53 M Progressive spasticparaparesis
Right dural AVF at L1 Su
11 53 M Progressive spasticparaparesis, sphincterdisturbances
Right dural AVF at L1 Su
12 50 M Progressive spasticparaparesis
Left dural AVF at L1 Su
O: motor outcome; G: motor power grade; O: outcome; P: poor, M: moderate, G: good;
Neurosurgery 125 (2014) 81–86
enhancement with gadolinium. Upon recognition of these featureson MRI, patients were referred for spinal angiography.
Spinal angiography: Spinal angiography was performed undereither local, general anaesthesia or under sedation, depending onthe co-operativity of the patient, as it is a lengthy procedure exam-ining all the spinal vascular accesses. A 5 or 6 french femoral sheathis introduced, and a 5 or 4 french diagnostic catheter is used. Vari-able shapes of catheters are usually available during the procedures,the most commonly utilized shapes were the C-shape, SIM I andthe shepherd hook, as these shapes can easily be introduced intothe radicular branches supplying the spinal cord. The whole spinalvascular access is usually examined, starting from the internal iliacarteries, going up examining the right and left radicular arteries,both vertebrals and both thyrocervical trunks. This protocol is fol-lowed even if the fistula is observed at the lower levels, in order todiagnose associated lesions that can be missed. We also emphasizeon examining the levels above and below the fistula on both sidesso any additional feeders can be diagnosed and properly addressed.
Follow-up: Patients were followed clinically and by radiologicalinvestigations, the duration of follow-up ranged between 3 monthsand 2 years. In cases when the patient was not able to show upfor examination, phone interview was conducted and it involved
questioning the patient about his motor power, sensory changes,sphincter control, and ability to conduct daily activities. Patient’sanswers were compared with his last follow-up and so a chart ofpatient progression could be postulated.eatment ALS MO O SO
Pre-op Post-op
rgical disconnection 5 5 G0–G1 P NI
dovascular embolizationith glue
4 4 G3–G3 M NI
dovascular embolization (atotherstitute) → recanalization viaht D11 → surgical
sconnection
3 0 G4–G5 G –
rgical disconnection 5 4 G2–G3 M I
rgical disconnection 4 4 G3–G3 M NI
rgical disconnection 3 3 G4–G4 M –
rgical disconnection 5 5 G0–G0 p NI
dovascular embolizationith Onyx → recanalizationm left D10
5 5 G0–G0 P NI
rgical disconnection 5 5 G2–G2 P NI
rgical disconnection 3 0 G4–G5 G –
rgical disconnection 5 4 G2–G3 M I
rgical disconnection 3 3 G4–G4 M –
SO: sphincter outcome; I: improved, NI: not improved.
S. Rashad et al. / Clinical Neurology and
Table 2Aminoff motor disability scale [15].
Disability Degree
Hypesthesia without gait restriction 1Reduced tolerance to exercise 2Need a cane for walking 3
3
cofiwtrshiftrw(
ltii
Aapa
FDsw
Need for two canes or crutches to walk 4Inability to stand: patient in wheelchair or in bed 5
. Results
Treatment choices: Nine patients were managed by surgical dis-onnection of the dural fistula via a posterior approach as the firstption. Two were managed by endovascular embolization as therst option for treatment, one with glue (NBCA) (patient 2) and oneith Onyx (patient 8), and one patient was managed by emboliza-
ion with glue at another institute (patient 3), but suffered fromecanalization of the fistula as the glue did not reach to the fistulaite and the draining vein and settled in the feeding artery only;e was managed by surgical disconnection. During embolization
n patient 8 arterial spasm occurred, which prevented the Onyxrom reaching the vein, his follow-up showed recanalization ofhe fistula; he is scheduled for another endovascular session as heemains in a poor medical condition to undergo surgery. Patient 2as managed by endovascular embolization as he refused surgery
Table 1).Anatomical distribution of cases: All cases had their fistulas
ocated between D9 and L1 levels and the feeding artery was inhese cases a radicular artery. Two cases had their fistulas originat-ng from the lateral sacral artery which is a branch of the internalliac artery; one was present at L5 root and the other at S1 (Table 1).
Clinical outcome: Clinical outcome was evaluated based on
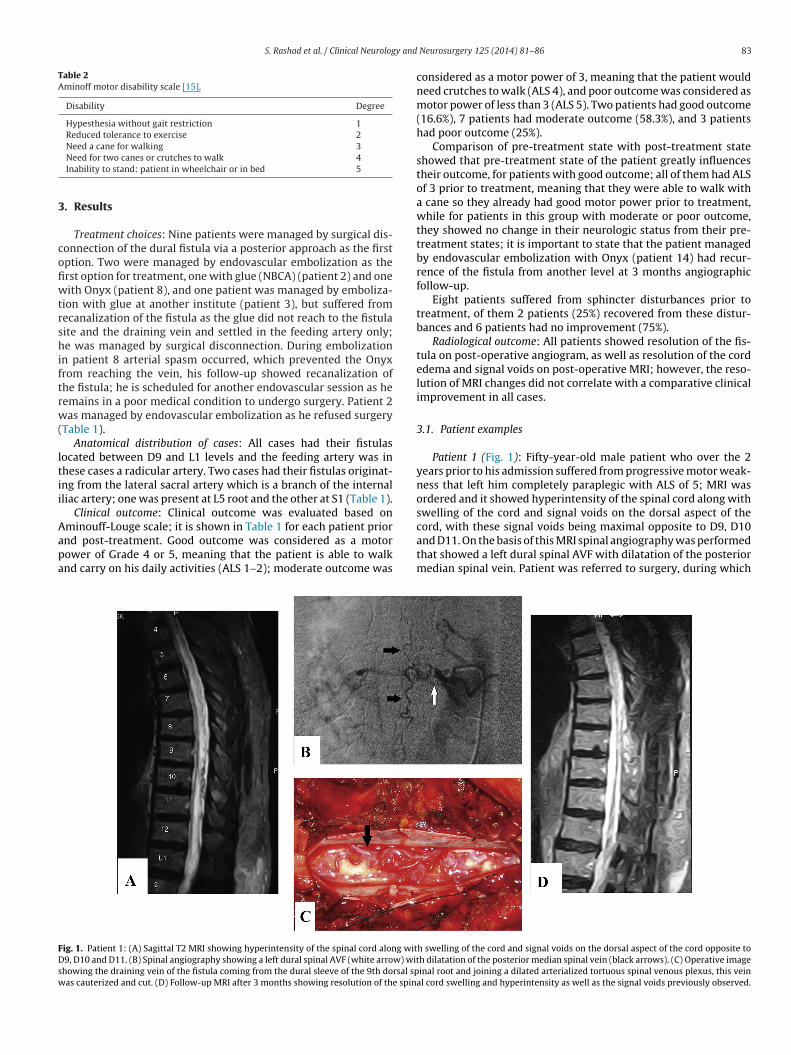
minouff-Louge scale; it is shown in Table 1 for each patient priornd post-treatment. Good outcome was considered as a motorower of Grade 4 or 5, meaning that the patient is able to walknd carry on his daily activities (ALS 1–2); moderate outcome wasig. 1. Patient 1: (A) Sagittal T2 MRI showing hyperintensity of the spinal cord along wit9, D10 and D11. (B) Spinal angiography showing a left dural spinal AVF (white arrow) wit
howing the draining vein of the fistula coming from the dural sleeve of the 9th dorsal spas cauterized and cut. (D) Follow-up MRI after 3 months showing resolution of the spin
Neurosurgery 125 (2014) 81–86 83
considered as a motor power of 3, meaning that the patient wouldneed crutches to walk (ALS 4), and poor outcome was considered asmotor power of less than 3 (ALS 5). Two patients had good outcome(16.6%), 7 patients had moderate outcome (58.3%), and 3 patientshad poor outcome (25%).
Comparison of pre-treatment state with post-treatment stateshowed that pre-treatment state of the patient greatly influencestheir outcome, for patients with good outcome; all of them had ALSof 3 prior to treatment, meaning that they were able to walk witha cane so they already had good motor power prior to treatment,while for patients in this group with moderate or poor outcome,they showed no change in their neurologic status from their pre-treatment states; it is important to state that the patient managedby endovascular embolization with Onyx (patient 14) had recur-rence of the fistula from another level at 3 months angiographicfollow-up.
Eight patients suffered from sphincter disturbances prior totreatment, of them 2 patients (25%) recovered from these distur-bances and 6 patients had no improvement (75%).
Radiological outcome: All patients showed resolution of the fis-tula on post-operative angiogram, as well as resolution of the cordedema and signal voids on post-operative MRI; however, the reso-lution of MRI changes did not correlate with a comparative clinicalimprovement in all cases.
3.1. Patient examples
Patient 1 (Fig. 1): Fifty-year-old male patient who over the 2years prior to his admission suffered from progressive motor weak-ness that left him completely paraplegic with ALS of 5; MRI wasordered and it showed hyperintensity of the spinal cord along withswelling of the cord and signal voids on the dorsal aspect of the
cord, with these signal voids being maximal opposite to D9, D10and D11. On the basis of this MRI spinal angiography was performedthat showed a left dural spinal AVF with dilatation of the posteriormedian spinal vein. Patient was referred to surgery, during whichh swelling of the cord and signal voids on the dorsal aspect of the cord opposite toh dilatation of the posterior median spinal vein (black arrows). (C) Operative imageinal root and joining a dilated arterialized tortuous spinal venous plexus, this vein
al cord swelling and hyperintensity as well as the signal voids previously observed.

84 S. Rashad et al. / Clinical Neurology and
Fig. 2. Patient 10: (A) MRI lumbosacral spine showing signal voids extending alongthe cauda equina, with spinal cord hyperintensity with peripheral hypointensityidp
ttatsas
sotbesasvof
4
lr
as
nvolving the conus medullaris. (B) Spinal angiography showing a right L1 spinalural AVF. (C) Post-operative angiogram showing complete obliteration of the fistulareviously observed at the same level.
he radiculomedullary draining vein of the fistula was observedo be coming from the dural sleeve of the 9th dorsal spinal rootnd joining a dilated arterialized tortuous spinal venous plexus,his vein was cauterized and cut. Follow-up MRI after 3 monthshowed resolution of the spinal cord swelling and hyperintensitys well as the signal voids previously observed. The patient did nothow significant clinical improvement.
Patient 10 (Fig. 2): Fifty-three-year-old male patient who wasuffering from progressive spastic paraparesis over the coursef several months and was mistakenly diagnosed and receivedreatment for spondylosis and transverse myelitis. MRI of the lum-osacral spine showed signal voids extending along the caudaquina, with spinal cord hyperintensity with peripheral hypointen-ity involving the conus medullaris. Spinal angiography was donend it revealed a right L1 spinal dural AVF. Surgery was done bytandard posterior approach with disconnection of the drainingein of the fistula. Post-operative angiogram showed completebliteration of the fistula. The patient showed full recovery onollow-up.
. Discussion
Spinal Dural AVFs are a direct communication between a radicu-omeningeal artery and a radiculomedullary vein [11,16–19]. They
epresent 70–80% of all spinal vascular lesions [1,2,4,5,18].Etiology of sDAVF is generally idiopathic in most cases, butcquired cases following surgery or trauma are reported [6,9,20].DAVF occurs mostly in men over 40 years old, with male to
Neurosurgery 125 (2014) 81–86
female ratio 4:1; their most common site for occurrence is thethoraco-lumbar region, with cervical sDAVF being extremely rare[3,6,18,20–22].
The most common presentation of sDAVFs is progressivemotor weakness which is present in 85–95% of patients, withpatients often reporting worsening during physical exertion(neurogenic claudication); other associated symptoms include:numbness, pain, sphincteric disturbances and sexual dysfunction[1,3,4,6,11,18,20,23].
The pathophysiology of the fistula induced myelopathy is due toa rise in venous pressure caused by shunting of arterial blood intothe venous side, causing venous congestion in the valveless spinalcord veins, reducing spinal cord arterial perfusion pressure, ulti-mately leading to spinal cord ischemia and progressive necrotizingmyelopathy that is irreversible in its final stage [6,8,11].
This classical progressive course has its exceptions; 5–15% ofpatients with sDAVFs have episodes of acute exacerbation of theirsymptoms called the “Foix-Alajouanine syndrome”; these episodesare believed to be due to acute thrombosis of the pathologicalveins draining the fistula, deterioration is unpredictable, and unlesstreated immediately irreversible loss of neurologic function mightoccur [6]. Also a course of acute progressive development of the dis-ease interrupted by periods of remission has been reported [1,3]. Ifthe disease is not treated promptly it will lead to progressive neu-rologic decline, leading to severe disability usually over a course of2–3 years till complete paraplegia and incontinence [6] occurs.
The first radiological investigation that can give clues to theexistence of the disease is MRI; which often demonstrates a serpen-tine pattern of low signal in the subarachnoid space on Tl-weightedand T2-weighted images. This pattern of signal void is due to flow indilated, tortuous vessels of the arterialized coronal venous plexus.These arterialized pial veins may focally indent the cord surfaceand produce a scalloped appearance on sagittal Tl-weighted images[6,8,20]. These flow voids can be mimicked by CSF flow artifact andtherefore are not a 100% sure sign for the presence of spinal fistulaand should be accompanied by more a consistent finding for venoushypertensive myelopathy [7,20].
Tl-weighted and T2-weighted images will also reveal an areaof focal cord expansion, most commonly affecting the conus, witha central area of low or high signal with Tl-weighted images andincreased signal intensity with T2 imaging in the thoracolum-bar segments of a cord swollen from venous congestion [1,4,6];peripheral T2 hypointensity around the area of increased T2 signalintensity can help determine that the abnormal high signal is fromvenous hypertensive myelopathy rather than a tumor, demyelinat-ing process or other cause [20].
It has recently been suggested that this peripheral hypointen-sity on T2 images of the spinal cord is a consistent and specificdiagnostic feature of venous congestion associated with dural AVF[6].
Elimination of the spinal AVF results in a decrease in spinal cordswelling, induces resolution of the abnormal T2 hyperintensity inthe spinal cord, and eliminates enhancement of the abnormal ves-sels of the coronal venous plexus over the weeks or months aftersurgery [6,24].
Spinal angiography is the gold standard in the diagnosis of spinalvascular lesions; the angiographic study will delineate the type ofthe fistula clearly and with 100% certainty, the anatomic positionof the fistula, and its angioarchitecture, helping in classifying thelesion and proper diagnosis and so proper management plan canbe conducted [16,20]. The angiography should include thoroughassessment of the entire spinal vascular tree, from the vertebral
arteries and thyrocervical trunks down to the radicular arteriesof the aorta and the internal iliac arteries, in order to diagnoseassociated lesions or other feeders in cases of multiple fistulas. Agood understanding of the spinal vasculature is mandatory when
y and
ctbp
aioMespsb
vcts
thma[ctcpdmabvutbst[
iattr[faot
papewfiaw(ttifa
symptoms or new symptoms (usually sphincter disturbances) at
S. Rashad et al. / Clinical Neurolog
onducting spinal angiography, as fistulas can have rare feeders ashe lateral sacral artery of the internal iliac artery, which woulde missed otherwise; we encountered this rare supply in 2 of ouratients (patients 5 and 9) [2,6,11,16,20,25,26].
Van Rooij et al. [24] reported 5 cases with sDAVF withtypical MRI findings, absence of cord edema, swelling and hyper-ntensities; those patients were referred for investigations ofnly back pain, and all showed dilated perimedullary veins onRI with no other findings suggesting sDAVF. They were prop-
rly diagnosed with spinal angiography and treated with eitherurgery or endovascular embolization. This report states clearly thearamount important of doing a spinal angiography in cases withuspicious MRI of vascular pathology, as those patients would haveeen missed otherwise.
The goal of treatment in spinal fistulas is the elimination of theenous congestion, hence giving a chance for recovery of the spinalord, this can be achieved by excision, obliteration or disconnec-ion of the fistula, which can be accomplished endovascularly orurgically [6,27].
Operative treatment of sDAVF can be achieved via a pos-erior spinal approach, with laminectomy, laminoplasty, oremi-laminectomy. After midline dural opening the arterializededullary vein is identified and it almost always pierces the dural
t the site of the dural penetration of the posterior nerve root6,9]. Confirmation that this is the target vein that should be dis-onnected to eliminate the fistula can be achieved by comparinghe anatomy with the angiography and by observing the vesselrossing the subarachnoid space to join the dilated coronal venouslexus [6]. After that the vessel is coagulated by bipolar forceps andisconnected, the color of the arterialized coronal venous plexusay change from red to blue after few minutes, but this is not
lways the case [6,27]. The use of micro-doppler monitoring cane of aid in detecting changes of flow pattern in the arterializedeins before and after disconnection of the fistula; we routinelyse micro-doppler during surgery for sDAVF for confirmation ofhe site of the fistula as well as disconnection [28]. It shoulde noted that excessive stripping of the venous plexus from thepinal cord will only lead to exacerbation of the venous conges-ion rather than eliminating it, leading to unfavorable outcome6,27].
Endovascular therapy for spinal vascular malformations is gain-ng popularity each day, as better catheters, embolic materialsnd better understanding of the angioarchitecture has led to bet-er results and higher cure rates than before [12]. As for sDAVF,he ease of surgery for these lesions and the higher recurrenceate with endovascular embolization made surgical disconnection6,27] usually the preferred option. The most important causes ofailure of endovascular therapy for sDAVF are when the fistula isngiographically occult, presence of multiple small feeders, failuref the microcatheter to reach the site of the fistula and failure ofhe embolic material to hit the draining vein [6,23,27].
Endovascular embolization was used in the management of 3atients in this series; only one patient had angiographic cure,lthough he did not show comparative clinical cure, and in 2atients the treatment failed. Of the 2 patients who had failedndovascular treatment; one patient was managed by embolizationith glue at another institute (patient 3) and had recurrence of thestula, his angiogram showed the glue residing within the feedingrtery and not reaching the nidus or the vein; another patient whoas subjected to endovascular embolization attempt with Onyx
patient 8) had recurrence in his 3 months follow-up angiogram,he cause of this recurrence was that the Onyx did not diffuse intohe fistula and penetrate to reach the draining vein, due to a feed-
ng artery spasm during the procedure; this is a common cause ofailure as feeding artery of sDAVF is usually small as the fistula isslow-flow fistula [6,23,27]. The key for endovascular obliterationNeurosurgery 125 (2014) 81–86 85
of a spinal fistula is good penetration of the embolization materialinto the draining vein, otherwise recurrence will occur [3,5,12].
Success rate for endovascular therapy of sDAVF varies between25% and 75%, while that for surgery reaches up to 98%[3,4,14,18,29,30], with recurrence rate between 40% and 70%[14,19,30,31]. Westphal argued in his report that though endovas-cular embolization has a high recurrence rate it can be attemptedduring angiography, since a number of patients would benefit andbe cured and it is safe and non-invasive, he also mentioned that thepresence of the embolic material in the artery can help localizationof the feeder and vein during surgery [31].
The first embolic agent to be used for sDAVF was polyvinyl alco-hol, but because of the high recurrence rates associated with itsuse it was completely abandoned [5]. NBCA was used with goodresults provided that it reached the draining vein, otherwise therisk of fistula recurrence still exists; it is considered to be safe andeffective with good clinical outcomes [3,5,12,32]. Rodesch et al. [13]reported the embolization of spinal cord AVFs with glue (NBCA);they reported 16% anatomical obliteration of the fistula, reduc-tion of more than 50% in 86% of patients, and no recanalizationwas observed in their follow-up. They reported good clinical out-come in 83% of the patients (15% asymptomatic, 43% improvedand 25% stable), while in 4% the disease was not stabilized. Theyreported complications in the form of transient deficits in 14% oftheir patients after embolization, and permanent severe complica-tions occurred in 4%. Song et al. [33] reported NBCA embolizationof sDAVF in 27 patients, of those, embolization was not feasible in7, and in the remaining 20, 2 had initial embolization failure and3 had fistula recurrence, those 5 patients were surgically treated.Patients who were successfully embolized showed improved gaitin 55% of cases and unchanged gait in 45%, while micturition dis-ability improved in 40%, remained unchanged in 45% and worsenedin 15%.
Onyx has evolved in the past few years to be the first choice forembolization of cranial AVMs and AVFs, and increasingly is beingreported to be used with success in the management of spinal fistu-las [5]. Nogueira et al. [5] reported the use of Onyx for embolizationof sDAVF in 3 patients, he reported no evidence of residual or recur-rent sDAVF after treatment, and stated that Onyx embolization forsDAVF is feasible, safe and highly effective as it allows for controlledpenetration of the embolic agent into the draining vein, but withthe disadvantage of longer exposure time than with NBCA, and theusage of less flexible DMSO compatible microcatheter to deliver theembolic agent.
Even after successful treatment of sDAVF, only two-third ofall patients show improvement of their motor symptoms andone-third show improvements of other symptoms such as sen-sory disturbances, pain, impotence and sphincter disturbances[1,3,14,34]. This was consistent in our patients, as most presentedlate in the course of the disease and hence most of them did notexperience significant improvement after treatment regardless ofradiological cure.
From the reported series in the literature it seems that the mostimportant factors linked to good outcome are better pre-operativeneurologic condition and younger age of the patient [6,23,34]. Sal-adino et al. [9] in their report stated that out of their 154 patientssurgically treated for sDAVF, 82.2% showed some improvement and14.4% showed stabilization of their symptoms. They also stated thatsymptoms other than motor weakness are less likely to improve,as numbness improved in only 51.5% of cases, neuropathic pain in32.6% and sphincter disturbances in 45% of patients. 15% of patientsin their series experienced subjective or objective worsening in
discharge, and in 6% this worsening persisted at follow-up despitefistula obliteration on imaging, though a worsening in symptomsshould raise the suspicion of fistula recanalization.

8 y and
riplttn
5
nsb
dnem
ag
R
[
[
[
[
[
[
[
[
[
[
[
[
[
[
[
[
[
[
[
[
[
[
[
[butyl 2-cyanoacrylate embolization of spinal dural arteriovenous fistulae. Am
6 S. Rashad et al. / Clinical Neurolog
In addition to the previous data, Cenzato et al. [34] in theireported an additional factor which can affect the outcome, whichs the anatomical position of the fistula; they stated that fistulasresent between T6 and T12 have a better outcome than those
ocated in the upper thoracolumbar region, attributing this findingo the better blood supply of the thoracolumbar region comparedo the upper thoracic spinal cord; however, this observation wasot mentioned elsewhere in the literature.
. Conclusion
The key to successful treatment of spinal fistulas is proper plan-ing and investigations, from adequately identifying the clinicalymptoms of the disease to proper interpretation of MRI followedy good and detailed angiographic.
Surgery is usually the first choice in the management of spinalural arteriovenous fistulas, being highly efficient, technicallyot challenging and minimally invasive; however, endovascularmbolization can be used in certain subset of patients who areedically unfit for surgery or refuse surgery.Pre-treatment status of the patient is the most important factor
ffecting the outcome; therefore, prompt treatment is the key toood outcome.
eferences
[1] Krings T, Lasjaunias PL, Hans FJ, Mull M, Nijenhuis RJ, Alvarez H, et al. Imagingin spinal vascular disease. Neuroimaging Clin N Am 2007;17(1):57–72.
[2] Nishio A, Ohata K, Takami T, Nishikawa M, Hara M. Atypical spinal dural arte-riovenous fistula with supply from the lateral sacral artery. J Clin Neurosci2007;14(1):65–8.
[3] Krings T, Thron AK, Geibprasert S, Agid R, Hans FJ, Lasjaunias PL, et al.Endovascular management of spinal vascular malformations. Neurosurg Rev2010;33(1):1–9.
[4] Ferch RD, Morgan MK, Sears WR. Spinal arteriovenous malformations: a reviewwith case illustrations. J Clin Neurosci 2001;8(4):299–304.
[5] Nogueira RG, Dabus G, Rabinov JD, Ogilvy CS, Hirsch JA, Pryor JC. Onyxembolization for the treatment of spinal dural arteriovenous fistulae: initialexperience with long-term follow-up. Technical case report. Neurosurgery2009;64(1):E197–8.
[6] Oldfield EH. Surgical treatment of spinal dural arteriovenous fistulas. SeminCerebrovasc Dis Stroke 2002;2(3):209–26.
[7] Rodesch G, Lasjaunias P. Spinal cord arteriovenous shunts: from imaging tomanagement. Eur J Radiol 2003;46(3):221–32.
[8] Song D, Garton HJ, Fahim DK, Maher CO. Spinal cord vascular malformations inchildren. Neurosurg Clin N Am 2010;21(3):503–10.
[9] Saladino A, Atkinson JL, Rabinstein AA, Piepgras DG, Marsh WR, Krauss WE,et al. Surgical treatment of spinal dural arteriovenous fistulae: a consecutiveseries of 154 patients. Neurosurgery 2010;67(5):1350–7.
10] Riina HA, Spetzler RF. Classification of vascular lesions affecting the spinal cord.Oper Tech Neurosurg 2003;6(3):106–15.
11] Jahan R, Vinuela F. Vascular anatomy, pathophysiology and classification of
spinal vascular malformations of the spinal cord. Semin Cerebrovasc Dis Stroke2002;2(3):186–200.12] McDougall CG, Deshmukh VR, Fiorella DJ, Albuquerque FC, Spetzler RF.Endovascular techniques for vascular malformations of the spinal axis. Neu-rosurg Clin N Am 2005;16(2):395–410.
[
Neurosurgery 125 (2014) 81–86
13] Rodesch G, Hurth M, Alvarez H, David P, Tadie M, Lasjaunias P. Emboliza-tion of spinal cord arteriovenous shunts: morphological and clinical follow-upand results – review of 69 consecutive cases. Neurosurgery 2003;53(1):40–9.
14] Steinmetz MP, Chow MM, Krishnaney AA, Andrews-Hinders D, Benzel EC,Masaryk TJ, et al. Outcome after the treatment of spinal dural arteriovenousfistulae: a contemporary single-institution series and meta-analysis. Neuro-surgery 2004;55(1):77–87.
15] Aminoff MJ, Logue V. The prognosis of patients with spinal vascular malforma-tions. Brain 1974;97:211–8.
16] Liu A, Gobin P, Riina H. Endovascular surgery for vascular malformations of thespinal cord. Oper Tech Neurosurg 2003;6(3):163–70.
17] Narvid J, Hetts SW, Larsen D, Neuhaus J, Singh TP, McSwain H, et al. Spinal duralarteriovenous fistulae: clinical features and long-term results. Neurosurgery2008;62(1):159–66.
18] Krings T, Geibprasert S. Spinal dural arteriovenous fistulas. Am J Neuroradiol2009;30(4):639–48.
19] Oran I, Parildar M, Derbent A. Treatment of slow-flow (type I) perimedullaryspinal arteriovenous fistulas with special reference to embolization. Am J Neu-roradiol 2005;26(10):2582–6.
20] Jackson J, Partovi S. Imaging of spinal cord vascular malformations. Oper TechNeurosurg 2003;6(3):125–40.
21] Cho KT, Lee DY, Chung CK, Han MH, Kim HJ. Treatment of spinal cord per-imedullary arteriovenous fistula: embolization versus surgery. Neurosurgery2005;56(2):232–41.
22] Antonietti L, Sheth SA, Halbach VV, Higashida RT, Dowd CF, Lawton MT, et al.Long-term outcome in the repair of spinal cord perimedullary arteriovenousfistulas. Am J Neuroradiol 2010;31(10):1824–30.
23] Nagata S, Morioka T, Natori Y, Matsukado K, Sasaki T, Yamada T. Factors thataffect the surgical outcomes of spinal dural arteriovenous fistulas. Surg Neurol2006;65(6):563–8.
24] van Rooij WJ, Nijenhuis RJ, Peluso JP, Sluzewski M, Beute GN, van der Pol B.Spinal dural fistulas without swelling and edema of the cord as incidentalfindings. Am J Neuroradiol 2012;33(10):1888–92.
25] Jin YJ, Kim KJ, Kwon OK, Chung SK. Perimedullary arteriovenous fistula of thefilum terminale: case report. Neurosurgery 2010;66(1):E219–20.
26] Veznedaroglu E, Nelson PK, Jabbour PM, Rosenwasser RH. Endovascular treat-ment of spinal cord arteriovenous malformations. Neurosurgery 2006;59(5Suppl. 3):S202–9.
27] Kim LJ, Spetzler RF. Classification and surgical management of spinal arte-riovenous lesions: arteriovenous fistulae and arteriovenousmalformations.Neurosurgery 2006;59(5 Suppl. 3):S195–201.
28] Kataoka H, Miyamoto S, Nagata I, Ueno Y, Hashimoto N. Intraoperativemicrodoppler monitoring for spinal dural arteriovenous fistulae. Surg Neurol1999;52(5):466–72.
29] Niimi Y, Berenstein A, Setton A, Neophytides A. Embolization of spinaldural arteriovenous fistulae: results and follow-up. Neurosurgery1997;40(4):675–82.
30] Van Dijk JM, TerBrugge KG, Willinsky RA, Farb RI, Wallace MC. Multidisciplinarymanagement of spinal dural arteriovenous fistulas: clinical presentation andlong-term follow-up in 49 patients. Stroke 2002;33(6):1578–83.
31] Westphal M, Koch C. Management of spinal dural arteriovenous fistulaeusing an interdisciplinary neuroradiological/neurosurgical approach: experi-ence with 47 cases. Neurosurgery 1999;45(3):451–7.
32] Rodesch G, Hurth M, Alvarez H, Tadie M, Lasjaunias P. Spinal cord intraduralarteriovenous fistulae: anatomic, clinical, and therapeutic considerations in aseries of 32 consecutive patients seen between 1981 and 2000 with emphasison endovascular therapy. Neurosurgery 2005;57(5):973–83.
33] Song JK, Gobin YP, Duckwiler GR, Murayama Y, Frazee JG, Martin NA, et al. N-
J Neuroradiol 2001;22(1):40–7.34] Cenzato M, Versari P, Righi C, Simionato F, Casali C, Giovanelli M. Spinal dural
arteriovenous fistulae: analysis of outcome in relation to pretreatment indica-tors. Neurosurgery 2004;55(4):815–22.




















