
An Arteriovenous Fistula Model of Intimal Hyperplasia for Evaluation of a Nitinol U-Clip Anastomosis
9
This article appeared in a journal published by Elsevier. The attached copy is furnished to the author for internal non-commercial research and education use, including for instruction at the authors institution and sharing with colleagues. Other uses, including reproduction and distribution, or selling or licensing copies, or posting to personal, institutional or third party websites are prohibited. In most cases authors are permitted to post their version of the article (e.g. in Word or Tex form) to their personal website or institutional repository. Authors requiring further information regarding Elsevier’s archiving and manuscript policies are encouraged to visit: http://www.elsevier.com/copyright
Transcript of An Arteriovenous Fistula Model of Intimal Hyperplasia for Evaluation of a Nitinol U-Clip Anastomosis

This article appeared in a journal published by Elsevier. The attachedcopy is furnished to the author for internal non-commercial researchand education use, including for instruction at the authors institution
and sharing with colleagues.
Other uses, including reproduction and distribution, or selling orlicensing copies, or posting to personal, institutional or third party
websites are prohibited.
In most cases authors are permitted to post their version of thearticle (e.g. in Word or Tex form) to their personal website orinstitutional repository. Authors requiring further information
regarding Elsevier’s archiving and manuscript policies areencouraged to visit:
http://www.elsevier.com/copyright

Author's personal copy
An Arteriovenous Fistula Model of Intimal Hyperplasia for Evaluation of a NitinolU-Clip Anastomosis
R.L. Varcoe a,b,c,*, A.B.P. Teo a,b, M.H. Pelletier a,b,c, Y. Yu a,b,c, J.-L. Yang a,b,c, P.J. Crowe a,b,c,W.R. Walsh a,b,c
aDepartment of Surgery, Prince of Wales Hospital, Sydney, Australiab Surgical and Orthopaedic Research Laboratories, Prince of Wales Clinical School, Faculty of Medicine, Australiac The University of New South Wales, Sydney, Australia
a r t i c l e i n f o
Article history:Received 17 May 2011Accepted 1 November 2011Available online 21 November 2011
Keywords:Arteriovenous fistulaHemodialysis vascular accessIntimal hyperplasiaOvine modelVascular anastomotic clip
a b s t r a c t
Objectives: The aim of this study was to create an ovine arteriovenous fistula (AVF) model which wouldclosely replicate a human forearm fistula and use this to quantify the degree of intimal hyperplasia inthose created with the U-Clip compared to a conventional sutured anastomosis.Materials and methods: Twenty AVFs were created in 10 Border LeicestereMerino sheep between thesuperficial femoral artery and vein of each hind limb. On one side the U-Clip and on the othera continuous polypropylene suture was used to perform the anastomosis. The animals were sacrificed at2 (n ¼ 3), 4 (n ¼ 4), 6 (n ¼ 3) weeks and histological slices were taken of each AVF in cross section todetermine the intimal media area per unit length (IMA/L).Results: Intimal hyperplasia (IH) was observed at all time points with one AVF found occluded withthrombus at the time of harvest. The IMA/L was significantly lower in the U-Clip groups by 24% at 2weeks, 32% at 4 weeks and 23% at 6 weeks (Two-way ANOVA, p ¼ 0.019, observed power ¼ 0.825, time orside p � 0.766, type p ¼ 0.001; Paired t-test, p < 0.001 between matched anastomotic types). Time takento perform the anastomosis was similar between the two anastomotic techniques (Polypropylene 14(8e18) vs. U-Clip 15.3(11e23) min; p ¼ 0.47).Conclusion: This ovine AVF model results in IH similar to that seen in a human AVF. The IH that occurswith the U-Clip is less than that of continuous polypropylene suture.
� 2011 European Society for Vascular Surgery. Published by Elsevier Ltd. All rights reserved.
Introduction
Intimal hyperplasia (IH) is ubiquitous after the vascular injurythat occurs during surgery. It affects all types of vascular anasto-mosis but is most pronounced in the arteriovenous fistula (AVF)created for hemodialysis access. This IH results in restenosis, whichthreatens AVF patency and causes significant morbidity. The failureor dysfunction of arteriovenous fistulae has an annual cost of morethan $1 billion dollars in the United States1e3 where there werealmost 328,000 patients receiving hemodialysis therapy at the endof 2006.4
The primary patency of an AVF is less than 50% after 3 years andmay be as low as 20% in patients who are elderly, diabetic or
female.5,6 Despite such poor durability alternatives to AVF such ascuffed central venous catheters and synthetic arteriovenous graftssuffer higher rates of infectious complications, central venousstenoses and even lower patency rates.6,7 The AVF remains there-fore the best option for patients with end stage renal disease whorequire hemodialysis.
The nitinol U-Clip device (Medtronic, Minneapolis, MN, USA) isdesigned to reduce the use of sutures thus eliminating knot tyingwhilst facilitating the creation of a circumferentially interruptedvascular anastomosis8 (Fig. 1). In support of this device’s efficacya single prospective human study has shown superior patency andmaturation rates of forearm AVFs created with U-Clips whencompared to continuous polypropylene suture.9 The aim of ourstudy was to create an AVF model with vessel size, handlingproperties, configuration and hemodynamic stresses akin to humanforearm AVFs to quantify the degree of intimal hyperplasia andmake comparison between continuous polypropylene suture andthe Nitinol U-Clip anastomosis.
* Corresponding author. R.L. Varcoe, Suite 8, Level 7, Prince of Wales PrivateHospital, Barker St, Randwick, NSW 2031, Australia. Tel.: þ61 2 96504981; fax: þ612 96504910.
E-mail address: [email protected] (R.L. Varcoe).
Contents lists available at SciVerse ScienceDirect
European Journal of Vascular and Endovascular Surgery
journal homepage: www.ejves.com
1078-5884/$ e see front matter � 2011 European Society for Vascular Surgery. Published by Elsevier Ltd. All rights reserved.doi:10.1016/j.ejvs.2011.11.002
European Journal of Vascular and Endovascular Surgery 43 (2012) 224e231

Author's personal copy
Materials and Methods
Animals
Ten 2-year old crossbred Border LeicestereMerino wetherswere used with the approval of our local Animal Care and EthicsCommittee (ACEC 08/113A). They were kept in the research facilityat the St. George Hospital Campus, University of New South Walesin accordance with the research guidelines of the National Healthand Medical Research Council of Australia.
Surgery
Sheep were first sedated with Intramuscular Zolazopam(8e12mg/kg), analgesedwith subcutaneous Carprofen (2e4mg/kg)and intramuscular Burprenorphine (0.005mg/kg) then administeredinhaled Isofluorane (2e3%) and 100% oxygen (3 L/min) throughoutthe surgery. Laryngoscopy was performed and an endotracheal tubeplaced above the carina for ventilation. Antibiotics (IntravenousCephalothin 0.016e0.024 mg/kg; Benacillin 0.079e0.122 ml/kg IM)were administered and crystalloid fluids (Hartmann’s solution)weregiven intravenously at 4e10ml/kg/h prior to and during the surgery.
Both hind limb groin creaseswere cleanedwith povidone-iodineand draped in accordance with conventional surgical practice. Skincrease incisionsweremade just below the inguinal ligament and the
incision deepened to expose both the superficial femoral artery andvein. 5000 IU of Sodium Heparin was administered intravenouslyand the vessels were double slung both proximally and distally toachieve hemostasis for AVF creation. A 2 cm length longitudinalarteriotomy and corresponding venotomy was performed in thesuperficial femoral vessels. This length was standardized for allanastomoses and all animals. A conventional Brescia-Cimino side-to-side anastomosis was created using continuous 6e0 poly-propylene (Prolene, Ethicon, Johnson& Johnson,Warren, NJ, USA) inone hind limb and interrupted U-Clips in the contralateral one10
(Fig. 2). In each anastomosis care was taken to evert the vesseledges and avoid adventitia within the suture line. Flushing withheparinised saline and hemostasis were given careful attention atthe time of sling release. A marking suture was placed at the ceph-alad and caudad ends of the anastomosis to aid and orient thecadaveric dissection. Patency of fistula was confirmed with pulseand thrill at the end of the anastomosis. Layered closure of fascia andskin with 3e0 polypropylene suture (Prolene, Ethicon, Johnson &Johnson, Warren, NJ, USA) was performed. The side of hind limbchosen for suture/U-Clip was alternated in consecutive animals.
The nitinol U-Clip is applied with a standard needle andsuturing action. It is connected to the surgical needle by a fine wireand released by grasping a trigger point with the teeth of the needleholder, at which point it resumes its circular shape holding theblood vessel walls in apposition (Fig. 1A,B). The retention knob at
Figure 1. The nitinol U-Clip with its delivery apparatus intact (A), demonstrating the release trigger point (B, Arrow) and resuming its circular shape (C). (B and C Images taken withenvironmental scanning electron microscopy (TM-1000, Hitachi, Japan)).
R.L. Varcoe et al. / European Journal of Vascular and Endovascular Surgery 43 (2012) 224e231 225

Author's personal copy
the end of the clip snugs against the vessel wall to prevent it pullingthrough (Fig. 1C). U-Clips are placed every 1e2 mm as one wouldwith an interrupted suture.
Study design
Ten Sheep were utilized to create 20 AVFs. They were sacrificedat 2 weeks (3 sheep, 6 AVF), 4 weeks (4 sheep, 8 AVF) and 6 weeks(3 sheep, 6 AVF).
Specimen explantation and preparation
Each sheep was administered 20,000 IU of intravenous SodiumHeparin prior to euthanasia with a lethal injection of Sodium
Pentothal. Hind limb dissection was carried out to identify andexcise each AVF en-bloc with its associated few centimeters offeeding artery and vein. The AVF was gently flushed with 10%buffered formalin so as not to remove any thrombus or IH and thenallowed to fix in formalin (40%) for 48 h. High resolution X-Ray wasused to confirm the presence of U-Clips and aid with orientation inthe 20 specimens. The specimens were then divided through thelongitudinal midpoint of the anastomosis in a cross sectional plane.Half of the specimen was processed for paraffin embedding afterremoval of the U-Clips, the other half for Polymethyl-Methacrylate(PMMA) embedding. The paraffin embedded blocks were cut fivemicrons thick on slides using a Leica RM 2165 microtome (LeicaMicrosystems, Germany), stained with Harris’s Hematoxylin andEosin (H&E) and Van Gieson for histological and morphometric
Figure 2. A diagram showing the formation of side-to-side arteriovenous fistulae in the superficial femoral artery and vein (A). Photography of the ovine surgery showing fistulaecreation with continuous polypropylene suture (B and C) and nitinol U-Clip (D and E).
R.L. Varcoe et al. / European Journal of Vascular and Endovascular Surgery 43 (2012) 224e231226
Author's personal copy
analysis. The PMMA embedded specimens were cut into tenmicronthick sections on a Leica SP 1600 saw microtome, acid etched, andstained with basic fuschin and methylene blue. The PMMA samplesallowed sectioning directly through the metallic U-Clips.
Histology and morphometric analysis
Sections from each block were examined to determine repre-sentative samples of cross section through the midsection of eachanastomosis. These cross sections were then processed to deter-mine intima media area per unit length. Digital images of H&E andVan Gieson stained slides were taken at 1.25, 2, 4, 10 and 20�objective magnifications on a BX51 Olympus microscope witha DP2-BSW camera and software (Olympus Corporation, Japan).
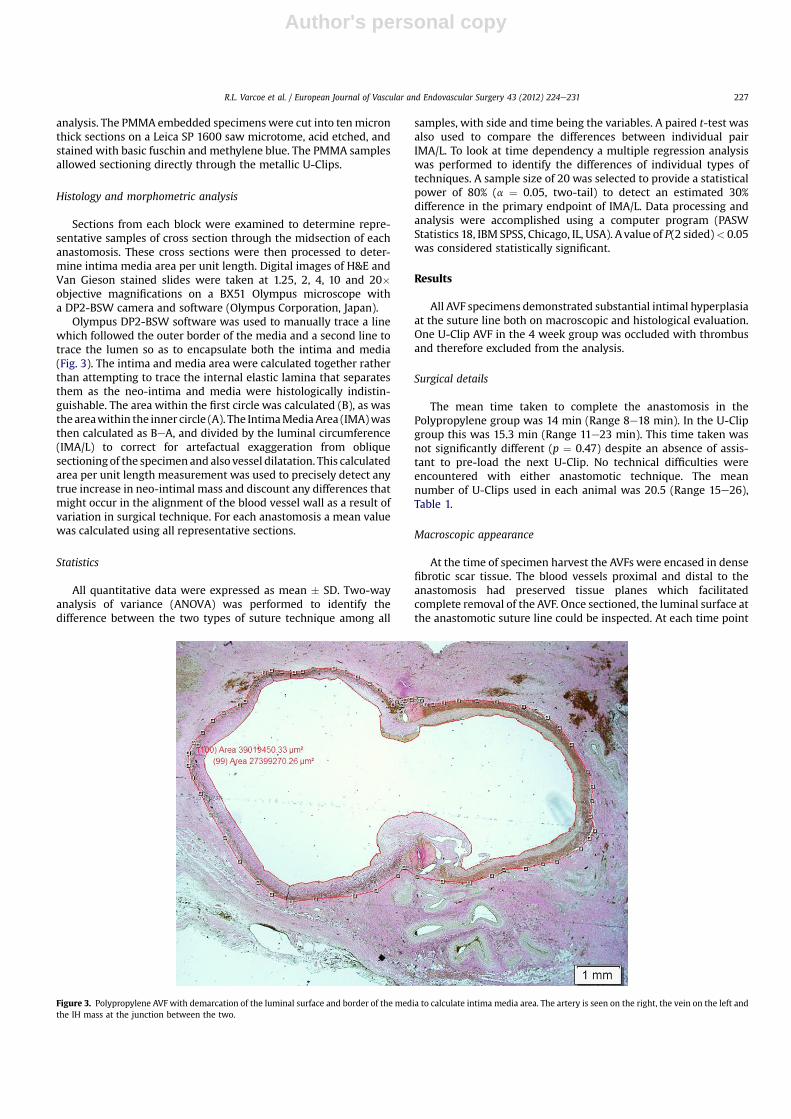
Olympus DP2-BSW software was used to manually trace a linewhich followed the outer border of the media and a second line totrace the lumen so as to encapsulate both the intima and media(Fig. 3). The intima and media area were calculated together ratherthan attempting to trace the internal elastic lamina that separatesthem as the neo-intima and media were histologically indistin-guishable. The area within the first circle was calculated (B), as wasthe areawithin the inner circle (A). The IntimaMediaArea (IMA)wasthen calculated as BeA, and divided by the luminal circumference(IMA/L) to correct for artefactual exaggeration from obliquesectioningof the specimen and also vessel dilatation. This calculatedarea per unit length measurement was used to precisely detect anytrue increase in neo-intimal mass and discount any differences thatmight occur in the alignment of the blood vessel wall as a result ofvariation in surgical technique. For each anastomosis a mean valuewas calculated using all representative sections.
Statistics
All quantitative data were expressed as mean � SD. Two-wayanalysis of variance (ANOVA) was performed to identify thedifference between the two types of suture technique among all
samples, with side and time being the variables. A paired t-test wasalso used to compare the differences between individual pairIMA/L. To look at time dependency a multiple regression analysiswas performed to identify the differences of individual types oftechniques. A sample size of 20 was selected to provide a statisticalpower of 80% (a ¼ 0.05, two-tail) to detect an estimated 30%difference in the primary endpoint of IMA/L. Data processing andanalysis were accomplished using a computer program (PASWStatistics 18, IBM SPSS, Chicago, IL, USA). A value of P(2 sided)< 0.05was considered statistically significant.
Results
All AVF specimens demonstrated substantial intimal hyperplasiaat the suture line both on macroscopic and histological evaluation.One U-Clip AVF in the 4 week group was occluded with thrombusand therefore excluded from the analysis.
Surgical details
The mean time taken to complete the anastomosis in thePolypropylene group was 14 min (Range 8e18 min). In the U-Clipgroup this was 15.3 min (Range 11e23 min). This time taken wasnot significantly different (p ¼ 0.47) despite an absence of assis-tant to pre-load the next U-Clip. No technical difficulties wereencountered with either anastomotic technique. The meannumber of U-Clips used in each animal was 20.5 (Range 15e26),Table 1.
Macroscopic appearance
At the time of specimen harvest the AVFs were encased in densefibrotic scar tissue. The blood vessels proximal and distal to theanastomosis had preserved tissue planes which facilitatedcomplete removal of the AVF. Once sectioned, the luminal surface atthe anastomotic suture line could be inspected. At each time point
Figure 3. Polypropylene AVF with demarcation of the luminal surface and border of the media to calculate intima media area. The artery is seen on the right, the vein on the left andthe IH mass at the junction between the two.
R.L. Varcoe et al. / European Journal of Vascular and Endovascular Surgery 43 (2012) 224e231 227

Author's personal copy
the blood vessels and suture lines were covered in a smooth, paleand homogeneous fibrosis tissue layer that appeared identical tothat seen in human IH.11 This had a similar appearance in both theU-Clip and sutured AVFs.
Histo-morphometric analysis
At each time point there was less IMA/L in the U-Clip groupcompared to the sutured anastomoses. The lower IMA/L in theU-Clip group was 24% at 2 weeks, 32% at 4 weeks and 23% at 6weeks which translated to a significant difference at all time points(Two-way ANOVA for the two types of techniques with side andtime as variates, F ¼ 4.224, p ¼ 0.019, observed power ¼ 0.825, sideor time p� 0.766, type p¼ 0.001). Fig. 4 summarizes the calculatedIMA/L data with respective p value and standard deviation at eachtime point. Fig. 5 represents the IMA/L data in its paired form todemonstrate the intra-animal difference in intimal hyperplasiawith the two types of anastomotic material. A multiple linearregression analysis investigating the effect of time on the types oftechniques showed no time-dependency (p ¼ 0.372).
When the matched data from different time points was pooledthe reduction in IMA/L was 26% which resulted in similar albeitgreater significant values favoring the U-Clip (IMA/L 432 � 43.8(polypropylene) vs. 318 � 53.4 (Nitinol U-Clip) mm; Paired t-test,t ¼ 5.795, p < 0.001).
Descriptive histology
In each AVF there was development of a thick fibrocellular layerbetween endothelium and internal elastic lamina both in the arteryand vein wall as well as overlying the suture line (Fig. 6). This layerconsisted of extracellular matrix separating abundant spindleshaped cells which had a similar appearance to that of a fibroblastwith additional features of the smooth muscle cells seen in the
adjacent vessel media. This appearancewas identical to that seen inthe human vascular smooth muscle cell that is pathognomonic forintimal hyperplasia, and was of a similar expected volume.12
An observed consistently raised deposit of intimal hyperplasiawas seen overlying the polypropylene anastomoses at the sutureline in each specimen (Fig. 6AeC). In contrast the intima over theU-Clip was consistently flush with that of the adjacent vessel anddid not protrude into or compromise the lumen (Fig. 6DeF). It wasalso apparent that the polypropylene was associated with a greaterdegree of necrosis adjacent to where it passed through the bloodvessel tissue and had a more pronounced surrounding inflamma-tory cellular infiltrate when compared to the tissue immediatelyadjacent to the U-Clip (Fig. 6). Although not objective theseobservations were found consistently across all specimens at eachtime point and were consistent with the quantitative differencesseen in IMA/L.
Discussion
Juxta-anastomotic restenosis and its subsequent reduction inpatency is a significant problem that threatens all forms of vascularsurgery. Of all types of vascular anastomoses created it is the AVFthat performs worst of all.5,6 IH is the major factor contributing torestenosis and is commonly found at the anastomosis or withina few centimeters of blood vessel either side. It is for this reasonwechose to examine the IH that develops after using the nitinol U-Clipto compare it directly with the conventional suturing techniquewhich is current practice for most vascular access surgeons.
The trigger for the development of IH is the vascular injury toendothelium andmedia that occurs during surgery.13 This results indisruption to endothelial and medial smooth muscle cells which inturn release principle factors, mitogens, and a host of cytokinesincluding basic fibroblast growth factor, transforming growthfactor-b, and vascular endothelial growth factor. Simultaneously,platelets adhere to the injured vessel and foreign suture material,degranulating and releasing platelet derived growth factor A and B.These growth promoters stimulate the quiescent vascular smoothmuscle cell into a synthetic phase. It is these cells that proliferateand migrate to the intimal layer to synthesize extracellular matrixand form the IH mass.14,15
The vascular smooth muscle cells responsible for IH have theirorigins in local blood vessel media and adventitia as well as fromcirculating progenitor cells.14e16 It is thought that in addition tosurgical trauma the altered hemodynamics of blood flow throughthe AVF anastomoses create low fluid shear stress and increasedwall stress forces that promotes ongoing vascular injury and resultsin continuing migration of these cells and accumulation of neo-intima.16,17 The hemodynamic disruption to laminar flow is exag-gerated in the AVF because of its unique low pressure outflow andsharp change in flow direction. It is thought that improvedcompliance at the anastomosis may result in less restenosis andbetter patency.
It has been established that interrupted suture technique fora vascular anastomosis results in improved compliance, which isthought to reduce blood flow turbulence and IH.18e20 In addition,the interrupted technique reduces the “purse-string” affect that canoccur with a continuous suture, thus allowing it to expand ina radial direction with each systole. Despite the benefits of inter-rupted suturing, it has not been adopted as a technique by themajority of vascular access surgeons because of the additional timetaken for knot tying and the technical difficulty involved.
The Nitinol used in the U-Clip is a shape-memory alloy madefrom Nickel and Titanium that was first described by the US NavalOrdnance Laboratory in 1963.21 It has the unusual properties ofthermal shape memory, super elasticity and force hysteresis that
Table 1Time taken to complete each anastomosis and number of U-Clips used.
Number Time point(weeks)
Polypropylene(min)
U-Clip(min)
U-Clipsused (n)
1 2 16 18 222 2 14 16 193 2 13 13 214 4 14 15 155 4 14 15 196 4 16 23 267 4 18 16 248 6 10 12 189 6 17 14 2110 6 8 11 20
Mean 14 15.3 20.5
Figure 4. Intimal media area per unit length over the three time points. Error barsrepresent standard deviation.
R.L. Varcoe et al. / European Journal of Vascular and Endovascular Surgery 43 (2012) 224e231228

Author's personal copy
make it ideal for an anastomotic clip.22,23 In both in-vitro and in-vivo studies Nitinol appears to be safe to cells and connectivetissues causing no toxicity and maintaining proliferative potentialthus allowing coverage by new intimal formation within the vessellumen.24e28 It is thought that these inert properties combined withreduced tissue trauma result in less inflammatory infiltrate,migration of activated smooth muscle cells and IH deposition.
A number of vascular anastomotic clips have been compared tointerrupted sutured anastomosis in the past and are known to havesimilar compliance properties at the anastomosis, both of which aresuperior to the continuous suture.29 The U-Clip is different fromother clips in that it uses a curved surgical needle and the samemotion of passage through each blood vessel as with a suture.8 Ithas similar compliance properties to an interrupted suture whilstreducing the technical difficulty and time required for anastomosiscompletion. It differs from suture in that it uses a new needle,followed by a fine connecting thread for each clip insertion. Thisdesign and suturing actionmay result in less tissue trauma and giveit a potential advantage over suture techniques both interruptedand continuous. The U-Clip thus provides a practical alternative tointerrupted suture likely to be accepted by most surgeons.
The macroscopic features of human AVF intimal hyperplasia arethat of a firm, pale homogenous fibrous layer of tissue on theluminal surface of the blood vessel. Histologically there is a fibro-cellular layer consisting of vascular smooth muscle cells withfeatures of the adjacent medial smooth muscle cell and the fibro-blast. These cells migrate to proliferate between the endotheliumand the internal elastic lamina secreting an extracellular matrixthat consists of hydrated proteoglycans (hyaluronan and versican)and type III collagen. In our ovine model the macroscopic andhistological appearance of the tissue layer that formed betweenendothelium and internal elastic lamina had all of the typicalfeatures of the intimal hyperplasia lesion seen in the humanAVF.11,12 This observation was implicit in the use of this model asa valid means to compare the IH response between the two suturemethods.
Our study has, for the first time, made a comparison betweenthe IH burden that is deposited after AVF surgery with conventionalcontinuous suture and with a nitinol U-Clip anastomoses. We have
found a significant reduction in the amount of IH around theanastomosis. We have also found the device to be feasible and safewhilst using it to form a vascular anastomosis which was simpleand free from technical difficulty. The time taken for each anasto-mosis was similar to suturing despite the absence of an assistant topre-load the new U-Clip into a second needle holder. This addi-tional help would make for an anastomosis that may be more timeefficient than the traditional continuous suture method.
The precise mechanism of the difference in generated IH has notbeen addressed in this study. We believe that improved complianceat the anastomosis, reduced vessel trauma during U-Clip placementcombined with the inert nature and low thrombogenicity of thenitinol are all contributing factors to the reduction seen here.Ongoing research is required to investigate the precise mechanismand role of each of these factors.
There are some limitations to our study. Firstly the sheep in thisstudy where not uremic and their fistulae were never cannulated.Despite this, they developed a neo-intimal hyperplastic reaction asone would see with human AVF histology. This reassured us thatour model sufficiently replicated the human biological response toprovide useful observations and data. Secondly, there was consid-erable variation in the degree of neo-intima formed betweenanimals, which is a feature also seen in humans. As a result we sawa non-linear temporal relationship through the progressive timepoints. In predicting this phenomenonwe performed both types offistula in each animal. Thus the animal was its own control, vali-dating the comparison between anastomotic materials. We decidedto compare the U-Clip device to the continuous polypropyleneanastomosis rather than an interrupted suture in order to enhancethe clinical generalizability and value of the result. A comparativetrial between the two types of interrupted techniques would haveprovided insight into the difference in intimal hyperplasia responseas a direct result of the materials used. However, it would not haveprovided a relevant comparison for the majority of surgeons whoare using a continuous suture technique and who may giveconsideration to the use of a clip device that is fast and simple touse. We did not examine the complete fistula circuit, in particularthe venous outflow arm which is responsible for many of thepatency threatening stenoses seen in the human. Our interest was
200
250
300
350
400
450
500
550
U-Clip Polypropylene
IMA/L(µm)
SUTURE MATERIAL
Sheep 1 (2 week)Sheep 2 (2 week)Sheep 3 (2 week)Sheep 4 (4 week)Sheep 5 (4 week)Sheep 6 (4 week)Sheep 7 (4 week)Sheep 8 (6 week)Sheep 9 (6 week)Sheep 10 (6 week)
Figure 5. Intimal media area per unit length (IMA/L) for each sheep demonstrating its response for the paired anastomoses. One side was created with the nitinol U-Clip, the otherwith a standard polypropylene suture.
R.L. Varcoe et al. / European Journal of Vascular and Endovascular Surgery 43 (2012) 224e231 229

Author's personal copy
focused on the local tissue reaction and intimal hyperplasiadevelopment at the vessel adjacent to the anastomosis which wefelt was the location most likely to be influenced by the differencein suture material and hemodynamic forces.
In conclusion, we have developed an ovine model of arteriove-nous fistula that closely replicates the macroscopic and histologicalappearance of IH development seen in the human lesion. Uponsubsequent validation this model may be utilized by the vascularsurgical community to test novel therapies for treating the ongoingproblem of AVF stenosis. Our study demonstrates the feasibility andpractical application of the U-Clip and found significantly less IHwith the nitinol U-Clip compared to a conventional continuouspolypropylene anastomotic technique. Additional studies will beneeded to delineate whether it is the improved compliance,reduced tissue trauma or inert nature of the nitinol which gives theU-Clip its advantage.
Acknowledgments
Thanks go to Medtronic Australasia for providing the nitinolU-Clip devices.
Conflict of InterestNone.
FundingNone.
References
1 Feldman HI, Kobrin S, Wasserstein A. Hemodialysis vascular access morbidity.J Am Soc Nephrol 1996;7(4):523e35.
2 McCarley P, Wingard RL, Shyr Y, Pettus W, Hakim RM, Ikizler TA. Vascularaccess blood flow monitoring reduces access morbidity and costs. Kidney Int2001;60(3):1164e72.
Figure 6. Micrographs of paraffin embedded sections. Neo-intima formed over both anastomotic materials, however was more pronounced and raised in the polypropylene group(A (B and C are higher magnification of the boxed areas)). This group also had more necrosis and inflammatory cellular infiltrate observed when compared to the U-Clip group (D (Eand F are higher magnification of the boxed areas)).
R.L. Varcoe et al. / European Journal of Vascular and Endovascular Surgery 43 (2012) 224e231230

Author's personal copy
3 LysaghtMJ, LysaghtMJ.Maintenancedialysis populationdynamics: current trendsand long-term implications. J Am Soc Nephrol 2002;13(Suppl. 1):S37e40.
4 U.S. Renal Data System. USRDS 2008 annual data report: atlas of chronic kidneydisease and end-stage renal disease in the United States.
5 KF-DOQI clinical practice guidelines for vascular access. New York: NationalKidney Foundation; 1997.
6 Manns B, Tonelli M, Yilmaz S, Lee H, Laupland K, Klarenbach S, et al. Estab-lishment and maintenance of vascular access in incident hemodialysis patients:a prospective cost analysis. J Am Soc Nephrol 2005;16(1):201e9.
7 Ishani A, Collins AJ, Herzog CA, Foley RN, Ishani A, Collins AJ, et al. Septicemia,access and cardiovascular disease in dialysis patients: the USRDS wave 2 study.Kidney Int 2005;68(1):311e8.
8 Ross JR. Creation of native arteriovenous fistulas with interrupted anastomosesusing a self-closing clip device e one clinic’s experience. J Vasc Access2002;3(4):140e6.
9 Lin PH, Bush RL, Nelson JC, Lam R, Paladugu R, Chen C, et al. A prospectiveevaluation of interrupted nitinol surgical clips in arteriovenous fistula forhemodialysis. Am J Surg 2003;186(6):625e30.
10 Brescia MJ, Cimino JE, Appel K, Hurwich BJ. Chronic hemodialysis using veni-puncture and a surgically created arteriovenous fistula. New Engl J Med1966;275(20):1089e92.
11 Cronenwett J, Johnston KW, editors. Rutherford’s vascular surgery. 7th ed.Philadelphia: Saunders Elsevier; 2010.
12 Dilley RJ, McGeachie JK, Prendergast FJ. A review of the histologic changes invein-to-artery grafts, with particular reference to intimal hyperplasia. Arch Surg1988;123(6):691e6.
13 Clowes AW, Kirkman TR, Clowes MM. Mechanisms of arterial graft failure. II.Chronic endothelial and smooth muscle cell proliferation in healing poly-tetrafluoroethylene prostheses. J Vasc Surg 1986;3(6):877e84.
14 Clowes AW, Gown AM, Hanson SR, Reidy MA. Mechanisms of arterial graftfailure. 1. Role of cellular proliferation in early healing of PTFE prostheses. Am JPathol 1985;118(1):43e54.
15 Majesky MW, Schwartz SM, Clowes MM, Clowes AW. Heparin regulates smoothmuscle S phase entry in the injured rat carotid artery. Circ Res1987;61(2):296e300.
16 Haruguchi H, Teraoka S, Haruguchi H, Teraoka S. Intimal hyperplasia andhemodynamic factors in arterial bypass and arteriovenous grafts: a review.J Artif Organs 2003;6(4):227e35.
17 Sivanesan S, How TV, Black RA, Bakran A. Flow patterns in the radio-cephalic arteriovenous fistula: an in vitro study. J Biomech 1999;32(9):915e25.
18 Lee BY, Brancato RF, Shaw WW, Browne S, Thoden WR, Madden JL. Effect ofsuture technique on blood velocity waveforms in the microvascular anasto-mosis of autogenous vein graft. Microsurgery 1983;4(3):151e6.
19 Baumgartner N, Dobrin PB, Morasch M, Dong QS, Mrkvicka R. Influence ofsuture technique and suture material selection on the mechanics of end-to-endand end-to-side anastomoses. J Thorac Cardiovasc Surg 1996;111(5):1063e72.
20 Hasson JE, Megerman J, Abbott WM. Suture technique and para-anastomoticcompliance. J Vasc Surg 1986;3(4):591e8.
21 Buehler WJ, Gilfrich J, Riley RC. Effect of low-temperature phase changes on themechanical properties of alloys near com-position TieNi. J Appl Phys 1963;34:1475e7.
22 Barras CD, Myers KA. Nitinol e its use in vascular surgery and other applica-tions. Eur J Vasc Endovasc Surg 2000;19(6):564e9.
23 Gisser KR, Geselbracht M, Capellari A, Hunsberger L, Ellis AE. Nickeletitaniummemory metal e a “smart” material exhibiting a solid state phase change andsuperelasticity. J Chem Educ 1994;71:334e40.
24 Putters JL, Kaulesar Sukul DM, de Zeeuw GR, Bijma A, Besselink PA. Comparativecell culture effects of shape memory metal (Nitinol), nickel and titanium:a biocompatibility estimation. Eur Surg Res 1992;24(6):378e82.
25 Ryhanen J, Niemi E, Serlo W, Niemela E, Sandvik P, Pernu H, et al. Biocompat-ibility of nickeletitanium shape memory metal and its corrosion behavior inhuman cell cultures. J Biomed Mater Res 1997;35(4):451e7.
26 Castleman LS, Motzkin SM, Alicandri FP, Bonawit VL. Biocompatibility of nitinolalloy as an implant material. J Biomed Mater Res 1976;10(5):695e731.
27 Ryhanen J, Kallioinen M, Tuukkanen J, Junila J, Niemela E, Sandvik P, et al.In vivo biocompatibility evaluation of nickeletitanium shape memory metalalloy: muscle and perineural tissue responses and encapsule membranethickness. J Biomed Mater Res 1998;41(3):481e8.
28 Cutright DE, Bhaskar SN, Perez B, Johnson RM, Cowan Jr GS. Tissue reaction tonitinol wire alloy. Oral Surg Oral Med Oral Pathol 1973;35(4):578e84.
29 Baguneid MS, Goldner S, Fulford PE, Hamilton G, Walker MG, Seifalian AM.A comparison of para-anastomotic compliance profiles after vascular anasto-mosis: nonpenetrating clips versus standard sutures. J Vasc Surg2001;33(4):812e20 [Comparative Study].
R.L. Varcoe et al. / European Journal of Vascular and Endovascular Surgery 43 (2012) 224e231 231




















