
Reporting Standards for Endovascular Treatment of Pulmonary Embolism
10
Reporting Standards for Endovascular Treatment of Pulmonary Embolism Filip Banovac, MD, Donna C. Buckley, MD, MS, William T. Kuo, MD, Denver Matthew Lough, BS, Louis G. Martin, MD, Steven F. Millward, MD, Timothy W.I. Clark, MD, MSc, Sanjoy Kundu, MD, Dheeraj K. Rajan, MD, David Sacks, MD, and John F. Cardella, MD, for the Technology Assessment Committee of the Society of Interventional Radiology J Vasc Interv Radiol 2010; 21:44 –53 Abbreviations: CDT catheter-directed therapy, DVT deep venous thrombosis, IVC inferior vena cava, PE pulmonary embolism PULMONARY embolism (PE) is a prev- alent disease with significant morbidity and mortality. The estimated annual in- cidence is 1.45 per 1,000 person-years (1), which translates to 1,350,000 cases per year in the United States (2). The incidence of massive PE approached 11% in a postmortem evaluation of all deaths in one series (3). The 30-day mor- tality rate for massive PE approached 30% (4), and the presence of shock in these patients defines a three- to seven- fold increase in mortality, with a major- ity of deaths occurring within 1 hour of presentation (5). The role of the interventional radiol- ogist in the diagnosis and treatment of PE continues to evolve. Traditionally, pulmonary angiography was per- formed as a diagnostic modality and for many years was the gold standard in the diagnosis of PE. With the evolution of computed tomographic (CT) angiog- raphy and marked improvement in the detection of thromboembolic events, as well as the development of endovascu- lar therapy with thrombectomy devices, the interventional radiologist’s role has shifted from diagnosis to treatment of PE. Although the mainstay of treatment remains anticoagulation, more aggres- sive treatment is now possible in the hemodynamically unstable patient. In cases of massive PE, interventional radiologists have used catheter-directed thrombolytic therapy, mechanical thrombectomy, or a combination of the two in an effort to rapidly restore pul- monary blood flow in a life-saving effort (6,7). Currently as of 2009, there are no clear evidence-based guidelines that identify those patients who should be treated more aggressively with endo- vascular therapies, nor are there stan- dard approaches to reporting clinical trial results in this area (8). The Ameri- can College of Chest Physicians recom- mends against the use of mechanical ap- proaches for most patients with PE, but the American College of Chest Physi- cians guidelines suggest that endovas- cular treatment of massive PE should be used in selected highly compromised patients who are unable to receive intra- venous systemic thrombolytic therapy or whose critical status does not allow suffi- cient time to infuse thrombolytics ( 9). The purpose of the current document is to facilitate improved quality and rel- evance of clinical trials of endovascular therapies for the treatment of PE by pro- viding a basic standardized framework for reporting results in the literature. Current treatment options, patient pop- ulation considerations, endpoints, fol- low-up modalities, clinical trial designs, and statistical plans will be discussed. CURRENT TREATMENT OPTIONS Anticoagulation and Systemic Thrombolytic Therapy Presently, anticoagulation remains the preferred treatment for deep venous thrombosis (DVT) and thromboembolic disease. There has been demonstrated reduction in mortality rates to an esti- mated 8% in patients who receive anti- coagulation for the treatment of PE (10), whereas untreated PE carries a mortal- ity rate of approximately 30% (9,11–13). Intravenous unfractionated heparin is commonly used during initial hospital- ization to prevent propagation of exist- ing thrombus, and it has been long es- tablished that heparin decreases the recurrence of life-threatening PE (14). From the Division of Interventional Radiology (F.B.) and the Departments of Radiology (D.C.B.) and Sur- gery (D.M.L.), Georgetown University Hospital, 3800 Reservoir Rd, NW, Washington, DC 20007; the Division of Vascular and Interventional Radiology, Stanford University Medical Center, Stanford, California (W.T.K.); the Department of Radiology, Division of Interventional Radiology, Emory Uni- versity School of Medicine, Emory University Hospital, Atlanta, Georgia (L.G.M.); the Depart- ment of Radiology, University of Western Ontario, London, and Peterborough Regional Health Cen- tre, Peterborough, Ontario, Canada (S.F.M.); the Department of Interventional Radiology, New York University School of Medicine, NYU Medical Center, New York, New York (T.W.I.C.); Scarbor- ough General Hospital, Toronto, Ontario, Canada (S.K.); the Division of Vascular and Interventional Radiology, Department of Medical Imaging, Univer- sity of Toronto, University Health Network, To- ronto, Ontario, Canada (D.K.R.); The Reading Hos- pital and Medical Center, Advanced Interventional Radiology, West Reading, Pennsylvania (D.S.); and Geisinger Health System, Danville, Pennsylvania (J.F.C.). Received September 1, 2009; accepted Sep- tember 28, 2009. Address correspondence to F.B.; E-mail: [email protected] T.W.I.C. is a paid consultant for, has patent owner- ship or part ownership in, and has a royalty agree- ment with Merit Medical Systems Inc. D.K.R. is a paid consultant for CR Bard. None of the other authors have identified a conflict of interest. © SIR, 2010 DOI: 10.1016/j.jvir.2009.09.018 44
-
Upload
independent -
Category
Documents
-
view
0 -
download
0
Transcript of Reporting Standards for Endovascular Treatment of Pulmonary Embolism
Reporting Standards for EndovascularTreatment of Pulmonary EmbolismFilip Banovac, MD, Donna C. Buckley, MD, MS, William T. Kuo, MD, Denver Matthew Lough, BS,
Louis G. Martin, MD, Steven F. Millward, MD, Timothy W.I. Clark, MD, MSc, Sanjoy Kundu, MD,Dheeraj K. Rajan, MD, David Sacks, MD, and John F. Cardella, MD, for the Technology Assessment Committeeof the Society of Interventional Radiology
J Vasc Interv Radiol 2010; 21:44–53
Abbreviations: CDT � catheter-directed therapy, DVT � deep venous thrombosis, IVC � inferior vena cava, PE � pulmonary embolism
PULMONARY embolism (PE) is a prev-alent disease with significant morbidityand mortality. The estimated annual in-cidence is 1.45 per 1,000 person-years(1), which translates to 1,350,000 casesper year in the United States (2). Theincidence of massive PE approached11% in a postmortem evaluation of alldeaths in one series (3). The 30-day mor-
From the Division of Interventional Radiology (F.B.)and the Departments of Radiology (D.C.B.) and Sur-gery (D.M.L.), Georgetown University Hospital,3800 Reservoir Rd, NW, Washington, DC 20007; theDivision of Vascular and Interventional Radiology,Stanford University Medical Center, Stanford,California (W.T.K.); the Department of Radiology,Division of Interventional Radiology, Emory Uni-versity School of Medicine, Emory UniversityHospital, Atlanta, Georgia (L.G.M.); the Depart-ment of Radiology, University of Western Ontario,London, and Peterborough Regional Health Cen-tre, Peterborough, Ontario, Canada (S.F.M.); theDepartment of Interventional Radiology, NewYork University School of Medicine, NYU MedicalCenter, New York, New York (T.W.I.C.); Scarbor-ough General Hospital, Toronto, Ontario, Canada(S.K.); the Division of Vascular and InterventionalRadiology, Department of Medical Imaging, Univer-sity of Toronto, University Health Network, To-ronto, Ontario, Canada (D.K.R.); The Reading Hos-pital and Medical Center, Advanced InterventionalRadiology, West Reading, Pennsylvania (D.S.); andGeisinger Health System, Danville, Pennsylvania(J.F.C.). Received September 1, 2009; accepted Sep-tember 28, 2009. Address correspondence to F.B.;E-mail: [email protected]
T.W.I.C. is a paid consultant for, has patent owner-ship or part ownership in, and has a royalty agree-ment with Merit Medical Systems Inc. D.K.R. is apaid consultant for CR Bard. None of the otherauthors have identified a conflict of interest.
© SIR, 2010
DOI: 10.1016/j.jvir.2009.09.018
44
tality rate for massive PE approached30% (4), and the presence of shock inthese patients defines a three- to seven-fold increase in mortality, with a major-ity of deaths occurring within 1 hour ofpresentation (5).
The role of the interventional radiol-ogist in the diagnosis and treatment ofPE continues to evolve. Traditionally,pulmonary angiography was per-formed as a diagnostic modality and formany years was the gold standard inthe diagnosis of PE. With the evolutionof computed tomographic (CT) angiog-raphy and marked improvement in thedetection of thromboembolic events, aswell as the development of endovascu-lar therapy with thrombectomy devices,the interventional radiologist’s role hasshifted from diagnosis to treatment ofPE. Although the mainstay of treatmentremains anticoagulation, more aggres-sive treatment is now possible in thehemodynamically unstable patient.
In cases of massive PE, interventionalradiologists have used catheter-directedthrombolytic therapy, mechanicalthrombectomy, or a combination of thetwo in an effort to rapidly restore pul-monary blood flow in a life-saving effort(6,7). Currently as of 2009, there are noclear evidence-based guidelines thatidentify those patients who should betreated more aggressively with endo-vascular therapies, nor are there stan-dard approaches to reporting clinicaltrial results in this area (8). The Ameri-can College of Chest Physicians recom-mends against the use of mechanical ap-
proaches for most patients with PE, butthe American College of Chest Physi-cians guidelines suggest that endovas-cular treatment of massive PE should beused in selected highly compromisedpatients who are unable to receive intra-venous systemic thrombolytic therapy orwhose critical status does not allow suffi-cient time to infuse thrombolytics (9).
The purpose of the current documentis to facilitate improved quality and rel-evance of clinical trials of endovasculartherapies for the treatment of PE by pro-viding a basic standardized frameworkfor reporting results in the literature.Current treatment options, patient pop-ulation considerations, endpoints, fol-low-up modalities, clinical trial designs,and statistical plans will be discussed.
CURRENT TREATMENTOPTIONS
Anticoagulation and SystemicThrombolytic Therapy
Presently, anticoagulation remainsthe preferred treatment for deep venousthrombosis (DVT) and thromboembolicdisease. There has been demonstratedreduction in mortality rates to an esti-mated 8% in patients who receive anti-coagulation for the treatment of PE (10),whereas untreated PE carries a mortal-ity rate of approximately 30% (9,11–13).Intravenous unfractionated heparin iscommonly used during initial hospital-ization to prevent propagation of exist-ing thrombus, and it has been long es-tablished that heparin decreases the
recurrence of life-threatening PE (14).
Banovac et al • 45Volume 21 Number 1
Typical regimens use unfractionatedheparin and/or low-molecular-weightheparin during hospitalization. Theseare later replaced by oral anticoagulants(eg, warfarin) for extended periods.
The standard American College ofChest Physicians–recommended medi-cal treatment for patients in extremisfrom massive PE (eg, failure to maintainblood pressure without supportive mea-sures) is systemic thrombolysis with tis-sue plasminogen activator (15). Use ofthis therapy has been considered on acase-by-case basis in the setting of per-sistent hypotension, severe hypoxemia,large perfusion defects, right ventriculardysfunction, free-floating right ventric-ular thrombus, and patent foramenovale (16,17). Systemic thrombolytictherapy compared with heparin was as-sociated with a significant reduction inrecurrent PE or death in trials that en-rolled patients with major (hemody-namically unstable) PE (18). However,the benefit of systemic thrombolytictherapy has not been established in pro-spective randomized trials and there is aknown increased risk of major hemor-rhage (ie, intracranial hemorrhage, ret-roperitoneal hemorrhage, bleedingleading to death, hospitalization ortransfusion) (19). The estimated rate ofmajor hemorrhage from systemic tissueplasminogen activator is approximately20%, including a 3%–5% rate of intrace-rebral hemorrhage, when used to treatacute PE (20,21).
A few nonrandomized clinical trialsand meta-analyses failed to demonstratea mortality benefit with thrombolytictherapy compared to anticoagulationalone (22,23), whereas others have sug-gested some mortality benefit (18,24). Ofnote is that most studies were designedto primarily evaluate the thrombolyticeffect and were not sufficiently poweredto detect differences in mortality. Somehave also suggested benefit of thrombo-lytics on important parameters includ-ing pulmonary arterial blood pressure,right ventricular function, pulmonaryperfusion, and reduced need for treat-ment of in-hospital events (25–28). Thetrue benefit of peripherally adminis-tered thrombolytic therapy, if any, hasto be established in prospective trials asnewer thrombolytic agents emerge. De-spite the lack of definitive data demon-strating a mortality benefit and theknown increased risk of major hemor-rhage, many clinicians may consider use
of systemic thrombolytics in patientswith hemodynamically unstable PE,who are at low risk for a bleeding event.
Catheter-directed Thrombolysis
Catheter-directed thrombolysis(CDT) is a technique that uses the deliv-ery of the thrombolytic agent directlyinto the thrombus through an endovas-cular catheter. CDT has been performedin patients with massive PE who couldnot tolerate systemic thrombolysis or inpatients who failed systemic thrombol-ysis.
In addition, CDT may be useful forpatients with relative contraindicationsto systemic anticoagulative treatmentsuch as recent abdominal surgery, preg-nancy, and severe allergic or idiosyn-cratic reactions to anticoagulants. CDThas been used in hemodynamically un-stable patients with massive PE who areat significant risk for bleeding complica-tions associated with systemic thrombo-lytic therapy. In addition, CDT has beenused to emergently treat massive PE re-fractory to systemic thrombolysis (29).
Because the main cause of death dueto massive PE is attributed to irrevers-ible right ventricular failure (30,31),early revascularization of the pulmo-nary bed in an effort to decrease rightventricular afterload has been a goal ofCDT. There is considerable debate re-garding the safety and efficacy of cath-eter-directed thrombolytic therapy, andthere is no evidence that direct infusioninto the pulmonary artery confersgreater benefit than peripheral venousinfusion (32). Nonetheless, some havesuggested that results from intrapulmo-nary thrombolytic infusion (ie, place-ment of catheter proximally in the pul-monary artery in a position remote fromthe embolus) may be inadequate andintra-embolus infusion is needed to pro-vide maximal pharmacologic and me-chanical lysis (33). Data are limited, andwell-controlled clinical trials are neces-sary to establish the safety and effective-ness profiles of catheter-directed throm-bolytic administration.
Mechanical Thrombectomy
There has been increased interest inthe use of mechanical thombectomy de-vices to treat PE. Many of these mechan-ical or rheolytic systems were originallydeveloped and/or approved for use insmaller blood vessels or grafts. Each of
these devices varies in design, ease ofuse, and efficacy in removing thrombus.They are designed to remove the throm-bus by suction (aspiration thrombec-tomy), macerate the thrombus and sendit distally (fragmentation), or create vor-tex forces that break up the thrombusand suction it into the catheter (rheolyticthrombectomy). Although some prelim-inary data regarding the treatment of PEwith the newer device technologies ap-pear promising, they are limited andnone of the endovascular techniqueshave been compared with other formsof therapy in prospective randomizedcontrolled studies.
Clinical data on the following de-vices have been reported in the litera-ture to date:
Fragmentation devices.—Varioustechniques have been reported to frag-ment thrombus in an effort to send par-ticles more distally and to expose alarger aggregate surface area of thethrombus to pharmacologic thrombo-lytic agents. There have been reports ofthe use of hand rotation of a standardpigtail catheter (34,35), a rotatable pig-tail catheter system (William Cook Eu-rope, Bjaeverskov, Denmark) (36), and asystem with an impeller that homoge-nizes clot (Amplatz Thrombectomy De-vice; Microvena, White Bear Lake, Min-nesota) (37). Adjunctive fragmentationwith an angioplasty balloon has alsobeen described (6,29).
Aspiration thrombectomy devices.—Various sheaths and guiding cathetershave been used in conjunction withfragmentation devices in an attempt toaspirate PE following clot fragmenta-tion. (29,38). The Aspirex device (StraubMedical, Wangs, Switzerland), a me-chanical thrombectomy catheter, con-sists of a high-speed rotational coil thataspirates, macerates, and removesthrombus through an L-shaped aspira-tion port at the catheter tip. In vitro andin vivo animal experiments demon-strated reversal of cardiogenic shock inthe setting of massive PE (39).
Rheolytic devices.—The Hydrolyserthrombectomy catheter (Cordis, Miami,Florida) (40–42) and Oasis thrombec-tomy catheter (40) (Boston Scientific,Natick, Massachusetts) create a vortexto draw thrombus into the catheter. TheAngioJet catheter (Possis Medical, Min-neapolis, Minnesota) (43,44) is a concep-tually similar over-the-wire system. Sev-eral complications have been reportedwith the AngioJet device, and it is un-
clear if its use for PE lysis should con-
ch th
46 • Reporting Standards for Endovascular Treatment of Pulmonary Embolism January 2010 JVIR
tinue. These complications include chestpain, hemolysis, hemoglobinuria, bra-dyarrhythmia, heart block, hypotension,and fatal hemoptysis (45–50).
Although evaluation of the safety andeffectiveness of endovascular mechani-cal thrombectomy is ongoing, a recentsystematic review and meta-analysis ofcatheter-based treatment for massive PEshowed a pooled clinical success rate of86.5% among 594 patients treated withmodern CDT, and the pooled rate ofmajor procedural complications was2.4% (51).
Surgical Embolectomy
Traditionally, massive PE wastreated by surgical embolectomy, withor without thrombolytic therapy. Surgi-cal embolectomy is performed as a lastresort in some institutions (52,53). In ad-dition to the aforementioned clinicalscenarios that may prompt more aggres-sive thrombolytic or catheter-basedtherapies, surgical embolectomy hasbeen prompted by echocardiographicevidence of right atrial or right ventric-ular clot as well as clot trapped in apatent foramen ovale (54). Surgical em-bolectomy has not been compared tocatheter-directed embolectomy or pri-mary thrombolytic therapy. However,outcomes data after surgical embolec-tomy are few. Actuarial survival aftersurgical embolectomy at 1-year fol-
Table 1Definitions of Terminology
PE IntravasProved PE PE prov
high-pmust
Symptomatic PE Clinicaltachy
Asymptomatic PE PE deteSuspected PE PE susp
not beVenous thromboembolism Single cDVT Presenc
methoMajor bleeding complication Intracra
and/oMajor vascular complication Any of
surgicnerve
Acute technical success SuccessfAcute procedural success Acute te
low-up was 86% at one center (55).
Placement of Inferior Vena Cava(IVC) Filters
IVC filters have been used to pre-vent large venous thrombi from em-bolizing to the lung by capturing theclot in the IVC. IVC filters have beenapproved by the U.S. Food and DrugAdministration for use in the manage-ment of acute PE in patients with anabsolute contraindication to anticoagu-lation or failure of anticoagulation. IVCfilters are also used in emergency treat-ment during massive PE as well aschronic, recurrent PE where anticoagu-lation has failed or is contraindicated. Inclinical practice, IVC filters have alsobeen placed in patients with poor car-diopulmonary reserve, patients whohave undergone embolectomy, and asprophylaxis in select patients (eg, malig-nancy, trauma) (56). Available data sug-gest that IVC filters decrease recurrentPE and increase recurrent DVT (57)without an effect on mortality (58).However, in a subgroup of patients withpersistent hypotension due to PE, a mor-tality benefit is suggested (16). To addressthe long-term complications with IVC fil-ter placement, removable filters have beendeveloped; however, data on their use arelimited and preliminary.
REPORTINGRECOMMENDATIONS
As new device technologies and
ar migration of a venous thrombus to theby a positive pulmonary angiogram, an u
bability ventilation-perfusion scan, or autoreportedsymptoms and/or signs such as chest paiiaon an imaging study in a patient withou
ed based on clinical symptoms and/or sigmade by imaging or autopsymon disease entity with two principal maf thrombus within a deep vein of the bodynd the extent of PE must be reported
l, intraocular, or retroperitoneal hemorrhagesulting in a hematocrit decrease �15% orfollowing related to the index procedure:
repair or US compression, false aneurysm,ury, retroperitoneal bleed, or procedure-redelivery of device to the site, operation ofnical success with achievement of intended
pharmaceuticals emerge, standardized
approaches to clinical evaluation willprove useful to facilitate comparabilityof results. Suggested standards of prac-tice for reporting those results are in-cluded below.
Definitions
Widely accepted definitions applica-ble to the current topic have been out-lined in the, “Reporting Standards forEndovascular Treatment of Lower Ex-tremity Deep Vein Thrombosis” (59).Relevant definitions from this documentas well as additional definitions are in-cluded in Table 1.
Patient Population
For clinical trials designed to assessthe use of endovascular therapies for thetreatment of PE, a thorough descriptionof the patient population is critical toallow for reasonable data interpretation.Standardized use of definitions as wellas customary approaches to patient se-lection including consideration of pa-tient risk factors, co-morbidities, andbaseline studies are important. A thor-ough discussion of the patient selectioncriteria is important to define the patientpopulation in consideration of knownand presumed independent risk factorsfor poor outcome, predisposing risk fac-tors for the development of PE, medicalco-morbidities that may affect outcome,and baseline diagnostic studies. Basic
lmonary arterial circulationuivocally positive helical CT scan, a; imaging method and the extent of PE
yspnea, hemoptysis, palpitations, or
inical symptomsbut for which definitive diagnosis has
stations: DVT and PEproved by diagnostic imaging; imaging
r any hemorrhage requiring transfusionmoglobin decrease �5 g/dL
atoma at access site �5 cm, vasculareriovenous fistula, peripheral ischemia/d transfusiondevice, and removal of the device
erapeutic goal
cul pued neqro psy
bePE n, d
cardcted t clect nsen
om nifee o asd a
nia e or r he
the hemal artinj lateul the
demographic data must be provided.

Banovac et al • 47Volume 21 Number 1
Study inclusion and exclusion criteriamust be specifically stated and themethod of assigning treatment to pa-tients must be described.
Risk factors for poor outcome.—Anti-coagulation has been shown to be effec-tive in reducing mortality associatedwith PE so the use of more aggressiveendovascular therapies is currently con-sidered indicated only for “high-risk”patients. Therefore, risk stratification iscritical in deciding which patientsshould undergo thrombolytic therapyor CDT. There are no definitive guide-lines to this effect; however, some inves-tigators have proposed criteria for endo-vascular treatment (7). Table 2 includesknown and presumed risk factors forpoor outcome from an acute PE. Con-sideration of this information, includingthe age and the functional status of thepatient, may prove useful in the devel-opment of relevant patient inclusion cri-teria and in the reporting of relevantbaseline characteristics. Furthermore,one may consider use of standardizedmeasures that have been used in priorstudies to assess the severity of illness.These include angiographic assess-ment scores (Miller index [60]), CTevaluation of the right ventriculardysfunction (61), the Urokinase Pul-monary Embolism Trial index (62),and the Shock index (63).
Risk factors for the development of ve-nous thromboembolism.—Considerationof predisposing risk factors for the de-velopment of venous thromboembolismmay also prove useful in secondaryanalyses of outcome. Known and pre-sumed predisposing risk factors for the
Table 2Risk Factors for Poor Outcome
Arterial hypotension �90 mm HgCirculatory collapse with need for
cardiopulmonary resuscitationShock with peripheral hypoperfusion
and hypoxiaRight heart strain at echocardiography
suggestive of pulmonaryhypertension
Significant PE on clinical basis and/orimaging in a patient withcontraindication to anticoagulationor thrombolytic therapy
Widened arterial-alveolar O2 gradient(�50 mm Hg)
Contraindication to anticoagulation
development of venous thrombosis
have been reported in the literature andare included in Table 3 (64–67).
Baseline evaluation.—Complete char-acterization of the baseline pretreatmentcondition is important to allow for clin-ical interpretation of study results, par-ticularly given that patients to be treatedwith endovascular techniques will likelybe a “high-risk” subset of PE patients.Baseline evaluation of the DVT distribu-tion and thrombus load and assessmentof PE location and severity should beincluded in the baseline evaluation.
Diagnosis and extent of DVT.—Ultrasonographic (US) examination ofthe lower extremities with localizationof the thrombus and overall thrombusburden should be performed and re-ported according to previously reportedstandards (59). Briefly, the baseline ana-tomic extent of thrombosis and the im-aging methods of diagnosis must bespecified. The proportion of patientswith calf vein DVT, femoropoplitealDVT, iliofemoral DVT, infrarenal IVCinvolvement, and suprarenal IVC in-volvement must be reported (59).
Diagnosis of extent and severity ofPE.—Currently, CT angiography hasbecome the clinically preferred modal-ity to diagnose PE and has largely re-placed pulmonary angiography at mostinstitutions (68,69). CT angiography of-fers good specificity for the detection ofPE in main, lobar, and segmental arter-ies and also facilitates the diagnosis ofother disease entities (17,70–72). The
Table 3Risk Factors for the Development ofVenous Thromboembolism
Chronic heart diseaseFracture of long boneHeavy cigarette smoking (�25
cigarettes per day)History of thromboembolismHypercoagulable state (primary and
acquired)HypertensionImmobilizationIncreased ageIndwelling venous cathetersMalignancyObesity (body mass index �29 kg/m2)Oral contraceptive usePreexisting respiratory diseasePregnancy and postpartum stateStrokeSurgeryVaricose veins
sensitivity and specificity of CT angiog-
raphy is expected to improve with im-proved CT technology (eg, higher con-trast resolution with better peripheralvisualization, less motion artifact) andgreater experience with scan interpreta-tion. CT angiography may also be usedto evaluate the extent and location ofclot and may, in some cases, give infor-mation regarding the severity of PE. Forexample, CT angiography may offer in-formation regarding noncontroversialindicators of severity (eg, right ventric-ular/left ventricular diameter ratio, IVCdiameter, and azygos diameter) as wellas controversial indicators of severity(eg, pulmonary artery clot load, pulmo-nary artery diameter, septal bowing,IVC contrast reflux) (73). While informa-tion regarding the predictors of severityincreases, it may prove useful to reportknown and potential imaging predic-tors for future analysis.
Other baseline testing.—Advancesare also being made with the use ofmagnetic resonance (MR) angiographyand diffusion imaging with hyperpolar-ized helium 3 in the diagnosis of PE. Astechnical problems (eg, respiratory/cardiac artifact, suboptimal resolution,susceptibility artifact from adjacentlung) and logistical problems (eg, MRscheduling, study time, screening is-sues) are addressed, MR angiographymay have an increased role in the diag-nosis of PE in the future (74).
Each patient being considered for en-dovascular therapy should undergobaseline imaging to diagnose PE (ie, CTangiography, ventilation-perfusionscanning, pulmonary angiography,and/or MR angiography), and the diag-nostic modality should be justified.Given current clinical practice, it is ex-pected that CT angiography will be thepreferred method to diagnose and char-acterize massive PE.
Patients who present with symptomsand signs of PE (ie, dyspnea, pleuriticchest pain, tachypnea, tachycardia) willoften get a preliminary work-up to in-clude vital signs, basic blood work(complete blood count, chemistries),electrocardiography, arterial bloodgases, and chest radiography. Thesetests are nonspecific and furtherevaluation is required for diagnosis.Additional tests that may have diag-nostic and/or prognostic roles in thedetection and treatment of PE are
included in Table 4.
48 • Reporting Standards for Endovascular Treatment of Pulmonary Embolism January 2010 JVIR
TREATMENT DESCRIPTION
Device Description and ProcedureDescription
Information regarding the device(s)selected for treatment should be pro-vided, including a description of the de-vice (name, model, manufacturer), itsmechanism of action, and the reasonwhy it was chosen. If multiple devicesare included in a single study, clarifica-tion should be provided regarding themethod by which devices were se-lected for use. Details regarding theprocedure should be provided, in-cluding technique, procedure length,need for sedation, venous access,and procedural medications. In par-ticular, details must be provided re-garding thrombolytic drug type anddose and the method of transluminalremoval of thrombus from the pul-monary arterial system.
Systemic thrombolysis refers to a formof pharmacologic thrombolysis wherethe infusion of the agent is administeredthrough an intravenous line that is dis-tant from the pulmonary system.
Flow-directed thrombolysis refers to aform of pharmacologic thrombolysiswhere the infusion is administeredthrough a catheter that is positioned inthe pulmonary artery proximal to thelocation of pulmonary artery throm-bus.
Catheter directed intrathrombus throm-bolysis refers to the delivery of the
Table 4Diagnostic Tests
Duplex US Duplex US hRegardingtherefore, eprior to int
BNP BNP may beAlthough tmay provid
Troponin Similar to BNto BNP, elewith PE (egthat includ
D-dimer D-dimer assaspecificityprognosis,
Echocardiography Echocardiogrdecreased r30%–40% (increase in
Note.—BNP � brain natriuretic peptide.
thrombolytic agent into the pulmonary
artery thrombus through an infusioncatheter, such as a multi-side-hole cath-eter, that is positioned into the throm-bus. In appropriate situations, a lacingdose or a bolus can be given into thethrombus–-usually at the initiation oftherapy.
Mechanical thrombectomy refers to amethod of thrombus removal through acatheter system that removes the throm-bus by aspiration, fragmentation ormaceration or combination of these.
Pharmacomechanical thrombectomy re-fers to thrombus removal using a com-bination of pharmacologic thrombolyticagents and a mechanical catheter-baseddevice.
Concomitant Medical Therapies andProcedures and Intention to TreatAnalysis
Concomitant medical therapies (eg,pharmacologic lysis for residual throm-bus) and procedures (eg, IVC filterplacement) will likely play a significantrole in the endovascular treatment ofPE; therefore, effort should be made todevelop prospective medical therapyregimens and/or algorithmic ap-proaches to treatment such that theirrole as confounding variables is limited.Data should be collected and reportedregarding the type of medications, dose,method of administration, and rationalefor use. Parenteral agents that may beused include anticoagulants or platelet
argely replaced diagnostic venography forcurrent topic, the presence of massive PE
uation for DVT is not intended to facilitatention and to serve as a potential covarianvated in acute PE presumed secondary tomagnitude of BNP elevation is nonspecificrognostic information regarding benign v
serum troponin I and troponin T are elevaed troponin is nonspecific but may also ofortality risk) (79). Recently, some have prcombination of BNP and troponin valuesfor the diagnosis of PE have good sensitiv. Attempts have been made to correlate Dthis approach is not widely accepted.ic evidence of right ventricular dysfunctiot ventricular function, tricuspid regurgitatRight ventricular dysfunction has been sh
-related mortality (83).
inhibitors. Drug doses and appropriate
laboratory values must be reported. Theauthors must state what treatment wasintended and what was actually admin-istered. Any use of adjunctive therapiesnot included in the original protocolshould be reported as deviations andconsidered intent-to-treat failures. Forexample, if the protocol for the endovas-cular procedure includes mechanicalthrombectomy alone, any use of addi-tional pharmacologic lysis would beconsidered a treatment failure. Con-versely, if the endovascular treatmentincludes planned adjunctive pharmaco-logic treatment (local or systemic) thenthese cases would not be treatment fail-ures. Nonetheless, the control group orcriteria to which the combined pharma-comechanical thrombectomy procedureis compared should be established toelucidate a difference (ie, benefit) withthe addition of the endovascular devicecompared to thrombolysis alone. Fur-thermore, the protocol should includespecific directions regarding the use ofIVC filters.
Control Group
Detailed information should be pro-vided regarding the control treatmentagainst which the endovascular treat-ment is compared. For example, com-parison to a thrombolytic agent shouldinclude details regarding the agent,dose (ie, bolus, infusion rate, infusion
e detection and characterization of DVT.uld not be a diagnostic dilemma;
iagnosis, rather to define vessel patencyegarding outcome.reased right ventricular wall stress.me have suggested that BNP levels
us complicated clinical course (77).in some patients with PE (78). Similarsome prognostic information in patientssed biomarker risk stratification models
).and negative predictive value, but poor
er values with extent of disease and
ie, increased right ventricular volume,) in patients is estimated to be onlyn to be associated with a two-fold
as l ththe shoval e derv t rele inche , soe p ersP, tedvat fer, m opo
e a (80ys ity(81) -dimbutaph n (igh ion
82). owPE
time) and method of administration.

Banovac et al • 49Volume 21 Number 1
FOLLOW-UP MODALITIESAND SCHEDULES
Currently, the vast majority of re-ports of interventional procedures con-ducted for the purpose of treating PEinclude retrospective analyses of casesconducted at one or a few institutions.For this reason, reports of outcome oftenrelate to the index procedure or to asubsequent review of the medicalrecord to draw conclusions regardingcomplications and overall medical con-dition. Ideally, trials should be con-ducted with prospective follow-up,with the frequency and type of fol-low-up depending on the specific re-search question. Nonetheless, there arestandard patient assessments thatshould be conducted and reported forall trials. Baseline evaluation should in-clude physical examination, basic labo-ratory tests (eg, chemistries includingcoagulation), CT angiography (or othermodality used to diagnose PE), and as-sessment of the severity of cardiopul-monary compromise. Follow-up evalu-ation should include at least a physicalexamination, monitoring laboratorystudies (eg, prothrombin time, partialthromboplastin time, international nor-malized ratio), assessment of residualPE, and assessment of overall medicalcondition. Follow-up should continue toevaluate for recurrence of PE, long-termeffects of therapy (eg, unintended vas-cular damage secondary to mechanicalthrombolysis), and stability of acute out-comes. The protocol must specify thenature and timing of clinical and imag-ing follow-up, and results of this fol-low-up must be reported. Prospectivelydeveloped Case Report Forms shouldbe used to record all relevant follow-upinformation and explanations should beprovided regarding any patients who
Table 5Endpoints
Safety DeathMajor bleedOther major
(eg, strokeretrospectiadjudicateit is preferreview (ie
Effectiveness Acute technAcute proce
missed a follow-up examination. The
outcomes such as of treatment can beevaluated with follow-up intervalsgraded as short-term (�30 days), mid-term (30 days to 1 year), or long-term(�1 year).
PRIMARY AND SECONDARYOUTCOMES MEASURES
Treatment decisions regarding endo-vascular therapies for the treatment ofPE will likely be based on the conceptthat the increased risk to the patient as-sociated with a more invasive treatmentmay be justified if the benefit to the pa-tient outweighs the risk. Therefore, rig-orous collection of both safety and effi-cacy outcome measures is essential.Table 5 includes a list of basic clinicallyrelevant endpoints that should be re-ported for all devices.
In developing primary and second-ary safety endpoints, one may con-sider the potential adverse eventslisted in Table 6. Additional relevantefficacy endpoints may also be consid-ered (eg, length of hospitalization).
Details regarding hemodynamic andphysiologic parameters of a procedureshould include baseline and posttreat-ment pulmonary artery pressures andoxygen saturations. Pulmonary angiog-raphy performed during the procedureshould include arterial, parenchymal,and venous phases. The contrast agentand the volume used during angiogra-phy should be reported.
When reporting clinical trial results,the measures that are primary and thosethat are secondary should be clear andprospectively established. Attemptsshould be made to choose primary end-points that have the most direct clinicalrelevance and would be the most mean-ingful to consider in future treatment
and major vascular complicationsverse events may be prospectively listedyocardial infarction) or establishedy. If events are retrospectivelynd categorized as “major” or “minor,”that each event undergo independent
inical Events Committee).successal success
decisions (eg, reduction in mortality,
acute clinical success). Surrogate pri-mary efficacy endpoints should beavoided where possible (eg, improve-ment in right ventricular dysfunction,reduction in clot burden). All complica-tions should be reported on a per-patient basis and categorized accordingto the SIR classification of Complica-tions by Outcome shown in Table 7 (75).
CLINICAL TRIAL DESIGNAND STATISTICAL PLAN
In general, the randomized con-
Table 6Potential and Observed AdverseEvents
AneurysmAnginaArrhythmiasArteriovenous fistulaCardiac tamponadeCardiogenic shockDissectionDrug reactions to contrast,
thrombolytics, or anticoagulationForeign body embolizationFistulizationHemoglobinuriaHemolysisHemoptysisHypo/hypertensionInfectionMyocardial infarctionPerforation or rupturePericardial effusionPseudoaneurysmRenal failureRespiratory failureStroke/transient ischemic attackValvular injury/insufficiency
Table 7SIR Classification of Complicationsby Outcome
Minor complicationsNo therapy, no consequenceNominal therapy, no consequence;
includes overnight admission forobservation only
Major complicationsRequire therapy, minor
hospitalization (�48 h)Require major therapy, unplanned
increase in level of care, prolongedhospitalization (�48 h)
Permanent adverse sequelaeDeath
ingad, mveld ared, Clicaldur
trolled trial is the preferred trial design
50 • Reporting Standards for Endovascular Treatment of Pulmonary Embolism January 2010 JVIR
to evaluate new treatments because ofinherent benefits to (a) minimize bias, (b)increase the likelihood that comparablegroups will actually be compared bybalancing known and unknown covari-ates, (c) allow for comparability of treat-ments in the current situation wherethere is the lack of a clear control group,and (d) provide the best evidence so asto avoid providing unnecessary treat-ment to some patients with all of itsattendant costs and risks. Unfortu-nately, it is recognized that randomizedtrials are difficult to conduct in the eval-uation of all new medical treatmentsand particularly difficult to employ inthe evaluation of treatments of “last re-sort.” This is the case for endovasculartreatment of PE, because patients withnonmassive PE are treated safely andeffectively pharmacologically and theanticipated increased risk with invasivetreatment is not expected to confer sig-nificant offsetting incremental benefit.Initially, it is expected that the evalua-tion of the feasibility of endovasculartreatment of PE will be reserved forpatients with massive PE; therefore,comparison may be made with mo-dalities that constitute current stan-dard of care given severity of illnessas defined by the patient selectioncriteria. For some trials, comparisonto the expected natural course of thedisease may be appropriate. For non-randomized trial designs, every effortshould be made to maximize method-ologic rigor—especially when evaluatingnew devices.
Reports should indicate the over-all trial design and identify the num-ber of patients and the number ofinvestigational sites. The rationalefor choosing a particular trial designshould be stated, and any limitationsof the chosen design should be dis-cussed. The process by which pa-tients have been screened, enrolled,and assigned to a particular treat-ment should be described.
All prospective trials should be de-signed with sufficiently powered sam-ple sizes calculated from estimatedevent rates based on the primary end-point. Randomized trials should alsobe performed in accordance with Con-solidated Standards of Reporting Trials(CONSORT) guidelines (76). Inclusionof the hypothesis in mathematical termsis helpful in focusing the reader on the
specific research question around whichthe trial is designed. If more novel sta-tistical methods are used (eg, Bayesian,sequential designs), a brief discussion ofthe statistical method should be in-cluded. Primary statistical analysesshould be reported on an intent-to-treatbasis. A per-protocol analysis may alsobe reported.
If more than one primary end-point is stated, the estimated samplesize should have sufficient power todetect differences between groupsfor all primary endpoints. Results forsecondary endpoints may be re-ported; however, caution should beused when making statements re-garding the significance of those re-sults. Discussion of significant find-ings should be restricted to those forwhich prospective statistical analy-ses were planned.
If more than one device is used, anexplanation should be provided regard-
Table 8Recommendations for Research Reportin
Data
Population descriptionInclusion/exclusion criteriaDemographic informationMethod of treatment assignmentImaging method of PE diagnosisChronicity (acute vs chronic)Detailed risk factor descriptionDescription of co-morbiditiesBaseline anatomic extent of embolusBaseline DVT distribution and extent
Treatment descriptionVenous access siteUse of concomitant anticoagulation, doRoute of delivery (systemic vs intrathroThrombolytic agent, dose, durationDevice used, manufacturer, modelDuration of device activation timeMechanical maceration used?Aspiration thrombectomy used?Concomitant IVC filter used?Standardized measures of severity of ilAdjunctive surgical procedures
Outcomes assessmentTechnical successClinical success and failureTime to symptom improvementDegree of thrombolysis by angiographyComplications classified by SIR outcomDescription of adverse events
AnalysisDescription of study designInstitutional review board approvalDescription of statistical methods
ing how the data were stratified and
how this issue was addressed duringthe prospective statistical plan.
CONCLUSIONS
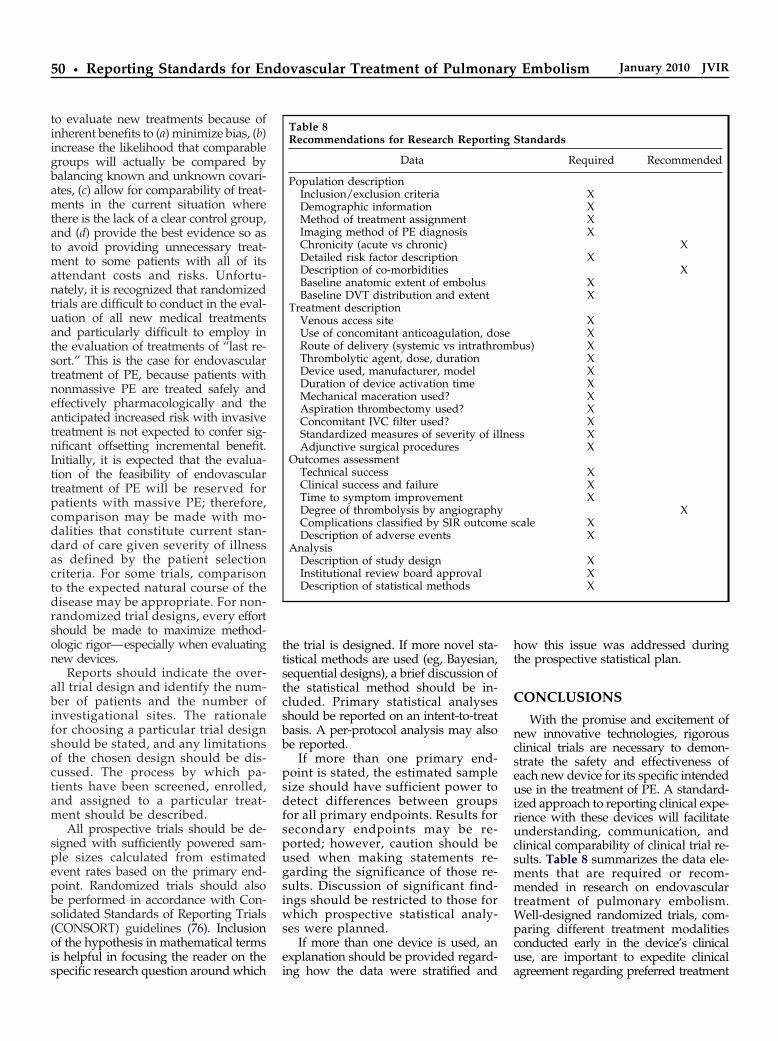
With the promise and excitement ofnew innovative technologies, rigorousclinical trials are necessary to demon-strate the safety and effectiveness ofeach new device for its specific intendeduse in the treatment of PE. A standard-ized approach to reporting clinical expe-rience with these devices will facilitateunderstanding, communication, andclinical comparability of clinical trial re-sults. Table 8 summarizes the data ele-ments that are required or recom-mended in research on endovasculartreatment of pulmonary embolism.Well-designed randomized trials, com-paring different treatment modalitiesconducted early in the device’s clinicaluse, are important to expedite clinical
Standards
Required Recommended
XXXX
XX
XXX
XX
us) XXXXXXX
ss XX
XXX
Xcale X
X
XXX
g
semb
lne
e s
agreement regarding preferred treatment

Banovac et al • 51Volume 21 Number 1
based on reasoned assessments of devicesafety and effectiveness and will ulti-mately allow more patients to receive thebest established treatment.
Acknowledgments: Filip Banovac au-thored the first draft of this document andserved as topic leader during the subsequentrevisions of the draft. Steven F. Millward isChair of the Technology Assessment Com-mittee. John F. Cardella is Councilor of theSIR Standards Division. Other members ofthe Technology Committee within SIR whoparticipated in the development of this Re-porting Standard are (listed alphabetically):Mark Baerlocher, MD, John Dean Barr, MD,Gary J. Becker, MD, Carl M. Black, MD, JohnJ. Borsa, MD, Matthew R. Callstrom, MD,Drew M. Caplin, MD, Thomas M. Carr, MD,William B. Crenshaw, MD, Michael D. Dake,MD, Aron Michael Devane, MD, B. JanneD’Othee, MD, Salomao Faintuch, MD, RonC. Gaba, MD, Joseph Gemmete, MD, DebraAnn Gervais, MD, Craig B. Glaiberman, MD,S. Nahum Goldberg, MD, Neil J. Halin, DO,Thomas B. Kinney, MD, Michael D Kuo,MD, John A. Lippert, MD, Llewellyn V.Lee, MD, Philip M. Meyers, MD, David A.Phillips, MD, Stefanie M. Rosenberg, PA,David A. Rosenthal, PA, James E. Silberz-weig, MD, Richard Towbin, MD, Michael J.Wallace, MD, and John York, MD.
References1. Tsai AW, Cushman M, Rosamond WD,
Heckbert SR, Polak JF, Folsom AR.Cardiovascular risk factors and venousthromboembolism incidence: the longi-tudinal investigation of thromboembo-lism etiology. Arch Intern Med 2002; 162:1182–1189.
2. Goldhaber SZ. Pulmonary embolism.Lancet 2004; 363:1295–1305.
3. Green J, Edwards C. Seasonal varia-tion in the necropsy incidence of mas-sive pulmonary embolism. J ClinPathol 1994; 47:58–60.
4. Heit JA, Silverstein MD, Mohr DN,Petterson TM, O’Fallon WM, Melton LJIII. Predictors of survival after deepvein thrombosis and pulmonary embo-lism: a population-based, cohort study.Arch Intern Med 1999; 159:445–453.
5. Wood KE. Major pulmonary em-bolism: review of a pathophysiologicapproach to the golden hour of hemody-namically significant pulmonary embo-lism. Chest 2002; 121:877–905.
6. De Gregorio MA, Gimeno MJ, MainarA, et al. Mechanical and enzymaticthrombolysis for massive pulmonaryembolism. J Vasc Interv Radiol 2002;13:163–169.
7. Uflacker R. Interventional therapyfor pulmonary embolism. J Vasc Interv
Radiol 2001; 12:147–164.8. Konstantinides S. Diagnosis and ther-apy of pulmonary embolism. Vasa 2006;35:135–146.
9. Hirsh J, Guyatt G, Albers GW, Har-rington R, Schunemann HJ. Executivesummary: American College of ChestPhysicians evidence-based clinical prac-tice guidelines (8th ed). Chest 2008; 133:71S–109S.
10. Carson JL, Kelley MA, Duff A, et al.The clinical course of pulmonary em-bolism. N Engl J Med 1992; 326:1240–1245.
11. Horlander KT, Mannino DM, LeeperKV. Pulmonary embolism mortalityin the United States, 1979–1998: ananalysis using multiple-cause mortal-ity data. Arch Intern Med 2003; 163:1711–1717.
12. Dismuke SE, Wagner EH. Pulmonaryembolism as a cause of death: thechanging mortality in hospitalized pa-tients. JAMA 1986; 255:2039–2042.
13. Dalen JE, Alpert JS. Natural historyof pulmonary embolism. Prog Cardio-vasc Dis 1975; 17:259–270.
14. Barritt DW, Jordan SC. Anticoagulantdrugs in the treatment of pulmonaryembolism: a controlled trial. Lancet1960; 1:1309–1312.
15. Buller HR, Agnelli G, Hull RD, HyersTM, Prins MH, Raskob GE.Antithrombotic therapy for venousthromboembolic disease: the SeventhACCP Conference on Antithromboticand Thrombolytic Therapy. Chest 2004;126:401S–428S.
16. Kucher N, Rossi E, De Rosa M, Gold-haber SZ. Massive pulmonary embo-lism. Circulation 2006; 113:577–582.
17. Guidelines on diagnosis and manage-ment of acute pulmonary embolism.Task Force on Pulmonary Embolism,European Society of Cardiology. EurHeart J 2000; 21:1301–1336.
18. Wan S, Quinlan DJ, Agnelli G, Eikel-boom JW. Thrombolysis comparedwith heparin for the initial treatment ofpulmonary embolism: a meta-analysisof the randomized controlled trials.Circulation 2004; 110:744–749.
19. Levine MN, Raskob G, Beyth RJ, Ke-aron C, Schulman S. Hemorrhagiccomplications of anticoagulant treat-ment: the Seventh ACCP Conferenceon Antithrombotic and ThrombolyticTherapy. Chest 2004; 126:287S–310S.
20. Goldhaber SZ, Visani L, De Rosa M.Acute pulmonary embolism: clinicaloutcomes in the International Cooper-ative Pulmonary Embolism Registry(ICOPER). Lancet 1999; 353:1386–1389.
21. Fiumara K, Kucher N, Fanikos J, Gold-haber SZ. Predictors of major hemor-rhage following fibrinolysis for acutepulmonary embolism. Am J Cardiol
2006; 97:127–129.22. Thabut G, Thabut D, Myers RP, et al.Thrombolytic therapy of pulmonaryembolism: a meta-analysis. J Am CollCardiol 2002; 40:1660–1667.
23. Dong B, Jirong Y, Liu G, Wang Q, WuT. Thrombolytic therapy for pulmo-nary embolism. Cochrane DatabaseSyst Rev 2006; CD004437.
24. Agnelli G, Becattini C, Kirschstein T.Thrombolysis vs heparin in the treat-ment of pulmonary embolism: a clini-cal outcome-based meta-analysis. ArchIntern Med 2002; 162:2537–2541.
25. Sharma GV, Burleson VA, SasaharaAA. Effect of thrombolytic therapyon pulmonary-capillary blood volumein patients with pulmonary embolism.N Engl J Med 1980; 303:842–845.
26. Come PC. Echocardiographic evalua-tion of pulmonary embolism and itsresponse to therapeutic interventions.Chest 1992; 101:151S–162S.
27. Goldhaber SZ, Haire WD, FeldsteinML, et al. Alteplase versus heparin inacute pulmonary embolism: random-ised trial assessing right-ventricularfunction and pulmonary perfusion.Lancet 1993; 341:507–511.
28. Konstantinides S, Geibel A, Heusel G,Heinrich F, Kasper W. Heparin plusalteplase compared with heparin alonein patients with submassive pulmo-nary embolism. N Engl J Med 2002;347:1143–1150.
29. Kuo WT, van den Bosch MA, HofmannLV. Catheter-directed embolectomy,fragmentation, and thrombolysis forthe treatment of massive pulmonaryembolism after failure of systemicthrombolysis. Chest 2007; 132:663S.
30. Pruszczyk P, Pacho R, Ciurzynski M,et al. Short term clinical outcome ofacute saddle pulmonary embolism.Heart 2003; 89:335–336.
31. Ribeiro A, Lindmarker P, Juhlin-Dann-felt A, Johnsson H, Jorfeldt L.Echocardiography Doppler in pulmo-nary embolism: right ventricular dys-function as a predictor of mortality rate.Am Heart J 1997; 134:479–487.
32. Verstraete M, Miller GA, BounameauxH, et al. Intravenous and intrapulmo-nary recombinant tissue-type plasmin-ogen activator in the treatment of acutemassive pulmonary embolism. Circu-lation 1988; 77:353–360.
33. Tapson VF, Gurbel PA, Witty LA, PieperKS, Stack RS. Pharmacomechanicalthrombolysis of experimental pulmonaryemboli: rapid low-dose intraembolic ther-apy. Chest 1994; 106:1558–1562.
34. Brady AJ, Crake T, Oakley CM.Percutaneous catheter fragmentationand distal dispersion of proximalpulmonary embolus. Lancet 1991; 338:1186 –1189.
35. Barbosa MA, Oliveira DC, Barbosa AT,
et al. Treatment of massive pulmo-
52 • Reporting Standards for Endovascular Treatment of Pulmonary Embolism January 2010 JVIR
nary embolism by percutaneous frag-mentation of the thrombus. Arq BrasCardiol 2007; 88:279–284.
36. Schmitz-Rode T, Janssens U, Duda SH,Erley CM, Gunther RW. Massive pul-monary embolism: percutaneous emer-gency treatment by pigtail rotationcatheter. J Am Coll Cardiol 2000; 36:375–380.
37. Uflacker R, Strange C, Vujic I. Massivepulmonary embolism: preliminary resultsof treatment with the Amplatz thrombec-tomy device. J Vasc Interv Radiol 1996;7:519–528.
38. Tajima H, Murata S, Kumazaki T, et al.Hybrid treatment of acute massive pul-monary thromboembolism: mechani-cal fragmentation with a modified ro-tating pigtail catheter, local fibrinolytictherapy, and clot aspiration followedby systemic fibrinolytic therapy. AJRAm J Roentgenol 2004; 183:589–595.
39. Kucher N, Windecker S, Banz Y, et al.Percutaneous catheter thrombectomydevice for acute pulmonary embolism:in vitro and in vivo testing. Radiology2005; 236:852–858.
40. Fava M, Loyola S, Bertoni H, DougnacA. Massive pulmonary embolism: per-cutaneous mechanical thrombectomyduring cardiopulmonary resuscitation. JVasc Interv Radiol 2005; 16:119–123.
41. Fava M, Loyola S, Huete I. Massivepulmonary embolism: treatment withthe hydrolyser thrombectomy cathe-ter. J Vasc Interv Radiol 2000; 11:1159 –1164.
42. Michalis LK, Tsetis DK, Rees MR.Case report: percutaneous removal ofpulmonary artery thrombus in a pa-tient with massive pulmonary embo-lism using the hydrolyser catheter: thefirst human experience. Clin Radiol1997; 52:158–161.
43. Koning R, Cribier A, Gerber L, et al. Anew treatment for severe pulmonaryembolism: percutaneous rheolyticthrombectomy. Circulation 1997; 96:2498–2500.
44. Zeni PT Jr, Blank BG, Peeler DW. Useof rheolytic thrombectomy in treat-ment of acute massive pulmonary em-bolism. J Vasc Interv Radiol 2003; 14:1511–1515.
45. Sze DY, Carey MB, Razavi MK.Treatment of massive pulmonary em-bolus with catheter-directed tenect-eplase. J Vasc Interv Radiol 2001; 12:1456–1457.
46. Kumar N, Janjigian Y, Schwartz DR.Paradoxical worsening of shock afterthe use of a percutaneous mechanicalthrombectomy device in a postpartumpatient with a massive pulmonary em-bolism. Chest 2007; 132:677–679.
47. Sharafuddin MJ, Hicks ME, Jenson ML,Morris JE, Drasler WJ, Wilson GJ.
Rheolytic thrombectomy with use ofthe AngioJet-F105 catheter: preclinicalevaluation of safety. J Vasc IntervRadiol 1997; 8:939–945.
48. Biederer J, Schoene A, Reuter M, HellerM, Muller-Hulsbeck S. Suspectedpulmonary artery disruption aftertransvenous pulmonary embolectomyusing a hydrodynamic thrombectomydevice: clinical case and experimentalstudy on porcine lung explants. J En-dovasc Ther 2003; 10:99–110.
49. Dwarka D, Schwartz SA, Smyth SH,O’Brien MJ. Bradyarrhythmias dur-ing use of the AngioJet system. J VascInterv Radiol 2006; 17:1693–1695.
50. Fontaine AB, Borsa JJ, Hoffer EK, BlochRD, So CR, Newton M. Type III heartblock with peripheral use of the Angio-jet thrombectomy system. J Vasc IntervRadiol 2001; 12:1223–1225.
51. Kuo WT, Gould MK, Louie JD, Rosen-berg JK, Sze DY, Hofmann LV.Catheter-directed therapy for the treat-ment of massive pulmonary embolism:systematic review and meta-analysis ofmodern techniques. J Vasc Interv Ra-diol 2009; 20:1431–1440.
52. Jamieson SW, Auger WR, Fedullo PF, etal. Experience and results with 150 pul-monary thromboendarterectomy opera-tions over a 29-month period. J ThoracCardiovasc Surg 1993; 106:116–126.
53. Archibald CJ, Auger WR, Fedullo PF, etal. Long-term outcome after pulmo-nary thromboendarterectomy. Am J Re-spir Crit Care Med 1999; 160:523–528.
54. Bloomfield P, Boon NA, de Bono DP.Indications for pulmonary embolec-tomy. Lancet 1988; 2:329.
55. Leacche M, Unic D, Goldhaber SZ, etal. Modern surgical treatment of mas-sive pulmonary embolism: results in 47consecutive patients after rapid diag-nosis and aggressive surgical ap-proach. J Thorac Cardiovasc Surg 2005;129:1018–1023.
56. Knudson MM, Ikossi DG, Khaw L,Morabito D, Speetzen LS.Thromboembolism after trauma: ananalysis of 1602 episodes from the Amer-ican College of Surgeons NationalTrauma Data Bank. Ann Surg 2004; 240:490–496, discussion 496–498.
57. Decousus H, Leizorovicz A, Parent F,et al. A clinical trial of vena caval fil-ters in the prevention of pulmonaryembolism in patients with proximaldeep-vein thrombosis. Prevention duRisque d’Embolie Pulmonaire par In-terruption Cave Study Group. N EnglJ Med 1998; 338:409–415.
58. Eight-year follow-up of patients withpermanent vena cava filters in the pre-vention of pulmonary embolism: thePREPIC (Prevention du Risque d’EmboliePulmonaire par Interruption Cave) ran-domized study. Circulation 2005; 112:416–
422.59. Vedantham S, Grassi CJ, Ferral H, et al.Reporting standards for endovasculartreatment of lower extremity deep veinthrombosis. J Vasc Interv Radiol 2006;17:417–434.
60. Miller GA, Sutton GC, Kerr IH, GibsonRV, Honey M. Comparison of strep-tokinase and heparin in treatment ofisolated acute massive pulmonary em-bolism. Br Med J 1971; 2:681–684.
61. van der Meer RW, Pattynama PM, vanStrijen MJ, et al. Right ventriculardysfunction and pulmonary obstruc-tion index at helical CT: prediction ofclinical outcome during 3-month fol-low-up in patients with acute pulmo-nary embolism. Radiology 2005; 235:798–803.
62. The urokinase pulmonary embolismtrial: a national cooperative study.Circulation 1973; 47(2 Suppl):II1–108.
63. Rady MY, Smithline HA, Blake H,Nowak R, Rivers E. A comparison ofthe shock index and conventional vitalsigns to identify acute, critical illness inthe emergency department. Ann EmergMed 1994; 24:685–690.
64. Value of the ventilation/perfusion scanin acute pulmonary embolism: resultsof the prospective investigation of pul-monary embolism diagnosis (PIOPED).The PIOPED Investigators. JAMA 1990;263:2753–2759.
65. Miniati M, Prediletto R, Formichi B, et al.Accuracy of clinical assessment in thediagnosis of pulmonary embolism. Am JRespir Crit Care Med 1999; 159:864–871.
66. Darze ES, Latado AL, Guimaraes AG,et al. Incidence and clinical predictorsof pulmonary embolism in severe heartfailure patients admitted to a coronarycare unit. Chest 2005; 128:2576–2580.
67. Goldhaber SZ, Grodstein F, StampferMJ, et al. A prospective study of riskfactors for pulmonary embolism inwomen. JAMA 1997; 277:642–645.
68. Ghaye B, Ghuysen A, Bruyere PJ, D’OrioV, Dondelinger RF. Can CT pulmo-nary angiography allow assessment ofseverity and prognosis in patients pre-senting with pulmonary embolism?What the radiologist needs to know. Ra-diographics 2006; 26:23–39, discussion39–40.
69. Schoepf UJ, Costello P. CT angiogra-phy for diagnosis of pulmonary embo-lism: state of the art. Radiology 2004;230:329–337.
70. Krishnan JA, Segal JB, Streiff MB, et al.Treatment of venous thromboembo-lism with low-molecular-weight hepa-rin: a synthesis of the evidence pub-lished in systematic literature reviews.Respir Med 2004; 98:376–386.
71. Washington L, Goodman LR, GonyoMB. CT for thromboembolic disease.
Radiol Clin North Am 2002; 40:751–771.
Banovac et al • 53Volume 21 Number 1
72. Rathbun SW, Raskob GE, Whitsett TL.Sensitivity and specificity of helical com-puted tomography in the diagnosis ofpulmonary embolism: a systematic re-view. Ann Intern Med 2000; 132:227–232.
73. Ghaye B, Ghuysen A, Willems V, et al.Severe pulmonary embolism: pulmo-nary artery clot load scores and cardio-vascular parameters as predictors ofmortality. Radiology 2006; 239:884–891.
74. Haage P, Piroth W, Krombach G, et al.Pulmonary embolism: comparison ofangiography with spiral computed to-mography, magnetic resonance an-giography, and real-time magnetic res-onance imaging. Am J Respir Crit CareMed 2003; 167:729–734.
75. Sacks D, Marinelli DL, Martin LG,Spies JB. Reporting standards forclinical evaluation of new peripheralarterial revascularization devices. J
Vasc Interv Radiol 2003; 14:S395–S404.76. Begg C, Cho M, Eastwood S, et al.Improving the quality of reporting ofrandomized controlled trials. TheCONSORT statement. JAMA 1996; 276:637–639.
77. Kucher N, Printzen G, Goldhaber SZ.Prognostic role of brain natriureticpeptide in acute pulmonary embolism.Circulation 2003; 107:2545–2547.
78. Meyer T, Binder L, Hruska N, Luthe H,Buchwald AB. Cardiac troponin I el-evation in acute pulmonary embolismis associated with right ventriculardysfunction. J Am Coll Cardiol 2000;36:1632–1636.
79. Giannitsis E, Muller-Bardorff M, Ku-rowski V, et al. Independent prognos-tic value of cardiac troponin T in patientswith confirmed pulmonary embolism.Circulation 2000; 102:211–217.
80. Kostrubiec M, Pruszczyk P, Bochowicz
A, et al. Biomarker-based risk assess-ment model in acute pulmonary embo-lism. Eur Heart J 2005; 26:2166–2172.
81. Goldhaber SZ, Simons GR, Elliott CG,et al. Quantitative plasma D-dimerlevels among patients undergoing pul-monary angiography for suspectedpulmonary embolism. JAMA 1993; 270:2819–2822.
82. Gibson NS, Sohne M, Buller HR.Prognostic value of echocardiographyand spiral computed tomography inpatients with pulmonary embolism.Curr Opin Pulm Med 2005; 11:380–384.
83. ten Wolde M, Sohne M, Quak E, MacGillavry MR, Buller HR. Prognosticvalue of echocardiographically as-sessed right ventricular dysfunctionin patients with pulmonary embo-lism. Arch Intern Med 2004; 164:
1685–1689.



















