
Endovascular treatment of cerebrovascular diseases and intracranial neoplasms
10
For personal use. Only reproduce with permission from The Lancet publishing Group. REVIEW 804 THE LANCET • Vol 363 • March 6, 2004 • www.thelancet.com Introduction Cerebrovascular diseases are a major global health problem, result in high morbidity and mortality, and are the leading cause of disability. 1 Over the past few years, developments in endovascular treatments for cerebrovascular diseases have expanded the horizon of treatment by use of minimally invasive techniques. In endovascular treatment, drugs and devices are introduced through catheters or microcatheters placed into blood vessels through the skin. The initial work of Haschek, Lindenthal, and Moniz 2 led to development of cerebral angiography as a diagnostic method. In the early 1960s, Luessenhop and Velasquez 3 showed that intracranial vessels could be catheterised with flow- directed balloon tipped catheters, and in 1974, Serbinenko 4 reported use of balloon tipped micro- catheters and detachable balloons for treatment of intracranial aneurysms—starting the use of endovascular procedures as a method of treatment. The basic principle of all endovascular procedures involves percutaneous entry into the femoral, radial, or brachial artery 5,6 by use of a modification of Seldinger’s technique. 7 Guide catheters or sheaths are introduced through the aorta into the supra-aortic vessel of interest. Microcatheters, balloon catheters, and stent delivery devices are introduced through the guide catheter and guided to the target lesion with flexible microwires. Advanced designs of microcatheters including flow directed and magnetically guided microcatheters 8 have allowed highly selective delivery of coils, embolic materials, and drugs into regions of interest. Acute ischaemic stroke In 1958, Sussmann and Fitch 9 reported successful recanalisation of an acutely occluded internal carotid artery after intra-arterial injection of plasmin. Subsequent attempts at intra-arterial administration of thrombolytics were unsuccessful because the time window for Lancet 2004; 363: 804–13 Cerebrovascular Diseases Program, Department of Neurology and Neurosciences, University of Medicine and Dentistry of New Jersey, Newark, NJ, USA (Prof A I Qureshi MD) Correspondence to: Prof Adnan I Qureshi, Neurological Institute of New Jersey, 90 Bergen Street, DOC-8100, University of Medicine and Dentistry of New Jersey, Newark, NJ 07103-2425, USA (e-mail: [email protected]) intervention was not clearly understood and doctors had little experience in guiding catheters into the intracranial vessels. With better understanding of the time window, randomised trials 10,11 showed the benefit of using intravenous alteplase for patients with ischaemic stroke presenting within 3 h of symptom onset. However, 57–58% of the patients given intravenous alteplase died or became dependent as a result of the stroke, highlighting the need for new strategies. 10–12 The intra-arterial approach has been promoted because a high concentration of thrombolytic agents can be delivered into the thrombus, complemented by mechanical disruption to facilitate thrombolysis. 13–15 Despite the observation in uncontrolled studies 13–15 that recanalisation rates were higher with intra- arterial thrombolysis than with intravenous thrombolysis, clinical benefit might be compromised with the delay before starting treatment with the intra-arterial approach. Use of the intra-arterial approach for patients with ischaemic stroke who are expected to have a limited response to intravenous treatment has gained more popularity than for the intra-arterial approach being used as a first-line approach. Criteria that have been proposed or used for selection of patients include severe neurological deficits (National Institute of Health Stroke Scale [NIHSS] score 10; 15,16 table 1), presentation between 3 h and 6 h after symptom onset, 17 recent history of major surgical procedures (within 14 days), 18 and occlusion of major cervical or intracranial vessels. 16,19,20 The procedure is done as follows: an initial angiogram is done to determine the site of occlusion and to identify Endovascular treatment of cerebrovascular diseases and intracranial neoplasms Adnan I Qureshi Cerebrovascular diseases are an important cause of morbidity and mortality worldwide. Endovascular treatment has emerged as a minimally invasive approach to treat cerebrovascular diseases and possibly intracranial neoplasms. Practice patterns for selection of patients for endovascular treatment are continuously being modified on the basis of new information derived from clinical studies. In this review, I discuss the various endovascular treatments for diseases such as ischaemic stroke, carotid and intracranial stenosis, intracranial aneurysms, arteriovenous malformations, malignant gliomas, and meningiomas. Search strategy and selection criteria I based my review on personal knowledge of the subject supplemented by data derived from multi-centre randomised trials, non-randomised controlled studies with independent outcome ascertainment, and selected observational studies. The information was identified with multiple searches on MEDLINE from 1985 to the present by cross referencing key words of cerebrovascular disease, stroke, intracranial neoplasms, or clinical trials, with intra-arterial thrombolysis, angioplasty, stent, embolisation, detachable coils, intra-arterial chemotherapy and intra-arterial infusion. I also reviewed abstracts from pertinent scientific meetings. Information about technological developments was also acquired through industrial resources available for clinical investigators (http:// image.thelancet.com/extras/03art6147webappendix.pdf). Review
-
Upload
independent -
Category
Documents
-
view
0 -
download
0
Transcript of Endovascular treatment of cerebrovascular diseases and intracranial neoplasms

For personal use. Only reproduce with permission from The Lancet publishing Group.
REVIEW
804 THE LANCET • Vol 363 • March 6, 2004 • www.thelancet.com
IntroductionCerebrovascular diseases are a major global healthproblem, result in high morbidity and mortality, and are the leading cause of disability.1 Over the past fewyears, developments in endovascular treatments forcerebrovascular diseases have expanded the horizon oftreatment by use of minimally invasive techniques. Inendovascular treatment, drugs and devices areintroduced through catheters or microcatheters placedinto blood vessels through the skin. The initial work ofHaschek, Lindenthal, and Moniz2 led to development ofcerebral angiography as a diagnostic method. In the early1960s, Luessenhop and Velasquez3 showed thatintracranial vessels could be catheterised with flow-directed balloon tipped catheters, and in 1974,Serbinenko4 reported use of balloon tipped micro-catheters and detachable balloons for treatment ofintracranial aneurysms—starting the use of endovascularprocedures as a method of treatment.
The basic principle of all endovascular proceduresinvolves percutaneous entry into the femoral, radial, orbrachial artery5,6 by use of a modification of Seldinger’stechnique.7 Guide catheters or sheaths are introducedthrough the aorta into the supra-aortic vessel of interest.Microcatheters, balloon catheters, and stent deliverydevices are introduced through the guide catheter andguided to the target lesion with flexible microwires.Advanced designs of microcatheters including flowdirected and magnetically guided microcatheters8 haveallowed highly selective delivery of coils, embolicmaterials, and drugs into regions of interest.
Acute ischaemic strokeIn 1958, Sussmann and Fitch9 reported successfulrecanalisation of an acutely occluded internal carotidartery after intra-arterial injection of plasmin. Subsequentattempts at intra-arterial administration of thrombolyticswere unsuccessful because the time window for
Lancet 2004; 363: 804–13
Cerebrovascular Diseases Program, Department of Neurology andNeurosciences, University of Medicine and Dentistry of New Jersey,Newark, NJ, USA (Prof A I Qureshi MD)
Correspondence to: Prof Adnan I Qureshi, Neurological Institute ofNew Jersey, 90 Bergen Street, DOC-8100, University of Medicineand Dentistry of New Jersey, Newark, NJ 07103-2425, USA(e-mail: [email protected])
intervention was not clearly understood and doctors hadlittle experience in guiding catheters into the intracranialvessels. With better understanding of the time window,randomised trials10,11 showed the benefit of usingintravenous alteplase for patients with ischaemic strokepresenting within 3 h of symptom onset. However,57–58% of the patients given intravenous alteplase died orbecame dependent as a result of the stroke, highlightingthe need for new strategies.10–12 The intra-arterial approachhas been promoted because a high concentration ofthrombolytic agents can be delivered into the thrombus,complemented by mechanical disruption to facilitatethrombolysis.13–15 Despite the observation in uncontrolledstudies13–15 that recanalisation rates were higher with intra-arterial thrombolysis than with intravenous thrombolysis,clinical benefit might be compromised with the delaybefore starting treatment with the intra-arterial approach.Use of the intra-arterial approach for patients withischaemic stroke who are expected to have a limitedresponse to intravenous treatment has gained morepopularity than for the intra-arterial approach being usedas a first-line approach. Criteria that have been proposedor used for selection of patients include severeneurological deficits (National Institute of Health StrokeScale [NIHSS] score �10;15,16 table 1), presentationbetween 3 h and 6 h after symptom onset,17 recent historyof major surgical procedures (within 14 days),18 andocclusion of major cervical or intracranial vessels.16,19,20
The procedure is done as follows: an initial angiogramis done to determine the site of occlusion and to identify
Endovascular treatment of cerebrovascular diseases andintracranial neoplasms
Adnan I Qureshi
Cerebrovascular diseases are an important cause of morbidity and mortality worldwide. Endovascular treatment hasemerged as a minimally invasive approach to treat cerebrovascular diseases and possibly intracranial neoplasms.Practice patterns for selection of patients for endovascular treatment are continuously being modified on the basis ofnew information derived from clinical studies. In this review, I discuss the various endovascular treatments fordiseases such as ischaemic stroke, carotid and intracranial stenosis, intracranial aneurysms, arteriovenousmalformations, malignant gliomas, and meningiomas.
Search strategy and selection criteria
I based my review on personal knowledge of the subjectsupplemented by data derived from multi-centre randomisedtrials, non-randomised controlled studies with independentoutcome ascertainment, and selected observational studies.The information was identified with multiple searches onMEDLINE from 1985 to the present by cross referencing keywords of cerebrovascular disease, stroke, intracranialneoplasms, or clinical trials, with intra-arterial thrombolysis,angioplasty, stent, embolisation, detachable coils, intra-arterialchemotherapy and intra-arterial infusion. I also reviewedabstracts from pertinent scientific meetings. Information abouttechnological developments was also acquired throughindustrial resources available for clinical investigators (http://image.thelancet.com/extras/03art6147webappendix.pdf).
Review
For personal use. Only reproduce with permission from The Lancet publishing Group.
randomly allocated to receive either saruplase (n=121) orplacebo (n=59) through a microcatheter placed in thethrombus over a 2 h period. The recanalisation rate wassignificantly higher in the saruplase group (66%) than inthe control group (18%, p<0·001). Despite a higher rateof symptomatic intracranial haemorrhages, the rate offavourable outcome (modified Rankin scale of 0–2 at90 days) was significantly higher in patients givensaruplase (40%) than in those given placebo (25%p=0·04).
Another approach under investigation is the starting ofintravenous thrombolysis in the period between initialassessment and intra-arterial treatment.27,28 In theInterventional Management of Stroke (IMS) study,28
80 patients with an initial NIHSS of 10 of greater weregiven intravenous thrombolysis followed by intra-arterialthrombolysis. Treatment was started within 3 h, with0·6 mg/kg intravenous alteplase followed by cerebralangiography in 78 patients. Intra-arterial alteplase (up to22 mg) was started in 64 of 78 patients in whom athrombus was seen. Part or complete recanalisation wasachieved in 41 of the 64 patients after intra-arterialtreatment. The rate of symptomatic intracerebralhaemorrhage within 36 h of treatment was 6·2%; overallmortality was 16%, and 30% of the patients had little orno disability at 90 days. An indirect comparison with thepatients given intravenous alteplase (0·9 mg/kg) in theprevious study10 did not show any significant differences inmortality or symptomatic intracerebral haemorrhagerates, although a higher rate of asymptomaticintracerebral haemorrhages was noted. The comparisonbetween different studies is limited by differences in
REVIEW
THE LANCET • Vol 363 • March 6, 2004 • www.thelancet.com 805
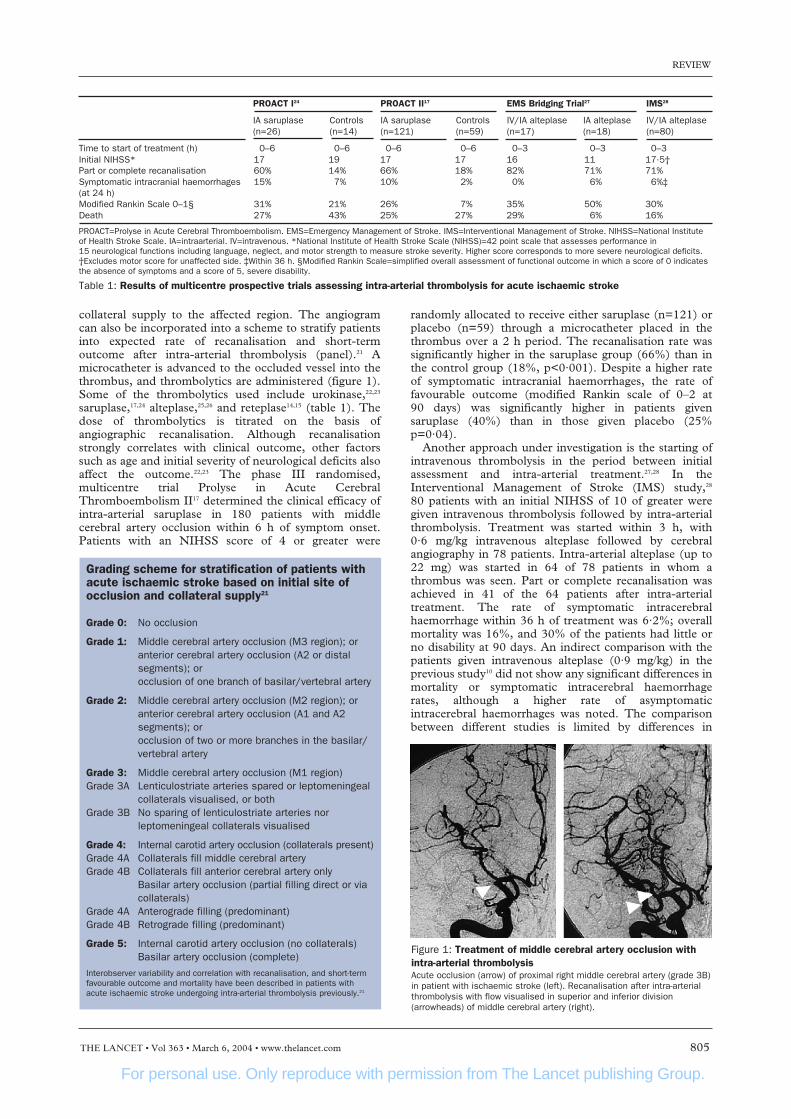
collateral supply to the affected region. The angiogramcan also be incorporated into a scheme to stratify patientsinto expected rate of recanalisation and short-termoutcome after intra-arterial thrombolysis (panel).21 Amicrocatheter is advanced to the occluded vessel into thethrombus, and thrombolytics are administered (figure 1).Some of the thrombolytics used include urokinase,22,23
saruplase,17,24 alteplase,25,26 and reteplase14,15 (table 1). Thedose of thrombolytics is titrated on the basis ofangiographic recanalisation. Although recanalisationstrongly correlates with clinical outcome, other factorssuch as age and initial severity of neurological deficits alsoaffect the outcome.22,23 The phase III randomised,multicentre trial Prolyse in Acute CerebralThromboembolism II17 determined the clinical efficacy ofintra-arterial saruplase in 180 patients with middlecerebral artery occlusion within 6 h of symptom onset.Patients with an NIHSS score of 4 or greater were
PROACT I24 PROACT II17 EMS Bridging Trial27 IMS28
IA saruplase Controls IA saruplase Controls IV/IA alteplase IA alteplase IV/IA alteplase(n=26) (n=14) (n=121) (n=59) (n=17) (n=18) (n=80)
Time to start of treatment (h) 0–6 0–6 0–6 0–6 0–3 0–3 0–3Initial NIHSS* 17 19 17 17 16 11 17·5†Part or complete recanalisation 60% 14% 66% 18% 82% 71% 71%Symptomatic intracranial haemorrhages 15% 7% 10% 2% 0% 6% 6%‡(at 24 h)Modified Rankin Scale 0–1§ 31% 21% 26% 7% 35% 50% 30%Death 27% 43% 25% 27% 29% 6% 16%
PROACT=Prolyse in Acute Cerebral Thromboembolism. EMS=Emergency Management of Stroke. IMS=Interventional Management of Stroke. NIHSS=National Instituteof Health Stroke Scale. IA=intraarterial. IV=intravenous. *National Institute of Health Stroke Scale (NIHSS)=42 point scale that assesses performance in 15 neurological functions including language, neglect, and motor strength to measure stroke severity. Higher score corresponds to more severe neurological deficits.†Excludes motor score for unaffected side. ‡Within 36 h. §Modified Rankin Scale=simplified overall assessment of functional outcome in which a score of 0 indicatesthe absence of symptoms and a score of 5, severe disability.
Table 1: Results of multicentre prospective trials assessing intra-arterial thrombolysis for acute ischaemic stroke
Figure 1: Treatment of middle cerebral artery occlusion withintra-arterial thrombolysisAcute occlusion (arrow) of proximal right middle cerebral artery (grade 3B)in patient with ischaemic stroke (left). Recanalisation after intra-arterialthrombolysis with flow visualised in superior and inferior division(arrowheads) of middle cerebral artery (right).
Grading scheme for stratification of patients withacute ischaemic stroke based on initial site ofocclusion and collateral supply21
Grade 0: No occlusion
Grade 1: Middle cerebral artery occlusion (M3 region); oranterior cerebral artery occlusion (A2 or distal segments); orocclusion of one branch of basilar/vertebral artery
Grade 2: Middle cerebral artery occlusion (M2 region); oranterior cerebral artery occlusion (A1 and A2 segments); orocclusion of two or more branches in the basilar/ vertebral artery
Grade 3: Middle cerebral artery occlusion (M1 region)Grade 3A Lenticulostriate arteries spared or leptomeningeal
collaterals visualised, or bothGrade 3B No sparing of lenticulostriate arteries nor
leptomeningeal collaterals visualised
Grade 4: Internal carotid artery occlusion (collaterals present)Grade 4A Collaterals fill middle cerebral arteryGrade 4B Collaterals fill anterior cerebral artery only
Basilar artery occlusion (partial filling direct or via collaterals)
Grade 4A Anterograde filling (predominant)Grade 4B Retrograde filling (predominant)
Grade 5: Internal carotid artery occlusion (no collaterals)Basilar artery occlusion (complete)
Interobserver variability and correlation with recanalisation, and short-termfavourable outcome and mortality have been described in patients withacute ischaemic stroke undergoing intra-arterial thrombolysis previously.21
For personal use. Only reproduce with permission from The Lancet publishing Group.
REVIEW
806 THE LANCET • Vol 363 • March 6, 2004 • www.thelancet.com
methods of administration, thrombolytic agents, anddoses.
Mechanical devices can facilitate binding ofthrombolytics to clot bound fibrin and promote the lyticprocess,29 and can be divided into devices that eitherdisrupt or retrieve the thrombus. Thrombus disruptiondevices include angioplasty balloon catheters; snaredevices; and specialised intravascular catheters that emitultrasound, pressurised saline solution with resorption, orphotoacoustic energy. Adequate safety and feasibility has
been shown in the phase I studies involving 14 patientstreated with ultrasound emitting catheter30 and 26 patientstreated with a photoacoustic energy emitting system31 forocclusions in the anterior and posterior circulation.A phase I study32 reported adequate safety and feasibilityof a helical retrieval wire that engages and subsequentlyremoves thrombi, in 30 patients treated within 8 h ofstroke onset.
Use of platelet glycoprotein IIb/IIIa inhibitors has beensuggested to prevent platelet activation and reocclusion,33
and is being investigated in several phase I studies asadjuvant treatment to intra-arterial thrombolysis.
Carotid stenosisRandomised trials have shown the benefit of carotidendarterectomy in reducing the risk of stroke in patientswith moderate to severe symptomatic (�50%)34–36 orasymptomatic (�60%)37 carotid artery stenosis. However,in general practice, perioperative complications aresometimes high enough that potential benefits areobscured when carotid endarterectomy is done onpatients with unfavourable clinical and anatomicalcharacteristics.38–42 Carotid angioplasty with stentplacement (CAS) was initially introduced as an alternativetreatment for revascularisation of carotid artery stenosis inhigh-risk surgical candidates43 on the basis of successfulclinical trials of endovascular revascularisation forcoronary and peripheral circulation.44,45 CAS can be donein high-risk surgical groups, including patients with severecoronary artery disease,46,47 anticipated coronary arterybypass surgery,48,49 congestive heart failure,50 high lyingcervical lesions,51 contralateral carotid occlusion,52
restenosis after the procedure,53 radiation inducedstenosis,54 or dissection-related stenosis,55 with high
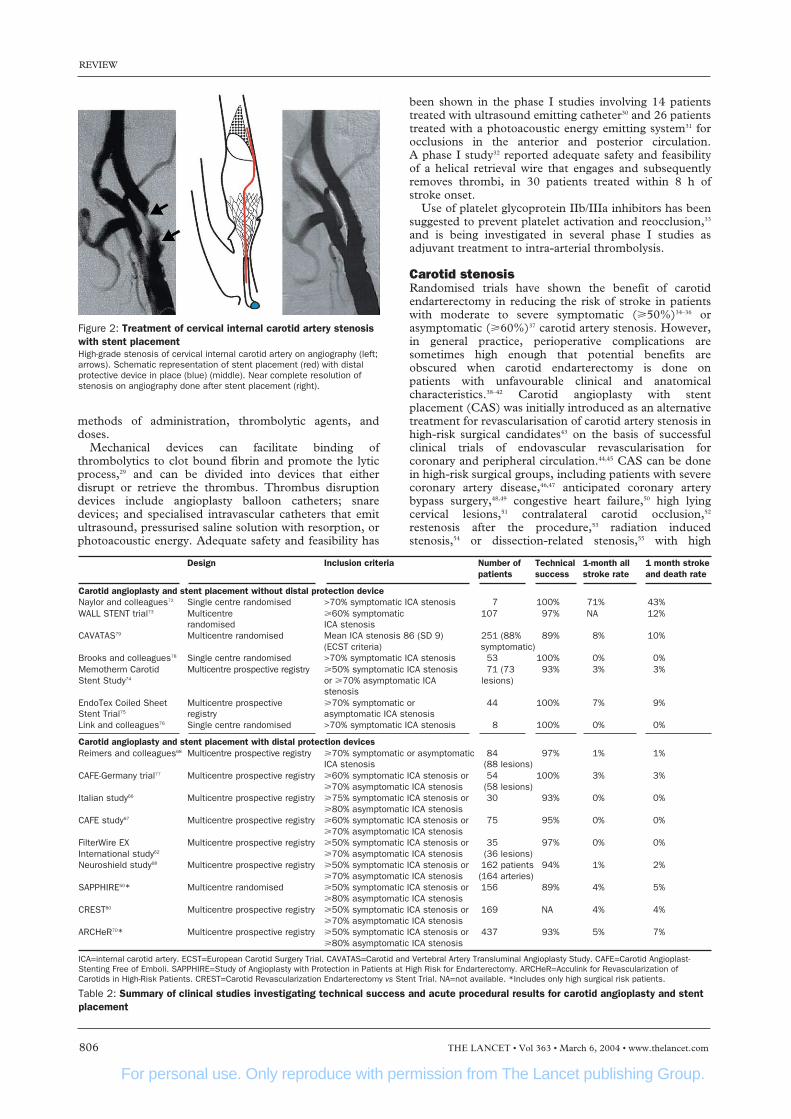
Figure 2: Treatment of cervical internal carotid artery stenosiswith stent placementHigh-grade stenosis of cervical internal carotid artery on angiography (left;arrows). Schematic representation of stent placement (red) with distalprotective device in place (blue) (middle). Near complete resolution ofstenosis on angiography done after stent placement (right).
Design Inclusion criteria Number of Technical 1-month all 1 month stroke patients success stroke rate and death rate
Carotid angioplasty and stent placement without distal protection deviceNaylor and colleagues72 Single centre randomised >70% symptomatic ICA stenosis 7 100% 71% 43%WALL STENT trial73 Multicentre �60% symptomatic 107 97% NA 12%
randomised ICA stenosis CAVATAS79 Multicentre randomised Mean ICA stenosis 86 (SD 9) 251 (88% 89% 8% 10%
(ECST criteria) symptomatic)Brooks and colleagues78 Single centre randomised >70% symptomatic ICA stenosis 53 100% 0% 0%Memotherm Carotid Multicentre prospective registry �50% symptomatic ICA stenosis 71 (73 93% 3% 3%Stent Study74 or �70% asymptomatic ICA lesions)
stenosisEndoTex Coiled Sheet Multicentre prospective �70% symptomatic or 44 100% 7% 9%Stent Trial75 registry asymptomatic ICA stenosisLink and colleagues76 Single centre randomised >70% symptomatic ICA stenosis 8 100% 0% 0%
Carotid angioplasty and stent placement with distal protection devicesReimers and colleagues68 Multicentre prospective registry �70% symptomatic or asymptomatic 84 97% 1% 1%
ICA stenosis (88 lesions)CAFE-Germany trial77 Multicentre prospective registry �60% symptomatic ICA stenosis or 54 100% 3% 3%
�70% asymptomatic ICA stenosis (58 lesions)Italian study66 Multicentre prospective registry �75% symptomatic ICA stenosis or 30 93% 0% 0%
�80% asymptomatic ICA stenosisCAFE study67 Multicentre prospective registry �60% symptomatic ICA stenosis or 75 95% 0% 0%
�70% asymptomatic ICA stenosisFilterWire EX Multicentre prospective registry �50% symptomatic ICA stenosis or 35 97% 0% 0%International study62 �70% asymptomatic ICA stenosis (36 lesions)Neuroshield study68 Multicentre prospective registry �50% symptomatic ICA stenosis or 162 patients 94% 1% 2%
�70% asymptomatic ICA stenosis (164 arteries)SAPPHIRE50* Multicentre randomised �50% symptomatic ICA stenosis or 156 89% 4% 5%
�80% asymptomatic ICA stenosisCREST80 Multicentre prospective registry �50% symptomatic ICA stenosis or 169 NA 4% 4%
�70% asymptomatic ICA stenosisARCHeR70* Multicentre prospective registry �50% symptomatic ICA stenosis or 437 93% 5% 7%
�80% asymptomatic ICA stenosis
ICA=internal carotid artery. ECST=European Carotid Surgery Trial. CAVATAS=Carotid and Vertebral Artery Transluminal Angioplasty Study. CAFE=Carotid Angioplast-Stenting Free of Emboli. SAPPHIRE=Study of Angioplasty with Protection in Patients at High Risk for Endarterectomy. ARCHeR=Acculink for Revascularization ofCarotids in High-Risk Patients. CREST=Carotid Revascularization Endarterectomy vs Stent Trial. NA=not available. *Includes only high surgical risk patients.
Table 2: Summary of clinical studies investigating technical success and acute procedural results for carotid angioplasty and stentplacement
For personal use. Only reproduce with permission from The Lancet publishing Group.
specified size of the pores of the filter. Another antiembolisystem consists of a guiding catheter with an occlusionballoon that induces reversal of intracranial flow toprevent intracranial flow of emboli. The results of phase Iand II studies50,66–70 have shown high technical success andlow rates of stroke or death associated with CAS whendone with distal protection devices (table 1). A systematicreview71 reported that occurrence of minor and majorstroke is lower in reports from CAS done with distalprotection compared with this procedure done withoutprotection.
Over the past few years, several non-randomised studiesand randomised comparisons with carotid endarterectomyhave investigated the safety and effectiveness of CAS(table 2) Two studies50,70 have strongly advocated thesafety and possible benefit of CAS with distal protectionin high-risk surgical patients. In the Study of Angioplastywith Protection in Patients at High Risk forEndarterectomy (SAPPHIRE) trial50 307 high-riskpatients were randomly allocated to either CAS or carotidendarterectomy, and 402 patients deemed not suitable forcarotid endarterectomy were enrolled into a stent registry.At 30-day follow-up, the combined rate of death, stroke,or myocardial infarction was significantly lower for the156 patients who had CAS and distal protection (6%)compared with the 151 patients who received carotidendarterectomy (13%). The combined rate of death,stroke, or myocardial infarction was 8% in the patientsenrolled in the stent registry. At 1 year, ipsilateral strokerate was 3·8% and 5·3% for patients who received CASand endarterectomy, respectively. Overall, 6·9% of thepatients who received CAS and 12·6% of those who hadan endarterectomy had died by 1 year. The non-randomised Acculink for Revascularisation of Carotids inHigh-Risk Patients (ARCHeR) study70 reported a rate of8% for the combined endpoint of death, stroke, ormyocardial infarction at 30 days in 437 high-risk patientsrecruited in the study. Subset analysis showed thatpatients with restenosis can be treated, with a less than1% rate of stroke or death. Secondary endpoints are beingassessed 6-monthly for up to 30 months.
Improvement in technology and operator experience,and results of clinical trials have led to broader acceptanceof the use of CAS in patients who are not at a high risk. Inthe multicentre randomised Carotid and Vertebral ArteryTransluminal Angioplasty Study (CAVATAS),79 the rateof perioperative major stroke or death with carotidstenosis in 251 patients randomly assigned to endovas-cular treatment was much the same as that for253 patients allocated to carotid endarterectomy (6% vs6%, respectively). Stents were used in 26% of thepatients treated with an endovascular procedure. Ahigher rate of cranial neuropathy and major neck andgroin haematomas was seen in patients assigned tocarotid endarterectomy than in those receivingendovascular treatment. No substantial difference in therate of ipsilateral stroke between the groups was noted,with survival analysis up to 3 years after randomisation.However, the rate of severe stenosis or occlusion in thetreated carotid artery at 1 year was higher afterendovascular treatment (18%) than after carotidendarterectomy (5%, p<0·001). The US NationalInstitute for Neurological Disorders and Stroke fundedCREST study (Carotid Revascularisation Endarterect-omy vs Stent Trial)80 is comparing the efficacy of CASwith carotid endarterectomy in 2500 patients withsymptomatic stenosis. A lead-in phase was set up fordoctors to do 20 CAS procedures before doing proce-dures on randomised patients. The early results from the
REVIEW
THE LANCET • Vol 363 • March 6, 2004 • www.thelancet.com 807
technical success rates and acceptable periproceduralcomplication rates. However, some patients who are athigh risk for carotid endarterectomy, such as those whoare older (�80 years),56 with fluctuating neurologicaldeficits,57 and intraluminal thrombus also seem to be athigh risk for CAS.
All patients receive aspirin and ticlopidine orclopidogrel before and up to 1 month after the procedureon the basis of data derived from coronary intervention.58
Balloon angioplasty and stent delivery are undertakenthrough guide sheaths placed in the common carotidartery proximal to the stenosis (figure 2). Two classes ofstents are currently used59—ie, balloon-expandable andself-expanding, which are made of either stainless steel orthermal expansion alloy (nitinol). Balloon angioplasty canbe done before stent placement to facilitate stent deliveryor after placement to treat residual stenosis. Theeffectiveness of adjuvant use of platelet glycoproteinIIb/IIIa inhibitors such as abciximab and eptifibatide inthe immediate perioperative period is controversial.60,61 Asmall randomised comparison62 between abciximab bolusbefore the CAS and standard antithrombotic treatmentdid not show any reduction in perioperative ischaemicevents (19% vs 8%, respectively).
Release of microemboli composed of thrombotic andplaque substances63 into the cerebral circulation isfrequent during CAS, as detected by transcranial dopplerultrasound.64 MRI suggests that 15% of patients developnew lesions in the brain after this procedure, although halfof them are asymptomatic.64 An indirect comparison65
suggests that the rate of new brain lesions is higher thanthe 5% rate reported for carotid endarterectomy. Distalprotective devices consisting of occlusive balloons, filterdevices, or flow-reversal devices have been introduced toreduce the incidence of embolic particles to the brain.50,66–70
A low-pressure occlusion balloon is placed distal to thesite of CAS to trap blood flow and embolic materialbefore entry in the intracranial circulation. Filtrationdevices placed intravascularly distal to the site of theintervention filter blood to retain particles exceeding the
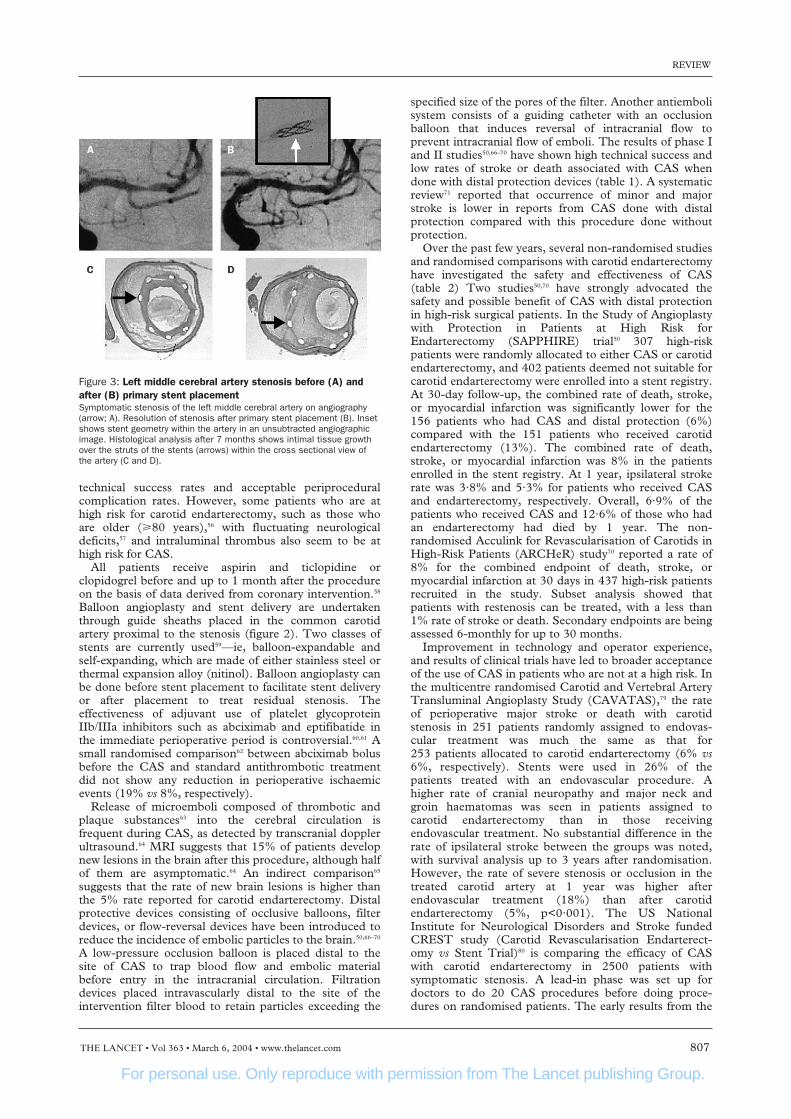
Figure 3: Left middle cerebral artery stenosis before (A) andafter (B) primary stent placementSymptomatic stenosis of the left middle cerebral artery on angiography(arrow; A). Resolution of stenosis after primary stent placement (B). Insetshows stent geometry within the artery in an unsubtracted angiographicimage. Histological analysis after 7 months shows intimal tissue growthover the struts of the stents (arrows) within the cross sectional view ofthe artery (C and D).

For personal use. Only reproduce with permission from The Lancet publishing Group.
REVIEW
808 THE LANCET • Vol 363 • March 6, 2004 • www.thelancet.com
169 patients treated in the lead-in phase set up reported acombined rate of death, stroke, or myocardial infarctionwithin 30 days after the procedure of 4%, suggesting apotential equivalence to carotid endarterectomy forpatients who are not high risk.
Intracranial stenosisIntracranial stenosis is responsible for 8–10% of allischaemic strokes.81,82 The yearly rate of recurrent strokein patients with intracranial stenosis is about 8–12%83,84
and for those who do not respond to antithrombotictreatment, the rate of recurrent ischaemic events can beas high as 52%.85 Patients with symptomatic vertebrobas-ilar stenosis have a low stroke-free survival rate of 76% at12 months and 48% at 5 years.82 Percutaneous translumi-nal angioplasty with possible stent placement has beenrecommended for treatment of intracranial stenosis,especially for patients who did not respond to anti-thrombotic treatment or who have vertebrobasilarstenosis. Small patient series86–88 have shown thefeasibility of percutaneous transluminal angioplasty orstent placement for symptomatic intracranial stenosis,with major complication rates of lower than 5%(figure 3). Long-term follow-up suggests encouragingipsilateral stroke prevention rates as high as 96% for thefirst year87 and about 87% for 3 years after endovasculartreatment.86 It should be stressed that no directcomparisons are available between best medicaltreatment and endovascular treatment for intracranialstenosis. The prospective multicentre Stenting inSymptomatic Atherosclerotic Lesions of Vertebral andIntracranial Arteries (SSYLVIA) study89 assessed43 patients with intracranial stenosis and 18 withextracranial vertebral artery stenosis. Successful stentplacement was achieved in 95% of the patients with a 1-month postprocedural stroke rate of 7%. At 6 months,recurrent stenosis of greater than 50% was recorded in30% of the intracranial arteries. Of the 42 patients with12-month follow-up, four patients had a stroke after 30 days that was related to the target lesion. Furtherdevelopments in stent design are expected to improvelong-term benefits of the procedure.
Intracranial aneurysmsIntracranial aneurysms are an important health problemworldwide, affecting about 2% of the population.90 In1941, Werner and colleagues91 inserted silver wires into anintracranial aneurysm by use of a transorbital approach toprevent rupture by protecting the susceptible wall of theaneurysm from the stress of pulsatile blood. Subsequently,placement of iron particles, detachable balloons, andpushable platinum coils was attempted.2 In the late 1980s,soft platinum coil soldered to astainless steel delivery wire wasintroduced that could be deliveredthrough a microcatheter into theaneurysm sac.92 Current applied to thedelivery wire resulted in a positivecharge on platinum coils that attractedred blood cells and platelets, inducinglocal thrombosis followed by detach-ment when the current dissolved thejunction between stainless steeldelivery wire and platinum coil. Theimmediate protection against ruptureoccurs by reduction of blood pulsa-tions within the fundus and might notinvolve a prominent thromboticresponse. Eventually, an organised
thrombus forms within the aneurysm, covered by anendothelialised layer of connective tissue that covers theneck’s ostium.93,94
Endovascular treatment is done under generalanaesthesia or awake state in selected patients.95
Endovascular coils are placed into the aneurysm sac untilno further filling is seen. Modifications in coil designshave improved the ability to obliterate the aneurysm sac.Several types of coil that use other detachmentmechanisms or have bioactive coating of coil surface arenow available. Strategies such as temporary inflation ofballoon (balloon remodelling technique),96 intravascularstent placement,97 and neck-bridge devices98 in front of theostium of the aneurysm have improved the results ofembolisation for broad neck aneurysms (figure 4). Aliquid embolic agent, an ethyl vinyl alcohol polymer, hasalso been used in conjunction with intravascular stents toobliterate complex aneurysms.99
In August, 2002, 100 000 patients with intracranialaneurysms were estimated to have been treated withdetachable coils at sites throughout the world.100 Initially,endovascular treatment was considered for patients whowere regarded as poor candidates for surgical clipping,which includes older patients (�65 years),101 those withpoor clinical grade,102 those whose aneurysms are locatedin the posterior circulation103 or cavernous segment ofinternal carotid artery,100 and those who present between3 and 10 days after symptom onset104 or have activecerebral vasospasm.105 In a meta-analysis106 of 37 studiesand 1256 patients, aneurysms were nearly obliterated in88% of patients and completely obliterated in 54% oftreated patients, with a permanent complication rate of4% and procedure-related mortality of 1·1%. Long-termfollow-up has reported a yearly haemorrhage rate of 1·4%over 141 patient-years.107 The magnitude of initialobliteration107 and the size of the intracranial aneurysm108
seem to affect the long-term risk of bleeding from treatedaneurysms. Occasional aneurysm regrowth andrecanalisation have been reported.109
With improvement in clinical experience and coildesigns, embolisation is being used for patients who couldbe treated by conventional surgical clipping.100 The firstrandomised phase II trial110,111 compared the outcomes ofsurgical clipping (n=57) and embolisation (n=52) inpatients with acute (within 72 h) aneurysmal sub-arachnoid haemorrhage. Significantly better angiographicresults were achieved after surgery in patients withanterior cerebral artery aneurysms and after endovasculartreatment in those with posterior circulation aneurysms.The technique-related mortality rate was 4% and 2% inthe surgical and endovascular groups, respectively. 1 yearafter the procedure, good or moderate recovery was seen
Figure 4: Treatment of distal vertebral artery aneurysm with placement of stent andcoilsRegrowth of distal vertebral artery aneurysm after initial coil placement (arrow; left). The anatomy wasunfavourable for primary coil placement because of a wide neck. Schematic representation (middle) ofstent placement in front of the ostium of the aneurysm to provide a base to retain the coils in theaneurysm. Near complete obliteration of the aneurysm after stent and coil placement (right).
For personal use. Only reproduce with permission from The Lancet publishing Group.
REVIEW
THE LANCET • Vol 363 • March 6, 2004 • www.thelancet.com 809
in 75% and 79% of surgically and endovascular treatedpatients, respectively. No late rebleedings have beenreported. The second randomised, multicentre phase IIIInternational Subarachnoid Aneurysm Trial (ISAT)112
compared the safety and efficacy of embolisation withneurosurgical clipping in 2143 patients with rupturedaneurysms suitable for either treatment. 1070 patientswere randomly assigned to surgery and 1073 toendovascular treatment. Recruitment was stopped prema-turely, after a planned interim analysis showed reduceddeath and disability in the embolisation group. A higherproportion of patients allocated to surgery (31% of 793)were dependent or dead at 1 year compared with thoseallocated to embolisation (24% of 801). However, asecond procedure was needed more frequently in patientsgiven endovascular treatment than those who underwentsurgery (121 patients vs 33 patients), with no significantdifference in time to second treatment. The risk ofrebleeding from the ruptured aneurysm after 1 year wastwo per 1276 and zero per 1081 patient-years for patientsallocated to endovascular and surgical treatment,respectively. The study will continue to ascertain therebleeding rate over 5 years to compare the durability ofthe two treatments.
A direct comparison between endovascular and surgicaltreatment for unruptured aneurysms is not available.
Hospital outcomes have improved for unrupturedintracranial aneurysms in the USA since detachable coilswere introduced.113 Johnston and colleagues114,115 did twoindirect comparisons of surgical clipping and embolisationfor unruptured intracranial aneurysms using a database of60 university hospitals (2357 patients) and a statewidedatabase (2069 patients), respectively. Lower in-hospitalmortality, stay, and costs were noted with endovasculartreatment compared with surgery in both analyses. Aretrospective comparison116 of outcomes between surgicaland endovascular treatment for unruptured aneurysmsthat are suitable for both methods showed a reduced rateof new disability, shorter stays and periods to completerecovery, and lower hospital costs with endovasculartreatment than with surgery.
Arteriovenous malformationsIn 1930, Brooks117 reported closure of carotid-cavernousfistula with surgical introduction of muscle embolus in thecarotid artery. Lussenhop and colleagues118 subsequentlyreported embolisation with silastic spheres and silksutures introduced into the internal carotid artery to treatcerebral arteriovenous malformation. Technical advancessuch as flow directed and other specialised microcathetersand new embolic agents have increased the therapeuticpotential of embolisation for cerebral arteriovenousmalformations. However, embolisation of cerebralarteriovenous malformations on its own is curative in lessthan a quarter of the lesions,119,120 and is one aspect of amultimodality approach to these lesions. Embolisation isindicated mainly before surgery or radiosurgicalintervention in large or giant arteriovenousmalformations120 Other indications include palliativeembolisation to halt progression of symptoms for largenon-surgical or non-radiosurgical arteriovenousmalformations in patients presenting with progressiveneurological deficit secondary to high flow or venoushypertension.120 It should be noted that the role ofembolisation in treatment of arteriovenous malformationsis based mainly on results from observational studies.
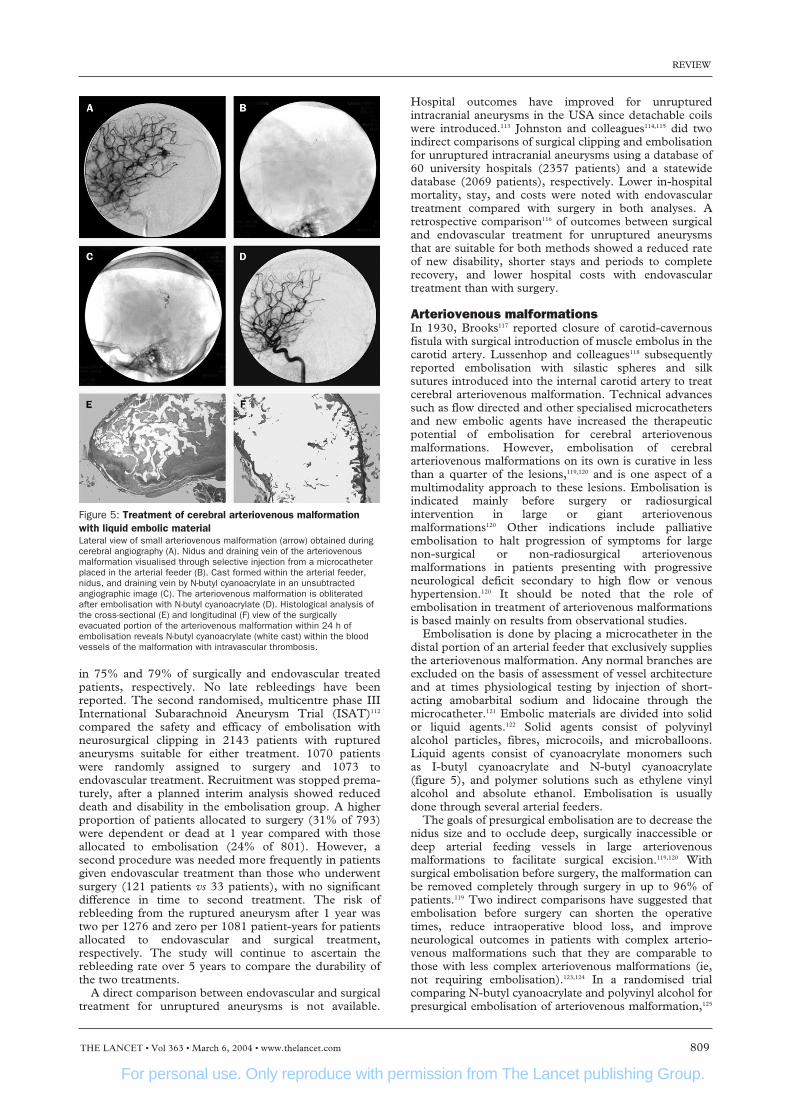
Embolisation is done by placing a microcatheter in thedistal portion of an arterial feeder that exclusively suppliesthe arteriovenous malformation. Any normal branches areexcluded on the basis of assessment of vessel architectureand at times physiological testing by injection of short-acting amobarbital sodium and lidocaine through themicrocatheter.121 Embolic materials are divided into solidor liquid agents.122 Solid agents consist of polyvinylalcohol particles, fibres, microcoils, and microballoons.Liquid agents consist of cyanoacrylate monomers such as I-butyl cyanoacrylate and N-butyl cyanoacrylate(figure 5), and polymer solutions such as ethylene vinylalcohol and absolute ethanol. Embolisation is usuallydone through several arterial feeders.
The goals of presurgical embolisation are to decrease thenidus size and to occlude deep, surgically inaccessible ordeep arterial feeding vessels in large arteriovenousmalformations to facilitate surgical excision.119,120 Withsurgical embolisation before surgery, the malformation canbe removed completely through surgery in up to 96% ofpatients.119 Two indirect comparisons have suggested thatembolisation before surgery can shorten the operativetimes, reduce intraoperative blood loss, and improveneurological outcomes in patients with complex arterio-venous malformations such that they are comparable tothose with less complex arteriovenous malformations (ie,not requiring embolisation).123,124 In a randomised trialcomparing N-butyl cyanoacrylate and polyvinyl alcohol forpresurgical embolisation of arteriovenous malformation,125
Figure 5: Treatment of cerebral arteriovenous malformationwith liquid embolic materialLateral view of small arteriovenous malformation (arrow) obtained duringcerebral angiography (A). Nidus and draining vein of the arteriovenousmalformation visualised through selective injection from a microcatheterplaced in the arterial feeder (B). Cast formed within the arterial feeder,nidus, and draining vein by N-butyl cyanoacrylate in an unsubtractedangiographic image (C). The arteriovenous malformation is obliteratedafter embolisation with N-butyl cyanoacrylate (D). Histological analysis ofthe cross-sectional (E) and longitudinal (F) view of the surgicallyevacuated portion of the arteriovenous malformation within 24 h ofembolisation reveals N-butyl cyanoacrylate (white cast) within the bloodvessels of the malformation with intravascular thrombosis.

For personal use. Only reproduce with permission from The Lancet publishing Group.
REVIEW
810 THE LANCET • Vol 363 • March 6, 2004 • www.thelancet.com
embolisation was not possible for technical reasons inthree of the 52 patients randomised to N-butyl cyano-acrylate, and there were two cross-overs from the groupallocated to polyvinyl alcohol. The final lesion reductionangiographically per patient after embolisation wasestimated as 79% for patients administered N-butyl cyano-acrylate and 87% for those given polyvinyl alcohol. Therates of good neurological recovery after embolisation were96% and 93%, respectively. No significant differenceswere recorded in intraoperated time and blood loss, andpostsurgical neurological recovery.
Embolisation is used to reduce the nidus of arteriovenousmalformations to less than 3 cm and obliterate intranidal orvenous aneurysms before radiosurgical intervention.126 In astudy126 of 125 patients who were poor surgical candidatesor who had refused surgery, embolisation produced totalocclusion in 11% of arteriovenous malformations andreduced the volume in 76% of arteriovenous malforma-tions, to make radiosurgery possible. Radiosurgeryproduced total occlusion in 65% of the partly embolisedarteriovenous malformations. Angiographic follow-up ofarteriovenous malformations embolised with cyanoacrylatedemonstrated a 12% recanalisation rate within 1 year.
Dural arteriovenous fistulas are derived from meningealarteries and drain into dural sinuses or meningeal veinsand can have retrograde drainage into subarachnoidveins.127 Treatment includes transarterial, transvenous, orcombined endovascular obliteration of the fistula byselective catheterisation and potentially the drainingsegment of the dural venous sinus. In patients where thefistulas are related to venous hypertension secondary tototal or part sinus occlusion, recanalisation withangioplasty and stent is sometimes effective.128
Intracranial tumours Intra-arterial delivery of chemotherapeutic agents into thevascular bed of intracranial tumours has been suggested toachieve a high concentration in selected regions of thebrain.129 A phase III trial130 showed no difference insurvival between the 153 patients with newly resectedmalignant glioma who were randomly allocated tointracarotid injection of carmustine and the 126 whoreceived this compound intravenously. Serious toxiceffects in the intra-arterial group, consisting of irreversibleencephalopathy, visual loss, and white matter necrosis,restricted the benefit. Improved tolerance of intra-arterialchemotherapy, particularly carboplatin, has been reportedwith a combination of selective intra-arterial delivery intointracranial vessels, pulsatile infusion, and dose based onestimation of local cerebral blood flow.131 A new approachhas used intra-arterial lobradimil, a bradykinin analogue,to increase the permeability of the brain tumour capillariesconcomitantly with carboplatin.132 A dose escalationstudy133 and a phase II study134 of intra-arterial lobradimiland carboplatin in patients with malignant recurrentgliomas have reported acceptable safety and tolerance. Inthe phase II study, the disease stabilised in 13 patients andprogressed in 28 patients after treatment.
The extensive vascularity of neoplasms is vulnerable tosuperselective intra-arterial injection of embolic particles.This notion has gained popularity for meningiomas as apreoperative adjuvant therapy.135 The highly vascular bedof meningiomas is easily identified on angiography, and isamenable to selective microcatheterisation if fed mainlyfrom the branches of external carotid artery. The goal is toinject embolic material such as polyvinyl alcohol particles,gelfoam powder, fibrin glue, microfibrillar collagen, orgelatin microspheres until the vascular blush is completelyobliterated. Indirect comparisons between results of
surgical removal of meningiomas with and withoutpreoperative embolisation suggest that embolisationreduces blood loss and the number of transfusions neededduring surgery.136 This benefit is more likely to be seen inlarge tumours than small,135 and when a high degree ofobliteration of tumour vascularity could be achieved.137
Preoperative embolisation has been recommended forgiant meningiomas, meningiomas with malignant orangioblastic characteristics, and those involving criticalvascular structures. The ideal time interval betweenembolisation and subsequent surgical evacuation iscontroversial, but an observational study138 suggested thatgreatest tumour softening is seen 7–9 days afterembolisation facilitating surgical removal.
Future applicationsThe safety and efficacy of endovascular procedures forcerebrovascular diseases is expected to improve with newtechnology. New applications such as intra-arterialdelivery of stem cells derived from bone marrow todamaged regions of the brain have shown promise inexperimental models.139 These cells can be deposited inthe regions of injured brain, survive, and express proteinssimilar to neurons. The intra-arterial route has also beenproposed as a method for delivering plasmid DNAincorporated into liposomes into regions of ischaemicinjury in the brain.140 Cationic liposomes protect the DNAfrom the extracellular environment and provide amechanism for DNA transfer to target cells by lipidfusion. Endovascular procedures are rapidly expandingthe range of treatment options for cerebrovasculardiseases and neoplasms. However, rigorous assessmentand understanding of these procedures is necessary toensure safe, effective, and appropriate use.
Conflict of interest statementA Qureshi has received grant support from Boston Scientific, CordisTherapeutics, Cor Therapeutics, Centocor therapeutics, C R Bard, andSan Francisco Science/PICS. He has also received consultant fees fromEndoTex Interventional Systems and Boston Scientific and anhonorarium from Boehringer Ingelheim.
References1 Kalache A, Aboderin I. Stroke: the global burden. Health Policy Plan
1995; 10: 1–21.2 Hopkins LN, Lanzino G, Guterman LR. Treating complex nervous
system vascular disorders through a “needle stick”: origins, evolution,and future of neuroendovascular therapy. Neurosurgery 2001; 48:463–75.
3 Luessenhop AJ, Velasquez AC. Observations on the tolerance of the intracranial arteries to catheterization. J Neurosurg 1964; 21:85–91.
4 Serbinenko FA. Balloon catheterization and occlusion of majorcerebral vessels. J Neurosurg 1974; 41: 125–45.
5 Kiemeneij F, Laarman GJ, Odekerken D, Slagboom T, van der Wieken R. A randomized comparison of percutaneoustransluminal coronary angioplasty by the radial, brachial and femoral approaches: the access study. J Am Coll Cardiol 1997; 29:1269–75.
6 Fessler RD, Wakhloo AK, Lanzino G, Guterman LR, Hopkins LN.Transradial approach for vertebral artery stenting: technical casereport. Neurosurgery 2000; 46: 1524–27.
7 Seldinger S. Catheter replacement of the needle in percutaneousangiography: a new technique. Acta Radiol 1953; 39: 368–76.
8 Moran CJ, Cross D, Talcott M, Garibaldi J, Dacey R. Magneticallycontrolled endovascular navigation: in vivo experience. J Neurosurg2000; 92: 205.
9 Sussman BJ, Fitch TSP. Thrombolysis with fibrinolysis in cerebralarterial occlusion. JAMA 1958; 167: 1705–09.
10 The National Institute of Neurological Disorders and Stroke rt-PAStroke Study Group: Tissue plasminogen activator for acuteischemic stroke: The National Institute of Neurological Disordersand Stroke rt-PA Stroke Study Group. N Engl J Med 1995; 333:1581–87.
For personal use. Only reproduce with permission from The Lancet publishing Group.
REVIEW
THE LANCET • Vol 363 • March 6, 2004 • www.thelancet.com 811
11 Hacke W, Kaste M, Fieschi C, et al. Randomized double-blindplacebo-controlled trial of thrombolytic therapy with intravenousalteplase in acute ischaemic stroke (ECASS II). Second European-Australasian Acute Stroke Study Investigators. Lancet 1998; 352:1245–51.
12 Albers GW, Bates VE, Clark WM, Bell R, Verro P, Hamilton SA.Intravenous tissue-type plasminogen activator for treatment of acutestroke: the Standard Treatment with Alteplase to Reverse Stroke(STARS) study. JAMA 2000; 283: 1145–50.
13 Qureshi AI, Ringer AJ, Suri MF, Guterman LR, Hopkins LN. Acuteinterventions for ischemic stroke: Present status and future directions.J Endovasc Ther 2000; 7: 423–28.
14 Qureshi AI, Ali Z, Suri MFK, et al. Intra-arterial third-generationrecombinant tissue plasminogen activator (reteplase) for acuteischemic stroke. Neurosurgery 2001; 49: 41–50.
15 Qureshi AI, Siddiqui AM, Suri MF, et al. Aggressive mechanical clotdisruption and low-dose intra-arterial third-generation thrombolyticagent for ischemic stroke: a prospective study. Neurosurgery 2002; 51:1319–27.
16 Tomsick T, Brott T, Barsan W, et al. Prognostic value of thehyperdense middle cerebral artery sign and stroke scale score beforeultraearly thrombolytic therapy. Am J Neuroradiol 1996; 17: 79–85.
17 Furlan A, Higashida R, Wechsler L, et al. Intra-arterial prourokinasefor acute ischemic stroke. The PROACT II study: a randomizedcontrolled trial. Prolyse in Acute Cerebral Thromboembolism.JAMA 1999; 282: 2003–11.
18 Chalela JA, Katzan I, Liebeskind DS, et al. Safety of intra-arterialthrombolysis in the postoperative period. Stroke 2000; 32: 1365–69.
19 del Zoppo GJ, Poeck K, Pessin MS, et al.Recombinant tissueplasminogen activator in acute thrombotic and embolic stroke.Ann Neurol 1992; 32: 78–86.
20 Sen S, Agarwal P, Eskhar N, Verro P. Differential response tointravenous versus intra-arterial thrombolysis in acute ischemic strokeon the basis of hyperdense middle cerebral artery sign. Stroke 2003;34: 285.
21 Qureshi AI. New grading system for angiographic evaluation ofarterial occlusions and recanalization response to intra-arterialthrombolysis in acute ischemic stroke. Neurosurgery 2002; 50:1405–15.
22 Suarez JI, Sunshine JL, Tarr R, et al. Predictors of clinicalimprovement, angiographic recanalization, and intracranialhemorrhage after intra-arterial thrombolysis for acute ischemic stroke.Stroke 1999; 30: 2094–100.
23 Ueda T, Sakaki S, Kumon Y, Ohta S. Multivariable analysis ofpredictive factors related to outcome at 6 months after intra-arterialthrombolysis for acute ischemic stroke. Stroke 1999; 30: 2360–65.
24 del Zoppo GJ, Higashida RT, Furlan AJ, Pessin MS, Rowley HA,Gent M. PROACT: a Phase II randomized trial of recombinant pro-urokinase by direct arterial delivery in acute middle cerebral arterystroke—PROACT Investigators: Prolyse in Acute CerebralThromboembolism. Stroke 1998; 29: 4–11.
25 Qureshi AI, Suri MF, Shatla AA, et al. Intraarterial recombinanttissue plasminogen activator for ischemic stroke: An acceleratingdosing regimen. Neurosurgery 2000; 47: 473–79.
26 Zeumer H, Freitag HJ, Zanella F, Thie A, Arning C. Local intra-arterial fibrinolytic therapy in patients with stroke: urokinase versusrecombinant tissue plasminogen activator (r-TPA). Neuroradiology1993; 35: 159–62.
27 Lewandowski CA, Frankel M, Tomsick TA, et al. Combinedintravenous and intra-arterial r-TPA versus intra-arterial therapy ofacute ischemic stroke: Emergency Management of Stroke (EMS)Bridging Trial. Stroke 1999; 30: 2598–605.
28 The IMS Investigators. The Interventional Management of Stroke(IMS) Study: safety results. Stroke 2003; 34: 247.
29 Kim S, Siddiqui A, Hanel R, et al. Mechanical thrombolysis for acuteischemic stroke. Neurointerventionist 2003; 4: 15–22.
30 Mahon BR, Nesbit GM, Barnwell SL, et al. North American clinicalexperience with the EKOS MicroLysUS infusion catheter fortreatment of embolic stroke. Am J Neuroradiol 2003; 24: 534–38.
31 Lutsep HL, Campbell M, Clark WM. EPAR therapy system fortreatment of acute stroke: safety study results. Stroke 2001; 32: 319b.
32 Starkman S, Gobin YP, Duckwiler GR, Higashida R. Mechanicalembolus removal in cerebral ischemia (MERCI) trial. 7thInternational Symposium on Thrombolysis and Acute StrokeTherapy, Lyons, France, May 2002.
33 Eckert B, Koch C, Thomalla G, Roether J, Zeumer H. Acute basilarartery occlusion treated with combined intravenous Abciximab andintra-arterial tissue plasminogen activator: report of 3 cases. Stroke2002; 33: 1424–27.
34 North American Symptomatic Carotid Endarterectomy TrialCollaborators. Beneficial effect of carotid endarterectomy insymptomatic patients with high-grade carotid stenosis. N Engl J Med1991; 325: 445–53.
35 Barnett HJ, Taylor DW, Eliasziw M, et al, for the North AmericanSymptomatic Carotid Endarterectomy Trial Collaborators. Benefit ofcarotid endarterectomy in patients with symptomatic moderate orsevere stenosis. N Engl J Med 1998; 339: 1415–25.
36 Randomised trial of endarterectomy for recently symptomatic carotidstenosis: final results of the MRC European Carotid Surgery Trial(ECST). Lancet 1998; 351: 1379–87.
37 Executive Committee for the Asymptomatic Carotid AtherosclerosisStudy. Endarterectomy for asymptomatic carotid artery stenosis. JAMA 1995; 273: 1421–28.
38 Stukenborg GJ. Comparison of carotid endarterectomy outcomes fromrandomized controlled trials and Medicare administrative databases.Arch Neurol 1997; 54: 826–32.
39 Wennberg DE, Lucas FL, Birkmeyer JD, Bredenberg CE, Fisher ES.Variation in carotid endarterectomy mortality in the Medicarepopulation: trial hospitals, volume, and patient characteristics.JAMA 1998; 279: 1278–81.
40 Goldstein LB, McCrory DC, Landsman PB, et al. Multicenter reviewof preoperative risk factors for carotid endarterectomy in patients withipsilateral symptoms. Stroke 1994; 25: 1116–21.
41 Goldstein LB, Samsa GP, Matchar DB, Oddone EZ. Multicenterreview of preoperative risk factors for endarterectomy for asymptomaticcarotid artery stenosis. Stroke 1998; 29: 750–53.
42 Rothwell PM, Slattery J, Warlow CP. Clinical and angiographicpredictors of stroke and death from carotid endarterectomy: systematicreview. BMJ 1997; 315: 1571–77.
43 Hanel RA, Xavier AR, Kirmani JF, Yahia AM, Qureshi AI.Management of carotid artery stenosis: comparing endarterectomy andstenting. Curr Cardiol Rep 2003; 5: 153–59.
44 Kerber CW, Hornwell LD, Loeden OL. Catheter dilatation of proximalcarotid stenosis during distal bifurcation endarterectomy. Am J Neuroradiol 1980; 1: 348–49.
45 Theron J, Raymond J, Casasco A, Courtheoux F. Percutaneousangioplasty of atherosclerotic and post surgical stenosis of carotidarteries. Am J Neuroradiol 1987; 8: 495–500.
46 Ouriel K, Hertzer NR, Beven EG, et al. Preprocedural riskstratification: identifying an appropriate population for carotid stenting.J Vasc Surg 2001; 33: 728–32.
47 Lopes DK, Mericle RA, Lanzino G, Wakhloo AK, Guterman LR,Hopkins LN. Stent placement for the treatment of occlusiveatherosclerotic carotid artery disease in patients with concomitantcoronary artery disease. J Neurosurg 2002; 96: 490–96.
48 Babatasi G, Massetti M, Theron J, Khayat A. Asymptomatic carotidstenosis in patients undergoing major cardiac surgery: can percutaneouscarotid angioplasty be an alternative? Eur J Cardiothorac Surg 1997; 11: 547–53.
49 Qureshi AI, Ali Z, Suri MF, et al. Open-label phase I clinical study toassess the safety of intravenous eptifibatide in patients undergoinginternal carotid artery angioplasty and stent placement. Neurosurgery2001; 48: 998–1004.
50 Yadar I, for the SAPPHIRE investigators. Stenting and angioplasty withprotection in patients at high risk for endarterectomy: the SAPPHIREstudy. 15th Annual Transcatheter Cardiovascular TherapeuticsSymposium. Washington, DC. Sept 15–19, 2003.
51 Kim SH, Mericle RA, Lanzino G, Qureshi AI, Guterman LR, Hopkins LN. Carotid angioplasty and stent placement in patients withtandem stenosis. Neurosurgery 1998; 43: 708A.
52 Mericle RA, Kim SH, Lanzino G, et al. Carotid artery angioplasty anduse of stents in high-risk patients with contralateral occlusions.J Neurosurg 1999; 90: 1031–36.
53 New G, Roubin GS, Iyer SS, et al. Safety, efficacy, and durability ofcarotid artery stenting for restenosis following carotid endarterectomy: amulticenter study. J Endovasc Ther 2000; 7: 345–52.
54 Houdart E, Mounayer C, Chapot R, Saint-Maurice JP, Merland JJ.Carotid stenting for radiation-induced stenoses: a report of 7 cases.Stroke 2001; 32: 118–21.
55 Malek AM, Higashida RT, Phatouros CC, et al. Endovascularmanagement of extracranial carotid artery dissection achieved usingstent angioplasty. Am J Neurorad 2000; 21: 1280–92.
56 Roubin GS, New G, Iyer S, et al. Immediate and late clinical outcomesof cartoid artery stenting in patients with symptomatic andasymptomatic cartoid artery stenosis: a 5-year perspective analysis.Circulation 2001; 103: 532–37.
57 Qureshi AI, Luft AR, Janardhan V, et al. Identification of patients atrisk for periprocedural neurological deficits associated with carotidangioplasty and stenting. Stroke 2000; 31: 376–82.
58 Qureshi AI, Luft AR, Sharma M, Guterman LR, Hopkins LN.Prevention and treatment of thromboembolic and ischemiccomplications associated with endovascular procedures: part II—Clinical aspects and recommendations. Neurosurgery 2000; 46: 1360–75.
59 Mukherjee D, Kalahasti V, Roffi M, et al. Self-expanding stents forcarotid interventions: comparison of nitinol versus stainless-steel stents.J Invasive Cardiol 2001; 13: 732–35.
For personal use. Only reproduce with permission from The Lancet publishing Group.
REVIEW
812 THE LANCET • Vol 363 • March 6, 2004 • www.thelancet.com
60 Qureshi AI. Adjunctive use of platelet glycoprotein IIb/IIIa inhibitorsfor carotid angioplasty and stent placement: time to say good bye?J Endovasc Ther 2003; 10: 42–44.
61 Qureshi AI, Suri MF, Ali Z, et al. Carotid angioplasty and stentplacement: a prospective analysis of perioperative complications andimpact of intravenously administered abciximab. Neurosurgery 2002;50: 466–73.
62 Hofmann R, Kerschner K, Steinwender C, Kypta A, Bibl D,Leisch F. Abciximab bolus injection does not reduce cerebralischemic complications of elective carotid artery stenting: arandomized study. Stroke 2002; 33: 725–27.
63 Grube E, Colombo A, Hauptmann E, et al. Initial multicenterexperience with a novel distal protection filter during carotid artery stent implantation. Cath Cardiovasc Intervent 2003; 58:139–46.
64 Van Heesewijk HPM, Vos JA, Louwerse ES, et al. Carotid PTA and Stenting Collaborative Research Group. New Brain lesions atMR imaging after carotid angioplasty and stent placement. Radiology 2002; 224: 361–65.
65 Barth A, Remonda L, Lovblad KO, Schroth G, Seiler RW. Silentcerebral ischemia detected by diffusion-weighted MRI after carotidendarterectomy. Stroke 2000; 31: 1824–28.
66 Adami CA, Scuro A, Spinamano L, et al. Use of the Parodi anti-embolism system in carotid stenting: Italian trial results. J Endovasc Ther 2002; 9: 147–54.
67 Whitlow PL, Lylyk P, Londero H, et al. Carotid artery stentingprotected with an emboli containment system. Stroke 2002; 33:1308–14.
68 Reimers B, Corvaja N, Moshiri S, et al. Cerebral protection with filterdevices during carotid artery stenting. Circulation 2001; 104: 12–15.
69 Al-Mubarak N, Colombo A, Gaines PA, et al. Multicenter evaluationof carotid artery stenting with a filter protection system. J Am Coll Cardiol 2002; 39: 841–46.
70 Wholey MH. ARCHeR: Acculink for Revascularization of carotids inHigh-Risk Patients: preliminary 30-day results. American College ofCardiology 52nd Annual Meeting Scientific Session; 2003 March30–April 2; Chicago, IL, USA.
71 Kastrup A, Groschel K, Krapf H, Brehm BR, Dichgans J, Schulz JB.Early outcome of carotid angioplasty and stenting with and withoutcerebral protection devices: a systematic review of the literature.Stroke 2003; 34: 813–19.
72 Naylor AR, Bolia A, Abbott RJ, et al. Randomized study of carotidangioplasty and stenting versus carotid endarterectomy: a stoppedtrial. J Vasc Surg 1998; 28: 326–34.
73 Alberts MA, for the Publications Committee of the WALLSTENT.Results of a multicenter prospective randomized trial of carotidstenting vs carotid endarterectomy. Stroke 2001; 32: 325.
74 Qureshi AI, Suri MF, New G, Wadsworth DC Jr, Dulin J,Hopkins LN. Multicenter study of the feasibility and safety of usingthe memotherm carotid arterial stent for extracranial carotid arterystenosis. J Neurosurg 2002; 96: 830–36.
75 Qureshi AI, Knape C, Maroney J, Suri MFK, Hopkins LN.Multicenter clinical trial of treatment of extracranial carotid arterystenosis using the Endotex coiled sheet stent: immediate results andlate clinical outcomes. J Neurosurg 2003; 99: 264–70.
76 Link J, Manke C, Rosin L, et al. Carotid endarterectomy and carotidstenting: a pilot study of a prospective, randomized and controlledcomparison. Radiologe 2000; 40: 813–20.
77 Tubler T, Schluter M, Dirsch O, et al. Balloon-protected carotidartery stenting: relationship of periprocedural neurologicalcomplications with size of particulate debris. Circulation 2001; 104:2791.
78 Brooks WH, McClure RR, Jones MR, Coleman TC, Breathitt L.Carotid angioplasty and stenting versus carotid endarterectomy:randomized trial in a community hospital. JAm Coll Cardiol 2001; 38:1589–95.
79 CAVATAS Investigators. Endovascular versus surgical treatment inpatients with carotid stenosis in the Carotid and Vertebral ArteryTransluminal Angioplasty Study (CAVATAS): a randomized trial.Lancet 2001; 357: 1729–37.
80 Hobson RW, and the CREST Executive Committee. Carotid stentingin the CREST lead-in phase: periprocedural stroke, myocardialinfarction, and death rates. Stroke 2003; 34: 238.
81 Wityk RJ, Lehman D, Klag M, Coresh J, Ahn H, Litt B. Race and sexdifferences in the distribution of cerebral atherosclerosis. Stroke 1996;27: 1974–80.
82 Qureshi AI, Suri MFK, Ziai WC, et al. Stroke free survival and itsdeterminants in patients with symptomatic vertebrobasilar stenosis.a multicenter study. Neurosurgery 2003; 52: 1033–40.
83 Bogousslavsky J, Barnett HJ, Fox AJ, Hachinski VC, Taylor W.Atherosclerotic disease of the middle cerebral artery. Stroke 1986; 17:1112–20.
84 Chimowitz MI, Kokkinos J, Strong J, et al. The Warfarin-Aspirin
Symptomatic Intracranial Disease Study. Neurology 1995; 45:1488–93.
85 Thijs VN, Albers GW. Symptomatic intracranial atherosclerosis:outcome of patients who fail antithrombotic therapy. Neurology 2000;55: 490–97.
86 Ali Z, Qureshi AI, Suri MFK, et al. Single-center study to evaluatelong-term effectiveness of angioplasty and/or stent placement forintracranial atherosclerotic disease. Neurology 2002; 58: A313.
87 Marks MP, Marcellus M, Norbash AM, Steinberg GK, Tong D,Albers GW. Outcome of angioplasty for atherosclerotic intracranialstenosis. Stroke 1999; 30: 1065–69.
88 Gomez CR, Misra VK, Liu MW, et al. Elective stenting ofsymptomatic basilar artery stenosis. Stroke 2000; 31: 95–99.
89 Lutsep HL, Barnwell SL, Mawad M, et al. Stenting of symptomaticatherosclerotic lesions in the vertebral or intracranial arteries(SSYLVIA): study results. Stroke 2003; 34: 253.
90 Rinkel GJ, Djibuti M, Algra A, van Gijn J. Prevalence and risk ofrupture of intracranial aneurysms: a systematic review. Stroke 1998;29: 251–56.
91 Werner SC, Blakemore AH, King BG. Aneurysm of the internalcarotid artery within the skull: wiring and electrothermic coagulation.JAMA 1941; 116: 578–82.
92 Guglielmi G, Vinuela F, Sepetka I, Macellari V. Electrothrombosis ofsaccular aneurysms via endovascular approach. Part 1:Electrochemical basis, technique, and experimental results.J Neurosurg 1991; 75: 1–7.
93 Macdonald RL, Mojtahedi S, Johns L, Kowalczuk A. Randomizedcomparison of Guglielmi detachable coils and cellulose acetatepolymer for treatment of aneurysms in dogs. Stroke 1998; 29: 478–85.
94 Stiver SI, Porter PJ, Willinsky RA, Wallace MC. Acute humanhistopathology of an intracranial aneurysm treated using Guglielmidetachable coils: case report and review of the literature. Neurosurgery1998; 43: 1203–08.
95 Qureshi AI, Suri MF, Khan J, et al. Endovascular treatment ofintracranial aneurysms by using Guglielmi detachable coils in awakepatients: safety and feasibility. J Neurosurg 2001; 94: 880–85.
96 Cottier JP, Pasco A, Gallas S, et al. Utility of balloon-assistedGuglielmi detachable coiling in the treatment of 49 cerebralaneurysms: a retrospective, multicenter study. Am J Neuroradiol 2001;22: 345–51.
97 Lanzino G, Wakhloo AK, Fessler RD, Hartney ML, Guterman LR,Hopkins LN. Efficacy and current limitations of intravascular stentsfor intracranial internal carotid, vertebral, and basilar arteryaneurysms. J Neurosurg 1999; 91: 538–46.
98 Raymond J, Guilbert F, Roy D. Neck-bridge device for endovasculartreatment of wide-neck bifurcation aneurysms: initial experience.Radiology 2001; 221: 318–26.
99 Mawad ME, Cekirge S, Ciceri E, Saatci I. Endovascular treatment ofgiant and large intracranial aneurysms by using a combination of stentplacement and liquid polymer injection. J Neurosurg 2002; 96:474–82.
100Johnston SC, Higashida RT, Barrow DL, et al. Committee onCerebrovascular Imaging of the American Heart Association Councilon Cardiovascular Radiology. Recommendations for the endovasculartreatment of intracranial aneurysms: a statement for healthcareprofessionals from the Committee on Cerebrovascular Imaging of theAmerican Heart Association Council on Cardiovascular Radiology.Stroke 2002; 33: 2536–44.
101Sedat J, Dib M, Lonjon M, et al.Endovascular treatment of rupturedintracranial aneurysms in patients aged 65 years and older: follow-upof 52 patients after 1 year. Stroke 2002; 33: 2620–25.
102Kremer C, Groden C, Hansen HC, Grzyska U, Zeumer H. Outcomeafter endovascular treatment of Hunt and Hess grade IV or Vaneurysms: comparison of anterior versus posterior circulation. Stroke1999; 30: 2617–22.
103Vallee JN, Aymard A, Vicaut E, Reis M, Merland JJ. Endovasculartreatment of basilar tip aneurysms with Guglielmi detachable coils:predictors of immediate and long-term results with multivariateanalysis 6-year experience. Radiology 2003; 226: 867–79.
104Baltsavias GS, Byrne JV, Halsey J, Coley SC, Sohn MJ, Molyneux AJ.Effects of timing of coil embolization after aneurysmal subarachnoidhemorrhage on procedural morbidity and outcomes. Neurosurgery2000; 47: 1320–29.
105Morizane A, Nakahara I, Sakai N, et al. Endovascular surgery foruntreated ruptured aneurysm with symptomatic vasospasm. Neurol Surg 1999; 27: 941–46.
106Brilstra EH, Rinkel GJE, van der Graaf Y, van Rooij WJJ, Algra A.Treatment of intracranial aneurysms by embolization with coils: asystematic review. Stroke 1999; 30: 470–76.
107Kuether TA, Nesbit GM, Barnwell SL. Clinical and angiographicoutcomes, with treatment data, for patients with cerebral aneurysmstreated with Guglielmi detachable coils: a single-center experience.Neurosurgery 1998; 43: 1016–25.
For personal use. Only reproduce with permission from The Lancet publishing Group.
REVIEW
THE LANCET • Vol 363 • March 6, 2004 • www.thelancet.com 813
108 Malisch TW, Guglielmi G, Vinuela F, et al. Intracranial aneurysmstreated with the Guglielmi detachable coil: midterm clinical results in aconsecutive series of 100 patients. J Neurosurg 1997; 87:176–83.
109 Makoui AS, Smith DA, Evans AJ, Cahill DW. Early aneurysmrecurrence after technically satisfactory Guglielmi detachable coiltherapy: is early surveillance needed? Case report. J Neurosurg 2000; 92:355–58.
110 Vanninen R, Koivisto T, Saari T, Hernesniemi J, Vapalahti M.Ruptured intracranial aneurysms: acute endovascular treatment withelectrolytically detachable coils: a prospective randomized study.Radiology 1999; 211: 325–36.
111 Koivisto T, Vanninen R, Hurskainen H, Saari T, Hernesniemi J,Vapalahti M. Outcomes of early endovascular versus surgical treatmentof ruptured cerebral aneurysms: a prospective randomized study. Stroke2000; 31: 2369–77.
112 Molyneux A, Kerr R, Stratton I, et al, for the InternationalSubarachnoid Aneurysm Trial (ISAT) Collaborative Group.International Subarachnoid Aneurysm Trial (ISAT) of neurosurgicalclipping versus endovascular coiling in 2143 patients with rupturedintracranial aneurysms: a randomized trial. Lancet 2002; 1267–74.
113 Qureshi AI, Suri MFK, Hanel RA, Hopkins LN. Trends in morbidityand mortality associated with hospitalization for ruptured andunruptured aneurysms in the United States. Stroke 2002; 33: 353.
114 Johnston SC, Dudley RA, Gress DR, Ono L. Surgical and endovasculartreatment of unruptured cerebral aneurysms at university hospitals.Neurology 1999; 52: 1799–805.
115 Johnston SC, Zhao S, Dudley RA, Berman MF. Gress DR. Treatmentof unruptured cerebral aneurysms in California. Stroke 2001; 32:597–605.
116 Johnston SC, Wilson CB, Halbach VV, et al. Endovascular and surgicaltreatment of unruptured cerebral aneurysms: comparison of risks. Ann Neurol 2000; 48: 11–19.
117 Brooks B. Discussion of paper by Noland L, Taylor AS. Trans South Surg Assoc 1931; 43: 176–77.
118 Luessenhop AJ, Kachmann R Jr, Shevlin W, Ferrero AA. Clinicalevaluation of artificial embolization in the management of large cerebralarteriovenous malformations. J Neurosurg 1965; 23: 400–17.
119 Vinuela F, Dion JE, Duckwiler G, et al. Combined endovascularembolization and surgery in the management of cerebral arteriovenousmalformations: experience with 101 cases. J Neurosurg 1991; 75:856–64.
120 Ogilvy CS, Stieg PE, Awad I, et al. A Special Writing Group of theStroke Council, American Stroke Association. AHA ScientificStatement: Recommendations for the management of intracranialarteriovenous malformations: a statement for healthcare professionalsfrom a special writing group of the Stroke Council, American StrokeAssociation. Stroke 2001; 32: 1458–71.
121 Purdy PD, Batjer HH, Risser RC, Samson D. Arteriovenousmalformations of the brain: choosing embolic materials to enhancesafety and ease of excision. J Neurosurg 1992; 77: 217–22.
122 Henkes H, Nahser HC, Berg-Dammer E, Weber W, Lange S,Kuhne D. Endovascular therapy of brain AVMs prior to radiosurgery.Neurol Res 1998; 20: 479–92.
123 Jafar JJ, Davis AJ, Berenstein A, Choi IS, Kupersmith MJ. The effect ofembolization with N-butyl cyanoacrylate prior to surgical resection of
cerebral arteriovenous malformations. J Neurosurg 1993; 78:60–69.
124 DeMeritt JS, Pile-Spellman J, Mast H, et al. Outcome analysis ofpreoperative embolization with N-butyl cyanoacrylate in cerebralarteriovenous malformations. Am J Neurorad 1995; 16: 1801–07.
125 The n-BCA Trail Investigators. N-butyl cyanoacrylate embolization ofcerebral arteriovenous malformations: results of a prospective,randomized, multi-center trial. Am J Neurorad 2002; 23: 748–55.
126 Gobin YP, Laurent A, Merienne L, et al. Treatment of brainarteriovenous malformations by embolization and radiosurgery.J Neurosurg 1996; 85: 19–28.
127 Roy D, Raymond J. The role of transvenous embolization in thetreatment of intracranial dural arteriovenous fistulas. Neurosurgery1997; 40: 1133–41.
128 Murphy KJ, Gailloud P, Venbrux A, Deramond H, Hanley D,Rigamonti D. Endovascular treatment of a grade IV transverse sinusdural arteriovenous fistula by sinus recanalization, angioplasty, andstent placement: technical case report. Neurosurgery 2000; 46: 497–500.
129 Langen KJ, Roosen N, Kuwert T, et al. Early effects of intra-arterialchemotherapy in patients with brain tumours studied with PET:preliminary results. Nucl Med Commun 1989; 10: 779–90.
130 Shapiro WR, Green SB, Burger PC, et al. A randomized comparison ofintra-arterial versus intravenous BCNU, with or without intravenous 5-fluorouracil, for newly diagnosed patients with malignant glioma. J Neurosurg 1992; 76: 772–81.
131 Cloughesy TF, Gobin YP, Black KL, et al. Intra-arterial carboplatinchemotherapy for brain tumors: a dose escalation study based oncerebral blood flow. J Neurooncol 1997; 35: 121–31.
132 Inamura T, Nomura T, Bartus RT, Black KL. Intracarotid infusion ofRMP-7, a bradykinin analog: a method for selective drug delivery tobrain tumors. J Neurosurg 1994; 81: 752–58.
133 Cloughesy TF, Black KL, Gobin YP, et al. Intra-arterial Cereport(RMP-7) and carboplatin: a dose escalation study for recurrentmalignant gliomas. Neurosurgery 1999; 44: 270–78.
134 Chow KL, Gobin YP, Cloughesy T, Sayre JW, Villablanca JP, Vinuela F. Prognostic factors in recurrent glioblastoma multiforme andanaplastic astrocytoma treated with selective intra-arterialchemotherapy. Am J Neurorad 2000; 21: 471–78.
135 Engelhard HH. Progress in the diagnosis and treatment of patients withmeningiomas. Part I: diagnostic imaging, preoperative embolization.Surg Neurol 2001; 55: 89–101.
136 Dean BL, Flom RA, Wallace RC, et al. Efficacy of endovasculartreatment of meningiomas: evaluation with matched samples. Am J Neurorad 1994; 15: 1675–80.
137 Bendszus M, Rao G, Burger R, et al. Is there a benefit of preoperativemeningioma embolization?. Neurosurgery 2000; 47: 1306–11.
138 Kai Y, Hamada J, Morioka M, Yano S, Todaka T, Ushio Y.Appropriate interval between embolization and surgery in patients withmeningioma. Am J Neurorad 2002; 23: 139–42.
139 Li Y, Chen J, Wang L, Lu M, Chopp M. Treatment of stroke in ratwith intracarotid administration of marrow stromal cells.Neurology 2001; 56: 1666–72.
140 Zlokovic BV, Apuzzo ML. Cellular and molecular neurosurgery:pathways from concept to reality: part II: vector systems and deliverymethodologies for gene therapy of the central nervous system.Neurosurgery 1997; 40: 805–12.




















