Pancreatic resections for cystic neoplasms: From the surgeon's presumption to the pathologist's...
8
Pancreatic resections for cystic neoplasms: From the surgeon’s presumption to the pathologist’s reality Roberto Salvia, MD, PhD, Giuseppe Malleo, MD, Giovanni Marchegiani, MD, Silvia Pennacchio, MD, Salvatore Paiella, MD, Marina Paini, MD, Antonio Pea, MD, Giovanni Butturini, PhD, Paolo Pederzoli, MD, and Claudio Bassi, MD, Verona, Italy Background. Current guidelines for the management of pancreatic cystic neoplasms are based on the assumption that these lesions can be classified correctly on the basis of features of cross-sectional imaging. However, a certain degree of overlap between different lesions exists, and little is known about the rate of inaccurate preoperative diagnoses. To address this issue, preoperative and final pathologic diagnoses of patients resected for a presumed pancreatic cystic neoplasm were compared. Methods. Retrospective analysis was undertaken of patients managed operatively between 2000 and 2010. Preoperative workup was reviewed to identify diagnostic pitfalls and potential risk factors for incorrect preoperative characterization of cystic lesions presumed to be neoplastic. Results. We analyzed 476 patients. Final pathologic diagnosis matched the preoperative diagnosis in 78% of cases. The highest accuracy was reached for solid pseudopapillary neoplasms (95%) and for main duct/mixed duct intraductal papillary mucinous neoplasms (81%). Surprisingly, 23 cysts (5%) were found to be ductal adenocarcinoma, whereas 45 patients (9%) underwent a pancreatic resection for a non-neoplastic condition. The use of a routine radiologic workup, including contrast-enhanced ultrasonography and magnetic resonance imaging, was associated with a favorably correct character- ization of the cystic lesion. Endoscopic ultrasonography did not seem to improve diagnostic accuracy. Increased levels of serum carbohydrate antigen (CA)19-9 resulted as risk factors for an incorrect diagnosis as well as for a final diagnosis of a ductal adenocarcinoma. Conclusion. The overall rate of inaccurate preoperative diagnoses in a tertiary care center with a broad experience in pancreatology approached 22%. Serum CA19-9 is an important complementary tool within the context of preoperative investigation of cystic neoplasms of the pancreas. (Surgery 2012;152:S135-42.) From the Unit of General Surgery B, Pancreas Institute, ‘‘G.B. Rossi’’ Hospital, Department of Surgery, University of Verona Hospital Trust, Italy PANCREATIC CYSTIC NEOPLASMS are encountered commonly in clinical practice and are often identi- fied incidentally on cross-sectional imaging per- formed for other complaints. 1 These lesions are heterogeneous histologically and encompass a wide spectrum of biologic behaviors. 2 Because management of these neoplasms is driven mainly by the presenting symptoms and radiologic characteristics, identification of suspicious features and accurate preoperative classification are crucial for selecting appropriate treatment. 3 Although a variety of invasive and noninvasive imaging modal- ities are applied routinely in the diagnostic workup, such as contrast-enhanced computed to- mography, magnetic resonance imaging (MRI) with magnetic resonance cholangiopancreatogra- phy (MRCP), contrast-enhanced ultrasonography (CEUS), and endoscopic ultrasonography (EUS) with cyst fluid aspirate, an ideal test or combina- tion of tests has not been found, and overall radi- ologic accuracy has been shown to be moderate to good. 4 There is little information about the clin- ical ability to determine the nature of pancreatic cysts in advance of tissue diagnosis, the rate of ag- gressive solid malignancies masqueraded by a cys- tic phenotype, and the burden of inappropriate Accepted for publication May 11, 2012. Reprint requests: Roberto Salvia, MD, PhD, Department of Sur- gery, General Surgery B – Pancreas Institute, ‘‘G.B. Rossi’’ Hos- pital, P.le L.A. Scuro 10, 37134 Verona, Italy. E-mail: roberto. [email protected]. 0039-6060/$ - see front matter Ó 2012 Mosby, Inc. All rights reserved. http://dx.doi.org/10.1016/j.surg.2012.05.019 SURGERY S135
Transcript of Pancreatic resections for cystic neoplasms: From the surgeon's presumption to the pathologist's...

Accepte
Reprintgery, Gepital, P.salvia@o
0039-60
� 2012
http://d
Pancreatic resections for cysticneoplasms: From the surgeon’spresumption to the pathologist’srealityRoberto Salvia, MD, PhD, Giuseppe Malleo, MD, Giovanni Marchegiani, MD, Silvia Pennacchio, MD,Salvatore Paiella, MD, Marina Paini, MD, Antonio Pea, MD, Giovanni Butturini, PhD,Paolo Pederzoli, MD, and Claudio Bassi, MD, Verona, Italy
Background. Current guidelines for the management of pancreatic cystic neoplasms are based on theassumption that these lesions can be classified correctly on the basis of features of cross-sectional imaging.However, a certain degree of overlap between different lesions exists, and little is known about the rate ofinaccurate preoperative diagnoses. To address this issue, preoperative and final pathologic diagnoses ofpatients resected for a presumed pancreatic cystic neoplasm were compared.Methods. Retrospective analysis was undertaken of patients managed operatively between 2000 and2010. Preoperative workup was reviewed to identify diagnostic pitfalls and potential risk factors forincorrect preoperative characterization of cystic lesions presumed to be neoplastic.Results. We analyzed 476 patients. Final pathologic diagnosis matched the preoperative diagnosis in78% of cases. The highest accuracy was reached for solid pseudopapillary neoplasms (95%) and formain duct/mixed duct intraductal papillary mucinous neoplasms (81%). Surprisingly, 23 cysts (5%)were found to be ductal adenocarcinoma, whereas 45 patients (9%) underwent a pancreatic resectionfor a non-neoplastic condition. The use of a routine radiologic workup, including contrast-enhancedultrasonography and magnetic resonance imaging, was associated with a favorably correct character-ization of the cystic lesion. Endoscopic ultrasonography did not seem to improve diagnostic accuracy.Increased levels of serum carbohydrate antigen (CA)19-9 resulted as risk factors for an incorrectdiagnosis as well as for a final diagnosis of a ductal adenocarcinoma.Conclusion. The overall rate of inaccurate preoperative diagnoses in a tertiary care center with a broadexperience in pancreatology approached 22%. Serum CA19-9 is an important complementary tool withinthe context of preoperative investigation of cystic neoplasms of the pancreas. (Surgery 2012;152:S135-42.)
From the Unit of General Surgery B, Pancreas Institute, ‘‘G.B. Rossi’’ Hospital, Department of Surgery,University of Verona Hospital Trust, Italy
PANCREATIC CYSTIC NEOPLASMS are encounteredcommonly in clinical practice and are often identi-fied incidentally on cross-sectional imaging per-formed for other complaints.1 These lesions areheterogeneous histologically and encompass awide spectrum of biologic behaviors.2 Becausemanagement of these neoplasms is driven mainlyby the presenting symptoms and radiologic
d for publication May 11, 2012.
requests: Roberto Salvia, MD, PhD, Department of Sur-neral Surgery B – Pancreas Institute, ‘‘G.B. Rossi’’ Hos-le L.A. Scuro 10, 37134 Verona, Italy. E-mail: roberto.spedaleuniverona.it.
60/$ - see front matter
Mosby, Inc. All rights reserved.
x.doi.org/10.1016/j.surg.2012.05.019
characteristics, identification of suspicious featuresand accurate preoperative classification are crucialfor selecting appropriate treatment.3 Although avariety of invasive and noninvasive imaging modal-ities are applied routinely in the diagnosticworkup, such as contrast-enhanced computed to-mography, magnetic resonance imaging (MRI)with magnetic resonance cholangiopancreatogra-phy (MRCP), contrast-enhanced ultrasonography(CEUS), and endoscopic ultrasonography (EUS)with cyst fluid aspirate, an ideal test or combina-tion of tests has not been found, and overall radi-ologic accuracy has been shown to be moderateto good.4 There is little information about the clin-ical ability to determine the nature of pancreaticcysts in advance of tissue diagnosis, the rate of ag-gressive solid malignancies masqueraded by a cys-tic phenotype, and the burden of inappropriate
SURGERY S135

SurgerySeptember 2012
S136 Salvia et al
operative management.5 This last aspect is of greatimportance, because pancreatic surgery is notwithout mortality, and major postoperative compli-cations (as well as of long-term impairment of pan-creatic function) are not negligible.6
The present study compares the preoperativeand final pathologic diagnoses in a cohort of 476patients who underwent resections for pancreaticcystic neoplasms over a 10-year period. Preopera-tive workup was reviewed retrospectively to identifydiagnostic pitfalls and potential risk factors forincorrect preoperative cysts characterization.
MATERIALS AND METHODS
Data acquisition. After institutional reviewboard approval, the pancreatic electronic databaseof the Department of Surgery, University of Ver-ona, was queried to identify patients with asuspected cystic neoplasm of the pancreas whounderwent resection from January 2000 throughDecember 2010. Demographic details, presentingsymptoms, tumor markers, radiologic, operative,and final pathologic data were collected andreviewed. In final pathologic reports, cystic neo-plasms were classified according to the WorldHealth Organization classification of the exocrineand endocrine neoplasms of the pancreas.7 Clini-cal charts and radiologic films of patients withmisdiagnosed cystic neoplasm were retrieved, re-viewed thoroughly, and then discussed by 2 seniorattending surgeons (CB and RS) who were notaware of the final pathologic report. In case of di-vergent opinions, a third expert attending surgeon(PP) was consulted. Once a consensus on the pre-operative diagnosis and indication for operationwas reached, the final pathologic report was exam-ined. Rare pancreatic cystic neoplasms and tumor-like lesions with cystic features were classifiedaccording to the proposal by Kosmahl et al.8
Radiologic workup. Most patients were referredto our institution with $1 imaging test. For thestudy period, our routine radiologic workup forpancreatic cysts included CEUS and MRI withMRCP. Contrast-enhanced computed tomographyis not performed routinely for cystic neoplasms,and most of the computed tomography studieswere carried out in other hospitals before referral.EUS with aspiration of cyst fluid was performedwhen cross-sectional imaging was unclear or whennew clinical manifestations of morphologic modi-fications of the cysts occurred during follow-up(which was scheduled on a yearly basis).
Indications for operation. Despite radiologicfindings, all symptomatic lesions were resected.Symptoms attributable to cystic neoplasm included
typical pancreatic pain, acute pancreatitis, recentonset of diabetes mellitus, pancreatic exocrineinsufficiency, unexplained weight loss, and jaun-dice. Pancreatic resection was also consideredwhen a substantial increase in serum tumormarkers was found, either at the time of diagnosisor during follow-up. In the absence of symptoms,the management was driven by current evidence.Serous cystic neoplasms (SCN) were considered tobe virtually always benign neoplasms. Resectionwas proposed to all surgically fit patients with largelesions (>4 cm) at the time of diagnosis (accord-ing to the findings by Tseng et al9), or when sub-stantial tumor growth occurred during follow-up.Resection was also considered in oligo- and macro-cystic variants indistinguishable from a mucinouscystic neoplasm (MCN). Sendai criteria were usedfor MCN and intraductal MCN (IPMN).10 Before2005, MCNs were always resected; selective man-agement (according to an institutional protocol)was applied to IPMNs.11 Resections was under-taken for all solid pseudopapillary neoplasms(SPT) and for cystic neuroendocrine neoplasms(C-NENs).12,13 In the suspicion of a C-NEN, appro-priate laboratory and radiologic workup wasperformed preoperatively. Before operations,doubtful clinical cases were discussed at our weeklymultidisciplinary meeting. Chronic pancreatitiswas ruled out by a careful analysis of potential eti-ologic factors (especially heavy cigarette smokingor heavy alcohol consumption).
Statistical analysis. Continuous variables wereexpressed as means with standard deviation; Stu-dent’s t-test was used to compare means. chi-squared tests (with Yates continuity correction ina 2 3 2 contingency table) was used for nominaldata; the 2-tailed Fisher’s exact test was used inthe case of a small expected frequency. Study ofpredictors of a final incorrect diagnosis was carriedout by employing binary logistic regression. Threedifferent models were designed. In the first, diag-nostic accuracy (correspondence between the pre-operative and the final pathologic diagnosis) wasconsidered as a dependent dichotic variable; inthe second, the dependent dichotic variable wasthe final diagnosis of ductal adenocarcinoma(yes/no); and in the third, the dependent dichoticvariable was a final diagnosis of non-neoplastic,nonepithelial lesions or of other alterations mim-icking cystic neoplasms (yes/no). The indepen-dent categorical variables with a potentialsignificance were gender, serum carbohydrate anti-gen (CA)19-9 levels, symptoms at the time of diag-nosis, tumor location, preoperative workup(routine workup [CEUS + MRI/MRCP], yes/no),

Table I. Demographic, radiologic, and surgicaldetails of patients (n = 476) who underwent apancreatic resection with a preoperative diagnosisof a cystic neoplasm
Characteristic n (%)
GenderMale 165 (34.7)Female 311 (65.3)
Active smokerYes 183 (38.4)No 293 (61.6)
History of alcohol abuseYes 87 (18.3)No 389 (81.7)
Serum CA19-9 levels (U/mL)>37 79 (16.6)<37 397 (83.4)
Symptoms at the diagnosisYes 280 (58.8)No 196 (41.2)
Location of the cystHead-uncinate process-neck 207 (43.5)Body-tail 269 (56.5)
Preoperative radiologic workup (%)CEUS 428/476 (89.9)CECT 353/476 (74.2)MRI/MRCP 356/476 (74.8)EUS 70/476 (14.7)
Preoperative diagnosis (%)SCN 69 (14.5)MCN 123 (25.8)MD/Mixed-IPMN 156 (32.8)BD-IPMN 75 (15.8)SPN 38 (8.0)
C-NEN 15 (3.2)ProceduresDistal pancreatectomy 241 (50.6)Pancreatoduodenectomy 164 (34.5)Total pancreatectomy 35 (7.3)Middle pancreatectomy 23 (4.9)Enucleation 13 (2.7)
Mortality 4 (0.8)
Median age at presentation was 54.2 ± 15.3 (SD).BD-IPMN, Branch duct intraductal papillary mucinous neoplasms; CA19-9,carbohydrate antigen 19-9; CEUS, contrast-enhanced ultrasonography;CECT, contrast-enhanced computed tomography;C-NEN, cystic neuroendo-crine neoplasms; EUS, endoscopic ultrasonography;MCN, mucinous cysticneoplasms; MD/Mixed-IPMN, main duct and mixed-type intraductal papil-lary mucinous neoplasms; MRI/MRCP, magnetic resonance imaging withmagnetic resonance cholangiopancreatography; SCN, serous cystic neo-plasms; SD, standard deviation; SPN, solid pseudopapillary neoplasms.
SurgeryVolume 152, Number 3S
Salvia et al S137
preoperative cyst classification (SCN, MCN, mainduct/mixed duct-IPMN, branch duct-IPMN, SPT,C-NEN). Age was handled as a covariate. For themultivariate models, a backward technique accord-ing to Wald’s test was used (probability for step-wise: entry = 0.05, removal = 0.01). Data arepresented with respective odds ratios (OR) and95% confidence intervals (CI). SPSS (release 19)programs were used for statistical analysis (SPSSInc, Chicago, IL).
RESULTS
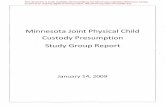
We observed 1,548 patients with a cystic neo-plasm of the pancreas; 497 (32.1%) underwent apancreatic resection, either at the time of diagno-sis (372/497, 74.8%) or during the period ofsurveillance (125/497, 25.2%). Complete preoper-ative details were not available in 21 of 497 patients(4.2%), who were excluded from the presentanalysis. Demographic, preoperative, and surgicaldetails of the study population are outlined inTable I. In 373 of 476 cases (78.4%), final patho-logic diagnosis matched with the preoperativeone, whereas in 103 of 476 cases (21.6%) the path-ologic diagnosis was different. The factors thatprompted operative intervention are summarizedin Table II, whereas an analysis of misdiagnosedneoplasms (with initial and final diagnoses) is pro-vided in Table III. Of note, malignant epithelialneoplasms (which normally present as solid le-sions) were found in 23 of 476 patients (4.8%, allmisdiagnosed). Twenty were ductal adenocarci-nomas and 3 were anaplastic carcinomas. In con-trast, 45 of 103 pancreatic resections (43.7%)were carried out for a non-neoplastic condition(9.4% of all resections for a preoperative diagnosisof a pancreatic cystic neoplasm). Of these 45 pa-tients, 12 were asymptomatic and had normalCA19-9 levels. The number of misdiagnosed neo-plasms divided by year is shown in the Figure.For the univariate analysis, diagnostic accuracy(well-diagnosed/misdiagnosed neoplasms) wasthe dependent variable. There was no differencein terms of operations performed and mortality be-tween the 2 groups (P = .695 and P = 1, data notshown). Male gender and serum CA19-9 levels>37 U/mL were associated univariately with an in-correct preoperative characterization. Perfor-mance of a standard, radiologic workup (CEUS +MRI/MRCP) was associated with a significantlygreater rate of correct diagnosis (Table IV). Theaddition of EUS did not seem to give any advan-tage over CEUS + MRI/MRCP alone (P = .225).Univariate Chi-square analysis by the type of neo-plasms revealed differences between the 2 groups,
mainly attributable to the very high accuracy indiagnosing SPTand to the very poor accuracy in di-agnosing C-NEN (Cramer’s V = 0.176; Goodman-Kruskal tau = 0.013). Table V summarizes theresults of logistic regression analysis. The firstmodel (dependent variable = diagnostic accuracy;overall prediction accuracy = 80.7%) showed that

Table II. Factors that prompted resection in 103misdiagnosed cystic lesions of the pancreas
Factor n (%)
Symptoms 63 (61.2)Radiologic features suspicious for malignancy
Septa 38 (36.9)Thick walls 10 (9.7)Mural nodules 8 (7.8)Tumor growth during follow-up 20 (19.4)Dilated main pancreatic duct 39 (37.9)
Serum CA19-9 levels >37 U/mL 31 (30.1)General suspicion of malignancy 58 (56.3)
Table III. Accuracy of preoperative diagnosis(comparison between principal preoperativediagnosis and final pathologic report) in 476patients resected for a pancreatic cystic neoplasm
Diagnosis n (%)
Well-diagnosed cystic neoplasms 373 (78.4)Misdiagnosed cystic neoplasms 103 (21.6)Serous cystic neoplasms (n = 69)
Well diagnosed 51 (73.9)Misdiagnosed 18 (26.1)
Mucinous cystic neoplasms (n = 123)Well diagnosed 98 (79.7)Misdiagnosed 25 (20.3)
Main duct/mixed-IPMN (n = 156)Well diagnosed 126 (80.7)Misdiagnosed 30 (19.3)
Branch duct-IPMN (n = 75)Well diagnosed 54 (72.0)Misdiagnosed 21 (28.0)
Cystic neuroendocrine neoplasms (n = 15)Well diagnosed 8 (53.3)Misdiagnosed 7 (46.7)
Solid pseudopapillary neoplasms (n = 38)Well diagnosed 36 (94.7)Misdiagnosed 2 (5.3)
IPMN, Intraductal papillary mucinous neoplasms.
Figure. Longitudinal analysis of well-characterized andmisdiagnosed resected cystic neoplasms of the pancreas(division by year).
SurgerySeptember 2012
S138 Salvia et al
performance of a routine radiologic workup(CEUS + MRI/MRCP) and a preoperative suspi-cion of a SPT were associated with a greater prob-ability of a correct final diagnosis (OR, 0.453 and0.160, respectively), whereas male gender andserum CA19-9 levels >37 U/mL were risk factorsfor a misdiagnosis (OR, 1.820 and 6.330, respec-tively). The second model (dependent variable = fi-nal diagnosis of ductal adenocarcinoma; overallprediction accuracy = 93.3%) indicated that serumCA19-9 levels >37 U/mL and male gender wererisk factors for a final diagnosis of ductal adenocar-cinoma (OR, 14.606 and 2.427, respectively). Thethird model (dependent variable = final diagnosis
of non-neoplastic nonepithelial lesions or of otheralterations mimicking cystic neoplasms; overallprediction accuracy = 96.0%) showed that patientswith a preoperative suspicion of main duct/mixedduct-IPMN were at greater risk of being diagnosedwith a non-neoplastic lesion (OR, 7.576). Further-more, age was a significant covariate (OR, 1.865).CA19-9 levels >37 U/mL were associated with alesser probability of a final diagnosis of a non-neoplastic condition (OR, 0.227; Table VI).
DISCUSSION
The decision on whether to observe or to operateon pancreatic cystic neoplasms depends on present-ing symptoms, patient age, comorbidities, andmorphologic features.14,15 Because of our increas-ing awareness of these lesions and technical ad-vances in imaging modalities, the identification ofcharacteristics indicatingmalignant changes has be-come more accurate, in the range from 67–70%.3
The variability of diagnostic accuracy may be attrib-uted to the presence of various atypical elementsand to a certain degree of morphologic overlap.Furthermore, the spectrum of dysplastic changesin mucin-producing lesions does not manifest asspecific feature on imaging.3 The additional valueof EUS is the ability to aspirate cystic lesions with ahigh level of safety. Nevertheless, cytologic yield isquite low, and although cyst-fluid carcinoembry-onic antigen levels are the most accurate marker,this type of analysis also suffers considerable overlapbetween mucinous and non-mucinous cysts.16 Therecognition of cystic neoplasms with aggressive biol-ogy helps in making the decision of resection, butlittle is known about the accuracy of preoperativeclinical and radiologic workup.
In this paper, we analyzed retrospectively datafrom patients who underwent pancreatic resectionfor a presumed cystic neoplasm, and identifiedthose cases with a discrepancy between preoperativeand histologic diagnoses. A thorough review of

Table IV. Analysis of misdiagnosed pancreatic cystic neoplasms (n = 103)
Final pathologic report
Preoperative diagnosis
SCN(n = 18)
MCN(n = 25)
MD/mixedIPMN (n = 30)
BD-IPMN(n = 21)
SPN(n = 2)
C-NEN(n = 7)
Neoplastic epithelialSCN — 6 1 4 0 2MCN 2 — 1 0 0 0IPMN 0 3 — — 0 0C-NEN 0 1 3 2 0 —Ductal adenocarcinoma 8 3 4 4 0 1Acinar cell cystadenoma 1 0 1 0 1 0Acinar cell cystadenocarcinoma 0 0 0 0 0 1Anaplastic carcinoma 0 1 0 1 1 0Pancreatoblastoma 0 0 0 0 0 1Hepatoid carcinoma 0 0 0 0 0 1Granular cell tumor 0 1 0 0 0 0
Neoplastic nonepithelialLymphangioma 0 1 0 0 0 0Mixoid tumor 0 0 1 0 0 0Leiomyoma 0 1 0 0 0 0
Non-neoplastic epithelialLymphoepithelial cyst 2 1 0 1 0 0Retention cyst 1 2 2 0 0 0Enterogeneous cyst 0 0 0 0 0 1Mucinous non-neoplastic cyst 0 0 0 1 0 0Parampullary duodenal wall cyst 0 0 1 0 0 0Unclassifiable cyst 1 1 0 0 0 0Ductal ectasia 0 0 6 4 0 0
Non-neoplastic nonepithelialPseudocyst 0 3 0 0 0 0
Other tissue alterations mimicking cystic neoplasmsChronic pancreatitis 0 0 8 3 0 0Fibrosis 3 1 2 0 0 0Autoimmune pancreatitis 0 0 0 1 0 0
MCN, Mucinous cystic neoplasms; MD/Mixed-IPMN, main duct and mixed-type intraductal papillary mucinous neoplasms; BD-IPMN, branch duct intra-ductal papillary mucinous neoplasms; C-NEN, cystic neuroendocrine neoplasms; SCN, serous cystic neoplasms; SPN, solid pseudopapillary neoplasms.
SurgeryVolume 152, Number 3S
Salvia et al S139
clinical details and preoperative radiologic studieswas performed to identify possible predictive factorsfor a misdiagnosis. The group at the MassachusettsGeneral Hospital in Boston has shown recently thatpreoperative workup led to an incorrect classifica-tion in one third of incidentally discovered pancre-atic cysts operated on at presentation.5 The greatestaccuracy was found formain duct-IPMNs (94%) andfor SCNs (83.3%). Of patients presumed to have abranch duct-IPMNs or a MCNs, 64% and 60%were confirmed as such after resection. The accur-acy for C-NENs and for a variety of other diagnoses(including SPTs) was of only 50%. All invasive can-cers met Sendai criteria. Of particular concern,20% of branch duct-IPMN had a main duct compo-nent and, conversely, 5% of resected cysts were non-neoplastic. Among patients who underwent delayedoperation, preoperative and final pathologic diag-noses matched 52% of the time.
Our data confirm that preoperative diagnosticaccuracy of pancreatic cystic neoplasms is far fromoptimal 78.4%. SPTs were almost always classifiedcorrectly, whereas the rate of correct diagnoses formain duct-IPMNs and SCNs was 80.7% and 73.9%,respectively. The diagnostic accuracy for branchduct-IPMNs and MCNs was of about 80%; 7 of 15of C-NENs (47%) were misclassified. Longitudinalanalysis (Figure) did not show any improvementover the years. Most patients are referred to ourcenter from community hospitals or from othertertiary care institutions with $1 imaging test.Our routine radiologic examinations for pancre-atic cysts include CEUS and MRI with MRCP. Theapplication of CEUS in different pancreatic dis-eases has been described recently.17 CEUS is fast,easy to perform in expert hands, and has beenshown to be as accurate as MRI in displaying theanatomic features of cystic neoplasms seen on

Table V. Univariate analysis of potential factors associated with an incorrect preoperative characterizationof pancreatic cystic neoplasms
Study population (n = 476)
Well-diagnosedcystic neoplasms
(n = 373), n (%)
Misdiagnosedcystic neoplasms
(n = 103), n (%) P value OR (95% CI)
Median age at the presentation (yrs) 53.66 (15.83) 56.10 (13.31) .118Gender
Male 119 (31.9) 46 (44.6) .022Female 254 (68.1) 57 (55.4) 0.581 (0.372–0.906)
Active smokerYes 137 (36.7) 46 (44.7) .177No 236 (63.3) 57 (55.3)
History of alcohol abuseYes 63 (16.9) 24 (23.3) .178No 310 (83.1) 79 (76.7)
Serum CA19-9 levels (U/mL)>37 47 (12.6) 32 (31.1) .0001<37 326 (87.4) 71 (68.9) 3.126 (1.863–5.244)
Symptoms at diagnosisYes 217 (58.2) 63 (61.2) .665No 156 (41) 40 (38.8)
Location of the cystHead-uncinate process 165 (44.2) 42 (40.8) .607Body-tail 208 (55.8) 61 (59.2)
Standard radiologic workup (CEUS + MRI/MRCP)Yes 290 (77.7) 65 (63.1) .003No 83 (22.3) 38 (36.9) 0.489 (0.306–0.782)
Preoperative diagnosisSCN 51 (13.7) 18 (17.5) .011*MCN 98 (26.3) 25 (24.3)MD/Mixed-IPMN* 126 (33.8) 30 (29.1)BD-IPMN 54 (14.5) 21(20.4)C-NEN 8 (2.1) 7 (6.8)SPN 36 (9.7)) 2 (1.9)
*Goodman-Kruskal Tau, P = .011; Cramer’s V = 0.176 (P = .011).BD-IPMN, Branch duct intraductal papillary mucinous neoplasms; CA19-9, carbohydrate antigen 19-9; CI, confidence interval; CEUS, contrast-enhancedultrasonography; C-NEN, cystic neuroendocrine neoplasms; MRI/MRCP, magnetic resonance imaging with magnetic resonance cholangiopancreatogra-phy; MCN, mucinous cystic neoplasms; MD/Mixed-IPMN, main duct and mixed-type intraductal papillary mucinous neoplasms; OR, odds ratio; SCN, serouscystic neoplasms; SPN, solid pseudopapillary neoplasms.
SurgerySeptember 2012
S140 Salvia et al
transabdominal ultrasonography.18,19 Hence, it isperformed in nearly all patients who are referredto our institution. Because of economic issues con-nected with resource utilization, cross-sectional re-imaging with MRI is not performed at the time ofreferral if available contrast-enhanced computedtomography shows a clear picture, or if an availableMRI with MRCP seems to be of good quality. Al-though employed routinely in other tertiary carecenters,20 EUS with aspiration of cyst fluid wasonly performed when high-quality, cross-sectionalimaging was unclear or when new clinical manifes-tations of morphologic modifications of the cystsoccurred during follow-up.
On univariate analysis, performance of a rou-tine, radiologic workup with CEUS and MRI/MRCP was associated favorably with a good cyst
characterization. In patients in whom CEUS, MRI/MRCP, and EUS were performed, EUS did notimprove the diagnostic accuracy (P = .225). Thisresult was confirmed on multivariate analysis, sug-gesting a greater probability of a correct final diag-nosis in patients who underwent CEUS + MRI/MRCP. Male gender was significantly associatedwith a greater rate of incorrect diagnoses and wasrevealed as an independent risk factor. In particu-lar, 9 of 12 of SCN in men were misdiagnosed, andthe majority of C-NENs (11/15) occurred in men.A substantially greater proportion of patients withan incorrect preoperative diagnosis had increasedserum CA19-9 levels. Although accumulatingevidence supports the role of intracystic fluid tu-mor markers,21,22 there is little information aboutthe importance of serum tumor markers in

Table VI. Results of the 3 binary logistic regression models investigating independent associations betweenpreoperative characterization and final pathologic diagnosis
Factor P value OR (Exp[B]) 95% CI
Model 1. Dependent dichotic variable = diagnostic accuracy (well-diagnosed/misdiagnosed cystic neoplasms)Preoperative radiologic workupCEUS + MRI/MRCP (level = yes) .004 0.453 0.263–0.779Gender (male) .040 1.820 1.029–3.218Serum CA19-9 levels (>37 U/mL) .0001 6.330 2.191–10.572
Preoperative diagnosisSPN .029 0.160 0.033–0.832
Model 2. Dependent dichotic variable = final diagnosis of ductal adenocarcinoma (yes/no)Serum CA19-9 levels (>37 U/mL) .0001 14.606 3.318–64.300Gender (male) .026 2.427 1.114–5.291
Model 3. Dependent dichotic variable = final diagnosis of non-neoplastic nonepithelial lesions or of other alterationsmimicking cystic neoplasms (yes/no)
Age .022 1.865 1.009–2.923Serum CA19-9 levels (>37 U/mL) .013 0.227 0.071–0.731Preoperative diagnosisMD-Mixed IPMN .010 7.576 1.636–35.078
CA19-9, Carbohydrate antigen 19-9; CEUS, contrast-enhanced ultrasonography; MD/Mixed-IPMN, main duct and mixed-type intraductal papillary muci-nous neoplasms; MRI/MRCP, magnetic resonance imaging with magnetic resonance cholangiopancreatography; SPN, solid pseudopapillary neoplasms.
SurgeryVolume 152, Number 3S
Salvia et al S141
malignant pancreatic cystic neoplasms.23 A recentstudy investigating the ability of serum CA19-9and carcinoembryonic antigen levels to distinguishbenign and invasive IPMNs showed that 80% ofpatients with an invasive IPMN had increased se-rum levels of CA19-9 (cutoff 37 U/mL) and/orcarcinoembryonic antigen, compared with only18% of those with a noninvasive tumor.24 There-fore, when a cystic mass presents with an unclearmorphology and increase in serum CA19-9 levels,the hypothesis of an invasive IPMN has to be alwaysconsidered. Our results show another surprisingscenario; of the 32 misclassified cysts presentingwith increased serum CA19-9 levels, 14 were ductaladenocarcinomas. Overall, the total number ofadenocarcinomas in patients with an incorrectpreoperative diagnosis was 23 of 103, and 8 SCNswere found to be ductal adenocarcinomas. Theincidence of a final diagnosis of a ductal adenocar-cinoma was 4.8% (23/497) in the resected popula-tion and 1.5% (20/1,548) in all patients observedfor a pancreatic cystic neoplasm. Accordingly, itmust be kept in mind that ductal adenocarcinomamay masquerade as cystic phenotype, especiallywhen large areas are found on imaging. In sucha situation, the actual diagnosis is established nor-mally at exploration, thereby leading to changes insurgical strategy (intraoperative fine needle aspira-tion, complete lymph node clearance, typicalresections).
In the multivariate model investigating possiblerisk factors for ductal adenocarcinoma, male gen-der and increased serum CA19-9 levels (with an
OR of 14.606) proved significant. In contrast, 9.4%of all resected cysts (45/476) were histologicallydiagnosed as non-neoplastic or as other pathologicconditions that mimic cystic neoplasms, and 12 ofthese operations were carried out in asymptomaticpatients with normal serum CA19-9 levels. Apartfrom pseudocysts (3 pseudocysts were diagnosedthat were preoperatively labeled as MCNs), little isknown about non-neoplastic pancreatic lesions;some of these lesions have a nonmucinous epithe-lium or are areas of yet nonclassified, althoughductal ectasia may be of metaplastic origin andeven potentially reversible. Other pancreatic pa-thology that mimics cystic neoplasms includeschronic pancreatitis, fibrosis, and mass-formingautoimmune pancreatitis (cystic variant). The mul-tivariate model investigating predictors of non-neoplastic lesions showed that these entities areless likely to present with increases in serum CA19-9 levels, and that age and preoperative diagnosis ofmain duct/mixed-IPMN are significant risk factors(OR, 1.865 and 7.656, respectively). Although inthe present series the greatest accuracy was foundfor main duct-IPMNs (126/156; 94%), 19 of 30 ofmisclassified main duct/mixed-IPMNs were non-neoplastic lesions, meaning that 19 of 45 (42.2%)resections for non-neoplastic conditions were car-ried out because of a preoperative diagnosis ofmain duct/mixed-IPMN (and 6 patients wereasymptomatic). The contribution of age may bedue to the greater degree of fibrosis foundnormally in older pancreata, which may act as aconfounding factor in the diagnostic workup.

SurgerySeptember 2012
S142 Salvia et al
Finally, the error in diagnosis may be unimpor-tant in somepatients (eg, branch duct-IPMNs foundto be MCNs) but was relevant, for instance, in 6MCNs that proved to be SCNs (3 asymptomatic). Asalready pointed out, because diagnostic overlapexists between these different entities, such errors(in either direction) seems to be unavoidable.
In summary, a critical analysis of 476 patientswho underwent resection for a presumed pancre-atic cystic neoplasm over a 10-year period showedthat the rate of inaccurate preoperative diagnosesin a tertiary care center with a broad experience inpancreatology was of 21.6%. The accuracy in diag-nosing rare entities such as C-NENSs was 50%,giving the same certainty as chance. Some ofmisclassified cysts (20.3%) harbored more con-cerning characteristics than expected and werefound to be ductal adenocarcinoma; other cysticlesions (43.6%) were even non-neoplastic. Despitebeing a retrospective study, these results show thatthe clinical and radiologic diagnosis of pancreaticcystic neoplasms is often inaccurate, and thisaspect is of particular importance, because thecurrent guidelines for the management of muci-nous neoplasms are based on the assumption thatthese lesions can be classified correctly on the basisof imaging features. Prospective studies, technol-ogy advancements and new biochemical and ge-netics techniques are therefore necessary toovercome current diagnostic pitfalls.
REFERENCES
1. Gaujoux S, Brennan MF, Gonen M, D’Angelica MI, DeMat-teo R, Fong Y, et al. Cystic lesions of the pancreas: changesin the presentation and management of 1,424 patients at asingle institution over a 15-year time period. J Am Coll Surg2011;212:590-600.
2. Brugge WR, Lauwers GY, Sahani D, Fernandez-del CastilloC, Warshaw AL. Cystic neoplasms of the pancreas. N EnglJ Med 2004;351:1218-26.
3. Sahani DV, Sainani NI, Blake MA, Crippa S, Mino-Kenud-son M, del-Castillo CF, et al. Prospective evaluation ofreader performance on MDCT in characterization of cysticpancreatic lesions and prediction of cyst biologic aggressive-ness. AJR Am J Roentgenol 2011;197:W53-61.
4. Procacci C, Carbognin G, Accordini S, Biasiutti C, GuariseA, Lombardo F, et al. CT features of malignant mucinouscystic tumors of the pancreas. Eur Radiol 2001;11:1626-30.
5. Correa-Gallego C, Ferrone CR, Thayer SP, Wargo JA, War-shaw AL. Fernandez-Del Castillo C. Incidental pancreaticcysts: do we really know what we are watching? Pancreatol-ogy 2010;10:144-50.
6. Balzano G, Zerbi A, Capretti G, Rocchetti S, Capitanio V, DiCarlo V, et al. Effect of hospital volume on outcome of pan-creaticoduodenectomy in Italy. Br J Surg 2008;95:357-62.
7. Bosman F, Carneiro F, Hruban R, Theise N, editors. WHOClassification of tumors of the digestive system. 4th ed.Lyon, France: IARC Press; 2010.
8. Kosmahl M, Pauser U, Peters K, Sipos B, Luttges J, KremerB, et al. Cystic neoplasms of the pancreas and tumor-like le-sions with cystic features: a review of 418 cases and a classi-fication proposal. Virchows Arch 2004;445:168-78.
9. Tseng JF, Warshaw AL, Sahani DV, Lauwers GY, Rattner DW,Fernandez-del Castillo C, et al. Serous cystadenoma of thepancreas: tumor growth rates and recommendations fortreatment. Ann Surg 2005;242:413-9.
10. Tanaka M, Chari S, Adsay V, Fernandez-del Castillo C, Fal-coni M, Shimizu M, et al. International consensus guide-lines for management of intraductal papillary mucinousneoplasms and mucinous cystic neoplasms of the pancreas.Pancreatology 2006;6:17-32.
11. Salvia R, Crippa S, Falconi M, Bassi C, Guarise A, Scarpa A,et al. Branch-duct intraductal papillary mucinous neo-plasms of the pancreas: to operate or not to operate? Gut2007;56:1086-90.
12. Salvia R, Bassi C, Festa L, Falconi M, Crippa S, Butturini G,et al. Clinical and biological behavior of pancreatic solidpseudopapillary tumors: report on 31 consecutive patients.J Surg Oncol 2007;95:304-10.
13. Boninsegna L, Partelli S, D’Innocenzio MM, Capelli P,Scarpa A, Bassi C, et al. Pancreatic cystic endocrine tumors:a different morphological entity associated with a less ag-gressive behavior. Neuroendocrinology 2010;92:246-51.
14. Salvia R, Crippa S, Partelli S, Malleo G, Marcheggiani G, Bac-chion M, et al. Pancreatic cystic tumours: when to resect,when to observe. EurRevMedPharmacol Sci 2010;14:395-406.
15. Ferrone CR, Correa-Gallego C, Warshaw AL, Brugge WR,Forcione DG, Thayer SP, et al. Current trends in pancreaticcystic neoplasms. Arch Surg 2009;144:448-54.
16. Correa-Gallego C, Warshaw AL, Fernandez-del Castillo C.Fluid CEA in IPMNs: a useful test or the flip of a coin?Am J Gastroenterol 2009;104:796-7.
17. Faccioli N, Crippa S, Bassi C, D’Onofrio M. Contrast-en-hanced ultrasonography of the pancreas. Pancreatology2009;9:560-6.
18. Claudon M, Cosgrove D, Albrecht T, Bolondi L, Bosio M,Calliada F, et al. Guidelines and good clinical practice rec-ommendations for contrast enhanced ultrasound (CEUS)- update 2008. Ultraschall Med 2008;29:28-44.
19. D’Onofrio M, Megibow AJ, Faccioli N, Malago R, Capelli P,Falconi M, et al. Comparison of contrast-enhanced sonogra-phy and MRI in displaying anatomic features of cystic pan-creatic masses. AJR Am J Roentgenol 2007;189:1435-42.
20. Brugge WR. Evaluation of pancreatic cystic lesions withEUS. Gastrointest Endosc 2004;59:698-707.
21. Cizginer S, Turner B, Bilge AR, Karaca C, Pitman MB,Brugge WR, et al. Cyst fluid carcinoembryonic antigen isan accurate diagnostic marker of pancreatic mucinous cysts.Pancreas 2011;40:1024-8.
22. Brugge WR, Lewandrowski K, Lee-Lewandrowski E, Cen-teno BA, Szydlo T, Regan S, et al. Diagnosis of pancreaticcystic neoplasms: a report of the cooperative pancreaticcyst study. Gastroenterology 2004;126:1330-6.
23. Bassi C, Salvia R, Gumbs AA, Butturini G, Falconi M, Peder-zoli P, et al. The value of standard serum tumor markers indifferentiating mucinous from serous cystic tumors of thepancreas: CEA, Ca 19-9, Ca 125, Ca 15-3. LangenbecksArch Surg 2002;387:281-5.
24. Fritz S, Hackert T, Hinz U, Hartwig W, Buchler MW, WernerJ, et al. Role of serum carbohydrate antigen 19-9 and carci-noembryonic antigen in distinguishing between benign andinvasive intraductal papillary mucinous neoplasm of thepancreas. Br J Surg 2011;98:104-10.