Interprosthetic femoral fractures—A challenge of treatment. A systematic review of the literature
7
Interprosthetic femoral fractures—A challenge of treatment. A systematic review of the literature G. Solarino, G. Vicenti *, L. Moretti, A. Abate, A. Spinarelli, B. Moretti Department of Neuroscience and Organs of Sense, Orthopedics Section, Faculty of Medicine and Surgery, University of Bari, Bari, Italy Introduction Total hip arthroplasty (THA) and total knee arthroplasty (TKA) are now common orthopaedic procedures [51]. The simultaneous increase in the number of annual implants and the average age of the population has inevitably led to an increase in the percentage of the population having more than one prosthetic implant. This explains the trends over time in the incidence of THA peripros- thetic fractures, which rose from 0.1–3.2% in 2003 [1] to 0.1–18% in 2011 [2], notwithstanding the use of new generation stems [3], while TKA periprosthetic fractures rose from 0.3% to 5.5% [4]. According to Kenny et al. [5], who described four interprosthetic fractures in 320 patients with ipsilateral hip and knee prosthetics, the incidence of these injuries was around 1.25%, although this number is destined to rise. They occur more frequently in cases of revision surgery [6,7] or severe osteoporosis [5,8]. They are also associated with higher mortality [52] and revision rates; revision rates being more than 50%, in accordance with Zuurmond et al., [9] and higher mortality rates compared with the reference popula- tion, in line with that reported by Bhattacharyya et al. [10]. In addition to the known and discussed general risk factors for the onset of periprosthetic fractures (Table 1, [11,12,53]), similar to interprosthetic fractures, it is important to emphasise the biomechanical aspect of such rare occurrences. In fact, it has been shown how femoral stiffness changes with the implantation of a proximal prosthesis to the point that, in the event of a fall on the respective side, the risk of fracture increases by 30% [13,14]. Also, the implantation of an ipsilateral intramedullary implant deter- mines a high risk of fracture, even with only half the energy needed to cause normal femoral fractures [13]. The increase in ‘‘pluriprosthetised’’ individuals leads to the logical consequence that rare and particular events, including the above-mentioned interprosthetic femoral fractures, may occur. These therefore determine femoral shaft fractures between two ipsilateral implants, both in primary and revision implants. With regards to this, in a biomechanical study carried out on 24 frozen fresh femurs of osteoporotic subjects, Lehmann et al. showed that the presence of two intramedullary implants in the same femur causes an increase of 30% [13] in the risk of fracture. This increase was well-described and documented in the 2003 work of Iesaka et al. [15], carried out on finished models, regarding what effects the size of the interprosthetic gap, stem stability and cortical thickness between two intramedullary and ipsilateral press-fit implants have on ‘‘stress risers’’. Nowadays, various studies have been published on the management of periprosthetic fractures of the hip and knee that Injury, Int. J. Care Injured 45 (2014) 362–368 A R T I C L E I N F O Article history: Accepted 18 September 2013 Keywords: Interprosthetic femur fractures Femur Knee TKA THA A B S T R A C T The success of prosthetic surgery has led to an increase in the percentage of the population having more than one prosthetic implant. This, combined with an increase in the average life expectancy and functional requirements for the elderly, has led to a higher incidence of periprosthetic and interprosthetic fractures. More precisely, the femoral shaft is compressed between two ipsilateral implants with most of these fractures being located on the supracondylar femoral shaft. Their treatment is not only technically demanding and challenging, but can also be associated with serious complications. Treatment must be determined and assessed according to the type of fracture, the stability of the prosthesis, the bone quality and the general condition of the patient. There is little information in the literature about this type of injury: there are several published case reports detailing unconventional solutions and the case studies presented are limited and not significant. This review aims to provide an updated and comprehensive list of diagnostic and therapeutic protocols accepted today, while recognising that these protocols are being continuously updated according to experience gained. ß 2013 Elsevier Ltd. All rights reserved. * Corresponding author at: Department of Neuroscience and Organs of Sense, Orthopaedics Section, University of Bari, Policlinico, Piazza Giulio Cesare 11, 70124 Bari, Italy. E-mail address: [email protected] (G. Vicenti). Contents lists available at ScienceDirect Injury jo ur n al ho m epag e: ww w.els evier .c om /lo cat e/inju r y 0020–1383/$ – see front matter ß 2013 Elsevier Ltd. All rights reserved. http://dx.doi.org/10.1016/j.injury.2013.09.028
Transcript of Interprosthetic femoral fractures—A challenge of treatment. A systematic review of the literature

Injury, Int. J. Care Injured 45 (2014) 362–368
Interprosthetic femoral fractures—A challenge of treatment.A systematic review of the literature
G. Solarino, G. Vicenti *, L. Moretti, A. Abate, A. Spinarelli, B. Moretti
Department of Neuroscience and Organs of Sense, Orthopedics Section, Faculty of Medicine and Surgery, University of Bari, Bari, Italy
A R T I C L E I N F O
Article history:
Accepted 18 September 2013
Keywords:
Interprosthetic femur fractures
Femur
Knee
TKA
THA
A B S T R A C T
The success of prosthetic surgery has led to an increase in the percentage of the population having more
than one prosthetic implant. This, combined with an increase in the average life expectancy and
functional requirements for the elderly, has led to a higher incidence of periprosthetic and
interprosthetic fractures. More precisely, the femoral shaft is compressed between two ipsilateral
implants with most of these fractures being located on the supracondylar femoral shaft. Their treatment
is not only technically demanding and challenging, but can also be associated with serious
complications. Treatment must be determined and assessed according to the type of fracture, the
stability of the prosthesis, the bone quality and the general condition of the patient. There is little
information in the literature about this type of injury: there are several published case reports detailing
unconventional solutions and the case studies presented are limited and not significant. This review
aims to provide an updated and comprehensive list of diagnostic and therapeutic protocols accepted
today, while recognising that these protocols are being continuously updated according to experience
gained.
� 2013 Elsevier Ltd. All rights reserved.
Contents lists available at ScienceDirect
Injury
jo ur n al ho m epag e: ww w.els evier . c om / lo cat e/ in ju r y
Introduction
Total hip arthroplasty (THA) and total knee arthroplasty (TKA)are now common orthopaedic procedures [51]. The simultaneousincrease in the number of annual implants and the average age ofthe population has inevitably led to an increase in the percentageof the population having more than one prosthetic implant. Thisexplains the trends over time in the incidence of THA peripros-thetic fractures, which rose from 0.1–3.2% in 2003 [1] to 0.1–18% in2011 [2], notwithstanding the use of new generation stems [3],while TKA periprosthetic fractures rose from 0.3% to 5.5% [4].According to Kenny et al. [5], who described four interprostheticfractures in 320 patients with ipsilateral hip and knee prosthetics,the incidence of these injuries was around 1.25%, although thisnumber is destined to rise. They occur more frequently in cases ofrevision surgery [6,7] or severe osteoporosis [5,8]. They are alsoassociated with higher mortality [52] and revision rates; revisionrates being more than 50%, in accordance with Zuurmond et al., [9]and higher mortality rates compared with the reference popula-tion, in line with that reported by Bhattacharyya et al. [10].
* Corresponding author at: Department of Neuroscience and Organs of Sense,
Orthopaedics Section, University of Bari, Policlinico, Piazza Giulio Cesare 11, 70124
Bari, Italy.
E-mail address: [email protected] (G. Vicenti).
0020–1383/$ – see front matter � 2013 Elsevier Ltd. All rights reserved.
http://dx.doi.org/10.1016/j.injury.2013.09.028
In addition to the known and discussed general risk factors forthe onset of periprosthetic fractures (Table 1, [11,12,53]), similar tointerprosthetic fractures, it is important to emphasise thebiomechanical aspect of such rare occurrences. In fact, it has beenshown how femoral stiffness changes with the implantation of aproximal prosthesis to the point that, in the event of a fall on therespective side, the risk of fracture increases by 30% [13,14]. Also,the implantation of an ipsilateral intramedullary implant deter-mines a high risk of fracture, even with only half the energy neededto cause normal femoral fractures [13].
The increase in ‘‘pluriprosthetised’’ individuals leads to thelogical consequence that rare and particular events, including theabove-mentioned interprosthetic femoral fractures, may occur.These therefore determine femoral shaft fractures between twoipsilateral implants, both in primary and revision implants. Withregards to this, in a biomechanical study carried out on 24 frozenfresh femurs of osteoporotic subjects, Lehmann et al. showed thatthe presence of two intramedullary implants in the same femurcauses an increase of 30% [13] in the risk of fracture. This increasewas well-described and documented in the 2003 work of Iesakaet al. [15], carried out on finished models, regarding what effectsthe size of the interprosthetic gap, stem stability and corticalthickness between two intramedullary and ipsilateral press-fitimplants have on ‘‘stress risers’’.
Nowadays, various studies have been published on themanagement of periprosthetic fractures of the hip and knee that

Table 1General risk factors for periprosthetic fractures around hip and knee prostheses
(according to [11,12]).
Patient-specific risk factors Osteoporosis
Osteomalacia
Chronic steroid therapy
Rheumatic diseases
Morbus Paget
Osteogenesisimperfecta
Implant-specific risk factors Design of the implant (geometry of the stem)
Loosening of the implant
Infections
Risk factors related to
surgical techniques
Cementless implantation technique
(press–fit fixation)
Osteolysis
Angular malalignment
Removal of implants and cement residues
Notching of the distal femoral anterior cortex
Bone screw fixation of navigation transmitters
Experience of the surgeon
G. Solarino et al. / Injury, Int. J. Care Injured 45 (2014) 362–368 363
indicate different types of treatment: stabilisation with angular-stable plates, non-angular-stable plates, cerclage wires, the use ofallografts and bone morphogenetic protein (BMP) or the revision ofthe prostheses [4,16,17]. Treatment with preconfigured plates hasbeen shown to be biomechanically superior compared with othertypes of treatment, provided there is no loosening of the prostheticcomponents [18–20].
On the other hand, interprosthetic fracture treatment is stillbeing debated because a unanimously recognised algorithm hasnot been defined. Indeed, this has been complicated by numerouselements, including the often advanced age of the patient, thepresence of proximal and distal prosthetic components to thefracture, poor bone quality and quantity for stable fixation,possible endosteal vascular insufficiency due to the necessaryreaming for the first implant, and the presence of cement in thefemoral canal.
Nevertheless, the aim of the treatment is to restore the length,axis and rotation of the fractured femur, heal the fracture whilepreserving the function of the adjacent prostheses and, at the end,ensure sufficiently stable fixation to enable rapid mobilisation andavoid further surgery.
This review aims to provide an updated and comprehensive listof diagnostic and therapeutic protocols accepted today, whilerecognising that these protocols are being continuously updatedaccording to experience gained [21].
Materials and methods – classifications
Fifteen articles were included by the PubMed and EMBASEdatabases: eight case reports [5,20–27], one cohort study [28],three comparative studies [29–31], two retrospective studies[32,33] and finally one multicentred study [34] integrated withfour other scientific works (two literature reviews [21,35] and twobiomechanical studies [13,36]). Our research does not claim todraw guidelines for the treatment of interprosthetic fractures, butrather aims to explore how, over time, they have been classified,diagnosed and treated on the basis of evidence that shows the bestand least satisfactory results, in order to identify possibleprognostic factors to fix in mind when faced with this type ofinjury.
When analysing interprosthetic fractures, an important issue isthat relating to their nosological classification. Up to now therehave been different classifications reported in the literature, oftenresulting from changes to those already known, such as Vancouverand SOFCOT. The former, developed by Duncan and Masri in 1995[37], is a simple classification approach that provides not only the
fracture level, implant stability and bone quality, but also thepossibility of planning a surgical strategy. It consists of three typesof fractures:
� Type A: fractures involving the trochanteric regions, Ag (greatertrochanter) and Al (lesser trochanter), which are generally stable.� Type B: fractures that are localised around the stem or
immediately below it and which, in turn, can be sub-classifiedinto B1, when the stem is stable and the bone stock adequate; B2,when the stem is unstable and the bone stock adequate; and B3when the stem is unstable and the bone stock inadequate.� Type C: fractures that occur distally to the stem, in some cases so
distal as to be considered and treated as conventional diaphysealfractures.
This classification was implemented and modified by Fink et al.in 2005 [27] to include possible interprosthetic fractures:
� Type IA (fracture between a primary hip prosthesis and a primaryknee prosthesis), characterised by the two subtypes IA1 (bothimplants stable) and IA2 (both implants mobilised).� Type IB (fracture located between a revision hip prosthesis and a
revision knee prosthesis) with two subtypes IB1 (both implantsstable) and IB2 (both implants mobilised).
Platzer et al., [33] modified the Vancouver classification,distinguishing interprosthetic fractures into three types, depend-ing on the fracture site and the vicinity of the prosthesis:
� Type I no adjacency.� Type II adjacency to one prosthesis.� Type III adjacency to both prostheses.
In addition, fractures were divided into three subtypes (A–C)depending on the state of stability of both prosthetic components;the B subtype was further divided into B1 (indicating hipcomponent loosening) and B2 (indicating knee componentloosening). The changes as summarised in the original articleare shown in Table 2.
Soenen et al. [34] proposed a modification to the VancouverClassification [37] and to that of the French Orthopaedic andTraumatologic Surgery (SoFCOT) [38], making the criticism thatboth did not take into account the state of the femoral shaftbetween the two prostheses (‘‘femoral pivot length’’), or the type ofknee prosthesis implanted (primary or revision). To extend suchclassifications to differentiate the prognosis and choose the mostappropriate type of treatment, in their study, Soenen et al.introduced D-type fractures, which are interprosthetic fractureslocated between THA with a standard or revision stem and TKAwith a revision stem (Fig. 1). Finally, important examples ofcombined classifications that describe interprosthetic fracturesusing two or more classifications are those used by Hou et al., [29](which have combined classifications of Vancouver [37] and Su[39]) and Mamczak et al. [32] (Vancouver [37] and Rorabeck [4]classifications).
Results and discussion
Our revision of the literature identified 124 cases of inter-prosthetic fractures described by 15 authors [5,20,22–34], seeTable 3.
Dave et al., [22] were the first to describe a single case ofinterprosthetic fracture in a 75-year-old patient with rheumatoidarthritis (RA) treated with a Mennen plate, three interfragmentaryscrews and a bone graft. The patient was mobile 48 h after the

Table 2Modified Vancouver classification for interprosthetic femoral fractures (according to [28]).
Classification Fracture adjacency to the prostheses
Type I (no adjacency) Type II (no adjacency to one prosthesis) Type III (no adjacency to both prosthesis)
Stability of the prostheses
Sub-type A (both stable) U U U
Sub-type B (one Stable, one loose)
B1 (loose hip component) � U U
B2 (loose knee component) � U U
Sub-type C (both loose) � � U
G. Solarino et al. / Injury, Int. J. Care Injured 45 (2014) 362–368364
operation with the use of a cane, early weight-bearing after 6weeks and fully weight-bearing after the twelfth week. Thistreatment led to clinical and radiographic fracture healing at sixthmonths post-surgery. Walker et al. [23] reported a single case ofinterprosthetic fracture in a patient with loosening of bothprosthetic implants; treatment with a Mennen plate led to earlyfailure inducing the authors to carry out a revision of both implantswith good final results. Kenny et al. [5] analysed four RA patients,aged between 73 and 86 years, who had a primary THA prosthesis,three with a revision TKA and one with a surface TKA, with Rx-graphical evidence of areas of multiple osteolyses. For the internalfixation, a Mennen plate, two plates and an AO-DCP DCS were used,but all fixation methods were insufficient and required revision. Intwo of the four patients, amputation was necessary due to the totalfailure of the treatment. These results indicate that rigid internalfixation in this type of fracture produces poor results because of thesignificant damage caused to soft tissues and the periosteal bloodsupply. Furthermore, the endosteal vessels are already compro-mised as a result of the previous boring during the implantation ofthe primary prosthesis.
The Mennen plate guarantees minimum local damage, butprovides poor fixation stability, which is why it was eventuallyabandoned. The AO-DCP plates used by the authors working incompression require precise configuration and close contact withthe bone that cause further damage to the periosteal vessels.
Urch et al. [24] described the case of an interprosthetic fracturein a patient who had already undergone three THR procedures,managed with DCS plates and ORIF technique, which subsequentlyled to a non-union of the fracture. The fracture was later subjectedto an allograft and simultaneous revision of both implants. DellaValle et al. [26] reported results concerning the use of the DCS platewith MIPO technique in a 66-year-old patient suffering from RAwith uncemented TKA-PS and cemented THA without signs ofloosening, affected by a comminuted diaphyseal fracture as a resultof an accidental fall in a domestic environment. The final successwas favoured by minimal damage to the periosteal blood supply,from stable fixation and subsequent early mobility (5 months).Despite accurate preoperative planning, implantation of the DCS
Fig. 1. Proposed type D (according to [29]).
plate, equipped with linear conformation, led to the medialisationof the distal femoral fragment: this causes excessive stress on theperiprosthetic ligamentous structures of the outer compartmentand potential loosening of the TKA.
Chakravarthy et al. [25] described a patient affected with anunclassified interprosthetic fracture treated with a lockingcompression plate (LCP) and ORIF technique. After healing, thisdeveloped into a stress fracture between the plate and the femoralcomponent of the knee and required fixation with a retrogradeintramedullary nail. The nailing, bypassing the fracture sitewithout affecting the intramedullary blood supply, was abiomechanically advantageous solution in this type of fracture.Duwelius et al. [30], in a similar scenario, also emphasised theimportance of preoperative planning. Fulkerson et al. [20]documented the treatment of three patients suffering frominterprosthetic fractures with ORIF LISS1 (Less Invasive Stabilisa-tion System, Synthes) plates, two of which healed, while the thirdrequired revision to the primary knee prosthesis due to the implantloosening.
Sah et al. [28] conducted a retrospective study of 22 patients(average age 75 years) who underwent surgery between 2002 and2006 for interprosthetic fractures in both stable (6 Vancouver B1,16 Vancouver C/Rorabeck II) prosthetic implants (6 cemented THA,16 uncemented THA, 6 THR with stem; all TKAs were primaryprostheses, 18 TKA-PS). All the patients were treated with a singleLCP with locked screws using MIPO technique without the use ofallograft. In only seven cases cerclage wires were added in theproximal area, all fractures healed in 14 weeks and, at the final 18-month follow-up, a clinical picture similar to the one preopera-tively was noted. Platzer et al., [33] also performed a retrospectivestudy (1992–2008) of 23 patients (15 women and 8 men, averageage 79.2 years), suffering from interprosthetic fractures classifiedaccording to the modified Vancouver Classification (as described inTable 1). The MIPO technique with LCP was used in 19 patients, twounderwent revision surgery with a long stem and two underwent arevision with a simultaneous LCP implant. Fastening screws wereused in 14 of the 19 patients treated with an LCP; in theremaining five patients cerclage wires were also used. Cerclagewires were also used in the two patients who underwent revisionsurgery and concomitant LCP implantation. Sixteen patientsrecovered all clinical functions, 19 patients (82%) were regardedas healed radiographically in 6 months, and four patientsexperienced a failure for a bad fracture reduction and fixation.Mamczak et al. [32] retrospectively studied 20 patients withinterprosthetic fractures treated with an LCP using the MIPOtechnique without the use of allograft, classified as Vancouver B1and Rorabeck II, with supracondylar fractures prevailing overthose of the diaphyseal area (2:1). Three defects of consolidation,loosening of a prosthetic stem and a superficial infection werenoted, while all the remaining patients were healed clinicallyand radiographically.
In a retrospective analysis, Hou et al. [29] assessed 13interprosthetic fractures classified separately according to theVancouver classification, introducing the concept of combined

Table 3Interprosthetic fractures in the literature.
Year Author P Age F-UP Treatment P Fracture healing Complications
Percentage Time in
months
2012 Soenen et al. [34] 14 72 (48–89) MIOS/LCP 5 42.85% 28.57% non-union, 7.14%
slowed fixation, 7.14%
refracture 7.14%
2011 Hou et al. [29] 13 81 (61–94) 28 MIOS/LCP 9 100% 4.7 22% lost in follow-up
TJRA 4
2011 Platzer et al. [33] 23 79 (59–89) 12 MIOS/LCP 19 82% <6 11% delayed union,
5% non-union, 100% i
nfection of the injury
TJRA 2
LCP/TJRA 2
2010 Michla et al. [31] 8 78 (53–92) 3–13 LISS 1 100% 3
Nail/conv. plate/DCS 5 100% 4
TJRA 2
2010 Mamczak et al. [32] 20 80 (56–98) 12 MIOS/LCP 20 100% 3.3 15% malunion,
5% stem loss THA
2010 Sah et al. [28] 22 17.7 MIOS/LCP 22 100% 3.5
2007 Fulkerson et al. [20] 3 77 (71–86) 12 ORIF LISS plate 2 66% 6.5 33% Non-union
2007 Chakravarthy
et al. [25]
1 75 12 LCP Fracture
2005 Fink et al. [27] 11 ORIF/conv. plate 10 100%
ORIF/plate + cerclage 1
2004 Duwelius et al. [30] 3 Single plate
2003 Della Valle et al. [26] 1 66 12 Percutaneus submuscular
12 hole 95 deg dynamic
screw
1 100%
1999 Walker et al. [23] 1 61 15 Mennen plate 0 0 Plate failure
1998 Urch et al. [24] 1 62 24 Entire femoral
allograft + revision
1998 Kenny et al. [5] 4 81 (73–86) ORIF/conv. plate 0% 100% plate failure
DCP/Mennen plate
1995 Dave et al. [22] 1 75 Mennen plate + bone
graft + 3 cortical screws
0 0 Screw broken
G. Solarino et al. / Injury, Int. J. Care Injured 45 (2014) 362–368 365
classifications in which interprosthetic fractures can be included inseveral classifications simultaneously (e.g. Vancouver Type C andType 1 SOFCOT). In four cases, a clear loosening of the prostheticcomponent was evident, making it necessary to replace theimplant with a revision stem implant. In the remaining nine cases,in the absence of any sign of prosthetic loosening, fixation wasconducted with an LCP and unicortical bi-locked screws with orwithout the addition of cerclage wires: all patients wereconsidered to be healed clinically and radiographically in anaverage of 4.7 months.
All these studies have demonstrated how the use of LCPs,minimally damaging to periosteal soft tissue, generate evidentadvantages in the treatment of these complicated injuries. Inaddition, Mamczak’s study [32] shows twice the incidence ofsupracondylar fractures compared with those of the diaphysealarea since the stressors are more concentrated at the stem apex ofthe TKA femoral component. Michla et al., [31] described, in detail,the treatment of eight interprosthetic fractures, six supracondylarfractures and two diaphyseal fractures, through different methods:one with revision and a Dall-Miles plate and strut graft, one with arevision and Dall-Miles cables, three with a retrograde femoralnail, one with a LISS lateral plate, one with the Dall-Miles systemand the last with a DCS plate. All fractures were considered to beclinically and radiographically healed within 6 months.
Finally, Soenen et al. [34] recently analysed 14 cases ofinterprosthetic fractures, introducing Type D into the Vancouverclassification and SOFCOT. Type D includes localised injuriesbetween standard stem or revision THA and revision stem TKA.They also report the results of their study: the first seven patients,who showed no signs of loosening or prosthetic wear, achievedsatisfactory clinical and radiographic results at 3 months, with noneed for revision surgery after treatment with a LISS plate (sixcases) and retrograde nail without the use of a graft (one case),with full weight-bearing allowed at 8 weeks. In contrast, theremaining seven patients (six revision TKA with type D classifiedfractures and two revision THA) presented an adverse trend due tomechanical failure of the treatment, in five cases represented byLISS plate fixation (in one case TKA revision surgery wasperformed), in one by retrograde nail fixation, in one withstabilisation using cerclage wires and in one case using a graft.Six of the seven patients were subjected to secondary surgery:three for TFR (Total Femoral Replacement), three for revision withplate; and one subject died. The failure of the intramedullary nail,documented by Soenen, is due to a zone of ‘‘stress risers’’, locatedbetween the apex of the stem of the femoral component and that ofthe nail.
These works show that there is no algorithm of predeterminedtreatment for these fractures, only personalised solutions.

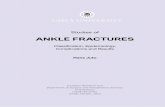
Fig. 3. Interprosthetic fracture treated at our institution with LCP. Note: segment B is
twice the size of segment A (diameter of the diaphysis) indicating an excellent
overlap of the plate proximally and distally to the injury as suggested by Soenen
et al. [25].
G. Solarino et al. / Injury, Int. J. Care Injured 45 (2014) 362–368366
Conclusions
The increase in the number of people with prostheses and inindividual functional requests along with an increase in lifeexpectancy has led to a higher incidence of interprostheticfractures, which are complicated to classify and treat. Treatmentoptions include the stabilisation of fractures using flat orpreconfigured plates, cerclage wires, autologous grafts or withBMP and revision with stemmed prosthesis [21]. However, to date,a suitable and widely accepted algorithm has not yet beenoutlined. The two interesting biomechanical studies of Lehmannet al. [13] and Iesaka [15] highlight how the presence of twointramedullary components in the femoral shaft reduces fractureresistance by 30%: this zone of ‘‘stress risers’’ is not so much relatedto the size of the interprosthetic gap as to the stability of the stem,whose loosening increases the local concentration of stress withincreased risk of fracture [40]. It is also related to cortical bonethickness, which has an important effect on the distribution ofstress: the lower the thickness, the higher is the concentration ofstress. In this context, the retrograde intramedullary nail is, inprinciple, the best treatment ‘‘biologically’’ for the fixation offractures with stable interprosthetic implants in order to bypassand stabilise the fracture site [33], as documented by Chakravarthyet al. [25]. Unfortunately, it is mechanically unfavourable becauseit creates a ‘‘stress riser’’ zone at the stem tip and there is a furtherarea of weakness corresponding to the fixation screws; this canlead to possible failures, as documented in the study of Soenenet al., [34] and empirically demonstrated in the recent biomechan-ical study of Lehmann et al., [36].
In their recent study [21], Ochs et al. present a treatmentalgorithm, based on the modified classification of Platzer et al.,[33], that describes the different therapeutic choices in thepresence of interprosthetic femoral fractures (Fig. 2) andemphasises the ‘use of the LISS plate1 and NCB-Plate1 (Non-Contact Bridging Plate, Zimmer), which allow a minimally invasivetechnique that respects soft tissues. Also discussed is the possibleuse of a ‘‘Locking attachment Plate1’’ (Synthes) that increases LISSplate stability, the further possibility of using unicortical screwsnear the stem prosthesis and, finally, the use of poly-axial screws(maximum angle 308) with the NCB-plate using a particularthreaded ‘‘cup’’ to screw on the previously placed screws.
These plates of suitable length and with a sufficient number ofscrews and cerclage wires, implanted with the MIPO technique,represent a solution that is more satisfying mechanically and
Fig. 2. Treatment strategies for interprosthetic femoral fractures (according to [21]).
biologically [41] because they promote fracture healing andprevent the onset of any refractures [33]. In particular, thepreconfigured LCP/LISS plates, long enough to allow the fixation ofat least two bicortical screws proximal to the end of the femoralstem of the hip prosthesis, generally ensure favourable results [26],bypassing the fracture site by more than twice the corticaldiameter [34] (Fig. 3), although this does not appear to have beenvalidated in any biomechanical study [35]. The hypotheticaladvantage of bypassing the entire interprosthetic area with a plateis that it would effectively eliminate any remaining femoral ‘‘stressriser’’ zone [32].
Another important point is that plate fixation, particularly atthe proximal extremity, should be conducted with a minimum ofsix, or preferably eight, cortical screws and the use of cerclagewires, if needed [28]. The latter serve to increase the stability of thescrews in the site proximal to the stem prosthesis given their lowerefficiency compared with the screws used for lateral plate fixation[42]. A minimally invasive instrument should be used and thecerclage wires should not be in contact with the bone to avoidcompromising the periosteal blood supply [43].
Bone grafts improve consolidation and reduce refracture risk byincreasing cortical thickness and supporting greater fixation [44–47]. Graft positioning requires an extensive exposition of thefemoral shaft, thereby precluding the use of a surgical techniquethat is as respectful as possible of the soft tissues [28], andincreasing the chances of revision surgery and implantation of atotal femoral prosthesis. A bone graft should be used only in casesof severe bone loss, preferably an autologous bone graft instead ofBMP, due to insufficient documented long-term evidence in theliterature [48].
McLean et al. [49] have reported good results in 20 patientswith a prosthetic femur replacement (15 proximal and five totalreplacements) as a possible treatment option for patients withperiprosthetic fractures and important bone loss; notably, inextreme cases, amputation may be necessary. Unfortunately, thisdifficult choice of treatment is indicated in patients with aninterprosthetic femoral fracture, who have undergone a TKR andhave a chronic periprosthetic infection or in cases with inter-prosthetic fractures that present a loosening of the revision kneeprosthesis [21].

G. Solarino et al. / Injury, Int. J. Care Injured 45 (2014) 362–368 367
Ultimately, interprosthetic fractures are a demanding chal-lenge for orthopaedic surgeons; the type of treatment to be usedvaries from case to case and should be adapted and personalisedas much as possible [21,31,34]. The use of LCPs, which exceed therespective prosthetic stems by at least 2 times the diameter ofthe femoral shaft, seems to ensure better medium-term results[50], with success rates of at least 85% [28,29,31–34], althoughthere are some exceptional cases of amputation, as describedabove.
In addition, fixation with LCPs to help prevent possiblerefracture should be used in special cases, such as patients atrisk of falls or with ‘‘stress riser’’ areas within the femoral shaftbecause of the presence of an intramedullary ipsilateral hip andknee implant. For this purpose, the use of an LCP that bypasses theentire interprosthetic area seems to be an excellent precautionaryexpedient [32].
Finally, we emphasise the extreme importance of executingprimary implant prosthetic surgery accurately and as respectfullyas possible of the surrounding soft tissues, with minimum reamingof the femoral canal and maximum safeguarding of the peripros-thetic bone. This prevents and simplifies possible revision surgeryin the presence of a periprosthetic fracture, and lays thefoundations for a more affordable surgical outcome.
Conflict of interest
The authors did not receive grants or outside funding in supportof their research or preparation of this manuscript. They did notreceive payments or other benefits or a commitment or agreementto provide such benefits from a commercial entity. No commercialentity paid or directed, or agreed to pay or direct, any benefits toany research fund, foundation, educational institution, or othercharitable or nonprofit organization with which the authors areaffiliated or associated.
References
[1] Springer BD, Berry DJ, Lewallen DG. Treatment of periprosthetic femoralfractures following total hip arthroplasty with femoral component revision.J Bone Joint Surg Am 2003;85-A:2156–62.
[2] Della Rocca GJ, Leung KS, Pape H-C. Periprosthetic fractures: epidemiology andfuture projections. J Orthop Trauma 2011;25(Suppl. 2):S66–70.
[3] Bhandari M, Schemitsch E, Jonsson A, Zlowodzki M, Haidukewych GJ. Gammanails revisited: gamma nails versus compression hip screws in the manage-ment of intertrochanteric fractures of the hip: a meta-analysis. J OrthopTrauma 2009;23:460–4.
[4] Rorabeck CH, Taylor JW. Classification of periprosthetic fractures complicatingtotal knee arthroplasty. Orthop Clin North Am 1999;30:209–14.
[5] Kenny P, Rice J, Quinlan W. Interprosthetic fracture of the femoral shaft. JArthroplasty 1998;13:361–4.
[6] Abendschein W. Periprosthetic femur fractures—a growing epidemic. Am JOrthop 2003;32:34–6.
[7] Tsiridis E, Haddad FS, Gie GA. The management of periprosthetic femoralfractures around hip replacements. Injury 2003;34:95–105.
[8] Franklin J, Malchau H. Risk factors for periprosthetic femoral fracture. Injury2007;38:655–60.
[9] Zuurmond RG, Pilot P, Verburg AD. Retrograde bridging nailing of peripros-thetic femoral fractures. Injury 2007;38:958–64.
[10] Bhattacharyya T, Chang D, Meigs JB, Estok DM, Malchau H. Mortalityafter periprosthetic fracture of the femur. J Bone Joint Surg Am 2007;89:2658–62.
[11] Erhardt JB, Grob K, Roderer G, Hoffmann A, Forster TN, Kuster MS. Treatment ofperiprosthetic femur fractures with the non-contact bridging plate: a newangular stable implant. Arch Orthop Trauma Surg 2008;128:409–16.
[12] Berry DJ. Epidemiology: hip and knee. Orthopedic Clin North Am1999;30:183–90.
[13] Lehmann W, Rupprecht M, Hellmers N, Sellenschloh K, Briem D, Puschel K,et al. Biomechanical evaluation of peri- and interprosthetic fractures of thefemur. J Trauma 2010;68:1459–63.
[14] Rupprecht M, Sellenschloh K, Grossterlinden L, Puschel K, Morlock M, AmlingM, et al. Biomechanical evaluation for mechanisms of periprosthetic femoralfractures. J Trauma 2011;70:E62–6.
[15] Iesaka K, Kummer FJ, Di Cesare PE. Stress risers between two ipsilateralintramedullary stems. J Arthroplasty 2005;20:386–91.
[16] Pavlou G, Pantaliadis P, Macdonald D, Timperley JA, Gie G, Bancroft G, et al. Areview of 202 periprosthetic fractures—stem revision and allograft improvesoutcome for type B fractures. Hip Int 2011;21:21–9.
[17] Rayan F, Konan S, Haddad FS. Uncemented revision hip arthroplasty in B2 andB3 periprosthetic femoral fractures—a prospective analysis. Hip Int 2010;20:38–42.
[18] Dennis MG, Simon JA, Kummer FJ, Koval KJ, DiCesare PE. Fixation of peripros-thetic femoral shaft fractures occurring at the tip of the stem: a biomechanicalstudy of 5 techniques. J Aarthroplasty 2000;15:523–8.
[19] Dennis MG, Simon JA, Kummer FJ, Koval KJ, Di Cesare PE. Fixation of peripros-thetic femoral shaft fractures: a biomechanical comparison of two techniques.J Orthop Trauma 2001;15:177–80.
[20] Fulkerson E, Tejwani N, Stuchin S, Egol K. Management of periprosthetic femurfractures with a first generation locking plate. Injury 2007;38:965–72.
[21] Ochs B, Stockle U, Gebhard F. Interprosthetic fractures—a challenge of treat-ment. Eur Orthop Traumatol 2012;4:1–7.
[22] Dave DJ, Koka SR, James SE. Mennen plate fixation for fracture of the femoralshaft with ipsilateral total hip and knee arthroplasties. J Arthroplasty 1995;10:113–5.
[23] Walker PS, Yoon WW, Cannon SR, Bentley G, Muirhead-Allwood SK. Designand application of combined hip–knee intramedullary joint replacements. JArthroplasty 1999;14:945–51.
[24] Urch SE, Moskal JT. Simultaneous ipsilateral revision total hip arthroplasty andrevision total knee arthroplasty with entire femoral allograft. J Arthroplasty1998;13:833–6.
[25] Chakravarthy J, Bansal R, Cooper J. Locking plate osteosynthesis for VancouverType B1 and Type C periprosthetic fractures of femur: a report on 12 patients.Injury 2007;38:725–33.
[26] Della Valle CJ, Tejwani N, Koval KJ. Interprosthetic fracture of the femoral shafttreated with a percutaneously inserted dynamic condylar screw: case report. JTrauma 2003;54:602–5.
[27] Fink B, Fuerst M, Singer J. Periprosthetic fractures of the femur associated withhip arthroplasty. Arch Orthop Trauma Surg 2005;125:433–42.
[28] Sah AP, Marshall A, Virkus WV, Estok DM, Della Valle CJ. Interprostheticfractures of the femur: treatment with a single-locked plate. J Arthroplasty2010;25:280–6.
[29] Hou Z, Moore B, Bowen TR, Irgit K, Matzo ME, Strohecker KA, et al. Treatment ofinterprosthetic fractures of the femur. J Trauma 2011;71:1715–9.
[30] Duwelius PJ, Schmidt AH, Kyle RF, Talbott V, Ellis TJ, Butler JB. A prospective,modernized treatment protocol for periprosthetic femur fractures. Orthop ClinNorth Am 2004;35:485–92.
[31] Michla Y, Spalding L, Holland JP, Deehan DJ. The complex problem of theinterprosthetic femoral fracture in the elderly patient. Acta Orthop Belg2010;76:636–43.
[32] Mamczak CN, Gardner MJ, Bolhofner B, Borrelli Jr J, Streubel PN, Ricci WM.Interprosthetic femoral fractures. J Orthop Trauma 2010;24:740–4.
[33] Platzer P, Schuster R, Luxl M, Widhalm HK, Eipeldauer S, Krusch-Mandl I, et al.Management and outcome of interprosthetic femoral fractures. Injury2011;42:1219–25.
[34] Soenen M, Migaud H, Bonnomet F, Girard J, Mathevon H, Ehlinger M. Inter-prosthetic femoral fractures: analysis of 14 cases. Proposal for an additionalgrade in the Vancouver and SoFCOT classifications. Orthop Traumatol Surg Res2011;97:693–8.
[35] Lehmann W, Rupprecht A, Rucker A, Hoffmann M, Morlock M, Puschel K, et al.Interprothetische Frakturen am Femur. Trauma und Berufskrankheit2012;14:190–5 [German].
[36] Lehmann W, Rupprecht M, Nuechtern J, Melzner D, Sellenschloh K, Kolb J, et al.What is the risk of stress risers for interprosthetic fractures of the femur? Abiomechanical analysis. Int Orthop 2012;36:2441–6.
[37] Duncan CP, Masri BA. Fractures of the femur after hip replacement. InstrCourse Lect 1995;44:293–304.
[38] Tricoire J-L, Vogt F, Laffosse JM. Periprosthetic fractures around total hip andknee arthroplasty. Radiographic evaluation in periprosthetic fractures aroundthe knee. Rev Chir Orthop Reparatrice Appar Mot 2006;92:2S57–60S.
[39] Su ET, DeWal H, Di Cesare PE. Periprosthetic femoral fractures above total kneereplacements. J Am Acad Orthop Surg 2004;12:12–20.
[40] Harris B, Owen JR, Wayne JS, Jiranek WA. Does femoral component looseningpredispose to femoral fracture? An in vitro comparison of cemented hips. ClinOrthop Relat Res 2010;468:497–503.
[41] Ricci WM, Loftus T, Cox C, Borrelli J. Locked plates combined with minimallyinvasive insertion technique for the treatment of periprosthetic supracondylarfemur fractures above a total knee arthroplasty. J Orthop Trauma 2006;20:190–6.
[42] Lever JP, Zdero R, Nousiainen MT, Waddell JP, Schemitsch EH. The bio-mechanical analysis of three plating fixation systems for periprostheticfemoral fracture near the tip of a total hip arthroplasty. J Orthop Surg Res2010;5:45.
[43] Perren SM, Fernandez Dell’Oca A, Lenz M, Windolf M. Cerclage, evolution andpotential of a Cinderella technology. An overview with reference to peripros-thetic fractures. Acta Chir Orthop Traumatol Cech 2011;78:190–9.
[44] Chandler HP, Tigges RG. The role of allografts in the treatment of periprostheticfemoral fractures. Instr Course Lect 1998;47:257–64.
[45] Haddad FS, Duncan CP, Berry DJ, Lewallen DG, Gross AE, Chandler HP.Periprosthetic femoral fractures around well-fixed implants: use of corticalonlay allografts with or without a plate. J Bone Joint Surg Am 2002;84-A:945–50.

G. Solarino et al. / Injury, Int. J. Care Injured 45 (2014) 362–368368
[46] Masri BA, Meek RM, Duncan CP. Periprosthetic fractures evaluation andtreatment. Clin Orthop Rel Res 2004;420:80–95.
[47] Nauth A, Miclau T, Bhandari M, Schemitsch EH. Use of osteobiologics in themanagement of osteoporotic fractures. J Orthop Trauma 2011;25(Suppl.2):S51–5.
[48] Razzouk S, Sarkis R. BMP-2: biological challenges to its clinical use. N Y StateDent J 2012;78:37–9.
[49] McLean AL, Patton JT, Moran M. Femoral replacement for salvage of peripros-thetic fracture around a total hip replacement. Injury 2012;43:1166–9.
[50] Larson JE, Chao EY, Fitzgerald RH. Bypassing femoral cortical defects withcemented intramedullary stems. J Orthop Res 1991;9:414–21.
[51] Hoffmann MF, Jones CB, Sietsema DL, Koenig SJ, Tornetta 3rd P. Outcome ofperiprosthetic distal femoral fractures following knee arthroplasty. Injury2012;43(July (7)):1084–9.
[52] Mitra B, Cameron PA. Optimising management of the elderly trauma patient.Injury 2012;43(July (7)):973–5.
[53] Phillips JR, Moran CG, Manktelow AR. Periprosthetic fractures around hiphemiarthroplasty performed for hip fracture. Injury 2013;44(June (6)):757–62.