
ANKLE FRACTURES - DiVA Portal
106
Studies of ANKLE FRACTURES Classification, Epidemiology, Complications and Results Hans Juto Sunderby Research Unit Department of Surgical and Perioperative Sciences Orthopaedics Umeå University Umeå, Sweden, 2022
-
Upload
khangminh22 -
Category
Documents
-
view
4 -
download
0
Transcript of ANKLE FRACTURES - DiVA Portal

Studies of
ANKLE FRACTURES
Classification, Epidemiology, Complications and Results
Hans Juto
Sunderby Research UnitDepartment of Surgical and Perioperative Sciences
OrthopaedicsUmeå University
Umeå, Sweden, 2022

This work is protected by the Swedish Copyright Legislation (Act 1960:729)Dissertation for a PhD
Studies of Ankle Fractures - Classification, Epidemiology, Complications and Results
ISBN: 978-91-7855-711-0 (print)ISBN: 978-91-7855-712-7 (pdf)
ISSN: 0346-6612New Series Number: 2166
Electronic version available at: http://umu.diva-portal.org
Layout and design by: Hans JutoIllustrations by: Pontus Andersson/Pontus Art Production and Isabelle Forslin
Printed by: Luleå Grafiska, Luleå, Sweden 2022
“One of the first things taught in introductory statistics textbooks is that correlation is not causation. It is also one of the first things forgotten.”
Thomas Sowell
To my family
TABLE OF CONTENTS
Abstract ............................................................................................6
Populärvetenskaplig sammanfattning ..........................................8
List of papers ................................................................................ 12
Additional papers by the author ................................................. 13
Abbreviations ................................................................................ 14
Definitions ...................................................................................... 15
1. Introduction ............................................................................... 17
1.1 The Swedish Fracture Register 17
1.2 Anatomy of the ankle joint 20
1.3 Definition and classification 25
1.4 Epidemiology 32
1.5 Complications 34
1.6 Outcome after ankle fractures 40
2. Aims of the studies .................................................................. 45
3. Methods ..................................................................................... 47
3.1 Study design 47
3.2 Data source and study subjects 47
3.3 Variables and outcome 50
3.4 Classification of fractures 53
3.5 Completeness and coverage 54
3.6 Statistics 54
3.7 Ethics 57

5Studies of ankle fractures
4. Results ....................................................................................... 59
4.1 Study I 59
4.2 Study II 60
4.3 Study III 64
4.4 Study IV 68
5. Discussion ................................................................................. 73
5.1 Accuracy of classification in the Swedish Fracture Register 73
5.2 Classifying ankle fractures 74
5.3 Epidemiology 76
5.4 Osteoporosis and the ankle fracture 77
5.5 Venous thromboembolism as a complication following an ankle fracture 78
5.6 Outcome and sick leave after ankle fractures 80
5.7 Strengths and limitations 82
6. Conclusions .............................................................................. 85
7. Future perspectives ................................................................. 87
8. Acknowledgements ................................................................. 91
9. References ................................................................................ 93
Papers .......................................................................................... 107

6
Hans JutoStudies of ankle fractures
ABSTRACT
The ankle fracture is one of the most common fractures in adult patients and is a hetero-geneous group of fractures. From the fully stable fracture on the most distal part of the fibula to severely unstable and even dislocated ankles. Patients with ankle fractures often report a good result after treatment, but a small group have persistent problems. The purpose of the dissertation is to investigate classification, epidemiology, complica-tions, and results in order to improve knowledge and management of ankle fractures. This dissertation is mainly based on data from the Swedish Fracture Register (SFR).
In Study I the accuracy of the AO/OTA classification, version 2007, of ankle fractures in the SFR was examined. Entry of data into the SFR is mainly performed by the attending doctors at the accident and emergency departments, often with varying experience of fracture classification. Classification of fractures can in some cases be difficult even for experienced orthopaedic surgeons. This is because the fractures to be categorized can be seen being on a spectrum and there will always be cases which is on the border between different categories. We created a reference group that classified several randomly selected ankle fractures from the SFR based on X-rays from treating orthopedic departments. The assessment that was then agreed upon was considered to be the gold standard classification and could in turn be compared to the classification found in the SFR. The agreement between the classification in the SFR and the classi-fication of the reference group was 88% for AO/OTA type level and 74% for AO/OTA group level. This corresponded to a kappa value of 0.77 and 0.66 respectively. The findings were equivalent to or higher than in previous studies.
In study II the aim was to examine the incidence of ankle fractures in Norrbotten county, as well as the relationship between AO/OTA-classes of ankle fractures with age, gender and low-energy trauma. Ankle fractures are increasing in an ageing po-pulation but are not generally seen as a fragility fracture. All ankle fractures treated at a hospital in the county were retrospectively identified, X-rays were inspected and classified, and the medical record reviewed. The study found 1,756 ankle fractures corresponding to an incidence of 179 per 100,000 person-years. Females had an increa-sing incidence with age while among males the incidence was more evenly distributed.

7Studies of ankle fractures
The type B fractures showed a slightly higher proportion of low-energy trauma and increased substantially with age. In contrast were the A21-subgroup and type C ankle fractures which had a lower mean age and proportion of women.
Study III investigated the association between the incidence of venous throm-boembolic event (VTE) and the use of low-molecular-weight heparin (LMWH) prop-hylaxis following an ankle fracture, as well as factors affecting the risk of VTE. VTE is a well-known complication after ankle fracture and especially after ankle fracture surgery. The use of LMWH prophylaxis is debated. Data on ankle fracture treatment from the Swedish Fracture Register was linked to data for VTE diagnosis and LMWH prescription from the Swedish National Patient Register and the Swedish Prescribed Drug Register. Cases of diagnosed VTE were identified among 222 of 14,954 ankle fractures. Orthopaedic departments with higher-than-average use of LMWH prophy-laxis among non-operatively treated ankle fractures had a lower incidence of VTE (OR 0.60, 95% CI, 0.39-0.92). Among patients treated operatively at departments with guidelines for routine use of LMWH prophylaxis there was an incidence of VTE of 1.6%, compared to 2,7% at departments without routine use of LMWH prophylaxis (OR 0.56, 95% CI, 0.37-0.86). During the first two weeks following injury, there was only one case of VTE in 5,332 patients with prescribed LMWH, compared to 39 cases of VTE among 9,622 patients without prescription.
Study IV examined the variations in the length of sick leave in ankle fracture pa-tients. Even though most patients with an ankle fracture report a satisfactory outcome there are still a number of patients with persistent pain and functional impairment. The aim of the study was to analyse how treatment, different types of ankle fracture and patients-related factors were associated with the length of sick leave by combining data from the SFR and Swedish Social Insurance Agency (SSIA). Fifty-three per cent of patients registered with an ankle fracture in the SFR had a period of paid sick leave from the SSIA. There was an association between the length of the sick leave and the severity of the fracture. A correlation was also seen between the length of the sick leave and a worse patient-reported outcome.

8
Hans JutoStudies of ankle fractures
POPULÄRVETENSKAPLIG SAMMANFATTNING
Fotledsfraktur är en av de vanligaste frakturerna hos vuxna patienter och utgör ungefär en tiondel av alla frakturer. Den är likt många andra frakturtyper påtagligt mångskif-tande i sin karaktär. Det innebär också att behandlingen och resultatet varierar efter frakturen. Den varierar från helt stabila frakturer på nedre delen av yttre fotknölen till kraftigt instabila och ibland påtagligt felställda fotleder. Ungefär hälften av alla fotleds-frakturer behandlas icke-operativt och då ofta med immobilisering i gips under en tid. Den andra hälften behandlas operativt, många gånger med fixering av frakturen med en platta och skruvar. Patienter med fotledsfrakturer rapporterar ofta ett bra resultat efter behandling men en mindre grupp har stora kvarstående besvär.
Syftet med den här avhandlingen är att med studier av klassificering, epidemio-logi, komplikationer och utfall efter fotledsfrakturer förbättra kunskap och omhänder-tagande av frakturen. Avhandlingen bygger i huvudsak på data från Svenska Fraktur-registret (SFR) och består av fyra olika studier.
SFR är ett helt webbaserat kvalitetsregister som startades 2011 vid Sahlgrenska Universitetssjukhuset i Göteborg. Under första året inkluderades endast överarms- och underbensfrakturer men från 2012 kan alla ortopediska frakturer registreras. Idag är samtliga ortopediska kliniker i Sverige anslutna. Täckningsgraden var 2018 i snitt ca 70% bland de anslutna klinikerna. Registreringen av frakturer är uppdelad i tre delar. Man registrerar data, med hjälp av hierarkiskt ordnade rullgardinsmenyer, om skadan, frakturen och behandlingen. I ett första steg registreras skademekanismen och i ett andra, den uppkomna frakturen. För att behandla en fraktur korrekt behöver den kunna beskrivas och klassificeras. Det finns ett flertal olika klassificeringssystem för fraktu-rer. I SFR används ett system beskrivet av AO Foundation och Orthopeadic Trauma Association (AO/OTA). Registreringen och klassificering av en fraktur sker genom val av frakturlokalisation på skelettet som därefter någon av de möjliga frakturtyper som finns som alternativ. Slutligen registreras en eller flera behandlingar kopplat till den registrerade frakturen. För att mäta resultatet och funktionellt utfall efter skada och behandling används ett formulär där patienten får skatta sin funktion både före och ett år efter skadan. Patienten fyller i formuläret direkt på SFRs hemsida.

9Studies of ankle fractures
Studie I i avhandlingen har undersökt hur korrekt frakturklassificeringen av fot-ledsfrakturer är i SFR. Detta är viktigt för att data ska vara pålitligt. Om inte grunddata stämmer i registret kommer det påverka pålitligheten på de senare analyserna. Regist-reringen och klassificeringen av frakturer sker av läkare som har varierande erfarenhet av frakturbedömning. Klassificering av vissa frakturer kan vara svår även för en erfaren ortoped då frakturerna man ska kategorisera kan ses som ett spektrum och att det alltid kommer finnas fall som ligger på gränsen mellan olika kategorier. Syftet med studie I var därför att jämföra den AO/OTA-klassificering som fanns registrerad i SFR med en ”korrekt” klassificering. Det skapades en erfaren bedömningsgrupp som klassificerade ett antal slumpmässigt utvalda fotledsfrakturer från SFR utifrån de röntgenbilder vi samlat in från behandlande ortopedkliniker. Granskarna i gruppen bedömde de utvalda frakturerna helt oberoende av varandra och vid två olika tillfällen. Den bedömning man sedan kom överens om ansågs vara den korrekta och kunde i sin tur jämföras med klassificeringen som fanns i SFR. Studie I visade att klassificeringen av fotleds-frakturer i SFR och den ”korrekta” klassificeringen stämde bra överens. Den stämde lika bra överens som resultatet mellan olika erfarna bedömare i andra studier som hade undersökt själva klassificeringssystemets tillförlitlighet. Därför var vår bedömning att klassificeringen av fotledsfrakturer i SFR är tillförlitlig och inte utgör något hinder av fortsatta analyser av data från registret.
I Studie II undersökte vi förekomsten av fotledsfrakturer och fördelningen av olika undergrupper till den. Bakgrunden till studien är att fotledsfrakturer inte bara är en av de vanligaste frakturerna utan att det också är en spretig grupp av frakturer. Man har tidigare kunnat se en tendens att t ex äldre patienter ådrar sig vissa typer av fotleds-frakturer vilket kan vara förknippat med ett skörare skelett. Syftet med studie II var att göra en så bra och exakt genomgång som möjligt av hur vanliga olika typer av fotledsfrakturer är. Vi gjorde bedömningen att de bästa förutsättningarna för att hitta en så stor andel av frakturerna som möjligt var att göra studien i en enskild region istället för på registerdata. Studien utgick från fotledsfrakturer på invånare i Region Norrbot-ten. Med hjälp av journalsystemet identifierades potentiella fall av fotledsfrakturer och därefter granskades röntgenbilderna av dessa. Därpå klassificerade tre olika bedömare varje fotledsfraktur med AO/OTAs system. Under de fem år som studien omfattade hittades 1756 fall av fotledsfraktur. Det gav en förekomst av 179 fall per 100 000 vuxna invånare och år. Fotledsfrakturer var vanligare hos kvinnor. I två tredjedelar av fallen orsakades frakturen av ett lågenergitrauma, dvs fall i samma plan. Hos kvinnor ökade förekomsten av fotledsfraktur med stigande ålder upp till sextioårsåldern. Hos män var den däremot relativt konstant genom hela livet. En typ av fraktur som skadar flera fotknölar och som är i höjd med syndesmosligamentet var vanligast hos äldre

10
Hans JutoStudies of ankle fractures
och kvinnor. En annan typ av fotledsfraktur som bara omfattar den inre fotknölen var tvärtom vanligare hos yngre män.
Efter en fraktur av till exempel fotleden finns en ökad risk för att utveckla blod-proppar i vensystemet. För att minska den risken används ofta förebyggande läkeme-del. På olika sjukhus finns det dock olika traditioner av hur ofta det används. Syftet med studie III var att utreda samvariationen mellan antalet venösa blodproppar efter en fotledsfraktur och hur olika ortopedkliniker i Sverige använder förebyggande behand-ling mot blodproppar.
I både studie III och IV kombinerades data från registrerade fotledsfrakturer i SFR med data från andra register. I studie III användes data från både patientregistret på dia-gnostiserade blodproppar samt läkemedelsregistret på förskrivningar av förebyggande läkemedel. Över 15 000 fall av fotledsfrakturer analyserades. Vår slutsats var att det fanns ett samband mellan hur ofta man använder den förebyggande behandlingen och antalet blodproppar. Det gällde både för fotledsfrakturer som behandlades med eller utan kirurgi. Sjukhus med ett mer frekvent användande av förebyggande behandling med lågmolekylärt heparin hade också en mindre andel fall med venösa blodproppar.
I studie IV undersöktes sjukskrivningar efter fotledsfraktur eftersom ett mindre antal patienter med fotledsfraktur blir sjukskrivna under lång tid. Samtidigt har tidigare studier kring resultat efter fotledsfraktur visat att ungefär var tionde patient rapporterar påtagliga besvär ett år efter skadan. Frågan är då om det är ett sämre utfall efter skadan i sig eller om det är andra faktorer som orsakar den förlängda sjukskrivningen. Samma grunddata från SFR användes för studie IV som till studie III, men nu även med ytter-ligare data om utbetalad sjukersättning från Försäkringskassan. Omfattning och längd på sjukskrivningen beräknades och en analys gjordes om hur frakturtyp, behandling och patientrapporterat resultat samvarierar med sjukskrivningen. Genom att titta på hur många dagar som en patient fått ersättning utbetald kunde vi utreda sambandet mellan svårighetsgrad av fraktur och längden av sjukskrivningen. I studien såg vi ett klart samband mellan svårighetsgraden på frakturen, vilket funktionellt resultat som patienten skattar ett år efter skadan och längden av sjukskrivningen. Det noterades även att förekomst av tidigare sjukskrivning var en riskfaktor för lång sjukskrivning efter fotledsfrakturen.

11Studies of ankle fractures
Slutsatser:Slutsatser:
• Trots att klassificeringen av fotledsfrakturer i SFR utförs av många läkare med varierande erfarenhet och kompetens var överenstämmelsen betydande mellan dem och expertgruppens klassificering.
• Förekomsten av fotledsfrakturer var 179 fall per 100 000 personer och år i Norrbotten. Förekomsten av fotledsfraktur ökade med åldern hos kvinnor, men inte hos män.
• Ett rutinmässigt användande av lågmolekylärt heparin efter operativt behandlade fotledsfrakturer är associerat med en lägre andel fall av venösa tromboemboliska händelser.
• Det finns ett tydligt samband mellan fotledsfrakturens svårighetsgrad, vilket resultat patienten rapporterar ett år efter skada och längden av sjukskrivning.

12
Hans JutoStudies of ankle fractures
LIST OF PAPERS
This thesis is based on the following studies, referred to in the text by their Roman numerals.
I. Substantial accuracy of fracture classification in the Swedish Fracture Register; evaluation of AO/OTA-classification in 152 ankle fractures. Juto H, Möller M, Wennergren D, Edin K, Apelqvist I, Morberg P. In-jury 2016; 47:2579-83.
II. Epidemiology of Adult Ankle Fractures: 1756 cases identified in Norr-botten County during 2009-2013 and classified according to AO/OTA. Juto H, Nilsson H, Morberg P. BMC Musculoskelet Disord 2018; 19:441.
III. Routine use of LMWH prophylaxis is associated with a lower incidence of venous thromboembolic events following an ankle fracture. Juto H, Hultin M, Möller M, Morberg P. Accepted for publication in Injury.
IV. The association beween sick leave and severity of ankle fractures. Juto H, Hultin M, Möller M, Morberg P. Manuscript.

13Studies of ankle fractures
ADDITIONAL PAPERS BY THE AUTHOR
Juto H, Gärtner Nilsson M, Möller M, Wennergren D, Morberg P. Evaluating non-responders of a survey in the Swedish fracture register: no indication of different functional result. BMC Musculoskelet Disord 2017;18:278.
Wennergren D, Bergdahl C, Ekelund J, Juto H, Sundfeldt M, Möller M. Epidemiology and incidence of tibia fractures in the Swedish Fracture Register. Injury 2018;49:2068-74.
14
Hans JutoStudies of ankle fractures
ABBREVIATIONS
AITFL Anterior inferior tibiofibular ligamentAO Arbeitsgemeinschaft für Osteosynthesefragen
(Working group for bone fusion issues)BMD Bone mineral densityDVT Deep venous thrombosisEQ-5D EuroQol Five Dimensions scaleICD-10 International Statistical Classification of Diseases
and Related Health Problems - 10th revision HIT Heparin-induced thrombocytopeniaLMWH Low-molecular-weight heparinMiDAS Microdata for analysis of the social insurance systemOMAS Olerud-Molander Ankle ScoreOTA Orthopaedic Trauma AssociationOR Odds ratioPE Pulmonary embolismPF4 Platelet factor 4PROM Patient-reported outcome measurePITFL Posterior inferior tibiofibular ligamentPTOA Posttraumatic osteoarthritisPTS Post-thrombotic syndromeR-RCT Registry-based randomized clinical trialSFR Swedish Fracture Register SMFA Short Musculoskeletal Function AssessmentNPR Swedish National Patient RegisterSPDR Swedish Prescribed Drug RegisterSSI Surgical site infectionSSIA Swedish Social Insurance AgencyVTE Venous thromboembolic eventUFH Unfractionated heparin

15Studies of ankle fractures
DEFINITIONS
AbductionThe rotation of the ankle away from the midline of the body.
AdductionThe rotation of the ankle towards the midline of the body.
Accuracy Accuracy is a description of how correct a measure is and the degree of closeness to the true value of something. In study I it is used as the measure between the classification in the SFR and the gold standard classification.
BiasSystematic deviation or error in interpretation of data as a result from inaccurate estima-tions and unfair sampling.
CompletenessThe proportion of cases reported or included in, for an example, a register, of the cases possible to include.
CoverageThe proportion of departments that register fractures.
Gold standard classification A gold standard test refers to the best available test under reasonable conditions. Here we refer to the consistent assessment by multiple experienced assessors made after multiple observations of projectional radiographs and hence to the ”true” fracture classification.
PronationRotating the sole of the foot downward which stretches the medial ligament apparatus of the ankle.
Reliability Is the overall consistency or repeatability of a measure. Can be used for example to evaluate the consistency between different assessors as inter-observer reliability or between same assessor at different assessments as intra-observer reliability.
SupinationRotating the soles of the foot upward which stretches the lateral ligament apparatus of the ankle.
Validity Validity and accuracy are used synonymously.

1

17Studies of ankle fractures
1. INTRODUCTION
1.1 THE SWEDISH FRACTURE REGISTER
The concept of a fracture register existed as early as the mid-1990s. It provided im-portant answers to orthopaedic trauma questions which cannot be obtained from the public health data registers, such as the Swedish National Patient Register (NPR). The quality of these registers is in some respects limited and important variables are missing. Another reason for the need for a fracture register is that many of questions regarding orthopaedic treatments are difficult to answer with randomised controlled trials as some concerns and questions require extensive data is to detect differences. For example, when the risk of complications is low, or the differences are in results is relatively small between treatments (Wennergren 2015, Wennergren 2018).
The Swedish Fracture Register (SFR) development began in 2007 at Sahlgrenska University Hospital. The goals were to include all types of orthopaedic fractures, re-gardless of treatment and to include follow-up with both patient-reported outcomes and reoperation frequency. A supplementary goal was the collection of more detailed data than that included in the public health data registers. When the variables were defined and determined during the development of the register, they needed to be so extensive that the data became value-creating yet limited in number to minimize the extra effort to register (Wennergren 2015).
The structure of the SFR was completed in 2009, and an early version of the system was completed in January 2011, so that the first fracture could be registered. Initially it was only possible to register fractures of the tibia and humerus in adults at Sahlgrenska University Hospital. In the following years, the register was developed and from 2015, all orthopaedic fractures could be registered. The orthopaedic departments in Sweden have gradually joined and started registering fractures. In January 2013, seven out of the 55 orthopaedic departments at hospitals in Sweden registered fractures. In January 2020, SFR reached full coverage despite being a voluntary register (Wennergren 2015, Wennergren 2018, SFR Annual Report 2020).

18
Hans JutoStudies of ankle fractures
The registration of injuries, fractures and treatments is now completely web-ba-sed. The collection of patient-reported outcomes was carried out with questionnaires in paper form until February 2019. Patients are now able to answer the survey on the SFR website. All data is linked to people resident in Sweden with a unique personal identity number. The data in the register is based on a specific injury occasion. One or more different fractures can be registered and linked to the injury. Similary can on each fracture, one or more different treatments can be registered. Patient-reported outcome measures (PROM) are collected after each injury. Drop-down menus with step-by-step multiple selection fields are used when entering data. The first three steps in the registration process are handled by the doctor at the department treating the fracture.
The first part of the registration is about data on the injury based on the mechanism of origin, place of injury and assessment of whether it is a low or high energy injury. These are selected from drop-down menus. In a second step, one or more fractures associated with the injury are registered. To register the fracture, the correct bone and segment are selected from an illustration of the skeleton. This also registers the correct side for the fracture. Thereafter, the fracture is classified and SFR mainly uses AO/OTA’s classification system. In the last stage, one or more treatments are registered for each fracture. The treatment choices are made from predefined alternatives based on common treatments related to the selected fracture. Both non-surgical and surgical treatments are registered. Primary treatment is distinguished from planned secondary treatment and reoperations. Reoperations that can be used as an outcome measure are subgrouped based on the cause of the reoperation.
The proportion of recorded injuries and fractures, described as completeness, is
Fig 1: Registration of fractures started in 2011. SFR publishes an annual report on activity, development and data collection.

19Studies of ankle fractures
important for the quality of data. Completeness clearly distinguishes between different departments and between different fractures. One way to measure completeness is to compare registered fractures in the SFR with those reported in the Swedish National Patient Register (NPR). For the largest fracture groups and registering departments, 64% of the fractures were found in both the SFR and the NPR (SFR Annual Report 2020). However, the NPR tends to overestimate the number of fractures, as some are registered on the same patient several times in different years. When validating the completeness of humeral fractures treated at Sahlgrenska University Hospital, it rose from 62% to 88% as to a raw comparison to the data between SFR and the NPR (Berg-dahl 2021).
To follow up the outcome after injury and treatment, patient-reported outcomes with two generic questionnaires are used. The first round of questionnaires is sent to the patient shortly after the first treatment of the fracture with the aim that the patient should report the function before the time of injury. Thereafter, identical questionnaires were sent out to the patient one year after the injury to evaluate function and outcome. The questionnaires used are the EQ-5D-3L, which was changed to 5L in 2019, and the Short Musculoskeletal Function Assessment (SMFA) (SFR Annual Report 2019).
A low response rate of PROM can however be a problem with patient involvement
Fig 2: Registration and classification of ankle fractures in the Swedish Fracture Register.
20
Hans JutoStudies of ankle fractures
in medical registries. The response rate of the patient reported outcome-surveys are visibly lower in the SFR than in registers of elective surgery. Loss to follow-up and low response rate may introduce bias to a survey and affect the validity of a study (Sheikh 1981, Gluud 2006, Kristman 2004, Corrigan 1997). This problem has been addressed in several earlier studies. Some of them were the non-responders or patients who are lost to follow-up, reported poorer functional results than initial responders. In others where a difference could not be seen (Kwon 2010, Kim 2004, Norquist 2000, Murray 1997). In our study, no indication of a difference in functional outcome between res-ponders and non-responders could be seen (Juto 2017).
The accuracy of the classification and interpretation of the data is of immense importance when using the register for research purposes. Entry of data into the SFR is performed by the attending doctors who have a wide variation of orthopaedic expe-rience. Registration, including classification, is mainly carried out at the accident & emergency departments by interns and registrars, sometimes with very limited expe-rience of fracture classification. Therefore, it is important to review how accurate the classification made in the SFR is.
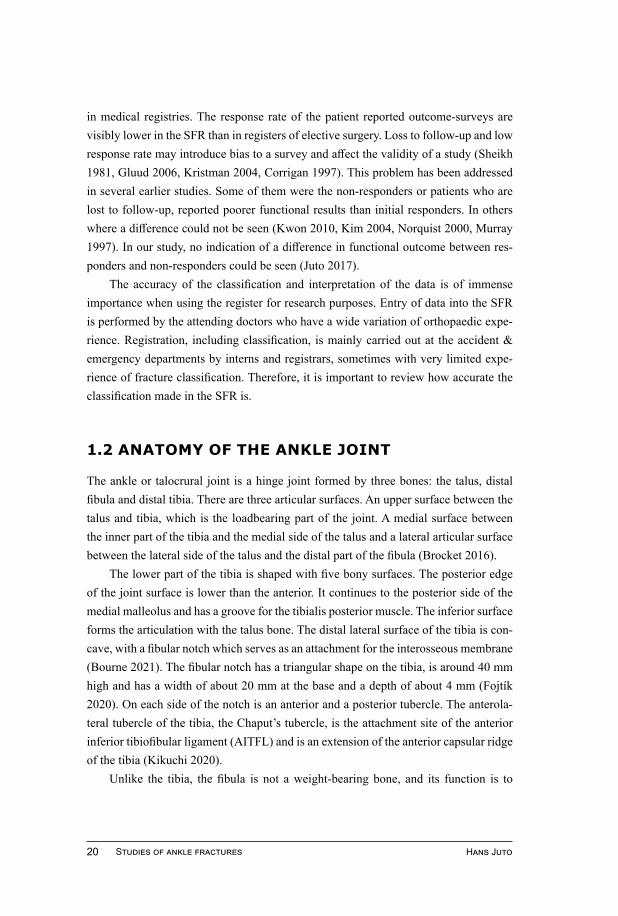
1.2 ANATOMY OF THE ANKLE JOINT
The ankle or talocrural joint is a hinge joint formed by three bones: the talus, distal fibula and distal tibia. There are three articular surfaces. An upper surface between the talus and tibia, which is the loadbearing part of the joint. A medial surface between the inner part of the tibia and the medial side of the talus and a lateral articular surface between the lateral side of the talus and the distal part of the fibula (Brocket 2016).
The lower part of the tibia is shaped with five bony surfaces. The posterior edge of the joint surface is lower than the anterior. It continues to the posterior side of the medial malleolus and has a groove for the tibialis posterior muscle. The inferior surface forms the articulation with the talus bone. The distal lateral surface of the tibia is con-cave, with a fibular notch which serves as an attachment for the interosseous membrane (Bourne 2021). The fibular notch has a triangular shape on the tibia, is around 40 mm high and has a width of about 20 mm at the base and a depth of about 4 mm (Fojtík 2020). On each side of the notch is an anterior and a posterior tubercle. The anterola-teral tubercle of the tibia, the Chaput’s tubercle, is the attachment site of the anterior inferior tibiofibular ligament (AITFL) and is an extension of the anterior capsular ridge of the tibia (Kikuchi 2020).
Unlike the tibia, the fibula is not a weight-bearing bone, and its function is to

21Studies of ankle fractures
provide stability to the ankle joint. The lower part of the fibula is attached to a large number of ligaments and has joint surfaces on the medial side. It widens distally and is surrounded by strong ligaments in all directions. On the anteromedial aspect of the distal fibula is the Wagstaffe-Le Fort tubercle, the fibular attachment site of the AITFL (Gupton 2021, Kikuchi 2020).
The talus is almost completely covered by the joint surface and cartilage without any attachment to muscles or tendons. It is however the attachment site for many li-gaments responsible for stabilizing the ankle joint. The upper part, leading to the ta-locrural joint is convex and slightly wider at the front than at the back, which results in increased stability in dorsiflexion (Kelikian 2011, Brocket 2016, Bartoníček 2003).
The deltoid ligament runs from the medial malleolus toward the navicular, the calcaneus, and the talus. It can be referred to as the medial collateral ligament and has a multifascicular appearance in two layers. Four fascicules can be found in the superfici-al layer and two in the deep layer. The superficial layer helps to maintain the alignment of the talus in the ankle joint, to hold the force of valgus stress as well as external rotation. The deep layer prevents lateral movement and stabilize against plantar flexion and external rotation (Savage-Elliott 2012, Campbell 2014).
The lateral collateral ligament complex of the ankle joint consists of the anterior talofibular ligament, the posterior talofibular ligament and the calcaneofibular ligament. The anterior talofibular ligament is the broadest of them but also the weakest while the calcaneofibular ligament is the strongest. Both talofibular ligaments are around 13 mm long and the calcaneofibular ligament is around 20 mm (Rochell 2020).
The distal tibiofibular syndesmosis consists of the convex surface of the fibula and the concave surface of the tibia, and these are stabilized by four ligaments: the AITFL, the posterior inferior tibiofibular ligament (PITFL), the transverse ligament, and the interosseous ligament. The syndesmotic recess starts distally from the tibiota-lar joint and ends cranially at the distal edge of the interosseous ligament. It is almost always present between the distal tibia and fibula but varies in size. At the base of the syndesmosis at a small area, the tibia and fibular are in direct contact with each other, the tibiofibular contact zone. The bones are covered by a thin layer of cartilage, about 0.5-1.0 mm thick. This cartilage area continues down the side of the tibia to a tibial plafond. Similary, the cartilage of the fibula continues down into the fibular facet of the fibulotalar joint (Hermans 2010, Ebraheim 2006).
The AITFL extends in an oblique direction from the anterior tubercle on the distal tibia, the Chaput’s tubercle, to the anterior tubercle on the distal fibula, the Wagnstaf-Le Forts tubercle, and has a trapezoidal shape. The uppermost part is thick and short but it
22
Hans JutoStudies of ankle fractures
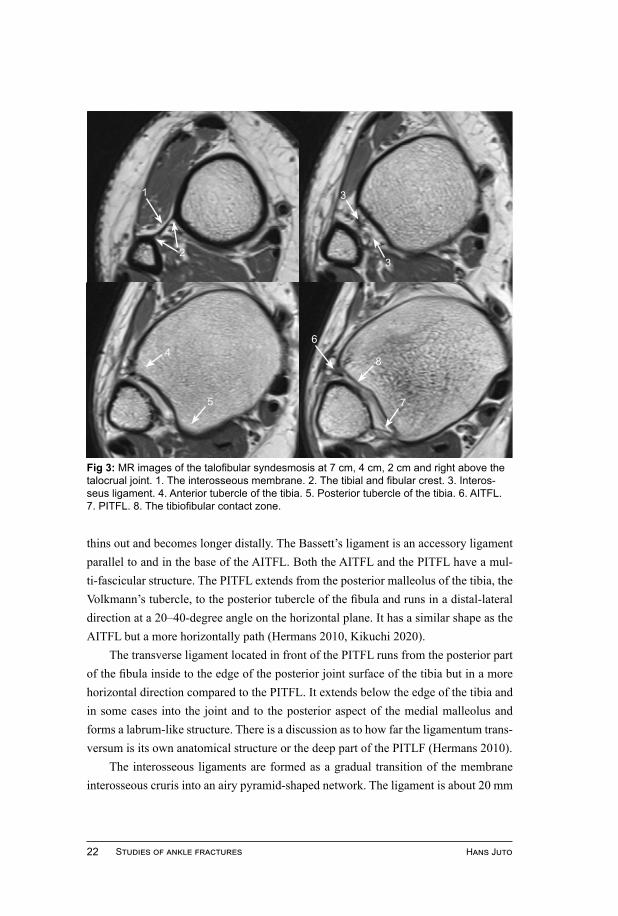
thins out and becomes longer distally. The Bassett’s ligament is an accessory ligament parallel to and in the base of the AITFL. Both the AITFL and the PITFL have a mul-ti-fascicular structure. The PITFL extends from the posterior malleolus of the tibia, the Volkmann’s tubercle, to the posterior tubercle of the fibula and runs in a distal-lateral direction at a 20–40-degree angle on the horizontal plane. It has a similar shape as the AITFL but a more horizontally path (Hermans 2010, Kikuchi 2020).
The transverse ligament located in front of the PITFL runs from the posterior part of the fibula inside to the edge of the posterior joint surface of the tibia but in a more horizontal direction compared to the PITFL. It extends below the edge of the tibia and in some cases into the joint and to the posterior aspect of the medial malleolus and forms a labrum-like structure. There is a discussion as to how far the ligamentum trans-versum is its own anatomical structure or the deep part of the PITLF (Hermans 2010).
The interosseous ligaments are formed as a gradual transition of the membrane interosseous cruris into an airy pyramid-shaped network. The ligament is about 20 mm
Fig 3: MR images of the talofibular syndesmosis at 7 cm, 4 cm, 2 cm and right above the talocrual joint. 1. The interosseous membrane. 2. The tibial and fibular crest. 3. Interos-seus ligament. 4. Anterior tubercle of the tibia. 5. Posterior tubercle of the tibia. 6. AITFL. 7. PITFL. 8. The tibiofibular contact zone.
1
23
3
6
7
84
5

23Studies of ankle fractures
Fig 4: The lateral, the posterior and the medial view of the ankle joint.
Anterior talofibular ligament
AITFLPITFL
Posterior talofibular ligament
Calcaneofibularligament
Tibionavicular ligament
Tibiospring ligament
Tibiocalcaneal ligament
Superficial poste-rior tibiotalar ligament
Spring ligament
Illus
tratio
n: Is
abel
le F
orsl
in
Calcaneo-fibularligament
Posterior talofibular ligament
PITFL
Interosseous membrane
24
Hans JutoStudies of ankle fractures
wide and 5 mm thick and transitions continuously distally to both AITFL and PITFL. It acts as a spring that allows a smaller separation between the malleolus during dorsi-flexion of the talocrural joint. Ogilvie-Harris et al. show that in the stability of the syn-desmosis AITFL accounts for 35%, ligamentum interosseous 22%, ligamentum tran-sversum 33% and PITFL 9% (Ebraheim 2006, Hermans 2010, Ogilvie-Harris 1994).
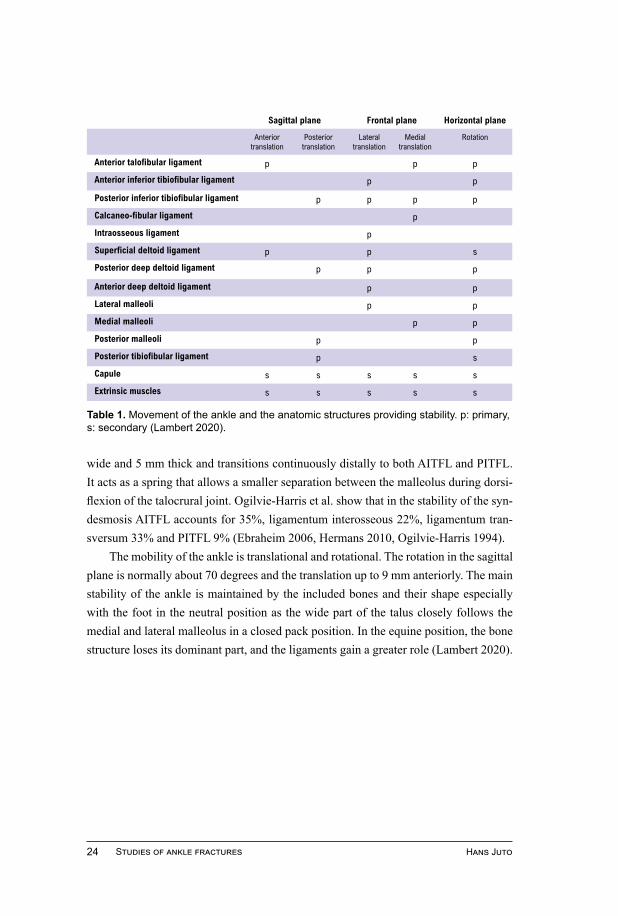
The mobility of the ankle is translational and rotational. The rotation in the sagittal plane is normally about 70 degrees and the translation up to 9 mm anteriorly. The main stability of the ankle is maintained by the included bones and their shape especially with the foot in the neutral position as the wide part of the talus closely follows the medial and lateral malleolus in a closed pack position. In the equine position, the bone structure loses its dominant part, and the ligaments gain a greater role (Lambert 2020).
Table 1. Movement of the ankle and the anatomic structures providing stability. p: primary, s: secondary (Lambert 2020).
Sagittal plane Frontal plane Horizontal plane
Anteriortranslation
Posterior translation
Lateral translation
Medial translation
Rotation
Anterior talofibular ligament p p p
Anterior inferior tibiofibular ligament p p
Posterior inferior tibiofibular ligament p p p p
Calcaneo-fibular ligament p
Intraosseous ligament p
Superficial deltoid ligament p p s
Posterior deep deltoid ligament p p p
Anterior deep deltoid ligament p p
Lateral malleoli p p
Medial malleoli p p
Posterior malleoli p p
Posterior tibiofibular ligament p s
Capule s s s s s
Extrinsic muscles s s s s s

25Studies of ankle fractures
1.3 DEFINITION AND CLASSIFICATION
Ankle fractures are a heterogeneous group of fractures with different mechanisms of origin, a wide variation in appearance and a clear difference in treatment and results. An ankle fracture is a fracture against the malleoli of the talocrural joint and/or the fibu-la proximal to the joint with or without an injury to the distal tibiofibular syndesmosis. The ankle fracture derives from rotational force of the talus in the talocrural joint.
Danis-WeberThe Belgian general surgeon Robert Danis (1880-1962) published ‘Théorie et prati-que de l’ostéosyntèse’ in 1949 with both an early version of the classification and the concept on stable internal fractures fix-ation (Dauwe 2020). The Swiss Bernhard Georg Weber (1927-2002) developed and published the classification in 1972 in ‘Die Verletzungen des oberen Sprunggelenkes’ (The injuries of the upper ankle) and he writes that ”...the level of the fibular lesion is directly related to the condition of the syndesmosis, regardless of whether the-re is medial ankle injury and what type it is.” (Weber 1972). The Danis-Weber classification only takes the fibula fracture into account and is equal to the first step of classifying the ankle fracture using the AO/OTA-system, the AO/OTA-type. Type A is a fracture distal to the syndesmosis and with the syndesmosis regarded as in-tact. In type B-fractures, the fracture of the fibula is at the level of the syndesmosis and
Malleolar segment
44A 44B 44C
Fig 5: The ankle fracure involves the malleolus segement of the talocrural joint and in type C fractures, the fibula proximal to the joint.

26
Hans JutoStudies of ankle fractures
the stability is regarded as variable. Lastly, in type C-fracture the injury of the fibula is proximal to the syndesmosis. Type C-fracture described as always unstable (Weber 1972).
Lauge-HansenLauge-Hansen’s classification system for ankle fractures is widely used and is based on a theoretical injury mechanism, which has a predictable pattern on X-rays and can thus be used for classification. Niels Lauge-Hansen (1899-1976) was a Danish radiolo-gist and active at the Central Hospital in Randers, Denmark. He published his article: ”Fractures of the ankle - analytic historical survey as the basis of new experimental, roentgenologic and clinical investigations” (Lauge 1948). He continued with several articles during the fifties which were based on experiments with cadaveric lower limb amputations and observations of injury patterns (Lauge-Hansen 1950, Tartaglione 2015).
Lauge-Hansen’s system uses three parts to divide the classification. The first is the position of the foot at the moment of injury, whether the foot has been pronated or supinated. Thus, defining which side and collateral ligament apparatus that has been stretched. The second stage describes the direction of the deforming force. Three pos-sibilities are used: abduction, adduction and outward (external) rotation. In the final stage, it describes how many structures are injured. It gives rise to four categories with thirteen subgroups/stages. Supination Adduction stage 1-2, Supination External Rota-tion stage 1-4, Pronation Abduction stage 1-3 and Pronation External Rotation stage 1-4 (Arimoto 1980, Shariff 2006, Tartaglione 2015).
Malleolar segment
44A 44B 44C
Fig 6: The Danis-Weber classification and the AO/OTA-type is equvivalent and describes the hight of the fibula fracture according to the syndesmotic ligament.
Malleolar segment
44A 44B 44C
Malleolar segment
44A 44B 44C
Illus
tratio
n: P
ontu
s A
nder
sson
Type A Type B Type C

27Studies of ankle fractures
AO
Lauge-Hansen
A B C
Supination-adduction Supination-exorotation Pronation-abduction Pronation-exorotation
1
2
22
2 2
3 3
3
4
44
1
1
11
AO
Lauge-Hansen
A B C
Supination-adduction Supination-exorotation Pronation-abduction Pronation-exorotation
1
2
22
2 2
3 3
3
4
44
1
1
11
Supination External Rotation
1. Injury of the AITFL.2. Oblique/spiral fracture of lateral malleolus.3. Posterior malleolus avulsion or injury of the PITFL.4. Medial malleolus fracture or deltoid ligament injury.
AO
Lauge-Hansen
A B C
Supination-adduction Supination-exorotation Pronation-abduction Pronation-exorotation
1
2
22
2 2
3 3
3
4
44
1
1
11
AO
Lauge-Hansen
A B C
Supination-adduction Supination-exorotation Pronation-abduction Pronation-exorotation
1
2
22
2 2
3 3
3
4
44
1
1
11
AO/OTA-type B
AO/OTA-type A
AO/OTA-type C
Supination Adduction
1. Injury to the lateral collateral li-gements or a transverse traction fracture of lateral malleolus.2. Vertical fracture of medial malleolus.
Pronation Abduction
1. Medial malleolus fracture or deltoid ligament injury. 2. Injury of the AITFL.3. Transverse or comminuted fracture of the fibula gener-ally just proximal to the tibial plafond.
Fig 7: Categories and stages of the Lauge-Hansen classifi-cation and the equvivalent AO/OTA-type.
Pronation External Rotation
1. Medial malleolus fracture or deltoid ligament injury. 2. Injury of the AITFL.3. Short spiral fracture proximal to the syndesmosis ligaments.4. Posterior malleolus avulsion or injury of the PITFL.
Illus
tratio
n: P
ontu
s A
nder
sson
AO
Lauge-Hansen
A B C
Supination-adduction Supination-exorotation Pronation-abduction Pronation-exorotation
1
2
22
2 2
3 3
3
4
44
1
1
1
1
oror
or
1
1
AO
Lauge-Hansen
A B C
Supination-adduction Supination-exorotation Pronation-abduction Pronation-exorotation
1
2
22
2 2
3 3
3
4
44
1
1
1
1
oror
or
1
1
AO
Lauge-Hansen
A B C
Supination-adduction Supination-exorotation Pronation-abduction Pronation-exorotation
1
2
22
2 2
3 3
3
4
44
1
1
1
1
oror
or
1
1
AO
Lauge-Hansen
A B C
Supination-adduction Supination-exorotation Pronation-abduction Pronation-exorotation
1
2
22
2 2
3 3
3
4
44
1
1
1
1
oror
or
1
1
28
Hans JutoStudies of ankle fractures
Even if the Lauge-Hansen classification system provides a model that combines patterns of the X-ray image with the injury mechanism, there are serious objections to the reproducibility and reliability of the classification system, which is described as oversimplified (Michelson 1997, Kwon 2015). Fonseca el al. show only a fair interrater agreement (kappa 0.32) between just the categories of the Lauge-Hansen classifica-tion (Fonseca 2018). Another study demonstrates that the Lauge-Hansen classification could only predict ligamentous injury and fracture morphology in half of the exami-ned cases (Gardner 2006). However, the Lauge-Hansen classification system is still considered the landmark achievement regarding the biomechanics of ankle fractures and contributes to our understanding of the injury mechanism and deforming forces (Tartaglione 2015).
AO/OTAMaurice E Müller (1918-2009), inspired by meetings with and the achievements of Robert Danis in the concept of stable fixation, was one of the architects and creator of the AO Foundation in 1958. Müller and the AO-foundation had recognized the need for a comprehensive classification system for all fractures since the mid-60s. Retired from teaching in the 80s, he concentrated on developing this classification system (Schatzker 2018). The Müller AO Classification of fractures was published in 1987 by the AO Foundations and an English version ”The comprehensive classification of fractures of long bones” in 1990. In 1996, together with the American Orthopaedic Trauma As-sociation Committee for Coding and Classification, their classification system for the entire skeleton was published as ”Fracture and Dislocation Compendium”. In 2007, a revised edition was published in which Müller/AO and OTA merged into a common system with unified coding (Marsh 2007). The Fracture and Dislocation Classification Compendium has been further updated in a new version (Meinberg 2018). The system is structured into five steps with an alphanumeric code. It is starts by defining the loca-tion of the fracture based on the number of the specific bone and the location on the bone and thus produces a two-digit code. For ankle fractures, the code becomes 44; 4 for the tibia and the 4th segment on the tibia. The final three positions in the code are used to describe the morphology of the fracture where it is divided into a type, a group and then a subgroup. These are defined differently, based on the fracture in question.
OtherThe Herscovici classification system is used for fractures of the medial malleolus (Ait-ken 2017). Another published, but seldom used classification system for ankle fractures is the Broos-Bisschop (Broos 1992, Alexandropoulos 2010).
29Studies of ankle fractures
Illus
tratio
n: P
ontu
s A
nder
sson
44A44A11
44A21
44A31
44A12
44A22
44A32
44A13
44A23
44A33
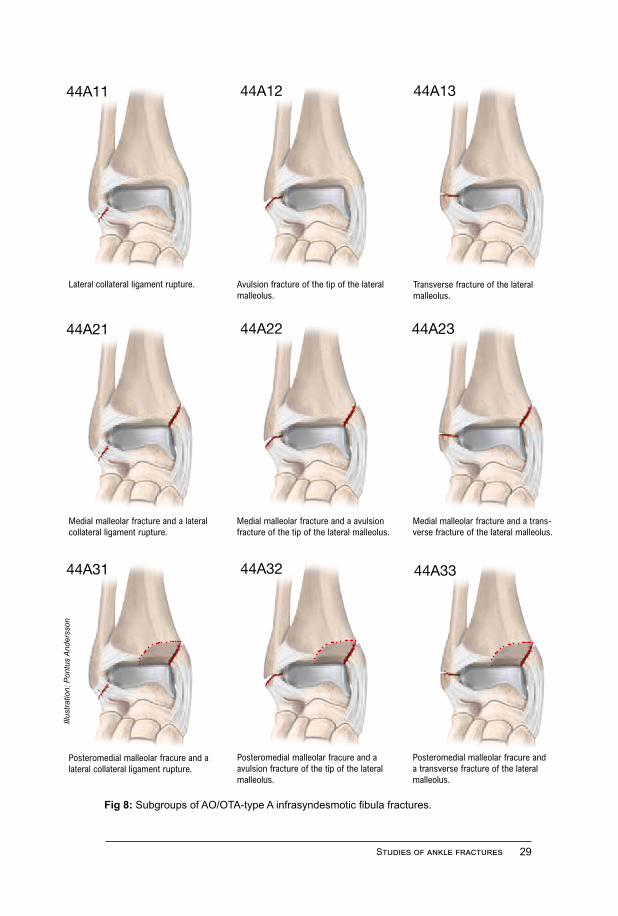
Lateral collateral ligament rupture. Avulsion fracture of the tip of the lateral malleolus.
Transverse fracture of the lateral malleolus.
Medial malleolar fracture and a lateral collateral ligament rupture.
Medial malleolar fracture and a avulsion fracture of the tip of the lateral malleolus.
Medial malleolar fracture and a trans-verse fracture of the lateral malleolus.
Posteromedial malleolar fracure and a lateral collateral ligament rupture.
Posteromedial malleolar fracure and a avulsion fracture of the tip of the lateral malleolus.
Posteromedial malleolar fracure and a transverse fracture of the lateral malleolus.
Fig 8: Subgroups of AO/OTA-type A infrasyndesmotic fibula fractures.
44A44A11
44A21
44A31
44A12
44A22
44A32
44A13
44A23
44A33
44A44A11
44A21
44A31
44A12
44A22
44A32
44A13
44A23
44A33
44A44A11
44A21
44A31
44A12
44A22
44A32
44A13
44A23
44A33
44A44A11
44A21
44A31
44A12
44A22
44A32
44A13
44A23
44A33

30
Hans JutoStudies of ankle fractures
44B44B11
44B21
44B31
44B12
44B22
44B32
44B13
44B23
44B33
44B44B11
44B21
44B31
44B12
44B22
44B32
44B13
44B23
44B33
44B44B11
44B21
44B31
44B12
44B22
44B32
44B13
44B23
44B33
Simple isolated fibula fracture. Isolated fibula fracture with a ruptu-re of the anterior syndesmosis.
Isolated multifragmentary fibula fracture.
Simple fibula fracture with a rupture of the deltoid ligament.
Simple fibula fracture with a medial malleolus fracture.
Multifragmentary fibula fracture with a medial injury.
Simple fibula fracture with a rupture of the deltoid ligament and a posterior malleolus fracture.
Simple fibula fracture with a medial and a posterior malleolus fracture.
Multifragmentary fibula fracture with a medial and a posterior malleolus fracture.
Fig 9: Subgroups of AO/OTA-type B transsyndesmotic fibula fractures.
Illus
tratio
n: P
ontu
s A
nder
sson

31Studies of ankle fractures
Fig 10: Subgroups of AO/OTA-type C suprasyndesmotic fibula fractures.
Simple fibula fracture with rupture of the deltoid ligament.
Isolated fibula fracture with a fractu-re of the medial malleolus.
Isolated fibula fracture with a fracture of the medial and posterior malleolus.
Multifragmentary fibula fracture with rupture of the deltoid ligament.
Multifragmentary fibula fracture with a fracture of the medial malleolus.
Multifragmentary fibula fracture with a fracture of the medial and posterior malleolus.
Proximal fibula injury with a medial side injury.
Proximal fibula injury with shortening and a medial side injury.
Proximal fibula injury with a medial side injury and a poserior melleo-lus fracture.
44C44C11
44C21
44C31
44C12
44C22
44C32
44C13
44C23
44C33
44C44C11
44C21
44C31
44C12
44C22
44C32
44C13
44C23
44C33
44C44C11
44C21
44C31
44C12
44C22
44C32
44C13
44C23
44C33
44C44C11
44C21
44C31
44C12
44C22
44C32
44C13
44C23
44C33
44C44C11
44C21
44C31
44C12
44C22
44C32
44C13
44C23
44C33
44C44C11
44C21
44C31
44C12
44C22
44C32
44C13
44C23
44C33
44C44C11
44C21
44C31
44C12
44C22
44C32
44C13
44C23
44C33
44C44C11
44C21
44C31
44C12
44C22
44C32
44C13
44C23
44C33
44C44C11
44C21
44C31
44C12
44C22
44C32
44C13
44C23
44C33
Illus
tratio
n: P
ontu
s A
nder
sson

32
Hans JutoStudies of ankle fractures
1.4 EPIDEMIOLOGY
The ankle fracture is a common injury and accounts for approximately one out of ten fractures registered in the Swedish Fracture Register (SFR annual report 2019). An in-cidence of 107-187 ankle fractures per 100,000 inhabitants and year is described (Daly 1987, Court-Brown 1998, Jensen 1998, Elsoe 2016). A general increase in incidence over time is stated and Thur et al. for example showed that inpatient care with ankle fracture increased by 0.2% per year (Bengnér 1986, Court-Brown 1998, Kannus 2002, Thur 2012).
Some variation in incidence between different seasons and days of the week has been reported. A higher frequency in winter and early summer and in years with more severe winters was seen. A higher incidence during weekends has also been shown (Jensen 1998, Elsoe 2016, Kannus 2002). Falls from standing height cause almost two thirds of fractures, while sports-related trauma accounts for about 16-36% (Bengnér 1986, Daly 1987, Thur 2012, Elsoe 2016, Scheer 2020). In Denmark and the United Kingdom, it was shown that the most common activity in sports-related ankle fractures was football, while in the USA was softball (Court-Brown 1998, Jensen 1998, Daly 1987). Morris et al. showed in a review of X-ray examinations of suspected ankle fractures that fractures were observed in 16% of the cases (Morris 2013).
Ankle fractures constitute approximately 55-63% of isolated lateral malleolar fractures, 8-10% of isolated medial malleolar fracture and about 26-35% of bi-, trimal-leolar and type C fractures. According to AO/OTA-type classification, type A fractu-res compose between 11-38%, type B 52-66% and type C fractures 10-14% (Bengnér 1986, Daly 1987, Court-Brown 1998, Jensen 1998, Elsoe 2016).
The fracture is described as equally common on both the left and right side (Daly 1997). Open injuries were seen in about 2% of the ankle fractures (Court-Brown 1998).
While there is still an ongoing discussion about ankle fracture and osteoporo-sis, the relationship to obesity is clearly shown. Increased weight generally means a reduced risk of fracture, but the opposite is seen in ankle fractures (De Laet 2005, Hasselman 2003, FitzGerald 2012, Hjelle 2021). Other described risk factors related to ankle fractures are elite sports, previous ankle injury, alcohol consumption and single households (Murphy 2003, Liu 2018).
There is a relatively even distribution of ankle fractures between women and men. Early on, an increase in the incidence of ankle fractures among women was seen. Bengnér showed that between 1950 and 1980, the proportion of women increased, alt-hough they still constituted a minority. In earlier studies ankle fractures were somewhat more common among men (Bengnér 1986, Daly 1987, Court-Brown 1998), while in
33Studies of ankle fractures
later publications, a slight predominance is seen in women (Fox 2005, Thur 2012, Elsoe 2016, Scheer 2020). This development was associated with the sharp increase in the proportion of older women (Bengnér 1986). In women over the age of 60, the increase in incidence was 0.9% per year (Thur 2012). It is now generally accepted that the incidence of ankle fractures is rising among the elderly and the female population. Most of the studies show that there is a rise in incidence among women up to the age of about 60 to 70 and thereafter it levels out or even declines, while in men it is more even or bimodal (Bengnér 1986, Daly 1987, Court-Brown 1998, Singer 1998, van Staa 2001, Thur 2012, Sommersalo 2014, Beerekamp 2017, Scheer 2020).
Kanus et al. examined the transformation of the incidence of ankle fractures in Finland in persons over 60, from 1970 to 1994. They saw a sharp increase from 57 to 150 cases per 100,000 person-years and that the increase was strongest in women, although the incidence decreased slightly thereafter (Kannus 2002, Kannus 2016).
According to Fox et al., women also tend to have a more stable fracture (Fox 2005). On the other hand, somewhat contradictory, older women seem to dominate the bi- and trimalleolar ankle fractures and those appear to increase more with age among female patients (Bengnér 1986, Koval 2005, Thur 2012). Daly et al. describe that the Lauge-Hansen Supination External Rotation type, which corresponds to AO/OTA type B fracture, increases most clearly with age in women (Daly 1997).
Osteoporosis and ankle fracturesThe knowledge of low bone mineral density (BMD) being associated to an increased risk of fractures is well established (Marshall 1996, Cummings 2002). A weakening of trabecular microstructure is a trait of osteoporosis and vertebral fractures is seen as the hallmark of osteoporosis with a very high risk of another fragile fracture (Lorentzon 2015). However, there has been a long discussion about which fractures should be seen as osteoporosis associated. A fragility fracture results from a low energy trauma that would not normally result in fracture. A low energy trauma is specified by the World Health Organization (WHO) as a fall from a standing height or less (NICE 2012). As the activity of osteoblasts and osteoclasts is affected by oestrogen, postmenopausal wo-men are particularly prone to osteoporosis (Ji 2015). Ankle fractures are not considered to be the typical fracture associated with osteoporosis, but it has been the subject of discussion (Guggenbuhl 2005, Hasselman 2003, Stein 2010).
An association between a fracture and osteoporosis becomes relevant if it can pre-dict an increased risk of another fracture and thus present an indication of osteoporosis treatment. There are several ways used to investigate a relationship. Comparing BMD with the incidence of fractures, comparing BMD in patients with fractures and with a

34
Hans JutoStudies of ankle fractures
control group and, to compare the incidence with age, gender and low-energy trauma are a few examples.
While some earlier studies on osteoporosis conclude that fractures of the wrist, humerus, vertebra and hip, for example, have a significant relationship to low BMD, ankle fractures however, do not. In a study that examined the correlation between BMD and fracture risk among 9,704 women whose bone density was measured, there was an association between most fractures, such as foot and hand and reduced BMD. Still, no correlation was seen between low BMD and ankle fractures (Seeley 1991). In a long-term follow-up of the same material, an association was seen however between almost all fractures that were included, inclusive ankle fractures. The ankle fractures still only had a weak association (Stone 2003). In somewhat contrast to this Stein et al. showed that postmenopausal women with low energy ankle fractures have an affected microar-chitecture and reduced stiffness in the trabecular bone (Stein 2010). In a similar study of 65-year-old women with ankle fractures, those with an ankle fracture had a lower areal bone mineral density and trabecular bone alternation compared with a control group, implying that ankle fractures are also a manifestation of bone fragility (Biver 2014). Furthermore, ankle fractures have been shown to increase the risk of a new fracture among postmenopausal women (Gunnes 1998). There is an ongoing debate how to assess the ankle fracture in this sense. Cummings et al. concluded however, that studying fractures epidemiology is crucial to improve strategies for identification and treatment of high-risk individuals (Cummings 2002).
1.5 COMPLICATIONS
Ankle fractures, and in particular, surgically treated ankle fractures are burdened with the risk of various complications. The early complications following an ankle fracture include venous thromboembolic events and wound infections. The stated risk of com-plications after ankle fracture surgery varies greatly in different studies and is described between 5-36%, depending on how it is measured and defined (Lynde 2012, Dodson 2013, Ovaska 2013, Belmont 2015, Macera 2018). A considerable portion of the sur-gically treated ankle fracture patients will at some point require a re-operation, but in the majority of cases, it is only concerning an implant removal. In a study by Pincus et al., fixation material was removed in 18% of patients and 1.5% had a re-operation for another reason, such as after infection (Pincus 2017).
Wound complications are common and can be divided into deep and superficial wound infections, wound rupture, and wound edge necrosis (Schepers 2013). It can

35Studies of ankle fractures
appear individually or in a mixed appearance. Other complications are non-union, ma-lunion and post-traumatic osteoarthritis. One of the most serious but still rare conse-quences following an ankle fracture is amputation. SooHoo et al. show that 0.2% of operated ankle fractures culminate in a lower leg amputation. An increased mortality has also been demonstrated following an ankle fracture. Belmont showed a 30-day mortality of 0.3% and SooHoo et al. reported a 90-day mortality of 1.1% (Belmont 2015, SooHoo 2009).
Among the described patient-related risk factors for early complications after an-kle fracture surgery are obesity, old age, diabetes, smoking, alcohol abuse and cardio-vascular disease (Anderson 2008, SooHoo 2009, Nåsell 2011, Lynde 2012, Ovaska 2013, Belmont 2015, Korim 2014, Pincus 2017, Benedick 2020). Anderson et al., for example, showed a greatly increased risk of complications in elderly patients. In the group older than 65 years of age, complications were seen in 40% of patients, while in younger patients, the figure was 11% (Andersson 2008). Complications are correlated to significant suffering and impaired functional outcome (Macera 2018, Schepers 2013, Korim 2014). In addition, complications heavily increase the length of stay at hospital and thereby the costs for healthcare and society increase (Thakore 2015, de Lissovoy 2009, Whithouse 2002).
Venous thromboembolic eventVenous thromboembolic event (VTE) is a multifactorial disease and a result of the interaction between exogenic and endogenic risk factors. The risk of thromboembolic events increases after musculoskeletal injuries and can have catastrophic consequen-ces. The Prussian pathologist Rudolf Virchow (1821-1902) laid the foundation for the understanding of and left lasting contributions in the area of VTE. Virchow established the term thrombosis and embolism. He opposed to the idea that inflammation was the cause of thrombosis and published ”Thrombose und Embolie. Gefässentzündung und septische Infektion” in 1856. His name has been given to the triad that forms the basis for understanding the pathogenesis of VTE, Virchow’s triad, where disturbed blood flow, vessel wall damage and affected coagulation are described as critical factors for the development (Kumar 2009, Bagot 2008).
In general, VTE is a disease of senescent with a low incidence of about 1 case per 10,000 person-year in younger people, but rises sharply after the age of 45, reaching 50-60 per 10,000 person-year in people in their 80s (Cushman 2007).
VTE formation can be described as provoked or unprovoked. Provoked VTE is associated with a time-limited risk factor (McLendon 2021). There are a large num-ber of risk factors described that are correlated with an increased prevalence of VTE.

36
Hans JutoStudies of ankle fractures
Among the known or suggested endogenous risk factors are malignancy, obesity, pre-vious VTE, family history of VTE, ethnicity, increasing age, autoimmune disorder and atherosclerosis. Examples of exogenous risk factors are infections, surgery, immobi-lisation, hospitalization, trauma or fracture, oral contraception, and pregnancy (White 2003, Cushman 2007, Heit 2015). There are several hypercoagulation conditions that increase the risk of a VTE. The patient is often unaware that they have the condition.
Illus
tratio
n: Is
abel
le F
orsl
in
Endothelial injury• Surgery
• Fracture
• Trauma
• Indwelling catheterization
• Atherosclerosis
Hypercoagulability• Thrombophilic disorder
• Cancer
• Major trauma
• Sepsis
• Ethnicity
• Autoimmune disorder
• Oral contraceptives
Venous stasis• Obesity
• Immobility
• Cancer
• Pregnancy
• Venous insufficiency
• Varicose veins
Fig 11: Rudolf Virchow and the triad he has given name to. The triad of critical factors in the development of VTE was described after his death.

37Studies of ankle fractures
These include antithrombin deficiency, protein C deficiency and Factor V Leiden mu-tation (McLendon 2021). A combination of underlying and acquired risk factors such as immobilisation can multiply the risk. Ocak et al. showed an increase in VTE OR by 1.7 in major illnesses, 10.9 in a combination of major illnesses and immobilisation and OR in 35-88 if there was also an underlying thrombophilia involved (Ocak 2013).
Through both an orthopaedic injury and fracture as well as the orthopaedic treat-ment, the pathophysiological mechanism behind VTE formation can be affected. Since, an ankle fracture, in some of the cases involves surgical treatment and in most cases a period of immobilisation. This contributes to increasing the risk of a VTE. However, while it is clear that patients with hip fractures as well as total hip and knee replacement should be administered VTE prophylaxis, controversy still exists regarding lower-leg injury (Flevas 2018). The incidence of symptomatic VTE is described as being around 2-3% in both operatively and non-operatively treated injuries below the knee joint level with immobilisation (Zee 2017, Chapelle 2014, Hickey 2018). Pulmonary em-bolism is reported in 0.3-0.7% of cases (Pelet 2012, SooHoo 2009, Lapidus 2013, Zee 2017, Hickey 2018). With asymptomatic VTE also included, the incidence apparently rises. For example, during routine ultrasound, VTE was observed in 28% of cases fol-lowing an ankle fracture, despite a week of low-molecular-weight heparin (LMWH) prophylaxis (Lapidus 2007) and Chapelle et al. reported 7.5% VTE including asymp-tomatic cases (Chapelle 2014).
There is substantial mortality associated with VTE and especially with pulmonary embolism (PE), even if fatality is greatly affected by increasing age and comorbid conditions. In a comprehensive study with approximately 100,000 cases, of all VTEs regardless of genesis, a 30-day mortality rate of deep venous thrombosis (DVT) was reported at 7% and 17% of PE. In another literature review, 6% and 12% mortality, respectively, are reported within 30 days. Both report a strong correlation between mortality and age as well as comorbidity (Tagalakis 2013, White 2003).
Other more common but still serious complications are post-thrombotic syndrome and recurrence of VTE (Leizorovicz 1998). Post-thrombotic syndrome (PTS) is a com-mon complication after DVT that develops in 20-50% of the cases, usually within a couple of years. Patients typically experience pain, cramping, itching, and swelling that worsens with walking and decreases at rest. A more severe form of venous ulceration is seen in between a quarter and a third of patients with PTS. Due to its chronic course, it can mean significant morbidity (Kahn 2004).
Heparin has been used as an anticoagulant for almost a century. Unfractionated heparin (UFH) was isolated in 1916 by Jay McLean and William Henry Howell from liver cells, which gave it its name (McLean 1959). It is produced in basophils and mast
38
Hans JutoStudies of ankle fractures
cells and consists of various glycosaminoglycans that bind to antithrombin (AT). The heparin-AT complex then inactivates coagulation factors such as factor Xa and factor IIa (thrombin). LMWH is produced by depolymerizing UFH where the molecular size is about one third as large as in UFH. LMWH has a more predictable effect and turno-ver in the body and less risk of side effects, which has made it the gold standard for VTE prophylaxis in orthopaedic patients (Flevas 2018).
The use of heparin is unfortunately fraught with some complications. Heparin-in-duced thrombocytopenia (HIT) is a rare but feared complication. It is the most com-mon drug-induced thrombocytopenia and is associated with significant mortality. HIT comes in two distinct forms: type I and type II. Type I is a non-immunological reaction in which heparin and platelets aggregate and produce a mild and transient thrombo-cytopenia. Type II, on the other hand, is an immune-mediated reaction in which heparin binds to platelet factor 4 (PF4). The molecule becomes immunogenic and induces the formation of antibodies that bind to the heparin-PF4 molecule. The heparin-PF4-IgG complex in turn activates platelets and initiates a coagulation cascade that can lead to thrombosis and thrombocytopenia. Despite thrombocytopenia, bleeding is uncommon, but HIT is associated with both venous and arterial thromboembolic events. HIT with thrombosis development is associated with 20-30% mortality and as many patients are left with permanent injuries such as sequela after a stroke and amputation. One to five
Fig 12: LMWH is given subcuta-neously. Tinzaparin is one of the common LMWH drugs used as VTE prophylaxis.
39Studies of ankle fractures
percent of patients receiving UFH develop HIT with thrombocytopenia. When using LMWH, the risk of HIT is reduced by over 90% (Ahmed 2007, Martel 2005).
Another less serious but more common complication is bleeding. A meta-study estimated the incidence of major bleeding to be 1 in 886 doses of LMWH after a foot and ankle trauma compared to 86 treated for each avoided symptomatic DVT (Hickey 2018). In another meta-analysis where LMWH was used as prophylaxis for several diagnoses and the orthopaedic ones accounted for about 5%, an increased risk of blee-ding was found. When using a medium dose of LMWH, one major bleeding was seen per 212 treatments and one avoided symptomatic VTE per 76 treatments (Eck 2019).
Surgical site infectionsSurgical site infections (SSI) are relatively common and in some cases serious compli-cations after surgical treatment of ankle fractures. It is divided into superficial and deep SSI. The frequency of SSI after an ankle fracture surgery is seen in about 7% of the cases, but various studies show a large variation (Shao 2018). Deep infections make up between a quarter and a half of SSI cases (Korim 2014, Saithna 2009, Orvaska 2013, Sun 2017). There are several identified risk factors for SSI that are associated with fracture and the surgical treatment. Fracture-related risk factors for SSI include open fractures, fracture dislocation, high-energy injuries and extended time required of the surgery (Sun 2017, Pincus 2017, Nåsell 2011, Ovaska 2013). A treatment-related factor that is discussed is the timing of the surgery and antibiotic prophylaxis. How widely delayed surgery affects the risk of wound infection and whether we should override the principle of performing the surgical fracture treatment “within 6 hours or after 6 days” (Saithna 2009). While Schepers et al. in a systematic literature review established a clear increased risk of SSI in the event of a delay in surgery, Shao et al. do not see that difference in their meta-analysis (Schepers 2013, Shao 2018).
The scientific support for using antibiotic prophylaxis to reduce the risk of SSI af-ter ankle surgery is somewhat limited. In the pooled results of two recent retrospective studies of univariate analysis, the proportion of SSI is smaller in patients who received perioperative prophylaxis in ankle fracture surgery, but that difference cannot be de-monstrated in their multivariate analysis (Shao 2018, Sun 2017, Sun 2018). Modha et al. showed in a systematic review of studies on antibiotic prophylaxis in elective foot and ankle surgery, a halving of the frequency SSI but at the same time call for new stu-dies of better quality (Modha 2018). For postoperative antibiotic prophylaxis, no effect on the frequency SSI has been demonstrated (Sun 2017, Sun 2018, Lachman 2018).
40
Hans JutoStudies of ankle fractures
Non-union after ankle fractureAnkle fracture non-union was a common complication before the implementation of the principles for stable fixation advocated by AO and the routine use of Open Reduc-tion and Internal Fixation (ORIF) in unstable fractures. It is now described as unusual (Capogna 2016). Bhadra et al. observed in a systematic literature review an incidence of non-union in fibula fracture of between 0.3-5.4% (Bhadra 2012). Risk factors for non-union are similar to those of complications in general. Fracture dislocation, some fracture pattern, high energy injury and malrotation of the distal fibula can also contri-bute to non-union. Common symptoms are pain and tenderness in the fracture area, ankle swelling and, in some cases, even a feeling of instability. Less than 20% of the non-unions were completely asymptomatic and the radiological finding was incidental (Bhadra 2012).
Traditionally, non-union is divided into hypertrophic, oligotrophic, and atrophic based on X-ray image. Roughly speaking, the hypertrophic non-unions, lack of sta-bility but has endogenous conditions for healing, while these are lacking in the atrop-hic non-unions (Capogna 2016). Hypertrophic non-unions were more often seen as symptomatic and painful, while atrophic non-unions were asymptomatic in most cases. Bhadra et al. showed in their review that the most common treatment for non-union is expectation, as most lead to spontaneous healing over time (Bhadra 2012). There is some support for ultrasound and electrical stimulation facilitates healing (Rutten 2007, Simonis 2003). ORIF together with bone grafts is the most commonly described opera-tive intervention. Drilling in the pseudoarthrosis as an isolated measure, bone grafting alone or solely extirpation of smaller distal fibula fragments are all described but the literature is limited supporting advantage of a methods over another (Bhadra 2012).
1.6 OUTCOME AFTER ANKLE FRACTURES
Patients who sustain an ankle fracture often report a good outcome with only a minor disability a year or more after the injury. The outcome after either non-operative or operative treatment for B-type fractures result in a mean score of around 90 out of 100 points, equivalent to an excellent result (Ponzer 1999, Van Schie 2011, Holmes 2016, Van Gerven 2020). However, there are still a substantial number of patients who expe-rience functional impairment after the fracture. Twelve percent of patients with operati-vely treated fractures reported moderate or severe pain a year after injury (Egol 2006).
The recovery in function after the injury is rapid for the first six months and the-reafter slows down. It was demonstrated in a meta-analysis of longitudinal studies that

41Studies of ankle fractures
about 78% of the function score was regained after six months. At 24 months a little further improvement was seen, 87% of the functional score (Beckenkamp 2014).
C-type fractures have been shown to result in a somewhat worse functional outco-me than type A and B fractures (Stufkens 2010, Yap 2020). When comparing the gait pattern after an ankle fracture, it has been seen that bi- and trimallolar fractures had a greater impact than unimalleolar fractures, which in turn showed an effect compared to the control group (Segal 2014).
During arthroscopy in connection with surgery of an ankle fracture, injury to car-tilage surfaces in the joint is often seen (Fuchs 2016). These injuries are in turn associ-ated both with a worse result in the short term but also with an increased frequency of post-traumatic osteoarthritis (Stufkens 2010). Simultaneously, patient-related factors such as gender, being overweight and substance abuse seem to account for a larger share of the variation in patient-reported outcomes compared with the injury itself (Audet 2020).
Early postoperative outcomes after operative fixation of ankle fractures suggest a significantly worse outcome for elderly patients. However, the long-term outcome for these patients were comparable to younger patients (Anderson 2008). In a study of un-stable ankle fractures in older patients, 66 points was reported at follow-up compared to 90 points before injury, which is worse than expected (Willet 2016). A seven-point worse result for each decade of increasing age was also reported (Beckenkamp 2014).
When examining the long-term results of non-operatively treated ankle fractures, a 20-year follow-up showed excellent or good results in 74% of the patients, according to Olerud-Molander Ankle Score (OMAS) and that no patient reported poor outcome (Donken 2011). A similar long-term follow-up with SER type II-IV fractures (equiva-lent to AO type B), showed that 93% of patients reported over 60 points, corresponding to good or excellent results on OMAS. The mean value was 95 points, and no signifi-cant differences were noted between the subgroups on the SER type (Donken 2012).
Sick leaveAn ankle fracture, sustained by a patient of working age, will in many cases result in a period of sick leave as it often is treated with a period of immobilisation, regardless of whether they are managed operatively or non-operatively. Six weeks of immobilisation in a cast has been the standard treatment for most ankle fractures, even if it is now up for debate (Thomas 2009, Dehghan 2016, Kortekangas 2019).
In some cases, the need for sick leave can be extended because of the less favou-rable functional outcome. It is reported that nearly half of the patients were having work-related limitations two years after injury (Ponzer 1999). Fractures of the lower

42
Hans JutoStudies of ankle fractures
leg and ankle usually renders longer spells of sick leave than fractures of the upper extremities (Alexanderson 2004, Lidwall 2011, Lidwall 2014). Some other risk factors however, not related to the injury, have been shown to be associated with higher sick leave in general. For example, gender, age, place of residence, socioeconomic status, and lifestyle can affect sick leave (Allebeck 2004).
About a third of the cost in the Swedish social insurance system is related to mus-culoskeletal disorders. The total cost of an operatively treated ankle fracture was asses-sed in a study. Forty per cent of the cost was derived from sick leave and about the same from hospitalization (Høiness 2002). The impact of sick leave is considerable not only for the society but also on an individual level. This can be seen not only during absence from work, but also after the sick leave as it may reduce future earnings (Marcussen 2012). Short-term sick leave in the Swedish context also seems to increase the risk for future long-term sick leave even adjusted for health status (Hultin 2012).
Posttraumatic osteoarthritisOsteoarthritis of the ankle constitutes only a very small part of all osteoarthritis diag-noses and unlike knee and hip joints, primary osteoarthritis of the ankle is uncommon. Posttraumatic osteoarthritis (PTOA) is described as explaining the majority of cases of symptomatic osteoarthritis of the talocrural joint. It is believed to be due to the biomechanics of the ankle and cartilage characteristics that differ from other joints. Unlike the cartilage in the knee joint, for example, the cartilage in the ankle joint is both thinner and stiffer (Delco 2017).
Valderrabano et al. showed that 78% of painful end-stage ankle osteoarthritis have post-traumatic genesis and only 9% are considered to be primary osteoarthritis. However, the Swedish ankle register estimated that 43% of have the post-traumatic genesis (Valderrabano 2009, Swedankle 2019).
Traumatic injuries leading to PTOA can, in addition to ankle fractures, be isola-ted fractures of the talus, Pilon injuries but also isolated cartilage damage to the talus dome, isolated ligament injuries in the ankle or tibia diaphyseal fractures. Ankle fractu-res account for half of the cases of PTOA (Valderrabano 2009).
Marcera et al. demonstrated that 5% of operated ankle fractures showed radiologi-cal signs of advanced osteoarthritis at a two-year follow-up and SooHoo et al. showed that about 1% of operated ankle fractures leads to re-operation as a result of end stage ostteoarthritis within five years (Marcera 2018, SooHoo 2009). Ankle arthrodesis or ankle prosthesis can be seen as the worst long-term consequence. According to the Swedish Ankle Register, during the period 2015-2019, approximately 65 ankle pro-stheses and 335 ankle arthrodesis were performed in Sweden annually (Swedankle

43Studies of ankle fractures
2019). There is a broad consensus in various studies that the severity of the fracture affects the risk of developing PTOA. Macera et al. did not see any case of PTOA in patients with type A fractures, 5.5% in type B and 13.5% in type C fractures (Macera 2018). Patients with a bimalleolar and especially trimalleolar fracture are at greater risk than patients with a lateral malleolar fracture (SooHoo 2009). Initial cartilage damage seen during arthroscopy, age, female gender and fracture dislocation are other risk factors for the development of osteoarthritis (Stufkens 2010, Lübbeke 2012).
A review of the latency period between injury and the development of end-stage ankle PTOA shows an average time of 21 years with a spread of 1-52 years. The laten-cy period after ankle fracture did not differ compared to a Pilon fracture. However, the severity of the fracture and the patient’s age were seen to be important (Horisberger 2009).
Fig 13: AO/OTA type B ankle fracture and posttraumatic osteoarthritis 11 years after injury.

2
45Studies of ankle fractures
2. AIMS OF THE STUDIES
The overall purpose of this dissertation is to investigate classification, epidemiology, complications and results in order to improve knowledge and management of ankle fractures. The specific aim of each study is stated below.
Study ITo evaluate the degree of accuracy of the AO/OTA-classification in which ankle fractu-res are recorded in the Swedish Fracture Register (SFR).
Study IITo examine the incidence of ankle fractures in Norrbotten county as well as the re-lationship between AO/OTA-classes of ankle fractures and age, gender, and trauma mechanism.
Study IIITo determine the incidence of symptomatic venous thromboembolic event (VTE) among operatively and non-operatively treated ankle fractures registered in the SFR, to investigate the use of low-molecular-weight heparin prophylaxis among the ortho-paedic departments affiliated to the SFR and how different use are associated the inci-dence of VTE.
Study IVTo examine the variations in the length of the sick leave after an ankle fracture and the relationship between the length and the patient reported outcome.

3

47Studies of ankle fractures
3. METHODS
3.1 STUDY DESIGN
The studies in this thesis were all retrospective and non-interventional studies. Study I was a reliability and validation study of fracture classification and study II was an observational classification study of the epidemiology. Study III was designed as a comparative retrospective cohort study and study IV, as a retrospective cohort study.
3.2 DATA SOURCE AND STUDY SUBJECTS
Study IThe patients included in study I, were injured in 2013, with ankle fractures (AO/OTA 44), and randomly selected from the Swedish Fracture Register (SFR). During that year, 3,040 cases of ankle fractures had been registered in the SFR at 17 different ortho-paedic departments. The department registering most ankle fractures reported 657 and
Study Study design Period of inclusion
Study popula-
tion
Measure of exposure Outcome
I Reliability and validation
2013 3,040 Registred AO/OTA classification, treating department
Agreement of classification
II Epidemiologyclassification
2009-2013 196,351 Age, gender, trauma mechanism Number of ankle fractures
and AO/OTA classes
III Retrospectiv cohort 2012-2016 14,954 Department’s use of prophylax-is, AO/OTA classification, age,
gender, earlier medication, ankle fracture treatment, type and length of LMWH-prophylaxis
Diagnosis and/or treatment
of VTE
IV Retrospectiv cohort 2012-2016 8,671 AO/OTA classification, former sick leave, age, gender, ankle fracture
treatment, SMFA-score
Length of sick leave
Table 2. Study design of each paper included in the thesis.
48
Hans JutoStudies of ankle fractures
two at the department registered the fewest. The selected cases of ankle fractures had been treated at 16 different departments. Digitized radiographs of 152 cases of ankle fractures were obtained from the departments.
The radiographs for all except two cases, included at least three standardized views (anteroposterior, mortise and lateral). In several cases there were additional ima-ges (range 2-11) of the ankle and most commonly we received four images (71% of cases). In 26 cases (17%) we also received images of the proximal fibula. In 25 cases (16%) there were only X-rays with casts taken. The registered AO/OTA-classification of these ankle fractures were retrieved from the SFR.
Study IIStudy II was an epidemiological study of ankle fractures in patients 20 years of age of older, during the study period 2009-2013 in Norrbotten county. All hospitals and departments in the county share the same computerized medical record system, VAS (Vårdadministrativt System), where digital radiographs are also available. To identify cases, ICD-10 diagnosis codes for ankle fractures (S82.50-S82.81) were used as well as diagnosis codes for other tibia and fibula fractures (S82.10-S82.41). This because we calculated that there would be some misclassification in the ICD-10 diagnosis re-gistry. Patients with those diagnoses were identified, and medical records and X-rays related to the injury were obtained.
Study IIIFor study III all patients aged 18 years or older in the SFR with a registered ankle fracture between January I, 2012, and June 30, 2016, were included. The dataset from the SFR formed the base and defined the range of the study. To this dataset, data from the Swedish National Patient Register and the Swedish Prescribed Drug Register was crosslinked using the patient’s unique Swedish personal identity number. The combi-nation of data and anonymization was carried out by the administrator of the registers before distributing the data for analysis.
The Swedish National Patient RegisterThe Swedish National Patient Register (NPR) is a mandatory national quality register with the purpose to monitor the development in health over time and contribute to the development in health care. NPR was started in 1964 and is administered by the National Board of Health and Welfare. It includes data from both private and public health caregivers from 2001 regarding diagnosis and surgical treatment from both in and outpatients in specialized care (Socialstyrelsen 2019a).

49Studies of ankle fractures
The Swedish Prescribed Drug RegisterThe Swedish Prescribed Drug Register (SPDR) was established in 2005 and is also administered by the National Board of Health and Welfare. It registers data on all prescribed drugs dispensed at pharmacies and can be used by researchers and public policymakers, to for example, enhance knowledge of the effects and safety of phar-maceuticals. The SPDR is mandatory for all prescribed drugs. The register collects data regarding the patient receiving the prescription (age, gender, city), the drug (ATC code, dose, size of package) and the prescriber (occupation, specialty, hospital etc.) (Socialstyrelsen 2019b).
Study IVThe same SFR dataset used in study III was used in study IV as a base, but it was also combined with data of sick leave and sick pay obtained from the MiDAS-system of the Swedish Social Insurance agency (SSIA). In this study the combination of data was also carried out before the data was distributed and all data were anonymized.
MiDAS - Swedish Social Insurance AgencyThe SSIA administer public social insurance in an event of illness, disability and for families with children. All adult residents in Sweden are insured through the SSIA and will receive compensation if they are unfit to work following an injury or an illness. The first day of the sick leave is not compensated and day benefits between days 2 to 14 are paid for by the employer. Other groups such as the unemployed receive bene-fits from the SSIA from the second day. From day 8, a doctor’s certificate is required (Lidwall 2011).
Data regarding the compensation of illness and injury are obtained from Mi-DAS-register (MicroData for Analysis of the Social Insurance System) at the SSIA. MiDAS was developed with the purpose of simplifying the process of receiving and analysing of data from the social security system (Försäkringskassan 2011).
Table 3. Data source of the included studies. Defining data source determined the inclu-ded cases.
Study Defining data source Complementary data source
I SFR Affiliated departments
II VAS Norrbotten County
III SFR NPR, SPDR, affiliated departments
IV SFR NPR, SPDR, SSIA

50
Hans JutoStudies of ankle fractures
3.3 VARIABLES AND OUTCOME
Study IStudy I was a validity study of classification and besides the registering hospital, the rater and the AO/OTA classification for type and group, no other variables were used. The calculated agreement between the registered classification and the gold standard classification were used as outcome.
Study IIIn study II were validated and classified ankle fractures compared to age, gender, and trauma mechanism. To validate and classify the ankle fractures, X-rays of cases in-cluded were extracted from the system, anonymized, and numbered. Patients who fractured their ankles more than once during the period of the study, or patients with a bilateral ankle fracture were identified. Medical records were examined if patients had an ankle fracture diagnosis recorded in different years, to lower the risk of not detecting multiple injuries.
To obtain information about the trauma mechanism, information in the referral text was mainly used, in some cases complemented with information from medical re-cords. Low-energy trauma was defined as a fall from a standing height or less, with an eventual physical activity not more than walking. The remaining fractures, including sports injuries and falls down stairs, were defined as non-low-energy trauma.
Study IIIStudy III was based on data from the SFR, and the dataset defined the cases included. It also contained data on the patient, the injury, the fracture, and the treatment of the fracture.
Information on all prescriptions of anticoagulants came from the SPDR. Low-mo-lecular-weight heparin (LMWH) was used both as prophylaxis and as treatment for venous thromboembolic events (VTE) and hence used both as an examined variable and outcome. All prescriptions of anticoagulant drugs were examined, and the use of LMWH prophylaxis was defined by the dose, the information of the prescription label and the time in relation to the injury and to an eventual VTE. Information on all pres-criptions of cardiovascular therapy, antidiabetic therapy came from the SPDR. From the NPR data of a cancer diagnosis was used as a variable.
Instead of prescribing LMWH, some orthopaedic departments in Sweden routine-ly distributes syringes of LMWH to patients have been admitted, which could introdu-ce bias to the study. Questionnaires were sent out to all orthopaedic departments which

51Studies of ankle fractures
SFR NPR SPDR (ATC code) Affilliated department
Variables Patient (age, gender)Injury (mechanism)
Fracture (side, AO/OTA-classification, open/closed)
Treatment (operative/non-operative)
Cancer diagnosis Cardiovascular therapyAntidiabetic therapy
Anticoagulants
Routin of LMWH-use in
operatively trea-ted fractures
Outcome VTE diagnosis Treatment VTE
Table 4. Crosstable of included investigated and outcome variables and their origin in study III.
register data on adult ankle fractures in the SFR about the use of LMWH prophylaxis. They were asked whether LMWH as prophylaxis was routinely used on patients with operatively treated ankle fractures and if they had written guidelines. A supplementary question was whether they mainly wrote prescriptions or distributed the syringes to the patients from the ward.
The outcome used was symptomatic VTE within 6 months from the fracture. Ca-ses of a VTE were identified as patients with an ankle fracture registered in the SFR and with an ICD-10 code in the NPR for VTE (I80.1-82.9 and/or I26.0-9). When the information on the prescriptions for an anticoagulant drug clearly stated treatment of VTE, these were also included. Pulmonary embolism (I26.0-9) was considered as a secondary outcome.
Study IVFrom the same dataset used in study III were the SFR data on sex and age, injury mechanism (high or low energy), fracture (AO type and group) and treatment (surgical or non-surgical) received. The modality of the treatment was defined from the first registered treatment in the SFR. Multiple treatments were also used as a variable and defined as more than one treatment registered after an ankle fracture regardless of the type of treatment.
The score of the Short Musculoskeletal Function Assessment (SMFA) questionn-aire was used as a variable to compare with the length of the sick leave. We also chose to use two single questions in the SMFA to further compare the function with the sick leave. The first question was: “How often do you walk with a limp?” The second ques-tion was: “How difficult it is to walk?” The questions in the SMFA can be answered in five grades. For example, questions concerning if one experienced problems can be an-swered with none/little/some/most/all of the time. We dichotomized it to none and little of the time in one group and some/most and all of the time in one group in the question on “how often do you walk with a limp?”. As with the second question, we gathered the
52
Hans JutoStudies of ankle fractures
answers “not at all difficult” and “a little difficult” in one group and moderately/very difficult and unable to do in another group.
In study IV data on sick leave from the SSAI was linked to the combined dataset form the SFR. The starting date of the sick leave, the ICD-10 diagnosis associated with the sick leave, the number of days on sick leave. In the study we needed to define whether the sick leave was related to the ankle fracture or not. We used both the time in accordance with the injury and the registered ICD-10 codes from the SSIA for the definition. Sick leave which started within the period from 14 days before in the date of the injury, registered in the SFR, to 30 days after were considered being related to the ankle fracture. The number of days of the sick leave related to the ankle fracture was then used as an outcome.
Sick leave due to a diagnosis unrelated to the ankle fracture was included in the dataset and was used as an independent variable. Patients with ongoing sick leave with another diagnosis at the time of the injury were excluded since the length of the sick leave related to the injury could not be assessed.
Short Musculoskeletal Function Assessment
The SMFA questionnaire consists of 46 items. It was designed to measure the functio-nal status of patients with a wide range of musculoskeletal injuries and disorders. It can be used to analyse the function of a patient over time or compare the patient with other patients with the same disorder. It is based on the longer, 101-item Musculoskeletal Function Assessment questionnaire. The 46-item SMFA questionnaire comprises of two parts: the dysfunction index with 34 items, which assesses patientsʼ perceptions of difficulties they have in the performance of certain functions. The bother index consists of 12 items, measuring how often the patients have difficulty when performing certain functions.
The dysfunction index can be further divided into four different categories: daily activities, function of the arm and hand, emotional status, and mobility. Each catego-ry’s score is transformed into one of the ranges from 0 to 100, with a low score repre-senting a higher function. Swiontkowski et al. described the questionnaire in 1999 and report excellent internal consistency and stability, content validity, few ceiling effects, and no floor effects (Swiontkowski 1999). The American version of the SMFA was translated and adapted for Swedish use in 2003. It was concluded that the SMFA is easy to use, has good reliability and is sensitive to changes in function (Ponzer 2003).

53Studies of ankle fractures
SFR MiDAS SPDR
Variables Patient (age, gender)Injury (mechanism)
Fracture (side, AO/OTA-classification, open/closed)
Treatment (operative/non-operative)PROM (SMFA score and single question)
Earlier sick leave Cardiovascular therapyAntidiabetic therapy
Outcome Days of sick leave
Table 5. Crosstable of included investigated and outcome variables and their origin in study IV.
3.4 CLASSIFICATION OF FRACTURES
For study I the classification of the fractures included in the study was carried out by a reference group of three observers with different levels of experience. The reference group was presented with the same radiographic images that had been available to the attending doctor at time of the original classification upon registration in the SFR. The three observers independently, at their own pace and without any clinical information, classified the fractures at two occacions, one month apart. The description of the AO/OTA-classification system in the SFR website as well as the AO online surgery referen-ce were available and used as guidelines of the classification in both study I and II. The results of the first classification were sealed. One month later the same three observers repeated the classification of the same cases.
In that case five or six out of six observations corresponded it was regarded as a final result. If the agreement was less, the reference group, discussed the fractures at a meeting until consensus was reached. The classification was then seen as a gold standard classification. It was then, in the final step of the validation process, compared with the classification recorded in the SFR at the various participating departments.
For study II the classification was made in a similar fashion, with a reference group of three but now only once since the purpose was not to achieve a gold standard but rather a high-quality classification. Around 6,000 radiographs of suspected ankle fractures were audited, and cases of ankle fractures classified. The classification was carried out independently by three observers but in this study, we deemed majority opinion as sufficient. In other words, two out of three were enough for a final result. In case of total disagreement, the fracture and the radiographs were discussed at a meeting until a majority decision.

54
Hans JutoStudies of ankle fractures
3.5 COMPLETENESS AND COVERAGE
The data in study III and study IV includes the first years of the Swedish Fracture Re-gister and the coverage and completeness rose as more departments joined the register. The estimated completeness of registered ankle fractures in the SFR for the first year of the study, 2012, was 5% and for the final year, 2016, it was 41%. The mean comple-teness of the contributing departments for all fractures of the extremities for 2018 was calculated to 70% (Socialstyrelsen - 2019c). However, the NPR tends to double-regis-ter and thus overestimate the actual number of fractures. Therefore, is the completeness of the SFR, somewhat higher (Bergdahl 2021). The datasets from the SFR contained about 15,000 ankle fractures for four and a half years. An estimate of the number of ankles fractures during the period would be 65,000 which gives about 23% complete-ness for study III and IV.
The diagnoses retrieved from the NPR were from the period between 2011 and 2017. The NPR started collecting data on inpatient discharge diagnoses in 1964. The coverage of inpatient discharge diagnosis is about 99% with a positive predictive value generally between 85-95%, depending on the diagnosis. Recording of diagnoses for outpatients began in 2001 and the missing data of the main diagnosis is reported to be around 3% (Ludvigsson 2011, Socialstyrelsen 2021).
All medical prescriptions in Sweden have been registered in the Swedish Prescri-bed Drug Register since 2005, as well as information about the date it was dispensed at the pharmacy. Recording of data for all prescribed drugs is mandatory and automated. The loss of data on prescribed drugs is estimated as negligible. However, data on over-the-counter drugs and drugs used at hospitals is not included in the register. Prescribed drugs constitute 84%, and hospital use is 3% of defined daily doses of the total quantity of pharmaceuticals sold in Sweden (Wettermark 2007, Socialstyrelsen 2021).
3.6 STATISTICS
Study IIn study I the statistical analysis was carried out using the IBM SPSS statistical pro-gram, version 23 and inter and intra-observer reliability determined using the Cohen’s kappa statistic. 95% confidence intervals (95% CI) were calculated from kappa value +/- 1.96 * standard error. A sample size analysis was made based on a power of 0.9 and significance level of 0.05. The calculation showed 144 cases were needed. Since a loss of 20% were accounted for 180 cases of ankle fractures were randomly selected form the SFR.
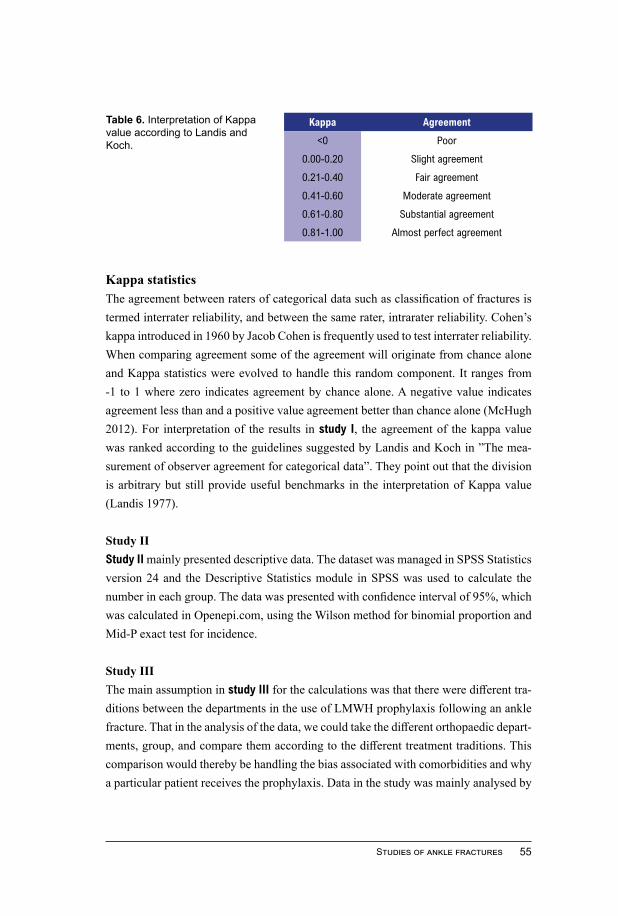
55Studies of ankle fractures
Kappa Agreement
<0 Poor
0.00-0.20 Slight agreement
0.21-0.40 Fair agreement
0.41-0.60 Moderate agreement
0.61-0.80 Substantial agreement
0.81-1.00 Almost perfect agreement
Kappa statisticsThe agreement between raters of categorical data such as classification of fractures is termed interrater reliability, and between the same rater, intrarater reliability. Cohen’s kappa introduced in 1960 by Jacob Cohen is frequently used to test interrater reliability. When comparing agreement some of the agreement will originate from chance alone and Kappa statistics were evolved to handle this random component. It ranges from -1 to 1 where zero indicates agreement by chance alone. A negative value indicates agreement less than and a positive value agreement better than chance alone (McHugh 2012). For interpretation of the results in study I, the agreement of the kappa value was ranked according to the guidelines suggested by Landis and Koch in ”The mea-surement of observer agreement for categorical data”. They point out that the division is arbitrary but still provide useful benchmarks in the interpretation of Kappa value (Landis 1977).
Study IIStudy II mainly presented descriptive data. The dataset was managed in SPSS Statistics version 24 and the Descriptive Statistics module in SPSS was used to calculate the number in each group. The data was presented with confidence interval of 95%, which was calculated in Openepi.com, using the Wilson method for binomial proportion and Mid-P exact test for incidence.
Study IIIThe main assumption in study III for the calculations was that there were different tra-ditions between the departments in the use of LMWH prophylaxis following an ankle fracture. That in the analysis of the data, we could take the different orthopaedic depart-ments, group, and compare them according to the different treatment traditions. This comparison would thereby be handling the bias associated with comorbidities and why a particular patient receives the prophylaxis. Data in the study was mainly analysed by
Table 6. Interpretation of Kappa value according to Landis and Koch.

56
Hans JutoStudies of ankle fractures
comparing the departments grouped according to traditions. The data was divided by treatment method in operatively and non-operatively as well as unknown treatment, and analysis of the data was preformed after this.
Comparing operatively treated ankle fractures was somewhat complicated becau-se of a tradition in some departments of giving the syringes to the patients when they were discharged, instead of writing a prescription. The lack of this data needed to be addressed. We compared data according to how the department stated that they use LMWH-prophylaxis, and this was confirmed by comparing it to data from the SPDR. The incidence of VTE and pulmonary embolism (PE) were compared between de-partments with guidelines stating routine use of LMWH prophylaxis to those without routine use.
Cases of non-operatively treated ankle fractures were compared to the depart-ment’s prescription rate in comparison with the mean rate of the entire study popula-tion. The mean value of the prescription was calculated. The departments were then grouped according to a lower or a higher-than-average use of LMWH. The incidence of both all VTEs (PE, DVT and unspecified VTE) and only PE in non-operative treated ankle fractures was compared between departments with a higher-than-average use of LMWH and departments with a lower-than-average use. Analyses of the period between the injury and the VTE were carried out on the data of the actual prescription of LMWH versus cases without a prescription.
Study IVIn study IV the number of days of sick leave was calculated and used as an outcome. Since the first 14 days of the sick leave is covered by the employer, this was not in-cluded in our data. Hence, patients who had not been on sick leave or on sick leave for 14 days or less were grouped into the same subgroup in the analysis: 0-2 weeks of sick leave.
We calculated both the proportion of patients receiving benefits from the SSAI (15 days or more of sick leave) and the mean time in days of the sick leave. This was then compared between different groups of ankle fracture patients.
We further calculated the difference between the SMFA score of the pre-injury and the 1-year follow-up survey as a value on how the injury had affected the function of the patient. According to the length of the sick leave, patients were placed into groups of four weeks in the analysis and then compared to the mean score of the difference in the SMFA. We also compared the dichotomized answers for the walking and limping questions for both the pre-injury and the 1-year follow-up survey to the length of the sick leave.

57Studies of ankle fractures
IBM SPSS Statistics was used for both study III and IV. For study III 95% confi-dence intervals were calculated using IBM SPSS Statistics version 24 and for study IV IBM SPSS Statistics version 26. It was derived from the custom table module in SPSS. SPSS uses the t-test for comparison of means and the z-test for comparison of propor-tions (IBM 2012). To minimize the risk of bias Directed Acyclic Graphs described by Shrier was used in the design of the statistical model in both study III and IV (Shrier 2008).
Regression analysisA logistic regression model was used for the analysis of variables associated to the odds of VTE in study III, for both operative and non-operative treated cases. The time between the injury and the VTE was compared in patients with and without a LMWH prescription. A logistic regression model was also created in study IV, on variables associated with a longer than the mean of 93 days. The logistic regression models for study III and IV was carried out in IBM SPSS Statistics version 24 and 26 respectively.
3.7 ETHICS
All the studies in this thesis were approved by the Regional Ethics Committee at Umeå University. As all of the studies were based on data from registers and medical records and as there was no involvement by the study participants, personal consent was not obtained.
Data in all studies was anonymized. In study I and II before classifications took place. In study III and IV was the anonymization carried out by the administrators of the registers before data was sent out. Hence this means that once the analysis started there was no possibility adding of new variables.
All data in the thesis and the included studies were presented in aggregated form.

4
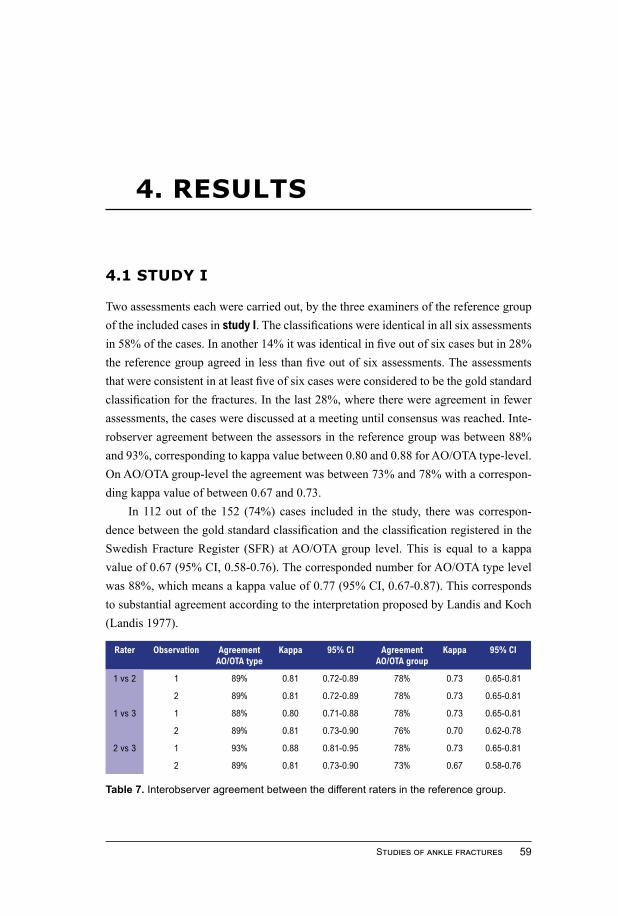
59Studies of ankle fractures
4. RESULTS
4.1 STUDY I
Two assessments each were carried out, by the three examiners of the reference group of the included cases in study I. The classifications were identical in all six assessments in 58% of the cases. In another 14% it was identical in five out of six cases but in 28% the reference group agreed in less than five out of six assessments. The assessments that were consistent in at least five of six cases were considered to be the gold standard classification for the fractures. In the last 28%, where there were agreement in fewer assessments, the cases were discussed at a meeting until consensus was reached. Inte-robserver agreement between the assessors in the reference group was between 88% and 93%, corresponding to kappa value between 0.80 and 0.88 for AO/OTA type-level. On AO/OTA group-level the agreement was between 73% and 78% with a correspon-ding kappa value of between 0.67 and 0.73.
In 112 out of the 152 (74%) cases included in the study, there was correspon-dence between the gold standard classification and the classification registered in the Swedish Fracture Register (SFR) at AO/OTA group level. This is equal to a kappa value of 0.67 (95% CI, 0.58-0.76). The corresponded number for AO/OTA type level was 88%, which means a kappa value of 0.77 (95% CI, 0.67-0.87). This corresponds to substantial agreement according to the interpretation proposed by Landis and Koch (Landis 1977).
Table 7. Interobserver agreement between the different raters in the reference group.
Rater Observation Agreement AO/OTA type
Kappa 95% CI Agreement AO/OTA group
Kappa 95% CI
1 vs 2 1 89% 0.81 0.72-0.89 78% 0.73 0.65-0.81
2 89% 0.81 0.72-0.89 78% 0.73 0.65-0.81
1 vs 3 1 88% 0.80 0.71-0.88 78% 0.73 0.65-0.81
2 89% 0.81 0.73-0.90 76% 0.70 0.62-0.78
2 vs 3 1 93% 0.88 0.81-0.95 78% 0.73 0.65-0.81
2 89% 0.81 0.73-0.90 73% 0.67 0.58-0.76

60
Hans JutoStudies of ankle fractures
In a comparison between the different orthopaedic departments included in the study, the proportion that corresponded between the gold standard classification and the registered classification varied between 62% and 100% at AO/OTA-type level and between 50% and 100% at AO/OTA-group level. Divided by AO/OTA-type, type A fractures have the highest agreement and type C the lowest.
4.2 STUDY II
During the period of the study 2009-2013, 1,851 unique adult patients were identified with at least one ICD-10 diagnosis of ankle fracture (S82.50-S82.81). When reviewing each case, 145 patients were found to be residing outside of the county and another 125 cases were classified from the X-rays, as non-ankle fractures. These cases were exclu-ded. When reviewing patients with an adjacent ICD-10 diagnosis (distal tibia or fibula shaft) an additional 156 ankle fractures in 154 patients were found to be incorrectly diagnosed. Another seven patients had fractured both ankles in the same injury and in eleven cases the patients had sustained another (in one case two more) ankle fractures within the study period. This led to an additional 19 fractures. In total this resulted in
Table 8. Distribution of the classification registered in the SFR and the gold standard classification for each case grouped by AO/OTA group.
Gold standard classificationA1 A21/2 A23 A31/2 A33 B1 B2 B3 C1 C2 C3 NF NP Total
SFR
SFR classifi-cation
A1 21 1 0 0 0 7 2 0 0 0 0 0 0 31
A21/2 0 9 0 0 0 0 0 0 0 0 0 1 0 10
A23 0 0 1 0 0 0 1 0 0 0 0 0 0 2
A31/2 0 0 0 0 0 0 0 0 0 0 0 0 1 1
A33 0 0 0 0 0 0 0 0 0 0 0 0 0 0
B1 2 0 0 0 0 46 6 0 0 1 0 0 1 56
B2 0 0 0 0 0 1 11 5 1 1 0 0 0 19
B3 0 0 0 0 0 0 3 13 0 0 0 0 0 16
C1 0 0 0 0 0 0 1 0 5 0 1 0 0 7
C2 0 0 0 0 0 0 0 0 2 1 0 0 0 3
C3 0 0 0 0 0 0 0 0 1 1 5 0 0 7
NA 0 0 0 0 0 0 0 0 0 0 0 0 0 0
Total GS
23 10 1 0 0 54 24 18 9 4 6 1 2 152
PA 91 90 100 - - 85 46 72 56 25 83 - -
GS: gold standard, PA: percentage of agreement, NF: non-fracture, NA: not able to classify.

61Studies of ankle fractures
1,756 validated adult ankle fractures in 1,735 patients. The incidence of adult ankle fractures in Norrbotten county was calculated to 179 cases per 100,000 person-years during the period of the study.
All ankle fractures were classified according to the AO/OTA-system by type, group, and subgroup. Divided by type 20% were classified as a type A fracture, 66% as a type B and 11% as a type C fracture. The distribution between the subgroups was heavily uneven and B11 was by far the largest subgroup with 28% of the cases. Some subgroups like A31-A33, C12 and C32 had only very few cases.
The incidence increased with age from 92 cases per 100,000 person-years at 30-39 years of age to 238 cases per 100,000 person-years at 60-69 years of age. Men had a much more even distributional incidence throughout their lives than females, with a dip between 30-39 years of age. Among females, the incidence increased from 83 per 100,000 person-years at 30-39 to 319 at 60-69 years.
The incidence of type B fractures increased substantially with age and had a si-milar pattern as ankle fractures in general. From 62 cases at 30-39 years to 158 at 80 years of age and older per 100,000 person-years. The incidence of type A fractures also increased similarly but not as markedly. Type C fractures had a quite even incidence but with a significantly lower incidence at 30-39 and 80 years of age or older.
Patients in the study with an ankle fracture had a mean age of 56 (range 20-101) years and 35% were 65 years of age or older. Fifty-eight per cent of the patients were female and 68% of the trauma causing the fracture was defined as low energy.
Fractures of the right ankle were somewhat more common than on the left side. There was a difference in the frequency of ankle fractures during the year, with the highest incidence in December and the lowest in September.
The infra-syndesmotic type A fractures showed a smaller amount of low-energy
1,851 unique adult patients with ICD-10
ankle fracture diagnosis
1,756 ankle fractures in
1,735 patients
145 patients resident outside
the county
125 other fractures or not
fractures
154 patients with ankle fractures were wrongly diagnosed with other fractures
41 bilataral or muliple fractures were indentified in 20 patients
Fig 14: Flowchart of the process of validating true ankle fractures.

62
Hans JutoStudies of ankle fractures
trauma compared with ankle fractures as a whole. Especially the A21-fracture, the iso-lated medial malleolus fracture, occurred significantly less frequently among females and after low-energy trauma. The trans-syndesmotic type B fractures, which constitu-ted two thirds of the total number of ankle fractures, had a slightly higher and signifi-cant number of low-energy fractures than type A and C fractures. The multi-malleolar type B fractures like B22, B32 and B33 have a somewhat higher frequency of females or/and elderly than unimalleolar. The supra-syndesmotic type C fractures were less common among elderly and female patients than ankle fractures as a whole and had a lower amount of low-energy trauma than type B fractures.
0
50
100
150
200
250
300
350
400
20-29 30-39 40-49 50-59 60-69 70-79 80-
Male Female
0
50
100
150
200
250
300
20-29 30-39 40-49 50-59 60-69 70-79 80-
Type A Type B Type C Total
Fig 15: Incidence of ankle fractures divided by age and AO/OTA type (95% CI).
Fig 16: Incidence of ankle fractures divided by age and sex (95% CI).

63Studies of ankle fractures
0,0%
2,0%
4,0%
6,0%
8,0%
10,0%
12,0%
14,0%
0,0%
2,0%
4,0%
6,0%
8,0%
10,0%
12,0%
14,0%
16,0%
18,0%
20,0%
Monday Tuesday Wednesday Thursday Friday Saturday Sunday
0,00%
10,00%
20,00%
30,00%
40,00%
50,00%
60,00%
Left Right
Fig 17: Side of the ankle fracture (95% CI).
Fig 18: Distri-bution of ankle fractures by day of the week (95% CI).
Fig 19: Dist-ribution of ankle fractures by month (95% CI).

64
Hans JutoStudies of ankle fractures
4.3 STUDY III
In study III 14,954 adult patients with an ankle fracture were included. 7,217 were tre-ated non-operatively, 7,310 operatively and in 427 cases the treatment was unknown.
Of the 30 affiliated departments which responded on our questionnaire, ten of them stated not having any guidelines of routine use of VTE prophylaxis on opera-tively treated patients with ankle fractures. Twelve departments routinely prescribed low-molecular-weight heparin (LMWH) and eight departments routinely distributed the syringes of LMWH for the rest of the treatment period when the patients were discharged.
In the study, 222 cases (1.5%) of VTE were identified within six months following the fracture. Of these, were 125 cases of VTE (1.7%) found in operatively treated patients, 91 cases (1.3%) in non-operatively treated patients, and six (1.4%) cases in patients with unknown treatment. There was only one case of VTE detected within the first two weeks among patients prescribed LMWH, compared to 39 cases among patients without LMWH-prescription.
Among the non-operative treated patients, 13% were prescribed LMWH. This group had higher comorbidity. When comparing lower-than-average using departments to higher-than-average using departments there was less of a difference in comorbidity. Of the operative treated patients, 58% were prescribed LMWH when all departments were included in the analysis.
In the patients treated operatively, there was a lower incidence of VTE treated in departments with guidelines for routine use of LMWH prophylaxis. In these depart-ments, 1.5% of the patients had a VTE compared to 2.6% among patients at depart-ments without routine use of LMWH prophylaxis (OR 0.56, 95% CI, 0.37-0.86).
In the final logistic regression model for the incidence of VTE among non-ope-ratively treated ankle fracture patients, three variables remained significant. A cancer diagnosis, higher age and being treated at a department with a lower-than-average use of LMWH were associated with higher odds of VTE. No other explanatory variable included in the model was significant. The final logistic regression model for the in-cidence of VTE among operatively treated ankle fractures contained two significant variables. Treatment for cardiovascular disease and being treated at a department with a guideline of routine use of LMWH were associated with lower odds. No other expl-anatory variable included in the model was significant.

65Studies of ankle fractures
Fig 20: Number of VTE-cases weeks after injury in patients with or without LMWH-prophylaxis prescription. All departments, 9,622 cases without and 5,332 cases with LMWH-prescription were included.
OR 95% CI
Increasing age (per year) 1.02 1.00-1.03
Malignancy diagnosis 11.6 2.5-54
Treatment at department with higher than mean use of LMWH
0.60 0.39-0.92
Table 9. Logistic regression with variables associated with VTE among non-operatively treated ankle fractures. Non-significant variables in the model were: gender, cardio-vas-cular drug, diabetes mellitus, AO/OTA type, complex injury (multiple/open/bilateral), other anticoagulant before injury, prescription of LMWH prophylaxis and length of LMWH prophylaxis.
OR 95% CI
Cardiovascular drug prescription 1.78 1.22-2.59
Treatment at department with routinely use of LMWH
0.56 0.37-0.86
Table 10. Logistic regression with variables associated with VTE among operatively treated ankle fractures. Non-significant variables in the model were: age, gender, malig-nancy diagnosis, diabetes mellitus, AO/OTA type, complex injury (multiple/open/bilateral fracture), other anticoagulant before injury, prescription of LMWH prophylaxis and length LMWH prophylaxis.
05
1015202530354045
1-2
3-4
5-6
7-8
9-10
11-1
213
-14
15-1
617
-18
19-2
021
-22
23-2
425
-26
without LMWH prescription
with LMWH prescription

66
Hans JutoStudies of ankle fractures
All included cases
Non-operatively treated cases Operatively treatment Unknown treatment
All non-operatively
treated cases
Depart-ments
with lower than mean precrip-tions (a)
Depart-ments with
higher than mean precriptions
(a)
All ope-ratively treated cases
LMWH use
after risk evalua-tion (b)
Routi-nely use LMWH
(b)
Unknown guideline
(b)
Number 14,954 7,217 3,487 3,730 7,310 1,143 5,460 707 427
Contributing departments,
(c)
33 33 17 16 33 8 22 3 29
Women 60 (59-60)
62 (60-63)
63 (61-64)
61 (59-62)
58 (56-59)
57 (54-60)
58 (56-59)
58 (54-61)
60 (55-64)
Age, mean in years
55 (55-56)
57 (57-57)
58 (57-59)
56 (56-57)
54 (53-54)
54 (53-55)
53 (53-54)
55 (54-56)
54 (52-56)
AO/OTA type A
24 (24-25)
41 (39-42)
39 (38-41)
42 (40-43)
9 (8-10)
10 (8-12)
9 (8-10)
7 (5-9)
18 (14-21)
AO/OTA type B
63 (62-64)
55 (54-56)
56 (54-57)
54(53-56)
71 (70-72)
69 (67-72)
71 (70-73)
72 (68-75)
64 (59-68)
AO/OTA type C
12 (11-12)
3 (3-4)
4 (3-4)
3 (2-4)
20 (19-20)
20 (18-22)
19 (18-20)
20 (18-24)
18 (14-21)
Open fractures
1.8 (1.6-2.0)
0.4 (0.2-0.5)
0.3 (0.2-0.6)
0.4 (0.2-0.6)
3.1 (2.7-3.5)
3.1 (2.3-4.3)
3.1 (2.7-3.6)
3.0 (1.9-4.4)
3.3 (1.9-5.3)
Cardiovasku-lar drug
41 (41-42)
44 (42-45)
45 (44-47)
42 (40-44)
39 (38-40)
41 (38-43)
39 (38-40)
39 (36-43)
41 (36-46)
Diabetes 9 (9-10)
10 (10-11)
11 (10-12)
10 (9-11)
8 (8-9)
9 (7-11)
8 (8-9)
8 (6-10)
11 (8-14)
Malignancy 1.1 (1.0-1.3)
0.2 (0.1-0.3)
0.2 (0.1-0.4)
0.2 (0.1-0.3)
2.0 (1.7-2.4)
2.1 (1.4-3.1)
2.0 (1.7-2.4)
2.3 (1.4-3.6)
1.2 (0.4-2.5)
LMWH prescription
36 (35-36)
13 (12-14)
8 (7-9)
18 (17-19)
58 (56-59)
20 (17-22)
66 (64-67)
56 (53-60)
46 (42-51)
Distribution LMWH type
(d)
25/10/1/1
9/3/0/0
4/2/1/1
15/3/0/0
39/17/2/1
7/9/2/1
43/20/2/1
55/1/1/0
35/8/3/1
Length prophylaxis,
mean in days
16 (15-16)
19 (18-20)
21 (18-25)
18 (17-19)
15 (14-15)
23 (21-26)
14 (14-14)
14 (13-16)
18 (16-20)
VTE 1.5 (1.3-1.7)
1.3 (1.0-1.5)
1.6 (1.2-2.1)
0.9 (0.7-1.3)
1.7 (1.4-2.0)
2.6 (1.8-3.7)
1.5 (1.2-1.8)
2.0 (1.1-3.2)
1.4 (0.6-2.9)
PE 0.2 (0.1-0.3)
0.2 (0.1-0.3)
0.1 (0.1-0.3)
0.2 (0.1-0.4)
0.2 (0.1-0.3)
0.3 (0.1-0.8)
0.1 (0.1-0.3)
0.3 (0.1-0.9)
0.5 (0.1-1.5)
VTE among non-
prescrip-tion(e)
1.4 (1.2-1.7)
1.2 (1.0-1.5)
1.6 (1.2-2.0)
0.9 (0.6-1.3)
1.8 (1.4-2.3)
2.7 (1.8-3.9)
1.6 (1.1-2.2)
0.3 (0.0-1.5)
0.9 (0.2-2.8)
VTE among prescrip-tion(e)
1.6 (1.3-2.0)
1.5 (0.9-2.4)
2.3 (1.0-4.6)
1.2 (0.6-2.3)
1.6 (1.3-2.1)
2.2 (0.9-4.8)
1.4 (1.1-1.9)
3.3 (1.8-5.4)
2.0 (0.7-4.7)

67Studies of ankle fractures
Table 11. Demography, characteristics, and amount of VTE according to treatment and use of LMWH. Values are proportions in percent (95% CI) unless otherwise specified.
a Cases in departments grouped by the departments prescription rate in accordance with the total mean of 13%.b Cases in departments grouped according to guideline of LMWH use.c Number of different departments contribution with cases to the subgroup.d Distribution of drug and dosage of LMWH (Dalteparin 5000 IU/Tinzaparin 4500 IU/Enoxaparin 4000 IU/other) counted for the whole group of patients included. e VTE among cases with or without prescription of LMWH.

68
Hans JutoStudies of ankle fractures
4.4 STUDY IV
There were 8,671 patients included in the study and 4,679 (54%) of them received benefits from the Swedish Social Insurance Agency (SSIA). The average period of sick leave was 93 (SD 96) days, 1,362 (16%) patients were on sick leave for more than three months and 386 (4%) for more than six months.
In the group of operatively treated patients with an ankle fracture, 63% received sick pay from the SSIA. The mean length of sick leave was almost four weeks longer than among the non-surgically treated patients. In both groups, sick leave was longer in cases with a more severe fracture. Both a higher level of AO/OTA classification as well as open fracture and multiple treatments were associated with a longer period of sick leave.
Patients on earlier sick leave unrelated to the ankle fracture during the 5-year study period, needed sick leave following the ankle fracture to a greater extent. The period of the sick leave among these patients was also longer. The earlier sick leave was mainly caused by psychiatric (25%) and musculoskeletal diagnoses (35%).
A correlation could be seen between the length of sick leave and the patient-repor-ted outcome. In patients on sick leave for a shorter period, a difference in outcome of 3-6 points was reported between the one-year follow-up survey and the pre-injury sur-vey in nearly every sub-index of the SMFA. These differences increased significantly with the length of sick leave and rose from between 4 and 7 points to between 15 and 21 points in the bother index and the dysfunction subindices apart from the arm/hand subindex. These differences were more noticeable for difficulty walking and how often the patients limped. Except for the group with an episode of sick leave of two weeks or less, only 1-3% reported ”moderate/very difficult” or ”unable to walk” at the time before the injury. In the one-year follow-up survey, this rose to 4% in the patients on sick leave for 2-5 weeks and to 28% in the patients on sick leave for 22 weeks or more. Similarities were seen regarding how often the patients limped, 4-8% reported ”lim-ping some/most” or ”all of the time” in the pre-injury survey. This rose to 25% among patients with an episode of sick leave for 2-5 weeks and 64% among the patients on sick leave for 22 weeks or more.
In a logistic regression model, the odds of being on sick leave for longer than the mean of 93 days increased in patients with a more serious fracture, with increasing age as well as with earlier sick leave. Females had longer periods of sick leave than men but in the logistic regression model this was not significant.

69Studies of ankle fractures
Bother index Dysfunction index
Mobility subindex
Emotional subindex
Daily activity subindex
Arm/hand subindex
Weeks of sick leave
Count Mean 95% CI
Mean 95% CI
Mean 95% CI
Mean 95% CI
Mean 95% CI
Mean 95% CI
0-1 939 5 3-6 4 3-5 7 6-8 6 4-7 4 3-5 1 0-1
2-5 196 3 2-5 3 2-4 6 4-8 4 3-6 3 2-4 0 0-0
6-9 533 6 4-7 5 4-5 7 6-9 7 6-8 4 3-5 0 0-1
10-13 361 9 8-11 7 6-8 11 9-12 11 9-13 6 5-8 0 0-1
14-17 135 12 9-15 10 8-12 14 11-16 15 11-18 9 7-11 1 0-2
18-21 51 12 7-18 12 8-15 17 12-22 17 12-22 11 7-16 1 0-2
22 or more
117 18 15-22 15 12-18 20 17-24 21 17-25 15 12-19 2 1-4
Table 12. Difference in the mean score between pre-injury and the one-year follow up survey of the SMFA grouped by the length of sick leave in weeks.
Fig 21: Number of patients and length of sick leave following an ankle fracture. Patients with sick leave for less than two weeks are not included.
Non-operative treated Operative treated
Count >14 days (%)
95% CI Mean 95% CI Count >14 days (%)
95% CI Mean 95% CI
All 4,040 44 42-45 73 70-77 4,393 63 62-64 100 85-115 Gender
Male 1,742 43 41-45 68 64-73 2,117 62 59-64 98 93-103 Female 2,298 45 43-47 77 72-82 2,276 65 63-66 110 104-116
Age under 36 years 961 44 40-47 65 59-71 1,155 61 58-63 91 84-98
36-50 years 1,170 47 44-50 77 71-84 1,331 69 67-72 106 99-113 over 50 years 1,909 42 40-45 75 70-79 1,907 61 58-63 114 107-120
AO/OTA-classification
A 1,681 37 35-39 68 60-75 367 62 57-67 85 74-94 A1 1,369 36 33-38 64 56-72 80 65 54-75 73 64-82
A2 247 43 37-49 83 62-105 236 62 56-68 85 70-99
A3 65 40 29-52 67 48-87 51 59 45-72 101 81-121
B 2,190 50 47-52 76 72-80 3,022 62 60-64 104 99-109 B1 2,090 50 48-52 75 71-79 869 63 60-65 91 85-96
B2 71 44 33-55 101 68-135 385 60 56-64 103 95-112
B3 29 41 25-60 97 40-155 618 62 59-65 123 113-134
C 115 40 31-49 87 66-107 975 67 64-70 112 104-120 C1 76 34 24-45 76 52-101 248 67 63-72 103 92-114
C2 9 44 17-75 127 0-283 180 69 63-74 125 105-145
C3 30 53 36-70 94 52-135 224 65 60-70 111 96-126
Earlier sick leave on other diagnosis
No 3,077 39 38-41 67 63-70 2,007 58 57-60 99 94-103 Yes 963 59 56-62 88 80-96 761 81 78-83 119 111-127
Open fracture
No 4,026 44 43-46 73 70-77 4,311 63 62-65 103 100-107 Yes 14 50 26-74 60 26-93 82 54 43-64 170 113-227
Multiple treatments
No 3,913 43 42-45 72 68-75 3,838 63 61-64 99 95-103 Yes 127* 61 53-70 108 89-127 555 65 61-69 143 126-161
Table 2. Number of patients with sick leave for more than 14 days and among them the mean time of the sick leave in days. Grouped according to treat-ment, gender, age of the patient, fracture classification, any earlier sick leave, open fracture, and multiple treatments.
Figure 2. Number of patietens and length of the sick leave after an ankle fracture. Patients with no sick leave or sick leave shorter than 2 weeks were not included in the bar chart.
0100200300400500600700800900
1000

70
Hans JutoStudies of ankle fractures
Non-operatively treatment Operatively treatment
Count >14 days (%)
95% CI Mean 95% CI Count >14 days (%)
95% CI Mean 95% CI
All 4,040 44 42-45 73 70-77 4,393 63 62-64 100 85-115
Gender
Male 1,742 43 41-45 68 64-73 2,117 62 59-64 98 93-103
Female 2,298 45 43-47 77 72-82 2,276 65 63-66 110 104-116
Age
20-35 years 961 44 40-47 65 59-71 1,155 61 58-63 91 84-98
36-50 years 1,170 47 44-50 77 71-84 1,331 69 67-72 106 99-113
51 years or older 1,909 42 40-45 75 70-79 1,907 61 58-63 114 107-120
AO/OTA classification
A 1,681 37 35-39 68 60-75 367 62 57-67 85 74-94
A1 1,369 36 33-38 64 56-72 80 65 54-75 73 64-82
A2 247 43 37-49 83 62-105 236 62 56-68 85 70-99
A3 65 40 29-52 67 48-87 51 59 45-72 101 81-121
B 2,190 50 47-52 76 72-80 3,022 62 60-64 104 99-109
B1 2,090 50 48-52 75 71-79 869 63 60-65 91 85-96
B2 71 44 33-55 101 68-135 385 60 56-64 103 95-112
B3 29 41 25-60 97 40-155 618 62 59-65 123 113-134
C 115 40 31-49 87 66-107 975 67 64-70 112 104-120
C1 76 34 24-45 76 52-101 248 67 63-72 103 92-114
C2 9 44 17-75 127 0-283 180 69 63-74 125 105-145
C3 30 53 36-70 94 52-135 224 65 60-70 111 96-126
Previous sick leave with other
diagnosis
No 3,077 39 38-41 67 63-70 2,007 58 57-60 99 94-103
Yes 963 59 56-62 88 80-96 761 81 78-83 119 111-127
Open fracture
No 4,026 44 43-46 73 70-77 4,311 63 62-65 103 100-107
Yes 14 50 26-74 60 26-93 82 54 43-64 170 113-227
Multiple treatments
No 3,913 43 42-45 72 68-75 3,838 63 61-64 99 95-103
Yes* 127 61 53-70 108 89-127 555 65 61-69 143 126-161
Table 13. Number of patients on sick leave for more than 14 days and, among them, the mean period of sick leave in days. Grouped according to treatment, gender, age of the patient, fracture classification, any earlier sick leave, open fracture and multiple treatments
*The first registered treatment defining non-surgical or surgical treatment.

71Studies of ankle fractures
OR 95% CI
Increasing age (per year)
1.02 1.01-1.02
Sick leave other diagnosis
1.91 1.66-2.20
Open fracture 2.21 1.24-3.92
AO/OTA type
A1 0.67 0.51-0.89
A2 0.92 0.67-1.28
A3 1.46 0.82-2.62
B1 ref ref
B2 1.52 1.20-1.93
B3 1.85 1.51-2.29
C1 1.45 1.10-1.93
C2 2.28 1.66-3.15
C3 1.51 1.12-2.02
Not classifiable 1.64 0.82-3.26
Non-operative treatment
ref ref
Operative treatment
1.94 1.62-2.32
Unknown treatment
2.03 1.37-3.02
Single treatment ref ref
Multiple treatment
2.42 1.96-2.99
Difficulty walking Often limp
Number of weeks of sick leave
Count Pre-injury PROM
95% CI One-year PROM
95% CI Pre-injury PROM
CI 95% One-yearPROM
95% CI
0-1 939 8 6-10 16 13-18 14 12-17 33 30-36
2-5 196 2 1-5 4 2-7 4 2-8 25 19-31
6-9 533 2 1-4 6 5-9 7 5-9 32 28-36
10-13 361 3 2-5 10 8-14 5 3-8 39 35-45
14-17 135 1 0-4 17 11-24 8 4-13 53 45-62
18-21 51 0 - 24 14-26 6 2-15 53 40-66
22 or more
117 1 0-4 28 20-37 8 4-15 64 55-72
Table 14. Proportion of patients stating in their answer to the SMFA question of how difficult it is to walk “moderate”, “very difficult” or “unable to”. The proportion in their answer to the question of how often the patient limps answering, “some of the time”, “most of the time” or “all of the time”. The proportion stated in percent of both the pre-injury and the one-year PROM with 95% confidence interval divided by the length of sick leave.
Table 15. Result of the logistic regression analysed with variables associated with an increasing odds of sick leave for longer than the mean of 93 days.
Non-significant variables in the model were: gender, month of the injury, left/right side.

5

73Studies of ankle fractures
5. DISCUSSION
5.1 ACCURACY OF CLASSIFICATION IN THE SWEDISH FRACTURE REGISTER
For data in a register to be reliable for future research, the ingoing data must be as ac-curate as possible. Therefore, it needs to be continuously validated. In the structure of Swedish Fracture Register (SFR), an incident of injury results in one or more fractures which result in one or more treatments. As further data is largely based on a classified fracture and treatment and outcome linked to the specific group or subgroup of the fracture, it is of great importance that this classification is as correct as possible. There are several difficulties in this. The classification itself is not clearly binary and there are elements of the classifications process where the boundaries between groups are vague. Furthermore, the assessments in most cases are carried out with the information of ordinary conventional X-rays. Hence, are there limited possibilities to assess all bony processes and other parts of the skeleton. In addition, the classifications are made, by doctors with varying degrees of orthopaedic experience and fracture classification.
The aim of study I was to investigate the accuracy of the registered classification of ankle fractures by comparing it of a randomly selected sample of ankle fractures from the SFR with a created gold standard classification for the same sample. Gold standard classifications were achieved by strictly using the guidelines of the AO/OTA classification and performing classifications independently six times on each fracture and if necessary, discussing until consensus was reached.
In Study I we observed a general agreement between the gold standard classifica-tion and the registered classification in the SFR of 88% equivalent to a kappa value of 0.77 on AO/OTA type level. On AO/OTA group level the agreement was 74% equi-valent to a kappa of 0.67. This corresponds to a substantial agreement according to Landis and Koch (Landis 1977). Even though many different doctors with a wide range of experience performed the actual classification recorded in the SFR, the agreement is as high as, or even higher than, the interobserver agreement in the previous studies
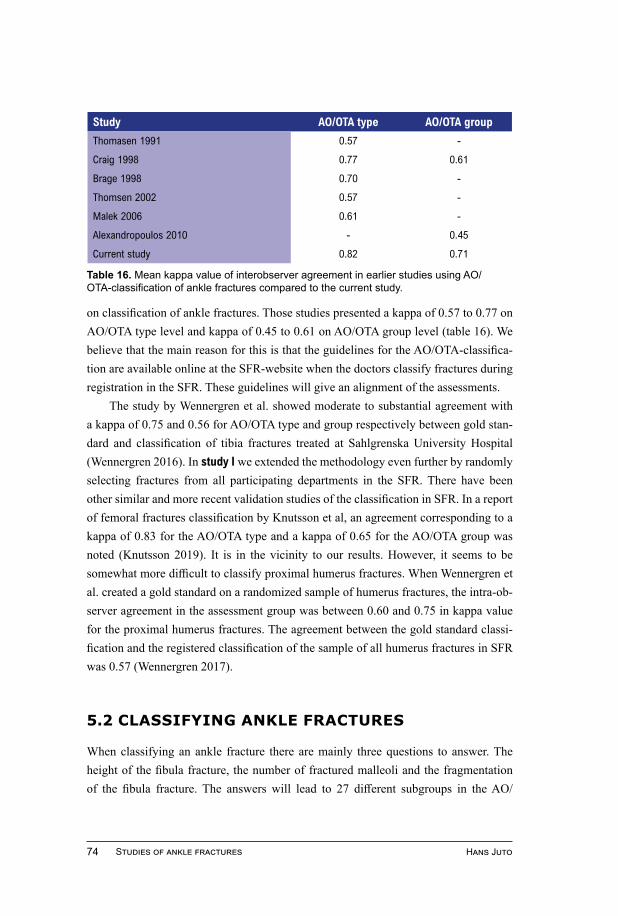
74
Hans JutoStudies of ankle fractures
on classification of ankle fractures. Those studies presented a kappa of 0.57 to 0.77 on AO/OTA type level and kappa of 0.45 to 0.61 on AO/OTA group level (table 16). We believe that the main reason for this is that the guidelines for the AO/OTA-classifica-tion are available online at the SFR-website when the doctors classify fractures during registration in the SFR. These guidelines will give an alignment of the assessments.
The study by Wennergren et al. showed moderate to substantial agreement with a kappa of 0.75 and 0.56 for AO/OTA type and group respectively between gold stan-dard and classification of tibia fractures treated at Sahlgrenska University Hospital (Wennergren 2016). In study I we extended the methodology even further by randomly selecting fractures from all participating departments in the SFR. There have been other similar and more recent validation studies of the classification in SFR. In a report of femoral fractures classification by Knutsson et al, an agreement corresponding to a kappa of 0.83 for the AO/OTA type and a kappa of 0.65 for the AO/OTA group was noted (Knutsson 2019). It is in the vicinity to our results. However, it seems to be somewhat more difficult to classify proximal humerus fractures. When Wennergren et al. created a gold standard on a randomized sample of humerus fractures, the intra-ob-server agreement in the assessment group was between 0.60 and 0.75 in kappa value for the proximal humerus fractures. The agreement between the gold standard classi-fication and the registered classification of the sample of all humerus fractures in SFR was 0.57 (Wennergren 2017).
5.2 CLASSIFYING ANKLE FRACTURES
When classifying an ankle fracture there are mainly three questions to answer. The height of the fibula fracture, the number of fractured malleoli and the fragmentation of the fibula fracture. The answers will lead to 27 different subgroups in the AO/
Table 16. Mean kappa value of interobserver agreement in earlier studies using AO/OTA-classification of ankle fractures compared to the current study.
Study AO/OTA type AO/OTA group
Thomasen 1991 0.57 -
Craig 1998 0.77 0.61
Brage 1998 0.70 -
Thomsen 2002 0.57 -
Malek 2006 0.61 -
Alexandropoulos 2010 - 0.45
Current study 0.82 0.71

75Studies of ankle fractures
OTA-classification system. In study II all identified ankle fractures were classified on a subgroup level. However, the subgroup classification is seldom used. The SFR uses the group level with nine options with the exception for A2 and A3 which are split into subgroups for clarification. Together with the option “not able to classify”, the SFR ends up with 12 possible options.
In the different fracture groups, there seems to be different difficulties in classify-ing correctly. A certain pattern of the misclassifications can be found. The A1-group seems to be difficult to differentiate from the B1-group rather than from the rest of type A-fractures. In contrast, the B2 and B3 fractures seems to be more closely “related” to each other and less likely to be misclassified as type A or C.
Consequently, we detected three areas of difficulties when classifying ankle fractu-res according to the AO/OTA-classification system. First, the level of the fibula fractu-re that differentiates between type A and type B fractures. In study I, 2 cases of A1 fractures had been misclassified as B1 fractures and 7 cases of B1 fractures had been misclassified as A1 fractures. It might be helpful to consider the trauma mechanism as described by Lauge-Hansen and this is also included in the AO/OTA-classification system (Tartaglione 2015). Accordingly, not only the level but also the pattern of the fibula fracture differentiates between a type A and a type B fracture. Type A (i.e., A13) is a transverse fracture due to an avulsion to the fibula and type B is an oblique fracture as a result of an external rotation or twisting force to the distal fibula.
Secondly, a difficulty arises when the number of fractured malleoli in type B fractures are taken into consideration. In both medial and posterior malleoli fractures is it somewhat difficult to determine when you should label a small fragment a malleolus fracture or a ligament rupture with a small bony avulsion. This is probably the reason for misclassification of several B2 fractures as B3 fractures and vice versa.
The third difficulty is to differentiate between C1- and C2-fractures. The division is between a simple and a multi fragmented fibula fracture. In our experience this is often challenging to perceive on plain radiographs. However, type C fractures only constitute roughly 10% of all ankle fractures. Therefore, no obvious pattern of misclas-sification could be detected.
In general, both study I and the other validation studies show a substantial accura-cy, which we interpret as that the classification in SFR can be considered reliable for further research. The question whether how adequately we can classify fractures will possibly be obsolete in the not-too-distant future when interpretations of fractures car-ried out by computers with the help of Artificial Intelligence will yield higher quality assessments (Berg 2017).

76
Hans JutoStudies of ankle fractures
5.3 EPIDEMIOLOGY
The intention of study II was to in detail and with high validity examine the epide-miology of ankle fractures. The study shows an incidence of 179 ankle fractures per 100,000 person-years in the Norrbotten county. In comparison to former and similar studies, it presents a slightly higher incidence. The incidence of ankle fractures has been reported as between 71 and 187 per 100,000 person-years (Bengnér 1986, Daly 1987, Court-Brown 1998, Jensen 1998, Thur 2012, Elsoe 2016). Different presuppo-sitions and methodology make it, obviously, difficult to make a completely identical comparison.
One reason for a higher incidence in study II is that many of the previous studies are twenty or thirty years old and there is an agreement that there has been a rise in the incidence of ankle fractures in the last decades. Elsoe et al. quite recently published a register-based epidemiology study of 9,767 ankle fracture in Denmark, reporting an in-cidence of 169 per 100,000 person-years (Elsoe 2016). In Norrbotten county the mean age of the population is a few years higher than Sweden’s general population. Adjusted for this age difference, our results are very similar to those of Elsoe et al. and it seems that this is the accurate incidence for the period of the study and the region.
Study II showed that one third of the adult ankle fracture patients in the study were 65 years or older. It also showed an increase in incidence from the age of 30–39 to the age of 60–69. This rise in incidence is almost totally caused by the nearly four times rise among women, whereas men have a more even incidence throughout their lives. A similar pattern of incidence was shown, but with a decreasing trend among men (Elsoe 2016).
Another factor that could explain a higher incidence is the long winter season in the county. The incidence increases markedly in the beginning and in the end of the winter, when the average temperature is around zero degrees Celsius, resulting in icy and slippery roads and pavements. Our data shows an increase in incidence during the weekend, implying a general increase in activity. This was expected and is also worth considering. Another difference was that more people had a fracture on the right side of the foot. It is a small but significant difference. This may be associated with most people being right footed.

77Studies of ankle fractures
5.4 OSTEOPOROSIS AND THE ANKLE FRACTURE
There is an ongoing discussion regarding whether ankle fractures should be characteri-sed as an osteoporotic fracture or not (Bengnér 1986, Seeley 1991, Kannus 1996, Kanis 2001, Valtola 2002, Hasselman 2003, Stone 2003, Guggenbuhl 2005, Court-Brown 2006, Stein 2011, FitzGerald 2012, Lee 2013, Biver 2015, Elsoe 2016). Since a fractu-re is one of the major risk factors for another fracture this is not without importance (Johnell 2005). Fragility fractures are characterized in a high proportion of woman, low-energy trauma and an incidence increasing along rising age (Valtola 2002, Kannus 1996). The proportion of low-energy trauma with a fall from standing height or less, was seen in two-thirds of the cases in this study. Thur et al. report similar proportions, but in comparison to earlier studies it is slightly higher (Thur 2012, Court-Brown 1998, Elsoe 2016).
The increase of incidence with age is shown in a number of previous studies where the highest incidence in females occurs after the age of 65 (Thur 2012, Court-Brown 1998, Elsoe 2016). Furthermore, one study has also more recently shown an associa-tion between lower bone mineral density and ankle fractures (Biver 2015).
It is difficult to explain the pattern with the rising incidence among women both by age and time, without considering it as being due to loss of strength of the bone. However, when using a definition of a fragile fracture due to low-energy trauma in an elderly person, they only constitute around one out of four fractures (Elsoe 2017, Kan-nus 2002). With a prominent component of osteoporosis as cause of the fracture, this would contradict the plateau in incidence reached after 60 years of age.
Study II shows some differences between the different classes of ankle fracture in the amount of low-energy trauma, gender, and age. At one end of the spectrum there are the multimalleolar trans-syndesmotic ankle fractures corresponding to B22–3 and B3 representing about every fifth ankle fracture. These occur in female patients in about three-quarters of the cases and are caused by low-energy trauma in 70% of cases. It is difficult not to see bone fragility, at least partly, as a cause of this.
At the other end of the spectrum, we found type A21 fractures and C fractures. A21 is equivalent to an isolated medial malleolus fracture and shows clear signs of being a non-osteoporotic fracture. It is the only subgroup in our population that stands out and has a low proportion of elderly people; caused in a majority of the cases by a non-low-energy trauma and the patients are mainly men. This is also in agreement with earlier studies (Thur 2012, Court-Brown 1998, Briet 2017).
The suprasyndesmotic type C ankle fracture has been described as less of an oste-oporotic fracture with a lower mean age and a lower frequency of low-energy trauma

78
Hans JutoStudies of ankle fractures
(Court-Brown 1998, Jensen 1998). Sakaki et al. demonstrate in their study in São Paulo of surgically treated ankle fractures with a high amount of high-energy trauma that type C fractures compose about 37% of the fractures. More than half of them were high-en-ergy traffic accidents (Sakaki 2014). Briet et al. show in a similar study that all Lau-ge-Hansen classes except supination external rotation fractures is, in a majority of the cases, caused by high energy trauma (Briet 2017). In our population, type C fractures show a similar pattern with fewer elderly females and low-energy trauma. However, low-energy trauma is still the cause of over 60% of type C fractures and still one out of four patients are 65 years of age and older.
Compared with Thur et al., we see a lot of similarities in the incidence pattern, except for two major differences. One is the decrease in incidence of bimalleolar and trimalleolar fractures after 70 years of age in their study. This can be due to the fact that type C is included in that category. The other difference is that the incidence of lateral malleolar fractures is very low. Our incidence of these is about 2–3 times higher, probably because their study only included inpatients.
Guggenbuhl et al. conclude that osteoporosis is not a major contributor to ankle fractures in women. Biomechanical factors seem to play a greater role than bone loss (Guggenbuhl 2005). It is a conclusion that is possibly somewhat reducing the signi-ficance of osteoporosis. A fracture is the result of an interaction between the type of trauma, the bone’s ability to maintain its integrity and the amount of energy to which it is exposed. We see almost a quadrupling of the incidence in women between 30 and 60 years. The increase in incidence could be explained in two ways. It can be explained by the fact that there is an increased risk of falling at the age of 60 compared to the age of 30 and/or the bone has a poorer ability to withstand energy. Since we do not see the increase in incidence among men which support the hypothesis that a poorer bone qu-ality is of importance for the increase in incidence. On the other hand, ankle fractures seem to be typically an outdoor fracture which restrain the incidence over a certain age.
5.5 VENOUS THROMBOEMBOLISM AS A COMPLICATION FOLLOWING AN ANKLE FRACTURE
Low-molecular-weight heparin (LMWH) prophylaxis prescribed to patients with ope-ratively treated ankle fractures is not controversial, however there is still an ongoing discussion on the benefit of the use. All departments in study III used LMWH prophy-laxis to some extent and most of the departments used it as a routine. The main research

79Studies of ankle fractures
questions in this study were if the routine use of LMWH prophylaxis would result in a reduction in the amount of venous thromboembolic events (VTE) compared to the use of a risk evaluation in operatively treated patients with ankle fractures. One third of the departments in the study responded that they use individual risk evaluations to decide if prophylaxis should be given. We observed that when comparing these departments to departments routinely using LMWH, there was a substantial reduction of incidence of VTE with an OR of 0.56, in favour of the departments routinely use. The results are similar to those presented by Zee et al. of VTE among operatively treated injuries to the lower leg (Zee 2017). Departments without guidelines of routine use of LMWH pres-cribed to a higher degree extended time prophylaxis. This strengthens the conclusion that there were mainly patients with risk factors or perceived risk factors for VTE who were prescribed LMWH in these departments.
The use of LMWH prophylaxis in patients with non-operatively treated ankle fractures is still controversial and, in our study, only 13% of non-operative treated patients were prescribed LMWH prophylaxis. Those who received prophylaxis had a higher number of comorbidities compared to patients without prophylaxis. Hence, it appears as if LMWH prophylaxis is mainly used after a risk assessment.
In the non-prophylactic group, there were more AO/OTA type A fractures. A type A fracture is not always treated with a cast and therefore probably at less risk of VTE. We do not see any effect in the logistic regression that a non-operatively treated AO/OTA type B or C would increase the risk of a VTE compared to an AO/OTA type A.
It was a remarkably pronounced difference in incidence between the higher- and the lower-than-mean using departments despite the difference in use of LMWH was only 8% vs 18%. This still gave a difference of 1.6% vs 0.9% of VTE and an OR of 0.58. It can be compared with an OR 0.31 in the combined result of five studies between intervention and control groups of LMWH in patients with lower limb injury (Zee 2017). Our result showed a substantial risk reduction with only a slightly higher use of LMWH. Our interpretation is that a wider use of prophylaxis in non-operative treated patients with ankle fractures and risk factors of VTE has an effect and is plau-sible.
An important finding was that patients who received prescription of prophylax-is but still developed VTE had a later onset of the VTE compared to those without prescription. Interestingly, there was only one VTE in the first two weeks in the group with prescription. Since the most common duration of prophylaxis was 10 days, this of course suggests that during that time the patients have considerable protection against VTE. There are still a substantial number of cases of VTE during the following weeks. Lapidus et al. compared one week and six weeks of prophylaxis in a randomised con-

80
Hans JutoStudies of ankle fractures
trolled trial and could not show any significant difference in asymptomatic DVT inci-dence (Lapidus 2007). With 228 patients, this study might have been underpowered to show a difference. In the logistic regression the extended LMWH prophylaxis did not affect the incidence of VTE. This was not expected either. In this context, long-term prophylaxis should be seen as a sign of the treated patient having risk factors of VTE. When interpreting the data of study III, the question still emerges if prophylaxis after an ankle fracture, especially an operatively treated, should be longer than ten days.
The use of LMWH can cause adverse effects that must be considered. In stu-dy III we have not investigated the complications following use of LMWH. However, bleeding and heparin-induced thrombocytopenia are well known and serious but rare complications (Eck 2019, Ahmed 2007). A doubling of minor adverse effects between patients with LMWH prophylaxis and those without has been reported and Hickey et al. showed that one major bleeding occurred in every ten avoided symptomatic DVTs (Hickey 2018, Zee 2017). Even if we show, in concurrence with earlier studies, that there is a substantial reduction of VTE among patients with prophylaxis there is still a question of risk and cost versus benefits. The reduction of diagnosed VTE by half but from a rather low level against the very rare but serious complications of the use of LMWH.
5.6 OUTCOME AND SICK LEAVE AFTER ANKLE FRACTURES
In study IV, we examined sick leave following an ankle fracture analysing data from the Swedish Social Insurance Agency in combination with data of the SFR. We saw a correlation that a more severe ankle fracture resulted in a longer sick leave and that patients with longer sick leaves report significantly worse outcome.
Among patients in our study with operatively treated fractures, 63% received sick pay from the SSIA for a mean period of 100 days. This can be compared to patients in a study from Norway where 54% received sick pay for 53 days (Høiness 2002). In non-operatively treated patients in the study, 44% received sick pay and the mean time was shorter. Both Port et al. and Ryd et al. demonstrated an average period of sick leave of six weeks for non-operatively treated isolated lateral malleolus fractures (Port 1996, Ryd 1992). With adjustments for the lack of information on sick leave for the first two weeks, our data would be very close to the data reported by Port et al. and Ryd et al.
Non-operatively treated patients have a sick leave to a lesser degree than opera-tively treated patients and in case of a sick leave is it shorter. Stable ankles fracture is

81Studies of ankle fractures
most often treated non-surgically with in many cases a shorter period of immobilisa-tion. This is especially the case among A1 fractures, which are more comparable with an ankle sprain. The non-operatively treated group of fractures constituted nearly 90% of the cases of a stable AO/OTA unimalleolar type A1 or B1 fracture. The outcome of these fractures is also expected to be superior.
The proportion of patients on sick leave decreased rapidly after two months. After three months only twelve per cent of patients were still receiving sick pay. In a study from Finland of both operatively and non-operatively treated ankle fractures, the aver-age period of sick leave was eleven weeks. A rapid decrease was seen after two months and proximately 90% were back at work within four months after the fracture injury (Tunturi 1983).
Among the operatively treated patients, there was an increase in the period of sick leave with increasing severity of the fracture type. This resembles what we know from previous studies about the outcome following an ankle fracture (Yap 2019, Stuftens 2010). Also, within the type A- and B-fractures, we could further see an increasing period of sick leave with bi- and trimalleolar fracture patterns, as compared to unimal-leolar fractures. This is also accordant with what is expected and the results of Segal et al. (Segal 2014). In type C fractures, the simple group C1 fracture correspondingly renders a shorter sick leave need than the multi-fragmented C2 fracture. We can only find limited data in earlier studies on the severity of the ankle fracture relating to the length of the sick leave. Tunturi et al. could not see any significant difference in the duration of sick leave after an ankle fracture by radiological end-result, patients’ age, fracture type or form of treatment (Tunturi 1983).
When evaluating the score of the Short Musculoskeletal Function Assessment (SMFA), there was a clear correlation as to the length of the sick leave. With the ex-ception of the arm and hand-subindex, the rest of the dysfunction subindices, as well as in the bother index showed a close resemblance. Egund et al. showed a similar result in a study on sick leave after distal radius fracture (Egund 2020). For the respondents of the 1-year SMFA-questionnaire, 13% reported at least moderate difficulties with walking and 36% reported that they limped some/most or all of the time. This finding was also strongly correlated to the length of the sick leave. There was a near linear relationship between the number of weeks of sick leave and the difficulties reported for walking with the exception of patients with short or no sick leave at all. It is of course reasonable that there is a relationship between a more severe fracture, a longer period of sick leave and a less favourable outcome. Still, the pronounced relationship was slightly surprising.
The length of the sick leave on an individual level is a much more complicated

82
Hans JutoStudies of ankle fractures
issue than just a reflection of the severity of the injury. Earlier studies have found an association between symptoms of employment grade and adjustment disorder, such as preoccupations with both the functional outcome after injury as well as the amount of long sick leave spells (Weimert 2020, Fuhrer 2002). In study IV we found that if the patients had a previous sick leave period due to another diagnosis, the need for sick leave following the ankle fracture was much higher, and the length of sick leave is also longer. The predisposition of longer sick leave spells among patients with a history of earlier sick leave can both reflect the physical and psychological requirement of the pa-tient’s work itself but also the patient’s vulnerability and response to illness and injury.
When managing sick leave after injury in patients with longer periods of sick le-ave, the question arises if the length of the sick leave is a result of the vulnerability of the patient or from a less favourable result after the ankle fracture. In study IV we show that there is at least an obvious relationship between the severity of the ankle fracture, how the patients grade the function after one year and the length of sick leave.
5.7 STRENGTHS AND LIMITATIONS
Study ISome limitations can be seen in study I. Both the coverage and completeness were somewhat meagre as the data in this study was from the earlier years of the SFR. Only 15 departments were included in the study and the majority of cases were from a few of them.
Another possible limitation of the study is that all observers work in the same department leading to a potential bias. The high interobserver agreement could be af-fected by this but it is somewhat contradicted by the high intraobserver agreement.
Study IIA major strength of study II is that we believe we have found almost every possible an-kle fracture in the county during the period of study and validated them by examining and classifying every case. However, the population of the county in the far north of Europe is relatively small. It can be questionable whether it is possible to generalize the results. Another weakness is that it is a quite low interobserver agreement of the subgroup level of the AO/OTA classification of ankle fracture that can affect the results in the smaller subgroups (e.g., A32 and A33). Even though we have worked rigorously to find all fractures there may be scenarios where we have missed cases. For example, if a patient is injured outside the county without follow-up visit to the local hospital.

83Studies of ankle fractures
Study IIIThere are obvious limitations of study III. The study design is a non-randomized re-trospective study. The reason for comparing departments instead of patients with and without prescriptions was to try to overcome the risk of bias in the comparison. Patients with prescriptions of LMWH were substantially sicker and would have a greater risk of developing a VTE. By comparing departments with departments this risk of bias was limited. It is unlikely that this risk would covary with the traditions in the use of LMWH.
One major weakness is the tradition in some departments of handing out patients syringes of LMWH when the patient is discharged. Therefore, parts of our data are less valid. Furthermore, we did not have data on known risk factors like obesity, physical status, family history of VTE or oral contraception. Another limitation, as this was a register study, was that we had no information on how the diagnosis of VTE in each case was carried out. We believe that the quality of the included data of diagnosed VTE is quite high, especially considering that we used both information from registered diagnosis as well as prescribed treatments to find cases of VTE.
The main strength of study III is the extent of the variables included in the data from the SFR and by combining the other registers with high quality data. This makes it possible to detect quite rare but very serious events like VTE in everyday ortho-pae dic settings. The large number of contributing departments in the SFR strengthen the external validity and gives the possibility of examining different treatment tradi-tions. Previously published meta-analyses show significant effects but have included different diagnoses and different treatment methods. The individual studies included in these meta-analyses, on the other hand, have a more defined study group but often the sample size is too small to be able to show a significant effect.
Study IVWe see some limitations of this study. The response rate to the 1-year follow-up survey and the patient-reported outcome measure is fairly low. Older women were the best re-sponders and younger men were less likely to respond to the questionnaires. However, an earlier validation study has shown that there were no signs of different results in patients who did not participate in the 1-year follow up (Juto 2017). A major obstacle in the study is the lack of data from the first two weeks of sick leave, because this period is paid for by the employer. Furthermore, we did not have data about the employment and what type of work it involved, which will surely affect the length of the sick leave.

6

85Studies of ankle fractures
6. CONCLUSIONS
Study IThere is a substantial agreement between classifications made in the SFR and the gold standard classification. The finding is equivalent to or higher than in previous studies. Consequently, we conclude that classifications of ankle fractures in the SFR are ac-curate and valid.
Study IIThe study shows an incidence of 179 adult ankle fractures annually per 100,000 per-sons. More than two thirds of the fractures were caused by a low-energy trauma and ankle fractures are more frequent among females. Females generally have an increa-sed incidence during their life, mainly between the ages of 30 and 60, in contrast to men who have more of an even distribution throughout their life. Multimalleolar type B-fractures were mainly found in women as a result of a low energy trauma in contrast to A21-fractures which were mainly found in younger men.
Study IIIRoutine use of LMWH in patients with operatively treated ankle fractures was associ-ated with a lower incidence of VTE. A more frequent use of LMWH among patients with non-operatively treated ankle fractures was associated with a lower incidence of VTE. The onset occurred later among patients with LMWH-prophylaxis who still suffered a VTE.
Study IVThere is a relationship between the severity of the injury and the length of sick leave following an ankle fracture, as well as between the patient-reported outcome after one year and the length of the sick leave.

7

87Studies of ankle fractures
7. FUTURE PERSPECTIVES
The ankle fracture is one of our most common fractures and there are still a significant number of questions surrounding it, where knowledge needs to be elaborated. This dis-sertation only scrapes the surface of some issues regarding ankle fractures. However, in several of the studies presented in the dissertation, we point to the possibilities with the considerable amount of data that the Swedish Fracture Register (SFR) offers.
In study I, we examined the accuracy of the classification of ankle fractures in the SFR. Several similar validations have been made e.g. on fractures of the tibia, femur and humerus. These largely show a similar result. Even if the classification is not per-fect, it is not inferior to what the classification system itself allows and is thus also reliable. On the other hand, there are probably still other areas of the register in need of further review. An example is the patient’s reported outcome. Since there is still a limited and not an optimal response rate, additional validation studies could contribute to raising the quality of data from the register.
When study II of ankle epidemiology began, the coverage of SFR was somewhat limited. Thus, it was chosen to only focus on a region’s own data to obtain a high-qua-lity material. As completeness and coverage now reach good or even excellent levels, it provides favourable opportunities to study the epidemiology of different fractures with data from the SFR.
In study III, we present a substantial material on patients with venous throm-boembolic event (VTE) after ankle fracture. However, it is retrospective material with all its shortcomings. Our data and results correspond with the existing meta-studies. Low-molecular-weight heparin (LMWH) seems to have a important effect in reducing the number of cases of VTE. However, the studies create several supplementary ques-tions; for example, which groups of patients have a significant benefit from LMWH prophylaxis in relation to the risk of complications and cost of treatment and for how long the prophylaxis should be used.
The SFR collects considerable amounts of data even out of relatively unusual fractures, with a cover over both time and area that would not be possible or immensely laborious to assemble in any other way. This should bring great opportunities to answer

88
Hans JutoStudies of ankle fractures
several questions when it comes to treatments, by utilizing differences in treatment traditions between different hospitals. A concern in, for example a treatment strategy, where there is no consensus will probably also have differences in the way it is hand-led. Several subgroups of ankle fractures or other fractures should be studied with a combination of data from SFR together with data from national patient data registers and possibly complemented with data from clinics, such as X-rays.
However, many questions will not be able to be answered with retrospective stu-dies, but large prospective studies are needed. In the case of VTE, the difficulty is visible. All randomized trials so far have been too small to answer several of the basic questions for us to be able to make a sensible risk-benefit analysis. It is difficult to extrapolate results from other studies, but we probably need to examine this particular group. To really answer these important questions, we would need to have a large enough and comprehensive prospective study with the possibility of subgrouping the patients.
A registry-based randomized clinical trial (R-RCT) gives great opportunities, but the effort and the costs are still high and consequently the number of research questions possible to undertake are limited. An important concern to answer is which fracture-related uncertainties can be answered with retrospective studies based on register data and in which questions is a R-RCT needed. There are many questions concerning the treatment of ankle fractures that would need further examination and where there should be possibilities to do it retrospectively. For example, where to draw the line between non-operative and operative treatment in several of AO subgroups such as A21, the isolated medial malleolar fractures. Also, how far certain patient groups whe-re the risk of complication is high could and should be treated with other methods than the classic AO osteosynthesis with plate and screws.
As the moderate response rate to patient-reported outcome measure (PROM) in the SFR, is a limiting circumstance other complementary approaches of evaluating the outcome could be favourable. In study IV was the length of sick leave used with interesting results. There was a great deal of agreement between the severity of the fracture, the PROM and the length of the sick leave. To obtain data on sick leave is itself revealing and contributes to understanding but it can probably also be used as an outcome variable in fracture related research. It is possibly a slightly imprecise measu-rement, nevertheless the advantage is that data on sick leave for longer than two weeks is of high quality. Also, the response rate is especially low among younger adults and hence, in this group it can complement this gap.

89Studies of ankle fractures

8

91Studies of ankle fractures
8. ACKNOWLEDGEMENTS
Den här avhandlingen har blivit till tack vare hjälp från många olika personer runt mig. Mina kollegor, medarbetare och chefer på Ortopeden i Norrbotten men även syskon, föräldrar och vänner som med uppmuntran och stor hjälp stöttat mig igenom med- och motgångar sedan jag tog mig an att börja med en forskarutbildning. Jag vill tacka er alla. Det är dock några som jag särskilt vill nämna:
Min huvudhandledare Per Morberg, som varit ett tryggt stöd genom hela arbetet och alltid ställt upp med tid för råd, bollande av idéer och diskussioner, nästan oavsett tid på dygnet och var än han har befunnit sig. Alltid positiv, kunnig och lösningsorienterad.
Mina bihandledare, Michael Möller och Magnus Hultin som med uppmuntran och många goda och kunniga råd lotsat mig framåt. Båda är personer med imponerade arbets kapacitet, kunskap och systematik.
Mina medförfattare, Klas Edin, Ida Apelqvist, David Wennergren och Helena Nils-son för ert arbete med insamling och tolkning av data, hjälp med manus och kloka kommentarer.
Robert Lundqvist, vår statistiker vid Region Norrbotten som alltid kunnat svara på stora som små frågor och gett mig verktyg att hantera de problem som har dykt upp.
Tarquin Shepherd, min engelskspråkiga korrekturläsare som har lagt ned ett hästjobb med att få min bitvis lite bristfälliga engelska att bli läsbar.
FoI-enheten Region Norrbotten som utan knorrande har finansierat min forskarut-bildning även fast den dragit ut lite på tiden.
Min tålmodiga och fantastiska fru Anna som både hjälpt till med manusarbetet och korrekturläsning men förstås även gjort det möjligt att få tid och utrymme att göra färdigt alla arbeten.
Mina underbara döttrar Elin och Tyra som på sina charmiga sätt hjälpt till att inte låta mig sitta ensam alltför länge åt gången.
Elisabet, Kjell och Karin som varit en enorm källa till kunskap och hjälp som jag fått ta del av under hela resan.

9

93Studies of ankle fractures
9. REFERENCES
1. Ahmed I, Majeed A, Powell R. Heparin induced thrombocytopenia: diagnosis and management update. Postgraduate Medical Journal 2007;83:575-82.
2. Aitken SA, Johnston I, Jennings AC, Chua ITH, Buckley RE. An evaluation of the Herscovici classification for fractures of the medial malleolus. Foot Ankle Surg 2017;23:317-320.
3. Alexanderson K, Norlund A. Swedish Council on Technology Assessment in Health Care (SBU). Chapter 1. Aim, background, key concepts, regulations, and current sta-tistics. Scand J Public Health Suppl. 2004;63:12-30.
4. Alexandropoulos C, Tsourvakas S, Papachristos J, Tselios A, Soukouli P. Ankle fracture classification: an evaluation of three classification systems: Lauge-Hansen, A.O. and Broos-Bisschop. Acta Orthop Belg 2010;76:521-5.
5. Allebeck P, Mastekaasa A. Swedish Council on Technology Assessment in Health Care (SBU). Chapter 5. Risk factors for sick leave - general studies. Scand J Public Health Suppl 2004;63:49-108.
6. Anderson SA, Li X, Franklin P Wixted JJ. Ankle fractures int the elderly; initial and long-term outcomes. Foot Ankle Int 2008;29:1184-8.
7. Arimoto HK, Forrester DM. Classification of ankle fractures; an algorithm. Am J Roentgenol 1980;135:1057-63.
8. Audet MA, Benedick A, Breslin MA, Schmidt T, Vallier HA. Determinants of func-tional outcome following ankle fracture. OTA Int 2020;4:e139.
9. Bagot CN, Arya R. Virchow and his triad: a question of attribution. Br J Haematol 2008; 143:180-90.
10. Bartonícek J. Anatomy of the tibiofibular syndesmosis and its clinical relevance. Surg Radiol Anat.2003;25:379-86.
11. Beckenkamp PR, Lin CW, Chagpar S, Herbert RD, van der Ploeg HP, Moseley AM. Prognosis of physical function following ankle fracture: a systematic review with meta-analysis. J Orthop Sports Phys Ther 2014;44:841-51.
12. Beerekamp MSH, de Muinck Keizer RJO, Schep NWL, Ubbink DT, Panneman MJM, Goslings JC. Epidemiology of extremity fractures in the Netherlands. Injury 2017;48:1355-1362.

94
Hans JutoStudies of ankle fractures
13. Belmont PJ Jr, Davey S, Rensing N, Bader JO, Waterman BR, Orr JD. Patient-Based and Surgical Risk Factors for 30-Day Postoperative Complications and Mortality Af-ter Ankle Fracture Fixation. J Orthop Trauma 2015;29:e476-82.
14. Benedick A, Audet MA, Vallier HA. The effect of obesity on post-operative compli-cations and functional outcomes after surgical treatment of torsional ankle fracture: A matched cohort study. Injury 2020;51:1893-98.
15. Bengnér U, Johnell O, Redlund-Johnell I. Epidemiology of ankle fracture 1950 and 1980. Increasing incidence in elderly women. Acta Orthop Scand 1986;57:35-7.
16. Berg HE. Will intelligent machine learning revolutionize orthopedic imaging? Acta Orthop 2017;88:577.
17. Bergdahl C, Nilsson F, Wennergren D, Ekholm C, Möller M. Completeness in the Swedish Fracture Register and the Swedish National Patient Register: An Assessment of Humeral Fracture Registrations. Clin Epidemiol 2021;13:325-33.
18. Bhadra AK, Roberts CS, Giannoudis PV. Nonunion of fibula: a systematic review. Int Orthop 2012;36:1757-65.
19. Biver E, Durosier C, Chevalley T, Herrmann FR, Ferrari S, Rizzoli R. Prior ankle fractures in postmenopausal women are associated with low areal bone mineral den-sity and bone microstructure alterations. Osteoporos Int 2015;26:2147-55.
20. Bourne M, Sinkler MA, Murphy PB. Anatomy, Bony Pelvis and Lower Limb, Tibia. Treasure Island (FL): StatPearls Publishing; 2021.
21. Brage ME, Rockett M, Vraney R, Anderson R, Toledano A. Ankle fracture classifi-cation: a comparison of reliability of three X-ray views versus two. Foot Ankle Int 1998;19:555-62.
22. Briet JP, Houwert RM, Smeeing DPJ, Dijkgraaf MGW, Verleisdonk EJ, Leenen LPH, Hietbrink F. Differences in classification between mono- and polytrauma and low- and high-energy trauma patients with an ankle fracture: a retrospective cohort study. J Foot Ankle Surg 2017;56:793–6.
23. Brockett CL, Chapman GJ. Biomechanics of the ankle. Orthop Trauma 2016;30:232-238.
24. Broos PL, Bisschop AP. A new and easy classification system for ankle fractures. Int Surg 1992;77:309-12.
25. Campbell KJ, Michalski MP, Wilson KJ, Goldsmith MT, Wijdicks CA, LaPrade RF, Clanton TO. The ligament anatomy of the deltoid complex of the ankle: a qualitative and quantitative anatomical study. J Bone Joint Surg Am 2014;96:e62.
26. Capogna BM, Egol KA. Treatment of Nonunions After Malleolar Fractures. Foot An-kle Clin 2016;21:49-62.
27. Chapelle C, Rosencher N, Jacques Zufferey P, Mismetti P, Cucherat M, Laporte S; Meta-Embol Group. Prevention of venous thromboembolic events with low-molecu-lar-weight heparin in the non-major orthopaedic setting: meta-analysis of randomized controlled trials. Arthroscopy 2014;30:987-96.

95Studies of ankle fractures
28. Corrigan JD, Bogner JA, Mysiw WJ, Clinchot D, Fugate L. Systematic bias in outcome studies of persons with traumatic brain injury. Arch Phys Med Rehabil. 1997;78:132-7.
29. Court-Brown CM, Caesar B. Epidemiology of adult fractures: a review. Injury 2006;37:691–7.
30. Court-Brown CM, McBirnie J, Wilson G. Adult ankle fractures – an increasing pro-blem? Acta Orthop Scand 1998;69:43-7.
31. Craig WL 3rd, Dirschl DR. Effects of binary decision making on the classification of fractures of the ankle. J Orthop Trauma 1998;12:280-3.
32. Cummings SR, Melton LJ. Epidemiology and outcomes of osteoporotic fractures. Lancet 2002;359:1761-7.
33. Cushman M. Epidemiology and risk factors for venous thrombosis. Semin Hematol 2007;44:62-9.
34. Daly PJ, Fitzgerald RH Jr, Melton LJ, Ilstrup DM. Epidemiology of ankle fractures in Rochester, Minnesota. Acta Orthop Scand 1987;58:539-44.
35. Dauwe J, Nijs S, Gueorguiev B, Richards RG. In Memoriam : Robert Danis, an in-spiration for Maurice Müller and origins of the AO Foundation. Acta Orthop Belg 2020;86:577-9.
36. Dehghan N, McKee MD, Jenkinson RJ, Schemitsch EH, Stas V, Nauth A, Hall JA, Ste-phen DJ, Kreder HJ. Early Weightbearing and Range of Motion Versus Non-Weight-bearing and Immobilization After Open Reduction and Internal Fixation of Unstable Ankle Fractures: A Randomized Controlled Trial. J Orthop Trauma. 2016;30:345-52.
37. Delco ML, Kennedy JG, Bonassar LJ, Fortier LA. Post-traumatic osteoarthritis of the ankle: A distinct clinical entity requiring new research approaches. J Orthop Res 2017;35:440-53.
38. Dodson NB, Ross AJ, Mendicino RW, Catanzariti AR. Factors affecting healing of ankle fractures. J Foot Ankle Surg 2013;52:2-5.
39. Donken CC, Goorden AJ, Verhofstad MH, Edwards MJ, van Laarhoven CJ. The out-come at 20 years of conservatively treated ’isolated’ posterior malleolar fractures of the ankle: a case series. J Bone Joint Surg Br 2011; 93:1621-5.
40. Donken CC, Verhofstad MH, Edwards MJ, van Laarhoven CJ. Twenty-one-year fol-low-up of supination-external rotation type II-IV (OTA type B) ankle fractures: a retrospective cohort study. J Orthop Trauma 2012;26:e108-14.
41. Ebraheim NA, Taser F, Shafiq Q, Yeasting RA. Anatomical evaluation and clinical importance of the tibiofibular syndesmosis ligaments. Surg Radiol Anat 2006;28:142-9.
42. Eck RJ, Bult W, Wetterslev J, Gans ROB, Meijer K, Keus F, van der Horst ICC. Intermediate Dose Low-Molecular-Weight Heparin for Thrombosis Prophylaxis: Sys-tematic Review with Meta-Analysis and Trial Sequential Analysis. Semin Thromb Hemost 2019;45:810-24.

96
Hans JutoStudies of ankle fractures
43. Egol KA, Tejwani NC, Walsh MG, Capla EL, Koval KJ. Predictors of short-term functional outcome following ankle fracture surgery. J Bone Joint Surg Am 2006;88: 974-9.
44. Egund L, Önnby K, Mcguigan F, Åkesson K. Disability and Pain are the Best Predictors of Sick Leave After a Distal Radius Fracture in Men. J Occup Rehabil 2020;30:656-64.
45. Elsoe R, Ostgaard SE, Larsen P. Population-based epidemiology of 9767 ankle fractu-res. Foot and Ankle Surg 2016;24:34-9.
46. FitzGerald G, Boonen S, Compston JE, Pfeilschifter J, LaCroix AZ, Hosmer DW Jr, Hooven FH, Gehlbach SH; GLOW Investigators. Differing risk profiles for individual fracture sites: evidence from the Global Longitudinal Study of Osteoporosis in Wo-men (GLOW). J Bone Miner Res 2012;27:1907-15.
47. Flevas DA, Megaloikonomos PD, Dimopoulos L, Mitsiokapa E, Koulouvaris P, Mav-rogenis AF. Thromboembolism prophylaxis in orthopaedics: an update. EFORT Open Rev 2018;3:136-48.
48. Fojtík P, Kostlivý K, Bartoníček J, Naňka O. The fibular notch: an anatomical study. Surg Radiol Anat 2020;42:1161-6.
49. Fonseca LLD, Nunes IG, Nogueira RR, Martins GEV, Mesencio AC, Kobata SI. Re-producibility of the Lauge-Hansen, Danis-Weber, and AO classifications for ankle fractures. Rev Bras Ortop 2017;53:101-6.
50. Fox A, Wykes P, Eccles K, Barrie J. Five years of ankle fractures grouped by stability. Injury 2005;36:836-41.
51. Fuchs DJ, Ho BS, LaBelle MW, Kelikian AS. Effect of Arthroscopic Evaluation of Acute Ankle Fractures on PROMIS Intermediate-Term Functional Outcomes. Foot Ankle Int 2016;37:51-7.
52. Fuhrer R, Shipley MJ, Chastang JF, Schmaus A, Niedhammer I, Stansfeld SA, Gold-berg M, Marmot MG. Socioeconomic position, health, and possible explanations: a tale of two cohorts. Am J Public Health 2002;92:1290-4.
53. Försäkringskassan [The Swedish Social Insurance Agency]. MiDAS – Sjukpenning och Rehabiliteringspenning. Mars 2011. Availabel at: https://www.forsakringskassan.se/wps/wcm/connect/f1e0dce5-e310-4d6d-8076-d4493534c10b/MiDAS_Sjukpen-ning_och_rehabiliteringspenning_version_1_02.pdf?mod=ajperes.
54. Gardner MJ, Demetrakopoulos D, Briggs SM Helfet DL, Lorich DG. The ability of the Lauge-Hansen classification to predict ligament injury and mechanism in ankle fractures: an MRI study. J orthop Trauma 2006;20:267-72.
55. Gluud LL. Bias in clinical intervention research. Am J Epidemiol 2006;163:493-501.
56. van Gerven P, Krijnen P, Zuidema WP, El Moumni M, Rubinstein SM, van Tulder MW, Schipper IB, Termaat MF; WARRIOR Trial Study Group. Omitting Routine Radiography of Traumatic Ankle Fractures After Initial 2-Week Follow-up Does Not Affect Outcomes: The WARRIOR Trial: A Multicenter Randomized Controlled Trial. J Bone Joint Surg Am 2020;102:1588-99.

97Studies of ankle fractures
57. Guggenbuhl P, Meadeb J, Chalès G. Osteoporotic fractures of the proximal humerus, pelvis, and ankle: epidemiology and diagnosis. Joint Bone Spine 2005;72:372-5.
58. Gupton M, Munjal A, Kang M. Anatomy, Bony Pelvis and Lower Limb, Fibula. Tre-asure Island (FL): StatPearls Publishing; 2021.
59. Gunnes M, Mellström D, Johnell O. How well can a previous fracture indicate a new fracture? A questionnaire study of 29,802 postmenopausal women. Acta Orthop Scand 1998;69:508-12.
60. Hasselman CT, Vogt MT, Stone KL, Cauley JA, Conti SF. Foot and ankle fractures in elderly white women. Incidence and risk factors. J Bone Joint Surg Am 2003;85: 820-4.
61. Heit JA. Epidemiology of venous thromboembolism. Nat Rev Cardiol 2015;12: 464-74.
62. Hermans JJ, Beumer A, de Jong TAW, Kleinrensink G-J. Anatomy of the distal tibio-fibular syndesmosis in adults: a pictorial essay with a multimodality approach. J Anat 2010;217:633-45.
63. Hickey BA, Watson U, Cleves A, Alikhan R, Pugh N, Nokes L, Perera A. Does throm-boprophylaxis reduce symptomatic venous thromboembolism in patients with below knee cast treatment for foot and ankle trauma? A systematic review and meta-analy-sis. Foot Ankle Surg 2018;24:19-27.
64. Hjelle AM, Apalset EM, Gjertsen JE, Nilsen RM, Lober A, Tell GS, Mielnik PF. As-sociations of overweight, obesity and osteoporosis with ankle fractures. BMC Mus-culoskelet Disord 2021;22:723.
65. Holmes JR, Acker WB 2nd, Murphy JM, McKinney A, Kadakia AR, Irwin TA. A Novel Algorithm for Isolated Weber B Ankle Fractures: A Retrospective Review of 51 Nonsurgically Treated Patients. J Am Acad Orthop Surg 2016;24:645-52.
66. Horisberger M, Valderrabano V, Hintermann B. Posttraumatic ankle osteoarthritis af-ter ankle-related fractures. J Orthop Trauma 2009;23:60-7.
67. Hultin H, Lindholm C, Malfert M, Möller J. Short-term sick leave and future risk of sickness absence and unemployment - the impact of health status. BMC Public Health 2012;10;12:861.
68. Høiness P, Engebretsen L, Strømsøe K. Cost of Surgical Treatment of Closed Ankle Fractures. Eur J Trauma 2002;28:258-62.
69. IBM SPSS Custom Tables - Create custom tables in no time. April 2012. Available at: https://www.ibm.com/downloads/cas/2QWB2WNR
70. Jensen SL, Andresen BK, Mencke S, Nielsen PT. Epidemiology of ankle fractures. A prospective population-based study of 212 cases in Aalborg, Denmark. Acta Orthop Scand 1998;69:48-50.
71. Ji MX, Yu Q. Primary osteoporosis in postmenopausal women. Chronic Dis Transl Med 2015;1:9-13.

98
Hans JutoStudies of ankle fractures
72. Johnell O, Kanis J. Epidemiology of osteoporotic fractures. Osteoporos Int 2005; 16(suppl 2):S3–7.
73. Juto H, Nilsson MG, Möller M, Wennergren D, Morberg P. Evaluatin non-responders of a survey in the Swedish fracture register: no indication of different functional re-sult. BMC Musculoskelet Disord 2017;18:278.
74. Kahn SR, Ginsberg JS. Relationship between deep venous thrombosis and the post-thrombotic syndrome. Arch Intern Med 2004;164:17-26.
75. Kanis JA, Oden A, Johnell O, Jonsson B, de Laet C, Dawson A. The burden of os-teoporotic fractures: a method for setting intervention thresholds. Osteoporos Int 2001;12:417–27.
76. Kannus P, Niemi S, Parkkari J, Sievänen H. Declining incidence of fall-induced nkle fractures in elderly adults: Finnish statistics between 1970 and 2014. Arch Orthop Trauma Surg 2016;136;1243-46.
77. Kannus P, Palvanen M, Niemi S, Parkkari J, Järvinen M. Increasing number and inci-dence of low-trauma ankle fractures in elderly people: finnish statistics during 1970-2000 and projections for the future. Bone 2002;31:430-3.
78. Kannus P, Parkkari J, Niemi S, Palvanen M. Epidemiology of osteoporotic ankle fractures in elderly persons in Finland. Ann Intern Med 1996;125:975-8.
79. Kelikian S, editor. Sarrafian’s anatomy of the foot and ankle: Descriptive, Topograp-hic, Functional. 3rd ed. Lippincott, Williams & Wilkins; 2011.
80. Kikuchi S, Tajima G, Sugawara A, Yan J, Maruyama M, Oikawa S, Saigo T, Oikawa R, Doita M. Characteristic features of the insertions of the distal tibiofibular ligaments on three-dimensional computed tomography- cadaveric study. J Exp Orthop 2020;7:3.
81. Kim J, Lonner JH, Nelson CL, Lotke PA. Response bias: effect on outcomes evalua-tion by mail surveys after total knee arthroplasty. J Bone Joint Surg Am 2004;86:15-21.
82. Knutsson SB, Wennergren D, Bojan A, Ekelund J, Möller M. Femoral fracture clas-sification in the Swedish Fracture Register - a validity study. BMC Musculoskelet Disord 2019;20:197.
83. Korim MT, Bhatia RP. A case-control study of surgical site infection following operative fixation of fractures of the ankle in large U.K. trauma unit. Bone Joint J 2014;96:636-40.
84. Kortekangas T, Haapasalo H, Flinkkilä T, Ohtonen P, Nortunen S, Laine HJ, Järvi-nen TL, Pakarinen H. Three week versus six week immobilisation for stable Weber B type ankle fractures: randomised, multicentre, non-inferiority clinical trial. BMJ 2019;364:k5432.
85. Koval KJ, Lurie J, Zhou W, Sparks MB, Cantu RV, Sporer SM, Weinstein J. Ankle fractures in the elderly: what you get depends on where you live and who you see. J Orthop Trauma 2005;19:635-9.
86. Kristman V, Manno M, Côté P. Loss to follow-up in cohort studies: how much is too much? Eur J Epidemiol 2004;19:751-60.

99Studies of ankle fractures
87. Kumar DR, Hanlin E, Glurich I, Mazza JJ, Yale SH. Virchow’s contribution to the understanding of thrombosis and cellular biology. Clin Med Res 2010;8:168-72.
88. Kwon JY, Gitajn IL, Walton P, Miller TJ, Appelton P, Rodriquez EK. A cadaver study revisiting the original methodology of Lauge-Hansen and a commentary on modern usage. J Bone Joint Surg Am 2015;97;604-9.
89. Kwon SK, Kang YG, Chang CB, Sung SC, Kim TK. Interpretations of the clinical outcomes of the nonresponders to mail surveys in patients after total knee arthro-plasty. J Arthroplasty. 2010;25:133-7.
90. Lachman JR, Elkrief JI, Pipitone PS, Haydel CL. Comparison of Surgical Site Infec-tions in Ankle Fracture Surgery With or Without the Use of Postoperative Antibiotics. Foot Ankle Int 2018;39:1278-82.
91. de Laet C, Kanis JA, Odén A, Johanson H, Johnell O, et al. Body mass index as a predictor of fracture risk: a meta-analysis. Osteoporos Int 2005;16:1330-8.
92. Landis JR, Koch GG. The measurement of observer agreement for categorical data. Biometrics. 1977;33:159-74.
93. Lambert LA, Falconer L, Mason L. Ankle stability in ankle fracture. J Clin Orthop Trauma. 2020;11:375-9.
94. Lapidus LJ, Ponzer S, Elvin A, Levander C, Lärfars G, et al. Prolonged thromboprop-hylaxis with Dalteparin during immobilization after ankle fracture surgery: A ran-domized placebo-controlled, double-blind study. Acta Orthopaedica 2007;78:528-35.
95. Lapidus LJ, Ponzer S, Pettersson H de Bari E. Symptomatic venous thromboembo-lism and mortality in orthopaedic surgery – an observational study of 45 968 conse-cutive procedures. BMC Musculoskelet Disord 2013;14:177.
96. Lauge-Hansen N. Fractures of the ankle II. Combined experimental-surgical and ex-perimental-roentgenologic investigations. Arch Surg 1950;60:957-85.
97. Lauge N. Fractures of the ankle; analytic historic survey as the basis of new experi-mental, roentgenologic and clinical investigations. Arch Surg 1948;56:259-317.
98. Lee KM, Chung CY, Kwon SS, Won SH, Lee SY, Chung MK, Park MS. Ankle fractu-res have features of an osteoporotic fracture. Osteoporos Int 2013;24:2819–25
99. Leizorovicz A. Long-term consequences of deep vein thrombosis. Haemostasis 1998;28 Suppl 3:1-7.
100. Liu S, Zhu Y, Chen W, Wang L, Zhang Y, et al. Demographic and socioeconomic factors influencing the incidence of ankle fractures, a national population-based sur-vey of 512187 individuals. Sci Rep 2018;8:10443.
101. Lidwall U. Sick leave diagnoses and return to work: a Swedish register study. Disabil Rehabil 2015;37:396-410.
102. Lidwall, U. Vad kostar olika sjukdomar i sjukförsäkringen? [What is the cost of dif-ferent diseases in the social insurance system?] Socialförsäkringsrapport 2011:4. [in Swedish] Försäkringskassan. Available at: http://www.forsakringskassan.se/statistik/publikationer/socialforsakringsrapporter (Accessed 22 Oct 2020).

100
Hans JutoStudies of ankle fractures
103. de Lissovoy G, Fraeman K, Hutchins V, Murphy D, Song D, Vaughn BB. Surgical site infections: Incidence and impact on hospital utilization and treatment costs. Am J infect Control 2009;37:387-397.
104. Lorentzon M, Cummings SR. Osteoporosis: the evolution of a diagnosis. J Intern Med 2015;277:650-61.
105. Lübbeke A, Salvo D, Stern R, Hoffmeyer P, Holzer N, Assal M. Risk factors for post-traumatic osteoarthritis of the ankle: an eighteen year follow-up study. Int Ort-hop 2012;36:1403-10.
106. Ludvigsson JF, Andersson E, Ekbom A, Feychting M, Kim J-L, Reuterwall C, et al. External review and validation of the Swedish national inpatient register. BMC Public Health. 2011; 11;450.
107. Lynde MJ, Sautter T, Hamilton GA, Schuberth JM. Complications after open reduction and internal fixation of ankle fractures in the elderly. Foot Ankle Surg 2012;18:103-7.
108. Macera A, Carulli C, Sirleo L, Onnocenti M. Postoperative complications and reope-ration rates following open reduction and internal fixation of ankle fracture. Joints 2018;21:110-115.
109. Malek IA, Machani B, Mevcha AM, Hyder NH. Inter-observer reliability and in-tra-observer reproducibility of the Weber classification of ankle fractures. J Bone Joint Surg Br 2006;88:1204-6.
110. Markussen S. The individual cost of sick leave. J Popul Econ. 2012;25:1287-1306.
111. Marsh JL, Slongo TF, Agel J, Broderick JS, Creevey W, DeCoster TA, Prokuski L, Sirkin MS, Ziran B, Henley B, Audigé L. Fracture and dislocation classification com-pendium - 2007: Orthopaedic Trauma Association classification, database and outco-mes committee. J Orthop Trauma 2007;21(10 Suppl):S1-133.
112. Marshall D, Johnell O, Wedel H. Meta-analysis of how well measures of bone mineral density predict occurrence of osteoporotic fractures. BMJ 1996;312:1254-9.
113. Martel N, Lee J, Wells PS. Risk for heparin-induced thrombocytopenia with unfrac-tionated and low-molecular-weight heparin thromboprophylaxis: a meta-analysis. Blood 2005; 106:2710-5.
114. McHugh ML. Interrater reliability: the kappa statistic. Biochem Med (Zagreb) 2012;22:276-82.
115. McLean J. The discovery of heparin. Circulation 1959;19:75-8.
116. McLendon K, Goyal A, Bansal P, Attia M. Deep Venous Thrombosis Risk Factors. 2021 Apr 22. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2021 Jan–. PMID: 29262230.
117. Meinberg EG, Agel J, Roberts CS, Karam MD, Kellam JF. Fracture and Dislocation Classification Compendium-2018. J Orthop Trauma 2018;32 Suppl 1:S1-S170.
118. Michelson J, Solocoff D, Waldman B, Kendell K, Ahn U. Ankle fractures. The Lau-ge-Hansen classification revisited. Clin Orthop Relat Res 1997;345:198-205.
101Studies of ankle fractures
119. Modha, MRK, Morriss-Roberts C., Smither M, Larholt J, Reilly I. Antibiotic prop-hylaxis in foot and ankle surgery: a systematic review of the literature. J Foot Ankle Res 2018:11;61.
120. Morris N, Lovell ME. Demographics of 3929 ankle injuries, seasonal variation in diagnosis and more fractures are diagnosed in winter. Injury 2013;44:998-1001.
121. Murphy DF, Connolly DA, Beynnon BD. Risk factors for lower extremity injury: a review of the literature. Br J Sports Med 2003;37:13-29.
122. Murray DW, Britton AR, Bulstrode CJ. Loss to follow-up matters. J Bone Joint Surg Br 1997;79:254-7.
123. National Institute for Health and Clinical Excellence. Osteoporosis: assessing the risk of fragility fracture. NICE clinical guideline 146. London: NICE; 2012. http://www.nice.org.uk/CG146 (accessed 24 Nov 2021)
124. Norquist BM, Goldberg BA, Matsen FA 3rd. Challenges in evaluating patients lost to follow-up in clinical studies of rotator cuff tears. J Bone Joint Surg Am. 2000;82:838-42.
125. Nåsell H, Otosson C, Törnqvist H, Lindé J, Ponzer S. The impact of smoking on com-plications after operatively treated ankle fractures – a follow-up study of 906 patients. J Orthop Trauma 2011;25:748-55
126. Ocak G, Vossen CY, Verduijn M, Dekker FW, Rosendaal FR, Cannegieter SC, Lijfe-ring WM. Risk of venous thrombosis in patients with major illnesses: results from the MEGA study. J Thromb Haemost 2013;11:116-23.
127. Ogilvie-Harris DJ, Reed SC, Hedman TP. Disruption of the ankle syndesmosis; bio-mechanical study of the ligamentous restraints. Arthroscopy 1994;10:558-560.
128. Ovaska MT, Mäkinen TJ, Madanat R, Huotari K, Vahlberg T, Hirvensalo E, Lindahl J. Risk factors for deep surgical site infection following operative treatment of ankle fractures. J Bone Joint Surg Am 2013;95:348-53.
129. Pelet S, Roger M-E, Belizile EL, Bouchard M. The incidence of thromboembolic events in surgically treated ankle fracture. J Bone Joint Surg Am 2012;94:502-6.
130. Pincus D, Veljkovic A, Zochowski T, Mahomed N, Ogilivie-Harris D, Wassertein D. Rato of and risk factors for Intermediate-term reoperation after ankle fracture fixa-tion: a populations-based cohort study. J Orthop Trauma 2017;31:e315-e320.
131. Ponzer S, Nåsell H, Bergman B, Törnkvist H. Functional outcome and quality of life in patients with Type B ankle fractures: a two-year follow-up study. J Orthop Trauma. 1999; 13:363-8.
132. Ponzer S, Skoog A, Bergström G. The Short Musculoskeletal Function Assessment Questionnaire (SMFA): cross-cultural adaptation, validity, reliability and responsive-ness of the Swedish SMFA (SMFA-Swe). Acta Orthop Scand 2003;74:756-63.
133. Port AM, McVie JL, Naylor G, Kreibich DN. Comparison of two conservative methods of treating an isolated fracture of the lateral malleolus. J Bone Joint Surg Br 1996; 78: 568-72.
102
Hans JutoStudies of ankle fractures
134. Rochelle DC, Herbert A, Ktistakis I, Redmond AC, Chapman GJ, Brockett CL. Mechanical characterisation of the lateral collateral ligament complex of the ankle at realistic sprain-like strain rates. J Mech Behav Biomed Mater 2020;102:103473.
135. Rutten S, Nolte PA, Guit GL, Bouman DE, Albers GH. Use of low-intensity pulsed ultrasound for posttraumatic nonunions of the tibia: a review of patients treated in the Netherlands. J Trauma 2007;62:902-8.
136. Ryd L, Bengtsson S. Isolated fracture of the lateral malleolus requires no treatment. 49 prospective cases of supination-eversion type II ankle fractures. Acta Orthop Scand 1992;63:443-6.
137. Saithna A, Moody W, Jenkinson E, Almazedi B, Sargeant I. The influence of timing of surgery on soft tissue complications in closed ankle fractures. Eur J Orthop Surg Traumatol 2009;19:481-4.
138. Sakaki MH, Matsumura BA, Dotta Tde A, Pontin PA, Dos Santos AL, Fernandes TD. Epidemiologic study of ankle fractures in a tertiary hospital. Acta Ortop Bras 2014; 22:90–3.
139. Savage-Elliott I, Murawski CD, Smyth NA, Golanó P, Kennedy JG. The deltoid liga-ment: an in-depth review of anatomy, function, and treatment strategies. Knee Surg Sports Traumatol Arthrosc 2013;21:1316-27.
140. Schazker J. Maurice Edmond Müller - In His Own Words. AO Foundation. 2018.
141. Scheer RC, Newman JM, Zhou JJ, Oommen AJ, Naziri Q, Shah NV, et al. Ankle fracture epidemiology in the United States: patient-related trends and mechanisms of injury. J Foot Ankle Surg 2020;59:479-83.
142. Schepers T, De Vries MR, Van Lieshout EMM, Van der Elst M. The timing of ankle fracture surgery and the effect on infectious complications; a case series and systema-tic review of the literature. Int Orthop 2013;37:489-94.
143. van Schie-van der Weert EM, van Lieshout EM, de Vries MR, van der Elst M, Sche-pers T. Determinants of outcome in operatively and non-operatively treated Weber-B ankle fractures. Arch Orthop Trauma Surg 2012;132:257-63.
144. Seeley DG, Browner WS, Nevitt MC, Genant HK, Scott JC, Cummings SR. Which fractures are associated with low appendicular bone mass in elderly women? The Study of Osteoporotic Fractures Research Group. Ann Intern Med 1991;115:837-42.
145. Segal G, Elbaz A, Parsi A, Heller Z, Palmanovich E, Nyska M, Feldbrin Z, Kish B. Clinical outcomes following ankle fracture: a cross-sectional observational study. J Foot Ankle Res 2014;7:50.
146. Shao J, Zhang H, Yin B, Li J, Zhu Y, Zhang Y. Risk factors for surgical site infection following operative treatment of ankle fractures: A systematic review and meta-ana-lysis. Int J Surg 2018;56:124-132.
147. Shariff SS, Nathwani DK. Lauge-Hansen classification – a literature review. Injury 2006; 37:888-90.
148. Sheikh K, Mattingly S. Investigating non-response bias in mail surveys. J Epidemiol Community Health. 1981;35:293-6.

103Studies of ankle fractures
149. Shrier I, Platt RW. Reducing bias through directed acyclic graphs. BMC Med Res Methodol. 2008;8:70.
150. Singer BR, McLauchlan GJ, Robinson CM, Christie J. Epidemiology of fractures in 15,000 adults: the influence of age and gender. J Bone Joint Surg Br 1998;80:243-8.
151. Simonis RB, Parnell EJ, Ray PS, Peacock JL. Electrical treatment of tibial non-union: a prospective, randomised, double-blind trial. Injury 2003;34:357-62.
152. Socialstyrelsen [The National Board of Health and Welfare]. Läkemedelsregistret - det statistiska registrets framställning och kvalitet [Swedish Prescribed Drug Register - the production and quality of the statistical register]. September 2021. Available at: https://www.socialstyrelsen.se/globalassets/sharepoint-dokument/dokument-webb/statistik/statistiska-registrets-framstallning-kvalitet-lakemedelsregistret.pdf.
153. Socialstyrelsen [The National Board of Health and Welfare]. Patientregistret – kan ge ledtrådar kring stroke och hjärtinfarkt. June 2019a. Available at: https://www.soci-alstyrelsen.se/globalassets/sharepoint-dokument/dokument-webb/ovrigt/halsodatare-gister-patientregistret-nyttan-med-register.pdf.
154. Socialstyrelsen [The National Board of Health and Welfare]. Läkemedelsregistret – ger säkra fakta om läkemedel på recept. June 2019b. Available at: lakemedelsregist-ret-nyttan-med-register.pdf.
155. Socialstyrelsen [The National Board of Health and Welfare]. Täckningsgrader 2019 – Jämförelser mellan nationella kvalitetsregister och hälsodataregistren. December 2019c. Available at: https://www.socialstyrelsen.se/globalassets/sharepoint-doku-ment/artikelkatalog/ovrigt/2019-12-6489-tabeller.xlsx (Accessed November 20, 2021)
156. Somersalo A, Paloneva J, Kautiainen H, Lönnroos E, Heinänen M, Kiviranta I. Inci-dence of fractures requiring inpatient care. Acta Orthop 2014;85:525-30.
157. SooHoo NF, Krenek L, Eagan MJ, Gurbani B, Ko CY, Zingmond DS. Complications rates following open reduction and internal fixation of ankle fractures. J Bone Joint Surg Am 2009;91:1042-9.
158. van Staa TP, Dennison EM, Leufkens HG, Cooper C. Epidemiology of fractures in England and Wales. Bone 2001;29:517-22.
159. Stein EM, Liu XS, Nickolas TL, Cohen A, Thomas V, McMahon DJ, Zhang C, Yin PT, Cosman F, Nieves J, Guo XE, Shane E. Abnormal microarchitecture and reduced stiffness at the radius and tibia in postmenopausal women with fractures. J Clin Endo-crinol Metab 2011;96:2041-8.
160. Stone KL, Seeley DG, Lui LY, Cauley JA, Ensrud K, Browner WS, Nevitt MC, Cum-mings SR; Osteoporotic Fractures Research Group. BMD at multiple sites and risk of fracture of multiple types: long-term results from the Study of Osteoporotic Fractures. J Bone Miner Res 2003;18:1947-54.
161. Stufkens SA, Knupp M, Horisberger M, Lampert C, Hintermann B. Cartilage lesions and the development of osteoarthritis after internal fixation of ankle fractures: a pro-spective study. J Bone Joint Surg Am 2010;92:279-86.

104
Hans JutoStudies of ankle fractures
162. Sun R, Li M, Wang X, Li X, Wu L, et al. Surgical site infection following open re-duction and internal fixation of a closed ankle fractures: A retrospective multicenter cohort study. Int J Surg 2017;48:86-91.
163. Sun Y, Wang H, Tang Y, Zhao H, Qin S, Xu L, Xia Z, Zhang F. Incidence and risk factors for surgical site infection after open reduction and internal fixation of ankle fracture: A retrospective multicenter study. Medicine (Baltimore) 2018;97:e9901.
164. Swedankle: Annual Report 2019 (in Swedish). Available at: https://swedankle.se/pu-blikationer/arsrapporter.
165. The Swedish Fracture Register: Annual Report 2019 (in Swedish). Available at: htt-ps://registercentrum.blob.core.windows.net/sfr/r/VGR0050_SFR_-rsrapport-2019_Digital-1-uppslag-BJl2qw9v38.pdf
166. The Swedish Fracture Register: Annual Report 2020 (in Swedish). Available at: htt-ps://registercentrum.blob.core.windows.net/sfr/r/VGR_SFR_-rsrapport-2020-SE-DI-GITAL-uppslag-B1xBpRe6q_.pdf
167. Swiontkowski MF, Engelberg R, Marin DP, Agel J. Short musculoskeletal function assessment questionnaire; validity, reliability and responsiveness. J Bone Joint Surg Am. 1999;81:1245-60.
168. Tagalakis V, Patenaude V, Kahn SR, Suissa S. Incidence of and mortality from venous thromboembolism in a real-world population: the Q-VTE Study Cohort. Am J Med 2013;126:832.e13-21.
169. Tartaglione JP, Rosenbaum AJ, Abousayed M, DiPreta JA. Classifications in Brief: Lauge-Hansen Classification of Ankle Fractures. Clin Orthop Relat Res 2015;473:3323-8.
170. Thakore RV, Greenberg SE, Shi H, et al. Surgical site infection in orthopedic trau-ma: A case-control study evaluating risk factors and cost. J Clin Orthop Trauma 2015;6:220-226.
171. Thomas G, Whalley H, Modi C. Early mobilization of operatively fixed ankle fractu-res: a systematic review. Foot Ankle Int 2009:30:666-74.
172. Thomsen NO, Olsen LH, Nielsen ST. Kappa statistics in the assessment of observer variation: the significance of multiple observers classifying ankle fractures. J Orthop Sci 2002;7:163-6.
173. Thomsen NO, Overgaard S, Olsen LH, Hansen H, Nielsen ST. Observer variation in the radiographic classification of ankle fractures. J Bone Joint Surg Br 1991;73:676-8.
174. Thur CK, Edgren G, Jansson KÅ, Wretenberg P. Epidemiology of adult ankle fractu-res in Sweden between 1987 and 2004; a populations-based study of 91,410 Swedish inpatients. Acta Orthop 2012;83:276-81.
175. Tunturi T, Kemppainen K, Pätiälä H, Suokans M, Tamminen O, Rokkanen P. Im-portance of anatomical reduction for subjective recovery after ankle fracture. Acta Orthop Scand 1983;54:641-647.
176. Valderrabano V, Horisberger M, Russell I, Dougall H, Hintermann B. Etiology of ankle osteoarthritis. Clin Orthop Relat Res 2009;467:1800-6.

105Studies of ankle fractures
177. Valtola A, Honkanen R, Kröger H, Tuppurainen M, Saarikoski S, Alhava E. Lifestyle and other factors predict ankle fractures in perimenopausal women: a population-ba-sed prospective cohort study. Bone 2002;30:238–42
178. Weber BG. Die Verletzungen des oberen Sprunggelsenkes. Huber. Bern. 1972.
179. Weimert S, Kuhn S, Rommens PM, Beutel ME, Reiner IC. Symptoms of adjustment disorder and smoking predict long-term functional outcome after ankle and lower leg fractures. J Rehabil Med 2020; 52:jrm00086
180. Wennergren D, Ekholm C, Sundfeldt M, Karlsson J, Bhandari M, Möller M. High reliability in classification of tibia fractures in the Swedish Fracture Register. Injury 2016;47:478-82.
181. Wennergren D, Ekholm C, Sandelin A, Möller M. The Swedish fracture register; 103,000 fractures registered. BMC Musculoskelet Disord 2015;16:338.
182. Wennergren D, Möller M. Implementation of the Swedish Fracture Register. Unfall-chirurg 2018;121:949-55.
183. Wennergren D, Stjernström S, Möller M, Sundfeldt M, Ekholm C. Validity of hu-merus fracture classification in the Swedish fracture register. BMC Musculoskelet Disord 2017;18:251.
184. Wettermark B, Hammar N, Fored CM, Leimanis A, Olausson PO, Bergman U, et al. The new Swedish Prescribed Drug Register – Opportunities for pharmacoepidemio-logical research and experience from the first six months. Pharmacoepidemiol Drug Saf 2007;16:726-35.
185. White RH. The epidemiology of venous thromboembolism. Circulation 2003;17;107(23 Suppl 1):I4-8.
186. Whitehouse JD, Friedman ND, Kirkland KB, Richardson WJ, Sexton DJ. The impact of surgical-site infections following orthopedic surgery at a community hospital and a university hospital: adverse quality of life, excess length of stay, and extra cost. Infect Control Hosp Epidemiol 2002;23:183-9.
187. Willett K, Keene DJ, Mistry D, Nam J, Tutton E, Handley R, Morgan L, Roberts E, Briggs A, Lall R, Chesser TJ, Pallister I, Lamb SE; Ankle Injury Management (AIM) Trial Collaborators. Close Contact Casting vs Surgery for Initial Treatment of Unstable Ankle Fractures in Older Adults: A Randomized Clinical Trial. JAMA 2016;316:1455-63.
188. Yap RY, Babel A, Phoon KM, Ward AE. Functional Outcomes Following Operative and Nonoperative Management of Weber C Ankle Fractures: A Systematic Review. J Foot Ankle Surg 2020;59:105-11.
189. Zee AA, van Lieshout K, van der Heide M, Janssen L, Janzing HM. Low molecular weight heparin for prevention of venous thromboembolism in patients with lower-limb immobilization. Cochrane Database Syst Rev 2017;8:CD006681.





















