Management of pathologic fractures
10
MANAGEMENT OF PATHOLOGIC FRACTURES CARLOS A. PEREZ, MD, JOHN S. BRADFIELD, MD, AND HARRY C. MORGAN, MD" The principles of management of pathologic fractures in the long bones are reviewed, and a series of 45 fractures treated by internal fixation is compared with 26 fractures treated by other nonsurgical procedures. Internal fixation and radiation therapy provide better and longer lasting palliative results in these patients, provided clear indications for this method of management are care- fully evaluated. Relief of pain is observed in over 80% of the patients and satisfactory healing and functional results in about 75%. The value of pro- phylactic fixation and irradiation of large osteolytic lesions in weight-bearing bones with a high risk of fracture is emphasized. LTHOUGH RELATIVELY INFREQUENT, PATHO- A logic fractures occurring in patients with advanced cancer present a multitude of prob- lems in management. Metastases to the long bones are much less frequent than to the flat bones, such as the clavicle, ribs, spine, and pelvi~.~4 Even though long bone metastasis represents less than 20% of all fractures, they are more important from a functional and therapeutic viewpoint. Patients with disseminated disease who de- velop pathologic fractures often are early in the course of their disease. Since nearly 50% of these patients survive for a year or more, an aggressive approach to management of these fractures is imperative, if one is to return com- fort and mobility to the patient so he may enjoy the remaining months. Furthermore, we agree with those who have advocated the pro- phylactic fixation and irradiation of destruc- tive lesions when they are discovered and be- fore an actual fracture o c c ~ r s . ~ ~ ~ ~ ~ J O T o facili- tate this approach, radiographic examination should be made with the least symptoms. Our purpose here is to review a group of patients with pathologic fractures treated at Barnes Hospital and the Division of Radia- tion Therapy, Mallinckrodt Institute of Ra- diology, Washington University Medical Cen- ter, St. Louis, between January 1963 and December 1969. A total of 39 patients with 45 fractures was treated by internal fixation and local irradiation. During the same period, an- From the Division of Radiation Therapy, Mallinck- rodt Institute of Radiology and the Department of Sur- gery, Division of Orthopedic Surgery,. Washington University School of Medicine, St. Louis, Mo. Address for reprints: C. A. Perez, MD, Mallinckrodt Institute of Radiology, 510 South Kingshighway, St. Louis, Mo. 61110. Received for publication August 6, 1971. other group of 26 patients with 36 fractures was treated by orthopedic methods other than internal fixation, combined with local irradia- tion (Table 1). The anatomical location of the lesions is summarized in Fig. lA, B. It is evident that most of the fractures occurred in the proximal humerus and in the proximal femur, usually in the intertrochanteric or subtrochanteric re- gions. A few fractures were noted in the ra- dius and the tibia, and one pathologic frac- ture was observed in the fibula. About one third of these patients expen- enced fractures in the flat bones, particularly the clavicles, ribs, pubic bones, acetabulum, as well as in the vertebrae. Since their manage- ment is usually conservative, consisting of im- mobilization, analgesics, and radiation ther- apy, they will not be discussed further. The sites of the primary tumors are listed in Table 2. The most frequent primary tumor was seen in women with advanced carcinoma of the breast (38.5y0). Patients with multiple myeloma and lymphoma represent the second most common site (15.4y0). Carcinoma of the lung not infrequently produces osteolytic me- TABLE I. Number of Fractures No. patie ts No. patients Internaf Other Fixatiori Treatment One fracture 34 19 Two fractures 4 4 Three or more 3 Total number or Total number of - fractures 1 patients 39 26 fractures 45 36 - 684
-
Upload
independent -
Category
Documents
-
view
2 -
download
0
Transcript of Management of pathologic fractures
MANAGEMENT OF PATHOLOGIC FRACTURES CARLOS A. PEREZ, MD, JOHN S. BRADFIELD, MD, AND HARRY C. MORGAN, MD"
The principles of management of pathologic fractures in the long bones are reviewed, and a series of 45 fractures treated by internal fixation is compared with 26 fractures treated by other nonsurgical procedures. Internal fixation and radiation therapy provide better and longer lasting palliative results in these patients, provided clear indications for this method of management are care- fully evaluated. Relief of pain is observed in over 80% of the patients and satisfactory healing and functional results in about 75%. The value of pro- phylactic fixation and irradiation of large osteolytic lesions in weight-bearing bones with a high risk of fracture is emphasized.
LTHOUGH RELATIVELY INFREQUENT, PATHO- A logic fractures occurring in patients with advanced cancer present a multitude of prob- lems in management. Metastases to the long bones are much less frequent than to the flat bones, such as the clavicle, ribs, spine, and pelvi~.~4 Even though long bone metastasis represents less than 20% of all fractures, they are more important from a functional and therapeutic viewpoint.
Patients with disseminated disease who de- velop pathologic fractures often are early in the course of their disease. Since nearly 50% of these patients survive for a year or more, an aggressive approach to management of these fractures is imperative, if one is to return com- fort and mobility to the patient so he may enjoy the remaining months. Furthermore, we agree with those who have advocated the pro- phylactic fixation and irradiation of destruc- tive lesions when they are discovered and be- fore an actual fracture o c c ~ r s . ~ ~ ~ ~ ~ J O T o facili- tate this approach, radiographic examination should be made with the least symptoms.
Our purpose here is to review a group of patients with pathologic fractures treated at Barnes Hospital and the Division of Radia- tion Therapy, Mallinckrodt Institute of Ra- diology, Washington University Medical Cen- ter, St. Louis, between January 1963 and December 1969. A total of 39 patients with 45 fractures was treated by internal fixation and local irradiation. During the same period, an-
From the Division of Radiation Therapy, Mallinck- rodt Institute of Radiology and the Department of Sur- gery, Division of Orthopedic Surgery,. Washington University School of Medicine, St. Louis, Mo.
Address for reprints: C. A. Perez, MD, Mallinckrodt Institute of Radiology, 510 South Kingshighway, St. Louis, Mo. 61110.
Received for publication August 6, 1971.
other group of 26 patients with 36 fractures was treated by orthopedic methods other than internal fixation, combined with local irradia- tion (Table 1).
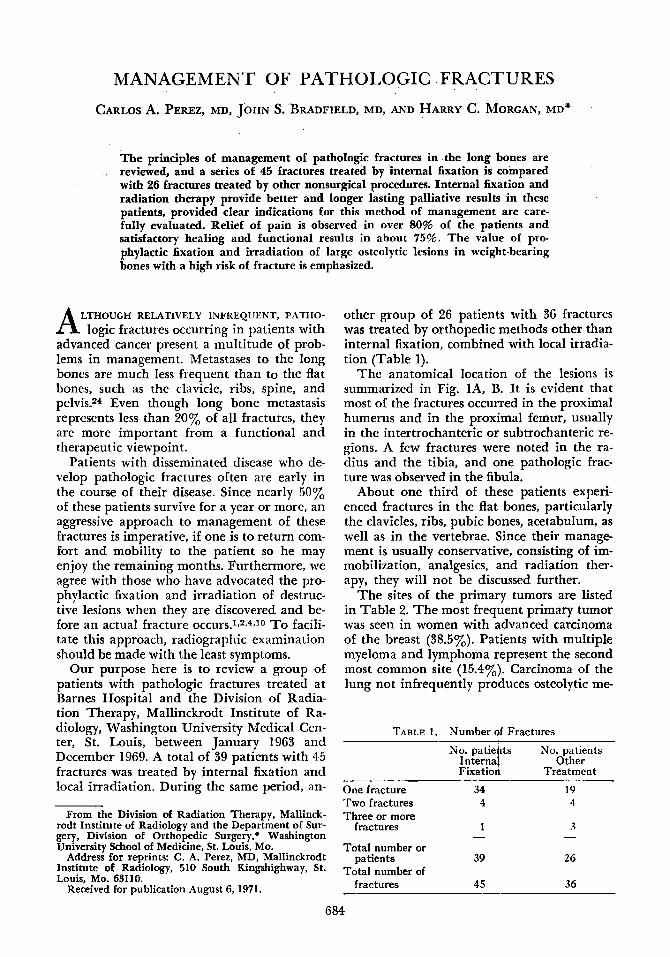
The anatomical location of the lesions is summarized in Fig. lA, B. It is evident that most of the fractures occurred in the proximal humerus and in the proximal femur, usually in the intertrochanteric or subtrochanteric re- gions. A few fractures were noted in the ra- dius and the tibia, and one pathologic frac- ture was observed in the fibula.
About one third of these patients expen- enced fractures in the flat bones, particularly the clavicles, ribs, pubic bones, acetabulum, as well as in the vertebrae. Since their manage- ment is usually conservative, consisting of im- mobilization, analgesics, and radiation ther- apy, they will not be discussed further.
The sites of the primary tumors are listed in Table 2. The most frequent primary tumor was seen in women with advanced carcinoma of the breast (38.5y0). Patients with multiple myeloma and lymphoma represent the second most common site (15.4y0). Carcinoma of the lung not infrequently produces osteolytic me-
TABLE I . Number of Fractures No. patie ts No. patients
Internaf Other Fixatiori Treatment
One fracture 34 19 Two fractures 4 4 Three or more
3
Total number or
Total number of
- fractures 1
patients 39 26
fractures 45 36
-
684
No. 3 PATHOLOGIC FRACTURES - Perez et al. 685
FIG. 1A and B. Anatomical location of pathologic fractures in long bones, in 45 instances treated by internal fixation and in 26 treated by other methods.
A. FRACNRES TREATED BY INTERNAL FIXAllON B. FRACTURES TREATED BY OTHER METHODS
tastasis in some of the long bones, and they comprise about 12% of all the cases.
MANAGEMENT
In the treatment of a patient with a malig- nant tumor suspected of having a pathologic fracture, the first step is immediate provi- sional immobilization, adequate clinical exam- ination, medication for relief of pain or shock, and radiographic studies to determine the presence of a fracture and its characteristics. Bone scanning with injection of Fluorine 18, Strontium 85, or Strontium 87M may be very helpful in localizing lesions not demonstrable by routine radiographs,6l*J4 even before a fracture occurs.
The aim of therapy is palliative, but never- theless an agressive approach will be rewarded b y early mobilization and complete relief of pain in most of the patients (Table 7). This prevents injury to adjacent normal tissues and may aid in local tumor control. When feasi- ble, permanent immobilization should be per- formed, followed by irradiation of the in- volved bone.
IMMOBILIZATION TECHNIQUES
Internal Fixation Before the possibility of internal fixation is
considered, an adequate amount of intact
strong bone must be present in the vicinity of the destructive lesion. The overall clinical condition and prognosis of the patient must be carefully evaluated when making a thera- peutic decision. At the time of the operative procedure, a biopsy should be performed to confirm the pathologic nature of the lesion. Forty-five fractures were treated by means of an operative fixation combined with irradia- tion of the involved bone (Table 4). Fractures of the neck and trochanteric areas of the femur were usually immobilized by means of a Jewett nail (17 cases) or a Smith-Peterson nail (2 patients). In one instance, the partially de- stroyed femur was replaced by an Austin-
TABLE 2. Site of Primary Tumor
Breast Lymphoreticular Lung Kidney Thyroid Head and neck Prostate
Internal Other fixation treatment
21 4 5 5 5 3 1 3
2 1 2
2
-
- -
Total
25 (38.5%) 10 (15.4%)
8 (12.3%)
4 ( 6.1%) 2 3 2
Bone (orrteosarcoma) - 2 2 Cervix and endometrium 2 1 3 Colon 1 2 3
Other 1 2 3
26 65 Total number of patients 39 - - -

686 CANCER March 1972 Vol. 29
TABLE 3. Types of Treatment in Patients without Internal Fixation
Humerus and Radius Hanging cast Half cast or splint Sling Amputation Unknown
Femur and Tibia Traction Cast Amputation
1 2 4 6 1 2 25
6 3 2 11
Moore prosthesis. Patients with fractures in the subtrochanteric area or in the shaft of the bone were treated by means of intramedullary nails (4 cases), Fig. 2A, B, 6). Two fractures
TABLE 4. Type of Internal Fixation
Humerus and Radius Rush Pins
Femur Jewett nail Lottes nail Kuntscher nail Kuntscher nail and Elliott plate Smith-Peterson Nail Austin-Moore prothesis Elliott nail and Eger’s plate Holt nail Knowles pin
Tibia Lottes nail
10
17 5 4 1 2 1 1 1 1
2
45 -
FIG. PA (left). Large mixed lytic and blastic metastasis in the proximal femur with suggestion of a small fracture line through the intertrochanteric region. Internal fixation was performed by means of a Jewett nail, and local irradiation (3,000 rads tumor dose in two weeks) was given. FIG. 2B (right). Follow-up radiograph 14 months after treatment showing marked healing of
the lesion and satisfactory position of the bone.
No. 3 PATHOLOCIC FRACTURES * Perez et al. 687 of the tibia were treated by means of intrame- dullary Lottes nails.
Three of the patients in the group were treated prophylactically by internal fixation, immobilized and irradiated for a large osteoly- tic lesion in the trochanteric area of the femur before fracture occurred. All of the humeral fractures treated by internal fixation were im- mobilized by means of Rush pins (9 patients), Fig. 3.
Nonsurgical The patients were treated with external
splintage, by means of a cast or a splint and in some cases of fracture of the humerus with a sling. One patient with massive destruction of the proximal humerus by metastatic thyroid carcinoma required an amputation which re- sulted in complete relief of pain for over 12 years. She developed a pathologic fracture in the opposite humerus 4 years later.
RADIATION THERAPY
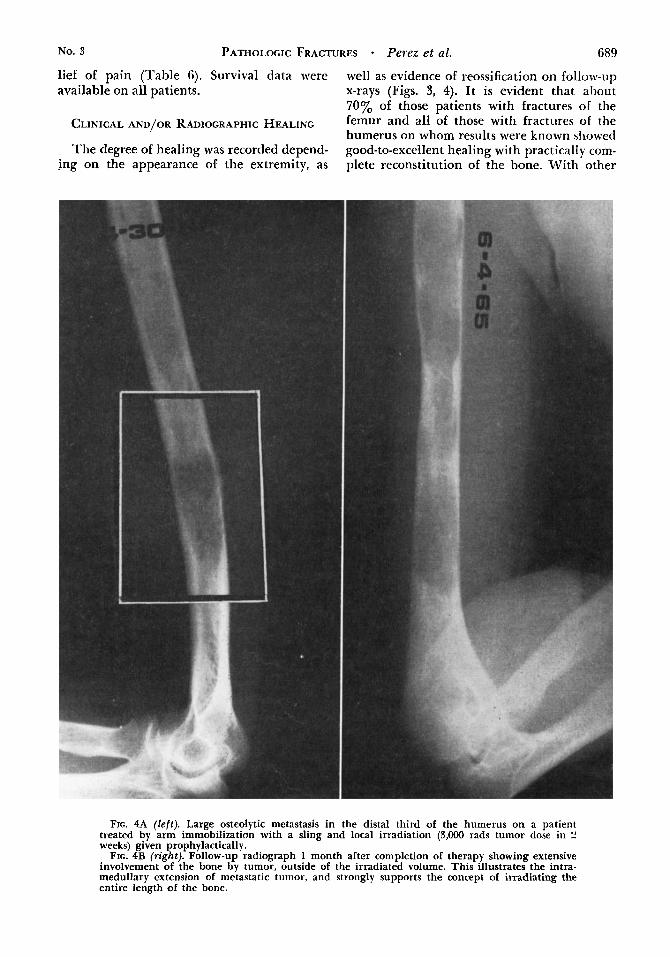
I n addition to the immobilization of the fractured bone, radiation therapy is an inte- gral part of the treatment of these patients. Because of the intramedullary spread of meta- static tumor in the long bones (Fig. 4A, B) and the possible dissemination of tumor cells during the operative procedure, the entire length of the bone should be irradiated. The most frequently used portals for the treatment of long bones have been published by Delclos in a comprehensive review of this subject.6 The dose is dependent upon the histologic na- ture of the tumor and the clinical condition of the patient. In general, adenocarcinoma of the breast and prostate responds to tumor doses of 3,000 rads administered in 2 weeks. However, in some instances, 2,000 rads tumor dose given in one week (5 fractions) yields sat- isfactory results. Patients with metastatic epi- dermoid carcinoma or adenocarcinoma pri- mary in sites other than the breast or the prostate need somewhat higher doses of radia- tion therapy. Usually 4,000 rads in 3 weeks (15 fractions) will give satisfactory tumor con- trol. In patients with leukemia, lymphoma, or multiple myeloma, doses in the range of 1,500-2,000 rads in one week (5 fractions) or 3,000 rads tumor dose in 2 weeks (8-10 fractions) are sufficient to produce relief of pain.
If the patients are treated as outpatients or if mobilization is somewhat difficult, the irra-
diation schedule can be modified, and 3 larger fractions per week can be given to complete the same total tumor dose.
Orthovoltage 250 kv x-rays are adequate to treat a significant portion of the patients with metastatic lesions in the extremities. However, the use of cobalt60 facilitates the delivery of higher doses at a faster rate (less number of fractions) without significant skin reaction. Patients treated through a cast need speciaI care to prevent the appearance of increased skin reaction. This is due to the loss of skin sparing effect which is characteristic of super- voltage, because of the electronic build-up when the beam traverses the cast.
OTHER THERAPEUTIC MEASURES
In addition to the surgical and radiothera- peutic procedures outlined above, an im- portant consideration in the treatment of these patients with a metastatic tumor is the use of adjuvant therapy, hormones or chemo- therapeutic agents, depending on the nature
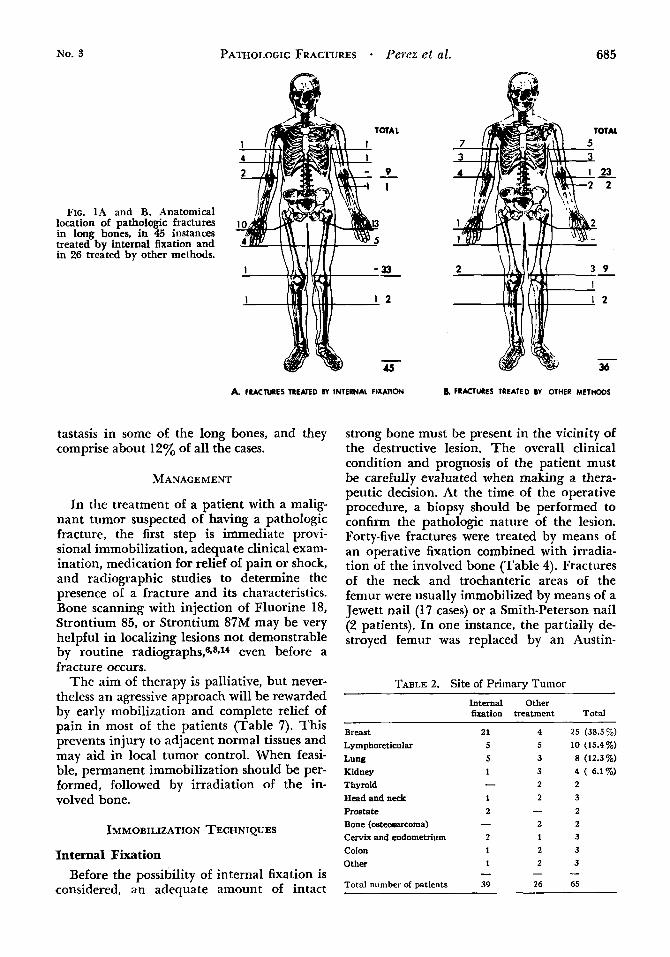
FIG. 3A. Spiral pathologic fracture in the mid-shaft of the humerus of a 45-year-old Caucasian woman with metastatic carcinoma of the breast. Intramedullary fixation and radiation therapy were given.

688 CANCER March 1972 Vol. 29
FIG. 3B (left). Follow-up radiograph 8 months after treatment, showing satisfactory position of the fracture and some new bone formation.
FIG. 3C (right). Subsequent follow-up 11/ years following treatment, showing further healing at the fracture site. There was complete r e k f of pain, and the patient has satisfactory function of the arm.
of the primary tumor, This subject has been reviewed in other publications and will not be further discussed here.9J5J01”2 Early ambu- lation and physical therapy are important adjuncts in the recovery of function in these patients.
Mobility in bed shortly after the operation when reasonably firm internal fixation has been secured and early nonweight-bearing walking on crutches or walk-aids is advised4 Most patients with these devices walk within 4-6 weeks after operation. Patients with frac- tures of the humerus are encouraged to exer- cise their arm soon after internal fixation.
It should be emphasized that continued pe- riodic evaluation of patients receiving radia-
tion therapy will often reveal other skeletal le- sions prior to fracture. Additional therapy can be instituted early preventing many of the dis- abling complications such as pain, deformity, prolonged bed confinement, and extensive nursing care.23
RESULTS
The follow-up records were complete in about 80% of the patients, which is reflected in the number of “unknowns” in evaluating some of the results. The data were retrospec- tively analyzed according to the criteria out- lined in Table 5 for clinical or radiographic evidence of healing, functional results, and re-
No. 3 PATHOLOGIC FRACTURES - Perez et al. 689
lief of pain (Table 6). Survival data were well as evidence of reossification on follow-up available on all patients. x-rays (Figs. 3, 4). It is evident that ahout
70% of those patients with fractures of the femur and all of those with fractures of the humerus on whom results were known showed good-to-excellent healing with practically com- plete reconstitution of the bone. With other
CLINICAL AND/OR RADIOGRAPHIC HEALING
The degree of healing was recorded depend- ing on the appearance of the extremity, as
FIG. 4A (left). Large osteolytic metastasis in the distal third of the humerus on a patient treated by arm immobilizatidn with a sling and local irradiation (3,000 rads tumor dose in 2 weeks) given prophylactically.
FIG. 4B (right). Follow-up radiograph 1 month after completion of therapy showing extensive involvement of the bone by tumor, outside of the irradiated volume. This illustrates the intra- medullary extension of metastatic tumor, and strongly supports the concept of irradiating the entire length of the bone.

CANCER March 1972 VOl. 29
TABLE 5. Pathologic Fractures
Clinical and/or radiographic healing Excellent
Good
Fair
Poor
Function Ex&eiit}
Fair
Poor
Relief of pain Excellent Good
Fair Poor
Complete healing without defor- mity.
Adequate repair of fracture and destroyed bone.
Incomplete reconstitution of bone or partial healing of fracture.
No significant bone repair a t fracture site.
No significant or slight limitation.
Moderate use of arm Crutches Wheel chair Bedridden Inability to use extremity
Complete Nearly complete. requiring oc-
Moderate relief No sienificant imDrovement
casional analgesics
I
treatments, mainly hanging plaster casts for the humerus and traction for the femur, only about half of the patients showed excellent or
good healing in the upper extremity and 33% (3 out of 9) in the lower extremity.
One of the reasons why the percentage of patients showing excellent or complete heal- ing of the fracture is not higher probably stems from the fact that about 25% of the pa- tients died within 3 months from the treat- ment of the fractureinadequate time for complete reconstitution of the bone.
FUNCTION
In the group treated by internal fixation, the recovery of function was excellent or good in all of the patients with humeral fractures and in 70% of those with fractures of the femur. Approximately half of the patients treated with other methods in the upper ex- tremity and 3 out of 10 of those with lesions in the lower extremities had satisfactory re- sults.
RELIEF OF PAIN
Again, satisfactory relief of pain was ob- served in over 80% of the patients with either
TABI;E 6. Results of Treatment* ~ ~~
Humerus and Radius Femur and Tibia
Internal fixation Other treatment Internal fixation Other treatment
Healing - Excellent 3 3 9
3 5 3 Fair -
Poor - 3 3 3 Unknown 2 4 6 2
Excellent 3 3 9 -
Fair - 5 6 4 Poor 4 3 3 Unknown 1 4 3 1
Excellent 4 3 10 1 Good 2 (100%) 8 (61%) 14 (80%) 3 (44%) Fair 4 4 3
3 2 2 Poor -
Unknown 1 3 3 2
During Rx 2 2 1
in above) 2 3
in above) 1 2
Good 2 (loo)%- 8 (65%) 10 (70%) 3 (33%)
Function
Good 3 (100%) 5 (47%) 12 (70%) 3 (30%)
-
Rclicf of pain
-
Postop. deaths
Refract lire ( i ncl u d d
Amputation (included
* Patients with “iinknown” results excluded from percentage calculations.

No. 3 PATHOLOCIC FRACTURES Perez et al. 69 1
humeral or femoral fractures treated by inter- nal fixation. These results were better than those obtained with conservative methods of treatment when only about 45-600/, of the pa- tients showed excellent or good relief of pain.
POSTOPERATIVE DEATHS
There were 4 postoperative deaths in the patients treated by internal fixation, 2 of them due to bronchopneumonia. Several patients experienced refracture through the treated sites, particularly when there was large de- struction of the bone and limited margins for the placement of internal devices were availa- ble. An example of this problem is illustrated in Fig. 2. Two patients with humeral frac- tures treated by hanging casts that showed considerable healing, refractured at a later time through the treated sites.
SURVIVAL AFTER TREATMENT OF PATHOLOCIC FRACTURE
Nearly 50% of the patients treated for a pathologic fracture survived over 1 year after the treatment of the first fracture and 25% survived 2 years or longer (Table 7).
DISCUSSION
One of the most significant problems in the palliation of advanced metastatic disease is
that of pathologic fracture in the long bones. Internal fixation has become a widely used method of treatment, usually combined with external radiation therapy. Experimentally, Bonarigo and Rubins demonstrated on arti- ficially produced fractures at the site of trans- planted tumors in rats that either the effects of ionizing irradiation or the presence of tumor interferes significantly with the healing of a fracture in the bone. However, when support was given to the bones by means of an intramedullary nail and the tumor was irradiated, there was rapid reconstitution of the bone. This observation has been re- peatedly confirmed on numerous clinical
This aggressive treatment is reinforced by the significant proportion of patients with pathologic fractures surviving for considerable lengths of time. Marcove and Yangl7 reported on a group of 63 patients with cancer of the breast who had pathologic fractures treated by internal fixation. Thirty-four percent of those with a single fracture and 26% of the patients with multiple fractures lived longer than one year. This finding is comparable to our own experience, in which almost half of the pa- tients survived longer than one year after the treatment of their first pathologic fracture.
The overall prognosis is strongly affected by the site of the primary tumor; carcinoma of the breast and multiple myeloma have a more favorable outlook, and patients with carci-
~~~~~~1.2.4.7,11-13,18,20,23
TABLE 7. Survival after Treatment
Internal Fixation Other Treatment
Single fixation Multiple furation Single fixation Multiple fixation
0-3 months 3-6 months 6-9 months
9-12 months 12-18 months 18-24 months 24-36 months Over 36 months
Total number patients
~
Alive at time of report (more than 2 Y = 4 9
*Postop. deaths 3 tDeaths during treatment -
3 -
2

692 CANCER March 1972 VOl. 29
noma of the lung or other undifferentiated carcinomas have a more unfavorable prognosis.19
In a recent review on the subject, Parrish and Murrayl9.20 reviewed the requirements which should be fulfilled before considering surgical treatment of a neoplastic fracture in a long bone. The general condition and prog- nosis of the patient must be good. The quality of the bone, both proximal and distal to the fracture, must be adequate for stable fixation. The operation should expedite early mobiliza- tion of the patient or facilitate general care. A surgical procedure is the treatment of choice for the treatment of pathologic fractures of the femur. Parrish and MurraylQ advocate prosthesis for the fractures in the femoral head and neck, nail-plate devices for intertro- chanteric fractures, and intramedullary fixa- tion for fractures of the femoral shaft. This is essentially the same treatment policies fol- lowed at this institution.
Although the pathologic fracture is quite often minimally displaced, it is extremely dif- ficult to pass an intramedullary device blindly, except in prophylactic fixations.’ This is prob- ably due to the friable nature of the surround- ing bone which makes it likely to create false passages. Because of this, an open approach is used in most instances, a technique which al- lows the surgeon to take a biopsy specimen for
histologic confirmation of the pathologic frac- ture. An accurate diagnosis of an unsuspected type of tumor may open the possibilities for other types of adjuvant therapy, such as hor- mones or chemotherapy.12 The possibility of tumor dissemination21 probably has little clin- ical implication on these patients.
Most authors agree that radiation therapy plays an integral role in the management of these patients.3b.l0.ll.l3.l9.23 Two points should be stressed: 1. irradiation of the entire length of the involved bones is important be- cause of the propensity of the tumor to spread along the medullary cavity (Fig. 4); 2. the use of relatively high doses of radiation therapy in a short period of time produces better tumor control for prolonged periods of time. The use of prophylactic internal fixation and radiation therapy for the treatment of “im- pending” fractures, particularly in weight- bearing bones with large osteolytic lesions, has received increasing publicity in recent years.192Jo Francis10 has outlined the primary indications for this method of treatment as follows: 1. The existence of a definite hazard of fracture; 2. A relatively isolated lesion; 3. Relatively localized disease, and 4. Satisfac- tory condition of the patient who should be fully ambulatory in most instances and pur- suing a normal life.
REFERENCES
1. Altman, H.: Intramedullary nailing for pathologic impending and actual fractures of long bones. Bul. Hosp. Joint Dis. 13:239-251.1952.
2. Bennish, E. L., and Hammong, G.: Treatment of actual and imminent pathological fractures of femur by intramedullary nailing. Surg. Clin. North Am. 35: 865-872, 1955.
3. Bonarieo, B. C.. and Rubin. P.: Nonunion of pathologic Gactures after radiation- therapy. Radiology 88~889-898, 1967.
4. Bremner. R. A., and Jelliffe, A. M.: The manage- ment of pathological fracture of the major long bones from metastatic cancer. J. Bone Joint Surg. 4:652-659. 1958.
5. Delclos, L.: Palliative irradiation of bone metas- tases. In Breast Cancer, Early and Late. Chicago, Year Book Medical Publishers, Inc., 1970; p. 351.
6. DeNardo. G. L.. Horner. R. W.. Leach. P. T.. and Bowes, D. J.1 Radioisotope skeletal suwey. 3 A M A 200:121-123. 1967.
7. Ehrenhaft, J. L.. and Tidrick, R. T., Intramedul- lary bone fixation in pathologic fractures. Surg. Gyne- col. Obstet. 88:519, 1949.
8. Faber, D. D., Wahman, G. E., Bailey, T. A., Flocks, R. H., Culp, D. A., and Morrison. R. T.: An evaluation of the 85 Sr scan for the detection and local-
ization of bone metastases from prostatic carcinoma. ]. Urol. 97:526-532, 1967.
9. Fracchia, A. A., Randall, H. T., and Farrow, J. H.: The results of adrenalectomy for advanced breast cancer in 500 consecutive patients. In Breast Cancer, Early and Late. Chicago, Year Book Medical Publish- ers, Inc., 1970; p. 369.
10. Francis, K. C.: Prophylactic internal fixation of metastatic osseous lesions. Cancer 13:75-76, 1960.
11. Francis, K. C., Higinbotham, N. L., Carroll, R. E., Jacobs, B. and Graham, W. D.: The treatment of pathological fractures of the femoral neck by resection. J. Trauma 2:465473,1962.
12. Higinbotham, N. L., and Marcove, R. C.: The management of pathologic fractures. J. Traumn
13. Johnson, E. W., Jr.: Intramedullary fixation of pathologic fractures. Clin. Orthop. 2108-114, 1953.
14. Kampffmeyer, H. G., Dworkin, H., Carr, E. A.. Jr., and Bull, F. E.: Effect of drug therapy on the up- take of radioactive fluorine by osseous metastases. Clin. Pharmacol. Ther. 8547-657, 1967.
15. Kennedy, B. J.: Hormonal therapies in Breast cancer: androgens versus estrogens. In Breast Cancer, Early and Late. Chicago, Year Book Medical Publish- ers, Inc., 1970; p. 381.
5~792-798, 1965.
No. 3 PATHOLOGIC FRACTURES - Perez et al. 693 16. Lewison, E. F.: Prophylactic versus therapeutic
castration. In Breast Cancer, Early and Late. Chicago, Year Book Medical Publishers, Inc., 1970: p. 363.
17. Marcove, R. C., and Yang, Dah-Jung; Survival times after treatment of pathologic fractures. Cancer 202154-2158. 1967.
18. McLaughlin. H. L.: Intramedullary fixation of pathologic fractures. Clin. Orthop. 2: 108-1 14, 1953.
19. Pamsh, F. F., and Murray, J. A.: Surgical treat- ment for secondary neoplastic fractures: a retrospective study of ninet six patients, J. Bone Joint Surg. 52-A:66!j-686, I&.
20. -, -* . Orthopedic aspects of breast car-
cinoma. In Breast Cancer, Early and Late. Chicago, Year Book Medical Publishers, Inc.. 1970; p. 355.
21. Peltier, L. F.: Theoretical hazards in the treat- ment of pathologic fractures by the Kuntscher intrame- dullary nail. Surgery 29446, 1951.
22. Sears, M. E.: Chemothera y for advanced breast cancer. In Breast Cancer, Ear& and Late. Chicago, Year Book Medical Publishers, Inc.. 1970; p. 387.
23. Takita, H., and Watne, A. L.: Operative treat- ment of pathologic fractures. Surg. Cynecol. Obstet. 116:683-692. 1963.
24. Welch, C. E.: Pathologic fractures due to malig- nant disease, Surg. Gynecol. Obstet. 62735-744, 1936.