Biomechanics of forearm rotation: force and efficiency of pronator teres
Upload
khangminh22Category
view
0download
0
4/19/2019
1
Atlanta Trauma Symposium
Pediatrics: Tips and Tricks
Jorge A. Fabregas, MDEducation Director at Children’s Healthcare of Atlanta at SRChief Of Pediatric Orthopaedics at AMC
Children’s Healthcare of Atlanta
• Forearm fracture fixation• Supracondylar pinning• Lateral condyle fractures• Elastic nails for femur
fractures
Children’s Healthcare of Atlanta
Diaphyseal Forearm
Fractures
WHAT TO ACCEPT
• Up to 10-20° angulation in kids < 10 y/o• No more than 10° angulation >10 y/o• Complete displacement• 30° malrotation• Stabilize floating elbow• Open Fractures • Monteggia ??
1
2
3
4/19/2019
2
Children’s Healthcare of Atlanta
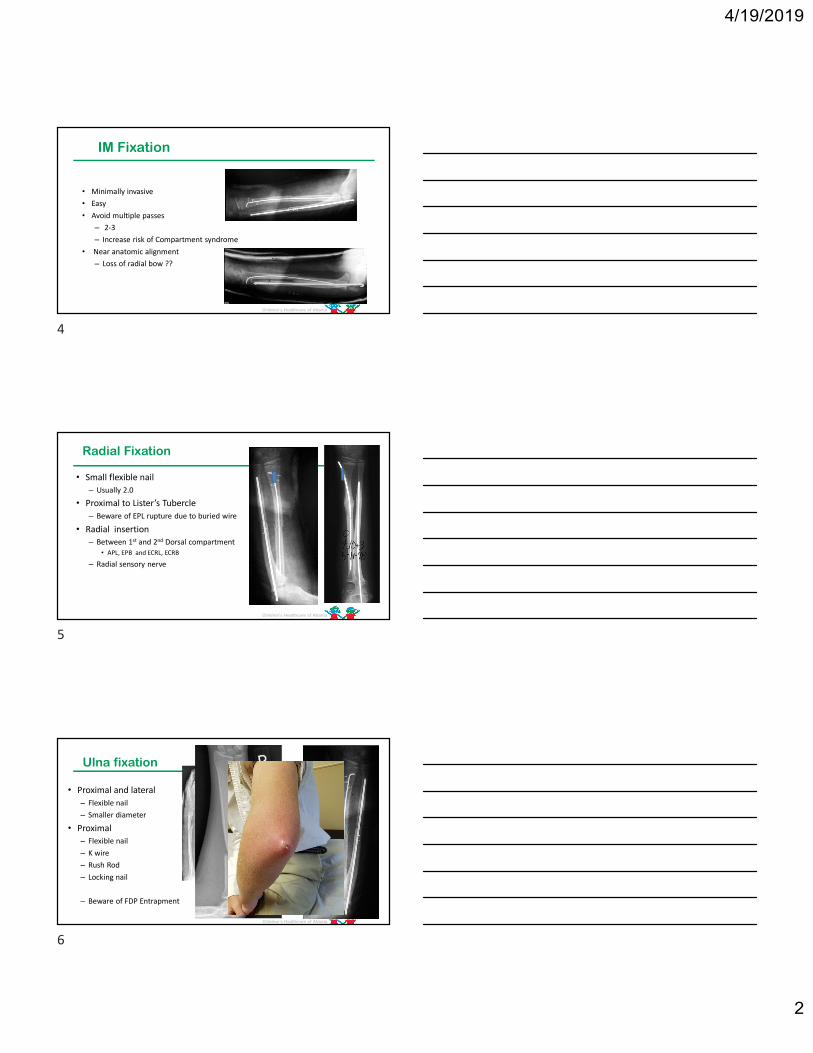
IM Fixation
• Minimally invasive• Easy• Avoid multiple passes
– 2-3– Increase risk of Compartment syndrome
• Near anatomic alignment– Loss of radial bow ??
Children’s Healthcare of Atlanta
Radial Fixation
• Small flexible nail – Usually 2.0
• Proximal to Lister’s Tubercle– Beware of EPL rupture due to buried wire
• Radial insertion– Between 1st and 2nd Dorsal compartment
• APL, EPB and ECRL, ECRB
– Radial sensory nerve
Children’s Healthcare of Atlanta
Ulna fixation
• Proximal and lateral– Flexible nail– Smaller diameter
• Proximal– Flexible nail– K wire– Rush Rod– Locking nail
– Beware of FDP Entrapment
4
5
6

4/19/2019
3
Children’s Healthcare of Atlanta
Single Bone Fixation
• BBFA with distal 1/3 fx radius – Avoid proximal radius fx
• Acceptable reduction• Enough time to remodel
– 8 to 12 year olds– At least 2 years of growth
• Older patients treat as adults
Children’s Healthcare of Atlanta
Plate Fixation
• Advantage– Rigid Fixation– Complete correction of
malrotation– Useful within 1-2 years
of skeletal maturity
• Disadvantage• Larger incisions• Cost• Increase tourniquet time
Children’s Healthcare of Atlanta
Supracondylar Humerus
FracturesPitfalls of Pin
Placement
• Pins Too Close together• Fracture displacement
• Access stability• Get one pin in lateral and one in
medial column
7
8
9

4/19/2019
4
Adequate Reduction?
• No varus/valgus• anterior hum line• minimal rotation• translation OK
From M. Rang, Children’s Fractures
Children’s Healthcare of Atlanta
Best Pinning Technique
• Lateral vs Crossed• Lab results proven in clinical practice• Avoid Late Displacement• Minimize of Cubitus Varus• Decrease Risk Iatrogenic nerve injury
– Median and ulnar nerve reported on both techniques
Children’s Healthcare of Atlanta
Lee et al. –JPO 2002
10
11
12

4/19/2019
5
Children’s Healthcare of Atlanta
Newton et al. JPO 2014
13mm pin spread at fracture site.
Children’s Healthcare of Atlanta
Lateral Pin Entry
maximize separation of pins at fracture siteMaximize
Engage medial and lateral columns proximal to fractureEngage
Engage sufficient bone in distal and proximal fragmentsEngage
Low threshold for 3rd pinLow
13
14
15
4/19/2019
6
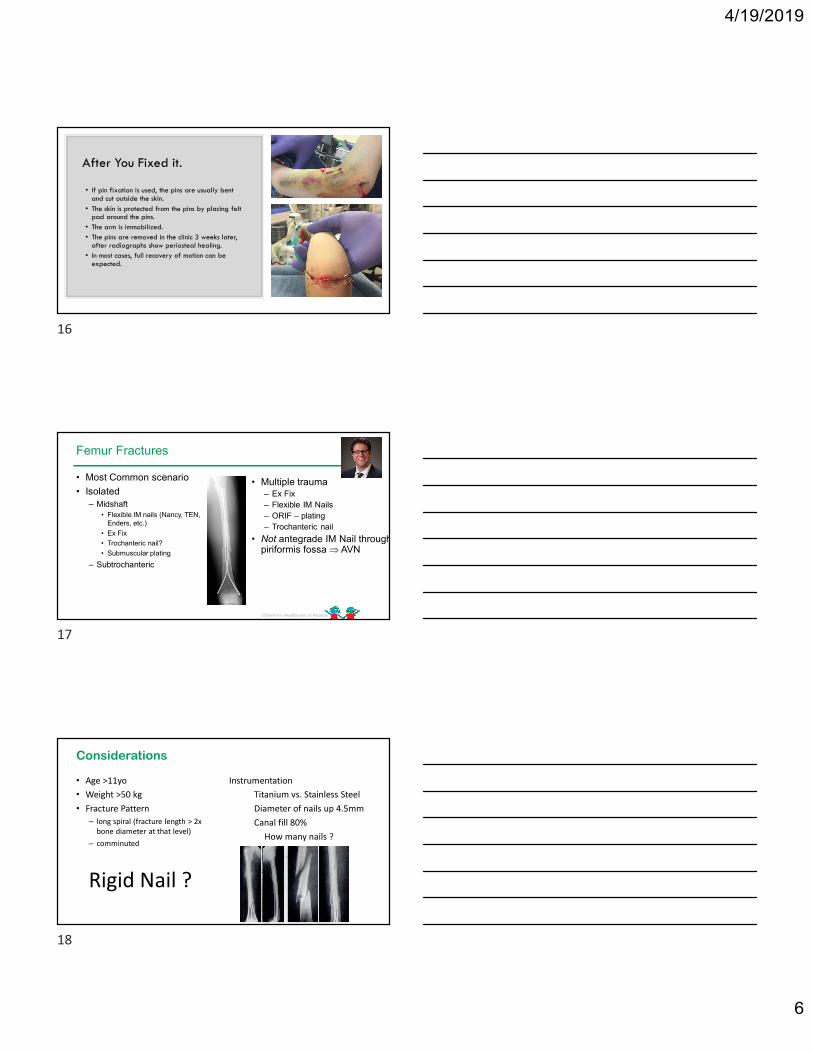
After You Fixed it.
• If pin fixation is used, the pins are usually bent and cut outside the skin.
• The skin is protected from the pins by placing felt pad around the pins.
• The arm is immobilized.• The pins are removed in the clinic 3 weeks later,
after radiographs show periosteal healing.• In most cases, full recovery of motion can be
expected.
Children’s Healthcare of Atlanta
Femur Fractures
• Most Common scenario
• Isolated– Midshaft
• Flexible IM nails (Nancy, TEN, Enders, etc.)
• Ex Fix
• Trochanteric nail?
• Submuscular plating
– Subtrochanteric
• Multiple trauma– Ex Fix– Flexible IM Nails– ORIF – plating– Trochanteric nail
• Not antegrade IM Nail through piriformis fossa AVN
Considerations
• Age >11yo• Weight >50 kg• Fracture Pattern
– long spiral (fracture length > 2x bone diameter at that level)
– comminuted
Rigid Nail ?
InstrumentationTitanium vs. Stainless SteelDiameter of nails up 4.5mmCanal fill 80%
How many nails ?
16
17
18

4/19/2019
7
Unstable Fracture Pattern: Can we flex nail it?
Standard Flexible Nail:Titanium Nails up to 4.5mm
•approach•all distal approach
•2cm incision medially and laterally at level of distal physis•spread with hemostat to starting point 2cm proximal to physis
•instrumentation•nail size determined by multiplying the width of the isthmus of femoral canal by 0.4•the goal is 80% canal fill•Slight bend on tip of nail
•complications•the most common complication is pain at insertion site near the knee
•in up to 40% of patients•recommended that < 25mm of nail protrusion and minimal bend of the nail outside the femur are present
19
20
21
4/19/2019
8
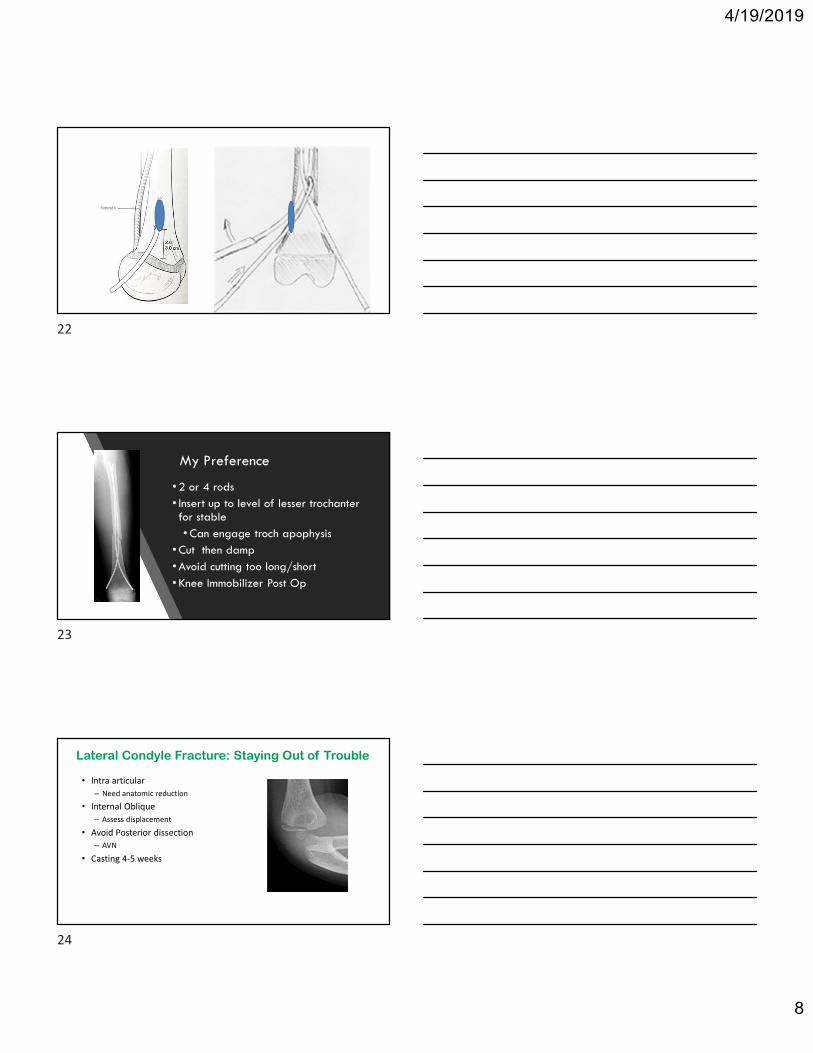
My Preference
• 2 or 4 rods• Insert up to level of lesser trochanter for stable• Can engage troch apophysis
• Cut then damp• Avoid cutting too long/short• Knee Immobilizer Post Op
Lateral Condyle Fracture: Staying Out of Trouble
• Intra articular – Need anatomic reduction
• Internal Oblique– Assess displacement
• Avoid Posterior dissection– AVN
• Casting 4-5 weeks
22
23
24

4/19/2019
9
Lateral Condyle :
Classification
CRPP
ORIF
Indications: CRPP
Children’s Healthcare of Atlanta
Arthrogram• Posterior• 1-2 cc• If prior to fixation may obscure landmarks
25
26
27
4/19/2019
10
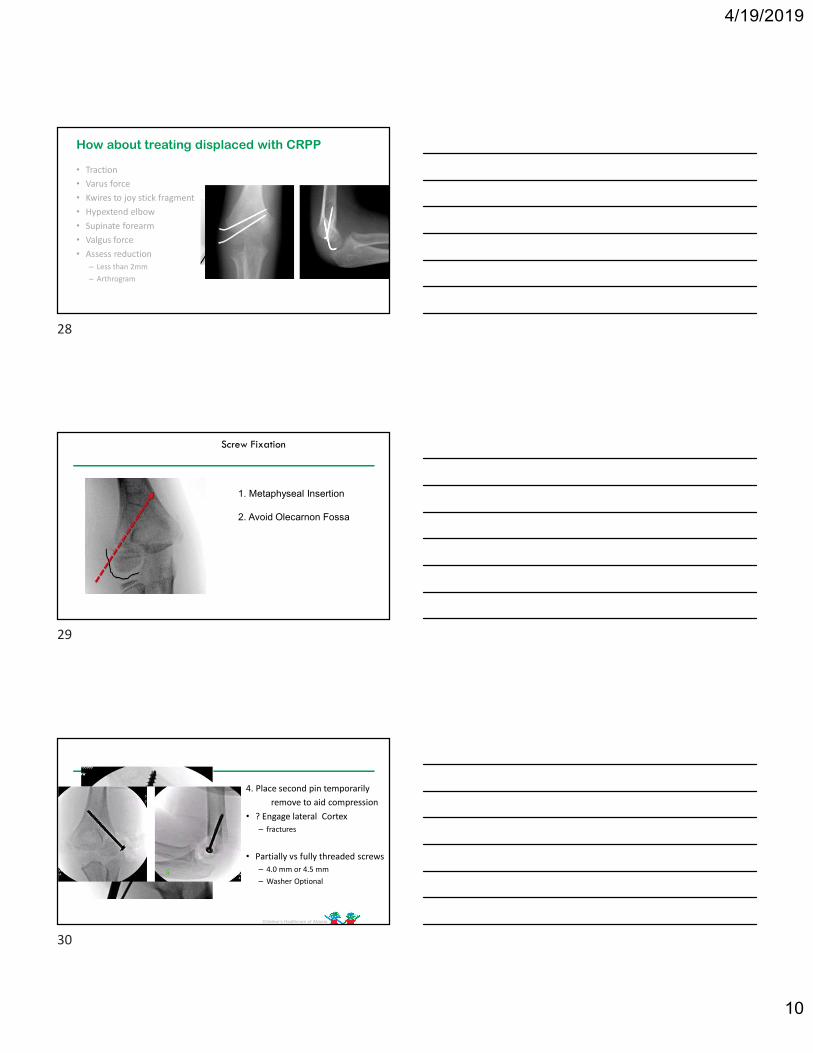
How about treating displaced with CRPP
• Traction• Varus force• Kwires to joy stick fragment• Hypextend elbow• Supinate forearm• Valgus force• Assess reduction
– Less than 2mm – Arthrogram
Alternative:
Screw Fixation
• Bicortical• Use depth gauge for
compression• Check ROM
– Crepitus/clicking• Arthrogram
1. Metaphyseal Insertion
2. Avoid Olecarnon Fossa
Children’s Healthcare of Atlanta
4. Place second pin temporarilyremove to aid compression
• ? Engage lateral Cortex– fractures
• Partially vs fully threaded screws– 4.0 mm or 4.5 mm– Washer Optional
28
29
30

4/19/2019
11
Children’s Healthcare of Atlanta
My Preference
• CRPP minimally displaced(2 to 4 mm) increasing displacement over time intra-articular extension on an arthrogram
• Can attempt closed reduction on displaced
• Displaced fractures are best treated with open reduction and internal fixation
• Pin FixationScrew fixation for delayed unionsUnreliable family
Children’s Healthcare of Atlanta
Thank You !
Jorge A. Fabregas, MDCel (770)880-8029
31
32
Copyright © 2022 FDOKUMEN