
Computerized tomography of proximal femoral trabecular patterns
12
Journal of Orthopaedic Resenrch 4:45-56, Raven Press, New York 0 1986 Orthopaedic Research Society Computerized Tomography of Proximal Femoral Trabecular Patterns Roger Kerr, Donald Resnick, David J. Sartoris, Sevil Kursunoglu, "Carlos Pineda, TParviz Haghighi, $Guerdon Greenway, and Jose Guerra, Jr. Departments of Diagnostic Radiology, *Medicine, and ?Pathology, Veterans Administration Medicnl Center and the University of California Hospital, San Diego, California; and #Department of Radiology, Baylor University Medical Center, Dallas, Texas Summary: A comprehensive imaging and pathologic investigation utilizing pa- tients and cadaver material was performed in order to identify the normal tra- becular pattern of the proximal femur and to assess alterations in this pattern in various disorders. Patients and specimens were studied with computed to- mography (CT), including three-dimensional CT image reconstruction in se- lected cases and plain film radiography. The CT imaging of the proximal femur provides insight into the dynamic state of bone in this region. Despite limited resolution, three-dimensional CT image reconstruction is capable of portraying the concentration and orientation of major trabeculae in the proximal femur. Increased trabecular spacing occurs in osteoporosis and is well depicted by CT. Proliferation and thickening of the most superior subchondral primary compressive trabeculae is an early sign of osteoarthritis. In the region of the calcar fernorale, crossing trabeculae, similar to the appearance of an enchon- droma or bone infarct, have been described in osteoporosis and osteoarthritis and probably represent unmasking of normally present reinforcing trabeculae. In ischemic necrosis, CT should be considered a useful modality for detection of early or mild alterations and may be valuable in treatment planning. Key Words: Femur head-Femur head necrosis-Femur neck-osteoarthritis- Osteoporosis. The internal architecture of the proximal femur has been well described and is composed of two major trabecular systems arranged along the lines of compressive and tensile stress produced during weight bearing (18,29,31). Adaptive alterations of these trabecular patterns occur when there is a Dr. Kerr's current address is Department of Radiology, Los Angeles County-University of Southern California Medical Center, Los Angeles, California. Dr. Pineda's current address is Instituto Nacional de Cardi- ologia, Ignacia Chavez, Mexico City, Mexico. Address correspondence and reprint requests to D. Resnick at Department of Radiology, Veterans Administration Medical Center, 3350 LaJolla Village Drive, San Diego, CA 92161, U.S.A. change in the vectors of forces acting upon the hip, with alteration in the external configuration of the proximal femur and in disease states characterized by bone resorption (2,20,27,35). In the past, con- ventional radiography has been used in order to as- sess the presence and extent of such alterations in the trabecular systems. Such alterations may be a clue to underlying disease and alternatively, in some locations, may simulate disease. For ex- ample, sequential resorption of trabecular units may indicate osteoporosis and interruption of the trabecular lines may be a subtle sign of fracture of the femoral neck. Computed tomography (CT) pro- vides excellent visualization of these trabeculae and, in comparison with conventional radiography, 45
Transcript of Computerized tomography of proximal femoral trabecular patterns

Journal of Orthopaedic Resenrch 4:45-56, Raven Press, New York 0 1986 Orthopaedic Research Society
Computerized Tomography of Proximal Femoral Trabecular Patterns
Roger Kerr, Donald Resnick, David J. Sartoris, Sevil Kursunoglu, "Carlos Pineda, TParviz Haghighi, $Guerdon Greenway, and Jose Guerra, Jr.
Departments of Diagnostic Radiology, *Medicine, and ?Pathology, Veterans Administration Medicnl Center and the University of California Hospital, San Diego, California; and #Department of Radiology,
Baylor University Medical Center, Dallas, Texas
Summary: A comprehensive imaging and pathologic investigation utilizing pa- tients and cadaver material was performed in order to identify the normal tra- becular pattern of the proximal femur and to assess alterations in this pattern in various disorders. Patients and specimens were studied with computed to- mography (CT), including three-dimensional CT image reconstruction in se- lected cases and plain film radiography. The CT imaging of the proximal femur provides insight into the dynamic state of bone in this region. Despite limited resolution, three-dimensional CT image reconstruction is capable of portraying the concentration and orientation of major trabeculae in the proximal femur. Increased trabecular spacing occurs in osteoporosis and is well depicted by CT. Proliferation and thickening of the most superior subchondral primary compressive trabeculae is an early sign of osteoarthritis. In the region of the calcar fernorale, crossing trabeculae, similar to the appearance of an enchon- droma or bone infarct, have been described in osteoporosis and osteoarthritis and probably represent unmasking of normally present reinforcing trabeculae. In ischemic necrosis, CT should be considered a useful modality for detection of early or mild alterations and may be valuable in treatment planning. Key Words: Femur head-Femur head necrosis-Femur neck-osteoarthritis- Osteoporosis.
The internal architecture of the proximal femur has been well described and is composed of two major trabecular systems arranged along the lines of compressive and tensile stress produced during weight bearing (18,29,31). Adaptive alterations of these trabecular patterns occur when there is a
Dr. Kerr's current address is Department of Radiology, Los Angeles County-University of Southern California Medical Center, Los Angeles, California.
Dr. Pineda's current address is Instituto Nacional de Cardi- ologia, Ignacia Chavez, Mexico City, Mexico.
Address correspondence and reprint requests to D. Resnick at Department of Radiology, Veterans Administration Medical Center, 3350 LaJolla Village Drive, San Diego, CA 92161, U.S.A.
change in the vectors of forces acting upon the hip, with alteration in the external configuration of the proximal femur and in disease states characterized by bone resorption (2,20,27,35). In the past, con- ventional radiography has been used in order to as- sess the presence and extent of such alterations in the trabecular systems. Such alterations may be a clue to underlying disease and alternatively, in some locations, may simulate disease. F o r ex- ample, sequential resorption of trabecular units may indicate osteoporosis and interruption of the trabecular lines may be a subtle sign of fracture of the femoral neck. Computed tomography (CT) pro- vides excellent visualization of these trabeculae and, in comparison with conventional radiography,
45

46 R. KERR E T A L
may allow earlier diagnosis of a variety of bone dis- eases. We set out to perform a comprehensive imaging and pathologic investigation utilizing pa- tients and cadaver material in order to identify the normal trabecular pattern of the femoral head and neck and to assess alterations in this pattern oc- curring in various disorders.
arches intersecting one another at roughly right angles (Fig. 1). The principal compressive trabec- ulae extend from the proximal medial cortex of the femoral neck to the superior articular surface of the femoral head in a fan-like radiating pattern. These represent the thickest and most tightly-packed tra- beculae in the upper femur. A secondary compres- sive group arises from the medial cortex just below
MATERIALS AND METHODS
Twenty patients, ten cadavers (VA Medical Center, San Diego, CA), and 35 macerated spec- imens (Museum of Man, San Diego, CA) were studied. Patients were selected on the basis of ra- diographic abnormalities of the proximal femoral trabecular pattern due to osteoporosis, ischemic necrosis, osteoarthritis, and other processes. In all patients and cadavers, plain film radiography and CT, using a Technicare 2060 Scanner, were ob- tained. The routine plain films consisted of antero- posterior and lateral projections of the hip (pa- tientdcadavers) or proximal femur (macerated specimens). The CT was accomplished utilizing 5-mm-thick axial slices obtained every 3 mm or every 5 mm from the superior aspect of the femoral head to a level just below the most caudal extent of the calcar femorale. Axial sections 3-5 mm in thickness from all specimens, derived from surgical material and cadavers, were radiographed in a Fax- itron, macerated in commercial Clorox solution, and photographed. Major trabecular groups, the subchondral bone plate, the cortex of the medial femoral neck, and the calcar, were identified.
Three macerated femoral specimens from the Hrdlicka collection of the San Diego Museum of Man were photographed, radiographed, and axially imaged with CT, using 2-mm-thick slices at 22 mm intervals. Each specimen represented a different pattern of proximal femoral morphology, including varus deformity, severe osteoarthritis with medial cortical buttressing, and normal architecture. Mul- tiplanar reformation and three-dimensional image reconstruction were performed from CT data using a Contour Medical Systems Cemax 1000 in order to optimize visualization of trabecular arrangement.
RESULTS
Normal Patterns
Conventional radiography reveals two principal and two secondary trabecular groups oriented as
the principal compressive group and curves up- wards and laterally towards the greater trochanter. The primary tensile group arises from the lateral cortex just below the greater trochanter and curves upward and medially across the femoral neck, ending at the inferomedial aspect of the femoral head. This group is thinner and less closely spaced compared to the primary compressive group. A secondary tensile group arises from the lateral cortex just inferior to the primary tensile group and arches upward and medially across the femoral neck, ending just after crossing the midline. A greater trochanter group of tensile trabeculae is variably identified, arising from the lateral cortex just above the principal tensile group and curving superolaterally toward the top of the greater tro- chanter. The principal and secondary compressive trabeculae and principal tensile trabeculae enclose an area with a relative paucity of bone trabeculae termed the “trigonum internum fernoris” or Ward’s triangle.
The CT imaging in the axial plane demonstrates the primary compressive trabeculae as a dense in-
PRINCIPAL
SECONDARY TENSILE GROUP
/ I FIG. 1. A schematic diagram depicts the principal and sec- ondary trabeculae in the stress regions of the proximal femur. Ward’s triangle lies within the neutral axis where compressive and tensile forces balance one another and contains thin, widely spaced trabeculae. Drawing after Singh, et al. (29).
J Orthop Res, Vol. 4, N o , I , 1986

PROXIMAL FEMORAL PATTERNS 47
terconnecting network of sheets composed of thick trabecular units. Inferiorly, these trabeculae blend into the medial femoral cortex. The cancellous bone of the primary compressive group and the me- dial femoral cortical bone are continuous and func- tion together to resist compressive stresses, which are maximal along this axis. The medial femoral cortex is thickest proximally and diminishes to a thickness equal to that of the remainder of the cortex at the level of the lesser trochanter. The pri- mary compressive trabeculae gradually become thinner and less closely spaced as they approach the superior articular surface of the femoral head where the compression forces are more widely dis- tributed.
The primary tensile group and, indeed, the re- mainder of the trabecular groups appear as an in- terwoven network of sheets; however, the indi- vidual trabeculae are not as thick nor as closely spaced as those of the primary compressive group. Axial sections through the femoral neck clearly demonstrate Ward’s triangle as an area of thin widely-spaced trabeculae bordered medially by the primary compressive group and laterally by the pri- mary tensile group (Fig. 2). The secondary com- pressive and tensile trabeculae are visualized within the medullary canal at approximately the level of the lesser tuberosity. Inferiorly, the central hollow of the medullary canal is visualized between these trabeculae.
Within the femoral head the primary compressive trabeculae and the medial portion of the primary tensile group combine to form an area of apparent condensation of bone that on axial section and axial CT imaging appears to radiate from the center in
the pattern of an asterisk or star (Fig. 3) (5 ) . The majority of the trabeculae constituting the asterisk are thick, closely-spaced primary compressive tra- beculae. The radiating pattern probably reflects a resistive response to a centripetal pattern of com- pressive force extending from a broad area of the articular surface toward the axis of the primary compressive trabeculae.
The calcar femorale is a dense vertical plate of bone that originates in the posteromedial cortex above the lesser trochanter and extends caudally for approximately 5 cm before merging with the trabeculae of the upper diaphysis. It is well visual- ized in a frog lateral view of the hip where it ap- pears to extend inferiorly into the cancellous bone as an extension of the posteromedial cortex. During growth the calcar develops as a cortical extension of the original shaft of the femur as the trochanters form and enlarge to points of tendon insertion (10). The calcar functions to preserve the continuity of the cylindrical femoral shaft, which is interrupted by the formation of the lesser trochanter and pro- vides resistance to the compressive stresses in this region (12). It is oriented transversely on axial sec- tions through its superior portion and on lower sec- tions it assumes a more oblique orientation ex- tending in a posterolateral direction from the me- dial cortex toward the gluteal tuberosity (Fig. 4). Its connection with the medial femoral cortex shifts progressively anteriorly as one proceeds in an infe- rior direction so that rather than being a flat sheet of bone the calcar more resembles a ribbon with a slight twist or a portion of a spiral (Fig. 5) . The calcar and medial cortex are both of maximal width and thickness superiorly at the upper margin of the
FIG. 2. A specimen photograph (A) and radiograph (B) of an axial section through the femoral neck reveal Ward’s triangle (black arrow) as an area of relative paucity of trabeculae, bordered medially by primary compressive trabeculae (white arrows) and laterally by primary tensile and secondary compressive trabeculae (arrowhead).
J Orthop Re.7, Vol, 4, No. I , I986
48
3A,B
R. KERR ET AL.
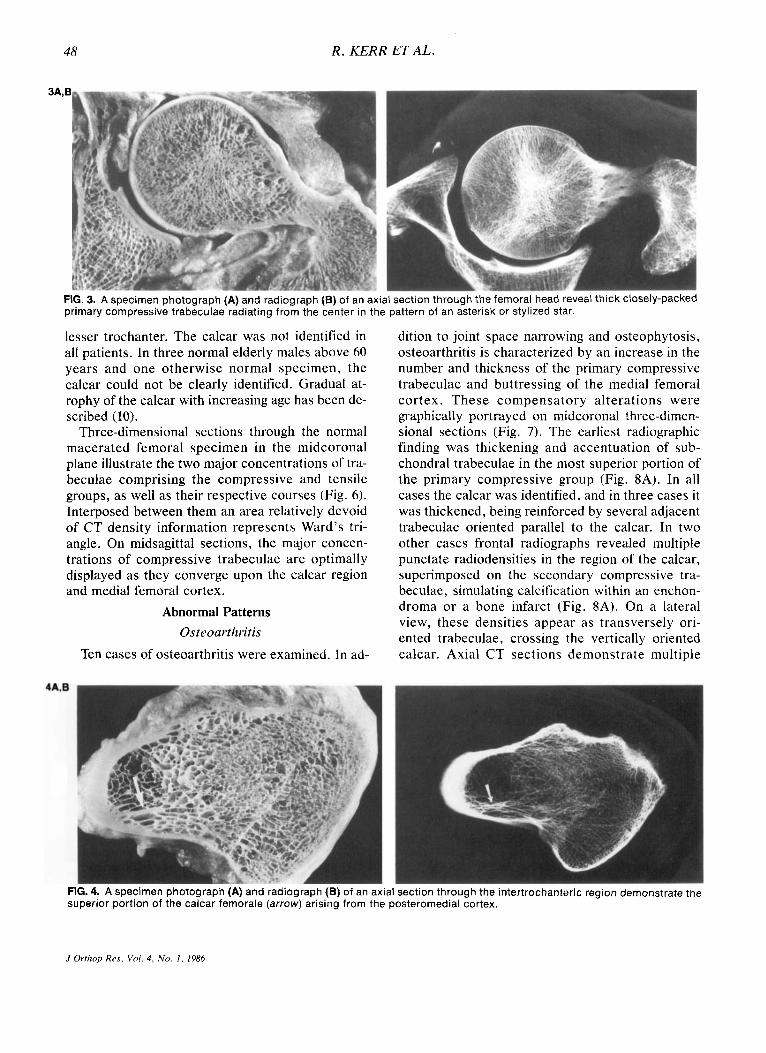
FIG. 3. A specimen photograph (A) and radiograph (B) of an axial section through the femoral head reveal thick closely-packed primary compressive trabeculae radiating from the center in the pattern of an asterisk or stylized star.
lesser trochanter. The calcar was not identified in all patients. In three normal elderly males above 60 years and one otherwise normal specimen, the calcar could not be clearly identified. Gradual at- rophy of the calcar with increasing age has been de- scribed (10).
Three-dimensional sections through the normal macerated femoral specimen in the midcoronal plane illustrate the two major concentrations of tra- beculae comprising the compressive and tensile groups, as well as their respective courses (Fig. 6). Interposed between them an area relatively devoid of CT density information represents Ward’s tri- angle. On midsagittal sections, the major concen- trations of compressive trabeculae are optimally displayed as they converge upon the calcar region and medial femoral cortex.
Abnormal Patterns Osteoarthritis
Ten cases of osteoarthritis were examined. In ad-
dition to joint space narrowing and osteophytosis, osteoarthritis is characterized by an increase in the number and thickness of the primary compressive trabeculae and buttressing of the medial femoral cortex. These compensatory alterations were graphically portrayed on midcoronal three-dimen- sional sections (Fig. 7). The earliest radiographic finding was thickening and accentuation of sub- chondral trabeculae in the most superior portion of the primary compressive group (Fig. 8A). In all cases the calcar was identified, and in three cases it was thickened, being reinforced by several adjacent trabeculae oriented parallel to the calcar. In two other cases frontal radiographs revealed multiple punctate radiodensities in the region of the calcar, superimposed on the secondary compressive tra- beculae, simulating calcification within an enchon- droma or a bone infarct (Fig. 8A). On a lateral view, these densities appear as transversely ori- ented trabeculae, crossing the vertically oriented calcar. Axial CT sections demonstrate multiple
FIG. 4. A specimen photograph (A) and radiograph (B) of an axial section through the intertrochanteric region demonstrate tne superior portion of the calcar femorale (arrow) arising from the posteromedial cortex.
J Orthop Res, Vol. 4, No. 1 , 1986

PROXIMAL FEMORAL PATTERNS 49
FIG. 5. A sagittal reformatted CT image (below) derived from reconstruction of axial CT images (above) reveals the calcar femorale (open arrow) extending anteriorly as it proceeds inferiorly. A, anterior; P, posterior; closed arrow, lesser tro- chanter.
linear trabeculae running in an anterior to posterior direction, intersecting the calcar at right angles (Fig. 8B). These trabeculae may function to but- tress the calcar. In one case, the “asterisk” tra- becular pattern of the femoral head was completely disrupted due to the formation of multiple large subchondral cysts. Such subchondral cysts of vari- able size were commonly identified in cases of moderate or severe osteoarthritis.
Coxa Vara and Coxa Valga
We examined six cases of acquired coxa vara and five cases of acquired coxa valga. In coxa vara there is a decrease in the angle between the neck and shaft of the femur with consequent increased tensile and bending stress across the femoral neck. In response to this shift in biomechanical demand, we observed considerable accentuation of the pri- mary tensile trabeculae and buttressing of the prox- imal medial femoral cortex. CT revealed thickening and closer spacing of trabecular units. Three-di-
FIG. 6. A midcoronal three-dimensional CT section of a normal macerated specimen demonstrates primary com- pressive trabeculae (arrow), secondary compressive tra- beculae (curved arrow), and Ward’s triangle (arrowhead).
mensional sections in the mid-coronal plane dem- onstrated prominent concentrations of tensile tra- beculae and mild medial cortical buttressing in the macerated femur with varus deformity. There was no .change in the appearance of the calcar. Sec- ondary changes of osteoarthritis were observed in three of the six cases with varying degrees of os- teophyte formation, sclerosis and eburnation, and subchondral cyst formation.
In coxa valga, the femoral neck and shaft form an
FIG. 7. Osteoarthritis: A midcoronal three-dimensional CT section of a macerated specimen with osteoarthritis reveals a flattened femoral head with inferomedial osteophytosis, thickening of the primary compressive group (arrow), and medial cortical buttressing (arrowhead).
J Ortkop Res , Vol . 4 . No. 1, 1986

50 R . KERR ET AL.
FIG. 8. Osteoarthritis: A frontal radiograph (A) reveals inferomedial osteophytosis and a wedge-shaped pattern of sclerosis and trabecular thickening involving the superior portion of the femoral head. Punctate and linear radiodensities identified in the calcar region (arrowheads) are seen on axial CT section (B) to represent curvilinear trabeculae (closed arrows) crossing perpen- dicular to the calcar (open arrow) in an anterior to posterior direction.
obtuse angle and compression forces are intensi- fied. An increase in the number and thickness of primary compressive trabeculae were observed on plain films and CT in all cases. Although CT pro- vides insight into the thickness and spacing of tra- beculae, the alteration in the overall trabecular pat- tern in coxa vara and coxa valga is more graphi- cally demonstrated by plain film radiography.
Osteoporosis
We examined fourteen proximal femora from eight specimens, two cadavers, and two patients with bone resorption corresponding to a Singh index of five or lower. The Singh index is a system
of roentgenographic grading that was devised to classify patterns of trabecular resorption in osteo- porosis with grade six representing the normal pat- tern and grade one severe osteoporosis (29). Grade four represents the border between normal and os- teoporosis.
We did not attempt to correlate the grades of the Singh index with the presence of spinal osteo- porosis or bone mineral content, recognizing that the validity of the Singh index as a measurement of osteoporosis has been questioned in several studies (17,19,21,34). Rather, we set out to correlate pat- terns of trabecular resorption with changes in the CT appearance of the trabecular meshwork. Where plain films revealed loss of compressive or tensile
FIG. 9. Osteopenia: A frontal radiograph (A) and an axial CT section (B) of a macerated specimen with bone resorption (Singh grade four) demonstrate increased trabecular spacing and enlargement of Ward's triangle (arrow).
J Orthop Res , Vol. 4, N o . 1 , 1986
PROXIMAL FEMORAL PATTERNS 51
trabeculae, CT revealed bony resorption, mani- fested as increased trabecular spacing in the corre- sponding areas on axial section (Fig. 9). All prox- imal femora with a grade of six (normal pattern) re- vealed a normal meshwork of trabeculae without focal or diffuse bony resorption.
In ten of fourteen patients and specimens with bone resorption, multiple linear transversely-ori- ented trabeculae intersected the calcar, coursing in an anterior to posterior direction and appeared as punctate radiodensities on the frontal view and as transverse lines on the lateral view. These trabec- ulae are identical to those described above in cases
of osteoarthritis and probably represent “un- masking” of pre-existent trabeculae by the resorp- tive process of osteoporosis.
One patient presented a similar plain film appear- ance of increased radiodensity in the calcar region and a Singh grade three trabecular pattern. How- ever, CT revealed multiple rounded radiodensities of variable size and truncation of the lateral portion of the calcar. The patient was later shown to have metastatic prostate carcinoma in this region and the above findings were due to blastic and lytic changes related to the local effects of tumor.
A 45-year-old woman with transient osteoporosis
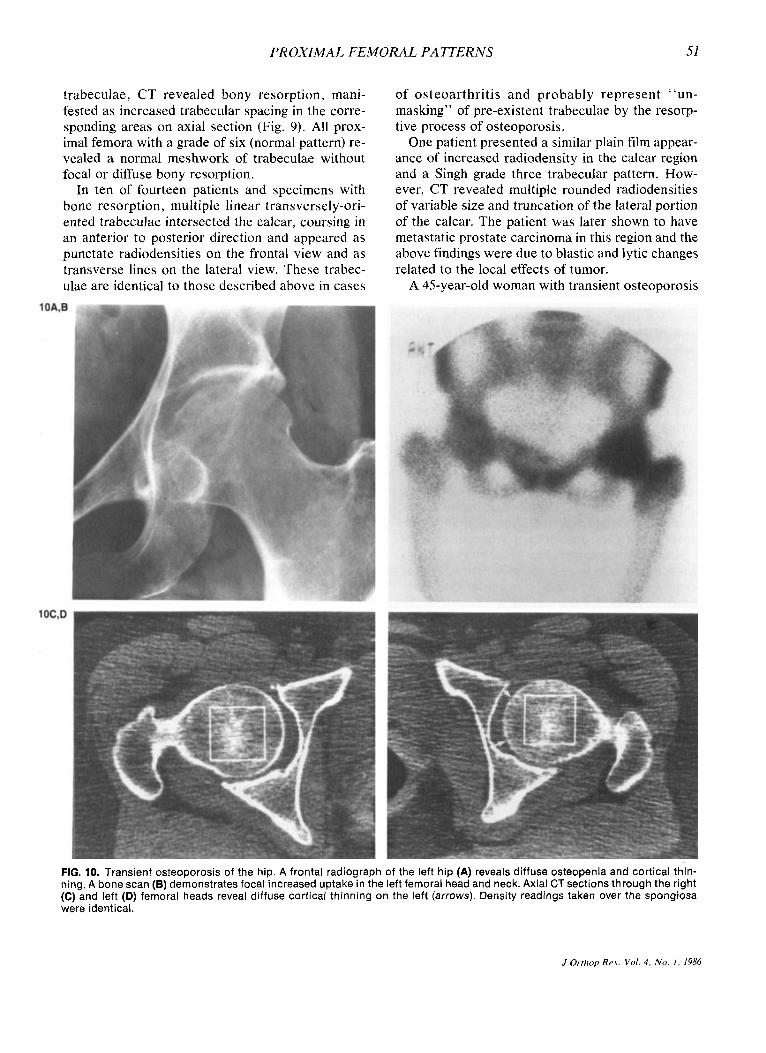
FIG. 10. Transient osteoporosis of the hip. A frontal radiograph of the left hip (A) reveals diffuse osteopenia and cortical thin- ning. A bone scan (B) demonstrates focal increased uptake in the left femoral head and neck. Axial CT sections through the right (C) and left (D) femoral heads reveal diffuse cortical thinning on the left (arrows). Density readings taken over the spongiosa were identical.
J Orthop Res, Vnl. 4, N o . I , 1986

52 R. KERR E T A L .
of the left hip was included in this study (Fig. 10). Hip pain began spontaneously without an ante- cedent history of trauma or infection. The clinical course was self-limited with full recovery after 8 months. Plain films revealed diffuse loss of bone density with preservation of the normal trabecular pattern in the femoral head and neck. On bone scan there was prominent focally increased uptake of the radiopharmaceutical in the region of the femoral head, probably reflecting hyperemia. CT examina- tion revealed loss of cortical bone without involve- ment of the cancellous bone, and upon healing, there was reconstitution of cortical bone. In the acute phase, there was no significant difference be- tween CT density readings taken over the spon- giosa of the involved and uninvolved femoral heads.
Ischemic Necrosis
We examined six patients and one specimen with varying stages of ischemic necrosis of the femoral head. On plain films, classic findings were ob- served including alternating radiolucency and scle- rosis, flattening or collapse of the femoral head, and a subchondral crescent sign. In two cases with mild plain film changes, CT revealed significant al- terations of the asterisk trabecular pattern in the femoral head consisting of clumping and sclerosis of peripheral trabeculae (Fig. 11). More advanced phases of necrosis were associated with central or peripheral circular areas of radiolucency sur- rounded by well-defined reactive bone sclerosis. In one case, CT revealed subtle collapse of the artic- ular surface and radiolucent gas within the femoral
head not appreciated on plain films. Reformatted imaging was utilized in selected cases and per- mitted identification of subchondral fracture and accurate assessment of the extent and distribution of collapse of the articular surface. More severe al- terations of the trabecular pattern in the femoral head, including complete bony disruption and wide- spread osteonecrosis, were identified in the most advanced cases.
Paget Disease
We examined one specimen with Paget disease. The apparent Singh index was grade six; however, CT revealed extensive osteolysis as large cystic spaces were present throughout the femoral head and neck (Fig. 12). The degree of osseous resorp- tion and trabecular spacing was comparable to that seen with a grade one Singh index. The primary compressive trabeculae, the calcar, and the endos- teal cortex were relatively spared from the lytic process and appeared dense and sclerotic com- pared to other remaining trabeculae. The entire outer circumference of the cortex was composed of low-density, apparently poorly mineralized, cor- tical, and periosteal pagetic bone.
DISCUSSION
The internal architecture of the proximal femur is composed of two major systems of bony trabeculae oriented along the lines of maximal compressive and tensile stresses. Their direction is dependent upon the external configuration of the proximal femur, the effects of muscle pull, and the resultant
FIG. 11. Ischemic necrosis. A frontal radiograph (A) reveals advanced changes of ischemic necrosis in the right femoral head with collapse, rarefaction, and sclerosis. The left femoral head is unremarkable except for possible sclerosis in its superior portion. An axial CT section (B) through the left femoral head reveals wedge-shaped sclerosis extending posteromedially to the periphery consistent with early reparative change of ischemic necrosis.
J Orthop Rrs, Vol. 4, No. I , I986

PROXIMAL FEMORAL PATTERNS 53
FIG. 12. Paget disease. A frontal radiograph (A) demonstrates cortical thickening and coarsened trabeculae throughout the proximal femur. Axial CT sections through the femoral head (6) and calcar (C) reveal extensive osteolysis with formation of large cyst-like spaces. The primary compressive trabeculae, endosteal cortex, and calcar are relatively preserved and are of increased density
vectors of compressive, tensile, bending, and shearing forces to which the femur is subjected upon weight bearing. The neutral axis defines a central region where compressive and tensile forces balance one another. Above the neutral axis the predominant stress is tensile and that below the neutral axis is compressive. The proximal femur has been compared to a streetlight bracket (33). The inner obliquely-oriented bar withstands com- pression and also acts to reduce the pulling effect on the screws fastening the tension bar to the lamp post. The central portion of the bracket does not offer significant support and is, therefore, designed as a gap in the metal structure similar to the devel- opment of Ward’s triangle.
It has been proposed that the guiding principle in skeletal modeling and remodeling is “strain reduc- tion” (8). This may be accomplished by bone for- mation and resorption to meet changing biome- chanical demands and minimize strain with a resul- tant change in the internal architecture or external configuration of bone, or both. For example, the anatomic varus position of the femoral neck func- tions to counteract the valgus bending force of the adductor muscles and confers a mechanical advan- tage on the abductor muscles by providing a lever arm. In coxa vara and coxa valga, alterations in the magnitude and direction of compressive and tensile forces result in a shift of the neutral axis and com- pensatory alterations in the principal compressive and tensile trabecular groups.
We have found that CT, with and without three- dimensional image reconstruction, is useful in de- fining alterations in the normal trabecular pattern in various disorders. The CT of a specimen with Paget
disease revealed the effects of biochemical factors in preservation of the most essential trabeculae for weight-bearing. The plain film appearance sug- gested a near normal Singh index; however, the CT findings indicate that this was due to trabecular coarsening and cortical thickening. The Singh index does not take into account cortical thickness and is not applicable to proximal femora with bone de- formity, such as coxa vara, coxa valga, or primary bone disease (19). CT revealed extensive osteolysis of the internal cancellous bone, reflecting the pre- vious lytic phase of disease. The only remaining trabeculae, which appeared increased in density, were the primary compressive group, the calcar, and the inner cortex of the proximal shaft. Maximal compressive force passes through an axis including the primary compressive trabeculae and the calcar and is distributed along the circumference of a tu- bular bone. Although their increased density may reflect apposition of dense mineralized pagetic bone, the relative preservation of these portions of the proximal femur in this specimen supports the concept of compressive and tensile forces acting in addition to local metabolic factors as mechanical effectors on bone formation in areas designed to re- sist these forces (7).
In the proximal femur, bone resorption occurs in a definite order depending on trabecular thickness, reflecting a hierachy of function of the trabecular groups in meeting the mechanical demands of weight bearing. The internal architecture is deter- mined by balancing the effect of compressive and tensile forces on bone formation against the resorp- tive effect of increasing age or osteoporosis. Plain film radiography demonstrates that secondary com-
J Orthop Rrs, Vol. 4, N o . I , 1986

54 R. KERR E T A L .
pressive and tensile trabeculae and the thin tra- beculae in the adjacent spongiosa are resorbed first and Ward’s triangle enlarges and becomes more ra- diolucent. This is followed by progressive loss of primary tensile trabeculae, with bone loss occur- ring centrally then peripherally until the entire pri- mary tensile group is no longer discernible. The thick and compact primary compressive group re- mains as the only prominent trabeculae and are the last to be resorbed with progression of osteo- porosis. Complete resorption of thinner trabeculae results in coarsening of the remaining trabeculae as they stand out against the background of adjacent marrow elements.
The Singh index was designed to reflect bone structure rather than bone quantity with the goal of providing a means of detecting osteoporosis without resorting to quantitation of bone density, mineral content, or cortical thickness. Singh rea- soned that the internal architecture of the femur is independent of these variables and the trabecular pattern will be normal when the total amount of bone is physiologic for any one individual (29). While its utility has been touted by some (4,13,30), other investigators report a lack of correlation of the Singh index with bone density, mass, or mineral content, and have concluded that it is not of prog- nostic value in predicting the risk of fracture (17,19,21,34). The results of several studies indicate that bone density or bone mass are the principal determinants of bone strength, and that the Singh index does not correlate with the force or stress re- quired to break bone (3,9,16,21).
The CT of 14 specimen and patient femora with mild degrees of bone resorption on plain films. Tra- becular resorption was most prominent in those areas with the thinnest trabeculae in accordance with histoquantitative data, which reveal a fourfold greater increase in trabecular spacing in such re- gions with increasing age compared to that in the principal compressive region (7). In those instances where assignment of a Singh index was difficult, we found analysis of the plain film appearance of Ward’s triangle useful. As one proceeds from grade five to grade three, Ward’s triangle progressively enlarges and contains fewer identifiable trabeculae. The CT confirmed assignment of Singh grade to the extent that trabecular spacing, as shown by CT, was qualitatively the same among proximal femora with the same Singh index.
The lack of correlation between the Singh index and bone mineral content or bone density remains
to be resolved. Plain film radiography and CT permit detection of increased trabecular spacing, reflecting complete resorption of trabecular units, but discrimination of trabecular thickness is poor due to limited resolution. This limitation may be significant, for changes in trabecular thickness dis- tributed throughout the volume of cancellous bone can lead to a significant loss of bone mass without noticeably affecting trabecular spacing (7). More- over, in imaging the proximal femur in vivo, problems arise owing to the large amount of over- lying soft tissue giving rise to scattered radiation, beam hardening, and nonuniformity of the beam over the entire field. Digital radiography offers methods to significantly reduce scattered radiation and beam hardening, and quantitative digital imaging of the proximal femur may provide further insight in the near future (6).
Methods to quantify osteoporosis involve the measurement of either cortical or trabecular bone mass. Cortical and cancellous bone do not neces- sarily demonstrate parallel involvement and the ex- tent of resorption of each depends on the type of osteoporosis and the site of measurement. For ex- ample, whereas senile osteoporosis involves a pro- portionate loss of both cortical and trabecular bone, postmenopausal osteoporosis involves a dis- proportionate loss of trabecular bone from the axial skeleton and cortical bone loss from the appen- dicular skeleton (26). In a 45-year-old woman with transient osteoporosis of the hip, we observed pre- dominant resorption of cortical bone in the absence of significant loss of trabecular bone.
A pattern of preferential resorption of compact cortical bone in a young individual would be diffi- cult to explain, given the greater surface area of trabecular bone. It has been argued that due to the greater surface-to-volume ratio of trabecular bone for the same degree of negative bone balance per surface unit, the volume of spongy bone will de- crease faster than that of cortical bone (14). How- ever, osteoporosis may develop faster in cortical than trabecular bone in middle-aged and elderly pa- tients due to the decline in trabecular bone, which begins in early adulthood. Complete resorption of thinner trabeculae and retention and buttressing of the thick remaining trabeculae cause a significant loss of surface area and the formation of porous cancellous bone. With continued bone resorption the porosity of such cancellous bone increases at a progressively decreasing rate. In cortical bone, en- dosteal and intracortical resorption result in a pro-
J Orthrip Res, Vol. 4, No. I , 1986

PROXIMAL FEMORAL PATTERNS 55
gressive increase in surface area and a progres- sively increasing or geometric rate of bone resorp- tion (22). Data exist in the middle-aged or elderly patient indicating that the effect of progressive or accelerated bone resorption is most readily de- tected in cortical bone (15). One cannot be certain if the predominant cortical bone loss in our patient is a reflection of the relative surface areas of cor- tical and trabecular bone or a reflection of primary involvement of cortical bone, as in hyperparathy- roidism.
In 71% (10/14) of patients and specimens with bone resorption, several fine radiodense lines were appreciated in the region of the calcar on the frog lateral view, appearing as punctate radiodensities when viewed en face on the frontal view. CT re- vealed multiple thin trabeculae oriented in an an- terior to posterior direction, crossing the calcar at roughly right angles. The appearance on plain films is reminiscent of the punctate calcification that may be seen within a bone infarct or a cartilaginous tumor such as an enchondroma. These trabeculae were also observed in two of ten cases of os- teoarthritis, suggesting they play a role in but- tressing of the calcar. The explanation most consis- tent with biomechanical principles is that these tra- beculae are normally present but hidden within the normal trabecular meshwork, and that with osteo- porosis they are “unmasked” as structurally and functionally less important trabeculae are resorbed. Alternatively, as primary and secondary compres- sive trabeculae are resorbed, and calcar may be asked to bear a larger portion of the compressive load, resulting in hypertrophy of these trabeculae. In osteoarthritis, hypertrophy of these trabeculae may be likened to buttressing of the medial cortex. When trabecular bone is elastically loaded in com- pression, the individual trabeculae bow out in a di- rection perpendicular to the applied stress (24). Strengthening may be accomplished by the forma- tion of sheets of bone perpendicular to the original trabeculae. It is postulated that these trabeculae function to resist compressive stress and may be “unmasked” or undergo hypertrophy.
A similar pattern of increased radiodensity in the calcar region was apparent on a frontal radiograph of a patient with metastatic prostate carcinoma. However, CT revealed significant variation from the usual pattern, demonstrating multiple rounded radiodensities and amputation of the lateral portion of the calcar. Metastatic disease was later proven in this region.
Plain films of ten cases of osteoarthritis revealed osteophytosis, increased prominence of the pri- mary compressive trabeculae, buttressing of the proximal medial cortex, and/or subchondral cyst formation. These changes were readily evident on CT and three-dimensional images that demon- strated reinforcement of the primary compressive trabeculae by formation of thicker and more closely-spaced trabeculae. The earliest change con- sisting of trabecular thickening was seen at the su- perior aspect of the primary compressive group, perhaps reflecting the effect of concentration of force at the contact area. Normally, the articular cartilage of the acetabulum and femoral head are incongruous with a small contact area at rest, but due to deformation of subchondral bone at maximal loading, the joint surfaces become congruent and maximum surface contact is achieved, diminishing the force per unit area (25). In osteoarthritis, de- generation and denudation of cartilage lead to con- centration of force over a limited contact area with loading of the hip (1,11,28). This concentration of force leads to focal cartilage degeneration and eventual joint space narrowing at the weight- bearing portions of the joint. With increasing se- verity there is further accentuation of primary com- pressive trabeculae accompanied by buttressing of the proximal medial cortex. In cases of moderate severity, we observed apparent reinforcement of the calcar by either appositional thickening of the calcar and adjacent parallel trabeculae or the for- mation or hypertrophy of trabeculae running per- pendicular to the calcar.
Although recent data indicate the utility of mag- netic resonance imaging in early diagnosis of ische- mic necrosis (23,32) CT is more widely available at this time and is also able to detect early changes of osteonecrosis when plain films reveal minimal or no abnormalities. Early detection of ischemic ne- crosis is important as prompt institution of therapy may prevent disease progression. Such detection depends on subtle alteration of the normal pattern of central trabeculae in the femoral head. On axial slices, the central trabeculae, most of which are primary compressive trabeculae, form a centrifugal radiating pattern that has been designated the as- terisk sign (5). In ischemic necrosis, the asterisk undergoes alterations consisting of central fusion, formation of broad sclerotic bands extending to the periphery, and peripheral clumping or fusion of sclerotic foci. With progression of reparative healing, more extensive sclerosis of the femoral
J Ovthop Rrs , Vol. 4 , N o . I , 1986

R. KERR E T A L .
head occurs. The pathomechanics of these alter- ations include microfracture of dead bone with callus formation and appositional deposition of bone in zones of ischemia and revascularization.
Various treatment alternatives are available for ischemic necrosis of the femoral head and selection of appropriate therapy is dependent upon the stage and extent of disease. For example, subtle flat- tening of the articular surface or the presence of subchondral gas (crescent sign) indicate mechanical deformation, and procedures designed to promote revascularization would be inadequate. CT, in- cluding reformatted imaging, is superior to routine radiography for detection of subtle abnormalities and determination of disease extent and thus may be an integral part of treatment planning.
Acknowledgment: We wish to thank Debra Trudell for preparat ion of the histologic specimens and Barbara Chapman and Geri Hubble for preparing this manuscript. Supported in pa r t b y Veterans Administration Grant #8615.
REFERENCES
I .
2.
3.
4.
5 .
6.
7.
8.
9.
10.
11.
Bullough P, Goodfellow J , O’Connor J: The relationship be- tween degenerative changes and load-bearing in the human hip. J Bone Joint Surg [Br] 55:746-758, 1973 Currey JD: The adaptation of bones to stress. J Theoret Biol
Dalen N , Hellstrom LG, Jacobson B: Bone mineral content and mechanical strength of the femoral neck. Acta Orthop Scand 4733-508, 1976 Dequeker J , Gautama K, Roh YS: Femoral trabecular pat- terns in asymptomatic spinal osteoporosis and femoral neck fracture. Clin Radio/ 25:243-246, 1974 Dihlmann W: CT analysis of the upper end of the femur: the asterisk sign and ischemic bone necrosis of the femoral head. Skeletal Radio/ 8:251-258, 1982 Dobbins JT, Mazess RB, Cameron JR: Scanning slit x-ray video-absorptiometry for measurement of bone mineral content. Med Phys 8563-569, 1981 Fazzalari NL, Darracott J , Vernon-Roberts B: A quantita- tive description of selected stress regions of cancellous bone in the head of the femur using automatic image analysis. Metab Bone Dis Re/ Re5 5:119-125, 1983 Frost HM: A determinant of bone architecture: the min- imum effective strain. CIin Orthop 175:286-292, 1983 Galante J , Rostoker W. Ray RD: Physical properties of tra- becular bone. Calcij‘ Tissue Res 5:236-243, 1970 Griffin JB: The calcar femorale redefined. CIin Orrhop
Harrison MHM, Schajowicz F, Trueta J: Osteoarthritis of the hip: a study of the nature and evolution of the disease. J Bone Joint Surg [BY] 3.5598-626, 1953
20:91-106, 1968
164:211-214, 1982
12.
13.
14.
15.
16.
17.
18.
19.
20.
21.
22.
23.
24.
25.
26.
27.
28
29.
30.
31.
32.
33.
34.
35.
Harty M: The calcar femorale and the femoral neck. JBone Joint Surg [Am] 39:625-630, 1957 Horsman A, Nordin C, Simpson M, Speed R: Cortical and trabecular bone status in elderly women with femoral neck fracture. Clin Orthop 166:143-151, 1982 Jaworski ZFG: Physiology and pathology of bone remod- eling. Orthop Clin North Am 12:485-512, 1981 Jensen PS, Lang R, Baron R, Orphanoudakis SC: Changes in cortical bone in metabolic bone disease. Radiological So- ciety of North America, Washington, D.C., 1984 Kazarian L, Graves GA: Compressive strength character- istics of the human vertebral centrum. Spine 2: I - 14, 1977 Khairi MRA, Cronin JH, Robb JA, Smith DM, Yu PL, Johnston CC: Femoral trabecular pattern index and bone mineral content measurement by photon absorption in senile osteoporosis. J Bone Joint Surg [Am] 58:221-226, 1976 Kock JC: The laws of bone architecture. Am J Anat 21: 177- 298, 1917 Kranendonk DH, Jurist JM, Lee HG: Femoral trabecular patterns and bone mineral content. J Bone Joint Surg [Am]
Kushner A: Evaluation of Wolff’s law on bone formation. J Bone Joint Slug 22:589-596, 1940 Leichter I, Margulies JY, Weinreb A, et al: The relationship between bone density, mineral content, and mechanical strength in the femoral neck. CIin Orthop 163:272-281, 1982 Martin RB: The effects of geometric feedback in the devel- opment of osteoporosis. J Biomechanics 5:447-455, 1972 Moon KL, Genant HK, Helms CA, Chafetz N I , Crooks LE, Kaufman L: Musculoskeletal applications of nuclear mag- netic resonance. Rudiology 147:161-171, 1983 Pugh JW, Rose RM, Radin EL: Elastic and viscoelastic properties of trabecular bone: dependence on structure. J Biomechanics 6:475-485, 1973 Radin EL: Biomechanics of the human hip. CIin Orthop
Riggs BL, Wahner HW, Dunn WL, Mazess RB, Offord KP, Melton LJ, 111: Differential changes in bone mineral density of the appendicular and axial skeleton with aging. J CIin In- vest 67:328-335, 1981 Rosenthal DI, Scott JA: Biomechanics important to inter- pret radiographs of the hip. Skeletal Rudio/9:185- 188, 1983 Rydell N: Biomechanics of the hip joint. CIin Orrlzop
Singh M, Nagrath AR, Maini PS: Changes in trabecular pat- tern of the upper end of the femur as an index of osteo- porosis. J Bone Joint Surg [Am] 52:457-467, 1970 Singh M, Riggs BL, Beabout JW, et al: Femoral trabecular pattern index for evaluation of spinal osteoporosis. Ann In- tern M e d 77:63-67, 1972 Tobin WJ: The internal architecture of the femur and its clinical significance. J Bone Joint Surg [Am] 37:57-71, 1955 Totty WG, Murphy WA, Ganz W1, Kumar B, Daum WJ, Siege1 BA: Magnetic resonance imaging of the normal and ischemic femoral head. AJR 143: 1273-1280, 1984 Ward FO: Outlines of Human Osteology. London: Henry Renshaw, 1838 Wicks M, Garrett R, Vernon-Roberts B, Fazzalari N: Ab- sence of metabolic bone disease in the proximal femur in patients with fracture of the femoral neck. J Bone Joint Surg [Br] 64:319-322, 1982 Wolff J: Das Gesetz der Transformation der Knochen. Berlin: Hirschwald, 1892
54~1472-1478, 1972
152:28-34, 1980
92:6-15, 1973
J Orthop Rrs, Vof. 4 , N o . 1 , 1986




















