
Insulin-loaded PLGA/cyclodextrin large porous particles with improved aerosolization properties: In...
11
This article appeared in a journal published by Elsevier. The attached copy is furnished to the author for internal non-commercial research and education use, including for instruction at the authors institution and sharing with colleagues. Other uses, including reproduction and distribution, or selling or licensing copies, or posting to personal, institutional or third party websites are prohibited. In most cases authors are permitted to post their version of the article (e.g. in Word or Tex form) to their personal website or institutional repository. Authors requiring further information regarding Elsevier’s archiving and manuscript policies are encouraged to visit: http://www.elsevier.com/copyright
-
Upload
independent -
Category
Documents
-
view
0 -
download
0
Transcript of Insulin-loaded PLGA/cyclodextrin large porous particles with improved aerosolization properties: In...
This article appeared in a journal published by Elsevier. The attachedcopy is furnished to the author for internal non-commercial researchand education use, including for instruction at the authors institution
and sharing with colleagues.
Other uses, including reproduction and distribution, or selling orlicensing copies, or posting to personal, institutional or third party
websites are prohibited.
In most cases authors are permitted to post their version of thearticle (e.g. in Word or Tex form) to their personal website orinstitutional repository. Authors requiring further information
regarding Elsevier’s archiving and manuscript policies areencouraged to visit:
http://www.elsevier.com/copyright

Author's personal copy
Insulin-loaded PLGA/cyclodextrin large porous particles with improvedaerosolization properties: In vivo deposition and hypoglycaemic activityafter delivery to rat lungs
Francesca Ungaro a, Roberta d'Emmanuele di Villa Bianca b, Concetta Giovino a, Agnese Miro a,Raffaella Sorrentino b, Fabiana Quaglia a,⁎, Maria Immacolata La Rotonda a
a Department of Pharmaceutical and Toxicological Chemistry, University of Naples Federico II, Via D. Montesano 49, 80131 Naples, Italyb Department of Experimental Pharmacology, University of Naples Federico II, Via D. Montesano 49, 80131 Naples, Italy
a b s t r a c ta r t i c l e i n f o
Article history:Received 1 August 2008Accepted 6 December 2008Available online 25 December 2008
Keywords:Large porous particlesPulmonary deliveryInsulinPLGACyclodextrin
The aim of the present work is to develop large porous particles (LPP) of poly (lactide-co-glycolide) (PLGA)containing insulin with optimal aerodynamic properties and to test their in vivo potential, in pulmonarydelivery. Insulin-loaded LPP were fabricated by a double emulsion method by aid of hydroxypropyl-β-cyclodextrin (HPβCD). Conceiving this system for the controlled release of insulin to the lungs, the aerosolizationproperties and the release features in simulated lung fluids of PLGA/HPβCD/insulin LPP were investigated indepth. The technological results show that the combination of appropriate amounts of insulin and HPβCD plays acrucial role to achieve PLGA/HPβCD/insulin LPPwith the desired bulk and aerodynamic properties, that is a highlyporous structure, a very low density (0.1 g/ml), an experimental mass mean aerodynamic diameter (MMADexp)ranging from4.01 to 7.00 and a fine particle fraction (FPF) estimated to be 26.9–89.6% at the different airflow ratestested (i.e. 30–90 l/min). Confocal microscopy studies, performed after administration of labeled PLGA/HPβCD/insulin LPP to the rat lung by means of a low-scale dry powder inhaler (DPI), suggest that particles reach alveoliand remain in situ after delivery. The pharmacological effect of PLGA/HPβCD/insulin LPP was confirmed by dose–response studies performed on both normoglycaemic and streptozotocin-induced diabetic rats. While insulinsolutions administered via pulmonary route are unable to cause a significant hypoglycaemic effect, insulin de-livered through PLGA/HPβCD/insulin LPP at the same doses (0.5–4.0 IU/kg) significantly reduces blood glucoselevel as a function of the administered dose in both animal models. The developed LPP, tested in hyperglycaemicrats at evident pathological conditions, exerts a very significant and longer hypoglycaemic effect even at insulindoses as low as 0.5 IU/kg (about 0.5 mg of PLGA/HPβCD/insulin LPP per rat) as compared to a insulin solution.Taken together, our results support the viability of a dry powder formulation based on biodegradable LPP for thecontrolled release of insulin to the lungs. In vivo data show that PLGA/HPβCD/insulin LPP are able to reach alveoli,release insulin, which is absorbed in its bioactive form.
© 2009 Elsevier B.V. All rights reserved.
1. Introduction
Recent advances in inhalation therapy have aroused considerableresearch interest in the development of novel formulations intendedfor protein pulmonary delivery, mainly driven by the medical need forinhaled insulin [1–4]. Advanced dry powder inhalers (DPIs), some-what overcoming solubility, bioavailability and stability issues relatedto protein delivery by means of classical metered-dose inhalers (MDIs),have further increased research attention on this matter [5–7]. Never-theless, efficient pulmonary delivery through the newest DPIs requiresdrug powders with well-defined bulk properties (e.g. particle size,density, and surface area), which affect particle flow, handling and
dispersibility and, therefore, its likelihood of depositing in the desiredregion of the lung [8,9].
To date, the only insulin-based dry powder approved by FDAfor the treatment of diabetic patients via pulmonary route has beenExubera®, a short or rapid acting insulin, able to reach peak concen-tration levels faster than some insulins administered by subcutaneousinjection [10–12]. The main limitation of the formulation is the factthat it is not self-consistent, that is both type 1 and type 2 diabeticpatients will still need an injection of long-acting insulin to maintaina basal level for a 24 hour period. Furthermore, to improve powderefficacy in term of capability to deposit in deep lung regions, the use ofan uncomfortable DPI is necessary. Exubera® is no more marketed byPfizer, which has recently spread the news of an increased incidence oflung cancer cases among former smokers [13]. Novel controlledrelease technologies can be of great help in developing new proteinformulations able to combine the ability of the powder to reach deep
Journal of Controlled Release 135 (2009) 25–34
⁎ Corresponding author. Tel./fax: +39 81678707.E-mail address: [email protected] (F. Quaglia).
0168-3659/$ – see front matter © 2009 Elsevier B.V. All rights reserved.doi:10.1016/j.jconrel.2008.12.011
Contents lists available at ScienceDirect
Journal of Controlled Release
j ourna l homepage: www.e lsev ie r.com/ locate / jconre l

Author's personal copy
lung (i.e. alveoli) with a long-term therapeutic activity [14,15]. Inparticular, carrier-based systems may not only increase the amount ofprotein reaching the site of action and prolong its residence time insitu, but also improve the in vivo stability of the macromolecule, allowco-localized deposition of other protein therapeutics or helperexcipients (e.g. absorption enhancers) as well as decrease formulationtoxicity caused by protein immunogenicity or its high initial doses[16].
Among carriers for the prolonged release of proteins, biodegrad-able poly(lactide-co-glycolide) (PLGA)-based particles hold greatpromise for protein delivery to the lungs due to the fact that theycan be differently engineered into aerosols meeting several importantcriteria, that are: i) a low mass mean aerodynamic diameter (MMAD)to direct the particle to the lung periphery; ii) a small surface contactarea for good dispersion and flow properties; iii) a minimal hygro-scopic nature [17]. Indeed, major improvements in aerosol perfor-mance of PLGA particles may be achieved by lowering particle massdensity (b0.4 g/ml) and increasing particle geometric size (10–20 µm).Large porous particles (LPP), by virtue of their porosity, display anaerodynamic diameter much lower than geometric one, facilitatingtheir deep lung deposition [18]. Furthermore, due to their large size,PLGA-based LPP have been demonstrated to escape macrophage up-take and permit an efficient delivery of inhaled insulin into the sys-temic circulation for long time periods [19].
In our recent work, hydroxypropyl-β-cyclodextrin (HPβCD) wasused to produce PLGA-based LPP intended for pulmonary delivery ofinsulin, so as to develop a carrier system for safe and efficient deliveryof the protein to the respiratory tract [19]. PLGA-based LPP are com-monly obtained by the double emulsion–solvent evaporation techni-que establishing a difference in the osmotic pressure between theinternal and the external aqueous phases of the emulsion [21]. Never-theless, in the case of insulin, the use of salts (e.g. calcium and sodiumchloride) in the internal water phase can be dangerous due to the factthat salts can cause protein precipitation/aggregation/inactivationas a function of salt type and concentration used [22–24]. The useof HPβCD as an alternative osmotic agent has been demonstrated avaluable mean to produce insulin-loaded LPP, without altering proteinintegrity [20].
The aim of the present work is to investigate the in vivo potentialof PLGA/HPβCD LPP for pulmonary delivery of insulin. To this end,in vitro aerosolization properties and release features in simulatedlung fluids of the developed LPP have been characterized in depth.Afterward, PLGA/HPβCD/insulin LPP have been administered to ratsby means of a low-scale DPI to assess their in vivo deposition patternand hypoglycaemic activity.
2. Materials and methods
2.1. Materials
Poly(D,L-lactide-co-glycolide) (50:50) (PLGA) (Resomer RG 504 H;Mw 41.9 kDa; inherent viscosity 0.5 dl/g) was purchased fromBoehringer Ingelheim (Germany). Insulin and Insulin-fluoresceineisothiocyanate (FITC-Insulin) from bovine pancreas, Hydroxypropyl-β-cyclodextrin (Mw 1380 Da, molar substitution 0.6) (HPβCD), poly-sorbate 80, polyvinylalcohol (PVA, Mowiol® 40–88), Trizma® base, tri-fluoroacetic acid (TFA), sodium azide, sulforhodamine 101 (free acid),sodium cacodylate buffer, formaldehyde, glutaraldehyde, and strep-tozotocin were obtained from Sigma-Aldrich (USA). Sodium pento-barbital was supplied by Carlo Sessa s.p.a (Italy). Analytical grademagnesium chloride hexahydrate, sodium chloride, potassium chlo-ride, sodium phosphate dibasic anhydrous, sodium sulphate anhy-drous, calcium chloride dehydrate, sodium acetate trihydrate, sodiumbicarbonate, sodium carbonate, sodium citrate, methylene chlorideand glacial acetic acid, HPLC grade acetonitrile and methanol weresupplied by Carlo Erba (Italy).
2.2. Animals
Male Wistar rats (Charles River, Italy) were used for ex vivoconfocal microscopy studies and for in vivo hypoglycaemic activity.Animals were housed in an environment with controlled temperature(21–24 °C) and lighting (12:12 h light–darkness cycle). Standard chowand drinking water were provided ad libitum. A period of 7 dayswas allowed for acclimatisation of rats before any experimental mani-pulation was undertaken. Animals use was in accordance with theguidelines of Italian (N. 116/1992) and European Council law (N.86/609/CEE) for animal care. The experimental procedures were ap-proved by the Animal Ethics Committee of the University of Naples“Federico II” (Italy).
2.3. Preparation of PLGA/HPβCD/insulin LPP
PLGA/HPβCD/insulin LPP were prepared by the double emulsion–solvent evaporation technique as previously reported [20]. Briefly,12.5 mg of bovine insulin (corresponding to 315 IU) and 12.5 mg ofHPβCD (corresponding to an initial insulin/HPβCD mole ratio of 1:4)were dissolved in 0.25 ml of 30% (v/v) aqueous acetic acid and pouredinto 2.5 ml of a PLGA solution in methylene chloride (20% w/v).The primary emulsion was generated by a high-speed homogenizer(Diax 900 equipped with a tool 6G, Heidolph, Germany) operatingat 15000 rpm for 2 min. Afterwards, the emulsion was added to 25 mlof 0.5% (w/v) aqueous PVA solution and homogenized at 8000 rpm(tool 10F) for 1 min to produce the multiple emulsion. Solvent eva-poration and subsequent particle hardening was achieved under mag-netic stirring (MR 3001K, Heidolph, Germany) at room temperature.After 3 h, particles were collected, washed three times with distilledwater by centrifugation (5000 rpm, 4 °C, 15 min) (Hettich Zentrifugen,Universal 16R) and freeze-dried for 24 h (0.01 atm, −60 °C) (Modulyo,Edwards, UK).
Microparticles containing only HPβCD at 2.3% loading (2.3 mgof HPβCD per 100 mg of microspheres) were produced for compar-ison. Labelled PLGA/HPβCD/insulin LPP loaded with FITC-insulin(50% w/w of the total insulin content) were produced for ConfocalLaser Scanning Microscopy (CLSM) studies.
2.4. PLGA/HPβCD/insulin LPP characterization
Particle shape andmorphologywere analysedby Scanning ElectronMicroscopy (SEM) (Leica S440, Germany). The samples were stuck ona metal stub and coated with gold under vacuum. For the analysisof internal morphology, the powders were previously dispersed inTissue-Tek® embedding medium, fixed in Cryomold® devices (SakuraFinetek, USA) and cryosectioned (Accu-Cut® SRM™ 200 RotaryMicrotome, Sakura Finetek, USA) at −24 °C (section thickness: 10 µm).
The mean geometric diameter and size distribution of the particleswere determined by laser light scattering (Coulter LS 100Q, USA) on adispersion of freeze-dried microspheres in 0.2% w/v aqueous PVA.Particle size is expressed as volume mean diameter±SD of valuescollected from three different batches.
Insulin amount actually encapsulated within PLGA/HPβCD/insulinLPP was determined by a solvent extraction method [25]. Briefly, 5 mgof microspheres were dissolved into 0.8 ml of an acetonitrile/watersolution (9:1 v/v) and the protein was extracted into 2 ml of 0.05 Nhydrochloric acid. The suspension was centrifuged (5000 rpm, roomtemperature, 15 min) and the supernatant analysed for insulin con-tent. Insulin analysis was carried out by High-Performance LiquidChromatography (HPLC) as previously reported [25,26]. The HPLCsystem consisted of a LC-10ADvp liquid chromatograph, a SIL-10ADvpautoinjector, a SPD-10Avp UV–Vis detector and a C-R6 integratorfrom Shimadzu (Japan). The quantitative analysis was performedby reverse-phase chromatography (RP-HPLC) on a Jupiter 5-µm C18column (250×4.6 mm, 300 Å) (Phenomenex, USA). The mobile phase
26 F. Ungaro et al. / Journal of Controlled Release 135 (2009) 25–34

Author's personal copy
was a mixture of water and acetonitrile (7:3 v/v) containing 0.1% v/vof TFA. The flow rate was 1 ml/min and the detection wavelength220 nm. The quality of insulin was further assessed by size-exclusionchromatography (SE-HPLC) performed on a Biosep SEC-S 2000 column(300×7.8 mm) (Phenomenex, USA). The mobile phase was a mixtureof acetonitrile and 2.5 M acetic acid containing 4 mM L-arginine(4:96 v/v). The flow rate was 1 ml/min and the detection performed at280 nm to avoid arginine interference.
Powder density was estimated by tapped density measurementsaccording to Ph.Eur. VI Ed. A known weight of particles (100 mg) wastransferred to a 10 (±0.05) ml graduated cylinder and the initial vol-ume recorded. The cylinder was thenmechanically tapped 1250 timesup to volume plateau, by means of a tapped density tester (Mod. IG/4,Giuliani, Italy). Tapped density (ρ) of PLGA/HPβCD/insulin LPP was ex-pressed as the ratio between sample weight (g) and the volume oc-cupied after 1250 tappings (ml).
To achieve information about PLGA/HPβCD/insulin LPP flowproperties, the compressibility index or Carr's Index was estimatedthrough the relative percent difference between bulk and tapped den-sity as stated by US Pharmacopeia 26:
Carr0s Index = 1−ρi=ρð ÞT100 ð1Þ
where ρ and ρi are tapped and bulk density of the powder, respec-tively. On the basis of Carr's Index value, powder flowability is definedas: 5–12%, excellent; 12–18%, good; 18–21%, fair; 21–25%, poor, fluid;25–32%, poor, cohesive; 32–38%, very poor; N40%, extremely poor.
The theoretical mass mean aerodynamic diameter (MMADt) ofthe particles was also estimated on the basis of the definition:
MMADt = d ρ=ρ0Xð Þ1=2 ð2Þ
where d is the geometric mean diameter, ρ0 is a reference densityof 1 g/ml and X is the dynamic shape factor, which is 1 for a sphere. Inthe case of porous particles of approximately spherical shape:
ρ≈ρs 1−ɛð Þ ð3Þ
where ρs is the skeletal mass density of the particle as measured bypycnometry, ε is the particle porosity. An approximate bulk measureof ρ as defined by Eq. (3) is provided by tapped density [27].
2.5. PLGA/HPβCD/insulin LPP aerosolization properties
The aerosolization properties of PLGA/HPβCD/insulin LPP weretested in vitro after delivery from Turbospin® (PH&T Pharma, Milano,Italy), a breath-activated, reusable DPI working with single unit cap-sule containing the dry powder. For each test, a hard gelatine capsule(size 2, Capsugel, USA) was filled with about 30 mg of the powder andplaced in the Turbospin®.
The pulmonary deposition of PLGA/HPβCD/insulin LPP was inves-tigated in vitro using a Astra Type Multi-Stage Liquid Impinger (MSLI),Type ALI 1000 (Erweka, Italy). Twenty millilitres of a polysorbate 20aqueous solution (0.5% w/v) were poured into each of the four stagesof the impinger to wet the collection surfaces. The capsule was thenpierced and the liberated powder drawn through the impactor operatedat 30, 60 or 90 l/min for 8, 4 or 2.7 s, respectively. This allowed theaspiration of 4 L of air through the apparatus as recommended byPh.Eur. VI Ed. The powder deposited on the four MSLI stages wasrecovered by agitating the apparatus, removing the initial solution andrinsing with additional fractions of the polysorbate 20 aqueous solu-tion. The powder deposited in the induction port and on the finalcollection site (i.e. filter) was also recovered by washing with a poly-sorbate 20 aqueous solution (0.5%w/v). In each case, the suspension ofPLGA/HPβCD/insulin LPP achieved was centrifuged (5000 rpm, roomtemperature, 15 min), washed twicewith water to remove any residualpolysorbate 20, and the solid residue lyophilized. Each deposition
experiment was performed in triplicate. Insulin content of the re-covered powder samples and, consequently, the amount of LPP de-posited in each MSLI stage, was determined by solvent extractionmethod as described for loading efficiency in the paragraph 2.4. Afterdissolution of the particles in an acetonitrile/water solution (9:1 v/v),the protein was extracted into 0.05 N hydrochloric acid. Controlexperiments were run to verify the ability of the method in de-termining all the powder collected from the stage. A known amount ofPLGA/HPβCD/insulin LPP (5, 10 and 30 mg) was suspended in 20 ml ofa polysorbate 20 aqueous solution (0.5% w/v), transferred into thestage 1 of MSLI and recovered as described above. The amount ofrecovered LPP was quantified after extraction of insulin into 0.05 Nhydrochloric acid. The experiment was run in triplicate and therecovery was found to be 67.6±9.99%.
The emitted dose (ED) was calculated by accurately weighing thecapsule before and after Turbospin® actuation. Results are expressedas percentage of powder actually delivered±SD of values collectedfrom three different batches.
The fine particle fraction (FPF), the experimental mass medianaerodynamic diameter (MMADexp) and the geometric standard devia-tion (GSD) were calculated according to Ph.Eur. VI Ed. deriving a plotof cumulative mass of powder detained in each stage (expressed aspercent of total mass recovered in the impactor) versus cut-off dia-meter of the respective stage. The cut-off diameter of each individualstage (D) was determined as
D =D60 60=Qð Þ1=2 ð4Þ
where D60 is the cut-off diameter at a flow-rate of 60 l/min (i.e., 13.0,6.8, 3.1 and 1.7 µm for stages 1 to 4, respectively) and Q is the flowrate employed in the test. The FPF was calculated by interpolationfrom the plot as the percentage of powder emitted from the inhalerwith an aerodynamic diameter less than 5 µm. The MMADexp of theparticles was determined from the same graph as the particle size atwhich the line crosses the 50% mark and the GSD was defined as
GSD = SizeX=SizeYð Þ1=2 ð5Þ
where size X is the particle size for which the line crosses the 84%mark and size Y the 16% mark.
2.6. In vitro release studies
Release studies of insulin from PLGA/HPβCD/insulin LPP wereperformed at 37 °C either in TRIS buffer or in simulated lung fluids by aclassical sampling–separation method. TRIS buffer (0.05 M Trizma®
base) contained 0.05% w/v sodium azide as preserving agent and0.02% v/v polysorbate 80 as dispersing agent. Prior to use, pH wasadjusted with 0.01 M HCl to 7.4. Simulated Interstitial Lung Fluid(SILF), used to study the effect of alveolar subphase fluid (AVSF) com-position on insulin release rate, was prepared carefully followingthe preparation instructions dictated by Moss [28]. The concentrationof each component is shown in Table 1. To investigate how the alveolarsurfactant system may affect insulin release profile, results achievedin SILF were compared with those observed in Simulated SurfactantLung Fluid (SSLF). For SSLF, an amount of DPPC (0.02% w/v), was pre-pared as phospholipid dispersions and added to SILF as recommendedby Cook et al. [29]. Briefly, 200 mg of DPPC were accurately weighedinto a 500 ml round bottom flask and dissolved in a 20 ml 50:50 chlo-roform:methanol mixture. The solvent was removed by rotary evapo-ration (Laborota model 4010, Heidolph, Germany). The dry lipid filmwas then rehydrated in the presence of 20 ml of SILF at 50 °C for about1 h. The warm phospholipid dispersion was extruded through poly-carbonate membranes (Nuclepore® Polycarbonate, Whatman®, USA)with sequentially smaller pore size (from 5 to 0.2 µm) at 50 °C undernitrogen. The hydrodynamic diameter and polydispersity index of
27F. Ungaro et al. / Journal of Controlled Release 135 (2009) 25–34

Author's personal copy
DPPC dispersions were evaluated by Photon Correlation Spectroscopyusing a N5 Submicron Particle Size Analyzer (Beckman–Coulter). Thephospholipid dispersion was diluted in Milli-Q® water and mea-surements were performed at 25 °C on 90° angle. Once prepared, SILFand SSLF were stored at 4 °C until required. Prior to use, pH wasadjusted to 7.2 with 0.01 M HCl.
Insulin release profiles were evaluated by suspending 3 mg ofdried microspheres in 2 ml of release medium in a thermostatic bathat 37 °C in static conditions. At scheduled time intervals, samples werecentrifuged (5000 rpm, 4 °C, 15 min), 500 µl of medium were with-drawn and analysed for insulin content by RP-HPLC and SE-HPLCas described in the paragraph 2.4. The release medium was replacedby the same amount of fresh buffer. Assuming that bovine insulin isstable at pH 7.4 and 37 °C for 1 day (data not shown), for longer timeintervals, the release medium was withdrawn and residual particlesanalysed for insulin content as described in the paragraph 2.4. for LPPloading efficiency. Experiments were run in triplicate for each timepoint of release kinetics.
The conformation of bovine insulin released from PLGA/HPβCD/insulin LPP in simulated lung fluids was assessed by circular dichro-ism (CD) as previously reported [25]. Briefly, after 6 h of release, therelease medium (i.e. SILF) was withdrawn, filtered through 0.45-µmcellulose filters (RC filters, Phenomenex, Italy) and analyzed by CD. Ascontrol, bovine insulin and bovine insulin/HPβCD (1:4 mole ratio)standard solutions at the same concentration in SILF or SSLF (insulin4.5×10−6 M) were analyzed. All CD spectra were recorded on a J-710Spectropolarimeter (JASCO, Tokyo, Japan) equipped with a J-710 forWindows software (JASCO, Tokyo, Japan). A 0.1-mm path cell for far-UV CD and a 1.0 cm path cell for near-UV CD were used. The instru-ment was calibrated by an aqueous solution of d-10-camphorsulfo-nic acid (0.6 mg/ml). Data are reported as mean residue ellipticity [θ].From CD spectra, the ratio between θ at 208 nm and θ at 223 nm wascalculated and considered an index of the insulin monomer to dimerratio in the adopted experimental conditions.
2.7. In vitro diffusion of insulin
Insulin diffusion from/to simulated lung fluids was followedin vitro by membrane dialysis from mucus simulant to SILF and fromSILF or SSLF to phosphate buffer at pH 7.4. The mucus simulant (MS)used for these studies was prepared in accordance to the methoddescribed by Shah et al. [30]. Briefly, an aqueous solution of poly-ethylene oxide (PEO; Mw 4,000,000) at 1.5% w/v was prepared addingPEO to water at 95 °C and stirring the dispersion overnight at roomtemperature. Phosphate buffer saline at pH 7.4 (PBS) (120 mM NaCl,2.7 mM KCl, 10 mM phosphate buffer salts) was used as externalmedium in case of SILF and SSLF.
An amount of microspheres (8 mg) was suspended in 0.3 ml ofdonor medium (MS, SILF or SSLF) and placed in a dialysis membranebag (MWCO: 50,000 Da, Spectra/Por®). The sample was dropped into6 ml of external medium and kept at 37 °C. At scheduled time inter-vals, 1 ml of external mediumwas withdrawn and analysed for insulin
content by RP-HPLC and SE-HPLC as described in the paragraph2.4. The medium was replaced by the same amount of fresh medium.For time intervals longer than 1 day, the external medium was with-drawn and residual particles analysed for insulin content as describedin the paragraph 2.4. for LPP loading efficiency. Experiments were runin triplicate for each time point of release kinetics.
2.8. In vivo PLGA/HPβCD/insulin LPP deposition
Confocal microscopy studies were performed as reported byBosquillon et al. [31]. Briefly, normoglycaemic male Wistar rats wereanesthetised by an intraperitoneal injection of pentobarbital (60 mg/kg) and about 3.5 mg of FITC-insulin labeled PLGA/HPβCD/insulin LPP(corresponding to an insulin dose of 4 IU/kg) were intratracheallydelivered using the low-scale DPI Model DP-4 from Penn-Century(USA). Thirty and ninety minutes after delivery, the rat abdominalcavity was incised and a catheter, connected to an infusion pump(Harvard pump type 22, Watson–Marlow), was inserted in the pos-terior vena cava. Both carotids arteries were severed and lungs werethen labeled by the infusion of two different buffer solutions. The firstinfusion (10 ml/min for 5 min) was performed by using a solutioncontaining 0.1% (w/v) sulforhodamine in PBS at pH 7.4 (138 nM NaCl,8.1 mM Na2HPO4, 1.1 mM KH2PO4, 2.7 mM KCl) and a second infusion(5 ml/min for 5 min) was carried out by using a cacodylate buffercontaining sulforhodamine (0.1% w/v), formaldhehyde (0.6% w/v) andglutaraldehyde (0.9% w/v), to fix the lungs. Afterward tissues wereremoved and lung lobes were roughly sectioned by a scalpel and thesections fixed in Cryomold® devices (Sakura Finetek, USA) and thencryosectioned (Accu-Cut® SRM™ 200 Rotary Microtome, SakuraFinetek, USA) (section thickness: 30 µm). Lung slices were analyzedby confocal laser scanning microscopy (CLSM). Control experimentswere run to asses the autofluorescence of the pulmonary tissue afterintra-tracheal delivery of unlabeled PLGA/HPβCD/insulin LPP.
2.9. Hypoglycaemic activity in normoglycaemic and instreptozotocin-induced diabetic rats
The hypoglycaemic activity of PLGA/HPβCD/insulin LPP after intra-tracheal delivery was assessed in normoglycaemic and in streptozo-tocin-induced diabetic rats. Rats (200–220 g) were randomly dividedin two groups, normoglycaemic and streptozotocin-induced diabeticrats. Streptozotocin (STZ, 60 mg/kg) or vehicle (50 mM sodium citratebuffer, pH 4.5) was administered intravenously, after animals' expo-sure to isofluorane (Abbott, Milan Italy); this experimental procedurecauses a diabetes type I condition [32]. After injection, the rats hadfree access to food andwater. Diabetes inductionwas established afterone week from STZ injection and the fasting blood glucose levels,collected from the tail vein, were determined by using the Accu-Chek®
monitoring kit (Roche Diagnostics, USA). After that, normoglycaemicand STZ-induced diabetic rats were anesthetised with pentobarbital(60 mg/kg, i.p.). Rats were then placed with the ventral side up on asurgical table provided with a temperature controlled pad tomaintainphysiological temperature. Different amounts of PLGA/HPβCD/insulinLPP (corresponding to insulin doses of 0.5, 1, 2 or 4 IU/kg) weredelivered to the anesthetised rats directly into the trachea through themouth using the DPI. As control, an intra-tracheal administration ofunloaded PLGA/HPβCD LPP, an amount equivalent to 4 IU/kg, wasperformed both in normoglycaemic and streptozotocin-induced rats.The actual insulin dose insufflated per rat was determined byweighing the device before/after powder filling and after insufflation.Similar experiments were performed by using insulin solutions insterile 10mMphosphate buffer at pH 7.4 (PBS). Briefly, a stock solutionof bovine insulin (0.3 mg/ml of native bovine insulin) was appro-priately diluted so as to achieve 100 µl solutions corresponding toinsulin doses of 0.5, 2 and 4 IU/kg. The prepared solutions were intra-tracheally spray instilled (MicroSprayer® model IA-1B, PennCentury,
Table 1Composition of simulated interstitial lung fluid (SILF)a
Chemical Concentration (g/L)
Magnesium chloride 0.203Sodium chloride 6.019Potassium chloride 0.298Sodium phosphate, dibasic 0.268Sodium sulphate 0.071Calcium chloride 0.368Sodium acetate 0.952Sodium bicarbonate 2.604Sodium citrate 0.097
a In SSLF DPPC was added in form of liposomes (mean size 150 nm; polydispersityindex 0.3).
28 F. Ungaro et al. / Journal of Controlled Release 135 (2009) 25–34

Author's personal copy
USA) in both normoglycaemic and streptozotocin-induced diabeticrats. In this case to avoid breathing problems, the rats were placed on aslanted board (30° from the vertical). Moreover to evaluate thepharmacological availability (PA) of PLGA/HPβCD/insulin LPP asubcutaneous administration of an insulin solution (4 IU/kg in PBS)was performed for comparison. At scheduled time intervals, bloodsamples were collected from the tail vein and glycaemia was assessedas described above. Generally, 3 h from intra-tracheal administration,rats were awake and had free access only to the water.
Blood glucose levels are expressed asmg/dl and reported asmean±SEM of n=3–5 single experiments for each treatment. Statisticalanalysis was performed using Graph Pad Prism (GraphPad Software,San Diego, CA) by two way analysis of variance (ANOVA) followed byBonferroni's post test. p values less than 0.05 were considered assignificant.
The area above the curve [AAC] was calculated by the lineartrapezoidal method and the relative PA (%) of PLGA/HPβCD/insulin LPPafter pulmonary administration was calculated from the followingequation [33–34]:
PA kð Þ = AAC½ �inhddoses:c:AAC½ �s:cddoseinh
� 100 ð6Þ
where [AAC]inh and [AAC]s.c. are the area above the curve relative toinhaled and subcutaneous insulin, respectively; doses.c. and doseinhare insulin doses (4 IU/kg) administered subcutaneously and byinhalation respectively.
3. Results
3.1. PLGA/HPβCD/insulin LPP preparation and characterization
Insulin-loaded LPP made of PLGA were prepared with good yieldsby a classical double emulsion technique using HPβCD as porosigen[20]. In the presence of HPβCD large particles characterized by a vol-ume mean diameter of 26.2±1.2 µm and a widespread external/inter-nal porosity were achieved (Fig. 1).
PLGA/HPβCD/insulin LPP overall properties are reported in Table 2.Insulin was entrapped within LPP in its native state with an efficiencyhigher than 50%. The results of the RP-HPLC analysis showed thatdesamido insulin content of microspheres was always lower than5%, that is a value commonly present as impurity in the commercialinsulin as stated by Ph.Eur. VI Ed. No covalent aggregate soluble inthe extraction mediumwas detected by SE-HPLC. As can be seen, highparticle porosity corresponded to a very low tapped density, whichwas found to be around 0.1 g/ml (Table 2). A Carr's Index as low as6.25% was calculated for PLGA/HPβCD/insulin LPP, suggesting excel-lent powder flowability. The preliminary estimation of particle MMADt,achieved by normalizing the geometric diameter with the powdertapped density according to Eq. (2), gave a value lower than 10 µm con-firming good flow properties for PLGA/HPβCD/insulin LPP (Table 2).
3.2. In vitro PLGA/HPβCD/insulin LPP aerosolization properties
The deposition pattern of PLGA/HPβCD/insulin LPP at differentairflowswas evaluated in aMSLI after delivery from a breath-activatedDPI. No residue particles were found in the inhaler and only a littlepercentage of the powder (about 20%) was recovered from the adaptor(i.e. throat) after DPI actuation. A significant amount of PLGA/HPβCD/insulin LPP, decreasing as the airflow rate increased,was detained fromthe stage 1 of MSLI. Thus, data analysis was performed considering ornot this fraction (m1) of LPP in the total mass collected.
The ED, FPF and MMADexp of PLGA/HPβCD/insulin LPP are listedin Table 3. The ED reached values between 94.5% and 103.0% andwas independent on the airflow rate (30–90 l/min). The FPF was 1.18%at 30 l/min, increased to 4.73% at 60 l/min and remained almost
constant at 90 l/min. The experimental MMADexp decreased whenincreasing theairflow from30 to60 l/minand thenplateaued at90 l/min(MMADexp=9.68 µm). Thegeometric standarddeviationvaried between1.21 and 1.28, independently on the airflow rate. Higher FPF (26.9, 61.3and 84.9% at 30, 60 and 90 l/min, respectively) and lower MMADexp
values (7.01, 5.02 and 4.01 µm at 30, 60 and 90 l/min, respectively) wereachieved when the amount of PLGA/HPβCD/insulin LPP on stage 1 wasneglected.
3.3. In vitro release of insulin from PLGA/HPβCD/insulin LPP in simulatedlung fluids
Release studies of insulin from PLGA/HPβCD/insulin LPP wereperformed by a sampling separation method at physiological pH andtemperature (pH 7.4 and 37 °C), or in simulated lung fluids.
Fig. 1. SEM micrographs of PLGA/HPβCD/insulin LPP: A) overall picture (×900 magnifi-cation); B) detail (×1600magnification); C) particle cross-section. Field is representativeof the formulation.
29F. Ungaro et al. / Journal of Controlled Release 135 (2009) 25–34
Author's personal copy
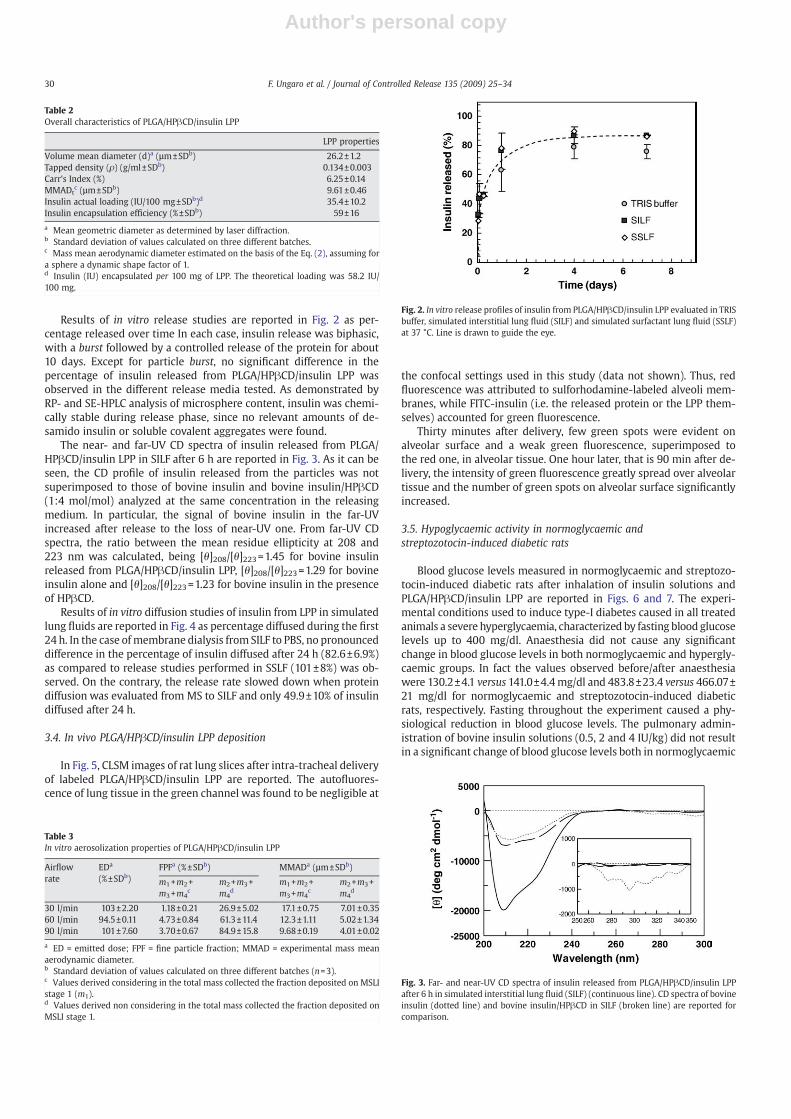
Results of in vitro release studies are reported in Fig. 2 as per-centage released over time In each case, insulin release was biphasic,with a burst followed by a controlled release of the protein for about10 days. Except for particle burst, no significant difference in thepercentage of insulin released from PLGA/HPβCD/insulin LPP wasobserved in the different release media tested. As demonstrated byRP- and SE-HPLC analysis of microsphere content, insulin was chemi-cally stable during release phase, since no relevant amounts of de-samido insulin or soluble covalent aggregates were found.
The near- and far-UV CD spectra of insulin released from PLGA/HPβCD/insulin LPP in SILF after 6 h are reported in Fig. 3. As it can beseen, the CD profile of insulin released from the particles was notsuperimposed to those of bovine insulin and bovine insulin/HPβCD(1:4 mol/mol) analyzed at the same concentration in the releasingmedium. In particular, the signal of bovine insulin in the far-UVincreased after release to the loss of near-UV one. From far-UV CDspectra, the ratio between the mean residue ellipticity at 208 and223 nm was calculated, being [θ]208/[θ]223=1.45 for bovine insulinreleased from PLGA/HPβCD/insulin LPP, [θ]208/[θ]223=1.29 for bovineinsulin alone and [θ]208/[θ]223=1.23 for bovine insulin in the presenceof HPβCD.
Results of in vitro diffusion studies of insulin from LPP in simulatedlung fluids are reported in Fig. 4 as percentage diffused during the first24 h. In the case ofmembrane dialysis from SILF to PBS, no pronounceddifference in the percentage of insulin diffused after 24 h (82.6±6.9%)as compared to release studies performed in SSLF (101±8%) was ob-served. On the contrary, the release rate slowed down when proteindiffusion was evaluated from MS to SILF and only 49.9±10% of insulindiffused after 24 h.
3.4. In vivo PLGA/HPβCD/insulin LPP deposition
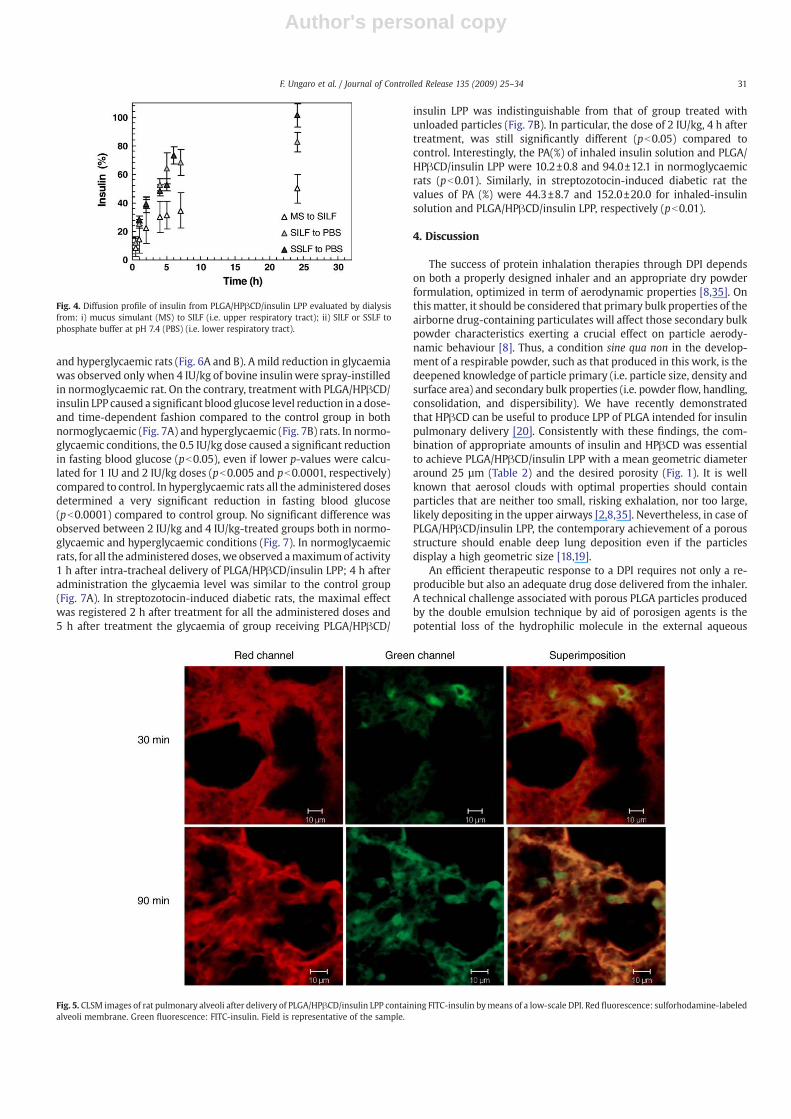
In Fig. 5, CLSM images of rat lung slices after intra-tracheal deliveryof labeled PLGA/HPβCD/insulin LPP are reported. The autofluores-cence of lung tissue in the green channel was found to be negligible at
the confocal settings used in this study (data not shown). Thus, redfluorescence was attributed to sulforhodamine-labeled alveoli mem-branes, while FITC-insulin (i.e. the released protein or the LPP them-selves) accounted for green fluorescence.
Thirty minutes after delivery, few green spots were evident onalveolar surface and a weak green fluorescence, superimposed tothe red one, in alveolar tissue. One hour later, that is 90 min after de-livery, the intensity of green fluorescence greatly spread over alveolartissue and the number of green spots on alveolar surface significantlyincreased.
3.5. Hypoglycaemic activity in normoglycaemic andstreptozotocin-induced diabetic rats
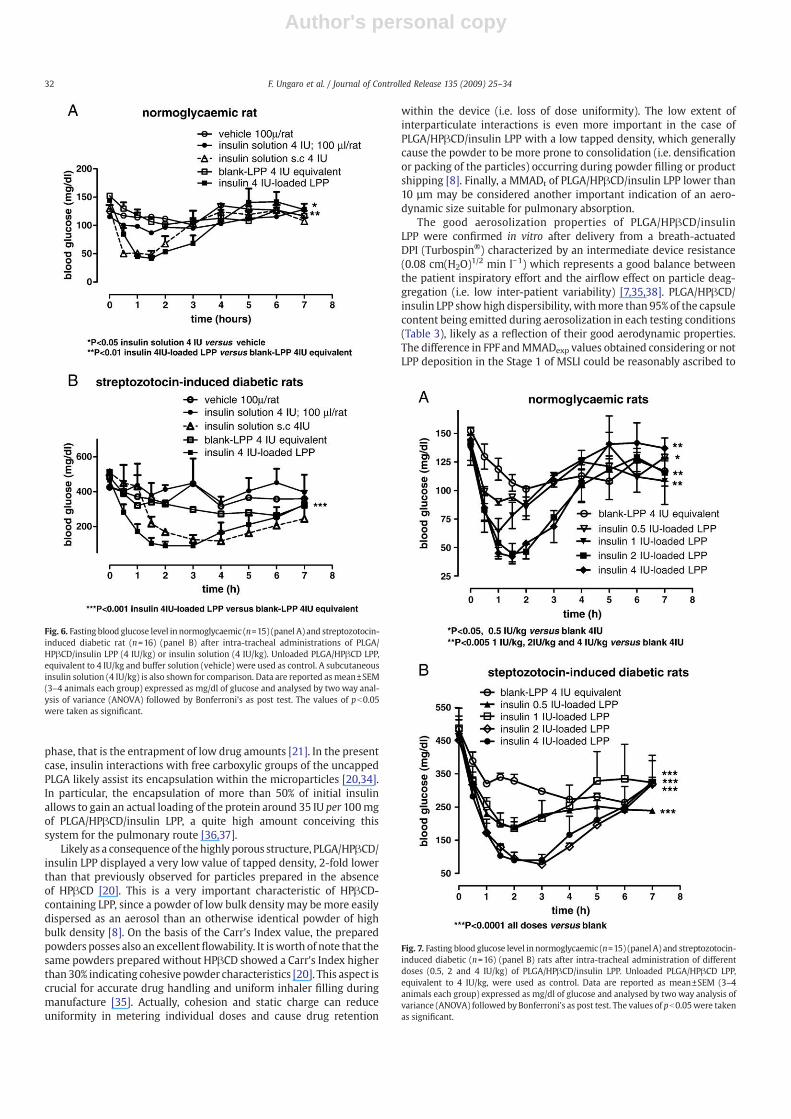
Blood glucose levels measured in normoglycaemic and streptozo-tocin-induced diabetic rats after inhalation of insulin solutions andPLGA/HPβCD/insulin LPP are reported in Figs. 6 and 7. The experi-mental conditions used to induce type-I diabetes caused in all treatedanimals a severe hyperglycaemia, characterized by fasting blood glucoselevels up to 400 mg/dl. Anaesthesia did not cause any significantchange in blood glucose levels in both normoglycaemic and hypergly-caemic groups. In fact the values observed before/after anaesthesiawere 130.2±4.1 versus 141.0±4.4mg/dl and 483.8±23.4 versus 466.07±21 mg/dl for normoglycaemic and streptozotocin-induced diabeticrats, respectively. Fasting throughout the experiment caused a phy-siological reduction in blood glucose levels. The pulmonary admin-istration of bovine insulin solutions (0.5, 2 and 4 IU/kg) did not resultin a significant change of blood glucose levels both in normoglycaemic
Table 2Overall characteristics of PLGA/HPβCD/insulin LPP
LPP properties
Volume mean diameter (d)a (µm±SDb) 26.2±1.2Tapped density (ρ) (g/ml±SDb) 0.134±0.003Carr's Index (%) 6.25±0.14MMADt
c (µm±SDb) 9.61±0.46Insulin actual loading (IU/100 mg±SDb)d 35.4±10.2Insulin encapsulation efficiency (%±SDb) 59±16
a Mean geometric diameter as determined by laser diffraction.b Standard deviation of values calculated on three different batches.c Mass mean aerodynamic diameter estimated on the basis of the Eq. (2), assuming fora sphere a dynamic shape factor of 1.d Insulin (IU) encapsulated per 100 mg of LPP. The theoretical loading was 58.2 IU/100 mg.
Table 3In vitro aerosolization properties of PLGA/HPβCD/insulin LPP
Airflowrate
EDa
(%±SDb)FPFa (%±SDb) MMADa (µm±SDb)
m1+m2+m3+m4
cm2+m3+m4
dm1+m2+m3+m4
cm2+m3+m4
d
30 l/min 103±2.20 1.18±0.21 26.9±5.02 17.1±0.75 7.01±0.3560 l/min 94.5±0.11 4.73±0.84 61.3±11.4 12.3±1.11 5.02±1.3490 l/min 101±7.60 3.70±0.67 84.9±15.8 9.68±0.19 4.01±0.02
a ED = emitted dose; FPF = fine particle fraction; MMAD = experimental mass meanaerodynamic diameter.b Standard deviation of values calculated on three different batches (n=3).c Values derived considering in the total mass collected the fraction deposited on MSLIstage 1 (m1).d Values derived non considering in the total mass collected the fraction deposited onMSLI stage 1.
Fig. 2. In vitro release profiles of insulin from PLGA/HPβCD/insulin LPP evaluated in TRISbuffer, simulated interstitial lung fluid (SILF) and simulated surfactant lung fluid (SSLF)at 37 °C. Line is drawn to guide the eye.
Fig. 3. Far- and near-UV CD spectra of insulin released from PLGA/HPβCD/insulin LPPafter 6 h in simulated interstitial lung fluid (SILF) (continuous line). CD spectra of bovineinsulin (dotted line) and bovine insulin/HPβCD in SILF (broken line) are reported forcomparison.
30 F. Ungaro et al. / Journal of Controlled Release 135 (2009) 25–34
Author's personal copy
and hyperglycaemic rats (Fig. 6A and B). Amild reduction in glycaemiawas observed only when 4 IU/kg of bovine insulinwere spray-instilledin normoglycaemic rat. On the contrary, treatment with PLGA/HPβCD/insulin LPP caused a significant blood glucose level reduction in a dose-and time-dependent fashion compared to the control group in bothnormoglycaemic (Fig. 7A) and hyperglycaemic (Fig. 7B) rats. In normo-glycaemic conditions, the 0.5 IU/kg dose caused a significant reductionin fasting blood glucose (pb0.05), even if lower p-values were calcu-lated for 1 IU and 2 IU/kg doses (pb0.005 and pb0.0001, respectively)compared to control. In hyperglycaemic rats all the administered dosesdetermined a very significant reduction in fasting blood glucose(pb0.0001) compared to control group. No significant difference wasobserved between 2 IU/kg and 4 IU/kg-treated groups both in normo-glycaemic and hyperglycaemic conditions (Fig. 7). In normoglycaemicrats, for all the administered doses,we observed amaximumof activity1 h after intra-tracheal delivery of PLGA/HPβCD/insulin LPP; 4 h afteradministration the glycaemia level was similar to the control group(Fig. 7A). In streptozotocin-induced diabetic rats, the maximal effectwas registered 2 h after treatment for all the administered doses and5 h after treatment the glycaemia of group receiving PLGA/HPβCD/
insulin LPP was indistinguishable from that of group treated withunloaded particles (Fig. 7B). In particular, the dose of 2 IU/kg, 4 h aftertreatment, was still significantly different (pb0.05) compared tocontrol. Interestingly, the PA(%) of inhaled insulin solution and PLGA/HPβCD/insulin LPP were 10.2±0.8 and 94.0±12.1 in normoglycaemicrats (pb0.01). Similarly, in streptozotocin-induced diabetic rat thevalues of PA (%) were 44.3±8.7 and 152.0±20.0 for inhaled-insulinsolution and PLGA/HPβCD/insulin LPP, respectively (pb0.01).
4. Discussion
The success of protein inhalation therapies through DPI dependson both a properly designed inhaler and an appropriate dry powderformulation, optimized in term of aerodynamic properties [8,35]. Onthismatter, it should be considered that primary bulk properties of theairborne drug-containing particulates will affect those secondary bulkpowder characteristics exerting a crucial effect on particle aerody-namic behaviour [8]. Thus, a condition sine qua non in the develop-ment of a respirable powder, such as that produced in this work, is thedeepened knowledge of particle primary (i.e. particle size, density andsurface area) and secondary bulk properties (i.e. powder flow, handling,consolidation, and dispersibility). We have recently demonstratedthat HPβCD can be useful to produce LPP of PLGA intended for insulinpulmonary delivery [20]. Consistently with these findings, the com-bination of appropriate amounts of insulin and HPβCD was essentialto achieve PLGA/HPβCD/insulin LPP with a mean geometric diameteraround 25 µm (Table 2) and the desired porosity (Fig. 1). It is wellknown that aerosol clouds with optimal properties should containparticles that are neither too small, risking exhalation, nor too large,likely depositing in the upper airways [2,8,35]. Nevertheless, in case ofPLGA/HPβCD/insulin LPP, the contemporary achievement of a porousstructure should enable deep lung deposition even if the particlesdisplay a high geometric size [18,19].
An efficient therapeutic response to a DPI requires not only a re-producible but also an adequate drug dose delivered from the inhaler.A technical challenge associated with porous PLGA particles producedby the double emulsion technique by aid of porosigen agents is thepotential loss of the hydrophilic molecule in the external aqueous
Fig. 4. Diffusion profile of insulin from PLGA/HPβCD/insulin LPP evaluated by dialysisfrom: i) mucus simulant (MS) to SILF (i.e. upper respiratory tract); ii) SILF or SSLF tophosphate buffer at pH 7.4 (PBS) (i.e. lower respiratory tract).
Fig. 5. CLSM images of rat pulmonary alveoli after delivery of PLGA/HPβCD/insulin LPP containing FITC-insulin bymeans of a low-scale DPI. Red fluorescence: sulforhodamine-labeledalveoli membrane. Green fluorescence: FITC-insulin. Field is representative of the sample.
31F. Ungaro et al. / Journal of Controlled Release 135 (2009) 25–34
Author's personal copy
phase, that is the entrapment of low drug amounts [21]. In the presentcase, insulin interactions with free carboxylic groups of the uncappedPLGA likely assist its encapsulation within the microparticles [20,34].In particular, the encapsulation of more than 50% of initial insulinallows to gain an actual loading of the protein around 35 IU per 100mgof PLGA/HPβCD/insulin LPP, a quite high amount conceiving thissystem for the pulmonary route [36,37].
Likely as a consequence of the highly porous structure, PLGA/HPβCD/insulin LPP displayed a very low value of tapped density, 2-fold lowerthan that previously observed for particles prepared in the absenceof HPβCD [20]. This is a very important characteristic of HPβCD-containing LPP, since a powder of low bulk density may bemore easilydispersed as an aerosol than an otherwise identical powder of highbulk density [8]. On the basis of the Carr's Index value, the preparedpowders posses also an excellentflowability. It isworth of note that thesame powders prepared without HPβCD showed a Carr's Index higherthan 30% indicating cohesive powder characteristics [20]. This aspect iscrucial for accurate drug handling and uniform inhaler filling duringmanufacture [35]. Actually, cohesion and static charge can reduceuniformity in metering individual doses and cause drug retention
within the device (i.e. loss of dose uniformity). The low extent ofinterparticulate interactions is even more important in the case ofPLGA/HPβCD/insulin LPP with a low tapped density, which generallycause the powder to be more prone to consolidation (i.e. densificationor packing of the particles) occurring during powder filling or productshipping [8]. Finally, a MMADt of PLGA/HPβCD/insulin LPP lower than10 µm may be considered another important indication of an aero-dynamic size suitable for pulmonary absorption.
The good aerosolization properties of PLGA/HPβCD/insulinLPP were confirmed in vitro after delivery from a breath-actuatedDPI (Turbospin®) characterized by an intermediate device resistance(0.08 cm(H2O)1/2 min l−1) which represents a good balance betweenthe patient inspiratory effort and the airflow effect on particle deag-gregation (i.e. low inter-patient variability) [7,35,38]. PLGA/HPβCD/insulin LPP showhigh dispersibility, withmore than 95% of the capsulecontent being emitted during aerosolization in each testing conditions(Table 3), likely as a reflection of their good aerodynamic properties.The difference in FPF andMMADexp values obtained considering or notLPP deposition in the Stage 1 of MSLI could be reasonably ascribed to
Fig. 7. Fasting blood glucose level in normoglycaemic (n=15) (panel A) and streptozotocin-induced diabetic (n=16) (panel B) rats after intra-tracheal administration of differentdoses (0.5, 2 and 4 IU/kg) of PLGA/HPβCD/insulin LPP. Unloaded PLGA/HPβCD LPP,equivalent to 4 IU/kg, were used as control. Data are reported as mean±SEM (3–4animals each group) expressed as mg/dl of glucose and analysed by two way analysis ofvariance (ANOVA) followed by Bonferroni's as post test. The values of pb0.05were takenas significant.
Fig. 6. Fasting blood glucose level in normoglycaemic (n=15) (panel A) and streptozotocin-induced diabetic rat (n=16) (panel B) after intra-tracheal administrations of PLGA/HPβCD/insulin LPP (4 IU/kg) or insulin solution (4 IU/kg). Unloaded PLGA/HPβCD LPP,equivalent to 4 IU/kg and buffer solution (vehicle) were used as control. A subcutaneousinsulin solution (4 IU/kg) is also shown for comparison. Data are reported asmean±SEM(3–4 animals each group) expressed as mg/dl of glucose and analysed by two way anal-ysis of variance (ANOVA) followed by Bonferroni's as post test. The values of pb0.05were taken as significant.
32 F. Ungaro et al. / Journal of Controlled Release 135 (2009) 25–34

Author's personal copy
LPPfloating inwater-containing stage 1 aswell as to the fact that throatregionwas not wetted during the experiment. AMMADexp higher than9.68 µm, calculatedwhen considering LPP present on stage 1, indicatesthat PLGA/HPβCD/insulin LPP would preferentially deposit in thecentral regions of the lung. Whether this in vitro deposition patternoccurs also in vivo, it will unavoidably affect the amount of dry powderdeposited in the oropharynx, where powder deposition is primarilydriven by inertial impaction. Even if this mechanism could be pro-moted in the case of large particles, at least two factors may preventPLGA/HPβCD/insulin LPP impaction in the oropharyngeal region thatis i) low powder bulk density which improves flow properties; ii) poorparticle wettabiliy, possibly limiting adhesion to mucosae. However,when the fraction of PLGA/HPβCD/insulin LPP deposited in stage 1wasneglected according to Ph.Eur. VI Ed., a MMADexp as low as 4.0 µmwascalculated at 90 l/min, a value more consistent with in vivo resultsachieved in this study. As a consequence, minimal deposition in theoropharyngeal region could be expected after inhalation in humanswhich, togetherwith the lack of deposition in the inhaler, could reducethe risk of lowbioavailability due todry powder swallowing. It isworthto note that, themain literature criticism toward in vitro aerosolizationtests, such as two-stage liquid impinger, MSLI and Andersen CascadeImpactor, is that none of them can effectively resemble the complex invivo respiratory apparatus (i.e. trachea, bronchi, bronchioles, alveoli).Thus, a definitive result can be obtained only by measuring pharma-cological effect in humans.
Conceiving PLGA/HPβCD/insulin LPP for lung delivery, insulinrelease studies were performed in experimental conditions able tosimulate the properties of the delivery site and, above all, the com-position of pulmonary biological fluids where the protein will bedelivered. On this matter, it should be considered that in the alveoli anaqueous biological fluid at pH 7 (alveolar subphase fluid or AVSF)covered by a surfactant film, consisting of 80% phospholipids (95% ofdipalmytoilphosphatidincoline or DPPC), 10% cholesterol and 10% ofsurfactant proteins (SP-A, SP-B, SP-C and SP-D) is present [39]. Toreproduce such a complex system in vitro, simulated alveolar fluids(SILF and SSLF) were used for insulin release studies as an alternativeto classical physiological buffer at pH 7.4. In all the release mediatested, the release profile of insulin occurred in two-steps, that is aburst followed by a slower release stage (Fig. 2). Insulin overall releaseprofile, and particularly burst, appeared highly affected by the particlemacroporous structure (Fig. 1C), further evolving with time due toprogressive polymer erosion [40,41]. Interestingly, no significant dif-ference in insulin release rate was observed in simulated alveolarfluids as compared to results achieved in buffer at pH 7.4, suggestingthat ion concentration and presence of DPPC in SSLF does not affectPLGA/HPβCD/insulin LPP release properties. Projecting these results inhumans, the fact that the developed LPP release insulin according to abiphasic kinetics can be regarded as a useful mean to mimic the phy-siological biphasic secretion of insulin, ensuring also a prolonged re-lease to maintain insulin basal serum level in the treatment of bothtype 1 and type 2 diabetes. The versatility of PLGA microspheres canalso allow to further prolong this sustained release phase by slightlymodifying formulation conditions [21].
The application of the dialysis technique to study insulin diffusionfrom SILF and SSLF to PBS pH 7.4 (Fig. 4) gave the possibility to betterfocus on the transport of insulin at alveolar level toward the blood-stream during the first 24 h. It should be noted that, differently fromrelease studies, insulin diffusion in PBS seems slightly accelerated inthe case of SSLF/PBS diffusion. Actually, an amount of insulin, otherthan released, remained adsorbed onto DPPC phospholipid disper-sions in the dialysis bag (data not shown) suggesting a role of lungsurfactant in controlling absorption rate. Whether the particles woulddeposit in the upper airways, the contribution of the mucus layer onprotein diffusion through lung epithelium should be considered. Thus,a mucus simulant (MS), able to mimic rheological properties of humanmucus [30], was used for diffusion studies and results compared with
those achieved with SILF/PBS or SSLF/PBS systems. Actually the de-creased diffusion rate observed for MS/SILF system highlights thatmucus rheological properties, and in particular its viscosity, may exertan effect on insulin release rate from the particles, slowing downinsulin diffusion as compared to results achieved from SILF or SSLF toPBS (Fig. 4).
The self-association state of insulin (i.e., monomer–dimer–hex-amer equilibrium) released from PLGA/HPβCD/insulin LPP in simu-lated lung fluids was also assessed since this is a key parameter thatcontrols in vivo bioavailability of the protein. Even if inhaled insulin isinitially absorbedmore rapidly than injected insulin, it results also in amore prolonged control over blood glucose level. This behaviour isconsistent with the presence in alveolar fluids of an insulin fractionable to be retained longer in situ. This effect may be attributed to theassociation form of insulin taking into account that monomeric insulinis absorbed more rapidly than hexameric form after subcutaneousinjection [1]. Our results confirm that insulin exists as an equilibriumof monomer–dimer–hexamer in fluids simulating in vivo environment(SILF) (Fig. 3) [42,43]. However, this equilibrium is shifted versus themonomeric form after release from PLGA/HPβCD/insulin LPP, suggest-ing that the protein can be rapidly absorbed in the alveoli.
Once fully characterized in vitro, PLGA/HPβCD/insulin LPPwere tested in vivo after dry powder delivery to normoglycaemic andstreptozotocin-induced diabetic rats. The fact that FITC-insulin waspresent in rat alveoli suggests that the formulated LPP are able to reachdeep lung. In particular, the presence of few green spots not super-imposed to red alveoli fluorescence 30 min after delivery (Fig. 5) arerepresentative of a protein amount likely remaining entrapped withinthe particles over alveolar surface. On the other hand, the contempor-ary appearance of a spread green fluorescence, superimposed to thered one, suggests that insulin released from PLGA/HPβCD/insulin LPPsignificantly diffuses in the alveolar tissue and is then adsorbed. Likelydue to the increasing amount of insulin released from LPP, proteindiffusion within the tissue speeded up and, at longer times, FITC-insulin appeared homogeneously spread in the alveolar epithelium.The parallel increase of spots characterized by an intense green fluo-rescence, unlikely ascribable only to PLGA/HPβCD/insulin LPP, can beattributed to a partial insulin uptake by alveolar macrophages [31].
The ability of insulin, once released into the alveoli, to cross theair-blood barrier and explicate its biological activity was confirmed byin vivo results. The pulmonary administration of insulin solutions didnot significantly affect blood glucose levels in both normoglycaemicand diabetic rats (Fig. 6). Actually, many studies have demonstratedthat pulmonary administration of insulin solutions did not result in anoptimal control of blood glucose due to the short-acting property ofthe protein in the formulation [44] and the presence of proteases thatcounteract the pulmonary absorption of insulin [45–47]. Interestingly,PLGA/HPβCD/insulin LPP, administered at the same doses used for thesolutions, significantly reduced fasting blood glucose as a function ofthe administered dose in both normoglycaemic and diabetic rats(Fig. 7). The potential of PLGA/HPβCD/insulin LPP formulationwas alsoconfirmed by pharmacological availability results showing a remark-able improvement in insulin absorption. The rapid onset of the hypo-glycaemic effect well correlates with a high insulin burst and proteinrelease in the rapidly absorbing monomeric form. In particular, bloodglucose profiles observed in the normoglycaemic group are consistentwith inhaled insulin (peak at 5–60 min), which is typically morerapidly absorbed than after subcutaneous injection (peak at 60–180 min) [37]. The short-lasting effect achieved in normoglycaemicrats is likely a consequence of glucose release from pancreas isletsgoverned by a feedback mechanism. Notable are rather the resultsachieved in the type I diabetic rats, where a severe hyperglycaemicstatus one week after streptozotocin injection was observed. PLGA/HPβCD/insulin LPP, tested at evident pathological conditions, exert avery significant and longer hypoglycaemic effect even at insulin dosesas low as 0.5 IU/kg. To our knowledge, no insulin formulation
33F. Ungaro et al. / Journal of Controlled Release 135 (2009) 25–34

Author's personal copy
for pulmonary delivery has been demonstrated to be efficient at thisdose level [37]. The 5-fold increase of pharmacological availability ofPLGA/HPβCD/insulin LPP as compared to inhaled insulin solutionfurther suggests that a powder mass not so high should beadministered on a regular basis in humans. Actually, high powderdoses are not compatible with modern DPI and may interfere withclearance and metabolism mechanisms that may operate moreefficiently at lower doses. Furthermore, the administration of lowpowder doses (i.e. a limited amount of excipients) can limit thetoxicological potential of PLGA/HPβCD/insulin LPP. Nonetheless,issues regarding a possible local irritancy and toxicity, long-termaccumulation, and immunogenicity all have to be addressed bysuitable immunotoxicological forthcoming studies.
5. Conclusions
Modern therapies in diabetes involve a great and early use ofintensive insulin regimens in order to achieve better control of bloodglucose levels and reduce the long-term risks associated with thediabetes condition. Inhaled insulin may provide an alternative formanagement of type 1 diabetes as part of a basal/bolus strategy inpatients who are unwilling or unable to use preprandial insulin injec-tions. Taken together, our results support the viability of a dry powderformulation based on biodegradable LPP for the controlled release ofinsulin to the lungs. In vivo data show that PLGA/HPβCD/insulin LPPare able to reach alveoli, release insulin in a rapidly absorbing and bio-active form and able to reduce blood glucose levels at very low doses.
Acknowledgements
The authors thankDrGianluca Grassia (Dept. of Experimental Phar-macology, University of Naples Federico II) for his kind and excellentassistance during in vivo lung deposition studies. The financial supportof Regione Campania (Legge 5/2005) is gratefully acknowledged.
References
[1] J.D. Brain, Inhalation, deposition, and fate of insulin and other therapeutic proteins,Diabetes Technol. Ther. 9 (Suppl 1) (2007) S4–S15.
[2] J.S. Patton, P.R. Byron, Inhalingmedicines: delivering drugs to the body through thelungs, Nat. Rev. Drug Discov. 6 (2007) 67–74.
[3] I.M. Shaikh, K.R. Jadhav, S. Ganga, V.J. Kadam, S.S. Pisal, Advanced approaches ininsulin delivery, Curr. Pharm. Biotechnol. 6 (2005) 387–395.
[4] W.T. Cefalu, Concept, strategies, and feasibility of noninvasive insulin delivery,Diabetes Care 27 (2004) 239–246.
[5] P.J. Atkins, Dry powder inhalers: an overview, Respir. Care 50 (2005) 1304–1312.[6] B.L. Laube, The expanding role of aerosols in systemic drug delivery, gene therapy,
and vaccination, Respir. Care 50 (2005) 1161–1176.[7] H.W. Frijlink, A.H. De Boer, Dry powder inhalers for pulmonary drug delivery,
Expert Opin. Drug Deliv. 1 (2004) 67–86.[8] L. Van Campen, G. Venthoye, Inhalation, dry powder, in: J. Swarbrick, J.C. Boylan
(Eds.), Encyclopedia of Pharmaceutical Technology, Marcel Dekker Inc., New York,2002, pp. 1529–1544.
[9] S.A. Shoyele, Engineering protein particles for pulmonary drug delivery, MethodsMol. Biol. 437 (2008) 149–160.
[10] P.A. Hollander, Evolution of a pulmonary insulin delivery system (Exubera) forpatients with diabetes, Med. Gen. Med. 9 (2007) 45.
[11] C. Dunn, M.P. Curran, Inhaled human insulin (Exubera): a review of its use in adultpatients with diabetes mellitus, Drugs 66 (2006) 1013–1032.
[12] A.H. Barnett, Exubera inhaled insulin: a review, Int. J. Clin. Pract. 58 (2004)394–401.
[13] G.S. Mack, Pfizer dumps Exubera, Nat. Biotechnol. 25 (2007) 1331–1332.[14] D.K. Malik, S. Baboota, A. Ahuja, S. Hasan, J. Ali, Recent advances in protein and
peptide drug delivery systems, Curr. Drug Deliv. 4 (2007) 141–151.[15] T.R. Kumar, K. Soppimath, S.K. Nachaegari, Novel delivery technologies for protein
and peptide therapeutics, Curr. Pharm. Biotechnol. 7 (2006) 261–276.[16] S.A. Cryan, Carrier-based strategies for targeting protein and peptide drugs to the
lungs, AAPS. J. 7 (2005) E20–E41.[17] F. Mohamed, C.F. van der Walle, Engineering biodegradable polyester particles
with specific drug targeting and drug release properties, J. Pharm. Sci. 97 (2008)71–87.
[18] D.A. Edwards, A. Ben Jebria, R. Langer, Recent advances in pulmonary drug deliveryusing large, porous inhaled particles, J. Appl. Physiol. 85 (1998) 379–385.
[19] D.A. Edwards, J. Hanes, G. Caponetti, J. Hrkach, A. Ben Jebria, M.L. Eskew, J. Mintzes,D. Deaver, N. Lotan, R. Langer, Large porous particles for pulmonary drug delivery,Science 276 (1997) 1868–1871.
[20] F. Ungaro, G. De Rosa, A. Miro, F. Quaglia, M.I. La Rotonda, Cyclodextrins in theproduction of large porous particles: development of dry powders for the sustainedrelease of insulin to the lungs, Eur. J. Pharm. Sci. 28 (2006) 423–432.
[21] G. De Rosa, M.I. La Rotonda, F. Quaglia, F. Ungaro, in: R. Kumar (Ed.), Use of Additivesin the Design of Poly(Lactide-Coglycolide) Microspheres for Drug Delivery, Hand-book of Particulate Drug Delivery, vol. 1, American Scientific Publishers, USA, 2008.
[22] J. Brange, L. Andersen, E.D. Laursen, G. Meyn, E. Rasmussen, Toward understandinginsulin fibrillation, J. Pharm. Sci. 86 (1997) 517–525.
[23] J.M. Pean, M.C. Venier-Julienne, F. Boury, P. Menei, B. Denizot, J.P. Benoit, NGFrelease from poly(D,L-lactide-co-glycolide) microspheres. Effect of some formula-tionparameters on encapsulatedNGF stability, J. Control. Release 56 (1998) 175–187.
[24] C. Perez, K. Griebenow, Effect of salts on lysozyme stability at thewater–oil interfaceand upon encapsulation in poly(lactic-co-glycolic) acid microspheres, Biotechnol.Bioeng. 82 (2003) 825–832.
[25] F. Quaglia, G. De Rosa, E. Granata, F. Ungaro, E. Fattal, M.I. La Rotonda, Feedingliquid, non-ionic surfactant and cyclodextrin affect the properties of insulin-loadedpoly(lactide-co-glycolide)microspheres prepared by spray-drying, J. Control. Release86 (2003) 267–278.
[26] G. De Rosa, D. Larobina, L.R. Immacolata, P. Musto, F. Quaglia, F. Ungaro, How cyclo-dextrin incorporation affects the properties of protein-loaded PLGA-based micro-spheres: the case of insulin/hydroxypropyl-beta-cyclodextrin system, J. Control. Release102 (2005) 71–83.
[27] R. Vanbever, J.D. Mintzes, J. Wang, J. Nice, D. Chen, R. Batycky, R. Langer, D.A.Edwards, Formulation and physical characterization of large porous particles forinhalation, Pharm. Res. 16 (1999) 1735–1742.
[28] O.R. Moss, Simulants of lung interstitial fluid, Health Phys. 36 (1979) 447–448.[29] R.O. Cook, R.K. Pannu, I.W. Kellaway, Novel sustained release microspheres for
pulmonary drug delivery, J. Control. Release 104 (2005) 79–90.[30] S. Shah, K. Fung, S. Brim, B.K. Rubin, An in vitro evaluation of the effectiveness of
endotracheal suction catheters, Chest 128 (2005) 3699–3704.[31] C. Bosquillon, V. Preat, R. Vanbever, Pulmonary delivery of growth hormone using
dry powders and visualization of its local fate in rats, J. Control. Release 96 (2004)233–244.
[32] C.T. Chien, H.F. Chien, Y.J. Cheng, C.F. Chen, S.M. Hsu, Renal afferent signalingdiuretic response is impaired in streptozotocin-induced diabetic rats, Kidney Int.57 (2000) 203–214.
[33] M. Morishita, T. Goto, K. Nakamura, A.M. Lowman, K. Takayama, N.A. Peppas, Noveloral insulin delivery systems based on complexationpolymerhydrogels: single andmultiple administration studies in type 1 and 2 diabetic rats, J. Control. Release 110(2006) 587–594.
[34] M. Miyazaki, H. Mukai, K. Iwanaga, K. Morimoto, M. Kakemi, Pharmacokinetic–pharmacodynamic modelling of human insulin: validity of pharmacological avail-ability as a substitute for extent of bioavailability, J. Pharm. Pharmacol. 53 (2001)1235–1246.
[35] S.P. Newman, W.W. Busse, Evolution of dry powder inhaler design, formulation,and performance, Respir. Med. 96 (2002) 293–304.
[36] B.L. Laube, Treating diabetes with aerosolized insulin, Chest 120 (2001) 99S–106S.[37] J.S. Patton, J. Bukar, S. Nagarajan, Inhaled insulin, Adv. Drug Deliv. Rev. 35 (1999)
235–247.[38] B.J. Meakin, P.M. Woodcock, A. Segu, F. Niccolai, C. Vecchio, Evaluation of the
resistance to airflow through Turbospin in comparison with dry powder inhalersavailable on the market., Boll. Chim. Farmaceutico-Anno135 125 (1996) 107–109.
[39] A.W. Ng, A. Bidani, T.A. Heming, Innate host defense of the lung: effects of lung-lining fluid pH, Lung 182 (2004) 297–317.
[40] R.P. Batycky, J. Hanes, R. Langer, D.A. Edwards, A theoretical model of erosion andmacromolecular drug release from biodegrading microspheres, J. Pharm. Sci. 86(1997) 1464–1477.
[41] V. Lemaire, J. Belair, P. Hildgen, Structural modeling of drug release from bio-degradable porous matrices based on a combined diffusion/erosion process, Int. J.Pharm. 258 (2003) 95–107.
[42] M.J. Ettinger, S.N. Timasheff, Optical activity of insulin. I. On thenature of the circulardichroism bands, Biochemistry 10 (1971) 824–831.
[43] Y. Pocker, S.B. Biswas, Conformational dynamics of insulin in solution. Circulardichroic studies, Biochemistry 19 (1980) 5043–5049.
[44] W.T. Cefalu, R.A. Geland, I.A. Kourides, Treatment of type 2 diabetes mellitus withinhaled human insulin: a 3-month, multicenter trial, Diabetes 47 (1998) A61.
[45] A. Yamamoto, S. Umemori, S. Muranishi, Absorption enhancement of intra-pulmonary administered insulin by various absorption enhancers and proteaseinhibitors in rats, J. Pharm. Pharmacol. 46 (1994) 14–18.
[46] A. Yamamoto, T. Fujita, S. Muranishi, Pulmonary absorption enhancement of pep-tides by absorption enhances and protease inhibitors, J. Control. Release 41 (1996)57–67.
[47] Z. Shen, Q. Zhang, S.Wey, T. Nagai, Proteolytic enzymes as a limitation of pulmonaryabsorption of insulin: in vitro and in vivo investigations, Int. J. Pharm. 192 (1999)115–121.
34 F. Ungaro et al. / Journal of Controlled Release 135 (2009) 25–34




















