
Optimization of in vitro test conditions for PLGA-based drug ...
Upload
independentCategory
view
5download
0
at SciVerse ScienceDirect
Biomaterials xxx (2011) 1e10
Contents lists available
Biomaterials
journal homepage: www.elsevier .com/locate/biomater ia ls
Periodontal regeneration using a bilayered PLGA/calcium phosphate construct
Emily C. Carlo Reis a,b,c, Andréa P.B. Borges a, Michel V.F. Araújo b,c, Vanessa C. Mendes b,c, Limin Guan d,John E. Davies b,c,d,*
aDepartamento de Veterinária, Universidade Federal de Viçosa, Campus Universitário s/n, Viçosa, Minas Gerais, CEP 36570-000, Brazilb Faculty of Dentistry, University of Toronto, 124 Edward Street, Toronto, Ontario, Canada M5G 1G6c Institute of Biomaterials and Biomedical Engineering, University of Toronto, 164 College Street, Toronto, Ontario, Canada M5S 3G9d Tissue Regeneration Therapeutics, 790 Bay St., Suite 512, Toronto, Ontario, Canada M5G 1N8
a r t i c l e i n f o
Article history:Received 28 July 2011Accepted 14 August 2011Available online xxx
Keywords:Periodontal tissue regenerationPLGA/CaP constructMacroporous topographyClot retentionClass II furcationCanine
* Corresponding author. Institute of BiomaterialsUniversity of Toronto, 164 College Street, Toronto,Tel.: þ1 416 978 1471; fax: þ1 416 946 5639.
E-mail address: [email protected] (J.E. Davies
0142-9612/$ e see front matter � 2011 Published bydoi:10.1016/j.biomaterials.2011.08.040
Please cite this article in press as: CarloBiomaterials (2011), doi:10.1016/j.biomateri
a b s t r a c t
The regeneration of tissues affected by periodontal disease is a complex process; it encompasses theformation of bone, cementum and periodontal ligament. We developed a semi-rigid PLGA (polylactide-co-glycolide acid)/CaP (calcium phosphate) bilayered biomaterial construct to promote periodontalregeneration, which has a continuous outer barrier membrane and an inner topographically complexcomponent. Our experimental model compared periodontal prophylaxis alone with prophylaxis andbiomaterial implantation in the treatment of class II furcation defects in dogs. Clinical evaluation, micro-computed tomography, histology and backscattered electron imaging were used for data analysis.Healing occurred uneventfully and bone volumetric values, trabecular number and trabecular thicknesswere all significantly greater in the treated group; while trabecular separation was significantly greater inthe control group. New cementum, bone, and periodontal ligament with Sharpey fibre insertions wereonly seen in the treated group. Although periodontal regeneration has been reported elsewhere, theadvantages of employing our bilayered PLGA þ CaP construct are twofold: 1)it did not collapse into thedefect; and, 2) its inner side was able to retain the blood clot throughout the buccal defect. The result wasgreater periodontal regeneration than has previously been reported with traditional flexible membranes.
� 2011 Published by Elsevier Ltd.
1. Introduction
Periodontal disease, or periodontitis, is an infectious diseasecharacterized by the destruction of tooth supporting tissues due toa severe inflammatory and immune response elicited by bacteriaharbored in tooth-retained plaque [1e3]. It is a worldwide healthproblem, reported toworsenwith age, which can be associatedwithlocal and systemic conditions [1,4e7]. Periodontitis is also the mostcommon disease in dogs and has become a very important issue inveterinary medicine as domestic pets reach older ages [8,9]. Inter-estingly, canine and human periodontal diseases share many traits;such as etiology [8,10,11], histological features that have beendescribed since the 1970’s [12], and the association with both coro-nary cardiovascular [6,13,14] and renal [7,13,14] diseases. Further-more, diagnostic tools such as clinical attachment level and probingdepth are used in both human and veterinary dental fields [15].
and Biomedical Engineering,Ontario, Canada M5S 3G9.
).
Elsevier Ltd.
Reis EC, et al., Periodontal rals.2011.08.040
Understanding the mechanisms of periodontal regeneration inhumans and dogs has been the subject of numerous studies as theperiodontium represents a uniquely challenging environmentrequiring the coordinated formation of cementum, periodontal liga-ment (PDL), alveolar bone and gingiva [2,16e19]. Different treatmentstrategies for periodontal regeneration have been reported in theliterature [20,21]. Scaling and root planing(SRP) comprise the firsttreatment option for periodontal defects [22e24], which is aimed atremoving the causative agent (i.e. plaque, calculus) and smoothingthe root surface for subsequent PDL attachment. However, thisstrategy fails to stabilize the clot and allows epithelial/connectivetissue ingress to periodontal defects, resulting in tissue repair ratherthan regeneration. In humans, scaling and root planing is commonlyused to prepare the periodontal environment for subsequent regen-erative procedures [2,22]. However, in dogsSRP currently representsthe best and most conservative alternative to tooth extraction.Nevertheless, in veterinary practice, tooth loss is still very commoneither by extraction or secondary to advanced periodontal disease[23,24]. Overall, oronasal fistulas and pathologic jaw fractures arecommon outcomes of the bone resorption that follows tooth loss onthe palatal aspect of themaxillary canine and the horizontal ramus ofthe mandible, respectively [23,25].
egeneration using a bilayered PLGA/calcium phosphate construct,

Fig. 1. Sequence of in vivo procedures. (A) Shows the 5 mm � 5 mm � 3 mm class II furcation defect partially exposing the roots. (B) Scaling and root planing was performed afterperiodontal disease induction by filling the defect with an impression materialfor 21 days. (C) Fourteen days later, the PLGA þ CaP bilayered biomaterial was placed covering thedefect of the treated group.
E.C. Carlo Reis et al. / Biomaterials xxx (2011) 1e102
Despite the severe outcomes of periodontitis, regeneration ofthe periodontal tissue is not the main goal in current veterinarypractice. Possible reasons for this could be the high cost of thelimited regenerative procedures available, or the fact that mostcanine regenerative strategies are still exploratory, including theuse of enamel matrix derivative proteins [26], autologous orsynthetic grafts [27,28], and guided tissue regeneration (GTR) [29].
Guided tissue regeneration utilizes barrier membranes fordefect site protection and clot stabilization while enablingprogenitor cell recruitment and migration from the perivascularcompartments of the surrounding PDL and alveolar bone. Thesemesenchymal progenitors will in turn direct the regeneration ofcementum (pre-cementoblasts), PDL (fibroblasts), and bone (pre-osteoblasts) [2,17]. Many different membranes have been used asGTR treatment in humans after experimental evaluations in dogs,including expanded polytetrafluoroethylene (ePTFE) [20,30],collagen [31e33], poly-L-lactic acid [34], lactic acid-glycolic acid co-polymer [35], and polylactide acetyl tributyl citrate [19]. Never-theless, these materials are strictly employed as physical barriers toprotect the clot and prevent soft tissue ingress to periodontaldefects [2].
Recently, new approaches to GTR membrane design have beensuggested. Owen et al. [36,37] modified the surface of polymericmembranes to provide smooth, grooved or etched topographies,and showed that such changes differentially affected the coloni-zation and proliferation of adherent cells in vitro. A differentapproach adopted by Liao et al. [38] relied on a functionally gradedthree layered design of a complex PLGA-based composite with littlemacroporosity but high mechanical strength, which they demon-strated to be a suitable culture substrate for MC3T3-E1 cells.However, neither group tested their materials in vivo.
Given the need for regenerative therapy of periodontal defectsin both dogs and humans, we have developed a new bilayeredbiomaterial construct based upon a three-phase resorbable scaffoldthat combines a co-polymer (polylactide-co-glycolide acid - PLGA)with two phases of calcium phosphate (CaP) d that we refer toherein as the “construct”. We have reported extensively elsewhereon the composition and structure of the scaffold [39,40] and alsoemployed it clinically as a bone graft material [41]. The construct isboth structurally stable and adaptable, characteristics that favorforming to different defect morphologies but preventingmembrane collapse. The inner side of this biomaterial was con-structed with a topographically complex macroporous surface,previously shown to be osteoconductive [42]. It was designed withhighly interconnected macroporosity, has an ability to wick upblood, and acts as a clot retention device [41]. The outer layer, on
Please cite this article in press as: Carlo Reis EC, et al., Periodontal rBiomaterials (2011), doi:10.1016/j.biomaterials.2011.08.040
the other hand, is a thin membrane that acts as a barrier to cellinvasion. We sought, in the work described herein, to investigatethe potential use of this construct for the regeneration of peri-odontal defects in the dog, both as a model for human therapy, andas a putative regenerative strategy for veterinary dentistry.
2. Materials and methods
2.1. Construct fabrication
Each PLGA þ CaP(polylactide-co-glycolide þ calcium phosphate) construct usedin this study comprised (i) a flatsmooth outer layer and (ii) a 1 mm thick roughmacroporous inner layer. Fabrication followed a 2-step procedure. First, the innermacroporous composite scaffold, composed of 75/25 polylactide-co-glycolide(PLGA) and 2 phases of calcium phosphate (CaP), was prepared according tomethods described in detail elsewhere [38]. Briefly, CaP particles (27 mm averagesize) were thoroughly mixed in dimethylsulfoxide-dissolved PLGA. The solutionwasdispersed onto a sugar mold [40] and allowed to solidify at �18 �C. Next,in order tocreate a porous structure the solidified block was soaked in distilled water for 3 daysto leach the sugar. Thin sections of approximately 1 cm � 1 cm � 1 mm wereproduced with a scalpel and then coated with a CaP layer by immersion in a mixedionic solution at 37 �C for 24 h [39].
The second step consisted of the preparation of a PLGA þ CaP solution that waspoured onto a Teflon-coated aluminum foil. The previously CaP coated thin sheetswere placed on this PLGA þ CaP solution just prior to setting. A final bilayered sheet(inner macroporous structure, outer membrane layer) was peeled off the teflon-coated aluminum foil and trimmed to detach the several membranes with indi-vidual sizes of 1.5 cm � 1.5 cm � 1 mm.
2.2. Surface analysis
Three constructs were coated with gold in an EMS550� sputter coater andanalyzed by scanning electron microscopy (SEM; LEO 1430VP, England and HitachiSU6600, Canada) at 15 kV and 5 kV. Ten pictures of both the inner and outer surfaceswere taken at increasing magnifications (100, 2 k and 18 k) for analysis of pore size.Macro and micropores were identified by the superimposition of a 10 � 10 grid oneach micrograph taken at�100 and�2 k magnifications respectively. Pore diameterwas then attained using the Analysis 5� software (Olympus, Japan).
2.3. In vivo experimental work
The in vivo procedures were reviewed and approved by the Ethics Committee onAnimal Research, Veterinary Department (Universidade Federal de Viçosa, Brazil).Ten healthy adult (4 male and 6 female) periodontal disease-free mongrel dogs,weighing about 10e15 kg were selected. The animals were fed soft dog chow for theentire experiment. Three days prior to each surgical procedure, animals receivedoral spiramycin (23.5 mg/kg/day) associated withdimetridazole (12.5 mg/kg/day)(Spiraphar�, Virbac do Brasil, Brazil) and the medication continued for a total of 6days.
The animals fasted for 8 h prior to anesthesia. Sedation was obtained usingacepromazine (0.1 mg/kg intravenously [IV]), and general anesthesia was inducedwith propofol (6 mg/kg IV), then maintained with a mixture of oxygen and iso-flurane. Chlorhexidine 0.12%was used to rinse the oral cavity of each dog during pre-and post-operative procedures.
egeneration using a bilayered PLGA/calcium phosphate construct,

Fig. 2. The membrane (A) and the macroporous (B) surfaces of the bilayered construct.Macro- (C), micro- (D) and nano-pores (E) are all seen by SEM on the macroporousside.
E.C. Carlo Reis et al. / Biomaterials xxx (2011) 1e10 3
2.3.1. Periodontal disease inductionBaseline clinical attachment level (CAL) was measured with a periodontal probe
(PCP-UNC 15, Hu-Friedy, USA) from the cemento-enamel junction (CEJ) to thebottom of the gingival sulcus (or periodontal pocket), at the central area of thefurcation of the lower 4th and upper 2nd right premolars. These teeth were selectedas they are very similar in size, morphology and periodontal disease progression[1,11,42]. Also, standardized periapical radiographs [8] were taken (Timex 70C,Gnatus, Brazil) prior to each of the procedures for a reference image of the furcationarea.
Mucoperiosteal flaps were elevated to expose the buccal bonewalls. Acylindricaldiamond bur (FG1016, KG Sorensen, Brazil) was used to create class II furcationdefects (exposing the roots on the buccal side but still keeping a lingual wall) withthe following dimensions: 5 mm apicocoronally (anatomical reference: CEJ at thecentre of the furcation), 5 mm mesiodistally and 3 mm buccolingually (anatomicalreference: buccal aspect of the alveolar bone) (Fig. 1A). Scaling was subsequentlyperformed to remove periodontal ligament fibers and debris from root surfaces andthe defects were completely filled with an impression material (Impregum Soft�,3M Brazil). The flaps were repositioned and closed with non-resorbable sutures (5e0nylon suture, J&J Ethicon), and post-operative radiographs were taken.
Sutures were removed after 10 days but the impression material was kept in thedefects for a total of 21 days. Immediately after the material was removed, a secondCAL measurement was performed followed by prophylaxis, which compriseda surgical open flap procedure for scaling (Fig. 1B), root planning and irrigation withchlorhexidine 0.12%. After the flap was closed, a new set of radiographs was taken.Surgical wounds were rinsed with chlorhexidine 0.12% every 12 h for 2 weeks.
2.3.2. Guided tissue regeneration (GTR)Two weeks after prophylaxis, animals were anesthetized and new radiographs
were taken. A surgical flap was raised once more and the defects were scaled toremove soft tissue. Each defect was measured in the apicocoronal, mesiodistal andbuccolingual directions, and these dimensions were compared to the initial ones of5 mm � 5 mm � 3 mm using one-way ANOVA. Using a round bur (FG1016, KGSorensen, Brazil), notches were made on the surface of the roots to serve as futurereference for the apical limit of the defect.
The lower 4th right premolar was assigned as the treated group. The PLGAþ CaPconstruct (approximately 1.5 cm � 1.5 cm � 1 mm) was immersed in sterile salinesolution at approximately 40 �C for 1 min to soften. Next, it was positioned to coverthe defect (Fig. 1C), with the margins extending approximately 3 mm mesially,distally and apically, as suggested by Christgau et al. [2], with the inner macroporoussurface toward the defect. The construct was then allowed to harden for a fewminutes and stabilized with a 1.5 mm � 6 mm screw (Ortovet, Brazil) positioned onthe apical portion of the furcation area (Fig. 1C). Finally, the flap was closed withnon-resorbable sutures (5e0 nylon suture, J&J Ethicon). The same surgical procedure(including screw insertion, but without a construct) was repeated in the controldefect on the upper 2nd right premolar. Thus, each dog had both treated(PLGA þ CaP construct) and control (no construct) groups. Post-operative radio-graphs were taken immediately after the surgical procedure. Spiramycin (23.5 mg/kg/day) withdimetridazole (12.5 mg/kg/day) (Spiraphar�, Virbac do Brasil, Brazil)were administered until suture removal (10 days post-operative).
Animals were clinically evaluated on a daily basis for 14 days post-operative fordehiscence, gingival recession, inflammation, bleeding, edema and membraneexposure to the oral cavity. During this time, surgical wounds were rinsed withchlorhexidine 0.12% every 12 h. By the end of this period, a tooth brushing routinewas implemented every other day until the end of the observation period (60 and120 days).
CAL measurements, radiographs and prophylaxis were performed monthly. Fiveanimals were euthanized by an overdose of general anesthetic at 60 days post-operative and the remaining five at 120 days. Biopsies comprising the teeth ofinterest and surrounding alveolar bone were harvested and fixed in 10% formalin.Themean CAL of the control and PLGAþ CaP construct groupswas compared at eachtime-point using one-way ANOVA, followed by Tukey test when necessary(p < 0.05).
2.4. Micro-computed tomography (MicroCT)
Groups of 3 biopsy specimens were stacked in a 30 mm cylindrical holder andscanned using a micro-computed tomography system (MicroCT40, Scanco,Switzerland) at 85 kV and 77 mA. After image reconstruction, two-dimensional (2D)images representing axial cuts (10 mm thick) of the harvested samples were used toselect the region of interest (ROI) for analysis. The defect’s coronal limit (ROI top)corresponded to the CEJ line. The apical limit (ROI bottom) was defined by a plane1 mm coronal to each defect height so that only new bone was included in themeasurement. The root canals were used as anatomical reference points for themesial, distal and lingual ROI limits. The buccal limit on the lower half of the defectwas set at a 0.5 mm distance measured from the root buccal surface. For the upperhalf of the defect the buccal ROI limit was set at the buccal root surface. Thesereference points were used to draw the defect area at different depths in the 2Dimages, which were morphed to form a 3D image representing the volume ofinterest. The quantification of bone formation (bone volume/total volume, or BV/TV)
Please cite this article in press as: Carlo Reis EC, et al., Periodontal rBiomaterials (2011), doi:10.1016/j.biomaterials.2011.08.040
as well as trabecular number, thickness and separationwas possible by determiningthe gray-level distribution at specific thresholds for samples at 60 and 120 dayspost-operative. Control and construct groups were compared using one-way ANOVAfor each of these quantification parameters, followed by Tukey test when necessary(p < 0.05).
2.5. Histology processing and analysis
Two samples of each group at both time-points (60 and 120 days) were decal-cified in formic acid and sodium citrate and embedded in paraffin. Samples were
egeneration using a bilayered PLGA/calcium phosphate construct,
E.C. Carlo Reis et al. / Biomaterials xxx (2011) 1e104
sectioned with a thickness of 7 mm. One sample was sectioned longitudinally d ina mesiodistal directiond in order to observe the most coronal part of the furcation.The other sample was sectioned in cross-section, so that the tissueemembraneinterface could be analyzed. Slides were stained with haematoxylin and eosin (H&E)for light microscopy (Aristoplan, Leitz, Germany).
The other 3 samples per group at both time-points were dehydrated in serialconcentrations of ethanol (70, 95 and 100 v/v) and embedded in poly-methylmethacrylate (Osteobed, Polysciences, USA) according to the manufacturer’sprotocol. Next, 30 mm-thick longitudinal sections were obtained using the EXAKTcutting and grinding system (Exakt Technologies Inc., USA). One sample was cut inthe buccolingual direction so that the membraneetissue interface would beexposed. The other two samples were sectioned in the mesiodistal direction foranalysis of the furcation area. The resulting slides were gold-coated for back-scattered electron imaging (BSEI) of the membraneetissue interface. After BSEIanalysis, samples were further ground to 15 mm thin sections and stained with H&Efor light microscopy (Aristoplan, Leitz, Germany).
Sectioning of the decalcified and non-decalcified samples were guided byreference points and linear measurements obtained from MicroCT images. Allsamples were assessed for the tissues formed in the furcation defect area, withspecial attention to the periodontal support formed by the connections betweenbone, periodontal ligament and cementum.
3. Results
3.1. Surface analysis
Surface topography evaluation, by SEM, of the flat outermembrane of the PLGA þ CaP bilayered construct (Fig. 2A) showedsparce pores, which did not traverse the membrane, and were-randomly distributed on an otherwise featureless surface. Ofthese, 61.67% were smaller than 50 mm (22.02 mm � 11.46) and2.59% were greater than 200 mm (269.88 mm � 12.53). On thecontrary, the 1 mm thickmacroporous side was characterized bythe presence of interconnected macropores (Fig. 2B and C), where66.17% were greater than 500 mm (703.01 mm � 134.20). Thesurface of the composite defining the pores was characterized byglobular particles and micropores (4.47 mm � 2.55) (Fig. 2D)
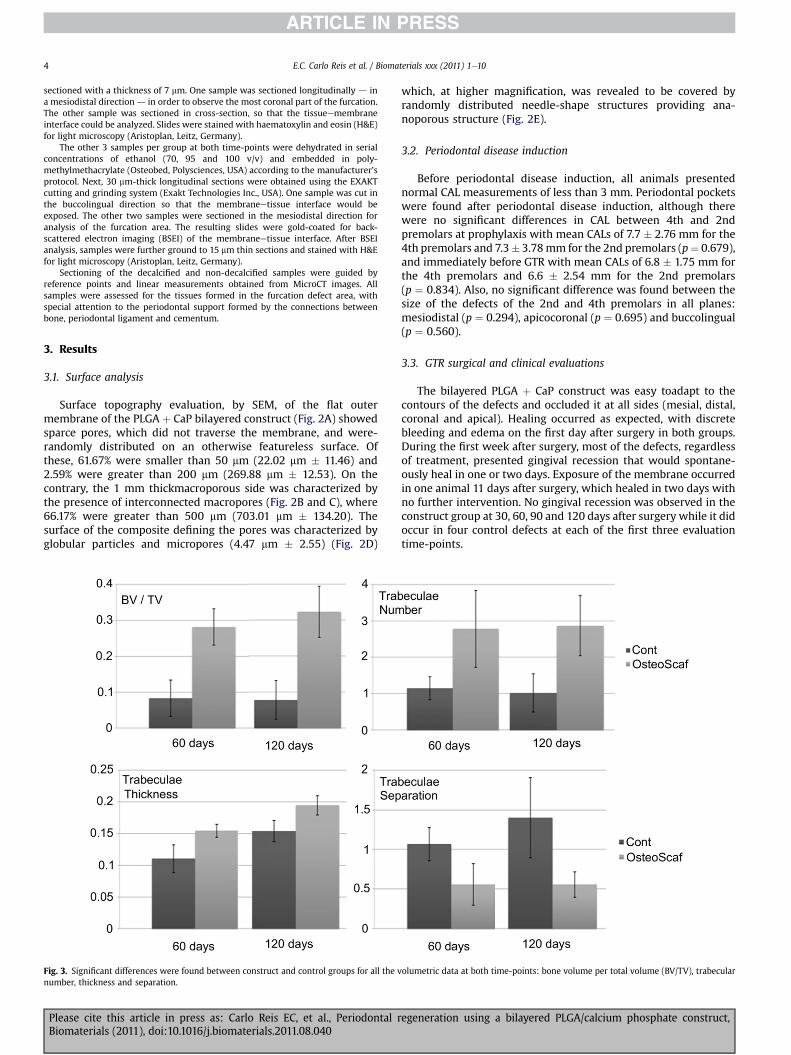
Fig. 3. Significant differences were found between construct and control groups for all the vnumber, thickness and separation.
Please cite this article in press as: Carlo Reis EC, et al., Periodontal rBiomaterials (2011), doi:10.1016/j.biomaterials.2011.08.040
which, at higher magnification, was revealed to be covered byrandomly distributed needle-shape structures providing ana-noporous structure (Fig. 2E).
3.2. Periodontal disease induction
Before periodontal disease induction, all animals presentednormal CAL measurements of less than 3 mm. Periodontal pocketswere found after periodontal disease induction, although therewere no significant differences in CAL between 4th and 2ndpremolars at prophylaxis with mean CALs of 7.7 � 2.76 mm for the4th premolars and 7.3� 3.78mm for the 2nd premolars (p¼ 0.679),and immediately before GTR with mean CALs of 6.8 � 1.75 mm forthe 4th premolars and 6.6 � 2.54 mm for the 2nd premolars(p ¼ 0.834). Also, no significant difference was found between thesize of the defects of the 2nd and 4th premolars in all planes:mesiodistal (p ¼ 0.294), apicocoronal (p ¼ 0.695) and buccolingual(p ¼ 0.560).
3.3. GTR surgical and clinical evaluations
The bilayered PLGA þ CaP construct was easy toadapt to thecontours of the defects and occluded it at all sides (mesial, distal,coronal and apical). Healing occurred as expected, with discretebleeding and edema on the first day after surgery in both groups.During the first week after surgery, most of the defects, regardlessof treatment, presented gingival recession that would spontane-ously heal in one or two days. Exposure of the membrane occurredin one animal 11 days after surgery, which healed in two days withno further intervention. No gingival recession was observed in theconstruct group at 30, 60, 90 and 120 days after surgery while it didoccur in four control defects at each of the first three evaluationtime-points.
olumetric data at both time-points: bone volume per total volume (BV/TV), trabecular
egeneration using a bilayered PLGA/calcium phosphate construct,
E.C. Carlo Reis et al. / Biomaterials xxx (2011) 1e10 5
The mean CAL for the construct group decreased to a normalvalue at a greater rate than the controls, although no significantdifference was found within time-points (p ¼ 0.10 at 30 days,p¼ 0.06 at 60 days, p¼ 0.13 at 90 days and p¼ 0.12 at 120 days). Forthe construct group, the mean CAL of 6.8 � 1.75 mm measuredimmediately before GTR, a value resulted from the previous peri-odontal disease condition, had decreased to 3.9 � 1.91 mm at 30days after GTR. At 60 days, mean CAL had reached a value consid-ered normal for dogs (2.6 � 1.17 mm), decreasing to 2.4 � 0.89 mmand 1.8� 0.44mm at 90 and 120 days, respectively. As for the meanCAL of the controls, the 6.6 � 2.54 mm CAL measured immediatelybefore GTR decreased to 5.0 � 0.81 mm at 30 days. From 60 daysforward, it remained slightly above normal values for dogs:3.6 � 1.17 mm, 3.6 � 1.34 mm at 90 days and 3.8 � 1.34 mm at 120days.
3.4. MicroCT
MicroCT volumetric values showed more bone volume per totalvolume (original defect volume) in construct samples than incontrols at 60 (p < 0.01) and 120 (p < 0.01) days. Also trabecular
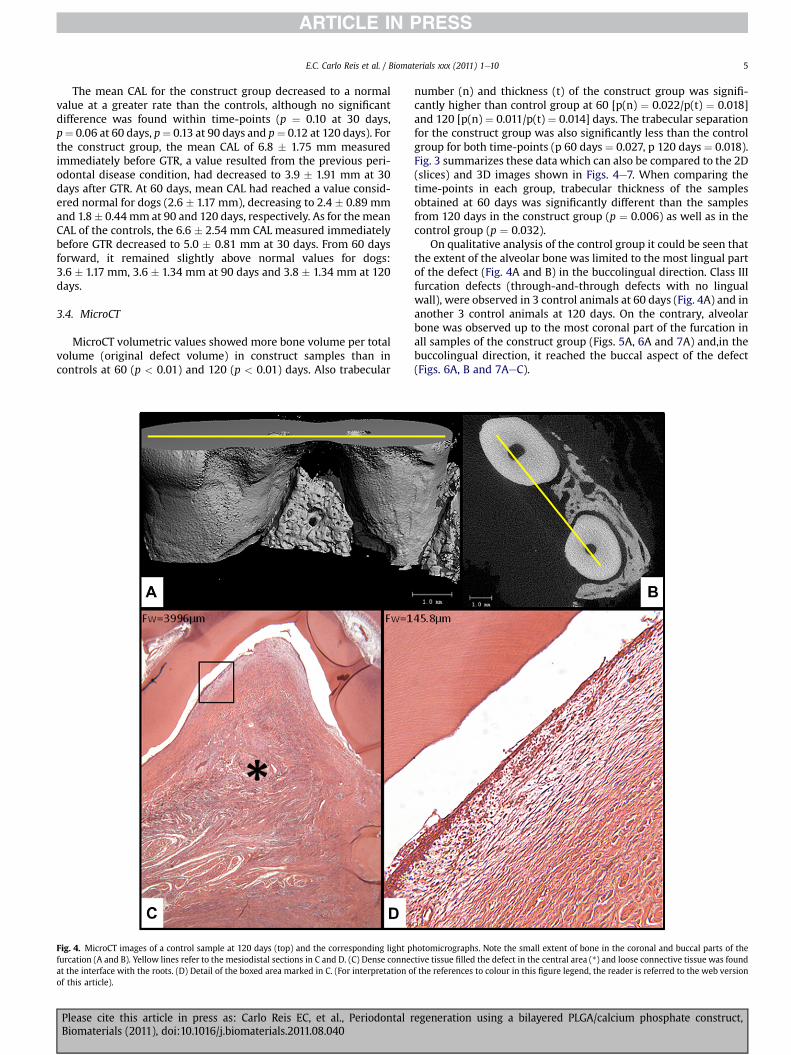
Fig. 4. MicroCT images of a control sample at 120 days (top) and the corresponding light pfurcation (A and B). Yellow lines refer to the mesiodistal sections in C and D. (C) Dense connecat the interface with the roots. (D) Detail of the boxed area marked in C. (For interpretation oof this article).
Please cite this article in press as: Carlo Reis EC, et al., Periodontal rBiomaterials (2011), doi:10.1016/j.biomaterials.2011.08.040
number (n) and thickness (t) of the construct group was signifi-cantly higher than control group at 60 [p(n) ¼ 0.022/p(t) ¼ 0.018]and 120 [p(n) ¼ 0.011/p(t) ¼ 0.014] days. The trabecular separationfor the construct group was also significantly less than the controlgroup for both time-points (p 60 days ¼ 0.027, p 120 days ¼ 0.018).Fig. 3 summarizes these data which can also be compared to the 2D(slices) and 3D images shown in Figs. 4e7. When comparing thetime-points in each group, trabecular thickness of the samplesobtained at 60 days was significantly different than the samplesfrom 120 days in the construct group (p ¼ 0.006) as well as in thecontrol group (p ¼ 0.032).
On qualitative analysis of the control group it could be seen thatthe extent of the alveolar bone was limited to the most lingual partof the defect (Fig. 4A and B) in the buccolingual direction. Class IIIfurcation defects (through-and-through defects with no lingualwall), were observed in 3 control animals at 60 days (Fig. 4A) and inanother 3 control animals at 120 days. On the contrary, alveolarbone was observed up to the most coronal part of the furcation inall samples of the construct group (Figs. 5A, 6A and 7A) and,in thebuccolingual direction, it reached the buccal aspect of the defect(Figs. 6A, B and 7AeC).
hotomicrographs. Note the small extent of bone in the coronal and buccal parts of thetive tissue filled the defect in the central area (*) and loose connective tissue was foundf the references to colour in this figure legend, the reader is referred to the web version
egeneration using a bilayered PLGA/calcium phosphate construct,

Fig. 5. MicroCT image of a mesiodistal view (A) of a PLGA þ CaP sample at 60 days and the corresponding light photomicrographs B, C, D and E. A. New alveolar bone fills the defectarea, emphasized by the green color on the sectioned bone. (B) The bottom of the defect, where remnants of the PLGA þ CaP construct can be seen (empty arrows), as well as newbone (thick arrow head), periodontal ligament (*) and cementum (thin arrow). (C) Section obtained from the most coronal part of the furcation, marked in A. Note the alveolar boneup to the most coronal part of the furcation, with the newly formed periodontal ligament. Cementoblasts and cementoid were seen in these areas (arrow in D) as well as osteoblastsand osteoid (arrow in E). (For interpretation of the references to colour in this figure legend, the reader is referred to the web version of this article).
E.C. Carlo Reis et al. / Biomaterials xxx (2011) 1e106
3.5. Histological analysis
The defect areas in control samples were mainly filled bya dense connective tissue (Fig. 4C) at both time-points. At theinterface with the root in the most coronal part of the defect, looseconnective tissue was found (Fig. 4D). Cementum and periodontalligament were observed along with alveolar bone only in a fewareas closer to the apical limit of the defect.
In contrast, the periodontiumhad been formed in the defects ofall samples of the construct group at both time-points. Newcementum and periodontal ligament were always present alongwith the new alveolar bone from the apical limit up to the mostcoronal part of the defect as well as from the lingual to the buccalarea (Figs. 5e7). At the apical limit of the defects, a reversal lineoutlined the interface between old and new alveolar bone-Trabeculae were densely covered by active osteoblasts and osteoidcould be easily distinguished in the undecalcified samples (Fig. 5E).Similarly, cementoid and highly active cementoblasts covered thenew cellular cementum, (Figs. 5D and 7F). No newly-formeda cellular cementum was observed. In cross-sections, cellularcementum was found in continuity with the old cementum alongthe root surface (Fig. 7F). Extrinsic collagen fibers emerged from thenew cementum to a well organized PDL with parallel and
Please cite this article in press as: Carlo Reis EC, et al., Periodontal rBiomaterials (2011), doi:10.1016/j.biomaterials.2011.08.040
perpendicular fibers and blood vessels. Under polarized micros-copy, the birefringent collagen fibers were seen to emerge from thenew cementum, crossing the periodontal ligament space andinserting into new bone (Fig. 7D and E). Remnants of the constructwere observed only in 60 daysamples (Fig. 5C) enveloped by, and indirect contact with, the new bone (Fig. 6C and D). No ankylosis orroot resorption were observed.
4. Discussion
We report herein the development of a PLGA þ CaP bilayeredbiomaterial construct and its use in optimal periodontal regener-ation. Our results have clearly shown that the construct hasenhanced the regeneration of cementum, PDL and alveolar bone inclass II furcation defects in dogs.
Membranes made of different biomaterials such as ePTFE [2,30],collagen [2,31], polydioxanon [2] and polylactic acid (PLA) [2,43]have previously been reported to favor the regeneration of class IIfurcation defects. However, these studies were based exclusively onthe histomorphometrical analyses of mesiodistal sections. Indeed,as already discussed by Christgau et al. [2], mesiodistal sections ofclass II furcation defects can be inadvertently taken from an areatoo close to the intact periodontal tissues on the lingual side. As
egeneration using a bilayered PLGA/calcium phosphate construct,

Fig. 6. A and B. MicroCT images of a PLGA þ CaP sample at 60 days. (A) 3D image showing reference planes to the images in B, C and D. Yellow line indicates the cross-section in B,where bone can be seen on the buccal side of the furcation. Red line indicates buccolingual sections on SEM backscattered electron images in C and D. Remnants of the PLGA þ CaPconstruct can be seen on the buccal side (arrows) surrounded and in direct contact with new alveolar bone. (D) Micrograph at higher magnification of the boxed area marked in C.(For interpretation of the references to colour in this figure legend, the reader is referred to the web version of this article).
E.C. Carlo Reis et al. / Biomaterials xxx (2011) 1e10 7
a result, histomorphometrical analysis of these sections can showmore tissue regeneration than those taken from more buccalre-gions located within the area of the defect. We have avoided thisproblem by combining information from two methods of analysis:histology and microCT. First, we used light microscopy to qualita-tively compare differences in periodontal regeneration betweentreated and control groups in three anatomical planes: mesiodistal,buccolingual and cross-sections. The next step comprised theprecise location and analysis of the histological planes of sectionthrough comparison with MicroCT slices. These qualitative evalu-ations showed more regeneration of PDL and cementumin theconstruct group.
In addition, we also quantified the volume of regeneratedalveolar bone by microCT. This analysis is more complete andaccurate than the linear measurements derived from 2D images asdescribed in the studies mentioned above [2,30,31,43], and offers
Please cite this article in press as: Carlo Reis EC, et al., Periodontal rBiomaterials (2011), doi:10.1016/j.biomaterials.2011.08.040
additional possibilities of quantification of trabecular number,thickness and separation. In our study, this combined datademonstrated the presence of more mature bone in the constructgroup. The quantitative analysis has enabled us to demonstratea greater degree of buccal bone regeneration than has been shownin previous reports using thinner, more flexible GTR membranes[2,32,34,35,44e46].
The stiffness of the construct prevented collapse of the materialinto the defect site, a problem that has been reported withresorbable membranes made of materials such as collagen [2,32],PLA [2,34] and PLGA [35]. By collapsing into the defect, a biomate-rial can occupy the space that should be available for periodontalregeneration. Thus, our construct can be considered a biodegrad-able space maintainer, providing a protective environment fortissue regeneration, and favoring periodontal tissue growth withinthe defect [34,47,48].
egeneration using a bilayered PLGA/calcium phosphate construct,

Fig. 7. MicroCT images of a PLGA þ CaP sample at 120 days. (A) The alveolar bone is extending to the most coronal part of the furcation as well as the buccal aspect of the furcation.Yellow and green reference lines mark the locations of the cross-sections in B and C respectively (plane on the same level as the control sample in Fig. 4B). (D) and E were obtainedfrom the boxed area in B. New cementum (thin arrows) and periodontal ligament (*) formed along with the new alveolar bone (large arrows). (E) shows the collagen fibers of theperiodontal ligament under polarized light, perpendicularly inserting in the new cementum, crossing the periodontal ligament and inserting in the bone on the opposite side. (F)New cellular cementum (thin arrow) continuous with the acellular (thick arrow) and cellular (empty arrow) layers of old cementum (the arrow inC shows the location of thissection). (For interpretation of the references to colour in this figure legend, the reader is referred to the web version of this article).
E.C. Carlo Reis et al. / Biomaterials xxx (2011) 1e108
Further to space maintenance, the macroporous aspect of theconstruct acts as a clot retention device [41]. The topographicallycomplex inner surface of the constructfavors fibrin matrix attach-ment [52,53]. Periodontal regeneration can only be attained afteran intricate, overlapping sequence of events has occurred [47].Briefly, platelet activation promotes blood clot formation, which isfollowed byangiogenesis with which perivascular progenitorsreach thewound site and initiate the formation of reparativematrix[2,49e51]. As the biomaterial is stiff and capable of maintaining itscontour, it prevents or limits wound contraction, providinga greater volume of provisional matrix through which regenerationoccurred. Additionally, the complex surface topography engenders
Please cite this article in press as: Carlo Reis EC, et al., Periodontal rBiomaterials (2011), doi:10.1016/j.biomaterials.2011.08.040
greater platelet adhesion and activation as well as osteoblastactivity [36,38,52,53]. Upon signaling, progenitor cells originatefrom the perivascular undifferentiated cells surrounding vessels inthe remaining PDL and alveolar bone as shown by McCulloch andcolleagues [54,55]. Hence, progenitor cells had both a greatervolume of matrix through which they could migrate and thesignaling for the migration toward a more buccal region, resultingon a greater regeneration of buccal bone in the furcation defect[2,32,34,35,44e46].
Different topographically complex membranes have beendeveloped to favor periodontal regeneration, including bone on thebuccal region. Their structure, degradation rate and influence on
egeneration using a bilayered PLGA/calcium phosphate construct,

E.C. Carlo Reis et al. / Biomaterials xxx (2011) 1e10 9
cell activity were analyzedin vitro, but are yet to be evaluated inperiodontal defects [36e38,53,56e60]. Indeed, it is known thatonly a portion of the periodontal defect can be successfullyregenerated by techniques and membranes available today [18].Experimental work and clinical trials have clearly shown a lack ofcomplete closure of furcation defects or have failed to evaluate theirentire volume [30,43,61e64]. In the present study, we were able todemonstrate regeneration of tissues inside the furcation and on thebuccal region. However, not the entire buccal periodontium wasformed, especially in the most coronal part of the defect. It isnoteworthy that remnants of the biomaterial were found insamples at 60 but not at 120 days, showing that the material wasdegraded or resorbed between these time-points. Based on theconcepts of space-provision, prevention of wound contraction andcell migration, we hypothesize that if the PLGA þ CaP bilayeredbiomaterial were to remain in place longer, more buccal bonewould be regenerated, as more cells would reach the buccal andcoronal areas. In fact the degradation rate of our PLGA þ CaPbilayered biomaterial can be fined-tuned across a wide range bymodifying both the polymer molecular weight and the co-polymerratio [39,40]. Such modification raises the possibility for thecomplete regeneration of a furcation defectto the extent of thepreviously healthy periodontium.
5. Conclusion
We have shown that a biodegradable PLGA þ CaP bilayeredbiomaterial construct can be adaptable to different anatomicalmorphologies, stiff enough to prevent collapse into the defect andpermit Periodontal regeneration in class II furcation defects in dogs.
Acknowledgments
The authors would like to thank CAPES for Dr. Carlo Reis’scholarship, CNPq for funding this project and Virbac do Brasil fortheir support. We would also like to express our gratitude to Fer-yalSarraf (U of T), Nancy Valiquette (U of T) and both CláudiaAlencarVanetti and Karla Veloso Gonçalves Ribeiro from the Núcleode Microscopia Eletrônica e Microanálises (CCB/UFV) for theirvaluable assistance.
References
[1] Loe H, Anerud A, Baysen H, Smith M. The natural history of periodontaldisease in man. The rate of periodontal destruction before 40 years of age.J Periodontol 1978;49:607e20.
[2] Christgau M, Caffesse RG, Schmalz G, D’Souza N. Extracellular matrixexpression and periodontal wound-healing dynamics following guided tissueregeneration therapy in canine furcation defects. J Clin Periodontol 2007;34:691e708.
[3] Kinane DF, Benhlund T, Lindhe J. Pathogenesis of periodontis. In: Lindhe J,Lang NP, Kaming T, editors. Clinical periodontology and implant dentistry.Munksgaard. Singapore: Blackwell; 2008. p. 286e306.
[4] Albandar JM, Rams TE. Global epidemiology of periodontal diseases: anoverview. Periodontology 2000;29:7e10. 2002.
[5] Brown LJ, Johns BA, Wall TP. The economics of periodontal diseases. Perio-dontol 2000;29:223e34. 2002.
[6] Paquette DW, Brodala N, Nichols TC. Cardiovascular disease, inflammation,and periodontal infection. Periodontol 2000;44:113e26. 2007.
[7] Craig RG. Interactions between chronic renal disease and periodontal disease.Oral Dis 2008;14:1e7.
[8] Wiggs RB, Lobprise HB. Periodontology. In: Wiggs RB, Lobprise HB, editors.Veterinary Dentistry. Principles and practice. Philadelphia: Lippincott-Ravens;1997. p. 186e231.
[9] Harvey CE. Periodontal disease in dogs: etiopathogenesis, prevalence, andsignificance. Vet Clin North Amer Small Anim Pract 1998;28:1111e28.
[10] Giannobile WV, Rd Finkelman, Lynch SE. Comparison of canine and non-human primate animal models for periodontal regenerative therapy: resultsfollowing a single administration of PDGF/IGF-I. J Periodontol 1994;65:1158e68.
Please cite this article in press as: Carlo Reis EC, et al., Periodontal rBiomaterials (2011), doi:10.1016/j.biomaterials.2011.08.040
[11] Weinberg MA, Bral M. Laboratory animal models in periodontology. J ClinPeriodontol 1999;26:335e40.
[12] Hull PS, Soames JV, Davies RM. Periodontal disease in a beagle dog colony.J Comp Path V 1974;84:143e50.
[13] Kortegaard HE, Eriksen T, Baelum V. Periodontal disease in research beagledogs e an epidemiological study. J Small Anim Pract 2008;49:610e6.
[14] Pavlica Z, Petelin M, Juntes P, Erzen D, Crossley DA. Periodontal disease burdenand pathological changes in organs of dogs. J Vet Dent 2008;25:97e105.
[15] Debowe Lj, Mosier D, Logan E, Harvey CE, Lowry S, Richardson DC. Associationof periodontal disease and histological lesions in multiple organs from 45dogs. J Vet Dent 1996;13:57e60.
[16] Nahás D, Martins LF, Passanezi E, Janson WA, Riveiro MC, Alves ME. Peri-odontal regeneration after autogenous grafting of cancellous bone tissue andmarrow material in dogs. Estomatol Cult 1974;8:287e95.
[17] Araújo MG, Lindhe J. GTR treatment of degree III furcation defects followingapplication of enamel matrix proteins. An experimental study in dogs. J ClinPeriodontol 1998;25:524e30.
[18] Bosshardt DD, Sculean A. Does periodontal tissue regeneration really work?Periodontol 2000;2009(51):208e19.
[19] Pretzl B, Kim TS, Steinbrenner H, Dörfer C, Himmer K, Eickholz P. Guidedtissue regeneration with bioabsorbable barriers III 10-year results in infrab-ony defects. J Clin Periodontol 2009;36:349e56.
[20] Caffesse RG, Smith BA, Duff B, Morrison EC, Merrill D, Becker W. Class IIfurcations treated by guided tissue regeneration in humans: case reports.J Periodontol 1990;61:510e4.
[21] Camargo PM, Lekovic V, Weinlaender M, Vasilic N, Madzarevic M, Kenney EB.Platelet-rich plasma and bovine porous bone mineral combined with guidedtissue regeneration in the treatment of intrabony defects in humans.J PeriodRes 2002;37:300e6.
[22] Becker W, Becker B. Clinical applications of guided tissue regeneration:surgical considerations. Periodontol 2000;1993(1):46e53.
[23] Marreta SM. Recognition and Treatment of Periodontal Disease. Proceedingsof the Atlantic Coast Veterinary Conference; 2001 Oct 9-11; New Jersey; 2001.
[24] Niemiec BA. Periodontal therapy. Top Companion Anim Med 2008;23:81e90.[25] Hale FA. Management of bilateral, pathologic, mandibular fractures in a dog.
J Vet Dent 2002;19:22e4.[26] Watanabe K, Kikuchi M, Okumura M, Kadosawa T, Fujinaga T. Efficacy of
enamel matrix protein applied to spontaneous periodontal disease in twodogs. J Vet Med Sci 2003;65:1007e10.
[27] Smith MM. Treatment of a mandibular periodontal interproximal defect witha bone graft in a dog. J Vet Dent 1995;12:59e62.
[28] DeForge DH. Evaluation of bioglass/perioglas� (consil�) synthetic bone graftparticulate in the dog and cat. J Vet Dent 1997;14:141e5.
[29] Shoukry M, Ali LB, Naby MA, Soliman A. Periodontal repair of experimentalplaque-induced periodontal disease in dogs. J Vet Dent 2007;24:152e65.
[30] Roriz VM, Souza SLS, Taba Jr M, Palioto DB, Grisi MFM. Treatment of class IIIfurcation defects with expanded polytetrafluoroethylenemembrane associatedor not with anorganic bone matrix/synthetic cell-binding peptide: a histologicand histomorphometric study in dogs. J Periodontol 2006;77:490e7.
[31] Cirelli JA, Marcatnonio Jr E, Marcantonio RAC, Lia RCC, Gaissis G, Rossa Jr C.Evaluation of anionic collagen membranes in the treatment of class II furca-tion lesions: an histometric analysis in dogs. Biomaterials 1997;18:1227e34.
[32] DeVicente JC, Recio O, Martin-Villa L, Junquera LM, López-Arranz JS. Histo-morphometric evaluation of guided bone regeneration around implants withSLA surface: an experimental study in beagle dogs. Int J Oral Maxil Surg 2006;35:1047e53.
[33] Carlo EC, Borges APB, Fófano G, Fontes EB, Carvalho TB, Sena MPT. Técnica daregeneração tecidual guiada (RTG) na reparação da mandíbula de cão. RevCeres 2006;53:350e6.
[34] Amano Y, Ota M, Sekiguchi K, Shibukawa Y, Yamada S. Evaluation of a poly-lactic acid membrane and membrane fixing pin for guided tissue regenera-tion on bone defects in dogs. Oral Surg Oral Med Oral Pathol Oral RadiolEndod 2004;97:155e63.
[35] Chang CY, Yamada S. Evaluation of the regenerative effect of a 25%doxycycline-loaded biodegradable membrane for guided tissue regeneration.J Periodontol 2000;71:1086e93.
[36] Owen GRH, Jackson J, Chehroudi B, Burt H, Brunette DM. A PLGA membranecontrolling cell behaviour for promoting tissue regeneration. Biomaterials2005;26:7447e56.
[37] Owen GRH, Jackson JK, Chehroudi B, Brunette DM, Burt H. An in vitro study ofplasticized poly(lactic-co-glycolic acid) films as possible guided tissueregeneration membranes: material properties and drug release kinetics.J Biomed Mater Res A 2010;95:857e69.
[38] Liao S, Wang W, Uo M, Ohkawa S, Akasaka T, Tamur K, et al. A three-layerednano-carbonated hydroxyapatite /collagen /PLGA composite membrane forguided tissue regeneration. Biomaterials 2005;26:7564e71.
[39] Lickorish D, Guan L, Davies JE. A three-phase, fully resorbable, polyester/calcium phosphate scaffold for bone tissue engineering: evolution of scaffolddesign. Biomaterials 2007;28:1495e502.
[40] Guan L, Davies JE. Preparation and characterization of a highly macroporousbiodegradable composite tissue engineering scaffold. J Biomed Mater Res2004;71A:480e7.
[41] Davies JE, Matta R, Mendes VC. Perri de Carvalho PS. Development, charac-terization and clinical use of a biodegradable composite scaffold for boneengineering in oro-maxillo-facial surgery. Organogenesis 2010;6:161e6.
egeneration using a bilayered PLGA/calcium phosphate construct,

E.C. Carlo Reis et al. / Biomaterials xxx (2011) 1e1010
[42] Harris RJ. Treatment of furcation defects with an allograft-alloplast-tetracycline composite bone graft combined with GTR: human histologicevaluation of a case report. Int J Periodontics Restorative Dent 2002;22:381e7.
[43] Keles GC, Cetinkaya BO, Baris S, Albayrak D, Simsek SB. Comparison of plateletpellet with or without guided tissue regeneration in the treatment of class IIfurcation defects in dogs. Clin Oral Invest 2009;13:393e400.
[44] Robert PM, Frank RM. Periodontal guided tissue regeneration with a newresorbable polylactic acid membrane. J Periodontol 1994;65:414e22.
[45] Murakami S, Takayama S, Kitamura M, Shimabukuro Y, Yanagi K, Ikezawa K,et al. Recombinant human basic fibroblast growth factor (bFGF) stimulatesperiodontal regeneration in class II furcation defects created in beagle dogs.J Periodont Res 2003;38:97e103.
[46] Wikesjö UME, Lim WH, Thomson RC, Cook AD, Wozney JM, Hardwich WR.Periodontal repair in dogs: evaluation of a bioabsorbable space-providingmacro-porous membrane with recombinant human bone morphogeneticprotein-2. J Periodontol 2003;74:635e47.
[47] Wikesjö UM, Sigurdsson TJ, Lee MB, Tatakis DN, Selvig KA. Dynamics of woundhealing in periodontal regenerative therapy. J Calif Dent Assoc 1995;23:30e5.
[48] Mardas N, Kostopoulos L, Stavropoulos A, Karring T. Evaluation of a cell-permeable barrier for guided tissue regeneration combined with demineral-ized bone matrix. Clin Oral Implants Res 2003;14:812e8.
[49] Araújo MG, Berglundh T, Lindhe J. On the dynamics of periodontal tissueformation in degree III furcation defects. An experimental study in dogs. J ClinPeriodontol 1997;24:738e46.
[50] OpreaWE, Karp JM, Hosseini MM, Davies JE. Effect of platelet releasate on bonecell migration and recruitment in vitro. J Craniofac Surg 2003;14:292e300.
[51] Davies JE. Understanding peri-implant endosseous healing. J Dent Educat2003;67:932e49.
[52] Kikuchi L, Park JY, Victor C, Davies JE. Platelet interactions with calcium-phosphate-coated surfaces. Biomaterials 2005;26:5285e95.
[53] Cho WJ, Kim JH, Oh SH, Nam HE, Kim JM, Lee JH. Hydrophilized poly-caprolactone nanofiber mesh-embedded poly(glycolic-co-llactic) membranefor effective guided bone regeneration. J Biomed Mater Res 2009;91A:400e7.
Please cite this article in press as: Carlo Reis EC, et al., Periodontal rBiomaterials (2011), doi:10.1016/j.biomaterials.2011.08.040
[54] McCulloch CA. Progenitor cell populations in the periodontal ligament ofmice. Anat Rec 1985;211:258e62.
[55] Sarugaser R, Ennis J, Sanford WL, Davies JE. Isolation, propagation, and char-acterization of human umbilical Cord perivascular cells (HUCPVCs). MethodsMol Biol 2009;482:269e79.
[56] Lawrence BJ, Maase EL, Lin HK, Madihally SV. Multilayer composite scaffoldswith mechanical properties similar to small intestinal submucosa. J BiomedMater Res 2009;88A:634e43.
[57] Inanç B, Arslan E, Seker S, Elçin AE, Elçin YM. Periodontal ligament cellularstructures engineered with electrospun poly(DL-lactide-co-glycolide) nano-fibrous membrane scaffolds. J Biomed Mater Res 2009;90A:186e95.
[58] Kim EJ, Yoon SJ, Yeo GD, Pai CM, Kang IK. Preparation of biodegradable PLA/PLGA membrane with PGA mesh and their application for periodontal guidedtissue regeneration. Biomed Mater 2009;4:055001.
[59] Park JK, Yeon J, Oh EJ, Reddy M, Kim JY, Cho DW, et al. Guided bone regen-eration by poly(lactic-co-glycolic acid) grafted hyalyronic acid bi-layer filmsfor periodontal barrier application. Acta Biomater 2009;5:3394e403.
[60] Santana RB, Mattos CML, Van Dyke T. Efficacy of combined Regenerative-Treatments in human MandibularClass II furcation defects. J Periodontol2009;80:1756e64.
[61] Kurtis B, Ünsal B, Çetiner D, Gültekin E, Özcan G, Çelebi N, et al. Effect ofpolylactide/glycolide (PLGA) membranes loaded with metronidazole onperiodontal regeneration following guided tissue regeneration in dogs.J Periodontol 2002;73:694e700.
[62] Deliberador TM, Nagata MJH, Furlaneto FAC, Melo LGN, Okamoto T,Sundefekd MLMM, et al. Autogenous bone graft with or without a calciumsulfate barrier in the treatment of class II furcation defects: a histologic andhistometric study in dogs. J Periodontol 2006;77:780e9.
[63] Lyons LC, Weltman RL, Moretti AJ, Trejo PM. Regeneration of degree IIfurcation defects with a 4% doxycycline hyclate bioabsorbable barrier.J Periodontol 2008;79:72e9.
[64] Pradeep AR, Pai S, Garg G, Devi P, Shetty SK. A randomized clinical trial ofautologous platelet-rich plasma in the treatment of mandibular degree IIfurcation defects. J Clin Periodontol 2009;36:581e8.
egeneration using a bilayered PLGA/calcium phosphate construct,
Copyright © 2022 FDOKUMEN




















