
Necrotizing stomatitis: a possible periodontal manifestation of deferiprone-induced agranulocytosis
7
Necrotizing stomatitis: a possible periodontal manifestation of deferiprone-induced agranulocytosis Shikha Tewari, BDS, MDS, a Sanjay Tewari, BDS, MDS, b Rajinder K. Sharma, BDS, MDS, c Pankaj Abrol, MD, d and Rajeev Sen, MD, e Rohtak, India GOVERNMENT DENTAL COLLEGE, PT. B. D. SHARMA POST GRADUATE INSTITUTE OF MEDICAL SCIENCES Thalassemia major is a rare inherited anemia, and affected children require blood transfusions every 2-4 weeks to survive. Repeated blood transfusions lead to a build-up of toxic levels of iron in the body, causing organ damage and premature death, primarily due to iron-induced heart disease. Deferiprone is one of a few drugs that are routinely used in medicine for the treatment of iron overload in thalassemic patients. This drug is usually administered daily at high doses (50-100 mg/kg) with a very low toxicity. Agranulocytosis is the most serious side effect of deferiprone, with a reported incidence of 0.6 per 100 patient-years. We document an illustrated case report of necrotizing gingivostomatitis, an oral manifestation of agranulocytosis secondary to deferiprone use involving the gingiva and palatal mucosa of a thalassemia major patient. Various causes of precipitation of agranulocytosis in these patients and a possible relationship of necrotizing gingivostomatitis with deferiprone are highlighted in this case report. (Oral Surg Oral Med Oral Pathol Oral Radiol Endod 2009;108:e13-e19) Thalassemia is single-gene autosomal disorder caused by genetic mutation and is one of the most challenging forms of hematologic disorders. 1,2 Patients require reg- ular packed red cell infusion as the most effective measure for prolonging life. However, the subtle im- balance of iron homeostasis in thalassemia major often results in accumulation of iron, leading to toxic damage to vital organs with severe life-threatening consequences. 3 Chelation therapy with an iron-binding agent is needed in such patients to increase life expect- ancy and prevent death from iron-mediated organ in- jury. As of today, there are 3 leading iron chelators available commercially: deferiprone, desferrioxamine, and deferasirox. In India and other Asian countries, deferiprone (also known as L1, CP20, Ferriprox, and Kelfer) is the most frequently used oral iron chelator, because of its better compliance and cost-effectiveness, relatively low toxicity, and superiority over other ch- elators in the removal of iron from specific target or- gans, such as heart and liver. 4,5 Deferiprone is now licensed in 50 countries. 6 The toxic side effects of deferiprone during clinical use in thousands of patients in the last 16 years at doses of 50-150 mg/kg/day are mainly: 1) transient agranu- locytosis in 0.6%; 2) neutropenia in 6%; 3) arthrop- athy (musculoskeletal and joint pains) in 16%; 4) gastric intolerance in 6%; and 5) zinc deficiency in 1%. 6,7 Agranulocytosis remains the major concern of patients receiving deferiprone. Safety trial studies showed that this complication occurs in 1% of pa- tients (incidence of 0.6 per 100 patient-years) who undergo weekly monitoring of their blood counts dur- ing chelation therapy with deferiprone. 8,9 Milder neu- tropenia (500-1500/L) is more common, occurring in 8% of patients. Results of another safety trial study showed the incidences of agranulocytosis and neutro- penia at 0.43 and 2.08 per 100 patient-years, respec- tively, among 532 patients with thalassemia major. 10 The incidences in these large trials are similar to those of combined data based on earlier studies carried out in several centers. 11,12 A few fatal cases of agranulocyto- sis have also been reported involving patients not ad- hering to the mandatory blood counts. 13 Although re- ported deaths related to agranulocytosis are extremely rare, the severely depressed neutrophil count, even though reversible, clearly represents a significant risk for sepsis which, therefore, leads to hospitalization and, in some cases, administration of granulocyte colony– stimulating factor (G-CSF). 13,14 The present manuscript describes a case report of deferiprone-induced neutropenia in a thalassemia pa- tient that led to severe necrotizing gingivostomatitis. Usually the drug-induced adverse oral reactions are a Professor, Department Of Periodontics. b Senior Professor, Department of Conservative Dentistry and End- odontics. c Professor, Department Of Periodontics. d Professor, Department of Pediatrics. e Senior Professor, Department of Pathology. Received for publication May 2, 2009; returned for revision Jun 23, 2009; accepted for publication Jun 27, 2009. 1079-2104/$ - see front matter © 2009 Published by Mosby, Inc. doi:10.1016/j.tripleo.2009.06.021 e13
Transcript of Necrotizing stomatitis: a possible periodontal manifestation of deferiprone-induced agranulocytosis

Necrotizing stomatitis: a possible periodontal manifestation ofdeferiprone-induced agranulocytosisShikha Tewari, BDS, MDS,a Sanjay Tewari, BDS, MDS,b Rajinder K. Sharma, BDS, MDS,c
Pankaj Abrol, MD,d and Rajeev Sen, MD,e Rohtak, IndiaGOVERNMENT DENTAL COLLEGE, PT. B. D. SHARMA POST GRADUATE INSTITUTE OF MEDICALSCIENCES
Thalassemia major is a rare inherited anemia, and affected children require blood transfusions every 2-4weeks to survive. Repeated blood transfusions lead to a build-up of toxic levels of iron in the body, causing organdamage and premature death, primarily due to iron-induced heart disease. Deferiprone is one of a few drugs that areroutinely used in medicine for the treatment of iron overload in thalassemic patients. This drug is usually administereddaily at high doses (50-100 mg/kg) with a very low toxicity. Agranulocytosis is the most serious side effect ofdeferiprone, with a reported incidence of 0.6 per 100 patient-years. We document an illustrated case report ofnecrotizing gingivostomatitis, an oral manifestation of agranulocytosis secondary to deferiprone use involving thegingiva and palatal mucosa of a thalassemia major patient. Various causes of precipitation of agranulocytosis in thesepatients and a possible relationship of necrotizing gingivostomatitis with deferiprone are highlighted in this case report.
(Oral Surg Oral Med Oral Pathol Oral Radiol Endod 2009;108:e13-e19)Thalassemia is single-gene autosomal disorder causedby genetic mutation and is one of the most challengingforms of hematologic disorders.1,2 Patients require reg-ular packed red cell infusion as the most effectivemeasure for prolonging life. However, the subtle im-balance of iron homeostasis in thalassemia majoroften results in accumulation of iron, leading to toxicdamage to vital organs with severe life-threateningconsequences.3 Chelation therapy with an iron-bindingagent is needed in such patients to increase life expect-ancy and prevent death from iron-mediated organ in-jury. As of today, there are 3 leading iron chelatorsavailable commercially: deferiprone, desferrioxamine,and deferasirox. In India and other Asian countries,deferiprone (also known as L1, CP20, Ferriprox, andKelfer) is the most frequently used oral iron chelator,because of its better compliance and cost-effectiveness,relatively low toxicity, and superiority over other ch-elators in the removal of iron from specific target or-gans, such as heart and liver.4,5 Deferiprone is nowlicensed in �50 countries.6
aProfessor, Department Of Periodontics.bSenior Professor, Department of Conservative Dentistry and End-odontics.cProfessor, Department Of Periodontics.dProfessor, Department of Pediatrics.eSenior Professor, Department of Pathology.Received for publication May 2, 2009; returned for revision Jun 23,2009; accepted for publication Jun 27, 2009.1079-2104/$ - see front matter© 2009 Published by Mosby, Inc.
doi:10.1016/j.tripleo.2009.06.021The toxic side effects of deferiprone during clinicaluse in thousands of patients in the last 16 years at dosesof 50-150 mg/kg/day are mainly: 1) transient agranu-locytosis in 0.6%; 2) neutropenia in �6%; 3) arthrop-athy (musculoskeletal and joint pains) in �16%; 4)gastric intolerance in �6%; and 5) zinc deficiency in1%.6,7 Agranulocytosis remains the major concern ofpatients receiving deferiprone. Safety trial studiesshowed that this complication occurs in �1% of pa-tients (incidence of 0.6 per 100 patient-years) whoundergo weekly monitoring of their blood counts dur-ing chelation therapy with deferiprone.8,9 Milder neu-tropenia (500-1500/�L) is more common, occurring in�8% of patients. Results of another safety trial studyshowed the incidences of agranulocytosis and neutro-penia at 0.43 and 2.08 per 100 patient-years, respec-tively, among 532 patients with thalassemia major.10
The incidences in these large trials are similar to thoseof combined data based on earlier studies carried out inseveral centers.11,12 A few fatal cases of agranulocyto-sis have also been reported involving patients not ad-hering to the mandatory blood counts.13 Although re-ported deaths related to agranulocytosis are extremelyrare, the severely depressed neutrophil count, eventhough reversible, clearly represents a significant riskfor sepsis which, therefore, leads to hospitalization and,in some cases, administration of granulocyte colony–stimulating factor (G-CSF).13,14
The present manuscript describes a case report ofdeferiprone-induced neutropenia in a thalassemia pa-tient that led to severe necrotizing gingivostomatitis.
Usually the drug-induced adverse oral reactions aree13
OOOOEe14 Tewari et al. October 2009
manifested in the form of vesiculobullous vesiculoul-cerative mucositis, osteonecrosis of the jaws, lichenoiddrug reactions, erythema multiforme, pemphigoid andlupus erythematosus–like reactions, and aphthous sto-matitis.
This is the first case of deferiprone-associated agran-ulocytosis in which the oral manifestations presented aswidespread necrosis of attached gingiva and palatalmucosa with absence of inflammation.
CASE REPORTA 14-year-old male thalassemia patient was referred to the
postgraduate department of Periodontics, Government DentalCollege Rohtak in November 2003. The patient was hospi-talized in the department of Pediatrics, Pt. B. D. Sharma PostGraduate Institute of Medical Sciences, Rohtak, Haryana,India, for high-grade fever, malaise and generalized weak-ness, loss of appetite, lymphadenopathy, and dysphagia. Onthe third day of hospitalization, remarkable changes devel-oped in the oral cavity of the patient. There was grayish-whitediscoloration of maxillary and mandibular gingiva with se-vere pain in the teeth. The medical history revealed that thepatient was diagnosed with �-thalassemia major at the age of6 months. Since then, he was on regular blood transfusiontherapy that was given every 2-3 weeks. The patient had beentaking the oral iron chelator drug deferiprone at the dose of 75mg/kg/day for last 3 years. There was no history of a newdrug being used or recent change in medication at the time ofhospitalization. The extraoral physical examination showedextreme pallor, bilateral submandibular lymphadenopathy,and splenomegaly. Intraoral examination revealed strikinglyobvious clinical presentation of grayish-white wide surfacenecrosis of the gingivae with no overt signs of inflammation,
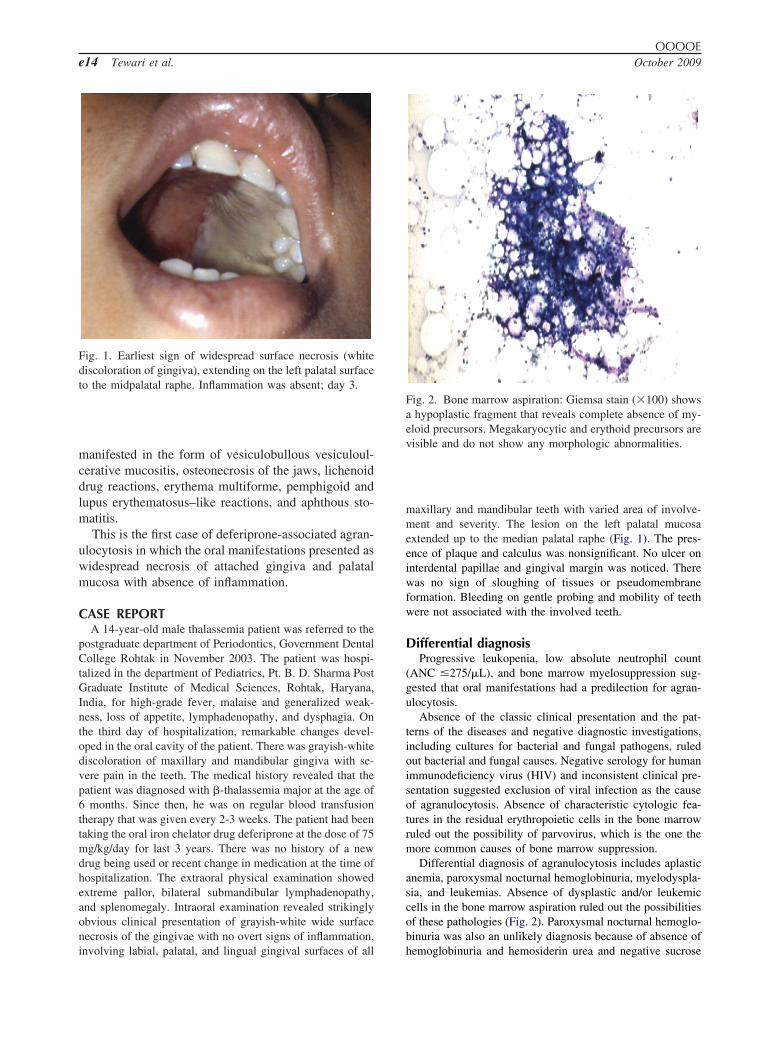
Fig. 1. Earliest sign of widespread surface necrosis (whitediscoloration of gingiva), extending on the left palatal surfaceto the midpalatal raphe. Inflammation was absent; day 3.
involving labial, palatal, and lingual gingival surfaces of all
maxillary and mandibular teeth with varied area of involve-ment and severity. The lesion on the left palatal mucosaextended up to the median palatal raphe (Fig. 1). The pres-ence of plaque and calculus was nonsignificant. No ulcer oninterdental papillae and gingival margin was noticed. Therewas no sign of sloughing of tissues or pseudomembraneformation. Bleeding on gentle probing and mobility of teethwere not associated with the involved teeth.
Differential diagnosisProgressive leukopenia, low absolute neutrophil count
(ANC �275/�L), and bone marrow myelosuppression sug-gested that oral manifestations had a predilection for agran-ulocytosis.
Absence of the classic clinical presentation and the pat-terns of the diseases and negative diagnostic investigations,including cultures for bacterial and fungal pathogens, ruledout bacterial and fungal causes. Negative serology for humanimmunodeficiency virus (HIV) and inconsistent clinical pre-sentation suggested exclusion of viral infection as the causeof agranulocytosis. Absence of characteristic cytologic fea-tures in the residual erythropoietic cells in the bone marrowruled out the possibility of parvovirus, which is the one themore common causes of bone marrow suppression.
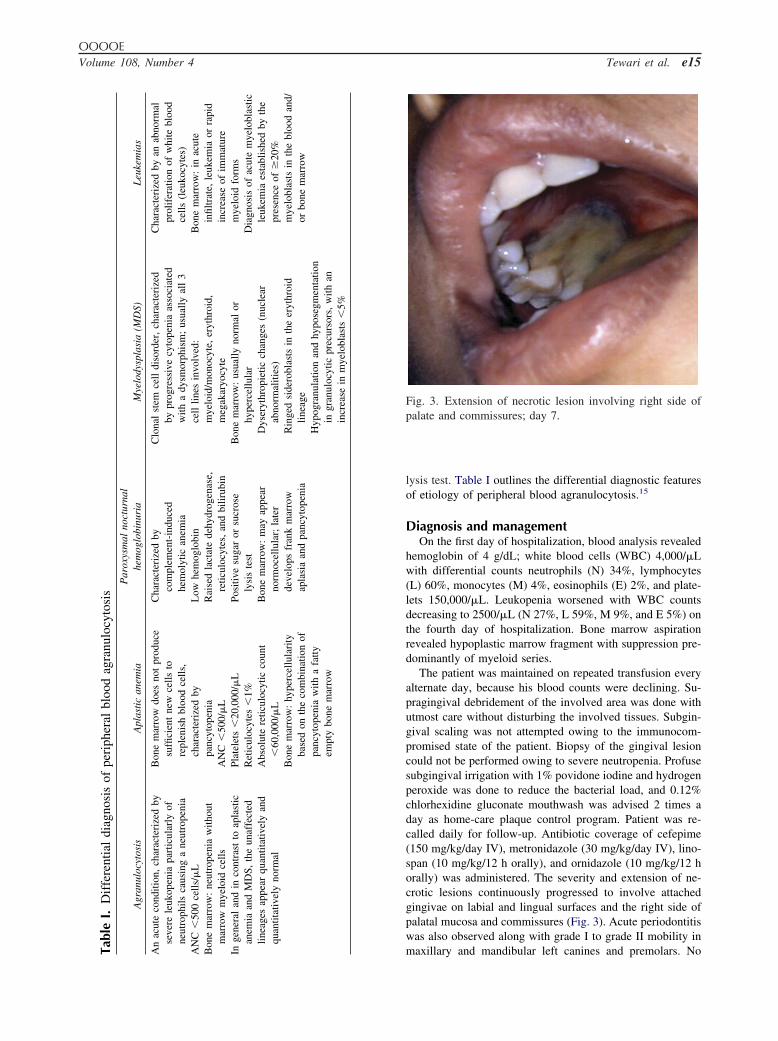
Differential diagnosis of agranulocytosis includes aplasticanemia, paroxysmal nocturnal hemoglobinuria, myelodyspla-sia, and leukemias. Absence of dysplastic and/or leukemiccells in the bone marrow aspiration ruled out the possibilitiesof these pathologies (Fig. 2). Paroxysmal nocturnal hemoglo-binuria was also an unlikely diagnosis because of absence of
Fig. 2. Bone marrow aspiration: Giemsa stain (�100) showsa hypoplastic fragment that reveals complete absence of my-eloid precursors. Megakaryocytic and erythoid precursors arevisible and do not show any morphologic abnormalities.
hemoglobinuria and hemosiderin urea and negative sucrose
ble
I.D
iffe
rent
ial
diag
nosi
sof
peri
pher
albl
ood
agra
nulo
cyto
sis
Agr
anul
ocyt
osis
Apl
asti
can
emia
Par
oxys
mal
noct
urna
lhe
mog
lobi
nuri
aM
yelo
dysp
lasi
a(M
DS)
Leu
kem
ias
acut
eco
nditi
on,
char
acte
rize
dby
ever
ele
ukop
enia
part
icul
arly
ofeu
trop
hils
caus
ing
ane
utro
peni
aC
�50
0ce
lls/�
Lne
mar
row
:ne
utro
peni
aw
ithou
tar
row
mye
loid
cells
gene
ral
and
inco
ntra
stto
apla
stic
nem
iaan
dM
DS,
the
unaf
fect
edin
eage
sap
pear
quan
titat
ivel
yan
dua
ntita
tivel
yno
rmal
Bon
em
arro
wdo
esno
tpr
oduc
esu
ffici
ent
new
cells
tore
plen
ish
bloo
dce
lls,
char
acte
rize
dby
panc
ytop
enia
AN
C�
500/
�L
Plat
elet
s�
20,0
00/�
LR
etic
uloc
ytes
�1%
Abs
olut
ere
ticul
ocyt
icco
unt
�60
,000
/�L
Bon
em
arro
w:
hype
rcel
lula
rity
base
don
the
com
bina
tion
ofpa
ncyt
open
iaw
itha
fatty
empt
ybo
nem
arro
w
Cha
ract
eriz
edby
com
plem
ent-
indu
ced
hem
olyt
ican
emia
Low
hem
oglo
bin
Rai
sed
lact
ate
dehy
drog
enas
e,re
ticul
ocyt
es,
and
bilir
ubin
Posi
tive
suga
ror
sucr
ose
lysi
ste
stB
one
mar
row
:m
ayap
pear
norm
ocel
lula
r;la
ter
deve
lops
fran
km
arro
wap
lasi
aan
dpa
ncyt
open
ia
Clo
nal
stem
cell
diso
rder
,ch
arac
teri
zed
bypr
ogre
ssiv
ecy
tope
nia
asso
ciat
edw
itha
dysm
orph
ism
;us
ually
all
3ce
lllin
esin
volv
ed:
mye
loid
/mon
ocyt
e,er
ythr
oid,
meg
akar
yocy
teB
one
mar
row
:us
ually
norm
alor
hype
rcel
lula
rD
yser
ythr
opie
ticch
ange
s(n
ucle
arab
norm
aliti
es)
Rin
ged
side
robl
asts
inth
eer
ythr
oid
linea
geH
ypog
ranu
latio
nan
dhy
pose
gmen
tatio
nin
gran
uloc
ytic
prec
urso
rs,
with
anin
crea
sein
mye
lobl
asts
�5%
Cha
ract
eriz
edby
anab
norm
alpr
olif
erat
ion
ofw
hite
bloo
dce
lls(l
euko
cyte
s)B
one
mar
row
:in
acut
ein
filtr
ate,
leuk
emia
orra
pid
incr
ease
ofim
mat
ure
mye
loid
form
sD
iagn
osis
ofac
ute
mye
lobl
astic
leuk
emia
esta
blis
hed
byth
epr
esen
ceof
�20
%m
yelo
blas
tsin
the
bloo
dan
d/or
bone
mar
row
OOOOEVolume 108, Number 4 Tewari et al. e15
lysis test. Table I outlines the differential diagnostic featuresof etiology of peripheral blood agranulocytosis.15
Diagnosis and managementOn the first day of hospitalization, blood analysis revealed
hemoglobin of 4 g/dL; white blood cells (WBC) 4,000/�Lwith differential counts neutrophils (N) 34%, lymphocytes(L) 60%, monocytes (M) 4%, eosinophils (E) 2%, and plate-lets 150,000/�L. Leukopenia worsened with WBC countsdecreasing to 2500/�L (N 27%, L 59%, M 9%, and E 5%) onthe fourth day of hospitalization. Bone marrow aspirationrevealed hypoplastic marrow fragment with suppression pre-dominantly of myeloid series.
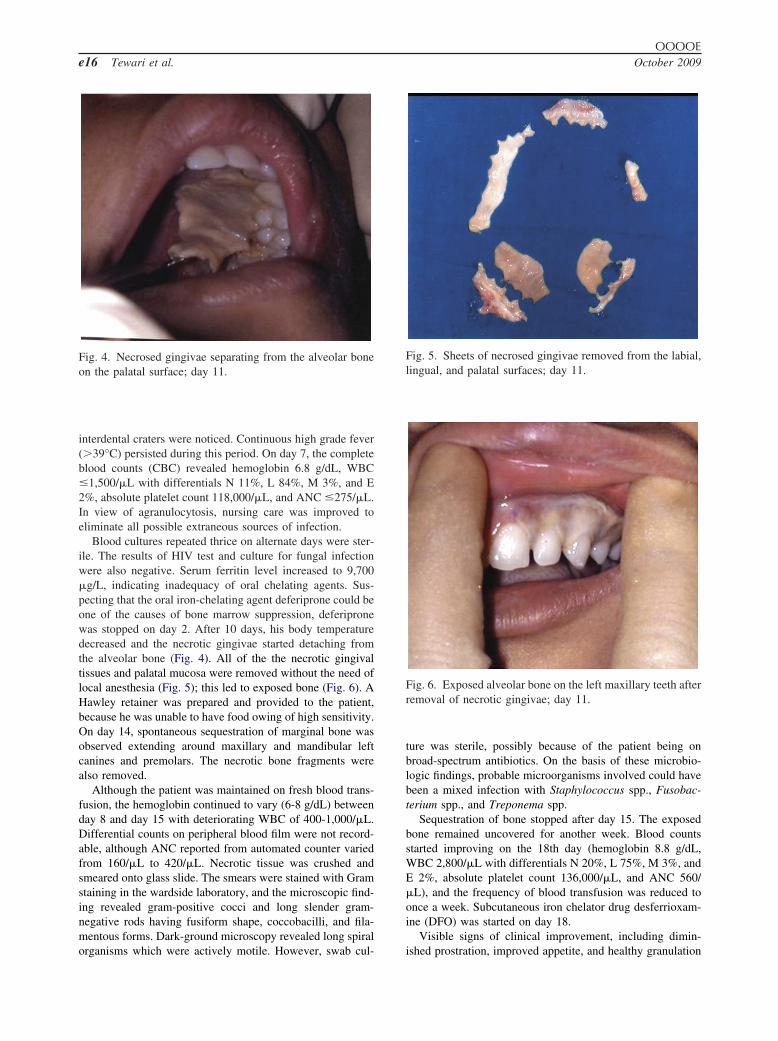
The patient was maintained on repeated transfusion everyalternate day, because his blood counts were declining. Su-pragingival debridement of the involved area was done withutmost care without disturbing the involved tissues. Subgin-gival scaling was not attempted owing to the immunocom-promised state of the patient. Biopsy of the gingival lesioncould not be performed owing to severe neutropenia. Profusesubgingival irrigation with 1% povidone iodine and hydrogenperoxide was done to reduce the bacterial load, and 0.12%chlorhexidine gluconate mouthwash was advised 2 times aday as home-care plaque control program. Patient was re-called daily for follow-up. Antibiotic coverage of cefepime(150 mg/kg/day IV), metronidazole (30 mg/kg/day IV), lino-span (10 mg/kg/12 h orally), and ornidazole (10 mg/kg/12 horally) was administered. The severity and extension of ne-crotic lesions continuously progressed to involve attachedgingivae on labial and lingual surfaces and the right side ofpalatal mucosa and commissures (Fig. 3). Acute periodontitiswas also observed along with grade I to grade II mobility in
Fig. 3. Extension of necrotic lesion involving right side ofpalate and commissures; day 7.
maxillary and mandibular left canines and premolars. NoTa An s n
AN
Bo m
Ina l q
OOOOEe16 Tewari et al. October 2009
interdental craters were noticed. Continuous high grade fever(�39°C) persisted during this period. On day 7, the completeblood counts (CBC) revealed hemoglobin 6.8 g/dL, WBC�1,500/�L with differentials N 11%, L 84%, M 3%, and E2%, absolute platelet count 118,000/�L, and ANC �275/�L.In view of agranulocytosis, nursing care was improved toeliminate all possible extraneous sources of infection.
Blood cultures repeated thrice on alternate days were ster-ile. The results of HIV test and culture for fungal infectionwere also negative. Serum ferritin level increased to 9,700�g/L, indicating inadequacy of oral chelating agents. Sus-pecting that the oral iron-chelating agent deferiprone could beone of the causes of bone marrow suppression, deferipronewas stopped on day 2. After 10 days, his body temperaturedecreased and the necrotic gingivae started detaching fromthe alveolar bone (Fig. 4). All of the the necrotic gingivaltissues and palatal mucosa were removed without the need oflocal anesthesia (Fig. 5); this led to exposed bone (Fig. 6). AHawley retainer was prepared and provided to the patient,because he was unable to have food owing of high sensitivity.On day 14, spontaneous sequestration of marginal bone wasobserved extending around maxillary and mandibular leftcanines and premolars. The necrotic bone fragments werealso removed.
Although the patient was maintained on fresh blood trans-fusion, the hemoglobin continued to vary (6-8 g/dL) betweenday 8 and day 15 with deteriorating WBC of 400-1,000/�L.Differential counts on peripheral blood film were not record-able, although ANC reported from automated counter variedfrom 160/�L to 420/�L. Necrotic tissue was crushed andsmeared onto glass slide. The smears were stained with Gramstaining in the wardside laboratory, and the microscopic find-ing revealed gram-positive cocci and long slender gram-negative rods having fusiform shape, coccobacilli, and fila-mentous forms. Dark-ground microscopy revealed long spiral
Fig. 4. Necrosed gingivae separating from the alveolar boneon the palatal surface; day 11.
organisms which were actively motile. However, swab cul-
ture was sterile, possibly because of the patient being onbroad-spectrum antibiotics. On the basis of these microbio-logic findings, probable microorganisms involved could havebeen a mixed infection with Staphylococcus spp., Fusobac-terium spp., and Treponema spp.
Sequestration of bone stopped after day 15. The exposedbone remained uncovered for another week. Blood countsstarted improving on the 18th day (hemoglobin 8.8 g/dL,WBC 2,800/�L with differentials N 20%, L 75%, M 3%, andE 2%, absolute platelet count 136,000/�L, and ANC 560/�L), and the frequency of blood transfusion was reduced toonce a week. Subcutaneous iron chelator drug desferrioxam-ine (DFO) was started on day 18.
Visible signs of clinical improvement, including dimin-
Fig. 5. Sheets of necrosed gingivae removed from the labial,lingual, and palatal surfaces; day 11.
Fig. 6. Exposed alveolar bone on the left maxillary teeth afterremoval of necrotic gingivae; day 11.
ished prostration, improved appetite, and healthy granulation

OOOOEVolume 108, Number 4 Tewari et al. e17
tissue on the exposed bone, were observed by early week 4.At the completion of 1 month, blood transfusions were main-tained at fortnight intervals, because hemoglobin level hadimproved to 11 g/dL and white blood cell and platelet countswere recorded in midnormal range. The patient was dis-charged from the hospital and instructed to report every weekfor follow up. Substantial regeneration of lost periodontaltissue was observed within 2 months.
DISCUSSIONAgranulocytosis, or severe neutropenia, is not a dis-
ease but a sign of an underlying disorder; it has a widerange of underlying causes. Decreased production ofneutrophils is associated with deficiencies of vitaminB12 and folic acid, aplastic anemia, tumors (leukemia,solid tumors that invade bone marrow), drugs, meta-bolic diseases (glycogen storage disease type 1b,methylomalonic acidaemia), nutritional deficiencies(malnutrition, copper deficiency, megaloblastic anemiasecondary to folate or vitamin B), radiation injury,immune mechanisms, and heritable genetic aberrations(congenital neutropenia, cyclic neutropenia). Certaininfections decrease the number of neutrophils in thecirculating blood because of increased migration ofneutrophils into the tissue, sequestration of neutrophils,or direct toxic effect of the microorganism and itstoxins on the bone marrow.16 Infections with viruses,particularly hepatitis A, HIV-1, and Epstein-Barr virus,are associated with neutropenia, and overwhelmingbacterial infection, particularly septicemia, can be ac-companied by neutropenia because the cells are used ata rapid rate to overcome the infection. Cyclic neutro-penia is a rare hematologic disorder, characterized byrepetitive episodes of fever, mouth ulcers, and infec-tions attributable to recurrent severe neutropenia(�200/�L) with a regular periodicity of 21 days,persisting for 3-5 days.17 Acquired agranulocytosis/neutropenia is far more common than congenital forms,often accompanying viral infection, or it may be attribut-able to drugs in �70% of cases,18 which is a rare andpotentially life-threatening condition, owing to either my-elosuppression or antibody-mediated destruction. Drugsassociated with agranulocytosis include antiepileptics,antithyroid drugs (carbimazole, methimazole, and propy-lthiouracil), antibiotics (penicillin, chloramphenicol, andcotrimoxazole), cytotoxic drugs, gold, nonsteroidal an-tiinflammatory drugs (indomethacin, naproxen, andphenylbutazone), mebendazole, the antidepressant mir-tazapine, and some antipsychotics (the atypical antipsy-chotic clozapine).19
Severe neutropenia has been implicated in the etiol-ogy of atypical oral ulcerations, destructive periodontaldisease, alveolar bone loss, acute ulcerative gingivitis,and oral mucosal infections.20-23 It may place patients
at increased risk of fevers, bacteremia, and bacterialinfections at any bacteria-laden or exposed area of thebody. Both indigenous oral flora and hospital-acquiredpathogens have been associated with bacteremias andsystemic infection.24 Necrotizing gingivostomatitis isan acute opportunistic infection of the gingiva. Trepo-nema spp., Selenomonas spp., Prevotella intermedia,Borrelias, gram-positive cocci, and �-hemolytic Strep-tococcus from group B have been shown to be signif-icant bacteria in the pathogenesis of this condition.25,26
Inflammatory signs may be masked due to underlyingmyelosuppression. Therefore, neutropenic mouth-careprotocols that reduce microbial colonization of the den-tition and periodontium are important during myelo-suppression.
The diagnosis of agranulocytosis was reached in thepresent case by excluding the infectious etiology, cyclicneutropenia, and other causes of bone marrow suppres-sion by means of negative blood culture, tissue culture,and serology for HIV infections and lack of clinical find-ings for common viral, bacterial, and fungal infections. Inthe present case, repeated CBC, ANC �160/�L to420/�L, positive history of deferiprone intake, andhypoplastic marrow fragment with transient bone mar-row suppression predominantly involving myeloid se-ries were consistent with the diagnosis of agranulocy-tosis (Table I). Clinical symptoms of agranulocytosiswere also present in the form of sudden onset of fever,rigors, sepsis, and sore throat. Neutropenic fevers oftenreflect an ANC of �500/�L. For potential drug-in-duced neutropenias, discontinuation of the suspecteddrug provides both the diagnosis and the cure. In thepresent patient, progressive necrotic lesions occurred inthe context of agranulocytosis which were attributedto a direct effect of deferiprone intake. The remissionof symptoms and restoration of absolute neutrophilcount to normal after discontinuation of drug ruled outaplastic anemia and confirmed the diagnosis of drug-induced transient suppression of bone marrow. How-ever, culture and polymerase chain reaction for viralinfection and drug assay for deferiprone level could notbe performed owing to lack of facilities; therefore, thediagnostic process was a bit limited in this case.
Deferiprone (1,2-dimethyl-3-hydroxypyrid-4-one, orL1) is the first oral iron chelator used clinically, mainlyin thalassemia patients. Deferiprone belongs to the fam-ily of the alpha-ketohydroxypyridines, a relatively newclass of chelating agents, some of which are naturallyoccurring. These have high affinity for binding iron andare able to remove it from proteins that transport andstore it in the body, largely sparing other biologicallyimportant metals. Olivieri and Brittenham27 postulatedthat the mechanism of deferiprone-induced neutropeniais unknown and that this adverse effect appears not to
be dose dependent but idiosyncratic and unpredictable.
OOOOEe18 Tewari et al. October 2009
Recently, it has been suggested that a potential mech-anism of deferiprone-induced neutropenia is maturationarrest of the granulocytic lineage or decreased produc-tion of GCSF.28 Regarding efficacy, deferiprone, at adose of 75 mg/kg/day, reduces or maintains iron storesin the majority of patients receiving regular red celltransfusions.29-31 In the present patient, serum ferritinlevel was 9,700 �g/L, indicating inadequacy of the oralchelating agent. Major studies show that an oral chela-tor ensures a negative iron balance in some, but not all,patients, and that close monitoring is required to iden-tify patients in whom additional chelating treatment isindicated (i.e., weekly monitoring of blood counts)because of an increased risk of neutropenia/agranulo-cytosis.32 Raising the dose of deferiprone to 100 mg/kg/day or combining therapy with deferiprone and des-ferrioxamine has usually proven to be very effective inreducing iron stores in such patients.33,34 The latterapproach is based on balance studies demonstratingadditive iron excretion when the 2 chelators are com-bined. Thus, combination therapy may have a dualrationale: increasing total iron excretion and takingadvantage of some organ selectivity.35 Deferasirox is anew, convenient, once-daily oral iron chelator that hasdemonstrated in various clinical trials good efficacy andacceptable safety profile in adult and pediatric pa-tients affected by transfusion-dependent thalassemiamajor and by different chronic anemias.36 Henter andKarlen13 concluded that because the agranulocytosisdevelops rapidly, weekly monitoring of blood countsduring deferiprone therapy is not sufficient to avoid thedevelopment of persistent and potentially fatal agranu-locytosis. Moreover, the rapid development of a pro-longed agranulocytosis, despite administering only60% of the recommended dose, suggests that this sideeffect may not be dose dependent.
Because the development of agranulocytosis is notpredictable, possibly not dose dependent, and notavoidable despite meticulous blood count monitoring,we suggest the role of the dentists to recognize the signsor symptoms that could be suggestive of agranulocyto-sis, because the oral condition may be the first or onlymanifestation of a systemic abnormality. Although themajor concern for pediatricians is the management ofthe acute febrile episodes, dental professionals can pro-vide valuable expertise for effective control of infectionand management of oral symptoms. Patton37 recom-mended that certain clinically relevant laboratory val-ues are important in the management of the hemato-logic status of patients with hematologic malignancy,idiopathic or drug-induced blood dyscrasias, and sickle-cell anemia. When oral surgical procedures are antici-pated, a platelet count of �50,000 cells/�L, absolute
neutrophil count of �500 cells/�L, and hemoglobinconcentration of �7 g/dL are recommended to com-fortably assure effective hemostasis and reduce the riskof postoperative bacterial infection.38,39 Patients suffer-ing from agranulocytosis require daily monitoring ofcomplete blood cell count when ANC is �500/�L,biweekly when ANC is �500-1,000/�L, and weeklywhen ANC is �1,000-1,500/�L.
In summary, the present paper presents a rare case ofnecrotizing gingivostomatitis secondary to deferiprone-induced agranulocytosis reported for the first time indental literature.
REFERENCES1. 1 Weatherall DJ, Clegg JB. Inherited haemoglobin disorders: an
increasing global health problem. Bull World Health Org 2001;79:704-12.
2. Angastiniotis M, Modell B. Global epidemiology of hemoglobindisorders. Ann N Y Acad Sci 1998;850:251-69.
3. Britton RS, Leicester KL, Bacon BR. Iron toxicity and chelationtherapy. Int J Hematol 2002;76:219-28.
4. Piga A, Caglioti C, Fogliacco E, Tricta F. Comparative effects ofdeferiprone and deferoxamine on survival and cardiac disease inpatients with thalassemia major: a retrospective analysis. Haema-tologica 2003;88:489-96.
5. Anderson LJ, Wonke B, Prescott E, Holden S, Walker JM,Pennell D. Comparison of effects of oral deferiprone andsubcutaneous desferrioxamine on myocardial iron concentra-tions and ventricular function in beta-thalassemia. Lancet2002;360:516-20.
6. Hoffbrand AV. Deferiprone therapy for transfusional iron over-loads. Clin Haematol 2005;18:299-317.
7. Cohen A, Galanello R, Piga A, Vullo C, Tricta F. A multi-centersafety trial of the oral iron chelator deferiprone. Ann N Y AcadSci 1998;850:223-6.
8. Cohen AR, Galanello R, Piga A, Dipalma A, Vullo C, Tricta F.Safety profile of the oral iron chelator deferiprone: a multicenterstudy. Br. J Haematol 2000;108:305-12.
9. Cohen A, Galanello R, Piga A, De Sanctis, Tricta F. Safety andeffectiveness of long-term therapy with the oral iron chelatordeferiprone. Blood 2003;102:1583-7.
10. Ceci A, Baiardi P, Felisi M, Cappellini MD, Carnelli V, DeSanctis V, et al. The safety and effectiveness of deferiprone in alarge-scale, 3-year study in Italian patients. Br J Haematol2002;118:330-6.
11. Al-Refaie FN, Wonke B, Hoffbrand AV. Deferiprone-associatedmyelotoxicity. Eur J Haematol 1994;53:298-301.
12. Al-Refaie FN, Hershko C, Hoffbrand AV, Kosaryan M, OlivieriNF, Tondury P, et al. Results of long-term deferiprone (L1)therapy: a report by the International Study Group on Oral IronChelators. Br J Haematol 1995;91:224-9.
13. Henter JI, Karlen J. Fatal agranulocytosis after deferipronetherapy in a child with Diamond-Blackfan anemia. Blood2007;109:5157-9.
14. Luzzi GA, Jones BJ. Treatment of neutropenic oral ulceration inhuman immunodeficiency virus infection with G-CSF. Oral SurgOral Med Oral Pathol Oral Radiol Endod 1996;8:53-4.
15. Young NS. Aplastic anemia, Myelodysplasia, and Related BoneMarrow Failure Syndromes. In: Kasper DL, Braunwald E, FauciAS, Hauser SL, Longo DL, Jameson JL, editors. Harrison’sprinciples of internal medicine. 16th ed. New York: McGraw-Hill; 2005. p. 617-25.
16. Rashmi SM, Alka DK, Ramakant SN. Neutrophils in health and
disease: An overview. J Oral Maxillofac Pathol 2006;10:3-8.
OOOOEVolume 108, Number 4 Tewari et al. e19
17. Dale DC, Hammond WP. Cycic neutropenia: a clinical review.Blood Rev 1988;2:78-85.
18. Andrès E, Maloisel F. Idiosyncratic drug-induced agranulocyto-sis or acute neutropenia. Curr Opin Hematol 2008;15:15-21.
19. Patton WN, Duffull SB. Idiosyncratic drug-induced haemato-logical abnormalities: incidence, pathogenesis, management andavoidance. Drug Safety 1994;11:445-62.
20. Robinson PG, Sheiham A, Challacombe SJ, Wren MWD, Zakr-zewska JM. Gingival ulceration in HIV infection: a case seriesand case control. J Clin Periodontol 1998;25:260-7.
21. Hasturk H, Tezcan I, Yel L, Ersoy F, Sanal O, Yamalik N, et al.A case of chronic severe neutropenia: oral findings and conse-quences of short-term granulocyte colony-stimulating factortreatment. Aust Dent J 1998;43:9-13.
22. Scully C, Gilmour G. Neutropenia and dental patients. Br Dent J1986;160:43-6.
23. Barrett AP. Neutropenic ulceration. A distinctive clinical entity.J Periodontol 1987;58:51-5.
24. Epstein JB, Chow AW. Oral complications associated with im-munosuppression and cancer therapies. Infect Dis Clin North Am1999;13:901-23.
25. Bermejo-Fenoll A, Sanchez-Perez A. Necrotising periodontaldiseases. Med Oral Patol Oral Cir Bucal 2004;9:108-19.
26. Novak MJ. Necrotizing ulcerative periodontitis. Ann Periodontol1999;4:74-8.
27. Olivieri NF, Brittenham GM. Iron-chelating therapy and thetreatment of thalassemia. Blood 1997;89:739-61.
28. Vlachaki E, Ioannidoapagiannaki E, Tziomalos K, Haralambi-dou-Vranitsa S, Perifanis V, Klonizakis I, et al. Peripheral bloodhaematopoietic progenitor cells in patients with beta thalas-saemia major receiving desferrioxamine or deferiprone as che-lation therapy. Eur J Haematol 2007;78:48-51.
29. Olivieri NF, Brittenham GM, Matsui D, Berkovitch M, BlendisLM, Cameron RG, et al. Iron-chelation therapy with oral de-feriprone in patients with thalassemia major. N Engl J Med1995;332:918-22.
30. Olivieri NF, Brittenham GM, McLaren CE, Templeton DM,
Cameron RG, McClelland RA, et al. Long-term safety and ef-fectiveness of iron-chelation therapy with deferiprone forthalassemia major. N Engl J Med 1998;339:417-23.
31. Maggio A, D’Amico G, Morabito A, Capra M, Ciaccio C,Cianciulli P, et al. Deferiprone versus deferoxamine in patientswith thalassemia major: a randomized clinical trial. Blood CellsMol Dis 2002;28:196-208.
32. Hoffbrand AV, Cohen A, Hershko C. Role of deferiprone inchelation therapy for transfusional iron overload. Blood 2003;102:17-24.
33. Wonke B, Wright C, Hoffbrand AV. Combined therapy with de-feriprone and desferrioxamine. Br J Haematol 1998;103:361-4.
34. Kattamis A, Ladis V, Berdousi H, Kelekis NL, Alexopoulou E,Papasotiriou I, et al. Iron chelation treatment with combinedtherapy with deferiprone and deferioxamine: a 12-month trial.Blood Cells Mol Dis 2006;36:21-5.
35. Mourad FH, Hoffbrand AV, Sheikh-Taha M, Koussa S, KhoriatyAI, Taher A. Comparison between desferrioxamine and com-bined therapy with desferrioxamine and deferiprone in iron over-loaded thalassaemia patients. Br J Haematol 2003;121:187-9.
36. Cappellini MD, Piga A. Current status in iron chelation inhemoglobinopathies. Curr Mol Med 2008;8:663-74.
37. Patton LL. Hematologic abnormalities among HIV-infected pa-tient: Associations of significance for dentistry. Oral Surg OralMed Oral Pathol Oral Radiol Endod 1999;88:561-7.
38. Lockhart PB, Gibson J, Pond SH, Leitch J. Dental managementconsiderations for the patient with an acquired coagulopathy.Part 2: Coagulopathies from drugs. Br Dent J 2003;195:495-501.
39. Patton LL, Ship JA. Treatment of patients with bleeding disor-ders. Dent Clin North Am 1994;38:465-82.
Reprint requests:
Dr Shikha TewariDepartment of PeriodonticsGovt. Dental College6/6-J Medical EnclaveRohtak, HaryanaIndia 124001
[email protected]



















