
Centrally Necrotizing Carcinomas of the Breast: A Distinct Histologic Subtype With Aggressive...
7
Centrally Necrotizing Carcinomas of the Breast A Distinct Histologic Subtype With Aggressive Clinical Behavior Rafael E. Jimenez, M.D., Tracy Wallis, B.S., and Daniel W. Visscher, M.D. Most breast carcinomas exhibit ductal differentiation. How- ever, recognition of less common histologic patterns provides clinically useful data. This report describes a distinctive sub- type of breast carcinoma that we have termed “centrally nec- rotizing carcinoma” (CNC; in this study, N 34), which is characterized by an unusual and aggressive natural history. Centrally necrotizing carcinomas are composed of well- circumscribed, unicentric nodules with extensive central necro- sis that are surrounded by a narrow rim of viable high-grade tumor cells. These tumor cells show minimal ductal differen- tiation (i.e., tubule formation), but are usually associated with focal ductal carcinoma in situ. The mean age of the patients in this study was 57.5 ± 11.6 years, and the mean tumor size was 2.5 ± 1.2 cm. Twenty-eight percent of the patients had positive axillary lymph nodes (mean number of lymph nodes involved, 2.1 ± 1.2). Ninety-four percent of cases were negative for es- trogen and progesterone receptors. In 21 patients (62%), local and/or distant recurrences developed (median time to recur- rence, 16.2 months), and, to date, 20 have died from breast cancer (median time to death, 22.5 months). Progression of disease (defined as the development of either a recurrence or death resulting from disease) occurred in 24 patients (71%). Comparison with a set of 26 poorly differentiated ductal car- cinomas with (nonextensive, patchy) necrosis matched for age, tumor size, and lymph node status showed a significantly worse progression-free survival rate for the CNC group (p <0.004). We conclude that CNC is an uncommon but readily identifiable subtype of breast carcinoma and is characterized by early sys- temic metastasis and an accelerated clinical course. Key Words: Breast cancer—Centrally necrotizing carcinoma—Necrosis—Prognosis—Poorly differentiated carcinoma. Am J Surg Pathol 25(3): 331–337, 2001. Breast cancer is characterized by generous morpho- logic heterogeneity. There are multiple, well-recognized, histologic subtypes (e.g., lobular, micropapillary, 11 mu- cinous, 14 medullary 9 ) that are associated with distinctive clinicopathologic features and/or a different prognosis than that of typical invasive ductal carcinomas, 5,13 which constitute the majority of cases (60–80%). Even within the category of ductal carcinoma there is considerable variability on microscopic examination of histologic growth pattern and cellular differentiation. Histologic grade and/or presence of vascular invasion are used routinely to define the clinical aggressiveness of these tumors. Necrosis is a relatively frequent, but usually focal, histologic finding in breast carcinoma, particularly in cases with ductal differentiation. It is generally consid- ered to be a feature of otherwise aggressive, poorly dif- ferentiated lesions 4,12 (i.e., in invasive tumors) and is thus not formally reported. In this report, we describe a series of histologically distinctive breast carcinomas that are characterized by a large, central, necrotic zone, with variable fibrosis, surrounded by a rim of residual high- grade tumor cells. The zone of necrosis typically consti- tutes a majority of the tumor volume. Per standard clas- sification systems, such cases would be classified as in- filtrating carcinomas, no special type, or as poorly differentiated, infiltrating ductal carcinomas. We have designated these tumors centrally necrotizing carcinomas (CNCs), and our objective herein is to perform a detailed clinicopathologic analysis of these tumors, with special consideration to their clinical outcome. MATERIALS AND METHODS Thirty-four CNCs of the breast were retrieved from the surgical pathology files of Harper Hospital and the Karmanos Cancer Institute, Detroit, Michigan. Cases ini- tially were diagnosed between 1981 and 1999. All tu- mors formed unicentric nodules, which were mostly formed by a large, central necrotic zone accounting for at least 70% of the cross-sectional area of each neoplasm. From the Department of Pathology Harper Hospital, the Karmanos Cancer Institute, and Wayne State University, Detroit, Michigan, U.S.A. Presented at the 89th United States and Canadian Academy of Pathology Annual Meeting, New Orleans, Louisiana, March 2000. Address correspondence and reprint requests to Daniel W. Visscher, MD, Harper Hospital, Department of Pathology, 3990 John R., Detroit, MI 48201, U.S.A. The American Journal of Surgical Pathology 25(3): 331–337, 2001 © 2001 Lippincott Williams & Wilkins, Inc., Philadelphia 331
-
Upload
independent -
Category
Documents
-
view
0 -
download
0
Transcript of Centrally Necrotizing Carcinomas of the Breast: A Distinct Histologic Subtype With Aggressive...
Centrally Necrotizing Carcinomas of the BreastA Distinct Histologic Subtype With AggressiveClinical Behavior
Rafael E. Jimenez, M.D., Tracy Wallis, B.S., and Daniel W. Visscher, M.D.
Most breast carcinomas exhibit ductal differentiation. How-ever, recognition of less common histologic patterns providesclinically useful data. This report describes a distinctive sub-type of breast carcinoma that we have termed “centrally nec-rotizing carcinoma” (CNC; in this study, N � 34), which ischaracterized by an unusual and aggressive natural history.Centrally necrotizing carcinomas are composed of well-circumscribed, unicentric nodules with extensive central necro-sis that are surrounded by a narrow rim of viable high-gradetumor cells. These tumor cells show minimal ductal differen-tiation (i.e., tubule formation), but are usually associated withfocal ductal carcinoma in situ. The mean age of the patients inthis study was 57.5 ± 11.6 years, and the mean tumor size was2.5 ± 1.2 cm. Twenty-eight percent of the patients had positiveaxillary lymph nodes (mean number of lymph nodes involved,2.1 ± 1.2). Ninety-four percent of cases were negative for es-trogen and progesterone receptors. In 21 patients (62%), localand/or distant recurrences developed (median time to recur-rence, 16.2 months), and, to date, 20 have died from breastcancer (median time to death, 22.5 months). Progression ofdisease (defined as the development of either a recurrence ordeath resulting from disease) occurred in 24 patients (71%).Comparison with a set of 26 poorly differentiated ductal car-cinomas with (nonextensive, patchy) necrosis matched for age,tumor size, and lymph node status showed a significantly worseprogression-free survival rate for the CNC group (p <0.004).We conclude that CNC is an uncommon but readily identifiablesubtype of breast carcinoma and is characterized by early sys-temic metastasis and an accelerated clinical course.Key Words: Breast cancer—Centrally necrotizingcarcinoma—Necrosis—Prognosis—Poorly differentiatedcarcinoma.
Am J Surg Pathol 25(3): 331–337, 2001.
Breast cancer is characterized by generous morpho-logic heterogeneity. There are multiple, well-recognized,
histologic subtypes (e.g., lobular, micropapillary,11 mu-cinous,14 medullary9) that are associated with distinctiveclinicopathologic features and/or a different prognosisthan that of typical invasive ductal carcinomas,5,13 whichconstitute the majority of cases (60–80%). Even withinthe category of ductal carcinoma there is considerablevariability on microscopic examination of histologicgrowth pattern and cellular differentiation. Histologicgrade and/or presence of vascular invasion are usedroutinely to define the clinical aggressiveness of thesetumors.
Necrosis is a relatively frequent, but usually focal,histologic finding in breast carcinoma, particularly incases with ductal differentiation. It is generally consid-ered to be a feature of otherwise aggressive, poorly dif-ferentiated lesions4,12 (i.e., in invasive tumors) and isthus not formally reported. In this report, we describe aseries of histologically distinctive breast carcinomas thatare characterized by a large, central, necrotic zone, withvariable fibrosis, surrounded by a rim of residual high-grade tumor cells. The zone of necrosis typically consti-tutes a majority of the tumor volume. Per standard clas-sification systems, such cases would be classified as in-filtrating carcinomas, no special type, or as poorlydifferentiated, infiltrating ductal carcinomas. We havedesignated these tumors centrally necrotizing carcinomas(CNCs), and our objective herein is to perform a detailedclinicopathologic analysis of these tumors, with specialconsideration to their clinical outcome.
MATERIALS AND METHODS
Thirty-four CNCs of the breast were retrieved fromthe surgical pathology files of Harper Hospital and theKarmanos Cancer Institute, Detroit, Michigan. Cases ini-tially were diagnosed between 1981 and 1999. All tu-mors formed unicentric nodules, which were mostlyformed by a large, central necrotic zone accounting for atleast 70% of the cross-sectional area of each neoplasm.
From the Department of Pathology Harper Hospital, the KarmanosCancer Institute, and Wayne State University, Detroit, Michigan,U.S.A.
Presented at the 89th United States and Canadian Academy ofPathology Annual Meeting, New Orleans, Louisiana, March 2000.
Address correspondence and reprint requests to Daniel W. Visscher,MD, Harper Hospital, Department of Pathology, 3990 John R.,Detroit, MI 48201, U.S.A.
The American Journal of Surgical Pathology 25(3): 331–337, 2001 © 2001 Lippincott Williams & Wilkins, Inc., Philadelphia
331

This zone was surrounded by a rim of infiltrating tumorcells, rendering a characteristic outline of the tissue sec-tion on gross examination of the glass slide (Fig. 1). Thecentral necrotic zone contained variable fibrosis, typi-cally focal, hyaline, and acellular. Tissue sections fromeach case were studied for the degree of associated lym-phoplasmacytic infiltrate, the extent of ductal carcinomain situ, and the presence of fibrocystic changes. Neo-plasms were graded according to the modified Scarff-Bloom-Richardson system.3 Size of the tumor and lymphnode status were recorded for each tumor, when suchdata were available.
Clinical data were obtained from patients’ medicalcharts and from the Harper Hospital/Karmanos CancerInstitute cancer registries. Cases were staged accordingto the 1997 TNM Staging system for breast cancer.1
Other retrieved data included age, race, recurrence (in-cluding local recurrence and/or distant metastasis), siteof metastasis, survival status, and cause of death.
Estrogen and progesterone receptor (ER/PR) status in-formation was available for 17 cases; in 8, determinationwas immunohistochemical, as described elsewhere,17
whereas in 9, determination was biochemical. S-phasefraction and ploidy analysis results were available for 6and 14 cases, respectively, and were determined by flowcytometry, as described elsewhere.18
For outcome analysis, the study group was comparedwith a set of 26 poorly differentiated ductal carcinomasthat contained multifocal necrosis, but without contigu-ous central zone involvement. Further, the growth pat-tern in the control series was mostly infiltrative. Thesecases were matched to the study group by age, tumorsize, and lymph node status. Comparisons between theCNC and control groups were performed by using the �2
test for frequencies and Student t test for means. Survivalcurves were plotted by using the Kaplan-Meier method,and the difference between the curves was analyzed withthe log rank test.
RESULTS
The mean age of the patients was 57.5 ± 11.6 years.(median age, 58.5 years). Of patients with available de-
mographic information, 12 were African-American, and10 were Caucasian. Mean tumor size was 2.5 ± 1.2 cm(10 tumors <2 cm, 19 tumors 2–5 cm, 2 tumors >5 cm).One tumor arose in the radiation field in a patient whohad undergone a lumpectomy for an invasive ductal car-cinoma 18 years earlier. Two others developed in pa-tients with previous contralateral breast carcinomas.
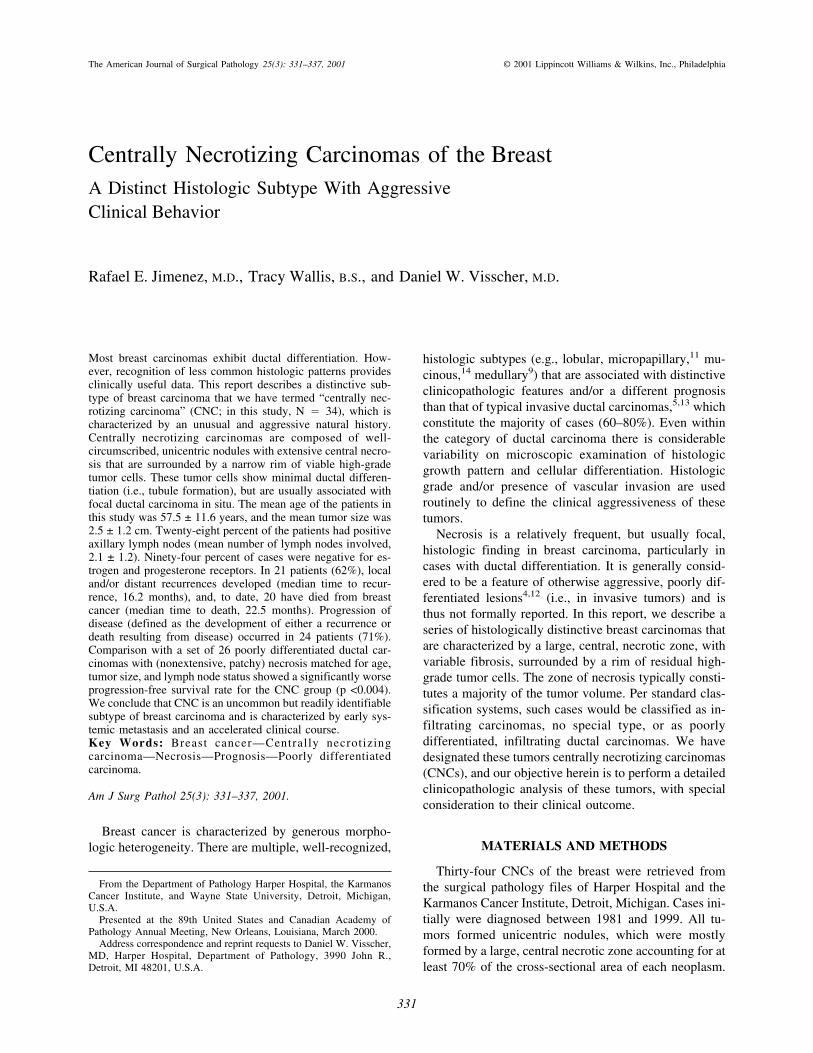
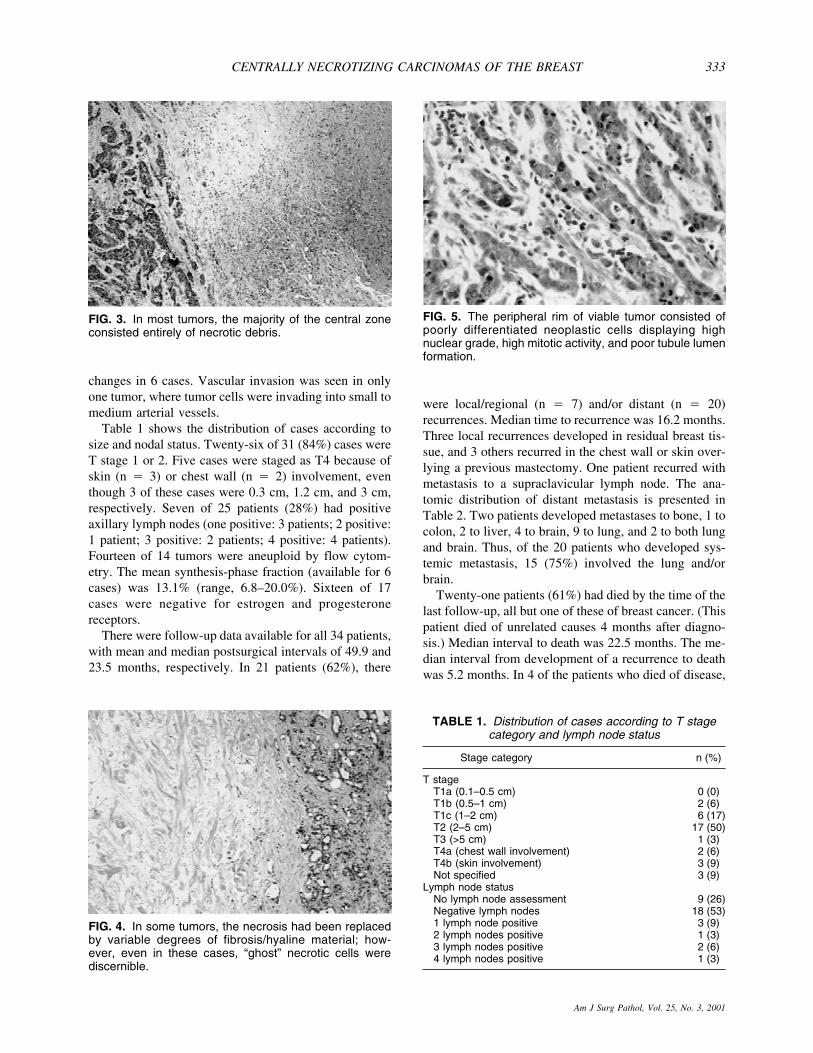
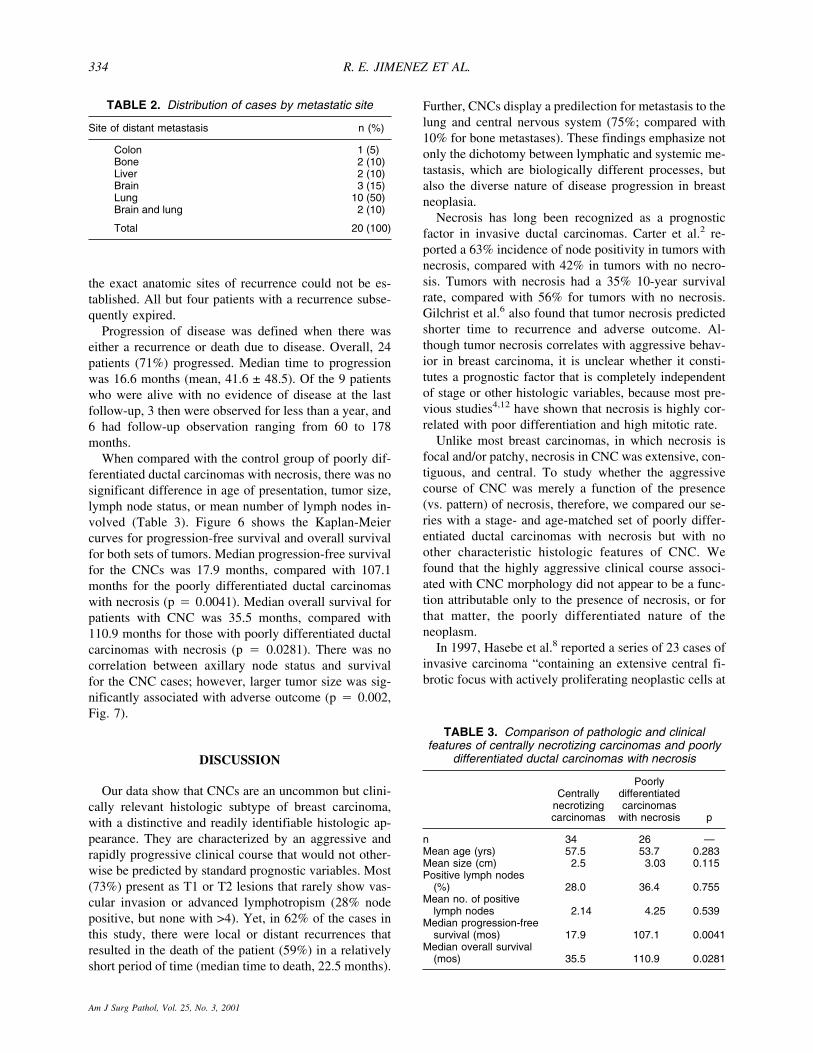
All tumors consisted of unicentric, symmetric noduleswith a prominent central, hypocellular zone, surroundedby a ring-like hypercellular area with a pushing border,sharply delineating it from the surrounding breast tissue(Fig. 2). In most tumors, the great majority of the centralzone consisted entirely of necrotic debris (Fig. 3). Insome, the necrosis had been replaced by variable degreesof fibrosis/hyaline material (Fig. 4); however, even inthese cases, “ghost” necrotic cells were discernible. Theperipheral rim of viable tumor cells displayed highnuclear grade in all cases, with numerous mitoses (>3 perHPF). Although the cells often were disposed in smallnests, there was lack of tubule lumen formation in thevast majority of cases (Fig. 5). All tumors were thuspoorly differentiated. In one case, there was focal squa-mous differentiation. In another, there was focal spindle-cell differentiation. The transition between the centralnecrotic zone and viable tumor was usually abrupt. Thecells did not grow in a syncytial fashion and were not inany case associated with prominent lymphoplasmacyticinfiltrates.
In 19 cases, there was an associated ductal carcinomain situ component. In 17 of these, the intraductal com-ponent represented less than 10% of the tumor volume.In 2 cases, a relatively extensive intraductal componentsurrounded the periphery of the invasive tumor nodule.Two additional cases were associated with lobular car-cinoma in situ. The adjacent benign breast tissue wasnormal or atrophic in 20 cases, had nonproliferative fi-brocystic changes in 6 cases, and proliferative fibrocystic
F I G . 1 .Characteristicoutline of CNC,recognizableeven with un-magnified ex-amination ofthe glass slide.
FIG. 2. Prominent, central, hypocellular zone, sur-rounded by a ring-like hypercellular area with a pushingborder.
R. E. JIMENEZ ET AL.332
Am J Surg Pathol, Vol. 25, No. 3, 2001
changes in 6 cases. Vascular invasion was seen in onlyone tumor, where tumor cells were invading into small tomedium arterial vessels.
Table 1 shows the distribution of cases according tosize and nodal status. Twenty-six of 31 (84%) cases wereT stage 1 or 2. Five cases were staged as T4 because ofskin (n � 3) or chest wall (n � 2) involvement, eventhough 3 of these cases were 0.3 cm, 1.2 cm, and 3 cm,respectively. Seven of 25 patients (28%) had positiveaxillary lymph nodes (one positive: 3 patients; 2 positive:1 patient; 3 positive: 2 patients; 4 positive: 4 patients).Fourteen of 14 tumors were aneuploid by flow cytom-etry. The mean synthesis-phase fraction (available for 6cases) was 13.1% (range, 6.8–20.0%). Sixteen of 17cases were negative for estrogen and progesteronereceptors.
There were follow-up data available for all 34 patients,with mean and median postsurgical intervals of 49.9 and23.5 months, respectively. In 21 patients (62%), there
were local/regional (n � 7) and/or distant (n � 20)recurrences. Median time to recurrence was 16.2 months.Three local recurrences developed in residual breast tis-sue, and 3 others recurred in the chest wall or skin over-lying a previous mastectomy. One patient recurred withmetastasis to a supraclavicular lymph node. The ana-tomic distribution of distant metastasis is presented inTable 2. Two patients developed metastases to bone, 1 tocolon, 2 to liver, 4 to brain, 9 to lung, and 2 to both lungand brain. Thus, of the 20 patients who developed sys-temic metastasis, 15 (75%) involved the lung and/orbrain.
Twenty-one patients (61%) had died by the time of thelast follow-up, all but one of these of breast cancer. (Thispatient died of unrelated causes 4 months after diagno-sis.) Median interval to death was 22.5 months. The me-dian interval from development of a recurrence to deathwas 5.2 months. In 4 of the patients who died of disease,
FIG. 4. In some tumors, the necrosis had been replacedby variable degrees of fibrosis/hyaline material; how-ever, even in these cases, “ghost” necrotic cells werediscernible.
FIG. 5. The peripheral rim of viable tumor consisted ofpoorly differentiated neoplastic cells displaying highnuclear grade, high mitotic activity, and poor tubule lumenformation.
TABLE 1. Distribution of cases according to T stagecategory and lymph node status
Stage category n (%)
T stageT1a (0.1–0.5 cm) 0 (0)T1b (0.5–1 cm) 2 (6)T1c (1–2 cm) 6 (17)T2 (2–5 cm) 17 (50)T3 (>5 cm) 1 (3)T4a (chest wall involvement) 2 (6)T4b (skin involvement) 3 (9)Not specified 3 (9)
Lymph node statusNo lymph node assessment 9 (26)Negative lymph nodes 18 (53)1 lymph node positive 3 (9)2 lymph nodes positive 1 (3)3 lymph nodes positive 2 (6)4 lymph nodes positive 1 (3)
FIG. 3. In most tumors, the majority of the central zoneconsisted entirely of necrotic debris.
CENTRALLY NECROTIZING CARCINOMAS OF THE BREAST 333
Am J Surg Pathol, Vol. 25, No. 3, 2001
the exact anatomic sites of recurrence could not be es-tablished. All but four patients with a recurrence subse-quently expired.
Progression of disease was defined when there waseither a recurrence or death due to disease. Overall, 24patients (71%) progressed. Median time to progressionwas 16.6 months (mean, 41.6 ± 48.5). Of the 9 patientswho were alive with no evidence of disease at the lastfollow-up, 3 then were observed for less than a year, and6 had follow-up observation ranging from 60 to 178months.
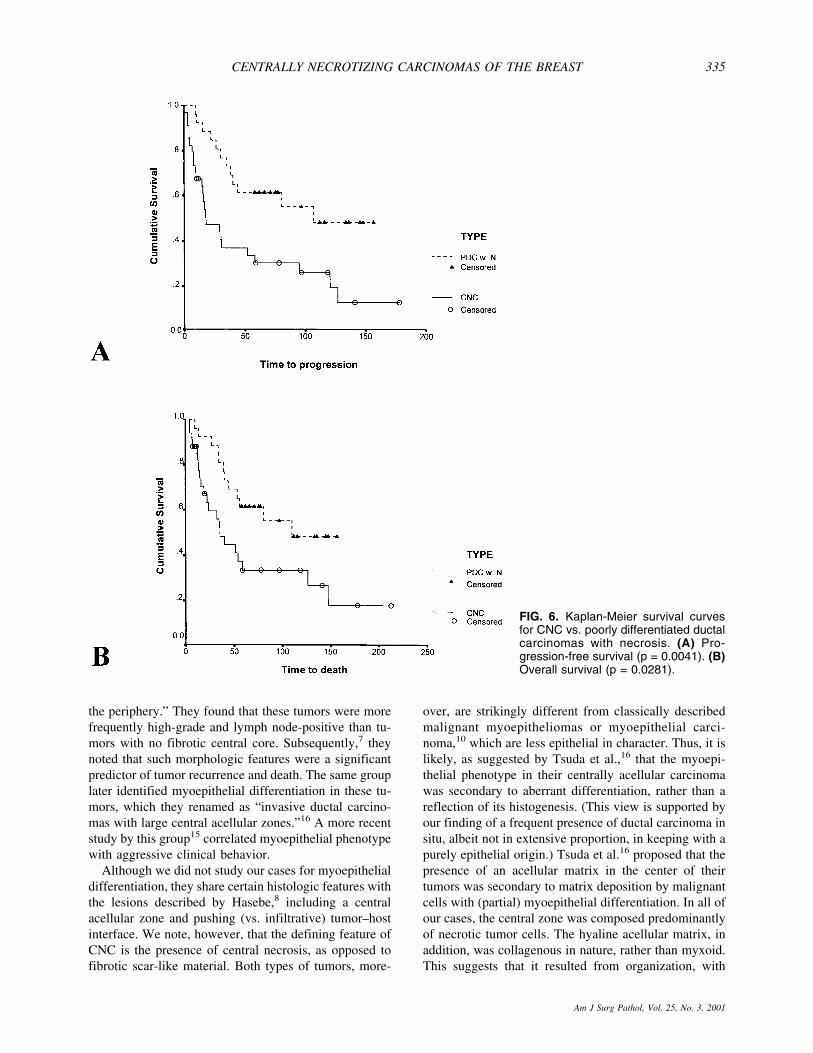
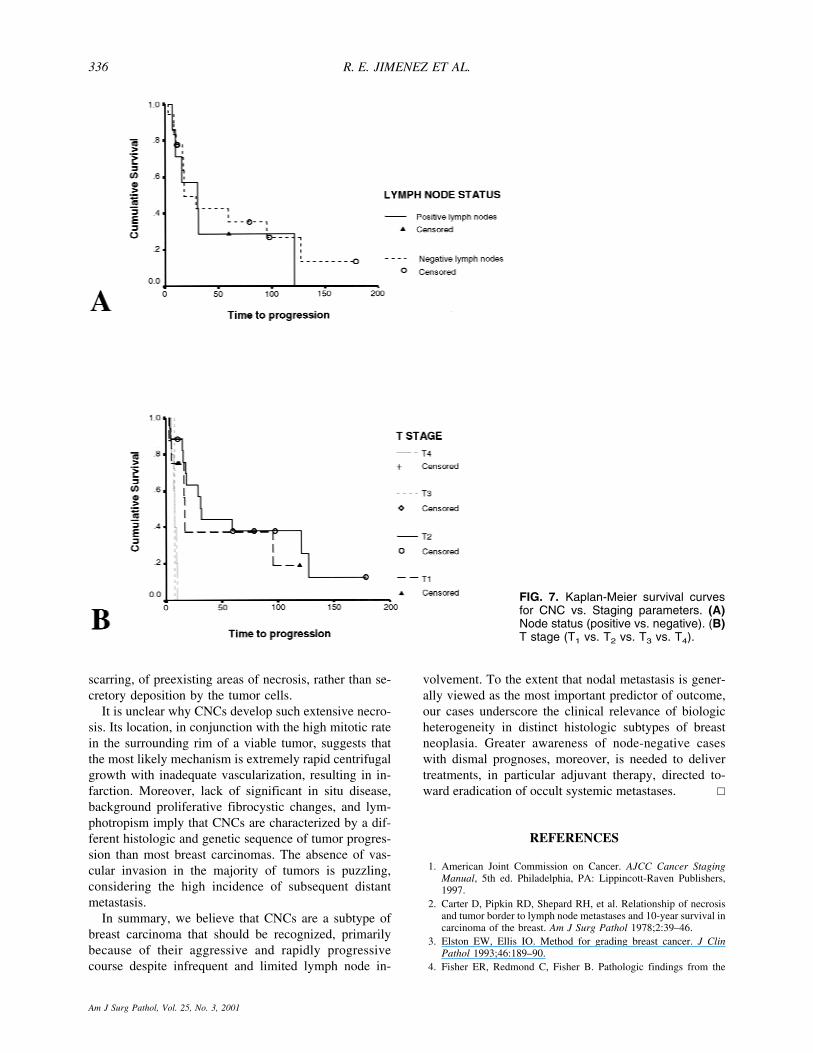
When compared with the control group of poorly dif-ferentiated ductal carcinomas with necrosis, there was nosignificant difference in age of presentation, tumor size,lymph node status, or mean number of lymph nodes in-volved (Table 3). Figure 6 shows the Kaplan-Meiercurves for progression-free survival and overall survivalfor both sets of tumors. Median progression-free survivalfor the CNCs was 17.9 months, compared with 107.1months for the poorly differentiated ductal carcinomaswith necrosis (p � 0.0041). Median overall survival forpatients with CNC was 35.5 months, compared with110.9 months for those with poorly differentiated ductalcarcinomas with necrosis (p � 0.0281). There was nocorrelation between axillary node status and survivalfor the CNC cases; however, larger tumor size was sig-nificantly associated with adverse outcome (p � 0.002,Fig. 7).
DISCUSSION
Our data show that CNCs are an uncommon but clini-cally relevant histologic subtype of breast carcinoma,with a distinctive and readily identifiable histologic ap-pearance. They are characterized by an aggressive andrapidly progressive clinical course that would not other-wise be predicted by standard prognostic variables. Most(73%) present as T1 or T2 lesions that rarely show vas-cular invasion or advanced lymphotropism (28% nodepositive, but none with >4). Yet, in 62% of the cases inthis study, there were local or distant recurrences thatresulted in the death of the patient (59%) in a relativelyshort period of time (median time to death, 22.5 months).
Further, CNCs display a predilection for metastasis to thelung and central nervous system (75%; compared with10% for bone metastases). These findings emphasize notonly the dichotomy between lymphatic and systemic me-tastasis, which are biologically different processes, butalso the diverse nature of disease progression in breastneoplasia.
Necrosis has long been recognized as a prognosticfactor in invasive ductal carcinomas. Carter et al.2 re-ported a 63% incidence of node positivity in tumors withnecrosis, compared with 42% in tumors with no necro-sis. Tumors with necrosis had a 35% 10-year survivalrate, compared with 56% for tumors with no necrosis.Gilchrist et al.6 also found that tumor necrosis predictedshorter time to recurrence and adverse outcome. Al-though tumor necrosis correlates with aggressive behav-ior in breast carcinoma, it is unclear whether it consti-tutes a prognostic factor that is completely independentof stage or other histologic variables, because most pre-vious studies4,12 have shown that necrosis is highly cor-related with poor differentiation and high mitotic rate.
Unlike most breast carcinomas, in which necrosis isfocal and/or patchy, necrosis in CNC was extensive, con-tiguous, and central. To study whether the aggressivecourse of CNC was merely a function of the presence(vs. pattern) of necrosis, therefore, we compared our se-ries with a stage- and age-matched set of poorly differ-entiated ductal carcinomas with necrosis but with noother characteristic histologic features of CNC. Wefound that the highly aggressive clinical course associ-ated with CNC morphology did not appear to be a func-tion attributable only to the presence of necrosis, or forthat matter, the poorly differentiated nature of theneoplasm.
In 1997, Hasebe et al.8 reported a series of 23 cases ofinvasive carcinoma “containing an extensive central fi-brotic focus with actively proliferating neoplastic cells at
TABLE 3. Comparison of pathologic and clinicalfeatures of centrally necrotizing carcinomas and poorly
differentiated ductal carcinomas with necrosis
Centrallynecrotizingcarcinomas
Poorlydifferentiatedcarcinomas
with necrosis p
n 34 26 —Mean age (yrs) 57.5 53.7 0.283Mean size (cm) 2.5 3.03 0.115Positive lymph nodes
(%) 28.0 36.4 0.755Mean no. of positive
lymph nodes 2.14 4.25 0.539Median progression-free
survival (mos) 17.9 107.1 0.0041Median overall survival
(mos) 35.5 110.9 0.0281
TABLE 2. Distribution of cases by metastatic site
Site of distant metastasis n (%)
Colon 1 (5)Bone 2 (10)Liver 2 (10)Brain 3 (15)Lung 10 (50)Brain and lung 2 (10)
Total 20 (100)
R. E. JIMENEZ ET AL.334
Am J Surg Pathol, Vol. 25, No. 3, 2001
the periphery.” They found that these tumors were morefrequently high-grade and lymph node-positive than tu-mors with no fibrotic central core. Subsequently,7 theynoted that such morphologic features were a significantpredictor of tumor recurrence and death. The same grouplater identified myoepithelial differentiation in these tu-mors, which they renamed as “invasive ductal carcino-mas with large central acellular zones.”16 A more recentstudy by this group15 correlated myoepithelial phenotypewith aggressive clinical behavior.
Although we did not study our cases for myoepithelialdifferentiation, they share certain histologic features withthe lesions described by Hasebe,8 including a centralacellular zone and pushing (vs. infiltrative) tumor–hostinterface. We note, however, that the defining feature ofCNC is the presence of central necrosis, as opposed tofibrotic scar-like material. Both types of tumors, more-
over, are strikingly different from classically describedmalignant myoepitheliomas or myoepithelial carci-noma,10 which are less epithelial in character. Thus, it islikely, as suggested by Tsuda et al.,16 that the myoepi-thelial phenotype in their centrally acellular carcinomawas secondary to aberrant differentiation, rather than areflection of its histogenesis. (This view is supported byour finding of a frequent presence of ductal carcinoma insitu, albeit not in extensive proportion, in keeping with apurely epithelial origin.) Tsuda et al.16 proposed that thepresence of an acellular matrix in the center of theirtumors was secondary to matrix deposition by malignantcells with (partial) myoepithelial differentiation. In all ofour cases, the central zone was composed predominantlyof necrotic tumor cells. The hyaline acellular matrix, inaddition, was collagenous in nature, rather than myxoid.This suggests that it resulted from organization, with
FIG. 6. Kaplan-Meier survival curvesfor CNC vs. poorly differentiated ductalcarcinomas with necrosis. (A) Pro-gression-free survival (p = 0.0041). (B)Overall survival (p = 0.0281).
CENTRALLY NECROTIZING CARCINOMAS OF THE BREAST 335
Am J Surg Pathol, Vol. 25, No. 3, 2001
scarring, of preexisting areas of necrosis, rather than se-cretory deposition by the tumor cells.
It is unclear why CNCs develop such extensive necro-sis. Its location, in conjunction with the high mitotic ratein the surrounding rim of a viable tumor, suggests thatthe most likely mechanism is extremely rapid centrifugalgrowth with inadequate vascularization, resulting in in-farction. Moreover, lack of significant in situ disease,background proliferative fibrocystic changes, and lym-photropism imply that CNCs are characterized by a dif-ferent histologic and genetic sequence of tumor progres-sion than most breast carcinomas. The absence of vas-cular invasion in the majority of tumors is puzzling,considering the high incidence of subsequent distantmetastasis.
In summary, we believe that CNCs are a subtype ofbreast carcinoma that should be recognized, primarilybecause of their aggressive and rapidly progressivecourse despite infrequent and limited lymph node in-
volvement. To the extent that nodal metastasis is gener-ally viewed as the most important predictor of outcome,our cases underscore the clinical relevance of biologicheterogeneity in distinct histologic subtypes of breastneoplasia. Greater awareness of node-negative caseswith dismal prognoses, moreover, is needed to delivertreatments, in particular adjuvant therapy, directed to-ward eradication of occult systemic metastases. �
REFERENCES
1. American Joint Commission on Cancer. AJCC Cancer StagingManual, 5th ed. Philadelphia, PA: Lippincott-Raven Publishers,1997.
2. Carter D, Pipkin RD, Shepard RH, et al. Relationship of necrosisand tumor border to lymph node metastases and 10-year survival incarcinoma of the breast. Am J Surg Pathol 1978;2:39–46.
3. Elston EW, Ellis IO. Method for grading breast cancer. J ClinPathol 1993;46:189–90.
4. Fisher ER, Redmond C, Fisher B. Pathologic findings from the
FIG. 7. Kaplan-Meier survival curvesfor CNC vs. Staging parameters. (A)Node status (positive vs. negative). (B)T stage (T1 vs. T2 vs. T3 vs. T4).
R. E. JIMENEZ ET AL.336
Am J Surg Pathol, Vol. 25, No. 3, 2001

National Surgical Adjuvant Breast Project (Protocol no. 4). VI:Discriminants for five-year treatment failure. Cancer 1980;46:908–18.
5. Gamel JW, Meyer JS, Feuer E, et al. The impact of stage andhistology on the long-term clinical course of 163,808 patients withbreast carcinoma. Cancer 1996;77:1459–64.
6. Gilchrist KW, Gray R, Fowble B, et al. Tumor necrosis is a prog-nostic predictor for early recurrence and death in lymph node-positive breast cancer: a 10-year follow-up study of 728 EasternCooperative Oncology Group patients. J Clin Oncol 1993;11:1929–35.
7. Hasebe T, Tsuda H, Hirohashi S, et al. Fibrotic focus in infiltratingductal carcinoma of the breast: a significant histopathologicalprognostic parameter for predicting the long-term survival of thepatients. Br Canc Res Tr 1998;49:195–208.
8. Hasebe T, Tsuda H, Tsubono Y, et al. Fibrotic focus in invasiveductal carcinoma of the breast: a histopathological prognostic pa-rameter for tumor recurrence and tumor death within three yearsafter the initial operation. Jpn J Cancer Res 1997;88:590–9.
9. Jensen ML, Kiaer H, Andersen J, et al. Prognostic comparison ofthree classifications for medullary carcinomas of the breast. His-topathology 1997;30:523–32.
10. Lakhani SR, O’Hare MJ, Monaghan P, et al. Malignant myoepi-thelioma (myoepithelial carcinoma) of the breast: a detailed cyto-keratin study. J Clin Pathol 1995;48:164–7.
11. Luna-More S, Gonzalez B, Acedo C, et al. Invasive micropapillary
carcinoma of the breast: a new special type of invasive mammarycarcinoma. Pathol Res Pract 1994;190:668–74.
12. Shek LL, Godolphin W. Model for breast cancer survival: relativeprognostic roles of axillary nodal status, TNM stage, estrogen re-ceptor concentration, and tumor necrosis. Cancer Res 1988;48:5565–9.
13. Tabar L, Fagerberg G, Chen HH, et al. Tumour development,histology and grade of breast cancers: prognosis and progression.Int J Cancer 1996;66:413–9.
14. Toikkanen S, Kujari H. Pure and mixed mucinous carcinomas ofthe breast: a clinicopathologic analysis of 61 cases with long-termfollow-up. Hum Pathol 1989;20:758–64.
15. Tsuda H, Takarabe T, Hasegawa F, et al. Large, central acellularzones indicating myoepithelial tumor differentiation in high-gradeinvasive ductal carcinomas as markers of predisposition to lungand brain metastases. Am J Surg Pathol 2000;24:197–202.
16. Tsuda H, Takarabe T, Hasegawa T, et al. Myoepithelial differen-tiation in high-grade invasive ductal carcinomas with large centralacellular zones. Hum Pathol 1999;30:1134–9.
17. Visscher DW, Sarkar F, Tabaczka P, et al. Clinicopathologicanalysis of bcl-2 immunostaining in breast carcinoma. Mod Pathol1996;9:642–6.
18. Visscher DW, Zarbo RJ, Jacobsen G, et al. Multiparametric de-oxyribonucleic acid and cell cycle analysis of breast carcinomas byflow cytometry: clinicopathologic correlations. Lab Invest 1990;62:370–8.
CENTRALLY NECROTIZING CARCINOMAS OF THE BREAST 337
Am J Surg Pathol, Vol. 25, No. 3, 2001




















