
Incidence, Etiology, Histologic Findings, and Course of Thoracic Inflammatory Aortopathies
8
DOI: 10.1016/j.athoracsur.2008.07.039 2008;86:1518-1523 Ann Thorac Surg Giuseppe Nicola Martinelli and Roberto Di Bartolomeo Davide Pacini, Ornella Leone, Simone Turci, Nicola Camurri, Francesca Giunchi, Aortopathies Incidence, Etiology, Histologic Findings, and Course of Thoracic Inflammatory http://ats.ctsnetjournals.org/cgi/content/full/86/5/1518 located on the World Wide Web at: The online version of this article, along with updated information and services, is Print ISSN: 0003-4975; eISSN: 1552-6259. Southern Thoracic Surgical Association. Copyright © 2008 by The Society of Thoracic Surgeons. is the official journal of The Society of Thoracic Surgeons and the The Annals of Thoracic Surgery by on June 13, 2013 ats.ctsnetjournals.org Downloaded from
Transcript of Incidence, Etiology, Histologic Findings, and Course of Thoracic Inflammatory Aortopathies

DOI: 10.1016/j.athoracsur.2008.07.039 2008;86:1518-1523 Ann Thorac Surg
Giuseppe Nicola Martinelli and Roberto Di Bartolomeo Davide Pacini, Ornella Leone, Simone Turci, Nicola Camurri, Francesca Giunchi,
AortopathiesIncidence, Etiology, Histologic Findings, and Course of Thoracic Inflammatory
http://ats.ctsnetjournals.org/cgi/content/full/86/5/1518located on the World Wide Web at:
The online version of this article, along with updated information and services, is
Print ISSN: 0003-4975; eISSN: 1552-6259. Southern Thoracic Surgical Association. Copyright © 2008 by The Society of Thoracic Surgeons.
is the official journal of The Society of Thoracic Surgeons and theThe Annals of Thoracic Surgery
by on June 13, 2013 ats.ctsnetjournals.orgDownloaded from

ICDFD
ildif
a(adb
aoT
Aapbnfvetaa
ffotlemeHir
1
A
AcV
©P
AD
ULT
CA
RD
IAC
ncidence, Etiology, Histologic Findings, andourse of Thoracic Inflammatory Aortopathies
avide Pacini, MD, Ornella Leone, MD, Simone Turci, MD, Nicola Camurri, MD,rancesca Giunchi, MD, Giuseppe Nicola Martinelli, MD, and Roberto Di Bartolomeo, MD
epartments of Cardiac Surgery and Pathology, S. Orsola-Malpighi Hospital, University of Bologna, Bologna, Italyaalwied3p
ioac
Background. The aims of this study were to detect thencidence of thoracic histologically proven aortitis in aarge series of 788 patients operated on for thoracic aorticisease, to describe the surgical and histologic features of
nflammatory thoracic aortopathies, and to evaluate therequency of postsurgical complications and mortality.
Methods. Thirty-nine patients (4.9%) were affected byortitis (mean age, 72.6 � 9.6). There were 24 women61.5%). Thirty-four (87.2%) were operated on because ofneurysms and 5 because of dissection. In all cases theiagnosis of aortitis was incidental and was made on theasis of histopathologic findings.Results. Histologically, there were 30 cases of giant cell
ortitis (76.9%), 3 inflammatory aneurysms (7.7%), 2 casesf aspecific lymphoplasmacellular aortitis (5.1%), 1 of
akayasu aortitis, 1 of systemic erythematosus lupus–tvint
aPatt
oodmf
P
PBttw1yc
9hirurgia, Università degli studi di Bologna, Policlinico S. Orsola-Malpighiia Massarenti, 9, Bologna, 40138, Italy; e-mail: [email protected].
2008 by The Society of Thoracic Surgeonsublished by Elsevier Inc
ats.ctsnetjournDownloaded from
ssociated aortitis, and 1 of Behçet’s disease–associatedortitis. The only case of infectious aortitis was a syphi-itic aortitis. In 79.5% of cases, inflammatory infiltratesere moderate to severe in degree; the most widespread
nflammation was seen in Takayasu aortitis, systemicrythematosus lupus–associated aortitis, and in Behçet’sisease. The overall in-hospital mortality was 10.3% (4 of9 patients). Neurologic complications occurred in 4atients (10.3%).Conclusions. During surgery of the thoracic aorta, an
nflammatory etiology of aneurysms is found in almost 5%f cases. The inflammatory process is in a histologicallydvanced phase, often with systemic development. Surgeryan be associated with high morbidity and mortality.
(Ann Thorac Surg 2008;86:1518–23)
© 2008 by The Society of Thoracic Surgeonsortitis is defined as an inflammation of the aorticwall with or without disruption of elastic fibers,
ortic wall necrosis, or fibrosis [1]: the inflammatoryrocess involves one or more layers of the aorta and cane caused by multiple mechanisms. Clinical features areonspecific such as malaise, low-grade fever, weight loss,
atigability, sweating, and weakness. There is also ele-ated erythrocyte sedimentation rate, leukocytosis, andlevated C-reactive protein. In addition, Ueda [2] foundhat 74% of patients have detectable levels of antiaorticntibodies in the serum. The presentation is variable:neurysm, dissection, or stenosis of the aorta.The overall incidence of aortitis is not easy to evaluate
rom the literature: in the United States, the most frequentorm, giant cell arteritis with aortic wall involvement in 15%f cases, is reported as 15 to 30 cases per year per 100,000 ofhe population older than 50 years of age [1, 3]. In theiterature, there are few data including histopathologicxaminations of large case records of surgical aortic speci-ens. In these few papers, the incidence of aortitis is
xtremely variable, ranging from 1% to 22% [4–7], andomme and colleagues [8] recently identified active non-
nfectious aortitis in 9% of 513 patients with surgicallyesected ascending aortic aneurysms.
A separate entity described by Walker and associates in972 [9] in the abdominal aorta and later also in the thoracic
ccepted for publication July 9, 2008.
ddress correspondence to Dr Pacini, c/o Unità Operativa di Cardio-
ract is inflammatory aortic aneurysm, whose incidencearies from 3% to 11% in the cases operated on for abdom-nal aortic aneurysms [1, 10]. Diagnosis is difficult with onlyoninvasive imaging studies, so histopathologic examina-
ion is required to confirm the presence of the disease.Surgical treatment leads to an increased risk of tearing
s well as of aortic rupture because of the softened tissue.rogressive dilatation of the remaining native aorta maylso occur in the absence of radical replacement of theract involved, or in the case of diffuse development ofhe disease.
The aims of our study were (1) to detect the incidencef thoracic histologically proven aortitis in a large seriesf 788 patients affected by thoracic aortic pathology; (2) toescribe the surgical and histologic features of inflam-atory thoracic aortopathies; and (3) to evaluate the
requency of postsurgical complications and mortality.
atients and Methods
atient Populationetween April 1997 and June 2004, we studied specimens of
horacic aorta obtained from 788 patients who underwenthoracic aortic resection. The overall mean age of patientsas 58.9 � 15.24: 449 were me (71.4%; mean age, 56.8 �
5.17 years) and 180 women (28.6%; mean age, 64.1 � 14ears). Of these patients, 507 (80.7%) were operated on be-ause of aneurysms and 124 (19.3%) because of dissection.
Thirty-nine patients (4.9%), with a mean age of 72.6 �
.6 years and range of 36.6 to 82.1 years, had microscopic0003-4975/08/$34.00doi:10.1016/j.athoracsur.2008.07.039
by on June 13, 2013 als.org

emaodob
bT(dntapdtawrpg
raSai((Iap
HTcdcstsM
cd
taawbsgm
cistahcshsfi
FCp2tqceb
R
HHd
T
P
P
C
T
LD
1519Ann Thorac Surg PACINI ET AL2008;86:1518–23 THORACIC INFLAMMATORY AORTOPATHIES
AD
ULT
CA
RD
IAC
vidence of active aortitis. There were 24 women (61.5%;ean age, 73.7 � 10.7 years) and 15 men (38.5%; mean
ge, 72.4 � 8.2 years). Thirty-four (87.2%) were operatedn because of aneurysms and 5 (12.8%) because ofissection (3 type A and 2 type B). Informed consent wasbtained from all patients, and the study was approvedy the institutional review board.In all cases, the diagnosis of aortitis was made on the
asis of histopathologic findings, and was incidental.wo patients were affected by connective tissue disorders
systemic lupus erythematosus [SLE] in 1 and Behçet’sisease in the other). In one 48-year-old woman, fever,ights sweats, weight loss, decreased pulses in the ex-
remities, and malaise were present. In another patient,ntitreponemal antibodies were positive. In the other 35atients, no signs or symptoms of systemic inflammatoryisease were present at the time of the operation, nor was
here a history of giant cell temporal arteritis, Takayasurteritis, or systemic vasculitis. Before surgery, patientsere evaluated by computed tomography (CT), magnetic
esonance imaging (MRI), or echocardiography. In allatients, the preoperative CT scan or MRI did not sug-est inflammatory aortic disease.The aneurysmal disease mainly involved the aortic
oot plus the ascending aorta (21 patients, 53.8%) and thescending aorta plus the aortic arch (9 patients, 23.1%).ix patients (15.4%) had diffuse involvement of the entireorta (ascending, arch, descending, and abdominal), andn 2 (5.1%) the aneurysm was limited to the thoracic aortaascending, arch, and descending aorta). One patient2.6%) had an aneurysm only of the aortic arch (Table 1).n all patients we performed total replacement of dilatedortic tracts. The extent of the repair and the associatedrocedures performed are shown in Table 2.
istologic Examinationhe aortic specimens available for histologic examinationonsisted of 34 ascending aorta, 3 arch, and 2 thoracicescending segments. All specimens, ranging from 5 to 10m, were fixed in formalin and embedded in paraffin, andix to eight samples were taken from each case and rou-inely processed. For histologic examination, 2-�m-thickections were cut and stained with hematoxylin and eosin,
allory trichrome, and elastic Weigert–Van Gieson.The cases of aortitis were classified as noninfective (giant
ell arteritis, Takayasu arteritis, aortitis of collagen vascular
able 1. Extension of Aortic Dilatation at Surgery
Involvement ExtensionNo. of
Patients Percent
ocal Ascending aorta 21 53.8iffuse Ascending aorta � arch 9 23.1
Ascending aorta � arch� descending aorta
2 5.1
Ascending aorta � arch� descending aorta� abdominal aorta
6 15.4
Arch 1 2.6
isease, inflammatory aneurysms, and sarcoidosis) or infec-Ag
ats.ctsnetjournDownloaded from
ive (syphilitic aortitis, tuberculosis, and pyogenic aortitis),s reported by Virmani and Burke [1]. For the cases withpparent lymphoplasmacytic aortitis, additional sectionsere prepared from three deeper levels in the paraffinlocks to evaluate the presence of giant cells more exten-ively. Takayasu arteritis and giant cell aortitis were distin-uished according to patient age and the presence of two orore established clinical criteria [11–13].According to a semiquantitative evaluation of the per-
entage of the entire length of the microscopic aortic wallnvolved, the extent of inflammatory infiltrates was con-idered as slight (one third of the surface), moderate (twohirds of the surface), or severe (the whole aortic wall). Inddition, on the basis of the predominance of active orealing lesions in the aortic wall, the inflammatory pro-ess was defined as active phase (prevalence of wide-pread inflammatory infiltrates, necrosis, and edema) orealing or healed phase (prevalence of medial fibrouscarring, fragmentation and disruption of medial elasticbers, fibrointimal thickening, and adventitial scarring).
ollow-Uplinical follow-up was available for all 35 dischargedatients and ranged from 26 to 125 months (mean, 52 �8 months). Information was obtained by examination ofhe patients or by communication (telephone or maileduestionnaire) with the patients or their referring physi-ians as well as from the CT, MRI, and echocardiographicvaluations carried out. All patients were followed eithery CT scan, MRI, or echocardiography.
esults
istopathologic Featuresistologically, cases of noninfectious aortitis were pre-ominant (38 of 39 patients, 97.4%): 30 cases of giant cell
able 2. Operative Procedures
rocedureNo. of
Patients Percent
rincipalAscending aorta replacement 20 51.3Arch replacement 17 43.6Hemiarch � ascending replacement 11Arch � ascending aorta replacement 4Isolated arch replacement 1Ascending � arch � descending
aorta replacement1
Descending aorta replacement 1 2.6Thoracoabdominal aorta
replacement1 2.6
oncomitantBentall 18 46.2CABG 7 17.9AVR 7 17.9Valve sparing 3 7.7MVR 1 2.6
VR � aortic valve replacement; CABG � coronary artery bypassrafting; MVR � mitral valve replacement.
by on June 13, 2013 als.org
ayiac2wymw
l
danatT
ia
((
Fe(ocmcmtnlm
FtW�tW�
1520 PACINI ET AL Ann Thorac SurgTHORACIC INFLAMMATORY AORTOPATHIES 2008;86:1518–23A
DU
LTC
AR
DIA
C
ortitis (GCA; 76.9%; 20 women; median age, 75.9 � 5.3ears; and 10 men; median age, 74.9 � 3.9 years), 3nflammatory aneurysms (7.7%, 2 men; 1 woman; mediange, 75.1 � 3.3 years), 2 cases of aspecific lymphoplasma-ellular aortitis (5.1%, 1 woman; 1 male; median age, 60 �2.6 years), 1 Takayasu aortitis (2.6%, 48-year-oldoman), 1 SLE-associated aortitis (2.6%, woman aged 55
ears), and 1 Behçet’s disease–associated aortitis (2.6%,an aged 23 years). The only case of infectious aortitisas syphilitic aortitis (2.6%, man aged 60 years).The inflammatory infiltrates consisted in all cases of
ymphocytes, monocytes, and plasma cells, but they
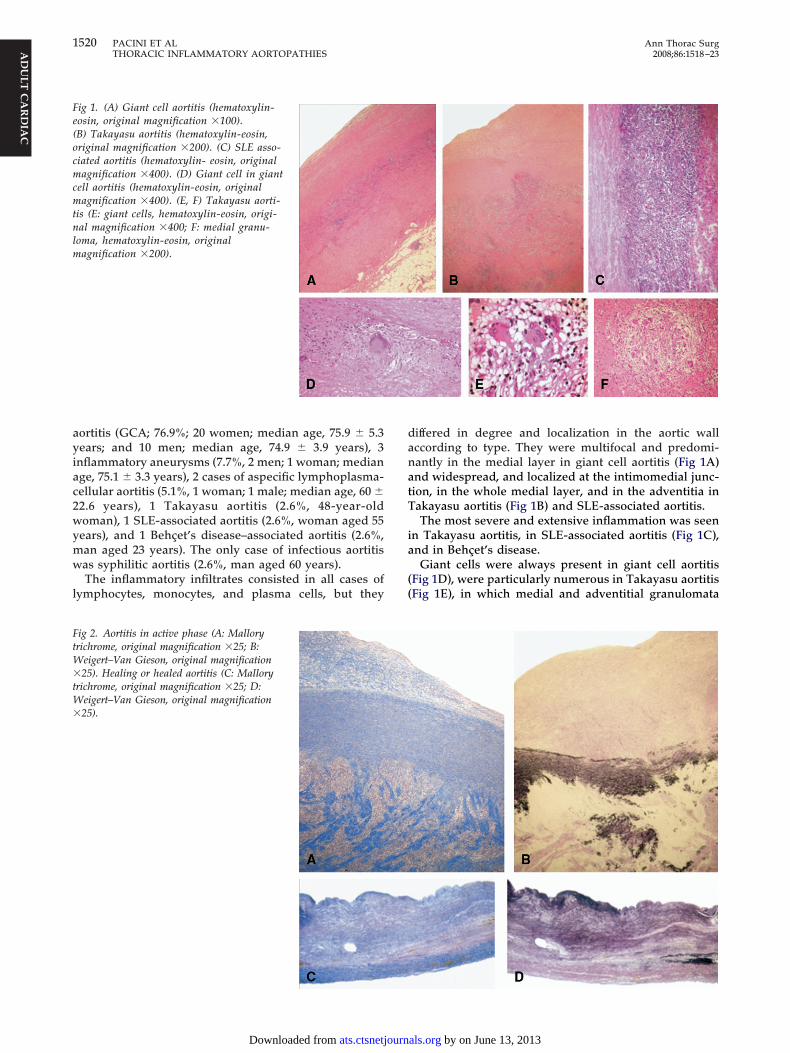
ig 1. (A) Giant cell aortitis (hematoxylin-osin, original magnification �100).B) Takayasu aortitis (hematoxylin-eosin,riginal magnification �200). (C) SLE asso-iated aortitis (hematoxylin- eosin, originalagnification �400). (D) Giant cell in giant
ell aortitis (hematoxylin-eosin, originalagnification �400). (E, F) Takayasu aorti-
is (E: giant cells, hematoxylin-eosin, origi-al magnification �400; F: medial granu-
oma, hematoxylin-eosin, originalagnification �200).
ig 2. Aortitis in active phase (A: Malloryrichrome, original magnification �25; B:
eigert–Van Gieson, original magnification25). Healing or healed aortitis (C: Mallory
richrome, original magnification �25; D:eigert–Van Gieson, original magnification25).
ats.ctsnetjournDownloaded from
iffered in degree and localization in the aortic wallccording to type. They were multifocal and predomi-antly in the medial layer in giant cell aortitis (Fig 1A)nd widespread, and localized at the intimomedial junc-ion, in the whole medial layer, and in the adventitia inakayasu aortitis (Fig 1B) and SLE-associated aortitis.The most severe and extensive inflammation was seen
n Takayasu aortitis, in SLE-associated aortitis (Fig 1C),nd in Behçet’s disease.Giant cells were always present in giant cell aortitis
Fig 1D), were particularly numerous in Takayasu aortitisFig 1E), in which medial and adventitial granulomata
by on June 13, 2013 als.org

wd
piaoah
wTss
SE
tpdarurcmuaowae
2tcbcmcs
lqL
wom8rdpfauwagiflmludwovapTo
aaaFe
C
Id
F
F
1521Ann Thorac Surg PACINI ET AL2008;86:1518–23 THORACIC INFLAMMATORY AORTOPATHIES
AD
ULT
CA
RD
IAC
ere also present (Fig 1F), and were scattered in Behçet’sisease.All cases of inflammatory aortic aneurysms showed com-
lex atherosclerotic plaque, severe parietal inflammatorynfiltrates, attenuated media with extensive fibrous scarringnd elastic fiber disruption, and severe fibrous thickeningf periadventitial tissue. The inflammatory process wasctive (Fig 2A, 2B) in 19 patients (48.7%) and healing orealed (Fig 2C, 2D) in 20 patients (51.3%).Apart from the aortic inflammatory process, patientsith SLE and Behçet’s disease had systemic involvement.he patient with Takayasu disease showed systemicymptoms. None of the GCA patients presented anyystemic clinical features.
urgical AnalysisARLY RESULTS. Four patients (10.3%) died after the opera-ion. The causes of hospital death were a stroke in 2atients (5.1%), bleeding in 1 patient (2.6%), and myocar-ial failure in 1 patient (2.6%). Three of these 4 had GCAnd 1 had SLE. Two patients with GCA underwent aorticoot replacement with composite valve graft, and bothnderwent an associated procedure: 1 had a mitral valveeplacement and died of bleeding, the other underwentoronary artery bypass grafting and hemiarch replace-ent and died of cardiac failure. The third patient
nderwent ascending aorta and hemiarch replacementssociated with coronary artery bypass grafting, and diedf a stroke. The patient with SLE was a 55-year-oldoman, who underwent composite valve replacement
nd hemiarch replacement and died on the 10th postop-rative day of a stroke.Neurologic complications occurred in 4 patients (10.3%):patients had a fatal stroke and 2 had transitory dysfunc-
ions that were completely resolved before hospital dis-harge. Three patients (7.7%) required rethoracotomy, 2 forleeding and 1 for sternal osteomyelitis. Cardiac compli-ations occurred in 3 patients (2 myocardial failures, 1yocardial ischemia), and postoperative renal insuffi-
iency requiring dialysis in 2 (5.1%). The patient with
ig 3. Actuarial survival for the entire cohort of patients.
yphilitic aneurysm of the aortic arch had severe venti- d
ats.ctsnetjournDownloaded from
atory insufficiency owing to tracheomalacia that re-uired stenting of the trachea and the main bronchi [14].ATE RESULTS. The follow-up of the 35 discharged patientsas 100% complete. No patient underwent corticosteroidr immunosuppressive therapy after diagnosis of inflam-atory aortic disease. The actuarial survival rate was
0.7% � 6.7% and 47.1% � 20.6% at 5 and 10 years,espectively (Fig 3). There were 5 late deaths (14.3%)uring follow-up. Cause of death was unknown in 1atient, stroke in 1, renal carcinoma in 1, myocardial
ailure in 1, and rupture of an unidentified abdominalorta aneurysm in 1. One patient with GCA died ofnknown cause 2 years after the operation. One patient,ho underwent surgery for ascending aorta and total
rch replacement associated with coronary artery bypassrafting, died of a stroke 3 months later: he had an
nflammatory aneurysm. One other patient with an in-ammatory aneurysm died of renal carcinoma with pul-onary metastases. One patient with GCA died 5 years
ater of hemorrhagic shock, owing to rupture of annrecognized abdominal aorta aneurysm. The fifth lateeath was a 24-year-old man affected by Behçet’s diseaseho underwent a Bentall procedure: he underwent re-peration after 3 years for detachment of the compositealve graft from the aortic annulus, and then underwentsecond reoperation for pseudoaneurysm owing to com-lete detachment of the coronary arteries from the graft.he patient died of cardiac failure 7 years after the initialperation.Thirty patients (76.9%) were alive at the latest check-up
nd are in good health. One patient (2.6%) underwentortic repair for development of a new aneurysm in thebdominal tract of aorta, 2 years after the first operation.reedom from reoperation or recurrent aneurysmal dis-ase on the remaining aorta is shown in Figure 4.
omment
n our extensive surgical population (n � 788), the inci-ence of inflammatory aortic disease was 4.9%: this
ig 4. Actuarial freedom from reoperation or recurrent aneurysmal
isease on the remaining aorta.by on June 13, 2013 als.org

fidapa
mtnm
(tdT
a(smfp
aadprfhaea
awewietwsm
otcssastot
aaPtc
esevftanIdrtcpfw
trpoHd
vaohar2epi
tmeBtcrlnloabptg
eir8aodo
1522 PACINI ET AL Ann Thorac SurgTHORACIC INFLAMMATORY AORTOPATHIES 2008;86:1518–23A
DU
LTC
AR
DIA
C
gure is rare but not exceptionally so. This result isifferent from the data (9% aortitis) reported by Hommend coworkers [8] in their recent paper regarding 513atients with surgically resected ascending aorticneurysms.In our study, women were affected slightly more thanen (61.5% versus 38.5%); in most of the data reported in
he literature women were more frequently or predomi-antly affected (2:1 to 4:1), although a higher incidence inen [5] has also been reported.The mean age of our population was relatively high
72.6 � 9.6 years), as reported by other authors [6, 15, 16];he youngest patients were affected by collagen syn-romes such as SLE and Behçet’s disease as well as byakayasu syndrome.Our histopathologic results showed that noninfective
ortitis is now much more frequent than infective forms97.4% versus 2.6%). Among the noninfectious forms, ouramples confirm that GCA (66.6% of these cases) is theost frequent histopathologic diagnosis (76.9%), as
ound by others [4, 6, 10, 15], especially among femaleatients (66.5%) [1].Moreover, among the 38 patients with noninfective
ortitis, the majority (36 patients, 92.3%) had isolatedortitis: in these patients, neither evidence of systemicisease nor known history of temporal arteritis wasresent at the time of surgery. In the literature, the dataegarding the percentage of isolated aortitis vary widely,rom 25% to 94.7% [5, 15–18]: as in our population, theigh percentage of this type of disease is partly attribut-ble to a less than exhaustive investigation of the pres-nce of systemic inflammatory disease. It is clear that inlarge group of patients aortitis is a localized disease.In the majority of our patients, the morphologic alter-
tions were in an advanced phase at the time of surgery,ith severe and widespread lesions in 74.4% of cases, and
ven more severe in female patients, who also showedidespread destruction of the aortic wall. Inflammatory
nfiltrates were present in all specimens, and they werextensive and moderate to severe in 80% of cases, par-icularly in aortitis associated with collagenopathies andith inflammatory aneurysms, in which all cases showed
evere infiltrates. However, in 20 (51.3%) patients inflam-ation was associated with healing aspects.These pathologic features are the cause of weakening
f the aortic wall and of aneurysm formation and evolu-ion. The near-complete disruption of the medial elasticomponent may induce rupture and dissection, even inmall aneurysms. Evans and associates [19] reported aeries of 9 patients, 4 (44%) of whom died suddenly ofortic dissection. Other authors cited a high proportion ofpecimen diagnoses made from ruptured aortic autopsyissue rather than from surgical specimens [17, 20, 21]. Inur patients, aortic dissections were less frequent than inhe literature: 5 (12.8%) of 39 patients.
The extension of both the aortic aneurysm and theortic replacement was limited to the ascending aortand the aortic arch in the majority of patients (76.9%).atients with GCA had a higher rate of involvement of
he proximal part of the thoracic aorta (90%). In these
ases, the Bentall operation is the treatment of choice pats.ctsnetjournDownloaded from
ven though the aortic valve cusps are usually macro-copically normal and histologic examination shows novidence of inflammatory process [22, 23]. The aorticalve could therefore be safely preserved in patients withunctionally normal valve leaflets. We mainly performedhe Bentall procedure (18 patients), but in 3 cases we did
valve-sparing operation according to the David tech-ique and none of the latter group required reoperation.
n aortitis, the more hemostatic reimplantation proce-ure should be preferred to remodeling to reduce theisk of bleeding from the proximal suture line. In fact, inhe case of inflammatory involvement, the aortic tissuean be fragile, leading to tearing of the suture line. Oneatient died of uncontrollable bleeding owing to a very
ragile aorta even though the suture lines were reinforcedith a Teflon felt strip.In our experience, surgical results of aortic repair seem
o be worse in inflammatory aneurysms than in aneu-ysms caused by other pathologic processes. In theresent series, the mortality rate was 23.1%, although inur overall experience it was approximately 10% [24–26].owever, these are not risk-adjusted populations andefinitive conclusions cannot be made.The incidence of neurologic complications (10.3%) was
ery high in this subgroup of patients who underwentortic surgery. Two patients experienced a stroke and 2thers had temporary neurologic dysfunction. So far weave performed more than 250 repairs of the thoracicorta for various diseases using antegrade selective ce-ebral perfusion, and we have had only 4 cases of stroke:
of these were affected by aortitis [24]. We cannotxplain this high rate of neurologic complications, but aossible explanation may be that it is related to specific
nflammatory disease.Surgical repair is important in aortitis and lifesaving in
he short term, but prognosis and treatment is deter-ined by the underlying cause of disease and pathologic
xamination may aid in clarifying the diagnosis [27].ecause of the worse results obtained and also because of
he aortic wall weakness we found in these patients, weould speculate that, in the case of inflammatory aneu-ysms, the elective treatment could be performed at aesser diameter than in noninflammatory ones. Unfortu-ately, the preoperative diagnosis is very hard: the radio-
ogic imaging (CT and MRI) did not show any suggestionf inflammatory disease. Owing to the fact that preoper-tive diagnosis is difficult and the incidence of aortitis isy no means negligible, it would be useful to routinelyerform a preoperative measurement of C-reactive pro-
ein and erythrosedimentation rate in all patients under-oing aortic surgery.During the follow-up, according to the CT and MRI
xaminations, there was a minimal growth of the remain-ng aorta. The freedom from aortic reoperation or recur-ent aneurysmal disease was 93.4% � 4.5% at 5 years and1.7% � 11.6% at 10 years. Two patients exhibited a newneurysm, both at the abdominal tract of the aorta; 1 wasperated on 2 years after the first operation, the otheried of abdominal aorta rupture 5 years after the firstperation. Both patients were affected by GCA. The
atient with Behçet’s disease underwent two reopera-by on June 13, 2013 als.org

tdamsrimHinnv
mteitp
soMphitciaams
eiwgPoohbrpit
R
1
1
1
1
1
1
1
1
1
1
2
2
2
2
2
2
2
2
2
2
1523Ann Thorac Surg PACINI ET AL2008;86:1518–23 THORACIC INFLAMMATORY AORTOPATHIES
AD
ULT
CA
RD
IAC
ions: one for prosthetic valve detachment and one foretachment of the coronary arteries. In patients withortitis syndrome, paravalvular leakage or valve detach-ent and anastomotic false aneurysm are the most
erious and frequent complications [28]. The major factoresponsible for the high incidence of these complicationss persistent inflammation. For this reason, adequate
onitoring of inflammation is extremely important.owever, the inflammation is sometimes difficult to
dentify before surgery, or in other cases surgery isecessary during the active phase. Special surgical tech-iques are required in such patients to prevent paraval-ular leakage or prosthetic graft detachment.Histopathologic examination of surgical aortic speci-ens is very important, because it not only can identify
he presence of inflammatory disease but also providesvidence of aortic inflammation activity and defines thenfectious or noninfectious etiology, which is importanto adopt an appropriate antimicrobial or immunosup-ressive therapy [16, 27].Medical treatment of aortitis consists mainly of cortico-
teroids, but there is no consensus on the dose or durationf steroid treatment after a histologic diagnosis of arteritis.ost physicians recommend steroid treatment in the active
hase of the disease. Prolonged steroid treatment has,owever, been known to affect the connective tissues by
nhibiting chondroitin sulfate and formation of granulationissue, and would probably influence the disintegration ofonnective tissue of the media aggravated by steroid-nduced long-standing hypertension [29]. Further studiesre required to define the utility of medical treatment inortitis, particularly the optimal immunosuppressive regi-en. No patient in our population was treated with either
teroid or immunosuppressive therapy.During surgery of the thoracic aorta, an inflammatory
tiology of aneurysms is found in almost 5% of cases. Thenflammatory process is in a histologically advanced phaseith active lesions, often with systemic involvement. Sur-ery can be associated with high morbidity and mortality.harmacologic therapy, which is so often forgotten becausef the absence of a histopathologic diagnosis, can be basedn steroid and immunosuppressive drugs. In addition, theigh incidence of diffuse aortic involvement and the possi-ility of further, long-lasting development of new aneu-ysms in different aortic tracts call for close monitoring ofatients by CT and MRI. Histologic examination is an
mportant diagnostic tool in aortic surgery, as it is relevanto both short-term and long-term results.
eferences
1. Virmani R, Burke AP. Nonatherosclerotic diseases of theaorta and miscellaneous diseases of the main pulmonaryarteries and large veins. In: Silver MD, Gotlieb AI, Schoen FJ,eds. Cardiovascular Pathology. Philadelphia, PA: ChurchillLivingstone, 2001:119–37.
2. Ueda H, Morooka S, Ito I, Yamaguchi H, Takea T. Clinicalobservation of 52 cases of aortitis syndrome. Jpn Heart J
1969;10:277–88.ats.ctsnetjournDownloaded from
3. Huston KA, Hunder GG, Lie JT, Kennedy RH, Elveback LR.Temporal arteritis: a 25-year epidemiologic, clinical, andpathologic study. Ann Intern Med 1978;88:162–70.
4. Bickerstaff LK, Pairolero PC, Hollier LH, et al. Thoracic aorticaneurysms: a population-based study. Surgery 1982;92:1103–8.
5. Pomerance A, Yacoub MH, Gula G. The surgical pathologyof thoracic aorta aneurysms. Histopathology 1977;1:257–76.
6. Rojo-Leyva F, Ratliff NB, Cosgrove DM, Hoffman GS. Studyof 52 patients with idiopathic aortitis from a cohort of 1204surgical cases. Arthritis Rheum 2000;43:901–7.
7. Klima T, Spjut HJ, Coelho A, et al. The morphology ofascending aortic aneurysms. Hum Pathol 1983;14:810–7.
8. Homme JL, Aubry MC, Edwards WD, et al. Surgical pathol-ogy of the ascending aorta: a clinicopathologic study of 513cases. Am J Surg Pathol 2006;30:1159–68.
9. Walker DI, Bloor K, Williams G, Gillie I. Inflammatoryaneurysms of the abdominal aorta. Br J Surg 1972;59:609–14.
0. Rasmussen TE, Hallett JW Jr. Inflammatory aortic aneu-rysms. A clinical review with perspectives in pathogenesis.Ann Surg 1997;225:155–64.
1. Sharma BK, Jain S, Suri S, Numano F. Diagnostic criteria forTakayasu arteritis. Int J Cardiol 1996;54(Suppl 1):S141–7.
2. Weyand CM, Goronzy JJ. Pathogenic principles in giant cellarteritis. Int J Cardiol 2000;75(Suppl 1):S9–15.
3. Weyand CM, Goronzy JJ. Pathogenic mechanisms in giantcell arteritis. Cleve Clin J Med 2002;69(Suppl 2):S28–32.
4. Pacini D, Mattioli S, Di Simone MP, et al. Syphilic aorticaneurysm: a rare case of tracheomalacia. J Thorac Cardio-vasc Surg 2003;126:900–2.
5. Miller DV, Isolato PA, Weyand CM, Edwards WD, AubryMC, Tazelaar HD. Surgical pathology of non-infectiousascending aortitis: a study of 45 cases with emphasis on anisolated variant. Am J Surg Pathol 2006;30:1150–8.
6. Kerr LD, Chang YJ, Spiera H, Fallon JT. Occult active giantcell aortitis necessitating surgical repair. J Thorac CardiovascSurg 2000;120:813–5.
7. Lie JT. Aortic and extracranial large vessel giant cell arteritis:a review of 72 cases with histopathologic documentation.Semin Arthritis Rheum 1995;24:422–31.
8. Liu G, Shupak R, Chiu BK. Aortic dissection in giant-cellarteritis. Semin Arthritis Rheum 1995;25:160–71.
9. Evans JM, O’Fallon WM, Hunder GG. Increased incidence ofaortic aneurysm and dissection in giant cell (temporal) arteritis:a population based study. Ann Int Med 1995;122:502–7.
0. Evans JM, Bowels CA, Bjornsson J, Mullany CJ, Hunder GC.Thoracic aortic aneurysm and rupture in giant cell arteritis, adescription study of 41 cases. Arthritis Rheum 1994;37:1539–47.
1. Petursdottir V, Nordborg E, Nordborg C. Atrophy of theaortic media in giant cell arteritis. APMIS 1996;104:191–8.
2. Gelsomino S, Romagnoli S, Gori F, et al. Annuloaortic ectasiaand giant cell arteritis. Ann Thorac Surg 2005;80:101–5.
3. Zehr KJ, Mathur A, Orszulak TA, Mullany CJ, Schaff HV.Surgical treatment of ascending aortic aneurysms in patientswith giant cell aortitis. Ann Thorac Surg 2005;79:1512–7.
4. Pacini D, Leone A, Di Marco L, et al. Antegrade selectivecerebral perfusion in thoracic aorta surgery: safety of mod-erate hypothermia. Eur J Cardiothorac Surg 2007;31:618–22.
5. Ergin MA, Galla JD, Lansman SL, Quintana C, Bodian C,Griepp RB. Hypothermic circulatory arrest in operation of thethoracic aorta: determinants of operative mortality and neuro-logical outcome. J Thorac Cardiovasc Surg 1994;107:788–99.
6. Kazui T, Yamashita K, Washiyama N, et al. Usefulness ofanterograde cerebral perfusion during aortic arch opera-tions. Ann Thorac Surg 2002;74(Suppl):S1806–9.
7. Mohan N, Kerr G. Aortitis. Curr Treat Options CardiovascMed 2002;4:247–54.
8. Kotsuka Y, Tanaka O, Takamoto S, Furuse A. Intravalvularimplantation technique for aortic valve replacement in aor-titis syndrome. Ann Thorac Surg 1999;67:89–92.
9. Takagi H, Mori Y, Iwata H, et al. Non dissecting aneurysm ofthe thoracic aorta with arteritis in systemic lupus erythem-
atosus. J Vasc Surg 2002;35:801–4.by on June 13, 2013 als.org

DOI: 10.1016/j.athoracsur.2008.07.039 2008;86:1518-1523 Ann Thorac Surg
Giuseppe Nicola Martinelli and Roberto Di Bartolomeo Davide Pacini, Ornella Leone, Simone Turci, Nicola Camurri, Francesca Giunchi,
AortopathiesIncidence, Etiology, Histologic Findings, and Course of Thoracic Inflammatory
& ServicesUpdated Information
http://ats.ctsnetjournals.org/cgi/content/full/86/5/1518including high-resolution figures, can be found at:
References http://ats.ctsnetjournals.org/cgi/content/full/86/5/1518#BIBL
This article cites 28 articles, 8 of which you can access for free at:
Citations
shttp://ats.ctsnetjournals.org/cgi/content/full/86/5/1518#otherarticleThis article has been cited by 5 HighWire-hosted articles:
Subspecialty Collections
http://ats.ctsnetjournals.org/cgi/collection/great_vessels Great vessels
following collection(s): This article, along with others on similar topics, appears in the
Permissions & Licensing
[email protected]: orhttp://www.us.elsevierhealth.com/Licensing/permissions.jsp
in its entirety should be submitted to: Requests about reproducing this article in parts (figures, tables) or
Reprints [email protected]
For information about ordering reprints, please email:
by on June 13, 2013 ats.ctsnetjournals.orgDownloaded from




















