
Friedreich's ataxia: Electrophysiologic and histologic findings in patients and relatives
13
Peripheral nerve conduction velocity and cortical evoked potentials were investigated in 48 patients with Friedreich’s disease and in 35 relatives. There were 14 patients and 2 relatives who underwent sural nerve biopsy. Inthe patients sensory conductionvelocity was moderately slowed, whereas sensory responses were markedly reduced. Nerve biopsy showed a severe loss of large myelinated fibers and no demyelination. On teased nerve fiber preparations, most fibers presented uniformly short internodes. No corre- lation was seen between sensory conduction findings or histologic abnor- malities and clinical disability. In patients SSEP changes, which were constant, and VEPs, which were frequently involved, were unrelated to the severity or duration of clinical disability. There were 14 relatives who showed clinical signs of Friedreich’s dis- ease. Slightly decreased distal conduction velocity along sensory fibers was observed in more than half of the relatives. Nerve biopsy was noncontrib- utory. In conclusion, we could not determine whether the abnormalities ob- served in the siblings were an expression of a heterozygotic condition, or whether they were early signs of the disease. MUSCLE & NERVE 10503-515 1987 FRIEDREICH’S ATAXIA: ELECTROPHYSIOLOGIC AND HISTOLOGIC FINDINGS IN PATIENTS AND RELATIVES G. CARUSO, MD, L. SANTORO, MD, A. PERRETTI, MD, R. MASSINI, MD, L. PELOSI, MD, C. CRISCI, MD, M. RAGNO, MD, G. CAMPANELLA, MD, and A. FILLA, MD Even though more than a century has passed since the first description of Friedreich’s ataxia,“ the dis- ease is still a “fascinating p~zzle.”~ Despite numer- ous studies, little is known on the relationship be- tween the obscure basic biocheniical defect and the pathology underlying the clinical and electrophys- iologic abnormalities that involve the central and peripheral nervous system. The disorder, which because of its complexity Barbeau5 prefers to call Friedreich’s disease rather than Friedreich’s ataxia, is a hereditary degenera- tive ataxia with a recessive autosomal transmission From the Department of Clinical Neurophysiology and the Neurologic Clinic of the 2nd School of Medicine. University of Naples, and the Fon- dazione Clinica del Lavoro. Campoli M T , Italy. Address reprint requests to Dr Caruso at the Department of Clinical Neu- rophystology, 2nd School of Medicine. University of Naples, Naples, Italy. Presented at the International Symposium of Peripheral Nerve Diseases, 32nd Annual Meeting of the American Association of Electromyography and Electrodiagnosis. Las Vegas, NV, October 1985 Accepted for publication August 21. 1986 ‘ 1987 John Wiley & Sons 0148-639X/1006/0503 $04.00/13 probably resulting from a genetic heterogeneity with a common phenotype.51 Friedreich’s ataxia appears in infancy or in ad- olescence and progresses slowly without remission. It is clinicallycharacterized by some “obligatory signs” for diagnosis that appear very early and that usu- ally remain stable, such as impairment of deep- tendon reflexes and disorders of vibratory sense and others such as dysarthria, gait ataxia, and py- ramidal signs that appear later and progress with time. Pes cuuus, kyphoscoliosis, and cardiologic ab- normalities are also frequent. The posterior- and lateral columns of the spinal cord are degenerated, and there is degeneration with secondary dernye- lination of the large myelinated sensory fibers of peripheral nerve^.^"^^^^^^ There is no definite evidence of a specific en- zymatic deficiency, even though several biochenii- cal abnormalities have been described, and Barbeau5 holds that the main problem in Friedreich’s ataxia involves taurine transport. Indeed significant dif- ferences have been observed between Friedreich’s ataxia patients and controls regarding the pyruvate response to glucose and serum bilirubin lev- Friedreich’s Ataxia MUSCLE & NERVE Jul/Aug 1987 503
-
Upload
independent -
Category
Documents
-
view
3 -
download
0
Transcript of Friedreich's ataxia: Electrophysiologic and histologic findings in patients and relatives

Peripheral nerve conduction velocity and cortical evoked potentials were investigated in 48 patients with Friedreich’s disease and in 35 relatives. There were 14 patients and 2 relatives who underwent sural nerve biopsy.
In the patients sensory conduction velocity was moderately slowed, whereas sensory responses were markedly reduced. Nerve biopsy showed a severe loss of large myelinated fibers and no demyelination. On teased nerve fiber preparations, most fibers presented uniformly short internodes. No corre- lation was seen between sensory conduction findings or histologic abnor- malities and clinical disability.
In patients SSEP changes, which were constant, and VEPs, which were frequently involved, were unrelated to the severity or duration of clinical disability.
There were 14 relatives who showed clinical signs of Friedreich’s dis- ease. Slightly decreased distal conduction velocity along sensory fibers was observed in more than half of the relatives. Nerve biopsy was noncontrib- utory. In conclusion, we could not determine whether the abnormalities ob- served in the siblings were an expression of a heterozygotic condition, or whether they were early signs of the disease.
MUSCLE & NERVE 10503-515 1987
FRIEDREICH’S ATAXIA: ELECTROPHYSIOLOGIC AND HISTOLOGIC FINDINGS IN PATIENTS AND RELATIVES
G. CARUSO, MD, L. SANTORO, MD, A. PERRETTI, MD, R. MASSINI, MD, L. PELOSI, MD, C. CRISCI, MD, M. RAGNO, MD, G. CAMPANELLA, MD, and A. FILLA, MD
Even though more than a century has passed since the first description of Friedreich’s ataxia,“ the dis- ease is still a “fascinating p ~ z z l e . ” ~ Despite numer- ous studies, little is known on the relationship be- tween the obscure basic biocheniical defect and the pathology underlying the clinical and electrophys- iologic abnormalities that involve the central and peripheral nervous system.
The disorder, which because of its complexity Barbeau5 prefers to call Friedreich’s disease rather than Friedreich’s ataxia, is a hereditary degenera- tive ataxia with a recessive autosomal transmission
From the Department of Clinical Neurophysiology and the Neurologic Clinic of the 2nd School of Medicine. University of Naples, and the Fon- dazione Clinica del Lavoro. Campoli M T , Italy.
Address reprint requests to Dr Caruso at the Department of Clinical Neu- rophystology, 2nd School of Medicine. University of Naples, Naples, Italy.
Presented at the International Symposium of Peripheral Nerve Diseases, 32nd Annual Meeting of the American Association of Electromyography and Electrodiagnosis. Las Vegas, NV, October 1985
Accepted for publication August 21. 1986
‘‘ 1987 John Wiley & Sons 01 48-639X/1006/0503 $04.00/13
probably resulting from a genetic heterogeneity with a common phenotype.51
Friedreich’s ataxia appears in infancy or in ad- olescence and progresses slowly without remission. It is clinically characterized by some “obligatory signs” for diagnosis that appear very early and that usu- ally remain stable, such as impairment of deep- tendon reflexes and disorders of vibratory sense and others such as dysarthria, gait ataxia, and py- ramidal signs that appear later and progress with time. Pes cuuus, kyphoscoliosis, and cardiologic ab- normalities are also frequent. The posterior- and lateral columns of the spinal cord are degenerated, and there is degeneration with secondary dernye- lination of the large myelinated sensory fibers of peripheral nerve^.^"^^^^^^
There is no definite evidence of a specific en- zymatic deficiency, even though several biochenii- cal abnormalities have been described, and Barbeau5 holds that the main problem in Friedreich’s ataxia involves taurine transport. Indeed significant dif- ferences have been observed between Friedreich’s ataxia patients and controls regarding the pyruvate response to glucose and serum bilirubin lev-
Friedreich’s Ataxia MUSCLE & NERVE Jul/Aug 1987 503

Moreover. Friedreich's ataxia patients show els.". It;.!!!)
a marked deficiency in linoleic acid in both plasma and high-densit y lipoproteins, 12.2 L,30,3 I an abnor- ma1 excretion o f taurine and &aIani~ie , ' . '~ .~~ and decreased niitochondrial malic enzyme activity in fi brohlasts 'rJ-'7 and in skeletal muscles.'",23 En- hanced :irachidonic acid levels (20:4) in total serum colestei-yl esters and in phospholipids has been ob- servetl b y us (uripublished data) in patients with only minor moclihcations of 18:2.
In this paper we summarize the electrophysio- logic and histologic findings accumulated within the framework of a large cooperative study that began in 1974. T h e aim of the study is to under- stand the underlying pathologic factors in patients with Friedreich's ataxia and to characterize the het- el-ozygotic condition in relatives.
ABSENCE OF TENDON REFLEXES
ONSET BEFORE AGE 20
PROGRESSIVE ATAXIA
MATERIAL
The Patients. From 38 fandies 48 patients (28 males and 20 females) were carefully selected according to the criteria of the Quebec Cooperative Study of Friedreich's Parental consanguinity was seen in I 1 cases. There were I S patients who underwent only one clinical examination; 15 pa- tients were followed for 2 years, 10 patients for 2-4 years, and 10 patients for 4-9 years.
At the time of the first observation, the patients were 9-44 years of age (average 22.3 years) with a duration of symptoms and signs from 1 to 24 years (average 9 years). I n all patients the typical signs of Friedreich's ataxia were well developed (Fig. l ) ,
1 LLU ,'. ' ,,,/
, 1
1
" I
but the severity of the disease was signihcantlv re- lated ( P < 0.001) t o the duration of symptoms. I 'he patients' clinical condition was evaluated with t w o scales: the Inherited Ataxias Progression Scale (IAPS)l6 and the Inlierited Atasias Clinical Rating Scale (IACRS)." The IAPS gives a rating of the patient's general condition according to four stagcs: stage I (asymptomatic patient detected among the siblings o f a known case). stage 11 (symptoms and signs are present, but are mild, and the patient (.;in
conduct an independcnt life, although work is somewhat restricted), stage I1 I (symptoms and signs are completely developed, and the patient, who cannot work, needs constant care), and stage I V (patients are confined to bed o r to a wheelchair). T h e IACRS is based on nine items: speech. t l y h -
metria, gait anti stance ataxia, hypotonia, musculai- strength, deep tendon reflexes, plantar reflex, and vibration sense. A score from 0 (normal) to 4 (highly pathological) is given for each item, and the final rating is the sum of the scores assigned to each item. According to the Inherited Ataxias Progres- sion 2 1 patients were confined to bed or to a wheelchair (stage IV) , 15 were unable to per- form any productive activity (stage 111). and 12 were only slightly disabled (stage 11). In following examinations, i t was found that the patient's per- formance significantly deteriorated in relation to the interval between observations.
N o differences in the severity of clinical clis- ability o r in the progression of' the disturbances were observed between inales and fernales.
0 20 40 60 80 100% t 6 AUTOSOMAL RECESSIVE INHERITANCE
. DECREASED VIBRATORY SENSE
KYPHOSCOLIOSIS 1
DYSARTHRIA 1
EXTENSOR PLANTAR RESPONSE I
DECREASED MUSCLE TONE 1
FIGURE 1. Percent distribution of clinical features in 48 patients with Friedreich's ataxia (white bars) and in 14 of their relatives (shaded bars).
504 Friedreich's Ataxia MUSCLE & NERVE Jul/Aug 1987

The Relatives. There were 14 paretits (7 fathers and 7 mothers) and 2 3 sihliiigs (16 brot1iei.s and 7 sis- ters) w h o underwent clinical esarninations. The parents' ages ranged from 34 t o 54 years (average 47 years), and the siblings' ages rarigetl Ironi 2 t o 29 years (average lti yearc). They were relatives of 13 pitierits and were anaiiinestically judged to he clinically normal. 71'hree additional sub-jeers ( two parents and one sihling ot' three utirelatecl patients) were not included in this material because of tlie possibility of neuropathy induced b y causes othei- than Friecireich's ataxia: alcohol abuse and diabetes niellitus. Lastly, we a l s o excluded two brothers ( 10 and 14 years of age) liecause, although they were described as healthy h y dieir families, they showed rriaiiy of the clinical signs characteristic of Fric- dreich's ataxia (ataxia, kyphoscoliosis, niusc~ul~tr h y - potonia, absence o f deep tendon reflexes, ancl /)P.\
plnn71s) and a slight to moderate degree of' slowing o f niaxiniiini sensory conduction velocity w i t h ;I
severe amplitude tleci-ease of sensoi-y evoked re- sponses.
Among the remaining 35 relatives, objective clinical neurologic signs were observed in a total ot ' 14: in 2 of the 14 parents and i i i 12 01 the 2 I siblings. Figure 1 illustrates the clistribution of tlicsc signs.
METHODS
'The procedures adopted in this study have beeti described in detail elsewhei-c.""' I Here we s1i;ill limited ourselves to a I'ew basic itenis.
Electromyography. The exatmitiation was ]lei.- forrriecl with concentric needle electrodes ( D I S A , 13L3 1) and DISA equipnient (1500 Digital EM(;- System, DISA Elcktroriik A/S, DK-2740 Skovlunde, Deriniark) in the brachial hi(-cps, abductor tligiti niininii, and anterior tibial niuscks according t o the classical procedure proi~osed h y Buchthal. I'
Motor Conduction. With needle electrodes, both for stimulating and recoi-ding. and D I S A equ i 1) me tit , motor conduction velocity was nieasured in the me- dian and tibial nerves. T h e metli;in nci-ve w;is stim- ulated at the wrist and elbow, tlie tibial nerve w;is stimulated at the medial malleolus and popliteal fossa. The evoked muscle potentials were recorded from the abductor pollicis brevis and from tlie ab- ductor hallucis miisc:les. respectively. T h e results were compared with the values obtained in normal age-matched subjects."
Sensory Conduction. Using DISA equipment and the procedure described by Buchthal and Kosen-
falckl" ; i n d Behse m c l Buchth~il. sensory contluc- t io i i velocily was ort1iocIr~~rnic:ally nieasuretl along tlie median, tlie tihial, ancl the s u r a l nerves. Along tlie meclim i nerve velocity was iiie:tsuid from digit 3 to the wrist and I'rom the wrist t o the elbow; along the tibial nerve, \docity w a s ~neasurecl from the I>ig toe t o Ihe medial iiialleolus and from the nie- dial m:illeolus to tlic popliteal t i m a : along the sirral nei-ve. velocity w x measured ti-oni thc cloi.sol:it- era1 aspect of the toot to the latei;il iiialleoliis. I'ixmi
the lateral niallcolus t o tlie sura or to the popliteal fossa, and from tlic sui-a to the popliteal tossa. Also, t licse i.esirlts were u )I I i prcd with values obtiii net1 ii i i i o i m a l subjects of (.oi-i-csi~oiitIing ages.'?
1 1 1 ;rtltlition, in f o u i - patielits iincler general ai i -
aesthesi;i, thc exposed sural nerve w;is examined intrao~~t:i~;itiveIy as previously described, I!' and the resiil ts were compared with those ohtainrtl tl uriiiu-
a. sui-gel.! in subjects with i i o systemic disorders of the peripheral nei-vous
Somatosensory Evoked Potentials. Short 1atenc.y s o - niatosensory cvoked potentials (SSEPs) t o stiiiiu- lation of' the iiictlian nerve at the wrist \%YIY rc- corded tlirougli surf'ice electrodes at Eih's poilit referred to the hand tiorsum, ;it the seventh cer- vical vertebra ((W7) against ;I hand and a mid- front;il I-cfereiice, atitl at the specitic soniatoseiisory area of the hatic1 on the scalp controlateral to the stiniulated side (C3') referred to the ear Iohc. I'eak- to-pe;ik ainplitude and peak latency of EI-11's poiiii, cervical ( N 1 3 wave) , arid scalp ( P I 4 ancl N 2 0 c o n - poiien t s) p( ) t ci i tials were ~rie;isir I-ed . Cent i ' ; ~ I co II-
cluction time \\:IS calculated b y measuring thr. la- te i icy difference between N 13 o f CV7 aiitl N 2 0 of tlie scalp responses. 'I'he clegi-cc of N 2 0 ternpoi-a1 dispersion was calculatecl by evaluating the latency diff'erciic:c between P 14 and the peak on the N 2 0 w;ivc. l'arametei's were coiisitleretl dm)rt i i : i l when they deviated b y more than 3 SDs t'roin i i ic' it i i \.allies obt;iiiiecl in 15 health): age-inatched voluiitcers.
Visual Evoked Potentials. Visual evoked potentials (VEPs) bv checkert)oaid revei.sal pittei-n ( I t i " 15') were recorded from 0 1 and 0 2 o f the 10-20 lntcr- national System against a (:z reference. 'l 'he PI00 componciit latency, its aniplitucle, and its teiiiporal dispersion expressed by the tiiiir. interval hetiveeti N 1 and N:! were evaluated. Wlieii latency and am- plitude deviated by inore than 2.5 SDs atid the temporal dispersion b y more than 2 SDs from the
were corisideretl alinormal. control value (15 s1Il~;ecls 22-23 years o f age), they
Friedreich's Ataxia MUSCLE & NERVE Jul/Aug 1987 505
Brain Stem Auditory Evoked Potentials. The brain stern auditory evoked potentials (BAEPs), induced by 80-dB SL click stimulation (or by 100 in the absence of a clear response), were recorded through surface disc electrodes from C z against the ear lobe homolateral to stimulation. T h e latency of the first five positive peaks and the 1-111, 111-V. and I-V intervals were measured. Results were compared with those obtained in 94 control age-matched sub- jects, and they were considered abnormal when above the C).5'$T confidence limits.
For ;I quantitative evaluation of the variations of the evoked responses, w e arbitrarily assigned one point for each significant latency increase or for each significant increase of interpeak interval and two points for each wave absence (I , I11 and V components).
Nerve Biopsy. I n 6 subjects under general anaes- thesia and in 1 0 under local anaesthesia, the sural nerve was removed in toto .just proximal to the lateral malleolus and prepared for morphometric measurements and for the study of teased fibers according to the technique described by Behse et aI." "' Samples for electron microscopy were pre- pared as previously described."'
RESULTS
hlost of the results obtained in the patients and in their relatives have already been detailed in pre-
vious repoi-ts.'x,''',4' Here we shall summarize our findings while stressing the more relevant aspects.
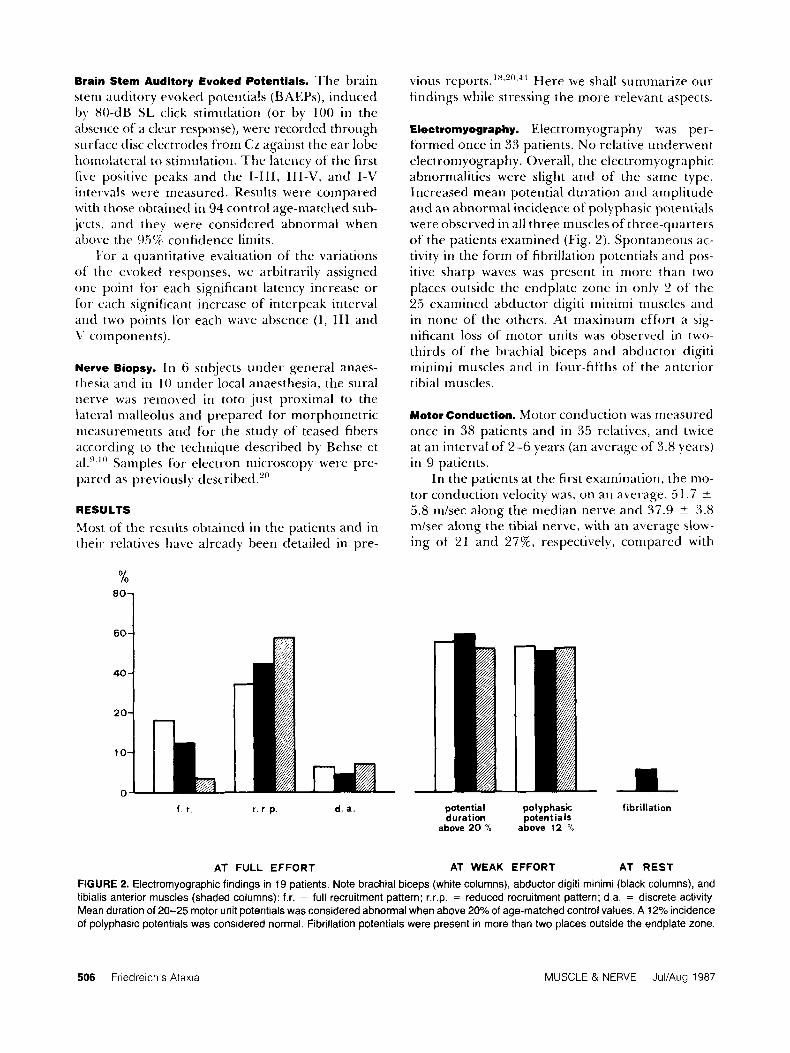
Electromyography. Electromyography was per- formed once in 33 patients. N o relative underwent electromyography. Overall, the electromyographic abnormalities were slight and of the same type. Increased mean potential duration and amplitude and an abnormal incidence of polyphasic potentials were observed in all three muscles of three-quarters of the patients examined (Fig. 2). Spontaneous ac- tivity in the form of fibrillation potentials and pos- itive sharp waves was present in more than two places outside the endplate zone in onlv 2 of the 25 examined abductor cligiti minimi muscles and in none of the others. At maximum effort a sig- nificant loss of motor units was observed in two- thirds of the brachial biceps arid abductor digiti mininii muscles and in four-fifths o f the anterior tibial muscles.
Motor Conduction. Motor conduction was measured once in 38 patients and in 35 relatives, and twice at an interval of 2-6 years (an average of 3.8 years) in 9 patients.
I n the patients at the first examination, the mo- tor conduction velocity was, on an average. 5 1.7 -t 5.8 mlsec along the median nerve and 37.9 2 3.8 m/sec along the tibial nerve, with an average slow- ing of 21 and 2776, respectively, compared with
40
20
10
0 f r r . r. p. d. a.
AT FULL EFFORT
potential po I y p hasic fibrillation duration potent ia Is
above 20 % above 12 'lo
AT WEAK EFFORT AT REST
FIGURE 2. Electromyographic findings in 19 patients. Note brachial biceps (white columns), abductor digiti minimi (black columns), and tibialis anterior muscles (shaded columns): f.r. = full recruitment pattern; r,r.p. = reduced recruitment pattern; d.a. = discrete activity. Mean duration of 20-25 motor unit potentials was considered abnormal when above 2O0lO of age-matched control values. A 12% incidence of polyphasic potentials was considered normal. Fibrillation potentials were present in more than two places outside the endplate zone.
506 Friedreich's Ataxia MUSCLE & NERVE Jul/Aug 1987

z C
v,
m P !%
Tabl
e 1.
Ind
ivid
ual s
enso
ry n
erve
con
duct
ion
velo
city
find
ings
and
clin
ical
ass
essm
ent.
Sen
sory
con
duct
ion
Med
ian
nerv
e Ti
bia1
ner
ve
Con
duct
ion
Con
duct
ion
Pot
entia
l P
oten
tial
Con
duct
ion
velo
city
P
oten
tial
Pot
entia
l C
ondu
ctio
n ve
loci
ty
Age
in
terv
al
stag
e at
wris
t at
elb
ow
digi
t Ill
-wris
t el
bow
at
med
ial m
alle
olus
at
pop
litea
l fos
sa
1st t
oe-M
ed
Mal
l Fo
ssa
Nam
e (y
ears
) (y
ears
) (1
) (P
V)
(PV
) (m
isec
) (m
isec
) (P
V)
(PV
) (m
isec
) (m
isec
)
ampl
itude
ve
loci
ty
Med
. Mal
l.-P
op1
Tim
e C
linic
al
ampl
itude
am
plitu
de
velo
city
w
rist-
ampl
itude
AF
17
IV 2
4 1.
4 1
3
45.6
61
.4
0.9
0.7
33 5
41
.6
4 IV
28
0.2
0.2
35.7
46
.4
0.3
0.2
26.3
45
.2
-
MM
25
111
21
0.1
0.1
40.5
56
.0
0.09
0
47.1
4
IV 2
6 0.
4 0.
3 46
.0
60.0
0.
1 0
40.4
RL
16
111 1
9 0.
5 0.
5 41
.9
63.1
0.
6 0
28.7
4
IV 2
8 0.
7 0.
3 34
.9
51.9
0.
1 0
40.0
VF
21
111 2
1 0.
3 0.
1 33
.5
32.4
0
0 3.
5 IV
26
0.2
02
52
.5
56.7
0
0
zc
20
111 2
1 0.
4 0.
3 49
.2
50.0
0
0 2
IV 2
6 0.
2 0.
3 50
.5
50.4
0.
2 0
2
29.2
49
.3
MP
20
111 1
9 0.
4 0.
3 45
.5
47.2
0
0 3
111 2
0 0.
7 0.
5 55
.1
53.8
0
6
0.3
35 0
46
9
PS
36
111 2
5 0.
5 0.
3 46
.0
53.6
1.
2 0.
4 37
.8
53.8
5
IV 2
9 1.
4 0.
8 43
.7
50.7
0.
5 0.
3 32
.1
45.0
6 IV
30
1.3
06
49
.3
57.1
0.
4 0.
7 34
4
50 3
vc
11
I1 18
0.
8 0.
7 48
.5
61.8
0.
3 0.
2 35
.1
52.2
3
II 19
1.
4 1 .o
37
.5
55.0
0.
5 0.
8 37
.9
42 6
-
-
-
-
-
__
-
-
-
-
-
CM
19
IV
27
2.5
10
50
.6
55.5
0.
4 0.
4 29
.2
53.4
Dat
a ac
cord
mg
to M
eri
ted
Ata
xias
Pro
gres
sion
Sca
/e16
(ord
mal
figu
res)
and
Inhe
rited
Ata
xias
C/in
/cal
Ral
ing
Sca
le:?
(car
dina
l fig
ures
) in
nin
e pa
tient
s on
initi
al e
xam
inat
ion
and
afte
r tu
ne in
terv
al a
s sp
ecl
ed
Se
e te
xt fo
r fu
rther
de
tah

controls. The distal latency on the first examination was 4.1 2 0.7 nisec and 6.8 5 1.3 msec, respec- tively, which corresponds to a mean increase of 43 and 77% over control values. T h e mean amplitude of muscle evoked potentials was 16.5 +- 7.7 mV and 10.2 ? 6 mV. which are within normal limits. No substantial differences were found in the 9 pa- tieiits seen a second time after an interval of 2-6 years when the clinical conditions had deteriorated (see Table 1 for clinical assessment). In fact, along the median nerve the motor conduction velocity from wrist to elbow was 50.8 * 5.1 m/sec at the first examination and 50.1 ? 4.1 mhec at the sec- ond; the distal latency from wrist to the abductor pollicis brevis muscle was first 4.1 ? 0.6 msec and then 3.9 2 0.8 msec; and the amplitude of the muscle response went from 18 ? 8.5 mV to 14.4 ?
5.9 m V . In the tibial nerve, at the first exaniina- tion conduction velocity from the popliteal fossa to the medial nialleolus was 39.8 I+_ 3.3 m/sec at
I potential amplitude at wrist
I E D I A N NERVE . .
the second i t was 38.5 ? 2.7 ndsec; the distal latency from the medial malleolus to the abductor hallucis muscle was first 6.8 -+ 1.6 msec and then (3.9 ?
1.1 msec; and the amplitude of the muscle com- pound potential increased from 11.7 ? 6.4 m V at the first examination to 12.3 5 4.2 mV at the sec- ond.
Motor velocity and distal latency were nornial in both the median and tibial nerves of' the 35 ex- amined relatives.
Sensory Conduction. Sensory conduction \+'as mca- sured once in 38 patients and in 37 relatives and 21
second time 2-6 years (average 3.8 years) late)- in 9 patients.
I n the patients at the first examination. the ah- normalities observed in orthodromic sensory con- duction velocity were similar in all explored nerves. Indeed, maximum conduction velocity appeal-eti
SENSORY VELOCITY
0
301 20
0
10- 0
conduction velocity digit 111 - wrin.
0
0
0
t--- conductmn velocity wrist - elbow
FIGURE 3. Median nerve: individual sensory conduction findings in patients ( 0 ) and relatives ( 0 ). The transverse continuous lines are the mean normal values; the dashed lines are the 95% upper and lower confidence limits.
508 Fnedreich's Ataxia MUSCLE & NERVE Jul/Aug 1987

normal or moderately reduced both in the distal and the proximal nerve segment, whereas the am- plitude of the sensory evoked responses was mark- edly reduced in most cases. In the median nerve (Fig. 3), sensory responses could not be evoked at the wrist in 7.9% and at the elbow in 16% of cases, whereas in the tibial nerve (Fig. 4) no potential could he recorded at the medial malleolus in 33% and at the popliteal in more than 51%. Similar re- sults were obtained along the sural nerve of the six patients in whom it was examined. In fact, although maximum conduction velocity along the exposed nerve was from 77 to 100% of control values, the potential amplitude was 99-90% less than normal. Therefore, both with the conventional procedure and with the intraoperative technique, velocity never fell below SO%, whereas the potential amplitude was, depending on the patient, 0.1-26% of normal values.
Similar findings were obtained in the 9 patients
3 0 0
4+ 2 0 O 0 0 0
0 j: 0. 0
0 I----+ 0.0 0.0
potential amplitude at medial malleolus I
. I B I A L N E R V E
n /s 70
60
5 0
40
30
2 0
10
who were examined a second time after an interval of 2-6 years when the clinical condition had sig- nificantly deteriorated. And in fact, as shown in Table 1 , the values obtained in these patients at the second examination were practically identical to those obtained at the first examination. This is true both when the single values of each patient are compared and when the average values are com- pared (paired t-test, and t-test for two independent samples of the same size).
In 21 of the 35 examined relatives, maximum orthodromic sensory conduction velocity along the distal segment of the median and tibial nerves showed an average slowing of 2770 and 29% com- pared with control values (Figs. 3 and 4). N o sig- nificant differences were found between the par- ents and the siblings. The potential amplitude was significantly reduced in only two cases at the wrist (Fig. 3) and in five cases at the medial malleolus (Fig. 4).
SENSORY V E L O C I T Y
m Is
0
a 0
0 0 0 0 0 0
O 0 0
- 1 - - conduction velocity
1st toe - medial malleolus
'0
b0
i0
LO
10
?O
1c
0 0
0
P conduction velocity
medial malleolus - popliteal fossa
FIGURE 4. Tibia1 nerve: individual sensory conduction in patients ( 0 ) and relatives ( 0 ). The transverse continuous lines are the mean normal values: the dashed lines are the 95% upper and lower confidence limits.
Friedreich's Ataxia MUSCLE & NERVE JullAug 1987 509

Somatosensory Evoked Potentials. Somatosensory evoked potentials were obtained once in 14 patients and 1 1 relatives.
I n all 13 patients SSEPs were abnormal in more than one parameter. Evoked responses were either no( detectahle or dubious at Erb’s point in nine patients, and in three patients no clear responses were recorded at CV7 or at C3‘. In all other cases the response amplitude was reduced by 67% to 855; compared with control values at all recording sites. l ’hc latency at Erb’s point and at CV7 was normal, except for one case in which it was slightly inc-rexed and for another in which it was at the upper limits of normal values. In all patients, on the contrary. the N 2 0 wave o f C3’ recordings had a delaved peak latencv compared with controls and ;in abnormally increased temporal dispersion. Cen- tral conduction time was on the average prolonged l y 70% compared with control values in all 8 pa- tients in whoiii it could be determined.
Although there was a correlation between SSEP lintlings and the peripheral abnornialities in that they were ~is~ially more altered in patients with the niore evident peripheral alterations, there ap- pwrecl to be no relation between the duration of the disease and SSEP alterations.
SSEPs were within normal limits in 8 of the 10 relatives examined arid altered in the remaining 2. The amplitude of the Erb‘s point response and of’ the “LO wave was slightly reduced in an 18-year- old brother who had bilateral pes cmuc and a slight tremor of the upper limbs associated with a slowing of sensory conduction along the distal segment of hoth the median arid tibial nerves. A reduction of the amplitude of the Erb’s point response and an inct-ease of the N9-N 13 interval was found in a 43- year-old mother who had a slight diadochokinesia, a recluction o f the amplitude of the median re- sponse, and a distal slowing of both median and tibial nerves.
Visual Evoked Potentials. Visual evoked potentials were examined once in 13 patients and in 10 rel- a tives .
VEl’s were impaired in eight patients with Frie- dreich’s ataxia, and the most frequent abnormality w a ~ n prolongation of the PI00 component latency. I n 6 patients the amplitude was, 011 an average, reduced by 60% of control values, and in 4 an in- crease of the time interval between N I and N2 waves added to the pathologic increased latency.
VEP alterations were present in all subjects with clinical ophthalmologic disease disturbance. In- deed, the more severe these disturbances, the more
evident the VEP abnormalities. On t h e contrary, there was no correlation between the severity of the clinical disorders of Friedreich’s disease and VEP alterations.
An abnornial prolongation of the P100 com- ponent latency was observed in only one relative, who also had abnormal SSEPs.
Brain Stem Auditory Evoked Potentials. Brain stem auditory evoked potentials were examined once in 13 patients arid in 14 relatives.
BAEPs were normal in only one of the patients examined. The reniaining 12 patients showed some degree of alteration. The niost evident changes were observed in five patients and consisted of either the complete abseiice of the response (even to 100-tlB SL click stimulation) or the pi-esence of‘ only one or t w o delinite peaks. In the other seven patients, BAEP abnormalities were less evident: wave V was the most frequently affected. I t was absent from one or both sites in five patients and had an in- creased latency in three. Peak I on the other hand was always detectable and had a normal latency except in one case. There was n o correlation be- tween BAEP findings and clinical hearing distur- bances, which, when present, were slight, whereas there was a significant correlation (P < 0.001) be- tween BAEPs and the degree o f Friedreich’s ataxia clinical disability assessed according to the Inher- ited Ataxias Progression Scale (Fig. 5). In fact, pa-
IV v + -I
0.3 $J
A
B
I I I l l I I I l l 1 0 2 4 6 8 ms 10
FIGURE 5. BAEPs from a normal subject (A) and from three patients with Friedreich’s ataxia. Definite recognition of only wave I in subject with an 1 1-year history (B); uncertain recognition of waves II and 111 and increased latency of wave V (?) in a subject with a 4-year history (C); impaired IV-V/I amplitude ratio and uncertain recognition of wave V in a patient with a 3-year his- t o v (D).
510 Friedreich’s Ataxia MUSCLE & NERVE JullAug 1987

tients with a slight clinical disability showed mild BAEP involvement, whereas those with severe, long- lasting clinical disturbances had pronounced, wide- spread BAEP changes.
BAEPs were normal in 12 of the 14 relatives examined. In a mother, who also had SSEP ab- normalities, there was increased latency of waves 111 and V and an increase of the 1-111 interpeak interval following stimulation of the right ear. In a father there was an increased latency in all the peaks obtained by stimulation of the left ear. How- ever, this increase was probably due to peripheral alterations.
Nerve Biopsy. Nerve biopsy was performed on 14 patients and 2 relatives. T h e cross-sectional histo- logic findings in 14 patients with Frieclreich’s ataxia are reported in Table 2.
The endoneurial area was moderately in- creased in only two nerves, and with only t w o ex- ceptions the total number of myelinated fibers per square millimeter was reduced with a severe loss of the large diameter fibers. T h e distribution of axoil diameters was unimodal, with a peak at 4-5 p i , which corresponded t o that of controls (Fig. (5).
‘ Ihe rare onion-bulb formations observed were small and had a simple aspect. Degenerated nerve
fibers were rare, and abnormalities of vessels or connective tissue were never noted.
For the teased nerve fiber prepai-ations, w e ob- tained 287 fibers, 7 p i o r more in diameter, from 9 sural nerves; 63 fibers were nornial with a uni- form distribution in the different nerves. En- hanced variability of internodal lengths was ob- served in 54 fibers. A total of 170 fibers had uniforndy short internodes in relation to other fi- bers of the same diameter, which tends to suggest regeneration after axonal degeneration rather than demyelination and remyelination. These changes were not correlated to the Friedreich’s ataxia clin- ical state.
T h e two parents in whom sural nerve biopsy was obtained were a 37-year-old mother of 3 chil- dren, 2 of whom had a 5-year history of definite signs of Friedreich’s ataxia, and a 5%year-olrt father of 2 children, 1 of- whom, a 22-year-old woinan, had a 14-year clinical history of Friedreich’s ataxia.
Table 3 reports the cross-sectional histologic findings of these two unrelated parents. 111 the nian, the teased nerve fiber preparation gave normal re- sults, and there was only a slight reduction in the number of fibers per square millimeter. I n the woman quantitative histology gave normal results, whereas there was a higher incidence (42%)) of fi- bers with a uniformly short internodal length and
Table 2. Cross-sectional histologic findings in 14 patients with Friedreich’s ataxia number and size distribution of myelinated nerve fibers
Case No
N 3 N 8 N 9 N 10 N 11 N 15 N 18 N 22 N 37 N 38 N 41 N 43 N 54 N 73 Range Mean SD Controlst
Age (years)
22 19 33 18 25 17 17 39 13 16 20 15 19 33
Duration of symptoms
(years) Clinical stage*
Endoneurial area (rnmz)
Total number of fibers
8 8
15 10 10 3 4
20 4 8 4 1 4 8
IV I1 IV IV 1 1 1 1 1 1 II IV II I1 II I1 I1
1 1 1
1 05 0 91 1 3 0 69 1 4 8 1 1 1 09 1 24 1 03 0 65 0 99 1 22 0 82 0 75
0 65-1 48 101 0 24
068-1 14
5,130 2,769 6,024 4,221 3,855 3,116 3,441 4,395 2,694 1,548 3,416 5,917 3,318 3,295
1,548-6,024 3,795 1,250
5,662-1 0,732
Density (fi bershnm‘)
6,180 2.520 4,634 6,117 2,605 3,091 3,157 3,544 2,616 2,382 3.451 4,850 4.046 4,393
2,382-6,180 3,827 1,265
6,081 - 1 2,196
Fibers >7 p m
(%I
Fibers >9 pm
(YO)
20 7 12 5 20 5 16 2 5 2 9 4
16 6 10 0 0 9 7 2
13 2 15 9
1 5 5 0
0 9-20 7 11 06 6 5
37 2-54 1
9 8 5 7 7 9 7 7 1 7 4 6 8 8 4 0 0 0 2 6 6 4 7 8 0 4 1 5
00-9 8 4 9 3 3
20-42
Fibers ->ll pm
(YO)
1 3 2 8 2 3 2 3 0 4 1 5 1 6 1 0 0 0 1 3 2 7 1 4 0 1 0 0
0 0-2 8 1 33 0 9
3 6-23 4
Clusters (No 1
36 3
15 0
10 0 0 4 0 0 3 6 0 0
0-36 5.5 9 8 0-20
’Inherited Ataxias Progression Scale 22
t€/even controls, aged 15-60 years
Friedreich’s Ataxia MUSCLE & NERVE JuliAug 1987 511


be followed by disorders of the cerebellar pathways and of the motor system.
The main electrophysiologic alterations ob- served in the peripheral nerves of patients of our earlier study2" and of the present report are a marked reduction of the amplitude of the sensory response and a slight slowing of conduction veloc- ity. These findings are in agreement with previous
1.25,:<2.:3H,1:3 and reflect a loss of the largest peripheral nerve fibers. Moreover, the quantitative histologic results of the sural nerve biopsy indicate a severe reduction of large myelinated fibers, and the uniformly short internodes observed on teased nerve fiber preparations suggest regeneration after axonal degeneration rather than demyelination and remy elination.
In contrast with other s t~d ie s , ' " . "~ .~~ our pre- vious study had shown that neither the histologic data nor the conduction velocity and amplitude of sensory potentials along the peripheral nerves were related to the duration or to the severity of Frie- dreich's ataxia clinical disability. In fact, findings were rather uniformly distributed and of the same extent regardless of whether the clinical signs had first appeared 2 or 20 years earlier or whether the disability was evaluated at stage I1 or at stage IV of the 1AP scale." These findings are supported by the present study. In fact, we did not observe any significant deterioration of the electrophysio- logic findings in the 9 patients who, reexamined after an interval of 2-6 years, showed a marked clinical deterioration. It therefore seems probable that the progressive clinical course of Friedreich's ataxia could depend on alterations advancing in structures outside the peripheral nerves.
The central evoked potential changes observed in our patients were as follows: (1 ) severe inipair- ment of somatosensory evoked potentials, which were impaired in all patients examined regardless of the duration or the severity of clinical disability; (2) high incidence (69%) of VEP abnormalities, usually a delayed latency of the PlOO component frequently associated with a reduced amplitude that was related to the clinical ophthalmic signs but not the degree of clinical involvement; and (3) BAEP abnormalities unrelated to hearing disorders but significantly ( P < 0.001) correlated with the Frie- cireich's ataxia clinical disorders.
1 hese results are in agreement with most stud- ies oll this ~ o p i c , l , 1 7 . 3 ~ , ~ ~ 4 . 3 7 . 4 1 J . ~ 1 . - 1 - 1 . 5 0 However, the pathophysiologic mechanisms underlying the al- terations found in Friedreich's ataxia patients have yet to be clarified. On one hand, the severe reduc- tion of the SSEP amplitude may be interpreted as
_ 1
a selective loss of large axons; whereas the increase of the central conduction time and the broadened waveform of the cortical response is probably due to other changes along the central somatosensory pathway .
The mechanism underlying the observed BAEP and VEP abnormalities is similarly intriguing. To explain these abnormalities Satya-Murti et al.44 pos- tulated degeneration beginning at Corti's spiral ganglion and progressing along the acoustic nerve to reach its central connections. However this hy- pothesis does not account for the longer persistance of BAEP wave I with the early disappearance of wave V. Moreover, from what is presently known regarding the visual system, the constant latency increase of the cortical visual response-even though associated with amplitude reduction and/or tem- poral dispersion of the P 100 component-cannot be explained solely on the basis of degeneration of the peripheral fibers that, in any case, have yet to be demonstrated .'I
The data obtained from the relatives of our patients with Friedreich's ataxia may be sunitna- I-ized as follows: (1) only two unrelated parents showed clinical signs typical of Friedreich's ataxia and distinct electrophysiological abnormalities; (2) over half the siblings had abnormal clinical find- ings, and in 86% they were associated with electro- physiological alterations; (3) the incidence of elec- trophysiologic changes was practically the same in parents (57%) and in siblings (62%); (4) the elec- trophysiologic abnormalities were moderate even though they were clearly evident. Severe alterations were found in only two brothers who were ex- cluded from the study because the clinical exami- nation led us to suspect Friedreich's ataxia.
The most frequent clinical abnormalities found in the relatives were reduced deep-tendon reflexes, pes cauus, and kyphoscoliosis. The most common and indeed the most important electrophysiologic sign (found in 2 1 of the 35 examined relatives) was a slowing of the maximum orthodromic sensory conduction velocity along the distal segment of the median and tibia1 nerves. In "dying-back" neuro- pathies, distal slowing may be present in the distal part of the large peripheral fibers, the most prox- imal segment retaining normal velocity until the arrival of the degenerative process.48,'q A di stal slowing of conduction velocitv occurs also in en- trapment neuropathies as a result of distal axonal
The sural nerve biopsy from the two relatives was noncontributory. Both subjects were clinically normal. The female subject was also electrophys-
atrophy.?.:%(j
Friedreich's Ataxia MUSCLE & NERVE JuliAug 1987 513

iologically normal, whereas the male had a distal reduction of the orthodromic sensory conduction velocity that reached 37%1 in the median nerve and 5 1% in the tibial nerve. At biopsy the man had only a slight reduction of myelinated fibers per square millimeter, whereas the woman had a 42% inci- dence of fibers with uniformly short internodes and the presence of paranodal globules in many fibers. Moreover, in the “unaffected” son (aged 23 years) ot‘ the male relative, there was bilateral pes cavus and a maximum orthodromic sensory velocity that was slowed by 34-37%. In the other two clinically
normal children of the female relative (a boy of 3 and a girl of 7 years), the maximum sensory con- duction velocity was slightly slowed in the distal segments of the median and tibial nerves.
In conclusion, in these relatives there did not appear to be any correlation either between clinical and electrophysiologic findings or between these findings and biopsy results. It remains to be seen whether the changes observed in the siblings will remain stable, thus representing a heterozygotic: condition, or whether they are harbingers of a clin- ical picture that will progressively deteriorate.
REFERENCES
514 Friedreich’s Ataxia
1 .
2.
3.
4.
5.
6 .
7.
8.
9.
10.
I I.
12.
13.
14.
15.
16.
17.
Amantini A , Rossi L, De Scisciolo CT, Bindi A: Coinponenti precoci e tardive del potenziale evocatu acustico (PEA) riell’atassia di Friedreich, in I Corso teorico pratico sui po- tenziali evocati. Potenriali evocati: principi e applicazioni cliniche. Milano 14-17 Feh. 1983, p p 156-163. Haha M, Fowlet- C:J, Jacobs Jbl , Gilliatt RW: Changes i n peripheral nerve fibres distal to constriction. J Neurol Sci 51: 197-2008. 19x2. Bai-beau A: Friedreich’s ataxia 1976: an overview. Cnn J Nsurol Scz 3:389-397, 1976. Barheau A: Friedreich’s ataxia 1980: an overview of phvs- iopathology. Ccin J Neurol Sci 73455-468, 1980. Barheau A: Frietlreich’s disease 1982: etiologic hypothe- sis-a personal analysis. Cnii J Nrurol Sci 9:243-263, 19082. Barheau A, Breton G. Lemieux B, Butterworth RF: Bili- rubin metabolism: preliiiiinary investigation. Cmz N w r d Sci 3:365-372. 1976. Barheau A. Patenaude F, Nadon G. Charhonneaii M . Clou- ticr . I . : A possible genetic pattern of taurine urinary excre- tion in Friedreich‘s ataxia. CniiJ lVrurul Scr 9:209-2 15, 1982. Behse F. Buchthal F: Normal sensory concluction i r i rirrves of thc leg in ma1i.J Neurol Neumsurg Psyriiic~t7y 34:404-4 14. 1971. Belise F, Buchthal F, Carlsen F, linappeis GG: Hereditarv ncuropathy with liability to pressure palsies: electrophvs- iological arid histopathological aspects. Bruin 95:777-794, 1972. Bchse F. Buchthal F. Carlsen F, Knappeis GG: Endoncurial space arid its constituents i n the sural nerve of patients w i t h neuropathy. Rrnm 97:773-784. 1974. Bergamini L, Bergamasco B, Fra L, Gandiglio G. Morlwlli A M . Mutani R: Reponses corticales et peripheriques Cvo- quees par stimulation du nerf dam la pathologie des cor- dons posterieurs. Rnj Nruro/ 115:99-1 12, 1966. Blache D, Bnuthillier D. Bat-hcau A, Davignon J: Plasma lipnprotein lipase and hepatic lipase activities in Friedreich’s ataxia. C a n J Nsrirol Sci 9:191-194. 1982. Hottacchi E, Di Ihna to S: Skeletal muscle NAD(P)+ and N ADP + : dependent malic enzyme in Friedreich’s ataxia.
Huchthal F: A n In/roduc./ion 10 Elecfromvogrnptr~. Copen- hagrn, Scandinavian University Books, 19.57, pp 1-43. Buchthal F. Roscnlalck A: Evoked action potentials arid tonductiori velocity in hunian sensory nerves. B ~ n i n Rcr 3 : 1-122, 1966. Campanella C;, Filla A, Dc Falco F, Mansi D. Dui-ivagc A, Uarlmiu A : Fricclreich‘s ataxia in the south of I taly: a clin- ical and biochemical survey of 23 patients. Caii I Neurol S C I 7::151-357. 1980. (hrroll WM, liriss A, Baraitscr M , Barrett G, Halliday A M : I ‘ h e incidence and nature o f visual pathway involverwrit
18.
19.
20.
21.
22.
23 .
24.
25.
26.
27.
28.
29.
30.
31.
in Frietlreich‘s ataxia: a clinical and visual cvokrtl potcnti:il study of 22 patients. BJnin 10R:l l?-434, 1980. C:artiso G. Santoro I., Perretti A, Campanella (;, Rosato R, Crisci C:, Ragno M , Massirii R: Electrophysiologi( at hndings in relatives of patients with Frietlreich’s ataxia. I / n l J ’Yrurol s c i -1:98-105, 1981. Cnru.;o C;, Santoro L, Perretti A , Corrado EM, Pa.$\aretti Ll, Amantea B: Inti-:ioperative EMG. in Caruso (;. Ludin H-P (eds): Eleclromyogr(ifih~ in //is Drng~io~is mid Mn~rcc,qrrncn~ uf Pcriptwrul Ncnw l ? ! j i m t z s . Berm, Swit/crlaiid, Hans Huber Puhlishers, 1983. pp 73-83. Caruso G, Santoro L. Perretti A. Serlciiga L. (;i-isci C, Ragno M. Barliieri F, Filla A : Frieclreich’\ ataxia: electrophysio- logiral arid histological hndings. Ac k r .l’rwrol .Sccitrd fi7:26-40, 1983. Davignon J , Huarig YS, Wolf JP , Barheau A : Fatty acid profile of major lipid classes in plasma lipoproteins of pa- tients with Friedreich’s ataxia: dcmonstratioii of ;a low lin- oleic acid content iiiost evident in the cholestci~o~cstei- frac- tion. C h i J N e z u o l Sci 6:275-‘2X3, 1 97!1. De Falco F. Mansi D, \’entola F, Filla A , Chiiipaiirlla (;: Propostn di uii;~ scheda di rilcvaniento rliiii( o dclle iitassie spino-cerchcllari. Q i r d Artn i\’rrtrol 39: 103- 109. 1979. Di Donato S, Pandollo M, k’irrocchiai-o G , Protti A : Skeletal mu\( Ir malic enzymes: a studv in Frirdreich’s clisc;ise. I / o l J h’cwfo/ Sti 4:51-40. 3984. Dyck PI, Lais A(;: E\itlericc for segmental dcmyelinatiori secondary to axonal dcgeneratiori i i i Friedreich’s ataxia, i i i
K;ikul;is BA (ed): C(inica1 Sfudir.t in Myology Anistci-dam. Escei-pt;i Medica. 1972, pp 253-263. Fiasclii A, k’errari C;, De Grandis D. Tomcllcri (;: Aspetti rlettromiograhci ed istologici in corso di nialattia di Fric- clrcicli. A d a Niwrol 31: 162-169, 1976. Filla A , Butterworth KF, Ckoffroy G , Leinieux €5. Bai-heau A : Serum and platelet lipoamidc dclivdrogrn;i\c in Frie- dreich’s ataxia. ( h t i J Nrt17ol .Sri 5:l 11-1 14, 1!)7X. Friedreich M: Ueber degcncrative Atrophic cler spinalell flinterstrange. I’rrc./ion~ Arch Pct//rol :Itiaf 27: 1-26. 1x63 Geoffroy C;. kirheau A. Bt-eton (;, Lcmieux C;, AuIw M , Leger C, Bouchard JP: Clinical description and rocntgeii- ologic evaluation 01. paticnts with Frirdreicli’q :jt:ixi:i. ( h i . /
Ntziirol Sr i 3:27!)-2Xfi. 1976. Hamcl E, Betlnrd I), I.aviolette F. Butterworth RE‘. Uarheau A: F;iniilial liypei-hilii-iihirierriia i i i Fi-irtlrcic h’s ataxia. ( h i
I h’cta.ol S r f ~ : l ( ) l - l ( ) ~ , 1978. Huang Y S . Marccl YL, Vehiii C:, Barheau A, Uavignon I : Lccithiii: cholesterol acyltranstcrasc activitv a i i t l fatty acid c()ni position of c ~ y t h rocyte phospholipids in Fi-icdrcich’s ataxia. (,”in J h’r~ i r rn l .Scr 7:42!)-134. 1980. Huang 1’s. Nesti-lick .4C. Bat-beau A , Rouch;irtl JI’. Dav- gnonJ: P1asrn;i lipids and lipoproteins in Frietlteiclr’~ ataxiii
MUSCLE & NERVE JuliAug 1987

and familial spastic ataxia: evidence for an abnormal com- position of high density lipoproteins. Can ./ Nmirol Src 5:
32 . Hughes JT. Brownell B, Hewer RL: The peripheral sensory pathway in Friedreich’s ataxia. Brain 91:803-818, 1968.
33. Jabbari B, Schwartz DM, MacNeil DM, Coker SB: Early abnormalities of brainstem auditory evoked potentials in Friedreich’s ataxia: evidence of primary brainstem dys- function. Neurology ( N Y ) 33:1071-1074, 1983.
34. Jones SJ, Baraitser M, Halliday AM: Peripheral and central somatosensory nerve conduction defects in Friedreich’s ataxia. J Nrurol Neurosurg P.\vchiutry 43:495-503. 1980.
35. Lemieux B. Barbeau A. Beroniade V . Shapcott D, Breton G. Geoffroy C;, Melancon s: Amino acid ntetaboiisrn in Friedreich’s ataxia. Can J Nrurul So 3:373-378, 1976.
36. Le Quesne PM. Casey EB: Recovery of conduction velocity distal to a compressive lesion. J N e w i d Neurosuig Psyrhicilry
37. Livingstone IR , Mastaglia FL, Edis R, Howe JW: Visual involvement in Ft-iedreich’s ataxia and hereditary spastic ataxia. Aich Nrurol 38:75-79, 1981.
38. McLeod,lC.: An elcctrophysiological and pathological study of peripheral nerves in Friedreich’s ataxia. J Neirrol Scz 12:
39. Ouvriei- RA, McLeod JG, C~onchin TE: Friedreich’s ataxia: early detection and progression of peripheral nerve ab- norma1ities.J A‘ercrol Sci 55: 137-145, 1982.
40. Peclersen L, Trojaborg U’: Visual, auditory and sotnato- sensory pathway involvement i n hereditary cerebellar ataxia, Friedreich’s ataxia and familial spastic paraplegia. Electmen- crphnlogr chi Ncurophysiol 52:283-297, 198 1.
4 1. Pclosi L, Fels A, Petrillo A. Senatore R, Russo G , Lonegren I;. Calace P, Caruso G : Friedreich’s ataxia: clinical involve-
149-156, 1978.
37: 1346-1 35 1 , 1974.
-349, 1971.
ment and evoked potentials. Acla h’vccrol Scuizd 70:360-3fi8, 1984.
42. Rosenfalck A, Kosrnfalck P: Elrctromygraphy Scrisoiy untl Motor Conduction: Fzndirigs 2 7 ~ N o n n d Sihjwh. Copen hiigen, Rigshospitalet, 1975, pp 1-49,
43. Santoro L, Serlenga L, Perretti A, Di Mitri A, Ragno hl, Di Lorenzo MR, Caruso G: Electrophysiological and morpho- logical findings in Friedreich’s ataxia, abstracted. Pharrrrtr- cology 22:69, 1982.
44. Satya-Murti S, Cacace A , Hanson P: .4uditory dysfunction in Friedreich’s ataxia: result of spiral ganglion dcgener;t- tion. N ~ t ~ l ~ g y (NY) 30:1047-1053, 1980.
45. Sttrmpf DA, Parker DW, Park>.) K , F.guren LA, Devore M A : Friedreich’s disease: tnalic enzyme studies. l ta l J Neurol Scr
46. Stunipf UA. Parks JK. Eguren LA, Haas K: Friedreich’s ataxia: 111. Mitochoiidi-ial in& enzyme deficiency. N e w nhgy ( N Y ) 32:221-227. 1982.
47. Stutnpf DA, Parks J K , Parkrr DW: Friedreich’s diseacc: I Y . Reduced mitochondria1 malic enzyme activity in hetcrozy- gotes. Neurology (NY) 33:780-783, 1983.
48. Sriinner AJ: Axonal polyncuropattties, in Sumner (ed): Thiz l‘hy.~iology of Pel-iphrral h’mle Disensc. Philadelphia, WB Saun- ders C o , 1980. pp 340-357.
49. Suniner AJ, Asbury AK: Physiological sttitlies of the dying- back phenornerron: effects of acrylamide on muscle stretch afferents. Brain 98:91-100, 1975.
50. Taylor h,lJ, McMenamin JB, ,4ndermann E, Wattcrs G V : Electrophysiological investigation ot the auditory system in Frirdreich’s ataxia. CanJ N e w d S c i ~I : l :~ l - l35 , 1982.
51. Winter K M , Harding AE. Baraitser M, Bravcry MU.. \ i i \ ~ - familial correlation in Frirdreich’s ataxia. C l r ~ G r n d ‘LO: 419-427, 1981.
4127-33. 1984.
Friedreich’s Ataxia MUSCLE & NERVE Jul/Aug 1987 515




















