
Electrophysiologic evaluation of phrenic nerves in severe respiratory insufficiency requiring...
6
DOI 10.1378/chest.88.2.211 1985;88;211-214 Chest S S Moorthy, O N Markand, Y Mahomed and J W Brown mechanical ventilation. severe respiratory insufficiency requiring Electrophysiologic evaluation of phrenic nerves in http://chestjournal.chestpubs.org/content/88/2/211 can be found online on the World Wide Web at: The online version of this article, along with updated information and services ) ISSN:0012-3692 http://chestjournal.chestpubs.org/site/misc/reprints.xhtml ( without the prior written permission of the copyright holder. reserved. No part of this article or PDF may be reproduced or distributed Chest Physicians, 3300 Dundee Road, Northbrook, IL 60062. All rights of been published monthly since 1935. Copyright1985by the American College is the official journal of the American College of Chest Physicians. It has Chest © 1985 American College of Chest Physicians by guest on July 11, 2011 chestjournal.chestpubs.org Downloaded from
-
Upload
independent -
Category
Documents
-
view
1 -
download
0
Transcript of Electrophysiologic evaluation of phrenic nerves in severe respiratory insufficiency requiring...
DOI 10.1378/chest.88.2.211 1985;88;211-214Chest
S S Moorthy, O N Markand, Y Mahomed and J W Brown mechanical ventilation.severe respiratory insufficiency requiring Electrophysiologic evaluation of phrenic nerves in
http://chestjournal.chestpubs.org/content/88/2/211
can be found online on the World Wide Web at: The online version of this article, along with updated information and services
) ISSN:0012-3692http://chestjournal.chestpubs.org/site/misc/reprints.xhtml(without the prior written permission of the copyright holder.reserved. No part of this article or PDF may be reproduced or distributedChest Physicians, 3300 Dundee Road, Northbrook, IL 60062. All rights
ofbeen published monthly since 1935. Copyright1985by the American College is the official journal of the American College of Chest Physicians. It hasChest
© 1985 American College of Chest Physicians by guest on July 11, 2011chestjournal.chestpubs.orgDownloaded from

CHEST I 88 I 2 I AUGUST, 1985 211
Electrophysiologic Evaluation of PhrenicNerves in Severe Respiratory InsufficiencyRequiring Mechanical Ventilation*S. S. Moorthy, M.D. , F.C.C.P;t Omkar N. Markand, M.D.4
Yousuf Mahomed, M. D. , F. C. C. P ;� andJohn W Brown, M. D. , F. C. C. P §
Diaphragmatic paralysis in patients with respiratory insuf-
ficiency compounds the problems in the management. Inthe presence oflower lobe atelectasis, pleural effusion, or apatient’s poor respiratory effort, fluoroscopic examination is
often not a reliable way to diagnose diaphragmatic paral-ysis. We observed that transcutaneous phrenic nerve slim-ulation in the neck and recording the diaphragmatic poten-
tials from electrodes placed on the lower part ofthe chest is
C ontraction of the diaphragm produces 60 percent
of the tidal volume in normal supine individuals
at rest.’ Evaluation ofdiaphragmatic function is, there-
fore, important in patients with respiratory insuffI-
ciency. Paralysis ofthe diaphragm is usually diagnosed
by an elevated diaphragm on the chest x-ray film and
paradoxic movement of the diaphragm observed with
inspiration during fluoroscopic examination. The radi-
ologic diagnosis is difficult in the presence of lower
lobar atelectasis, pleural effusion, or with poor respira-
tory effort of the patient. It may also be difficult
sometimes to transport a critically ill patient to the
radiology unit for fluoroscopic study. We observed that
electrophysiologic studies of phrenic nerves provide a
useful technique for diagnosing diaphragmatic dys-
function in critically ill patients.
MATERIALS AND METHODS
Because of our interest in the electrophysiologic studies of the
diaphragm, we were asked to evaluate 21 patients who had respira-
tory insufficiency of recent onset requiring mechanical ventilation.
Fourteen patients developed respiratory dysfunction in the
postoperative period following a surgical procedure, usually a
thoracotomy. An elevated diaphragm on the chest x-ray film,
persistent lower lobe atelectasis, inability to wean from ventilatory
support, and suspicion of phrenic nerve damage during surgery
prompted the anesthesiologist and the surgeon to seek a study of
phrenic nerve conduction in these patients. One patient had
traumatic quadriplegia due to a high cervical cord injury. The
remaining six patients had decreased respiratory effort on the basis of
severe polyradiculoneuropathy of the Guillain-Barr#{233} type (five
patients) or myasthenia gravis (one patient).
*From Indiana University School of Medicine, Indianapolis.
tDepartment of Anesthesia.Wepartment of Neurology.§Section of Cardiovascular Surgery.Manuscript received November 29; revision accepted January 17.Reprint requests: Mr James May, Department ofNeurology, EM125,545 Barnhill Drive, Indianapolis 46223
a simple, reliable, and noninvasive technique to diagnose
diaphragmatic dysfunction at the bedside in critically illpatients. In 14 postoperative patients and one with cervicalspinal cord injury with respiratory failure, we found tenpatients who showed phrenic nerve dysfunction. Besidesdiagnostic utility, the electrophysiologic evaluation ofphrenic-diaphragmatic function provides critical informa-tion needed for therapy.
With the patient lying supine and the head in midline, we
stimulated the right and left phrenic nerves transcutaneously behind
the sternocleidomastoid muscle at the level of the upper border of
thyroid cartilage by conventional bipolar stimulating electrodes
(TECA Corp) The cathode was placed close to the clavicle. A disk
electrode over the manubrium sterni acted as a ground electrode.
Suprathreshold square-wave pulses ofO.1 to 0.5 msec at a rate of Jlsec
were delivered. The frequency response of the amplifier was set at
1.6 Hz to 32 kHz (- 3 dB). By adjusting the position of the
stimulating electrodes, the phrenic nerve could be selectively
stimulated with minimal brachial plexus stimulation.
The diaphragmatic evoked potentials were recorded from two
surface disk electrodes 8 mm in diameter; one was placed at the
seventh intercostal space (7ICS) close to the costochondral junction
and the other over the xiphoid process (XP). The electrodes were
held to the skin by electrolyte paste (Grass) and further secured with
cloth tape (Scotch). The ipsilateral 7ICS electrode was connected to
the input terminal 2 (red terminal) and the XP electrode to the input
terminal 1 (black terminal) of the electromyograph (TECA-TE42).
Using this XP-7ICS derivation, positivity at the 7ICS electrode
yielded an upgoing waveform. The details of the technique are
reported by Markand et al.’
The upper limits of the phrenic nerve conduction time in normal
adults is less than 9.75 msec (mean ± 2.5 SD). The amplitude of the
diaphragmatic potential is greater than 0.4 mV. In children the
latency is shorter (4.3 to 4.9 msec) and is dependent on the length of
the chest. The amplitude ratio of left and right responses are
normally over 0.6 and less than 1.6.
RESULTS
All patients with polyradiculoneuropathy (Guillain-
Barr#{233}syndrome) had abnormal electrophysiologic
studies of the diaphragm, the details of which have
been previously described.2 The amplitude of the
diaphragmatic response was significantly decreased
bilaterally. In two, the phrenic nerves were totally
inexcitable during the height ofthe illness. When the
diaphragmatic responses were elicitable, the latencies
were usually prolonged. Two patients had serial studies
starting less than a week from the onset of Guillain-
© 1985 American College of Chest Physicians by guest on July 11, 2011chestjournal.chestpubs.orgDownloaded from
Phrenic Nerve Studyt
Patient, Right LeftSex, Precipitating Cause �-�------� �-�---�
Age (yr) of Respiratory Failure* Radiologic Fmdingst Amp Let Amp Let
1, M, 61 CABG LLL atel; L p1 eff; � L hemidiaphragm 0.28 9.0 NR ...
2, M, 3 mo Repair of coarctation of aorta R lung inf/atel; LUL inf/atel; � L
hemidiaphragm
0.90 4. 1 NR ...
3, M, 73 CABG 5 yr ago; recent cholecystectomy L hemidiaphragm NR . . . NR ...4, F, 9 mo Repair ofcongenital MI RUL atel/inf; bil perthilar inf;
paradoxical movement of R
diaphragm (?)
0.80 4.5 1.00 4.0
5, M, 37 Ca of testes; thoracotomy for metastases R hemidiaphragm NR . . . 0.38 ...6, F, 4 Repair of artrioventricular canal RUL atellinf; bil LL inf 0.55 4.3 0.40 4.4
7, F, 4 Repair of congenital VSD R p1 eff; bil pulmonary inf; t L
hemidiaphragm
0.55 4.9 0.60 4.9
8, F, 71 CABG LLL atel; L p1 eff 0. 18 8.5 NR ...9, M, 62 CABG Bibasilar atellinf; bil p1 eff 0.45 9.5 0.65 9.5
10, F, 54 Right upper lobeetomy for Ca oflung RUL inf; R eff; L inf; fluoroparadoxical
movement R
NR . . . 1.30 8.0
11, M, 62 Colectomy for Ca and resection of
metastases in left lung
LLL inf/atel; L p1 eff 1. 10 8.5 NR ...
12, M, 3 mo Repair oftruncus arteriosus LLL atel/infand p1 eff 1.25 6.2 NR ...13, M, 12 Crouwn�s disease LLL atel/inf; RUL inf 0.70 6.0 0.25 10.2
14, F, 78 AV and MV replacement LLL inflate!; bil p1 eff 0.50 8.2 NR ...15, M, 7 Fracture ofcervical spine LUL atellinf; RUL atel 0. 10 6.5 NR ...
mitral valve.
tLLL, Left lower lobe; atel, atelectasis; L, left; p1, pleural; eff, effusion;
upper lobe; bil, bilateral; and LL, lower lobe.
tAmp, Amplitude; Let, latency; and NR, no response.
*CABG, Coronary arterial bypass graft; MI, mitral incompetence; Ca, carcinoma; VSD, ventricular septal defect; AV, aortic valve; and MV,
t , elevated; R, right; inf infiltrate; LUL, left upper lobe; RUL, right
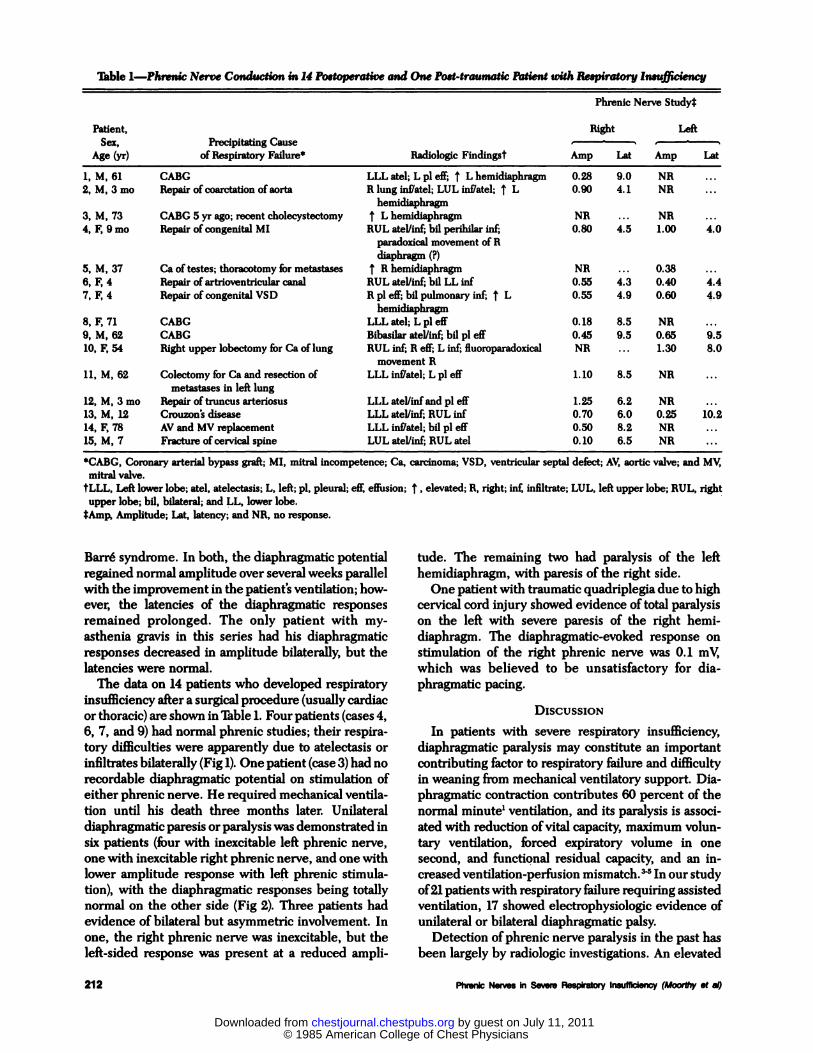
Table 1-Phrenic Nerve Conduction in 14 Postoperative and One Post-traumatic Patient with Respiratory Insufficiency
212 Phrenic Nerves in Severe Respiratory Insufficiency (Moorthy et a!)
Barr#{233}syndrome. In both, the diaphragmatic potential
regained normal amplitude over several weeks parallel
with the improvement in the patient’s ventilation; how-
ever, the latencies of the diaphragmatic responses
remained prolonged. The only patient with my-
asthenia gravis in this series had his diaphragmatic
responses decreased in amplitude bilaterally, but the
latencies were normal.
The data on 14 patients who developed respiratory
insufficiency after a surgical procedure (usually cardiac
or thoracic) are shown in Table 1. Four patients (cases 4,
6, 7, and 9) had normal phrenic studies; their respira-
tory difficulties were apparently due to atelectasis or
infiltrates bilaterally (Fig 1). One patient (case 3) had no
recordable diaphragmatic potential on stimulation of
either phrenic nerve. He required mechanical ventila-
tion until his death three months later. Unilateral
diaphragmatic paresis or paralysis was demonstrated in
six patients (four with inexcitable left phrenic nerve,
one with inexcitable right phrenic nerve, and one with
lower amplitude response with left phrenic stimula-
tion), with the diaphragmatic responses being totally
normal on the other side (Fig 2). Three patients had
evidence of bilateral but asymmetric involvement. In
one, the right phrenic nerve was inexcitable, but the
left-sided response was present at a reduced ampli-
tude. The remaining two had paralysis of the left
hemidiaphragm, with paresis of the right side.
One patient with traumatic quadriplegia due to high
cervical cord injury showed evidence of total paralysis
on the left with severe paresis of the right hemi-
diaphragm. The diaphragmatic-evoked response on
stimulation of the right phrenic nerve was 0.1 mV,
which was believed to be unsatisfactory for dia-
phragmatic pacing.
DIsCuSsIoN
In patients with severe respiratory insufficiency,
diaphragmatic paralysis may constitute an important
contributing factor to respiratory failure and difficulty
in weaning from mechanical ventilatory support. Dia-
phragmatic contraction contributes 60 percent of the
normal minute’ ventilation, and its paralysis is associ-
ated with reduction ofvital capacity, maximum volun-
tary ventilation, forced expiratory volume in one
second, and functional residual capacity, and an in-
creased ventilation-perfusion mismatch.� In our study
of2l patients with respiratory failure requiring assisted
ventilation, 17 showed electrophysiologic evidence of
unilateral or bilateral diaphragmatic palsy.
Detection of phrenic nerve paralysis in the past has
been largely by radiologic investigations. An elevated
© 1985 American College of Chest Physicians by guest on July 11, 2011chestjournal.chestpubs.orgDownloaded from

�J 500
6 msec
FIGURE 1. Normal and symmetric diaphragmatic potentials evoked by right and left phrenic nerve
stimulation in four-year-old child four days after repair of congenital heart disease (case 7).
RT. PHRENIC STIM. LT. PHRENIC SlIM.
CHEST I 88 I 2 I AUGUST, 1985 213
F � � :� � / I I / / / I I / / I / :r i : : � ; ; � :�
hemidiaphragm on the chest x-ray film with atelectasis
or infiltrates of the lower lobe on the affected side
suggests unilateral phrenic paralysis . Fluoroscopic
examination ofthe chest demonstrating reduced excur-
sion of the hemidiaphragm and paradoxic motion is
considered diagnostic ofdiaphragmatic paralysis.6 Un-
fortunately, fluoroscopic study may be delayed due to
the difficulties in transportation of the critically ill
patient to the radiology unit. Furthermore, the radi-
ologic findings are not pathognomonic ofphrenic palsy.
Similar findings may also occur with eventration of the
diaphragm, local pulmonary conditions (infiltrates,
atelectasis, effusion, etc), and subphrenic pathologic
abnormalities.7 The radiologic diagnosis of dia-
phragmatic weakness is, therefore, difficult and often
impossible in the presence of coexisting pulmonary
pathologic abnormalities. Such a complicating situa-
tion is commonly encountered in patients with respira-
tory failure in the postoperative period following a
surgical procedure on the chest (eg, coronary arterial
bypass graft). These patients not only show severe
pulmonary infiltrates or atelectasis, but are also at risk
RI. PHRENIC STIM.
to develop phrenic nerve damage secondary to surgical
trauma, traction, or hypothermia.8 In two of our
patients, radiologic studies raised the suspicion of
diaphragmatic paralysis, but electrophysiologic stud-
ies indicated normal phrenic-diaphragmatic function.
Although electrophysiologic techniques for study-
ing phrenic nerves and diaphragmatic function have
been available since the original work ofDavis9 in 1967,
they have not been widely employed in critically ill
patients due to lack ofa standardized, noninvasive, and
reliable technique of phrenic nerve stimulation and
recording. The availability of portable electrophysio-
logic instruments and experience with transcutaneous
phrenic stimulation and recording of diaphragmatic
potential make this technique feasible and reliable and
simple to perform in the intensive care unit. We found
that stimulation of the phrenic nerve by surface elec-
trodes was effective and without discomfort. The
invasive technique of stimulation through a needle
electrode placed close to the phrenic nerve as pro-
posed by some’#{176}is not necessary.
Both latency and amplitude of the diaphragmatic
LI. PHRENIC SlIM.
_j 500 �sv
10
FIGURE 2. Absence ofdiaphragmatic potential on left phrenic stimulation in 78-year-old patient two weeks
following aortic and mitral valvular repairs. Diaphragmatic response is normal to right phrenic stimulation
(case 14).
© 1985 American College of Chest Physicians by guest on July 11, 2011chestjournal.chestpubs.orgDownloaded from

214 Phrenic Nerves in Severe Respiratory Insufficiency (Moorthy et a!)
potential are important for the diagnosis of dia-
phragmatic dysfunction. Prolongation of the latency
provides unequivocal evidence of slowed conduction
along the phrenic nerve, a common finding in poly-
radiculoneuropathies and in some patients with in-
traoperative injuries ofthe phrenic nerves. The ampli-
tude ofthe diaphragmatic potential, on the other hand,
provides a measure of the number of diaphragmatic
muscle fibers activated by phrenic nerve stimulation.
Abnormalities of amplitude may be the sole evidence
of diaphragmatic paresis in patients who develop
respiratory insufficiency on the basis of myasthenia
gravis and motor neuron disease and also in patients
with intraoperative phrenic nerve injuries in the
thorax.
Diagnosis of phrenic palsy is not only helpful in
understanding the pathophysiology, but also in plan-
ning therapy in patients with respiratory insufficiency.
Patients with bilateral phrenic dysfunction are likely to
need continued positive-pressure ventilation or con-
tinuous positive airway pressure for their respiratory
support. “-‘� Unilateral diaphragmatic paralysis causes
respiratory insufficiency only if there are other com-
plicating factors such as intrinsic pulmonary or pleural
pathologic abnormalities. Correction of these compli-
cations is, therefore, crucial in restoring normal yen-
tilation. In patients with diaphragmatic paralysis,
plication of diaphragm is useful.’3 In patients with
traumatic quadriplegia with respiratory insufficiency
due to cervical cord injury, phrenic studies are crucial
in deciding if diaphragmatic pacing (electrophrenic
respiration) would have a place in the management of
the ‘#{176}If phrenic nerve stimulation elicits more
or less normal diaphragmatic responses, it can be
assumed that the anterior horn cells and their axons
innervating the diaphragm are intact. Diaphragmatic
pacing would be indicated in such patients. On the
other hand, if phrenic stimulation produces no re-
sponse or a low-amplitude response, diaphragmatic
pacing would not be beneficial, as was the case in our
patient with high cervical cord injury with quadri-
plegia.
We conclude that transcutaneous phrenic stimula-
tion with surface recording ofthe diaphragmatic poten-
tial is a noninvasive and reliable technique for diag-
nosis of diaphragmatic dysfunction. The test can be
performed easily at the bedside ofa critically ill patient
with pulmonary insufficiency. Electrophysiologic eval-
uation of phrenic nerves must be included in the
assessment of all patients who develop respiratory
insufficiency. When performed with customary radi-
ologic investigation, such evaluation provides useful
diagnostic and therapeutic information in such pa-
tients.
REFERENCES
1 Wang CS, Josenhans WI Contribution ofdiaphragmaticlabdom-
inal displacement to ventilation in supine man. J Appl Physiol
1971; 31:576-80
2 Markand ON, Kincaid JC, Pourmand BA, Moorthy 55, King
RD, Mohamed Y, et al. Electrophysiologic evaluation of dia-
phragm by transcutaneous phrenic nerve stimulation. Neurology
1984; 34:604-14
3 McCredie M, Lovejoy FW Jr. Kaltreider NL. Pulmonary func-
tion in diaphragmatic paralysis. Thorax 1962; 17:213-17
4 Arborelius M Jr, Lilja B, Senykj. Regional and total lung function
studies in patients with hemidiaphragmatic paralysis. Respira-
tion 1975; 32:253-64
5 Easton PA, Fleetham JA, DeLaRocha A, Anthonisen NR. Respi-
ratory function after paralysis of the right hemidiaphragm. Am
Rev Respir Dis 1983; 127:125-28
6 Loh L, Goldman M, Davis JN. The assessment of diaphragm
function. Medicine 1977; 56:165-69
7 Moosa A. Phrenic nerve conduction in children. Dev Med Child
Neurol 1981; 23:434-48
8 Markand ON, Moorthy 55, Mohamed Y, King RD, Brown JW.
Postoperative phrenic nerve palsy in patients with open heart
surgery. Ann Thorac Surgery 1985; 39:68-73
9 Davis JN. Phrenic nerve conduction in man. J Neurol Neurosurg
Psychiat 1967; 30:420-26
10 MacLean IC, Mattioni TA. Phrenic nerve conduction studies: a
new technique and its application in quadriplegic patients. Arch
Phys Med Rehabil 1981; 62:70-3
11 Robotham JL, Chipps BE, Shermeta DW. Continuous positive
airway pressure in hemidiaphragmatic paralysis. Anesthesiology
1980; 52:167-70
12 Robotham JL. A physiological approach to hemidiaphragm
paralysis. Crit Care Med 1979; 7:563-66
13 Haller BJ Jr. Pickard LR, Tepas JJ, Rogers MC, Robotham JL,
Shorter N, et al. Management of diaphragmatic paralysis in
infants with special emphasis on selection of patients for oper-
ative plication. J Pediatr Surg 1979; 14:779-85
14 Sivak ED, Razavi M, Groves LK, Loop FD. Long-term manage-
ment of diaphragmatic paralysis complicating prosthetic valve
replacement. Crit Care Med 1983; 11:438-40
© 1985 American College of Chest Physicians by guest on July 11, 2011chestjournal.chestpubs.orgDownloaded from

DOI 10.1378/chest.88.2.211 1985;88; 211-214Chest
S S Moorthy, O N Markand, Y Mahomed and J W Browninsufficiency requiring mechanical ventilation.
Electrophysiologic evaluation of phrenic nerves in severe respiratory
July 11, 2011This information is current as of
http://chestjournal.chestpubs.org/content/88/2/211Updated Information and services can be found at:
Updated Information & Services
http://chestjournal.chestpubs.org/content/88/2/211#related-urlsThis article has been cited by 2 HighWire-hosted articles:
Cited Bys
http://www.chestpubs.org/site/misc/reprints.xhtmlonline at: Information about reproducing this article in parts (figures, tables) or in its entirety can be foundPermissions & Licensing
http://www.chestpubs.org/site/misc/reprints.xhtmlInformation about ordering reprints can be found online:
Reprints
the right of the online article.Receive free e-mail alerts when new articles cite this article. To sign up, select the "Services" link to
Citation Alerts
slide format. See any online figure for directions. articles can be downloaded for teaching purposes in PowerPointCHESTFigures that appear in Images in PowerPoint format
© 1985 American College of Chest Physicians by guest on July 11, 2011chestjournal.chestpubs.orgDownloaded from




















