The origin of the inferior phrenic artery: a study in 32 South Indian cadavers with a review of the...
6
ORIGINAL ARTICLE The origin of the inferior phrenic artery: a study in 32 South Indian cadavers with a review of the literature Origem da artéria frênica inferior: estudo em 32 cadáveres da Índia do Sul com revisão da literatura Thejodhar Pulakunta 1 , Bhagath Kumar Potu 1 , Vasavi Rakesh Gorantla 1 , Muddanna S. Rao 1 , Sampath Madhyastha 2 , Venkata Ramana Vollala 3 Abstract Background: Considering the paucity of information presently available concerning inferior phrenic arteries, a more definitive study seemed appropriate and necessary, both for its potential clinical applications and to provide additional data to contemporary anatomical literature. Objective: Most anatomical textbooks of gross anatomy offer very little information concerning the anatomy and distribution of the inferior phrenic artery (IPA). For that reason, the origin of the IPA has been studied and the available literature has been reviewed. Methods: Thirty-two human adult cadavers preserved in formalin obtained from the departments of Anatomy, Kasturba Medical College, Manipal and Mangalore were dissected and the origin of the IPA was studied. Results: The IPA had its usual origin from the abdominal aorta in 28 cases but in the remaining four cases, two were arising from the celiac trunk, one from the left gastric artery and one from the right renal artery. Conclusion: The IPA usually originates from the aorta or celiac artery, and less frequently from the renal, hepatic or left gastric arteries. The IPA is a major source of collateral or parasitized arterial supply to hepatocellular carcinoma, second only to the hepatic artery. Literature on the IPA origin and clinical implications of variation in its origin have been reviewed in this article. Keywords: Inferior phrenic arteries, hepatocellular carcinoma, embolization, vascular variations. Resumo Contexto: Considerando a escassez de informações atualmente disponíveis sobre artérias frênicas inferiores, um estudo mais definitivo nos pareceu apropriado e necessário, tanto por suas potenciais aplicações clínicas quanto para fornecer dados adicionais à literatura anatômica contemporânea. Objetivo: A maioria dos livros-texto de anatomia oferece muito poucas informações referentes à anatomia e distribuição da artéria frênica inferior (AFI). Por este motivo, a origem da AFI foi investigada e a literatura disponível foi revisada. Métodos: Trinta e dois cadáveres humanos adultos preservados em formol e obtidos dos departamentos de anatomia do Kasturba Medical College, Manipal and Mangalore foram dissecados, e a origem da AFI foi investigada. Resultados: A AFI teve sua origem habitual na aorta abdominal em 28 casos; no entanto, nos quatro casos restantes, duas originavam-se do tronco celíaco, uma da artéria gástrica esquerda e uma da artéria renal direita. Conclusão: A AFI geralmente origina-se da aorta ou artéria celíaca, e menos freqüentemente das artérias renal, hepática ou gástrica esquerda. A AFI é a maior fonte de fornecimento arterial colateral ou parasitado para carcinoma hepatocelular, ficando atrás somente da artéria hepática. A literatura sobre a origem da AFI e as implicações clínicas de variação em sua origem foram revisadas neste artigo. Palavras-chave: Artérias frênicas inferiores, carcinoma hepatocelular, embolização, variações vasculares. Introduction Although descriptions of the right inferior phrenic artery (RIPA) and left inferior phrenic artery (LIPA) are typically very brief and lacking in detail in anatomy text- books, they have received increased attention in recent years in the clinical literature. This stems largely from the discovery of the involvement of the right (most fre- quently) or left inferior phrenic arteries in the arterial supply and growth of hepatocellular carcinoma (HCC). 1,2 Indeed, the great importance of such knowl- edge lies in the fact that an unresectable HCC can be treated by transcatheter embolization of not only its typi- cal blood supply, the right or left hepatic arteries, but also by embolization of a RIPA, if involved. 1-4 Accordingly, with the appropriately targeted utiliza- tion of certain current cancer treatments hinging on a 1. Department of Anatomy, Kasturba Medical College, Manipal, Karnataka, India. 2. Department of Anatomy, Kasturba Medical College, Mangalore, Karnataka, India. 3. Department of Anatomy, Melaka Manipal Medical College, Manipal, Karnataka, India. Manuscript received May 21, 2007, accepted for publication Jun 08, 2007. J Vasc Bras 2007;6(3):225-230. Copyright © 2007 by Sociedade Brasileira de Angiologia e de Cirurgia Vascular 225
-
Upload
independent -
Category
Documents
-
view
0 -
download
0
Transcript of The origin of the inferior phrenic artery: a study in 32 South Indian cadavers with a review of the...

ORIGINAL ARTICLE
The origin of the inferior phrenic artery: a study in 32South Indian cadavers with a review of the literature
Origem da artéria frênica inferior: estudo em 32 cadáveres da Índiado Sul com revisão da literatura
Thejodhar Pulakunta1, Bhagath Kumar Potu1, Vasavi Rakesh Gorantla1, Muddanna S. Rao1,Sampath Madhyastha2, Venkata Ramana Vollala3
AbstractBackground: Considering the paucity of information presently
available concerning inferior phrenic arteries, a more definitive studyseemed appropriate and necessary, both for its potential clinicalapplications and to provide additional data to contemporaryanatomical literature.
Objective: Most anatomical textbooks of gross anatomy offer verylittle information concerning the anatomy and distribution of theinferior phrenic artery (IPA). For that reason, the origin of the IPAhas been studied and the available literature has been reviewed.
Methods: Thirty-two human adult cadavers preserved in formalinobtained from the departments of Anatomy, Kasturba MedicalCollege, Manipal and Mangalore were dissected and the origin of theIPA was studied.
Results: The IPA had its usual origin from the abdominal aorta in28 cases but in the remaining four cases, two were arising from theceliac trunk, one from the left gastric artery and one from the rightrenal artery.
Conclusion: The IPA usually originates from the aorta or celiacartery, and less frequently from the renal, hepatic or left gastric arteries.The IPA is a major source of collateral or parasitized arterial supplyto hepatocellular carcinoma, second only to the hepatic artery.Literature on the IPA origin and clinical implications of variation inits origin have been reviewed in this article.
Keywords: Inferior phrenic arteries, hepatocellular carcinoma,embolization, vascular variations.
ResumoContexto: Considerando a escassez de informações atualmente
disponíveis sobre artérias frênicas inferiores, um estudo mais definitivonos pareceu apropriado e necessário, tanto por suas potenciaisaplicações clínicas quanto para fornecer dados adicionais à literaturaanatômica contemporânea.
Objetivo: A maioria dos livros-texto de anatomia oferece muitopoucas informações referentes à anatomia e distribuição da artériafrênica inferior (AFI). Por este motivo, a origem da AFI foi investigadae a literatura disponível foi revisada.
Métodos: Trinta e dois cadáveres humanos adultos preservadosem formol e obtidos dos departamentos de anatomia do KasturbaMedical College, Manipal and Mangalore foram dissecados, e a origemda AFI foi investigada.
Resultados: A AFI teve sua origem habitual na aorta abdominalem 28 casos; no entanto, nos quatro casos restantes, duas originavam-sedo tronco celíaco, uma da artéria gástrica esquerda e uma da artériarenal direita.
Conclusão: A AFI geralmente origina-se da aorta ou artériacelíaca, e menos freqüentemente das artérias renal, hepática ou gástricaesquerda. A AFI é a maior fonte de fornecimento arterial colateral ouparasitado para carcinoma hepatocelular, ficando atrás somente daartéria hepática. A literatura sobre a origem da AFI e as implicaçõesclínicas de variação em sua origem foram revisadas neste artigo.
Palavras-chave: Artérias frênicas inferiores, carcinomahepatocelular, embolização, variações vasculares.
IntroductionAlthough descriptions of the right inferior phrenic
artery (RIPA) and left inferior phrenic artery (LIPA) aretypically very brief and lacking in detail in anatomy text-books, they have received increased attention in recentyears in the clinical literature. This stems largely fromthe discovery of the involvement of the right (most fre-quently) or left inferior phrenic arteries in the arterial
supply and growth of hepatocellular carcinoma(HCC).1,2 Indeed, the great importance of such knowl-edge lies in the fact that an unresectable HCC can betreated by transcatheter embolization of not only its typi-cal blood supply, the right or left hepatic arteries, butalso by embolization of a RIPA, if involved.1-4
Accordingly, with the appropriately targeted utiliza-tion of certain current cancer treatments hinging on a
1 . Department of Anatomy, Kasturba Medical College, Manipal, Karnataka, India.2 . Department of Anatomy, Kasturba Medical College, Mangalore, Karnataka, India.3 . Department of Anatomy, Melaka Manipal Medical College, Manipal, Karnataka, India.
Manuscript received May 21, 2007, accepted for publication Jun 08, 2007.
J Vasc Bras 2007;6(3):225-230.Copyright © 2007 by Sociedade Brasileira de Angiologia e de Cirurgia Vascular
225

thorough knowledge of the origin of the IPA, our cur-
rent study aimed at establishing this very fact. There are
few publications concerning the role and detailed
anatomy of the IPA with respect to their involvement in
HCC1,2,5 and, similarly, few have been produced with
direct focus on the elucidation of the origin and distri-
bution of these arteries.1,2,6 Quain, quoted by Pick &
Anson,7 was the first author to describe the origin of
the IPA. Tanabe et al.1 referred only to general textbook
descriptions of these arteries and Gokan et al.2 reported
on frequency of origin of the RIPA in a study of 16
patients. A study of 74 cadavers by Adachi8 is the larg-
est available concerning IPA. Modern anatomy text-
books offer few details of the anatomy of the inferior
phrenic arteries.9-11 Because transcatheter embolization
of HCC and other hepatic neoplasms often involves find-
ing the root of the RIPA, the interventional radiologist
or oncologist could potentially benefit from knowledge
of common variations in origin of these vessels and their
respective frequencies of occurrence. The importance of
the IPA is not limited to the treatment of HCC. Practi-
cally any hepatic neoplasm (including metastatic dis-
ease to the liver) may receive blood supply from the IPA.
In addition, there have been reports of gastric hemor-
rhage due to bleeding from the LIPA after treatment of
the left gastric artery with embolization.12
Vascular variations are constantly observed in dis-
section of adult cadavers.13 The inferior phrenic arter-
ies usually originate from the aorta or celiac artery, and
less frequently from the renal, hepatic or left gastric arter-
ies. The roentgenographic anatomy of the phrenic arter-
ies has been described in detail by Kahn et al.14 They
contribute to the arterial supply of the adrenal glands
and are thus important in angiographic examinations
for adrenal lesions.14,15
In general, these vessels, which supply the dia-
phragm, are of small caliber.13,16,17 The purpose of this
study was to analyze the origin of the inferior phrenic
arteries.
Methods
Thirty-two human adult cadavers preserved in for-
malin, obtained from the departments of anatomy, Kas-
turba Medical College, Manipal and Mangalore were
dissected and the origin of the inferior phrenic artery
was studied. The ages of the cadavers ranged between
28-56 years. To dissect the abdominal aorta, the pan-
creas was removed with the aid of scissors. All the gan-
glions and the nervous tissue around the arteries were
removed with the aid of a pincer and scissors to allow
observing the disposition of these inferior phrenic arter-
ies. After resection of tissues subjacent to the diaphrag-
matic crura and adherent tissues all along the median
arcuate ligament, these structures were exposed, allow-
ing observation of the origin of the IPA.
Results
The inferior phrenic artery showed a variant origin
in four out of 32 cases. It was seen to arise directly from
the celiac trunk in two cases (Figures 1 and 2) and there
was one case arising from the left gastric artery (Figure 3)
and another from the right renal artery (Figure 4). The
observations have been tabulated below in Table 1 and
Figure 5.
Table 1 - Gender, age, side and origin of the variant cases
Serial no Gender Age Side Origin
Case 1 Male 43 Left Celiac Trunk
Case 2 Female 29 Bilateral Celiac Trunk
Case 3 Male 35 Left Gastric Artery
Case 4 Female 54 Right Renal Artery*
* A coexisting supernumerary right renal artery from the aorta was also observed.
226 J Vasc Bras 2007, Vol. 6, Nº 3 The origin of the inferior phrenic artery – Pulakunta T et al.

Discussion
Considering the paucity of information presently
available concerning these arteries, a more definitive
study seemed appropriate and necessary, both for its
potential clinical applications and to provide additional
data to contemporary anatomical literature. In describ-
ing the origins of the IPA, the fourth edition of Mastery
of Surgery11 gives only brief mention of the aorta or
AA = abdominal aorta; ARRA = accessory right renal artery; IVC = inferiorvena cava; RIPA = right inferior phrenic artery; RK = right kidney; RRA =right renal artery; RSRG = right suprarenal gland.
Figure 4 - Right inferior phrenic artery arising from the rightrenal artery (case 4)
AA = abdominal aorta; CHA = common hepatic artery; CT = celiac trunk;LIPA = left inferior phrenic artery; SA = splenic artery.
Figure 1 - Left inferior phrenic artery arising from the celiactrunk (case 1). Splenic artery is reflected to the rightside, to show the origin of left inferior phrenicartery from celiac trunk
BD = bile duct; CA = cystic artery; CHA = common hepatic artery; CT = celiactrunk; GDA = gastroduodenal artery; LGA = left gastric artery; LHA = lefthepatic artery; LIPA = left inferior phrenic artery; RHA = right hepatic artery;RIPA = right inferior phrenic artery; RLL = right lobe of the liver; SA = splenicartery.
Figure 2 - Right and left inferior phrenic arteries arising fromthe celiac trunk (case 2)
CT = celiac trunk; LGA = left gastric artery; LIPA = left inferior phrenic artery;SA = splenic artery; SMA = superior mesenteric artery.
Figure 3 - Left inferior phrenic artery arising from the leftgastric artery (case 3)
The origin of the inferior phrenic artery – Pulakunta T et al. J Vasc Bras 2007, Vol. 6, Nº 3 227
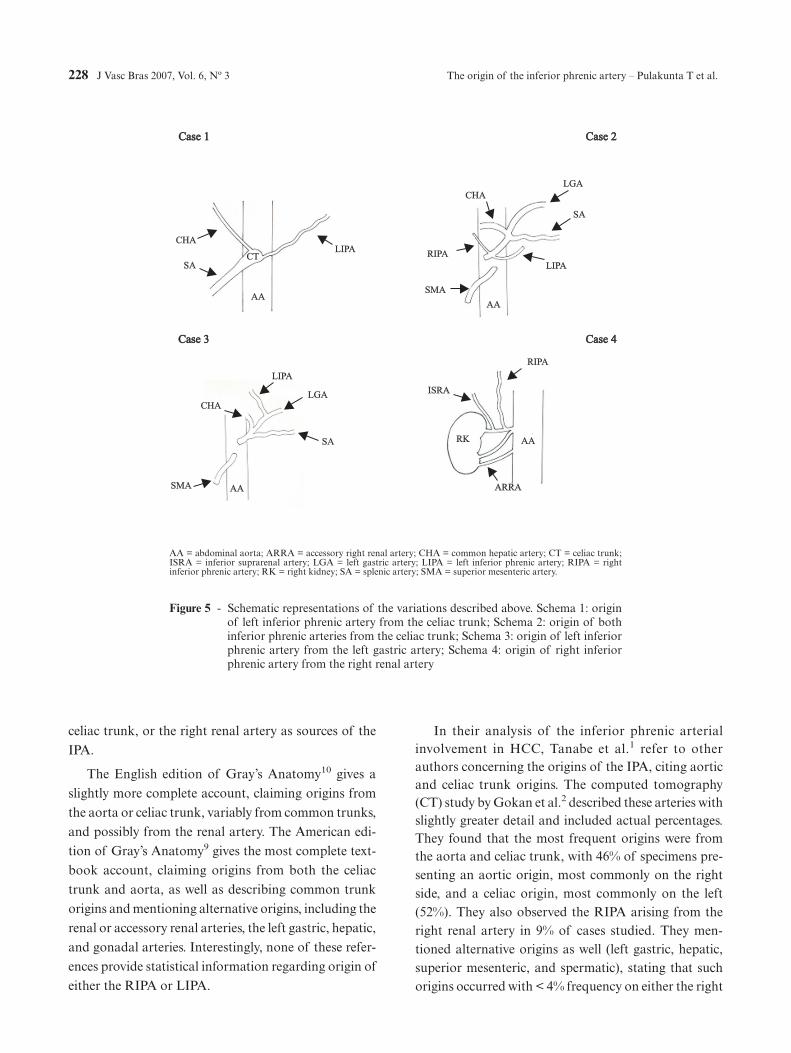
celiac trunk, or the right renal artery as sources of the
IPA.
The English edition of Gray’s Anatomy10 gives a
slightly more complete account, claiming origins from
the aorta or celiac trunk, variably from common trunks,
and possibly from the renal artery. The American edi-
tion of Gray’s Anatomy9 gives the most complete text-
book account, claiming origins from both the celiac
trunk and aorta, as well as describing common trunk
origins and mentioning alternative origins, including the
renal or accessory renal arteries, the left gastric, hepatic,
and gonadal arteries. Interestingly, none of these refer-
ences provide statistical information regarding origin of
either the RIPA or LIPA.
In their analysis of the inferior phrenic arterialinvolvement in HCC, Tanabe et al.1 refer to otherauthors concerning the origins of the IPA, citing aorticand celiac trunk origins. The computed tomography(CT) study by Gokan et al.2 described these arteries withslightly greater detail and included actual percentages.They found that the most frequent origins were fromthe aorta and celiac trunk, with 46% of specimens pre-senting an aortic origin, most commonly on the rightside, and a celiac origin, most commonly on the left(52%). They also observed the RIPA arising from theright renal artery in 9% of cases studied. They men-tioned alternative origins as well (left gastric, hepatic,superior mesenteric, and spermatic), stating that suchorigins occurred with < 4% frequency on either the right
Case 1Case 1 Case 2Case 2
Case 3Case 3 Case 4Case 4
CT
CHA
AA
SA
LIPA
SMA
CHA
AA
SA
LIPA
LGA
LGA
CHA
SA
LIPA
SMA
AA
RIPA
AARK
RIPA
ARRA
ISRA
AA = abdominal aorta; ARRA = accessory right renal artery; CHA = common hepatic artery; CT = celiac trunk;ISRA = inferior suprarenal artery; LGA = left gastric artery; LIPA = left inferior phrenic artery; RIPA = rightinferior phrenic artery; RK = right kidney; SA = splenic artery; SMA = superior mesenteric artery.
Figure 5 - Schematic representations of the variations described above. Schema 1: originof left inferior phrenic artery from the celiac trunk; Schema 2: origin of bothinferior phrenic arteries from the celiac trunk; Schema 3: origin of left inferiorphrenic artery from the left gastric artery; Schema 4: origin of right inferiorphrenic artery from the right renal artery
228 J Vasc Bras 2007, Vol. 6, Nº 3 The origin of the inferior phrenic artery – Pulakunta T et al.

or left sides. Anatomical studies by Anson & McVay18
provided illustrations that depicted the IPA situated at
various levels vertically, but originating only from the
aorta or celiac trunk. No numerical data were provided
in their study. In an examination of 68 Japanese cadav-
ers, Piao et al.6 found the majority of the IPA arising
from the aorta (61.6%), with 28.2% of the IPA originat-
ing from the celiac trunk, and the remainder originating
from either renal, left gastric, or middle adrenal arter-
ies. Pick & Anson7 gave an impressive account of their
findings concerning various aspects of the inferior
phrenic arteries in their dissection of 200 cadavers.
Regarding origins, they found aortic and celiac sources
to be the most common (45.1 and 47.8%, respectively).
They claimed common trunks variably for both as well,
and even a common origin with the right internal sper-
matic artery. They found that < 7% arose variably from
the renal (5.8%), left gastric (2.3%), or hepatic arteries
(0.3%). This work is by far the most complete account
to date of the IPA origins.
However, in the current study the origin of the IPA
arteries from the celiac trunk was observed in two cases
(6.25%), one from the left gastric artery (3.125%) and
one from the right renal artery (3.125%) out of the 32
cadavers. In the remaining 28 cases it had its normal ori-
gin from the abdominal aorta. Loukas et al.19 reported
that, out of 300 cadavers they studied, the right IPA
originated from: a) celiac trunk in 40% of the speci-
mens; b) aorta in 38%; c) renal in 17%; d) left gastric in
3%; and e) hepatic artery proper in 2% of the speci-
mens. The left IPA originated from: a) celiac trunk in
47%; b) aorta in 45%; c) renal in 5%; d) left gastric in
2%; and e) hepatic artery proper in 1% of the speci-
mens. The current study showed similar findings, except
for the fact that the frequency of the IPA originating
from the celiac trunk was much lesser.
The IPA is a major source of collateral or parasit-
ized arterial supply to HCC, second only to the hepatic
artery.19 The right IPA was always associated with HCC
and served as the major collateral artery adjunct to the
hepatic artery. These findings could have major impli-
cations in the transcatheter embolization of HCC
patients. The knowledge of this type of variation shows
that surgeons must be cautious to avoid unintentional
sectioning of small-caliber arteries, as it may occur dur-
ing celiac artery decompression in compression syn-
drome of the celiac trunk by the median arcuate
ligament.
Presence of a supernumerary renal artery (as
observed in case 4) is due to the abnormal disappear-
ance or lack of formation of the lateral mesonephric
arteries and their connecting channels.20,21
We hope this study has provided valuable data to
researchers, clinicians and anatomists alike by enhanc-
ing the understanding of both the specific anatomy of
the inferior phrenic arteries and their potential signifi-
cance in supplying HCC and any number of other
tumors, primary or metastatic, to the liver, such as cho-
langiocarcinoma, hepatoblastoma and subcapsular
adenoma.22 For the clinician, in particular, treatments
such as transcatheter embolization of HCC call for
extensive knowledge of all possible variations of these
vessels, particularly their origins, and it is conceivable
that the application of this data will prove useful in the
discussion and treatment of other hepatic, suprarenal
or even diaphragmatic lesions unforeseen at the present
time.19
Acknowledgements
We would like to thank Dr. Narga Nair, Professor
and Head of the Department of Anatomy, KMC,
Manipal for her support. We would also like to thank
Mr. Nagaraj, Senior Artist, Center for Basic Sciences,
KMC, Manipal for his assistance with the illustrations.
A special thanks to Dr. Marios Loukas, MD, PhD,
Department of Anatomy, American University of the
Caribbean, Jordan Road, Cupecoy, Lowlands, Saint
Maarten, Netherlands Antilles for his help.
References1. Tanabe N, Iwasaki T, Chida N, et al. Hepatocellular carcino-
mas supplied by inferior phrenic arteries. Acta Radiol.1998;39:443-6.
2. Gokan T, Hashimoto T, Matsui S, Kushihashi T, NobusawaH, Munechika H. Helical CT demonstration of dilated rightinferior phrenic arteries as extrahepatic collateral arteries ofhepatocellular carcinomas. J Comput Assist Tomogr.2001;25:68-73.
The origin of the inferior phrenic artery – Pulakunta T et al. J Vasc Bras 2007, Vol. 6, Nº 3 229
http://www.ncbi.nlm.nih.gov/entrez/query.fcgi?cmd=Retrieve&db=pubmed&dopt=abstract&list_uids=9685835

3. Chung JW, Park JH, Han JK, Choi BI, Kim TK, Han MC.Transcatheter oily chemoembolization of the inferior phrenicartery in hepatocellular carcinoma: the safety and potentialtherapeutic role. J Vasc Interv Radiol. 1998;9:495-500.
4. Duprat G, Charnsangavej C, Wallace S, Carrasco CH. Infe-rior phrenic artery embolization in the treatment of hepaticneoplasms. Acta Radiol. 1988;29:427-9.
5. Andrews JC, Williams DM, Cho KJ, Knol JA, Wahl RL, Ens-minger WD. Unsatisfactory hepatic perfusion after place-ment of an implanted pump and catheter system: angiographiccorrelation. Radiology. 1989;173:779-81.
6. Piao DX, Ohtsuka A, Murakami T. Typology of abdominalarteries, with special reference to inferior phrenic arteries andtheir esophageal branches. Acta Med Okayama.1998;52:189-96.
7. Pick JW, Anson BJ. The inferior phrenic artery: origin andsuprarenal branches. Anat Rec. 1940;78:413-27.
8. Adachi B. Das arteriensystem der japaner. Kyoto: Kaierlich-Japanichen Universitat; 1928;1:29-41.
9. Gray H. Anatomy of the human body. 30th ed. Baltimore:Williams & Wilkins; 1985. p. 746-7.
10. Gray H. Gray’s anatomy. 38th ed. London: Churchill Living-stone; 1999. p. 1558.
11. Baker RJ, Fischer JE. Mastery of surgery. 4th ed. In: Philadel-phia: Lippincott, Williams & Wilkins; 2001; p. 691–692.
12. Northrop CH, Studley MA, Smith GR. Hemorrhage from thegastroesophageal junction. A cryptic angiographic diagnosis.Radiology. 1975;117(3 Pt 1):531-2.
13. Lipshutz B. A composite study of the coeliac trunkartery. Am.Surg. 1917;65:159-69.
14. Kahn PC. Selective angiography of inferior phrenic arteries.Radiology. 1967;88:1-8.
15. Kahn PC, Nickrosz LV. Selective angiography of adrenalglands. Am J Roentgenol Radium Ther Nucl Med.1967;101:739-49.
16. Michels NA. The hepatic, cystic and retroduodenal arteriesand their relations to the biliary ducts. Ann. Surg.1951;133:503-24.
17. Michels NA. Collateral arterial pathways to the liver after liga-tion of the hepatic artery and removal of the celiac axis. Can-cer. 1953;6:708-24.
18. Anson BJ, McVay CB. The topographical positions and themutual relations of the visceral branches of the abdominalaorta: a study of 100 consecutive cadavers. Anat Rec.1936;67:7-15.
19. Loukas M, Hullett J, Wagner T. Clinical anatomy of the infe-rior phrenic artery. Clin. Anat. 2005;18:357-65.
20. Moore KL. The developing human. Philadelphia: WB Saun-ders; 1973. p. 221.
21. Gray H. Gray's anatomy. 37th ed. Edinburgh: Churchill Liv-ingstone; 1989. p. 256-8; 1407-9.
22. Cotran RS, Kumar V, Robbins SL. Robbins pathologic basisof disease. 5th ed. Philadelphia: WB Saunders; 1994. p. 831-71.
Correspondence:Bhagath Kumar.PotuDepartment of Anatomy, Center for Basic SciencesKasturba Medical College576104Manipal, Karnataka – IndiaTel.: + 91 820 2922327E-mail: [email protected]
230 J Vasc Bras 2007, Vol. 6, Nº 3 The origin of the inferior phrenic artery – Pulakunta T et al.
http://www.ncbi.nlm.nih.gov/entrez/query.fcgi?cmd=Retrieve&db=pubmed&dopt=abstract&list_uids=9618112
http://www.ncbi.nlm.nih.gov/entrez/query.fcgi?cmd=Retrieve&db=pubmed&dopt=abstract&list_uids=9618112
http://www.ncbi.nlm.nih.gov/entrez/query.fcgi?cmd=Retrieve&db=pubmed&dopt=abstract&list_uids=9618112
http://www.ncbi.nlm.nih.gov/entrez/query.fcgi?cmd=Retrieve&db=pubmed&dopt=abstract&list_uids=3408603
http://www.ncbi.nlm.nih.gov/entrez/query.fcgi?cmd=Retrieve&db=pubmed&dopt=abstract&list_uids=3408603
http://www.ncbi.nlm.nih.gov/entrez/query.fcgi?cmd=Retrieve&db=pubmed&dopt=abstract&list_uids=3408603
http://www.ncbi.nlm.nih.gov/entrez/query.fcgi?cmd=Retrieve&db=pubmed&dopt=abstract&list_uids=2813786
http://www.ncbi.nlm.nih.gov/entrez/query.fcgi?cmd=Retrieve&db=pubmed&dopt=abstract&list_uids=2813786
http://www.ncbi.nlm.nih.gov/entrez/query.fcgi?cmd=Retrieve&db=pubmed&dopt=abstract&list_uids=2813786
http://www.ncbi.nlm.nih.gov/entrez/query.fcgi?cmd=Retrieve&db=pubmed&dopt=abstract&list_uids=9781269
http://www.ncbi.nlm.nih.gov/entrez/query.fcgi?cmd=Retrieve&db=pubmed&dopt=abstract&list_uids=9781269
http://www.ncbi.nlm.nih.gov/entrez/query.fcgi?cmd=Retrieve&db=pubmed&dopt=abstract&list_uids=9781269
http://www.ncbi.nlm.nih.gov/entrez/query.fcgi?cmd=Retrieve&db=pubmed&dopt=abstract&list_uids=1081239
http://www.ncbi.nlm.nih.gov/entrez/query.fcgi?cmd=Retrieve&db=pubmed&dopt=abstract&list_uids=1081239
http://www.ncbi.nlm.nih.gov/entrez/query.fcgi?cmd=Retrieve&db=pubmed&dopt=abstract&list_uids=6015613
http://www.ncbi.nlm.nih.gov/entrez/query.fcgi?cmd=Retrieve&db=pubmed&dopt=abstract&list_uids=6060063