Postoperative Phrenic Nerve Palsy in Patients with Open-Heart Surgery
6
Postoperative Phrenic Nerve Palsy in Patients with Open-Heart Surgery Omkar N. Markand, M.D., F.R.C.P.(C), S. S. Moorthy, M.D., Yousuf Mahomed, M.D., Robert D. King, M.D., and John W. Brown, M.D. ABSTRACT We prospectively studied patients undergo- ing open-heart surgical procedures to evaluate the role of phrenic nerve palsy in the causation of the high incidence of pulmonary complications reported in these patients. Al- though atelectasis, or infiltrates, or both developed in the left lower lobe of 98% of the patients (43 of 44) with or without similar changes on the right side, only 5 (11%) of the 44 patients had diaphragmatic dysfunction following operation. in 1, the left phrenic nerve became inexcitable; 2 had paresis of the left hemidiaphragm, and 2 had paresis of the right hemidiaphragm. Although damage to the phrenic nerve can occur during open-heart operations, a relatively low incidence of this complication does not sup- port it as the major cause of postoperative pulmonary com- plications. Atelectasis, usually of the left lower lobe, has been rec- ognized as a common postoperative complication in pa- tients undergoing open-heart surgical procedures, but the cause has remained controversial. Mechanical fac- tors, such as retraction of the left lower lobe during oper- ation or postoperative gastric distention, have been con- sidered by some, whereas others have implied transient paresis of the left hemidiaphragm secondary to surgical or hypothermic injury to the phrenic nerve [l, 21. We carried out a prospective study of patients undergoing open-heart surgical procedures to evaluate their dia- phragmatic function by transcutaneous phrenic nerve stimulation in the neck before and after the operation. Material and Methods Fifty patients undergoing open-heart procedures at the Indiana University Hospital from January to June, 1983, were included in the study. The study had prior ap- proval by the Indiana University School of Medicine committee on protection of human subjects. Informed consent was obtained before each patient entered the study. The patients ranged in age from 31 to 72 years with a mean age of 56 years. There were 38 men and 12 women. The surgical procedures included 35 coronary artery bypass operations, 7 aortic valve replacements, 4 mitral valve replacements, 1 combined aortic and mitral valve replacement, 2 combined coronary artery bypass From the Departments of Neurology, Anesthesia, and Surgery, Indiana University School of Medicine, Indianapolis, IN. Accepted for publication Mar 30, 1984. Address reprint requests to Dr. Markand, Department of Neurology, Riley A599N, 702 Barnhill Dr, Indianapolis, IN 46223. and aortic valve replacement procedures, and 1 repair of a congenital atrial septa1 defect. None of the patients undergoing coronary artery bypass in this series had internal mammary artery grafts. Phrenic nerve conduction was assessed usually 1 to 2 days before the operation and repeated 6 to 8 days after the operation, by which time the lateral part of the lower chest was free of bandages and a satisfactory recording could be obtained. We recently described the technique of transcutaneous phrenic nerve stimulation in detail [3]. In short, the left and right phrenic nerves were stimu- lated percutaneously at the posterior border of the ster- nocleidomastoid muscles at the level of the upper part of the thyroid cartilage. The diaphragmatic potential was recorded from surface disc electrodes placed over the ipsilateral seventh intercostal space close to the costal margin (7CS) with reference to an electrode over the xiphoid process (XP) or the opposite knee. The graphs were plotted such that the positivity at the 7CS electrode resulted in an upgoing waveform. To ensure exactly the same location of the XP and 7CS recording electrodes for the preoperative and postopera- tive phrenic studies, distances were measured in each patient between the suprasternal notch and XP electrode and between the XP and the two 7CS electrodes at the time of preoperative assessment. These measurements allowed proper placement of electrodes during the post- operative study when the landmarks were not easily identifiable because of the midsternal incision and the associated superficial edema. A diaphragmatic potential of less than 0.4 mV in am- plitude or more than 10 msec in latency was considered abnormal. Also, a leftkight amplitude ratio of the dia- phragmatic potential of more than 2.0 or less than 0.5 was considered abnormal. All patients had radiographs of the chest before the operation and at variable intervals (usually three to five times) during the first week after the operation. The presence and location of infiltrates and atelectasis and the position of the hemidiaphragm were noted for each examination. We also obtained the following data: dura- tion of cardiopulmonary bypass, use of topical ice or cold solution for cardiac cooling, lowest myocardial tem- perature, length of intubation, and duration of hospital stay. Student t and chi-square tests were used for statis- tical analysis; a p value less than 0.05 was considered statistically significant. During the same study period, an additional 7 pa- tients were evaluated with phrenic studies because they had respiratory difficulty after cardiothoracic surgical procedures. 68
-
Upload
independent -
Category
Documents
-
view
5 -
download
0
Transcript of Postoperative Phrenic Nerve Palsy in Patients with Open-Heart Surgery

Postoperative Phrenic Nerve Palsy in Patients with Open-Heart Surgery Omkar N. Markand, M.D., F.R.C.P.(C), S. S. Moorthy, M.D., Yousuf Mahomed, M.D., Robert D. King, M.D., and John W. Brown, M.D.
ABSTRACT We prospectively studied patients undergo- ing open-heart surgical procedures to evaluate the role of phrenic nerve palsy in the causation of the high incidence of pulmonary complications reported in these patients. Al- though atelectasis, or infiltrates, or both developed in the left lower lobe of 98% of the patients (43 of 44) with or without similar changes on the right side, only 5 (11%) of the 44 patients had diaphragmatic dysfunction following operation. in 1, the left phrenic nerve became inexcitable; 2 had paresis of the left hemidiaphragm, and 2 had paresis of the right hemidiaphragm. Although damage to the phrenic nerve can occur during open-heart operations, a relatively low incidence of this complication does not sup- port it as the major cause of postoperative pulmonary com- plications.
Atelectasis, usually of the left lower lobe, has been rec- ognized as a common postoperative complication in pa- tients undergoing open-heart surgical procedures, but the cause has remained controversial. Mechanical fac- tors, such as retraction of the left lower lobe during oper- ation or postoperative gastric distention, have been con- sidered by some, whereas others have implied transient paresis of the left hemidiaphragm secondary to surgical or hypothermic injury to the phrenic nerve [l, 21. We carried out a prospective study of patients undergoing open-heart surgical procedures to evaluate their dia- phragmatic function by transcutaneous phrenic nerve stimulation in the neck before and after the operation.
Material and Methods Fifty patients undergoing open-heart procedures at the Indiana University Hospital from January to June, 1983, were included in the study. The study had prior ap- proval by the Indiana University School of Medicine committee on protection of human subjects. Informed consent was obtained before each patient entered the study. The patients ranged in age from 31 to 72 years with a mean age of 56 years. There were 38 men and 12 women. The surgical procedures included 35 coronary artery bypass operations, 7 aortic valve replacements, 4 mitral valve replacements, 1 combined aortic and mitral valve replacement, 2 combined coronary artery bypass
From the Departments of Neurology, Anesthesia, and Surgery, Indiana University School of Medicine, Indianapolis, IN.
Accepted for publication Mar 30, 1984.
Address reprint requests to Dr. Markand, Department of Neurology, Riley A599N, 702 Barnhill Dr, Indianapolis, IN 46223.
and aortic valve replacement procedures, and 1 repair of a congenital atrial septa1 defect. None of the patients undergoing coronary artery bypass in this series had internal mammary artery grafts.
Phrenic nerve conduction was assessed usually 1 to 2 days before the operation and repeated 6 to 8 days after the operation, by which time the lateral part of the lower chest was free of bandages and a satisfactory recording could be obtained. We recently described the technique of transcutaneous phrenic nerve stimulation in detail [ 3 ] . In short, the left and right phrenic nerves were stimu- lated percutaneously at the posterior border of the ster- nocleidomastoid muscles at the level of the upper part of the thyroid cartilage. The diaphragmatic potential was recorded from surface disc electrodes placed over the ipsilateral seventh intercostal space close to the costal margin (7CS) with reference to an electrode over the xiphoid process (XP) or the opposite knee. The graphs were plotted such that the positivity at the 7CS electrode resulted in an upgoing waveform.
To ensure exactly the same location of the XP and 7CS recording electrodes for the preoperative and postopera- tive phrenic studies, distances were measured in each patient between the suprasternal notch and XP electrode and between the XP and the two 7CS electrodes at the time of preoperative assessment. These measurements allowed proper placement of electrodes during the post- operative study when the landmarks were not easily identifiable because of the midsternal incision and the associated superficial edema.
A diaphragmatic potential of less than 0.4 mV in am- plitude or more than 10 msec in latency was considered abnormal. Also, a leftkight amplitude ratio of the dia- phragmatic potential of more than 2.0 or less than 0.5 was considered abnormal.
All patients had radiographs of the chest before the operation and at variable intervals (usually three to five times) during the first week after the operation. The presence and location of infiltrates and atelectasis and the position of the hemidiaphragm were noted for each examination. We also obtained the following data: dura- tion of cardiopulmonary bypass, use of topical ice or cold solution for cardiac cooling, lowest myocardial tem- perature, length of intubation, and duration of hospital stay. Student t and chi-square tests were used for statis- tical analysis; a p value less than 0.05 was considered statistically significant.
During the same study period, an additional 7 pa- tients were evaluated with phrenic studies because they had respiratory difficulty after cardiothoracic surgical procedures.
68
69 Markand et al: Phrenic Nerve Palsy after Open-Heart Surgery
Results All 50 patients included in the study had preoperative assessment of their phrenic nerve function, but postop- erative evaluation could be completed in only 44 pa- tients. Four patients declined postoperative phrenic studies because of discomfort associated with the electri- cal stimulation of the phrenic nerves during the preoperative evaluation. Two patients could not be re- studied because the electrophysiologist (0. N. M.) was not available to perform the test. Thus, data were ana- lyzed for the 44 patients who had both preoperative and postoperative electrophysiological studies.
The preoperative radiographs of the chest showed no infiltrate or atelectasis except in 1 patient with subseg- mental bibasilar atelectasis that was more extensive on the left side. Postoperatively all patients had three or more studies in the first week after operation. Forty- three patients (98%) showed atelectasis, or infiltrates, or both in one or more of the postoperative radiographs. Changes occurred only in the left base in 13 (30%), whereas 30 (70%) had bilateral changes. In patients with bilateral pulmonary atelectasis, infiltrates, or both, the alterations generally were more severe on the left side. The changes initially occurred on the left side with sub- sequent development of similar abnormalities on the
right side. The chest radiographs usually showed more severe alterations 2 days after the operation rather than in the immediate postoperative period.
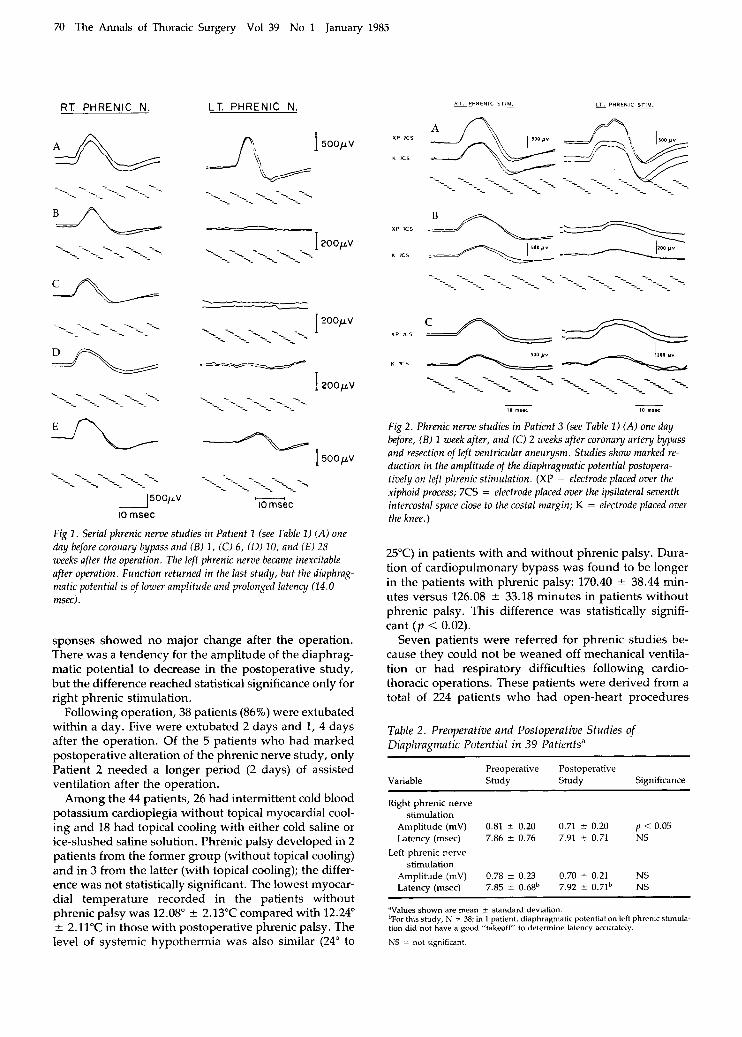
In all patients, the amplitude and the latency of the diaphragmatic potential were normal in the preoperative studies. Postoperatively, 5 patients had marked changes in their phrenic studies (Table 1). Patient 1 had the most prominent change; his left phrenic nerve became totally inexcitable. It remained so for four months before the function returned in the last study performed 28 weeks after the operation (Fig 1). In 2 patients (Nos. 3, 4, see Table 1) the left and in 2 (Nos. 2, 5), the right phrenic responses were markedly reduced in amplitude (Fig 2). The 3 patients with abnormal electrical responses to left phrenic stimulation also demonstrated elevation of the left hemidiaphragm on chest radiograph. On the other hand, the 2 patients with right phrenic abnormality on electrical study failed to show radiological findings of hemidiaphragmatic paresis.
After the 5 patients with obvious postoperative changes in phrenic nerve function were excluded, the mean values for amplitude and latency of the diaphrag- matic potential in the remaining 39 patients in the opera- tive and postoperative studies were compared (Table 2). The latency of the right and left diaphragmatic re-
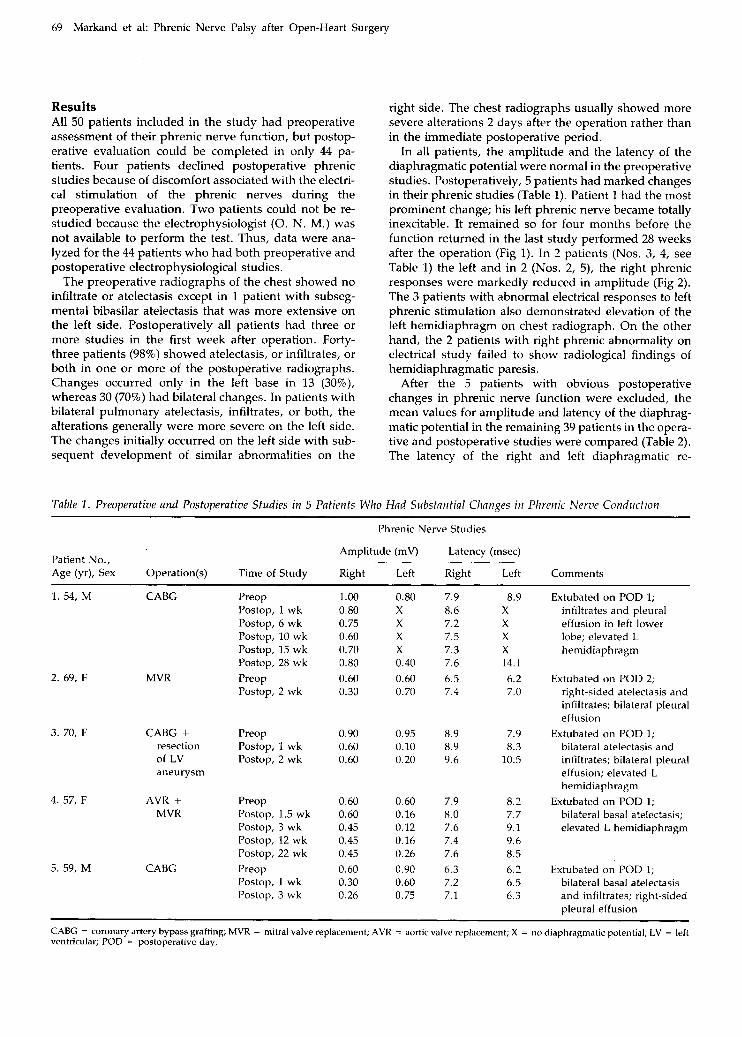
Table 1. Preoperative and Postoperative Studies in 5 Patients Who Had Substantial Changes in Phrenic Nerzv Conduction
Phrenic Nerve Studies
Amplitude (mV) Latency (msec) Patient No., ~ _ _ _ ~ Age (yr), Sex Operation(s) Time of Study Right Left Right Left Comments
1. 54, M CABG
2. 69, F MVR
3. 70, F CABG + resection of LV aneurysm
4. 57, F AVR + MVR
5. 59, M CABG
Preop Postop, 1 wk Postop, 6 wk Postop, 10 wk Postop, 15 wk Postop, 28 wk Preop Postop, 2 wk
Preop Postop, 1 wk Postop, 2 wk
Preop Postop, 1.5 wk Postop, 3 wk Postop, 12 wk Postop, 22 wk Preop Postop, 1 wk Postop, 3 wk
1.00 0.80 0.75 0.60 0.70 0.80 0.60 0.30
0.90 0.60 0.60
0.60 0.60 0.45 0.45 0.45 0.60 0.30 0.26
0.80 7.9 X 8.6 X 7.2 X 7.5 X 7.3 0.40 7.6 0.60 6.5 0.70 7.4
0.95 8.9 0.10 8.9 0.20 9.6
0.60 7.9 0.16 8.0 0.12 7.6 0.16 7.4 0.26 7.6 0.90 6.3 0.60 7.2 0.75 7.1
8.9 X X X X 14.1 6.2 7.0
7.9 8.3
10.5
8.2 7.7 9.1 9.6 8.5 6.2 6.5 6.3
Extubated on POD 1; infiltrates and pleural effusion in left lower lobe; elevated L hemidiap hragm
Extubated on POD 2; right-sided atelectasis and infiltrates; bilateral pleural effusion
bilateral atelectasis and infiltrates; bilateral pleural effusion; elevated L hemidiaphragm
Extubated on POD 1; bilateral basal atelectasis; elevated L hemidiaphragm
Extubated on POD 1;
Extubated on POD 1; bilateral basal atelectasis and infiltrates; right-sided pleural effusion
CABG = coronary artery bypass grafting; MVR = mitral valve replacement; AVR = aortic valve replacement; X = no diaphragmatic potential; LV = left ventricular; POD = postoperative day.
70 The Annals of Thoracic Surgery Vol 39 No 1 January 1985
RT PHRENIC N.
*&
1 5 0 0 p V
10 msec
L T PHRENIC N.
Fig 1 . Serial phrenic nerve studies in Patient I (see Table 1) (A) one day before coronary bypass and ( B ) 1 , (C) 6 , ( D ) 10, and (€) 28 weeks after the operation. The left phrenic nerve became inexcitable after operation. Function returned in the last study, but the diaphrag- matic potential is of lower amplitude and prolonged latency (14.0 rnsec) .
sponses showed no major change after the operation. There was a tendency for the amplitude of the diaphrag- matic potential to decrease in the postoperative study, but the difference reached statistical significance only for right phrenic stimulation.
Following operation, 38 patients (86%) were extubated within a day. Five were extubated 2 days and 1, 4 days after the operation. Of the 5 patients who had marked postoperative alteration of the phrenic nerve study, only Patient 2 needed a longer period (2 days) of assisted ventilation after the operation.
Among the 44 patients, 26 had intermittent cold blood potassium cardioplegia without topical myocardial cool- ing and 18 had topical cooling with either cold saline or ice-slushed saline solution. Phrenic palsy developed in 2 patients from the former group (without topical cooling) and in 3 from the latter (with topical cooling); the differ- ence was not statistically significant. The lowest myocar- dial temperature recorded in the patients without phrenic palsy was 12.08" f 2.13"C compared with 12.24' k 2.11"C in those with postoperative phrenic palsy. The level of systemic hypothermia was also similar (24" to
X P I C S C A I -
~ __ I D rnOCC 10 msec
Fig 2. Phrenic nerve studies in Patient 3 (see Table 1) (A) one day before, ( B ) 1 week after, and (C) 2 weeks after corona y arte y bypass and resection of left ventricular aneurysm. Studies show marked re- duction in the amplitude of the diaphragmatic potential postopera- tively on left phrenic stimulation. (XP = electrode placed over the xiphoid process; 7CS = electrode placed over the ipsilateral seventh intercostal space close to the costal margin; K = electrode placed over the knee.)
25°C) in patients with and without phrenic palsy. Dura- tion of cardiopulmonary bypass was found to be longer in the patients with phrenic palsy: 170.40 k 38.44 min- utes versus 126.08 k 33.18 minutes in patients without phrenic palsy. This difference was statistically signifi- cant ( p < 0.02).
Seven patients were referred for phrenic studies be- cause they could not be weaned off mechanical ventila- tion or had respiratory difficulties following cardio- thoracic operations. These patients were derived from a total of 224 patients who had open-heart procedures
Table 2. Preoperative and Postoperative Studies of Diaphragmatic Potential in 39 Patients"
Preoperahve Postoperative Variable Study Study Significance
Right phrenic nerve stimulation
Amplitude (mV) 0.81 C 0.20 0.71 2 0.20 y < 0.05 Latency (msec) 7.86 2 0.76 7.91 t- 0.71 NS
Left phrenic nerve stimulation
Amplitude (mV) 0.78 2 0.23 0.70 * 0.21 NS Latency (msec) 7.85 2 0.68b 7.92 t- 0.7Ib NS
'Values shown are mean f standard deviation. bFor this study, N = 38; in 1 patient, diaphragmatic potential on left phrenic stimula- tion did not have a good "takeoff" to determine latency accurately.
NS = not significant.
71 Markand et al: Phrenic Nerve Palsy after Open-Heart Surgery
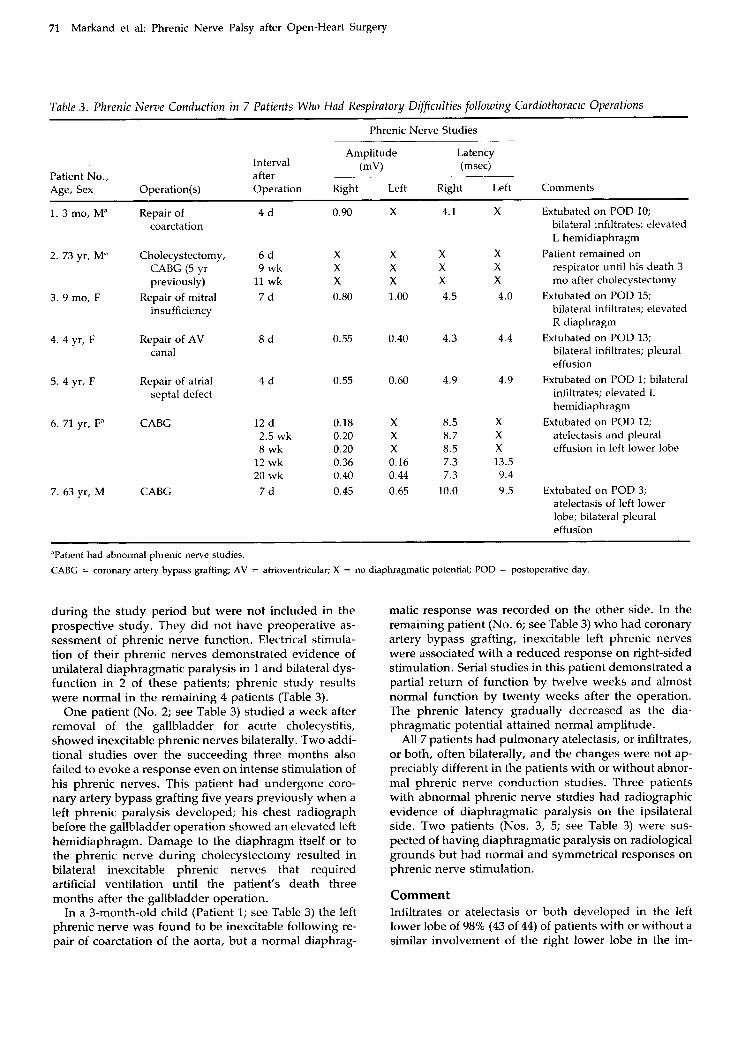
Table 3 . Phrenic Nerve Conduction in 7 Patients Who Had Respiratory Difficulties following Cardiothoracic Operations
Phrenic Nerve Studies
Amplitude Latency Interval (mv) (msec)
Patient No., after Age, Sex Operation(s) Operation Right Left Right Left Comments
1. 3 mo, Ma Repair of 4 d 0.90 X 4.1 X Extubated on POD 10; coarctation bilateral infiltrates; elevated
L hemidiaphragm 2. 73 yr, Ma Cholecystectomy, 6 d X X X X Patient remained on
CABG (5 yr 9 wk X X X X respirator until his death 3 previously) 11 wk X X X X mo after cholecystectomy
insufficiency bilateral infiltrates; elevated Repair of mitral 7 d 0.80 1 .00 4.5 4.0 Extubated on POD 15; 3. 9 mo, F
R diaphragm 4. 4 yr, F Repair of AV 8 d 0.55 0.40 4.3 4.4 Extubated on POD 13;
canal bilateral infiltrates; pleural effusion
5. 4 yr, F Repair of atrial 4 d 0.55 0.60 4.9 4.9 Extubated on POD 1; bilateral septa1 defect infiltrates; elevated L
hemidiaphragm 6. 71 yr, F” CABG 12 d 0.18 X 8.5 X Extubated on POD 12;
2.5 wk 0.20 X 8.7 X atelectasis and pleural 8 wk 0.20 X 8.5 X effusion in left lower lobe
12 wk 0.36 0.16 7.3 13.5 20 wk 0.40 0.44 7.3 9.4
7. 63 yr, M CABG 7 d 0.45 0.65 10.0 9.5 Extubated on POD 3; atelectasis of left lower lobe; bilateral pleural effusion
“Patient had abnormal phrenic nerve studies.
CABG = coronary artery bypass grafting; AV = atrioventricular; X = no diaphragmatic potential; POD = postoperative day
during the study period but were not included in the prospective study. They did not have preoperative as- sessment of phrenic nerve function. Electrical stimula- tion of their phrenic nerves demonstrated evidence of unilateral diaphragmatic paralysis in 1 and bilateral dys- function in 2 of these patients; phrenic study results were normal in the remaining 4 patients (Table 3).
One patient (No. 2; see Table 3) studied a week after removal of the gallbladder for acute cholecystitis, showed inexcitable phrenic nerves bilaterally. Two addi- tional studies over the succeeding three months also failed to evoke a response even on intense stimulation of his phrenic nerves. This patient had undergone coro- nary artery bypass grafting five years previously when a left phrenic paralysis developed; his chest radiograph before the gallbladder operation showed an elevated left hemidiaphragm. Damage to the diaphragm itself or to the phrenic nerve during cholecystectomy resulted in bilateral inexcitable phrenic nerves that required artificial ventilation until the patient’s death three months after the gallbladder operation.
In a 3-month-old child (Patient 1; see Table 3) the left phrenic nerve was found to be inexcitable following re- pair of coarctation of the aorta, but a normal diaphrag-
matic response was recorded on the other side. In the remaining patient (No. 6; see Table 3) who had coronary artery bypass grafting, inexcitable left phrenic nerves were associated with a reduced response on right-sided stimulation. Serial studies in this patient demonstrated a partial return of function by twelve weeks and almost normal function by twenty weeks after the operation. The phrenic latency gradually decreased as the dia- phragmatic potential attained normal amplitude.
All 7 patients had pulmonary atelectasis, or infiltrates, or both, often bilaterally, and the changes were not ap- preciably different in the patients with or without abnor- mal phrenic nerve conduction studies. Three patients with abnormal phrenic nerve studies had radiographic evidence of diaphragmatic paralysis on the ipsilateral side. Two patients (Nos. 3, 5; see Table 3) were sus- pected of having diaphragmatic paralysis on radiological grounds but had normal and symmetrical responses on phrenic nerve stimulation.
Comment Infiltrates or atelectasis or both developed in the left lower lobe of 98% (43 of 44) of patients with or without a similar involvement of the right lower lobe in the im-

72 The Annals of Thoracic Surgery Vol 39 No 1 January 1985
mediate postoperative period. These findings are similar to the observations of Good and colleagues [l] and Ben- jamin and associates [2], who reported an incidence of more than 85% for similar complications following coro- nary artery bypass. Three causes have been proposed for such a high incidence of postoperative pulmonary complications: (1) gastric distention following operation with elevation of the hemidiaphragm, (2) damage to the phrenic nerves as a result of direct surgical trauma or from topical hypothermia secondary to ice cooling of the heart, and (3) trauma to the lung, particularly the left lower lobe secondary to retraction during operation.
The role of gastric distention can be virtually elimi- nated because nasogastric tubes inserted before the op- eration failed to prevent pulmonary complications. Mechanisms similar to the postoperative atelectasis ob- served in upper abdominal operations are also not re- sponsible, as the routine use of positive end-expiratory pressure has been found to be ineffective in preventing pulmonary complications following coronary artery by- pass grafting [l].
Transient paralysis of the left phrenic nerve resulting from hypothermic injury secondary to ice cooling of the heart has been strongly supported by evidence from Benjamin and co-workers [2]. They reported left lower lobe infiltrates and atelectasis in 63 to 85% of their pa- tients who underwent operation with topical cooling of the heart using ice compared with an incidence of 32.5% in patients without such intraoperative cooling. These authors found a high incidence (69.2%) of abnormal dia- phragmatic motion in the chest radiographs of patients with left lower lobe abnormality, but they did not carry out electrophysiological studies of the phrenic nerves. That transient phrenic nerve dysfunction can develop secondary to hypothermic injury has been shown ex- perimentally by Marco and colleagues [4], who found that application of ice to the phrenic nerves of dogs for 30 to 60 minutes resulted in paralysis lasting one to four weeks. Whether this paralysis is the sole mechanism for the almost invariable development of infiltrates and atelectasis observed after open-heart operations in hu- man beings, however, can be questioned on several grounds. First, a high incidence of pulmonary complica- tions following open-heart surgery has been reported, even when ice cooling of the heart was not carried out. In our series all but 1 of the patients had these postop- erative complications. Second, we and other groups [l] have shown that the incidence of atelectasis and infiltrates is higher 2 or more days following rather than immediately after operation, a finding that would be difficult to explain if the changes were due to hy- pothermic phrenic nerve injury sustained during the op- eration. Third, our electrophysiological evaluation of phrenic nerve-diaphragm function assessed in patients before and after open-heart procedures established that 89% (39/44) of the patients had no marked changes in phrenic nerve conduction following operation.
We think that trauma to the lungs secondary to retrac- tion and subsequent pulmonary contusion is probably
the most common cause for the high incidence of pulmo- nary complications seen in the immediate postoperative period following open-heart surgical procedures. De- creased ability to cough secondary to chest pain and sedation with resultant retained secretions may be addi- tional causative factors. The more common and severe involvement of the left side probably reflects more se- vere operative trauma due to the retraction of the left lung. There is also an increasing body of evidence that microaggregates of platelets, fibrin, and leukocytes lodg- ing in the pulmonary vasculature during extracorporeal circulation may contribute to pulmonary complications after open-heart surgery [5].
Undoubtedly a small proportion of patients do sustain phrenic nerve damage during cardiothoracic operations; the incidence of this complication was 11% (5 of 44 pa- tients) in our prospective study. The incidence of total phrenic paralysis, however, was lower: only 1 of the 44 had total lack of response on stimulation of the left phrenic nerve after the operation. Three other patients with total phrenic nerve paralysis were identified among 224 open-heart operations conducted during the same study period-an incidence of approximately 1.5%. Others [6-81 have reported a similar incidence of this complication following cardiothoracic operations. We think that phrenic nerve damage is primarily a stretch injury, which may occur during retraction of the ster- num or prolonged pericardial stretch applied through weights during the operation. Although the use of top- ical cardiac cooling or the lowest myocardial tempera- ture during operation had no major influence when con- sidered individually, hypothermic injury may play an important additive role in causing phrenic palsy. Longer duration of cardiopulmonary bypass in patients in whom phrenic palsy developed would support the no- tion that longer duration of stretch and prolonged sys- temic hypothermia may be crucial etiological factors. Re- ducing the duration of both the systemic hypothermia and the pericardial stretch during operation may help reduce the incidence of intraoperative phrenic injury.
The present investigation had one notable limitation in that the electrophysiological evaluation was per- formed at least 6 days after the operation because of the technical difficulties in the immediate postoperative pe- riod. It is therefore possible that we may have missed cases of transient postoperative diaphragmatic dysfunc- tion, which might have recovered by the time of the electrical evaluation. Nonetheless, our investigation strongly suggests that diaphragmatic paresis of a clini- cally significant degree occurs in a much smaller per- centage of patients after open-heart procedures than the incidence of postoperative pulmonary complications would dictate.
We found no change in the latency but a slight de- crease (10%) in the mean amplitude of the diaphrag- matic potential following open-heart operation (see Table 2). The change, which was slightly greater for the right-sided stimulation, remains unexplained. It may be due to increased tissue impedance secondary to postop-

73 Markand et al: Phrenic Nerve Palsy after Open-Heart Surgery
erative alterations in the intrathoracic and superficial tis- sues.
The effect of phrenic nerve palsy on the mechanics of respiration varies according to the status of other respi- ratory muscles and associated pulmonary complications. Unilateral phrenic nerve palsy in the presence of pulmo- nary infiltrates or effusion may compromise ventilation to the extent that prolonged ventilatory support is re- quired, as was the case in 3 of our 4 patients who had total paralysis of the diaphragm on one or both sides. The only patient with bilateral inexcitable phrenic nerves required mechanical ventilation until his death. Stephens [6] reported that compared with older chil- dren, infants with unilateral phrenic paralysis did less well in the immediate postoperative period because they more commonly required prolonged ventilatory support and, rarely, diaphragmatic plication. The long-term out- come of unilateral phrenic paralysis, even when com- plete, appears to be favorable, at least in adults, because all of the patients in our series attained normal ventila- tory status after 2 to 3 weeks.
The stretch injury to the phrenic nerve is mainly to the axons, and the integrity of the nerve remains largely intact; hence, recovery may be expected. The time taken for recovery depends on the site of injury and the rate of regeneration. When the phrenic nerve was crushed in the neck as a therapeutic procedure to treat tuberculosis, the majority of patients had return of diaphragmatic mo- tion over the following six months [9]. Similar nerve injury in the thorax is expected to take a shorter period for recovery. Three of our 4 patients who had follow-up studies extending beyond ten weeks of the operation showed evidence of recovery of the phrenic nerve func- tion; the recovery time appears to be between three and six months.
In the past phrenic nerve paralysis has been detected largely by radiological investigations. Electrophysiolog- ical assessment of the phrenic nerve function has been mentioned only rarely in patients who experienced phrenic paralysis following cardiothoracic operations [lo-121. An elevated hemidiaphragm in radiographs of the chest with atelectasis and infiltrates of the lower lobe on that side is suggestive of unilateral phrenic paralysis, but local pulmonary pathology, eventration of the dia- phragm, or infradiaphragmatic disease may produce similar findings. A fluoroscopic examination of the chest that demonstrates reduced excursion of the hemidia- phragm and paradoxical motion is considered diagnostic of diaphragmatic paralysis, although fluoroscopy may be delayed because of the condition of the patient. The findings also may be difficult to interpret, particularly in the presence of pleural effusion or atelectasis. Un-
equivocal evidence of phrenic nerve damage, on the other hand, can be quickly established by percutaneous phrenic nerve stimulation. The technique is easy, can be performed at the bedside of the patient, and can be re- peated as often as desired. Serial studies may also pro- vide the earliest evidence of return of phrenic nerve function. Therefore, electrophysiological evaluation of phrenic nerves should be included in the assessment of patients who have ventilatory difficulties, pulmonary atelectasis and infiltrates, and elevation of hemidia- phragm in the postoperative period following car- diothoracic surgical procedures.
We thank the cardiovascular surgical house staff for their coop- eration in obtaining preoperative and postoperative phrenic nerve studies on patients in their care. We also thank Mrs. Martha Stanley for typing the manuscript.
References 1. Good JT Jr, Wolz JF, Andersen JT, et al: The routine use of
positive end-expiratory pressure after open heart surgery. Chest 76~397, 1979
2. Benjamin JJ, Cascade PN, Rubenfire M, et al: Left lower lobe atelectasis and consolidation following cardiac surgery: the effect of topical cooling on the phrenic nerve. Radiology 142:11, 1982
3. Markand ON, Kincaid JC, Pourmand RA, et al: Electro- physiologic evaluation of diaphragm by transcutaneous phrenic nerve stimulation. Neurology 34:604, 1984
4. Marco JD, Hahn JW, Barner HB: Topical cardiac hypother- mia and phrenic nerve injury. Ann Thorac Surg 23235, 1977
5. Ratliff NB, Young WG Jr, Hackel DB, et al: Pulmonary in- jury secondary to extracorporeal circulation. J Thorac Car- diovasc Surg 65:425, 1973
6. Stephens JW: Neurological sequelae of congenital heart surgery. Arch Neurol 7450, 1962
7. Mickell JJ, Oh KS, Siewers RD, et al: Clinical implications of postoperative unilateral phrenic nerve paralysis. J Thorac Cardiovasc Surg 76297, 1978
8. Lederman RJ, Breuer AC, Hanson JR, et al: Peripheral ner- vous system complication of coronary artery bypass graft surgery. Ann Neurol 12:297, 1982
9. Iverson LI, Mittal A, Dugan DJ, et al: Injuries to the phrenic nerve resulting in diaphragmatic paralysis with special ref- erence to stretch trauma. Am J Surg 132:263, 1976
10. Davis JN: Phrenic nerve conduction in man. J Neurol Neurosurg Psychiatry 30:420, 1967
11. Shaw RK, Glenn WWL, Hogan JF, Phelps ML: Electrophys- iological evaluation of phrenic nerve function in candidates for diaphragm pacing. J Neurosurg 53345, 1980
12. Moosa A: Phrenic nerve conduction in children. Dev Med Child Neurol 23:434, 1981