Factors Associated With Postoperative Delirium After Thoracic Surgery
8
2005;79:1004-1009 Ann Thorac Surg Bekiroglu and Mustafa Yüksel Bedrettin Yildizeli, M. Oguzhan Özyurtkan, Hasan F. Batirel, Kemal Kuscu, Nural Factors Associated With Postoperative Delirium After Thoracic Surgery http://ats.ctsnetjournals.org/cgi/content/full/79/3/1004 located on the World Wide Web at: The online version of this article, along with updated information and services, is Print ISSN: 0003-4975; eISSN: 1552-6259. Southern Thoracic Surgical Association. Copyright © 2005 by The Society of Thoracic Surgeons. is the official journal of The Society of Thoracic Surgeons and the The Annals of Thoracic Surgery by on June 7, 2013 ats.ctsnetjournals.org Downloaded from
-
Upload
independent -
Category
Documents
-
view
4 -
download
0
Transcript of Factors Associated With Postoperative Delirium After Thoracic Surgery

2005;79:1004-1009 Ann Thorac SurgBekiroglu and Mustafa Yüksel
Bedrettin Yildizeli, M. Oguzhan Özyurtkan, Hasan F. Batirel, Kemal Kuscu, Nural Factors Associated With Postoperative Delirium After Thoracic Surgery
http://ats.ctsnetjournals.org/cgi/content/full/79/3/1004located on the World Wide Web at:
The online version of this article, along with updated information and services, is
Print ISSN: 0003-4975; eISSN: 1552-6259. Southern Thoracic Surgical Association. Copyright © 2005 by The Society of Thoracic Surgeons.
is the official journal of The Society of Thoracic Surgeons and theThe Annals of Thoracic Surgery
by on June 7, 2013 ats.ctsnetjournals.orgDownloaded from

FABKD
saWf
crwt
t4agagMd
DcomPcctadfcopsfceAot
A
AMe
©P
GEN
ERA
LT
HO
RA
CIC
actors Associated With Postoperative Deliriumfter Thoracic Surgery
edrettin Yıldızeli, MD, M. Oguzhan Özyurtkan, MD, Hasan F. Batırel, MD,emal Kuscu, MD, Nural Bekiroglu, PhD, and Mustafa Yüksel, MD
epartments of Thoracic Surgery, Psychiatry, and Biostatistics, Marmara University Hospital, Istanbul, Turkey
vtst0waga
mCpagr
Background. Postoperative delirium is an acute confu-ional state characterized by fluctuating consciousnessnd is associated with increased morbidity and mortality.e analyzed the incidence and risk factors of delirium
ollowing thoracic surgery.Methods. All patients (n � 432) who underwent thora-
otomy or sternotomy from 1996 to 2003 were analyzedetrospectively. The diagnosis of postoperative deliriumas based on Diagnostic and Statistical Manual of Men-
al Disorders- IV criteria.Results. Postoperative delirium developed in 23 pa-
ients (5.32%) between postoperative days 2 to 12 (mean,.4 � 2.6 days). There were 15 males and 8 females, withmean age of 59.4 years (24 to 77 years). The delirium
roup was older (59.4 � 14.6 vs 51.3 � 15.5 years, p < 0.01)nd had a longer operation time than the nondeliriousroup (5.34 � 1.58 vs 4.38 � 1.6 hours, p � 0.005).orbidity and mortality rates were not significantly
ifferent between the two groups (56.5% vs 47.1%; 13.0%
agep
P
TwmdwcT
pcaai(lTdaarmara University Hospital, PK 97, 34718 Acıbadem, Istanbul, Turkey;
-mail: [email protected].
2005 by The Society of Thoracic Surgeonsublished by Elsevier Inc
ats.ctsnetjournDownloaded from
s 3.66%, respectively). Univariate analysis showed thathe older age, markedly abnormal postoperative levels ofodium, potassium, or glucose, sleep deprivation, opera-ion time, and diabetes mellitus were risk factors (p <.05). According to multivariate analyses, four factorsere selected as predictive risk factors: (1) markedly
bnormal postoperative levels of sodium, potassium, orlucose (p � 0.038); (2) sleep deprivation (p � 0.05); (3)ge (p � 0.033); and (4) operation time (p � 0.041).
Conclusions. Postoperative delirium may cause higherorbidity and mortality rates after thoracic surgery.lose postoperative follow-up and early identification ofredisposing factors such as older age, sleep deprivation,bnormal postoperative levels of sodium, potassium, orlucose, and longer operation time can prevent occur-ence of postoperative delirium.
(Ann Thorac Surg 2005;79:1004–9)
© 2005 by The Society of Thoracic Surgeonselirium is defined as a reversible, global impairmentof cognitive processes, usually of sudden onset,
oupled with disorientation, impaired short-term mem-ry, altered sensory perceptions (hallucinations), abnor-al thought process, and inappropriate behavior [1].
ostoperative delirium (POD) is also defined as an acutehange in cognitive status characterized by fluctuatingonsciousness and inattention, occurring after an opera-ion [2]. The overall incidence of POD has been reporteds 36.8% within a range of 0% to 73.5% [2]. Postoperativeelirium is related to higher mortality rates, difficulties in
unctional recovery, longer recovery periods, and in-reased period of hospitalization [3]. Developments inperative and anesthetic techniques have enabled olderatients, and those with more serious cases, to undergourgery. This may be a cause of the increase in therequency of delirium. It is important to investigate theauses and risk factors of delirium in order to developffective treatment and prevention techniques. In 1994,akerlund and Rosenberg [4] published the initial reportn POD in patients undergoing thoracic surgery. Sincehen, no study has been designed to find out the factors
ccepted for publication June 4, 2004.
ddress reprint requests to Dr Yüksel, Department of Thoracic Surgery,
ssociated with postoperative delirium after thoracic sur-ery. In this study, we attempt to determine the periop-rative risk factors of POD in order to predict andrevent delirium after thoracic surgery.
atients and Methods
he records of 432 patients older than 18 year of age whoere admitted to our hospital between 1996 and 2003 forajor elective or urgent thoracic surgery operations,
efined as an expected length of stay of 2 or more days,ere retrospectively reviewed. Profiles and surgical indi-
ations of the enrolled 432 patients are summarized inable 1.Thoracic epidural catheters (T6–8) were routine for
ostoperative pain management, other than contraindi-ations or misplacement. Intravenous patient-controllednalgesia (PCA) was instituted in those situations. Fent-nyl and bupivacaine (at concentrations of 0.125%) werenfused from the epidural catheter, whereas morphine1.0 to 1.5 mg, lockout 10 minutes) or meperidine (15 mg,ockout 10 minutes) were used in intravenous PCA.ypical duration for the use of the catheters was 3 to 5ays, after which a nonsteroidal antiinflammatory drugnd opioid derivative were started for pain control.
A psychiatric consultation was requested once delir-0003-4975/05/$30.00doi:10.1016/j.athoracsur.2004.06.022
by on June 7, 2013 als.org
idMhiba
ptodlro
drrbelewsmodr[ottwttr
ewpdfaiw
TP
AMLLLD
I
1005Ann Thorac Surg YILDIZELI ET AL2005;79:1004–9 DELIRIUM IN THORACIC SURGERY
GEN
ERA
LT
HO
RA
CIC
um symptoms were first noted after the operation. Aiagnosis was made based on the Diagnosis and Statisticalanual of Mental Disorders (DSM-IV) [5]. Antipsychotics,
aloperidol, risperidone, and quetapine have been usedn treating delusions, paranoia, and perceptual distur-ances. Benzodiazepines were used in alcohol and sed-tive withdrawal syndromes.The preoperative and postoperative assessments were
erformed accordingly [3, 6]. The preoperative evalua-ion included a medical history highlighting the presencef either chronic or acute illnesses like pulmonary, car-iac, renal, and liver disease, presence of diabetes mel-
itus (DM), alcohol abuse, previous psychological or neu-ologic diseases, and history of delirium. The definitionf alcohol abuse was made based on DSM-IV [5] that
Abbreviations and Acronyms
DFP � delirium free protocolDM � diabetes mellitusDSM-IV � Diagnosis and Statistical Manual of
Mental Disorders-IVICU � intensive care unitNSAID � non-steroidal anti-inflammatory drugPCA � patient-controlled analgesiapO2 � partial pressure of oxygenpCO2 � partial pressure of carbon dioxidePOD � postoperative deliriumSD � standard deviation
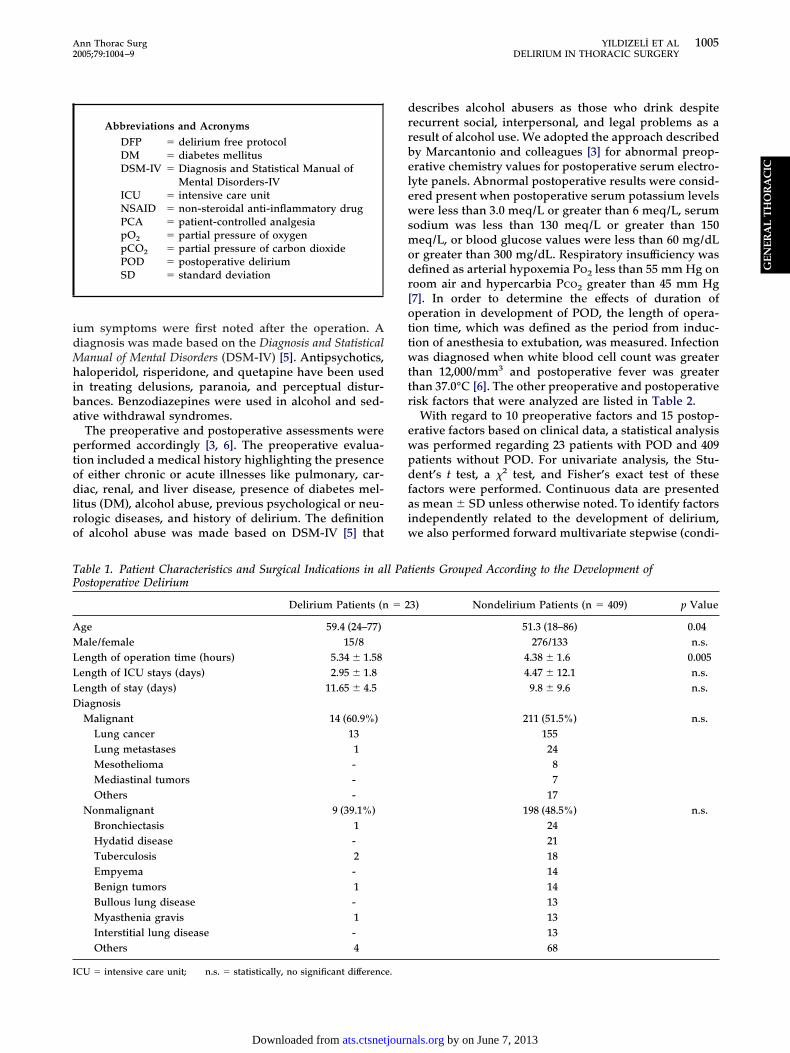
able 1. Patient Characteristics and Surgical Indications in alostoperative Delirium
Delirium Patients (n
ge 59.4 (24–77)ale/female 15/8
ength of operation time (hours) 5.34 � 1.58ength of ICU stays (days) 2.95 � 1.8ength of stay (days) 11.65 � 4.5iagnosisMalignant 14 (60.9%)
Lung cancer 13Lung metastases 1Mesothelioma -Mediastinal tumors -Others -
Nonmalignant 9 (39.1%)Bronchiectasis 1Hydatid disease -Tuberculosis 2Empyema -Benign tumors 1Bullous lung disease -Myasthenia gravis 1Interstitial lung disease -Others 4
CU � intensive care unit; n.s. � statistically, no significant difference.
ats.ctsnetjournDownloaded from
escribes alcohol abusers as those who drink despiteecurrent social, interpersonal, and legal problems as aesult of alcohol use. We adopted the approach describedy Marcantonio and colleagues [3] for abnormal preop-rative chemistry values for postoperative serum electro-yte panels. Abnormal postoperative results were consid-red present when postoperative serum potassium levelsere less than 3.0 meq/L or greater than 6 meq/L, serum
odium was less than 130 meq/L or greater than 150eq/L, or blood glucose values were less than 60 mg/dL
r greater than 300 mg/dL. Respiratory insufficiency wasefined as arterial hypoxemia Po2 less than 55 mm Hg onoom air and hypercarbia Pco2 greater than 45 mm Hg7]. In order to determine the effects of duration ofperation in development of POD, the length of opera-ion time, which was defined as the period from induc-ion of anesthesia to extubation, was measured. Infectionas diagnosed when white blood cell count was greater
han 12,000/mm3 and postoperative fever was greaterhan 37.0°C [6]. The other preoperative and postoperativeisk factors that were analyzed are listed in Table 2.
With regard to 10 preoperative factors and 15 postop-rative factors based on clinical data, a statistical analysisas performed regarding 23 patients with POD and 409atients without POD. For univariate analysis, the Stu-ent’s t test, a �2 test, and Fisher’s exact test of these
actors were performed. Continuous data are presenteds mean � SD unless otherwise noted. To identify factorsndependently related to the development of delirium,e also performed forward multivariate stepwise (condi-
ients Grouped According to the Development of
3) Nondelirium Patients (n � 409) p Value
51.3 (18–86) 0.04276/133 n.s.
4.38 � 1.6 0.0054.47 � 12.1 n.s.9.8 � 9.6 n.s.
211 (51.5%) n.s.15524
87
17198 (48.5%) n.s.
242118141413131368
l Pat
� 2
by on June 7, 2013 als.org
ttwM
R
Of1t7Ptf2cpelph
drlpctmi
t�s((
tp(Pcc1gsP
simlo0vaoos
pr
TP
F
P
P
a
b
Ppd
T
C
OAWRPAS
BVPI
1006 YILDIZELI ET AL Ann Thorac SurgDELIRIUM IN THORACIC SURGERY 2005;79:1004–9
GEN
ERA
LT
HO
RA
CIC
ional) logistic regression. A p value of less than or equalo 0.05 was considered significant. Approval for this studyas granted by the Institutional Review Board of thearmara University School of Medicine.
esults
f the 432 patients, 291 were males (67.4%) and 141 wereemales (32.6%). Mean age was 51.7 (range, 18 to 86, SD5.5) years. Postoperative delirium occurred in 23 pa-ients (5.32%) with a mean age of 59.4 � 14.6 (range, 24 to7 years) (Table 1). The mean age of patients withoutOD was 51.3 � 15.5 (range, 18 to 86 years, p � 0.04). Of
hese 23 patients, 15 were males (65%) and 8 wereemales (35%). The onset of the delirium ranged from dayto day 12 after surgery (mean, 4.4 � 2.6 days). The most
ommon signs and symptoms were agitation (10 of 23atients, 43%), hallucination (6 of 23 patients, 26%),motional disturbances (5 of 23 patients, 21.7%), sleep-essness (2 of 23 patients, 8%), and anxiety (3 of 23atients, 13%). Patients with POD were treated with
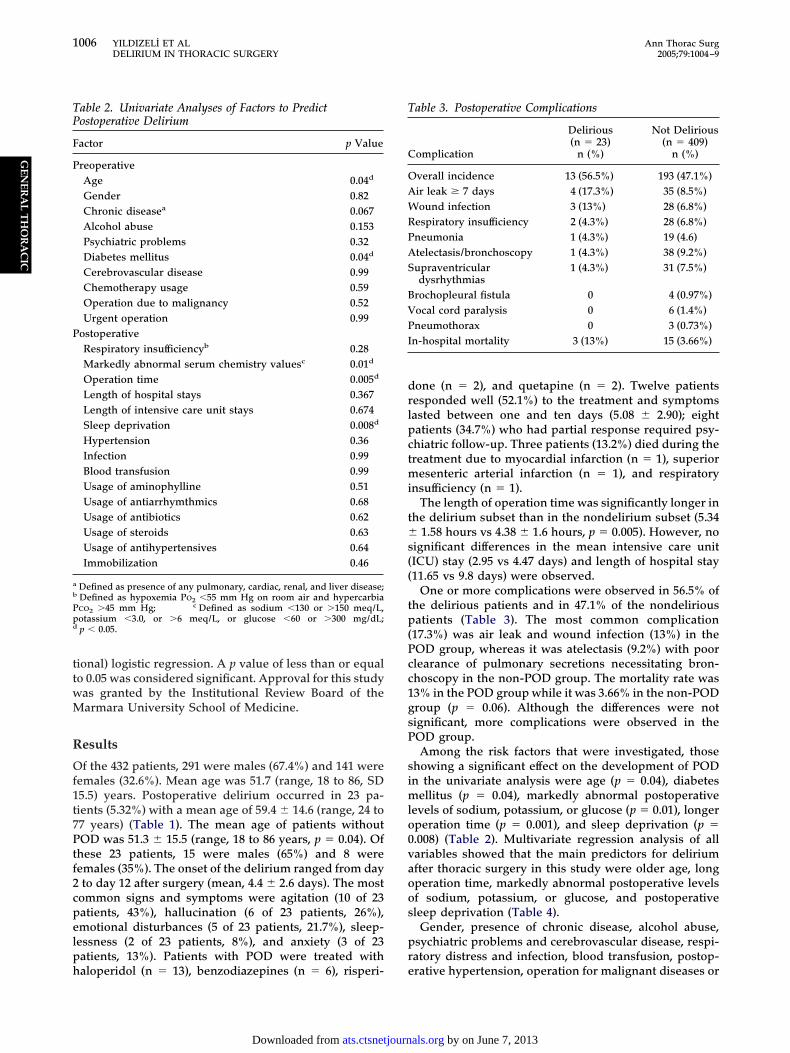
able 2. Univariate Analyses of Factors to Predictostoperative Delirium
actor p Value
reoperativeAge 0.04d
Gender 0.82Chronic diseasea 0.067Alcohol abuse 0.153Psychiatric problems 0.32Diabetes mellitus 0.04d
Cerebrovascular disease 0.99Chemotherapy usage 0.59Operation due to malignancy 0.52Urgent operation 0.99
ostoperativeRespiratory insufficiencyb 0.28Markedly abnormal serum chemistry valuesc 0.01d
Operation time 0.005d
Length of hospital stays 0.367Length of intensive care unit stays 0.674Sleep deprivation 0.008d
Hypertension 0.36Infection 0.99Blood transfusion 0.99Usage of aminophylline 0.51Usage of antiarrhymthmics 0.68Usage of antibiotics 0.62Usage of steroids 0.63Usage of antihypertensives 0.64Immobilization 0.46
Defined as presence of any pulmonary, cardiac, renal, and liver disease;Defined as hypoxemia Po2 �55 mm Hg on room air and hypercarbiaco2 �45 mm Hg; c Defined as sodium �130 or �150 meq/L,otassium �3.0, or �6 meq/L, or glucose �60 or �300 mg/dL;p � 0.05.
aloperidol (n � 13), benzodiazepines (n � 6), risperi- e
ats.ctsnetjournDownloaded from
one (n � 2), and quetapine (n � 2). Twelve patientsesponded well (52.1%) to the treatment and symptomsasted between one and ten days (5.08 � 2.90); eightatients (34.7%) who had partial response required psy-hiatric follow-up. Three patients (13.2%) died during thereatment due to myocardial infarction (n � 1), superior
esenteric arterial infarction (n � 1), and respiratorynsufficiency (n � 1).
The length of operation time was significantly longer inhe delirium subset than in the nondelirium subset (5.34
1.58 hours vs 4.38 � 1.6 hours, p � 0.005). However, noignificant differences in the mean intensive care unitICU) stay (2.95 vs 4.47 days) and length of hospital stay11.65 vs 9.8 days) were observed.
One or more complications were observed in 56.5% ofhe delirious patients and in 47.1% of the nondeliriousatients (Table 3). The most common complication
17.3%) was air leak and wound infection (13%) in theOD group, whereas it was atelectasis (9.2%) with poorlearance of pulmonary secretions necessitating bron-hoscopy in the non-POD group. The mortality rate was3% in the POD group while it was 3.66% in the non-PODroup (p � 0.06). Although the differences were notignificant, more complications were observed in theOD group.Among the risk factors that were investigated, those
howing a significant effect on the development of PODn the univariate analysis were age (p � 0.04), diabetes
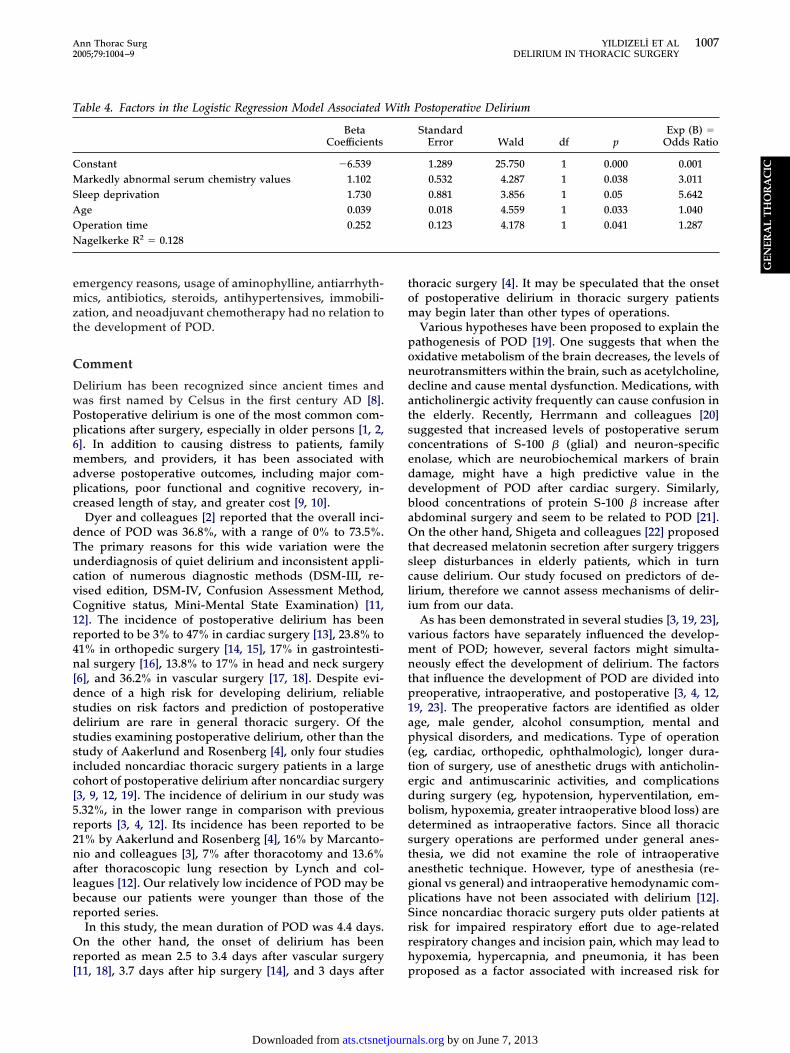
ellitus (p � 0.04), markedly abnormal postoperativeevels of sodium, potassium, or glucose (p � 0.01), longerperation time (p � 0.001), and sleep deprivation (p �.008) (Table 2). Multivariate regression analysis of allariables showed that the main predictors for deliriumfter thoracic surgery in this study were older age, longperation time, markedly abnormal postoperative levelsf sodium, potassium, or glucose, and postoperativeleep deprivation (Table 4).
Gender, presence of chronic disease, alcohol abuse,sychiatric problems and cerebrovascular disease, respi-atory distress and infection, blood transfusion, postop-
able 3. Postoperative Complications
omplication
Delirious(n � 23)
n (%)
Not Delirious(n � 409)
n (%)
verall incidence 13 (56.5%) 193 (47.1%)ir leak � 7 days 4 (17.3%) 35 (8.5%)ound infection 3 (13%) 28 (6.8%)
espiratory insufficiency 2 (4.3%) 28 (6.8%)neumonia 1 (4.3%) 19 (4.6)telectasis/bronchoscopy 1 (4.3%) 38 (9.2%)upraventriculardysrhythmias
1 (4.3%) 31 (7.5%)
rochopleural fistula 0 4 (0.97%)ocal cord paralysis 0 6 (1.4%)neumothorax 0 3 (0.73%)
n-hospital mortality 3 (13%) 15 (3.66%)
rative hypertension, operation for malignant diseases or
by on June 7, 2013 als.org
emzt
C
DwPp6mapc
dTucvC1r4n[dsdssic[5r2nalbr
Or[
tom
pondatsceddbaOtscli
vmntp1ap(tedbdstagpSrrh
T
CMSAON
1007Ann Thorac Surg YILDIZELI ET AL2005;79:1004–9 DELIRIUM IN THORACIC SURGERY
GEN
ERA
LT
HO
RA
CIC
mergency reasons, usage of aminophylline, antiarrhyth-ics, antibiotics, steroids, antihypertensives, immobili-
ation, and neoadjuvant chemotherapy had no relation tohe development of POD.
omment
elirium has been recognized since ancient times andas first named by Celsus in the first century AD [8].ostoperative delirium is one of the most common com-lications after surgery, especially in older persons [1, 2,]. In addition to causing distress to patients, familyembers, and providers, it has been associated with
dverse postoperative outcomes, including major com-lications, poor functional and cognitive recovery, in-reased length of stay, and greater cost [9, 10].
Dyer and colleagues [2] reported that the overall inci-ence of POD was 36.8%, with a range of 0% to 73.5%.he primary reasons for this wide variation were thenderdiagnosis of quiet delirium and inconsistent appli-ation of numerous diagnostic methods (DSM-III, re-ised edition, DSM-IV, Confusion Assessment Method,ognitive status, Mini-Mental State Examination) [11,2]. The incidence of postoperative delirium has beeneported to be 3% to 47% in cardiac surgery [13], 23.8% to1% in orthopedic surgery [14, 15], 17% in gastrointesti-al surgery [16], 13.8% to 17% in head and neck surgery
6], and 36.2% in vascular surgery [17, 18]. Despite evi-ence of a high risk for developing delirium, reliabletudies on risk factors and prediction of postoperativeelirium are rare in general thoracic surgery. Of thetudies examining postoperative delirium, other than thetudy of Aakerlund and Rosenberg [4], only four studiesncluded noncardiac thoracic surgery patients in a largeohort of postoperative delirium after noncardiac surgery3, 9, 12, 19]. The incidence of delirium in our study was.32%, in the lower range in comparison with previouseports [3, 4, 12]. Its incidence has been reported to be1% by Aakerlund and Rosenberg [4], 16% by Marcanto-io and colleagues [3], 7% after thoracotomy and 13.6%fter thoracoscopic lung resection by Lynch and col-eagues [12]. Our relatively low incidence of POD may beecause our patients were younger than those of theeported series.
In this study, the mean duration of POD was 4.4 days.n the other hand, the onset of delirium has been
eported as mean 2.5 to 3.4 days after vascular surgery
able 4. Factors in the Logistic Regression Model Associated
BetaCoefficients
onstant �6.539arkedly abnormal serum chemistry values 1.102
leep deprivation 1.730ge 0.039peration time 0.252agelkerke R2 � 0.128
11, 18], 3.7 days after hip surgery [14], and 3 days after p
ats.ctsnetjournDownloaded from
horacic surgery [4]. It may be speculated that the onsetf postoperative delirium in thoracic surgery patientsay begin later than other types of operations.Various hypotheses have been proposed to explain the
athogenesis of POD [19]. One suggests that when thexidative metabolism of the brain decreases, the levels ofeurotransmitters within the brain, such as acetylcholine,ecline and cause mental dysfunction. Medications, withnticholinergic activity frequently can cause confusion inhe elderly. Recently, Herrmann and colleagues [20]uggested that increased levels of postoperative serumoncentrations of S-100 � (glial) and neuron-specificnolase, which are neurobiochemical markers of brainamage, might have a high predictive value in theevelopment of POD after cardiac surgery. Similarly,lood concentrations of protein S-100 � increase afterbdominal surgery and seem to be related to POD [21].n the other hand, Shigeta and colleagues [22] proposed
hat decreased melatonin secretion after surgery triggersleep disturbances in elderly patients, which in turnause delirium. Our study focused on predictors of de-irium, therefore we cannot assess mechanisms of delir-um from our data.
As has been demonstrated in several studies [3, 19, 23],arious factors have separately influenced the develop-ent of POD; however, several factors might simulta-
eously effect the development of delirium. The factorshat influence the development of POD are divided intoreoperative, intraoperative, and postoperative [3, 4, 12,9, 23]. The preoperative factors are identified as olderge, male gender, alcohol consumption, mental andhysical disorders, and medications. Type of operation
eg, cardiac, orthopedic, ophthalmologic), longer dura-ion of surgery, use of anesthetic drugs with anticholin-rgic and antimuscarinic activities, and complicationsuring surgery (eg, hypotension, hyperventilation, em-olism, hypoxemia, greater intraoperative blood loss) areetermined as intraoperative factors. Since all thoracicurgery operations are performed under general anes-hesia, we did not examine the role of intraoperativenesthetic technique. However, type of anesthesia (re-ional vs general) and intraoperative hemodynamic com-lications have not been associated with delirium [12].ince noncardiac thoracic surgery puts older patients atisk for impaired respiratory effort due to age-relatedespiratory changes and incision pain, which may lead toypoxemia, hypercapnia, and pneumonia, it has been
Postoperative Delirium
StandardError Wald df p
Exp (B) �Odds Ratio
1.289 25.750 1 0.000 0.0010.532 4.287 1 0.038 3.0110.881 3.856 1 0.05 5.6420.018 4.559 1 0.033 1.0400.123 4.178 1 0.041 1.287
With
roposed as a factor associated with increased risk for
by on June 7, 2013 als.org

dwusmaleposagd
tdasiai
wdpans
a[vimapaatmqusppatbm
soacOoa[
occsewauSami
iimviD�
ruwcdt1wwstbcosppcsiccddsntIapost9dps
1008 YILDIZELI ET AL Ann Thorac SurgDELIRIUM IN THORACIC SURGERY 2005;79:1004–9
GEN
ERA
LT
HO
RA
CIC
elirium [3, 4, 9, 12, 19]. Since inadequate oxygenationas proposed for the development of POD in patientsndergoing thoracotomy for pulmonary malignancy,upplementary oxygen has been advised for the treat-ent of delirium [4]. Hypocarbia, sepsis, more postoper-
tive blood transfusions and postoperative hematocritess than 30%, sensory deprivation or overload, andlectrolyte or metabolic problems have also been re-orted as postoperative factors that influence the devel-pment of POD. Our findings are consistent with othertudies [3, 12, 19, 23]; that patients who are old, havebnormal postoperative levels of sodium, potassium, orlucose, a presence of sleep deprivation, and longeruration of surgery, are at high risk of developing POD.In our study, operation time was significantly longer in
he POD group than in the non-POD group. As theefinition implies, this period includes instrumentationnd catheterization by the anesthesia team and theurgical procedure. The use of staplers is limited in ournstitution during a regular resection, therefore the aver-ge operation times are acceptable for such a trainingnstitution.
Although delirium appeared to be strongly associatedith alcohol abuse [3], no alcohol abuse was related toelirium; possibly due to the small number of theseatients in our sample. However, patients with alcoholbuse were more common in the POD group than in theon-POD group (13.0% vs 5.6%, respectively, notignificant).
Primary prevention is more effective than interventionnd supportive measures after the manifestation of POD14]. The prediction score, which is based on a cross-alidation analysis, has been suggested to quantify anndividual patient’s risk for POD [18]. Although non-
odifiable patient clinical characteristics, such as agend preexisting central nervous system disease, placeatients at higher risk for POD, a multimanagementpproach may prevent delirium. It includes eliminatingll medications that can precipitate delirium, optimizinghe patient’s fluid status, aggressively treating pain, pro-
oting early ambulation, and ensuring a familiar, tran-uil postoperative care setting [19, 24]. If it is possible,sing restraints, intravenous lines, and Foley cathetershould be avoided. In our study group, the patients withostoperative delirium were not restrained and if aatient developed POD the Foley catheter was immedi-tely removed; if otherwise there was no contraindica-ion. In about 16% of patients no cause for delirium maye found and then efforts should focus on supportiveeasures [24].Effective pain management after a thoracotomy is es-
ential to reduce pulmonary complications. An epiduralr intrathecal infusion of opioids, with or without localnesthetic, is effective with parenteral opioids. Patientontrolled analgesia should be used whenever possible.ur policy is to place an epidural catheter preoperatively
r to use intravenous PCA. Because the anticholinergicctivity of meperidine may increase the risk of delirium3], we avoid its use especially in older adults.
Pharmacologic treatment is essential to prevent injury h
ats.ctsnetjournDownloaded from
r to allow further evaluation. A high-potency antipsy-hotic, haloperidol (doses of 0.5 to 2.0 mg), is the mostommonly used drug [19]. It is useful in treating delu-ions, paranoia, and perceptual disturbances. Benzodiaz-pines are the drug of choice in alcohol and sedativeithdrawal syndromes. Recently, successful use of mel-
tonin has been reported in treating severe POD that isnresponsive to antipsychotics or benzodiazepines [25].ince most of our POD patients presented with agitationnd hallucinations, and they also required rapid phar-acologic intervention, haloperidol was used as the
nitial treatment in our cohort of patients.Aizawa and colleagues [26] have suggested “the delir-
um-free protocol treatment” (DFP) for controlling PODn elderly patients after general surgery. By using intra-
uscular injection of diazepam and a continuous intra-enous infusion of flunitrazepam and pethidine, thencidence of POD was reported significantly lower in theFP group than that of the non-DFP group (5% vs 35%, p0.023).The prognosis of delirium is related to the prompt
ecognition and the appropriate management of thenderlying cause(s). Studies clearly show that patientsho develop delirium have increased rates of major
omplications, longer lengths of stay, and higher rates ofischarge to long-term care or rehabilitative facilities
han patients who did not develop this complication [3,8]. During the index admission, mortality for patientsith delirium ranges from 10% to 26%, then increasesith the length of follow-up [24]. At 1 year after admis-
ion mortality is 38%, and at 5 years is 51% [27]. But inhis study, we could not find any significant relationshipetween the development of POD and postoperativeomplications. The small number and quite younger agesf our delirious patients compared to those of reportederies may explain why we did not observe more com-lications in this study. However, more than half of theatients with POD presented at least one major compli-ation and mortality occurred in 13% of them. In thistudy, postoperative delirium did not lead to a significantncrease in ICU stay but did lead, although not signifi-ant, to an increase in length of hospital stay. Thisonflicting result is due to the fact that the mean onset ofelirium in our study was 4.4 days and our patients whoeveloped POD had already been moved from ICU to theurgical ward in a mean of 2.95 days. Therefore we didot observe more patients with POD in the ICU unit. On
he other hand, our patients with POD did not need moreCU stay; it is also our policy to promote early ambulationnd to ensure a tranquil postoperative care setting foratients who undergo a thoracic surgery operation. Inrder to achieve this, we try to transfer our patients asoon as possible when they no longer need ICU moni-oring. In addition, another possible reason for a mean of.8 days of hospital stay in the non-POD group may beue to our cultural habit for a longer hospital stay foratients who undergo a major thoracic surgery. A large-cale international study in older patients found 25.8%
ad postoperative cognitive dysfunction after major ab-by on June 7, 2013 als.org

dt
dPTde
caTioaagnp
R
1
1
1
1
1
1
1
1
1
1
2
2
2
2
2
2
2
2
2
1009Ann Thorac Surg YILDIZELI ET AL2005;79:1004–9 DELIRIUM IN THORACIC SURGERY
GEN
ERA
LT
HO
RA
CIC
ominal or orthopedic surgery, and 9.9% still had cogni-ive impairment three months after surgery [28].
Our results have led us to develop a prospective trialesigned to identify risk factors for the development ofOD within a population of thoracic surgery patients.he study was designed to predict the individual risk foreveloping POD at the end of surgery based on preop-rative data and intraoperative course.In conclusion, delirium may cause more postoperative
omplications in thoracic surgery patients and its vari-ble presentation may mask the diagnosis and its cause.o prevent the development of postoperative delirium,
ntensive care should be provided for patients who arelder and present with postoperative sleep deprivation,nd who also have longer operation time and markedlybnormal postoperative levels of sodium, potassium, orlucose. Therefore, we recommend detecting and elimi-ating these risk factors during the preoperative andostoperative periods to prevent the occurrence of POD.
eferences
1. Szokol JW, Vender JS. Anxiety, delirium and pain in theintensive care unit. Crit Care Clin 2001;17:821–42.
2. Dyer CB, Ashton CM, Teasdale TA. Postoperative delirium.A review of 80 primary data-collection studies. Arch InternMed 1995;155:461–5.
3. Marcantonio ER, Goldman L, Mangione CM, et al. A clinicalprediction rule for delirium after elective noncardiac sur-gery. JAMA 1994;271:134–9.
4. Aakerlund LP, Rosenberg J. Postoperative delirium: treat-ment with supplementary oxygen. Br J Anaesth 1994;72:286–90.
5. American Psychiatric Association. Diagnostic and statisticalmanual of mental disorders. 4th ed. Washington, DC: Amer-ican Psychiatric Association APA Press; 1997.
6. Wang SG, Lee UJ, Goh EK, Chon KM. Factors associatedwith postoperative delirium after major head and necksurgery. Ann Otol Rhinol Laryngol 2004;113:48–51.
7. Marino PL. Hypoxemia and hypercapnia. In: Paul L. Marino,ed. The ICU book. 2nd ed. Baltimore: Lippincott Williamsand Wilkins; 1998:339–54.
8. Lipowski ZJ. Delirium: how its concept has developed. IntPsychogeriatr 1991;3:115–20.
9. Marcantonio ER, Goldman L, Orav EJ, Cook EF, Lee TH. Theassociation of intraoperative factors with development ofpostoperative delirium. Am J Med 1998;105:380–4.
0. Franco K, Litaker D, Locala J, Bronson D. The cost of
delirium in the surgical patient. Psychomatics 2001;42:68–73.ats.ctsnetjournDownloaded from
1. Sasajima Y, Sasajima T, Uchida H, et al. Postoperativedelirium in patients with chronic lower limb ischaemia: whatare the specific markers? Eur J Vasc Surg 2000;20:132–7.
2. Lynch EP, Lazor MA, Gellis JE, et al. The impact of postop-erative pain on the development of postoperative delirium.Anesth Analg 1998;86:781–5.
3. van der Mast RC, van der Broek WW, Fekkes D, Pep-plinkhuizen L, Habbema JD. Incidence of and preoperativepredictors for delirium after cardiac surgery. J PsychosomRes 1999;46:479–83.
4. Galanakis P, Bickel H, Gradinger R, Gumppenberg SV,Forstl H. Acute confusional state in the elderly following hipsurgery: incidence, risk factors and complications. Int JGeriatr Psychiatry 2001;16:349–55.
5. Williams-Russo P, Urquhart BL, Sharrock NE, Charlson ME.Post-operative delirium: predictors and prognosis in theelderly orthopedic patients. J Am Geriatr Soc 1992;40:759–67.
6. Kaneko T, Takahashi S, Naka T, Hirooka Y, Inoue Y, KaibaraN. Postoperative delirium following gastrointestinal surgeryin elderly patients. Surg Today 1997;27:107–11.
7. Schneider F, Böhner H, Habel U, et al. Risk factors forpostoperative delirium in vascular surgery. Gen Hosp Psy-chiatry 2002;24:28–34.
8. Böhner H, Hummel TC, Habel U, et al. Predicting deliriumafter vascular surgery. A model based on pre- and intraop-erative data. Ann Surg 2003;238:149–56.
9. Winawer N. Postoperative delirium. Med Clin North Am2001;85:1229–39.
0. Herrmann M, Ebert AD, Galazky I, Wunderlich MT, KunzWS, Huth C. Neurobehavioral outcome prediction aftercardiac surgery: role of neurobiochemical markers of dam-age to neuronal and glial brain tissue. Stroke 2000;31:645–50.
1. Rasmussen LS, Christiansen M,Rasmussen H KristensenPA, Moller JT. Do blood concentrations of neurone specificenolase and S-100 beta protein reflect cognitive dysfunctionafter abdominal surgery? ISPOCD Group. Br J Anaesth2000;84:242–4.
2. Shigeta H, Yasui A, Nimura Y, et al. Postoperative deliriumand melatonin levels in elderly patients. Am J Surg 2001;182:449–54.
3. Parikh SS, Chung F. Postoperative delirium in the elderly.Anesth Analg 1995;80:1223–1332.
4. Chan D, Brennan NJ. Delirium: making the diagnosis, im-proving the prognosis. Geriatrics 1999;54:28–42.
5. Hanania M, Kitain E. Melatonin for treatment and preven-tion of postoperative delirium. Anesth Analg 2002;94:338–9.
6. Aizawa K, Kanai T, Saikawa Y, et al. A novel approach to theprevention of postoperative delirium in the elderly aftergastrointestinal surgery. Surg Today 2002;32:310–4.
7. Trzepac ZPT. Delirium: advances in diagnosis, pathophysi-ology and treatment. Psychiatr Clin North Am 1996;19:429–49.
8. Moller JT, Cluitmans P, Rasmussen LS, et al. Long-termpostoperative cognitive dysfunction in the elderly. ISPOCD
1 study. Lancet 1998;351:857–61.by on June 7, 2013 als.org

2005;79:1004-1009 Ann Thorac SurgBekiroglu and Mustafa Yüksel
Bedrettin Yildizeli, M. Oguzhan Özyurtkan, Hasan F. Batirel, Kemal Kuscu, Nural Factors Associated With Postoperative Delirium After Thoracic Surgery
& ServicesUpdated Information
http://ats.ctsnetjournals.org/cgi/content/full/79/3/1004including high-resolution figures, can be found at:
References http://ats.ctsnetjournals.org/cgi/content/full/79/3/1004#BIBL
This article cites 26 articles, 6 of which you can access for free at:
Citations
shttp://ats.ctsnetjournals.org/cgi/content/full/79/3/1004#otherarticleThis article has been cited by 11 HighWire-hosted articles:
Subspecialty Collections
http://ats.ctsnetjournals.org/cgi/collection/lung_other Lung - other
following collection(s): This article, along with others on similar topics, appears in the
Permissions & Licensing
[email protected]: orhttp://www.us.elsevierhealth.com/Licensing/permissions.jsp
in its entirety should be submitted to: Requests about reproducing this article in parts (figures, tables) or
Reprints [email protected]
For information about ordering reprints, please email:
by on June 7, 2013 ats.ctsnetjournals.orgDownloaded from