SSR182289A, a selective and potent orally active thrombin inhibitor
Upload
independentCategory
view
3download
0
1998;65:352-358 Ann Thorac SurgDaniel McKenna, Evelio Rodriguez and Herbert Reich
Victor A. Ferraris, Suellen P. Ferraris, Amandeep Singh, Wendy Fuhr, Darren Koppel, The Platelet Thrombin Receptor and Postoperative Bleeding
http://ats.ctsnetjournals.org/cgi/content/full/65/2/352the World Wide Web at:
The online version of this article, along with updated information and services, is located on
ISSN: 0003-4975; eISSN: 1552-6259. Southern Thoracic Surgical Association. Copyright © 1998 by The Society of Thoracic Surgeons. Print
is the official journal of The Society of Thoracic Surgeons and theThe Annals of Thoracic Surgery
by on June 1, 2013 ats.ctsnetjournals.orgDownloaded from

The Platelet Thrombin Receptor and PostoperativeBleedingVictor A. Ferraris, MD, PhD, Suellen P. Ferraris, PhD, Amandeep Singh,Wendy Fuhr, MD, Darren Koppel, MD, Daniel McKenna, Evelio Rodriguez, MD, andHerbert Reich, MDDivision of Cardiothoracic Surgery, Albany Medical College, Albany, New York
Background. We hypothesized that small amounts ofthrombin desensitize the platelet thrombin receptor dur-ing cardiopulmonary bypass (CPB), resulting in postop-erative platelet dysfunction and bleeding.
Methods. Seventy-nine patients were entered into astudy designed to measure changes in platelet thrombinreceptor function during CPB and to correlate them topostoperative bleeding. In addition to measurements ofclinical blood loss, platelet function tests of aggregation,activation, and cell–cell adhesion were used. The throm-bin receptor agonist peptide (TRAP) was used to activatethe platelets. Flow cytometry was used to measure vari-ous platelet surface markers and platelet–white cell in-teractions during CPB.
Results. Compared with preoperative values, both ag-gregometry and flow cytometry measured a significantreduction of TRAP-induced activation immediately andup to 24 hours after CPB. The response of other activating
agents returned to normal by 24 hours. Postoperatively, 8of 79 patients required excessive blood transfusion (>210units of blood products) and had significantly decreasedTRAP-induced aggregation response.
Conclusions. Our results show that (1) platelet activa-tion, aggregation, and adhesion to leukocytes induced byTRAP are reduced after CPB, (2) decreased thrombinreceptor responsiveness is associated with excessivepostoperative blood loss, and (3) because the aggregationand activation responses are different for TRAP andthrombin, there may be a second thrombin receptor onplatelets that is protected from damage during CPB.These results imply that prevention of the CPB-inducedeffects on the thrombin receptor will lessen postoperativemorbidity associated with blood transfusion.
(Ann Thorac Surg 1998;65:352–8)© 1998 by The Society of Thoracic Surgeons
Thrombin is one of several proteolytic enzymes thatare generated during cardiopulmonary bypass
(CPB). Active thrombin is present during CPB in spite ofapparently adequate heparin levels [1, 2]. The stimulusfor thrombin generation is activation of the extrinsiccoagulation pathway both from contact of blood withsynthetic surfaces and from exposure of blood within thesurgical wound [3]. Cellular and humoral mechanismsinvolving thrombin play an important part in the com-plex molecular processes initiated by CPB.
One of the molecular mechanisms of thrombin-induced platelet activation recently has been elucidated,and one platelet thrombin receptor has been cloned [4].Thrombin activates cells by a proteolytic mechanism thatcleaves a portion of the amino terminus of a seven-transmembrane domain thrombin receptor (STTR). Thisproteolytic step exposes a “tethered ligand” that partici-pates in an extracellular signaling mechanism. The teth-ered ligand binds to another extracellular site on the
STTR and induces a cellular response by coupling withcytoplasmic G-proteins. Short peptide chains, calledthrombin receptor agonist peptides (TRAPs), that dupli-cate the amino terminal of the tethered ligand are capa-ble of inducing many, but not all, of the effects ofthrombin [5]. They can activate platelets and mimic theeffect of thrombin on the STTR [6, 7]. The stimulation ofplatelets using TRAPs ensures that the STTR is activatedand is the likely intermediary of the platelet-specificeffect.
Abnormalities of platelet function generally are con-sidered to be a major mechanism of perioperative bleed-ing in patients undergoing CPB [8, 9]. It has been difficultto identify a specific, intrinsic abnormality in these plate-lets. Because thrombin is the preeminent platelet agonist,newer information has focused on the effect of thrombinon platelets during CPB. Recent interest in the STTR [10]caused us to evaluate the platelet responsiveness toTRAPs during CPB. We found that the thrombin receptoris dysfunctional after CPB [11–13]. This led us to thehypothesis that thrombin interaction with target systems(particularly platelets) is dysfunctional after CPB andmay cause excessive postoperative bleeding. This studyattempted to test this hypothesis by determining theclinical relevance of thrombin receptor–related abnor-malities after CPB.
Presented at the Poster Session of the Thirty-third Annual Meeting of TheSociety of Thoracic Surgeons, San Diego, CA, Feb 3–5, 1997.
Address reprint requests to Dr Ferraris, 2828 1st Ave, Suite 510, Hunting-ton, WV 25702.
© 1998 by The Society of Thoracic Surgeons 0003-4975/98/$19.00Published by Elsevier Science Inc PII S0003-4975(97)01348-9
by on June 1, 2013 ats.ctsnetjournals.orgDownloaded from

Material and Methods
Patient SelectionSeventy-nine patients were entered into a research pro-tocol that was approved by the institutional review boardat our institution. The study was designed to measurechanges in platelet function during operations usingCPB. Patients were entered into the study if they wereundergoing elective or urgent cardiac procedures. Pa-tients who were undergoing emergency procedures wereexcluded. Any patient older than 21 years of age waseligible for entry. Patients were required to have normallaboratory values for commonly measured hemostaticparameters, including platelet count, activated partialthromboplastin time, and prothrombin time. No attemptwas made to exclude patients who were taking antiplateletdrugs before operation and, in fact, nearly every patient inthe study had taken aspirin within 7 days of operation.
MaterialsAdenosine diphosphate, collagen, and ristocetin wereobtained from Chronolog (Havertown, PA). Botha-thrombin and g-thrombin were prepared by John W.Fenton, II, M.D. (Albany, NY) and TRAPs (amino acidsequence SFLLRN) were prepared by Thomas T.Andersen, M.D. (Albany, NY). GPRP (H-gly-pro-arg-pro-OH) and fluorescein isothiocyanate (FITC-celite) wereobtained from Calbiochem (LaJolla, CA) and formyl-methionyleucyl-phenylalanine was obtained from Sigma(St. Louis, MO). PAC-1 murine monoclonal antibody(specific for activated platelet glycoprotein IIb/IIIa com-plex) was obtained from the Cell Center at the Universityof Pennsylvania (Philadelphia, PA). S-12 monoclonal an-tibody (specific for P-selectin) was a generous gift fromRodger McEver, M.D. at the University of Oklahoma(Oklahoma City, OK). CD-42b-PE (specific for plateletglycoprotein Ib/IX), nonspecific IgG-FITC, nonspecificIgG-PE, and nonspecific IgM-FITC were obtained fromImmunotech (Westbrook, ME). CD-45-PerCP monoclo-nal antibody (specific for human leukocytes of any type)and CD-14-FITC monoclonal antibody (specific for hu-man monocytes) were obtained from Becton-Dickinson(San Jose, CA).
Preparation of SamplesBlood samples were drawn through a flushed, indwellingarterial line during the perioperative period at the fol-lowing three times: (1) before skin incision but after theinduction of anesthesia, (2) 30 minutes after the reversalof heparin as judged by the presence of a normal acti-vated clotting time, and (3) 18 to 24 hours after operation.All samples were drawn into a syringe containing sodiumcitrate (0.38% final concentration). The sample wasplaced in a plastic tube and mixed by gentle inversion. Acomplete blood count was obtained using a Coulter STKS(Coulter, Hialeah, FL).
Whole Blood AggregometryPortions of the blood were placed in cuvettes containingisotonic saline solution and warmed to 37°C before un-
dergoing aggregometry. Standard whole blood aggre-gometry methods were used [14, 15]. All samples werediluted to a final platelet count of 125,000/mL by addingan appropriate volume of saline solution to the wholeblood samples. Previous studies have shown that dilutionof samples to a final count as low as 80,000/mL providesreproducible aggregation results. Tests were performed30 to 90 minutes after sampling. Previous studies haveshown that platelet function screening in whole bloodwithin 3 hours of blood collection gives satisfactoryresults [16].
Whole blood aggregometry was performed using aChronolog (Havertown, PA) dual-purpose aggregometerby measuring the increase in impedance (in ohms) be-tween two electrodes as aggregation occurred. Aggrega-tion was allowed to proceed for 8 to 12 minutes, andmaximum impedance measured after 8 minutes wasdefined as the maximal aggregation response. The fol-lowing aggregating agents were used (final concentra-tions): adenosine diphosphate (20 mmol/L), g-thrombin(16 mg/mL), TRAP-6 (10 and 12 mmol/L), and collagen(3 mg/mL). These concentrations were high to ensure thatany change in response seen after CPB was not due to ashift in the dose-response curve.
Flow CytometryA subset of the study patients (10 to 20 patients) hadmeasurements of platelet activation and adhesion per-formed using flow cytometry. Whole blood was diluted1:10 in a modified Tyrode’s buffer (137 mmol/L NaCl, 2.8mmol/L KCl, 1 mM MgCl2, 12 mmol/L NaHCO3, 0.4mmol/L Na2HPO4, 10 mmol/L N-(2-hydroxyethyl)pipera-zine-N9-2-ethanesulphonic acid, 0.35% bovine serum al-bumin, and 5.5 mmol/L glucose; pH 7.4) within 10 min-utes of the blood drawing, and 45-mL aliquots wereincubated for 10 minutes at room temperature with either5 mL of buffer or agonist. The agonists used werea-thrombin (2 U/mL) or TRAP-6 (12 mmol/L). The pep-tide GPRP was added to all a-thrombin samples toprevent fibrin formation. The samples then were incu-bated for 20 minutes at room temperature with a satu-rating concentration of the appropriate antibodies.
For dual-color platelet activation analysis in wholeblood, the monoclonal antibody CD-42b-PE, specific forplatelets (glycoprotein Ib/IX), was added to all samples.In addition, one of the following was used: PAC-1-FITC,specific for activated platelets (glycoprotein IIb/IIIa acti-vation complex); S-12-FITC, specific for platelet P-selectin; IgG-FITC, used as a control for S-12; or IgM-FITC, used as a control for PAC-1.
Samples for tricolor platelet–white blood cell (WBC)interaction analyses were prepared by diluting citratedwhole blood 3:7 with the modified Tyrode’s buffer. Ali-quots (100 mL) were incubated for 10 minutes at roomtemperature with either an agonist or buffer. The follow-ing monoclonal antibodies were used: CD-45-PerCP,specific for all WBCs; CD-14-FITC, specific for all mono-cytes; and either CD-42b-PE, specific for all platelets, orIgG-PE, used as a control for CD-42b-PE. All sampleswere fixed with 1% paraformaldehyde for 60 minutes at
353Ann Thorac Surg FERRARIS ET AL1998;65:352–8 THROMBIN RECEPTOR, BLEEDING, AND CPB
by on June 1, 2013 ats.ctsnetjournals.orgDownloaded from

room temperature, stored at 4°C, and processed within 24hours. All antibodies that required conjugation with afluorescent marker (PAC-1 or S-12) were titrated beforeuse.
Samples were analyzed by a FACScan Flow Cytometer(Becton-Dickinson, Mountain View, CA) using Becton-Dickinson’s Cell Quest software for analysis.
Platelets in dual-color samples were identified by thecharacteristic forward and side scatter pattern of PE-labeled events. Activation of the platelets was measuredby the percentage of platelets that expressed the greenfluorescence of the PAC-1 or S-12 antibody above that oftheir respective controls and the mean fluorescence in-tensity (MFI; in arbitrary fluorescence units) of the totalplatelet population. Each sample analyzed 10,000 plateletevents.
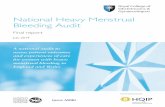
White blood cells with adherent platelets in wholeblood were analyzed by a tricolor method that firstidentified the three WBC populations (monocytes, lym-phocytes, and polymorphonuclear leukocytes) and thenmeasured the PE-positive events (specific for platelets)within these populations (Fig 1). The identification of
these three populations was accomplished by collectingall events that were positive for CD-45-PerCP (all WBCs)and placing electronic bit maps (or gates) around popu-lations that were (1) positive for CD-14-FITC (mono-cytes), (2) partly positive for CD-14-FITC (polymorpho-nuclear leukocytes), and (3) negative for CD-14-FITC(lymphocytes). Figure 1A shows a representative dot-plotobtained using tricolor flow cytometry. The percentage ofWBCs with adherent platelets was determined by mea-suring the percentage of events positive for CD-42b-PE(platelets) within each WBC population above that of theIgG-PE control. Figure 1B shows representative histo-grams of platelet events in the polymorphonuclear leu-kocyte population for 1 patient, using TRAP as theagonist.
Correlation of Thrombin Receptor Function andPostoperative BleedingIn a previous study [17], we found that patients whoreceive more than 10 units of blood products during andafter CPB exceed the 90th percentile of the postoperativepatient population. In view of this finding, and to provide
Fig 1. Tricolor flow cytometry re-sults for thrombin receptor agonistpeptide (TRAP)–induced plateletadhesion to polymorphonuclear leu-kocytes (PMNs). (A) The three leu-kocyte populations. (B) TRAP-stimu-lated platelet populations adherentto PMNs before, immediately after,or 24 hours after cardiopulmonarybypass. (FITC 5 fluorescein isothio-cyanate.)
354 FERRARIS ET AL Ann Thorac SurgTHROMBIN RECEPTOR, BLEEDING, AND CPB 1998;65:352–8
by on June 1, 2013 ats.ctsnetjournals.orgDownloaded from

a sufficiently large number of patients in the excessiveblood loss group, an arbitrary transfusion level of 10donor units was defined as excessive. Platelet functionmeasurements were compared between high-transfusion($10 units of blood products) and low-transfusion (,10units of blood products) groups.
StatisticsWhole blood aggregation response to the various aggre-gating agents before, 30 minutes after, and 24 hours afterCPB were compared using repeated-measures analysis ofvariance with corrected t-tests for intergroup compari-sons. Platelet aggregation responses in the high- andlow-transfusion groups were compared using the Mann-Whitney rank-sum test. Flow cytometry parameters inthe three treatment groups (before, 30 minutes after, and24 hours after CPB) were compared by repeated-measures analysis of variance with adjusted t tests forintergroup comparisons. Probability values of 0.05 or lesswere considered statistically significant.
Results
Whole Blood AggregationThe whole blood aggregation response in 79 patientsduring CPB is shown in Figure 2. The solid areas of thebars represent the 95th percentile above or below themean, the error bars represent 2 standard deviationsabove or below the mean, and the waist in the solid arearepresents the mean value for each aggregating agent ateach time interval. The mean TRAP-induced whole bloodaggregation response decreased significantly both imme-diately after (6.5 6 1.6 V) and 24 hours after (5.6 6 1.4 V)CPB compared with preoperative values (12.8 6 1.5 V;p , 0.01). These were the only statistically significantdifferences for any of the aggregating agents at any of thetime points.
Aggregation Response and Blood TransfusionEight of 79 patients required excessive blood transfusionafter CPB (.10 units of blood products). Ten percent ofthe patients accounted for more than 70% of all the bloodproducts transfused. The TRAP-induced aggregation re-sponse 24 hours after CPB was decreased significantly inthe 8 patients who required excessive blood transfusion(2.1 6 2.4 V) compared with the patients who did notrequire excessive blood transfusion (6.1 6 1.6 V; p , 0.05)(Fig 3). The TRAP-induced aggregation response imme-diately after CPB showed similar results (data notshown). Other aggregating agents did not show statisti-cally significant differences between the high- and low-transfusion groups (Fig 3).
Effect of Cardiopulmonary Bypass on Markers ofPlatelet Activation (Activated Glycoprotein IIb/IIIa andP-selectin)The platelet activation response was measured usingdual-color flow cytometry. Activated platelets express avariety of substances on their surface to improve adhe-sion and facilitate blood clotting. One of these substancesis the activated form of the platelet fibrinogen receptor.On platelet activation, the fibrinogen receptor undergoesa conformational change that facilitates the binding offibrinogen and allows platelet plug formation. The mono-clonal antibody, PAC-1, is a specific probe of the acti-vated platelet fibrinogen receptor (activated glycoproteinIIb/IIIa). Fluorescence-tagged PAC-1 was used to moni-tor agonist-induced platelet activation. Figure 4 showsthe effect of TRAP-induced platelet expression of theactivated fibrinogen receptor during CPB. PAC-1 expres-sion on platelets was decreased significantly in responseto TRAP 30 minutes after CPB (76 6 13 MFI) and 24 hoursafter CPB (94 6 17 MFI) compared with preoperativevalues (143 6 27 MFI; p , 0.01).
Platelets also express P-selectin on their surface, andthis protein is considered a marker of the platelet activa-
Fig 2. Whole blood aggregation responses to various aggregatingagents before (pre-op), immediately after (immed p-op), and 24hours after (24 h p-op) cardiopulmonary bypass. (ADP 5 adeno-sine diphosphate; TRAP 5 thrombin receptor agonist peptide.)
Fig 3. Thrombin receptor agonist peptide (TRAP)–induced wholeblood (WB) aggregation response 24 hours after cardiopulmonarybypass (24th post-op) in patients who required excessive bloodtransfusion (white bars) compared with those who did not requireexcessive blood transfusion (dark bars).
355Ann Thorac Surg FERRARIS ET AL1998;65:352–8 THROMBIN RECEPTOR, BLEEDING, AND CPB
by on June 1, 2013 ats.ctsnetjournals.orgDownloaded from

tion response. A fluorescence-tagged monoclonal anti-body specific for P-selectin (S-12-FITC) was used tomonitor agonist-induced platelet activation. Platelet P-selectin expression was decreased significantly in re-sponse to TRAP 30 minutes after CPB (83 6 13 MFI) and24 hours after CPB (82 6 14 MFI) compared with preop-erative values (105 6 13 MFI, p , 0.01; data not shown).The TRAP-induced expression of two activation markers,activated fibrinogen and P-selectin, was decreased sig-nificantly for up to 24 hours after CPB.
Effect of Cardiopulmonary Bypass on Platelet–WhiteBlood Cell Adhesion (Tricolor Flow Cytometry)Leukocytes are thought to have a modulating effect onplatelet function, and platelets express surface moleculesthat facilitate leukocyte–platelet adhesion. Tricolor flowcytometry was used to measure agonist-induced plate-let–leukocyte adhesion in response to TRAP and a non-specific leukocyte stimulant, formyl-methionyleucyl-phenylalanine (used as a control). Figure 5 summarizesthe results of these experiments. The percentage ofpolymorphonuclear leukocytes that contained adherentTRAP-stimulated platelets was decreased significantlyimmediately after CPB (37% 6 12%; p , 0.001) comparedwith preoperative values (76% 6 22%) and values ob-tained 24 hours after CPB (64% 6 18%).
Comment
Many studies have looked at the effect of CPB on plateletfunction [13, 18–21]. It is surprising that a consistentabnormality has not been found in most of these studies.Such abnormalities as in vitro platelet aggregation de-fects [13, 22] or deficiencies in a-granule release [21] havebeen identified, but two well-done studies did not iden-tify any intrinsic platelet abnormality resulting from CPB[23, 24]. Few, if any, of these studies evaluated themolecular mechanisms involving thrombin responsive-ness of platelets during CPB. The present study attempts
to detail a wide spectrum of platelet responses to stimu-lation of the STTR during CPB. Our results indicate thatthe STTR is desensitized or inactivated after CPB. Thisdesensitization is associated with diminished TRAP-induced platelet aggregation, decreased expression ofplatelet activation markers, and limitation of agonist-induced cell–cell adhesion. Further, this CPB-induceddesensitization is associated with excessive postoperativeblood transfusion. These findings suggest that STTRdesensitization is an important and consistent plateletdefect induced by CPB.
The platelet whole blood aggregation response toTRAP, but not to thrombin, is decreased after CPB (seeFig 2). This divergence of results between two agoniststhat presumably stimulate the same receptor deservesfurther discussion. Recently, a putative second thrombinreceptor has been identified using “knockout” mice thatare deficient in the gene for the conventional thrombinreceptor originally cloned in Coughlin’s laboratory [4, 25,26]. The second thrombin receptor identified in knockoutmice is inferred from studies using TRAPs. The plateletsin knockout mice are normally responsive to thrombin,but their fibroblasts do not respond either to TRAPs or tothrombin [25]. This is strong inferential evidence that asecond thrombin receptor exists on mouse platelets. Ourresults, shown in Figure 2, support the concept of asecond thrombin receptor, distinct from the STTR, onhuman platelets. The thrombin responsiveness of theputative second thrombin receptor seems to be relativelyprotected from the damaging effects of CPB. Furtherstudies are required to elaborate on this preliminaryfinding.
Increased blood use is associated with CPB-inducedSTTR desensitization. This suggests that the generationof thrombin and perhaps other proteolytic enzymes dur-ing CPB may be responsible for desensitizing the STTRand compromising hemostasis after operation. This
Fig 4. Thrombin receptor agonist peptide (TRAP)–induced expres-sion of activated fibrinogen receptor on platelets during cardiopul-monary bypass. (Immed post-op 5 immediately after operation;pre-op 5 before operation; 24th post-op 5 24 hours after opera-tion.)
Fig 5. Alterations in thrombin receptor agonist peptide (TRAP)–induced platelet–leukocyte adhesion during cardiopulmonary bypass(CPB). (FMLP 5 formyl-methionyleucyl-phenylalanine; PMNs 5polymorphonuclear leukocytes; post-CPB 5 after cardiopulmonarybypass; pre-op 5 before operation; 24th p-op 5 24 hours after op-eration.)
356 FERRARIS ET AL Ann Thorac SurgTHROMBIN RECEPTOR, BLEEDING, AND CPB 1998;65:352–8
by on June 1, 2013 ats.ctsnetjournals.orgDownloaded from

thrombin-related hemostatic defect involves at least twosteps: (1) generation of thrombin (eg, from extrinsicpathway activation through tissue factor and factor VII[1]), and (2) desensitization or incomplete activation ofthe STTR on target cells such as platelets and endothelialcells. It would follow that strategies aimed at limiting theharmful effects of thrombin during CPB would result inimproved hemostasis.
Drugs or antibodies that are STTR antagonists mayhave clinical benefit in limiting postoperative blood loss.It is reasonable to suggest that trials aimed at protectingthe STTR during CPB, perhaps using hirudin or otherSTTR antagonists in conjunction with heparin, are indi-cated to limit blood transfusion in high-risk patients [27,28].
Leukocytes are thought to modulate platelet function,and various soluble mediators play a role in this regula-tion [29]. For example, thrombin-induced platelet activa-tion is downregulated by neutrophils in vitro [29]. Acti-vated platelets translocate adhesion molecules to theirsurface that facilitate the binding of WBCs. One of theseadhesion molecules is P-selectin. Blockade of P-selectin–mediated binding of platelets to WBCs results in down-regulation of thrombin-induced platelet activation [29].We observed a significant decrease in the expression ofP-selectin on TRAP-activated platelets after CPB. Simul-taneously, we found a very significant decrease in plate-let–polymorphonuclear leukocyte binding in response toTRAP after CPB (Fig 5). Likewise, Rinder and co-workers[30, 31] found that CPB induces the loss of plateletadhesion receptors, the formation of platelet–leukocyteconjugates, and the activation of leukocytes. Our studiessuggest that abnormalities in TRAP-induced plateletfunctions, including platelet–leukocyte adhesion, are cor-related with excessive postoperative blood transfusion.Taken together, these results suggest that thrombin-induced platelet leukocyte adhesion contributes to he-mostasis, especially after CPB.
The adhesion molecule or molecules responsible forthis decreased agonist-induced platelet–leukocyte bind-ing is uncertain. However, because platelet P-selectin isknown to induce platelet–leukocyte adhesion, and inview of our results using a specific monoclonal antibodydirected at platelet P-selectin, it seems likely that P-selectin–mediated platelet–leukocyte adhesion is at leastpartly responsible for the observed effect. Other adhesionmolecules also may play a part in this effect. Further-more, our results and those of others [28] suggest aprocoagulant role for thrombin-induced P-selectin–mediated binding of platelets to leukocytes (and perhapsendothelial cells). Further work needs to be done tocharacterize the significance of multicellular (especiallyplatelet–leukocyte) modulation of molecular processesduring CPB and their effect on postoperative hemostasis.
In summary, platelet responses to TRAP are decreasedafter CPB, and this defect is associated with increasedpostoperative blood transfusion. This suggests that thegeneration of thrombin and resultant activation of thethrombin receptor are important causes of postoperativebleeding. Attempts to control blood loss during CPB,
especially in high-risk patients, should include the pro-tection of the thrombin receptor and limitation of throm-bin generation during operation.
We thank Mrs Ruth Myer for her expert help in the preparationof the manuscript.
References
1. Boisclair MD, Lane DA, Philippou H, Sheikh S, Hunt B.Thrombin production, inactivation and expression duringopen heart surgery measured by assays for activation frag-ments including a new ELISA for prothrombin fragmentF1 1 2. Thromb Haemost 1993;70:253–8.
2. Brister SJ, Ofosu FA, Buchanan MR. Thrombin generationduring cardiac surgery: is heparin the ideal anticoagulant?Thromb Haemost 1993;70:259–62.
3. Edmunds LH Jr, Ellison N, Colman RW, et al. Plateletfunction during cardiac operation: comparison of membraneand bubble oxygenators. J Thorac Cardiovasc Surg 1982;83:805–12.
4. Vu TK, Hung DT, Wheaton VI, Coughlin SR. Molecularcloning of a functional thrombin receptor reveals a novelproteolytic mechanism of receptor activation. Cell 1991;64:1057–68.
5. Connolly TM, Condra C, Feng DM, et al. Species variabilityin platelet and other cellular responsiveness to thrombinreceptor-derived peptides. Thromb Haemost 1994;72:627–33.
6. Nanevicz T, Ishii M, Wang L, et al. Mechanisms of thrombinreceptor agonist specificity. Chimeric receptors and comple-mentary mutations identify an agonist recognition site. J BiolChem 1995;270:21619–25.
7. Lerner DJ, Chen M, Tram T, Coughlin SR. Agonist recogni-tion by proteinase-activated receptor 2 and thrombin recep-tor. Importance of extracellular loop interactions for receptorfunction. J Biol Chem 1996;271:13943–7.
8. Bracey AW, Radovancevic R. The hematologic effects ofcardiopulmonary bypass and the use of hemotherapy incoronary artery bypass grafting. Arch Pathol Lab Med 1994;118:411–6.
9. Woodman RC, Harker LA. Bleeding complications associ-ated with cardiopulmonary bypass. Blood 1990;76:1680–97.
10. Coughlin SR. Molecular mechanisms of thrombin signaling.Semin Hematol 1994;31:270–7.
11. Ferraris VA, Ferraris SP, Reich H, et al. Thrombin receptor-related hemostatic defect after cardiopulmonary bypass.Semin Thromb Hemost 1996;22:351–6.
12. Rodriguez E, Ferraris VA, Ferraris SP, et al. Abnormalities inthe platelet thrombin receptor are associated with excessiveblood transfusion after cardiopulmonary bypass. Surg Fo-rum 1996;47:258–60.
13. Ferraris VA, Rodriguez E, Ferraris SP, et al. Platelet aggre-gation abnormalities after cardiopulmonary bypass [Letter;Comment]. Blood 1994;83:299–301.
14. Ingerman-Wojenski C, Smith JB, Silver MJ. Evaluation ofelectrical aggregometry: comparison with optical aggregom-etry, secretion of ATP, and accumulation of radiolabeledplatelets. J Lab Clin Med 1983;101:44–52.
15. Zilla P, Fasol R, Deutsch M, et al. Whole blood aggregometryand platelet adenine nucleotides during cardiac surgery.Scand J Thorac Cardiovasc Surg 1988;22:165–9.
16. Sweeney JD, Hoernig LA, Michnik A, Fitzpatrick JE. Wholeblood aggregometry, influence of sample collection anddelay in study performance on test results. Am J Clin Pathol1989;92:676–9.
17. Ferraris VA, Ferraris SP. Limiting excessive postoperativeblood transfusion after cardiac procedures. A review. TexHeart Inst J 1995;22:216–30.
18. Greilich PE, Carr ME Jr, Carr SL, Chang AS. Reductions inplatelet force development by cardiopulmonary bypass areassociated with hemorrhage. Anesth Analg 1995;80:459–65.
357Ann Thorac Surg FERRARIS ET AL1998;65:352–8 THROMBIN RECEPTOR, BLEEDING, AND CPB
by on June 1, 2013 ats.ctsnetjournals.orgDownloaded from

19. Irani MS, Izzat NN, Jones JW. Platelet function, coagulationtests, and cardiopulmonary bypass: lack of correlation be-tween pre-operative and intra-operative whole blood lumi-aggregometry and peri-operative blood loss in patients re-ceiving autologous platelet-rich plasma. Blood CoagulFibrinolysis 1995;6:428–32.
20. Ray MJ, Marsh NA, Hawson GA. Relationship of fibrinolysisand platelet function to bleeding after cardiopulmonarybypass. Blood Coagul Fibrinolysis 1994;5:679–85.
21. Harker LA, Malpass TW, Branson HE, Hessel EA II, SlichterSJ. Mechanism of abnormal bleeding in patients undergoingcardiopulmonary bypass: acquired transient platelet dys-function associated with selective alpha-granule release.Blood 1980;56:824–34.
22. Jung G, Razafindranaibe F, Elkouby A, Durasnel P, Panes F,Monassier JP. Modifications of platelet shape change andATP release during cardiopulmonary bypass. Haemostasis1995;25:149–57.
23. Kestin AS, Valeri CR, Khuri SF, et al. The platelet functiondefect of cardiopulmonary bypass. Blood 1993;82:107–17.
24. Bertolino G, Locatelli A, Noris P, et al. Platelet compositionand function in patients undergoing cardiopulmonary by-pass for heart surgery. Haematologica 1996;81:116–20.
25. Connolly AJ, Ishihara H, Kahn ML, Farese RV Jr, Coughlin
SR. Role of the thrombin receptor in development andevidence for a second receptor. Nature 1996;381:516–9.
26. Darrow AL, Fung-Leung W, Ye RD, et al. Biological conse-quences of thrombin receptor deficiency in mice. ThrombHaemost 1996;76:860–6.
27. Walenga JM, Bakhos M, Messmore HL, et al. Comparison ofrecombinant hirudin and heparin as an anticoagulant in acardiopulmonary bypass model. Blood Coagul Fibrinolysis1991;2:105–11.
28. Callas D, Bacher P, Iqbal O, Hoppensteadt D, Fareed J.Fibrinolytic compromise by simultaneous administration ofsite-directed inhibitors of thrombin. Thromb Res 1994;74:193–205.
29. Valles J, Santos MT, Marcus AJ, et al. Downregulation ofhuman platelet reactivity by neutrophils. Participation oflipoxygenase derivatives and adhesive proteins. J Clin Invest1993;92:1357–65.
30. Rinder CS, Gaal D, Student LA, Smith BR. Platelet-leukocyteactivation and modulation of adhesion receptors in pediatricpatients with congenital heart disease undergoing cardio-pulmonary bypass. J Thorac Cardiovasc Surg 1994;107:280–8.
31. Rinder CS, Fitch JC. Amplification of the inflammatoryresponse: adhesion molecules associated with platelet/whitecell responses. J Cardiovasc Pharmacol 1996;27:S6–S12.
The Thoracic Surgery Foundation for Research andEducation: Continuing Education Programs in HealthCare PolicyThe Thoracic Surgery Foundation for Research and Ed-ucation invites you to attend a limited enrollment exec-utive program on health policy, Understanding the NewWorld of Health Care, to be held at the Kennedy Schoolof Government, March 28–April 5, 1998. The programcovers the following topics: the basics of health econom-ics, the workings of the political environment and themedia, hospital and physician reimbursement programs,the structure of Medicare and Medicaid, the inner work-ings of managed care, the role of information technology,
the relevant aspects of antitrust, professional and corpo-rate liability, and the nature and extent of health carefraud. A limited number of tuition scholarships areavailable.
Applications for a year-long sabbatical at HarvardUniversity to do graduate studies are also available.
For more information on the Executive Program or theyear-long sabbatical, please contact Amy Hedmark inThe Foundation office: telephone: (312) 644-6610; fax:(312) 527-6635; e-mail: [email protected].
358 FERRARIS ET AL Ann Thorac SurgTHROMBIN RECEPTOR, BLEEDING, AND CPB 1998;65:352–8
© 1998 by The Society of Thoracic Surgeons Ann Thorac Surg 1998;65:358 • 0003-4975/98/$19.00Published by Elsevier Science Inc
by on June 1, 2013 ats.ctsnetjournals.orgDownloaded from

1998;65:352-358 Ann Thorac SurgDaniel McKenna, Evelio Rodriguez and Herbert Reich
Victor A. Ferraris, Suellen P. Ferraris, Amandeep Singh, Wendy Fuhr, Darren Koppel, The Platelet Thrombin Receptor and Postoperative Bleeding
& ServicesUpdated Information
http://ats.ctsnetjournals.org/cgi/content/full/65/2/352including high-resolution figures, can be found at:
References http://ats.ctsnetjournals.org/cgi/content/full/65/2/352#BIBL
This article cites 31 articles, 10 of which you can access for free at:
Citations http://ats.ctsnetjournals.org/cgi/content/full/65/2/352#otherarticles
This article has been cited by 22 HighWire-hosted articles:
Permissions & Licensing
[email protected] or email: http://www.us.elsevierhealth.com/Licensing/permissions.jsp
entirety should be submitted to: Requests about reproducing this article in parts (figures, tables) or in its
Reprints [email protected]
For information about ordering reprints, please email:
by on June 1, 2013 ats.ctsnetjournals.orgDownloaded from
Copyright © 2022 FDOKUMEN