
Electrophysiologic properties and antiarrhythmic actions of a novel antianginal agent
9
Electrophysiologic properties and antiarrhythmic mechanisms of intravenous Macetylprocainamide in patients with ventricular dysrhythmias To define electrophysiologic properties and antiarrhythmic mechanisms of N-acetylprocainamide (NAPA), we studied 16 patients with symptomatic ventricular dysrhythmias. Electrophysiologic studies were performed before and after intravenous infusion of NAPA at 20 mg/kg over 20 minutes, achieving plasma concentrations of 24 + 3.2 to 35.5 f 4.5 pg/ml. NAPA did not significantly change sinus cycle length or atrioventricular (AV) conduction times (PA, AH, HV, and QRS), but it lengthened the QTc interval (p < 0.001) during sinus rhythm. Programmed atrial stimulation revealed that NAPA had no discernible effects on AV nodal conduction; however, it exerted depressive effects on the His-Purkinje system in g of 16 patients. In 7 of 16 patients who manifested frequent ventricular premature beats (VPBs), NAPA abolished VPBs in only three of them; NAPA induced progressive prolongation of the premature coupling interval before complete abolition of VPBs. In 8 of 16 patients who had inducible repetitive ventricular response (RVR) because of reentry within the His-Purkinje system, NAPA narrowed or abolished the RVR zone in 3 patients and slowed the RVR rate with widening of the RVR zone in the remaining 5 patients. In 2 of 16 patients with slow ventricular tachycardia (VT), NAPA had no antiarrhythmic effects. By contrast, in the other 2 of 16 patients in whom sustained VT could be reproducibly elicited with programmed ventricular stimulation, NAPA slowed the rate of VT and suppressed VT inducibility. We conclude that electrophysiologic properties of NAPA are slightly different from those of procainamide and that NAPA is not uniformly effective for suppressing ventricular dysrhythmias, but its antiarrhythmic mechanisms are similar to those of procainamide. (AM HEART J 105:811, 1983.) Ruey J. Sung, M.D., Zulfikar Juma, M.D., and Sanjeev Saksena, M.D. Miami, Flu. Pharmacokinetic studies of procainamide have shown that N-acetylprocainamide (NAPA) is the major metabolite in human subjects.‘,* Animal stud- ies and isolated tissue studies have further demon- strated that NAPA possesses important pharmaco- logic and antiarrhythmic properties.3-7 Recent clini- cal studies have confirmed that NAPA has antiar- rhythmic effects in patients with chronic ventricular dysrhythmias.3s 8. g Using the technique of intracardiac recordings along with the method of programmed electrical stimulation, we studied 16 patients with symptom- atic ventricular dysrhythmias. The study was From the Clinical Cardiac Electrophysiology Laboratory, Jackson Memo- rial Hospital, and the Department of Medicine, University of Miami School of Medicine. Received for publication Dec. 1, 1981; revision received Feb. 8, 1982; accepted Mar. 3, 1982. Reprint requests: Ruey J. Sung, M.D., Director, Clinical Electrophysiology Laboratory, Suite 575, Moffitt Hospital, University of California, San Francisco, CA 94143. designed to delineate electrophysiologic properties, as well as antiarrhythmic mechanisms, of intrave- nous NAPA in patients with symptomatic ventricu- lar dysrhythmias. METHODS Patient population. The study group comprised 16 patients: 12 men and 4 women ranging in age from 22 to 70 years (mean 49.8 years) (Table I). All had symptomatic ventricular dysrhythmias manifesting as frequent ventric- ular premature beats of more than 50/hr and/or recurrent ventricular tachycardia. Of these 16 patients, 8 had asso- ciated arteriosclerotic heart disease with or without prior myocardial infarction (4 of 8 had left ventricular aneu- rysm), 2 had cardiomyopathy, 2 had mitral valve prolapse syndrome, and the remaining 4 had no apparent heart disease. Except for 4 patients with prior myocardial infarction pattern, all of them had normal PR interval and QRS duration during sinus rhythm. Of the 16 patients, 10 were previously unresponsive or intolerant to oral prepa- rations of conventional drugs, including quinidine, pro- cainamide, propranolol, and disopyramide, used alone or in various combinations. 811
-
Upload
independent -
Category
Documents
-
view
1 -
download
0
Transcript of Electrophysiologic properties and antiarrhythmic actions of a novel antianginal agent

Electrophysiologic properties and antiarrhythmic mechanisms of intravenous Macetylprocainamide in patients with ventricular dysrhythmias
To define electrophysiologic properties and antiarrhythmic mechanisms of N-acetylprocainamide (NAPA), we studied 16 patients with symptomatic ventricular dysrhythmias. Electrophysiologic studies were performed before and after intravenous infusion of NAPA at 20 mg/kg over 20 minutes, achieving plasma concentrations of 24 + 3.2 to 35.5 f 4.5 pg/ml. NAPA did not significantly change sinus cycle length or atrioventricular (AV) conduction times (PA, AH, HV, and QRS), but it lengthened the QTc interval (p < 0.001) during sinus rhythm. Programmed atrial stimulation revealed that NAPA had no discernible effects on AV nodal conduction; however, it exerted depressive effects on the His-Purkinje system in g of 16 patients. In 7 of 16 patients who manifested frequent ventricular premature beats (VPBs), NAPA abolished VPBs in only three of them; NAPA induced progressive prolongation of the premature coupling interval before complete abolition of VPBs. In 8 of 16 patients who had inducible repetitive ventricular response (RVR) because of reentry within the His-Purkinje system, NAPA narrowed or abolished the RVR zone in 3 patients and slowed the RVR rate with widening of the RVR zone in the remaining 5 patients. In 2 of 16 patients with slow ventricular tachycardia (VT), NAPA had no antiarrhythmic effects. By contrast, in the other 2 of 16 patients in whom sustained VT could be reproducibly elicited with programmed ventricular stimulation, NAPA slowed the rate of VT and suppressed VT inducibility. We conclude that electrophysiologic properties of NAPA are slightly different from those of procainamide and that NAPA is not uniformly effective for suppressing ventricular dysrhythmias,
but its antiarrhythmic mechanisms are similar to those of procainamide. (AM HEART J 105:811, 1983.)
Ruey J. Sung, M.D., Zulfikar Juma, M.D., and Sanjeev Saksena, M.D. Miami, Flu.
Pharmacokinetic studies of procainamide have shown that N-acetylprocainamide (NAPA) is the major metabolite in human subjects.‘,* Animal stud- ies and isolated tissue studies have further demon- strated that NAPA possesses important pharmaco- logic and antiarrhythmic properties.3-7 Recent clini- cal studies have confirmed that NAPA has antiar- rhythmic effects in patients with chronic ventricular dysrhythmias.3s 8. g
Using the technique of intracardiac recordings along with the method of programmed electrical stimulation, we studied 16 patients with symptom- atic ventricular dysrhythmias. The study was
From the Clinical Cardiac Electrophysiology Laboratory, Jackson Memo- rial Hospital, and the Department of Medicine, University of Miami School of Medicine.
Received for publication Dec. 1, 1981; revision received Feb. 8, 1982; accepted Mar. 3, 1982.
Reprint requests: Ruey J. Sung, M.D., Director, Clinical Electrophysiology Laboratory, Suite 575, Moffitt Hospital, University of California, San Francisco, CA 94143.
designed to delineate electrophysiologic properties, as well as antiarrhythmic mechanisms, of intrave- nous NAPA in patients with symptomatic ventricu- lar dysrhythmias.
METHODS
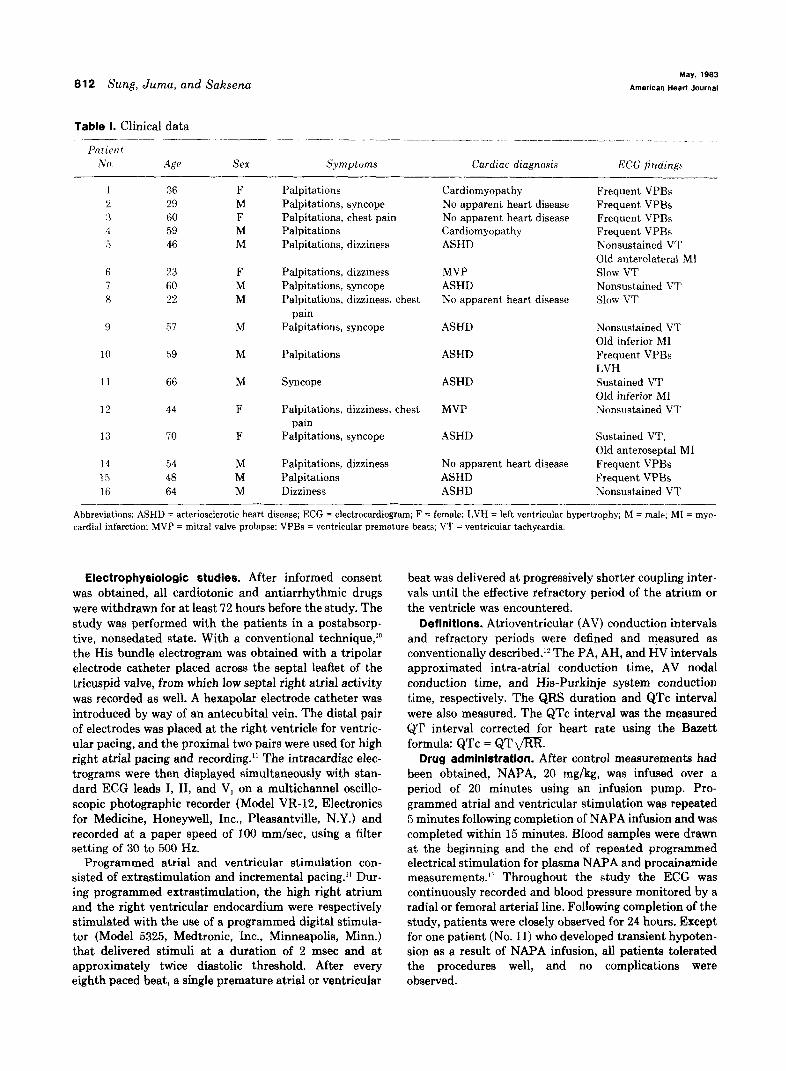
Patient population. The study group comprised 16 patients: 12 men and 4 women ranging in age from 22 to 70 years (mean 49.8 years) (Table I). All had symptomatic ventricular dysrhythmias manifesting as frequent ventric- ular premature beats of more than 50/hr and/or recurrent ventricular tachycardia. Of these 16 patients, 8 had asso- ciated arteriosclerotic heart disease with or without prior myocardial infarction (4 of 8 had left ventricular aneu- rysm), 2 had cardiomyopathy, 2 had mitral valve prolapse syndrome, and the remaining 4 had no apparent heart disease. Except for 4 patients with prior myocardial infarction pattern, all of them had normal PR interval and QRS duration during sinus rhythm. Of the 16 patients, 10 were previously unresponsive or intolerant to oral prepa- rations of conventional drugs, including quinidine, pro- cainamide, propranolol, and disopyramide, used alone or in various combinations.
811
812 Sung, Juma, and Saksena
Table I. Clinical data ___-------- -.-. - --... -- --.. ~-- ._-_ ~-. ~_. _.._____ ___. __.
PatiPnf No. Age Sex S.vmptoms Cardiac diagnosis ECG findings
__- 1 36 F Palpitations Cardiomyopathy Frequent VPBs 2 29 M Palpitations, syncope No apparent heart disease Frequent VPBs 3 60 F Palpitations, chest pain No apparent heart disease Frequent VPBs 3 59 M Palpitations Cardiomyopathy Frequent VPBs 5 46 M Palpitations, dizziness ASHD Nonsustained VT
Old anterolateral MI 6 23 F Palpitations, dizziness MVP Slow VT 7 60 M Palpitations, syncope ASHD Nonsustained VT 8 22 M Palpitations, dizziness, chest No apparent heart disease Slow VT
pain 9 57 M Palpitations, syncope ASHD Nonsustained VT
Old inferior MI 10 59 M Palpitations ASHD Frequent VPBs
LVH 11 66 M Syncope ASHD Sustained VT
Old inferior MI 12 44 F Palpitations, dizziness, chest MVP Nonsustained VT
pain 13 70 F Palpitations, syncope ASHD Sustained VT,
Old anteroseptal MI 14 54 M Palpitations, dizziness No apparent heart disease Frequent VPBs 15 48 M Palpitations ASHD Frequent VPBs 16 64 M Dizziness ASHD Nonsustained VT
-_I-____ Abbreviations: ASHD = arteriosclerotic heart disease; ECG = electrocardiogram; F = female; LVH = left ventricular hypertrophy; M = male: MI = myo- cardial infarction: MVP = mitral valve prolapse: VPBs = ventricular premature beats; VT = ventricular tachycardia.
Electrophysiologic studies. After informed consent was obtained, all cardiotonic and antiarrhythmic drugs were withdrawn for at least 72 hours before the study. The study was performed with the patients in a postabsorp- tive, nonsedated state. With a conventional technique,‘O the His bundle electrogram was obtained with a tripolar electrode catheter placed across the septal leaflet of the tricuspid valve, from which low septal right atria1 activity was recorded as well. A hexapolar electrode catheter was introduced by way of an antecubital vein. The distal pair of electrodes was placed at the right ventricle for ventric- ular pacing, and the proximal two pairs were used for high right atria1 pacing and recording.” The intracardiac elec- trograms were then displayed simultaneously with stan- dard ECG leads I, II, and V, on a multichannel oscillo- scopic photographic recorder (Model VR-12, Electronics for Medicine, Honeywell, Inc., Pleasantville, N.Y.) and recorded at a paper speed of 100 mm/set, using a filter setting of 30 to 500 Hz.
Programmed atria1 and ventricular stimulation con- sisted of extrastimulation and incremental pacing.” Dur- ing programmed extrastimulation, the high right atrium and the right ventricular endocardium were respectively stimulated with the use of a programmed digital stimula- tor (Model 5325, Medtronic, Inc., Minneapolis, Minn.) that delivered stimuli at a duration of 2 msec and at approximately twice diastolic threshold. After every eighth paced beat, a single premature atria1 or ventricular
beat was delivered at progressively shorter coupling inter- vals until the effective refractory period of the atrium or the ventricle was encountered.
Definitions. Atrioventricular (AV) conduction intervals and refractory periods were defined and measured as conventionally described.12 The PA, AH, and HV intervals approximated intra-atria1 conduction time, AV nodal conduction time, and His-Purkinje system conduction time, respectively. The QRS duration and QTc interval were also measured. The QTc interval was the measured QT interval corrected for heart rate using the Bazett formula: QTc = QT fl.
Drug administration. After control measurements had been obtained, NAPA, 20 mg/kg, was infused over a period of 20 minutes using an infusion pump. Pro- grammed atria1 and ventricular stimulation was repeated 5 minutes following completion of NAPA infusion and was completed within 15 minutes. Blood samples were drawn at the beginning and the end of repeated programmed electrical stimulation for plasma NAPA and procainamide measurements.” Throughout the study the ECG was continuously recorded and blood pressure monitored by a radial or femoral arterial line. Following completion of the study, patients were closely observed for 24 hours. Except for one patient (No. 11) who developed transient hypoten- sion as a result of NAPA infusion, all patients tolerated the procedures well, and no complications were observed.

Volume 105
Number 5 Antiarrhythmic mechanisms of N-acetylprocainamide 813
Table II. Effects of NAPA on AV conduction during sinus rhythm
AV conduction intervals (msec) Patient SCL
No. Phase (msec) PA AH HV QRS QTc
1 Pre 680 25 100 40 90 390
Post 620 30 90 40 90 480
2 Pre 700 20 60 40 80 400
Post 680 20 55 40 80 485
3 Pre 750 30 80 35 90 420
Post 720 35 90 35 95 490
4 Pre 820 30 85 45 85 430
Post 700 30 70 50 85 475
5 Pre 615 30 95 50 95 390
Post 610 30 75 50 95 480
6 Pre 875 10 85 45 80 430
Post 710 15 80 40 80 485
7 Pre 940 25 90 55 90 450
Post 950 20 90 55 95 540
8 Pre 750 25 110 45 85 425
Post 670 25 loo 45 85 485
9 Pre 760 20 75 35 80 430
Post 740 25 80 35 80 540
10 Pre 860 25 120 45 90 440
Post 850 30 110 45 90 500
11 Pre 580 20 100 40 85 380
Post 620 30 100 40 90 535 12 Pre 650 25 85 50 85 390
Post 750 20 80 50 85 485
13 Pre 730 25 100 55 95 440
Post 720 25 90 50 95 550
14 Pre 625 20 90 50 80 390 Post 615 25 85 45 85 490
15 Pre 630 20 110 50 75 380 Post 540 25 100 45 80 495
16 Pre 540 25 95 50 80 380
Post 530 20 95 50 85 470
Mean Pre 720 f 25 23 I!Z 8 92 2 5 45 + 4 85 3 410 1 -1- 12 Post 689 + 28 25 -I 3 86 t 10 44 k 3 87 499 -t 2 4 13
p value NS NS NS NS NS NS <O.OOl
Abbreviations: AV = atrioventricular; Pre = before infusion of NAPA; Post = after infusion of NAPA; SCL = sinus cycle length; NS = not significant,
RESULTS
plasma NAPA concentration. At the beginning of repeated programmed electrical stimulation (5 minutes after completion of NAPA infusion), the plasma mean NAPA concentration measured 29.2 to 56.1 pg/ml (Mean + standard error of the mean = 35.5 2 4.5 pg/ml). The study protocol was usually completed in 15 minutes, at which time the plasma NAPA concentration ranged from 18.6 to 28.7 pg/ml (mean + standard error of the mean = 24 + 3.2 pg/ml). In all patients there was no measurable procainamide in any of the plasma blood samples.
Effects of NAPA on AV conduction and refractori- ness. The overall sinus rate was slightly increased 5 minutes after completion of NAPA infusion. The
mean sinus cycle length was 720 f 25 msec (mean t- standard error of the mean) before NAPA infusion and 689 k 28 msec after NAPA infusion (Table II). The change did not reach statistical significance.
During sinus rhythm, the PA, AH, and HV inter- vals were 23 -+ 8, 92 + 5, and 45 f 4 msec, respec- tively, before NAPA infusion and 25 k 3, 86 + 10, and 44 f 3 msec, respectively, after NAPA infusion. None of these changes was statistically significant (Table II). In all patients the QRS duration during sinus rhythm remained relatively unchanged (85 +- 3 msec vs 87 f 4 msec). However, the QTc interval was significantly lengthened following NAPA infu- sion (410 * 12 vs 499 f 13 msec; p value < 0.001) (Table II).
Although NAPA seemed to have had no signifi-

a14 Sung, Juma, and Saksena May, 1983
lmmrican mart Journal
cant effect on the HV interval and QRS duration during sinus rhythm, atria1 extrastimulation revealed that it could potentially affect His-Pur- kinje system conduction and refractoriness. In 9 of the 16 patients (Nos. 1, 3,4, 6, 7, 10, 11, 14, and 161, atrial extrastimulation induced aberrant ventricular conduction of the right or left bundle-branch block pattern only after NAPA infusion. At atrial driving cycle lengths between 540 and 850 msec, the effec- tive refractory periods of right bundle branch (6 patients) measured 360 to 420 msec, and those of left bundle branch (3 patients) measured from 350 to 370 msec after NAPA infusion. In addition, 2 of the 9 patients (Nos. 3 and 7) developed progressive bundle-branch block and HV interval prolongation leading to second-degree infranodal AV block dur- ing incremental atria1 pacing (Fig. 1). The magni- tude of the His-Purkinje system conduction distur- bance induced by programmed atria1 stimulation did not seem to correlate with plasma NAPA con- centrations.
B s $00 s s I h
II VI
HRA- AH" \ \ \
AH " \ V\ V
AH HBE-r-f C
AH AH AH " 100 llO4 110 110
45 100 140 150
II ----A A--A- L
VI ----v HRA i
V \ \ P-
AH AH AH
SOOmrec. llIIIiiIIlI
Fig. 1. NAPA-induced conduction disturbance in the His-Purkinje system. Panel A: During atria1 pacing at a cycle length of 360 msec, AV conduction is 1: 1. The corresponding AV nodal conduction time (AH interval) ranges from 155 to 175 msec, and His-Purkinje system conduction time (HV interval) is 40 msec. Panel B: Following NAPA infusion, the atrium is driven at a cycle length of 400 msec. Note development of 5: 4 AV block below the level of the His bundle. This is preceded by prolongation of the His-Purkinje conduction time (HV interval lengthened from 45 to 150 msec) associated with progression of bundle-branch block-development of incomplete right bundle-branch block (second QRS com- plex), incomplete left bundle-branch block (third QRS complex), and complete left bundle-branch block (fourth QRS complex). Panel C: Further progression to 3:2 and 2: 1 AV block in the His-Purkinje system. In this illustra- tion and in Figs. 3 and 4, ECG leads I, II, and V, are simultaneously recorded with high right atrial (HRA) and His bundle electrographic (HBE) leads. S = stimulus; A = atrial electrogram; H = His bundle deflection.
The right atrium and the right ventricle were respectively driven at cycle lengths between 540 and 850 msec. In each patient the driving cycle length was kept constant before and after NAPA adminis- tration. In all patients the effective refractory peri- ods of the atrium and the ventricle were significant- ly prolonged following NAPA infusion (234 rfr 5 vs 263 + 8 and 215 t 8 vs 248 i- 9 msec; both p val- ues < 0.001). On the other hand, the effect of NAPA on AV nodal refractoriness was minimal. The mean effective and functional refractory periods of the AV node were 315 +- 20 msec and 446 + 16 msec, respectively, before NAPA infusion and 315 + 16 msec and 450 f 18 msec, respectively, after NAPA infusion. These changes had no statistical signifi- cance.
Effects of NAPA on ventricular premature beats. In 7
of the 16 patients (Nos. 1, 2, 3, 4, 10, 14, and 16), frequent premature beats (more than 50/hr) were noted during sinus rhythm before NAPA infusion. Of these 7 patients, intravenous NAPA abolished ventricular premature beats in only 3 patients (Nos. 4, 10, and 14). Characteristically, NAPA induced prolongation of the ventricular premature coupling interval before complete abolition of ventricular premature beats (Fig. 2). Intravenous NAPA did not affect ventricular premature beats in the remaining 4 patients (Nos. 1, 2,3, and 16). The plasma NAPA concentrations in these patients were comparable to those in whom ventricular premature beats could be suppressed by NAPA infusion (Nos. 4, 10, and 14).
Effects of NAPA on repetitive ventricular response due to reentry within the His-Purkinje system. During

Volume105
Number 5 Antiarrhythmic mechanisms of N-acetylprocainamide 815
Fig. 2. Suppression of ventricular premature beats with intravenous NAPA. Panel A: Frequent ventricular premature beats before NAPA infusion. Panel B: A decrease in the frequency of ventricular premature beats with marked lengthening of the ventricular premature coupling interval during NAPA infusion. Panel C: Complete suppression of ventricular premature beats after NAPA infusion. Numerical numbers in PaneZs A and B are ventricular premature coupling intervaIs expressed in seconds.
programmed ventricular stimulation, repetitive ven- tricular response related to reentry within the His- Purkinje systemI could be elicited in 8 of the 16 patients (Table III). Following intravenous infusion of NAPA, the zone of repetitive ventricular response was abolished in 1 patient (No. l), narrowed and shifted rightward in 2 patients (Nos. 4 and 13), and widened in the remaining 5 patients (Nos. 2, 7, 8, 9 and 10). Despite variable effects of NAPA, the cycle length of repetitive ventricular response was consis- tently lengthened whenever it remained inducible after NAPA infusion. One such example is illus- trated in Fig. 3.
Effects of NAPA on ventricular tachycardia. Of the 16 patients, 9 had clinically documented episodes of ventricular tachycardia. Two patients (Nos. 6 and 8) had recurrent slow ventricular tachycardia (or accel- erated idioventricular rhythm) ranging between 75 and 90 bpm. None of them were taking digitalis. Programmed electrical stimulation could neither elicit nor terminate the ventricular tachycardia. Intravenous infusion of NAPA exerted no suppres- sive effect in these 2 patients. The remaining 7 patients had recurrent ventricular tachycardia at rates ranging from 130 to 250 bpm. Five of these patients (Nos. 5,7,9,12, and 16) clinically manifest- ed nonsustained ventricular tachycardia (self-termi- nating and lasting less than 10 beats), and 2 patients (Nos. 11 and 13) sustained ventricular tachycardia (lasting more than 30 seconds or requiring pharma- cologic or electrical intervention). The effects of intravenous NAPA on nonsustained ventricular tachycardia could not be evaluated, because pro- grammed electrical stimulation did not elicit ven- tricuIar tachycardia in these patients. In the 2 patients (Nos. 11 and 13) with sustained ventricular
Table Ill. Effects of NAPA on repetitive ventricular response due to reentry within the His-Purkinje system
RVR zone RVR zone (msec) width (msec)
Patient DCL No. fmsec) B A B A
I 540 170-240 70 0 2 630 210-220 230-270 10 40 3 670 240-280 220-250 40 30 7 820 250-280 260-300 30 40 8 570 240-250 260-280 10 20 9 680 230-280 250-360 50 110
10 700 220-240 230-280 20 50 13 650 270-320 300-320 50 20
Abbreviations: A = after NAPA infusion; B = before NAPA infusion; DCL = driving cycle length; RVR = repetitive ventricular response; - = RVR not inducible.
tachycardia, programmed electrical stimulation could reproducibly elicit the ventricular tachycar- dia. Intravenous infusion of NAPA abolished induc- ibility of sustained ventricular tachycardia in 1 patient (No. 13; Fig. 4) and slowed the ventricular tachycardia in the other (No. 11).
DISCUSSION
This study has demonstrated that NAPA pos- sesses certain electrophysiologic and antiarrhythmic properties similar to those of its parent compound, procainamide.15-25
Effects of NAPA on AV conduction and refractorl- ness. In agreement with observations made by Jail- Ion et a1.,7,26 our study showed that NAPA increased atria1 and ventricular refractoriness and prolonged the QTc interval but had no significant effect on the intra-atria1 conduction time (PA interval), AV nodal

816 Sung, Juma, and Saksena May, 1983
American Heart Journal
A 700 240s 290 5, 300 260 s I 2 /
B *, 700 s, 2802 380 480
I--
I 500msec.
d
Fig. 3. Effects of NAPA on repetitive ventricular response due to reentry within the His-Purkinje system. Panel A: Right ventricle is driven at a cycle length (Si to SIJ of 700 msec. A ventricular premature beat (&‘A with a premature coupling interval (S, to SJ of 240 msec induces repetitive ventricular responses. The zone of repetitive ventricular response ranges from ventricular premature coupling intervals (S, to SJ of 220 to 240 msec. Panel B: Following NAPA infusion, the right ventricle is driven at the same cycle length of 700 msec. The zone of repetitive ventricular response is shifted to the right and ranges from premature coupling intervals (S, to SA of 230 to 280 msec. Thus the zone of repetitive ventricular response is widened from 20 msec to 50 msec. In addition, the cycle length of repetitive ventricular resnonse is lengthened from between 260 and 300 msec (panel A) to between 380 and 480 msec (panel B) following NAPA infusion.
conduction time (AH interval), and AV nodal refrac- toriness. The lack of effect of NAPA on the AV nodal conduction properties as compared to its parent compound was attributed to the absence of vagolytic effect of NAPA.7,21
NAPA did not appear to affect the QRS duration and conduction time (HV interval) of the His- Purkinje system during sinus rhythm. However, our study demonstrated that 9 of the 16 patients devel- oped aberrant ventricular conduction of the right or left bundle-branch block pattern only after NAPA infusion with atrial extrastimulation. Furthermore, in 2 of these 9 patients, incremental atrial pacing induced progressive prolongation of the HV interval and bundle-branch conduction disturbance followed by development of second-degree infranodal con- duction block (Fig. 1). These observations suggest that NAPA may depress His-Purkinje system con- duction and therefore should be administered cau-
tiously, particularly to those patients with preexist- ing His-Purkinje system disease.“j
The effects of NAPA on the His-Purkinje system observed in our study are somewhat different from those found by Jaillon et a1.26 The differences can be explained by the patient population selected for study, the dosage of NAPA infused, and the timing of electrophysiologic measurements performed. We studied patients with symptomatic ventricular dys- rhythmias; 4 of the 16 patients additionally had prior myocardial infarction. Jaillon et a1.26 studied patients with normal atrioventricular conduction undergoing routine cardiac catheterization. We infused NAPA at a dose of 20 mg/kg over 20 minutes, resulting in a peak plasma concentration of 35.5 + 4.5 pg/ml, which then fell to 24 rt 3.2 &ml at the end of the electrophysiologic study; Jaillon et al.26 administered NAPA at a total dose of 10.5 mg/kg with one loading infusion over 15 minutes

Volume 105
Number 5 Antiarrhythmic mechanisms of N-acetylprocainamide 8 17
Fig. 4. Suppression of induction of sustained ventricular tachycardia with intravenous NAPA. Panel A: Before NAPA infusion the right ventricle is driven at a cycle length (S, to SJ of 700 msec. A ventricular premature beat (SJ with a premature coupling interval (S, to SJ of 240 msec elicits a paroxysm of sustained ventricular tachycardia at a cycle length of 220 msec. Panel B: After NAPA infusion, the right ventricle is driven at the same cycle length (S, to SJ of 700 msec. A ventricular premature beat (Sb elicits a short burst of nonsustained ventricular tachycardia at a cycle length of 310 msec.
and one maintenance infusion for 30 minutes to achieve an average plasma concentration of approx- imately 15 pg/ml. Nevertheless, intravenous infu- sion of NAPA had no effect on the resting AV interval and QRS duration despite relatively high plasma concentrations achieved in the present study. We agree that this finding suggests that NAPA is electrophysiologically somewhat different from its parent compound.15-‘7
Antiarrhythmic mechanisms of NAPA. The antiar- rhythmic action of NAPA was evaluated with respect to three types of ventricular arrhythmias: ventricular premature beats, repetitive ventricular response caused by reentry within the His-Purkinje system,14 and inducible ventricular tachycardia. NAPA was not uniformly effective in suppressing ventricular premature beats. It abolished ventricu- lar premature beats in only three of seven patients despite comparable plasma NAPA concentrations. In these three patients, NAPA gradually prolonged the ventricular premature coupling interval before total suppression of ventricular premature beats (Fig. Z), a finding similar to that seen during procai-
namide therapy. 2o This observation suggests that NAPA, similar to its parent compound, can cause exit or conduction delay of a reentrant pathway, thereby eliminating ventricular premature beatszO
Effects of NAPA on repetitive ventricular response resulting from reentry within the His- Purkinje system14 were also similar to those of procainamide.21~22 NAPA could either facilitate or suppress reentry (Table III). Notably, whenever repetitive ventricular response remained inducible following NAPA infusion, the rate of repetitive ventricular response was significantly slowed (Fig. 3). These findings provide further evidence that NAPA affects conduction and refractoriness of the His-Purkinje system.
Although the number of patients is small, NAPA seemed to exert no antiarrhythmic effect on slow ventricular tachycardia (or accelerated idioventricu- lar rhythm) at rates ranging from 60 to 90 bpm. This form of ventricular tachycardia is presumed to be caused by automaticity, since it can be neither elicited nor terminated with programmed ventricu- lar stimulation.

ala Sung, Juma, and Saksena
The antiarrhythmic action of NAPA on inducible sustained ventricular tachycardia is similar to those of procainamide (Fig. 4). 23-25 The mechanism under- lying this form of ventricular tachycardia is pre- sumed to be reentry. NAPA slowed the rate of ventricular tachycardia and could suppress the inducibility of ventricular tachycardia during pro- grammed electrical stimulation. NAPA is thus capa- ble of affecting the reentrant pathway of inducible sustained ventricular tachycardia.
Electrophysiologic and therapeutic implications. Based on the observations made in the present study, there are several important clinical implica- tions relating to the clinical use of NAPA: (1) Intravenous infusion of NAPA at a dosage of 20 mg/kg over 20 minutes is safe and rarely causes hypotension. (2) Similar to procainamide, NAPA lengthens the QTc interval during sinus rhythm and prolongs atria1 and ventricular refractoriness. (3) Unlike procainamide, NAPA exerts negligible effects on AV nodal conduction and refractoriness and has no effects on the QRS duration and His- Purkinje conduction time (HV interval) during sinus rhythm in the presence of relatively high plasma concentrations. However, NAPA may have depressive effects on the His-Purkinje system as revealed by atrial extrastimulation and incremental atria1 pacing. NAPA should be given cautiously to patients, particularly those with preexisting His- Purkinje system disease. (4) NAPA is not uniformly effective for controlling ventricular dysrhythmias. Nevertheless, its antiarrhythmic mechanisms of suppressing ventricular premature beats and ven- tricular tachycardias (Figs. 2 to 4) are similar to those of its parent compound. NAPA is thus of clinical use in selected groups of patients with ventricular dysrhythmias.
We thank Ms. Lynn Whittier for excellent secretarial assis- tance and preparation of this manuscript. The study was support- ed by the American Critical Care, McGaw Park, Illinois.
REFERENCES
I.
2.
3 <.
4.
fi.
Dreyfuss J, Ross JJ Jr, Schreiber EC: Absorption, excretion, and biotransformation of procainamide-Cn in the dog and rhesus monkey. Arzneim Forsch 21:948, 1971. Dreyfuss J, Bigger JT Jr, Cohen AI, Schreiber EC: Metabo- lism of procainamide in rhesus monkey and man. Clin Pharmacol Ther 13:366, 1972. Elson J, Strong JM, Lee WK, Atkinson AJ Jr: Antiarrhyth- mic potency of N-acetylprocainamide. Clin Pharmacol Ther 17:134, 1975. Bagwell EE, Walle T, Drayer DE, Reidenberg MM, Pruett JK: Correlation of the electrophysiological and antiarrhyth- mic properties of the N-acetyl metabolite of procainamide with plasma and tissue drug concentrations in the dog. J Pharmacol Exp Ther 197:38, 1976. Refsum H, Frislid K, Lunde PKM, Landmark KH: Effects of
6
7
8
9.
IO
11.
12
13
14.
15.
16
17.
18.
19.
20.
21.
22.
23.
24.
May. 1983
American Heart Journal
N-acetylprocainamide as compared with procainamide 11~ isolated rat atria. Eur J Pharmacol 33:47, ! 975. Minchin RF, Llett KF, E’att,erson ~JW: Antiarrhvthmrc poten cy of procainamide and N-acrtvlprocainamide in rnhhits. l&r J Pharmacol 47:51, 197X. Jaillon P, Winkle RA: Electrophysiologic comparative study of procainamide and N-acetylprocainamide in anest,hetized dogs: Concentration-response relationships (“irclilatitrn 60:1385, 1979. Atkinson AJ, 1,ee WL. Quinn MI,, Kushner W. Kevin M.J. Strong ,JM: Dose-ranging trial of A’-acetylprocainamide in patients with premature ventricular contractions. Clin Phar- macol Ther 2 1:595. 1977. Kluger .I, Drayer D, Reidenberg M, Ellis G, Lloyd V. Tyberg T, Hayes .I: The clinical pharmacology and antiarrhythmic efficacy of acetylprocainamide in patients with arrhythmias. Am .J Cardiol 45:1250, 1980. Scherlag BJ, Lau SH, Helfant RH. Berkowitz WD, Stein E, Damato AN: Catheter technique for recording His bundle activity in man. Circulation 39:13, 1969. Sung RJ, Castellanos A. Mallon SM, Gelband H, Mendoza 1. Myerburg RJ: Mode of initiation of reciprocating tachycardia during programmed ventricular stimulation in the Wolff- Parkinson-White syndrome: With reference to various pat- terns of ventriculo-atria1 conduction. Am .I Cardiol 40:24. 1977. Wit AL, Weiss MB, Berkowitz WD, Rosen KM, Sterner C. Damato AN: Patterns of atrioventricular conduction in the human heart, Circ Res 27:345, 1970. Rocco RM, Ahhott DC, Giese RW, Karger BL: Analysis for procainamide and N-acetylprocainamide in plasma or serum by high performance liquid chromatography. Clin Chem 23:705. 1977. Akhtar M, Damato AN, Batsford WP, Ruskin JN, Ogunkelu .JB, Vargas G: Demonstration of reentry within the His- Purkinje system in man. Circulation 50:1150. 1971. Josephson ME, Caracta AR, Riccuitti MA, Lau SH, Damato AN: Electrophysiologic properties of procainamide in man. Am .J Cardiol 33:597. 1974. Scheinman MM, Weiss AN, Shafton E, Benowitz N, Rowland M: Electrophysiologic effects of procainamide in patients with intraventricular conduction delay. Circulation 49~522, 1974. Ogunkelu JB, llamato AN, Akhtar M, Reddy CP. Caracta AR. Lau SH: Electrophysiologic effects of procainamide in subtherapeutic to therapeutic doses on human atrioventricu- tar conduction system. Am .J Cardiol 37:724, 1976. Kastor ,JA, -Josephson ME, Guss SB, Horowitz LN: Human ventricular refractoriness. II. Effects of procainamide. Circu- lation 56:462. 1977. Camardo .JS, Greenspan AM, Horowitz LN, Spielman SR, ?Josephson ME: Strength-interval relation in the human ventricle: Effett. of procainamide. Am ,J Cardiol 45:856, 1980. Giardina EG, Bigger JT <Jr: Procaine amide against reentrant ventricular arrhythmias: Lengthening of R-V intervals of coupled ventricular premature depolarizations as an insight into the mechanism of action of procaine amide. Circulation 48:959. 1973. Reddy CP, Damato AN, Akhtar M, Dhatt M, Games JA, Calon T: Effect of procainamide on reentry within the His-Purkinje system in man. Am J Cardiol 40:957, 1977. Reddy CP. Lvnch M: Abolition and modification of reentry within the His-Purkinje system by procainamide in man. Circulation 58:1010, 1978. Wellens HJJ, Bar FWHM, Lie KI, Duren DR, Dohmen HJ: Effect of procainamide, propranolol and verapamil on mech- anism of tachycardia in patients with chronic recurrent ventricular tachycardia. Am J Cardiol 40:579, 1977. Horowitz LN, dosephson ME, Farshidi A, Spielman SR. Michelson El,. Greenspan AM: Recurrent sustained ventric-

Volume 105
Number 5 Antiarrhythmic mechanisms of N-acetylprocainamide 819
ular tachycardia. 3. Role of the electrophysiologic study in selection of antiarrhythmic regimens. Circulation 58:986, 1978.
25. Engel TR, Meister SG, Luck JC: Modification of ventricular tachycardia by procainamide in patients with coronary artery disease. Am J Cardiol 46:1033, 1980.
26. Jaillon P, Rubenson D, Peters F, Mason J, Winkle RA:
Electrophysiologic effects of N-acetylprocainamide in human beings. Am J Cardiol47:1134, 1981.
27. Amlie JP, Nes,je OA, Frislid K, Lunde PKM, Landmark KH: Serum levels and electrophysiological effects of N-acetylpro- cainamide as compared with procainamide in the dog heart in situ. Acta Pharmacol Toxic01 42:280, 1978.
BOUND VOLUMES AVAILABLE TO SUBSCRIBERS
Bound volumes of the AMERICAN HEART JOURNAL are available to subscribers (only) for the 1983 issues from the
Publisher at a cost of $42.00 ($53.00 international) for Vol. 105 (January-June) and Vol. 106 (July-December). Shipping charges are included. Each bound volume contains a subject and author index and all advertising is removed. Copies are shipped within 30 days after publication of the last issue in the volume. The binding is durable buckram with the journal name, volume number, and year stamped in gold on the spine. Payment must accompany all orders. Contact Mr. Deans Lynch at The C. V. Mosby Company, 11830 Westline Industrial Drive, St. Louis, Missouri 63141, USA.
Subscriptions must be in force to qualify. Bound volumes are not available in place of a regular Journal subscription.




















