
Epicardial and thoracic fat - Noninvasive measurement and clinical implications
Upload
independentCategory
view
0download
0
NH
DA*PH
BwipgcMotBpgSlwgdaTa2bgfrpnatgcA
Hpdcggt
CLINICAL GASTROENTEROLOGY AND HEPATOLOGY 2006;4:306–314
oninvasive Versus Histologic Detection of Gastric Atrophy in aispanic Population in North America
AVID Y. GRAHAM,* ZHANNAT Z. NURGALIEVA,* HALA M.T. EL-ZIMAITY,* ANTONE R. OPEKUN,*RMANDO CAMPOS,‡ LEONCIO GUERRERO,‡ ALFREDO CHAVEZ,‡ and VICTOR CARDENAS§
Department of Medicine, Veterans Affairs Medical Center, and Baylor College of Medicine, Houston, Texas; §University of Texas School ofublic Health, Division of Epidemiology, El Paso Regional Campus, El Paso, Texas; and ‡Mexican Institute for Social Security, General
ospital for Region 6, Ciudad Juarez, Chihuahua, Mexicohcwtiwp
tilppTsstiiPwlio
itaptpm
cCu
ackground & Aims: Cancer risk is directly correlatedith the severity and extent of mucosal atrophy, making
dentification of atrophy a goal in cancer preventionrograms. The aim of this study was to compare tar-eted histology with noninvasive testing for the identifi-ation of antral and/or corpus atrophy in North America.ethods: In a cross-sectional study of a random samplef households, 8 gastric biopsy specimens were ob-ained from defined locations in the antrum and corpus.iopsies were scored for the presence of Helicobacterylori and gastric atrophy (defined as loss of normallandular components). Atrophy was scored by using theydney system and a system based on the number and
ocation of corpus biopsies with atrophy. Patients’ seraere examined for pepsinogen I, pepsinogen II, andastrin-17 (fasting and stimulated). Results: One hun-red eighty volunteers, approximately 30 per age groupnd ranging in age from 18–82 years, participated.here were 76 men. The overall weighted prevalence ofcorpus atrophy was 4.7% (95% confidence interval,
.3–7.0). There was a significant inverse relationshipetween the grade of corpus atrophy and the pepsino-en I/pepsinogen II ratio (R � �0.31, P < .01). Weailed to confirm the usefulness of the proposed algo-ithm by using gastrin-17, H pylori serology, and serumepsinogens to categorize the gastric histology. The Syd-ey system underestimated the prevalence of corpustrophy by approximately 25%. Conclusion: Noninvasiveesting is both possible and practical by using pepsino-en assays for the identification of the precancerousondition of moderate to severe corpus atrophy in Northmerican Hispanic patients.
elicobacter pylori infection causes inflammation of thegastric mucosa, which might progress to gastric atro-
hy with intestinal metaplasia and in some patients toysplasia (intraepithelial neoplasia) and to gastric adenocar-inoma. The incidence of gastric cancer varies in differenteographic areas and is linked to the prevalence of atrophicastritis.1,2 Gastric cancer is a major problem in Japan, such
hat population-based gastric cancer prevention programsave been instituted3 with the goal of identifying gastricancer before it becomes incurable. The initial approachas to perform radiographic screening with barium meal
o examine large segments of the population. Individualsn whom radiographic abnormalities were discoveredould be referred for endoscopic examination and appro-riate therapy.More recently, noninvasive techniques have been used
o enrich the proportion of cases undergoing endoscopyn whom cancer is found.4–9 Noninvasive testing isargely based on changes in serum concentrations ofepsinogens, which are the precursor proteins for theroteolytic enzymes, pepsins, produced by the stomach.he 2 major pepsinogens, pepsinogen I (PGI) and pep-
inogen II (PGII), are produced in different regions of thetomach, such that measuring their respective levels canheoretically provide information about the functionalntegrity of the gastric antrum and corpus mucosa. PGIs produced exclusively in the oxyntic mucosa, whereasGII is produced in the gastric antrum and corpus asell as the duodenum. A low serum PGI level and/or a
ow PGI level in relation to PGII level (PGI:PGII ratio)s indicative of the presence of atrophy or severe gastritisf the gastric corpus.10 –12
Gastrin is produced by G cells in the gastric antrum, andts release is finely regulated by intraluminal contents, par-icularly the presence of protein-containing food, and bycidity. Gastrin is released in response to a rise in luminalH and is suppressed as the pH falls below 3. The regula-ion of gastrin release is perturbed in the presence of an Hylori infection, resulting in mild elevations of fasting andeal-stimulated gastrin levels and an impaired response to
Abbreviations used in this paper: ANOVA, analysis of variance; CI,onfidence interval; EIA, enzyme immunoassay; G-17, gastrin-17; HM-AP, high molecular weight cell-associated protein; IgG, immunoglob-lin G; PGI, pepsinogen I; PGII, pepsinogen II.© 2006 by the American Gastroenterological Association Institute
1542-3565/06/$32.00
PII: 10.1053/S1542-3565(05)01091-8
ptdmmbrAHGGpbssamaiap
HpmPHaHtpa
iwfmsfiubhwic(1tt
osmt
wcfleoabfcmHh
satmatTi
wbttI
Fr
March 2006 NONINVASIVE DIAGNOSIS OF GASTRIC ATROPHY 307
H-related regulation of gastrin release. 13–15 Changes inhe serum gastrin-17 (G-17) concentrations also have pre-ictive value in relation to the functional status of the antralucosa. For example, a low serum G-17 concentrationight result from physiologic suppression of gastrin release
y highly acidic stomach contents or loss of G cells as aesult of moderate or severe atrophy of the antral mucosa.n exaggerated meal-stimulated gastrin is associated with pylori–induced antral inflammation.15 Very high levels of-17 typically reflect the physiologic response of the antralcells to markedly reduced acid production as is found in
ernicious anemia with severe corpus atrophy, achlorhydria,ut normal antral mucosa. Thus theoretically, assessment oferum pepsinogens, H pylori status, and the level of G-17hould provide an overview of the functional status of thentral and corpus mucosa. For example, in pernicious ane-ia one expects a marked elevation in serum G-17 levels
nd low serum PGI levels and a low PGI:PGII ratio reflect-ng corpus atrophy. In contrast, a low serum PGI level andlow PGI:PGII ratio and a low G-17 would suggest theresence of antral and corpus atrophy.
Recently, a panel of 4 tests (Gastropanel; Biohit Plc,elsinki, Finland) has been introduced with the goal of
roviding information regarding the status of the gastricucosa. The panel consists of assays of the levels of serumGI, serum PGII, PGI:PGII ratio, serum G-17 levels, andpylori immunoglobulin G (IgG) antibodies. An associated
lgorithm combines the results of gastrin, pepsinogen, andpylori tests to suggest a likely diagnosis. We examined
he utility of this combination of tests in a North Americanopulation with a high prevalence of H pylori infection andn increased risk of gastric cancer.
MethodsStudy Design
The study was done in Ciudad Juarez, Mexico, whichs on the US-Mexico border contiguous to El Paso, Texas. Thisas a cross-sectional study in which volunteers were recruited
rom a random sample of households selected by means of aultistage cluster, self-weighted design. The survey was de-
igned to be self-weighted and stratified by age and sex. In therst stage, census tracts were selected (ie, primary samplingnit) with probability proportional to their size. In the second,locks were selected by using simple random sampling. Allouseholds within selected blocks were listed, and householdsere selected by using systematic random sampling. Finally,
ndividuals were listed by age and invited to participate ac-ording to specific age-strata recruitment goals: 36 subjects18 men and 18 women) in each of the following age groups:8–29, 30–39, 40–49, 50–59, and 60 and more years of age,o oversample the older high-risk population and compare
hem with equal numbers of persons in younger age strata and Hptimize the statistical testing of the study hypothesis. Theampling sites were obtained by using an updated digital cityap obtained from the (Mexican) National Institute of Statis-
ics, Geography and Informatics.
Study Population
The adult population consisted of both men andomen age 18 years or older. Exclusion criteria included
ontraindications for endoscopy such as recent myocardial in-arction, severe respiratory impairment, or severe cardiovascu-ar disease. Also excluded were patients with an incompletendoscopic examination, those with endoscopy performed forther than diagnostic reasons, patients whose endoscopic ex-mination was done as an “emergency examination” as forleeding, and patients whose treatment required immediateollow-up treatment. Those who were allergic to egg, soy,ereals, chocolate, or milk products were also excluded. Alledicines that might affect gastric acid secretion, such as
2-receptor antagonists or proton pump inhibitors, were pro-ibited for at least 1 week before any part of the study.After obtaining written informed consent, a face-to-face
tructured interview was completed at the time of the initialppointment. The interviewer collected demographic informa-ion, as well as information regarding previous medical treat-ents for dyspepsia, including proton pump inhibitors and
ntibiotics for H pylori eradication. The study was approved byhe institutional review boards at Baylor College of Medicine,he University of Texas Health Science Center, and the Mex-
can Institute for Social Security.
Endoscopy
Experienced gastroenterologists received training asell as endoscopic photographs and a map (similar to Figure 1ut in color) showing the biopsy sites. Copies were posted inhe endoscopy units. Endoscopic procedures were performed athe endoscopic facility of the main hospital of the Mexicannstitute for Social Security or at a private practice at the
igure 1. The biopsy sites are shown both in a diagram and asepresentative endoscopic pictures.
ospital Guernika in Ciudad Juárez. Gastric mucosal biopsy

scttscasccuTflfM
mptwGafItnicsaw
moevge
rbabrBsmrasa
sfpbawT
oggbganof01mmisac
l1fm(mwp
u(u(riwwt
ugTmmnu
308 GRAHAM ET AL CLINICAL GASTROENTEROLOGY AND HEPATOLOGY Vol. 4, No. 3
pecimens were collected by using large biopsy forceps (Mi-roVasive Radial Jaw without needle, 2.2-mm diameter; Bos-on Scientific, Natick, MA). Four biopsies were collected fromhe antrum and 4 from the corpus (Figure 1). Biopsies werepecifically identified with respect to site, such that the resultsould be specifically related to the site. Site A3 was the gastricngle; B2 was taken approximately 2–4 cm proximal to thetart of the first fold on the greater curve of the stomach (distalorpus). Two biopsies (1 antral and 1 corpus) were taken forulture separately, and 1 antral biopsy was taken for rapidrease testing (Hpfast; Chek-Med Systems, Camp Hill, PA).he biopsies for histology were formalin-fixed in 10% neutral
ormalin. The biopsies for H pylori culture were placed inabeled tubes containing transport media and immediatelyrozen at �70°C until shipment to the laboratories at the VA
edical Center in Houston.
Histology
Each specimen was placed in a separate bottle of for-alin labeled as to site on the gastric map. Samples were
rocessed at the Gastrointestinal Mucosal Pathology Labora-ory in Houston, Texas, where they were embedded in paraffinax and cut at 4 �m, and serial sections were stained with theenta triple strain. Each specimen was scored by using a visual
nalog scale from 0 (absent/normal) to 5 (maximal intensity)or H pylori, active inflammation, and intestinal metaplasia.16
n addition, the type of epithelium (antral, oxyntic, transi-ional) was also recorded. Atrophy was defined as the loss oformal glands with and without its replacement with fibrosis,ntestinal metaplasia, and/or pseudopyloric metaplasia (alsoalled pyloric metaplasia or mucus metaplasia). There is con-iderable interobserver variability in scoring antral atrophy,nd to reduce that variability, areas with lymphoid folliclesere excluded from the analysis for atrophy.17
The presence of pseudopyloric metaplasia was defined asucosa that was phenotypically antral but was anatomically
btained from a region in which corpus mucosa would bexpected. In addition, in all cases the final arbitrator of antralersus pseudopyloric was made on the basis of the presence oflands that stained positively for PGI, a marker for corpuspithelium as previously described.18
Scoring of Atrophy
Corpus atrophy was scored 2 ways, according to theecommendations of the updated Sydney system with the 5iopsies recommended (A1, A3, A4, B4, and B6) (Figure 1)nd by a system based on the number and location of corpusiopsies with atrophy (the Houston system) and designed toecord the extent of pyloro-corporal advancement of atrophy.19
ecause the sites recommended for biopsy with the Sydneyystem would theoretically systematically not sample atrophicucosa that had not yet extended sufficiently to involve the
ecommended proximal sites (ie, B4 and B6; Figure 1),19 wedded a site (B5) between the gastric angle and the Sydneyystem proximal site (B4) and one (B2) between the antrum
nd the Sydney system proximal site (B6) (Figure 1). The B2 mite was approximately 4 cm proximal to the end of the corpusolds. The B5 site was intended to be located at least 3–4 cmroximal to the gastric angle and thus to provide a siteetween the site recommended by the Sydney system and thentrum. Unfortunately, the majority (�90%) of the specimensere taken close to the angle and were anatomically antral.hat site was therefore excluded from all analyses.The Houston system was based on the fact that the degree
f damage is initially more severe in the non–acid-secretingastric antrum, but over time the damage progresses into theastric corpus. This can be visualized as an advancing atrophicorder that involves the lesser curvature more rapidly than thereater curvature.20 –22 As parietal and chief cells in the corpusre replaced by mucus cells, the mucosal biopsy appears phe-otypically like antral mucosa and is called mucus metaplasiar pseudopyloric metaplasia.17,18 The Houston system there-ore scored the stage of atrophy on a 4-point scale ranging from� none to 3 � severe, with 0 � atrophy at no corpus site,� mild or atrophy only at the lesser curve site (B4), 2 �oderate or atrophy at the distal corpus site (B2) and involve-ent of the lesser curve site B4, and 3 � severe atrophy and
ncluded the proximal greater curve site (B6) (see Figure 1 forites). As predicted by the concept of atrophy occurring as andvancing front, all with involvement of the proximal greaterurve site, B6, also had involvement of the distal site, B2.20 –24
Pepsinogen and Gastrin-17 BloodCollection
A fasting sample (6–8 mL) of venous blood was col-ected without preservatives into plastic tubes (Venoject VP-00 SP; Terumo Somerset, NJ), which was placed into ice bathor coagulation. A food-stimulated blood sample was taken 20inutes after a protein drink that contained 10 g of protein
Biohit Plc) was given with 100 mL of water according to theanufacturer’s directions. Fasting and meal-stimulated seraere stored at �70°C until assay in Houston by using the kitsrovided by the manufacturer (Biohit).Evaluation of anti–H pylori IgG antibodies was done by
sing the H pylori IgG enzyme immunoassay (EIA) test kitBiohit Inc) and a kit for IgG antibody to the high molec-lar weight cell-associated proteins (HM-CAPs) of H pyloriSCANLISA H pylori HM-CAP IgG Assay; Scimedx Corpo-ation, Denville, NJ). The results were interpreted accord-ng to the manufacturer’s instructions. H pylori infectionas defined as a positive EIA result. The H pylori antibodiesere expressed according to the formulas included in the
est kits.Levels of serum G-17, PGI, and PGII were determined by
sing specific EIA tests (Gastrin-17 EIA Test Kit, Pepsino-en-I EIA Test Kit, and Pepsinogen-II EIA Test Kit; Biohit).ests were performed on a microwell plate according to theanufacturer’s instructions. All EIA techniques were based oneasuring the absorbance after a peroxidation reaction at 450
m. Between the reaction steps, the plates were washed bysing ELx405 Automated Plate Washer (BIO-TEK Instru-
ents Inc, Winooski, VT). The absorbance was measured by
uSdolh
Hphb
cvaapu8SuujtdCtamwaa
swbccswwow
fT
dasi
pawlo[wwyege(otfpp6�n
saa1i
Fa
March 2006 NONINVASIVE DIAGNOSIS OF GASTRIC ATROPHY 309
sing a microwell plate reader Microplate Spectrophotometerpectra Max 190 (Molecular Devices, Sunnyvale, CA). Foretermination of serum PGI and G-17 values, second-order fitsn standard concentrations were used to interpolate/extrapo-ate unknown sample concentrations automatically with theelp of the BP800 built-in software.
Helicobacter pylori Status
H pylori infection was defined as a positive culture forpylori or a positive histology and rapid urease tests. A
resumed positive was defined as culture negative but positiveistology with a score of 2 or greater in at least 2 separateiopsies (n � 2).
Statistical Analyses
The goal was to test the performance of the assays inlassifying corpus atrophic gastritis in approximately 36 indi-iduals in each of the age strata. At the same time, the studyllowed us to describe the prevalence of atrophic gastritisccording to age, gender, and other risk factors including Hylori infection. Prevalence estimates for the study populationsed weighted analyses using SAS-callable SUDAAN (version.1; Research Triangle Institute, Research Triangle Park, NC).ampling weights, ie, the number of individuals in the pop-lation that each study subject represents, were calculated bysing the probability of selection of each individual and ad-usting for nonresponse. Sampling weights were used only inhis report to estimate overall prevalence figures. Analyses wereone with Stata Software (Stata Release 8; Stata Corporation,ollege Station, TX). The unpaired Student t tests were used
o compare the means of PGI:PGII ratios and grade of corpustrophy. Fisher exact probability test was used from nonpara-etric tests to test 2 independent samples when small samplesere compared. The relation between pepsinogen values and
trophy scores was evaluated by using 1-way analysis of vari-nce (ANOVA) and Kruskal-Wallis 1-way ANOVA on ranks.
The classification of the study participants according to thetatus of their gastric mucosa by histology (ie, gold standard)as also compared with the classification of atrophy on theasis of the tests in the Biohit panel. To that end, data wereross-tabulated, and �2 or Fisher exact tests were used toompare the proportions classified by the different tests. Sen-itivity, specificity, and predictive value of a positive test resultere evaluated by using standard definitions, and sensitivitiesere plotted against 1-specificities of the test (ie, receiver-perator characteristic curves), and the area under the curveas computed by using STATA.
ResultsStudy Population Demographics andPrevalence of Helicobacter pylori Infection
A total of 180 adult volunteers ranging in agerom 17–82 years participated, 76 men and 104 women.
he overall seropositivity rate of H pylori infection as fefined above was 76%, increasing from 55.2% in thege 17–29 group to 90.3% at ages 50–59. There was noignificant difference in the overall prevalence of H pylorinfection between men and women (78.4% vs 74.5%).
Prevalence of Gastric Atrophy
Adequate biopsy specimens to assess corpus atro-hy were available from 178 subjects, and data for antraltrophy were available on 179 subjects. Corpus atrophyas found in 16 (9%) of the study subjects. The preva-
ence of a corpus atrophy weighted for oversampling oflder individuals was 4.7% (95% confidence intervalCI], 2.3–7.0), (n � 178); 62% of the patients wereomen. The mean age for women with corpus atrophyas 52.1 � 11.5 years, and for men it was 63.5 � 9.9ears (P � .06). With unweighted analyses, no differ-nces were found in the prevalence of corpus atrophy byender: prevalence ratio, 1.1; 95% CI, 0.7–1.6. How-ver, corpus atrophy increased significantly with ageFigure 2), from none among those younger than 30 yearsf age to 2.6%, 11.6%, 9.7%, and 19.4% for those inheir 30s, 40s, 50s, and 60s or more, respectively (�2 testor linear trend, P � .004). The overall unweightedrevalence of corpus atrophy among those with active Hylori infections was 9.6% (n � 135) compared with.9% among those without an active H pylori infection (n
43). However, the CI of this difference included theull value (prevalence ratio, 1.4; 95% CI, 0.4–4.6).Antral atrophy was found in 47 (26.3%) of the study
ubjects (n � 179). The overall prevalence of antraltrophy was 19.6% (95% CI, 13.1–26.1). Unweightednalyses showed that antral atrophy increased from3.8% in the age group 17–29 years and reached 52.6%n the oldest age group. No differences by gender were
igure 2. The age-weighted increase in gastric antral and corpustrophy is shown.
ound, but antral atrophy was present in 30.9% of those
w1(
Bamtttmcsa(
pHH(an
okswpsh
c
IreaHtEk
fiarwv
P3sawo9
slap
F
T
H
B
A
310 GRAHAM ET AL CLINICAL GASTROENTEROLOGY AND HEPATOLOGY Vol. 4, No. 3
ith active H pylori infections (n � 136) compared with1.6% (n � 43) of those without active H pylori infectionprevalence ratio, 2.6; 95% CI, 1.1–6.3).
Comparison of Sydney and HoustonGrading Systems for Atrophy
The intention was to take a gastric biopsy at site5, which was at least 3–4 cm proximal to the gastricngle, and thus provide a site between the site recom-ended by the Sydney system and the antrum. Unfor-
unately, the majority of the specimens were taken closeo the angle and were anatomically antral, as shown byhe absence of staining for PGI, the marker for corpusucosa. This site was therefore excluded from the cal-
ulations, thus basing the comparison of the “Houstonystem” and the Sydney system on the outcome by usingn additional site on the greater curve that is more distalB2) than the Sydney site curve site (B6).
The Sydney system underestimated prevalence of cor-us atrophy by approximately 25% compared with theouston system (ie, 12.3% vs 16.2% for the Sydney andouston systems, respectively). The results were similar
24%) when the analyses were restricted to those withctive H pylori infections (14.1% vs 18.5% for the Syd-ey and Houston systems, respectively).
Helicobacter pylori Serology
Sixteen subjects were excluded from the analysisf the seroprevalence of H pylori infection with the Biohitit because a serum sample was not collected for 1ubject, and 15 had indeterminate results. Twenty-oneere dropped from the analysis of the seroprevalence of H
ylori infection with H pylori HM-CAP IgG assay. Aerum sample was not collected from 1 subject, and 20ad indeterminate results.The overall seroprevalence of H pylori infection was
able 1. H pylori Infection Serology as Detected by HM-CAPEIA and Hp IgG EIA According to Biopsy-BasedDiagnosis in Residents of Ciudad Juarez, Mexico,2004
Hp status
Positive Negative
M-CAPPositive 99 (93.4%) 1Negative 7 38 (97.4%)
iohitPositive 84 (79.2%) 1Negative 22 38 (97.4%)
bbreviation: Hp, H pylori.
omparable by using either the HM-CAP or the H pylori s
gG EIA test kit (74.8%, n � 159, and 74.4%, n � 164,espectively) (Table 1). The anti–H pylori ELISAs werevaluated against the gold standard for H pylori positivitys defined above. The sensitivity and specificity for theM-CAP IgG test were 93% and 97% as compared with
he gold standard, whereas these figures for the BiohitIA were 79% and 97%, respectively. Thus the Biohitit had a larger yield of false-negative results (Table 1).
Serum Pepsinogen I and II andHelicobacter pylori Infection
Serum samples from 179 subjects were availableor testing. The serum PGI levels in H pylori–infectedndividuals were higher than among those without anctive H pylori infection (125.5 � 59 vs 69.6 � 26.4,espectively) (P � .01). Similarly, the serum PGII levelsere higher in those with H pylori infection (17.3 � 11s 6.7 � 3, respectively) (P � .01).
Serum Pepsinogen I and II and CorpusAtrophy
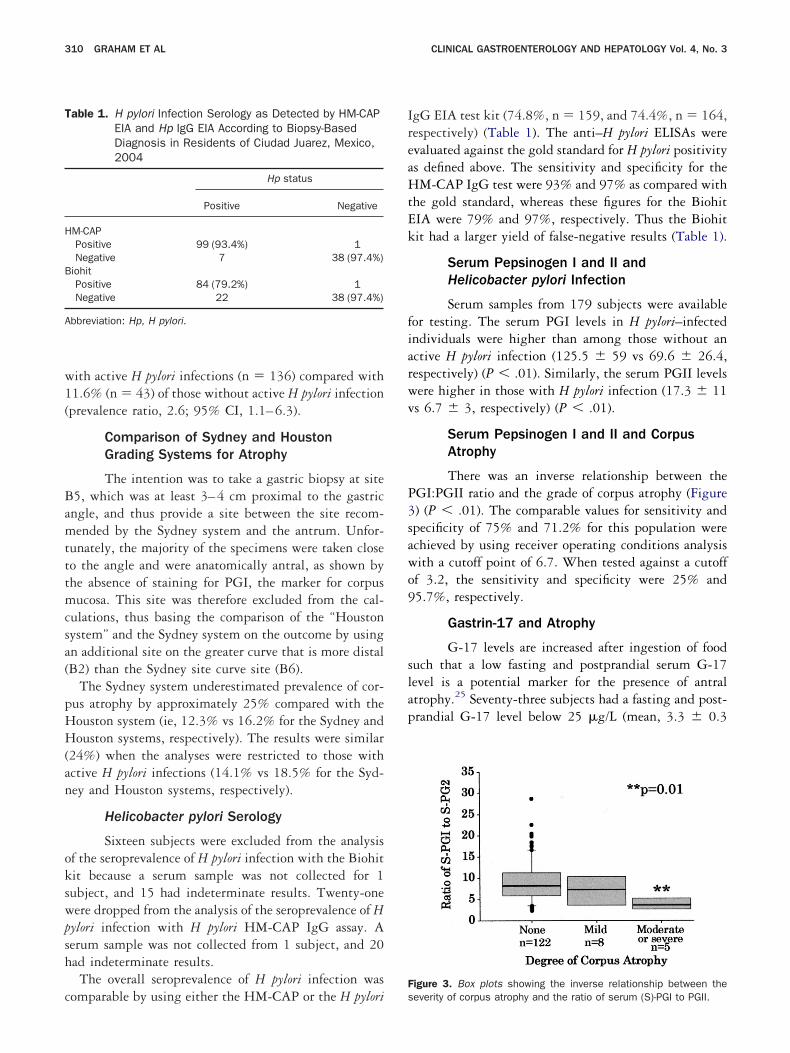
There was an inverse relationship between theGI:PGII ratio and the grade of corpus atrophy (Figure) (P � .01). The comparable values for sensitivity andpecificity of 75% and 71.2% for this population werechieved by using receiver operating conditions analysisith a cutoff point of 6.7. When tested against a cutofff 3.2, the sensitivity and specificity were 25% and5.7%, respectively.
Gastrin-17 and Atrophy
G-17 levels are increased after ingestion of fooduch that a low fasting and postprandial serum G-17evel is a potential marker for the presence of antraltrophy.25 Seventy-three subjects had a fasting and post-randial G-17 level below 25 �g/L (mean, 3.3 � 0.3
igure 3. Box plots showing the inverse relationship between the
everity of corpus atrophy and the ratio of serum (S)-PGI to PGII.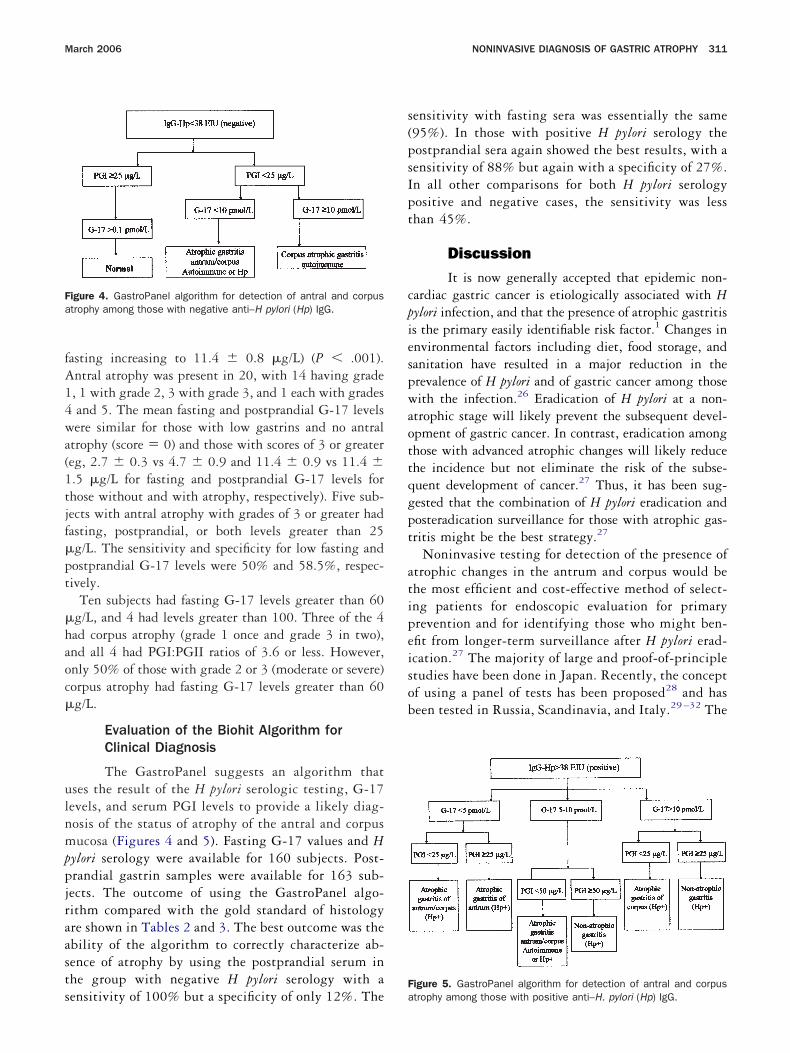
fA14wa(1tjf�pt
�haoc�
ulnmppjraasts
s(psIpt
cpiespwaottqgpt
atipeisob
Fa
F
March 2006 NONINVASIVE DIAGNOSIS OF GASTRIC ATROPHY 311
asting increasing to 11.4 � 0.8 �g/L) (P � .001).ntral atrophy was present in 20, with 14 having grade, 1 with grade 2, 3 with grade 3, and 1 each with gradesand 5. The mean fasting and postprandial G-17 levelsere similar for those with low gastrins and no antral
trophy (score � 0) and those with scores of 3 or greatereg, 2.7 � 0.3 vs 4.7 � 0.9 and 11.4 � 0.9 vs 11.4 �.5 �g/L for fasting and postprandial G-17 levels forhose without and with atrophy, respectively). Five sub-ects with antral atrophy with grades of 3 or greater hadasting, postprandial, or both levels greater than 25g/L. The sensitivity and specificity for low fasting andostprandial G-17 levels were 50% and 58.5%, respec-ively.
Ten subjects had fasting G-17 levels greater than 60g/L, and 4 had levels greater than 100. Three of the 4ad corpus atrophy (grade 1 once and grade 3 in two),nd all 4 had PGI:PGII ratios of 3.6 or less. However,nly 50% of those with grade 2 or 3 (moderate or severe)orpus atrophy had fasting G-17 levels greater than 60g/L.
Evaluation of the Biohit Algorithm forClinical Diagnosis
The GastroPanel suggests an algorithm thatses the result of the H pylori serologic testing, G-17evels, and serum PGI levels to provide a likely diag-osis of the status of atrophy of the antral and corpusucosa (Figures 4 and 5 ). Fasting G-17 values and H
ylori serology were available for 160 subjects. Post-randial gastrin samples were available for 163 sub-ects. The outcome of using the GastroPanel algo-ithm compared with the gold standard of histologyre shown in Tables 2 and 3 . The best outcome was thebility of the algorithm to correctly characterize ab-ence of atrophy by using the postprandial serum inhe group with negative H pylori serology with a
igure 4. GastroPanel algorithm for detection of antral and corpustrophy among those with negative anti–H pylori (Hp) IgG.
ensitivity of 100% but a specificity of only 12%. The a
ensitivity with fasting sera was essentially the same95%). In those with positive H pylori serology theostprandial sera again showed the best results, with aensitivity of 88% but again with a specificity of 27%.n all other comparisons for both H pylori serologyositive and negative cases, the sensitivity was lesshan 45%.
DiscussionIt is now generally accepted that epidemic non-
ardiac gastric cancer is etiologically associated with Hylori infection, and that the presence of atrophic gastritiss the primary easily identifiable risk factor.1 Changes innvironmental factors including diet, food storage, andanitation have resulted in a major reduction in therevalence of H pylori and of gastric cancer among thoseith the infection.26 Eradication of H pylori at a non-
trophic stage will likely prevent the subsequent devel-pment of gastric cancer. In contrast, eradication amonghose with advanced atrophic changes will likely reducehe incidence but not eliminate the risk of the subse-uent development of cancer.27 Thus, it has been sug-ested that the combination of H pylori eradication andosteradication surveillance for those with atrophic gas-ritis might be the best strategy.27
Noninvasive testing for detection of the presence oftrophic changes in the antrum and corpus would behe most efficient and cost-effective method of select-ng patients for endoscopic evaluation for primaryrevention and for identifying those who might ben-fit from longer-term surveillance after H pylori erad-cation.27 The majority of large and proof-of-principletudies have been done in Japan. Recently, the conceptf using a panel of tests has been proposed28 and haseen tested in Russia, Scandinavia, and Italy.29 –32 The
igure 5. GastroPanel algorithm for detection of antral and corpus
trophy among those with positive anti–H. pylori (Hp) IgG.
HgcihJ
sadaa
tlrhst
fttghtGaGworbnsa
em
T
D
D
A FN,
T
N(A
(C
(
A
312 GRAHAM ET AL CLINICAL GASTROENTEROLOGY AND HEPATOLOGY Vol. 4, No. 3
ispanic population in North America is a high-riskroup for development of gastric cancer, with gastricancer being the second leading cause of cancer deathsn Mexico in 2003 (http://www.salud.gob.mx/apps/tdocs/estadisticas/mortalidad/mortalidad.htm, accesseduly 22, 2005).
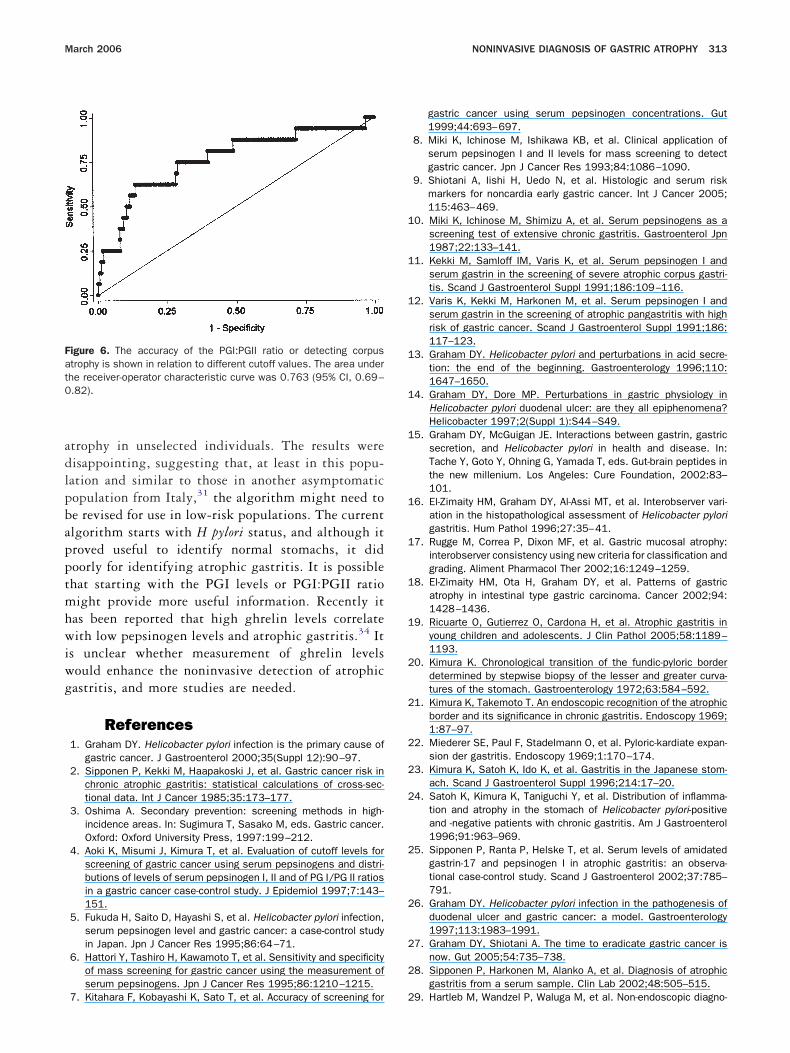
Our study confirmed that a low ratio of serum PGI:erum PGII was indicative of moderate or severe corpustrophy, and a ratio below 6.5 was able to accuratelyiagnose 76% (95% CI, 69%–82%) of patients withtrophic corpus gastritis (Figure 6). Larger scale studiesre needed to better refine the best cutoff values.
The place for G-17 testing in relation to evaluatinghe status of the gastric mucosa remains unclear. G-17evels are increased in H pylori infections but typicallyemain within the normal range unless antral atrophyas occurred.15 A high G-17 level implies low acidecretion, which in the absence of anti-secretory drugherapy implies corpus atrophy. The presence of a low
able 2. GastroPanel Algorithm Using Sera That Were H pylo
iagnosis Hp negativeNo atrophy (fasting)(fed)Atrophic gastritis, corpus or antrum, autoimmune or Hp (fasting)(fed)Corpus atrophic gastritis autoimmune (fasting)(fed)
iagnosis: Hp positiveAtrophic gastritis, corpus or antrum, Hp (fasting)(fed)Antrum atrophy (fasting)(fed)Atrophic gastritis, corpus or antrum, autoimmune or Hp (fasting)(fed)Non atrophic gastritis (Hp�) (fasting)(fed)Atrophic gastritis corpus (Hp�) (fasting)(fed)Non atrophic gastritis (Hp�) (fasting)(fed)
bbreviations: TP, true positive; TN, true negative; FP, false positive;
able 3. GastroPanel Algorithm Using All Sera With the Outco
Diagnosis: Hp positive or negative Histology Panel
o atrophy (fasting) 111 150fed) 114 159trophic gastritis, corpus or antrum,autoimmune or Hp (fasting)
47 0
fed) 47 0orpus atrophic gastritisautoimmune (fasting)
14 2
fed) 14 2
bbreviations: Hp, H pylori; TP, true positive; TN, true negative; FP, false
asting and a normal postprandial G-17 level ishought to reflect acid-associated suppression of gas-rin release. In contrast, a low fasting and postprandialastrin level is postulated to reflect antral atrophy;owever, in this study it had a relatively low sensi-ivity and specificity for antral atrophy. High fasting-17 levels were restricted to those with severe corpus
trophy. The presence of a low pepsinogen and high-17 level has been suggested as a marker for thoseith severe atrophic gastritis and a high risk of havingr developing gastric cancer.11,33 This hypothesis hasecently been confirmed in a study in which the com-ination of serum pepsinogen testing (eg, PGI � 45g/mL and serum G-17 � 60 pg/mL) gave the bestensitivity and specificity for identifying cancermong high-risk patients. 9
We tested the proposed GastroPanel algorithm tovaluate whether it would provide an accurate esti-ate of the presence or absence of antral or corpus
sitive or H pylori Negative (Figures 4 and 5 for Details)
tology Panel N TP TN FP FN Se Sp
53 65 70 50 2 15 3 94 1255 70 72 55 2 15 0 100 1217 0 70 0 53 0 17 0 10017 0 72 0 55 0 17 0 100
8 2 70 2 62 0 6 25 1008 2 72 2 64 0 6 25 100
30 0 88 0 58 0 30 0 10030 0 89 0 59 0 30 0 10027 27 88 7 42 20 20 26 6827 6 90 2 59 4 25 7 9430 1 88 0 57 1 30 0 9830 0 89 0 59 0 30 0 10058 19 88 16 27 3 42 28 9059 9 89 6 27 3 53 10 90
6 0 89 0 83 0 6 0 1006 0 90 0 84 0 6 0 100
58 41 88 24 13 17 34 41 4359 74 89 52 8 22 7 88 27
false negative; Se, sensitivity; Sp, specificity; Hp, H pylori.
Shown in Figure 4
N TP TN FP FN Se Sp
58 108 3 44 3 97 661 114 2 45 0 100 458 0 111 0 47 0 100
61 0 114 0 47 0 10059 2 145 0 12 14 100
61 2 147 0 12 14 100
ri Po
His
me
111
11
1
positive; FN, false negative; Se, sensitivity; Sp, specificity.
adlpbapptmhwiwg
1
1
1
1
1
1
1
1
1
1
2
2
2
2
2
2
2
2
2
Fat0
March 2006 NONINVASIVE DIAGNOSIS OF GASTRIC ATROPHY 313
trophy in unselected individuals. The results wereisappointing, suggesting that, at least in this popu-ation and similar to those in another asymptomaticopulation from Italy,31 the algorithm might need toe revised for use in low-risk populations. The currentlgorithm starts with H pylori status, and although itroved useful to identify normal stomachs, it didoorly for identifying atrophic gastritis. It is possiblehat starting with the PGI levels or PGI:PGII ratioight provide more useful information. Recently it
as been reported that high ghrelin levels correlateith low pepsinogen levels and atrophic gastritis.34 It
s unclear whether measurement of ghrelin levelsould enhance the noninvasive detection of atrophicastritis, and more studies are needed.
References1. Graham DY. Helicobacter pylori infection is the primary cause of
gastric cancer. J Gastroenterol 2000;35(Suppl 12):90–97.2. Sipponen P, Kekki M, Haapakoski J, et al. Gastric cancer risk in
chronic atrophic gastritis: statistical calculations of cross-sec-tional data. Int J Cancer 1985;35:173–177.
3. Oshima A. Secondary prevention: screening methods in high-incidence areas. In: Sugimura T, Sasako M, eds. Gastric cancer.Oxford: Oxford University Press, 1997:199–212.
4. Aoki K, Misumi J, Kimura T, et al. Evaluation of cutoff levels forscreening of gastric cancer using serum pepsinogens and distri-butions of levels of serum pepsinogen I, II and of PG I/PG II ratiosin a gastric cancer case-control study. J Epidemiol 1997;7:143–151.
5. Fukuda H, Saito D, Hayashi S, et al. Helicobacter pylori infection,serum pepsinogen level and gastric cancer: a case-control studyin Japan. Jpn J Cancer Res 1995;86:64–71.
6. Hattori Y, Tashiro H, Kawamoto T, et al. Sensitivity and specificityof mass screening for gastric cancer using the measurement ofserum pepsinogens. Jpn J Cancer Res 1995;86:1210–1215.
igure 6. The accuracy of the PGI:PGII ratio or detecting corpustrophy is shown in relation to different cutoff values. The area underhe receiver-operator characteristic curve was 0.763 (95% CI, 0.69–.82).
7. Kitahara F, Kobayashi K, Sato T, et al. Accuracy of screening for 2
gastric cancer using serum pepsinogen concentrations. Gut1999;44:693–697.
8. Miki K, Ichinose M, Ishikawa KB, et al. Clinical application ofserum pepsinogen I and II levels for mass screening to detectgastric cancer. Jpn J Cancer Res 1993;84:1086–1090.
9. Shiotani A, Iishi H, Uedo N, et al. Histologic and serum riskmarkers for noncardia early gastric cancer. Int J Cancer 2005;115:463–469.
0. Miki K, Ichinose M, Shimizu A, et al. Serum pepsinogens as ascreening test of extensive chronic gastritis. Gastroenterol Jpn1987;22:133–141.
1. Kekki M, Samloff IM, Varis K, et al. Serum pepsinogen I andserum gastrin in the screening of severe atrophic corpus gastri-tis. Scand J Gastroenterol Suppl 1991;186:109–116.
2. Varis K, Kekki M, Harkonen M, et al. Serum pepsinogen I andserum gastrin in the screening of atrophic pangastritis with highrisk of gastric cancer. Scand J Gastroenterol Suppl 1991;186:117–123.
3. Graham DY. Helicobacter pylori and perturbations in acid secre-tion: the end of the beginning. Gastroenterology 1996;110:1647–1650.
4. Graham DY, Dore MP. Perturbations in gastric physiology inHelicobacter pylori duodenal ulcer: are they all epiphenomena?Helicobacter 1997;2(Suppl 1):S44–S49.
5. Graham DY, McGuigan JE. Interactions between gastrin, gastricsecretion, and Helicobacter pylori in health and disease. In:Tache Y, Goto Y, Ohning G, Yamada T, eds. Gut-brain peptides inthe new millenium. Los Angeles: Cure Foundation, 2002:83–101.
6. El-Zimaity HM, Graham DY, Al-Assi MT, et al. Interobserver vari-ation in the histopathological assessment of Helicobacter pylorigastritis. Hum Pathol 1996;27:35–41.
7. Rugge M, Correa P, Dixon MF, et al. Gastric mucosal atrophy:interobserver consistency using new criteria for classification andgrading. Aliment Pharmacol Ther 2002;16:1249–1259.
8. El-Zimaity HM, Ota H, Graham DY, et al. Patterns of gastricatrophy in intestinal type gastric carcinoma. Cancer 2002;94:1428–1436.
9. Ricuarte O, Gutierrez O, Cardona H, et al. Atrophic gastritis inyoung children and adolescents. J Clin Pathol 2005;58:1189–1193.
0. Kimura K. Chronological transition of the fundic-pyloric borderdetermined by stepwise biopsy of the lesser and greater curva-tures of the stomach. Gastroenterology 1972;63:584–592.
1. Kimura K, Takemoto T. An endoscopic recognition of the atrophicborder and its significance in chronic gastritis. Endoscopy 1969;1:87–97.
2. Miederer SE, Paul F, Stadelmann O, et al. Pyloric-kardiate expan-sion der gastritis. Endoscopy 1969;1:170–174.
3. Kimura K, Satoh K, Ido K, et al. Gastritis in the Japanese stom-ach. Scand J Gastroenterol Suppl 1996;214:17–20.
4. Satoh K, Kimura K, Taniguchi Y, et al. Distribution of inflamma-tion and atrophy in the stomach of Helicobacter pylori-positiveand -negative patients with chronic gastritis. Am J Gastroenterol1996;91:963–969.
5. Sipponen P, Ranta P, Helske T, et al. Serum levels of amidatedgastrin-17 and pepsinogen I in atrophic gastritis: an observa-tional case-control study. Scand J Gastroenterol 2002;37:785–791.
6. Graham DY. Helicobacter pylori infection in the pathogenesis ofduodenal ulcer and gastric cancer: a model. Gastroenterology1997;113:1983–1991.
7. Graham DY, Shiotani A. The time to eradicate gastric cancer isnow. Gut 2005;54:735–738.
8. Sipponen P, Harkonen M, Alanko A, et al. Diagnosis of atrophicgastritis from a serum sample. Clin Lab 2002;48:505–515.
9. Hartleb M, Wandzel P, Waluga M, et al. Non-endoscopic diagno-

3
3
3
3
3
SAc
MHDHdotG
314 GRAHAM ET AL CLINICAL GASTROENTEROLOGY AND HEPATOLOGY Vol. 4, No. 3
sis of multifocal atrophic gastritis; efficacy of serum gastrin-17,pepsinogens and Helicobacter pylori antibodies. ActaGastroenterol Belg 2004;67:320–326.
0. Pasechnikov VD, Chukov SZ, Kotelevets SM, et al. Invasive andnon-invasive diagnosis of Helicobacter pylori-associated atrophicgastritis: a comparative study. Scand J Gastroenterol 2005;40:297–301.
1. Ricci C, Vakil N, Rugge M, et al. Serological markers for gastricatrophy in asymptomatic patients infected with Helicobacter py-lori. Am J Gastroenterol 2004;99:1910–1915.
2. Vaananen H, Vauhkonen M, Helske T, et al. Non-endoscopicdiagnosis of atrophic gastritis with a blood test: correlation be-tween gastric histology and serum levels of gastrin-17 and pep-sinogen I: a multicentre study. Eur J Gastroenterol Hepatol 2003;15:885–891.
3. Hallissey MT, Dunn JA, Fielding JW. Evaluation of pepsinogen Aand gastrin-17 as markers of gastric cancer and high-risk patho-logic conditions. Scand J Gastroenterol 1994;29:1129–1134.
4. Suzuki H, Masaoka T, Hosoda H, et al. Plasma ghrelin con-
centration correlates with the levels of serum pepsinogen I cand pepsinogen I/II ratio: a possible novel and non-invasivemarker for gastric atrophy. Hepatogastroenterology 2004;51:1249–1254.
Address requests for reprints to: Victor Cardenas, MD, MPH, PhD, UTchool of Public Health El Paso Regional Campus, 1100 N Stantonvenue, Suite 110F, El Paso, Texas 79902. e-mail: [email protected]; fax: (915) 747-8512.Supported in part by the Office of Research and Development,edical Research Service, Department of Veterans Affairs, by Publicealth Service grant DK56338 which funds the Texas Gulf Coastigestive Diseases Center, and by a grant from Biohit Diagnostics,elsinki, Finland. No for-profit company had any input into the studyesign or analyses. Dr Graham receives royalties from Baylor Collegef Medicine from a patent on the antigen used in the HM-CAP serologicest. The Mexican Institute for Social Security authorized the use of theeneral Hospital Region 6 endoscopic facility and staff support to
onduct the endoscopies.Copyright © 2022 FDOKUMEN







![[Posterior cortical atrophy]](https://static.fdokumen.com/doc/165x107/6331b9d14e01430403005392/posterior-cortical-atrophy.jpg)












