Appendiceal CT in 140 cases diagnostic criteria for acute and necrotizing appendicitis
20
APPENDICEAL CT IN 140 CASES DIAGNOSTIC CRITERIA FOR ACUTE AND NECROTIZING APPENDICITIS YOUNG H. CHOI, MD, EVA FISCHER, MD, SYED A. HODA, MD, WILLIAM A. RUBENSTEIN, MD, KEVIN P. MORRISSEY, MD, DOUGLAS HERTFORD, MD, KIM HWANG, MD, ELIZABETH RAMIREZ DE ARELLANO, MD, AND ELIAS KAZAM, MD Computed tomography (CT) was performed in 140 citis (8–40). Excellent results have been reported for both US and CT, with accuracy of 90% to 95% in patients with suspected acute appendicitis. Thin col- limation (5 mm), intravenous contrast enhancement, several studies (17–20, 29, 30). Direct visualization of the abnormal appendix gives sectional imaging a 1-second scan times, and supplementary cecal air in- sufflation were emphasized. CT accuracy was 98% substantial advantage over conventional radiography, which relies mainly on indirect signs for diagnosing overall (137/140), and 99% in the 124 cases with early surgery. Necrotizing appendicitis was diagnosed by appendicitis (41–45). US is ideal for initial imaging of thin patients, premenopausal and pregnant CT with 86% accuracy and 90% positive predictive value. Elsevier Science Inc., 1998 women (20, 23, 25, 30), and pediatric patients (33– 40). CT is more sensitive than US in the diagnosis of acute appendicitis and its complications (46), and is KEY WORDS: most useful for patients where sonography is found Appendicitis; Appendix CT; Appendix; Appendix abscess to be, or likely to be, nondiagnostic. In this article we report on a series of 140 consecutive surgically proven CT scans in patients with equivocal clinical INTRODUCTION diagnoses of appendicitis, performed in our hospital The relatively high rate of negative appendectomy during the last 3 years. Emphasis was placed on con- (20% to 35%) (1–7), and the widespread availability tiguous thin sections (5 mm), 1-second scan times, of computed tomography (CT) and sonography (US) and intravenous contrast enhancement (CECT) (Ta- have stimulated the use of these imaging procedures ble 1). We evaluate the usefulness of supplementary for patients with clinically suspected acute appendi- scans after colonic air distension in the lateral de- cubitus position, and we assess the diagnostic value of CECT for necrotizing appendicitis. From the Departments of Radiology (Y.H.C., W.A.R., O.H., K.H., E.R.D.A., E.K.), Surgery (E.F., K.P.M.), and Pathology (S.A.H.), New York Hospital-Cornell Medical Center, New York, New York. Address reprint requests to: Elias Kazam, MD, Department of METHODS Radiology, The New York Hospital-Cornell Medical Center, 525 E. CT Methods 68th Street, Room ST839, New York, NY 10021. Current address for Dr. Choi: Young H. Choi, MD, Department Patients were referred for CT scanning predominantly of Radiology, Chung Ang Univ Medical Center 81-1, Phil Dong Chung Gu, Seoul, Korea. from the surgical emergency room, because of an From the paper presented at the 81st annual meeting of the Ra- equivocal or atypical clinical presentation for acute diological Society of North America (RSNA) in Chicago, Illinois, appendicitis. Thin patients, premenopausal or preg- November 26–December 1, 1995. Received November 5, 1996; accepted November 15, 1996. nant women, and pediatric patients were referred CLINICAL IMAGING 1998;22:252–271 Elsevier Science Inc., 1998. All rights reserved. 0899-7071/98/$19.00 655 Avenue of the Americas, New York, NY 10010 PII S0899-7071(97)00080-6
Transcript of Appendiceal CT in 140 cases diagnostic criteria for acute and necrotizing appendicitis

APPENDICEAL CT IN 140 CASESDIAGNOSTIC CRITERIA FOR ACUTE ANDNECROTIZING APPENDICITIS
YOUNG H. CHOI, MD, EVA FISCHER, MD, SYED A. HODA, MD,WILLIAM A. RUBENSTEIN, MD, KEVIN P. MORRISSEY, MD,DOUGLAS HERTFORD, MD, KIM HWANG, MD,ELIZABETH RAMIREZ DE ARELLANO, MD,AND ELIAS KAZAM, MD
Computed tomography (CT) was performed in 140 citis (8–40). Excellent results have been reported forboth US and CT, with accuracy of 90% to 95% inpatients with suspected acute appendicitis. Thin col-
limation (5 mm), intravenous contrast enhancement, several studies (17–20, 29, 30). Direct visualizationof the abnormal appendix gives sectional imaging a1-second scan times, and supplementary cecal air in-
sufflation were emphasized. CT accuracy was 98% substantial advantage over conventional radiography,which relies mainly on indirect signs for diagnosingoverall (137/140), and 99% in the 124 cases with early
surgery. Necrotizing appendicitis was diagnosed by appendicitis (41–45). US is ideal for initial imagingof thin patients, premenopausal and pregnantCT with 86% accuracy and 90% positive predictive
value. Elsevier Science Inc., 1998 women (20, 23, 25, 30), and pediatric patients (33–40). CT is more sensitive than US in the diagnosis ofacute appendicitis and its complications (46), and isKEY WORDS:
most useful for patients where sonography is foundAppendicitis; Appendix CT; Appendix; Appendix abscessto be, or likely to be, nondiagnostic. In this article wereport on a series of 140 consecutive surgicallyproven CT scans in patients with equivocal clinicalINTRODUCTIONdiagnoses of appendicitis, performed in our hospital
The relatively high rate of negative appendectomy during the last 3 years. Emphasis was placed on con-(20% to 35%) (1–7), and the widespread availability tiguous thin sections (5 mm), 1-second scan times,of computed tomography (CT) and sonography (US) and intravenous contrast enhancement (CECT) (Ta-have stimulated the use of these imaging procedures ble 1). We evaluate the usefulness of supplementaryfor patients with clinically suspected acute appendi- scans after colonic air distension in the lateral de-
cubitus position, and we assess the diagnostic valueof CECT for necrotizing appendicitis.From the Departments of Radiology (Y.H.C., W.A.R., O.H.,
K.H., E.R.D.A., E.K.), Surgery (E.F., K.P.M.), and Pathology(S.A.H.), New York Hospital-Cornell Medical Center, New York,New York.
Address reprint requests to: Elias Kazam, MD, Department of METHODSRadiology, The New York Hospital-Cornell Medical Center, 525 E.
CT Methods68th Street, Room ST839, New York, NY 10021.Current address for Dr. Choi: Young H. Choi, MD, Department
Patients were referred for CT scanning predominantlyof Radiology, Chung Ang Univ Medical Center 81-1, Phil DongChung Gu, Seoul, Korea. from the surgical emergency room, because of an
From the paper presented at the 81st annual meeting of the Ra- equivocal or atypical clinical presentation for acutediological Society of North America (RSNA) in Chicago, Illinois,
appendicitis. Thin patients, premenopausal or preg-November 26–December 1, 1995.Received November 5, 1996; accepted November 15, 1996. nant women, and pediatric patients were referred
CLINICAL IMAGING 1998;22:252–271 Elsevier Science Inc., 1998. All rights reserved. 0899-7071/98/$19.00655 Avenue of the Americas, New York, NY 10010 PII S0899-7071(97)00080-6

253JULY/AUGUST 1998 CT IN ACUTE APPENDICITIS
TABLE 1. Acute Appendicitis: CT in 124 Cases with Early Surgerya
CECT NECT Total(n 5 117) (n 5 7) (n 5 124)
CT Diagnosis Accuracy 123/124 5 99%True positive 104 7b 111 Sensitivity 104/104 5 100%True negative 12 0 12 Specificity 12/13 5 92%False positive 1 0 1 Positive Pred. Value 104/105 5 99%
a Surgery within 1 week (98% within 3 days) of the CT scan.b Includes one case of granulomatous appendicitis.
initially for sonography, and came to CT only if US subsequent batched axial 1-second scans, beginning1–1.5 minutes after the end of the contrast infusion.was nondiagnostic—or if further definition of the ex-
tent of disease was desired. Contiguous CT thin sec- Oral contrast (2% Gastrografin) was administered atleast one half hour before the CT scan, but was nottions (5 mm) and intravenous contrast enhancement
were used whenever possible. The entire abdomen considered absolutely essential, unless intravenouscontrast was contraindicated. Intravenous glucagonand pelvis were scanned routinely. Nonenhanced
(NECT) 1-second axial scans were obtained initially (0.3 or 0.5 mg) was given in nearly half the cases, es-pecially if supplementary lateral decubitus viewsfrom the diaphragmatic dome inferiorly to the S1
vertebral level, using 5-mm (or occasionally 7-mm) were performed.In 47 of the 140 cases studied (34%), additionalcollimation, and followed by intravenous contrast
enhanced spiral scans (CECT) with 5-mm (occasion- 5-mm contiguous 1-second scans were obtained inthe left lateral decubitus position, after air distentionally 7-mm) collimation and a pitch of 1. The remain-
der of the lower abdomen and pelvis were then im- of the ascending colon and cecum, for one or more ofthe following indications: (a) the appendix was notaged with contiguous 5-mm 1-second CECT scans in
the batched axial mode. clearly visualized, or its lumen was not clearly delin-eated from its wall, on the initial scans; (b) the cecumA 120-ml volume of a 30 g/dl iodinated solution
was used for intravenous contrast enhancement. was not sufficiently distended to allow for clearidentification of the caput cecum on the initial im-10 ml of this solution were initially administered
nearly 5 minutes before the main infusion. This gave ages; and (c) the terminal ileum, ileocecal junction,or portions of the sigmoid colon were not clearlysufficient time for opacification of the renal calyces
and pelves in 85% of the cases. The main infusion identifiable or sufficiently distended on the initialscans. Rectal air (average 250 ml) was administeredwas then carried out in three phases with a 90-sec-
ond prep delay: (a) 30 ml at 0.6 ml/sec for 50 seconds gradually with a 30-ml syringe over a 3- to 5-minuteinterval via a 7 French red rubber catheter, using the(to give time for parenchymal, bowel wall, hepatic
vein, and calyceal opacification), followed by (b) 60 patient’s feeling of distention, and the physician’sassessment of colonic backpressure as endpoints. CTml at 1.5 ml/sec for 40 seconds to augment the initial
contrast opacification, and then (c) 20 ml ar 1.1 ml/ evidence for severe colitis, diverticulitis, or extralu-minal air on the initial scans precluded colonic airsec to maintain arterial and portal opacification dur-
ing the first part of the spiral scan. Because of limita- insufflation.The CECT diagnosis of acute appendicitis dependedtions in the heat capacity of the X-ray tube, only the
upper abdomen was scanned in the spiral mode. mainly on the presence of wall enhancement or hy-peremia (Table 2, Figures 1–5). Appendicoliths andMost or all of the appendiceal bed was scanned with
TABLE 2. Acute Appendicitis: CECT Diagnostic Criteria in 105 Surgically Proven Cases
No. ofCT Sign Figure cases (%)
Ring sign: Enhanced wall 1 lucent lumen 1, 2 92 (87)Double ring sign: Two enhanced rings 3 7a (7)Thick enhanced wall 1 isodense lumen 4 3 (3)Appendix not seen 1 abscess in appendix bed 7 3 (3)Periappendiceal edema (6 extraluminal air) 105 (100)
a All associated with necrotizing appendicitis.


255JULY/AUGUST 1998 CT IN ACUTE APPENDICITIS
periappendiceal edema were valuable confirmatory ble, maximally tender bowel loop in the expected lo-cation of the appendix (Figures 2e and 13e). Hyper-signs (Figure 6). The presence of an abscess within
the appendiceal bed was considered diagnostic of vascularity on color Doppler, fecaliths, and ascitesacute appendicitis if the appendix was not visual- were associated findings. Necrotizing appendicitis wasized, and there was no CT evidence for intrinsic cecal diagnosed when sonography demonstrated a periappen-or ileal disease (Figure 7). One case was complicated diceal collection. Markedly asymmetric wall thicken-by liver abscesses (Figure 8). These same criteria were ing and loss of submucosal echogenicity were consid-used in the interpretation of supplementary left lateral ered suspicious findings for necrotizing appendicitis,decubitus CECT scans (Figures 9–12). especially if accompanied by an appendicolith.
The CECT diagnosis of necrotizing appendicitis For this study, 140 consecutive CT scans with sub-depended mainly on focal absence of wall enhance- sequent surgical verification were reviewed by twoment or continuity (Table 3, Figures 1 and 3–6), and radiologists without knowledge of the final diagnosison the presence of extraluminal abscess or air (Fig- (Table 1). In the three cases (2%) where disagree-ures 4 and 5). ment occurred, a consensus opinion was reached
NECT diagnosis of acute appendicitis depended after a joint discussion of the CT findings. The CT di-on visualization of a thickened wall .3 mm, and the agnoses were then compared to the surgical and pa-presence of periappendiceal edema, collection, or thology findings, as they appeared on the operativeextraluminal air to indicate an active inflammatory and pathology reports, and to the initial CT diagno-process. ses as they appeared on the radiology report.
Since the original pathology reports did not al-ways contain a detailed description of the extent ofUltrasound Methodsinflammation within the appendiceal wall, the pa-
Seventeen patients had concomittant sonograms. US thology slides form 105 patients who had CECTwas obtained for initial imaging in 13, and to supple- scans were reviewed with particular attention to thement the CT scan by determining the site of maximal nature and extent of the inflammatory process. Am-tenderness in four cases. The examination was per- biguous and imprecise terminology such as, “acuteformed in the supine position with the thighs flexed suppurative, acute phlegmonous, acute gangrenous,to decrease tension in the anterior abdominal wall. and acute perforating appendicitis” was avoided. In-The patient was encouraged to point to the site of stead the extent of appendicitis was graded objec-maximal tenderness with one finger. A wide diameter tively in the following manner:(58 mm) linear 5 MHz transducer with multiplanar fo-
Grade 0: Negative for acute appendicitis. No evi-cusing was then used for graded compression of thisdence of acute inflammation on gross or micro-site. The examiner’s finger was applied directly toscopic examination.the structure visualized in real time to determine
whether it corresponded to the point of maximal ten- Grade 1: Early acute appendicitis. Acute inflam-derness. Rebound tenderness was also elicited. The matory cellular infiltrate limited to the mucosasonograms were supplemented with color and spec- and submucosa, without evidence for necrosis.tral Doppler, and with left and right decubitus views.
Grade 2: Classic acute appendicitis without per-Adjacent structures such as right kidney, gallblad-foration. Acute inflammatory cell infiltrate in-der, paracolic gutter, adnexa, uterus, and cul de sacvolving mucosa, submucosa, and musculariswere routinely imaged.propria, but sparing the serosa.Sonographic diagnosis of acute appendicitis was
based on the presence of a thickened, noncompressi- Grade 3: Acute necrotizing appendicitis with per-
FIGURE 1. Acute necrotizing appendicitis with ”ring sign” in a 36-year-old man. Composite of four contrast enhanced,5-mm thick, CT images from superior (a) to inferior (d). Enhanced (hyperemic) appendiceal wall (white arrows and arrow-head), encircles a fluid filled distended lumen. Wall thickness varies between 1–2 mm superiorly (white arrowhead) and3–4 mm inferiorly (white arrows), (b). Focal loss of wall continuity (black arrows) suggests necrosis. Preservation of en-hancement at the appendiceal tip (curved black arrows), (c and d), despite loss of wall continuity above it, is attributableto the arterial supply of the appendix (e). The appendicular artery terminates at the appendiceal tip, after sending multipleside branches to supply the upper appendix. Fecalith (f). Edema of the periappendiceal fat (open arrows). Ascites (asc).Thickened, hyperdense (hyperemic) peritoneum (p). Ureter (ur). Appendectomy within 1 day of the CT scan confirmedacute necrotizing appendicitis. Figure 1e reprinted with permission from [58]: Williams PL, Warwick R eds. Gray’s Anat-omy. 36th Ed. Philadelphia: WB Saunders Co. 1980 (Fig 6.89, p 716).
256 CHOI ET AL. CLINICAL IMAGING VOL. 22, NO. 4
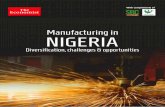
FIGURE 2. Acute appendicitis with heterogeneous wallenhancement-correlation with ultrasound. Composite offour contrast enhanced, 5-mm thick, CT images from supe-rior (a) to inferior (d), in a 23-year-old man. A 3–6 mm en-hanced (hyperemic) appendiceal wall (black arrows) withlucent mural foci (small white arrows, c and d) surroundsa narrow lucent lumen. The wall lucencies probably liewithin the submucosa, which appears hyperechogenic anddiffusely thickened on corresponding sonogram (smallwhite, e). Periappendiceal edema (white arrowheads).Thickening of cecum, terminal, and distal ileum (openarrows) suggested possible enteritis, but the CT and USfindings, and the localization of maximal tenderness to theappendix by US, strongly favored primary appendicitiswith secondary bowel edema. This was confirmed at sur-gery 2 hours later.

257JULY/AUGUST 1998 CT IN ACUTE APPENDICITIS
FIGURE 3. Acute necrotizing appendicitis with ”double ring” sign. Composite of four contrast enhanced, 5-mm thick, CTimages from superior (a) to inferior (d), in a 51-year-old man. Wall enhancement (hyperemia) is noted in the appendix(small white arrows, a and b) and lower cecum (C, a). A double ring of wall enhancement is noted more inferiorly (largewhite arrows, a and d). The inner ring may represent hyperemic mucosa, separated by edematous lucent submucosa fromthe outer ring of hyperemic muscularis propria. Necrotizing appendicitis is suggested by the focal loss of wall contour(white arrowhead), and, as found on subsequent review of this series, by the double ring sign. Periappendiceal edema (openwhite arrows). Findings were confirmed pathologically after appendectomy within 1 day of the CT scan.
foration. Transmural acute inflammatory cell were verified with early surgery (Table 1), and atleast 88% in the 16 cases with delayed appendec-infiltrate with necrosis, leading to gross or mi-
croscopic appendiceal perforation. tomy. The appendix was pelvic in location in 80 pa-tients (57%), retrocecal (ascending behind, lateral, or
For the purpose of this study, either a pathologic medial to the cecum) in 37 (26%), subcecal (coursinggrade of 3 and/or the surgical finding of appendiceal at and slightly below the level of the cecum) in 15perforation was accepted as proof of acute necrotiz- (11%), transversely oriented with its tip to the left ofing appendicitis, because a grossly necrotic segment midline in four (3%), and nonvisualized in four (3%).of appendix at surgery may not be available for sub-sequent pathologic examination if it is located at the Early Surgical Confirmationsite of resection.
All but one of the cases in this group (111 with acuteappendicitis and 13 with either a normal or chroni-cally inflamed appendix) were diagnosed correctly
RESULTS (Table 1). The single exception was a false positiveIn the study group of 140 surgically verified cases, CECT scan in a patient with an enhanced tender ap-CT accuracy for diagnosing acute appendicitis was pendix containing tiny fecaliths at its base, who had
appendiceal lymphoid hyperplasia, and chronic ap-98% overall (147/140), 99% in the 124 cases which

258 CHOI ET AL. CLINICAL IMAGING VOL. 22, NO. 4
FIGURE 4. Necrotizing appendicitis with small periappendiceal abscess. Composite of four contrast enhanced, 5-mmthick, CT images from superior (a) to inferior (d), in a 35-year-old man. The appendix courses superiorly after originating(a) from a moderately edematous cecum (small curved arrow, d). The thickened appendiceal wall is heterogeneously en-hanced (large black arrows) with multiple scattered lucent foci, and irregularly delineated outer contour (black arrow-heads). A small multiloculated collection with a hyperemic wall (large curved arrows) confirms the suspicion of wall necro-sis leading to abscess formation. The appendiceal lumen is poorly defined. Marked appendiceal edema (small black arrows)extends medial to the right common iliac vessels. Right ureter (ur). Hyperplastic lymph nodes (ln).
pendicitis at the tip on pathologic examination (Ta- minal air on CT, presumably due to appendiceal mi-croperforation, were reported to have nonperforatedble 1, Figure 13). Subsequent stool cultures were posi-
tive for Campylobacter in this patient. One patient acute appendicitis at surgery. The interval betweenthe CT scan and surgery for these nine cases washad granulomatous appendicitis (Figure 14). One of
the true negative cases had an intraluminal appendi- within: 1 day in seven, 2 days in one case, and 3 daysin the remaining case.colith near the tip, but no CECT criteria for acute ap-
pendicitis. There were no false negative cases. The Appendiceal perforation was also a source of dis-crepancy between the surgery and pathology reports.accuracy and positive predictive value of CT for
acute appendicitis in this series were both 99%. Three cases with perforated or necrotic appendicesat surgery were diagnosed as non-necrotizing acuteOther than the single false positive CT diagnosis
for acute appendicitis, the main source for discrep- appendicitis (Grades 1 or 2) at pathology. Thesecases were classified as necrotizing appendicitis inancy between CT and surgery among the 124 cases
with early exploration was the presence of appendi- this study, because of the likelihood that the necroticsegment(s) of appendix were not available for patho-ceal perforation. There were nine such cases in this
series. Seven patients with a CT diagnosis of nonper- logic examination, possibly due to location at themargin of resection.forated acute appendicitis were found to have perfo-
ration (including two with small abscesses) at early The CECT diagnosis of acute appendicitis wasbased on direct visualization of the appendix, exceptsurgery. Also two patients with tiny foci of extralu-

259JULY/AUGUST 1998 CT IN ACUTE APPENDICITIS
FIGURE 5. Necrotizing appendicitis with extraluminal air. Composite of four contrast enhanced, 5-mm thick, CT imagesfrom superior (a) to inferior (d), in a 40-year-old man. The appendiceal wall is mildly enhanced and irregular in contour(closed white arrows, c and d). Focal loss of enhancement and wall continuity (small white arrows, b and c) suggests necro-tizing appendicitis. A small contained appendiceal rupture is suggested by tiny foci of local and distant extraluminal air(curved white arrows, a and b). Fecalith (f). Edema of mesenteric fat (open arrows) and of cecum and distal ileum (arrow-heads). Thickened posterior peritoneum (p). Right ureter (ur). Necrotizing appendicitis was confirmed by surgery withinone day of the CT scan.
in three cases with abscesses in the appendiceal bed hyperplasia and chronic appendicitis at the tip werefound after appendectomy. The subsequently positiveand nonvisualized appendices at CT or surgery (Ta-
ble 2). The frequency of the CECT diagnostic criteria stool cultures for Campylobacter suggest that a chroni-cally inflamed appendix may have been secondarilyand pertinent illustrations are listed in Table 2. As-
sociated findings included appendicoliths, which involved by a diffuse enteritis.CECT signs of necrotizing appendicitis and perti-were seen in 44/105 cases (42%) (Figures 1, 2, 5, and
6), and periappendiceal edema and/or infiltration nent illustrations are listed in Table 3. Based on thesecriteria necrotizing appendicitis was diagnosed withwhich were noted in all 105 CECT cases.
In the single false positive CECT scan for acute ap- an accuracy of 86% and a positive predictive valueof 90% (Table 4). Of interest, all seven cases with apendicitis, there was a clear ring sign with an en-
hanced appendiceal wall, tiny fecaliths at the appendi- double ring sign of appendiceal wall enhancementhad necrotizing appendicitis on subsequent correla-ceal base, and periappendiceal edema (Figure 13). The
cecum, lower ascending colon, and ileum were moder- tion with the pathologic findings. Similarly 34/45(76%) of the cases with appendicoliths and CT signsately thickened, and there was enhancement of the co-
lonic mucosa (Figure 13a,b). The localization of maxi- of acute appendicitis were associated with eithernecrotizing appendicitis (23 cases) or appendicealmal direct and rebound tenderness to the appendix by
ultrasound (Figure 13e) strongly favored a primary, abscess (11 cases).NECT signs for acute appendicitis, seen in allrather than secondary appendicitis. Only lymphoid

260 CHOI ET AL. CLINICAL IMAGING VOL. 22, NO. 4
FIGURE 6. False positive CT scan for appendiceal wall necrosis. Composite of four contrast enhanced, 5-mm thick, CTimages from superior (a) to inferior (d), in a 32-year-old man. The appendix courses posterolaterally and inferiorly fromits origin (A, b), and has an enhanced slightly thickened wall (large white arrows). Foci of wall thinning and/or discontinu-ity (white arrowheads, b and d) suggest appendiceal necrosis. The appendiceal lumen is dilated inferiorly and containsfluid, air, and fecaliths (f). Periappendiceal edema (small arrows). Surgery on the same day confirmed appendicitis, butwithout gross or pathologic evidence of appendiceal necrosis.
seven cases, were: a thickened appendiceal wall .3 The subsequent pathologic findings confirmed theinitial CT diagnosis in 14/16 (88%) of the cases withmm surrounding a relatively lucent lumen, and peri-
appendiceal edema or fat infiltration (with or with- delayed surgery, mainly by showing evidence forchronic appendicitis or periappendicitis (Table 5).out extraluminal air) to indicate an active inflamma-
tory process. An intraluminal fecalith was evident in Of interest, there was residual acute appendicitis infour cases, with appendiceal necrosis in three. In anone case.additional case a focus of subacute appendicitis witheosinophilic infiltration was superimposed on acuteDelayed Surgeryinflammation. The two cases without confirmationIn the group of 16 cases with delayed surgery (Tablehad pathologic diagnoses of “normal appendix” and5) CECT was performed in 14, and NECT in two“lymphoid hyperplasia” (Table 5).cases. Surgery was delayed for 15 of these 16 patients
to allow for resolution of the inflammatory processDiagnostic Value of Left Lateral Decubitus Scansafter antibiotic therapy (Table 5). Eleven of these, in-
cluding three with appendicoliths, had CT evidence Supplementary decubitus CT scans were obtainedfor perforated acute appendicitis with abscess forma- after colonic air insufflation in 47/140 (34%) cases,tion (Table 5). The remaining patient, with recurring to further delineate the appendix and to assess theright lower quadrant and pelvic pain, had elective distensibility of its lumen, and of adjacent cecumdelayed surgery for CT findings of a proximal appendi- and ileum. The amount of air introduced with this
technique varied between 100 ml and 400 ml, (aver-colith with thickened periappendiceal fatty septa.

261JULY/AUGUST 1998 CT IN ACUTE APPENDICITIS
FIGURE 7. Appendiceal abscess without visualized appendix. Composite of four contrast enhanced, 5-mm thick, CT im-ages from superior (a) to inferior (d), in a 44-year-old man. A markedly edematous cecum (open white arrow, a) is indentedand partially invaginated by a multiloculated collection with an enhanced, hyperemic wall directly below the cecum (blackarrows, b and c). There is marked edema of the adjacent terminal ileum (white arrow, d). Although the appendix was notvisualized, the location of the collection within the appendiceal bed and the marked edema and hyperemia led to a CT diag-nosis of perforated appendicitis with abscess. Partial intussusception of the abscess into the base of the cecum was postu-lated on CT. Surgery within 15 hours showed an appendiceal abscess impinging on, but not intussuscepting into the baseof the cecum. The appendix was not identified, even at surgery.
age 250 ml), depending on the patient’s report of full- was noted in 64 cases (50%) (Figures 2, 5, and 7), andness and the physician’s assessment of colonic back was moderate to severe in 11 cases (9%). Peritonealpressure. In 16/47 cases (34%) the decubitus scans thickening, or thickened/edematous retroperitonealprovided no additional information, and in 22/47 fatty septa were found in 66 cases (52%), (Figures 1, 3,(47%) the additional information did not significantly and 5), while periappendiceal abscess was present ininfluence the final CT diagnosis. In the remaining 9/ 35 cases (27%), (Figures 4, and 7). Other associated47 (19%) of the cases—9/140 (6%) of the entire study findings included mesenteric lymphadenopathy in 66group—the decubitus view was essential for the cor- cases (52%) (Figure 4), ascites in 62 cases (48%), (Fig-rect diagnosis, because of the additional information ure 1), sigmoid colon thickening/edema in 11 casesit provided about patency of the appendiceal lumen, (9%), partial small bowel obstruction in 13 cases (10%)focal hyperemia in the appendiceal wall, and the (Figures 11 and 12), adynamic ileus in 9 cases (7%),morphology of adjacent small and large bowel (Fig- and right hydronephrosis in 3 cases (2%).ures 9–12).
CT findings which were associated with appendi-Sonographycitis in this study included cecal thickening or edemaAmong the 17 sonograms in this study, nine werein 68 cases (53% of the 128 positive scans for the entiretrue positives for acute appendicitis (Figure 2), threestudy group), (Figures 1, 2, 4, 5 and 7). This was moder-
ate to severe in 33 cases (26%). Ileal thickening/edema were true negatives, one was false positive (Figure
262 CHOI ET AL. CLINICAL IMAGING VOL. 22, NO. 4
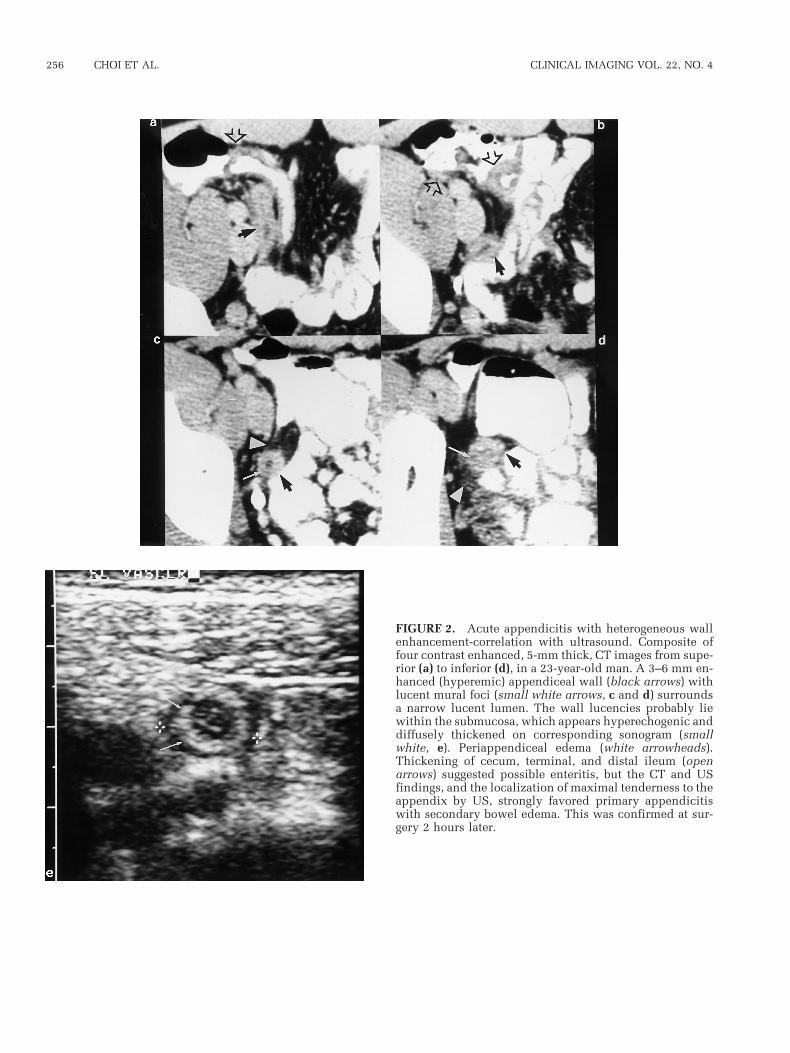
FIGURE 8. Liver abscesses secondary to appendicitis. Contrast enhanced CT scans of a 50-year-old man who presentedwith sepsis and hypotension. There are large multiloculated liver abscesses in the left and right lobes (black arrows, a).Gallbladder (gb), hepatic flexure of colon (hc). The appendiceal wall is mildly enhanced (large white arrow) with scatteredfocal lucencies (small white arrows), consistent with a mild appendicitis. This was confirmed at surgery, which was per-formed 3 days later because of incomplete percutaneous drainage of the liver abscesses. Pathologic exam showed Grade 2acute appendicitis without necrosis. This was the only identifiable source for the liver abscesses.
13), and four were false negative. The accuracy, sen- tributable to the emphasis on contiguous thin sec-tions (5 mm) and intravenous contrast enhancement.sitivity, and specificity of sonography were 71%,
69%, and 75%, respectively. The use of thin sections increased the likelihood ofvisualizing the appendix, allowing for direct ratherFor the entire study group of 140 patients, the di-
agnosis based on review of the CT and US scans dif- than inferred diagnoses. Only three abnormal appen-dices were not visualized by CT in this series, andfered from the original reported diagnoses in only
two cases (1.4%). A case with an appendicolith and these same appendices were also not visualized atsurgery, due to rupture and abscess formation. In allperiappendiceal thickening, but no wall enhance-
ment on CECT, was diagnosed as “subacute appendi- three cases the correct CT diagnosis of appendicitiswas inferred because the appendix was not visual-citis” initially, versus “chronic appendicitis” subse-
quently. In the other case the etiology of appendicitis ized despite detailed imaging, and the CT findings orwas not specified on the initial report, but a diagno- clinical history made primary disease of adjacentsis of granulomatous appendicitis was made on the small or large bowel unlikely. One normal appendixsecond reading (Figure 14). was not visualized by CT. In this case, the CT find-
ings indicated obstructive uropathy as the likelysource of right-sided abdominal pain in a pregnant
DISCUSSION woman, precluding further attempts to delineate theappendix.The high accuracy and positive predictive value of
CT for acute appendicitis in this series (99%) are at- Although the site of maximal pain correlates with

263JULY/AUGUST 1998 CT IN ACUTE APPENDICITIS
FIGURE 9. Early acute appendicitis (Grade 1)—value of colonic air contrast in the left lateral decubitus position. A com-posite of four contrast enhanced, 5-mm thick, CT images from superior (a) to inferior (d), in a 34-year-old woman. The ap-pendix takes origin (A, c and d) from a medially oriented cecum. It then courses laterally and superiorly (large white arrow,a). There is poor delineation of the appendiceal wall from its lumen, except at the appendiceal tip, where an air filled lumenis surrounded by a thin, clearly delineated wall (crossed white arrow, a). Mild edema of the periappendiceal fat (smallarrows, b and d) and of the terminal ileum (arrowhead, c).
the location of the appendiceal base (47), we elected and precluded the need for measurements of appendi-ceal thickness. From correlations with pathology andnot to begin the CT scan in the region of maximal ten-
derness. Sequential spiral scanning of the abdomen US, we were unable to ascertain the exact layer(s)within the appendiceal wall where enhancement oc-and pelvis makes it possible to examine other organ
systems in an orderly fashion. The appendiceal wall curred. We believe that diffuse hyperemia of the en-tire appendiceal wall was being perceived in mostis still well enhanced because it is imaged within
1 to 1.5 minutes of the end of contrast infusion. instances. In the cases with a “double ring” of wallenhancement, a sign which was also described byThe importance of intravenous contrast opacifica-
tion is emphasized by the finding that ring enhance- Balthazar et al. (12), the enhanced rings may repre-sent the mucosa and muscularis propria, with an in-ment , indicating hyperemia of the appendiceal wall,
was the most frequent direct CECT sign of appendici- tervening layer of relatively lucent edematous sub-mucosa (Figure 3). Of note, a previous study, basedtis (Table 2, Figures 1 and 2). This sign was described
by Balthazar et al. in several publications (12, 17, on in vitro US-pathology correlation, showed thatthe layers of the appendiceal wall became distorted46). In our series it was exceeded in frequency only
by the CECT finding of edema or thickening of the and difficult to delineate in the presence of appendi-citis (48).connective tissue septa in periappendiceal fat, a less
specific indirect confirmatory sign. Contrast enhance- Oral contrast, unlike intravenous contrast, wasnot considered absolutely essential. Since lumenalment made it possible to diagnose appendicitis with
minimal wall thickening on CECT (Figures 8–10), obstruction may not always be the primary etiologic

264 CHOI ET AL. CLINICAL IMAGING VOL. 22, NO. 4
FIGURE 10. Same patient as in Figure 9. Repeat 5-mm CT scans with colonic air contrast, obtained in the left lateral de-cubitus position but displayed conventionally, clearly show a slightly thickened, enhanced (hyperemic) segment in thewall of the midappendix (white arrow, a), with edema of the adjacent fat (open arrow). The more proximal mid appendix(crossed white arrow, b) appeared normal. Direct tenderness without rebound was localized to this region by US, but theappendix was not visualized sonographically. Minimal appendicitis was suspected by CT. Surgery 2 hours later revealeda grossly unremarkable appendix with slight hyperemia of its serosa. Pathologic exam revealed a focus of Grade 1 appendi-citis with associated lymphoid hyperplasia. Culture of periappendiceal fluid obtained at surgery was subsequently positivefor E. coli.
factor in appendicitis (49, 50), lumenal contrast sections. Using appendiceal wall thickening (diame-ter .6 mm), associated changes in the periappendi-could obscure contiguous wall enhancement in pa-
tients with early appendicitis and a patent lumen. ceal fat, and appendicoliths as diagnostic criteria,Malone et al. reported NECT accuracy of 93% forLumenal contrast could also obscure appendicoliths
(12). For further delineation of appendiceal wall acute appendicitis with sensitivity of 87% and speci-ficity of 97%, based on 94 surgically proven casesfrom lumen we resorted to left lateral decubitus CT
scans after air distention of the cecum (Figures 9– with contiguous 10-mm CT scans (15). In our series,seven patients were diagnosed correctly with NECT12). These supplementary views were essential for
the correct CT diagnosis in 6% of the 140 cases in this (Figure 14). Clearly NECT is a valuable diagnostictest for appendicitis. In addition mildly calcified ap-series, because they helped to: (a) delineate the par-
tially visualized or nonvisualized appendix; (b) ascer- pendicoliths which are easily seen with NECT can beobscured by CECT (Figure 15). Nevertheless, thetain patency of the appendiceal lumen of focal hyper-
emia of the appendiceal wall; and (c) exclude primary higher accuracy and positive predictive value ofCECT make it the preferred imaging procedure.lesions of adjacent cecum, sigmoid, and small bowel.
It is certainly possible to make accurate CT diag- The availability of contiguous thin sections andoptimal intravenous contrast enhancement facilitatednoses of acute appendicitis without contrast enhance-
ment (NECT), and even without the advantage of thin the CECT diagnosis of necrotizing appendicitis by

265JULY/AUGUST 1998 CT IN ACUTE APPENDICITIS
FIGURE 11. Acute appendicitis causing partial jejunal obstruction to the left of midline. Value of left lateral decubitusscans. A composite of four contrast enhanced, 5-mm thick, CT images from superior (a) to inferior (d), in a 55-year-oldwoman with left mid-abdominal pain and vomiting. The appendix with its enhanced wall (large black arrows) is visibleto the left of midline superiorly (a and b), and in the midline more inferiorly (c). Its more proximal portion is obscured byadjacent bowel (j, d). Periappendiceal (small arrows) and mesenteric (open arrow) edema are noted superiorly (a and b),but its effect on adjacent jejunum (j) is not clearly shown.
allowing differentiation of ischemic segments within In two of 16 patients with delayed surgery, the finalpathologic findings (“lymphoid hyperplasia,” “nor-the appendiceal wall from partial volume artifacts.
Focal loss of wall enhancement or wall continuity, mal appendix”) suggested that the initial CT diagno-ses of acute appendicitis may have been falsely posi-and focal thinning proved to be relatively reliable
CECT signs of necrotizing appendicitis (Table 4). tive (Table 5). It seems just as likely in our opinionthat these are cases of healed appendicitis. The con-Subsequent analysis also showed that all seven cases
with a “double ring” of wall enhancement had necro- cept of chronic, recurrent appendicitis is well de-scribed in the published literature (20, 25, 29, 32,tizing appendicitis. This preliminary observation re-
quires further future verification. Nearly three quar- 51–53). Since appendicitis may resolve spontane-ously, it may well have healed after antibiotic ther-ters of patients with CT signs of acute appendicitis
and an appendicolith had appendiceal abscesses apy in our two cases.The overlap of lymphoid hyperplasia with appendi-and/or necrotizing appendicitis. Thus the old clini-
cal maxim that appendicoliths are associated with a citis in some cases (Figures 9, 10, and 13) is probablymore than coincidental. The appendiceal mucosa ismore virulent acute appendicitis (8, 49) seems to apply
as well to the tiny appendicoliths (2–8 mm diameter) rich in lymphatic tissue in its lamina propria, espe-cially in young individuals (48). Lymphoid hyperpla-detected with thin section CT in this series. Overall a
reliable CT diagnosis of necrotizing appendicitis may sia due to bacterial or viral infections may impinge onthe appendiceal lumen, and cause obstruction withhave clinical significance, as appendiceal necrosis sug-
gests the need for early surgical intervention. secondary appendicitis (6, 49, 50, 54). The lymphoid

266 CHOI ET AL. CLINICAL IMAGING VOL. 22, NO. 4
FIGURE 12. Same patient as in Figure 11. Left lateral decubitus CT scans, obtained after air distention of the colon, dis-played conventionally, clearly show the attachment of the appendix (A) to the cecum (d), and its course superiorly and tothe left (large white arrows, a–c). Sigmoid colon (sig). Edema of periappendiceal fat (small arrow, a and b). Focal thickeningand angulation of adjacent jejunum (curved arrow, a and b) with secondary partial small bowel obstruction. Findings wereconfirmed at surgery 2 hours later.
hyperplasia which was noted in our single false posi- pendicitis with minimal wall thickening, or for im-tive CECT scan (Figure 13), has been reported pre- aging appendices which are obscured by overlying gasviously in association with Campylobacter enteritis or fat, or by marked abdominal wall tenderness and(55), and may have accounted in part for the wall en- guarding (46). The results are not representative ofhancement. An acute “endoappendicitis” involving sonography as a whole. This is primarily a study ofonly the mucosa may accompany Campylobacter en- appendiceal CT and does not include many patientsteritis (55). In our case, however, predominant who were referred initially and diagnosed correctlylymphoid hyperplasia was superimposed on chronic by US alone, without subsequent CT scanning.appendicitis with small fecaliths.
In our case of granulomatous appendicitis, theTABLE 3. Necrotizing Appendicitis: CECTcorrect CT diagnosis was based on the presence ofDiagnostic Criteriaother foci of small and large bowel inflammation,
and not on the appearances of the appendix alone No. of False positiveCT Sign Figure cases diagnosis(Figure 14). It seems unlikely that CT can differenti-
ate the more common form of isolated granuloma- Focal loss wall enhancement 1, 4 33 4tous appendicitis, which is not associated with Focal loss wall continuity 3, 5 27 1
Focal wall thinning 6 17 2Crohn’s disease (56, 57), from classic appendicitis.Extraluminal air, no abscess 5 11 0The lower accuracy, sensitivity, and specificity ofPeriappendiceal abscess 4, 7 24a 0US—relative to CT—in the subgroup of 17 patients in
a Includes three cases with nonvisualized appendix.this series reflects its limitations for detecting early ap-

267JULY/AUGUST 1998 CT IN ACUTE APPENDICITIS
FIGURE 13. False positive CT for acute appendicitis. Acomposite of four contrast enhanced, 5-mm thick, CT im-ages from superior (a) to inferior (d), in a 16-year-old womanshows an enhanced appendiceal wall (black arrows) sur-rounding an air containing lumen superiorly (b) and afluid containing lumen inferiorly (c and d). Periappendi-ceal edema (small arrows). Tiny appendicoliths (f) at theappendiceal base (d). Moderate edema and hyperemia ofthe cecum (open arrow, b) and enhanced, hyperemic mu-cosa (black arrowheads, a) in a thickened ascending colonsuperiorly. Enteritis was considered clinically, but the lo-calization of direct and rebound tenderness to a noncom-pressible appendix on sonography (large white arrow, e),combined with the CT findings of appendiceal hyperemiaand surrounding edema, led to the radiographic diagnosisof primary appendicitis. At appendectomy several hourslater, the appendix did not appear acutely inflamed. Patho-logical exam revealed lymphoid hyperplasia and chronicappendicitis at the tip, but no acute appendicitis. Stoolculture was subsequently positive for Campylobacter.
The wide variety of associated CT findings in pa- diagnoses such as granulomatous appendicitis (Fig-ure 14), pyelonephritis (Figure 16), ureteral stone,tients with appendicitis demonstrates the effective-
ness of this method for imaging periappendiceal tis- ovarian torsion, pancreatitis, diverticulitis, smallbowel obstruction, and mesenteric adenitis. Of par-sues and organs. Thus it is possible for CT not only to
delineate the extent of disease, but to make specific ticular interest is the relatively high prevalence of ce-

268 CHOI ET AL. CLINICAL IMAGING VOL. 22, NO. 4
TABLE 4. Necrotizing Appendicitis: CECT in 105 duce significantly the rate of unnecessary laparot-Proven Casesa
omy for clinically suspected acute appendicitis.No. of
Diagnosis casesREFERENCES
Accuracy 90/105 5 86%True positives 61 Sensitivity 61/69 5 88% 1. Chang FC, Hogle HH, Welling DR. The fate of the negative ap-
pendix. Am J Surgery 1973;126:752–754.False negatives 8 Positive Pred Value 61/68 5 90%False positives 7 Specificity 29/36 5 81% 2. Lewis FR, Holcroft JW, Boey J, Dunphy E. Appendicitis. ArchTrue negatives 29 Negative Pred Value 29/37 5 78% Surgery 1975;110:677–684.
3. Jess P, Bjerregaard B, Brynitz S, Holst-Christensen J, Kalaja E,a Necrotizing appendicitis at pathology and/or perforation at surgery.Lund-Kristensen J. Acute appendicitis. Prospective trial con-cerning diagnostic accuracy and complications. Am J Surg1981;141:232–234.
4. Dunn ER, Moore EE, Elerding SC, Murphy JR. The unneces-sary laparatomy for appendicitis—can it be decreased? Amer-ican Surgeon 1982;48(7):320–323.cal and ileal edema, which was moderate to severe in
5. Williams GR. Presidential address: a history of appendicitis.26% and 9% of the cases, respectively. This findingAnnals of Surgery 1983;197:495–497.should not detract from the diagnosis of primary
6. Buchman TG, Zuidema GD. Reasons for delay of the diagnosisacute appendicitis, in the presence of appendicealof acute appendicitis. Surgery Gynecol Obstet 1984;158:260–
wall enhancement and/or maximal tenderness. 266.It must be emphasized that this is not an exhaus- 7. Berry J, Malt RA. Appendicitis near its centenary. Ann Sur-
gery 1984;200:567–575.tive evaluation of CT for all patients with acute ap-8. Jones B, Fishman EK, Siegelman SS. Computed tomographypendicitis. Patients with a clear clinical diagnosis of
and appendiceal abscess: special applicability in the elderly.this entity went directly to surgery without CT im-J Comput Assist Tomogr 1983;7(3):434–438.
aging, as did those with equivocal clinical but clear9. Gale ME, Birnbaum S, Gerzof SC, Sloan G, Johnson WC, Rob-
US diagnoses of acute appendicitis. Since only pa- bins AH. CT appearance of appendicitis and its local compli-cations. J Comput Assist Tomogr 1985;9(1):34–37.tients with surgical verification were included in
10. Balthazar EJ, Megibow AJ, Hulnick D, Gordon RB, Naidichthis study, the true percentages of false positive andDP, Beranbaum ER. CT of appendicitis. AJR 1986;147:705–false negative CT diagnoses are unknown, as there is710.
no documentation for those who were not treated 11. Balthazar EJ, Megibow AJ, Gordon RB, Whelan CA, Hulnicksurgically. Nevertheless, CT seems to be a powerful D. Computed tomography of the abnormal appendix. J Com-
put Assist Tomogr 1988;12(4):595–601.tool for imaging the appendix in patients with equiv-12. Balthazar EJ, Gordon RB. CT of appendicitis. Seminars in US,ocal clinical diagnoses of acute appendicitis, espe-
CT, & MRI 1989;10(4):326–340.cially if thin sections and intravenous contrast en-13. Gaeta M, Volta S, Minutoli A, Bartiroma G, Pandolfo I. Four-hancement are used. Acute appendicitis can be nier gangrene caused by a perforated retroperitoneal appen-
diagnosed with accuracy and positive predictive dix: CT demonstration. AJR 1991;156:341–342.value of 99%, while necrotizing appendicitis is diag- 14. Grosskreutz S, Goff WB, Balsara Z, Burkhard TK. CT of the
normal appendix. J Comput Assist Tomogr 1991;15(4):575–nosable with accuracy and positive predictive value577.of 86% and 90%, respectively. The use of CT in cases
15. Malone AJ, Wolf CR, Malmed AS, Melliere BF. Diagnosis ofwhere the clinical diagnosis is equivocal and US is acute appendicitis: value of unenhanced CT. AJR 1993;160:
763–766.either nondiagnostic or difficult to perform, can re-
TABLE 5. Delayed Surgerya in 16 Cases with Positive CT for Acute Appendicitis
No. of cases CT diagnosis Surgery diagnosis Pathology diagnosis
4 AA, no perforation Neg appendix (2) Neg appendix (1)Periappendiceal thickening (2) LH (1)
LH 1 Subacute inflammation (1)Chronic periappendicitis (1)
11 AA 1 perforation and abscess Thick appendix and Periappendix (8) Chronic inflammation (8)Phlegmon/abscess (2) Chronic 1 Gr3 AA (3)Necrotic stump (1)
1 Fecalith 1 periappendix infilt Periappendiceal thickening (1) Chronic 1 Gr1 AA (1)
Abbreviations: AA 5 acute appendicitis; LH 5 lymphoid hyperplasia.a Surgery 14–191 days, median 52 days after CT scan.

269JULY/AUGUST 1998 CT IN ACUTE APPENDICITIS
FIGURE 14. Granulomatous appendicitis. A composite of four noncontrast enhanced CT images (NECT) from superior (a)to inferior (d), shows a clearly thickened appendix with a hyperdense wall (large white arrow, b), thickened periappendi-ceal fat (small white arrows) and posterior peritoneum (P). The wall thickening of cecum (C), ascending colon (AC), sigmoidcolon (SC), and terminal ileum (TI) is considerably out of proportion to the relatively minor appendiceal changes. Skip areasof relatively normal colon were observed. Granulomatous disease of the small bowel and colon, with secondary involve-ment of the appendix were diagnosed, and confirmed at surgery and pathology 3 days later.
16. Wong CH, Trinh TM, Robbins AN, Rowen SJ, Cohen AJ. Diag- entiated from appendicitis using graded-compression sonog-raphy. AJR 1989;152:1229–1230.nosis of appendicitis: imaging findings in patients with atypi-
cal clinical features. AJR 1993;161:1199–1203. 25. Abu-Yousef MM, Franken EA. An overview of graded com-17. Balthazar EJ, Megibow AJ, Siegel SE, Birnbaum BA. Appendi- pression sonography in the diagnosis of acute appendicitis.
citis: prospective evaluation with high-resolution CT. Radiol- Semin US, CT, and MR 1989;10(4):352–363.ogy 1991;180:21–24. 26. Borushok KF, Jeffrey RB, Laing FC, Townsend RR. Sono-
18. Puylaert JBCM. Acute appendicitis: US evaluation using graphic diagnosis of perforation in patients with acute appen-graded compression. Radiology 1986;158:355–360. dicitis. AJR 1990;154:275–278.
19. Abu-Yousef MM, Bleicher JJ, Maher JW, Urdaneta LF, Fran- 27. Worrell JA, Drolshagen LF, Kelly TC, Hunton DW, Durmonken EA, Metcalf AM. High resolution sonography of acute ap- GR, Fleischer AC. Graded compression ultrasound in the di-penditicis. AJR 1987;149:53–58. agnosis of appendicitis—a comparison of diagnostic criteria.
J Ultrasound Med 1990;9:145–150.20. Jeffrey RB, Laing FC, Lewis FR. Acute appendicitis: high-reso-lution real-time US findings. Radiology 1987;163:11–14. 28. Brown JJ. Acute appendicitis: the radiologist’s role. Radiology
1991;180:13–14.21. Adams DH, Fine C, Brooks DC. High-resolution real time ul-trasonography. Amer J of Surg 1988;155(1):93–97. 29. Rioux M. Sonographic detection of the normal and abnormal
appendix. AJR 1992;158:773–778.22. Jeffrey RB, Laing FC, Townsend RR. Acute appendicitis: sono-graphic criteria based on 250 cases. Radiology 1988;167:327– 30. Lim HK, Bae SH, Seo GS. Diagnosis of acute appendicitis in329. pregnant women: value of sonography. AJR 1992;159:539–
542.23. Gaensler EHL, Jeffrey RB, Laing FC, Townsend RR. Sonogra-phy in patients with suspected acute appendicitis: value in 31. Chesbrough RM, Burkhard TK, Balsara ZN, Goff WB, Davisestablishing alternative diagnosis. AJR 1989;152:49–51. DJ. Self-localization in US of appendicitis: an addition to
graded compression. Radiology 1993;187:349–351.24. Townsend RR, Jeffrey B, Laing FC. Cecal diverticulitis differ-

270 CHOI ET AL. CLINICAL IMAGING VOL. 22, NO. 4
FIGURE 15. Appendicolith obscured by intravenous and oral contrast. Contrast enhanced 5-mm CT scan in a 38-year-oldwoman with recurrent right lower quadrant pain shows apparent thickening of the proximal appendix (large arrow, a), witha bright pinpoint lumen. There is slight thickening of the connective tissue septa in adjacent fat (small arrows, a), but nocontiguous periappendiceal edema. The distal appendix contained intraluminal contrast and air (open arrow), precludingproximal obstruction. Repeat 5-mm CT scan was performed 20 months later for recurring pain, without oral or intravenouscontrast enhancement (b). A doughnut-shaped appendicloth is now evident in the proximal appendix (arrow, b). Its air con-taining lumen was filled with luminal contrast in a, while its faint calcifications were obscured by intravenous contrast,leading to the mistaken impression of focal wall thickening in a. The remainder of the appendix remained unremarkable.Findings were confirmed at subsequent appendectomy.
32. Jeffrey RB, Jain KA, Nghiem HV. Sonographic diagnosis of mal jejunum: a new sign for acute appendicitis. Gastrointesti-nal Radiology 1989;14(2):172–175.acute appendicitis: interpretive pitfalls. AJR 1994;162:55–59.
43. Garcia CJ, Rosenfield NS. The barium enema in the diagnosis33. Kao SCS, Smith WL, Abu-Yousef MM, Franken EA, Sato Y,of acute appendicitis. Seminars in US, CT, and MR 1989;Kimura K, Soper RT. Acute appendicitis in children: sono-10(4):314–320.graphic findings. AJR 1989;153:375–379.
44. El Ferzli G, Ozuner G, Davidson PG, Isenberg JS, Redmond P,34. Slovis TL, Haller JO, Cohen HL, Berdon WE, Watts FB. Com-Worth MH. Barium enema in the diagnosis of acute appendi-plicated appendiceal inflammatory disease in children: py-citis. Surg Gynecol Obstet 1990;171:40–42.lephlebitis and liver abscess. Radiology 1989;171:823–825.
45. Shust N, Blane CE, Oldham KT. Perforation associated with35. Wong CNG, Yaghmai I. Unusual sonographic appearance a barium enema in acute appendicitis. Pediatric Radiol 1993;
perforated appendiceal abscess. Pediatric Radiol 1989;19: 23:289–290.335–336.
46. Balthazar EJ, Birnbaum BA, Yee J, Megibow AJ, Roshkow J,36. Ceres L, Alonso I, Lopez P, Parra G. Echeverry J. Ultrasound Gray C. Acute appenditicis: CT and US Correlation in 100 pa-
study of acute appendicitis in children with emphasis upon tients. Abdominal and Gastrointestional Radiology 1994;190:the diagnosis of retrocecal appendicitis. Pediatric Radiol 31–35.1990;20:258–261.
47. Ramsden WH, Mannion AJ, Simpkins KC, DeDombal FT. Is37. Sivit CJ, Newman KD, Boenning DA, et al. Appendicitis: use- the appendix where you think it is and if not does it matter?
Clinical Radiology 1993;47:100–103.fulness of US in diagnosis in a pediatric population. PediatricRadiol 1992;185:549–552. 48. Spear R, Kimmey MB, Wang KY, Sillery JK, Benjamin DR,
Sawin RS. Appendiceal US scans: histologic correlation. Ra-38. Siegel MJ. Acute appendicitis in childhood: the role of US.diology 1992;183:831–834.Radiology 1992;185:341–342.
49. Butler C. Surgical pathology of acute appendicitis. Human Pa-39. Hayden CK, Kuchelmeister J, Lipscomb TS. Sonography ofthology 1981;12(10):870–878.acute appendicitis in childhood: perforation versus nonperfo-
50. Arnbjornsson E, Bengmark S. Obstruction of the appendix lu-ration. J Ultrasound Med 1992;11:209–216.men in relation to pathogenesis of acute appendicitis. Acta
40. Quillin SP, Siegel MJ. Appendicitis: efficacy of color Doppler Chir Scand 1983;149:789–791.sonography. Pediatric Radiol 1994;191:557–560.
51. Grossman EJ. Chronic appendicitis. Surg Gynecol Obstet41. Brooks DW, Killen DA. Roentgenographic findings in acute 1978;146:596–598.
appendicitis. Surgery 1965;57(3):377–384.52. Lee AW, Bell LRM, Griffen WO. Recurrent appendiceal colic.
Surg Gynecol Obstet 1985;161:21–24.42. Mowji PJ, Jones MD, Cohen AJ. Localized ileus of the proxi-

271JULY/AUGUST 1998 CT IN ACUTE APPENDICITIS
FIGURE 16. Pyelonephritis mimicking appendicitis. Composite of four contrast enhanced CT scans from superior (a) toinferior (b) in a 30-year-old woman with persistent right lower quadrant pain, despite antibiotic therapy for pyelonephritis.The appendix (large white arrows) ascends medial to the cecum (C), in contiguity to a low lying right kidney (RK). Thereis periappendiceal and perirenal edema (small white arrows). A segmental focus of diminished nephrogram (open blackarrow, a) is consistent with acute bacterial nephritis. The possibility of associated appendicitis arose cliniclly because ofpersistent pain in the region, but a sonogram showed maximal tenderness over the right kidney, and not the appendix. Peri-appendiceal edema secondary to pyelonephritis was diagnosed radiographically, and was confirmed by appendectomy.
53. Savrin RA, Clausen K, Martin EW. Chronic and recurrent ap- 56. Allen DC, Biggart JD. Granulomatous disease in the vermi-pendicitis. Am J Surgery 1979;137:355–357. form appendix. J Clin Pathol 1983;36:632–638.
54. Reif RM. Viral appendicitis. Human Pathology 1981;12(2): 57. Dudley TH, Dean PJ. Idiopathic granulomatous appendicitis193–196. or Crohn’s disease of the appendix revisited. Human Pathol-
ogy 1993;24(6):595–601.55. Van Spreeuwel JP, Lindeman J, Bax R, Elbers HJR, Sybrandy R,Meijer CJLM. Campylobacter-associated appendicitis: preva- 58. Williams PL, Warwick R (eds). Gray’s Anatomy. 36th Edition.lence and clinicopathologic features. Pathology Annual 1987; Philadelphia: WB Saunders 1980; Fig 6,89,p. 716.22(1):55–56.