Ingestible gastrointestinal sampling devices: state-of-the-art and future directions
16
Critical Reviews TM in Biomedical Engineering, 42(1): 1-15 (2014) 1 0278-940X/14/$35.00 © 2014 Begell House, Inc. www.begellhouse.com Ingestible Gastrointestinal Sampling Devices: State-of-the-Art and Future Directions Yaw Amoako-Tuffour 1, * Mitchell L. Jones 1,2, * Nabil Shalabi, 3 Alain Labbé, 2 Srikar Vengallatore, 3 & Satya Prakash 1,2, ** 1 Biomedical Technology and Cell Therapy Research Laboratory, Dept. of Biomedical Engineering, Faculty of Medicine, McGill University, 3775 University Street, Montreal, Quebec, H3A2B4, Canada 2 Micropharma Limited, 4200 St-Laurent Blvd, 4th Floor, Unit 409, Montreal, Quebec, H2W 2R2, Canada 3 Department of Mechanical Engineering, McGill University, 817 Sherbrooke Street West, Montreal, Quebec, H3A2K6, Canada * Equal contributors. **Address all correspondence to: Satya Prakash; Biomedical Technology and Cell Therapy Research Laboratory, Dept. of Biomedical Engineering, Faculty of Medicine, McGill University, 3775 University Street, Montreal, Quebec, H3A2B4, Canada; Tel: 1-514-398-3676; Fax: 1-514-398-7461; Email: [email protected]. ABSTRACT: Despite the significant contribution of gastrointestinal diseases to the global disease burden and the increasing recognition of the role played by the intestinal microbiota in human health and disease states, conventional methods of exploring and collecting samples from the gastrointestinal tract remain invasive, resource intensive, and often unable to capture all the information contained in these heterogeneous samples. A new class of gastrointestinal sampling capsules is emerging in the literature, which contains the components required for an autonomous intra-luminal device and preserves the spatial and temporal information of the gastrointestinal samples. In this paper, we identify the primary design requirements for gastrointestinal sampling capsules, and we review the state-of-the-art for different components and functionalities. We also suggest two design concepts, and we highlight future directions for this class of biomedical devices. KEY WORDS: Autonomous ingestible device, electromechanical capsule, luminal intestinal content collection. I. INTRODUCTION Gastrointestinal diseases comprise a substantial por- tion of the global disease burden. 1,2 In North Amer- ica and Europe, gastrointestinal cancers account for 25% of all cancer deaths. 3 Bacterial populations in the gastrointestinal tract also play an important, though poorly understood, role in gastrointestinal and host physiology that has implications in meta- bolic diseases and obesity, which are both signifi- cant contributors to the disease burden. 4–7 As the primary channel through which materials enter and exit the human body, the gastrointestinal (GI) tract, or alimentary canal, is a large repository of information. Histological samples (i.e., tissue and mucosal) contain information on the disease state of the GI tract itself. Samples of its contents, investi- gated with analytic techniques such as quantitative polymerase chain reaction (qPCR), 16S pyrose- quencing, and mass spectrometry may reveal bio- markers from various locations throughout the body through marked increases or decreases in known analytes due to metabolic pathways being perturbed by disease. These histological, morphological, and biochemical indicators of disease have historically been collected through fecal sampling, visualization, and various endoscopic-assisted biopsy techniques. Though effective, these techniques are invasive and are often incapable of retrieving physical samples from the entirety of the small intestine. In the case of stool samples, spatial and temporal information are poorly preserved. Less invasive means of exploring the GI tract would increase the frequency at which these investigations could be conducted and could facilitate high-throughput screening (HTS) required to study and identify new biomarkers.
-
Upload
independent -
Category
Documents
-
view
2 -
download
0
Transcript of Ingestible gastrointestinal sampling devices: state-of-the-art and future directions

Critical ReviewsTM in Biomedical Engineering, 42(1): 1-15 (2014)
10278-940X/14/$35.00 © 2014 Begell House, Inc. www.begellhouse.com
Ingestible Gastrointestinal Sampling Devices: State-of-the-Art and Future Directions Yaw Amoako-Tuffour1,* Mitchell L. Jones1,2,* Nabil Shalabi,3 Alain Labbé,2 Srikar Vengallatore,3 & Satya Prakash1,2,**
1Biomedical Technology and Cell Therapy Research Laboratory, Dept. of Biomedical Engineering, Faculty of Medicine, McGill University, 3775 University Street, Montreal, Quebec, H3A2B4, Canada 2Micropharma Limited, 4200 St-Laurent Blvd, 4th Floor, Unit 409, Montreal, Quebec, H2W 2R2, Canada3Department of Mechanical Engineering, McGill University, 817 Sherbrooke Street West, Montreal, Quebec, H3A2K6, Canada
* Equal contributors. **Address all correspondence to: Satya Prakash; Biomedical Technology and Cell Therapy Research Laboratory, Dept. of Biomedical Engineering, Faculty of Medicine, McGill University, 3775 University Street, Montreal, Quebec, H3A2B4, Canada; Tel: 1-514-398-3676; Fax: 1-514-398-7461; Email: [email protected].
ABSTRACT: Despite the significant contribution of gastrointestinal diseases to the global disease burden and the increasing recognition of the role played by the intestinal microbiota in human health and disease states, conventional methods of exploring and collecting samples from the gastrointestinal tract remain invasive, resource intensive, and often unable to capture all the information contained in these heterogeneous samples. A new class of gastrointestinal sampling capsules is emerging in the literature, which contains the components required for an autonomous intra-luminal device and preserves the spatial and temporal information of the gastrointestinal samples. In this paper, we identify the primary design requirements for gastrointestinal sampling capsules, and we review the state-of-the-art for different components and functionalities. We also suggest two design concepts, and we highlight future directions for this class of biomedical devices.
KEY WORDS: Autonomous ingestible device, electromechanical capsule, luminal intestinal content collection.
I. INTRODUCTION
Gastrointestinal diseases comprise a substantial por-tion of the global disease burden.1,2 In North Amer-ica and Europe, gastrointestinal cancers account for 25% of all cancer deaths.3 Bacterial populations in the gastrointestinal tract also play an important, though poorly understood, role in gastrointestinal and host physiology that has implications in meta-bolic diseases and obesity, which are both signifi-cant contributors to the disease burden.4–7
As the primary channel through which materials enter and exit the human body, the gastrointestinal (GI) tract, or alimentary canal, is a large repository of information. Histological samples (i.e., tissue and mucosal) contain information on the disease state of the GI tract itself. Samples of its contents, investi-gated with analytic techniques such as quantitative
polymerase chain reaction (qPCR), 16S pyrose-quencing, and mass spectrometry may reveal bio-markers from various locations throughout the body through marked increases or decreases in known analytes due to metabolic pathways being perturbed by disease. These histological, morphological, and biochemical indicators of disease have historically been collected through fecal sampling, visualization, and various endoscopic-assisted biopsy techniques. Though effective, these techniques are invasive and are often incapable of retrieving physical samples from the entirety of the small intestine. In the case of stool samples, spatial and temporal information are poorly preserved. Less invasive means of exploring the GI tract would increase the frequency at which these investigations could be conducted and could facilitate high-throughput screening (HTS) required to study and identify new biomarkers.

Critical ReviewsTM in Biomedical Engineering
Amoako-Tuffour et al.2
In the year 2000, the first commercial endo-scopic capsule was made available by Given Imag-ing (Yoqneam, Israel).8,9 This capsule made it pos-sible to non-invasively image the GI tract, including the entirety of the small intestine, a location never before fully accessed by conventional tethered en-doscopic devices.8,9 Since then, researchers have been developing technologies capable of perform-ing a multitude of non-invasive procedures in the GI, such as drug delivery and tissue biopsy, which require more versatile control over the locomotion and positioning of devices in the GI tract.9–14 One application that has received relatively little atten-tion is the ability to collect the physical luminal content and exfoliates from the GI tract. These ma-terials are of interest because they contain elements of the microbiome and metabolome, which are potential biomarkers for disease. Biomarkers may indicate the future risk, or current progress, of a par-ticular disease prior to the development of clinical symptoms and thus increase the likelihood of inter-ventional success. The study of this ecosystem and its relation to various disease states could lead to a decrease in morbidity associated with these disease states. Collecting digestive fluids using stand-alone capsules has been mentioned only briefly in the lit-erature.10,15 To the best of our knowledge, only one stand-alone capsular device exists currently that is capable of performing fluid collection with results for in vivo sampling.15 However, numerous designs have been proposed for such medical devices and several of the disparate components required are ac-tively being developed. In this paper, we review the present state-of-the-art in ingestible gastrointestinal sampling devices.
II. GASTROINTESTINAL SAMPLING DEVICE DESIGN
Ingestible medical devices intended for clinical use must comply with guidelines set by the governing agencies in the target market (e.g., the Food and Drug Administration in the United States). These guidelines specify the materials and technologies that may be used in the device, minimum safety standards, as well as limitations to its operation,
such as acceptable levels of interference that it may generate or receive. Paramount in these guidelines is the demonstration that the device causes no harm during the course of its operation and can perform, to a specified degree, its intended functions. For minimally invasive gastrointestinal sampling de-vices, these guidelines translate into the following general requirements: (1) devices should be ingest-ible, capable of transiting safely though the GI, and retrievable; (2) devices should be designed to col-lect biologically relevant samples, whether liquid, solid, or a heterogeneous mixture, which may later undergo conventional and advanced analytical tech-niques; (3) sampling devices should be biocompat-ible and maintain structural integrity upon exposure to digestive and other bodily fluids; (4) for clinical use, medical devices should have fault tolerance in-corporated into the physical design and underlying software; and (5) the sample collection mechanism should not damage the structures of the GI tract.16
A. Size and Shape
The pyloric sphincter, the most restrictive fea-ture along the length of the human gastrointesti-nal tract, limits the dimensions of non-degrading ingestible devices.17 However, the risk of capsule retention is present throughout the length of the GI, and may be elevated in patients with clinical histo-ries of intestinal stenosis and Crohn’s disease.18,19 Commercial endoscopic capsules and “smart” pills designed for the adult population range in length from 18 to 35 mm and diameter from 6 to 12 mm. The incidence of capsule retention for devices within these dimensions is reported to be below 2%.20,21 The lower limit for the dimensions of gas-trointestinal sampling devices is the volume of bio-logically relevant sample required to perform the desired analysis, which depends on the application under consideration. For instance, sample volumes of 10–50 µL are typical for qPCR.22
B. Materials
The definition of biocompatibility depends on the nature of body contact (an ingestible capsule

Volume 42, Number 1, 2014
Ingestible Gastrointestinal Sampling Devices: State-of-the-Art and Future Directions 3
is considered a “surface device” in contact with a mucosal membrane) and the contact duration (in this case a prolonged >24 h < 30 d period of time).23 A biocompatible designation describes the absence of an adverse reaction, immunological or chemical, due to a given material in the pres-ence of human bodily fluids.24,25 These materials may range from degradable polymeric coatings, fluoropolymers, and elastomers, to durable ther-moplastics, metal and glass.26–30 Durable materials are preferred for the exterior of devices that are required to retain function and structural integrity throughout the length of the GI tract as is the case for endoscopic capsules, monitoring pills, and gas-trointestinal sampling devices. The use of different materials for various internal components may en-able functionalization of specific surfaces for in-teraction with proteins, antibodies, and other bio-markers.31 Compliant (elastic) materials have also been incorporated in capsule designs as protective diaphragms for pressure transducers, deformable reservoirs, and energy storage devices.
C. Control
The human GI tract is divided into anatomically and physiologically distinct segments with unique characteristics, functions, and pathologies. In cer-tain applications, the collection of eukaryotic cells leaving the sphincter of Oddi may be used to di-agnose pancreatic disease, whereas collection just after the ileocecal valve may be used to diagnose colonic disease. In other applications, mucosal samples may be used to assess coeliac changes. Thus, the control of sample collection is of central importance in the design of gastrointestinal sam-pling devices. Collection mechanisms aided by endoscopic imaging are under the direct control of the physician. Upon visualizing the desired sample location, the physician is able to manually actuate the collection mechanism. In contrast, autonomous sample collection methods may employ mechani-cal systems, chemical compounds, or microcon-troller units (MCUs) to control sample collection. A common control method for gastrointestinal sampling devices is the use of phase-change trig-
gers sensitive to specific chemicals and intestinal geographies.32,33 Enteric compounds that undergo significant physical changes upon exposure to spe-cific chemical compounds, enzymatic action, or environmental conditions are often used as trig-gers.32 Such compounds are best suited for appli-cations requiring relatively low precision, such as drug delivery, in which compound degradation and absorption may span several hours.33 Shape memory alloys (SMAs) may also be used in this manner; however, microcontroller units (MCUs) are typically required to initiate the resistive heat-ing required for phase change and mechanical actuation.34 Electromechnical systems controlled by embedded MCUs offer a high level of preci-sion and autonomy. These systems may be pre-programmed to react to specified environmental conditions, time, or location; they can be triggered externally upon reaching the target location; and they respond on the scale of microseconds.35 The major design considerations for an electromechan-ical sampling device are the power consumption and power supply, localization methods, means of communication with the external world, capacity for environmental awareness, and its sample col-lection mechanism.
D. Localization
Accurate device localization and sample timing are critical to determining the site of biopsy and inter-vention, rate and location of metabolic processes, and the bacterial profile of the GI tract. These de-tails can be used to target locations for sampling before ingesting the capsule or to trace the source of samples after testing. Three-dimensional track-ing of devices within the GI in real-time has proven challenging, as the intestines have few fixed ana-tomical locations and move freely within the peri-toneum.36 Further adding to this challenge is the patient’s natural movement over the course of gas-trointestinal transit. Radiographic methods, able to visualize through soft tissue, are inappropriate for continuous or intermittent imaging over the many hours (>30) required for device transit.37 The long duration of GI transit also makes impractical

Critical ReviewsTM in Biomedical Engineering
Amoako-Tuffour et al.4
all methods requiring the continuous presence of human operators. For these reasons, autonomous localization methods are preferred for tracking devices inside the tract using timing, computer vi-sion, triangulation methods, inertial navigation and external monitoring.38–42 The most basic form of localization within the GI uses typical gastric and small bowel transit times as guidelines for deter-mining the physical location of the pill at a given time point. This method can be inaccurate because the transit times in any individual can vary signifi-cantly from statistical norms. However, it may be possible to standardize transit times through di-etary restriction (e.g., fasting state), bowel prepara-tion, and co-administration with prokinetic agents to help the motion of the device by overcoming stoppages at sphincter regions.9,43
Inertial navigation and positioning systems are based on the integration of measurements from an array of on-board multi-axial accelerometers and gyroscopes.44,45 This method is computationally in-tensive, requiring a large number of measurements as the capsule follows a complicated trajectory in-side the GI.46
Computer vision is being developed as a means to retroactively determine the location of endoscopic capsules. During the course of transit, an endoscopic capsule may take between 40,000 and 60,000 images, which are later reviewed for abnormalities.47 Algorithms based on pattern recognition and texture analysis have been dem-onstrated to accurately segment the GI tract into distinct anatomical regions of interest.47–49 These post-procedural techniques, however, are unable to provide real-time or actionable information to the transiting capsule, thereby preventing targeted sample collection.
A number of triangulation methods, analo-gous to the global positioning system (GPS), have been used to localize ingested capsules in three-dimensional (3D) space.41,42,50 The received signal strength indication (RSSI) uses the ingested device as a radio frequency (RF) emitter and an exter-nal sensor array to measure RF signal strength at fixed locations on the abdomen. The relative signal strengths are then used to calculate the 3D posi-
tion of the device.50 The average error with this method is estimated at approximately 38 mm due to varying signal attenuation by the differing body tissues.10,50 Time of arrival (TOA) is another form of triangulation in which the 3D position of the sampling device is calculated from the difference in reception time of an electromagnetic (EM) sig-nal at three receivers located externally on the ab-domen. A high degree of synchronization (within 1 ns) of the receivers is required to achieve 0.3-m resolution.51 Magnetic tracking is immune to atten-uation by body tissue. The strength of a magnetic field generated by a permanent magnet within the device is detected by a skin-mounted magneto-resistive sensor array to estimate 3D position with precision of approximately 3 mm.10,42 Magnetore-sistive tracking does not increase power consump-tion but is susceptible to interference by external magnetic fields and high-voltage electrical de-vices. Furthermore, the large permanent magnet diminishes potential sampling volume within the device. A general weakness of triangulation meth-ods is the positional error that occurs due to natural body movement.52
Conventional clinical imaging may be used to localize sampling devices. Ultrasound imag-ing is based on ultrasonic pulses transduced on the body’s exterior at low frequencies (100 kHz to 5 MHz) 11 and has been demonstrated as an effective localization method for medical devices within the GI.53 Radioactive tracers may also be placed in compartments within the medical device such that its transit through the GI may be tracked by gamma cameras.54 Imaging methods based on ion-izing radiation such as X-ray are not suitable for continuous device tracking.
E. Locomotion
Gastrointestinal sampling collection techniques based on endoscopy or double-balloon enteroscopy (or any tube-based technique) reach their target lo-cation through the application of force at the prox-imal end of the device. In contrast, the majority of ingestible electromechanical sampling devices reach their target locations, and continue to transit

Volume 42, Number 1, 2014
Ingestible Gastrointestinal Sampling Devices: State-of-the-Art and Future Directions 5
through the GI tract, passively under the force of peristalsis.55–57 Passive locomotion requires no pro-pulsive hardware but may be erratic. A number of active locomotion techniques have been developed for ingestible capsules: (1) micro-mechanical legs, paddles, or propellers;55,58–60 (2) the controlled ex-pansion of compressed gas to provide propulsion;11 or (3) propulsive forces transmitted by an exter-nal system, typically a magnetic field, in which devices have embedded magnets or coatings and are directed with an external magnetic driving de-vice.39,40,61 Furthermore, modifications to the mate-rial surface properties of a device could influence locomotion, such as micropillar polymer arrays coated with viscous oil that could improve adhe-sion to the microvilli of the intestinal mucosa.62–64
Externally driven locomotion systems rely on large magnetic field generators and are impracti-cal over the long course (>30 h) of GI transit.37,39 Locomotion mechanisms internal to the capsule are voluminous. In a 12-legged robotic capsule designed by Quirini et. al., the motors responsible for locomotion alone consumed greater than 20% of the available volume in a capsule sized ~11 × 26 mm.55 With the addition of an internal power supply, mechanical legs, controller, and support-ing mechanisms, little volume is left for physical sample storage or the mechanism used to collect the sample.
F. Environmental Awareness
Environmental sensors provide a means of de-vice localization within the GI tract and facilitate real-time decision making based on the surround-ing environment. Parameters typically measured include the gastrointestinal pH,65 pressure,66 tem-perature,67,68 oxygenation (i.e., measuring dis-solved oxygen), and oxidation/reduction using cyclic voltammetry, and electrical conductivity.8,69 The concentration of hydrogen ions (pH) can be measured using antimony and glass pH electrodes and ion-sensitive field-effect transistors (ISFETs), which have been implemented in a number of ingestible devices, including the SmartPill® GI monitoring system (Given Imaging, Israel) and
the Phillips-Medimetrics device.69–72 Acidity may be useful in monitoring intestinal activity. When combined with time, it can provide localization information for drug delivery or sample acquisi-tion.73 Notably, ISFET pH sensors are sensitive to changes in temperature and must be calibrated at regular intervals to provide accurate pH measure-ments.74
Temperature measurement is performed using thermistors, resistive thermal devices (RTDs), as is the case in the VitalSense® ingestible telemetric physiological monitoring system pill (Mini Mitter Co., Inc., Bend, OR),75 or by monitoring frequency shifts in temperature-sensitive crystals (CorTemp® Pill system by HQ Inc, Palmetto, FL, USA).14 Silicon diode temperature sensors and forward biased pn junctions have also been used for this purpose.69,72
Radiant energy can be a means of environmen-tal sensing for ingested devices. These technolo-gies include fluorescence endoscopy, optical co-herence tomography, confocal micro-endoscopy, light-scattering spectroscopy, Raman spectros-copy, and molecular imaging for optical biopsy or the use of transmission spectroscopy for detecting intestinal bleeding.76,77
G. Communications
Endoscopic and monitoring capsules routinely em-ploy wireless communication to transmit and re-ceive commands and to offload data.78,79 A major design consideration is the extent to which the data transmission rate and transmission distance affect power consumption. Wireless signals from ingest-ible medical devices must not interfere with stan-dard hospital equipment but must be sufficiently robust to overcome external interferences. The dedicated RF communication standard is the Med-ical Implant Communication Service, operating in the 402–405 MHz range, although other Industrial Scientific and Medical bands, such as 433.92 MHz, are acceptable.80,81 Several systems use electric-field propagation that exploits the human body as a conductive medium for data transmission, which may offer higher data rates with lower power con-

Critical ReviewsTM in Biomedical Engineering
Amoako-Tuffour et al.6
sumption than existing RF technologies due to the elimination of power-consuming RF transmission components.14 Infrared communications protocols, such as IrDA, may also be used for short range, line-of-sight, data transfer between ingestible cap-sules and programmers, with marginal additional cost and design complexity.82,83
H. Power Supply
The power supply for electromechanical gastroin-testinal sampling devices may be integrated into the device or disconnected and external to the de-vice. Silver oxide coin cells and lithium polymer batteries are commonly used as internal power supplies for ingestible and implantable medical devices.35,84,85 External power supplies are used to achieve compact designs, to power inaccessible devices such as permanent implants, and to oper-ate devices with high energy consumption. Wire-less energy transmission through biological tissue is achieved by creating an inductive link between an external primary coil (worn around the patient’s torso) and a secondary coil (embedded within the capsule).57,86,87 Excitation of the primary coil in-duces electrical current in the secondary coil, pro-viding power to the device. Thus, external power supplies can lead to compact device designs with extended operational capabilities, but they require significant supporting infrastructure.
I. Sample Collection
Sample collection may be based on active and/or passive mechanisms. Active mechanisms gen-erally provide a high level of control and the po-tential to gather heterogeneous sample material. Passive mechanisms do not require power sup-plies and may be made more compact and basic in their design. For the purposes of this review, active sampling mechanisms are defined as those requir-ing the controlled release of mechanical energy to collect sample from the lumen of the gastrointes-tinal tract. Additionally, sampling in this context refers to the collection of physical material from the intestinal lumen as opposed to environmental
sensing and recording by a medical device during transit. Physical samples may further be subdivid-ed into live tissue, exfoliate, intestinal fluids, and solids.
Several active sampling mechanisms for in-gestible capsular devices have been described in the literature, utilizing shape memory alloys, com-pressed springs, air pressure, motors, and elastic materials to actuate plungers, pistons, and biopsy forceps.88–91 Electric thermoactuators are often used to trigger the release of stored mechanical energy by destroying a degradable material (e.g., nylon monofilament) that holds the actuating el-ement in a “high-energy” state.15 Shape memory alloys are unique in that they undergo conforma-tional changes with the application of electrical current and do not require a secondary trigger to release mechanical energy. A number of micro-pumps have been proposed for fluid sampling and drug dosing in smart pills. These include mechani-cal pumps based on electrostatic and piezoelec-tric forces and non-mechanical pumps based on electrokinetic principles such as electroosmosis.92 Though the mechanical micropumps have been demonstrated to achieve high pressures (31 kPa) and flow rates (850 µL min-1), they require very high supply voltages (200 V) to operate.93 Non-mechanical micropumps or electrokinetic pumps, such as those driven by electro-osmotic, capillary, or electrohydrodynamic forces, require fluid that is polar, free of particulate matter, and non-viscous.92 These requirements are incompatible with the het-erogeneous and highly variable luminal contents of the GI tract.
Passive collection mechanisms include micro-fluidic capillary tubes and the selective exposure of absorptive materials to the fluid of the GI.94,95
III. GASTROINTESTINAL SAMPLING CAPSULES
An intestinal biopsy capsule, popularly known as the Crosby Capsule, was developed by in 1957 to perform jejunal biopsies.88 The device is a stainless steel cylindrical capsule with rounded ends mea-suring 11 mm in diameter and 20 mm in length. A

Volume 42, Number 1, 2014
Ingestible Gastrointestinal Sampling Devices: State-of-the-Art and Future Directions 7
5-mm-diameter aperture on the side of the capsule serves as the port of entry for the mucosal sample, and a separate 2-mm-diameter aperture at the end of the device accommodates polyethylene tubing. At-tached to the external end of the polyethylene tube is a syringe through which pneumatic control of the sampling mechanism is exerted. The sampling mechanism consists of a knife atop a cylindrical block. The cylindrical block is attached to a spring under both torsion and linear compression in its initial state. At the desired site of sample collection (indicated by the length of tubing ingested), the sy-ringe piston is drawn to create a vacuum within the polyethylene tube. This vacuum draws in mucosa through the 5-mm sampling aperture and triggers the release of the cylindrical block. As the block advances, the attached knife rotates and biopsies the mucosa. Though the Crosby Capsule was dem-onstrated to provide biopsies with high diagnostic value in disorders such as Celiac Sprue, Whipple’s Disease, Abetalipoprotinemia, and Agammaglobu-linemia, there were a number of challenges associ-ated with its use,96 including bleeding and perfo-ration.97,98 Additionally, withdrawal of the device from the patient occasionally required the intrave-nous injection of 15 mg propantheline bromide in 10 mL of saline to relax pyloric spasm.99
In 1996, Gu and Gu applied for a patent de-scribing a pill-shaped container with a hollow body, opening, seal, and a vacuum interior.94 Upon reaching the target sampling location, indicated by pH, enzymatic activity, or the presence of a par-ticular chemical compound, the seal would dis-solve, allowing intraluminal contents to enter the storage area. The capsule could be subdivided into as many as three subcompartments, each with its own vacuum, opening, and seal. The seals differ in thickness to vary degradation rates, allowing the administrator to collect samples from different locations along the GI tract. Enteric compounds are also used as seals in microfluidic sampling de-vices. In a patent application by Sprenkels et al., a microfluidic-based GI fluid sampling concept is described that uses capillary forces to draw in samples from the GI.95 Prior to administration, the channels are sealed with enteric compounds sensi-
tive only to the fluids targeted for sampling col-lection. Upon contact with these fluids, the seals dissolve and allow the passage of fluid into the channels under capillary motion. These devices offer passive, solid-state designs that are inde-pendent of external infrastructure. In both design categories, however, no provision is made for re-sealing the chambers following sample collection, and the design remains susceptible to downstream contamination. Furthermore, the designs require a priori knowledge of the target fluids and cannot accommodate variations in physical or chemical composition of intestinal fluid.
Cui et al. designed a sampling capsule using micromechanisms based on microelectromechani-cal systems (MEMS) technologies. The capsule uses miniaturized pistons to elute medication into the GI tract and simultaneously draws luminal content into the sampling chambers.15 At 10.2 mm in diameter and 30 mm in length, the polycarbon-ate capsule elutes an average drug volume of 0.5 ml and captures an average sample volume of 0.2 ml. The position of the device is tracked us-ing a combination of microscale magnets embed-ded in the capsule and a Hall sensor array fixed on a waistcoat worn by the patient. Commands are transmitted to the device from an external RF signal emitter. Three internal silver-oxide batter-ies (1.55 V, 40 mAh, 9.5 mm × 2.09 mm) provide electrical power for operation. This MEMS-based design contains many important elements for au-tonomous gastrointestinal sampling such as GI localization, wireless communication, and large sample volume. However, the device is limited to collecting a single liquid sample that is not isolat-ed from downstream contaminants, and the rela-tively small ports are susceptible to obstruction by particulate matter in the GI tract. These limitations also apply to another mechanical sampling tool, designed by Park et al. in 2008, to perform tis-sue biopsies in the GI.89 The sampling mechanism, which was designed to augment the capabilities of existing endoscopic capsules, consists of a torsion spring that can be released using a resistive heater to locally melt a polymer string; a slider-crank mechanism to convert rotary motion into transla-

Critical ReviewsTM in Biomedical Engineering
Amoako-Tuffour et al.8
tion; and a toothed lance that extends into the lu-men of the GI tract and retracts into the capsule with tissue trapped in its teeth.
A concept for an advanced sampling capsule was described in a 2003 patent application by Tang et al. which utilizes counter-rotating cylindrical blades to collect samples from the lumen of the GI tract.91 This device is designed as an in vivo diag-nostic tool with an on-board micro-spectrometer and biosensors. It uses miniaturized motors in the sample collecting mechanism and has the ability to transmit information wirelessly to an external receiver. To our knowledge, this design has not yet been prototyped and characterized.
Table 1 summarizes the technologies that are currently used or in development for sampling the GI tract.
IV. DEVICE CONCEPTS AND FUTURE DIRECTIONS
The future of GI exploration lies in small, autono-mous sampling devices that can provide research-ers and clinicians with high levels of specificity, localization, and sensitivity. A survey of the litera-ture revealed numerous approaches to achieve this goal. Based on this review, and taking into con-sideration the diverse design requirements listed earlier in this document, we conclude that it is feasible to develop an autonomous gastrointestinal sampling device consisting of an electromechani-cal system controlled by an onboard microproces-sor that will be propelled by peristalsis along the GI tract. The device will be equipped with an in-ternal power supply and its position will be tracked using a combination of transit time and localized environmental changes. Finally, the device will be equipped with an active sampling mechanism to accommodate a diverse set of materials collected from the GI tract. Multiple, and discrete, samples will be collected and isolated from contaminants until their recovery.
Adhering to the precedents established by commercial endoscopic capsules with respect to dimensions, component materials, power supply, and intestinal locomotion allows the develop-
ment of a new sampling capsule to benefit from past and ongoing research on the safety of endo-scopic capsules and their ability to transit safely through the gastrointestinal tract without causing discomfort. Control of the sampling device will be implemented through an onboard Microcontroller Unit (MCU). The MCU will be expandable and interface with communications modules, ADCs, switches, and non-volatile memory. Following the development phase of a GI sampling device, its components may be integrated into an Application Specific Integrated Circuit (ASIC) to further min-iaturize the device.
Three-dimensional localization of a sampling devices using one of the numerous triangulation methodologies such as RSSI, and magnetoresistive tracking, may be of limited value due to the poten-tial for large errors to be introduced by torsional and abdominal movement, individual variability, and intestinal mobility within the abdominal cav-ity. For the purposes of targeted sampling within the GI, greater value may be obtained from the de-tection of transition points along the GI tract and/or fixed anatomical markers. Gastric emptying and colonic emptying times are the most variable com-ponents of GI transit.37 Provided the relatively con-sistent transit time of the small intestine, a basic timing mechanism coupled with an environmental sensing system to detect the transition into and out of the small intestine could be utilized as a totally independent auto-localization system within the capsule. The efficacy of localization techniques may be assessed by radiographic imaging such as scintigraphy.107
Most commercially available endoscopic and environment sensing capsules are intended for sin-gle usage and are not retrieved. As such, ongoing wireless RF communication is required to offload recorded data and images to an external device. The proposed GI sampling capsule, in contrast, must be retrieved to study the sampled contents. The mandatory retrieval of the capsule allows any relevant transit data (e.g., timings, environmental recordings, and error logs) to be stored onboard the device rendering real-time data transmission unnecessary, except when the user wishes to trig-

Volume 42, Number 1, 2014
Ingestible Gastrointestinal Sampling Devices: State-of-the-Art and Future Directions 9
TAB
LE 1
: Rev
iew
of g
astr
oint
estin
al s
ampl
ing
tech
nolo
gies
Tiss
ue a
nd lu
min
al
cont
ent s
ampl
ing
Loca
lizat
ion
Sam
ple
Pow
er
Dim
ensi
ons
Ref
eren
ces
Forc
eps,
net
s, b
aske
ts, s
nare
s,
cyto
logy
bru
sh, fi
ne n
eedl
e as
pi-
ratio
n (F
NA
)(E
ndos
copi
c at
tach
men
ts)
Visu
aliz
atio
n, e
ndos
copi
c gu
idan
ce.
End
osco
pic
ultra
soun
d gu
idan
ce (f
na)
Muc
osa,
mus
cu-
laris
,B
iliar
y st
ones
, po
lyps
, exf
olia
te
Man
ual -
mec
hani
cal
Varia
ble.
~2–5
mm
Leng
th: 1
.8 –
6 m
mS
nare
s: 1
0–33
mm
100,
101
Suc
tion
biop
sy (C
rosb
y ca
psul
e)In
serte
d se
ctio
n le
ngth
Muc
osal
pat
ch, 5
m
m ⦰
Rot
ary
knife
bio
psy.
(oro
phar
ynx
to
ileoc
ecal
val
ve)
Man
ual -
pne
umat
ic~1
1 ×
20 m
m88
Cui
cap
sule
Mag
netic
hal
l sen
sor a
rray
Lum
inal
flui
d
(262
μl)
Ext
erna
l RF
tri
gger
ing
Inte
rnal
(silv
er o
xide
co
in-c
ell)
~10.
2 ×
30 m
m15
Visu
al b
iops
y
End
osco
py, e
nter
osco
py
Visu
aliz
atio
nIm
age,
vid
eoE
xter
nal (
mai
ns)
Dia
met
er: 8
.5–1
2.2
mm
102,
103
End
osco
pic
caps
ules
Com
pute
r vis
ion,
pos
t- tra
nsit
imag
e pr
oces
sing
Imag
e, v
ideo
In
tern
al (s
ilver
oxi
de)
Ext
erna
l (w
irele
ss
trans
mis
sion
)
Dia
met
er: 6
–12
mm
Leng
th: 1
8–35
mm
9,47
,79
Opt
ical
coh
eren
ce to
mog
raph
yVi
sual
izat
ion
Mic
rost
ruct
ure
imag
e, (r
esol
utio
n 1–
15 μ
m)
Ext
erna
l (m
ains
)D
iam
eter
: 8.5
–12.
2 m
m10
4,10
5
Envi
ronm
enta
l sen
sing
Sm
artP
ill® G
I mon
itorin
g sy
stem
, pH
pill
, cor
e te
mpe
ratu
re p
illVi
sual
izat
ion,
tele
met
ryA
cidi
ty (p
H),
tem
-pe
ratu
re, p
ress
ure
Inte
rnal
(bat
tery
)D
iam
eter
: 6–1
2 m
mLe
ngth
: 18–
35 m
m
66,1
06-1
08

Critical ReviewsTM in Biomedical Engineering
Amoako-Tuffour et al.10
ger sampling based on external interpretation of transmitted data. An autonomous device, however, should be able to trigger sampling independently; thus, a communication link is only required imme-diately prior to and following transit. Short-range IR communication could provide this functionality at minimal cost and with moderate design com-plexity. Furthermore, unlike RF, optical commu-nication is not susceptible to interference or mali-cious attacks during transit in the GI tract.109 This ideal device configuration is further described in Table 2.
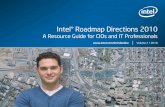
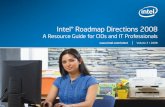
Figures 1 and 2 illustrate what this new class of devices might look like and how they could operate based on the features highlighted in this review (Table 2). The concepts comprise electro-mechanical systems housed in protective plastic enclosures. They feature microcontroller units (MCUs) and communications modules such as RF transceivers. MCUs offer versatility, as their capabilities may be expanded using additional
modules such as Analog-to-Digital Converters (ADCs). ADCs allow a variety of sensors to be incorporated into the system so that the device can be aware of the surrounding intestinal envi-ronment as well as its own orientation and ac-celeration within the intestine. An active sample collection mechanism is implemented using a miniature motor to achieve the necessary level of control over the sampling process and to account for physical and chemical variations in the mate-rials being sampled. Concept A is powered with a lithium polymer battery cell and Concept B is powered with two silver-oxide coin-cell batteries. Each device contains a minimum of three sam-pling chambers, each with a capacity of approxi-mately 100 µL, to ensure a biologically relevant sample quantity for a wide range of analytical processes. Multiple sampling chambers are dis-crete and isolated from contamination to facilitate redundant sampling or distributed sampling with a single capsule.
TABLE 2: Design of an ideal GI sampling device
Specification Examples ReferencesDimensions Length: 18–35 mm
Diameter: 6–12 mmPillCam, SmartPill 9,47,79
Materials (external) Biocompatible thermoplastics and alloys
Polycarbonate,Polyethylene, PEEK, PTFE, PMMA medical
grade silicone, stainless steel
15,25,88
Locomotion Passive, peristaltic pressure Norika, enterion, BRAVO pill,
9,15,79,110,111
Control Onboard MCU, with ADC, radio module, UART/USART, high
current output
ATMEL ATMega48 35,55
Localization Environmental sensing, timing PH-ISFET, solid state manometer, RTD
51
Communications Low-power wireless RF, ANT, infrared 112
Sample Luminal content (liquid, solid;), mucosa, exfoliate
Target size: 3 × 100 µl
Cui drug delivery and sampling pill (> 200 µl)
15,94,95
Power Internal (battery) Silver oxide, lithium, lithium ion
78,84,85

Volume 42, Number 1, 2014
Ingestible Gastrointestinal Sampling Devices: State-of-the-Art and Future Directions 11
V. CONCLUSIONS
With the high disease burden associated with gas-trointestinal ailments and the potential to infer other disease states from biomarkers and the microbi-ome found in the gastrointestinal tract, the need for non-invasive GI sampling techniques is becoming evident. Existing GI exploration techniques such as
endoscopy, colonoscopy, and double-balloon enter-oscopy are capable of collecting luminal and tissue samples for biopsy from much of the digestive tract, but they are invasive, resource-intensive, and thus ill-suited for high-throughput research required to identify novel biomarkers and observe physiologi-cal processes in the GI tract. These limitations, in addition to the very high cost of the medical proce-
FIG. 1: Gastrointestinal sampling pill Concept A
FIG. 2: Gastrointestinal sampling pill Concept B

Critical ReviewsTM in Biomedical Engineering
Amoako-Tuffour et al.12
dures, also make the existing methods unsuitable as easily administered diagnostic, monitoring, and in-tervention tools. The commercial device cost will be highly dependent on the components used, produc-tion volume, regulatory requirements, and other fac-tors. The device-associated cost will, however, be easily offset by the reduction in the cost of medical procedures and the improved quality of the samples collected. Beyond the development of a candidate device, the collected samples must be characterized to ensure that they are representative of the locations targeted for sampling. The continued development of this device class will yield a greater understand-ing of the relationship between the GI contents and various disease states and serve as a powerful re-source in the discovery of disease biomarkers and development of novel therapies.
ACKNOWLEDGMENTS
The authors acknowledge the contributions from Starfish Medical. This work was supported by Mi-cropharma Limited. M.L. Jones and S. Prakash acknowledge a conflict of interest as they are co-founders and shareholders of Micropharma. A. Labbé is employed by Micropharma.
REFERENCES
1. Everhart JE, Ruhl CE. Burden of digestive diseases in the United States part I: overall and upper gastrointestinal diseases. Gastroenterology. 2009 Feb;136(2):376–86.
2. Peery AF, Dellon ES, Lund J, Crockett SD, McGowan CE, Bulsiewicz WJ, Gangarosa LM, Thiny MT, Stizen-berg K, Morgan DR, Ringel Y, Kim HP, Dibonaventura MD, Carroll CF, Allen JK, Cook SF, Sandler RS, Kap-pelman MD, Shaheen NJ.. Burden of gastrointestinal dis-ease in the United States: 2012 update. Gastroenterology. 2012 Nov;143(5):1179–87.
3. Jankowski JA, Odze RD. Biomarkers in gastroenterol-ogy: between hope and hype comes histopathology. Am J Gastroenterol. 2009 May;104(5):1093–6.
4. Cani PD, Neyrinck AM, Fava F, Knauf C, Burcelin RG, Tuohy KM, Gibson GR, Delzenne NM. Selective increases of bifidobacteria in gut microflora improve high-fat-diet-induced diabetes in mice through a mecha-nism associated with endotoxaemia. Diabetologia. 2007 Nov;50(11):2374–83.
5. Neish AS. Microbes in gastrointestinal health and dis-ease. Gastroenterology. 2009 Jan;136(1):65–80.
6. Ouwehand A, Isolauri E, Salminen S. The role of the in-testinal microflora for the development of the immune system in early childhood. Eur J Nutr. 2002 Nov;41 Sup-pl 1:I32–I37.
7. Tang WH, Wang Z, Levison BS, Koeth RA, Britt EB, Fu X, Wu Y, Hazen SL. Intestinal microbial metabolism of phosphatidylcholine and cardiovascular risk. N Engl J Med. 2013 Apr 25;368(17):1575–84.
8. Jesudoss P, Mathewson A, Twomey K, Stam F, Wright WM. A swallowable diagnostic capsule with a direct access sensor using Anisotropic Conductive Adhesive. IEEE Int Reliab Phys Symp Proc. 2011.
9. Moglia A, Menciassi A, Dario P, Cuschieri A. Capsule endoscopy: progress update and challenges ahead. Nat Rev Gastroenterol Hepatol. 2009 Jun;6(6):353–62.
10. Lin L, Rasouli M, Kencana AP, Tan SL, Wong KJ, Ho KY, Phee SJ. Capsule endoscopy-A mechatronics per-spective. Front Mech Eng China. 2011;6(1):33–9.
11. McCaffrey C, Chevalerias O, O’Mathuna C, Twomey K. Swallowable-capsule technology. IEEE Perv Comput. 2008;7(1):23–9.
12. Menciassi A, Quirini M, Dario P. Microrobotics for fu-ture gastrointestinal endoscopy. Minim Invasive Ther Al-lied Technol. 2007;16(2):91–100.
13. Sharma VK. The future is wireless: advances in wireless diagnostic and therapeutic technologies in gastroenterol-ogy. Gastroenterology. 2009 Aug;137(2):434–9.
14. Toennies JL, Tortora G, Simi M, Valdastri P, Webster R. Swallowable medical devices for diagnosis and surgery: the state of the art. Proc Inst Mechan Engineers, Part C: J Mechan Engineer Sci. 2010;224(7):1397–414.
15. Cui J, Zheng X, Hou W, Zhuang Y, Pi X, Yang J. The study of a remote-controlled gastrointestinal drug de-livery and sampling system. Telemed J E Health. 2008 Sep;14(7):715–9.
16. Chandrappan J, Ruiqi L, Su N, Yi GHY, Vaidyanathan K. Thermo-mechanical actuator-based miniature tagging module for localization in capsule endoscopy. J Micro-mech Microeng. 2011;21(4):960–1317.
17. Maton A. Human biology and health. Englewood Cliffs, N.J.: Prentice Hall; 1993.
18. Cheifetz AS, Kornbluth AA, Legnani P, Schmelkin I, Brown A, Lichtiger S, Lewis BS. The risk of reten-tion of the capsule endoscope in patients with known or suspected Crohn’s disease. Am J Gastroenterol. 2006 Oct;101(10):2218–22.
19. Ho KK, Joyce AM. Complications of capsule endoscopy. Gastrointest Endosc Clin N Am. 2007 Jan;17(1):169–1ix.
20. Cave D, Legnani P, de FR, Lewis BS. ICCE consensus for capsule retention. Endoscopy. 2005 Oct;37(10):1065–7.
21. Rondonotti E, Herrerias JM, Pennazio M, Caunedo A, Mascarenhas-Saraiva M, de FR. Complications, limita-tions, and failures of capsule endoscopy: a review of 733 cases. Gastrointest Endosc. 2005 Nov;62(5):712–6.

Volume 42, Number 1, 2014
Ingestible Gastrointestinal Sampling Devices: State-of-the-Art and Future Directions 13
22. Taylor S, Wakem M, Dijkman G, Alsarraj M, Nguyen M. A practical approach to RT-qPCR-Publishing data that conform to the MIQE guidelines. Methods. 2010 Apr;50(4):S1–S5.
23. 510(k) Memorandum - #G95-1 Table 1 Initial Evaluation Tests for Consideration. U S Food and Drug Administra-tion 1995 May 1. Available from: URL: http://www.fda.gov/MedicalDevices/DeviceRegulationandGuidance/guidancedocuments/ucm080742.htm
24. Ratner BD, Bryant SJ. Biomaterials: where we have been and where we are going. Annu Rev Biomed Eng. 2004;6:41–75.
25. Williams DF. On the mechanisms of biocompatibility. Biomaterials. 2008 Jul;29(20):2941–53.
26. Casaletto M, Ingo G, Kaciulis S, Mattogno G, Pan-dolfi L, Scavia G. Surface studies of in vitro biocom-patibility of titanium oxide coatings. Applied Surf Sci. 2001;172(1):167–77.
27. Della Valle F, Calderini G, Rastrelli A, Romeo A. Biocom-patible perforated membranes, processes for their prepara-tion, their use as a support in the in vitro growth of epithe-lial cells, the artificial skin obtained in this manner, and its use in skin grafts. Cell Transplantation. 1995;4(5):iii–iii.
28. Han A, Oh KW, Bhansali S, Thurman Henderson H, Ahn CH. A low temperature biochemically compatible bond-ing technique using fluoropolymers for biochemical mi-crofluidic systems. Micro Electro Mechanical Systems. 2000 MEMS 2000 2000;414–8.
29. Saad B, Neuenschwander P, Uhlschmid GK, Suter UW. New versatile, elastomeric, degradable polymeric mate-rials for medicine. Int J Biol Macromol. 1999 Jun;25(1-3):293–301.
30. Scott G. Why Degradable Polymers? In: Scott G, editor. Degradable polymers. Netherlands: Springer; 2002. p. 1–15.
31. Rohr T, Ogletree DF, Svec F, Fréchet JM. Surface func-tionalization of thermoplastic polymers for the fabrication of microfluidic devices by photoinitiated grafting. Adv-Funct Mater. 2003;13(4):264–70.
32. Heller J. Controlled release of biologically active com-pounds from bioerodible polymers. Biomaterials. 1980 Jan;1(1):51–7.
33. Porter SC, Ridgway K. The permeability of enteric coat-ings and the dissolution rates of coated tablets. J Pharm Pharmacol. 1982 Jan;34(1):5–8.
34. Kim B, Lee S, Park JH, Park J-O. Inchworm-like micro-robot for capsule endoscope. Robotics and Biomimetics, 2004 ROBIO. 2004 2004;458–63.
35. Wang L, Tang TB, Johannessen E, Astaras A, Ahmadian M, Murrary A, Cooper JM, Beaumont SP, Flynn BW, Cumming DR. Integrated micro-instrumentation for dy-namic monitoring of the gastro-intestinal tract. Special Topic Conf Microtechnol Med Biol, 2nd Ann Int IEEE-EMB. 2002;219–22.
36. Standring S. Gray’s anatomy. Churchill Livingstone, El-sevier; 2008.
37. Madsen JL. Effects of gender, age, and body mass in-dex on gastrointestinal transit times. Dig Dis Sci. 1992 Oct;37(10):1548–53.
38. Bulat J, Duda K, Duplaga M, Fraczek R, Skalski A, So-cha M, Turcza P, Zielinski TP. Data processing tasks in wireless GI endoscopy: image-based capsule localization and navigation and video compression. EMBS 2007. 29th Ann Int Conf IEEE. 2815–8. 2007. IEEE.
39. Carpi F, Kastelein N, Talcott M, Pappone C. Magneti-cally controllable gastrointestinal steering of video cap-sules. IEEE Trans Biomed Eng. 2011 Feb;58(2):231–4.
40. Ciuti G, Donlin R, Valdastri P, Arezzo A, Menciassi A, Morino M, Dario P. Robotic versus manual control in magnetic steering of an endoscopic capsule. Endoscopy. 2010 Feb;42(2):148–52.
41. Hou J, Zhu Y, Zhang L, Fu Y, Zhao F, Yang L, Rong G.Design and implementation of a high resolution local-ization system for in-vivo capsule endoscopy. 8th IEEE Int Conf on Dependable, Autonomic and Secure Com-puting. 2009 DASC ‘09 2009;209–14.
42. Wang X, Meng M-H, Hu C. A localization method us-ing 3-axis magnetoresistive sensors for tracking of cap-sule endoscope. EMBS 2006 28th Ann Int Conf IEEE. 2006;2522–5.
43. Davis SS, Hardy JG, Fara JW. Transit of pharmaceuti-cal dosage forms through the small intestine. Gut. 1986 Aug;27(8):886–92.
44. Kaler KV, Mintchev MP, inventors. Inertial naviga-tion method and apparatus for wireless bolus tran-sit monitoring in gastrointestinal tract. US patent US20060169294A1. 2005.
45. Tan C-W, Park S. Design of accelerometer-based inertial navigation systems. IEEE Trans Instrumentation Meas. 2005;54(6):2520–30.
46. Barshan B, Durrant-Whyte HF. Inertial navigation systems for mobile robots. IEEE Trans R. 1995;11(3):328–42.
47. Cunha JS, Coimbra M, Campos P, Soares JM. Automated topographic segmentation and transit time estimation in endoscopic capsule exams. IEEE Trans Med Imaging. 2008;27(1):19–27.
48. Li B, Meng MQ-H. Texture analysis for ulcer detection in capsule endoscopy images. Image Vision Comput. 2009;27(9):1336–42.
49. Liu L, Hu C, Cai W, Meng M-H. Capsule endoscope lo-calization based on computer vision technique. EMBC 2009 Ann Int Conf IEEE. 2009;3711–4.
50. Arshak K, Adepoju F. Adaptive linearized methods for tracking a moving telemetry capsule. IEEE Int Symp Ind Electronics. 2007 ISIE 2007 2007;2703–8.
51. Than TD, Alici G, Zhou H, Li W. A review of localiza-tion systems for robotic endoscopic capsules. IEEE Trans Biomed Engineer. 2012;59(9):2387–99.

Critical ReviewsTM in Biomedical Engineering
Amoako-Tuffour et al.14
52. Khan UI, Pahlavan K, Makarov S. Comparison of TOA and RSS based techniques for RF localization inside hu-man tissue. EMBC, 2011 Annual International Confer-ence of the IEEE. 2011;5602–7.
53. Nagy Z, Fluckiger M, Ergeneman O, Pané S, Probst M, Nelson BJ. A wireless acoustic emitter for passive local-ization in liquids. IEEE Int Conf Robotics Automation. 2009 ICRA ‘09 2009;2593–8.
54. Prior DV, Connor AL, Wilding IR. The enterion capsule. In: Rathbone MJ, Hadgraft J, Roberts MS, editors. Mod-ified-release drug delivery technology. 126 ed. Marcel Dekker AG; 2002. p. 273–88.
55. Quirini M, Webster R, Menciassi A, Dario P. Design of a pill-sized 12-legged endoscopic capsule robot. IEEE Int Conf Robotics Automation. 2007 2007;1856–62.
56. Tortora G, Valdastri P, Susilo E, Menciassi A, Dario P, Rieber F, Schurr MO. Propeller-based wireless device for active capsular endoscopy in the gastric district. Minim Invasive Ther Allied Technol. 2009;18(5):280–90.
57. Uehara A, Hoshina K. Capsule endoscope NORIKA sys-tem. Minimally invasive therapy & allied technolo-gies. MITAT. 2003;12(5):227–34.
58. Kim B, Lee S, Park JH, Park J-O. Design and fabrication of a locomotive mechanism for capsule-type endoscopes using shape memory alloys (SMAs). IEEE/ASME Trans Mechatron. 2005;10(1):77–86.
59. Park H, Park S, Yoon E, Kim B, Park J, Park S. Paddling based microrobot for capsule endoscopes. IEEE Intl Conf Robotics Automation. 2007 2007;3377–82.
60. Simi M, Valdastri P, Quaglia C, Menciassi A, Dario P. Design, fabrication, and testing of a capsule with hybrid locomotion for gastrointestinal tract exploration. IEEE/ASME Trans Mechatron. 2010;15(2):170–80.
61. Sendoh M, Ishiyama K, Arai K-I. Fabrication of magnet-ic actuator for use in a capsule endoscope. IEEE/ASME Trans Magnet. 2003;39(5):3232–4.
62. Jeong HE, Kwak MK, Suh KY. Stretchable, adhesion-tunable dry adhesive by surface wrinkling. Langmuir. 2010 Feb 16;26(4):2223–6.
63. Murphy MP, Kim S, Sitti M. Enhanced adhesion by gecko-inspired hierarchical fibrillar adhesives. ACS Appl Mater Interfaces. 2009 Apr;1(4):849–55.
64. Reddy S, Arzt E, del Campo A. Bioinspired surfaces with switchable adhesion. Adv Mater. 2007;19(22):3833–7.
65. Mojaverian P. Evaluation of gastrointestinal pH and gastric residence time via the Heidelberg radiotelem-etry capsule: pharmaceutical application. Drug Dev Res. 1996;38(2):73–85.
66. Sang-Hyo W, Jyung-Hyun L, Min-Kyu K, Chul-Ho W, Jin-Ho C. Telemetry capsule for pressure monitoring in the gastrointestinal tract. IEICE Trans Fund Elect Comm Comput Sci. 2006;89-A(6):1699–1700.
67. Cutchis PN, Hogrefe AF, Lesho JC. The ingestible ther-mal monitoring system. Johns Hopkins APL Technical Digest. 1988;9:16–21.
68. Zhou G-X. Swallowable or implantable body tempera-ture telemeter-body temperature radio pill. Proceedings of the 1989 Fifteenth Annual Northeast Bioengineering Conference. 1989;165–6.
69. Wang L, Johannessen EA, Hammond PA, Cui L, Reid SW, Cooper JM, Cumming DR. A programmable micro-system using system-on-chip for real-time biotelemetry. IEEE Trans Biomed Eng. 2005 Jul;52(7):1251–60.
70. Ask P, Edwall G, Johansson KE, Tibbling L. On the use of monocrystalline antimony pH electrodes in gastro-oe-sophageal functional disorders. Med Biol Eng Comput. 1982 May;20(3):383–9.
71. Savarino V, Mela GS, Zentilin P, Magnolia MR, Scal-abrini P, Valle F, Moretti M, Bonifacino G, Celle G. Gas-tric aspiration versus antimony and glass pH electrodes. A simultaneous comparative in vivo study. Scand J Gas-troenterol. 1989 May;24(4):434–9.
72. Wang L, Yang G-Z, Huang J, Zhang J, Yu L, Nie Z, Cum-ming DR. A wireless biomedical signal interface system-on-chip for body sensor networks. IEEE Trans Biomed Circ Syst. 2010;4(2):112–7.
73. Evans DF, Pye G, Bramley R, Clark AG, Dyson TJ, Hardcastle JD. Measurement of gastrointestinal pH profiles in normal ambulant human subjects. Gut. 1988 Aug;29(8):1035–41.
74. Chiang J-L, Jan S-S, Chou J-C, Chen Y-C. Study on the temperature effect, hysteresis and drift of pH-ISFET de-vices based on amorphous tungsten oxide. Sensors and Actuators B: Chemical. 2001;76(1):624–8.
75. McKenzie J, Osgood D. Validation of a new tele-metric core temperature monitor. J Thermal Biology. 2004;29(7):605–11.
76. Shim MG, Song LM, Marcon NE, Wilson BC. In vivo near-infrared Raman spectroscopy: demonstration of fea-sibility during clinical gastrointestinal endoscopy. Photo-chem Photobiol. 2000 Jul;72(1):146–50.
77. Tearney GJ, Brezinski ME, Southern JF, Bouma BE, Boppart SA, Fujimoto JG. Optical biopsy in human gas-trointestinal tissue using optical coherence tomography. Am J Gastroenterol. 1997 Oct;92(10):1800–4.
78. Gong F, Swain P, Mills T. Wireless endoscopy. Gastroin-test Endosc. 2000 Jun;51(6):725–9.
79. Iddan G, Meron G, Glukhovsky A, Swain P. Wireless capsule endoscopy. Nature. 2000 May 25;405(6785):417.
80. Savci HS, Sula A, Wang Z, Dogan NS, Arvas E. MICS transceivers: regulatory standards and applications [med-ical implant communications service]. SoutheastCon, 2005 Proc IEEE. 2005;179–82.
81. Zhen B, Li H-B, Kohno R. IEEE body area networks and medical implant communications. Proceedings of the ICST 3rd International Conference on Body Area Net-works. 2008. ICST (Institute for Computer Sciences, So-cial-Informatics and Telecommunications Engineering).
82. Kahn JM, Barry JR. Wireless infrared communications. Proc IEEE. 1997;85(2):265–98.

Volume 42, Number 1, 2014
Ingestible Gastrointestinal Sampling Devices: State-of-the-Art and Future Directions 15
83. Williams S. IrDA: past, present and future. Pers Comm IEEE. 2000;7(1):11–9.
84. Schmidt CL, Skarstad PM. The future of lithium and lithium-ion batteries in implantable medical devices. J Power Sources. 2001;97–98(July):742–6.
85. Takeuchi KJ, Leising RA, Palazzo MJ, Marschilok AC, Takeuchi ES. Advanced lithium batteries for implantable medical devices: mechanistic study of SVO cathode syn-thesis. J Power Sources. 2003;119–121(June):973–8.
86. Carta R, Thoné J, Puers R. A wireless power supply sys-tem for robotic capsular endoscopes. Sensors and Actua-tors A: Physical. 2010;162(2):177–83.
87. Lenaerts B, Puers R. An inductive power link for a wireless endoscope. Biosens Bioelectron. 2007 Feb 15;22(7):1390–5.
88. Crosby WH, Kugler HW. Intraluminal biopsy of the small intestine; the intestinal biopsy capsule. Am J Dig Dis. 1957 May;2(5):236–41.
89. Park S, Koo K, Bang SM, Park JY, Song SY. A novel microactuator for microbiopsy in capsular endoscopes. J Micromech Microeng. 2008;18(2):25–32.
90. Prout BJ. A rapid method of obtaining a jejunal biopsy using a Crosby capsule and a gastrointestinal fiberscope. Gut. 1974 Jul;15(7):571–2.
91. Tang J, Wang L, Ying J, Lee W, Ho P, inventors; Jing Tang, Leming Wang, Jinpin Ying, Weilong Lee, Pingpei Ho, assignees. Apparatus and methods of using built-in micro-spectroscopy micro-biosensors and specimen col-lection system for a wireless capsule in a biological body in vivo. US20050154277A1. 2003.
92. Tsai N-C, Sue C-Y. Review of MEMS-based drug deliv-ery and dosing systems. Sensors and Actuators A: Physi-cal Sensors and Actuators A: Physical 2007;134(2):555–64.
93. Zengerle R, Ulrich J, Kluge S, Richter M, Richter A. A bidirectional silicon micropump. Sensors and Ac-tuators A: Physical Sensors and Actuators A: Physical. 1995;50(1):81–6.
94. Gu HH, Gu HL, inventors. Intestinal fluid sampler. US5971942A. 1999.
95. Sprenkels A, Jenneboer A, Johannes S, Venema K, van den Berg A, De Vos W, inventors; Vos Willem Meindert De, Antonius Johannes St Jenneboer, Adrianus Joseph Sprenkels, Den Berg Albert Van, Konraad Venema, as-signees. Sampling device for in vivo sampling of liquids from the gastrointestinal tract, process for the production thereof and mould or mask for use in the production pro-cess.WO. 2007061305. 2007.
96. Trier JS. Diagnostic value of peroral biopsy of the proximal small intestine. N Engl J Med. 1971 Dec 23;285(26):1470–3.
97. Clarke SW. Jenunal perforation with the CROSBY cap-sule. Lancet. 1964 Oct 3;2(7362):727–8.
98. Vidinli M, Finlay JM. Massive hemorrhage follow-ing small bowel biopsy. Can Med Assoc J. 1964 Dec 5;91:1223–5.
99. Salem SN, Salt RH, Truelove SC. CROSBY small-in-testinal capsule with radio-opaque tube and latex sheath. Gut. 1965 Feb;6:99–100.
100. Diehl DL, Adler DG, Conway JD, Farraye FA, Kantse-voy SV, Kaul V, Kethu SR, Kwon RS, Mamula P, Ro-driguez SA, Tierney WM. Endoscopic retrieval devices. Gastrointest Endosc. 2009 May;69(6):997–1003.
101. Vilmann P, Krasnik M, Larsen SS, Jacobsen GK, Cle-mentsen P. Transesophageal endoscopic ultrasound-guided fine-needle aspiration (EUS-FNA) and endo-bronchial ultrasound-guided transbronchial needle aspiration (EBUS-TBNA) biopsy: a combined approach in the evaluation of mediastinal lesions. Endoscopy. 2005 Sep;37(9):833-839.
102. Mellinger JD. Upper gastrointestinal endoscopy: current status. Semin Laparosc Surg. 2003 Mar;10(1):3–12.
103. Yamamoto H, Kita H. Double-balloon endoscopy. Curr Opin Gastroenterol. 2005 Sep;21(5):573–7.
104. Fujimoto JG. Optical coherence tomography for ultra-high resolution in vivo imaging. Nat Biotechnol. 2003 Nov;21(11):1361–7.
105. Izatt JA, Kulkarni MD, Wang H-W, Kobayashi K, Sivak Jr MV. Optical coherence tomography and microscopy in gastrointestinal tissues. Sel Top Quantum Elect IEEE J. 1996;2(4):1017–28.
106. Lesho JC, Hogrefe AF, inventors; Arthur F. Hogrefe, Jef-fery C. Lesho, assignees. Ingestible size continuously transmitting temperature monitoring pill. US 4844076 A. 1989.
107. Maqbool S, Parkman HP, Friedenberg FK. Wireless cap-sule motility: comparison of the SmartPill GI monitoring system with scintigraphy for measuring whole gut tran-sit. Dig Dis Sci. 2009 Oct;54(10):2167–74.
108. O’Brien C, Hoyt RW, Buller MJ, Castellani JW, Young AJ. Telemetry pill measurement of core temperature in humans during active heating and cooling. Med Sci Sports Exerc. 1998 Mar;30(3):468–72.
109. Leavitt N. Researchers fight to keep implanted medical devices safe from hackers. Computer. 2010;43(8):11–14.
110. Fawaz N, Jansen D. A new platform of an electronic pill with bidirectional communication system for min-iaturized and low power biomedical applications. MPC-Workshop July 2007. Hochschule Offenburg.
111. Humphries TJ, Castell DO. Pressure profile of esopha-geal peristalsis in normal humans as measured by di-rect intraesophageal transducers. Am J Dig Dis. 1977 Jul;22(7):641–5.
112. Puers R, Carta R, Thoné J. Wireless power and data transmission strategies for next-generation capsule endo-scopes. J Micromech Microeng. 2011;21:054008.