
Inclusion of Sevoflurane in Cardioplegia Reduces Neutrophil Activity During Cardiopulmonary Bypass
6
Inclusion of Sevoflurane in Cardioplegia Reduces Neutrophil Activity During Cardiopulmonary Bypass Nader D. Nader, MD, PhD, Hratch L. Karamanoukian, MD, Roberta L. Reedy, MSc, Firooz Salehpour, MD, and Paul R. Knight, MD, PhD Objective: The purpose of this study was to examine the effects of sevoflurane cardioplegia on neutrophil response and complement activation after cardiopulmonary bypass (CPB). Design: A prospective, randomized clinical investigation. Setting: University-affiliated hospital; single institutional. Participants: Twenty-one male patients undergoing coro- nary bypass surgery using CPB. Interventions: Eleven patients were randomly assigned to receive sevoflurane 2% as a part of the cardioplegic mixture (SEV). The control group (n 10) received no sevoflurane in their cardioplegia (control). Measurements and Main Results: Myeloperoxidase activ- ity (MPO) was assayed in coronary sinus blood as a surro- gate for neutrophilic response at the termination of CPB. MPO activity in the coronary sinus blood was lower in the patients who received sevoflurane compared with controls. MPO activity was higher in patients with cardiac events at 4-year follow-up when compared with asymptomatic pa- tients. IL-8, C4b, C3d, C5a, and CH50 were assessed in cor- onary sinus and peripheral blood at time of CPB initiation (T0) and upon the termination of CPB (T2). Peripheral blood sampling occurred at the sixth hour after T0 (T6). IL-8 levels were significantly inhibited in the SEV group when com- pared with controls at T2 and T6. CH50 (an index of global activation of complement system) decreased 30% at T2 and 52% at T6. The classic component of the complement path- way (C4b) was effectively inhibited in the SEV group, whereas the common pathway (C3d and C5a) was similar in both groups. Conclusions: The addition of sevoflurane to cardioplegia is associated with an inhibition of neutrophils after CPB. A major component of the neutrophil response appears to be IL-8 mediated, although the classic complement pathway is also inhibited by sevoflurane. © 2006 Elsevier Inc. All rights reserved. KEY WORDS: cardiac surgery, cardiopulmonary bypass, neu- trophil, complement, interleukins N EUTROPHILS CONTRIBUTE to the expansion of myo- cardial injury after an ischemic injury. 1 An increase in the number of neutrophils in the blood is commonly observed during myocardial infarction (MI). 2,3 After ischemia, reperfu- sion further exacerbates the injury to the myocardium. This is caused by a continuation of inflammatory responses that in- crease the risk of extending injury to surviving but vulnerable myocardial tissue. Periods of ischemia-reperfusion (IR) are inevitable during coronary revascularization procedures. The pathogenesis of IR-related myocardial injury involves the interaction of a com- plex series of responses to low tissue oxygen tensions, deple- tion of critical nutrients, and the accumulation of metabolic waste products. A large inflammatory response is thought to be an important contributor to the pathophysiology of IR injury. 2 Reperfusion of previously ischemic myocardium results in pro- duction of reactive species of oxygen. Altering the intracellular redox potential increases the expression of inflammatory cyto- kines. Prior research has suggested that interleukin (IL)-6, IL-8, IL-1, tumor necrosis , and transforming growth factor 1 have important roles in IR by promoting inflammation, cellular adhesion, and the production of vasoactive mediators and vas- cular growth factors. 4-6 Furthermore, the utilization of extra- corporeal circulation stimulates and activates circulating neu- trophils and the complement system by either direct contact or through the release of systemic chemotactic factors. Myocardial injury because of IR is mediated by neutrophils and inflammatory mediators released by these cells. The inhi- bition of neutrophil activation and function therefore will limit the extent of myocardial damage after cardiopulmonary bypass (CPB) with the use of aortic cross-clamping. Both volatile and intravenous anesthetics, when combined with opioids, suppress reflex sympathetic activity that mitigates surgical stress-asso- ciated myocardial ischemia in an already compromised heart. Volatile anesthetics may also protect against inflammatory ischemic insults by direct actions on cellular mechanisms in- volved in ion transport and myocardial contraction. 7-9 This study examined the effects of sevoflurane, administered directly to the coronary circulation during CPB via the car- dioplegic solution, on the activation of peripheral neutrophils and complement, as well as the production and release of the CXC chemokine IL-8. It was hypothesized that a reduction in the myocardial inflammatory response during IR decreases the release of locally produced IL-8 and therefore partially pre- vents the activation of neutrophils. Furthermore, it was thought that the activation of complement is independent of IR but also is affected by administration of sevoflurane. METHODS Human subject enrollment was reviewed and approved by the insti- tutional review board at the VA Western NY Healthcare System. After obtaining informed consent, 21 patients scheduled to undergo coronary artery bypass graft (CABG) surgery using CPB were enrolled in the study, and 11 were randomly assigned to receive sevoflurane 2% as a part of the cardioplegic mixture (SEV). The control group (n 10) received no sevoflurane in their cardioplegia (control). Inclusion crite- ria consisted of coronary artery disease requiring elective surgical revascularization. Exclusion criteria consisted of fresh myocardial in- farction (7 days), left ventricular ejection fraction 40%, ongoing inflammation, and patient refusal. Demographics between the groups were not significantly different (mean age, preoperative ejection frac- From the VA Medical Center, Buffalo, NY. Supported by a mid-career award from the Society of Cardiovascu- lar Anesthesiologists to N.D.N. Address reprint requests to Nader D. Nader, MD, PhD, Rm 203 C, VA Medical Center, 3495 Bailey Avenue, Buffalo, NY 14215. E-mail: [email protected] © 2006 Elsevier Inc. All rights reserved. 1053-0770/06/2001-0012$32.00/0 doi:10.1053/j.jvca.2005.07.030 57 Journal of Cardiothoracic and Vascular Anesthesia, Vol 20, No 1 (February), 2006: pp 57-62
Transcript of Inclusion of Sevoflurane in Cardioplegia Reduces Neutrophil Activity During Cardiopulmonary Bypass

e
a
(
n
r
(
t
i
g
M
p
M
4
Nndsccm
cIptwaRdrkIhacctt
abt(ircV
J
Inclusion of Sevoflurane in Cardioplegia Reduces Neutrophil Activity DuringCardiopulmonary Bypass
Nader D. Nader, MD, PhD, Hratch L. Karamanoukian, MD, Roberta L. Reedy, MSc, Firooz Salehpour, MD, and
Paul R. Knight, MD, PhDt
o
(
s
w
p
a
5
w
w
b
a
m
I
a
©
K
Objective: The purpose of this study was to examine the
ffects of sevoflurane cardioplegia on neutrophil response
nd complement activation after cardiopulmonary bypass
CPB).
Design: A prospective, randomized clinical investigation.
Setting: University-affiliated hospital; single institutional.
Participants: Twenty-one male patients undergoing coro-
ary bypass surgery using CPB.
Interventions: Eleven patients were randomly assigned to
eceive sevoflurane 2% as a part of the cardioplegic mixture
SEV). The control group (n � 10) received no sevoflurane in
heir cardioplegia (control).
Measurements and Main Results: Myeloperoxidase activ-
ty (MPO) was assayed in coronary sinus blood as a surro-
ate for neutrophilic response at the termination of CPB.
PO activity in the coronary sinus blood was lower in the
atients who received sevoflurane compared with controls.
PO activity was higher in patients with cardiac events at
olatile anesthetics may also protect against inflammatory
iv
ddaCtrvti
toasprrrfiw
l
Vn
ournal of Cardiothoracic and Vascular Anesthesia, Vol 20, No 1 (February
ients. IL-8, C4b, C3d, C5a, and CH50 were assessed in cor-
nary sinus and peripheral blood at time of CPB initiation
T0) and upon the termination of CPB (T2). Peripheral blood
ampling occurred at the sixth hour after T0 (T6). IL-8 levels
ere significantly inhibited in the SEV group when com-
ared with controls at T2 and T6. CH50 (an index of global
ctivation of complement system) decreased 30% at T2 and
2% at T6. The classic component of the complement path-
ay (C4b) was effectively inhibited in the SEV group,
hereas the common pathway (C3d and C5a) was similar in
oth groups.
Conclusions: The addition of sevoflurane to cardioplegia is
ssociated with an inhibition of neutrophils after CPB. A
ajor component of the neutrophil response appears to be
L-8 mediated, although the classic complement pathway is
lso inhibited by sevoflurane.
2006 Elsevier Inc. All rights reserved.
EY WORDS: cardiac surgery, cardiopulmonary bypass, neu-
-year follow-up when compared with asymptomatic pa- trophil, complement, interleukins
EUTROPHILS CONTRIBUTE to the expansion of myo-cardial injury after an ischemic injury.1 An increase in the
umber of neutrophils in the blood is commonly observeduring myocardial infarction (MI).2,3 After ischemia, reperfu-ion further exacerbates the injury to the myocardium. This isaused by a continuation of inflammatory responses that in-rease the risk of extending injury to surviving but vulnerableyocardial tissue.Periods of ischemia-reperfusion (IR) are inevitable during
oronary revascularization procedures. The pathogenesis ofR-related myocardial injury involves the interaction of a com-lex series of responses to low tissue oxygen tensions, deple-ion of critical nutrients, and the accumulation of metabolicaste products. A large inflammatory response is thought to be
n important contributor to the pathophysiology of IR injury.2
eperfusion of previously ischemic myocardium results in pro-uction of reactive species of oxygen. Altering the intracellularedox potential increases the expression of inflammatory cyto-ines. Prior research has suggested that interleukin (IL)-6, IL-8,L-1�, tumor necrosis �, and transforming growth factor �1ave important roles in IR by promoting inflammation, cellulardhesion, and the production of vasoactive mediators and vas-ular growth factors.4-6 Furthermore, the utilization of extra-orporeal circulation stimulates and activates circulating neu-rophils and the complement system by either direct contact orhrough the release of systemic chemotactic factors.
Myocardial injury because of IR is mediated by neutrophilsnd inflammatory mediators released by these cells. The inhi-ition of neutrophil activation and function therefore will limithe extent of myocardial damage after cardiopulmonary bypassCPB) with the use of aortic cross-clamping. Both volatile andntravenous anesthetics, when combined with opioids, suppresseflex sympathetic activity that mitigates surgical stress-asso-iated myocardial ischemia in an already compromised heart.
schemic insults by direct actions on cellular mechanisms in-olved in ion transport and myocardial contraction.7-9
This study examined the effects of sevoflurane, administeredirectly to the coronary circulation during CPB via the car-ioplegic solution, on the activation of peripheral neutrophilsnd complement, as well as the production and release of theXC chemokine IL-8. It was hypothesized that a reduction in
he myocardial inflammatory response during IR decreases theelease of locally produced IL-8 and therefore partially pre-ents the activation of neutrophils. Furthermore, it was thoughthat the activation of complement is independent of IR but alsos affected by administration of sevoflurane.
METHODS
Human subject enrollment was reviewed and approved by the insti-utional review board at the VA Western NY Healthcare System. Afterbtaining informed consent, 21 patients scheduled to undergo coronaryrtery bypass graft (CABG) surgery using CPB were enrolled in thetudy, and 11 were randomly assigned to receive sevoflurane 2% as aart of the cardioplegic mixture (SEV). The control group (n � 10)eceived no sevoflurane in their cardioplegia (control). Inclusion crite-ia consisted of coronary artery disease requiring elective surgicalevascularization. Exclusion criteria consisted of fresh myocardial in-arction (�7 days), left ventricular ejection fraction �40%, ongoingnflammation, and patient refusal. Demographics between the groupsere not significantly different (mean age, preoperative ejection frac-
From the VA Medical Center, Buffalo, NY.Supported by a mid-career award from the Society of Cardiovascu-
ar Anesthesiologists to N.D.N.Address reprint requests to Nader D. Nader, MD, PhD, Rm 203 C,
A Medical Center, 3495 Bailey Avenue, Buffalo, NY 14215. E-mail:[email protected]© 2006 Elsevier Inc. All rights reserved.1053-0770/06/2001-0012$32.00/0
doi:10.1053/j.jvca.2005.07.03057), 2006: pp 57-62

tAm
cdimattactosts(bAaehdagtadosutAphe
cT64mmfdioLpecamwsav
csc
bh
nfcyawCCss1(a(bMtp
uMrbiataawp5
navaarbtvdl1(ctsmeI1in
cAwap
58 NADER ET AL
ion, American Society of Anesthesiologists status, New York Heartssociation classification, aortic cross-clamp time, use of left internalammary artery, and the number of venous grafts).Both groups were anesthetized using total intravenous anesthesia
onsisting of fentanyl (10 �g/kg), midazolam (0.1 mg/kg), and etomi-ate (0.2-0.5 mg/kg). Endotracheal intubation was facilitated withntravenous administration of rocuronium (0.9 mg/kg). Anesthesia wasaintained with a continuous infusion of propofol (75-150 �g/kg/min)
nd fentanyl (3 �g/kg/h). Muscle relaxation was provided by intermit-ent bolus administration of rocuronium that was periodically moni-ored using a peripheral nerve stimulator. A peripheral arterial catheter,
right internal jugular introducer port, and an oxymetric continuousardiac output pulmonary artery catheter were placed under sterileechnique. All surgeries were performed via median sternotomy. Cor-nary revascularization used the left internal mammary artery andaphenous vein grafts. After cannulation of the aorta and right atrium,he surgeon placed a coronary sinus catheter. After conclusion of theurgical procedure, patients were transferred to the intensive care unitICU) and mechanically ventilated. Sedation in the ICU was providedy the infusion of propofol until the patient met extubation criteria.fter surgery, all patients were monitored in the ICU for 24 to 48 hours
fter which time the patient returned to the floor. Any acute cardiacvent (new ischemia, ventricular or supraventricular arrhythmias, andospital death) was recorded. The criteria for new ischemia wereefined electrocardiographically as a Q-wave MI evidenced by theppearance of new persistent (�24 hours) Q waves �0.04 seconds inreater than or equal to 2 contiguous leads of the same vascularerritory or equivalent R-wave increments (R/S ratio �1 in leads V1nd V2). A non–Q-wave MI was diagnosed by ST-segment elevation orepression �1 mV 0.08 seconds after the J-point or T-wave inversionf 1 to 2 mV 0.08 seconds after the J-point in 2 contiguous leads of theame vascular territory. Ventricular arrhythmias consisted of ventric-lar fibrillation, ventricular tachycardia, or persistent premature ven-ricular beats requiring the administration of an antiarrhythmic agent.trial arrhythmias consisted of persistent atrial fibrillation or flutter. Allatients were followed up for a period of 4 years by review of theirospital records for the incidence of previously mentioned adversevents.
Upon the initiation of CPB, an aortic cross-clamp was applied andardioplegia was delivered in both antegrade and retrograde fashion.he following cardioplegia formula was used: cold (temperature 5°-°C) plasmalyte-based solution containing 165 mEq of sodium,5 mEq of potassium, 3 mEq of magnesium, 138 mEq of chloride, 27Eq of acetate, 25 mEq of bicarbonate, 23 mEq of gluconate, and 100g of lidocaine mixed with cold blood in a 4:1 ratio in an antegrade
ashion. Using a separate pediatric oxygenator (Capiox; Terumo Car-iovascular System, Elkton, MD), the cardioplegia mixture was vapor-zed with 2% sevoflurane and oxygen in the SEV group and withxygen only in the control group. Oxygen was delivered at a rate of 2/min. While distal anastomoses were constructed, retrograde cardio-legia was administered continuously through the coronary sinus cath-ter. Immediately before the release of the aortic cross-clamp, warmardioplegia was administered both in antegrade and retrograde fashiont a rate of 100 mL/min. Sevoflurane 2% was added to the cardioplegiaixture in the treatment cohort by the perfusionist. The sevofluraneas administered through a separate vaporizer. The concentration of
evoflurane in the soluble form was not measured. Both the surgeonnd the anesthesiologist were blinded to the treatment by shielding theaporizer setting from view.Baseline blood samples were obtained from the arterial and the
oronary sinus catheters before the commencement of CPB (T0). Theecond set of blood samples were obtained from the arterial and the
oronary sinus catheters upon termination of CPB (T2). The final set of tlood samples were obtained from the peripheral arterial catheter 6ours after the initiation of CPB (T6).Myeloperoxidase (MPO) activity was measured as a marker of
eutrophil infiltration in the heart. In brief, the buffy coat harvestedrom the coronary sinus blood samples was resuspended in bufferontaining 50 mmol/L of KH2PO4, 13.7 mmol/L of hexadecyltrimeth-lammonium bromide, and 5 mmol/L of ethylenediaminetetraaceticcid (pH � 6.0; Sigma Chemical, St Louis, MO). The cell suspensionas then sonicated on ice for 4 � 10-second pulses using a Sonifierell Disruptor 350 with microtip probe (Branson Ultrasonics, Danbury,T) and centrifuged at 2,300 � g for 30 minutes at 4°C. The resultant
upernatant was assayed for MPO activity by combining 50 �L ofample with 1.5 mL of assay buffer containing 50 mmol/L of KH2PO4,76 �mol/L of H2O2, and 525 �mol/L of o-dianisidine dihydrochloridepH � 6.0; Sigma Chemical) in a cuvette and continually recording thebsorbency at 460 nm for 2 minutes using a DU-650 spectrophotometerBeckman Instruments, Palo Alto, CA). The spectrophotometer waslanked with 50 mmol/L of phosphate buffer before measurement.PO activity was normalized to protein concentration and expressed as
he absorbency change (at 460 nm) per minute (absorbance/min/mg ofrotein) over the linear portion of the curve.10
IL-8 levels were measured by enzyme-linked immunosorbent assaysing a commercially available kit (Quantikine IL-8 kit; R&D Systems,inneapolis, MN). In brief, standard solutions were prepared from
ecombinant cytokines. Plasma samples (50 �L) were added to anti-ody-coated 96-microwell plates and incubated for 2 hours. Horserad-sh perioxidase conjugate antibody was added after a series of washesnd incubated for an additional 2 hours. The plates were washed 4imes, and TMB (3,3=,5,5=-tetramethylbenzidine) substrate was addednd incubated for 20 minutes. The reaction was stopped using sulfuriccid (H2SO4), and the absorbency was read by a plate reader at 450-nmavelength. The minimum detectable dose of IL-8 ranged was 3.5g/mL with intra-assay variation of 4.6% and interassay variation of.2%Hemolytic complement activity (CH-50) and complement compo-
ents were measured. Serum samples were diluted with buffer anddded to a 96-well flat-bottom Linbro (Aliso Viejo, CA) plate in a finalolume of 100 �L. Sensitized sheep red blood cells (100 �L) were thendded to each well. The plate was incubated at 37°C for 90 minutes,gitated on a shaker, and then read by a BioRad (Hercules, CA) plateeader at 630 nm. The reading was converted to percentage hemolysisy using both a buffer blank and a complete hemolysis blank (saponin);hese values were applied to the Von Krogh equation to yield a CH50alue. A customized enzyme immunoassay technique was used toetect C3d, C4b, and C5a complement components using highly se-ective monoclonal antibodies. In brief, plasma samples were diluted:100 (100 �L/well) and incubated for 1 hour at room temperature18°-25°C). After rinsing off the unbound native protein, peroxidase-onjugated mouse monoclonal antibody was used for the detection ofhe complement protein. The reactions were stopped by 100 �L ofulfuric acid into the wells and the absorbance was measured with aicrotiter plate reader (BioRad) at a 450-nm wavelength and a refer-
nce wavelength of 550 nm. Substrate control was served as blank.ntra-assay precision for this enzyme-linked immunosorbent assay was2.8%, and interassay precision ranged between 12.1-14.7%. The min-mum detectable concentration was 0.12 ng/mL for C3d and 0.06g/mL for C5a.Baseline demographic nonparametric data and risk factors were
ompared and analyzed using cross-tabulation and a Fisher exact test.ll data are presented as mean � standard error of the mean. Data thatere not normally distributed were compared between the treatment
nd the control groups using a Kruskal-Wallis test. The time that theatients first presented with a new cardiac event was calculated using
he Kaplan-Meier survival analysis and was compared between the 2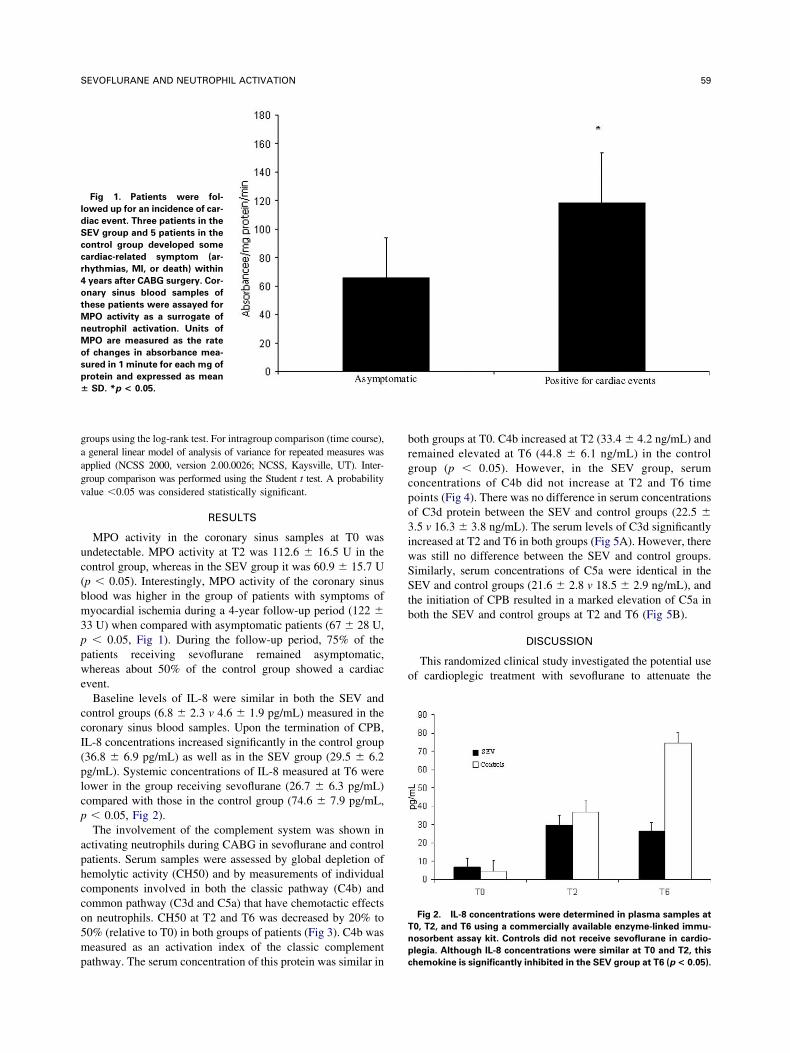
gaagv
uc(bm3ppwe
ccI(plcp
aphcco5mp
brgcpo3iwSStb
o
l
d
S
c
c
r
4
o
t
M
n
M
o
s
p
�
T
n
59SEVOFLURANE AND NEUTROPHIL ACTIVATION
roups using the log-rank test. For intragroup comparison (time course),general linear model of analysis of variance for repeated measures was
pplied (NCSS 2000, version 2.00.0026; NCSS, Kaysville, UT). Inter-roup comparison was performed using the Student t test. A probabilityalue �0.05 was considered statistically significant.
RESULTS
MPO activity in the coronary sinus samples at T0 wasndetectable. MPO activity at T2 was 112.6 � 16.5 U in theontrol group, whereas in the SEV group it was 60.9 � 15.7 Up � 0.05). Interestingly, MPO activity of the coronary sinuslood was higher in the group of patients with symptoms ofyocardial ischemia during a 4-year follow-up period (122 �
3 U) when compared with asymptomatic patients (67 � 28 U,� 0.05, Fig 1). During the follow-up period, 75% of the
atients receiving sevoflurane remained asymptomatic,hereas about 50% of the control group showed a cardiac
vent.Baseline levels of IL-8 were similar in both the SEV and
ontrol groups (6.8 � 2.3 v 4.6 � 1.9 pg/mL) measured in theoronary sinus blood samples. Upon the termination of CPB,L-8 concentrations increased significantly in the control group36.8 � 6.9 pg/mL) as well as in the SEV group (29.5 � 6.2g/mL). Systemic concentrations of IL-8 measured at T6 wereower in the group receiving sevoflurane (26.7 � 6.3 pg/mL)ompared with those in the control group (74.6 � 7.9 pg/mL,� 0.05, Fig 2).The involvement of the complement system was shown in
ctivating neutrophils during CABG in sevoflurane and controlatients. Serum samples were assessed by global depletion ofemolytic activity (CH50) and by measurements of individualomponents involved in both the classic pathway (C4b) andommon pathway (C3d and C5a) that have chemotactic effectsn neutrophils. CH50 at T2 and T6 was decreased by 20% to0% (relative to T0) in both groups of patients (Fig 3). C4b waseasured as an activation index of the classic complement
Fig 1. Patients were fol-
owed up for an incidence of car-
iac event. Three patients in the
EV group and 5 patients in the
ontrol group developed some
ardiac-related symptom (ar-
hythmias, MI, or death) within
years after CABG surgery. Cor-
nary sinus blood samples of
hese patients were assayed for
PO activity as a surrogate of
eutrophil activation. Units of
PO are measured as the rate
f changes in absorbance mea-
ured in 1 minute for each mg of
rotein and expressed as mean
SD. *p < 0.05.
athway. The serum concentration of this protein was similar inp
c
oth groups at T0. C4b increased at T2 (33.4 � 4.2 ng/mL) andemained elevated at T6 (44.8 � 6.1 ng/mL) in the controlroup (p � 0.05). However, in the SEV group, serumoncentrations of C4b did not increase at T2 and T6 timeoints (Fig 4). There was no difference in serum concentrationsf C3d protein between the SEV and control groups (22.5 �.5 v 16.3 � 3.8 ng/mL). The serum levels of C3d significantlyncreased at T2 and T6 in both groups (Fig 5A). However, thereas still no difference between the SEV and control groups.imilarly, serum concentrations of C5a were identical in theEV and control groups (21.6 � 2.8 v 18.5 � 2.9 ng/mL), and
he initiation of CPB resulted in a marked elevation of C5a inoth the SEV and control groups at T2 and T6 (Fig 5B).
DISCUSSION
This randomized clinical study investigated the potential usef cardioplegic treatment with sevoflurane to attenuate the
Fig 2. IL-8 concentrations were determined in plasma samples at
0, T2, and T6 using a commercially available enzyme-linked immu-
osorbent assay kit. Controls did not receive sevoflurane in cardio-
legia. Although IL-8 concentrations were similar at T0 and T2, this
hemokine is significantly inhibited in the SEV group at T6 (p < 0.05).

iicngcitrpbsrb
2e n
piricp
gimovTscbtmic
T
c
m
t
E
T
c
a
w
a
60 NADER ET AL
nflammatory response to an expected period of myocardialschemia with subsequent reperfusion. The study subjects in-luded relatively low-risk patients undergoing surgical coro-ary revascularization. Sevoflurane is commonly used in thisroup of patients; however, the inclusion of sevoflurane in theardioplegic formula is a novel technique of distribution allow-ng for relatively selective intramyocardial delivery. Althoughhe authors did not measure tissue concentrations of sevoflu-ane in the heart or in cardioplegia solutions, the volumeercent concentration in the cardioplegia would be expected toe 1.4% (blood/gas partition coefficient at 37°C is 0.69). Con-idering a muscle blood partition coefficient of 3.6 for sevoflu-ane, myocardial concentrations of this vapor are estimated toe around 4.5%.The present study showed that the addition of sevoflurane
% to the cardioplegia solution during aortic cross-clampingffectively reduces the generation of IL-8 and the subsequent
Fig 3. CH-50 was measured in serum samples of the patients at
0, T2, and T6 based on its hemolytic activity on sheep red blood
ells. Values at T0 time point were used as baseline, and the other
easurements were expressed as a percent value compared with
he baseline measurements.
Fig 4. Serum levels of C4b were measured using a customized
LISA. There is a significant increase in C4b concentration at T2 and
c6 time points in the control group (s). Administration of sevoflurane
ompletely blunts this increase (p < 0.05).
eutrophilic and C4b complement response after CPB. It wasostulated that sevoflurane protects the myocardium by inhib-ting early activation of neutrophil-dependent inflammatoryesponses, thereby improving the well-being of the previouslyschemic myocardium. These findings are of significance be-ause activated neutrophils are known to be involved in theathogenesis of IR injury.11-13
MPO is a heme protein and an elevation in its activity isenerally regarded as an index of neutrophil activation.14 Theres growing evidence that MPO and neutrophil inflammation areechanistically linked to both acute and chronic manifestations
f cardiovascular disease,15,16 whereas the incidence of cardio-ascular diseases is reduced in MPO-deficient populations.17
he present results show that MPO activity in the coronaryinus blood increases after the application of the aortic cross-lamp, suggesting that there is increased neutrophil recruitmentecause of myocardial ischemia. Accordingly, attenuating neu-rophil-endothelial adherence after coronary revascularizationay reduce neutrophil-mediated injury.18 The study was lim-
ted by the removal of the coronary sinus catheter before chestlosure, precluding the measurement of MPO activity in the
Fig 5. (A) C3d levels were measured in serum samples that show
n increase at T2 and T6 compared with baseline (T0). (B) C5a levels
ere measured in serum samples that show a similar increase at T2
nd T6 compared with baseline (T0).
oronary sinus at T6. The results show that the addition of

sc
sctconAseatfl
tmecodtvrt
bairaasktiytmchTmm
tlcaw
cwtaisencIC
iadtccmepb
tno“wptaigtintpa
ts(aittrcr
af
i2
61SEVOFLURANE AND NEUTROPHIL ACTIVATION
evoflurane to cardioplegia decreased MPO activity in theoronary sinus blood after IR.
The findings also indicate that MPO activity in the coronaryinus blood is higher in patients who show early adverseardiac events after coronary revascularization. Although pa-ients in the study with a relatively lower MPO activity inoronary sinus blood also had fewer adverse cardiac eventsver the 4-year postoperative period, because of the smallumber of study subjects, a firm conclusion cannot be derived.dditionally, it remains to be clarified whether the effect of
evoflurane delivered via the cardioplegia is better than theffect produced by the administration of sevoflurane purely fornesthetic purposes or whether the improved myocardial pro-ection resulted from an improvement in the collateral bloodow leading to the better delivery of cardioplegia.Most volatile anesthetic agents inhibit the adhesion of neu-
rophils to the vascular endothelium in an ex vivo model ofyocardial ischemia.19,20 This may be because of the interfer-
nce of highly hydrophobic volatile anesthetics with the vas-ular endothelium membrane effect. Furthermore, the infusionf isolated hearts with activated neutrophils results in myocar-ial depression and the occurrence of reperfusion arrhythmiashrough the release of platelet-activating factor from the acti-ated neutrophils.1 Exposure of neutrophils to either sevoflu-ane or isoflurane effectively restores myocardial function inhese hearts.21
The cardioprotective role of volatile anesthetics remains toe clarified both physiologically and biochemically. Volatilenesthetics appear to exert their beneficial influence via cellularonic and metabolic processes that attenuate the inflammatoryesponse to IR.21,22 Decreasing inflammation has been associ-ted with reduced IR injury. At the cellular level, volatilenesthetics possess the ability to stimulate the production ofmall amounts of reactive species of oxygen, activate proteininase C, and subsequently prime mitochondrial adenosineriphosphate-regulated potassium (KATP) channels, probably byncreasing their phosphorylation status.23 Primed or phosphor-lated KATP channels allow earlier and more intense opening athe initiation of ischemia.23 The activation of KATP channelsaintains myocardial cell integrity and energy stores while
oronary circulation is interrupted. Volatile anesthetics alsoave the ability to reduce the adhesion of neutrophils after IR.20
hus, the use of a volatile anesthetic before an ischemic insultay lessen the inflammatory response generated by IR of theyocardium and its subsequent injurious effects.Neutrophil activation during CPB may also occur because of
he release of complement chemotactic products or local re-ease of IL-8. These results show that both IL-8 and theomplement system are activated during CPB. However, thedministration of sevoflurane attenuated the release of IL-8
ithout a significant effect on activation of the complement pREN
56, 2003
wat
r
ascade. Myocardial ischemia and reperfusion are associatedith the release of IL-8 and other chemoattractants in response
o locally produced endothelin-1 proteins.24,25 Patients withcute myocardial infarction have a transient but significant risen serum IL-8 concentration within 24 hours after the onset ofymptoms. The upregulation of mRNA for IL-8 and its pres-nce in the inflammatory infiltrate near the border betweenecrotic and viable myocardium have also been reported in aanine model of myocardial ischemia.26 Thus, it is believed thatL-8 is likely involved in the pathogenesis of IR injury afterABG surgery.Local generation of complement-related chemotactic factors
s also presumed to be involved in the infiltration of neutrophilst inflammatory sites in IR injury. C3d and C5a are generateduring activation of the complement system via the classic orhe alternative pathway, whereas C4b is released only duringlassic activation of the complement system. Release of myo-ardial subcellular components, such as mitochondria, com-only occurs during myocardial ischemia. These subcellular
lements are strong activators of proximal complement com-artments even in the absence of specific circulating autoanti-ody.27,28
The present data suggest activation of the complement sys-em during CPB as assessed by consumption of CH50, which isot generally inhibited by sevoflurane. However, the generationf a specific component of this system (C4b) involved in theclassic pathway” is blocked by sevoflurane. The classic path-ay of complement is triggered by an antigen-antibody com-lex and its role in IR is unknown. The alternative pathway ofhe complement cascade, on the other hand, is systemicallyctivated during aortic cross-clamping and utilization of CPBndependent of antigen. Activation of complement during sur-ical revascularization also occurs because of several factorshat are purely related to the patient response to the stressnduced by surgery and/or administered medications and mayot be controlled by anesthetic manipulations. Examination ofhe complement system during off-pump CABG surgery mayartially clarify this question by eliminating the effects of CPBnd reducing the number of heparin-protamine complexes.
In conclusion, cardiac surgery incites a vigorous inflamma-ory response, which may result in injurious consequences inome patients. The contribution of the inflammatory responseneutrophil, cytokine, and complement cascade activation) todverse patient outcomes is potentially modified by the admin-stration of sevoflurane. The development of optimal strategieso control these responses remains to be elucidated. Overall,hese findings confirm the anti-inflammatory effects of sevoflu-ane as suggested by previous studies. This may have importantlinical application in patients undergoing surgical coronaryevascularization in lieu of previous studies that have shown
rotective functional effects in myocardial ischemia.REFE
1. Montrucchio G, Alloatti G, Mariano F, et al: Role of platelet-ctivating factor in polymorphonuclear neutrophil recruitment in reper-used ischemic rabbit heart. Am J Pathol 142:471-480, 1993
2. Ren G, Dewald O, Frangogiannis NG: Inflammatory mechanismsn myocardial infarction. Curr Drug Targets Inflamm Allergy 2:242-
CES
3. Wong CK, French JK, Gao W, et al: Relationship between initialhite blood cell counts, stage of acute myocardial infarction evolution
t presentation, and incidence of thrombolysis in myocardial infarc-ion-3 flow after streptokinase. Am Heart J 145:95-102, 2003
4. Kukielka GL, Youker KA, Michael LH, et al: Role of early
eperfusion in the induction of adhesion molecules and cytokines in
p1
3
m2
th
ic
tA
ce
iB
o6
tiP
tr
sC
m1
e1
lc
ae
ac
wA
iod
tci
iC
iH
iJ
cv5
ci
62 NADER ET AL
reviously ischemic myocardium. Mol Cell Biochem 147:5-12,995
5. Nose PS: Cytokines and reperfusion injury. J Card Surg 8:305-08, 1993 (suppl)
6. Pudil R, Pidrman V, Krejsek J, et al: Cytokines and adhesionolecules in the course of acute myocardial infarction. Clin Chim Acta
80:127-134, 1999
7. Crystal GJ, Gurevicius J, Salem MR, et al: Role of adenosineriphosphate-sensitive potassium channels in coronary vasodilation byalothane, isoflurane, and enflurane. Anesthesiology 86:448-458, 1997
8. Drenger B, Ginosar Y, Chandra M, et al: Halothane modifiesschemia-associated injury to the voltage-sensitive calcium channels inanine heart sarcolemma. Anesthesiology 81:221-228, 1994
9. Wilde DW, Gutta R, Haney MF, et al: Effects of volatile anes-hetics on the intracellular Ca2� concentration in cardiac muscle cells.dv Exp Med Biol 301:125-141, 1991
10. Bradley PP, Priebat DA, Christensen RD, et al: Measurement ofutaneous inflammation: Estimation of neutrophil content with annzyme marker. J Invest Dermatol 78:206-209, 1982
11. Kilgore KS, Lucchesi BR: Reperfusion injury after myocardialnfarction: The role of free radicals and the inflammatory response. Cliniochem 26:359-370, 1993
12. Kraemer R, Mullane KM: Neutrophils delay functional recoveryf the post-hypoxic heart of the rabbit. J Pharmacol Exp Ther 251:620-26, 1989
13. Williams FM, Collins PD, Tanniere-Zeller M, et al: The rela-ionship between neutrophils and increased microvascular permeabilityn a model of myocardial ischaemia and reperfusion in the rabbit. Br Jharmacol 100:729-734, 1990
14. Biasucci LM, Liuzzo G, Caligiuri G, et al: Episodic activation ofhe coagulation system in unstable angina does not elicit an acute phaseeaction. Am J Cardiol 77:85-87, 1996
15. Baldus S, Heeschen C, Meinertz T, et al: Myeloperoxidaseerum levels predict risk in patients with acute coronary syndromes.irculation 108:1440-1445, 2003
16. Brennan ML, Penn MS, Van Lente F, et al: Prognostic value ofyeloperoxidase in patients with chest pain. N Engl J Med. 349:1595-
604, 2003 1
17. Podrez EA, Abu-Soud HM, Hazen SL: Myeloperoxidase-gen-rated oxidants and atherosclerosis. Free Radic Biol Med 28:1717-725, 200018. Chello M, Mastroroberto P, Patti G, et al: Simvastatin attenuates
eukocyte-endothelial interactions after coronary revascularization withardiopulmonary bypass. Heart 89:538-543, 2003
19. Mobert J, Zahler S, Becker BF, et al: Inhibition of neutrophilctivation by volatile anesthetics decreases adhesion to cultured humanndothelial cells. Anesthesiology 90:1372-1381, 1999
20. Kowalski C, Zahler S, Becker BF, et al: Halothane, isoflurane,nd sevoflurane reduce postischemic adhesion of neutrophils in theoronary system. Anesthesiology 86:188-195, 1997
21. Hu G, Vasiliauskas T, Salem MR, et al: Neutrophils pretreatedith volatile anesthetics lose ability to cause cardiac dysfunction.nesthesiology 98:712-718, 200322. Novalija E, Kevin LG, Eells JT, et al: Anesthetic precondition-
ng improves adenosine triphosphate synthesis and reduces reactivexygen species formation in mitochondria after ischemia by a redox-ependent mechanism. Anesthesiology 98:1155-1163, 200323. Light PE, Allen BG, Walsh MP, et al: Regulation of adenosine
riphosphate-sensitive potassium channels from rabbit ventricular myo-ytes by protein kinase C and type 2A protein phosphatase. Biochem-stry 34:7252-7257, 1995
24. Boyle EM Jr, Kovacich JC, Hebert CA, et al: Inhibition ofnterleukin-8 blocks myocardial ischemia-reperfusion injury. J Thoracardiovasc Surg 116:114-121, 199825. Abe Y, Kawakami M, Kuroki M, et al: Transient rise in serum
nterleukin-8 concentration during acute myocardial infarction. Breart J 70:132-134, 199326. Kukielka GL, Smith CW, LaRosa GJ, et al: Interleukin-8 gene
nduction in the myocardium after ischemia and reperfusion in vivo.Clin Invest 95:89-103, 199527. Pinckard RN, Olson MS, Giclas PC, et al: Consumption of
lassical complement components by heart subcellular membranes initro and in patients after acute myocardial infarction. J Clin Invest6:740-750, 197528. Weisman HF, Bartow T, Leppo MK, et al: Soluble human
omplement receptor type 1: In vivo inhibitor of complement suppress-ng postischemic myocardial inflammation and necrosis. Science 249:
46-151, 1990



















