Cardiopulmonary resuscitation: Knowledge and personal experience among dentists in Udaipur, India
9
Resuscitation (2008) 79, 490—498 available at www.sciencedirect.com journal homepage: www.elsevier.com/locate/resuscitation SIMULATION AND EDUCATION PAPER Cardiopulmonary resuscitation: Knowledge and opinions among the U.S. general public State of the science-fiction Catherine A. Marco a,∗ , Gregory L. Larkin b a St. Vincent Mercy Medical Center, Toledo, OH, United States b Yale University School of Medicine, United States Received 18 April 2008; received in revised form 11 July 2008; accepted 17 July 2008 KEYWORDS Cardiac arrest; Resuscitation; Public opinion Summary Background and objective: Cardiopulmonary resuscitation is undertaken more than 250,000 times annually in the United States. This study was undertaken to determine knowledge and opinions of the general public regarding cardiopulmonary resuscitation. Design: Validated multisite community-based cross-sectional survey. Outcome measures: Knowledge and opinions about resuscitative practices and outcomes, using hypothetical clinical scenarios and other social, spiritual, and environmental considerations. Results: Among 1831 participants representing 38 states, markedly inaccurate perceptions of cardiac arrest were reported. Participants’ mean estimate of predicted survival rate after car- diac arrest was 54% (median 50%, IQR 35—75%), and mean estimated duration of resuscitative efforts in the ED was 28 min (median 15 min; IQR 10—30). Projected age and health status were independent predictors of resuscitation preferences in a series of 4 hypothetical sce- narios. Participants indicated that physicians should consider patient and family wishes as the most important factors when making resuscitation decisions. Participants considered advanced technology and physician communication to be the most important actions during attempted resuscitation. Conclusions: Inaccurate perceptions regarding resuscitation and survival rates exist among the lay public. Participants indicated strong preferences regarding resuscitation and advance directives. © 2008 Elsevier Ireland Ltd. All rights reserved. A Spanish translated version of the summary of this arti- cle appears as Appendix in the final online version at doi:10.1016/j.resuscitation.2008.07.013. ∗ Corresponding author at: University of Toledo College of Medicine, 3045 Arlington Avenue, Mail Stop 1050, Toledo, OH 43614, United States. Tel.: +1 419 383 6343. E-mail address: [email protected] (C.A. Marco). Introduction Cardiopulmonary resuscitation is undertaken more than 250,000 times annually in the United States. Reported incidence rates vary significantly, and range from 35.7 to 128.3 per 100,000 (mean 62). 1—3 $58 million in Medicare expenditures are estimated to result from unsuccessful 0300-9572/$ — see front matter © 2008 Elsevier Ireland Ltd. All rights reserved. doi:10.1016/j.resuscitation.2008.07.013
-
Upload
independent -
Category
Documents
-
view
3 -
download
0
Transcript of Cardiopulmonary resuscitation: Knowledge and personal experience among dentists in Udaipur, India

Resuscitation (2008) 79, 490—498
avai lab le at www.sc iencedi rec t .com
journa l homepage: www.e lsev ier .com/ locate / resusc i ta t ion
SIMULATION AND EDUCATION PAPER
Cardiopulmonary resuscitation: Knowledge andopinions among the U.S. general publicState of the science-fiction!
Catherine A. Marcoa,∗, Gregory L. Larkinb
a St. Vincent Mercy Medical Center, Toledo, OH, United Statesb Yale University School of Medicine, United States
Received 18 April 2008; received in revised form 11 July 2008; accepted 17 July 2008
KEYWORDSCardiac arrest;Resuscitation;Public opinion
SummaryBackground and objective: Cardiopulmonary resuscitation is undertaken more than 250,000times annually in the United States. This study was undertaken to determine knowledge andopinions of the general public regarding cardiopulmonary resuscitation.Design: Validated multisite community-based cross-sectional survey.Outcome measures: Knowledge and opinions about resuscitative practices and outcomes, usinghypothetical clinical scenarios and other social, spiritual, and environmental considerations.Results: Among 1831 participants representing 38 states, markedly inaccurate perceptions ofcardiac arrest were reported. Participants’ mean estimate of predicted survival rate after car-diac arrest was 54% (median 50%, IQR 35—75%), and mean estimated duration of resuscitativeefforts in the ED was 28 min (median 15 min; IQR 10—30). Projected age and health statuswere independent predictors of resuscitation preferences in a series of 4 hypothetical sce-narios. Participants indicated that physicians should consider patient and family wishes as themost important factors when making resuscitation decisions. Participants considered advancedtechnology and physician communication to be the most important actions during attemptedresuscitation.Conclusions: Inaccurate perceptions regarding resuscitation and survival rates exist amongthe lay public. Participants indicated strong preferences regarding resuscitation and advancedirectives.© 2008 Elsevier Ireland Ltd. All rights reserved.
! A Spanish translated version of the summary of this arti-cle appears as Appendix in the final online version atdoi:10.1016/j.resuscitation.2008.07.013.
∗ Corresponding author at: University of Toledo College ofMedicine, 3045 Arlington Avenue, Mail Stop 1050, Toledo, OH 43614,United States. Tel.: +1 419 383 6343.
E-mail address: [email protected] (C.A. Marco).
Introduction
Cardiopulmonary resuscitation is undertaken more than250,000 times annually in the United States. Reportedincidence rates vary significantly, and range from 35.7 to128.3 per 100,000 (mean 62).1—3 $58 million in Medicareexpenditures are estimated to result from unsuccessful
0300-9572/$ — see front matter © 2008 Elsevier Ireland Ltd. All rights reserved.doi:10.1016/j.resuscitation.2008.07.013

Cardiopulmonary resuscitation: Knowledge and opinions among the U.S. general public 491
resuscitations annually in the U.S.4 Resuscitative effortsdemand extensive investments of resources, of equipment,physical space, personnel, and other resources. Recentreviews report widely variable survival rates for victims ofcardiac arrest, dependent on a number of factors, includingtime elapsed since arrest (down time),5—7 initial rhythm,8,9
response to prehospital ALS protocols,10,11 and long-termcare. Overall, survival for victims of cardiac arrest to hospi-tal discharge has been estimated between 0% and 10%.12—16
Despite this relatively low success rate, many hospitalpolicies (and out-of-hospital policies for EMS providers)typically suggest or mandate resuscitation for all patientsexcept those with prior Do Not Resuscitate (DNR) ordersor clear signs of death, such as rigor mortis or dependentlividity.on available data, several authors have suggestedproposed criteria for withholding resuscitative efforts.Several authors have suggested withholding resuscitativeefforts for patients in certain clinical settings with lowlikelihood of successful resuscitation (i.e. apneic, pulseless>10 min prior to EMS arrival, no response to ACLS, rhythmsof asystole or pulseless electrical activity, absence of pupil-lary reactions, pre-existing terminal disease).17,18 Althoughnumerous authors have suggested certain approaches toresuscitative decision making, the opinions of the generalpublic regarding resuscitation, financial investments inresuscitative efforts, and personal opinions are largelyunknown. This study was undertaken to identify the accu-racy of knowledge, and establish opinions of the generalpublic regarding cardiopulmonary resuscitation.
Methods
Approval for the study was obtained from the InstitutionalReview Boards of both institutions. This cross-sectionalsurvey was administered in community settings to 1831volunteer participants over a 4-month period in 2000.Community settings included airports, bus stations, and hos-pital waiting rooms in Pennsylvania and Ohio. The surveywas self-administered. Respondents indicated demographicinformation, responses to questions regarding personalhealth, advance directives, and knowledge base regardingcardiopulmonary resuscitation.
Survey instrument development and validation
The survey instrument was developed by the authors, inpart based on previously validated survey questions,19,20
and also included some innovative questions to addresspersonal opinions regarding resuscitation (Appendix B).Prior to the initiation of data collection, the surveyinstrument was piloted among lay volunteers and focusgroups. The survey instrument was also piloted among sur-vey experts, physicians, nurses, and medical students forcontent and question validity. Where appropriate, surveyrevisions were made to enhance clarity, readability, andaccuracy.
The survey was validated for internal reliability (Cron-bach’s alpha coefficient 0.9105). The survey instrument wasalso validated for consistency over time. Test—retest stabil-ity was assessed by administering the survey to 20 volunteerswho took the same test under the same conditions at 2-week intervals. The percentage of agreement index was.9856 or 98.6% index of agreement (95% CI = .9810—.9900).Table 1 summarizes hypothetical scenarios contained in thesurvey.
The survey was administered in the following communitysettings in Pennsylvania and Ohio: airport terminals, bus ter-minals, hospital waiting rooms, shopping malls, and collegecampuses.
Results
Demographics
Among 1831 participants representing 38 states, the meanage was 39 (median 40.0, range 14—98), and 55% werefemales; 72% had completed high school, and 57% reportedhousehold incomes of over $30,000 (Table 2).
Knowledge about cardiopulmonary resuscitation
Markedly inaccurate perceptions of cardiac arrest werenoted. Participants’ mean estimate of predicted survivalrate after cardiac arrest was 54% (median 50%, IQR 35—75%),and mean estimated duration of resuscitative efforts in
Table 1 Four hypothetical clinical scenarios.
1. Imagine you are very healthy, for example, 25 years old, and almost drowned, and your heart stoppedbeating. Would you want resuscitation attempted for you in the hospital ER?
Yes No UNSURE
2. Imagine that you are very healthy, 75 years old, and almost drowned, and your heart stopped beating.Would you want resuscitation attempted for you in the hospital ER?
—– Yes —– No —– UNSURE
3. Imagine that you are 25 years, terminally ill with cancer, with less than 6 months to live. If your heartstopped beating, would you want resuscitation attempted for you in the hospital ER?
—– Yes —– No —– UNSURE
4. Imagine that you are 75 years old, terminally ill with cancer, with less than 6 months to live. If yourheart stopped beating, would you want resuscitation attempted for you in the hospital ER?
—– Yes —– No —– UNSURE

492 C.A. Marco, G.L. Larkin
Table 2 Demographic information for 1831 studyparticipants.
Study participantsUS census 2000 data34
AgeMedian 40.0 years Median 35.5 yearsMean 39 yearsRange 14—98 years
GenderMale 45% 49.1%Female 55% 50.9%
RaceWhite 78.6% 75.1%Afro-American 17.1% 14.7%Hispanic 0.8% 12.5%Asian 2.1% 3.6%Other 1.3% 5.5%
Marital statusSingle 35.0% 27.1%Married 45.0% 56.2%Divorced 8.5% 10.0%Widowed 5.3% 6.5%
Education<High school 28% 58%High school+ 72% 42%
Income<$30,000 43% Median $37,000>$30,000 57%
the ED was 28 min (median 15 min; IQR 10—30). Compar-atively, data demonstrate the mean survival rate to be<5%,26—32 and mean resuscitation duration interval to be16.03 min.21
Personal resuscitation preferences
Participants rated each of the factors listed in Table 3, forimportance in the event of their own cardiac arrest. Par-ticipants also indicated which factors should be consideredby physicians making decisions regarding the initiation andtermination of resuscitative efforts (Table 4).
Participants indicated their own preferences in the eventof cardiac arrest, for a series of hypothetical scenarios
Table 3 Actions considered important to patients in theevent of cardiac arrest.
Action % who rankedimportant orvery important
Most advanced technology 90Physician communication with family 85Family presence in the hospital 72Prayer/other religious acts 57Clergy communication with family 53Family presence in resuscitation room 31
Table 4 Factors physicians should consider when makingresuscitation decisions.
Factor % who ranked importantor very important
Patient wishes 87Family wishes 60Health status 58Physician opinion/prediction
of outcome54
Age 37Occupation/role in society 14Citizenship 10
Table 5 Hypothetical scenarios: participants who woulddesire resuscitative efforts.
Scenario % of participants
25 years old, healthy patient,near-drowning
94
75 years old, healthy patient,sudden death
79
25 years old, terminally illpatient, sudden death
40
75 years old, terminally illpatient, sudden death
28
(Table 5). Although both projected age and health statuswere independent predictors of resuscitation preferences ina series of hypothetical scenarios, health status had greaterimpact on preferences.
Knowledge base regarding survival rates was stronglyassociated with resuscitation preferences. Participants whowould prefer resuscitative efforts for a hypothetical scenar-ios involving a young patient were more likely to estimate ahigher survival rate after cardiac arrest. Among patients whowould prefer resuscitative efforts for a 25 years old patient,the median estimated survival rate following cardiac arrestwas 50% (IQR 40—75%, p = 0.002, by Kruskal—Wallis nonpara-metric test), compared to an estimated survival rate of 30%(IQR 20—65%) among participants who would refuse resusci-tative efforts. There was no significant association betweenestimated survival rate and preferences involving an elderlypatient. Additionally, increased age of participants was asso-ciated with increased likelihood of refusal of resuscitativeefforts. Patient who would refuse resuscitative efforts inscenarios had a median age of 43, compared to median ageof 37 for patients who would agree to resuscitative efforts(p < 0.001, Kruskal—Wallis nonparametric test).
Most participants (N = 1606; 88%) indicated that thereshould be no age limit, beyond which resuscitative effortsshould routinely be withheld.
Advance directives
Although the majority of respondents had a personal physi-cian (N = 1476, 80.6%) only 10.9% (N = 200) of respondentshad ever discussed death or resuscitation with their physi-cians. Most respondents (N = 1411; 77.1%) believe that

Cardiopulmonary resuscitation: Knowledge and opinions among the U.S. general public 493
Table 6 Invasive procedures: percentage of participants who would find procedure acceptable.
Procedure Lay description Participants who find procedureacceptable
CPR CPR (chest compressions) 1352 (74%)Mouth-to-mouth Mouth-to-mouth breathing 1197 (65%)Defibrillation Electrical shocks (defibrillation) 1120 (61%)IV medicines Intravenous medicines 983 (54%)Endotracheal intubation Breathing tube in the windpipe (trachea) 884 (48%)Ventilator Artificial breathing on a respirator 777 (42%)Central line Large intravenous lines in the neck or groin 559 (31%)Unproven experimental technology Same 243 (13%)All of the above Same 590 (32%)
emergency department doctors and nurses should askpatients about advance directives, even if their lives arenot in danger.
Invasive procedures
Most participants (N = 1669; 91%) indicated a willingness toundergo cardiopulmonary resuscitative efforts, were they tohave a cardiac arrest at their current age and health status.Participants found the procedures in Table 6 (described inlayman’s terms) acceptable for themselves, in the event ofa cardiac arrest.
Financial issues
Many respondents indicated that the high costs paid bysociety are appropriate for attempted cardiac resuscitation(not necessarily successful) (Table 2). These opinions maybe supported by unrealistically optimistic expectations ofsurvival following cardiac arrest, as these participants esti-mated that 54% (mean; median 50% IQR 35—75%) of patientswill survive and function at baseline, following a cardiacarrest. Patients who estimated survival rates of over 50%were slightly more likely to indicate willingness to spendmore than $1000 on resuscitation attempts (67%), com-pared to those who estimated survival rates of under 50%(63%, p = 0.06, ! 2). Interestingly, participants also indicateda willingness to pay significant out-of-pocket expenses forthe individuals listed in Table 7.
Discussion
Knowledge
The findings of this study confirm previously reported unre-alistically high expectations of survival following cardiacarrest.22 Improved knowledge base regarding resuscitationmay affect patient preferences regarding resuscitation, andmay contribute to a heightened awareness and compliancewith advance directives.
Several recent reports indicate markedly inaccurate per-ceptions of the success rate of cardiac resuscitation. Manyin the general public presume that 50—60% of patients
with cardiac arrest will be successfully resuscitated.23 As ithas been demonstrated that accurate knowledge regardingprobability of survival influences patient preferences,24 theimportance of improved public education is underscored.The role of accurate public education is further accentu-ated by the dramatically unrealistic portrayals of successfulresuscitations by the media.25
Certain disparities in the acceptability of invasiveprocedures suggest knowledge deficiencies regarding resus-citation and associated procedures. For example, while70% of participants found endotracheal intubation accept-able, only 65% found a ventilator acceptable. The disparitybetween certain procedures (for example, only 77% foundintravenous medications acceptable) indicates a potentiallack of understanding of the significance of various inter-ventions.
Improving education of the general public is essential toimprovement in the determination and communication ofend of life medical care. A recent prospective interventionalstudy demonstrated that education of the general public
Table 7 Financial issues.
Maximum appropriate cost % of participants
A. Maximum appropriate cost to society per attemptedresuscitation$0—99 4$100—499 10$500—999 18$1000—5000 32>$5000 28
B. Individuals for which participants indicatedwillingness to pay >$1000 out-of-pocket expenses forattempted resuscitationIndividual % of participants willing to
pay >$1000 out-of-pocketChild/grandchild 76Spouse 74Elderly parent 69Self 68Penniless stranger 42President of the U.S. 42

494 C.A. Marco, G.L. Larkin
using an educational video can lead to improved knowl-edge about resuscitation, and affect personal preferencesregarding resuscitation.26 Future directions in public educa-tion may include increased uniform education of the generalpublic through the media, publications, or other venues.
Resuscitation preferences
Previous data demonstrates the general trend among emer-gency physicians was to attempt cardiac resuscitation for allvictims of cardiac arrest (unless a legal advance directiveexists).27 One speculation for justification of this practiceis the assumption that societal consensus regarding criti-cal care medical decision making is unachievable. However,this study affirms previous reports demonstrating consistenttrends for refusal of resuscitative efforts in hypotheticalsituations with previously documented poor outcomes.28,29
Inadequacy of advance directives to communicatetreatment preferences
Despite public education, education within the medicalcommunity, and legal mandates (such as the 1991 Fed-eral Patient Self-Determination Act) to increase publicawareness of the importance of advance directives, onlya minority of patients (estimated 10—20%) have com-pleted advance directives.28,29 Without advance directivesphysicians and families often erroneously assume incor-rect information regarding patients’ wishes.30 Even whenan advance directive exists, compliance may be vari-able, dependent upon the clinical circumstances.31 Theseinadequacies of advance directives suggests the needfor additional rational approaches to improving physicianawareness of patients’ wishes. Although some health careproviders are reluctant to discuss issues such as end-of-lifecare and advance directives, this study reaffirms previousfindings demonstrating that patients welcome the opportu-nity to discuss their wishes.32,33
Despite the fact that most people want to discuss deathand dying with their physicians, only a minority have doneso. Additionally, participants believe that physicians andnurses should routinely ask about end of life preferences,even in situations where their lives are not in danger.
Limitations
This study has limitations common to all self-administeredsurvey data. Participants’ responses may accurately rep-resent knowledge and opinions. Because participation wasvoluntary, participants may represent those who have strongopinions about the issues, or may represent those with moretime available to participate in the survey.
Sampling techniques may have also introduced bias.The study was conducted primarily in Pennsylvania andOhio. Only 38 states were represented among participants.Because a large percentage of participants were recruited
in travel settings (airports, bus stations), they may repre-sent the more mobile segments of society. Although thepopulation sampled closely resembles the data from theU.S. census (Table 2), certain differences may have affectedresults (including slightly higher mean age, under represen-tation of the Hispanic population, slightly increased % ofsingle participants, and increased educational level).
Conclusions
Inaccurate perceptions regarding resuscitation and survivalrates exist among the lay public. Many people have strongpersonal opinions regarding resuscitation, personal prefer-ences, financial issues, and factors that should be consideredwhen making resuscitation decisions. Respondents supporthigh financial expenditures for attempted cardiac resusci-tation. Improved public education regarding resuscitation,and heightened efforts to improve communication regardingresuscitation preferences are indicated.
Conflict of interest statement
The authors have no conflicts of interest to disclose.
Acknowledgement
The authors wish to thank Nancy Buderer, MS, for her assis-tance with data analysis.
Funding/support: This project was supported in part bygrants from The Douglass Foundation, Toledo, Ohio, andMercy Foundation of Pittsburgh, Pittsburgh, Pennsylvania.
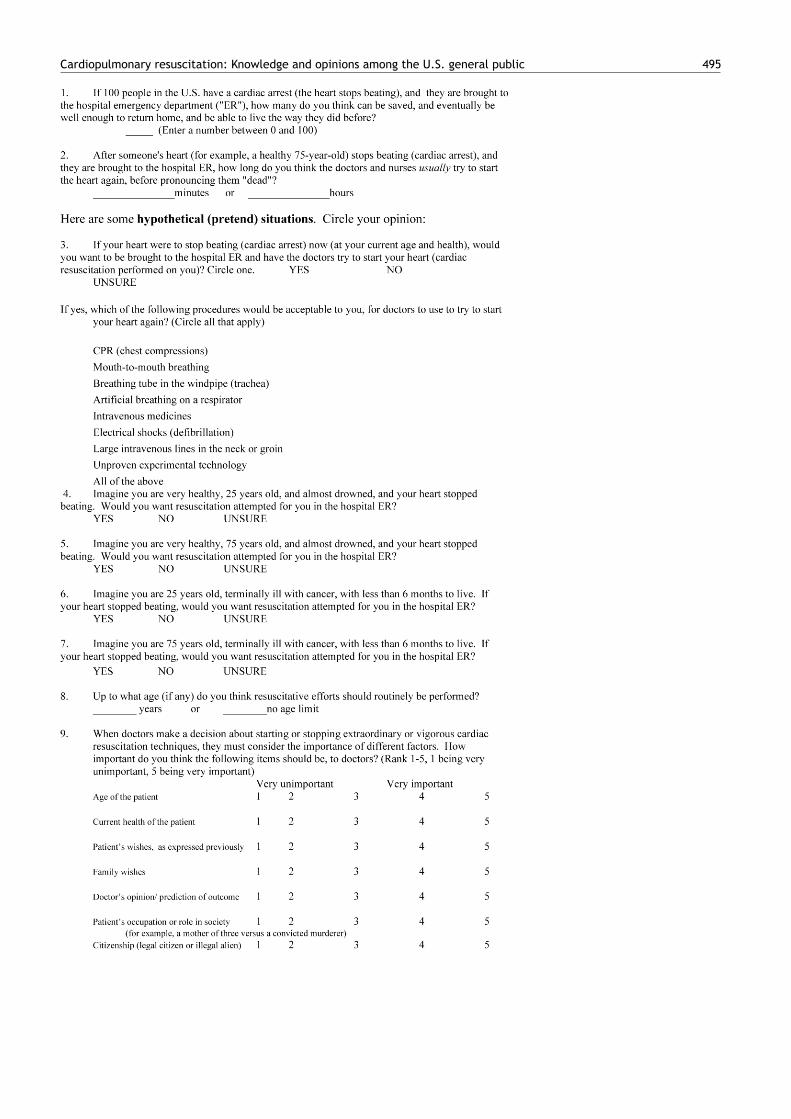
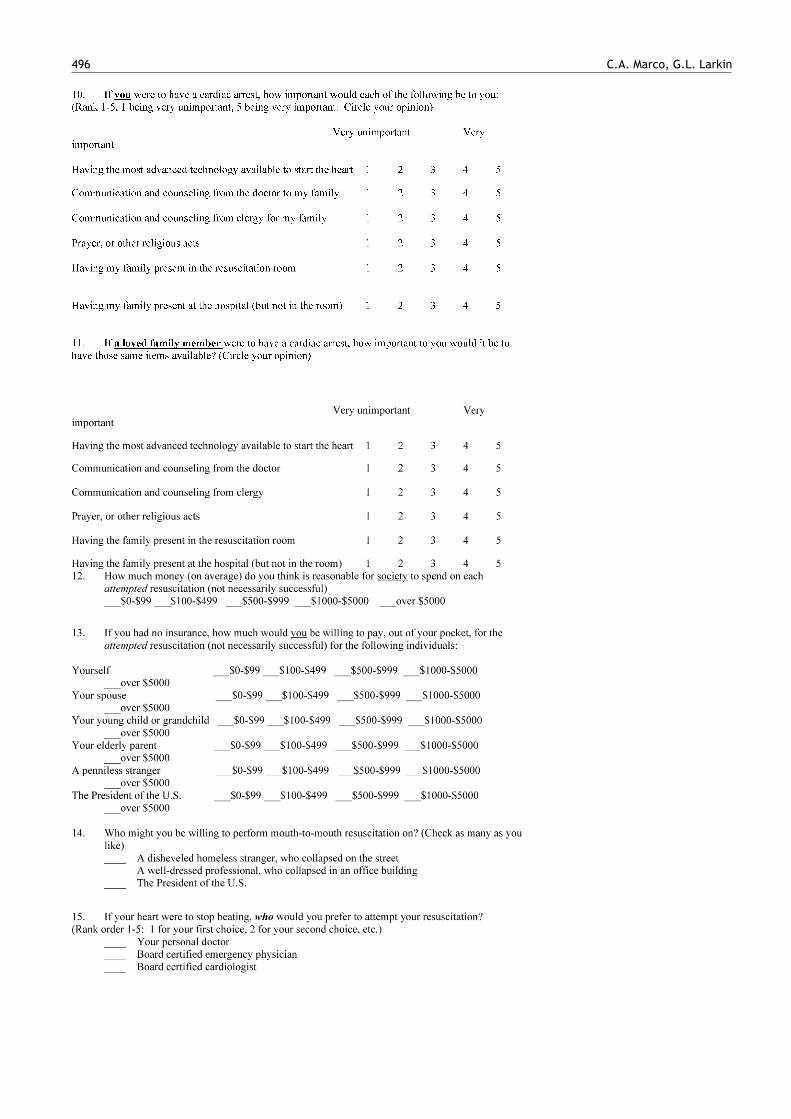
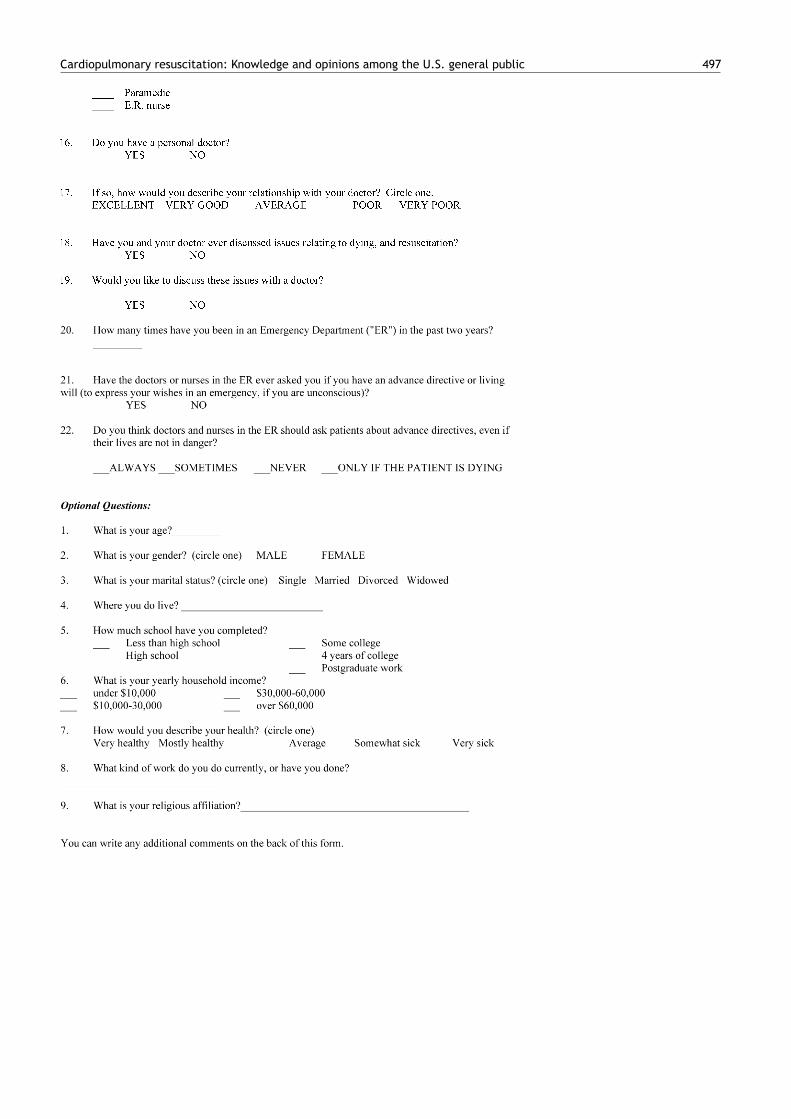
Appendix A. SURVEY
The following brief questions are part of a research sur-vey about ‘‘cardiac arrest’’ (when the heart stops beating).We need to learn more about what people think about theefforts of doctors, nurses, and paramedics to start the heartagain, after it has stopped (‘‘cardiac resuscitation’’).
The results will be kept anonymous and confidential. Yourname will not be on any part of the study. Your participationis voluntary. Your participation, or lack of participation, willin no way affect the care of you, your friends, or your family.You can change your mind at any time, and drop out of thestudy. We expect the study to take about 5—10 min of yourtime.
All the questions are about ‘‘cardiac arrest’’ (when theheart stops beating), and ‘‘cardiac resuscitation’’ (effortson the part of the doctors and nurses to start the heartagain). We are not asking these questions because of anyrisk for cardiac arrest, on your part. We just want to knowwhat you think about these issues.
Please answer the following questions to the best ofyour ability. Do not worry about whether your answersare right or wrong. We want to know what you think.
Cardiopulmonary resuscitation: Knowledge and opinions among the U.S. general public 495
496 C.A. Marco, G.L. Larkin
Cardiopulmonary resuscitation: Knowledge and opinions among the U.S. general public 497
498 C.A. Marco, G.L. Larkin
References
1. Ballew KA, Philbrick JT. Causes of variation in reportedin-hospital CPR survival: a critical review. Resuscitation1995;30:203—15.
2. American Heart Association. Heart and stroke statisticalupdate. Dallas, Texas: American Heart Association, 2002.
3. Zheng ZJ, Croft JB, Giles WH, Mensah GA. Sudden cardiacdeath in the United States, 1989 to 1998. Circulation 2001;104:2158.
4. Suchard JR, Fenton FR, Powers RD. Medicare expenditureson unsuccessful out-of-hospital resuscitations. J Emerg Med1999;17:801—5.
5. Vukmir RB. Witnessed arrest, but not delayed bystander car-diopulmonary resuscitation improves prehospital cardiac arrestsurvival. Emerg Med J 2004;21:370—3.
6. Vukmir RB. Sodium bicarbonate study group: the influence ofurban, suburban, or rural locale on survival from refractoryprehospital cardiac arrest. Am J Emerg Med 2004;22:90—3.
7. The Public Access Defibrillation Trial Investigators. Public-access defibrillation and survival after out-of-hospital cardiacarrest. N Engl J Med, 2004; 351:637—46.
8. Nadkarni VM, Larkin GL, Peberdy MA, et al. First documentedrhythm and clinical outcomes from in-hospital cardiac arrestamong children and adults. JAMA 2006;295:50—7.
9. Bobrow BJ, Clark LL, Ewy GA, et al. Minimally interruptedcardiac resuscitation by emergency medical services for out-of-hospital cardiac arrest. JAMA 2008;299:1158—65.
10. Schoenenberger RA, von Planta M, von Planta I. Survival afterfailed out-of-hospital resuscitation: are further therapeuticefforts in the emergency department futile? Arch Intern Med1994;154:2433—8.
11. Bonnin MJ, Pepe PE, Kimball KT, et al. Distinct criteria for ter-mination of resuscitation in the out-of-hospital setting. JAMA1993;270:1457—62.
12. Nichol G, Stiell IG, Laupacis A, Pham B, De Maio VJ,Wells GA. A cumulative meta-analysis of the effectiveness ofdefibrillator-capable emergency medical services for victims ofout-of-hospital cardiac arrest. Ann Emerg Med 1999 Oct;34(4 Pt1):517—25.
13. Bohm K, Rosenqvist M, Herlitz J, et al. Survival is similarafter standard treatment and chest compression only in out-of-hospital bystander cardiopulmonary resuscitation. Circulation2007;116:2908—12.
14. Callaham M, Madsen CD. Relationship of timeliness of paramedicadvanced life support interventions to outcome in out-of-hospital cardiac arrest treated by first responders withdefibrillator. Ann Emerg Med 1995;27:638—48.
15. Stratton SJ, Niemann JT. Outcome from out-of-hospital cardiacarrest caused by nonventricular arrhythmias: contribution ofsuccessful resuscitation to overall survivorship supports the cur-rent practice of initiating out-of-hospital ACLS. Ann Emerg Med1998;32:448—53.
16. Varon J, Fromm RE. In-hospital resuscitation among the elderly:substantial survival to hospital discharge. Am J Emerg Med1996;14:130—2.
17. Bonnin MJ, Pepe PE, Kimball KT, Clark Jr PS. Distinct criteriafor termination of resuscitation in the out-of-hospital setting.JAMA 1993;270:1457—62.
18. Kellerman AL, Hackman BB, Somes G. Predicting the outcomeof unsuccessful prehospital advanced cardiac life support. JAMA1993;270:1433—6.
19. Marco CA, Schears RM. Resuscitation preferences: feasibility ofestablishing societal consensus (abstract). Ann Emerg Med 1998October, abstract number 166.
20. Marco CA, Schears RM. Resuscitation preferences amongthe general public (abstract). Acad Emerg Med 2000;7:532—3.
21. Schears RM, Marco CA, Larkin GL. Does gender bias exist inresuscitation practices? (abstract) Presented at Society for Aca-demic Emergency Medicine Regional Research Forum. Michigan:Ann Arbor, 1999 September.
22. Roberts D, Hirschman D, Scheltema K. Adults and pediatric CPR:attitudes and expectations of health professionals and layper-sons. Am J Emerg Med 2000;18:465—8.
23. Jones GK, Brewer KL, Garrison HG. Public expectations of sur-vival following cardiopulmonary resuscitation. Acad Emerg Med2000;7:48—53.
24. Murphy DJ, Burrows D, Santilli S, et al. The influence of theprobability of survival on patients’ preferences regarding car-diopulmonary resuscitation. N Engl J Med 1994;330:545—9.
25. Diem SJ, Lantos JD, Tulsky JA. Cardiopulmonary resuscita-tion on television: miracles and misinformation. N Engl J Med1996;334:1578—82.
26. Marco CA, Larkin GL. Public education regarding resuscita-tion: effects of a multimedia intervention. Ann Emerg Med2003;42:256—60.
27. Marco CA, Schoenfeld CN, Bessman ES, Kelen GD. Ethical issuesof cardiopulmonary resuscitation: a survey of emergency physi-cians. Acad Emerg Med 1997;4:898—904.
28. Teno J, Lynn J, Wenger N, et al. Advance directives for seri-ously ill hospitalized patients. J Am Geriatr Soc 1997;45:508—12.
29. The SUPPORT Principle Investigators. A controlled trial toimprove care for seriously ill hospitalized patients. JAMA 274,1995: 1591—98.
30. Layson RT, Adelman HM, Wallach PM, Pfeifer MP, Johnston S,McNutt RA. Discussions about the use of life-sustaining treat-ments: a literature review of physicians’ and patients’ attitudesand practices. J Clin Ethics 1994;5:195—203.
31. Dull SM, Graves JR, Larsen MP, Cummins RO. Expected death andunwanted resuscitation in the prehospital setting. Ann EmergMed 1994;23:997—1001.
32. Kerridge IH, Pearson SA, Rolfe IE, Lowe M. Decision making inCPR: attitudes of hospital patients and healthcare profession-als. Med J Austr 1998;169:128—31.
33. Uhlmann RF, Pearlman RA. Perceived quality of life and prefer-ences for life-sustaining treatment in older adults. Arch InternMed 1991;151:495—7.
34. US Census Data. www.governmentguide.com, accessed Septem-ber 20, 2002.