
A Reliable Method for Rhythm Analysis during Cardiopulmonary Resuscitation

http://prf.sagepub.com
Perfusion
DOI: 10.1177/0267659108094739 2008; 23; 117 Perfusion
F Urdaneta, EB Lobato, T Beaver, JD Muehlschlegel, DS Kirby, C Klodell and A Sidi analog
Treating pulmonary hypertension post cardiopulmonary bypass in pigs: milrinone vs. sildenafil
http://prf.sagepub.com/cgi/content/abstract/23/2/117 The online version of this article can be found at:
Published by:
http://www.sagepublications.com
can be found at:Perfusion Additional services and information for
http://prf.sagepub.com/cgi/alerts Email Alerts:
http://prf.sagepub.com/subscriptions Subscriptions:
http://www.sagepub.com/journalsReprints.navReprints:
http://www.sagepub.co.uk/journalsPermissions.navPermissions:
http://prf.sagepub.com/cgi/content/refs/23/2/117 Citations
by Avner Sidi on October 17, 2008 http://prf.sagepub.comDownloaded from
Treating pulmonary hypertension postcardiopulmonary bypass in pigs:milrinone vs. sildenafil analogF Urdaneta1,3, EB Lobato1,3, T Beaver2, JD Muehlschlegel1, DS Kirby3, C Klodell2 and A Sidi1
1Department of Anesthesiology, University of Florida College of Medicine, and Anesthesia Service; 2Department ofSurgery, University of Florida College of Medicine, and Anesthesia Service; 3Malcom Randall Veterans AdministrationMedical Center, Gainesville, Florida
Procedures using cardiopulmonary bypass (CPB) and aor-tic cross-clamping are associated with a variable degreeof ischemia/reperfusion of the lungs, leading to acute pul-monary hypertension (PHT). The purpose of this studywas to compare the effects of the sildenafil analog(UK343-664), a phosphodiesterase type V(PDEV) inhibi-tor, with milrinone, a PDE type III inhibitor, in a porcinemodel of acute PHT following CPB. After the pigs wereanesthetized, pressure-tipped catheters were placed inthe right ventricle and carotid and pulmonary arteries.Cardiac output was measured with an ultrasound probeon the ascending aorta. After heparinization and place-ment of aortic and right atrial cannulae, non-pulsatileCPB was instituted and cardioplegia administered follow-ing aortic cross-clamping. After 30 minutes, the clampwas removed and the animals re-warmed and separatedfrom CPB in sinus rhythm. The animals were randomizedto 3 groups, and 16 animals were studied to completion:milrinone (n=5) 50 μg/kg; sildenafil-analog (n=5)500 μg/kg; and normal saline (NS) (n=6). Hemodynamic
data were collected at baseline pre-CPB and, followingtermination of CPB, at baseline, 5, 10 and 30 minutesafter administration of the drug. Pulmonary hypertensionwas present in all groups following CPB. After adminis-tration of the drugs, mean pulmonary artery pressuredecreased in all 3 groups; however, only in thesildenafil-analog group did pulmonary vascular resis-tance(PVR) decrease by 35%, from 820 to 433 dynes · cm ·sec-5 at 5 minutes (p<0.05), and continued to be decreasedat 10 minutes by 26% (P<0.05). Pulmonary selectivity wasdemonstrated with sildenafil-analog, because there wereno similar changes in systemic vascular resistance(SVR)and no significant changes in systemic hemodynamics.Sildenafil-analog, a PDEV inhibitor, shows a promisingrole for managing the PVR increases that occur followingCPB. Perfusion (xx) 23, 117–125.
Key words: Pulmonary Hypertension; Milrinone; Cardio-pulmonary Bypass; Sildenafil
Introduction
Procedures using cardiopulmonary bypass (CPB)and aortic cross-clamping are associated with a vari-able degree of ischemia/reperfusion of the lungs,leading to acute pulmonary vasoconstriction. Theentity of “post-perfusion lung injury” after prolongedcardiopulmonary bypass has been well known sincethe 1960s and was related to various postulatedetiologies.1 We know, today, that extensive contactbetween blood and artificial surfaces during CPBactivates a host of mediators, including the comple-ment cascade, thrombin, oxygen free radicals and
vasoactive mediators. This results in the activationof platelets and neutrophils. In addition to theseexcessive stimuli, CPB is associated with functionalalteration of the endothelial cells, which may play amajor role in the development of post-CPB pulmo-nary hypertension (PHT).2 Endothelial cells producevasodilators such as nitric oxide (NO), and vasocon-strictors such as thromboxane A2 and endothelin I.Thus, the increase in pulmonary vascular resistance(PVR) is partially mediated by the release of cyto-kines, oxygen radicals, and inflammatory mediatorsthat lead to pulmonary vasospasm, PHT and perivas-cular edema.
Acute PHT and elevated pulmonary vascular resis-tance, associated with cardiac surgery involving car-diopulmonary bypass (CPB), can be a cause ofmorbid-ity and mortality during the post-operative period.3 Atranspulmonary gradient of >15 mmHg and a PVR ofmore than eight Wood units are associated with a sig-nificantly increased incidence of right ventricular dys-function as well as peri-operative morbidity andmortality.4 Failure of the right ventricle(RV) is an
Perfusion 2008; 23: 117–125
Correspondence to: Avner Sidi, MD, Department of Anesthesiol-ogy, University of Florida College of Medicine, Box 100254,JHMHSC, 1600 SW Archer Road, Gainesville, Florida.Email: [email protected]
Support was provided solely from institutional and/ordepartmental funds. No reprints are available from the author.Presented in part at: 25th Annual Meeting of the Society of Cardio-vascular Anesthesiologists, April 26-30, 2003, Miami, FL [AnesthAnalg 96:SCA75, 2003].
© 2008 SAGE Publications, Los Angeles, London, New Delhi and Singapore 10.1177/0267659108094739 by Avner Sidi on October 17, 2008 http://prf.sagepub.comDownloaded from

important life-threatening problem in this specific set-ting and may account for approximately 1/2 of all car-diac complications and 1/5 of all early deaths.5 Theprognostic significance of intraoperative hemody-namic abnormalities, including PHT, in relation toadverse post-operative outcomes was reported byReich, et al.6 In patients with pre-existing PHT, theexaggerated pulmonary vasoreactivity at the end ofCPB can lead to acute right ventricular dysfunctionand an increased risk of peri-operative morbidity andmortality.7–15 Preventing and treating PHT post-bypassshould improve outcome.
The pulmonary vasculature is rich in phosphodies-terase enzymes type III (PDEIII) and type V (PDEV),which inactivate cyclic AMP (cAMP) and cyclicGMP (cGMP), respectively.16–20 The increased genera-tion of these two secondary intracellular mediatorsinduces smooth muscle relaxation. Agents that blockthe activity of these enzymes have received significantinterest for their potential therapeutic benefits. Milri-none, an inhibitor of PDEIII, is commonly used toimprove heart function after CPB. Furthermore, thisdrug has been particularly useful in patients with con-comitant PHT.21 The PDEV inhibitor, sildenafil, hasbeen shown to reduce pulmonary vascular resistancein patients with chronic PHT.22 Similarly, the prelimi-nary use of sildenafil has been effective in reducingpost-operative PHT in children following heartsurgery.23 In addition, we have shown, in a porcinemodel, that the pulmonary vascular effects of thenew intravenous sildenafil analog, UK343-664, arecomparable to those of milrinone during acute PHT.24
Early clinical experience with sildenafil in patientswith PHT post cardiac surgery is encouraging25–27
and better than with PDEIII inhibitors,28,29 especiallyin view of its selective effect on the pulmonary circu-lation similar to other PDEV inhibitors.30–32 As men-tioned above, the intravenous sildenafil analog,UK343-664, has been shown previously to comparefavorably to the PDEIII inhibitor milrinone duringthromboxane-mediated PHT.24 However, because thepossible mechanisms of post-bypass PHT are not iden-tical to this specific thromboxane model, the purposeof this study was to compare the effects of intravenoussildenafil-analog with milrinone in a porcine model ofacute PHT following CPB.
Material and methods
The protocol was approved by the University of Flor-ida Institutional Animal Care and Use Committee.Animals were handled in accordance with guide-lines established by the National Institutes of Health(NIH publication 85-23, revised 1985).
Twenty-one domestic swine weighing 50 to 55 kgwere sedated with intramuscular ketamine (35 mg/kg)and anesthetized with one percent isoflurane in 100%oxygen. A tracheostomy was then performed and theanimals mechanically ventilated at 12 breaths perminute, with tidal volumes of 12 mL/kg, to maintainan end-tidal CO2 between 32 and 36 mmHg. Anesthe-sia and mechanical ventilation were maintained withthe use of a Narkomed 4 anesthesia machine (NorthAmerican Drager, Telford, PA). Pancuronium wasused for muscle relaxation during the surgicalpreparation.
After the pigs were anesthetized, pressure-tippedcatheters were placed in the right ventricle andcarotid and pulmonary arteries. A seven French (Fr),pressure-tipped, flotation pulmonary artery catheter(Millar Instruments Inc, Houston, TX) was insertedvia the right internal jugular vein into the main pul-monary artery through an eight Fr Cordis introducer(Arrow International, Reading, PA). A seven Fr, tri-ple lumen, central venous catheter was placedthrough the left internal jugular vein. The left carotidartery was exposed, and a five Fr pressure-tippedcatheter (Millar Instruments Inc.) was placed andadvanced into the ascending aorta for continuousarterial pressure monitoring. A median sternotomywas then performed and the heart placed in a peri-cardial cradle. Cardiac output (CO) was measuredwith a 10 mm perivascular ultrasound probe placedin the main pulmonary artery. All transducers wereconnected to a biomedical amplifier (Grass model7D, Grass Instruments Co, Quincy, MA). The signalswere digitized and continuously recorded at 200 Hzon a personal computer for later analysis (Sono-metrics Corp, London, Ontario, Canada). Systemicanticoagulation was induced with 300 IU/kg of hep-arin to achieve an ACT > 480 seconds. Following theplacement of ascending aortic and right atrial two-stage venous cannulae, non-pulsatile CPB was insti-tuted with the use of a roller pump (Bard, Haverhill,MA). The circuit was primed with 1000 mL of Hart-mann’s solution, 20 grams of mannitol, and 60 mgof heparin. A non-pulsatile flow of 2.5 L/min/m2
was used, and the animals were cooled to 28°C.The hematocrit was kept between 25% and 28%throughout CPB, using fluids (crystalloids) to controlits level. After placement of the aortic cross-clamp, asingle dose (20 mEq KCl) of hyperkalemic, antegradecardioplegia was administered. The aortic clampwas removed after 30 minutes, and the animalswere re-warmed and weaned from CPB without theuse of inotropes after normal sinus rhythm wasaccomplished. The animals were weaned from CPBwithout pharmacological assistance. The heart wasgradually filled, titrating to CVP and blood pressure.
Hypertension, sildenafil, bypassF Urdaneta, et al.
118
by Avner Sidi on October 17, 2008 http://prf.sagepub.comDownloaded from

The CO was measured following weaning from CPB(and, with it, PVR and SVR were derived).
Protamine reversal of heparinization was notundertaken after weaning from CPB, in order toavoid its influence on pulmonary vasoactivity.There was no attempt to control and titrate PAP/PAOP or CO (PAOP=pulmonary artery occlusionpressure) to a given level, or to keep the pre-loadhemodynamic end-point at a certain level. The onlyparameters that were controlled were the CPB time,aortic cross-clamp time, bypass flow, and hematocrit.
Approximately 10 minutes following the separa-tion from CPB in the presence of hemodynamic sta-bility, the animals were randomized to three separategroups: the first group (n = seven) received milrinone(loading dose of 50 μg/kg); the second group (n =seven) received UK343-664 (500 μg/kg); and thethird group (n = seven) served as control andreceived 20 mL of normal saline solution.
Hemodynamic measurementsHemodynamic measurements included systemicarterial pressure, pulmonary artery pressure, centralvenous pressure, pulmonary artery occlusion pres-sure, and CO. Baseline data were collected prior toCPB once the animals were fully instrumented. Post-CPB data were collected 10 minutes after cessation ofCPB with stable hemodynamics, and at baseline,five, 10 and 30 minutes after the administration ofthe drugs.
Pulmonary and systemic vascular resistances werecalculated using standard formulas (PVR= MPAP-PAOP/CO; SVR=MAP-CVP/CO; where PVR = pulmo-nary vascular resistance, SVR= systemic vascularresistance, MPAP=mean pulmonary artery pressure,PAOP=pulmonary artery occlusion pressure,CVP=central venous pressure, and CO=cardiacoutput).
Drug preparationLyophilized UK343-664 (Pfizer Pharmaceuticals,Sandwich, Kent, UK) was mixed with sterile water.This solution was diluted in normal saline to rendera final concentration of 10 mg/mL. Milrinone lactateat a concentration of 1 mg/mL was administeredintravenously undiluted (Sanofi-Synthelabo, Pharm,New York, NY).
All drugs were administered through a centralvenous catheter over five minutes via an infusionpump (Medfusion 2010, Medex Inc, Duluth, GA).
Statistical analysisData were expressed as mean ± standard deviations.A repeated two-way analysis of variance (ANOVA)was utilized, followed by the Student Newman-
Keuls test for multiple comparisons. A p<0.05 wasconsidered significant.
Results
Sixteen pigs were studied to completion; the numberof subjects lost to study was similar for all threegroups studied. Three animals (one in each group)did not survive the entire experiment due to hemo-dynamic instability with PHT; two animals (one ineach of the treatment groups), did not survive dueto technical difficulty in the CBP preparation accord-ing to the protocol. Thus, 16 animals were studied tocompletion: 5 in each one of the treatment groups(UK343-664 and milrinone), and 6 in the controlgroup.
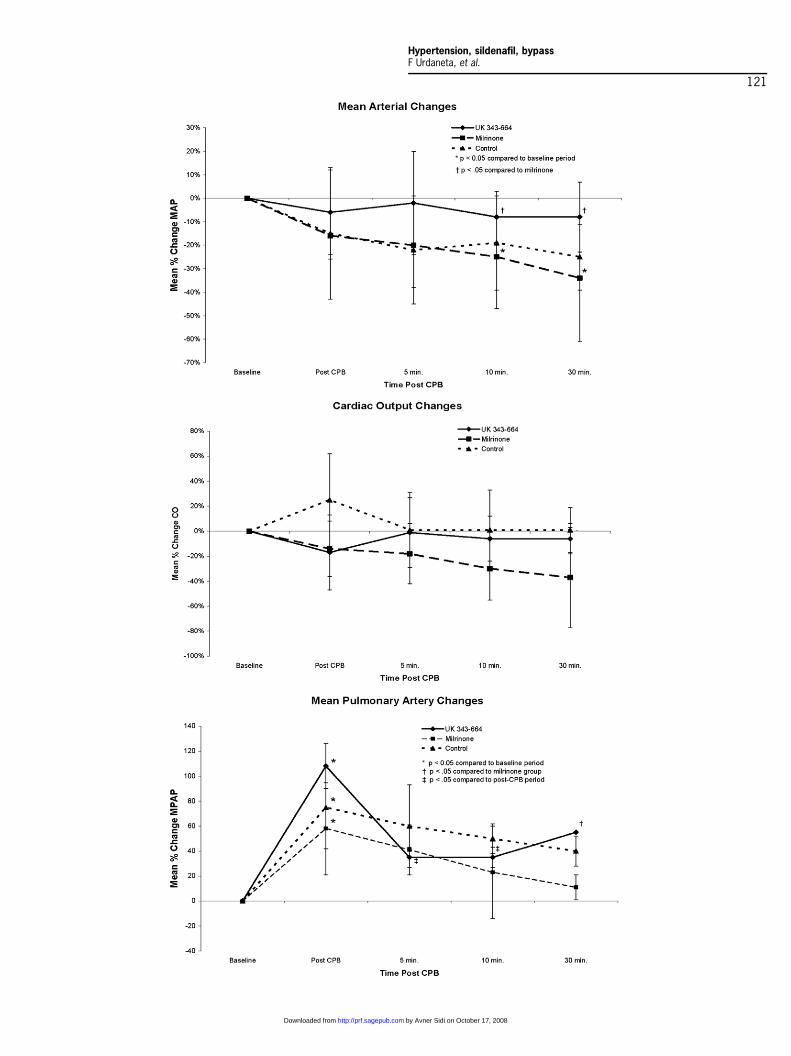
Table 1 shows the measured hemodynamic datain the three groups, and Figure 1 shows the %changes from baseline of the systemic mean arteialand pulmonary pressures, and the CO, in differentstages pre and post CPB. There were no significantdifferences among them at baseline (Table 1).
Following CPB, mean arterial pressure (MAP) wasessentially unchanged. In the milrinone group, MAPdecreased immediately post CPB by 16% comparedto baseline (Figure 1, top), and CO was alsodecreased by 14% in this group (Figure 1, middle);however, the changes were not statistically signifi-cant. Only in the control group was there a modest,but still not significant, increase in CO compared tothe treatment groups. Pulmonary hypertension waspresent in all groups following CPB, and all the ani-mals had an increase in MPAP and CVP followingCPB (Table 1 and Figure 1, bottom) (p<0.05). In allanimals, the MPAP was elevated immediately fol-lowing CPB, with a % change magnitude that wasnot statistically different among the 3 groups (108 ±18, 58 ± 33, and 75 ± 37% in the UK343-664, milri-none, and control groups, respectively) (Figure 1,bottom).
The administration of the drugs changed the sys-temic pressures significantly, but only after the first10 minutes following CPB (Figure 1, top). All ani-mals had preserved systemic hemodynamics in thefirst 10 minutes following CPB. Thirty minutes fol-lowing drug administration, MAP was significantlyreduced in the milrinone group (40 ± 10% changefrom baseline), although, in the UK343-664 group,MAP was reduced only by 8 ± 15% (p<0.05) (Fig-ure 1, top). After the administration of the drugs,mean pulmonary arterial pressure (MPAP) decreasedin all three groups (from 108 ± 18 to 35 ± 8%, from58 ± 33 to 41 ± 33%, from 75 ± 37 to 60 ± 20%,respectively); however, only in the UK343-664
Hypertension, sildenafil, bypassF Urdaneta, et al.
119
by Avner Sidi on October 17, 2008 http://prf.sagepub.comDownloaded from

group did the decrease reach statistical significance(Table,1 Figure 1, bottom) (p<0.05). Also, the % dropin MPAP within 5 minutes was greatest in theUK343-664 group (73%, 17%, and 15% drop, respec-tively). This trend persisted for the first 10 minutes ofthe post-CPB period.
The trend of decreasing from PHT post-CPB, per-sisted throughout the period following CBP and drugadministration, for the control and milrinone groups,and up to 10 minutes post drug administration in theUK343-664 group. However, after 30 minutes, therecovery toward baseline levels was significantlybetter (11 ± 12% change from baseline) in the milri-none group (Figure 1, bottom) than in the UK343-664group (55 ± 0%) (p < 0.05).
Stable (increase of 1±18%) CO in the controlgroup persisted, even 30 minutes following CPB,and was not significantly different from the decreasein CO in the milrinone group, which was 37 ± 40%(Figure 1, middle).
Pulmonary and systemic vascular resistance valuesare presented in Figures 2 and 3, respectively.Figure 2 demonstrates the changes in PVR. In boththe control and milrinone groups, there was no signif-icant change in PVR after the administration of thedrug. In the UK343-664 group, PVR decreased by35%, from 820 to 433 dynes · cm · sec-5 at five minutes(p < 0.05) and by 26% (p < 0.05) at 10 minutes. At 30minutes, there was only an additional 17% reduction(non-significant). Figure 3 demonstrates the changesin SVR. There were no significant changes in SVRwithin or among the groups following CPB.
Dicussion
The major findings in this study demonstrate thatPHT, which was present in all groups followingCPB, was treated effectively only by the sildenafilanalog, UK343-664. The pulmonary pressure and
Table 1 Measured hemodynamic data in the three groups (sildenafil analog [UK343-664], milrinone, and control group) in differenttime periods throughout the experiment. Baseline data were collected prior to cardiopulmonary bypass. Post-CPB data were collectedat baseline, 10 minutes after-CPB and at five, 10 and 30 minutes after drug administration
Hemodynamic variables Group Baseline After CPB 5 min 10 min 30 min
MPAP (mm Hg) UK343-664 20 ± 11 41.5 ± 13* 27 ± 9† 27 ± 9† 31 ± 11Milrinone 17 ± 6 27 ± 8* 24 ± 8 21 ± 5 19 ± 5Control 20 ± 5 35 ± 8* 32 ± 7 30 ± 8 28 ± 6
MAP (mm Hg) UK343-664 68 ± 9 65 ± 11 70 ± 15 63 ± 10 63 ± 10Milrinone 84 ± 16 71 ± 3 68 ± 11 63 ± 9 56 ± 9Control 88 ± 7 76 ± 16 75 ± 13 72 ± 11 76 ± 12
CVP (mm Hg) UK343-664 6 ± 2 15 ± 4* 12 ± 2 13 ± 4 13 ± 4Milrinone 4 ± 2 12 ± 3* 14 ± 2 10 ± 5 10 ± 5Control 6 ± 2 14 ± 3* 14 ± 2 12 ± 4 11 ± 5
POAP (mmHg) UK343-664 8 ± 4 9 ± 3 9 ± 4 11 ± 3 11 ± 4Milrinone 10 ± 4 12 ± 4 8 ± 3 9 ± 4 10 ± 2Control 8 ± 2 11 ± 3 12 ± 3 10 ± 4 9 ± 2
HR (bpm) UK343-664 95 ± 14 110 ± 7 103 ± 14 105 ± 15 105 ± 15Milrinone 92 ± 18 119 ± 11 127 ± 24 124 ± 24 103 ± 7Control 98 ± 6 120 ± 6 115 ± 8 110 ± 8 117 ± 6
CO (L/min) UK343-664 3.34 ± 1.34 2.78 ± 1.39 3.32 ± 1.73 3.16 ± 1.73 3.16 ± 1.73Milrinone 3 ± 0.7 2.6 ± 0.3 2.46 ± 0.5 2.3 ± 0.5 1.9 ± 1Control 3.0 ± 1.5 4.0 ± 1.4 3.1 ± 1.0 3.1 ± 1.1 3.1 ± 1
*p<0.05 compared to baseline; †p<0.05 compared to after-CPB.All values are mean +/-standard deviation. CO=cardiac output; CPB=cardiopulmonary bypass; CVP=central venous pressure; HR=heartrate; MAP=mean arterial pressure; MPAP=mean pulmonary arterial pressure; PAOP=pulmonary artery occlusion pressure.
Figure 1 Changes in systemic hemodynamic variables from baseline values described as percent (%) changes of MAP (top), CO (mid-dle), MPAP (bottom) in the three groups – sildenafil analog (UK343-664), milrinone, and control group - in different time periodsthroughout the experiment. Baseline data were collected prior to cardiopulmonary bypass (CPB). Post-CPB data were collected 10 min-utes after CPB (after-CBP), and at five, 10 and 30 minutes after the administration of the drugs. Thirty minutes following drug adminis-tration, MAP was significantly reduced in the milrinone group (40±10% change from baseline), when UK343-664 group was reducedonly by 8±15% (p0.05) (Figure 1 top). A minimal and non-significant increase (1±18%) in CO in the control group persisted even30 minutes following CPB, and was not significantly different from the decrease in CO in the milrinone group which was 37±40% (Fig-ure 1, middle). Pulmonary hypertension was present in all groups following CPB. However, after 30 minutes the recovery to baselinelevels was significantly better (11±12% change from baseline) in the milrinone group (Figure 1, bottom) than in the UK343-664 group(55±0%) (p0.05). All values represent mean ±SEM. CPB=cardio?pulmonary bypass; MAP=mean arterial pressure; CO=cardiac output;MPAP=mean pulmonary artery pressure. *p0.05 compared to baseline period; †p0.05 compared to milrinone group, in the sameperiod; ‡p0.05 compared to Post-CPB period.
Hypertension, sildenafil, bypassF Urdaneta, et al.
120
by Avner Sidi on October 17, 2008 http://prf.sagepub.comDownloaded from
Hypertension, sildenafil, bypassF Urdaneta, et al.
121
by Avner Sidi on October 17, 2008 http://prf.sagepub.comDownloaded from

resistance were significantly decreased at five and at10 minutes only in the sildenafil-analog group. Onlythe sildenafil-analog group demonstrated decreasedpulmonary resistance within five minutes from drugadministration by more than one-third of the maxi-mal values, and it remained significantly lower foranother five minutes. The pulmonary selectivitywas demonstrated, because there were no similarchanges in systemic resistance, and hemodynamicvariables remained stable. Thirty minutes followingdrug administration, systemic and pulmonary pres-sure were significantly decreased in the milrinonegroup, systemic pressure was not decreased in thesildenafil-analog group, and pulmonary pressurechanges were similar in the milrinone and control,but different from the sildenafil-analog group. Thisprobably means that the sildenafil-analog effect onPHT with this dose lasted for less than 30 minutes.
The experimental designThe porcine model is quite reliable for demonstrat-ing PHT immediately following CPB. The majority ofpulmonary perfusion in the porcine model isthrough the pulmonary artery, and only a smallamount is by the bronchial arteries. In the absenceof pulmonary flow, and following reperfusion inthis model, the lungs exhibit physiological and path-ological changes of “ischemia-reperfusion” injury. Ithas been demonstrated that CPB produces a dramaticand steady increase over 120 min in both mean pul-monary arterial pressure (>75%) and pulmonary vas-cular resistance (>200%).33 In our study, pulmonarypressure increased one and one-half to two-foldpost-CBP in all three groups. This increase was notsignificantly different among the groups. Systemicpressure at the same time was decreased by approxi-mately 10%. Thus, the systemic-to-pulmonary pres-sure ratio decreased from four-to-one to two-to-one,clearly indicating pulmonary hypertension in allthree groups. To simulate clinical conditions, thelevel of PHT was not controlled or titrated, but ratherwas a result of a “natural course” of the CPB. Therewas no attempt to manipulate cardiac pressures, or tomaintain a particular hemodynamic endpoint. Thus,the only parameters that were controlled were theCPB time, aortic cross-clamp time, bypass flow, andhematocrit.
The dose of sildenafil or its analog given is consis-tent with several studies that used the same amount(500 μg/kg i.v.).27,34,35 The suggested oral dose is 0.5to 1 mg/kg34,35 and the intravenous dose is 0.25 to1 mg/kg. The milrinone dose was similar to the effec-tive dose used in animals,32 or to the clinically usedlow-dose of 25 μ/kg/min.10 This study did notattempt to determine a dose-response curve, but
rather evaluate any drug-related hemodynamiceffects based on prior observations (sildenafil) orrecommended clinical dose (milrinone).
Limitations of the studyWe did not assess any drug combination in the pres-ent study, since we did not aim to evaluate the effectof PDEIII inhibitor with PDEV inhibitor in a model ofacute PHT following CPB. We already demonstratedin a recent study36 that the combination of PDEV andPDEIII inhibitors may provide a better hemodynamicprofile, with the advantage of greater pulmonaryvasodilatation and biventricular inotropism.
Superficially, it may look like there is a statisticalartifact when pulmonary pressure is increased themost in the UK343-664 group before drug adminis-tration, and, therefore, the decrease in this groupwith the drug is more pronounced. However, relativechange post-CBP of 108 ± 18% is not different from58 ± 33% and 75 ± 37% and represents a similar oneand one-half to two-fold increase post-CBP in allthree groups. However, the relative decrease from108 ± 18 to 35 ± 8% is significantly different fromthe decrease from 58 ± 33 to 41 ± 33%, and from75 ± 37 to 60 ± 20%. Thus, the difference betweenthe three groups was in pulmonary pressureresponse to drug: UK343-664 caused pulmonarypressure to decrease from the peak post-CBP hyper-tension level, while milrinone and placebo (control)did not. These differences were amplified when rel-ative changes were calculated. It is not surprising tofind an enhanced reactivity or response to an anti-hypertensive drug, in situations of increased pulmo-nary hypertension, as we found with the dramaticeffect on elevated pulmonary pressure usingUK343-664.37 In a similar way, enhanced pressorresponse was demonstrated in chronically hypoxicrats treated with captopril, probably attributable toincreased sensitivity to angiotensin II.38
Several reports have recently described the use oforal sildenafil in cardiac surgical patients to facilitatethe withdrawal of NO during placement ofventricular assist devices or in the post-operativeperiod,25,26,39 suggesting a possible role for sildenafilin the treatment of peri-operative PHT. The efficacyof sildenafil in achieving pulmonary vascularrelaxation has been demonstrated in the acute andchronic settings.22,27,40 There is general agreementthat the effects of sildenafil in the pulmonary circu-lation are a result of PDEV inhibition, thus, enhanc-ing intracellular cyclic GMP (cGMP) levels.41
Although the negative inotropic effects of increasedcGMP have been described, there is little evidencethat sildenafil decreases contractility. In fact, recentdata suggest a cardioprotective effect of sildenafil
Hypertension, sildenafil, bypassF Urdaneta, et al.
122
by Avner Sidi on October 17, 2008 http://prf.sagepub.comDownloaded from

against myocardial ischemia and reperfusioninjury.42 The improvement in CO was not statisti-cally significant in our study with the sildenafil ana-log, UK343-664, but no negative inotropic effectswere found either.
It is important to mention that we, like others,observed a relative degree of pulmonary selectivityafter the administration of sildenafil.23,25–27,36 Sys-
temic vascular resistance, however, was relativelypreserved when compared to the group that receivedmilrinone. As this study demonstrated, the use of thesildenafil analog, UK343-664, post bypass surgeryduring acute pulmonary vasoconstriction is veryeffective without the risk of increased systemic vaso-dilation. This combination has the potential forcreating better hemodynamic conditions in the
Figure 3 Changes in systemic vascular resistance (SVR) in the three groups – sildenafil analog (UK343-664), milrinone, and controlgroup - in different time periods throughout the experiment. Baseline data were collected prior to cardiopulmonary bypass (CPB). Post-CPB data were collected 10 minutes after CPB (after-CBP), and at five, 10 and 30 minutes after the administration of the drugs. Therewere no significant changes in SVR within or between the groups following CPB. All values represent mean ±SEM. SVR units are indynes · cm · sec-5.
Figure 2 Changes in pulmonary vascular resistance (PVR) in the three groups – sildenafil analog (UK343-664), milrinone, and controlgroup - in different time periods throughout the experiment. Baseline data were collected prior to cardiopulmonary bypass (CPB). Post-CPB data were collected 10 minutes after CPB (after-CBP), and at five, 10 and 30 minutes after the administration of the drugs. Pulmo-nary hypertension was present in all groups following CPB. In the UK343-664 group, PVR decreased by 35% at five minutes, (p<0.05)and by 26% (p<0.05) at 10 minutes. At 30 minutes, there was a 17% reduction (non-significant). All values represent mean±SEM. PVRunits are in dynes · cm · sec-5. *p<0.05 compared to baseline; †p<0.05 compared to After-CPB.
Hypertension, sildenafil, bypassF Urdaneta, et al.
123
by Avner Sidi on October 17, 2008 http://prf.sagepub.comDownloaded from

post-bypass period, thus facilitating weaning frommechanical ventilation, inhaled NO, and other ino-tropes and pulmonary vasodilators. The peri-operative treatment of acute PHT with traditionalagents such as nitrosodilators, beta adrenergic ago-nists, and PDEIII inhibitors is limited by the risk ofhypotension as a result of their non-selectivity andsystemic vasodilatory effects.38,39,43 Patients withpre-existing PHT seem to be at higher risk becausethey frequently require high doses of these agents.Inhibition of PDEIII by drugs such as milrinone isassociated with systemic vasodilatation and tendsto occur due to the lack of pulmonaryselectivity.28,29 On the other hand, the inhibition ofPDEV by certain drugs, such as zaprinast, dipyrida-mole, or sildenafil, is associated with selectivepulmonary vasodilatation.30–32 Although inhaledNO is a potent selective pulmonary vasodilator, ithas several limitations; it requires a specializeddelivery system, and its use is still not widely avail-
able even though it is used at many centers that carefor newborns or when PHT patients (e.g. post-cardiacsurgery) are seen.12–15 Another alternative for NO isinhaled prostacyclin.11,18,44 Both inhaled prostacyclinand inhaled nitrosodilators are much more pulmo-nary specific than when given parenterally.
In conclusion, this preliminary study demon-strated that the administration of the sildenafilanalog UK343-664 was associated with greater pul-monary relaxation and a more stable hemodynamicprofile than milrinone. Future studies will betterdefine the role of sildenafil and other PDEV inhibi-tors as part of a multimodal approach in the treat-ment of peri-operative PHT.
Acknowledgments
Support was provided solely from institutional and/or departmental funds.
References
1 Tilney, NL, Hester, WJ. Physiologic and histologicchanges in the lungs of patients dying after prolongedcardiopulmonary bypass: an inquiry into the nature ofpost-perfusion lung. Ann Surg. 1967; 166: 759–766.
2 Wessel, DL, Adatia, I, Giglia, TM, Thompson, JE, Kulic,TJ. Use of inhaled nitric oxide and acetylcholine in theevaluation of pulmonary artery hypertension andendothelial function after cardiopulmonary bypass.Circulation 1993; 88: 447–453.
3 Hopkins, RA, Bull, C, Haworth, SG, Leval, MR, Stark, J.Pulmonary hypertensive crises following surgery forcongenital heart defects in young children. Eur JCardio-thorac Surg 1991; 5: 628–634.
4 Wahlers, TH, Beer, C, Fieguth, HG, et al. Right heartfailure following orthotopic cardiac transplantation.Clin Transplant 1988; 2: 252–256.
5 Kaye, MP. The registry of the International Society forHeart and Lung Transplantation: 10th official report—1993. J Heart Lung Transplant 1993; 12: 541–548.
6 Reich, DL, Bodian, CA, Krol, M, Kuroda, M, Osinski, T,Thys, DM. Intraoperative hemodynamic predictors ofmortality, stroke, and myocardial infarction after coro-nary artery bypass surgery. Anesth Analg. 1999; 89:814–822.
7 Ocal, A, Kiris, I, Erdinc, M, Peker, O, Yavuz, T, Ibrisim,E. Efficiency of prostacyclin in the treatment ofprotamine-mediated right ventricular failure andacute pulmonary hypertension. Tohoku J Exp Med2005; 207: 51–58.
8 Fattouch, K, Sbraga, F, Sampognaro, R, et al. Treatmentof pulmonary hypertension in patients undergoingcardiac surgery with cardiopulmonary bypass: a ran-domized, prospective, double-blind study. J Cardio-vasc Med (Hagerstown) 2006; 7: 119–123.
9 Ibrahim, M, Hendry, P, Masters, R, et al. Managementof acute severe perioperative failure of cardiac allo-grafts: a single-centre experience with a review of theliterature. Can J Cardiol 2007; 23: 363–367.
10 Oztekin, I, Yazici, S, Oztekin, DS, Goksel, O, Issever, H,Canik, S. Effects of low-dose milrinone on weaningfrom cardiopulmonary bypass and after in patientswith mitral stenosis and pulmonary hypertension.Yakugaku Zasshi 2007; 127: 375–383.
11 Lowson, SM, Doctor, A, Walsh, BK, Doorley, PA.Inhaled prostacyclin for the treatment of pulmonaryhypertension after cardiac surgery. Crit Care Med2002; 30: 2762–2764.
12 Ichinose, F, Roberts, JD, Zapol, W. Inhaled nitric oxide:a selective pulmonary vasodilator: current uses andtherapeutic potentials. Circulation 2004; 109: 3106–3111.
13 Fullerton, DC, Mc Intyre, RC Jr. Inhaled nitric oxide:therapeutic applications in cardiothoracic surgery.Ann Thorac Surg 1996; 61: 1856–1864.
14 Schmid, ER, Burki, C, Engel, MH, Schmidlin, D,Tornic, M, Seifert, B. Inhaled nitric oxide versus intra-venous vasodilators in severe pulmonary hypertensionafter cardiac surgery. Anesth Analg 1999; 89: 1108–1115.
15 McMullan, DM, Bekker, JM, Johengen, MJ, et al.Inhaled nitric oxide-induced rebound pulmonaryhypertension: role for endothelin-1. Am J PhysiolHeart Circ Physiol 2001; 280: H777–H785.
16 Bradford, KK, Deb, B, Pearl, RG. Combination therapywith inhaled nitric oxide and intravenous dobutamineduring pulmonary hypertension in the rabbit. J Cardio-vasc Pharmacol 2000; 36: 146–151.
17 Pascual, JM, Fiorelli, AI, Bellotti, GM, Stolf, NA, Jatene,AD. Prostacyclin in the management of pulmonaryhypertension after heart transplantation. J Heart Trans-plant 1990; 9: 644–651.
18 Van Obbergh, LJ, Charbonneau, M, Blaise, G. Combina-tion of inhaled nitric oxide with IV nitroglycerin orwith a prostacyclin analogue in the treatment of exper-imental pulmonary hypertension. Br J Anaesth 1996;77: 227–231.
Hypertension, sildenafil, bypassF Urdaneta, et al.
124
by Avner Sidi on October 17, 2008 http://prf.sagepub.comDownloaded from

19 Tonz, M, von Segesser, LK, Schilling, J, et al. Treat-ment of acute pulmonary hypertension with inhalednitric oxide. Ann Thorac Surg 1994; 58: 1031–1035.
20 Dent, G, Magnussen, H, Rabe, KF. Cyclic nucleotidephosphodiesterases in the human lung. Lung 1994;172: 129–146.
21 Chen, EP, Bittner, HB, Davis, RD, Van Trigt, P. Hemo-dynamic and inotropic effects of milrinone after hearttransplantation in the setting of recipient pulmonaryhypertension. J Heart Lung Transplant 1998; 17: 669–678.
22 Bhatia, S, Frantz, RP, Severson, CJ, Durst, LA, McGoon,MD. Immediate and long-term hemodynamic and clin-ical effects of sildenafil in patients with pulmonaryarterial hypertension receiving vasodilator therapy.Mayo Clin Proc 2003; 78: 1207–1213.
23 Schulze-Neick, I, Hartenstein, P, Li, J, et al. Intravenoussildenafil is a potent pulmonary vasodilator in childrenwith congenital heart disease. Circulation 2003; 108(Suppl 1): II167–II173.
24 Bonnell, M, Urdaneta, F, Kirby, DS, Valdez, N, Beaver,TM, Lobato, EB. Effects of a sildenafil analog UK343-664 on a porcine model of acute pulmonary hyperten-sion. Ann Thorac Surg 2004; 77: 238–242.
25 Atz, AM, Wessel, DL. Sildenafil ameliorates effect ofinhaled nitric oxide withdrawal. Anesthesiology 1999;91: 307–310.
26 Mychaskiw, G, Sachdev, V, Heath, BJ. Sildenafil(Viagra) facilitates weaning of inhaled nitric oxide fol-lowing placement of a biventricular device. J ClinAnesth 2001; 13: 218–220.
27 Weimann, J, Ullrich, R, Hromi, J, et al. Sildenafil is apulmonary vasodilator in awake lambs with acute pul-monary hypertension. Anesthesiology 2000; 92: 1702–1712.
28 Tanaka, H, Tajimi, K, Moritsune, O, Kobayashi, K,Okada, K. Effects of milrinone on pulmonary vascula-ture in normal dogs and in dogs with pulmonaryhypertension. Crit Care Med 1991; 19: 68–74.
29 Tanaka, H, Tajimi, K, Matsumoto, A, Kobayashi, K.Vasodilatory effects of milrinone on pulmonary vascu-lature in dogs with pulmonary hypertension due topulmonary embolism: a comparison with those ofdopamine and dobutamine. Clin Exp Pharmacol Phy-siol 1990; 17: 681–690.
30 Tsai, BM, Wang, M, Pitcher, JM, Kher, A, Crisostomo,P, Meldrum, DR. Zaprinast attenuates hypoxic pulmo-nary artery injury and causes less aortic relaxation thanmilrinone. Shock 2005; 24: 417–420.
31 Schermuly, RT, Krupnik, E, Tenor, H, et al. Coaeroso-lization of phosphodiesterase inhibitors markedlyenhances the pulmonary vasodilatory response toinhaled iloprost in experimental pulmonary hyperten-sion. Maintenance of lung selectivity. Am J Respir CritCare Med 2001; 164: 1694–1700.
32 Matot, I, Gozal, Y. Pulmonary responses to selectivephosphodiesterase-5 and phosphodiesterase-3 inhibi-tors. Chest 2004; 125: 644–651.
33 Carteaux, JP, Roux, S, Siaghy, M, et al. Acute pulmo-nary hypertension after cardiopulmonary bypass inpig: the role of endogenous endothelin. Eur J Cardi-othorac Surg 1999; 15: 346–352.
34 Trachte, AL, Lobato, EB, Urdaneta, F, et al. Oral silden-afil reduces pulmonary hypertension after cardiac sur-gery. Ann Thorac Surg 2005; 79: 194–197.
35 Ghofrani, HA, Voswinckel, R, Reichenberger, F, et al.Differences in hemodynamic and oxygenation responsesto three different phosphodiesterase-5 inhibitors inpatients with pulmonary arterial hypertension: a ran-domized prospective study. J Am Coll Cardiol 2004; 44:1488–1496.
36 Lobato, EB, Beaver, T, Muehlschlegel, J, Kirby, DS,Klodell, C, Sidi, A. Treatment with phosphodiesteraseinhibitors type III and V: milrinone and sildenafil is aneffective combination during thromboxane-inducedacute pulmonary hypertension. Br J Anaesth 2006; 96:317–322.
37 Steiner, MK, Preston, IR, Klinger, JR, Hill, NS. Pulmo-nary hypertension: inhaled nitric oxide, sildenafil andnatriuretic peptides. Curr Opin Pharmacol 2005; 5:245–250.
38 Russell, PC, Emery, CJ, Cai, YN, Barer, GR, Howard, P.Enhanced reactivity to bradykinin, angiotensin I andthe effect of captopril in the pulmonary vasculature ofchronically hypoxic rats. Eur Respir J 1990; 3: 779–785.
39 Madden, BP, Sheth, A, Ho, TB, Park, JE, Kanagasabay,RR. Potential role for sildenafil in the management ofperioperative pulmonary hypertension and right ven-tricular dysfunction after cardiac surgery. Br J Anaesth2004; 93: 155–156.
40 Mikhail, GW, Prasad, SK, Li, W, et al. Clinical and hae-modynamic effects of sildenafil in pulmonary hyper-tension: acute and mid-term effects. Eur Heart J 2004;25: 431–436.
41 Rybalkin, SD, Yan, C, Bornfeldt, KE, Beavo, JA. CyclicGMP phosphodiesterases and regulation of smoothmuscle function. Circ Res 2003; 93: 280–291.
42 Ockaili, R, Salloum, F, Hawkins, J, Kukreja, RC. Silden-afil (Viagra) induces powerful cardioprotective effectvia opening of mitochondrial K (ATP) channels in rab-bits. Am J Physiol Heart Circ Physiol 2002; 283:H1263–H1269.
43 Kieler-Jensen, N, Milocco, I, Ricksten, SE. Pulmonaryvasodilation after heart transplantation. A comparisonamong prostacyclin, sodium nitroprusside, and nitro-glycerin on right ventricular function and pulmonaryselectivity. J Heart Lung Transplant 1993; 12: 179–184.
44 Lowson, SM. Inhaled alternatives to nitric oxide. Anes-thesiology 2002; 96: 1504–1513.
Hypertension, sildenafil, bypassF Urdaneta, et al.
125
by Avner Sidi on October 17, 2008 http://prf.sagepub.comDownloaded from
Copyright © 2022 FDOKUMEN




















