
The Christocentric Principle: Promise, Pitfalls, and Proposal
Upload
independentCategory
view
2download
0
Pitfalls Of Surgical Technique For Coronary Artery Bypass Surgery
Ito Puruhito MD*, Heru Kusbianto MD*, Jai Raman MD§, Brian Buxton FRACS §,
Tri Wahyu MD¥, Rahim Sobarna MD**
* Airlangga University, Surabaya, Indonesia
§ Austin Repatriation Hospital, Melbourne, Australia
¥ Hasan Sandiki Hospital, Bandung, Indonesia
** R.S. Harapan Kita, Jakarta, Indonesia
Despite increasing numbers of patients receiving venous and arterial grafts during coronary artery bypass graft surgery, cardiac surgeons still face a number of pitfalls. Based on our experience with 8,000 patients during the past 20 years, we describe some of the most common pitfalls in coronary artery bypass surgery. (Asia Pacific J Thorac Cardiovasc Surg 1995;4(2);60-66)
Introduction
The surgical technique of coronary artery bypass grafting (CAB G) has evolved from the use of internal mammary artery grafts and saphenous vein grafts to the use of abdominal arteries such as the gastroepiploic and the inferior epigastric arteries. More recently, radial arteries have been used as bypass conduits.
Despite the evolution from venous to arterial bypass grafts, many pitfalls are common to these operations. A description of some pitfalls of grafting using the saphenous vein and arterial grafts may be helpful to the surgeon entering the field of CABG surgery. This paper is based on the experience of about 8,000 CABG procedures performed in Surabya and in Melbourne between 1975 and 1995.
The Distal Anastomosis
Eccentric arteriotomy
Ideally, the artery should be opened longitudinally in its midline. Calcification, an eccentric plaque, a thin arterial wall, or an intramyocardial location may predispose to a surgical error when performing the arteriotomy.
Eccentric entry into the lumen or entry into the wall of the artery may be the result of a large plaque on one side (Fig. lA).
Usually this is easily corrected by extending the arteriotomy proximally and distally so that the incision finishes in the midline of the artery. Although the anastomosis may be longer than usual, careful attention to the suture line at either end of the artery will provide a good result.
60
Fig. 1. A. Eccentric opening of coronary artery. B. Dissection of coronary artery. C. Perforation of posterior wall of coronary artery.
Dissection
Coronary artery dissection occurs occasionally when opening into an area of an artery with an atheromatous or calcified plaque, and occurs more frequently in patients with loose attachment between the inner and outer layers of the arterial wall (Fig. IB). Coronary artery dissection can be avoided in most cases by careful selection of the site of the arteriotomy, avoiding the diseased segments.
A localised dissection may be used as the site of origin for an endarterectomy. However this procedure has become less popular because of the poor long-term results. Management of a coronary artery dissection requires careful suturing with apposition of the 2 layers during the anastomosis. Failure to include the inner layer of the sac with the dissection is likely to result in graft occlusion (Fig. 2A). The correct suture technique is shown in Fig. 2B.
Asia Pacific J Thorac Cardiovasc Surg 1995;4(2)
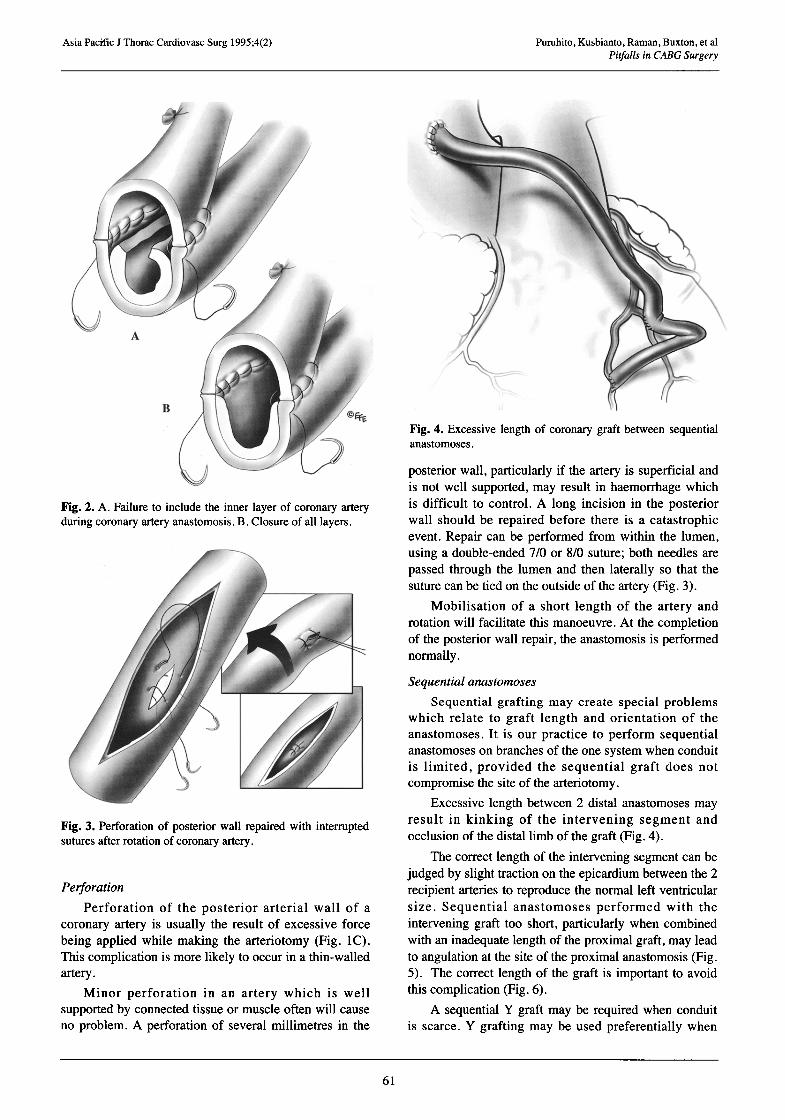
Fig. 2. A. Failure to include the inner layer of coronary artery during coronary artery anastomosis. B. Closure of all layers.
Fig. 3. Perforation of posterior wall repaired with interrupted sutures after rotation of coronary artery.
Perforation
Perforation of the posterior arterial wall of a coronary artery is usually the result of excessive force being applied while making the arteriotomy (Fig. IC). This complication is more likely to occur in a thin-walled artery.
Minor perforation in an artery which is well supported by connected tissue or muscle often will cause no problem. A perforation of several millimetres in the
61
Puruhito, Kusbianto, Raman, Buxton, et al Pitfalls in CABG Surgery
Fig. 4. Excessive length of coronary graft between sequential anastomoses.
posterior wall, particularly if the artery is superficial and is not well supported, may result in haemorrhage which is difficult to control. A long incision in the posterior wall should be repaired before there is a catastrophic event. Repair can be performed from within the lumen, using a double-ended 7/0 or 8/0 suture; both needles are passed through the lumen and then laterally so that the suture can be tied on the outside of the artery (Fig. 3).
Mobilisation of a short length of the artery and rotation will facilitate this manoeuvre. At the completion of the posterior wall repair, the anastomosis is performed normally.
Sequential anastomoses
Sequential grafting may create special problems which relate to graft length and orientation of the anastomoses. It is our practice to perform sequential anastomoses on branches of the one system when conduit is limited, provided the sequential graft does not compromise the site of the arteriotomy.
Excessive length between 2 distal anastomoses may result in kinking of the intervening segment and occlusion of the distal limb of the graft (Fig. 4).
The correct length of the intervening segment can be judged by slight traction on the epicardium between the 2 recipient arteries to reproduce the normal left ventricular size. Sequential anastomoses performed with the intervening graft too short, particularly when combined with an inadequate length of the proximal graft, may lead to angulation at the site ofthe proximal anastomosis (Fig. 5). The correct length of the graft is important to avoid this complication (Fig. 6).
A sequential Y graft may be required when conduit is scarce. Y grafting may be used preferentially when

Asia Pacific J Thorac Cardiovasc Surg 1995;4(2) Puruhito, Kusbianto, Raman, Buxton, et al Pitfalls in CABG Surgery
Fig. 5. Inadequate length of graft between sequential anastomoses and short segment of proximal graft, resulting in angulation.
Fig. 6. Correct lie of a sequential anastomosis.
Fig. 7. Excessive length may cause kinking.
Fig. 8. Correct lie of aortocoronary bypass grafts.
there is a reversed bifurcation in the saphenous vein, which divides proximally into 2 branches. Excessive length may cause kinking (Fig. 7).
The desired length of graft is best obtained by performing the proximal graft-to-graft anastomosis with a partial occlusion clamp on the aorta with the heart beating. However, most surgeons prefer to perform anastomoses during aortic cross clamping, in which case the ventricle and pulmonary arteries should be distended and adjustment made for left ventricular filling, which will occur after release of the aortic clamp.
The Proximal Anastomosis
When performing the proximal anastomosis between the aorta and the graft, a number of anatomic judgements need to be made correctly for the anastomosis to lie well and for the graft to function satisfactorily. This is achieved when the graft is the appropriate length, the position on the aorta is well chosen, and the anastomosis is orientated correctly (Fig. 8).
Excessive tension on the anastomosis between the aorta and the graft should be avoided because of the risk of rupture. To minimise tension on the aortic anastomosis, the diameter of the graft should be greater than that of the aortotomy. This is achieved by making the aortotomy small and increasing the diameter of the graft by cutting it obliquely.
Position on the aorta If the aortic anastomosis is placed on the far side of
the aorta and the graft is marginally short, compression of the graft may occur when the aorta is distended. For example, this is likely to occur if a left-sided graft is placed too far to the right on the aorta (Fig. 9A). The problem should be corrected by relocating the aortic anastomosis towards the left (Fig. 9B).
Positioning of the right coronary anastomosis low on
62
Asia Pacific .J Thorac Cardiovasc Surg 1995;4(2) Puruhito, Kusbianto, Raman, Buxton, et al Pitfalls in CABG Surgery
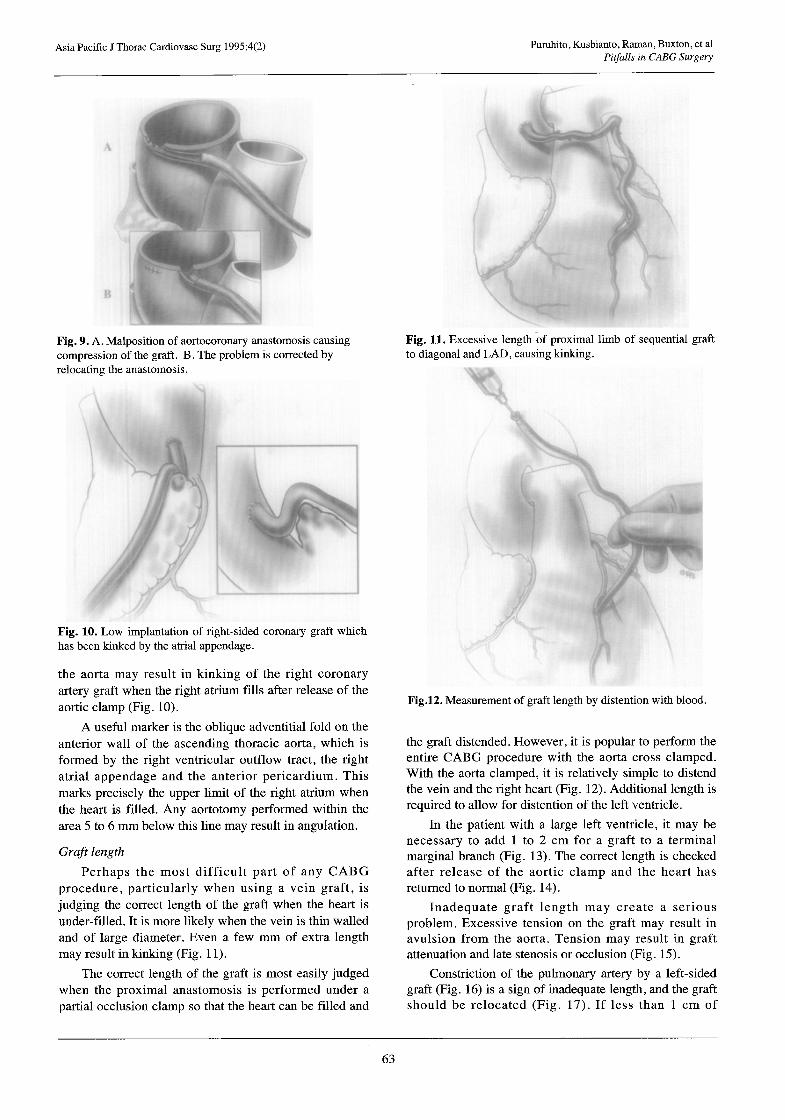
Fig. 9. A. Malposition of aortocoronary anastomosis causing compression of the graft. B. The problem is corrected by relocating the anastomosis .
Fig. 10. Low implantation of right-sided coronary graft which has been kinked by the atria1 appendage.
the aorta may result in kinking of the right coronary artery graft when the right atrium fills after release of the aortic clamp (Fig. 10).
A useful marker is the oblique adventitial fold on the anterior wall of the ascending thoracic aorta, which is formed by the right ventricular outflow tract, the right atria1 appendage and the anterior pericardium. This marks precisely the upper limit of the right atrium when the heart is filled. Any aortotomy performed within the area 5 to 6 mm below this line may result in angulation.
Graft length
Perhaps the most difficult part of any CABG procedure, particularly when using a vein graft, is judging the correct length of the graft when the heart is under-filled. It is more likely when the vein is thin walled and of large diameter. Even a few mm of extra length may result in kinking (Fig. 11).
The correct length of the graft is most easily judged when the proximal anastomosis is performed under a partial occlusion clamp so that the heart can be filled and
Fig. 11. Excessive length of proximal limb of sequential to diagonal and LAD, causing kinking.
g’ raft
Fig.12. Measurement of graft length by distention with blood.
the graft distended. However, it is popular to perform the entire CABG procedure with the aorta cross clamped. With the aorta clamped, it is relatively simple to distend the vein and the right heart (Fig. 12). Additional length is required to allow for distention of the left ventricle.
In the patient with a large left ventricle, it may be necessary to add 1 to 2 cm for a graft to a terminal marginal branch (Fig. 13). The correct length is checked after release of the aortic clamp and the heart has returned to normal (Fig. 14).
Inadequate graft length may create a serious problem. Excessive tension on the graft may result in avulsion from the aorta. Tension may result in graft attenuation and late stenosis or occlusion (Fig. 15),
Constriction of the pulmonary artery by a left-sided graft (Fig. 16) is a sign of inadequate length, and the graft should be relocated (Fig. 17). If less than 1 cm of
63

Asia Pacific .I Thorac Cardiovasc Surg 1995;4(2)
Fig.
Puruhito, Kusbianto, Raman, Buxton, et al Pitfalls in CABG Surgery
showing slight excess in length.
Fig. 14. The correct length is checked after release of the aortic clamp.
Fig. 17. Relocation of anastomosis to provide an additional 1 cm in graft length.
Fig. 15. Inadequate length of proximal graft showing attenuation of the graft.
Fig. 18. Anastomosis of additional length of graft, and re-anastomosis to the aorta.
64

Asia Pacific .I Thorac Cardiovasc Surg 1995;4(2) Puruhito, Kusbianto, Raman, Buxton, et al Pitfalls in CABG Surgery
Fig. 19. Attachment of graft to the pulmonary artery and to the pericardium using a sling technique.
Fig. 20. Rotation of graft and correction by re-anastomosis to the aorta.
additional length is required, the graft can be relocated on the aorta. If a graft is very short, there is usually no option but to add an additional length of conduit (Fig. 18).
Normally a little extra graft length is desirable. Vein grafts in particular tend to contract by about 10% and should be left without tension. If the graft is slightly longer than required, extra length can be accommodated by placing the graft in a gentle arc. This may require tacking the graft to maintain the position. An alternative
Fig. 21. Correction of rotation using a partial exclusion clamp.
Fig. 22. Correction of a large aortotomy by plication of the aorta.
technique is to tether the graft indirectly by means of a Sergicel Sling (Fig. 19).
Graft rotation
Rotation of a graft creates special problems. Whilst in arterial grafts a small rotation is well tolerated, rotation of 360” is usually unacceptable, and the graft will need to be refashioned. This is done by detaching the graft from the aorta, correcting the rotation and resuturing it to the same site (Fig. 20). An alternative method is to divide
65

Asia Pacific J Thorac Cardiovasc Surg 1995;4(2) Puruhito, Kusbianto, Raman, Buxton, et al Pitfalls in CABG Surgery
Fig. 23. Aortic dissection and repair.
and re-anastomose the graft. This is performed readily under the cross clamp.
If graft rotation is found at the end of the procedure after cessation of bypass, another method is to use a side biting clamp to include the rotated segment of graft and then divide and re-anastomose the graft (Fig. 21). Excessive pressure by the clamp on the graft is undesirable as it may cause late stenosis. In general, it is safer to use a non-clamp technique. The aortotomy
An oversized aortotomy may cause excessive tension on an aortocoronary anastomosis and rupture of the graft. This is a particular problem when using arterial grafts with a small diameter. It is important that the
circumference of the end of the graft is larger than that of the aortotomy.
Distention of the aorta after release of the clamp may put tension on the graft. If the aortotomy is too large, plication of one end of the anastomosis will correct the problem (Fig. 22).
Aortic dissection Aortic dissection can occur as the result of an
inadequate proximal anastomosis between the aorta and the grafts (Fig. 23). This is a particular problem if a thick layer of atheroma is in the aorta, making it difficult to include the inner layer in the suture.
The dissection is also more prone to occur in patients with medial degeneration and an abnormally soft aortic wall. Dissection may be the result of vigorous clamping of the aortic wall, particularly when using a partial occlusion clamp, or from injury from aortic cannulation or the introduction of cardioplegia. Deep sutures incorporating all layers of the arterial wall during the construction of a proximal anastomosis between the aorta and the graft will normally prevent this complication.
In the rare event of a confined aortic dissection, repair can be achieved by the use of the glycerol resorcinol formaldehyde (GRF or French glue). The aorta is re-clamped, the anastomosis taken down and the dissection glued. While the glue is polymerising, the aorta is distended with a gauze swab or Foley catheter placed through a separate aortotomy. Anastomosis is performed at the same site after repair or at a different site if this seems desirable.
If there is an extensive aortic dissection, there is usually no alternative but to replace the ascending thoracic aorta, usually after repositioning the aortic cannula in the groin.
Acknowledgment
The authors would like to thank medical artist Dr Levent Efe for his illustrations.
Journal Referees For 1995 The Editors wish to thank the referees who greatly assisted with the selection of papers for the Journal in 1995.
J. Angus H. Barner A. Bobik T. Cartmill P. Clarke J. Fuller T. Gardner Guo-Wei He R. Jeremy
T. Karl A. Keogh S. Lubicz D . McGiffin C. Munsch P. Myles M. Newman M. Rabinov D. Ross
R. Salamonsen G. Shardey P. Skillington G. Stirling J. Tatoulis A. Tonkin J. Wisheart
66
Copyright © 2022 FDOKUMEN




















