Platelet protection by low-dose aprotinin in cardiopulmonary bypass: Electron microscopic study
6
Platelet Protection by Low-Dose Aprotinin in Cardiopulmonary Bypass: Electron Microscopic Study Jacob Lavee, MD, Zvi Raviv, MD, Aram Smolinsky, MD, Naphtali Savion, PhD, David Varon, MD, Daniel A. Goor, MD, and Rephael Mohr, MD Department of Cardiac Surgery, The Maurice and Gabriela Goldschleger Eye Institute, and The National Hemophilia Center, The Chaim Sheba Medical Center, and The Sackler Faculty of Medicine, Tel Aviv University, Tel Hashomer, Israel. To evaluate the effect of low-dose aprotinin during cardiopulmonary bypass on platelet function and clinical hemostasis, 30 patients undergoing various cardiopul- monary bypass procedures employing bubble oxygen- ators were randomized to receive either low-dose aproti- nin (2 X lo6 KIU in the cardiopulmonary bypass priming solution, 15 patients [group A]) or placebo (15 patients [group B]). Blood samples were collected before and after cardiopulmonary bypass to assess platelet count and aggregation on extracellular matrix, which was studied by a scanning electron microscope. On a scale of 1 to 4 preoperative mean platelet aggregation grades were sim- ilar in both groups (3.8 f 0.5 and 3.5 f 0.5 for groups A and B, respectively). Postoperatively, platelet aggrega- tion on extracellular matrix decreased slightly in group A ne of the major causes of bleeding after cardiac 0 operations using cardiopulmonary bypass (CPB) is platelet dysfunction [I, 21. This problem could be over- come by transfusing the patients with fresh whole blood postoperatively [3, 41. However, in recent years, the use of the protease inhibitor aprotinin during CPB has emerged as a promising prophylactic measure in reducing postoperative bleeding and blood transfusion require- ments [5-151. This clinical effect has been shown [7, 151to be mediated by preservation of the platelet function. Most studies reporting the use of aprotinin have used the high-dose regimen, whereby the patient would re- ceive a total of 6 to 7 X lo6 KIU aprotinin, starting with a loading dose before sternotomy and continuing during operation. Recently, several studies [7, 16, 171 have re- ported using the low-dose regimen, whereby only 2 x lo6 KIU aprotinin is added to the priming volume of the oxygenator, with good clinical results. The aim of the present study was to evaluate the clinical effect of using aprotinin in the low-dose regimen employ- ing bubble oxygenators, and to correlate this effect to platelet function. We evaluated platelet function by using the extracellular matrix (ECM) that simulates the in vivo adhesion and aggregation of platelets on the subendothe- Accepted for publication April 27, 1992 Address reprint requests to Dr Goor, MD, Department of Cardiac Surgery, The Chaim Sheba Medical Center, Tel Hashomer 52621, Israel. (2.8 +. 1.3; p < 0.01) and significantly in group B (1.3 f 0.5; p < 0.001). Eleven of the 15 patients in group A remained in aggregation grade 3 or 4 compared with none of the group B patients. Platelet count was similar in both groups preoperatively and postoperatively. Total 24-hour postoperative bleeding and blood requirement were lower in the aprotinin group (487 f 121 mL and 2.3 f 1.0 units) than in the placebo group (752 f 404 mL and 6.8 f 5.1 units; p < 0.01). These results show that the use of low-dose aprotinin during cardiopulmonary bypass provides improved postoperative hemostasis, which might be related to the protection of the platelet aggre- gating capacity. (Ann Thorac Surg 1993;55:114-9) lium [MI. The extracellular matrix is produced by cultured bovine corneal endothelial cells and closely resembles the human vascular subendothelial basal lamina in origin and chemical composition [MI. The ECM has served as an in vitro model in the study of platelet-subendothelial inter- action [4, 18-21]. The incubation of human platelets on ECM induces platelet adhesion, aggregation, thrombox- ane A, formation, and a release reaction [18-211. In the present study, platelet aggregation on ECM was studied with the scanning electron microscope. Patients and Methods Thirty patients undergoing various CPB procedures (Ta- ble 1) were randomized to receive either low-dose aproti- nin (study group [group A], 15 patients) or placebo (control group [group B], 15 patients). The study group received 2 x lo6 KIU aprotinin (Trasylol; Bayer, Le- verkusen, Germany) added to the priming volume of the oxygenator. No additional aprotinin doses were given to the patients. Each patient in the control group (group B) received equivalent volumes of placebo solution (saline solution 0.9%) added to the priming volume of the oxy- genator. The mean age of the patients was 61 & 9 years (range, 40 to 78 years), with no difference between the two groups (see Table 1). No patient had been receiving dipyridamole or aspirin-containing drugs during the 4 weeks preceding 0 1993 by The Society of Thoracic Surgeons 0003-4975/93/$6.00
-
Upload
independent -
Category
Documents
-
view
2 -
download
0
Transcript of Platelet protection by low-dose aprotinin in cardiopulmonary bypass: Electron microscopic study

Platelet Protection by Low-Dose Aprotinin in Cardiopulmonary Bypass: Electron Microscopic Study Jacob Lavee, MD, Zvi Raviv, MD, Aram Smolinsky, MD, Naphtali Savion, PhD, David Varon, MD, Daniel A. Goor, MD, and Rephael Mohr, MD Department of Cardiac Surgery, The Maurice and Gabriela Goldschleger Eye Institute, and The National Hemophilia Center, The Chaim Sheba Medical Center, and The Sackler Faculty of Medicine, Tel Aviv University, Tel Hashomer, Israel.
To evaluate the effect of low-dose aprotinin during cardiopulmonary bypass on platelet function and clinical hemostasis, 30 patients undergoing various cardiopul- monary bypass procedures employing bubble oxygen- ators were randomized to receive either low-dose aproti- nin (2 X lo6 KIU in the cardiopulmonary bypass priming solution, 15 patients [group A]) or placebo (15 patients [group B]). Blood samples were collected before and after cardiopulmonary bypass to assess platelet count and aggregation on extracellular matrix, which was studied by a scanning electron microscope. On a scale of 1 to 4 preoperative mean platelet aggregation grades were sim- ilar in both groups (3.8 f 0.5 and 3.5 f 0.5 for groups A and B, respectively). Postoperatively, platelet aggrega- tion on extracellular matrix decreased slightly in group A
ne of the major causes of bleeding after cardiac 0 operations using cardiopulmonary bypass (CPB) is platelet dysfunction [I, 21. This problem could be over- come by transfusing the patients with fresh whole blood postoperatively [3, 41. However, in recent years, the use of the protease inhibitor aprotinin during CPB has emerged as a promising prophylactic measure in reducing postoperative bleeding and blood transfusion require- ments [5-151. This clinical effect has been shown [7, 151 to be mediated by preservation of the platelet function.
Most studies reporting the use of aprotinin have used the high-dose regimen, whereby the patient would re- ceive a total of 6 to 7 X lo6 KIU aprotinin, starting with a loading dose before sternotomy and continuing during operation. Recently, several studies [7, 16, 171 have re- ported using the low-dose regimen, whereby only 2 x lo6 KIU aprotinin is added to the priming volume of the oxygenator, with good clinical results.
The aim of the present study was to evaluate the clinical effect of using aprotinin in the low-dose regimen employ- ing bubble oxygenators, and to correlate this effect to platelet function. We evaluated platelet function by using the extracellular matrix (ECM) that simulates the in vivo adhesion and aggregation of platelets on the subendothe-
Accepted for publication April 27, 1992
Address reprint requests to Dr Goor, MD, Department of Cardiac Surgery, The Chaim Sheba Medical Center, Tel Hashomer 52621, Israel.
(2.8 +. 1.3; p < 0.01) and significantly in group B (1.3 f 0.5; p < 0.001). Eleven of the 15 patients in group A remained in aggregation grade 3 or 4 compared with none of the group B patients. Platelet count was similar in both groups preoperatively and postoperatively. Total 24-hour postoperative bleeding and blood requirement were lower in the aprotinin group (487 f 121 mL and 2.3 f 1.0 units) than in the placebo group (752 f 404 mL and 6.8 f 5.1 units; p < 0.01). These results show that the use of low-dose aprotinin during cardiopulmonary bypass provides improved postoperative hemostasis, which might be related to the protection of the platelet aggre- gating capacity.
(Ann Thorac Surg 1993;55:114-9)
lium [MI. The extracellular matrix is produced by cultured bovine corneal endothelial cells and closely resembles the human vascular subendothelial basal lamina in origin and chemical composition [MI. The ECM has served as an in vitro model in the study of platelet-subendothelial inter- action [4, 18-21]. The incubation of human platelets on ECM induces platelet adhesion, aggregation, thrombox- ane A, formation, and a release reaction [18-211. In the present study, platelet aggregation on ECM was studied with the scanning electron microscope.
Patients and Methods Thirty patients undergoing various CPB procedures (Ta- ble 1) were randomized to receive either low-dose aproti- nin (study group [group A], 15 patients) or placebo (control group [group B], 15 patients). The study group received 2 x lo6 KIU aprotinin (Trasylol; Bayer, Le- verkusen, Germany) added to the priming volume of the oxygenator. No additional aprotinin doses were given to the patients. Each patient in the control group (group B) received equivalent volumes of placebo solution (saline solution 0.9%) added to the priming volume of the oxy- genator.
The mean age of the patients was 61 & 9 years (range, 40 to 78 years), with no difference between the two groups (see Table 1). No patient had been receiving dipyridamole or aspirin-containing drugs during the 4 weeks preceding
0 1993 by The Society of Thoracic Surgeons 0003-4975/93/$6.00

Ann Thorac Surg 1993;55:114-9
Table I. Clinical mid Operatizie Data
Group A: Group B: Aprotinin Placebo
Variable (n = 15) (n = 15)
Age (Y) Sex (M/F) Bypass time (min) Aortic cross-clamp time (min) Lowest body temperature (“C) Procedure
CABG Redo CABG Valve replacement CABG + valve replacement
CABG = coronary artery bypass grafting.
62 2 11 1312
145 & 42 52 t 35 27 t 4.8
9 3 1 2
60 2 9 11/4
130 2 48 40 2 24 27 -t 3.7
12 2 1
. . .
the operation. For all patients a Sarns pump (Sarns Inc, Ann Arbor, MI) and bubble oxygenator (Bentley Labora- tories, Inc, Irvine, CA) were used. The oxygenators were primed with 1,500 mL of Hartmann’s solution and 500 mL of dextrose 5% solution.
The two groups were similar regarding bypass time, aortic cross-clamping time, and lowest body temperature (see Table 1). All patients were rewarmed to 35°C before discontinuation of CPB. Reversal of the heparin effect by protamine was monitored by the activated clotting time.
LAVEE ET AL 115 LOW-DOSE APROTlNlN IN CPB
All pump blood was returned to the patient through the aortic cannula or intravenously by infusion bags without hemoconcentration. None of the patients had to be re- turned to the operating room because of excessive medi- astinal bleeding.
Blood samples from each patient, obtained through a flushed arterial catheter, were collected before and at termination of CPB to assess platelet count and aggrega- tion. Platelet count was measured with a Coulter- Counter-S-Plus I1 (Luton, England).
Platelet aggregation was evaluated by the ECM model, using a scanning electron microscope [4, 221.
Preparation of Dishes Coated With Extracellular Matrix Corneal endothelial cells were grown on 24-well-type culture plates (Nunc CmbH, Roskilde, Denmark) with 5% dextran T-40 (Pharmacia, Fine Chemicals, Sweden) added to the growth medium [18, 20, 211. Cultures were washed once with phosphate-buffered saline (PBS) and exposed to 0.5% Triton-X 100 solution in PBS (volume per volume) followed by exposure to ammonium hydroxide solution, 0.1 mol/L, and washing in PBS. Extracellular matrix- coated dishes containing PBS were stored before use at 4°C for periods up to 3 months.
Platelet Reactivity With Extracellular Matrix Whole blood, 0.5 mL, in a citrate buffer from each sample was added to the tissue culture well coated with ECM
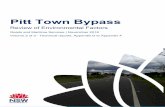
Fig 1. bcanning electron rrricrographs of the four aggregation grades on extracellular matrix: (a) grade 1 ; fb ) grade 2; fc) grade 3; ( d ) grade 4 . S w text for details. ( ~ 8 , 0 0 0 . )

116 LAVEEETAL LOW-DOSE APROTININ IN CPB
Ann Thorac Surg 1993;55:11&9
PLT Agg Grade 4 r
p<O.OOl I
Preop Post CPB
Aprotinin 0 Placebo
Fig 2 . Mean platelet aggregation (PLT Agg) grades of the two groups preoperatively and after cardiopulmona y bypass (CPB).
(16-mm diameter) and shaken (Orbit Shaker, Lab-Line Instruments, Melrose Park, IL; 100 rpm) for 30 minutes at room temperature. At the end of the incubation period, all the blood from the culture dish was collected and the dish was gently flushed several times with PBS.
Preparation for Study With Scanning Electron Microscope The ECM-coated dishes, now containing platelet aggre- gates, were fixed by 2.5% phosphate-buffered glutaralde- hyde (pH 7.2), then washed in the same buffer and postfixed by osmium tetroxide 2%. The third fixation was by a solution of 2% tannic acid-guanidine hydrochloride. The triple-fixed samples were dehydrated in graded alco- hol solutions, and thereafter the alcohol was exchanged to Freon 112 by graded Freon solutions (Du Pont Company, Wilmington, DE). The samples were air-dried, gold- coated, and examined by a Jeol 840 scanning electron microscope (Jeol USA Inc, Peabody, MA).
Grading Platelet Aggregates on Extracellular Matrix As a method of quantitating the aggregation of platelets on ECM as seen by the scanning electron microscope, four distinct aggregation grades were defined according to the
Fig 3 . Changes in individual platelet aggregation (PLT Agg) grades in the two groups from before operation to after cardiopulmona y bypass (CPBI. Numbers indicate number of patients.
Apro tinin Grade
various platelet morphologic types previously described [23] (Fig 1).
In grade 1 (see Fig la), the platelets are discoid with lentiform appearance, have a smooth surface, and lack any pseudopodia. In this grade the platelets do not adhere to each other, and each platelet can be seen individually.
In grade 2 (see Fig lb), the platelets display the first signs of activation, and they appear with slender dentrite- like pseudopodia, still separated from each other.
In grade 3 (see Fig lc), the aggregation process is more advanced: The platelet body spreads, showing multiple dentritic pseudopodia, and the platelets start to cluster. In this immature aggregate, each platelet can still be identi- fied separately.
Grade 4 (see Fig Id) consists of a mature aggregate in which large clumps of platelets are seen and in which individual platelets are difficult to define.
In each sample, 40 scanning electron microscopic fields containing platelets were examined at a magnification of 8,000, each given an individual grade. The final aggrega- tion grade of each sample was derived by calculating the arithmetic mean of the individual grades. Although ag- gregates of different grades could be found in any given sample, a dominant grade for each sample could always be identified. To avoid any element of subjectivity in the grading process, the observers assigned grades ”blindly,” that is, they were not aware of the group to which each sample belonged while grading it.
Blood Transfusion Policy The policy of blood transfusion in the intensive care unit differed in the immediate and late postoperative periods. Most blood transfusions were given in the first 8 postop- erative hours. The indications for blood transfusion were hemodynamic parameters, such as low systemic and left atrial pressures, and constricted periphery. The amount transfused depended strongly on the amount of blood lost through the chest tubes. Once the patient’s condition had stabilized completely, the indication for further blood transfusion was a hemoglobin level less than 10 g/lOO mL. Platelet concentrate transfusions were administered only to patients with active bleeding if platelet count was less than 100 x 109/L.
Blood loss from the chest tubes, the number of blood
Preop Post CPB
Placebo PLT Agg Grade
I Preop Post CPB

Ann Thorac Surg 1993;55: 114-9
LAVEE ET AL 117 LOW-DOSE APROTININ IN CPB
Fig 4. Scanning clectron micrographs of a patient from the aprotinin group: (a) preoperative (grade 4); (b) after cardiopulmonary bypass (grade 4). (X8,OOO.)
units required, and the total number of blood products transfused (red blood cells, plasma, and platelet units) in the initial 24 hours after the patient arrived a t the inten- sive care unit were recorded for evaluation of clinical hemostasis.
Statistical Analysis Results were expressed as mean k standard deviation. Paired and nonpaired t tests were used for parametric variables, and Fisher‘s exact test and the Mann-Whitney test for nonparametric variables.
Results Preoperative platelet count in group A (aprotinin group; 172 ? 44 x lO’/L) did not differ significantly from that in group B (152 * 50 x lO’/L). Similarly, both groups showed significantly lower platelet count after CPB (97 ?
23 and 88 ? 30 x 1O’/L for groups A and B, respectively; p < 0.001), with no significant difference between the two groups.
The mean grade of platelet aggregation on ECM before CPB was similar in both groups (3.8 * 0.5 and 3.5 2 0.5 for groups A and B, respectively; p = not significant) (Fig 2). Postoperatively, mean platelet aggregation grade on
ECM was slightly decreased in group A (2.8 k 1.3; p < 0.01) and significantly decreased in group B (1.2 2 0.5; p < 0.001) (see Fig 2). Eleven of the 15 patients in group A remained in grades 3 or 4, and only 4 could not form aggregates on ECM (grades 1 or 2) (Fig 3). Conversely, all patients in the control group (group 8) showed significant decrease of their postoperative aggregation grades to grades 1 or 2, and none showed normal aggregation (see Fig 3). Scanning electron micrographs of patients from each group are shown in Figures 4 and 5.
Total 24-hour blood loss in group A was significantly lower than in group B (Table 2). Patients in the aprotinin group received fewer homologous red blood cell units. Only 1 patient in this group received platelet transfusion, and this accounted for the extremely low exposure to homologous blood products (see Table 2).
Comment The protease inhibitor aprotinin has been shown in re- cently published studies to be a promising prophylactic agent in managing CPB-related bleeding [5-141. We [15] and others [5-141 have shown that when given in a high dose, namely, before and during the entire procedure, aprotinin has the capacity to reduce postoperative blood
Fig 5 . Scanning electron micrographs of a patient from thc placebo group: (a) preoperatizie (grade 4); (b) after cardioptrlmonary bypass (grade I). fx8,OOO.)

118 LAVEE ET AL LOW-DOSE APROTININ IN CPB
Ann Thorac Surg 1993;55:114-9
Table 2 . Postoperative Bleeding and Blood Requirement
Variable (Aprotinin) (Placebo) p Value Group A Group B
24-hour bleeding (mL) 487 f 121 752 f 404 0.05 RBC (U) 2.1 2 1.1 3.6 2 1.8 0.01 Total blood products (U) 2.3 f 1.0 6.8 f 5.1 0.01
RBC = red blood cells; platelets.
Total blood products = RBC + plasma +
loss and blood transfusion requirement by preserving the platelets’ adhesive and aggregatory functions.
As the high-dose regimen was devised on theoretical grounds [14, 241, few attempts have been reported [7, 16, 171 using a low-dose regimen, namely, 2 X lo6 KIU aprotinin in the priming solution of the oxygenator. In our study we used the low-dose regimen and demonstrated clinical beneficial results in terms of reduced postopera- tive bleeding and blood transfusion similar to those ob- served by previous groups who reported the use of the low-dose regimen [7, 16, 171.
Moreover, using the ECM model we have shown that the improved clinical hemostasis observed with the low- dose aprotinin regimen may be attributed to the partially preserved platelet aggregatory capacity. Seven of the 15 patients who received low-dose aprotinin maintained normal platelet aggregation (grade 4) after CPB, and another 4 displayed near-normal aggregation (grade 3), as opposed to none of the placebo group patients, who all displayed deranged aggregation (grades 1 and 2). Similar results, albeit somewhat better, were shown by us when the high-dose aprotinin regimen was tested [15]. In that group all patients maintained normal or near-normal platelet aggregation after CPB.
Previous reports [7, 251 have correlated the improved hemostasis provided by aprotinin to the preservation of the platelet glycoprotein Ib-dependent adhesive capacity. By using the ECM model as an in vitro model for the study of platelet subendothelium interaction [18-211, we have demonstrated an additional effect of CPB on plate- lets represented by the deranged aggregatory capacity foli-id in all patients in the placebo group, who showed some platelet adhesion to the ECM (grades 1 and 2), but no signs of aggregation. The lack of aggregation on ECM in the placebo group might be due to fibrinogen receptor defect, as Glanzman’s thrombasthenic platelets (which are deficient of glycoprotein IIb/IIIa) exhibit the same response to ECM [19]. These results concur with those of Rinder and colleagues [26, 271, who have shown selective decreases in platelet glycoprotein IIb/IIIa, in addition to Ib, as a result of CPB. The assumption that other agonists present in the ECM, such as collagen or fibronectin, might be responsible for the improved aggregation found in those patients who received aprotinin is negated by the fact that those agonists did not play any role in the placebo group.
It should be noted that the discrepancy in the mode of action of aprotinin between our observation and that of others [7,25] may be explained at least partially by the use
of bubble oxygenators in our study and membrane oxy- genators by the others. It is known that platelet aggrega- tion is better preserved by membrane than by bubble oxygenators [28].
As platelet aggregation on ECM requires both fibrino- gen [19] and von Willebrand’s factor [29] as ligands for the activated glycoprotein IIbAIIa, our model is not sensitive enough to differentiate which domain on the glycoprotein IIb/IIIa was protected by aprotinin. The preserved aggre- gatory capacity of platelets in the aprotinin group of our study suggests that at least part, if not all, of the glyco- protein IIb/IIIa was protected.
A possible explanation for the protective effect of apro- tinin on blood loss during CPB has recently been sug- gested [14, 301. According to this hypothesis, plasmin, generated during CPB, activates the platelets and causes changes in the distribution of glycoproteins IIbLIIa and Ib on the platelet’s membrane [31]. This effect is further enhanced by the lower temperatures used for the CPB procedure [32]. Activated platelets might become nonre- active or cleared from the blood by interaction with components of the CPB system, and thus bleeding ten- dency is increased. Aprotinin, by its known antifibrin- olytic effect [33, 341, may protect postoperative platelet aggregation by inhibiting the high deleterious plasmin level [33]. Our study has not addressed the antifibrinolytic effects of aprotinin but has shown that the final pathway, namely, platelet aggregatory capacity, is preserved by the drug.
We conclude that the use of low-dose aprotinin during CPB, using bubble oxygenators, provides improved post- operative hemostasis by preserving the platelet aggrega- tory capacity. These beneficial effects of aprotinin have reconfirmed the utmost importance of platelets in postop- erative hemostasis.
We greatly appreciate the technical expertise and assistance of Jacob Langsam, MSc, the Electron Microscopy Unit, Life Sciences Department, Bar llan University, and of Mr Henry Fridman, Chief Perfusionist at the Sheba Medical Center, Tel Hashomer, Israel.
References 1. Mohr R, Golan M, Martinowitz U, Rosner E, Goor DA. Effect
of cardiac operation on platelets. J Thorac Cardiovasc Surg 1986;9243441.
2. Woodman RC, Harker LA. Bleeding complications associ- ated with cardiopulmonary bypass. Blood 1990;76:1680-97.
3. Mohr R, Martinowitz U, Lavee J, Amroch D, Ramot B, Goor DA. The hemostatic effect of transfusing fresh whole blood versus platelet concentrates after cardiac operations. J Thorac Cardiovasc Surg 1988;96530-4.
4. Lavee J, Martinowitz U, Mohr R, et al. The effect of transfu- sion of fresh whole blood versus platelet concentrates after cardiac operations. A scanning electron microscope study of platelet aggregation on extracellular matrix. J Thorac Cardio- vasc Surg 1989;97204-12.
5. Van Oeveren W, Jansen NJG, Bidstrup BP, et al. Effects of aprotinin on hemostatic mechanisms during cardiopulmo- nary bypass. Ann Thorac Surg 1987;44:64&5.
6 . Royston D, Bidstrup BP, Taylor KM, Sapsford RN. Effect of aprotinin on need for blood transfusion after repeat open- heart surgery. Lancet 1987;2:1289-91.

Ann Thorac Surg 1993;55:11&9
LAVEE ET AL 119 LOW-DOSE APROTININ IN CPB
7.
8.
9.
10.
11.
12.
13.
14.
15.
16.
17.
18.
19.
Van Oeveren W, Harder MP, Roozendaal KJ, Eijsman L, Wildevuur CRH. Aprotinin protects platelets against the initial effect of cardiopulmonary bypass. J Thorac Cardiovasc Surg 1990;99:788-97. Dietrich W, Spannagl M, Jochum M, et al. Influence of high-dose aprotinin treatment on blood loss and coagulation patterns in patients undergoing myocardial revasculariza- tion. Anesthesiology 1990;73: 11 19-26. Alajmo F, Calamai G, Pemia AM, et al. High-dose aprotinin: hemostatic effects in open heart operations. Ann Thorac Surg 1989;48:536-9. Bidstrup BP, Royston D, Sapsford RN, Taylor KM. Reduction in blood loss and blood use after cardiopulmonary bypass with high dose aprotinin (Trasylol). J Thorac Cardiovasc Surg 1989;97:364-72. Dietrich W, Barankay A, Dilthey G, et al. Reduction of homologous blood requirement in cardiac surgery by intra- operative aprotinin application-clinical experience in 152 cardiac surgical patients. Thorac Cardiovasc Surg 1989;37: 92-8. Graedrich G, Weber C, Bernard C, Hettwer A, Schlosser V. Reduction of blood transfusion requirement in open heart surgery by administration of high doses of aprotinin- preliminary results. Thorac Cardiovasc Surg 1989;3789-91. Harder MP, Eijsman L, Roozendael KJ, van Oeveren W, Wildevuur CRH. Aprotinin reduces intraoperative and post- operative blood loss in membrane oxygenator cardiopulmo- nary bypass. Ann Thorac Surg 1991;51:936-41. Royston D. High-dose aprotinin therapy: a review of the first five years’ experience. J Cardiothorac Anesth 1992;16:76-100. Lavee J, Savion N, Smolinsky A, Goor DA, Mohr R. Platelet protection by aprotinin in cardiopulmonary bypass: electron microscopic study. Ann Thorac Surg 1992;53:477-81. Wildevuur CRH, Eijsman L, Roozendaal KJ, Harder MP, Chang M, van Oeveren W. Platelet preservation during cardiopulmonary bypass with aprotinin. Eur J Cardiothorac Surg 1989;3:533-8. Carrel T, Bauer E, Laske A, von Segesser L, Turina M. Low dose aprotinin for reduction of blood loss after cardiopulmo- nary bypass [Letter]. Lancet 1991;337673. Vlodavsky I, Eldor A, HyAm E, Atzom R, Fuks Z. Platelet interaction with the extracellular matrix produced by cul- tured endothelial cells: a model to study the thrombogenecity of isolated subendothelial basal lamina. Thromb Res 1982;28: 179-91. Eldor A, Vlodavsky I, Martinowicz U, Fuks Z, Coller BS. Platelet interaction with subendothelial extracellular matrix: platelet-fibrinogen interactions are essential for platelet ag- gregation but not for the matrix-induced release reaction. Blood 1985;65:1477-83.
20. Gospodarowicz D, Vlodavsky I, Savion N. The extracellular matrix and the control of proliferation of vascular endothelial and vascular smooth muscle cells. J Supramol Struc 1980;13:
21. Gospodarowicz D, Vlodavsky I, Savion N. The extracellular matrix. Endocr Rev 1980;1:201-7.
22. Golan M, Modan M, Lavee L, et al. Transfusion of fresh whole blood stored (4°C) for short period fails to improve platelet aggregation on extracellular matrix and clinical he- mostasis after cardiopulmonary bypass. J Thorac Cardiovasc Surg 1990;99:354-60.
23. Zilla P, Groscurth P, Rhyner K, von Felten A. Surface morphology of human platelets during in vitro aggregation. Scand J Haematol 1984;33:440-7.
24. Bidstrup BP. Discussion of [7]. J Thorac Cardiovasc Surg 1990;99:796-7.
25. Lu H, Soria C, Commin PL, et al. Hemostasis in patients undergoing extracorporeal circulation: the effect of aprotinin (Trasylol). Thromb Haemost 1991;166:633-7.
26. Rinder CS, Bohnert J, Rinder HM, Mitchell J, Ault K, Hillman R. Platelet activation and aggregation during cardiopulmo- nary bypass. Anesthesiology 1991;175:3&93.
27. Rinder CS, Mathew JP, Rinder HM, Bonan J, Ault KA, Smith BR. Modulation of platelet surface adhesion receptors during cardiopulmonary bypass. Anesthesiology 1991;75:563-70.
28. Edmunds LH Jr, Ellison N, Colman RW, et al. Platelet function during cardiac operation: comparison of membrane and bubble oxygenators. J Thorac Cardiovasc Surg 1982;83: 805-12.
29. OBrien JR. Shear-induced platelet aggregation. Lancet 1990;
30. Edmunds LH, Niewarowski S, Colman RW. Invited letter concerning aprotinin. J Thorac Cardiovasc Surg 1991;lOl: 11034.
31. Cramer EM, Lu H, Caen JP, Soria C, Berndt MC, Tanza D. Differential redistribution of platelet glycoproteins Ib and 1%-IIIa after plasmin stimulation. Blood 1991;77:69&9.
32. Lu H, Soria C, Cramer EM, et al. Temperature dependence of plasmin-induced activation or inhibition of human platelets. Blood 1991;77996-1005.
33. Blauhut B, Gross C, Necek S, Doran JE, Spath P, Hansen PL. Effects of high-dose aprotinin on blood loss, platelet func- tion, fibrinolysis, complement, and renal function after car- diopulmonary bypass. J Thorac Cardiovasc Surg 1991;lOl: 958-67.
34. Haven M, Teufelsbauer H, Knob1 P, et al. Effect of intraop- erative aprotinin administration on postoperative bleeding in patients undergoing cardiopulmonary bypass operation. J Thorac Cardiovasc Surg 1991;101:968-72.
339-72.
335~7113.