Antioxidant defence during cardiopulmonary bypass surgery
6
Antioxidant defence during cardiopulmonary bypass surgery Chris R. Luyten a , Frans J. van Overveld a , Lieve A. De Backer a , Anna M. Sadowska a, * , Inez E. Rodrigus b , Stefan G. De Hert c , Wilfried A. De Backer a a Department of Respiratory Medicine, University of Antwerp, Universiteitsplein 1, B-2610 Antwerpen-Wilrijk, Belgium b Department of Cardiac Surgery, University Hospital Antwerp, Antwerpen-Wilrijk, Belgium c Department of Anesthesiology, University Hospital Antwerp, Antwerpen-Wilrijk, Belgium Received 15 July 2004; received in revised form 3 December 2004; accepted 13 December 2004; Available online 13 January 2005 Abstract Objective: Cardiac surgery may lead to severe oxidative stress due to formation of oxidation products generated during ischemia and reperfusion. We investigated to which extent oxidative stress influences a number of endogenous antioxidants and markers of cellular activation. Methods: At six time points blood was withdrawn from patients undergoing coronary artery bypass grafting, using the on-pump procedure. Results: Both glutathione peroxidase and superoxide dismutase show a gradual and strong increase in activity during surgery (40 and 30%, respectively), returning to baseline values 24 h after surgery. The total antioxidant capacity has a maximum increase of 60%. Markers of cellular activation, such as eosinophil cationic protein and tryptase also increase during the procedure. Conclusion: Cardiac surgery results in systemic inflammation accompanied or caused by severe oxidative stress. The human body has a strong innate oxidative defence screen, which is probably not sufficient to fully compensate for the total amount of oxidative damage. q 2004 Elsevier B.V. All rights reserved. Keywords: Bypass surgery; Antioxidants; Glutathione peroxidase; Superoxide dismutase; Oxidative stress 1. Introduction Although open cardiac coronary artery by-pass grafting (CABG) surgery has become a routine procedure worldwide, patient morbidity and mortality due to adverse post- operative complications are still unacceptably high. The endothelial injury and/or cardiac, renal, hepatic or pulmon- ary dysfunction associated with CABG surgery have been linked to the inflammatory responses and systemic oxidative stress directly caused by this procedure but the underlying mechanisms have not been fully elucidated yet. It has been suggested that in addition to the damage caused directly in the myocardium, a significant proportion of the adverse outcomes may also be caused by the systemic effects of cardiopulmonary bypass (CPB) [1]. It has moreover been demonstrated that on-pump procedure gives rise to a more pronounced systemic inflammation and oxidative stress than the off-pump procedure [2]. The mechanisms explaining these observations may be related to several deleterious events occurring during CPB [3] which are either material-dependent (caused by exposure of blood to non- physiologic surfaces and conditions during the extracorpor- eal circulation, ECC) or material-independent (caused by surgical trauma, ischemia-reperfusion and changes in body temperature). One of the most damaging consequences of these events is the formation of reactive oxygen species (ROS) and radicals, which originate from various cellular and enzymatic sources such as myocardial cells, activated neutrophils [4] or endothelial xanthine oxidase. These are closely linked to inflammatory responses, including comp- lement activation, release of cytokines and leukocyte activation, along with expression of adhesion molecules [5]. Many studies have described the nature of these ROS and the time course of their formation during CPB [6]. The nature of these oxidative events leads to depletion of plasma antioxidants, increased lipid peroxidation and formation of other damaging metabolites [7–9]. In order to counter- balance this sequence of events and to diminish oxidative injury, several studies have investigated the use of anti- oxidant supplements during ECC [10,11]. Less is known about the consequences of CPB on the endogenous antioxidant capacity that is derived from the activity of antioxidant enzymes such as glutathione peroxidase (GPx) and super- oxide dismutase (SOD), responsible for the clearance of peroxides and superoxide, respectively. In order to investigate this question, our study focused on the time course of innate antioxidant activity (antioxidant enzymes and global antioxidant capacity in plasma) in patients undergoing cardiopulmonary bypass surgery. In particular, we were interested in analysing to which extent 1010-7940/$ - see front matter q 2004 Elsevier B.V. All rights reserved. doi:10.1016/j.ejcts.2004.12.013 European Journal of Cardio-thoracic Surgery 27 (2005) 611–616 www.elsevier.com/locate/ejcts * Corresponding author. Tel: C32 3 820 2591; fax: C32 3 820 2590. E-mail address: [email protected] (A.M. Sadowska).
-
Upload
independent -
Category
Documents
-
view
4 -
download
0
Transcript of Antioxidant defence during cardiopulmonary bypass surgery

Antioxidant defence during cardiopulmonary bypass surgery
Chris R. Luytena, Frans J. van Overvelda, Lieve A. De Backera, Anna M. Sadowskaa,*,Inez E. Rodrigusb, Stefan G. De Hertc, Wilfried A. De Backera
aDepartment of Respiratory Medicine, University of Antwerp, Universiteitsplein 1, B-2610 Antwerpen-Wilrijk, BelgiumbDepartment of Cardiac Surgery, University Hospital Antwerp, Antwerpen-Wilrijk, BelgiumcDepartment of Anesthesiology, University Hospital Antwerp, Antwerpen-Wilrijk, Belgium
Received 15 July 2004; received in revised form 3 December 2004; accepted 13 December 2004; Available online 13 January 2005
Abstract
Objective: Cardiac surgery may lead to severe oxidative stress due to formation of oxidation products generated during ischemia andreperfusion. We investigated to which extent oxidative stress influences a number of endogenous antioxidants and markers of cellularactivation. Methods: At six time points blood was withdrawn from patients undergoing coronary artery bypass grafting, using the on-pumpprocedure. Results: Both glutathione peroxidase and superoxide dismutase show a gradual and strong increase in activity during surgery (40 and30%, respectively), returning to baseline values 24 h after surgery. The total antioxidant capacity has a maximum increase of 60%. Markers ofcellular activation, such as eosinophil cationic protein and tryptase also increase during the procedure. Conclusion: Cardiac surgery results insystemic inflammation accompanied or caused by severe oxidative stress. The human body has a strong innate oxidative defence screen, whichis probably not sufficient to fully compensate for the total amount of oxidative damage.q 2004 Elsevier B.V. All rights reserved.
Keywords: Bypass surgery; Antioxidants; Glutathione peroxidase; Superoxide dismutase; Oxidative stress
1. Introduction
Although open cardiac coronary artery by-pass grafting(CABG) surgery has become a routine procedure worldwide,patient morbidity and mortality due to adverse post-operative complications are still unacceptably high. Theendothelial injury and/or cardiac, renal, hepatic or pulmon-ary dysfunction associated with CABG surgery have beenlinked to the inflammatory responses and systemic oxidativestress directly caused by this procedure but the underlyingmechanisms have not been fully elucidated yet.
It has been suggested that in addition to the damagecaused directly in the myocardium, a significant proportionof the adverse outcomes may also be caused by the systemiceffects of cardiopulmonary bypass (CPB) [1]. It has moreoverbeen demonstrated that on-pump procedure gives rise to amore pronounced systemic inflammation and oxidativestress than the off-pump procedure [2]. The mechanismsexplaining these observations may be related to severaldeleterious events occurring during CPB [3] which are eithermaterial-dependent (caused by exposure of blood to non-physiologic surfaces and conditions during the extracorpor-eal circulation, ECC) or material-independent (caused by
1010-7940/$ - see front matter q 2004 Elsevier B.V. All rights reserved.doi:10.1016/j.ejcts.2004.12.013
* Corresponding author. Tel: C32 3 820 2591; fax: C32 3 820 2590.E-mail address: [email protected] (A.M. Sadowska).
surgical trauma, ischemia-reperfusion and changes in bodytemperature). One of the most damaging consequences ofthese events is the formation of reactive oxygen species(ROS) and radicals, which originate from various cellular andenzymatic sources such as myocardial cells, activatedneutrophils [4] or endothelial xanthine oxidase. These areclosely linked to inflammatory responses, including comp-lement activation, release of cytokines and leukocyteactivation, along with expression of adhesion molecules[5]. Many studies have described the nature of these ROS andthe time course of their formation during CPB [6]. The natureof these oxidative events leads to depletion of plasmaantioxidants, increased lipid peroxidation and formation ofother damaging metabolites [7–9]. In order to counter-balance this sequence of events and to diminish oxidativeinjury, several studies have investigated the use of anti-oxidant supplements during ECC [10,11]. Less is known aboutthe consequences of CPB on the endogenous antioxidantcapacity that is derived from the activity of antioxidantenzymes such as glutathione peroxidase (GPx) and super-oxide dismutase (SOD), responsible for the clearance ofperoxides and superoxide, respectively.
In order to investigate this question, our study focused onthe time course of innate antioxidant activity (antioxidantenzymes and global antioxidant capacity in plasma) inpatients undergoing cardiopulmonary bypass surgery. Inparticular, we were interested in analysing to which extent
European Journal of Cardio-thoracic Surgery 27 (2005) 611–616
www.elsevier.com/locate/ejcts

C.R. Luyten et al. / European Journal of Cardio-thoracic Surgery 27 (2005) 611–616612
antioxidants were being generated or activated during CPB.In order to elucidate the relationship between the changes inantioxidant status and the activation of inflammatory cellsduring CPB, we also monitored markers of leukocyteactivation such as tryptase and eosinophil cationic protein.
2. Materials and methods
2.1. Study population
Ten patients (6 males, 4 females, mean age 68.4 yrsG7.7 SD) undergoing elective coronary artery bypass graftingwere included in this study. Perioperative data are shown inTable 1. This study was in accordance to the principlesoutlined in the Declaration of Helsinki. Patients wereinformed of the procedure and the ethical committee ofthe University Hospital of Antwerp approved the studyprotocol.
2.2. Cardiopulmonary bypass
Anaesthesia with endotracheal intubation and balancedadministration of premedication and transfusions wasuniform in all cases. The CPB equipment consisted of aBentley membrane oxygenator (Bentley Oxygenation systemCM50, Baxter, Ivina CA, USA). The pump-oxygenator systemwas primed with 1800 ml crystalloid solution (Plasma-Lyte A,Baxter) and 6% HetaStarch. Anticoagulation was achieved by300 U/kg heparin (Leo Pharma, Denmark). All patients werecooled to 28 8C. Surgery was performed using the inter-mittent cross-clamp technique. Fifteen minutes afterdecannulation, heparin was neutralised with protaminechloride (1:1 ratio; Roche, Belgium). Patients only receivedautologous transfusion with residual blood left in the pumpafter CPB.
2.3. Blood sampling
Blood samples were collected into sterile Lithium-heparintubes and SST-tubes with clotting activator (Vacutainer,Becton Dickinson) at several time points during and aftercardiac surgery: (a) 10 min after induction of anaesthesia(left radial artery), (b) 10 min after start of ECC (arterial sideof pump), (c) at the end of ECC (arterial side of pump), (d)10 min after protamine administration (left radial artery),(e) 4 h and (f) 24 h after surgery (left radial artery). Bloodsamples were processed within 10 min after sampling toavoid auto-oxidation of antioxidants. Hematocrit values
Table 1Patient characteristics, operative and postoperative data
Number of patients 10Male/female 6/4Age (yrs) 72 (56–77)BMI (kg/m2) 26.4G3.4Elective/urgent 10/0Graft/patient 4 (2–5)Cardiopulmonary bypass time (min) 119 (83–186)Cross-clamp time (min) 52 (35–126)Fluid balance (mL) 648G446
Data presented as meanGSD or median (minimum–maximum).
were measured in every blood sample. In order to takedilution with the priming solution of the CBP system intoaccount, the value of the first blood sample (pre-surgery)was set as a reference baseline value. All obtained data werethen corrected for haemodilution using the hematocritvalues to calculate the appropriate correction factor.
2.4. Antioxidant measurements
Trolox equivalent antioxidant capacity (TEAC) wasmeasured in plasma according to the method of Rice-Evansand Miller. TEAC is a measure that is indicative for the wholepool of antioxidants in plasma and thus for the totalantioxidant capacity of plasma. Trolox is a synthetic vitaminE analog with antioxidant activity, which is able to preventradical generation by H2O2 in a reaction mixture containingmetmyoglobine and 2, 2 0-azino-bis (3-ethylbenzthiazoline-6-sulfonic acid (ABTS). When antioxidant activity in the milieuis depleted, ABTS forms stable coloured radicals that can bemeasured by spectrophotometry (absorption at 734 nm).Plasma antioxidant capacity is compared with a calibrationcurve of trolox concentration and thus trolox equivalentantioxidant capacity can be calculated. Intra and inter-assayCV was 5 and 14%.
Glutathione peroxidase (GPx) in full blood was measuredwith a Ransel Glutathione Peroxidase kit (Randox Labora-tories Ltd), and is based on the method of Paglia andValentine: GPx catalyses the oxidation of glutathione (GSH)by cumene hydroperoxide. In the presence of glutathionereductase and the oxidized glutathione (GSSG) is immedi-ately converted to the reduced form with a concomitantoxidation of nicotinamide adenine dinucleotide phosphate,reduced form (NADPH) to NADPC. The decrease in absor-bance of NADPH can be measured at 340 nm. Intra- andinter-assay CV was 2 and 6%.
Superoxide dismutase (SOD) was measured with a RanSODsuperoxide dismutase kit (Randox Laboratories Ltd). Therole of SOD is to accelerate the dismutation of the toxicsuperoxide radical OK
2 to hydrogen peroxide and molecularoxygen. The Randox method uses xanthine and xanthineoxidase to generate superoxide radicals that react with 2-(4-iodophenyl)-3-(4-nitrophenol)-5-phenyltetrazolium (I.N.T.)to form a red formazan dye. The SOD activity is thencalculated from the degree of inhibition of this reactioncompared to a standard curve of SOD. Intra- and inter-assayCV was 6 and 15%.
Alpha-tocoferol and retinol in serum were measured byHigh Performance Liquid Chromatography (Dionex, HPLCwith a 100% methanol mobile phase) with detection at 292and 325 nm, respectively. Intra- and inter-assay CV was 5and 13%.
2.5. Markers of cellular activation
Eosinophil cationic protein (ECP) was measured in serumusing a fluoroenzymeimmunoassay provided by Pharmacia(Uppsala, Sweden). Anti-ECP, covalently coupled to Immu-noCAP, reacts with the ECP in the patient’s serum specimen.After washing, enzyme-labelled antibodies against ECP areadded to form a complex. After incubation, unboundenzyme-anti-ECP is washed away and the bound complex is

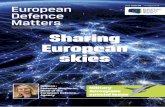
Fig. 1. Levels of glutathione peroxidase (GPx) in full blood before, during, andafter cardiopulmonary bypass surgery. *P!0.05 when compared to the valuebefore surgery.
Fig. 3. Concentrations of a-tocopherol (vitamin E) in serum before, during,and after cardiopulmonary bypass surgery. *P!0.05 when compared to thevalue before surgery.
C.R. Luyten et al. / European Journal of Cardio-thoracic Surgery 27 (2005) 611–616 613
then incubated with a developing agent. After stopping thereaction, the fluorescence is measured. The fluorescence isinversely correlated with the concentration of ECP in theserum sample. Measuring range is 2–200 mg/l. Within assayCV is 3.8%.
Tryptase is a serine protease released by mast cells uponactivation. It can be measured in serum applying animmunoassay from Pharmacia, according to the sameprinciple as described for ECP. Measuring range for undilutedsample is 1–200 mg/l. Within assay CV is 3%.
2.6. Statistical analysis
Data are shown as meanGSEM. Analysis of variance forrepeated measures was used to compare changes in time.Differences were considered significant at P value less than0.05.
The power of the primary end-points (GPX, SOD andTEAC) was O0.7.
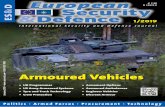
Fig. 2. Levels of superoxide dismutase (SOD) from red blood cells before,during, and after cardiopulmonary bypass surgery. *P!0.05 when comparedto the value before surgery.
3. Results
Enzyme activity of the antioxidants GPx and SOD in fullblood increased significantly in the initial stages ofsurgery. When looking at the changes within each individual(in-patient), GPx rose by an average of 20% at 10 min afterstarting the ECC compared to pre-surgery values, andreached a maximum average increase of 40% at the end ofcross-clamp circulation (Fig. 1). SOD reached a 30%maximum rise in activity at the end of surgery, after theadministration of protamine (Fig. 2).
Serum concentration of retinol and a-tocopherol variedrather widely between patients in all measurements. We sawthat both retinol (data not shown) and a-tocopherolremained constant during CBP (Fig. 3). It is only from 4 hafter surgery that serum concentration of these antioxidantsdecreased significantly.
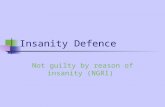
Total antioxidant capacity of plasma (TEAC) (Fig. 4)increased from 0.9 mM Trolox equivalents to 1.45 mM at10 min of ECC, corresponding to an increase of plasmaantioxidant capacity of 60%.
Fig. 4. The total antioxidant capacity (TEAC) of plasma before, during, andafter cardiopulmonary bypass surgery. *P!0.05 when compared to the valuebefore surgery.

Fig. 5. Levels of serum tryptase before, during, and after cardiopulmonarybypass surgery. *P!0.05 when compared to the value before surgery.
C.R. Luyten et al. / European Journal of Cardio-thoracic Surgery 27 (2005) 611–616614
Tryptase levels in serum increased markedly (by 60%,P!0.05) during ECC (Fig. 5), gradually returning to baselinevalues after surgery. As for ECP, serum concentration was upto 4 times higher at the end of ECC (P!0.01) (Fig. 6),decreasing again to baseline values towards the end andafter the procedure. An artefact in two blood samplescaused the seemingly high values at 24 h after surgery.
4. Discussion
The systemic increase in oxidative stress during CABG iswell-documented [5,7] but the various components of theoxidant-antioxidant balance and the contribution of thevarious mechanisms involved have not been fully evaluatedyet. This study aimed at describing the changes inendogenous antioxidant capacity in patients undergoingCABG under procedures which are known to enhanceproduction and release of oxidants. Firstly, the intermittentclamp technique used under the CPB is a direct cause ofischemia-reperfusion with, as a consequence, release ofsuperoxide by the xanthine-oxidase system [2]. In addition,extracorporeal circulation, by increasing contact of blood
Fig. 6. Concentrations of eosinophil cationic protein (ECP) in serum before,during, and after cardiopulmonary bypass surgery. *P!0.05, **P!0.01 whencompared to the value before surgery.
with foreign substances, will induce systemic inflammatoryresponses associated with complement activation, cytokinerelease and cellular activation of neutrophils [1]. These areall sources of ROS production [12] which will ultimately leadto depletion of plasma antioxidants [8]. In a previous studywe already described a decrease in plasma glutathioneduring CPB [9]. In the present study, we used TEAC as amarker for total antioxidant capacity in plasma. Unexpect-edly, we did not document a decrease of TEAC value, or—inother words—a depletion of plasma antioxidants, but analmost twofold increase. The nature of this increase is notknown. Two abundant plasma molecules with antioxidantactivity, namely albumin and uric acid are the maindeterminants of the TEAC value. Albumin concentration inplasma, however, did not increase significantly during CPB(data not shown) and could therefore, not have contributedto the increase of TEAC value. The contribution of uric acidherein could not be assessed, due to technical limitations.Another possible cause of increased TEAC value could havebeen haemolysis of red blood cells during or after sampling.Hemoglobin has been shown to interfere with the TEACmeasurements. Thus the impact of free hemoglobin and uricacid in plasma should be taken into account when measuringglobal antioxidant capacity in future studies.
The activity of the enzymatic antioxidants glutathioneperoxidase (GPx) and superoxide dismutase (SOD) increasedsignificantly during ECC. This could explain the time courseof depletion of GSH we observed previously, because GPxuses GSH as a cofactor [10]. Moreover, when comparing ourtime course of GPx activation and the time course of TBA-reactive peroxides as described by Davies [6], we see a closematch. This parallelism suggests that glutathione peroxidaseforms a first barrier against the reactive oxygen speciesbeing formed during the operation. Our findings confirm theresults obtained by Arduini et al. [13], who also found anincrease in GPx activity. Others studies, however, observeda decrease in GPx activity [14], or no change during CPB [15].Most of these studies, however, were performed on animalmodels, which may explain part of the discrepancy betweenour study and the ones just mentioned.
SOD, the enzyme responsible for converting superoxideanion into hydrogen peroxide, was also strongly activated, afairly acute response lasting from early CPB until afterprotamine administration. This can be explained by the factthat contact of blood with polymers of the CPB circuitreleases cytokines and activates neutrophils [12], indepen-dent of heparin coating. Activated neutrophils will via therespiratory burst generate superoxide anion which isdetoxified by SOD. These two findings illustrate that GPxand SOD form a strong first line of defence against reactiveoxygen species. Moreover, GPx and SOD are enzymaticantioxidants which are not consumed during their detox-ification activities. In contrast, antioxidants which act asfree radical scavengers are consumed during oxidativeprocesses and the time courses of depletion vary dependingon the nature of the antioxidant.
Retinol is not considered to be a very potent antioxidant,although its precursors of the carotenoid group are. Alpha-tocopherol on the other hand is well known for itsantioxidative capacity. However, its role is rather contro-versial, for some studies find supplementation of patients

C.R. Luyten et al. / European Journal of Cardio-thoracic Surgery 27 (2005) 611–616 615
with a-tocopherol prior to CPB to be beneficial [16], whileseveral big-scale studies such as the Heart OutcomesPrevention Evaluation (HOPE) study, clearly demonstratedthat vitamin E supplementation, independently of surgery,had no apparent effect on cardiovascular outcomes [11].Also, the role and consumption of a-tocopherol during CPBare debatable. Some studies state that a-tocopherol leveldecreases during and after CPB [17], while others find aslight or non-significant decrease in serum a-tocopherolconcentration [18]. Our results, after correction for haemo-dilution, are similar to the ones published by Barsacchi et al.[17] who found a decrease of a-tocopherol concentrationunder conditions of ischemia and reoxygenation. However,the decrease observed in our study was only significant aftersurgery. This time course suggests that it can be the result ofpost-ischemic repair of (membrane) lipid peroxides. Anadded cause can be the depletion of vitamin C during CPB.Since vitamin C is able to regenerate vitamin E from itsradical intermediate, consumption of a-tocopherol is morelikely if vitamin C is depleted [19]. Ballmer et al. have shownthat vitamin C is strongly depleted after CPB [20]. Theseobservations suggest that the oxidative burden during CPBwould, in a first instance, consume vitamin C, together withreduced glutathione, which are the most effective water-soluble non-enzymatic antioxidants under conditions ofoxidative stress. Their ensuing depletion and, as a conse-quence, that of a-tocopherol, may seriously alter the rest ofthe anti-oxidative cascade and result in systemic whole-bodyinflammation which then increases the risk of post-ischemicdamage.
In order to elucidate the relationship between the changesin antioxidant status and the activation of inflammatory cellsduring CABG, we also monitored markers of leukocyteactivation. Evidence of neutrophil activation during ECC hasbeen provided by other authors [4]. In addition, in a previousstudy performed at our institution by Jorens et al. [21], IL-8response was monitored and found to be significantlyincreased during CPB, returning to normal values 20 h post-operative. In the present study we found a peri-operativeincrease in serum eosinophil cationic protein (ECP) andtryptase levels. This suggests that both eosinophils and mastcells were activated during or after CABG and points out to apossible anaphylactoid reaction. Nevertheless, ECP release isnot only a sign of eosinophil activation as it is supposed to betransported by neutrophils [22]. Moreover, despite the factthat ECP is of eosinophilic origin, in some studies in asthmapatients no relationship was found between eosinophilnumber and ECP levels in sputum [23]. This observationsuggests that the ECP sputum concentrations are not merely afunction of the eosinophil numbers but could also be anindirect marker of neutrophil activation.
With regard to the activation of mast cells during CABG,several underlying mechanisms could explain this obser-vation. Mast cells are heavily granulated wandering cellsfound in connective tissue and are abundant beneathepithelial surfaces. The release of their granule content(heparin, histamine and many proteases such as tryptase)can be triggered by physical factors (mechanical trauma,changes in temperature), toxins, endogenous mediators(proteins, tissue proteases) and immune mechanisms (IgEdependent and independent). Also complement activation
can cause mast cell degranulation (anaphylotoxins C5a, C3aand C4a are formed during complement activation) [24]. Allthese processes can occur during the ischemia-reperfusionand ECC of the CPB procedure and can, moreover, be linkedto the oxidative activity. For example, activation of C5areceptors on mast cells during CPB may trigger degranula-tion. Furthermore, tryptase released from mast cells canfurther stimulate the release of IL-8 and up-regulate ICAM-1on epithelial cells [24]. Based on these facts, the activationof mast cells during CPB is not necessarily a sign of allergybut could just be a consequence of complement activation.There is also a growing body of evidence that mast cells areactivated during ischemia-reperfusion. The increased influxof oxidants occurring at the onset of reperfusion may thusalso be responsible for mast cell activation [25]. It hasalready been reported that superoxide is known to activatethese cells [26] which in turn play a role in neutrophilactivation and infiltration into the lung [27], thus, in theirturn, further aggravating the release of ROS.
In summary, this study, performed in a small number ofselected patients, showed that there was a strong innateantioxidant response under the conditions of acuteoxidative stress occurring during CABG. However, it iswell documented that post-ischemic oxidative damage stilloccurs. This indicates that this antioxidant response is notsufficient to counteract the heavy oxidant burden of thesesurgical procedures. It would be interesting to investigatewhether supplementation with antioxidant mixtures suchas vitamin C plus glutathione could, in a first instance,prevent their depletion during CPB, and, in a secondinstance, suppress the post-ischemic inflammatoryresponse.
This study also showed that there was a significant andparallel release of markers of anaphylaxis. The role playedherein by mast cell and eosinophil activation needs furtherinvestigation. The information collected in such studies willaid in the search for effective systemic measures to preventpost-ischemic damage and thus ensure a better outcome forpatients undergoing cardiac surgery.
References
[1] Wan S, LeClerc JL, Vincent JL. Inflammatory response to cardiopulmon-ary bypass: mechnism involved and possible therapeutic strategies.Chest 1997;112:676–92.
[2] Gerritsen WBM, van Boven WJP, Driessen AHG, Haas FJLM, Aarts LPHJ.Off-pump versus on-pump coronary artery bypass grafting: oxidativestress and renal function. Eur J Cardiothorac Surg 2001;20:923–9.
[3] Elgebaly SA, Houser SL, el Kerm AF, Doyle K, Gilles C, Galecki K.Evidence of cardiac inflammation after open heart operations. AnnThorac Surg 1994;57:391–6.
[4] Wachtfogel YT, Kucich U, Greenplate J, Gluszko P, Abrams W,Weinbaum G, Wenger RK, Rucinski B, Niewiarowski S, Edmunds Jr LH.Human neutrophil degranulation during extracorporeal circulation.Blood 1987;69:324–30.
[5] Biglioli P, Cannata A, Alamanni F, Naliato M, Porqueddu M, Zanobini M,Tremoli E, Parolari A. Biological effects of off-pump vs. on-pumpcoronary artery surgery: focus on inflammation, hemostasis andoxidative stress. Eur J Cardiothorac Surg 2003;24:260–9.
[6] Davies SW, Duffy JP, Wickens DG, Underwood SM, Hill A, Alladine MF,Feneck RO, Dormandy TL, Walesby RK. Time-course of free radicalactivity during coronary artery operations with cardiopulmonary bypass.J Thorac Cardiovasc Surg 1993;105:979–87.

C.R. Luyten et al. / European Journal of Cardio-thoracic Surgery 27 (2005) 611–616616
[7] Dhalla NS, Elmoselhi AB, Hata T, Makino N. Status of myocardialantioxidantsin ischemia-reperfusion injury. Cardiovasc Res 2000;47:446–56.
[8] Pyles LA, Fortney JE, Kudlak JJ, Gustafson RA, Einzig S. Plasmaantioxidants depletion after cardiopulmonary bypass in operationsfor congenital heart disease. J Thorac Cardiovasc Surg 1995;110:165–71.
[9] Toivonen HJ, Ahotupa M. Free radical reaction products and antioxidantcapacity in arterial plasma during coronary artery bypass grafting.J Thorac Cardiovasc Surg 1994;108:140–1.
[10] De Backer WA, Amsel B, Jorens PG, Van Damme J, van Overveld FJ,Bossaert L, Walter P, Herman AG, Rampart M. N-acetylcysteinepretreatment of cardiac surgery patients influences plasma neutrophilelastase and neutrophil influx in bronchoalveolar lavage fluid. IntensiveCare Med 1996;22:900–8.
[11] Yusuf S, Dagenais G, Pogue J, Bosch J, Sleigh P. Vitamin E supplemen-tation and cardiovascular events in high-risk patients. The HeartOutcomes Prevention Evaluation Study Investigators. N Engl J Med2000;342:154–60.
[12] Li JM, Shah AM. Endothelial cell superoxide generation: regulation andrelevance for cardiovascular pathophysiology. Am J Physiol Regul IntegrComp Physiol 2004;287:R1014–R30.
[13] Arduini A, Mezzet A, Porecca E, Lapenna D, DeJulia J, Marzio L,Polidoro G, Cuccurullo F. Effect of ischemia reperfusion on antioxidantenzymes and mitochondrial inner membraneproteins in perfused ratheart. Biochim Biophys Acta 1988;970:113–21.
[14] Van Jaarsveld H, Groenewald AJ, Potgieter GM, Barnard SP,Vermaak WJ, Barnard HC. Effect of nrmothermic ischemic cardiac arrestand of reperfusion on the free oxygen radical scavenger enzymes andxanthine oxidase. Enzyme 1988;39:8–16.
[15] Inal M, Alatas O, Kanbak G, Akyuz F, Sevin B. Changes of antioxidantenzyme activities during cardiopulmonary bypass. J Cardiovasc Surg1999;373–6.
[16] Yau TM, Weisel RD, Mickle DA, Burton GW, Ingold KU, Ivanov J,Mohabeer MK, Tumiati L, Carson S. Vitamin E for coronary bypassoperations. J Thorac Cardiovasc Surg 1994;108:302–10.
[17] Barsacchi R, Pelosi G, Maffei S, Baroni M, Salvatore L, Ursini F,
Verunelli F, Biagini A. Myocardial vitamin E is consumed during
cardiopulmonary bypass: indirect evidence of free radical generation
in human ischemic heart. Int J Cardiol 1992;37:339–43.
[18] Schindler R, Berndt S, Schroeder P, Oster O, Rave G, Sievers HH. Plasma
vitamin E and A changes during cardiopulmonary bypass and in the
postoperative course. Langenbeck’s Arch Surg 2003;387:372–8.
[19] May JM, Qu Zc, Mendiratta S. Protection and recycling of [alpha]-
Tocopherol in human erythrocytes by intracellular ascorbic acid. Arch
Biochem Biophys 1998;349:281–9.
[20] Ballmer PE, Reinhart WH, Jordan P, Buhler M, Moser UK, Gey KF.
Depletion of plasma vit C but not of vit E in response to cardiac
operations. J Thorac Cardiovasc Surg 1994;108:311–20.
[21] Jorens PG, De Jongh RF, De Backer WA, Van Damme J, van
Overveld FJ, Bossaert L, Walter P, Herman AG, Rampart M. Inter-
leukin-8 production in patients undergoing cardiopulmonary bypass.
The influence of pre-treatment with methylprednisolone. Am Rev
Respir Dis 1993;148:890–5.
[22] Bystrom J, Garcia RC, Hakansson L, Karawajczyk M, Moberg L,
Soukka J, Venge P. Eosinophil cationic protein is stored in, but not
produced by, peripheral blood neutrophils. Clin Exp Allergy 2002;32:
1082–91.
[23] Virchow Jr JC, Kroegel C, Hage U, Kortsik C, Matthys H, Werner P.
Comparison of sputum-ECP levels in bronchial asthma and chronic
bronchitis. Allergy 1993;48:112–8.
[24] Payne V, Kam PCA. Mast cell tryptase: a review of its physiology and
clinical significance. Anaesthesia 2004;59:695–703.
[25] Blum H, Summers JJ, Schnall MD, Barlow C, Leigh Jr JS, Chance B,
Buzby GP. Acute intestinal ischemia studies by phosphorus nuclear
magnetic resonance spectroscopy. Ann Surg 1986;204:83–8.
[26] Kubes P, Kanwar S, Niu XF, Gaboury JP. Nitric oxide synthesis inhibition
induces leukocyte adhesion via superoxide and mast cells. Fed Am Soc
Exp Biol J 1993;7:1293–9.
[27] Kubes P, Granger DN. Leukocyte-endothelial cell interactions evoked by
mast cells. Cardiovasc Res 1996;32:699–708.