QUS Defence
14
MSc. Research Dissertation DefenceSEA060L414Y MSc. Research Dissertation Defence of work SEA060L414Y Richard Brennan BRE11333662 Richard Brennan BRE11333662
-
Upload
sportscienceconsultants -
Category
Documents
-
view
0 -
download
0
Transcript of QUS Defence

MSc. Research Dissertation DefenceSEA060L414Y
MSc. Research Dissertation
Defence of work SEA060L414Y
Richard BrennanBRE11333662
Richard Brennan BRE11333662

MSc. Research Dissertation DefenceSEA060L414Y
Using Quantitative Ultrasound (QUS) measurements of thecalcaneus to predict vertebral bone mineral density (BMD) and
fracture risk.
Quantitative Ultrasound
Quantitative Ultrasound (QUS) is used to identify changes in bone tissue bought about by aging, menopause and osteoporosis as well as changes in activity levels and nutrition. Measurements of Broadband Ultrasound Attenuation (BUA) and Speed of Sound (SOS) can provide clinicians and researchers with information that can be used to determine fracture risk, monitor skeletal changes and the efficacy of treatments and interventions and, also, as a basis for comparison with normative data from a given population.
Fig. 1: Brandi, M. (2009) Microarchitecture, the key to bone quality. Rheumatology. 48, iv3-iv8.
A mechanical wave is passed through the bone with a frequency between 20 kHz-150MHz. The shape, intensity and speed of the wave are altered by the physical and mechanical properties of the bone. The velocity and attenuation of the wave are measured in metres per second (m/s) and decibels per megahertz(dB/Mhz) respectively. The values measured are dependent on the bone mineral content (BMC), microstructure and elasticity
Richard Brennan BRE11333662
Normal bone:Trabecular architecture
Osteoporotic bone:Trabecular architecture
MSc. Research Dissertation DefenceSEA060L414Y
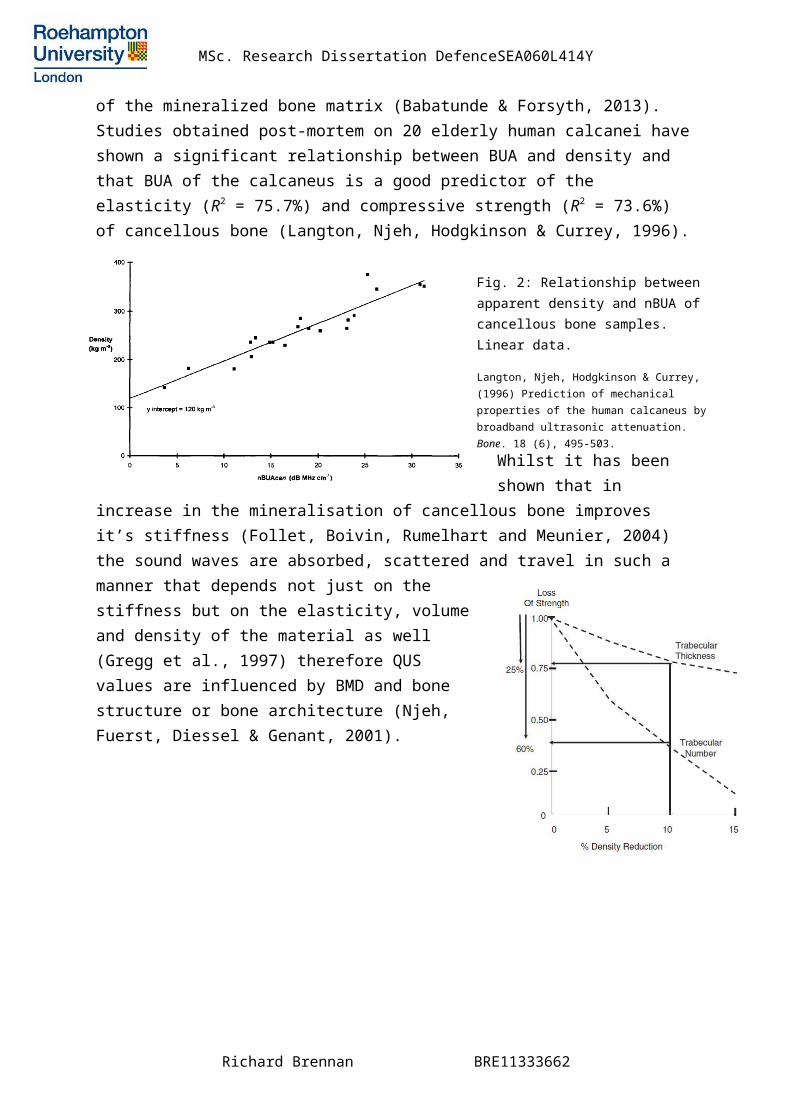
of the mineralized bone matrix (Babatunde & Forsyth, 2013). Studies obtained post-mortem on 20 elderly human calcanei haveshown a significant relationship between BUA and density and that BUA of the calcaneus is a good predictor of the elasticity (R2 = 75.7%) and compressive strength (R2 = 73.6%) of cancellous bone (Langton, Njeh, Hodgkinson & Currey, 1996).
Whilst it has been shown that in
increase in the mineralisation of cancellous bone improves it’s stiffness (Follet, Boivin, Rumelhart and Meunier, 2004) the sound waves are absorbed, scattered and travel in such a manner that depends not just on thestiffness but on the elasticity, volumeand density of the material as well(Gregg et al., 1997) therefore QUSvalues are influenced by BMD and bonestructure or bone architecture (Njeh,Fuerst, Diessel & Genant, 2001).
Richard Brennan BRE11333662
Fig. 2: Relationship between apparent density and nBUA of cancellous bone samples. Linear data.
Langton, Njeh, Hodgkinson & Currey, (1996) Prediction of mechanical properties of the human calcaneus bybroadband ultrasonic attenuation. Bone. 18 (6), 495-503.

MSc. Research Dissertation DefenceSEA060L414Y
QUS and Precision
Graafmans, Lingen, Ooms, Bezemer & Lips (1996) studied the precision of QUS measurements of the calcaneus and found that no significant differences between readings of BUA and SOS in short-term (5 consecutive measurements in 1 hour) and long-term (6 within 6 months) measurements. They also found that QUS measurements of the calcaneus correlated well with BMD at the same site.
It is recommended that a manufacturer supplied ‘phantom’ is used as a diagnostic tool prior to measuring in order to checkcorrect function of the scanning device. The probes should also be clean, the foot being scanned should be still and in exactly the same position on each subsequent occasion and ultrasound gel should be used taking care to remove any remaining old gel beforehand. Ambient temperature should also be taken and ideally be the same for subsequent measurements (Guglielmi & de Terlizzi, 2009).
Frost, Blake & Fogelman (1999) examined the precision of QUS in a study consisting of 422 healthy women with no risk factors associated with osteoporosis and 93 women with one or more vertebral fractures. They suggested that changes in the mechanical loading of the calcaneus may be due to a change in dynamic posture bought about by the pain associated with vertebral fractures. They also suggested that bone structure would change due to immobility.
BUA measurements can be positively affected by certain activities. Jones, Hardman, Hudson & Norgan (1991) have shown that brisk walking increases BUA at the calcaneus through the osteogenic effect of the heel-strike which causes strain related remodeling.
QUS measurements at the calcaneus are commonly taken in the mediolateral direction along the transverse axes. This method
Richard Brennan BRE11333662

MSc. Research Dissertation DefenceSEA060L414Y
shows good correlations between all ultrasonic measurements and BMD (Nicholson et al., 1998).
Applications of QUS
QUS appears to perform similarly in men and women (Moayyeri etal., 2012) and is at least comparable to DXA in the predictionof fractures in the elderly (Moayyeri et al., 2009). Lifestylefactors such as physical activity, alcohol consumption and smoking can affect QUS measurements (Pye et al., 2010) and modification of these factors may help reduce the risk of fracture (Pye et al., 2010). A review of cross-sectional studies suggests that lower QUS values are related to an increased risk of fractures and low bone mass (Gregg et al., 1997) and the EPIC-Norfolk study of 14,824 men and women aged 42-82 years showed that quantitative calcaneum ultrasound predicts total and hip fracture risk in men and women (Khaw, Reeve, Luben, Bingham, Welch, et al., 2004).
Unlike DXA QUS does not measure Bone Mineral Density (BMD) directly however QUS can provide indirect information on BMD as well as more direct information on bone micro-architecture.Bone micro-architecture (trabecular number, connectivity and orientation) is an important component of bone quality and therefore bone strength. Recent studies have looked at combining Trabecular Bone Score (TBS) with BMD in order to ascertain fracture risk (Roux, Wegryzn, Boutroy, Bouxsein, Hans & Chapurlat, 2013; Hans, Goertzen, Krieg & Leslie, 2011) because BMD alone cannot provide sufficient information to determine bone quality. An increase in BMD may not necessarilyresult in an improvement in bone strength as the improved areamay be the discontinuous end of a bony trabeculum as opposed to strengthening a joined trabecular structure (Khan et al.,
2001).
Richard Brennan BRE11333662E., Chappard, D., Pascaretti, C., DuQuenne, M., Krebs, S. Rohmer, V. & Basle, M. (2000) Trabecular Bone Microarchitecture, Bone Mineral Density and Vertebral Fractures in Male Osteoporosis.
Fig.3: When BMD alone is not enough, the combinationof BMD + TBS enables to identify patients with high risk of fracture likely to have fractures whereas the patients are in theosteopenic zone
MSc. Research Dissertation DefenceSEA060L414Y
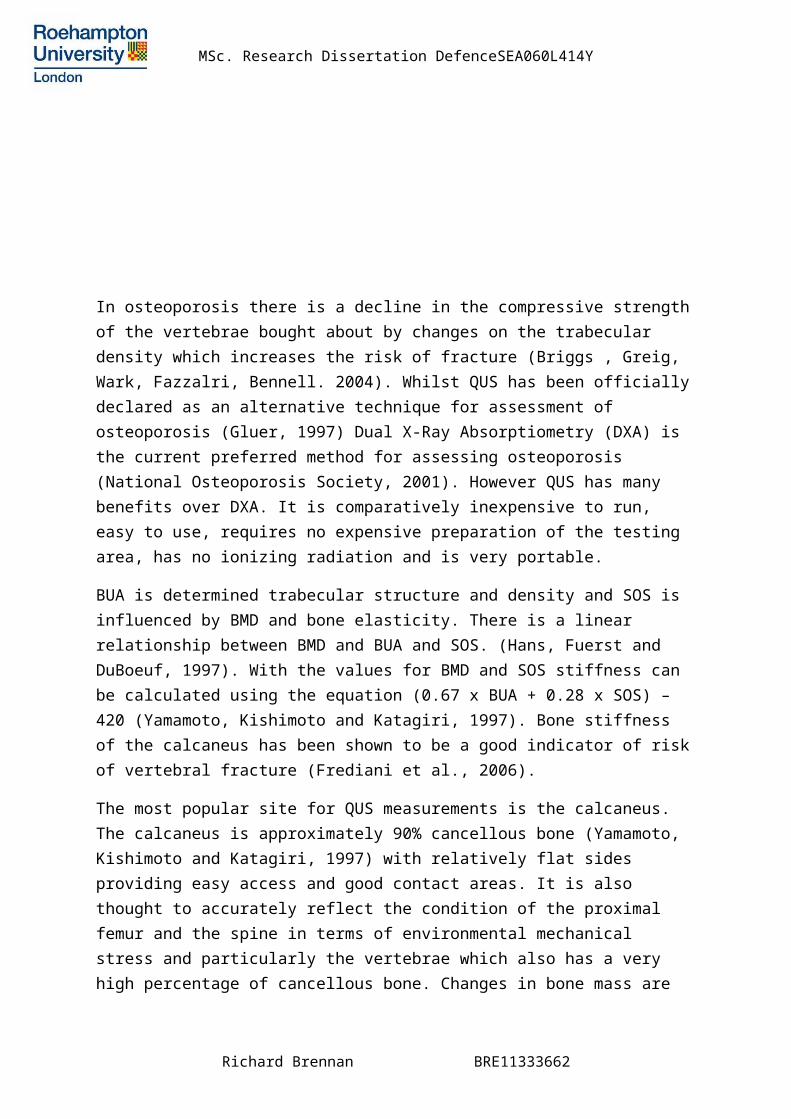
In osteoporosis there is a decline in the compressive strengthof the vertebrae bought about by changes on the trabecular density which increases the risk of fracture (Briggs , Greig, Wark, Fazzalri, Bennell. 2004). Whilst QUS has been officiallydeclared as an alternative technique for assessment of osteoporosis (Gluer, 1997) Dual X-Ray Absorptiometry (DXA) is the current preferred method for assessing osteoporosis (National Osteoporosis Society, 2001). However QUS has many benefits over DXA. It is comparatively inexpensive to run, easy to use, requires no expensive preparation of the testing area, has no ionizing radiation and is very portable.
BUA is determined trabecular structure and density and SOS is influenced by BMD and bone elasticity. There is a linear relationship between BMD and BUA and SOS. (Hans, Fuerst and DuBoeuf, 1997). With the values for BMD and SOS stiffness can be calculated using the equation (0.67 x BUA + 0.28 x SOS) – 420 (Yamamoto, Kishimoto and Katagiri, 1997). Bone stiffness of the calcaneus has been shown to be a good indicator of riskof vertebral fracture (Frediani et al., 2006).
The most popular site for QUS measurements is the calcaneus. The calcaneus is approximately 90% cancellous bone (Yamamoto, Kishimoto and Katagiri, 1997) with relatively flat sides providing easy access and good contact areas. It is also thought to accurately reflect the condition of the proximal femur and the spine in terms of environmental mechanical stress and particularly the vertebrae which also has a very high percentage of cancellous bone. Changes in bone mass are
Richard Brennan BRE11333662
E., Chappard, D., Pascaretti, C., DuQuenne, M., Krebs, S. Rohmer, V. & Basle, M. (2000) Trabecular Bone Microarchitecture, Bone Mineral Density and Vertebral Fractures in Male Osteoporosis.
MSc. Research Dissertation DefenceSEA060L414Y
greater and occur earlier in trabecular bone than in bones that are primarily corticol.
QUS and Bone Mineral Density
BMD measurements are used to assess osteoporosis. A reduction in BMD of 1 SD of the population is associated with 2-4 times higher fracture risk. However decreased BMD is only one of several factors influencing bone fragility. (Hans, Fuerst and DuBoeuf, 1997). Changes in bone quality, which QUS measures, are stronger predictors of fracture risk than clinical risk factors (National Osteoporosis Society, 2001). In a study of 654 women Yamamoto, Kishimoto and Katagiri (1997) demonstratedthat QUS measurements were more sensitive than BMD in diagnosing vertebral fracture and for evaluating fracture risk. 89 women (14.7%) had vertebral fracture 42 (9.3%) of the451 healthy women and 47 (23.2%) of the osteoporotic women). In the osteoporotic group QUS values decreased after 1 year even though BMD had increased suggesting QUS parameters represent bone properties other than BMD. An increase in BMD may not always be accompanied by an increase in bone strength.In a study of 91 female subjects (aged 56.9 + 9.6 years) 30 categorised as normal, 38 oseopenic and 23 osteoporotic Langton & Langton (2000) found that QUS calcaneal measurementsand BMD as measured by DXA were comparable in their discriminatory ability to identify osteoporotic or osteopenic subjects.
QUS and Bone Micro-Architecture
Gonnelli S, Cepollaro C, Agnusdei D, Palmieri R, Rossi S, Gennari C. (1995) Found that SOS, BUA and Stiffness were all independent predictors of fracture risk. Cheng et al. (1997) took spinal BMD measurements using DXA and QCT and calcaneal measurements using DXA and QUS of 62 adult cadavers and found calcaneal DXA, BMD, bone velocity and BUA correlated well witheach other (r2 – 0.67-0.76) but less so when compared with DXA and QCT measurements of the vertebra. Their data also suggested that about 40% of the variability of vertebral
Richard Brennan BRE11333662
MSc. Research Dissertation DefenceSEA060L414Y
strength is unaccounted for by BMD measurements. They concluded that ultrasound measurements of the calcaneus may reflect more fracture risk than bone fragility.
Nicholson and Alkalay (2007) also found the predictive performance of QUS measurements of vertebral bodies comparableto or greater than BMD when predicting vertebral failure load.Mezaros et al. (2007) have reached a more specific conclusion.Their results suggest that BUA values are closely related to BMD but that SOS values are able to predict fractures. They found no connection between BUA and vertebral fracture risk but a strong positive association between SOS and vertebral fracture risk. SOS is thought to be influenced by mineral density and the elastic characteristics of bone and BUA is thought to be influenced by the structural characteristics of bone and by bone mass (Mezaros, et al. 2007).
In a study of 463 women aged 20-39 and 2,374 women aged 55-79 Gluer et al., (2004) found that QUS of the calcaneus worked aswell as central DXA for identification of women at high risk for prevalent osteoporotic vertebral fractures. Mariconda et al., 2004 studied 117 patients with low back pain and found that evidence of degenerative changes and stenosis in the lumbar spine correlated with ultrasonographic parameters (SOS and stiffness) of the calcaneus, p = 0.019 for SOS and p = 0.039 for stiffness.
Pluijm, Graafmans, Bouter & Lips, (1999) studied 132 men and 578 women aged 70 years and older (mean age + SD: 82.8 + 5.9) over a 1 year period and found that low BUA values and immobility were the strongest predictors of hip fracture as well as any other fracture including pelvic and femoral fractures.
QUS can provide information on the ‘non-mass’ characteristics of bone. In a study of 108 men LeGrand et al., (2000) found that bone trabecular micro-architecture is a major determinantof vertebral fractures in middle-aged men with severe osteopenia. They concluded that the biomechanical competence
Richard Brennan BRE11333662
MSc. Research Dissertation DefenceSEA060L414Y
of bone is not dependent on BMD alone but also its three-dimensional configuration. A meta-analysis by Marin, Gonzalez-Macias, Diez-perez, Palm & Delgado-Rodriguez (2006) found thatthe values of the parameters measured by QUS at the calcaneus are lower in women with a history of osteoporotic fracture regardless of the BMD values determined by DXA.
QUS and Vertebral Fracture
Since a significant proportion of vertebral fractures are asymptomatic (Mezaros et al., 2007) QUS measurements could be an easy to use, inexpensive and quick method to better distinguish between those who are more likely to benefit from a more expensive DXA or QCT scan. A low QUS reading may also highlight those who are asymptomatic but who could be suffering from a vertebral fracture or who are more at risk ofsuffering any fracture including a vertebral one and this would allow better targeting of preventative care. Frost, Blake & Fogelman (1999) found that contact ultrasound can detect age and menopause related changes in bone status in women and that it can also distinguish between healthy women and women with a vertebral fracture.
QUS measurements of the calcaneus have been shown to predict the risk of hip and non-spine fracture in men (Bauer et al., 2007) and predict risk of vertebral fracture in postmenopausalwomen in vivo (Bauer, Gluer, Genant & Stone, 1995) although one study has shown that QUS measurements of the calcaneus in vitro are poor predictors of vertebral strength (Cheng et al, 1997).In a study of 566 postmenopausal women (mean age 74 + 5) QUS measurements of the calcaneus have been shown to predict vertebral deformity and that spine BMD measurements provided no additional information (Ross, Huang, Imose, yates, Vogel & Wasnich, 1995). In a retrospective, cross-sectional study looking specifically at the relationship between calcaneal ultrasonometry and vertebral fracture risk Frediani et al., (2006) selected 764 post-menopausal women with non-traumatic
Richard Brennan BRE11333662
MSc. Research Dissertation DefenceSEA060L414Y
vertebral fractures and 770 women with normal morphometry as acontrol group and found that QUS stiffness measurements of thecalcaneus were valid and reliable predictors of vertebral fracture even when correcting for confounding factors such as age, weight, height and years since menopause and they concluded that QUS of the calcaneus is an excellent substitutefor BMD of the axial skeleton by DXA. Huopio et al., (2004) found that calcaneal QUS is able to predict early postmenopausal fractures as well as or even better than axial BMD. They found a 1SD decrease in BUA values increased the risk of future fracture by 43% equalling the risk of 1SD decrease in spinal BMD however only QUS measurements were ableto predict risk of fracture when allowing for confounding variables.
Conclusion
QUS measurements of BUA and SOS at the calcaneus can provide useful information on bone quality of the calcaneus. Research shows that these measurements can help predict total fracture risk including hip and vertebral fracture risk in men and pre and postmenopausal women. QUS measurement of the calcaneus is a relatively inexpensive, portable, easy to use and quick to administer test that requires no special environmental adaptations since there is no ionizing radiation. Measuring bone quality may be an adequate if not better substitute for measuring BMD. QUS measurements may help to identify those at risk of fracture without incurring significant costs.
References
Babatunde, O., Forsyth, J. (2013). Quantitative ultrasound and bone’s response to exercise: A meta-analysis. Bone. 311-318.
Bauer, D., Ewing, S., Cauley, J., Ensrud, K., Cummings, S. & Orwoll, E. (2007). Quantitative ultrasound predicts hip and non-spine fracture in men:the MrOS study. Osteoporosis International. 18, 771-777.
Bradi, M. (2009). Microarchitechture, the key to bone quality. (2009). Rheumatology. 48, iv3-iv8.
Richard Brennan BRE11333662
MSc. Research Dissertation DefenceSEA060L414Y
Briggs, A., Grieg, A., Wark, J., Fazzalari, N. & Bennell, K. (2004). A review of anatomical and mechanical factors affecting vertebral body integrity. International Journal of Medical Sciences. 1, 170-180.
Cheng, X., Nicholson, P., Boonen, S., Lowet, G., Brys, P., Aerssens, J., Van Der Perre, G. & DeQueker, J. (1997). Prediction of vertebral strength in vitro by spinal bone densitometry and calcaneal ultrasound. Journal of Bone and Mineral Research. 12 (10), 1721-1728.
Follet, H., Boivin, G., Rumelhart, C. & Meunier, P. (2004). The degree of mineralization is a determinant of bone strength: A study on human calcanei. Bone. 783-789.
Frediani, B., Acciai, C., Falsetti, P., Baldi, F., Filippou, G., Siagkri, C., Spreafico, A., Galeazzi, M. & Marcolongo, R. (2006). Calcaneus ultrasonometry and dual-energy x-ray absorptiometry for the evaluation of vertebral fracture risk. Calcified Tissue International. 79, 223-229.
Frost, M., Blake, G. & Fogelman, I. (1999). Contact quantitative ultrasound: An evaluation of precision, fracture discrimination, age-related bone loss and applicability of the WHO criteria. Osteoporosis International. 10, 441-449.
Gluer, C. (1997). Quantitative ultrasound techniques for the assessment of osteoporosis: Expert agreement on current status. Journal of Bone and Mineral Research. 12 (8), 1280-1288.
Gluer, C. et al. (2004). Association of five quantitative ultrasound devices and bone densitometry with osteoporotic vertebral fractures in a population-based sample: The Opus Study. Journal of Bone and Mineral Research. 19 (5), 782-793.
Graafmans, W., Lingen, A., Ooms, M., Bezemer, P. & Lips, P. (1996). Ultrasound measurements of the calcaneus: precision and its relation with bone mineral density of the heel, hip and lumbar spine. Bone. 19 (2), 97-100.
Gonnelli, S., Cepollaro, C., Agnusdei, D., Palmier,i R., Rossi, S. & Gennari, C. (1995). Diagnostic value of ultrasound analysis and bone densitometry as predictors of vertebral deformity in postmenopausal women. Osteoporosis International. 5(6), 413-418.
Gregg, E., Kriska, A., Salamone, L., Roberts, M., Anderson, S., Ferrell, R., Kuller, L. & Cauley, J. (1997). The epidemiology of quantitative ultrasound: a review of the relationships with bone mass, osteoporosis and fracture risk. Osteoporosis International. 7, 89-99.
Richard Brennan BRE11333662
MSc. Research Dissertation DefenceSEA060L414Y
Guglielmi, G. & Terlizzi, F. (2009). Quantitative ultrasound in the assessment of osteoporosis. European Journal of Radiology. 71, 425-431.
Hans, D., Arlot. M., Schott, A., Roux, J., Kotzki, P. & Meunier, P. (1995).Do ultrasound measurements on the Os Calcis reflect more the bone architechture than the bone mass? A two-dimensional histomorphometric study. Bone. 16 (3), 295-300.
Hans, D., Fuerst, T. & DuBoeuf, F. (1997). Quantitative ultrasound measurement. European Radiology. 7 (Suppl. 2), S43-S50.
Hans, D., Goertzen, A., Kreig, M. & Leslie, W. (2011). Bone microarchitechture assessed by TBS predicts osteoporotic fractures independent of bone density: The Manitoba Study. Journal of Bone and Mineral
Huopio, J., Kroger, H., Honkanen, R., Jurvelin, J., Saarikoski, S. & Alhava, E. (2004) Calcaneal ultrasound predicts early postmenopausal fractures as well as axial BMD. A prospective study of 422 women. Osteoporosis International. 15, 190-195.
Jones, P., Hardman, A., Hudson, A. & Norgan, N. (1991) Influence of brisk walking on the broadband ultrasound attenuation of the calcaneus in previously sedentary women aged 30-61 years. Calcified Tissue International. 49, 112-115.
Khaw, K., Reeve, J., Luben, R., Bingham, S., Welch, A., Wareham, N. Oakes, S. Day, N. (2004). Prediction of total and hip fracture risk in men and women by quantitative ultrasound of the calcaneus: EPIC-Norfolk prospectivepopulation study. The Lancet. 363, 197-202.
Langton, C. & Langton, D. (2000). Comparison of bone mineral density and quantitative ultrasound of the calcaneus: a site-matched correlation and discrimination of axial BMD status. The British Journal of Radiology. 73, 31-35.
Langton, C. & Njeh, C. (2008). The measurement of broadband ultrasonic attenuation in cancellous bone – a review of the science and technology. IEEE Transactions on Ultrasonics, Ferroelectrics and Frequency Control. 55 (7), 1546-1554.
Langton, C., Njeh, C., Hodgskinson, R. & Currey, J. (1996). Prediction of mechanical properties of the human calcaneus by broadband ultrasonic attenuation. Bone. 18 (6), 495-503.
LeGrand, E. , Chappard, D., et al., (2000). Trabecular Bone Microarchitecture, Bone Mineral Density, and Vertebral Fractures in Male Osteoporosis. Journal of Bone and Mineral Research. 15 (1), 13-19.
Richard Brennan BRE11333662

MSc. Research Dissertation DefenceSEA060L414Y
Mariconda, M., Lotti, G., Fava, R., Midolo, R., Longo, C. & Milano, C. (2004). Quantitative ultrasound measurements of the calcaneus in the prediction of lumbar spine degeneration. European Spine Journal. 13, 346-353.
Marin, F., Gonzalez-Macias, J., Diez-Perez, A., Palma, S. & Delgado-Rodriguez, M. (2006). Relationship between bone quantitative ultrasound andfractures: A meta-analysis. Journal of Bone and Mineral Research. 21 (7), 1126-1135.
Moayyeri, A., Adams, J., Adler, R., Krieg, M., Hans, D., Compston, J. & Lewiecki, E. (2012). Quantitative ultrasound of the heel and fracture risk assessment: an updated meta-analysis. Osteoporosis International. 23, 143-153.
Moayyeri, A., Kaptoge, S., Dalzell, N., Bingham, S., Luben, R., Wareham, N., Reeve, J. & Khaw, K. (2009). Is QUS or DXA better for predicting the 10-year absolute risk of fracture? Journal of Bone and Mineral Research. 24 (7), 1319-1325.
Nicholson, P. & Alkalay, R. (2006). Quantitative ultrasound predicts bone mineral density and failure load in human lumbar vertebrae. Clinical Biomechanics. 22, 622-629.
Nicholson, P., Muller, R., Lowet, G., Cheng, X., Hilderbrand, T., Ruegsegger, P., Van Der Perre, G., DeQueker, J. & Boonen, S. (1998). Do quantitative ultrasound measurements reflect structure independently of density in human vertebral cancellous bone? Bone. 23 (5), 425-431.
Njeh, C., Fuerst, T., Diessel, E. & Genant, H. (2001). Is quantitative ultrasound dependent on bone structure? A reflection. Osteoporosis International.(2001). 12, 1-5.
Pluijm, S., Graafmans, W., Bouter, L. & Lips, P. (1999). Ultrasound measurements for the prediction of osteoporotic fractures in elderly people. Osteoporosis International. 9, 550-556.
Pye, S., et al. (2010). Influence of lifestyle factors on quantitative heelultrasound measurements in middle-aged and elderly men. Calcified Tissue International. 86, 211-219.
Ross, P., Huang, C., Davis, J., Imose, K., Yates, J., Vogel, J. & Wasnich, R. (1995). Predicting vertebral deformity using bone densitometry at various skeletal sites can calcaneus ultrasound. Bone. 16 (3). 325-332.
Seeman, E. (2008). Bone quality: The material and structural basis of bone strength. Journal of Bone and Mineral Metabolism. 26, 1-8.
Yamamoto, A., Kishimoto, H. & Katagiri, H. (1997). Clinical and experimental studies of quantitative ultrasound measurement in the os
Richard Brennan BRE11333662

MSc. Research Dissertation DefenceSEA060L414Y
calcis: Prevalence and incidence of vertebral fracture. Journal of Orthopaedic Science. 2, 64-74.
Richard Brennan BRE11333662